Submitted:
22 August 2025
Posted:
25 August 2025
You are already at the latest version
Abstract
Background/Objectives: Heart failure (HF) remains a leading cause of hospitalization and mortality worldwide, representing a significant burden on patients and healthcare systems. Despite advances in pharmacological and device-based therapies, readmission rates remain high, and traditional monitoring approaches often fail to detect early physiological deterioration. This review aims to critically examine current evidence on the clinical utility, cost-effectiveness, and implementation challenges of remote hemodynamic monitoring in HF management. Method: A comprehensive narrative review was conducted using PubMed, Scopus, and Web of Science databases to identify peer-reviewed English-language studies published in the past ten years. Results: Monitoring hemodynamic status is essential for preventing HF readmissions, as elevated filling pressures often precede symptoms. Previous studies suggest that traditional methods may be less effective in detecting early changes, which could contribute to delays in initiating treatment. Remote monitoring offers continuous, individualized assessment and has shown potential to reduce hospitalizations, though its effectiveness varies across populations and settings. Remote hemodynamic monitoring presents notable clinical advantages, although its widespread adoption faces several challenges (i.e., the invasiveness of some monitoring systems; limited patient adherence due to technical complexity or cognitive and physical barriers; variability in the efficacy of monitoring strategies across populations; difficulties faced by healthcare teams in managing and interpreting large volumes of real-time data; cost-effectiveness issues related to devices and infrastructure costs). Addressing these limitations will be essential to fully understanding the potential of remote monitoring in heart failure care. Conclusions: Remote hemodynamic monitoring enables early detection of physiological deterioration in HF, allowing timely interventions that reduce hospitalizations and improve outcomes. Emerging evidence suggests that, in contrast to traditional approaches, this method has the potential to support more personalized, data-driven care. Integrating biopsychosocial, gender, and intersectional perspectives further aligns this strategy with precision medicine, enhancing its effectiveness and equity in clinical practice. Despite promising recent advances, further research is essential to broaden the scientific evidence base and to enhance support for clinical decision-making.
Keywords:
Hemodynamic Monitoring
; Heart Failure
; HF
; Challenges
; Adherence
1. Introduction
Heart failure (HF) is a complex clinical syndrome that results from structural or functional impairments of the ventricles, ultimately leading to compromised systolic and/or diastolic performance and symptomatic left ventricular dysfunction. Clinically, it is primarily manifested through cardinal symptoms such as exertional dyspnea, fatigue, reduced exercise tolerance, and signs of fluid overload including peripheral edema and pulmonary congestion [1].
Beyond its clinical complexity, heart failure represents a major global and worldwide health challenge due to its high prevalence, significant morbidity and mortality, and recurrent hospitalizations. From an epidemiological perspective, it exerts a substantial burden on healthcare systems, particularly in aging populations, and is associated with poor long-term prognosis despite advances in pharmacological and device-based therapies. The progressive nature of heart failure and its frequent exacerbations highlight the urgent need for innovative strategies aimed at early detection, close monitoring, and individualized management [2].
Heart failure represents a critical public health concern in the world, requiring urgent attention and the implementation of effective healthcare policies [1,2,3]. Cardiovascular diseases are the leading cause of mortality worldwide, accounting for an estimated 17.9 million deaths in 2019. In Spain, more than 770,000 individuals are currently living with heart failure, with prevalence rates ranging from 4.7% to 6.8% among adults over the age of 45. Heart failure is responsible for over 25% of all hospital admissions due to cardiovascular conditions, underscoring its significant clinical and systemic impact. In-hospital mortality associated with heart failure exceeds 10%, rising to nearly 20% within the first-year post-discharge, and reaching 40% to 50% at five years [3].
From an economic perspective, heart failure imposes a substantial burden on the Spanish healthcare system. The estimated annual cost is approximately €2.5 billion, accounting for around 3.8% of total national health expenditure, with hospital-related costs alone surpassing €470 million. These figures highlight the urgent need to strengthen coordination across levels of care, develop robust preventive strategies, promote healthy lifestyle behaviors, and allocate sufficient resources to support the accreditation and operation of specialized heart failure units. In this context, advancing the use of remote hemodynamic monitoring may offer a promising strategy to optimize disease management, reduce preventable hospitalizations, and improve clinical outcomes in patients with heart failure [3].
Hemodynamic monitoring has emerged as a valuable strategy in reducing hospital readmissions among patients with heart failure by enabling early detection of decompensation and guiding proactive management. One of its primary advantages is related to its ability to detect subclinical congestion. Techniques such as pulmonary artery pressure monitoring can identify elevations in cardiopulmonary pressures well before the onset of overt symptoms, providing an essential timeframe for early therapeutic intervention. This early detection allows for timely optimization of treatment regimens, as hemodynamic data can inform clinicians’ decisions regarding adjustments in pharmacologic therapy based on predefined pressure thresholds. By maintaining patients within target hemodynamic ranges, this approach mitigates the progression of heart failure and decreases the likelihood of acute exacerbations requiring hospitalization [4].
In the same line, CardioMEMS is an FDA-approved remote hemodynamic monitoring system that uses a wireless sensor implanted in a pulmonary artery to measure hemodynamic pressures. This system has proven effective in reducing heart failure hospitalizations, as demonstrated in the CHAMPION trial, which showed a 28% reduction in heart failure admissions at 6 months, with sustained benefits beyond 2 years. The system enables patient management based on hemodynamic goals, independent of symptoms, providing an opportunity for early therapeutic interventions. It is applicable to both preserved and reduced ejection fraction patients, broadening its use across the heart failure population. However, it faces challenges such as the need for daily patient compliance to transmit data, the system’s cost, and the required infrastructure to monitor large numbers of patients. Additionally, it involves an invasive procedure for sensor implantation [4,5].
Similarly, evidence from clinical trials, such as the CHAMPION study [5,6], supports a protocol-driven model of care in which management decisions are based on hemodynamic targets rather than symptom severity alone. This strategy has been shown to significantly reduce hospital admissions by maintaining pulmonary artery pressures below high-risk thresholds. Moreover, by intervening during the early stages of hemodynamic deterioration, clinicians can prevent the development of symptomatic decompensation and avoid the need for acute hospital-based care. Notably, the benefits of hemodynamic monitoring extend across the heart failure spectrum, showing efficacy in patients with both preserved and reduced ejection fraction. Furthermore, these positive outcomes appear to be lasting over time, with sustained reductions in hospitalization rates and improved long-term clinical trajectories [4,5,6].
Remote monitoring, particularly wireless hemodynamic monitoring, has emerged as a valuable tool in the comprehensive management of heart failure. By enabling early detection of physiological deterioration, these technologies contribute to optimized patient care through timely therapeutic adjustments, ultimately reducing hospitalizations and enhancing quality of life. Clinical trials have demonstrated notable benefits in select populations; however, the heterogeneity of trial results underscores the relevance of linking remote device data to structured and effective clinical decision-making pathways. The utility of remote monitoring depends not only on technological capabilities but also on the ability to act upon the data in a timely and personalized manner [4,5,6,7].
Recent advances in cardiac device technology -characterized by increased miniaturization, improved automation, and greater patient usability- have positioned remote monitoring as a potentially indispensable component of modern heart failure care system. This evolution has been further accelerated by the shift toward virtual consultations and telehealth models, particularly during and following the COVID-19 pandemic. Looking ahead, future developments in artificial intelligence, machine learning, and real-time data integration are expected to enhance the predictive power and clinical utility of remote monitoring systems. These innovations will likely play a central role in enabling more proactive, personalized, and scalable approaches to heart failure management [7].
Despite its positive results up to date, the broader implementation of hemodynamic monitoring is challenged by factors such as the invasive nature of certain monitoring systems, patient adherence to monitoring protocols, and concerns about cost-effectiveness. Addressing these barriers will be essential to fully realizing the potential of hemodynamic-guided management in heart failure care [4,5,6].
Therefore, these comprehensive reviews aim to analyse the challenges and strategies of remote monitoring to reduce rehospitalizations in heart failure patients, highlighting its effectiveness and clinical relevance.
2. Materials and Methods
This study employed a comprehensive narrative review methodology to explore the current evidence on remote hemodynamic monitoring in the management of heart failure. A targeted search was conducted across PubMed, Scopus, and Web of Science databases, focusing on peer-reviewed articles published in English over the past ten years. To ensure comprehensiveness, illustrative examples from prior articles of substantial relevance were also considered in the review. The search strategy was developed using Medical Subject Headings (MeSH) terms to increase precision and consistency in the identification of relevant literature. The initial screening of studies was performed based on titles and abstracts, followed by a full-text review of the selected articles. The selection mainly focused on randomized controlled trials, cohort studies, and cost-effectiveness analyses related to remote hemodynamic monitoring technologies. A critical analysis of the included literature was carried out to synthesize findings and evaluate the methodological rigor and clinical relevance of each study, with the aim of addressing the primary objective of this comprehensive review.
3. Results
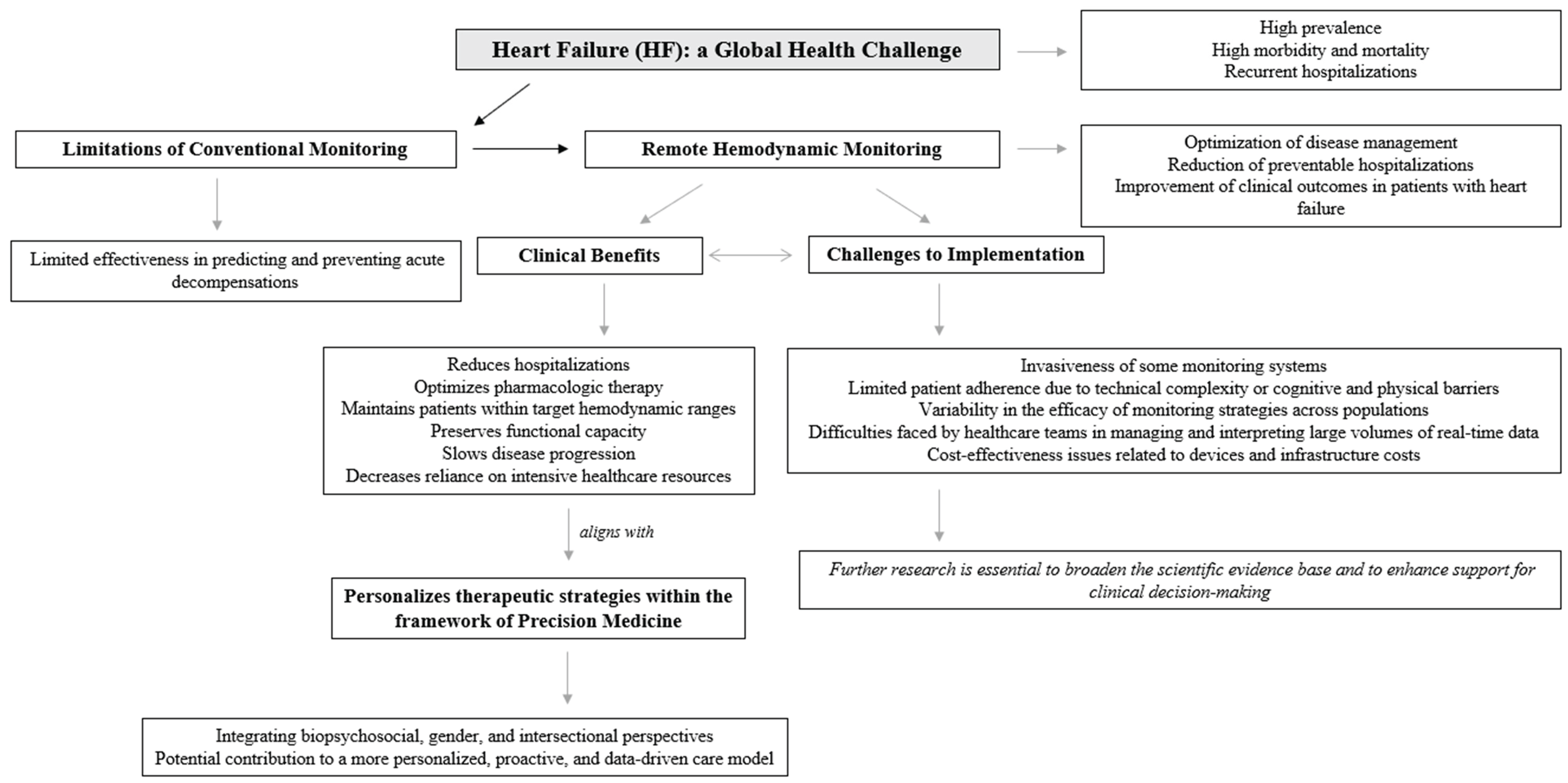
These comprehensive reviews analyse the challenges and strategies of remote monitoring to reduce rehospitalizations in heart failure patients, highlighting their effectiveness, challenges, and clinical relevance. Figure 1 provides a detailed conceptual map of remote hemodynamic monitoring in heart failure, derived from the present narrative review.
3.1. The role of Hemodynamic Monitoring in Heart Failure
Heart failure is a complex and heterogeneous clinical syndrome that presents significant challenges in preventing hospital readmissions, largely due to its chronic progression, clinical variability, and high burden of comorbidities. The condition encompasses both reduced and preserved ejection fraction phenotypes, each with distinct pathophysiological mechanisms and therapeutic responses, further complicating individualized treatment strategies. Patients with heart failure frequently present with multiple coexisting chronic conditions -such as chronic kidney disease, diabetes mellitus, and atrial fibrillation- which contribute to clinical instability and require the use of complex, often burdensome pharmacological treatments. Unlike acute cardiovascular events such as myocardial infarction, which are typically episodic in nature, heart failure requires continuous, long-term disease management and patient self-care. Following episodes of decompensation, patients often experience a progressive decline in functional capacity and quality of life, increasing their reliance on intensive healthcare resources. This downward clinical trajectory underscores the urgent need for integrated, proactive approaches that address not only the hemodynamic profile but also the broader biopsychosocial complexity of patients living with heart failure [8,9].
Hemodynamic monitoring plays a crucial role in the clinical management of heart failure by providing direct and continuous assessment of cardiopulmonary congestion and informing individualized therapeutic strategies. Among its most significant contributions is the ability to measure intrathoracic pressures, particularly pulmonary artery pressures, which are tightly correlated with the pathophysiological progression of heart failure. These measurements facilitate the early detection of decompensation before the onset of overt symptoms, enabling timely intervention and preventing clinical deterioration. Through the continuous tracking of hemodynamic parameters, clinicians can tailor pharmacologic and non-pharmacologic treatments to maintain values within predefined safe thresholds, thereby reducing the incidence of hospital readmissions and acute episodes [4]. Remote hemodynamic monitoring, such as CardioMEMS, has been found to be cost-effective in optimizing care for chronic heart failure patients, improving quality of life, and reducing hospitalizations [10].
Among the available technologies for remote hemodynamic monitoring, the CardioMEMS heart failure system is the most extensively studied and validated device to date. Multiple randomized controlled trials, including CHAMPION, GUIDE-HF, and MONITOR-HF, have consistently demonstrated that the use of CardioMEMS is associated with significant reductions in heart failure-related hospitalizations. These trials reported hospitalization rate reductions ranging from 28% to 44% across diverse clinical settings and healthcare systems, supporting the generalizability of the findings. Furthermore, real-world observational studies have supported these results, with some reporting reductions in hospitalization rates as high as 80%, underscoring the device’s potential when integrated into standard care pathways [11].
In addition to clinical effectiveness, cost-effectiveness analyses- predominantly focused on the CardioMEMS system- have shown favorable incremental cost-effectiveness ratios (ICERs), typically remaining below the commonly accepted threshold of $50,000 per quality-adjusted life year (QALY) gained. These favorable economic outcomes are largely attributed to the significant reduction in hospitalizations, which offset the upfront costs related to device implantation, infrastructure, and ongoing monitoring. While the majority of cost-effectiveness data is centred on CardioMEMS, emerging devices such as the Cordella heart failure system and the V-LAP monitoring system are currently under evaluation, with preliminary results indicating promising clinical and economic potential [12].
Successful implementation of remote hemodynamic monitoring in routine heart failure care depends on several critical factors, including appropriate patient selection, integration within multidisciplinary care models, and the use of structured telemonitoring platforms. Patients with moderate to severe heart failure symptoms- particularly those classified as New York Heart Association (NYHA) class III- appear to derive the greatest benefit from these interventions. Overall, remote hemodynamic monitoring represents a transformative advancement in the management of heart failure, with the potential to improve clinical outcomes, enhance quality of life, and reduce the long-term burden on healthcare systems [12].
The temporal advantage offered by hemodynamic monitoring lies in its capacity to identify changes in pressure and volume status that precede symptomatic worsening. This preclinical time framework is critical for implementing interventions aimed at stabilizing the patient and preventing progression to more severe states of decompensation. The efficacy of remote hemodynamic monitoring systems -such as the CardioMEMS device- has been well established in clinical trials, where they have consistently demonstrated significant and sustained reductions in heart failure-related hospitalizations. These benefits have been observed across a broad spectrum of patients, including those with preserved and reduced ejection fraction, underscoring the wide applicability of this approach in diverse heart failure phenotypes [2,5,13]. Overall, while remote monitoring technologies improve heart failure management and reduce hospitalizations, their impact on all-cause mortality remains modest, emphasizing the need for further advancements in monitoring and therapeutic strategies [10].
Nonetheless, the implementation of hemodynamic monitoring is not without challenges. The invasive nature of device implantation, the need for consistent patient adherence to daily measurements, and the reliance on well-resourced healthcare infrastructure can limit its feasibility and scalability in routine clinical practice. Despite these limitations, hemodynamic monitoring remains the most effective remote monitoring strategy currently available for reducing heart failure readmissions. Continued technological innovation and integration with personalized care models are necessary to address existing barriers and enhance clinical utility [4].
For remote monitoring strategies to be clinically effective in heart failure, the parameters employed must meet several essential criteria. These include high accuracy in detecting true hemodynamic deterioration without being confounded by other physiological processes, as well as strong sensitivity and specificity to reliably identify early warning signs and avoid unnecessary interventions. Moreover, the ideal parameters should allow for early detection that provides sufficient time for therapeutic adjustment, and they must be easy to measure on a regular basis without causing discomfort or disrupting patients’ daily routines. Notably, these parameters must yield actionable insights that can directly inform and guide clinical decision-making to improve outcomes [4].
Several categories of monitoring parameters have been explored in this context. Hemodynamic variables, such as pulmonary artery pressure, offer a direct reflection of central congestion and are among the most precise indicators of volume status. Bioimpedance analysis has also been employed to estimate fluid accumulation and systemic congestion. Additionally, biomarkers such as natriuretic peptides provide biochemical insights into myocardial stress and fluid overload. Conventional measures, including body weight, blood pressure, and heart rate, along with patient-reported symptoms, continue to be used but are limited by low sensitivity and specificity, especially in the early stages of deterioration. Ultimately, the choice of monitoring parameters must strike a balance between diagnostic accuracy, level of invasiveness, and practical feasibility for both patients and healthcare systems [4].
Remote monitoring has emerged as a valuable tool in the management of heart failure, particularly for reducing hospitalizations associated with disease decompensation. One of its principal advantages lies in the early detection of changes in intracardiac filling pressures, which are key indicators of impending clinical deterioration. Unlike traditional monitoring approaches- such as symptom tracking or daily weight measurements- remote hemodynamic monitoring provides direct and continuous physiological data that reflect the underlying pathophysiology of heart failure. Devices such as the CardioMEMS system have demonstrated the ability to detect subtle increases in pulmonary artery pressure several weeks before the onset of symptoms or hospital admission, offering a critical window for timely therapeutic intervention [12].
By enabling daily assessments of hemodynamic status, remote monitoring supports a proactive, individualized approach to pharmacological management. Clinicians can make small, frequent adjustments to medications such as diuretics, nitrates, and renin-angiotensin-aldosterone system antagonists in response to real-time changes in pressure, thereby maintaining optimal ventricular filling and preventing decompensation. This level of precision allows for targeted interventions that go beyond reactive symptom management and contributes to improved clinical stability. Furthermore, remote monitoring enhances communication between patients and healthcare providers, fostering continuous engagement and rapid response to hemodynamic shifts. Together, these mechanisms illustrate how remote hemodynamic monitoring offers a path toward more dynamic, responsive, and personalized heart failure care [12].
3.2. Adherence to Telemonitoring in Heart Failure Patients
Patient adherence to telemonitoring interventions for heart failure management is influenced by a range of interrelated factors that behavioral aspects, technical, and systemic domains. One significant barrier is the complexity associated with self-monitoring routines. Many patients struggle to understand and consistently follow self-care instructions, which contributes to low rates of compliance. The usability of telemonitoring systems also plays a critical role; platforms that are perceived as difficult to operate or that require substantial effort may discourage regular use. Additionally, when telemonitoring disrupts patients established daily routines, adherence may be further compromised [4,9,14,15].
Motivational and cognitive engagement are equally essential. A lack of awareness or understanding regarding the clinical relevance of telemonitoring can result in diminished patient participation. While ongoing support from healthcare providers -such as reminders or interactive follow-ups- has been proposed to enhance adherence, clinical trials have demonstrated only modest improvements using these strategies. Furthermore, technical limitations such as unreliable devices, intermittent connectivity, and data transmission failures can create feelings of frustration and hinder sustained use of telemonitoring systems [4,14,15].
Certain patient populations may also face intrinsic challenges to adherence. Individuals with physical disabilities or cognitive impairments often experience greater difficulties engaging with technology-dependent interventions. In addition, scepticism regarding the accuracy, relevance, and/or usefulness of the collected data may negative influence trust in the system, reducing the likelihood of consistent use. Addressing these challenges through the development of user-friendly interfaces, comprehensive patient education, and accessible technical support is essential to improving adherence rates and maximizing the clinical impact of telemonitoring in heart failure care [4,14,15].
Interventions designed to reduce heart failure readmissions should focus on identifying barriers to the implementation of guideline-directed medical therapy (GDMT) and on developing comprehensive strategies to overcome them [9].
3.3. Challenges in Remote Monitoring for Heart Failure
Despite the potential of remote monitoring to transform heart failure management, several critical challenges must be addressed to improve its clinical utility, scalability, and overall impact. One of the primary obstacles lies in the selection of appropriate monitoring parameters. Ideal parameters should offer high accuracy and sensitivity while enabling the early detection of worsening heart failure without being confounded by unrelated physiological changes. However, identifying such parameters remains a significant research and clinical challenge [4].
As we previously analyse, patient’s adherence represents another major limitation. Compliance with self-monitoring strategies is frequently suboptimal, often due to the complexity of the systems, technological barriers, and the degree of disruption they pose to patients’ daily routines. Reported adherence rates can be as medium or low varying from 35 to 9%, severely compromising the effectiveness of even the most sophisticated monitoring technologies [4,14,15].
At the same time, healthcare providers face substantial challenges in managing the volume and complexity of transmitted data. Large datasets generated by remote systems require timely and accurate interpretation, and failure to act appropriately on these insights can diminish the intended benefits of early intervention. Additionally, several technological limitations persist. For example, bioimpedance-based monitoring typically depends on the presence of implantable devices, thereby restricting its use to a subset of patients. Although non-invasive alternatives are in development, they have yet to demonstrate equivalent efficacy or reliability [4].
Efficacy also remains a central concern. Many commonly used remote monitoring strategies, including daily weight tracking, biomarker surveillance, and impedance measurements, have shown limited effectiveness in reducing heart failure-related hospitalizations in large-scale clinical trials. In contrast, remote hemodynamic monitoring systems such as CardioMEMS have demonstrated clear benefits in this regard, but their use requires invasive implantation procedures, which may not be appropriate or acceptable for all patients [2,5,13].
Moreover, the cost-effectiveness of advanced remote monitoring technologies remains under scrutiny. Devices such as CardioMEMS demand significant infrastructure for widespread implementation and ongoing management, raising concerns about their scalability in real-world healthcare settings. Furthermore, these systems often rely on patient-initiated actions -such as triggering daily measurements- which introduces another potential point of failure, as non-adherence can undermine the benefits of monitoring and compromise clinical outcomes [2,5,13].
The successful implementation of remote hemodynamic monitoring in heart failure care requires more than technological advancement; it necessitates the structural integration of these systems into routine clinical workflows, along with well-defined protocols for patient selection and efficient strategies for data management and clinical response. As this review has demonstrated, remote hemodynamic monitoring holds considerable potential to transform the management of heart failure by enabling earlier detection of decompensation, facilitating personalized therapeutic adjustments, and ultimately reducing hospitalizations and improving patient outcomes. However, realizing these benefits on a broad scale depends on the ability of healthcare systems to embed remote monitoring into multidisciplinary care models, ensure equitable access, and promote adherence through patient-centered approaches. Moving forward, the integration of remote hemodynamic monitoring into personalized, proactive heart failure care represents a meaningful step toward improving quality of life and reducing the overall burden of the disease [12].
In sum, these challenges underscore the need for further innovation and refinement in remote monitoring strategies for heart failure. Future efforts should focus on developing more accessible, reliable, and patient-friendly technologies that offer clinically actionable data while minimizing invasiveness and cost. Reaching an optimal equilibrium among accuracy, accessibility, and scalability will be critical to translating the theoretical benefits of remote monitoring into tangible improvements in heart failure outcomes.
Figure 1.
Remote hemodynamic monitoring in heart failure.
4. Discussion
Monitoring hemodynamic status and congestion plays a critical role in preventing hospital readmissions among patients with heart failure. Elevated intracardiac filling pressures, particularly in the pulmonary circulation, frequently precede the onset of clinical symptoms, providing a valuable opportunity for early detection and intervention before overt decompensation occurs. Traditional approaches based on symptom reporting or periodic assessments often fail to capture these early hemodynamic changes, resulting in delayed therapeutic action and increased risk of hospitalization. In this context, remote hemodynamic monitoring technologies have emerged as a promising strategy to enable continuous assessment of congestion and guide timely, individualized management. Clinical evidence suggests that such systems can significantly reduce heart failure-related hospital admissions by facilitating early therapeutic adjustments based on objective physiological data rather than relying solely on patient-reported outcomes or physical examination findings [8,9].
Reducing hospital readmissions appears to remain as a major challenge for the heart failure community, despite advances in pharmacological management and care coordination. While several remote monitoring strategies have been introduced with the aim of decreasing rehospitalization rates, their overall impact has been inconsistent across patient populations and clinical settings [4,10]. Differences in efficacy, limited patient access, technological complexity, and the financial burden associated with certain interventions-particularly those requiring invasive implantation or specialized infrastructure- represent significant barriers to widespread implementation [4]. Furthermore, disparities in digital literacy, adherence, and healthcare resource availability exacerbate these challenges, particularly among vulnerable or underserved populations. The development of more accessible, accurate, and cost-effective monitoring solutions that integrate physiological, psychological, and contextual data will be essential to overcoming these limitations. Future research should focus not only on technological innovation but also on health system integration, equity of access, and personalized care pathways. Ongoing progress in this area is indispensable for transforming remote monitoring from an emerging intervention into a clinically validated and widely implementable component of standard heart failure care [4].
Therefore, reducing hospital readmissions in heart failure remains a persistent and multifaceted clinical challenge. This difficulty stems largely from the progressive and relapsing nature of the disease, as well as the limited capacity to fully prevent recurrent decompensations. Heart failure is marked by high rates of early readmission following hospitalization, often within 30 days of discharge, and is associated with a steady decline in functional status and quality of life. The transition from stable chronic heart failure to acute decompensated heart failure is particularly concerning, as it dramatically increases the risk of adverse outcomes. Epidemiological data indicate that all-cause mortality rises from 6.4% to 23.6% within one year of an acute decompensation episode, reflecting the severity and fragility of this clinical trajectory [9,16,17,18].
Notably, recent analyses have challenged the assumption that readmissions are largely preventable. Estimates suggest that fewer than 25% of heart failure readmissions can be avoided through current interventions, highlighting the need to recalibrate expectations and strategies in managing post-discharge care. Moreover, although initiatives aimed at reducing 30-day readmission rates have yielded modest improvements in hospitalization metrics, they have coincided with a paradoxical 1.3% increase in short-term mortality. This unintended consequence raises important concerns about the validity of readmission-based performance benchmarks and underscores the need for more nuanced, patient-centered outcome measures that capture the complexity of disease progression and care transitions in heart failure [9,16,17,18].
These challenges underscore the necessity of strategic planning, targeted training, and appropriate resource allocation to support the successful integration of remote monitoring technologies into routine clinical practice. The adoption of such systems is not merely a matter of technological acquisition but requires a fundamental reconfiguration of existing care pathways. This includes the development of clear implementation protocols, the designation of clinical responsibilities within multidisciplinary teams, and the establishment of infrastructure for real-time data analysis and timely clinical decision-making. Additionally, healthcare professionals must receive adequate training to interpret hemodynamic data, adjust treatment regimens accordingly, and engage patients in the monitoring process to ensure adherence and optimize outcomes. From a systems perspective, adequate funding, institutional support, and alignment with broader health policy goals are essential to ensure long-term sustainability. Without addressing these organizational and operational dimensions, the clinical benefits demonstrated in controlled trials may not be fully achieved in real-world settings [12,19].
Moreover, given the multifactorial nature of heart failure and the complexity of remote hemodynamic monitoring, there is a growing need to adopt a comprehensive biopsychosocial approach to patient management. While current strategies emphasize physiological parameters such as pulmonary artery pressure and cardiac output, long-term adherence and clinical success are also related to behavioral, psychological, and social factors. Patient engagement with self-monitoring technologies, understanding of their clinical condition, emotional responses to chronic disease management, and the presence of supportive healthcare and social networks also play a critical role in the effective implementation of remote monitoring strategies. Integrating these psychosocial dimensions into heart failure care models not only enhances patient adherence and outcomes but also aligns monitoring interventions with the principles of personalized and precision medicine [20]. Future research and clinical protocols should therefore prioritize transdisciplinary collaboration and the inclusion of psychological science frameworks alongside technological innovation.
In addition to the biopsychosocial perspective, incorporating a gender-sensitive and intersectional approach [21] is essential for advancing equity and effectiveness in remote hemodynamic monitoring for heart failure. Evidence increasingly indicates that sex and gender differences influence not only the epidemiology and pathophysiology of heart failure but also patients’ access to care, engagement with health technologies, and clinical outcomes. Women, for instance, are often underrepresented in clinical trials and may experience different symptom profiles and treatment responses compared to men. Moreover, intersectional factors such as age, socioeconomic status, ethnicity, education, and caregiving responsibilities can further shape how individuals experience heart failure and interact with monitoring systems. Ignoring these dimensions risks reinforcing existing disparities and limiting the applicability of monitoring interventions across diverse patient populations. Therefore, research and clinical implementation efforts must systematically consider gender and intersectionality to ensure that remote monitoring strategies are inclusive, equitable, and responsive to the complex realities of those living with heart failure.
These considerations are closely aligned with the Sustainable Development Goals (SDGs), particularly Goal 3, which advocates for universal health coverage and access to quality essential healthcare services, and Goal 5, which emphasizes gender equality and the empowerment of all women and girls. By integrating biopsychosocial, gender-sensitive, and intersectional frameworks into remote hemodynamic monitoring strategies, healthcare systems can contribute to reducing health disparities and promoting equitable, person-centred care in line with global development priorities.
Related to the clinical implications of these findings, the integration of remote hemodynamic monitoring into clinical practice has the potential to significantly transform the management of heart failure by shifting from a reactive to a proactive care model. Clinical implementation of these technologies enables early identification of hemodynamic deterioration, facilitating timely pharmacological adjustments and reducing the incidence of acute decompensations and hospital readmissions. For clinicians, this means moving beyond symptom-driven management toward data-informed decision-making that is tailored to the individual physiological profile of each patient. To achieve these benefits, healthcare systems must establish dedicated protocols for incorporating remote monitoring into routine workflows, including appropriate patient selection; particularly those with persistent congestion, recurrent hospitalizations, or functional class III symptoms-and clear pathways for clinical response.
Furthermore, successful adoption requires the development of interdisciplinary care teams trained in the interpretation of remote hemodynamic data and supported by digital infrastructures that ensure efficient communication between patients and providers. Clinical practice must also address challenges related to patient engagement, digital literacy, and adherence, particularly in vulnerable populations such as older adults or people with limited access to technology. Additionally, the incorporation of remote monitoring into heart failure management aligns with the broader goals of precision medicine by enabling individualized care based on real-time physiological data. Accordingly, clinicians should be equipped not only to interpret this information but also to act upon it in a timely and appropriate manner, supported by evolving clinical guidelines, institutional infrastructures, and reimbursement frameworks that acknowledge the value of technology-enabled chronic disease management.
In summary, remote hemodynamic monitoring is currently one of the most effective strategies for reducing heart failure readmissions, nevertheless, all remote monitoring methods face challenges related to adherence, sensitivity, invasiveness, and cost. Future research needed to address these barriers and improve outcomes for the broader heart failure population.
Future research also should prioritize the integration of remote hemodynamic monitoring into standardized, multidisciplinary care pathways to determine its effectiveness across broader patient populations and healthcare settings. Large-scale, pragmatic clinical trials are needed to evaluate not only hospitalization and mortality outcomes, but also long-term effects on quality of life, functional capacity, and healthcare resource utilization. A particular emphasis should be placed on identifying which patient subgroups derive the greatest benefit from remote monitoring technologies, considering variables such as age, sex, comorbidities, socioeconomic status, and digital health literacy. Additionally, efforts should focus on improving the clinical interpretability and actionability of remotely acquired data, including the development of dynamic algorithms that integrate hemodynamic parameters with biomarkers, symptom reports, and behavioral metrics.
Emerging opportunities include the application of artificial intelligence to enhance predictive modeling and real-time clinical decision support, as well as the continued miniaturization and automation of devices to improve usability and patient adherence. Future studies should also explore the cost-effectiveness of remote monitoring in routine clinical practice and assess its alignment with value-based care models. Notably, an intersectional and gender-sensitive approach must be incorporated into future research frameworks to ensure equitable access, reduce disparities, and enhance the relevance of interventions across diverse populations. As remote monitoring technologies evolve, their success will ultimately depend on efficient integration into personalized care strategies supported by digital infrastructure, training, and policy-level engagement.
5. Conclusions
Remote hemodynamic monitoring has emerged as a promising strategy to reduce hospitalizations related to heart failure and to improve overall patient outcomes. Despite significant advancements in pharmacological and device-based therapies, conventional approaches to heart failure management have shown limited effectiveness in predicting and preventing acute decompensations. Traditional monitoring, often reliant on symptoms and periodic clinical evaluations, frequently fails to identify early hemodynamic deterioration, resulting in missed opportunities for timely intervention. In contrast, remote hemodynamic monitoring offers a proactive model of care by detecting subtle increases in intracardiac filling pressures; often weeks before the onset of clinical symptoms that typically prompt hospitalization. This early physiological insight enables clinicians to initiate tailored pharmacological adjustments and optimize volume status before patients reach a critical point of decompensation. As such, remote monitoring represents a key advancement in the transition toward anticipatory, individualized, and data-driven heart failure management.
The integration of biopsychosocial, gender-sensitive, and intersectional perspectives into remote hemodynamic monitoring strategies aligns closely with the principles of precision medicine. Precision medicine seeks to tailor healthcare interventions to the unique biological, psychological, and social characteristics of each individual, moving beyond the traditional “one-size-fits-all” or “generic treatment” strategy. By considering not only hemodynamic and physiological parameters but also behavioral patterns, gender-related differences, and socio-contextual factors, clinicians can more accurately predict risk, personalize therapeutic targets, and improve adherence to monitoring technologies. Such multidimensional profiling enhances the capacity to deliver interventions that are both clinically effective and contextually relevant, thereby advancing a truly patient-centered model of care. Remote monitoring technologies, when embedded within this precision framework, offer a powerful platform for dynamic, individualized, and equitable heart failure management. Although recent advances have introduced promising alternatives, further investigation remains necessary to strengthen the scientific evidence base and to provide more robust support for clinical decision-making in this field.
Author Contributions
Carmen M. Galvez-Sánchez: Conceptualization; Formal analysis; Methodology; Roles/Writing - original draft; Writing - review & editing, Visualization; Resources; Project administration; Supervision; Validation; Visualization. Julio Á. Camacho-Ruiz: Conceptualization; Data curation; Formal analysis; Investigation; Methodology; Resources; Validation; Visualization; Roles/Writing - original draft; Writing - review & editing. Lorys Castelli: Investigation; Methodology; Resources; Validation; Visualization; Roles/Writing - original draft. Rosa M. Limiñana-Gras: Conceptualization; Formal analysis; Methodology; Roles/Writing - original draft; Writing - review & editing, Visualization; Resources; Project administration; Supervision; Validation; Visualization.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
This is a narrative review based on published literature. All referenced sources are publicly available, and any additional materials can be provided by the corresponding author upon request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Puggia, I.; Rowland, T.J.; Miyamoto, S.D.; Sinagra, G.; Mestroni, L. Molecular and Cellular Mechanisms in Heart Failure. In: Heart Failure in the Child and Young Adult. Jefferies, J.L.; Chang, A.C.; Rossano, J.W.; Shaddy, R.E.; Towbin, J.A., Eds.; Elsevier: Philadelphia, PA, USA, 2018; pp. 3–19.
- Azari, S.; Mousavi, S.H.; Markazi Moghaddam, N.; Rezapour, A.; Zargar Balaye Jame, S.; Kolivand, P.; Sarabi Asiabar, A. Cost-Effectiveness of Remote Cardiac Monitoring With the CardioMEMS Heart Failure System: A Systematic Review. Med. J. Islam. Repub. Iran 2023, 37, 16. [CrossRef]
- Sociedad Española de Médicos Generales y de Familia-SEMG.. Objetivo 2025: Insuficiencia cardíaca [Spanish Society of General Practitioners and Family Physicians (SEMG). Objective 2025: Heart Failure]. 2021. Available online: https://www.semg.es/images/2021/Noticias/objetivo_2025_insf.cardiaca.pdf URL (accessed on 21st August 2025).
- Emani, S. Remote Monitoring to Reduce Heart Failure Readmissions. Curr. Heart Fail. Rep. 2017, 14, 40–47. [CrossRef]
- Adamson, P.B.; Abraham, W.T.; Aaron, M.; Aranda, J.M. Jr.; Bourge, R.C.; Smith, A.; et al. CHAMPION trial rationale and design: the long-term safety and clinical efficacy of a wireless pulmonary artery pressure monitoring system. J. Card. Fail. 2011, 17, 3–10. [CrossRef]
- Abraham, W.T.; Adamson, P.B.; Bourge, R.C.; Aaron, M.F.; Costanzo, M.R.; Stevenson, L.W.; et al. Wireless pulmonary artery haemodynamic monitoring in chronic heart failure: a randomised controlled trial. Lancet 2011, 377, 658–666. [CrossRef]
- Lander, M.M.; Aldweib, N.; Abraham, W.T. Wireless Hemodynamic Monitoring in Patients with Heart Failure. Curr. Heart Fail. Rep. 2021, 18, 12–22. [CrossRef]
- Picano, E.; Gargani, L.; Gheorghiade, M. Why, when, and how to assess pulmonary congestion in heart failure: pathophysiological, clinical, and methodological implications. Heart Fail. Rev. 2010, 15, 63–72. [CrossRef]
- Goldgrab, D.; Balakumaran, K.; Kim, M.J.; Tabtabai, S.R. Updates in heart failure 30-day readmission prevention. Heart Fail. Rev. 2019, 24, 177–187. [CrossRef]
- Tabrizchi, R. Adequacy of Ambulatory Hemodynamic Assessments for Reducing All-Cause Mortality in Individuals With Heart Failure. Int. J. Heart Fail. 2024, 6, 149–158. [CrossRef]
- Tolu-Akinnawo, O.; Akhtar, N.; Zalavadia, N.; Guglin, M. CardioMEMS Heart Failure System: An Up-to-Date Review. Cureus 2025, 17, e77816. [CrossRef]
- Clephas, P.R.D.; de Boer, R.A.; Brugts, J.J. Benefits of remote hemodynamic monitoring in heart failure. Trends Cardiovasc. Med. 2024, 34, 468–476. [CrossRef]
- Kapelios, C.J.; Liori, S.; Bonios, M.; Abraham, W.T.; Filippatos, G. Effect of pulmonary artery pressure-guided management on outcomes of patients with heart failure outside clinical trials: A systematic review and meta-analysis of real-world evidence with the CardioMEMS Heart Failure System. Eur. J. Heart Fail. 2025, advance online publication. [CrossRef]
- Moser, D.K.; Doering, L.V.; Chung, M.L. Vulnerabilities of patients recovering from an exacerbation of chronic heart failure. Am. Heart J. 2005, 150, 984. [CrossRef]
- van der Wal, M.H.; Jaarsma, T.; Moser, D.K.; Veeger, N.J.; van Gilst, W.H.; van Veldhuisen, D.J. Compliance in heart failure patients: the importance of knowledge and beliefs. Eur. Heart J. 2006, 27, 434–440. [CrossRef]
- VanWalraven, C.; Jennings, A.; Forster, A.J. A meta-analysis of hospital 30-day avoidable readmission rates. J. Eval. Clin. Pract. 2012, 18, 1211–1218. [CrossRef]
- Nuckols, T.K.; Keeler, E.; Morton, S.; Anderson, L.; Doyle, B.J.; Pevnick, J.; Booth, M.; Shanman, R.; Arifkhanova, A.; Shekelle, P. Economic evaluation of quality improvement interventions designed to prevent hospital readmission. JAMA Intern. Med. 2017, 177, 975–985. [CrossRef]
- Crespo-Leiro, M.G.; Anker, S.D.; Maggioni, A.P.; Coats, A.J.; Filippatos, G.; Ruschitzka, F.; Ferrari, R.; Piepoli, M.F.; Delgado Jimenez, J.F.; Metra, M.; et al. European Society of Cardiology Heart Failure Long-Term Registry (ESC-HF-LT): 1-year follow-up outcomes and differences across regions. Eur. J. Heart Fail. 2016, 18, 613–625. [CrossRef]
- Buttar, C.; Lakhdar, S.; Nso, N.; Guzman-Perez, L.; Dao, T.; Mahmood, K.; Hendel, R.; Lavie, C.J.; Collura, G.; Trandafirescu, T. Meta-Analysis Comparing Outcomes of Remote Hemodynamic Assessment Versus Standard Care in Patients With Heart Failure. Am. J. Cardiol. 2023, 192, 79–87. [CrossRef]
- Bamba, H.; Singh, G.; John, J.; Inban, P.; Prajjwal, P.; Alhussain, H.; Marsool, M.D.M. Precision Medicine Approaches in Cardiology and Personalized Therapies for Improved Patient Outcomes: A systematic review. Curr. Probl. Cardiol. 2024, 49, 102470. [CrossRef]
- Crenshaw, K. Demarginalizing the Intersection of Race and Sex: A Black Feminist Critique of Antidiscrimination Doctrine, Feminist Theory and Antiracist Politics. Univ. Chic. Legal Forum 1989, 1, 139–167.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



