
Submitted:
29 August 2025
Posted:
01 September 2025
You are already at the latest version
Abstract
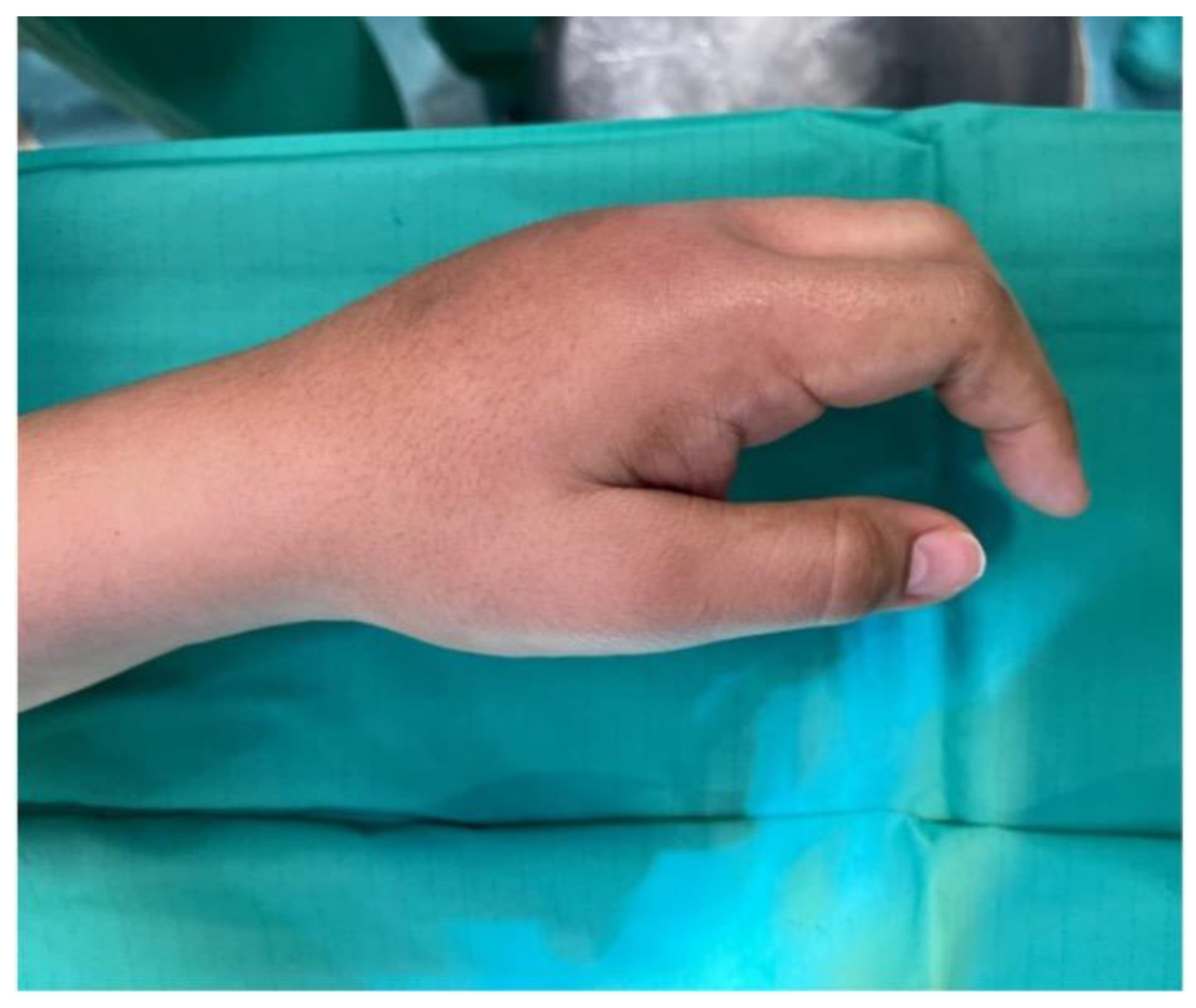
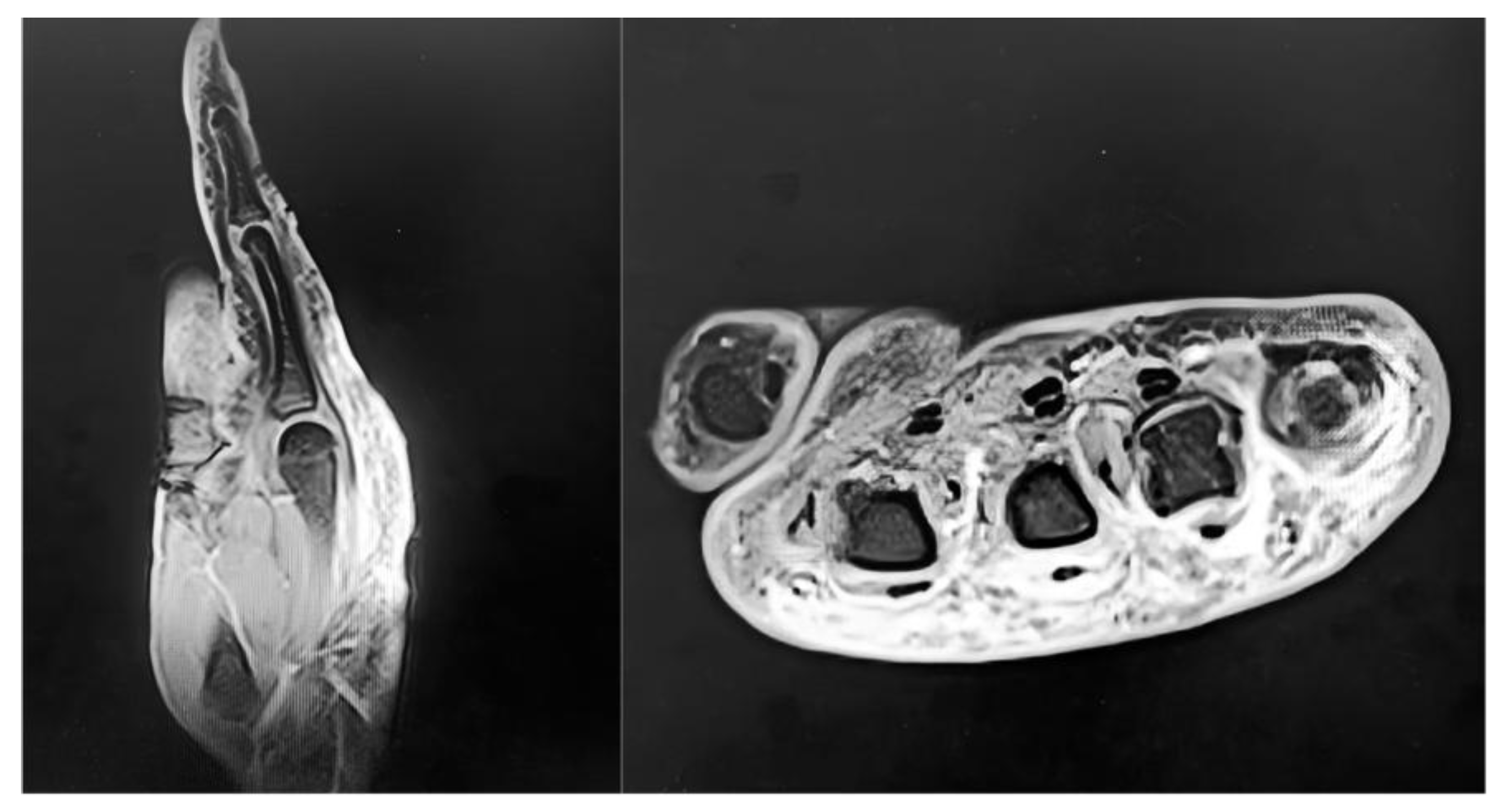
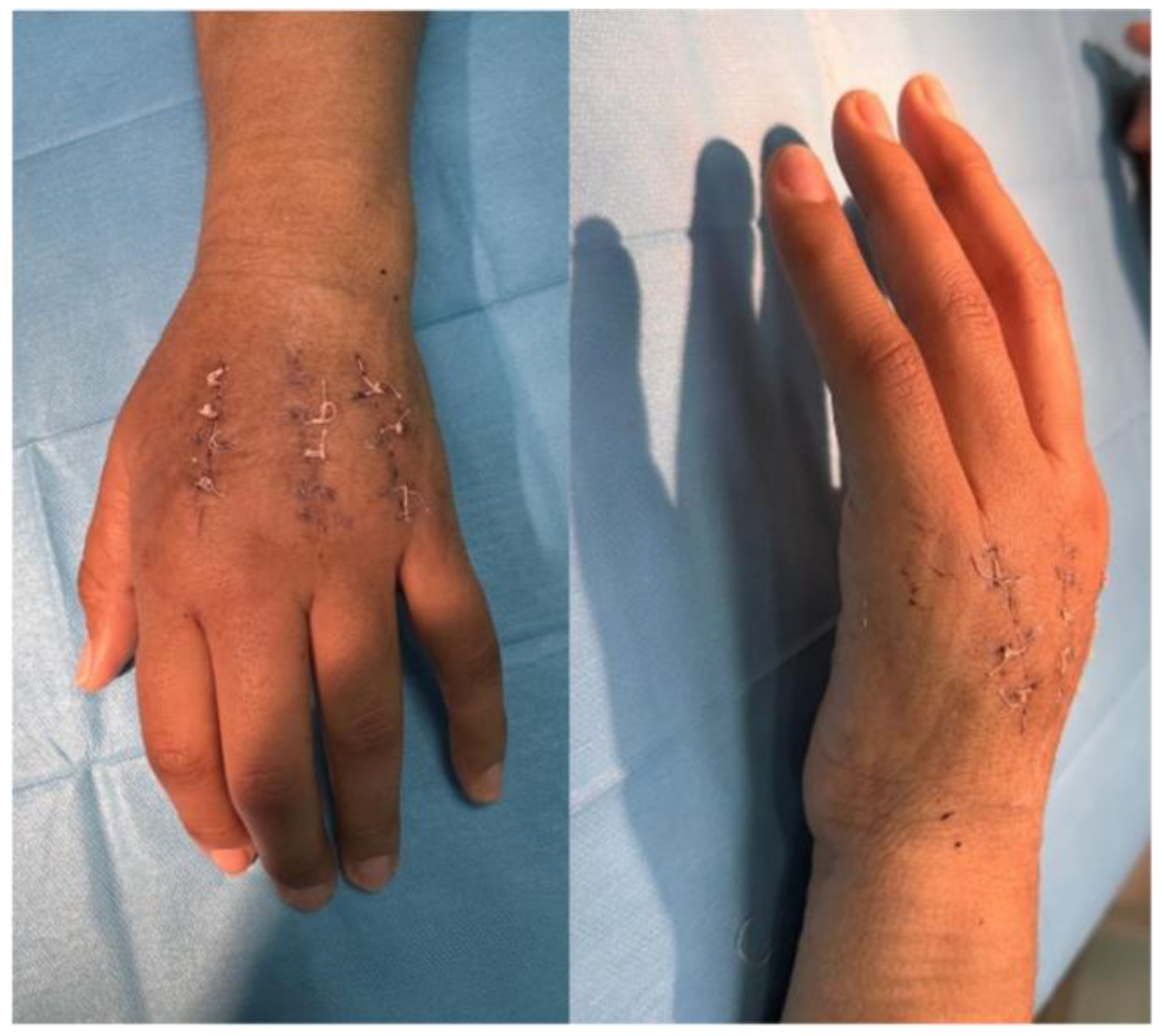
Background: Secretan’s syndrome is a rare and under-recognized condition characterized by chronic, indurated, non-pitting edema of the dorsal hand with thumb sparing. Fewer than a few dozen cases have been reported worldwide, mostly as isolated case reports, and its pathogenesis remains debated between traumatic, inflammatory, and factitious mechanisms. This article presents a surgically managed hyperplastic case and a review of the literature, emphasizing how principles of precision medicine can guide diagnosis and treatment. Materials and Methods: A 36-year-old healthcare worker developed progressive dorsal swelling of the left hand following minor trauma, with marked restriction of metacarpophalangeal flexion. Laboratory tests and radiographs were normal. MRI demonstrated peritendinous fibrosis encasing the extensor tendons. Psychiatric evaluation excluded factitious behavior. Given the functional limitation and MRI evidence of fibrosis, selective dorsal fasciotomies and extensor tendon tenolysis were performed. A systematic literature review was conducted to summarize epidemiology, clinical and imaging features, histopathology, and management options. Results: Histology revealed fibro-adipose tissue with chronic inflammatory changes and CD68+ histiocytic aggregates; microbiological cultures were negative. Postoperative rehabilitation enabled significant functional recovery. The literature review confirmed the scarcity of published cases and the absence of standardized guidelines. MRI consistently proved to be the most informative imaging tool, while surgical treatment was described only in hyperplastic, refractory forms. Conclusions: This case and review illustrate how a precision medicine approach can optimize management of rare disorders. Early MRI-based diagnosis, multidisciplinary assessment, and phenotype-driven surgical intervention allowed tailored treatment and favorable outcome. Personalized care that integrates clinical features, imaging findings, and patient-specific factors may improve results in hyperplastic Secretan’s syndrome despite the limited evidence base.
Keywords:
1. Introduction
2. Materials and Methods of Literature Review
3. Review of the Literature
3.1. Epidemiology
3.2. Clinical Presentation
3.3. Imaging
3.4. Histology
.3.5 Management
4. Detailed Case Description
4.1. Patient Information
4.2. Clinical Findings
4.3. Diagnostic Assessment
4.4. Therapeutic Intervention
4.5. Microbiological and Histological Findings
4.6. Follow-Up and Outcomes
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| CRPS | Complex Regional Pain Syndrome |
| ICD-9-CM | International Classification of Diseases, Ninth Revision, Clinical Modification |
| MCP | Metacarpophalangeal |
| MRI | Magnetic Resonance Imaging |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| VAS | Visual Analog Scale |
References
- Angelini, G.; Meneghini, C.L.; Vena, G.A. Secretan’s syndrome: An artefact oedema of the hand. Contact Dermatitis 1982, 8, 345–346. [Google Scholar] [CrossRef] [PubMed]
- Demircioğlu, D.; Öztürk Durmaz, E.; Sezer, E.; Şahin, S. Secretan syndrome: A fluctuating case of factitious lymphedema. Cutis 2021, 108, E23–E24. [Google Scholar] [CrossRef] [PubMed]
- Abnousi, F.; Chou, L.B. Secretan’s disease of the foot: A case report and review. Foot Ankle Int. 2008, 29, 248–250. [Google Scholar] [CrossRef] [PubMed]
- Whitney, T.M.; Jones, N.F. Magnetic resonance imaging findings in Secretan’s disease. J. Hand Surg. Am. 1995, 20, 464–466. [Google Scholar] [CrossRef] [PubMed]
- Lemmens, L.; van Doninck, J.; de Smet, L. Secretan’s syndrome: Case report. Acta Chir. Belg. 2019, 119, 123–124. [Google Scholar] [CrossRef] [PubMed]
- Tebbaa El Hassali, A.; Barrached, M.; Lachkar, A.; Abdeljaouad, N.; Yacoubi, H. Secretan’s syndrome: It is time to talk about it. Cureus 2024, 16, e62580. [Google Scholar] [CrossRef] [PubMed]
- Fleming, J.P. Secretan’s disease. Plast. Reconstr. Surg. 1977, 60, 617–618. [Google Scholar] [CrossRef] [PubMed]
- Collet, S.; Forli, A.; Carpentier, P.H.; Laviolette, F.; Imbert, B.; Blaise, S. Secretan’s syndrome: Myth or pathomimia? J. Mal. Vasc. 2014, 39, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Redfern, A.B.; Curtis, R.M.; Wilgis, E.F.S. Experience with peritendinous fibrosis of the dorsum of the hand. J. Hand Surg. Am. 1982, 7, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Grobmyer, A.J., 3rd; Bruner, J.M.; Dragstedt, L.R., 2nd. Closed lymphangioplasty in Secretan’s disease. Arch. Surg. 1968, 97, 81–83. [Google Scholar] [CrossRef] [PubMed]
- Winkelmann, R.K.; Barker, S.M. Factitious lymphoedema, Secretan’s syndrome. Dermatol. Clin. 1990, 8, 205. [Google Scholar] [CrossRef]
- Birman, M.V.; Lee, D.H. Factitious disorders of the upper extremity. J. Am. Acad. Orthop. Surg. 2012, 20, 78–85. [Google Scholar] [CrossRef] [PubMed]


| Author, Year | No. of Cases | Site | Diagnostic Findings | Management | Outcome |
|---|---|---|---|---|---|
| Secretan, 1901 | Original description | Hand | Indurated dorsal edema, thumb sparing | Conservative | Chronic, variable resolution |
| Angelini et al., 1982 [1] | 1 | Hand | Non-pitting edema, histology: fibrosis | Conservative | Partial resolution |
| Redfern et al., 1982 [9] | 4 | Hand | Peritendinous fibrosis | Surgical release | Functional improvement |
| Grobmyer et al., 1968 [10] | 1 | Hand | Attempted closed lymphangioplasty | Surgical | Persistent edema |
| Fleming, 1977 [7] | 1 | Hand | Indurated dorsal edema, fibrotic tissue | Conservative | Chronic course |
| Whitney & Jones, 1995 [4] | 1 | Hand | MRI: peritendinous fibrosis | Conservative | Persistent limitation |
| Winkelmann & Barker, 1990 [11] | 2 | Hand | Factitious lymphedema suspected | Psychiatric + conservative | Resolution with follow-up |
| Abnousi & Chou, 2008 [3] | 1 | Foot | Dorsal edema, fibrotic band | Surgical excision | Symptom resolution |
| Collet et al., 2014 [8] | 3 | Hand | Chronic edema, possible factitious cases | Conservative, psychiatric | Variable |
| Lemmens et al., 2019 [5] | 1 | Hand | Classic phenotype, biopsy fibrosis | Conservative | Persistent symptoms |
| Demircioğlu et al., 2021 [2] | 1 | Hand | Fluctuating edema, factitious suspicion | Psychiatric + conservative | Symptom control |
| Tebbaa El Hassali et al., 2024 [6] | 1 | Hand | Chronic indurated edema | Conservative | Stable with follow-up |
| Birman & Lee, 2012 [12] | Review | Upper limb | Factitious disorders of the extremity | Psychiatric/varied | Highlights diagnostic overlap |
| Timepoint | VAS (0–10) | QuickDASH (0–100) | Grip Strength (Jamar, % vs contralateral) |
|---|---|---|---|
| Preoperative Early post-op (1 month) 3-Month Follow-up |
8 | 65 | 40% |
| 5 | 50 | 50% | |
| 4 | 35 | 65% | |
| 6-Month Follow-up | 2 | 20 | 75% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



