
Submitted:
03 September 2025
Posted:
03 September 2025
You are already at the latest version
Abstract
Background: Combination checkpoint inhibitor therapy with ipilimumab plus nivolumab has significantly improved the treatment of patients with metastatic melanoma. This regimen has induced durable complete remissions and improved survival. However, these benefits are associated with a high risk of immune-related side effects. We evaluated the usefulness of potential prognostic biomarkers as predictors of eventual treatment benefit. Methods: A retrospective chart review was conducted of all metastatic melanoma patients treated by a single oncologist with ipilimumab plus nivolumab for advanced cutaneous or subungual melanoma. Baseline biomarkers including BRAF mutation status, serum lactate dehydrogenase levels, PD-L1 expression, and tumor mutation burden were correlated with progression-free survival (PFS). Results: Treatment outcomes were analyzed in 54 sequential patients. BRAF mutation status did not correlate with PFS. Only rare patients presented with an elevated lactate dehydrogenase (LDH); thus, this marker did not prove informative. There was a strong correlation of increased PD-L1 expression with treatment response, and an independent correlation of tumor mutation burden with prolonged PFS. An exploratory analysis suggested that the combination of low tumor cell PD-L1 expression and a low tumor mutation burden predicted a very poor immunotherapy response. Conclusions: Tumor mutation burden and PD-L1 represent potential prognostic biomarkers for response to combination CKI therapy, while LDH and BRAF offer limited prognostic value. Further work will be needed to develop a predictive nomogram to better aid in predicting potential treatment benefit.
Keywords:
PD-1 ligand
; tumor mutation burden
; cancer immunotherapy
; checkpoint inhibitor
; malignant melanoma
1. Introduction
Melanoma is an aggressive form of skin cancer that has been steadily increasing in incidence in many parts of the world. From 2015 to 2019, the number of individuals who developed melanoma increased by 2-3% annually in the United States (US) [1]. It has, therefore, been estimated that over 100,000 new cases of invasive melanoma will occur in the US in 2025, resulting in more than 8,000 deaths [1]. Fortunately, there has been dramatic progress in the development of more effective melanoma treatments over the past 2 decades, including the discovery of targeted therapy as well immune checkpoint inhibitor (ICI)-based immunotherapy [2]. These treatments have dramatically improved survival of patients with metastatic disease [3]. The recent EA6134 DREAMseq trial firmly established combination immunotherapy as the preferred first line therapy for metastatic melanoma patients, in comparison to initial BRAF-mutation directed targeted therapy [4].
Combination immunotherapy utilizing antibodies directed against the inhibitory immune checkpoints PD-1 (nivolumab) and CTLA-4 (ipilimumab) has been shown to induce a high frequency of objective clinical responses. Dual checkpoint blockade further prolonged progression-free (PFS) and overall survival (OS), compared to single agent immunotherapy. With a median 10 years of follow-up, the combination regimen of nivolumab and ipilimumab achieved a remarkable median OS of 71.9 months [5]. In contrast, the median survival was only 36.9 months following monotherapy with nivolumab and 19.9 months with ipilimumab alone. Overall, 31% of ipilimumab plus nivolumab treated patients achieved a durable complete remission and remained free of any recurrence by the end of the study [5]. Notably, if patients were in remission at 3 years, the ten-year melanoma specific survival was 96% [5].
Even though ipilimumab plus nivolumab treatment improved outcomes for metastatic melanoma patients, this treatment resulted in substantial risks. Combination immunotherapy resulted in grade 3 or greater immune-related adverse effects (irAE) in at least 68.7% of patients [6]. These side effects represent over-activation of the immune system and the development of autoimmunity. Commonly reported immunotherapy side effects include rash, colitis, hepatitis, and pneumonitis, but could possibly affect any other organ system [7]. Most of these acute toxicities proved to be manageable with steroids and other immunosuppressive agents. Acute toxicities eventually improved following discontinuation of treatment [8,9,10]. Unfortunately, there have been recent reports of long-term sequelae, such as endocrinopathy, arthropathy, and potentially accelerated atherosclerotic disease, that need to be considered when planning treatment for patients [11,12].
Given the substantial risk of toxicity, it is important to define potentially responsive subsets of patients, who are the most likely to benefit from ICI therapy. In addition, it would also be helpful to identify poor risk patients, who are unlikely to benefit. A few previously reported biomarkers appeared to correlate with the outcome of melanoma treatment. These predictive biomarkers were generally identified from ICI monotherapy trials. Potential poor-risk markers included gene mutations at the BRAF V600 locus [13,14], elevated serum lactate dehydrogenase (LDH) [15], a low percentage of tumor cells expressing programmed cell death protein 1 ligand (PD-L1) [16], as well as a low tumor mutation burden per megabase genomic DNA (TMB) [17]. It is not clear how useful these predictive biomarkers are, given the expanded utilization of current combination ICI therapy with ipilimumab plus nivolumab.
The purpose of our study, therefore, was to evaluate the utility of these potential biomarkers as predictors of PFS. The current analysis is based on consistent first-line ipilimumab plus nivolumab therapy for metastatic melanoma in a community oncology clinic, delivered by a single medical oncologist.
2. Materials and Methods
2.1. Study Design
We performed a retrospective analysis of potential predictive biomarkers for combination immune checkpoint inhibition (ICI) therapy response. Potential subjects were identified by a computer search of a HIPAA compliant electronic patient care database (iKnowMed G2, McKesson, Houston, TX, US). The database was searched for all patients treated by a single physician (W.S.) with concurrent ipilimumab plus nivolumab between 2016 and 2024. Patients were eligible for analysis if they had unresectable, locally advanced or metastatic cutaneous melanoma (including acral or subungual disease). Patients were excluded if they had uveal, mucosal melanomas, or other cancers treated with combination ICI therapy. Patients who received only one dose of ICI therapy or were receiving 2nd line or later therapy were also excluded. Patients who had received prior adjuvant single-agent ICI therapy for high-risk locoregional melanoma were also eligible for analysis.
2.2. Data Extraction
Each patient’s record was individually accessed. Relevant data was extracted and compiled in a password-protected Excel spreadsheet (Version 16.95 Microsoft Corporation, Redmond, WA, USA). A unique patient identification number was assigned to each patient. Age, primary diagnosis, site of metastases, and genetic mutations were recorded. The ICI treatment regimen, duration of therapy, patient outcome, adverse effects of immunotherapy, and current patient status were noted. Pretreatment tumor cell PD-L1 expression, tumor mutation burden (TMB, expressed as mutations/Mb), and serum LDH (units/l) were also recorded. Following data extraction, patient identifiers were removed. This study design was reviewed by the Western IRB chair and deemed exempt from full board review.
2.3. Treatment Regimens
All patients were assessed for oncogene mutation status by next-gen sequencing (Tempus, Chicago, IL or Foundation Medicine, Cambridge, MA) to identify potentially targetable mutations. Most patients also were assessed for tumor cell PD-L1 expression by immunostaining, generally using the Dako PD-L122C3 monoclonal antibody. Patients were treated with 4 doses of either the standard induction regimen (ipilimumab 3 mg/kg plus nivolumab 1 mg/kg every 3 weeks i.v.) [6], or the alternate regimen (“flipped dose” regimen; ipilimumab 1 mg/kg plus nivolumab 3 mg/kg every 3 weeks I.V.) [18]. After completion of induction therapy, maintenance treatment with a fixed dose of 480 mg nivolumab I.V. monthly was continued in responding patients. Patients who achieved a confirmed complete remission were considered for elective treatment discontinuation following an institutional protocol [19].
2.4. Evaluation of Outcomes
The best objective response (BOR) to therapy at 12 months was utilized to determine individual patient response to treatment based on RECIST 1.1 criteria [20]. A patient achieved a complete response (CR) if they had resolution of all known sites of disease. A partial response (PR) was characterized by an over 30% decrease in the sum of bidimensional measurements of index lesions. Progressive disease (PD) resulted from a greater than 20% increase in the sum of bidimensional tumor dimensions. Patients who did not achieve CR, PR or PD were characterized as having stable disease (SD).
2.5. Statistical Analyses
Descriptive statistics, including range, median, standard deviation, were calculated with the use of the Excel spreadsheet. PFS and OS were calculated from the start of immunotherapy via Kaplan Meier analysis [21]. A log-rank test was used to compare progression-free survival curves [22]. The data of last clinic follow-up, progression or death was used to calculate PFS and OS. Responding patients were censored at the date of last follow-up. The date of the final analysis was November 25th, 2024.
3. Results
3.1. Demographics
A total of 54 patients diagnosed with advanced or metastatic cutaneous melanoma underwent first line therapy ICI therapy with ipilimumab plus nivolumab. There were 51 patients (94.4%) with cutaneous melanoma and 3 patients (5.6%) with acral or subungual melanoma. A total of 34 patients were men (63.0%) and 20 were women (37.0%). The median age at diagnosis was 63 ± 15 years (± standard deviation), with a range from 20 to 92 years. Forty-nine patients were Caucasian (90.7%). There were four Hispanic individuals (7.4%), and one patient of Asian descent (1.9%). Individual descriptions of patient demographics are provided (Supplemental data Table S1).
3.2. Characterization of Potential “Driver” Mutation Profile
Tumor cell expression of non-overlapping “driver” mutations was evaluated by Next Gen sequencing. This testing revealed that 20 patients had a BRAF V600 mutation (37.0%), 14 with a BRAF V600E mutation and 6 with a BRAF V600K mutation. Additionally, 19 patients had RAS mutations (35.2%), and 5 patients had a NF1 mutation (9.3%). Two patients had a C-KIT mutation (3.7%), and eight patients were “quadruple negative” (no BRAF, RAS, NF-1 or C-KIT mutations) (14.8%).
3.3. Treatment Outcome
Of our 54 patients, 18 (33.3%) received the standard treatment regimen of 3 mg/kg ipilimumab and 1 mg/kg nivolumab, while the remaining 36 patients (66.7%) received the alternate (or “flipped”) regimen of ipilimumab plus nivolumab [18]. The PFS of the standard and alternate treatment regimens was not statistically different, so results were pooled for analysis (data not shown). The median potential follow-up of our patients was 48.5 ± 22.6 months. For the entire cohort of patients, median PFS was indeterminate and appeared to plateau after 2 years. At 4 years of follow-up, 51.8% of patients remained progression-free (Figure 1A). The median OS also remained undefined (Figure 1B), with 59.8% of patients alive at 4 years. Individual descriptions of patient outcome are provided (Supplemental data Table S2).
3.4. Analysis of Potential Predictive Markers for Ipilimumab/Nivolumab Response
We evaluated whether commonly utilized risk factors, such as BRAF V600 mutations, serum LDH, PD-L1 expression, and TMB, predicted response to subsequent combination ICI treatment in our patient population.
BRAF mutations are thought to associate with more aggressive clinical behavior of melanoma [14]. We evaluated whether patients with BRAF mutations had adverse clinical outcome following combined ipilimumab plus nivolumab therapy. Subgroup analysis based on BRAF mutation status demonstrated that PFS of patients with BRAF mutations versus those with other “driver” mutations (NRAS, NF-1, C-KIT or quadruple negative) was similar following ipilimumab plus nivolumab treatment (Figure 1C)(p=0.95). There were no detectable differences in OS between groups of patients with and without BRAF mutations (Figure 1D)(p=0.90). In subsequent biomarker analyses, we therefore focused on PFS as a surrogate for long-term outcome.
Elevated pre-treatment serum LDH levels have been proposed to identify patients who are less likely to benefit from ICI therapy [13,15,23]. The pretreatment serum LDH was available for all 54 patients. The median pretreatment LDH level was 187 ± 87 U/L (normal 120-250 U/L). In our patient population, patients presenting with an elevated LDH were infrequent. Only 8 patients (18.5%) exhibited elevated LDH levels (≥ 250 U/L).
We evaluated whether pre-treatment LDH levels correlated with outcome. A scatter plot directly comparing pretreatment LDH with the duration of PFS following treatment is shown (Figure 2A). There was minimal correlation of numerical LDH value and PFS.
Progression-free survival in patients with a normal (n=44) versus an elevated LDH (n=8) was also evaluated by Kaplan-Meier analysis (Figure 2B). Although there was a trend toward inferior outcome in patient with elevated LDH, this did not reach statistical significance (p=0.53), perhaps due to the limited number of patients who presented with an elevated LDH in our clinical practice.
PD-L1 expression on tumor cells has been correlated with immunotherapy response in numerous tumor types, including melanoma [16,24]. PD-L1 testing was not considered standard-of-care over the interval of this study. Thus, PD-L1 tumor proportion scores (TPS) were available for only 42 of our patients (77.8%). Twenty-nine of 42 patients (69.1%) had increased PD-L1 expression (TPS ≥ 1%), while 13 patients (30.9%) had minimal PD-L1 expression (TPS < 1%).
A plot of the percentage of tumor cells expressing PD-L1 showed a modest linear correlation with PFS (Figure 2C). While BRAF mutant patients tended to have lower PD-1 ligand scores, this was not associated with a worse outcome.
PFS was also stratified by PD-L1 expression using empirically selected cutoff values to ensure adequate group sizes for comparison (Figure 2D). Generally, PD-L1 expression over 1% is accepted as clinically significant [16]. The poorest outcomes were observed in patients with PD-L1 <1%, where only 16.5% remained progression-free at 36 months (p=0.03 by log-rank test). However, in our patient series, tumors with PD-L1 expression >5% experienced the most favorable outcomes, with 67.0% remaining progression-free at 36 months. Those with PD-L1 scores between 1–5% showed moderately improved outcomes, with 51.3% progression-free at 36 months.
Tumor mutation burden is also thought to correlate with ICI treatment outcome in many cancers, including melanoma [17,24]. A TMB of 10 mutations/Mb has been associated with an increased likelihood of PD-1 monotherapy response [17]. TMB data was available for 52 of our patients (96.3%). TMB assessment was indeterminant in the other two individuals. Thirty-seven of 52 patients (71.2%) had a TMB score ≥ 10 mutations/Mb, and 15 patients (28.8%) had a TMB score < 10 mutations/Mb.
We evaluated the effect of tumor mutation burden on PFS in our patients treated with combination therapy. TMB was plotted versus PFS. This analysis revealed a significant linear correlation between an elevated TMB and prolonged PFS (Figure 2E). While patients with BRAF mutations tended to have a lower tumor mutation burden, a relationship to worsened PFS was not apparent.
PFS was also plotted based on empirically selected TMB cutoff values intended to ensure sufficient sample sizes for meaningful comparison (Figure 2F). Patients with a low TMB (<10 mutations/Mb) had a relatively poor outcome with only 26.5% of these patients remaining progression-free at 36 months. In patients with an intermediate TMB between 10–20 mutations/Mb, 57.1% were progression-free at the same time point (p=0.06). In contrast, patients with TMB >20 mutations/Mb demonstrated the most favorable outcomes, with 79.0% remaining progression-free at 36 months.
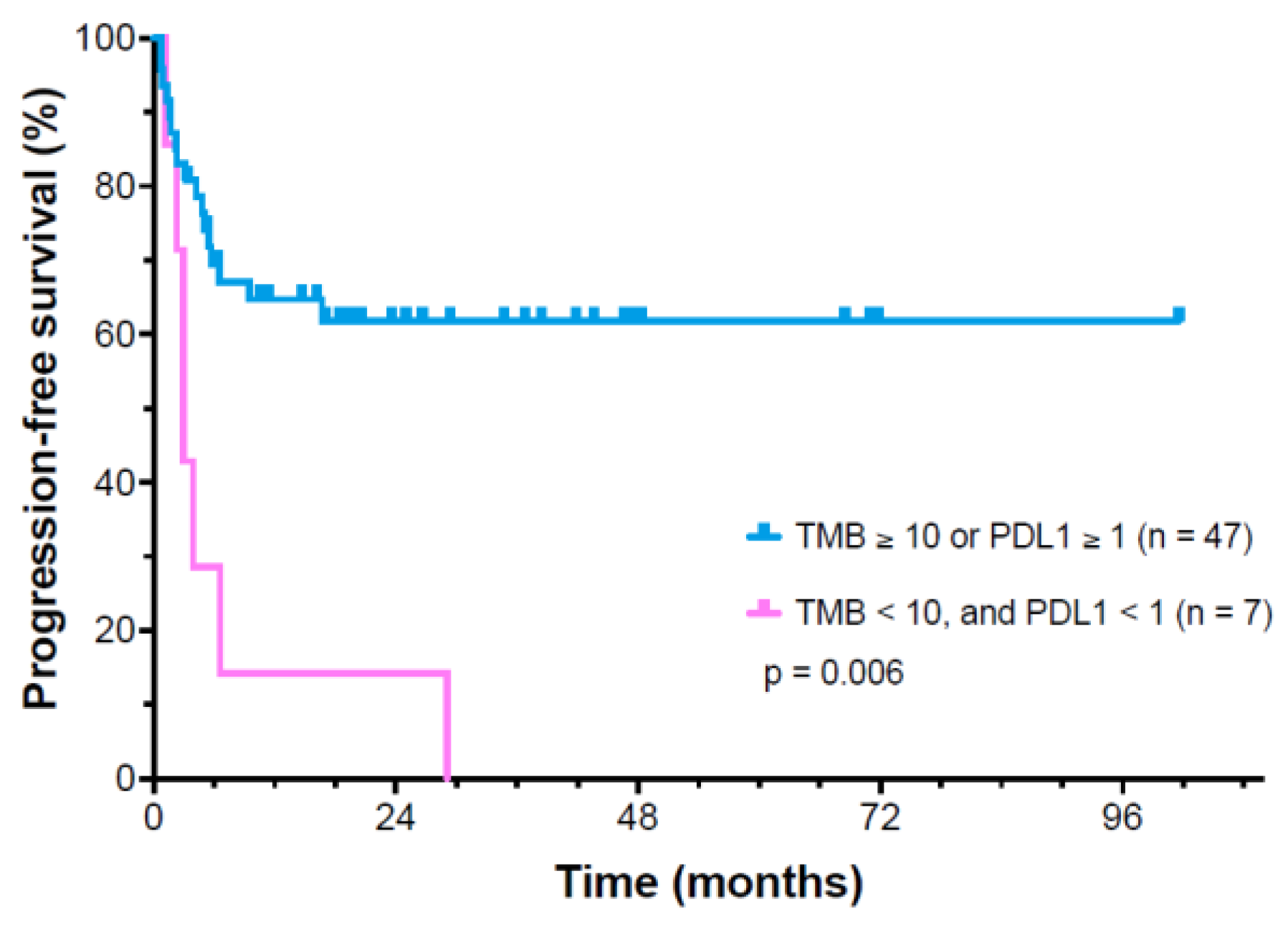
A further exploratory analysis of patients with combined low PD-1 ligand score (<1%) and a low TMB (<5/Mb) was attempted. This was limited by the low numbers of patients who shared both characteristics (n=7). These seven patients responded very poorly to ipilimumab plus nivolumab therapy with a median PFS of only 3 months (Figure 3). All patients with both low PD-L1 and TMB rapidly died due to metastatic disease.
4. Discussion
Following the advent of immune checkpoint inhibitor therapy, the prognosis of patients with metastatic melanoma has improved significantly. A number of potential prognostic markers for melanoma have previously been identified for patients with metastatic melanoma, including BRAF V600E mutation status, LDH, PD-L1, and TMB. However, the usefulness of these factors in predicting the outcome of ipilimumab and nivolumab combination therapy administered in a community setting remains to be established. We therefore performed a retrospective review of treatment data from 54 sequentially treated patients who received ipilimumab plus nivolumab as their initial therapy for metastatic melanoma.
The goal of the study was to evaluate whether potential biomarkers, evaluated at the time of diagnosis, had prognostic significance. Progression-free survival was utilized as the primary endpoint, as patients can have significant clinical benefit from 2nd or 3rd line treatment, which is likely to confound assessment of overall survival.
BRAF V600 mutation status has historically been associated with decreased recurrence-free survival (RFS) and disease-specific survival (DSS) [25]. Patients with resected stage IIIB and IIIC melanoma with a BRAF V600 mutation had an increased risk of recurrence and metastases [14]. In the Checkmate-067 trial, patients with BRAF mutations had an inferior outcome following checkpoint inhibitor monotherapy, compared to dual ICI treatment [13]. Our current patient series demonstrated that the presence or absence of BRAF V600 mutations had minimal effect on progression-free and overall survival in patients receiving combination ipilimumab plus nivolumab therapy.
In addition to BRAF mutations, serum lactate dehydrogenase (LDH) has long been recognized as an adverse prognostic biomarker in metastatic melanoma [26]. Elevated LDH levels is typically correlated with more aggressive disease kinetics. Yet, it is currently rare in our clinic for patients with newly diagnosed melanoma to present with an elevated LDH at the start of therapy. We could only identify 8 patients in our entire patient series who had an elevated LDH at baseline. The low frequency of LDH elevations seen in our study is consistent with similar trends reported by Gershenwald et al. [27]. Long et al. found that the effectiveness of ipilimumab and nivolumab immunotherapy was markedly reduced in patients with an elevated LDH [13]. However, in our patient series, the low prevalence of LDH elevation limited its utility as a biomarker for dual immunotherapy response. There was, at best, a weak association with PFS, that did not reach statistical significance. Thus, serum LDH was not a practical marker for predicting progression-free survival in our patients.
We believe that the decreasing frequency of patients with elevated LDH may be the result of more diligent follow-up of high-risk patients. Ultimately, there appears to be a trend toward earlier detection and treatment of metastatic disease. Currently, only rare patients present with a massive disease burden and high LDH. This finding may also reflect changes in referral patterns, sites of metastatic disease, as well as the effects of previous treatment (e.g., adjuvant immunotherapy).
Other tumor biomarkers, such as TMB and PD-L1, both had a strong correlation with objective responses following PD-1/PD-L1 monotherapy across multiple tumor types [24,28]. PD-L1 expression and TMB are independent prognostic factors in most cancers evaluated to date [24]. The impact of TMB and PD-L1 scores on the potential outcome of combination immunotherapy in metastatic melanoma is controversial.
Patients with elevated PD-L1 expression on tumor cells have an increased responsiveness to ICI therapy across a broad variety of cancers [24,28]. It should be noted that PD-L1 expression on melanoma tumor cells is generally lower than is observed in other cancers, such as NSCLC or renal cell carcinoma [29]. As a result, there is some disagreement concerning the degree of correlation of PD-L1 expression on tumor cells with clinical responses [30,31].
Our analysis demonstrated a significant relationship of increasing levels of PD-L1 expression and progression-free survival following first-line therapy. Patients with PD-L1 <1% on tumor cells had an estimated 4-year progression-free survival of 16%. PFS was 51% in patients with 1-5% PD-L1 expression and 67% in patients with PD-L1 >5%. In our patient series, patients with BRAF mutations trended to be associated with lower tumor cell PD-L1 expression, however this did not appear to adversely affect outcomes. It should also be noted that low PD-L1 levels (<1%) did not preclude durable responses to dual checkpoint inhibition.
In a separate retrospective analysis, increased TMB (>10 mutations/MB) also identified a subgroup of patients across multiple tumor types who generated a robust tumor response following pembrolizumab monotherapy [17]. This observation was subsequently confirmed in 8000 patients with multiple cancer types treated with PD-1/PD-L1 antibodies. Based on this data, Gandara et al., proposed a TMB cutoff >10 mutations per megabase, as this correlated significantly with OS [32]. This cut-off has subsequently been widely employed in clinical trials.
Generally, in metastatic melanoma patients, an increased TMB was found to be associated with improved survival, if a BRAF mutation was not present [33]. Andrews et al subsequently evaluated a cohort of deidentified melanoma patients from a large 8genomic database [34]. These patients all had comprehensive genomic profiling and TMB scoring. Patients were treated with either PD-1 monotherapy or combination immunotherapy. TMB-high status (≥10 mutations per megabase) was independently predictive of superior progression-free survival and overall survival in both mono and combination ICI therapy patients. In another melanoma-specific study, elevated TMB was associated with significantly longer progression-free survival following dual-agent ICI therapy (HR 0.26, 95% CI 0.07-0.90, p = 0.033, log-rank test) [35,36]. In contrast, a meta-analysis by Ning et. al., found that patients with high TMB showed significantly improved OS and PFS following PD-1 monotherapy [37]. However, this increased benefit was not observed in patients receiving combination immunotherapy in the same report [37]. Thus, measurement of PD-L1 and TMB as prognostic markers in dual checkpoint inhibitor therapy for metastatic melanoma is not a current standard-of-care.
Within our cohort of metastatic melanoma patients, we also identified a strong correlation of TMB with long-term PFS. In patients with TMB <10/MB, 48 month estimated progression-free survival was 26%, which increased to 57% in patients with TMB 10-20/MB and 79% if TMB was >20/MB. It should be noted that durable responses were seen at all levels of TMB expression. Thus, TMB alone was not sufficient to identify a group of patients who would fail to respond to combination ICI therapy. It should also be noted that the optimal cut-points for either PD-L1 or TMB as a prognostic markers have not been established to date [38]. Optimal cut-off values are likely to differ in various tumor types [38].
Considering the apparent usefulness of PD-1 ligand and TMB scores in our patient cohort, we performed an exploratory analysis of the uncommon patients that had both PD-L1 <1% and TMB <10/Mb compared to the rest of the cohort. Despite a small sample size (7 patients), we found that these patients had an extremely poor outcome and were unlikely to respond to combination checkpoint inhibitor therapy. We believe that it is important to identify these high-risk patients as candidates for novel treatment options and further research.
Potential limitations of our study include a small sample size and uncertainty surrounding the optimal cutoff values for PD-L1 and TMB. Due to the limited cohort size, threshold values for these biomarkers were selected to preserve statistical power and allow for meaningful subgroup comparisons. Additionally, it should be noted that PD-L1 testing was not routinely performed as part of standard clinical care. These factors restricted the number of evaluable patients, limiting our ability to fully evaluate the prognostic impact of this test. Thus, our data should be considered exploratory and in need of confirmation in a larger series of patients.
Furthermore, while our analysis focused on key biomarkers, this approach excluded a more comprehensive evaluation of other potentially relevant biomarkers, such as driver mutations in RAS, NF1, and KIT. These additional prognostic markers need evaluation. Finally, the number of patients with both a low TMB and PD-L1 score were quite small. The markedly adverse impact of this combination of biomarkers will also require further evaluation in a larger patient series.
5. Conclusions
While BRAF mutation status and serum LDH have shown potential prognostic significance in previous trials, these markers were not informative in our patient population. Our findings suggest that increasing PD-L1 expression and tumor mutational burden (TMB) were individually associated with improved outcomes in patients receiving dual immune checkpoint inhibitor therapy for advanced melanoma. The combined testing of PD-L1 and TMB may offer a more nuanced approach to patient stratification, particularly in identifying individuals who may derive limited benefit from current therapies or those that could be prioritized for novel treatment strategies or clinical trials. However, the small cohort size and variability in biomarker testing limit the generalizability of our findings. Future prospective studies with larger, more diverse populations are needed to validate optimal biomarker thresholds and to generate a prognostic nomogram that can more accurately guide discussions of potential clinical benefit versus toxicity risks in metastatic melanoma patients.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Table S1: Patient demographics; Table S2: Patient outcomes.
Author Contributions
Conceptualization, W.S and B.A.; methodology, W.S and B.A.; validation, W.S and B.A.; formal analysis, W.S and B.A.; investigation, W.S and B.A.; resources, W.S.; data curation, W.S and B.A.; writing—original draft preparation, B.A.; writing—review and editing, W.S and B.A.; visualization, W.S.; supervision, W.S.; project administration, W.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded in part by the US National Institutes of Health (NIH) grant 5U10CA035421. The publication fees for this article were supported by the Kirk Kerkorian School of Medicine at the UNLV Open Article Fund.
Institutional Review Board Statement
This retrospective data analysis project was formally reviewed by the Western IRB Chair and deemed exempt from full board review because the use of the protected health information involved no more than minimal risk to the individuals. After initial chart review, individual patient information was deidentified, with protections against inadvertent disclosure. In addition, the research could not be practicably conducted without access to medical records and the waiver.
Informed Consent Statement
Patient consent was waived due to protections against in advertent disclosure of identifiable patient information derived from this retrospective chart review.
Data Availability Statement
De-identified primary data is provided in supplemental table and additional data will be made available upon reasonable request to the corresponding author.
Acknowledgments
I We would like to express our appreciation to patients and their families and the clinical staff of Comprehensive Cancer Centers of Nevada. Critical review of the manuscript by Suzanne Samlowski, M Arch, is also appreciated.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| TLA | Three letter acronym |
| LD | Linear dichroism |
| PD-L1 | PD-1 ligand |
| ICI | Immune checkpoint inhibitor |
| LDH | Lactate dehydrogenase |
| PFS | Progression-free survival |
| OS | Overall survival |
| irAE | Immune-related adverse event |
| TMB | Tumor mutation burden (per megabase) |
| BOR | Best objective response |
| CR | Complete remission |
| PR | Partial response |
| SD | Stable disease |
| PD | Progressive disease |
| SD | Standard deviation |
References
- Siegel, R.L.; Kratzer, T.B.; Giaquinto, A.N.; Sung, H.; Jemal, A. Cancer statistics, 2025. CA Cancer J Clin 2025, 75, 10–45. [Google Scholar] [CrossRef] [PubMed]
- Boutros, A.; Croce, E.; Ferrari, M.; Gili, R.; Massaro, G.; Marconcini, R.; Arecco, L.; Tanda, E.T.; Spagnolo, F. The treatment of advanced melanoma: Current approaches and new challenges. Crit Rev Oncol Hematol 2024, 196, 104276. [Google Scholar] [CrossRef] [PubMed]
- Didier, A.J.; Nandwani, S.V.; Watkins, D.; Fahoury, A.M.; Campbell, A.; Craig, D.J.; Vijendra, D.; Parquet, N. Patterns and trends in melanoma mortality in the United States, 1999-2020. BMC Cancer 2024, 24, 790. [Google Scholar] [CrossRef]
- Atkins, M.B.; Lee, S.J.; Chmielowski, B.; Tarhini, A.A.; Cohen, G.I.; Truong, T.G.; Moon, H.H.; Davar, D.; O'Rourke, M.; Stephenson, J.J.; et al. Combination Dabrafenib and Trametinib Versus Combination Nivolumab and Ipilimumab for Patients With Advanced BRAF-Mutant Melanoma: The DREAMseq Trial-ECOG-ACRIN EA6134. J Clin Oncol 2022, JCO2201763. [Google Scholar] [CrossRef]
- Wolchok, J.D.; Chiarion-Sileni, V.; Rutkowski, P.; Cowey, C.L.; Schadendorf, D.; Wagstaff, J.; Queirolo, P.; Dummer, R.; Butler, M.O.; Hill, A.G.; et al. Final, 10-Year Outcomes with Nivolumab plus Ipilimumab in Advanced Melanoma. N Engl J Med 2025, 392, 11–22. [Google Scholar] [CrossRef]
- Larkin, J.; Chiarion-Sileni, V.; Gonzalez, R.; Grob, J.J.; Cowey, C.L.; Lao, C.D.; Schadendorf, D.; Dummer, R.; Smylie, M.; Rutkowski, P.; et al. Combined Nivolumab and Ipilimumab or Monotherapy in Untreated Melanoma. N Engl J Med 2015, 373, 23–34. [Google Scholar] [CrossRef]
- Michot, J.M.; Bigenwald, C.; Champiat, S.; Collins, M.; Carbonnel, F.; Postel-Vinay, S.; Berdelou, A.; Varga, A.; Bahleda, R.; Hollebecque, A.; et al. Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur J Cancer 2016, 54, 139–148. [Google Scholar] [CrossRef]
- Olsson-Brown, A.; Jain, A.; Frazer, R.; Farrugia, D.; Carser, J.; Houghton, J.; Lewis, R.D.; D'Mello, S.; Emanuel, G. Clinical Management and Outcomes of Immune-Related Adverse Events During Treatment with Immune Checkpoint Inhibitor Therapies in Melanoma and Renal Cell Carcinoma: A UK Real-World Evidence Study. Oncol Ther 2025. [Google Scholar] [CrossRef]
- Keam, S.; Turner, N.; Kugeratski, F.G.; Rico, R.; Colunga-Minutti, J.; Poojary, R.; Alekseev, S.; Patel, A.B.; Li, Y.J.; Sheshadri, A.; et al. Toxicity in the era of immune checkpoint inhibitor therapy. Front Immunol 2024, 15, 1447021. [Google Scholar] [CrossRef]
- Brahmer, J.R.; Abu-Sbeih, H.; Ascierto, P.A.; Brufsky, J.; Cappelli, L.C.; Cortazar, F.B.; Gerber, D.E.; Hamad, L.; Hansen, E.; Johnson, D.B.; et al. Society for Immunotherapy of Cancer (SITC) clinical practice guideline on immune checkpoint inhibitor-related adverse events. J Immunother Cancer 2021, 9. [Google Scholar] [CrossRef]
- Ghisoni, E.; Wicky, A.; Bouchaab, H.; Imbimbo, M.; Delyon, J.; Gautron Moura, B.; Gerard, C.L.; Latifyan, S.; Ozdemir, B.C.; Caikovski, M.; et al. Late-onset and long-lasting immune-related adverse events from immune checkpoint-inhibitors: An overlooked aspect in immunotherapy. Eur J Cancer 2021, 149, 153–164. [Google Scholar] [CrossRef] [PubMed]
- van Dorst, D.C.H.; Uyl, T.J.J.; Van der Veldt, A.A.M.; Andrawes, T.; Joosse, A.; Oomen-De Hoop, E.; Danser, A.H.; Mathijssen, R.H.J.; Bos, D.; Versmissen, J. Onset and progression of atherosclerosis in patients with melanoma treated with immune checkpoint inhibitors. J Immunother Cancer 2025, 13. [Google Scholar] [CrossRef] [PubMed]
- Long, G.V.; Larkin, J.; Schadendorf, D.; Grob, J.J.; Lao, C.D.; Marquez-Rodas, I.; Wagstaff, J.; Lebbe, C.; Pigozzo, J.; Robert, C.; et al. Pooled Long-Term Outcomes With Nivolumab Plus Ipilimumab or Nivolumab Alone in Patients With Advanced Melanoma. J Clin Oncol 2025, 43, 938–948. [Google Scholar] [CrossRef] [PubMed]
- Barbour, A.P.; Tang, Y.H.; Armour, N.; Dutton-Regester, K.; Krause, L.; Loffler, K.A.; Lambie, D.; Burmeister, B.; Thomas, J.; Smithers, B.M.; et al. BRAF mutation status is an independent prognostic factor for resected stage IIIB and IIIC melanoma: implications for melanoma staging and adjuvant therapy. Eur J Cancer 2014, 50, 2668–2676. [Google Scholar] [CrossRef]
- Van Wilpe, S.; Koornstra, R.; Den Brok, M.; De Groot, J.W.; Blank, C.; De Vries, J.; Gerritsen, W.; Mehra, N. Lactate dehydrogenase: a marker of diminished antitumor immunity. Oncoimmunology 2020, 9, 1731942. [Google Scholar] [CrossRef]
- Donia, M.; Prasad, V. Dual Checkpoint Inhibition in Melanoma With >/=1% PD-L1-Time to Reassess the Evidence. JAMA Oncol 2024, 10, 860–862. [Google Scholar] [CrossRef]
- Marabelle, A.; Fakih, M.; Lopez, J.; Shah, M.; Shapira-Frommer, R.; Nakagawa, K.; Chung, H.C.; Kindler, H.L.; Lopez-Martin, J.A.; Miller, W.H., Jr.; et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol 2020, 21, 1353–1365. [Google Scholar] [CrossRef]
- Lebbe, C.; Meyer, N.; Mortier, L.; Marquez-Rodas, I.; Robert, C.; Rutkowski, P.; Menzies, A.M.; Eigentler, T.; Ascierto, P.A.; Smylie, M.; et al. Evaluation of Two Dosing Regimens for Nivolumab in Combination With Ipilimumab in Patients With Advanced Melanoma: Results From the Phase IIIb/IV CheckMate 511 Trial. J Clin Oncol 2019, 37, 867–875. [Google Scholar] [CrossRef]
- Perez, L.; Samlowski, W.; Lopez-Flores, R. Outcome of Elective Checkpoint Inhibitor Discontinuation in Patients with Metastatic Melanoma Who Achieved a Complete Remission: Real-World Data. Biomedicines 2022, 10, 1144. [Google Scholar] [CrossRef]
- Eisenhauer, E.A.; Therasse, P.; Bogaerts, J.; Schwartz, L.H.; Sargent, D.; Ford, R.; Dancey, J.; Arbuck, S.; Gwyther, S.; Mooney, M.; et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer 2009, 45, 228–247. [Google Scholar] [CrossRef]
- Kaplan, E.L.; Meier, P. Nonparametric Estimation from Incomplete Observations. Journal of the American Statistical Association 1958, 53, 457–481. [Google Scholar] [CrossRef]
- Bland, J.M.; Altman, D.G. The logrank test. BMJ 2004, 328, 1073. [Google Scholar] [CrossRef] [PubMed]
- Diem, S.; Kasenda, B.; Spain, L.; Martin-Liberal, J.; Marconcini, R.; Gore, M.; Larkin, J. Serum lactate dehydrogenase as an early marker for outcome in patients treated with anti-PD-1 therapy in metastatic melanoma. Br J Cancer 2016, 114, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Yarchoan, M.; Albacker, L.A.; Hopkins, A.C.; Montesion, M.; Murugesan, K.; Vithayathil, T.T.; Zaidi, N.; Azad, N.S.; Laheru, D.A.; Frampton, G.M.; et al. PD-L1 expression and tumor mutational burden are independent biomarkers in most cancers. JCI Insight 2019, 4. [Google Scholar] [CrossRef]
- Wilson, M.A.; Zhao, F.; Letrero, R.; D'Andrea, K.; Rimm, D.L.; Kirkwood, J.M.; Kluger, H.M.; Lee, S.J.; Schuchter, L.M.; Flaherty, K.T.; et al. Correlation of somatic mutations and clinical outcome in melanoma patients treated with Carboplatin, Paclitaxel, and sorafenib. Clin Cancer Res 2014, 20, 3328–3337. [Google Scholar] [CrossRef]
- Eton, O.; Legha, S.S.; Moon, T.E.; Buzaid, A.C.; Papadopoulos, N.E.; Plager, C.; Burgess, A.M.; Bedikian, A.Y.; Ring, S.; Dong, Q.; et al. Prognostic factors for survival of patients treated systemically for disseminated melanoma. J Clin Oncol 1998, 16, 1103–1111. [Google Scholar] [CrossRef]
- Gershenwald, J.E.; Scolyer, R.A.; Hess, K.R.; Sondak, V.K.; Long, G.V.; Ross, M.I.; Lazar, A.J.; Faries, M.B.; Kirkwood, J.M.; McArthur, G.A.; et al. Melanoma staging: Evidence-based changes in the American Joint Committee on Cancer eighth edition cancer staging manual. CA Cancer J Clin 2017, 67, 472–492. [Google Scholar] [CrossRef]
- Mariam, A.; Kamath, S.; Schveder, K.; McLeod, H.L.; Rotroff, D.M. Biomarkers for Response to Anti-PD-1/Anti-PD-L1 Immune Checkpoint Inhibitors: A Large Meta-Analysis. Oncology (Williston Park) 2023, 37, 210–219. [Google Scholar] [CrossRef]
- Kluger, H.M.; Zito, C.R.; Turcu, G.; Baine, M.K.; Zhang, H.; Adeniran, A.; Sznol, M.; Rimm, D.L.; Kluger, Y.; Chen, L.; et al. PD-L1 Studies Across Tumor Types, Its Differential Expression and Predictive Value in Patients Treated with Immune Checkpoint Inhibitors. Clin Cancer Res 2017, 23, 4270–4279. [Google Scholar] [CrossRef]
- Simeone, E.; Grimaldi, A.M.; Ascierto, P.A. Anti-PD1 and anti-PD-L1 in the treatment of metastatic melanoma. Melanoma Manag 2015, 2, 41–50. [Google Scholar] [CrossRef]
- Schmitt, A.M.; Larkin, J.; Patel, S.P. Dual Immune Checkpoint Inhibition in Melanoma and PD-L1 Expression: The Jury Is Still Out. J Clin Oncol 2025, 43, 122–124. [Google Scholar] [CrossRef] [PubMed]
- Gandara, D.R.; Agarwal, N.; Gupta, S.; Klempner, S.J.; Andrews, M.C.; Mahipal, A.; Subbiah, V.; Eskander, R.N.; Carbone, D.P.; Riess, J.W.; et al. Tumor mutational burden and survival on immune checkpoint inhibition in >8000 patients across 24 cancer types. J Immunother Cancer 2025, 13. [Google Scholar] [CrossRef] [PubMed]
- Hodi, F.S.; Wolchok, J.D.; Schadendorf, D.; Larkin, J.; Long, G.V.; Qian, X.; Saci, A.; Young, T.C.; Srinivasan, S.; Chang, H.; et al. TMB and Inflammatory Gene Expression Associated With Clinical Outcomes Following Immunotherapy in Advanced Melanoma. Cancer Immunol Res 2021. [Google Scholar] [CrossRef] [PubMed]
- Andrews, M.C.; Li, G.; Graf, R.P.; Fisher, V.A.; Mitchell, J.; Aboosaiedi, A.; O'Rourke, H.; Shackleton, M.; Iddawela, M.; Oxnard, G.R.; et al. Predictive Impact of Tumor Mutational Burden on Real-World Outcomes of First-Line Immune Checkpoint Inhibition in Metastatic Melanoma. JCO Precis Oncol 2024, 8, e2300640. [Google Scholar] [CrossRef]
- Haugh, A.M.; Osorio, R.C.; Francois, R.A.; Tawil, M.E.; Tsai, K.K.; Tetzlaff, M.; Daud, A.; Vasudevan, H.N. Targeted DNA Sequencing of Cutaneous Melanoma Identifies Prognostic and Predictive Alterations. Cancers (Basel) 2024, 16. [Google Scholar] [CrossRef]
- Forschner, A.; Battke, F.; Hadaschik, D.; Schulze, M.; Weissgraeber, S.; Han, C.T.; Kopp, M.; Frick, M.; Klumpp, B.; Tietze, N.; et al. Tumor mutation burden and circulating tumor DNA in combined CTLA-4 and PD-1 antibody therapy in metastatic melanoma - results of a prospective biomarker study. J Immunother Cancer 2019, 7, 180. [Google Scholar] [CrossRef]
- Ning, B.; Liu, Y.; Wang, M.; Li, Y.; Xu, T.; Wei, Y. The Predictive Value of Tumor Mutation Burden on Clinical Efficacy of Immune Checkpoint Inhibitors in Melanoma: A Systematic Review and Meta-Analysis. Front Pharmacol 2022, 13, 748674. [Google Scholar] [CrossRef]
- Zheng, M. Tumor mutation burden for predicting immune checkpoint blockade response: the more, the better. J Immunother Cancer 2022, 10. [Google Scholar] [CrossRef]
Figure 1.
caption.
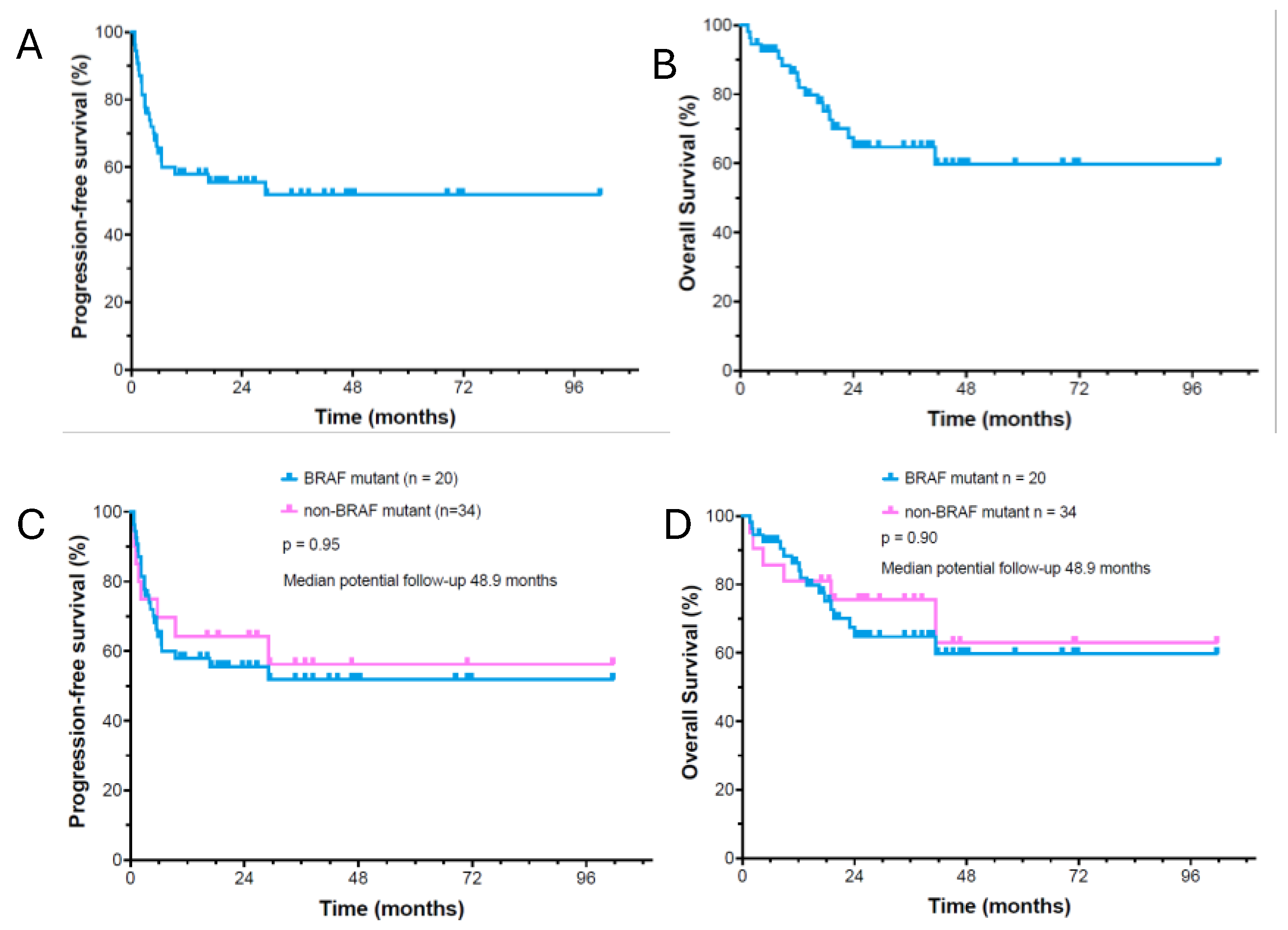
Figure 2.
caption.
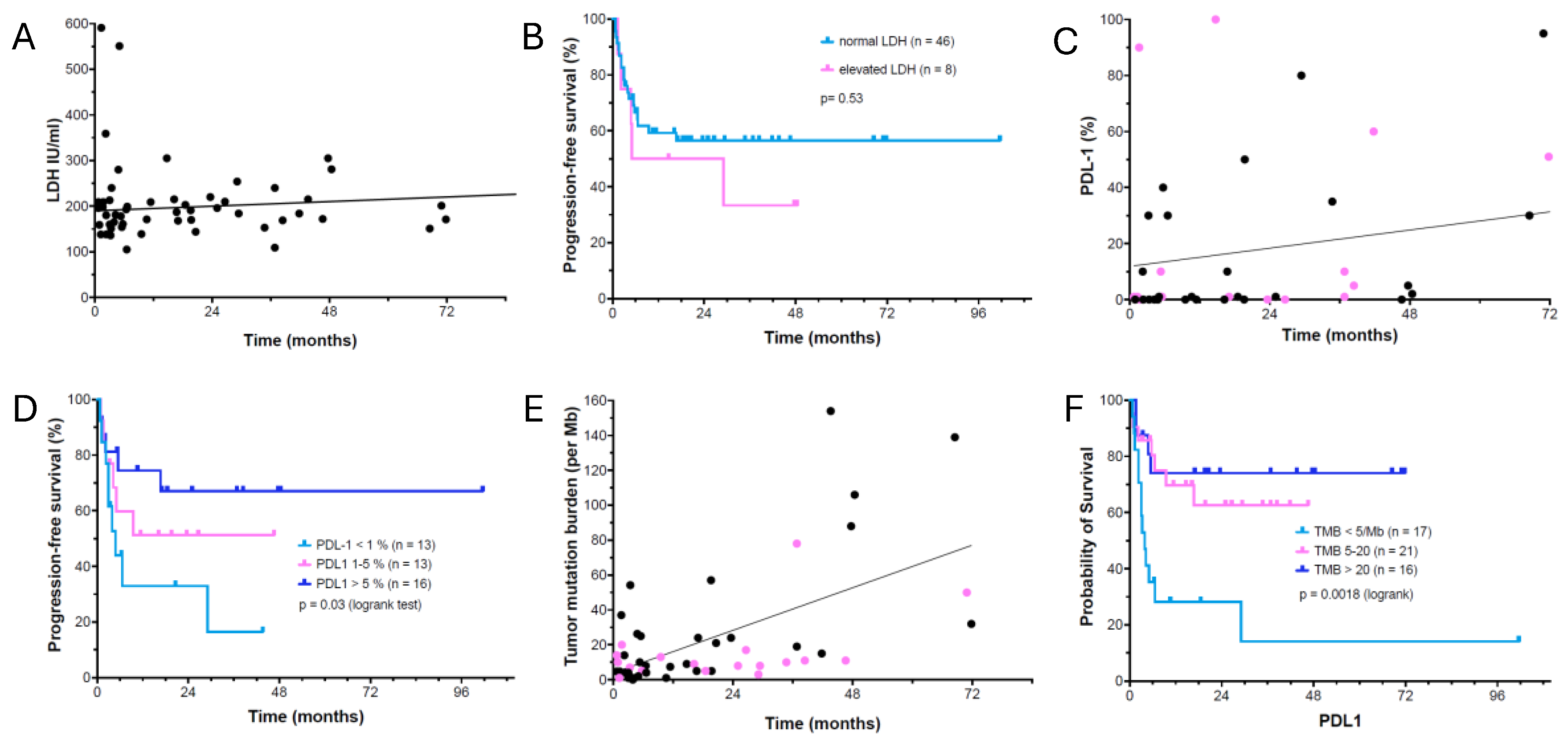
Figure 3.
caption.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



