
Submitted:
28 August 2025
Posted:
29 August 2025
You are already at the latest version
Abstract
To evaluate the association of the inflammation marker, such as monocyte/lymphocyte ratio (MLR), with adverse cardiac remodeling and clinical biochemical indexes in atrial fibrillation (AF) patients, this study investigated the association of MLR with clinical biochemical indexes and cardiac remodeling in elderly with AF. In a cross-sectional study, a total of 1154 hospitalized Chinese elderly (aged ≥ 65 years) with AF were collected retrospectively in a single medical care center. The patients were divided into low (≤ 0.293), moderate (> 0.293 to ≤ 0.460) and high (> 0.460) MLR ratio groups according to the tertiles of MLR. Regression analysis of MLR (> 0.460) with clinical biochemical indexes and echocardiographic parameters has been done. It revealed that high MLR (> 0.460) was independently associated with male gender, decreased estimated glomerular filtration rate (eGFR), lower level of plasma albumin, cardiac ventricular dilatation and dysfunction (All P < 0.05). In conclusion, high MLR was linked to male gender, decreased eGFR, lower plasma albumin level and adverse cardiac remodeling in elderly with AF.
Keywords:
atrial fibrillation
; monocyte/lymphocyte ratio
; glomerular filtration dysfunction
; cardiac remodeling
; elderly
1. Introduction
Atrial fibrillation (AF) is a common supraventricular arrhythmia in clinical practice, especially in elderly population. Increased stroke risk has been confirmed in patients with AF [1]. The death rate resulted from thromboembolism-related events in elderly with AF has been shown to decrease after treatment with anticoagulant medication. However, the risk of death from cardiovascular events remains elevated in the AF patients even treated with appropriate anticoagulant medication [2]. Serious arrhythmias are usually firstly considered to be responsible for the increased cardiovascular death in the patients with AF [1]. Furthermore, cardiac adverse remodeling might be an important pathologic substrate for higher cardiovascular mortality in the patients with AF [3,4]. Studies have suggested that chronic inflammation was associated with increased incidence of AF in patients with cardiac adverse structural abnormalities [5,6]. The elevated inflammatory markers such as C-reactive protein and interleukin-6 have been reported to be associated with cardiac adverse remodeling and increased cardiovascular death in patients with AF [7,8]. Meanwhile, additional easily available inflammatory marker is monocyte/lymphocyte ratio (MLR) that has been reported to be associated with increased cardiovascular death [9]. However, it remains unclear whether the MLR is associated with cardiac adverse remodeling. Therefore, this study investigated the association of MLR with cardiac remodeling and related clinical biochemical indexes in elderly with AF.
2. Materials and Methods
2.1. Study Design and Participants
A cross-sectional study was conducted, in which 1154 of hospitalized Chinese elderly (aged ≥ 65 years) with non-valvular AF [persistent AF (n=596); long-term persistent AF (n=442); permanent AF (n=116)] were collected retrospectively by review of medical records from 2014 to 2021 in our geriatric inpatient department. All of the patients completed electrocardiographic examination, color Doppler echocardiography and biochemical tests [10]. This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the First Affiliated Hospital of Chongqing Medical University (No. 2022-K390). The ethics committee waived the need for patients’ written informed consent because of anonymous nature of the clinical data acquired retrospectively.
White blood cell (WBC) count in peripheral blood was assessed using a Sysmex XN-1000 Analyzer (Sysmex Corporation, Kobe, Japan). The MLR was then calculated manually. The WBC and MLR were measured averagely of three times within the first week of hospitalization for each patient, respectively. The patients with AF were divided into low MLR ratio group (the ratio ≤ 0.293, n=382), moderate MLR ratio group (the ratio > 0.293 to ≤ 0.460, n=392) and high MLR ratio group (the ratio > 0.460, n=380) according to the tertiles of MLR ratio.
We excluded patients with acute stroke or myocardial infarction (MI), gout attack, hypertrophic, restrictive or dilated cardiomyopathy, valvular or congenital heart diseases, chronic obstructive pulmonary disease, infection, autoimmune diseases, glomerulonephritis and malignant tumor. The patients without electrocardiographic and echocardiographic examination and the necessary blood biochemical data have been excluded.
2.2. Diagnostic Criteria for Comorbidities:
Type 2 diabetes mellitus (DM) was defined as fasting plasma glucose (FPG) ≥7.0 mmol/L, and/or the plasma glucose ≥ 11.1mmol/L at 2 hours after oral 75 g glucose-loaded tolerance test, meanwhile the plasma insulin level was normal or elevated, or previously diagnosed type 2 DM in which the insulin or oral glucose-lowering medication has been used in the patients, meanwhile the patients with diabetic ketoacidosis or hyperosmolar state, or other types of DM were excluded [11].
Primary hypertension was defined as followings: after 10 minutes rest and two measurements of blood pressure (BP), the averaged arterial systolic BP ≥ 140mmHg and/or diastolic BP ≥ 90mmHg on different days without taking antihypertensive drugs; or the hypertension was diagnosed previously, and the antihypertensive medications have been used regularly, meanwhile secondary hypertension was excluded [12].
Gout was defined as urate crystals in the joints with gouty stones, arthralgia and arthritis [13].
The coronary heart disease (CHD) was considered if the patients had at least one main branch with atherosclerotic lumen stenosis (≥ 50%) in coronary artery confirmed by angiography; or the patient had diagnosed MI; or they had a history of coronary stent placement [14]. The severity of coronary artery lesions was assessed using the Gensini score [15].
Stroke was defined as positive brain imaging evidences from electronic computed tomography (CT) or magnetic resonance imaging (MRI), or previously confirmed stroke with or without a previous history of hemiparesis [16].
2.3. Measurement of Plasma Lipids, Glucose, Glycated Hemoglobin and High Sensitivity C-Reactive Protein
Plasma glucose was measured by hexokinase colorimetric method, and glycosylated hemoglobin (HbA1c) was measured by high performance liquid chromatography. Triglycerides and total cholesterol were measured by enzyme colorimetric method, and high-density lipoprotein cholesterol (HDL-C) was determined by homogeneous enzyme colorimetric method. Low-density lipoprotein cholesterol (LDL-C) was calculated using the Friedewald formula [17]. Albumin was measured by bromocresol green method. D-dimer was determined by immunoturbidimetric method [18]. High sensitivity C-reactive protein (hs-CRP) was determined by immunoturbidimetric assay.
2.4. Calculation of Glomerular Filtration Rate and Body Mass Index
For men, serum creatinine (Scr) > 80 µmol/L, estimated glomerular filtration rate (eGFR) = 141 × (Scr µmol / L / 88.4 / 0.9)-1.209 × 0.993Age (years); Scr ≤ 80 µmol/L, eGFR = 141 × (Scr µmol / L / 88.4 / 0.9)-0.411 × 0.993Age (years). For women, Scr > 62 µmol / L, eGFR = 144 × (Scr µmol / L / 88.4 / 0.7)-1.209 × 0.993Age (years); Scr ≤ 62 µmol / L, eGFR = 144 × (Scr µmol / L / 88.4 / 0.7)-0.329 × 0.993Age (years) [19,20]. Body mass index (BMI) was calculated as body weight (kg) / [height (m)]2 [21].
2.5. Measurement of Cardiac Structure and Function
With the GE Vivid7 full digital color Doppler ultrasound diagnostic instrument, transthoracic two-dimensional M-mode echocardiography was used to determine [22]: right atrial internal diameter (RAD), right ventricular internal diameter (RVD), left atrial internal diameter (LAD), interventricular septal thickness (IVST), left ventricular posterior wall thickness (LVPWT), left ventricular end-systolic internal diameter (LVESD), left ventricular end-diastolic internal diameter (LVEDD), pulmonary artery pressure (PAP) and left ventricular ejection fraction (LVEF) [23,24,25].
2.6. Statistical Analysis
The statistical package for social science (SPSS) 26.0 software (IBM Company, Chicago, IL, USA) was used for the statistical analysis. The cutoff values of tertile MLR values used in the current study were calculated by the SPSS software, according to the MLR values of the elderly subjects in the present study. The continuous data were expressed as mean ± standard deviation. The normally distributed continuous data were analyzed by t-test between the two groups. If the continuous data did not follow normal distribution, the Mann Whitney U test was conducted between the two groups. The counting data is expressed as a percentage (%), meanwhile the chi square test was used. The Pearson or Spearman correlation analysis was performed for univariate analysis. Dichotomized logistic regression analysis was performed for multifactorial analysis. Because hs-CRP, neutrophil and WBC were collinear with MLR, these parameters were not included in the regression analysis. A 2-tailed value of P < 0.05 was considered significant statistically.
3. Results
3.1. Clinical Characteristics According to Tertile MLR
The clinical characteristics of subjects according to tertile of MLR are shown in Table 1. Compared with the low MLR (≤ 0.293) group, the moderate MLR (> 0.293 to ≤ 0.460) group had older age, higher prevalence rate of smoking, alcohol consumption and gout, D-dimer, hs-CRP and neutrophil (All P < 0.05, Table 1), and lower BMI, diastolic BP, TG, LDL-C, albumin and eGFR (All P < 0.05, Table 1); the high MLR (> 0.460) group had older age, higher prevalence rate of male gender, smoking, alcohol consumption and gout, D-dimer, hs-CRP, neutrophil and WBC (All P < 0.05, Table 1), and lower BMI, diastolic BP, TG, LDL-C, HDL-C, albumin and eGFR (All P < 0.05, Table 1). Compared with the moderate MLR (> 0.293 to ≤ 0.460) group, the high MLR (> 0.460) group had older age, higher prevalence rate of smoking and alcohol consumption, hs-CRP, neutrophils and WBC (All P < 0.05, Table 1), and lower HDL-C, albumin and eGFR (All P < 0.05, Table 1).
The univariate correlation analysis showed that MLR was positively correlated with age, and the prevalent ratio of male gender, smoking, alcohol consumption and gout, D-dimer, hs-CRP, neutrophils and WBC (All P < 0.05, Table 1); and negatively correlated with BMI, diastolic BP, TG, LDL-C, HDL-C, albumin and eGFR (All P < 0.05, Table 1).
3.2. Cardiac Remodeling According to Tertile MLR
Compared with the low MLR group, RAD, RVD and LAD were larger in the moderate MLR group (All P < 0.05, Table 2); RAD, RVD, LAD, LVESD and LVEDD were larger, while PAP was higher, LVEF was lower in the high MLR group (All P < 0.05, Table 2). Compared with the moderate MLR group, RAD, RVD, LVESD, LVEDD were larger, while PAP was higher, LVEF was lower in the high MLR group (All P < 0.05, Table 2).
3.3. Multivariate Logistic Regression Analysis of MLR with Clinical Characteristics and Echocardiographic Parameters
Multivariate logistic binary regression analysis of high MLR group (MLR > 0.460) with clinical characteristics and echocardiographic parameters showed that high MLR was independently associated with male gender, decreased level of plasma albumin, lower eGFR, larger RVD, LVESD and LVEDD, and lower LVEF (All P < 0.05, Table 3; Figure 1, Figure 2, Figure 3, Figure 4, Figure 5, Figure 6 and Figure 7).
4. Discussion
This study showed that high MLR was independently associated with male gender, decreased level of plasma albumin, lower eGFR, cardiac adverse remodeling and dysfunction in elderly patients with AF.
Studies have suggested that dyslipidemia and obesity were associated with high-fat diet, and contributed to lipid deposition and lipotoxicity in kidney [26,27,28]. It can lead to insulin resistance and impede glucose utilization by kidney cells. Energy supply by fat oxidation was forced to increase subsequently. However, this way of energy supply can lead to release lots of pro-inflammatory factors, which increased apoptosis and necrosis of endothelial and epithelial cells in glomeruli [27,29,30], elevated urinary albumin, decreased level of plasma albumin and eGFR [31,32,33] and complicated renal dysfunction [34]. With declined eGFR and increased retention of plasma toxin, the suppressed appetite, decreased protein intake and increased leakage of plasma albumin ultimately lead to hypoalbuminemia in the metabolic nephropathy [35]. High MLR has been associated with low eGFR in chronic kidney disease [36]. However, to our knowledge, this study firstly demonstrated that high MLR was associated with low eGFR and decreased level of plasma albumin in elderly with AF. Studies have found that unhealthy lifestyles such as cigarette smoking and alcohol consumption were associated with increased systemic inflammation especially in older men [37,38]. However, our present study firstly confirmed that high inflammatory marker MLR was more tightly associated with elderly men in AF patients.
Studies have confirmed that dyslipidemia, overweight, obesity, insulin resistance, hyperglycemia, type 2 DM and hypertension were associated with the development of AF [39,40,41,42,43,44,45]. A growing body of data from both epidemiological and clinical studies have demonstrated that epicardial fat is associated with the severity of AF. Some studies have found a relationship between epicardial fat accumulation and atrial myocardial adipocyte infiltration due to increased body fatness. The Framingham heart study with CT analysis suggested that total amount of epicardial fat is associated with AF risk. These are potential mechanisms linking overweight, obesity, epicardial fat amount and AF that potentially leads to anisotropic conduction in the atrium wall, profibrotic adipokines leading to fibrosis formation, remodeling, inflammation and automatic nervous system (ANS) dysfunction. Since the imbalance of ANS represents one of the most important pathophysiological mechanisms in the genesis of AF. Positive modulation such as decreased obesity, physical activity and enhanced cardiorespiratory fitness are crucial for improving ANS function [45,46].
The metabolic disorders were tightly associated with adverse cardiac structural and dysfunctional remodeling. Epicardial fat may lead to structural and dysfunctional remodeling of the heart by both direct (e.g., by the infiltration of adipose tissue) and indirect mechanisms (e.g., by myocardial inflammation and oxidative stress) [47,48,49,50,51]. High-fat diets have been confirmed to be associated with dyslipidemia, overweight and obesity [26]. The retained lipids in tissues were considered to be responsible for the development of insulin resistance, impaired glucose tolerance and type 2 DM [52]. Insulin resistance leads to prevent cells from utilizing glucose for their energy supply, and forces them to utilize fat oxidation to provide their energy supply. As a result, more pro-inflammatory molecules were produced, while apoptosis and necrosis were increased in cardiomyocytes [53,54]. Then myocardial adverse remodeling and cardiac dysfunction occurred consequently [55,56,57,58]. Furthermore, high MLR has been proved to be associated with an increased risk of cardiac death [9,59]. However, to our knowledge, this is the first study to confirm that high MLR is associated with adverse cardiac remodeling and dysfunction in elderly with AF.
Higher MLR has been reported to be associated with the severity of coronary artery atherosclerotic stenosis in a study [60]. However, in our present study, the association of MLR with prevalent CHD has not been found. The association of MLR with the severity of CHD is needed to reconfirm furthermore in the future.
However, the present study is not without its limitations. Firstly, although this study noticed that the monocyte-to-lymphocyte ratio was associated with renal dysfunction and cardiac adverse remodeling, as this study was conducted in a single center, there is a possibility of selection bias, and therefore, caution should be exercised when generalizing the findings. Secondly, the retrospective nature of the study may have resulted in the presence of residual confounding factors, despite our attempts to adjust for possible confounders. The design was retrospective, and important data may be missing. The reasons for the missing data (especially those of estimated glomerular filtration rate and plasma albumin) were challenging to determine based on the available information. Inflammatory markers such as interleukins, cytokines were not measured in this study. Thirdly, this study included a moderate sample size and selection bias could not be avoided.
5. Conclusions
Our study suggested that high MLR is associated with male gender, decreased level of plasma albumin, low eGFR, cardiac adverse remodeling and dysfunction in elderly patients with AF. High MLR can be used as a marker of subclinical chronic kidney disease and adverse cardiac remodeling among AF patients.
Author Contributions
Conceptualization, X.C. and G.L.; formal analysis, X.C. and G.L.; investigation, X.C., L.W. and Y.L.; resources, G.L.; data curation, X.C. and G.L.; writing—original draft preparation, X.C. and G.L.; writing—review and editing, H.M. and J.A.L.; visualization, X.C. and G.L.; supervision, G.L. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by the Chongqing Medical Key Discipline and Regional Medical Key Discipline Development Project (No. 0201(2022) No.144 202325) and medical science & technology research fund of Health Bureau of Chongqing City, China (No. 2009-2-290).
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of the First Affiliated Hospital of Chongqing Medical University (No. 2022-K390).
Informed Consent Statement
The ethics committee waived the need for patients’ written informed consent because of anonymous nature of the clinical data acquired retrospectively.
Data Availability Statement
The authors confirm that all data generated in our study, and analyses are included in the published article and its supplementary files. Further details may be obtained from the co-author, XC, upon reasonable request. The data were included and referenced in the article.
Acknowledgments
We acknowledge the inpatient database established by The First Affiliated Hospital of Chongqing Medical University for supporting our work.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chung, S.C.; Sofat, R.; Acosta-Mena, D.; Taylor, J.A.; Lambiase, P.D.; Casas, J.P.; Providencia, R. Atrial fibrillation epidemiology, disparity and healthcare contacts: A population-wide study of 5.6 million individuals. Lancet Reg. Health Eur. 2021, 7, 100157. [Google Scholar] [CrossRef] [PubMed]
- Proietti, M.; Laroche, C.; Nieuwlaat, R.; Crijns, H.; Maggioni, A.P.; Lane, D.A.; Boriani, G.; Lip, G.Y.H. Registry E-AGP, Euro Heart Survey on AFI: Increased burden of comorbidities and risk of cardiovascular death in atrial fibrillation patients in Europe over ten years: A comparison between EORP-AF pilot and EHS-AF registries. Eur. J. Intern. Med. 2018, 55, 28–34. [Google Scholar] [CrossRef]
- Inciardi, R.M.; Giugliano, R.P.; Claggett, B.; Gupta, D.K.; Chandra, A.; Ruff, C.T.; Antman, E.M.; Mercuri, M.F.; Grosso, M.A.; Braunwald, E.; et al. Left atrial structure and function and the risk of death or heart failure in atrial fibrillation. Eur. J. Heart Fail. 2019, 21, 1571–1579. [Google Scholar] [CrossRef]
- Kartas, A.; Samaras, A.; Akrivos, E.; Vrana, E.; Papazoglou, A.S.; Moysidis, D.V.; Papanastasiou, A.; Baroutidou, A.; Botis, M.; Liampas, E.; et al. Tauhe association of heart failure across left ventricular ejection fraction with mortality in atrial fibrillation. ESC. Heart Fail. 2021, 8, 3189–3197. [Google Scholar] [CrossRef] [PubMed]
- Hu,Y. F.; Chen,Y.J.; Lin, Y.J.; Chen, S.A. Inflammation and the pathogenesis of atrial fibrillation. Nat. Rev. Cardiol. 2015, 12, 230–243. [Google Scholar] [CrossRef]
- Ihara, K.; Sasano,T. Role of inflammation in the pathogenesis of atrial fibrillation. Front. Physiol. 2022, 13, 862164. [Google Scholar] [CrossRef]
- Aulin, J.; Siegbahn, A.; Hijazi, Z.; Ezekowitz, M.D.; Andersson, U.; Connolly, S.J.; Huber, K.; Reilly, P.A.; Wallentin, L.; Oldgren, J. Interleukin-6 and C-reactive protein and risk for death and cardiovascular events in patients with atrial fibrillation. Am. Heart J. 2015, 170, 1151–1160. [Google Scholar] [CrossRef]
- Pol, T.; Hijazi, Z.; Lindback, J.; Oldgren, J.; Alexander, J.H.; Connolly, S.J.; Eikelboom, J.W.; Ezekowitz, M.D.; Granger, C.B.; Lopes, R.D.; et al. Using multimarker screening to identify biomarkers associated with cardiovascular death in patients with atrial fibrillation. Cardiovasc. Res. 2022, 118, 2112–2123. [Google Scholar] [CrossRef]
- Hua, Y.; Sun, J.Y.; Lou, Y.X.; Sun, W.; Kong, X.Q. Monocyte-to-lymphocyte ratio predicts mortality and cardiovascular mortality in the general population. Int. J. Cardiol. 2023, 379, 118–126. [Google Scholar] [CrossRef]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomstrom-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The task force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur. Heart J. 2021, 42, 373–498. [Google Scholar] [PubMed]
- ElSayed, N.A.; Aleppo, G.; Aroda, V.R.; Bannuru, R.R.; Brown, F.M.; Bruemmer, D.; Collins, B.S.; Hilliard, M.E.; Isaacs, D.; Johnson, E.L.; et al. Classification and diagnosis of diabetes: Standards of care in diabetes-2023. Diabetes Care 2023, 46 (Suppl 1), S19–S40. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Thiruvengadam, R. Hypertension in an ageing population: Diagnosis, mechanisms, collateral health risks, treatments, and clinical challenges. Ageing Res. Rev. 2024, 98, 102344. [Google Scholar] [CrossRef]
- Anderson, I.J.; Davis, A.M.; Jan, R.H. Management of gout. JAMA. 2021, 326, 2519–2520. [Google Scholar] [CrossRef] [PubMed]
- Miller, R.J.H.; Gransar, H.; Rozanski, A.; Dey, D.; Al-Mallah, M.; Chow, B.J.W.; Kaufmann, P.A.; Cademartiri, F.; Maffei, E.; Han, D.; et al. Simplified approach to predicting obstructive coronary disease with integration of coronary calcium: Development and external validation. J. Am. Heart Assoc. 2023, 12, e031601. [Google Scholar] [CrossRef]
- Serruys, P.W.; Morice, M.C.; Kappetein, A.P.; Colombo, A.; Holmes, D.R.; Mack, M.J.; Stahle, E.; Feldman, T.E.; van den Brand, M.; Bass, E.J.; et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N. Engl. J. Med. 2009, 360, 961–972. [Google Scholar] [CrossRef]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the prevention of stroke in patients with stroke and transient ischemic attack: A guideline from the American Heart Association/American Stroke Association. Stroke 2021, 52, e364–e467. [Google Scholar] [CrossRef]
- Miida, T.; Nishimura, K.; Hirayama, S.; Miyamoto, Y.; Nakamura, M.; Masuda, D.; Yamashita, S.; Ushiyama, M.; Komori, T.; Fujita, N.; et al. Homogeneous assays for LDL-C and HDL-C are reliable in both the postprandial and fasting state. J. Atheroscler. Thromb. 2017, 24, 583–599. [Google Scholar] [CrossRef]
- Keeling, D.M.; Wright, M.; Baker, P.; Sackett, D. D-dimer for the exclusion of venous thromboembolism: Comparison of a new automated latex particle immunoassay (MDA D-dimer) with an established enzyme-linked fluorescent assay (VIDAS D-dimer). Clin. Lab. Haematol. 1999, 21, 359–362. [Google Scholar] [CrossRef]
- Song, L.; Buggs, V.; Samara, V.A.; Bahri, S. Calculation of the estimated glomerular filtration rate using the 2021 CKD-EPI creatinine equation and whole blood creatinine values measured with radiometer ABL 827 FLEX. Clin. Chem. Lab. Med. 2022, 60, 867–876. [Google Scholar] [CrossRef]
- Song, X.; Li, G.; Zhu, Y.; Laukkanen, J.A. Glomerular filtration dysfunction is associated with cardiac adverse remodeling in menopausal diabetic Chinese women. Clin. Interv. Aging 2021, 16, 603–609. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Li, G.; Laukkanen, J.A.; Liu, C.; Song, X.; Zhu, Y. Low body mass is associated with reduced left ventricular mass in Chinese elderly with severe COPD. Sci. Rep. 2021, 11, 13074. [Google Scholar] [CrossRef]
- Zhu, Y.; Li, G.; Laukkanen, J.A.; Song, X.; Zhang, J.; Wei, L.; Chen, X.; Li, Y.; Liu, C. Higher neutrophil to lymphocyte ratio is associated with renal dysfunction and cardiac adverse remodeling in elderly with metabolic syndrome. Front. Cardiovasc. Med. 2022, 9, 921204. [Google Scholar] [CrossRef] [PubMed]
- Lang, R.M.; Badano, L.P.; Mor-Avi,V. ; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. Eur. Heart J. Cardiovasc. Imaging 2015, 16, 233–270. [Google Scholar]
- Li, Y.; Li, G.; Laukkanen, J.A.; Wei, L.; Chen, X. Higher LDL-C/HDL-C ratio is associated with elevated HbA1c and decreased eGFR levels and cardiac remodeling in elderly with hypercholesterolemia. J. Cardiovasc. Dev. Dis. 2024, 11. [Google Scholar] [CrossRef]
- Wei, L.; Laukkanen, J.A.; Li, Y.; Chen, X.; Li, G. Association of high apoB/apoA1 ratio with increased erythrocytes, platelet/lymphocyte ratio, D-dimer, uric acid and cardiac remodeling in elderly heart failure patients: A retrospective study. Int. J. Gen. Med. 2024, 17, 2151–2161. [Google Scholar] [CrossRef]
- Pan, L.; Shi, K.; Lv, J.; Pang, Y.; Guo, Y.; Pei, P.; Du, H.; Millwood, I.; Yang, L.; Chen, Y.; et al. Association of dietary patterns, circulating lipid profile, and risk of obesity. Obesity (Silver Spring) 2023, 31, 1445–1454. [Google Scholar] [CrossRef]
- Escasany, E.; Izquierdo-Lahuerta, A.; Medina-Gomez, G. Underlying mechanisms of renal lipotoxicity in obesity. Nephron 2019, 143, 28–32. [Google Scholar] [CrossRef] [PubMed]
- Sandino, J.; Martin-Taboada, M.; Medina-Gomez, G.; Vila-Bedmar, R.; Morales, E. Novel insights in the physiopathology and management of obesity-related kidney disease. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Ren, L.; Cui, H.; Wang, Y.; Ju, F.; Cai, Y.; Gang, X.; Wang, G. The role of lipotoxicity in kidney disease: From molecular mechanisms to therapeutic prospects. Biomed. Pharmacother. 2023, 161, 114465. [Google Scholar] [CrossRef] [PubMed]
- Diaz-Ricart, M.; Torramade-Moix, S.; Pascual, G.; Palomo, M.; Moreno-Castano, A.B.; Martinez-Sanchez, J.; Vera, M.; Cases, A.; Escolar, G. Endothelial damage, inflammation and immunity in chronic kidney disease. Toxins (Basel) 2020, 12. [Google Scholar] [CrossRef]
- Fornoni, A. Proteinuria, the podocyte, and insulin resistance. N. Engl. J. Med. 2010, 363, 2068–2069. [Google Scholar] [CrossRef] [PubMed]
- Cheng, T.; Wang, X.; Han, Y.; Hao, J.; Hu, H.; Hao, L. The level of serum albumin is associated with renal prognosis and renal function decline in patients with chronic kidney disease. BMC. Nephrol. 2023, 24, 57. [Google Scholar] [CrossRef]
- Liu, G.; Tao, L.; Zhu, Q.; Jiao, X.; Yan, L.; Shao, F. Association between the metabolic score for insulin resistance (METS-IR) and estimated glomerular filtration rate (eGFR) among health check-up population in Japan: A retrospective cross-sectional study. Front. Endocrinol. (Lausanne) 2022, 13, 1027262. [Google Scholar] [CrossRef]
- Ebert, T.; Neytchev, O.; Witasp, A.; Kublickiene, K.; Stenvinkel, P.; Shiels, P.G. Inflammation and oxidative stress in chronic kidney disease and dialysis patients. Antioxid. Redox. Signal. 2021, 35, 1426–1448. [Google Scholar] [CrossRef]
- Carrero, J.J.; Aguilera, A.; Stenvinkel, P.; Gil, F.; Selgas, R.; Lindholm, B. Appetite disorders in uremia. J. Ren. Nutr. 2008, 18, 107–113. [Google Scholar] [CrossRef]
- Zhang, M.; Wang, K.; Zheng, H.; Zhao, X.; Xie, S.; Liu, C. Monocyte lymphocyte ratio predicts the new-onset of chronic kidney disease: A cohort study. Clin. Chim. Acta 2020, 503, 181–189. [Google Scholar] [CrossRef]
- Xu, S.J.; Jiang, C.Q.; Zhang,W. S.; Cheng, K.K.; Schooling, C.M.; Xu, L.; Liu, B.; Jin, Y.L.; Hubert Lam, K.B.; Lam, T.H. Alcohol sensitivity, alcohol use and high-sensitivity C-reactive protein in older Chinese men: The Guangzhou biobank cohort study. Alcohol. 2016, 57, 41–48. [Google Scholar] [CrossRef]
- Lei, N.; Sun, Y.; Zhou, H.; Liu, Q.; Zhao, Y.; Yin, P.; Ping, P.; Fu, S. Relationships between smoking behavior, systemic inflammation, and myocardial infarction and their effects on long-term outcomes in older Chinese patients with coronary artery disease: A prospective study with a 10-year follow-up. MedComm (2020) 2023, 4, e240. [Google Scholar] [CrossRef] [PubMed]
- Mauriello, A.; Correra, A.; Maratea, A.C.; Caturano, A.; Liccardo, B.; Perrone, M.A.; Giordano, A.; Nigro, G.; D’Andrea, A.; Russo, V. Serum lipids, inflammation, and the risk of atrial fibrillation: Pathophysiological links and clinical evidence. J. Clin. Med. 2025, 14. [Google Scholar] [CrossRef] [PubMed]
- Alonso, A.; Yin, X.; Roetker, N.S.; Magnani, J.W.; Kronmal, R.A.; Ellinor, P.T.; Chen, L.Y.; Lubitz, S.A.; McClelland, R.L.; McManus, D.D.; et al. Blood lipids and the incidence of atrial fibrillation: The multi-ethnic study of atherosclerosis and the Framingham heart study. J. Am. Heart Assoc. 2014, 3, e001211. [Google Scholar] [CrossRef] [PubMed]
- Sha, R.; Baines, O.; Hayes, A.; Tompkins, K.; Kalla, M.; Holmes, A.P.; O’Shea, C.; Pavlovic, D. Impact of obesity on atrial fibrillation pathogenesis and treatment options. J. Am. Heart Assoc. 2024, 13, e032277. [Google Scholar] [CrossRef] [PubMed]
- Carna, Z.; Osmancik, P. The effect of obesity, hypertension, diabetes mellitus, alcohol, and sleep apnea on the risk of atrial fibrillation. Physiol. Res. 2021, 70 (Suppl4), S511–S525. [Google Scholar] [CrossRef]
- Latini, R.; Staszewsky, L.; Sun, J.L.; Bethel, M.A.; Disertori, M.; Haffner, S.M.; Holman, R.R.; Chang, F.; Giles, T.D.; Maggioni, A.P.; et al. Incidence of atrial fibrillation in a population with impaired glucose tolerance: The contribution of glucose metabolism and other risk factors. a post hoc analysis of the nateglinide and valsartan in impaired glucose tolerance outcomes research trial. Am. Heart J. 2013, 166, 935–940. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Y.; Xie, Z.; Li, J.; Chen, C.; Cai, W.; Dong, Y.; Xue, R.; Liu, C. Meta-analysis of metabolic syndrome and its individual components with risk of atrial fibrillation in different populations. BMC. Cardiovasc. Disord. 2021, 21, 90. [Google Scholar] [CrossRef]
- Mauriello, A.; Correra, A.; Maratea, A.C.; Caturano, A.; Liccardo, B.; Perrone, M.A.; Giordano, A.; Nigro, G.; D’Andrea, A.; Russo, V. Serum lipids, inflammation, and the risk of atrial fibrillation: Pathophysiological links and clinical evidence. J. Clin. Med. 2025, 14, 1652. [Google Scholar] [CrossRef]
- Wong, C.X.; Ganesan, A.N.; Selvanayagam, J.B. Epicardial fat and atrial fibrillation: Current evidence, potential mechanisms, clinical implications, and future directions. Eur. Heart J. 2017, 38, 1294–1302. [Google Scholar] [CrossRef]
- Thanassoulis, G.; Massaro, J.M.; O’Donnell, C.J.; Hoffmann, U.; Levy, D.; Ellinor, P.T.; Wang, T.J.; Schnabel, R.B.; Vasan, R.S.; Fox, C.S.; et al. Pericardial fat is associated with prevalent atrial fibrillation: The Framingham heart study. Circ. Arrhythm. Electrophysiol. 2010, 3, 345–350. [Google Scholar] [CrossRef]
- Tadic, M.; Ivanovic, B.; Cuspidi, C. Metabolic syndrome and right ventricle: An updated review. Eur. J. Intern. Med. 2013, 24, 608–616. [Google Scholar] [CrossRef]
- Saadeh, R.; Abu Jaber, B.; Alzuqaili, T.; Ghura, S.; Al-Ajlouny, T.; Saadeh, A.M. The relationship of atrial fibrillation with left atrial size in patients with essential hypertension. Sci. Rep. 2024, 14, 1250. [Google Scholar] [CrossRef]
- Zhong, J.; Huang, Z.; Tang, X.; Peng, L.; Zhang, A.; Zhang, H.; Li, S. Monocyte to high-density lipoprotein cholesterol ratio is associated with subclinical left cardiac remodeling and dysfunction in type 2 diabetes mellitus. Int. Heart J. 2022, 63, 524–530. [Google Scholar] [CrossRef] [PubMed]
- Chahal, H.; McClelland, R.L.; Tandri, H.; Jain, A.; Turkbey, E.B.; Hundley, W.G.; Barr, R.G.; Kizer, J.; Lima, J.A.C.; Bluemke, D.A.; et al. Obesity and right ventricular structure and function: The MESA-right ventricle study. Chest 2012, 141, 388–395. [Google Scholar] [CrossRef] [PubMed]
- Seko, Y.; Kato, T.; Haruna, T.; Izumi, T.; Miyamoto, S.; Nakane, E.; Inoko, M. Association between atrial fibrillation, atrial enlargement, and left ventricular geometric remodeling. Sci. Rep. 2018, 8, 6366. [Google Scholar] [CrossRef]
- Dahik, V.D.; Frisdal, E.; Le Goff, W. Rewiring of lipid metabolism in adipose tissue macrophages in obesity: Impact on insulin resistance and type 2 diabetes. Int. J. Mol. Sci. 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Lopaschuk, G.D. Fatty acid oxidation and its relation with insulin resistance and associated disorders. Ann. Nutr. Metab. 2016, 68, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Martinez, J.A. Mitochondrial oxidative stress and inflammation: An slalom to obesity and insulin resistance. J. Physiol. Biochem. 2006, 62, 303–306. [Google Scholar] [CrossRef]
- Larsen, T.S.; Jansen, K.M. Impact of obesity-related inflammation on cardiac metabolism and function. J. Lipid Atheroscler. 2021, 10, 8–23. [Google Scholar] [CrossRef]
- Saotome, M.; Ikoma, T.; Hasan, P.; Maekawa, Y. Cardiac insulin resistance in heart failure: The role of mitochondrial dynamics. Int. J. Mo.l Sci. 2019, 20. [Google Scholar] [CrossRef]
- Dahiya, R.; Shultz, SP.; Dahiya, A.; Fu, J.; Flatley, C.; Duncan, D.; Cardinal, J.; Kostner, K.M.; Byrne, N.M.; Hills, A.P.; et al. Relation of reduced preclinical left ventricular diastolic function and cardiac remodeling in overweight youth to insulin resistance and inflammation. Am. J. Cardiol. 2015, 115, 1222–1228. [Google Scholar] [CrossRef]
- Beyer, C.; Tokarska, L.; Stuhlinger, M.; Feuchtner, G.; Hintringer, F.; Honold, S.; Fiedler, L.; Schonbauer, MS.; Schonbauer, R.; Plank, F. Structural cardiac remodeling in atrial fibrillation. JACC. Cardiovasc. Imaging 2021, 14, 2199–2208. [Google Scholar] [CrossRef]
- Zhai, G.; Liu, Y.; Wang, J.; Zhou, Y. Association of monocyte-lymphocyte ratio with in-hospital mortality in cardiac intensive care unit patients. Int. Immunopharmacol. 2021, 96, 107736. [Google Scholar] [CrossRef]
- Chen, H.; Li, M.; Liu, L.; Dang, X.; Zhu, D.; Tian, G. Monocyte/lymphocyte ratio is related to the severity of coronary artery disease and clinical outcome in patients with non-ST-elevation myocardial infarction. Medicine (Baltimore) 2019, 98, e16267. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The monocyte / lymphocyte ratio in male and female.
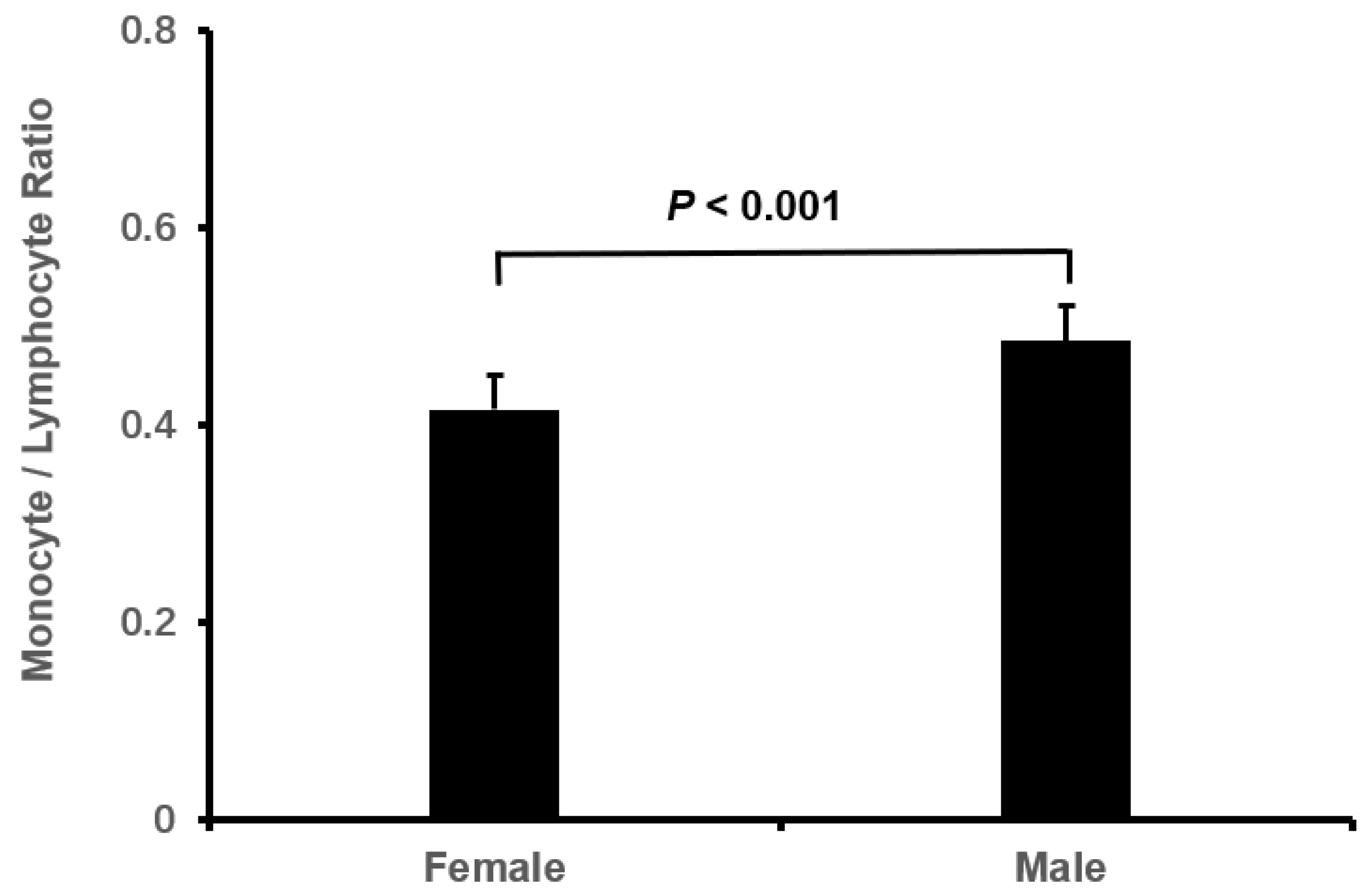
Figure 2.
The association of monocyte / lymphocyte ratio with plasma albumin.
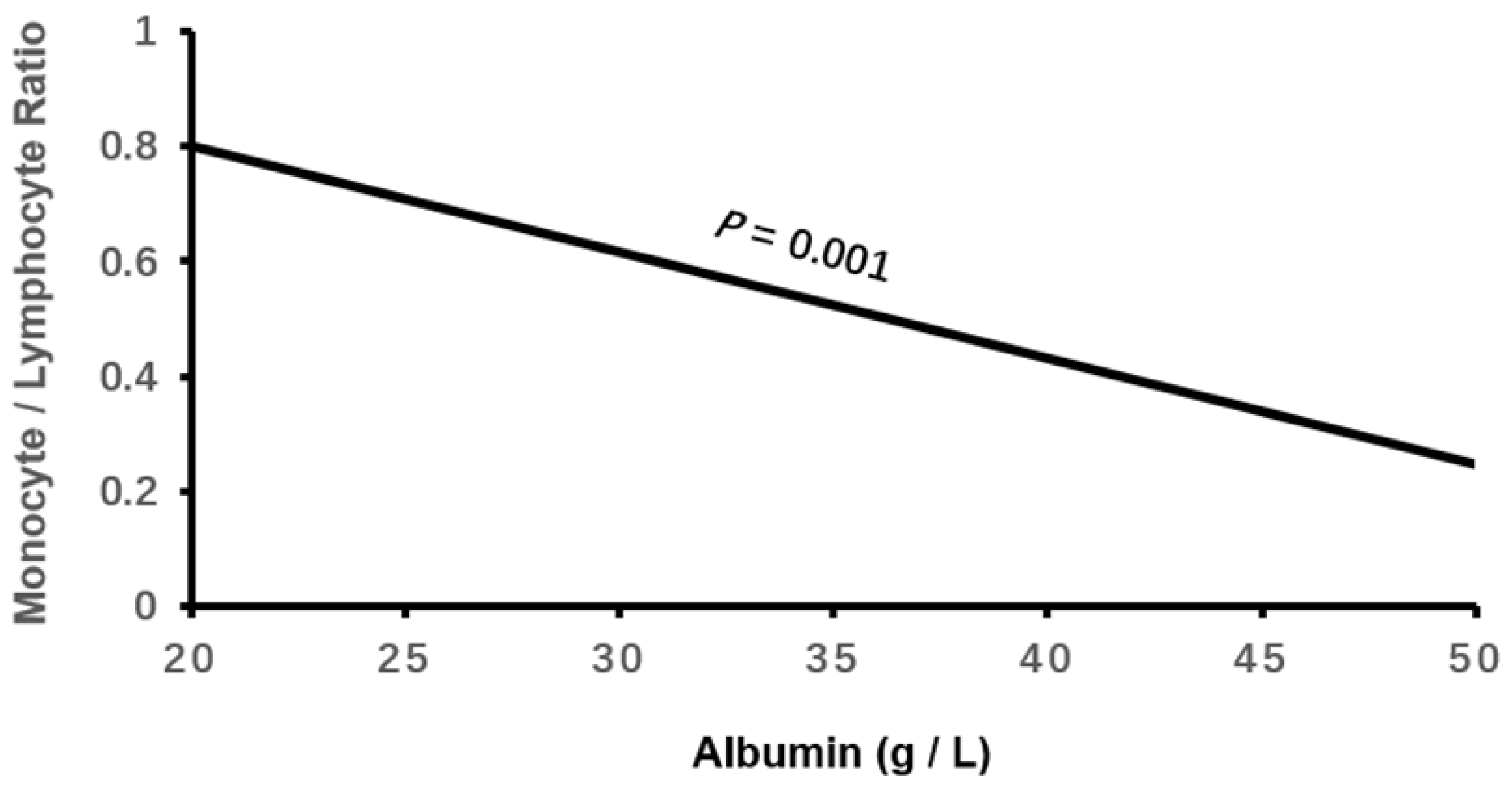
Figure 3.
The association of monocyte / lymphocyte ratio with estimated glomerular filtration rate.
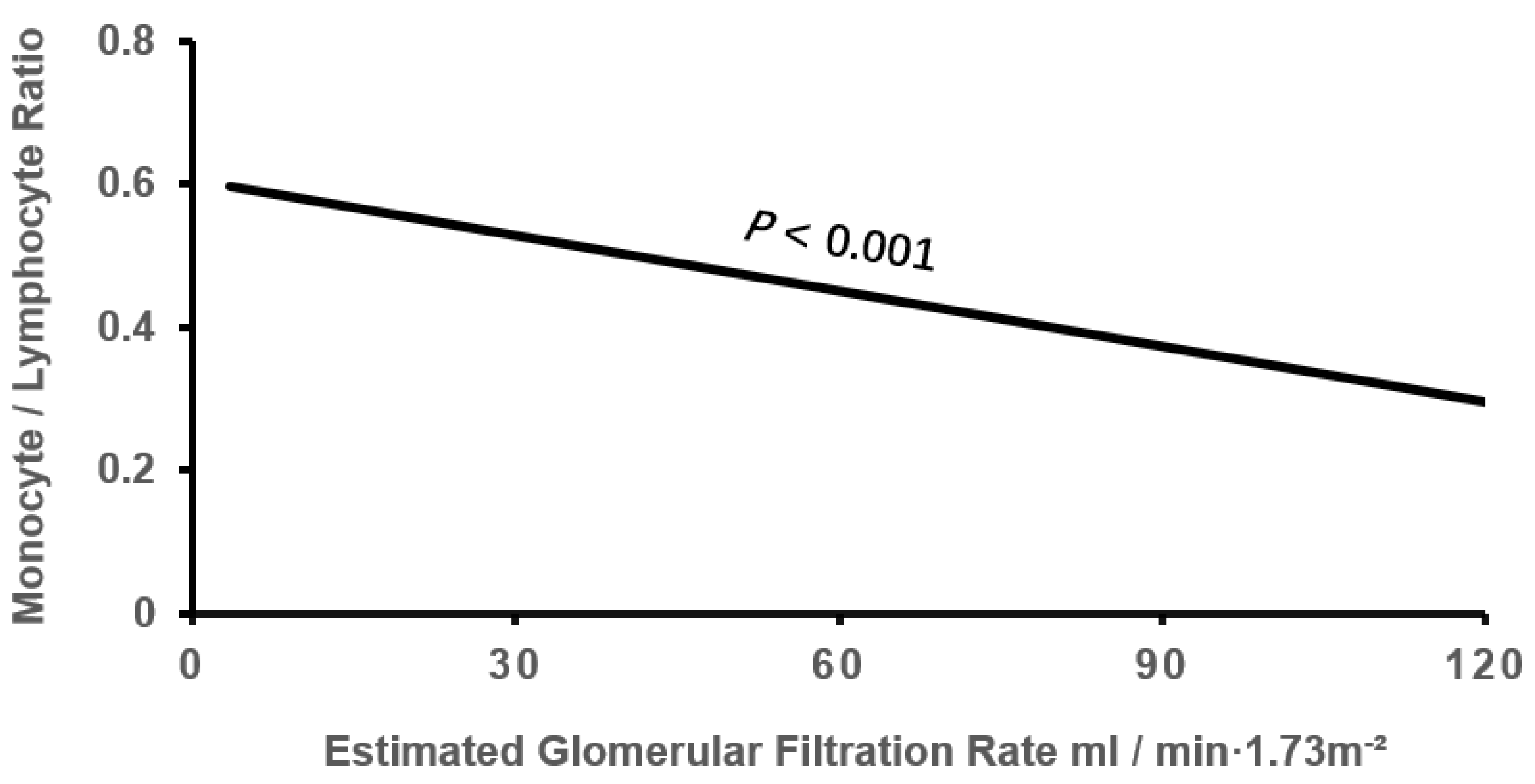
Figure 4.
The association of monocyte / lymphocyte ratio with right ventricular diameter.
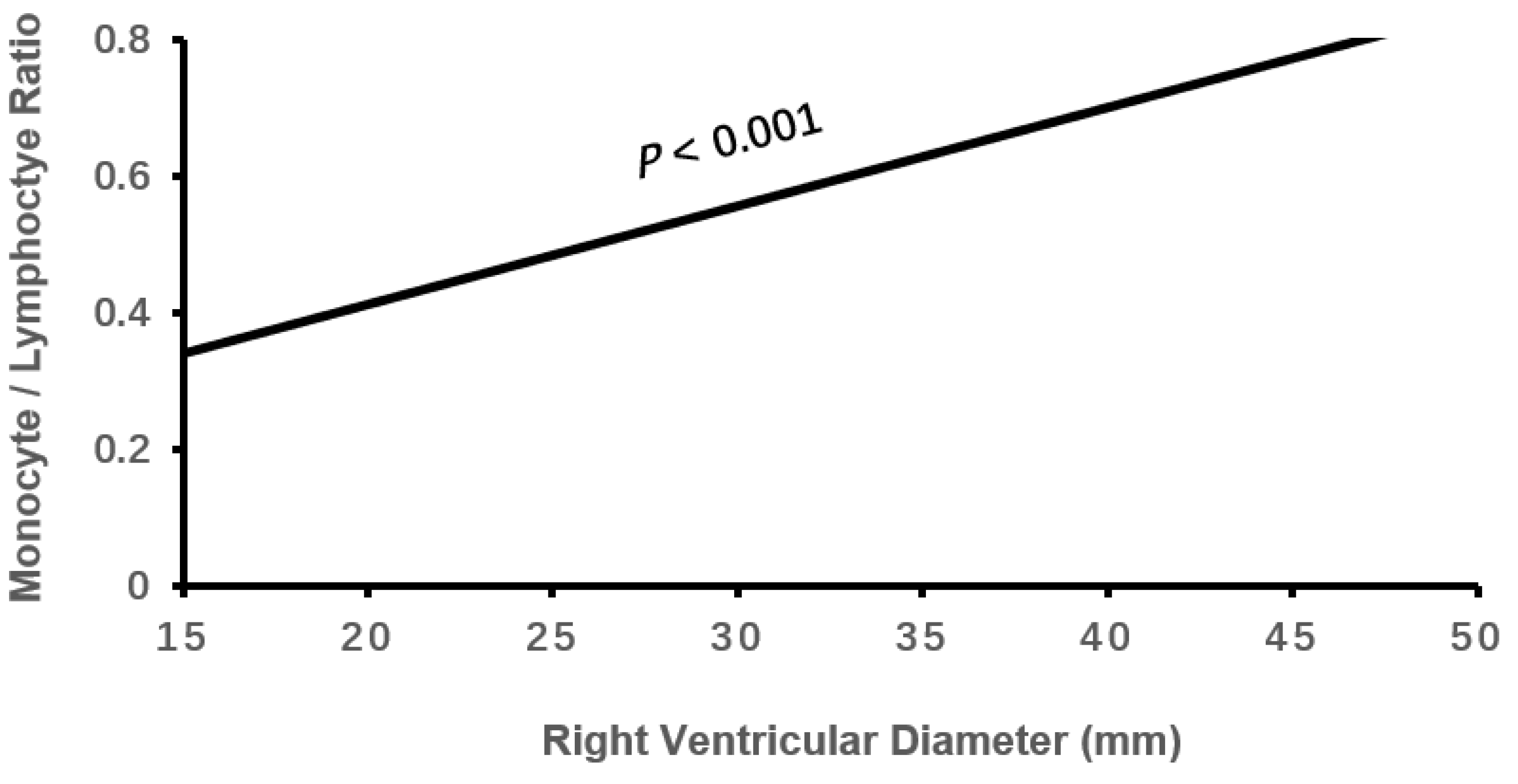
Figure 5.
The association of monocyte / lymphocyte ratio with left ventricular end-systolic diameter.
Figure 5.
The association of monocyte / lymphocyte ratio with left ventricular end-systolic diameter.
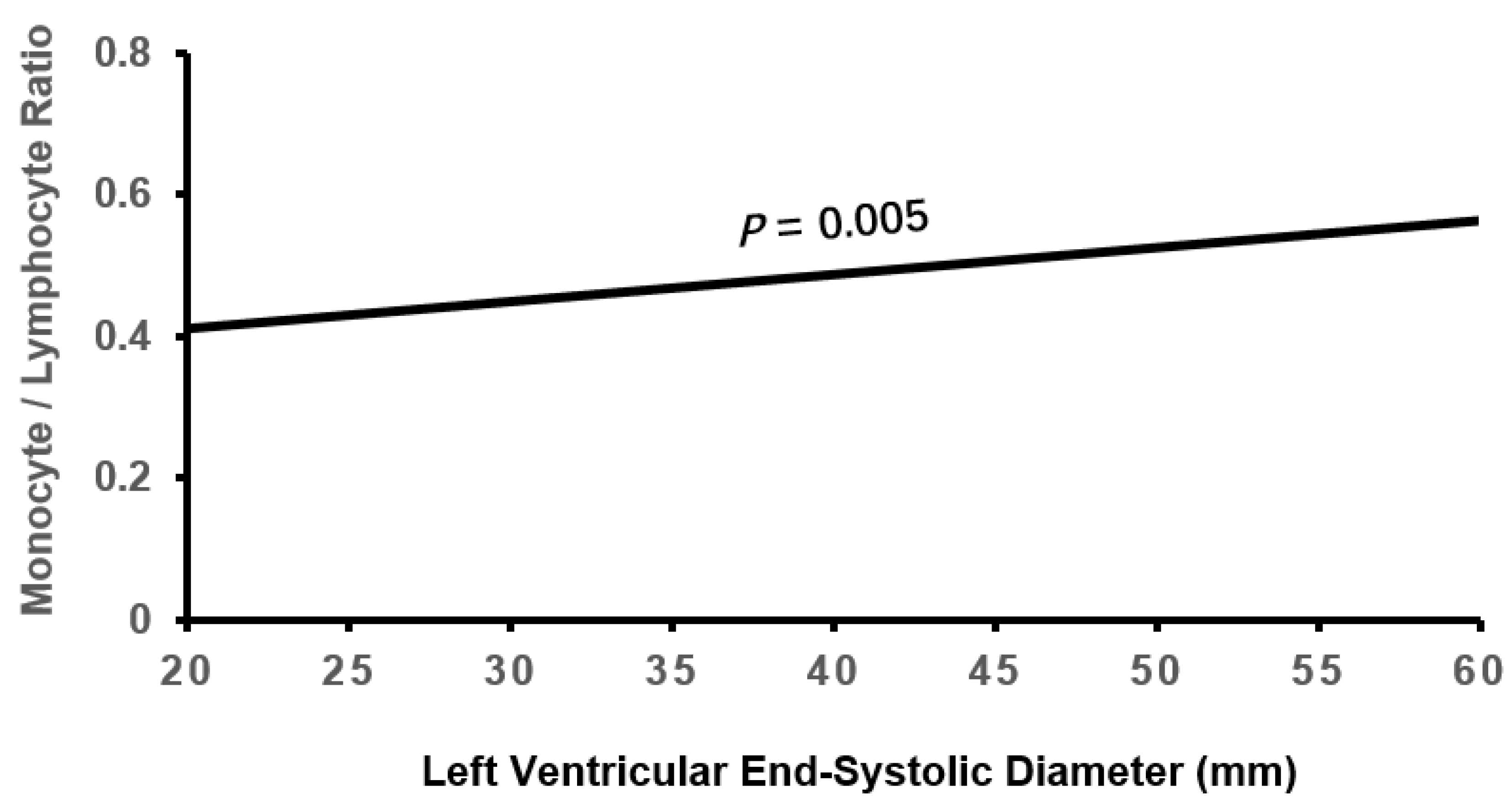
Figure 6.
The association of monocyte / lymphocyte ratio with left ventricular end-diastolic diameter.
Figure 6.
The association of monocyte / lymphocyte ratio with left ventricular end-diastolic diameter.
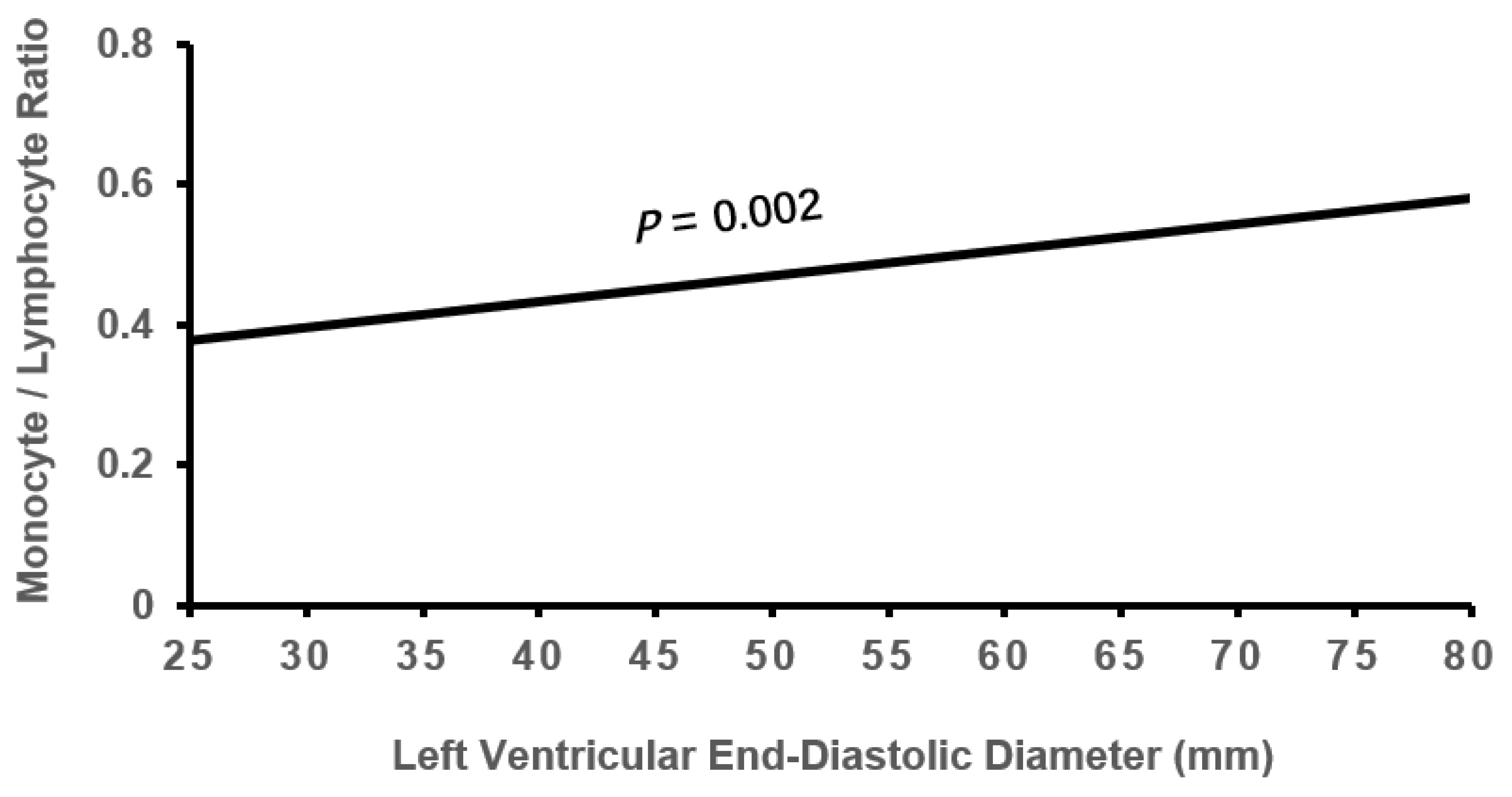
Figure 7.
The association of monocyte / lymphocyte ratio with left ventricular ejection fraction.
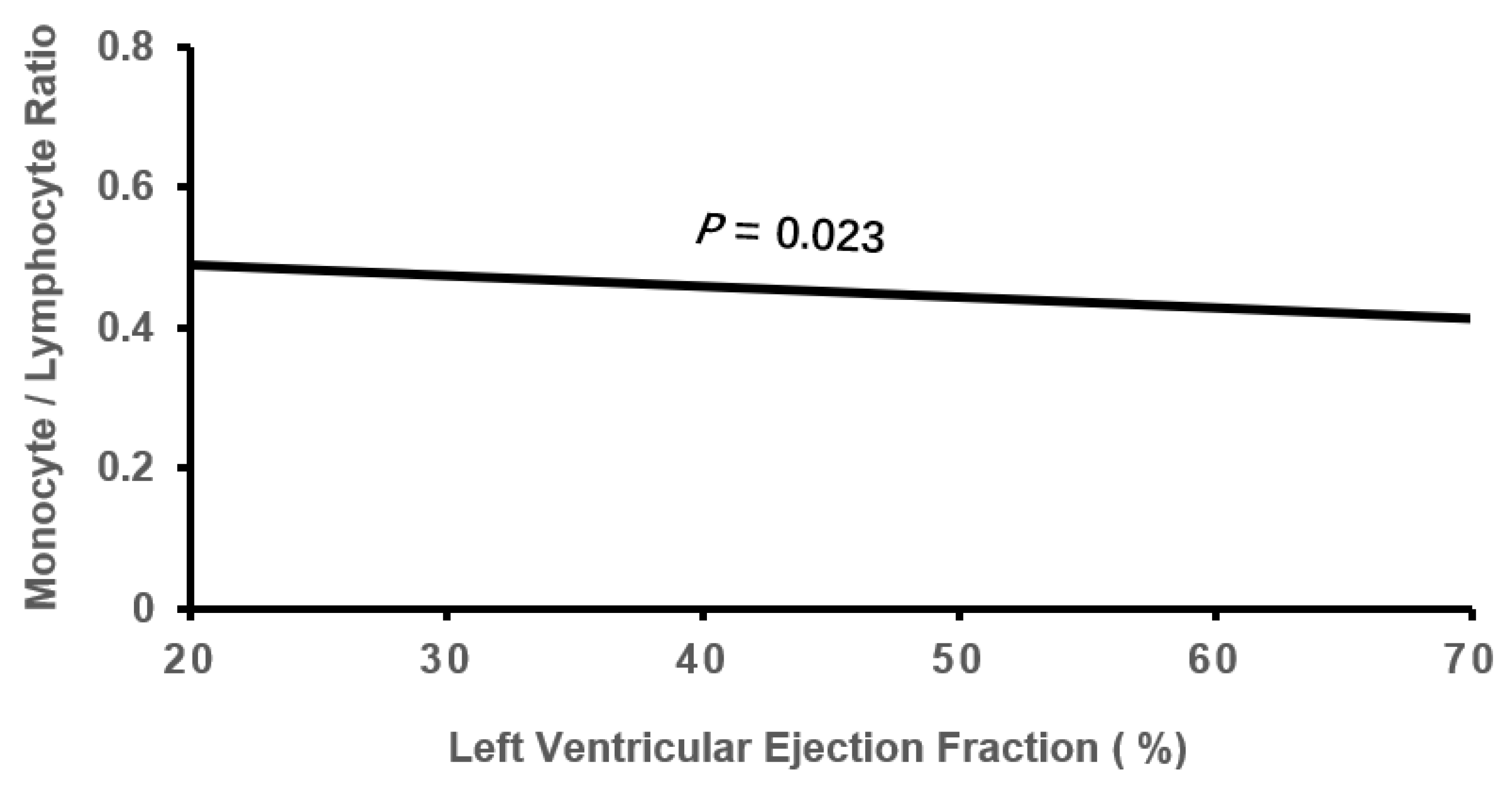

Table 1.
Comparison of clinical characteristics among tertile MLR groups.
| Low MLR | Moderate MLR | High MLR | r | P | |
| MLR ≤ 0.293 | 0.293 < MLR ≤ 0.460 | MLR > 0.460 | |||
| n=382 | n=392 | n=380 | |||
| MLR | 0.217 ± 0.05 | 0.36 ± 0.05* | 0.75 ± 0.38*† | 1 | <0.001 |
| male, n (%) | 132 (34.6) | 158 (40.3) | 199 (52.4)* | 0.146 | <0.001 |
| age, year | 76.93 ± 7.30 | 78.03 ± 6.71* | 80.22 ± 7.26*† | 0.185 | <0.001 |
| BMI, kg/m2 | 24.51 ± 3.90 | 23.95 ± 3.97* | 23.45 ± 4.26* | -0.112 | 0.001 |
| Smoking, n (%) | 73 (19.1) | 96 (24.5)* | 104 (27.4)*† | 0.079 | 0.024 |
| Drinking, n (%) | 45 (11.8) | 63 (16.1)* | 71 (18.7)*† | 0.078 | 0.028 |
| Systolic BP, mmHg | 132.02 ± 20.30 | 131.90 ± 21.49 | 130.76 ± 23.95 | -0.023 | 0.702 |
| Diastolic BP, mmHg | 80.50 ± 14.66 | 78.18 ± 15.13* | 76.09 ± 15.69 * | -0.117 | <0.001 |
| Persistent AF, n (%) | 193 (50.5) | 205 (52.3) | 198 (52.1) | 0.013 | 0.869 |
| Long term persistent AF, n (%) | 152 (39.8) | 142 (36.2) | 148 (38.9) | -0.007 | 0.569 |
| Permanent AF, n (%) | 37 (9.7) | 45 (11.5) | 34 (8.9) | -0.010 | 0.492 |
| Type 2 DM, n (%) | 120 (31.4) | 125 (31.9) | 126 (33.2) | 0.015 | 0.874 |
| DM duration, years | 2.64 ± 5.93 | 3.04 ± 6.81 | 3.36 ± 7.07 | 0.044 | 0.329 |
| Hypertension, n (%) | 278 (72.8) | 290 (74.0) | 264 (69.5) | -0.030 | 0.355 |
| Hypertensive duration, years | 9.87 ± 11.49 | 11.16 ± 12.26 | 11.16 ± 12.30 | 0.044 | 0.215 |
| Gout, n (%) | 7 (1.8) | 22 (5.6)* | 22 (5.8)* | 0.078 | 0.010 |
| Gout duration, year | 0.08 ± 0.92 | 0.38 ± 2.71 | 0.34 ± 2.27 | 0.050 | 0.103 |
| Coronary heart disease, n (%) | 166 (43.5) | 167 (42.6) | 185 (48.7) | 0.043 | 0.187 |
| Gensini score | 3.33 ± 9.48 | 4.01 ±11.23 | 3.97 ± 11.61 | 0.024 | 0.621 |
| Stroke, n (%) | 78 (20.4) | 98 (25.0) | 99 (26.1) | 0.054 | 0.151 |
| HbA1c, % | 6.37 ± 1.17 | 6.35 ± 1.17 | 6.46 ± 1.44 | 0.028 | 0.498 |
| Triglyceride, mmol/L | 1.30 ± 0.73 | 1.11 ± 0.75* | 1.07 ± 0.65* | -0.131 | <0.001 |
| LDL-C, mmol/L | 2.24 ± 0.81 | 1.98 ± 0.75* | 1.90 ± 0.72* | -0.181 | <0.001 |
| HLD-C, mmol/L | 1.23 ± 0.38 | 1.22 ± 0.37 | 1.13 ± 0.36*† | -0.114 | <0.001 |
| D-dimer, mmol/L | 0.90 ± 1.54 | 1.29 ± 2.40* | 1.47 ± 1.94* | 0.113 | 0.001 |
| Albumin, g/L | 40.97 ± 4.43 | 39.82 ± 4.61* | 37.57 ± 4.69*† | -0.289 | <0.001 |
| eGFR, mL/min/1.73m2 | 67.76 ± 19.19 | 63.27 ± 20.31* | 58.92 ± 24.56*† | -0.163 | <0.001 |
| hs-CRP, mg/L | 3.21 ± 4.93 | 4.97 ± 6.20 * | 9,12 ± 7.60 *† | 0.354 | <0.001 |
| monocyte, ×109/L | 0.37 ± 0.13 | 0.47 ± 0.14* | 0.60 ± 0.21 *† | 0.545 | <0.001 |
| Lymphocyte, ×109/L | 1.72 ± 0.59 | 1.30 ± 0.40 * | 0.89 ± 0.35*† | -0.674 | <0.001 |
| Neutrophil, ×109/L | 3.83 ± 1.25 | 4.05 ± 1.30* | 4.67 ± 1.59*† | 0.445 | <0.001 |
| White blood cell, ×109/L | 6.07 ± 1.53 | 5.97 ± 1.55 | 6.30 ± 1.73*† | 0.059 | 0.018 |
Values presented as mean ± SD or n (%). *p < 0.05 vs. Low MLR group; †p < 0.05 vs. Moderate MLR Group; MLR, Monocyte/lymphocyte ratio; BMI, Body mass index; DM, diabetes mellitus; BP, blood pressure; HbA1c, glycated hemoglobin; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; eGFR, estimated glomerular filtration rate; hs-CRP, high sensitivity C-reactive protein.
Table 2.
Comparison of echocardiographic parameters among tertile MLR groups.
| Low MLR group | Moderate MLR Group | High MLR group | r | P | |
| MLR≤0.293 | 0.293<MLR≤0.460 | MLR>0.460 | |||
| n=382 | n=392 | n=380 | |||
| RAD, mm | 41.94±5.32 | 43.56±6.75* | 44.75±6.82*† | 0.178 | <0.001 |
| RVD, mm | 20.60±3.06 | 21.34±3.44* | 22.30±4.40*† | 0.184 | <0.001 |
| LAD, mm | 39.96±6.09 | 41.09±6.04* | 41.92±6.15* | 0.129 | <0.001 |
| IVST, mm | 10.65±1.19 | 10.69±1.39 | 10.68±1.49 | 0.010 | 0.881 |
| LVPWT, mm | 10.48±1.13 | 10.52±1.26 | 10.52±1.28 | 0.012 | 0.875 |
| LVESD, mm | 33.45±6.23 | 33.95±7.00 | 35.33±8.08*† | 0.107 | 0.001 |
| LVEDD, mm | 47.66±6.01 | 48.44±6.90 | 49.61±7.94*† | 0.113 | 0.001 |
| PAP, mmHg | 39.04±10.22 | 40.40±10.23 | 43.54±12.26*† | 0.165 | <0.001 |
| LVEF, % | 58.38±8.30 | 58.05±8.79 | 56.15±9.79*† | -0.100 | 0.002 |
Values presented as mean ± SD. *P < 0.05 vs. Low MLR group; †P < 0.05 vs. Moderate MLR group; MLR, Monocyte/lymphocyte ratio; RAD, right atrial diameter; RVD, right ventricular diameter; LAD, left atrial diameter; IVST, interventricular septal thickness; LVPWT, left ventricular posterior wall thickness; LVESD, left ventricular end-systolic diameter; LVEDD, left ventricular end-diastolic diameter; PAP, pulmonary artery pressure; LVEF, left ventricular ejection fraction.
Table 3.
Regression analysis of clinically echocardiographic parameters with MLR>0.460.
| β | SE | Wald χ2 | P | OR (95%CI) | |
| Male | 1.173 | 0.292 | 16.192 | <0.001 | 3.233(1.825-5.725) |
| Age | 0.011 | 0.017 | 0.44 | 0.507 | 1.011(0.978-1.046) |
| BMI | -0.009 | 0.026 | 0.128 | 0.720 | 0.991(0.941-1.043) |
| Smoking | -0.344 | 0.383 | 0.804 | 0.370 | 0.709(0.334-1.503) |
| Drinking | -0.321 | 0.39 | 0.677 | 0.411 | 0.725(0.337-1.559) |
| Diastolic BP | -0.008 | 0.007 | 1.201 | 0.273 | 0.992(0.978-1.006) |
| Gout | 0.314 | 0.478 | 0.433 | 0.510 | 1.370(0.537-3.494) |
| Triglyceride | 0.174 | 0.211 | 0.684 | 0.408 | 1.190(0.788-1.800) |
| LDL-C | 0.063 | 0.155 | 0.163 | 0.686 | 1.065(0.786-1.442) |
| HDL-C | -0.186 | 0.318 | 0.341 | 0.559 | 0.831(0.446-1.549) |
| D-dimer | -0.027 | 0.07 | 0.147 | 0.701 | 0.974(0.849-1.116) |
| Albumin | -0.136 | 0.027 | 25.513 | <0.001 | 0.872(0.827-0.92) |
| eGFR | -0.013 | 0.005 | 5.852 | 0.016 | 0.987(0.977-0.998) |
| RAD | -0.021 | 0.023 | 0.851 | 0.356 | 0.979(0.936-1.024) |
| RVD | 0.105 | 0.036 | 8.486 | 0.004 | 1.110(1.035-1.192) |
| LAD | -0.016 | 0.022 | 0.562 | 0.453 | 0.984(0.943-1.026) |
| LVESD | -0.153 | 0.072 | 4.575 | 0.032 | 0.858(0.746-0.987) |
| LVEDD | 0.108 | 0.053 | 4.207 | 0.040 | 1.114(1.005-1.234) |
| PAP | 0.018 | 0.01 | 3.318 | 0.069 | 1.018(0.999-1.038) |
| LVEF | -0.071 | 0.029 | 6.239 | 0.012 | 0.931(0.880-0.985) |
MLR, Monocyte/lymphocyte ratio; β, regression coefficient; SE, standard error; Wald, Chi square value; CI, confidence interval; OR, odds ratio; BMI, Body mass index; BP, blood pressure; LDL-C, low-density lipoprotein cholesterol; HDL-C, high-density lipoprotein cholesterol; eGFR, estimated glomerular filtration rate; RAD, right atrial diameter; RVD, right ventricular diameter; LAD, left atrial diameter; LVESD, left ventricular end-systolic diameter; LVEDD, left ventricular end-diastolic diameter; PAP, pulmonary artery pressure; LVEF, left ventricular ejection fraction.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



