
Submitted:
22 August 2025
Posted:
25 August 2025
You are already at the latest version
Abstract
Background: Acute infections in children are prevalent and often lead to antibiotic overuse due to the lack of evidence-based alternative approaches. Phytotherapeutic and homeopathic treatments are frequently sought as alternative or adjunctive therapies. This scoping review aims to map the existing evidence on the efficacy and safety of these interventions in managing acute pediatric infections. Methods: A comprehensive literature search was conducted across multiple databases to identify studies assessing the use of phytotherapeutic and homeopathic remedies in children with acute infections. Gastrointestinal infections were not considered since the use of non-antibiotic treatments (probiotics) in these conditions has been widely addressed. Results: Phytotherapeutic agents demonstrated promising results in reducing symptom severity and duration. Data on homeopathic remedies were limited and inconsistent. Regarding safety, both interventions were generally well-tolerated, with few adverse events reported. No studies or very limited evidence were available for other acute infections such as urinary, dermatological, osteoarticular and nervous system infections. Conclusions: Phytotherapeutic interventions show potential as effective and safe options for managing acute respiratory tract infections. However, the evidence for other infectious conditions and for homeopathic treatments is very limited or inconsistent. Further high-quality, large-scale studies on different types of pediatric infections are needed.
Keywords:
infections
; children
; homeopathy
; phytotherapy
; immunostimulants
; natural remedies
1. Introduction
Acute infections are highly prevalent in childhood, encompassing a broad spectrum of conditions affecting various organ systems [1]. These infections pose a significant burden on both public health and healthcare systems worldwide and are typically caused by viral agents, although bacterial etiologies can also play a relevant role. Among these, dermatological infections [2], urinary tract infections (UTIs) [3], upper respiratory tract infections (URTIs) [4] are particularly common. Also, gastrointestinal (GI) and central nervous system (CNS) infections are particularly concerning due to their frequency and potential severity, respectively.
Acute pediatric infections present a diverse array of symptoms, including irritability, discomfort, and disruption to daily routines. These manifestations not only affect the child but also significantly impact parents and caregivers. Parents sometimes experience increased distress, worry, and anxiety when their child is ill and this emotional burden can lead to disruptions in family life, including changes in daily schedules and social activities [5,6]. While most of these illnesses are self-limiting, their management primarily focuses on symptom relief and preventing complications. Conventional pharmacological treatments, including antipyretics, analgesics, and antibiotics for bacterial infections, are commonly prescribed [7,8].
Nutraceuticals and dietary supplements might be potential adjunctive therapies in the management of these common pediatric conditions. According to the national and European definition, phytotherapy is the “science-based medicinal use of plants and preparations derived from them, in the treatment, alleviation, and/or prevention of disease or injury, according to recognized standards of quality, safety and efficacy” [9]. Natural remedies encompass various therapeutic approaches, including homeopathy, which derives from the Greek words “homoios” (similar) and pathos” (suffering). This system of medicine is grounded in the principle of similars: the idea that a substance capable of inducing symptoms in a healthy individual may stimulate the body’s self-healing mechanisms in someone exhibiting similar symptoms [10]. These substances may possess immunomodulatory, anti-inflammatory, antimicrobial properties, offering potential benefits in alleviating symptoms, supporting immune functions, and potentially reducing the duration of illness [11,12]. Despite their growing popularity and inclusion in integrative pediatric care, the efficacy and safety of phytotherapeutic and homeopathic remedies in children remain a topic of ongoing debate, as many products lack robust clinical validation and the quality of the available evidence is often inconsistent.
Recent concerns about antibiotic resistance, side effects of pharmacological treatments, and a growing preference for natural healthcare solutions have spurred interest in the use of homeopathic and phytotherapeutic alternative remedies for pediatric acute infections. A recent systematic review and meta-analysis [13] examined the role of minerals and vitamin supplementation in respiratory infections, revealing limited efficacy, with only modest benefits observed in certain contexts. However, the analysis primarily focused on respiratory infections and did not consider other common pediatric infections. It also excluded phytotherapeutic and homeopathic treatments.
This scoping review aims to synthesize the current literature on the use of phytotherapeutic and homeopathic remedies in managing acute infections in children. Specifically, it aims to evaluate the state of the art on the interventions in pediatric populations with acute infections. Furthermore, it aims to summarize the efficacy, safety, and mechanisms of action of these remedies in common pediatric illnesses, comparing them to conventional treatments or placebos. Finally, the review seeks to identify gaps in the literature and propose directions for future research on the role of nutraceuticals in pediatric acute infections.
2. Materials and Methods
This study was initially conceived as a systematic review (PROSPERO, CRD42025639694). However, during the exploratory phase and after a preliminary analysis of the available literature, it was deemed more appropriate to adopt a scoping review approach, as the evidence was too heterogeneous in terms of populations, interventions, study designs, and outcomes to allow for formal systematic synthesis. Additionally, data were entirely lacking in several relevant areas. The scoping review thus enabled us to map the breadth, nature, and gaps in the existing evidence
This scoping review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) 2020 guidelines (Figure 1). The methodological framework for scoping reviews was used, made up of five stages: identifying the research question, identifying relevant and recent studies, selecting studies, charting the data, and summarizing and reporting the findings.
2.1. Aims and Eligibility Criteria
This review sought to analyze the existing literature regarding the use of phytotherapeutic and homeopathic agents in the treatment of acute infections among children aged 0 to 18 years. Eligible studies were original articles published in English or Italian, focusing on acute infections. Included studies comprised randomized controlled trials, cohort studies, and case-control studies. We excluded papers published exclusively as abstract or research letters, studies involving adults, animals (non-human studies), ex vivo or in vitro research, opinion articles, editorials, non-comparative study designs, narrative reviews, and studies on pharmaceutical drugs. Papers addressing conditions without a clear context of infections were also ruled out. Gastrointestinal infections were not considered since the use of non-antibiotic treatments (e.g., probiotics) in these conditions has been already widely addressed [14].
2.2. Search Strategy
The following databases: Pubmed/MEDLINE, Embase, Web of Science, and CINAHL. The following terms were used to search the above databases: “infections”, “bacterial”, “viral”, “children”, “pediatric”, “pediatric community”, “pediatric population”, “homeopathy”, “phytotherapy”, “immunostimulants”, “natural remedies”. The full string employed for each database is reported in the online supplementary material. The search was conducted on December 20, 2024 and the literature search update was conducted on April 01, 2025. Two authors independently performed the initial selection of titles and abstracts, retrieved the full-text articles, and assessed their relevance. Any discrepancies during the full-text screening process were resolved through discussion between the two reviewers and, when necessary, with input from one of the lead investigators.
2.3. Data Extraction
Data extraction was carried out using an Excel dataset to collect information from the selected studies. The following data were extracted: name of the first author, year of publication, country, study design, sample size, age, ethnicity, relevant characteristics, type of infection, intervention, dose of intervention, duration, infection course, aims and outcomes, and results (including safety and tolerability). All data were independently extracted by two authors using a standardized form to ensure both consistency and accuracy throughout the process. Disagreements during this process were resolved through discussion or by consulting an additional reviewer.
2.4. Quality Assessment
The Cochrane Collaboration tool was used to assess the risk of bias (RoB) for RCTs, while the Strobe Statement was applied to evaluate observational studies. Two reviewers independently performed the quality assessment, evaluating the potential for bias in the literature and categorizing studies as “high risk,” “low risk,” or “unclear risk”.
2.5. Outcomes
The primary outcomes focus on the reduction in the duration and severity of symptoms, improvement in recovery rates, and decreased use of antibiotics.
The secondary outcomes assess the safety and tolerability of the phytotherapeutic, and homeopathic remedies used for the symptomatic treatment of infections in the pediatric population. These include monitoring for adverse effects, evaluating overall treatment adherence, and comparing tolerability profiles with standard pharmacological therapies.
2.6. Data Synthesis and Statistical Analysis
Characteristics of the included studies were reported using descriptive tables. A narrative synthesis of the key findings was performed. We divided the different nutraceuticals into two main groups: phytotherapeutic and homeopathic substances. For the treatment of URTIs, bee products, such as honey, propolis, and royal jelly, were considered phytotherapeutic elements, based on the indications in scientific literature.
3. Results
A total of thirty-five studies were identified, including two observational studies [18,23] and thiry-three randomized controlled trials [15,16,17,19,20,21,22,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49]. According to the World Bank classification [50], the two observational studies were conducted in high income level countries. Of the randomized controlled trials, 18 were conducted in high income level countries [15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32] , 15 in upper middle-income countries [33,34,35,36,37,38,39,40,41,42,43,44,45,46,47], and two in lower middle-income countries [48,49]. One multicenter study involved both high- and upper-middle income countries (Ukraine and Germany) [46].
3.1. Quality Assessment
In the two observational studies [18,23] both were assessed as having a low risk of bias based on title and abstract and on the introduction. However, the evaluation of study methods divided into study design, setting, participants, variables, data sources/measurement, bias, study size, quantitative variables, and statistical methods, revealed some concerns. Notably, one study [23] demonstrated a high risk of bias in the domain of bias, and the other [18] showed a high risk in statistical methods.
The assessment of the results section, which was organized into participants, descriptive data, outcome data, main results, and additional analyses, indicated that one study raised some concerns in other analyses, while the remaining sections showed a low risk of bias.
In terms of discussion, all three studies were assessed as having a low risk of bias in reporting key results. However, interpretation and generalizability showed some concerns. One study presented a high risk of bias in limitation.
Finally, the evaluation of funding sources found a low risk of bias across both observational studies [18,23].
Among the thirty-three randomized controlled trials, 24% (n=8) were identified as having low overall risk of bias regarding overall risk of bias, 67% (n=22) of the trials were assessed as having some concerns, and 9% (n= 3) were found to have a high risk of bias [15,22,32].
Regarding the randomization process, three studies [15,22,32] exhibited high risk of bias while eight studies [27,31,33,35,40,42,43,46] showed some concerns. For the domain assessing deviations from intended interventions, nine studies [16,17,22,28,33,39,44,47,48] showed some concerns, while the remainder were assessed as having a low risk of bias.
In terms of missing outcome data, only four studies [26,28,40,45] showed some concerns. For the measurement of the outcome, six studies [20,30,39,40,44] were found to have some concerns. Lastly, in the domain of selection of the reported results, fourteen studies [16,19,20,21,26,29,31,42,43,44,45,47,48,49] exhibited some concerns. Details of the quality assessment are presented in Supplementary Materials.
3.2. Efficacy
The available evidence suggests that certain complementary approaches might potentially contribute to symptom relief and support recovery in pediatric acute infections, either independently or alongside standard therapies. While some studies have indicated possible improvements in symptom duration and severity, these findings remain inconclusive due to variations in study design and product formulations. Additionally, the safety and tolerability profiles of these interventions appear to be generally favorable when used as adjunctive treatments. However, the heterogeneity of product composition and the methodological limitations of existing studies underscore the necessity for more rigorous and standardized research to clarify their efficacy and ensure their safe integration into pediatric infection treatments. Data on the efficacy of phytotherapeutic and homeopathic remedies according to the different infectious conditions are provided below.
3.3. URTIs
Numerous studies [15,16,17,24,27,28,29,32,33,35,38,40,41,42,44,45,49] have evaluated the efficacy of various herbal and homeopathic treatments for URTIs in children. These investigations encompass a range of natural substances, including Echinacea purpurea extract, Pelargonium sidoides, honey and other bee products, and a range of plant-derived extracts such as gentian root, vervain herb, elderflower (Sambuci flox), sorrel herb (Rumex herba), primrose flowers, Bambusae textilis McClure, Crocus sativus, Radix solms-laubachiae, Santali albi lignum, and Lagotis brevituba Maxim. These natural substances were evaluated for their potential in alleviating symptoms and shortening illness duration.
3.3.1. Phytotherapeutic Remedies
3.3.1. a Echinacea Purpurea Extract
Three clinical studies [28,29,32] investigated the efficacy of Echinacea purpurea in treating URTIs in children, yielding mixed results. Taylor et al. [29] performed an RCT involving 524 children aged 2 to 11 years. Their findings indicated no significant differences between the Echinacea and placebo groups concerning the duration or severity of URTI symptoms. Additionally, Echinacea use was associated with an increased risk of rash. Conversely, Spasov et al. [28] reported that Kan Jang, a fixed herbal combination, significantly reduced the duration of nasal secretion and congestion (p < 0.05) and accelerated recovery rates compared to the Echinacea group. Children treated with Kan Jang also exhibited a substantial reduction in the need for additional medications. Weishaupt et al. [32] examined an Echinacea purpurea extract in 79 children with cold episodes. The study observed a reduction in the mean number of cold episodes by up to 1.7 days (p =0.02), and a 4-6% decrease in antibiotic prescriptions. Higher doses of the extract led to improvements in symptoms such as runny nose, cough, and sore throat, although these findings were not statistically significant. Regarding school absenteeism, the high-dose group recorded 410 missed school days compared to 494 in the low-dose group.
Overall, the products described were well tolerated, with no serious adverse effects reported.
3.3.1. b Pelargonium sidoides
Five RCT studies [15,33,35,40,45] assessed the therapeutic efficacy of Pelargonium Sidoides in children and adolescents with conditions such as the common cold, nasal congestion, and acute tonsillopharyngitis. All studies reported improvements in respiratory symptoms, particularly in alleviating nasal congestion cough, and substantial reduction in the Tonsillitis Severity Score (TSS) [28,29,30]. Specifically, Patiroglu et al. [40] observed an increase in appetite among treated children (p = 0.022), while Gökçe et al. [35] noted a statistically notable reduction in cough frequency (p = 0.023). In all trials, the treatment was considered effective without adverse effects, suggesting a favorable safety profile for pediatric use.
3.3.1. c Honey and Bee Products
Seven studies investigated the efficacy of honey and other bee products [16,17,24,27,41,44,49] in treating children, focusing primarily on symptom severity and duration.
Specifically, Cohen et al. [17] and Waris et al. [49] reported improvements in cough severity and frequency, as well as overall health status, including enhanced sleep quality for both children and parents (p < 0.014, p< 0.018, respectively). In Cohen et al. [16], many children experienced complete resolution of cough symptoms within seven days of initiating supplementation. Peixoto et al. [41] evaluated a honey-bromelain combination in 60 children with irritative cough, comparing it to a placebo group. Both groups showed a reduction in cough episodes within 30 minutes of administration; however, these results were not statistically significant, aligning with the findings of Nishimura et al. [24].
Seçilmiş et al. [27] demonstrated an influential reduction in Canadian Acute Respiratory Illness and Flu Scale (CARIFS) scores in the treatment group receiving conventional antibiotics combined with various bee products compared to the antibiotic-alone group (p < 0.05). Lastly, Shadkam et al. [44] compared the effects of honey with dextromethorphan and diphenhydramine in children aged 24-60 months on their nightly cough. The study found statistically significant improvements in cough frequency and severity in the honey group compared to the control group. The different types of honey and bee products were well tolerated, with no adverse effects reported.
3.3.1. d Various Medical Plants
Two studies dealt with the effectiveness of medicinal plant combinations [38,43] in reducing the severity and duration of symptoms, as well as improving recovery rates in pediatric patients. Both studies also investigated the potential to reduce the duration of cough and rhinosinusitis-related symptoms and the need for antibiotic prescriptions.
Popovych et al. [43] did not yield statistically significant results but demonstrated good tolerability of the herbal formulation. In contrast, Luo et al. [38] reported that the treatment group experienced a significantly shorter time to cough resolution (p=0.003), with a median of 2 days compared to 3 days in the conventional treatment group (p < 0.001). Moreover, the 4-day cough resolution rate was higher in the treatment group (94.4%) than in the control group (74.6%, p = 0.001).
3.3.2. Homeopathic Remedies
Seven different studies [20,31,39,42,46,47] investigated the use of homeopathic remedies in the symptomatic treatment of URTIs, focusing on symptoms relief and severity. All studies reported positive outcomes regarding the effectiveness and safety of the treatments. Torbicka et al. [31] assessed a homeopathic combination containing Vincetoxicum hirundinaria in patients with RSV infection. They found that the average Symptom Intensity Score (SIS) was lower in the treatment group compared to the control group (3.0 ± 1.6), indicating greater symptom improvement. Malapane et al. [39] administered a homeopathic complex to a pediatric population with acute viral tonsillitis and observed a difference in mean pain ratings between the homeopathic and placebo group (U=38.000; p=0.001). Additionally, there was a notable decrease in mean tonsil scores in the treatment group compared to the placebo group. Van Haselen, Jacobs, and Voss et al. [20,46,47] observed reductions in symptom duration and significant improvements in symptoms such as runny nose, fever, and malaise. They also noted decreases in scores such as the Wisconsin Upper Respiratory Symptom Survey (WURSS-21) and CARIFS. Popovych et al. [42] treated a group of 238 children with BNO 1030 extract and showed improvements in various symptoms from day 1 to day 4, along with a reduction in antipyretic use.
3.4. Bronchitis
3.4.1. Phytotherapeutic Remedies
Several studies have investigated the efficacy of herbal and homeopathic treatments for pediatric bronchitis, focusing on symptom severity, particularly cough, and overall infection duration. Notably, research on herbal compounds has yielded significant findings, while evidence supporting homeopathic remedies remains limited.
Pelargonium sidoides, particularly the EPs 7630 extract, has been extensively studied for its effectiveness in treating acute bronchitis in children [18,21,23,34,36].
Haidvogl and Kamin et al. [18,21] found a significant reduction in the Bronchitis Severity Scale (BSS), from 6-0 ± 3.0 at baseline to 2.7 ± 2.5 after one week and 1.4 ± 2.1 by the end of the study (p < 0.001). Improvements were most pronounced for symptoms such as cough and pulmonary rales upon auscultation. The onset of therapeutic effects was rapid, with significant improvements observed as early as day 1-2 and 3-4 (p<0.0001). After 7 days of administration, the EPs 7630 exhibited a greater reduction in BSS compared to the placebo group, indicating both enhanced efficacy and a faster onset of symptom relief. Similarly, Chen et al. [34] reported that children treated with a multi-herbal extract formulation experienced a significant reduction in VAS scores after 7 days of treatment compared to controls (6.35 ± 3.45 vs. 3.73 ± 3.98; p < 0.001).
3.4.2. Homeopathic Remedies
No studies have been identified regarding the use of homeopathic products in children with acute lower respiratory tract infections.
3.5. Otitis
3.5.1. Phytotherapeutic Remedies
Articles have been identified that focus solely on the use of homeopathic remedies in the symptomatic treatment of otitis, while there is a lack of material concerning phytotherapeutics such as Echinacea, Pelargonium sidoides, and bee and other similar products.
3.5.2. Homeopathic Remedies
While herbal treatments have demonstrated efficacy in managing bronchitis, evidence supporting the use of homeopathic remedies for otitis media is limited. Several studies have explored the effects of homeopathic compounds such as Chamomilla, Belladonna, Agraphis nutans, Thuya occidentalis, and Kalium muriaticum, in pediatric patients with Acute Otitis Media (AOM) or otitis media with effusion [19,25,26,30,48]. However, only a few studies have assessed the relationship between these treatments and pain relief.
In a randomized, double-blind, placebo-controlled pilot study, Jacobs et al. [19] administered individualized homeopathic remedies to 75 children aged 18 months to 6 years with AOM. The study found a significant decrease in symptom scores within 24 to 64 hours following treatment, indicating a positive effect of homeopathy on symptom relief. However, the study also noted that the differences between the homeopathic and placebo groups were not statistically significant over the longer term.
Conversely, Sinha [48] conducted a trial comparing homeopathic treatment with conventional therapy in 81 children. The results showed limited efficacy of homeopathic treatment: by day 7, only 7.58% of children in the treatment group had recovered, compared to 53% in the conventional group (p=0.356); by day 10, recovery was observed in 10.9% of the homeopathic group versus 100% in the conventional group.
Pedrero-Escalas [25] evaluated the impact of homeopathic treatment on symptom relief in children. In the experimental group, 61.9% of children were cured compared to 56.8% in the placebo group, with no significant difference. Adverse events are similar, except for fewer URTIs in the first group (3 vs 13, p=0.001). Overall, homeopathic treatment showed no significant efficacy. Therefore, it cannot be considered an effective treatment for children with AOM.
3.6. Hand-Foot-Mouth Disease (HFMD)
3.6.1. Phytotherapeutic Remedies
Regarding HFMD, a viral illness, literature offers limited evidence. One of the most relevant studies is by Liu et al. [37], which evaluated the efficacy of Jinzhen oral liquid, a formulation containing Salgae tataricae cornu, Fritillaria usuriensis maxim, Scutellaria baicalensis georgi, and other herbal extracts, in a pediatric population of 399 children aged 1-7 years, over a 7-day period. The study assessed outcomes such as time to the first disappearance of oral ulcers and hand/foot vesicles and time to fever clearance. Results showed that children treated with Jinzhen experienced a significantly shorter time to symptom resolution compared to placebo (4.9 vs 5.7 days; p=0.0036), faster fever reduction (43.42 h vs 54.92 h; p=0.0161), and a 28.5% lower risk of persistent symptoms (p=0.0032).
3.6.2. Homeopathic Remedies
No studies have been identified regarding the use of homeopathic products in children with HFMD.
3.7. Flu
3.7.1. Phytotherapeutic Remedies
The only available data concerning the treatment of flu A with herbal medicine, specifically Mao-to, a traditional Japanese herbal remedy, comes from a study by Kubo [22]. This study observed the effectiveness of phytotherapeutic treatment in reducing the duration of symptoms, particularly fever. In the study, 24 children of the treated group were administered only Mao-to for two days, and the average duration of fever was found to be significantly shorter in the treatment group compared to the control group (p<0.01). The treatment appears to be safe, as no side effects were reported.
3.7.2. Homeopathic Remedies
No studies have been identified regarding the use of homeopathic products in children with flu.
4. Discussion
4.1. Efficacy of Phytotherapeutic and Homeopathic Interventions in Pediatric Acute Infections
This scoping review synthesized data from 35 studies, predominantly RCTs and double-blind designs, with only 2 observational studies considered of good quality. This methodological rigor enhances the reliability of the findings. However, variability in treatment protocols, dosages, and outcome measures across studies introduces heterogeneity, complicating direct comparisons and meta-analytic synthesis. A few phytotherapeutic agents may be effective in alleviating symptoms in specific, well-defined pediatric infectious conditions such as URTIs, bronchitis, and otitis media.
These main results of this scoping review can be summarized as follows: i) certain herbal treatments, such as Pelargonium sidoides and honey have shown moderate efficacy in alleviating symptoms of respiratory acute infections, whereas the available evidence on homeopathy is very limited and sometimes inconsistent ii) both phytotherapeutic and homeopathic remedies are generally safe when used appropriately iii) the existing literature presents several limitations, including a lack of data on non-respiratory infections, such as urinary tract, dermatological, central nervous system, and osteoarticular infections. While some studies are of good quality, there is notable heterogeneity in methodologies and outcomes, limiting the generalizability of results. These findings underscore the need for further research to establish the efficacy and safety of phytotherapeutic and homeopathic remedies across a broader range of infections.
4.2. Phytotherapeutic Treatments in Pediatric Acute Infections
Phytotherapeutic agents, especially Pelargonium sidoides, Echinacea purpurea, honey, and various plant extracts, have been extensively studied in pediatric populations for conditions such as URTIs, bronchitis, HFMD, and flu. Among these, Pelargonium sidoides has shown consistent efficacy in reducing symptoms like cough and improving overall health status in children with acute bronchitis. The safety profile of this herb is favorable, with minimal adverse effects reported. The mechanisms underlying its efficacy include antimicrobial effects, immunomodulatory actions, and mucociliary enhancement [51]. About the first effect, in vitro studies have shown that Pelargonium sidoides exhibits bacteriostatic and bactericidal properties against both Gram-positive and negative bacteria. It also demonstrated antifungal activity by inhibiting enzymes like laccase, leading to fungal cell death. Additionally, its antiviral effects involve the inhibition of viral surface glycoproteins, preventing viral attachment and replication. Also, his extract enhances the release of cytokines (e.g., IL-1, IL-10) and interferon, which boosts phagocytosis and intracellular killing. Moreover, it increases ciliary beat frequency in the respiratory tract, facilitating mucus clearance. At least, Pelargonium sidoides has been shown to increase ciliary beat frequency in nasal epithelial cells, promoting better clearance of mucus and pathogens from the respiratory tract [52]. These multifaceted mechanisms might contribute to the therapeutic potential of Pelargonium sidoides in treating pediatric acute infections. Also, Echinacea purpurea and honey and bee products are considered effective phytotherapeutic agents, but sometimes some studies yield statistically insignificant results.
Echinacea purpurea has demonstrated potential benefits due to its potential immunoboosting properties. Traditionally, it has been employed to prevent and treat common colds and other respiratory infections. It believes to stimulate the immune system by enhancing the activity of macrophages, natural killer, and other immune cells. It contains bioactive compounds such as polysaccharides and alkamides, that modulate cytokine production and reduce inflammation. These immunomodulatory effects might help the body better respond to infections, particularly respiratory tract infections [53].
Honey has been used particularly for its wound healing and antimicrobial properties [54]. It exerts its therapeutic effects through multiple mechanisms. It has strong antimicrobial properties due to its high sugar content, low pH, and the production of hydrogen peroxide by the enzyme glucose oxidase. Additionally, honey contains various antioxidants and bioactive compounds [55] that help reduce inflammation and promote tissue healing. Its viscous texture also creates a protective barrier, aiding wound healing and soothing irritated mucous membranes [56]. Overall, the results of the current review support the findings of previous analysis in the literature [57,58].
4.3. Homeopathic Treatments in Pediatric Acute Infections
Homeopathic remedies have been evaluated in pediatric patients with URTIs and otitis media. Homeopathic preparations include Vincetoxicum hirundinaria, BNO 1030 extract, and combinations containing Chamomilla, Belladonna, Agraphis nutans, Thuya occidentalis, and Kalium muriaticum. Some RCTs [18,20,31,39,42,46,47] focusing on URTIs demonstrated a reduction in symptom severity, particularly concerning cough and the need for conventional antipyretics, but several results were not statistically significant or included very small samples. Similarly, few studies [19,30,48] on otitis media have reported improvements in earache, transient hearing loss, and fluid accumulation, alongside decreased school absenteeism. None of the studies mentioned were of high quality. The only high-quality study did not identify any effectiveness on children with acute otitis media with effusion [25].
4.4. Gaps in the Current Literature and Future Research Perspectives
This scoping review identified a significant gap in the literature concerning the efficacy of homeopathic and phytotherapeutic treatments for pediatric acute infections beyond the upper respiratory tract, such as urinary tract and dermatological infections. No relevant studies were found addressing these conditions, indicating a need for further research in these areas. Additionally, studies focusing on the prevention of various infections using homeopathic and phytotherapeutic products were excluded, underscoring the lack of data on preventive applications. The included studies predominantly addressed infections of bacterial or viral origin, with no references to fungal or other types of infections, limiting the generalizability of the findings. Most of the studies found focused on URTIs, and there isn’t much information on other types of sudden infections in children, showing that more thorough research is needed in these less studied areas. Despite promising findings, literature reveals significant gaps. Data on the efficacy of these treatments in conditions such as HFMD and flu are scarce or absent. Another limitation pertains to the age distribution of the study populations. Phytotherapeutic treatments were primarily tested in children aged 1 year and older, with a focus on those up to 14 years of age. In contrast, homeopathic treatments were evaluated across a broader age range, including neonates and infants under 1 year [25,30,31,47]. This discrepancy in age groups may introduce variability in treatment outcomes and complicate direct comparisons between the two therapeutic approaches. Therefore, future studies should aim to standardize age groups to facilitate more accurate comparison and to better understand the efficacy of these treatments across different pediatric age ranges. Finally, emerging data suggest a potential role of probiotics in the treatment of upper respiratory tract infections. Future studies should evaluate the combined approach of phytoterapics (e.g., bee) with other functional compounds (e.g., probiotics and/or probiotics). In Table 1, the current areas of gaps regarding clinical research and future possible studies to address these gaps are listed.
4.5. Limitations of the Scoping Review
This scoping review has several limitations that warrant consideration. The included studies exhibited significant heterogeneity in methodologies, populations, and outcomes, which may affect the generalizability of our findings. Additionally, some data was self-reported, introducing potential biases such as recall or social desirability bias. Socioeconomic disparities among the study population were also evident, which could influence the outcomes and their applicability to different demographic groups. Furthermore, four studies were industry sponsored, raising questions about potential conflicts of interest and the risk of reporting bias. These factors collectively underscore the need for cautious interpretation of our findings and highlight areas for improvement in future research as previously detailed.
5. Conclusions
Phytotherapeutic agents such as Pelargonium sidoides and honey have shown moderate evidence of efficacy in reducing symptom severity and duration in children and adolescents (1-18 years) with URTIs. In contrast, homeopathic treatments demonstrated inconsistent results, with higher-quality trials generally not supporting their efficacy. Both treatment modalities were generally well-tolerated, with only mild adverse effects reported. Given these findings, some phytotherapeutic agents may be considered as complementary options in pediatric acute respiratory infections. On the other hand, these findings cannot be generalized to other types of acute infections, which deserve future studies. The use of homeopathic remedies for pediatric infections is not currently supported by available evidence.
Author Contributions
CB and IA equally contributed to perform literature search, extract data, perform quality assessments, conceptualize, supervise and write the manuscript. GPM edited and revised the manuscript. NP, SZ e CA approved the final version of the manuscript. All authors gave a significant contribution in his field of expertise and critically reviewed the manuscript.
Funding
No funding was received for this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| RCTs | Randomized Controlled Trials |
| UTIs | Urinary Tract Infections |
| URTIs | Upper Respiratory Tract Infections |
| GI | Gastrointestinal Infection |
| CNS | Central Nervous Systema |
| TSS | Tonsillitis Severity Score |
| SIS | Symptom Severity Score |
| WURSS-21 CARIFS |
Wisconsin Upper Respiratory Symptom Survey-21 Canadian Acute Respiratory Illness and Flud Scale |
| BSS | Bronchitis Severity Scale |
| AOM | Acute Otitis Media |
| HFMD | Hand Foot Mouth Disease |
Appendix A
Literature search
Pubmed
phytotherapy OR herbal medicine OR medicinal plants OR plant extracts OR homeopathy OR homeopathic remedies OR complementary medicine OR immune stimulants OR natural remedies
AND infection OR infections OR infectious disease OR bacterial infection OR viral infection OR fungal infection
AND child OR children OR pediatric OR infant OR newborn
Embase
‘phytotherapy’/exp OR phytotherapy OR ‘herbal medicine’/exp OR ‘herbal medicine’ OR (herbal AND (‘medicine’/exp OR medicine)) OR ‘medicinal plants’/exp OR ‘medicinal plants’ OR (medicinal AND (‘plants’/exp OR plants)) OR ‘plant extracts’/exp OR ‘plant extracts’ OR ((‘plant’/exp OR plant) AND extracts) OR ‘homeopathy’/exp OR homeopathy OR ‘homeopathic remedies’ OR (homeopathic AND remedies) OR ‘complementary medicine’/exp OR ‘complementary medicine’ OR (complementary AND (‘medicine’/exp OR medicine)) OR ‘immune stimulants’ OR ((‘immune’/exp OR immune) AND stimulants) OR ‘natural remedies’ OR ((‘natural’/exp OR natural) AND remedies)
Web of science:
((ALL=(phytotherapy OR herbal medicine OR medicinal plants OR plant extracts OR homeopathy OR homeopathic remedies OR complementary medicine OR immune stimulants OR natural remedies)) AND ALL=(infection OR infections OR infectious disease OR bacterial infection OR viral infection OR fungal infection)) AND ALL=(child OR children OR pediatric OR infant OR newborn)
Cinhal
(“phytotherapy” OR “herbal medicine” OR “medicinal plants” OR “plant extracts” OR “homeopathy” OR “homeopathic remedies” OR “complementary medicine” OR “immune stimulants” OR “immunomodulators” OR “natural remedies”)
AND (“infection” OR “infections” OR “infectious disease” OR “bacterial infection” OR “viral infection” OR “fungal infection”)
AND (“child” OR “children” OR “pediatric” OR “infant” OR “newborn”)
Figure A1.
Quality assessment (RCTs).
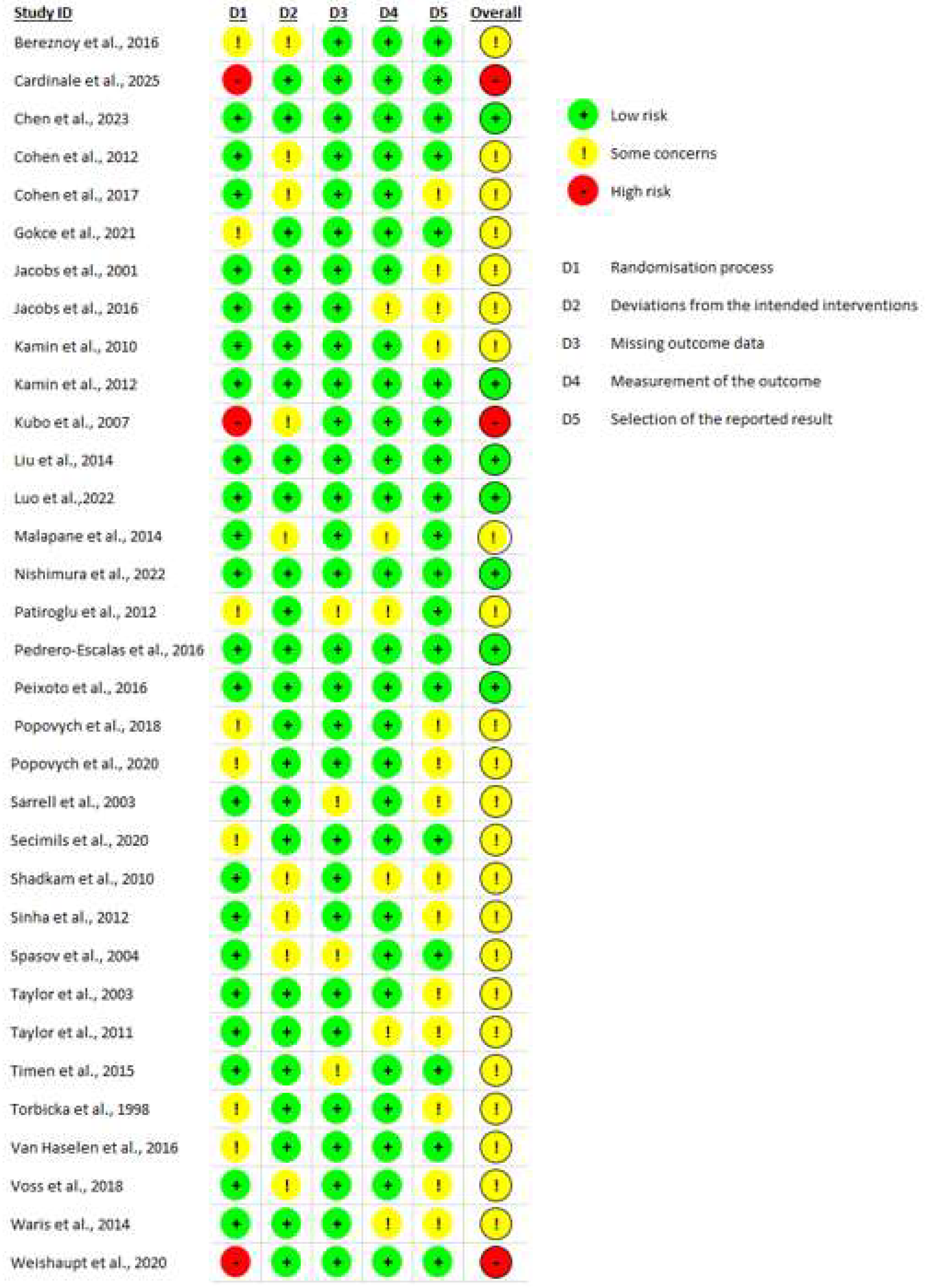
Figure A2.
Quality assessment (observational studies).
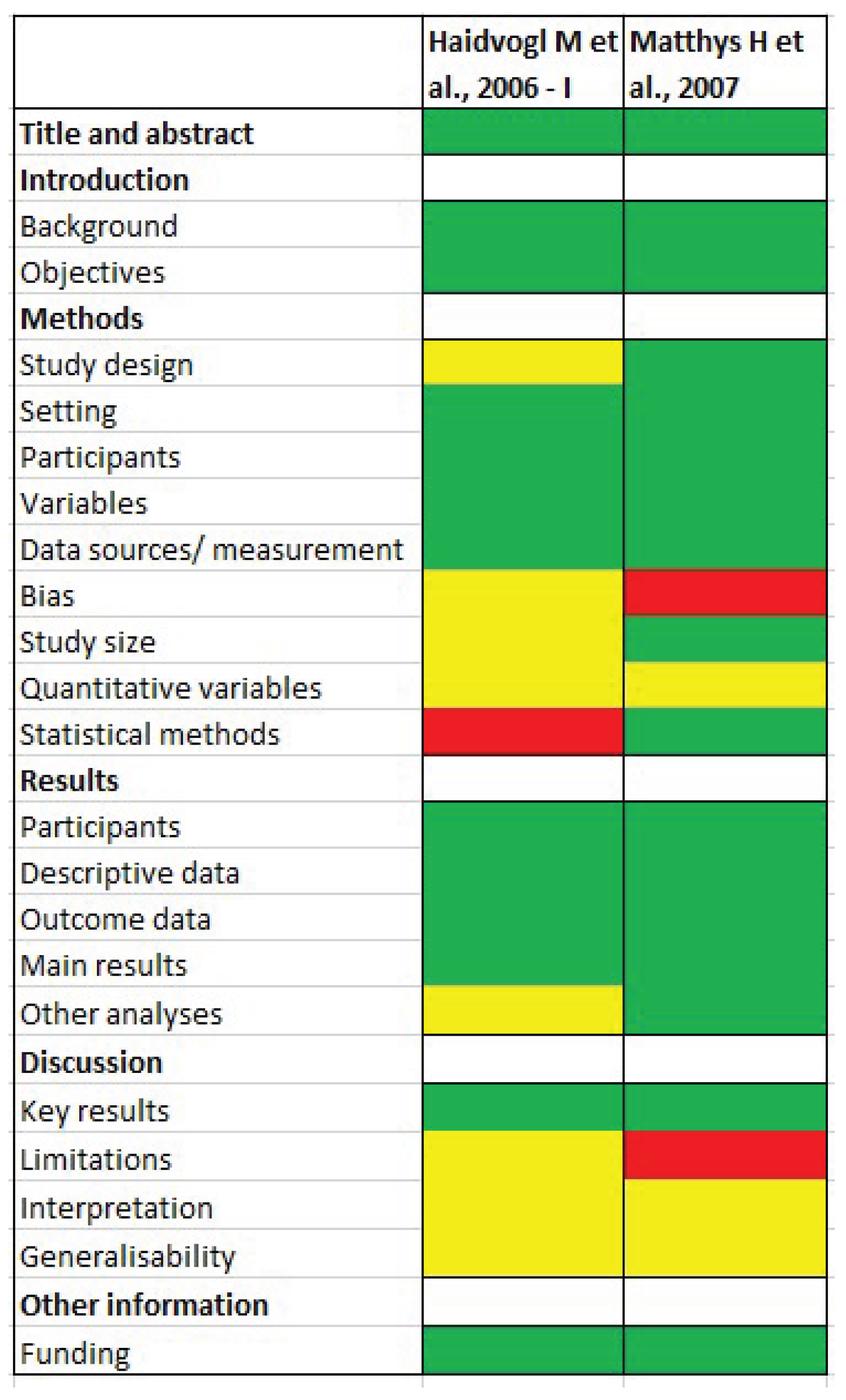

Table A1.
RCTs and observational studies 1.
| Author | Country | Income | Study design | Population size | Age | Infection | Category of dietary supplementation | Actives | Intervention vs Placebo or standard therapy |
|---|---|---|---|---|---|---|---|---|---|
| Bereznoy VV et al., 2016 [29] | Ukraine | Upper -middle income | RCT | 126 | 6-10 years | URTI | Phytotherapy | Pelargonium Sidoides | Treatment vs Placebo |
| Cardinale F et al., 2025 [30] | Romania | High income | RCT | 130 | 3-10 years | URTI | Phytotherapy | Pelargonium Sidoides, honey, propolis and zinc | Treatment + standard therapy vs Standard therapy |
| Chen HF et al., 2023 [40] | China | Upper -middle income | RCT | 443 | 1-14 years | Bronchitis | Phytotherapy | Arctium Lappa, Morus Alba, Mentha Haplo Calyx,Sabillina Tenuifolia, Fritillaria Unibracteata, Peucedanum Praeruptorum Dunn, Aster Tataricus, Citrus Aurantium, Isatis Indogotica, Glycyrrhiza Uralensis. | Treatment vs 10% treatment |
| Cohen HA et al., 2017 [21] | Israel | High income | RCT | 141 | 2-5 years | URTI | Phytotherapy | Polysaccharides, Resin, Honey | Treatment vs standard |
| Cohen HA et al., 2012 [20] | Israel | High income | RCT | 270 | 1-5 years | URTI | Phytotherapy | Eucalyptus honey, citrus honey, labiatae honey | Treatment 1 or treatment 2 or treatment 3 vs placebo |
| Gökçe Ş et al., 2021 [19] | Turkey | Upper -middle income | RCT | 164 | 1-18 years | URTI | Phytotherapy | Pelargonium Sidoides | Treatment vs placebo |
| Haidvogl M et al., 2007 [38] | Germany | High income | Observational study | 742 | 1-12 years | Bronchitis | Phytotherapy | Pelargonium Sidoides | x |
| Jacobs J et al., 2001 [43] | United States | High income | RCT | 75 | 18 months – 6 years | Acute otitis media | Homeopathy | Pulsatilla Ngrans, Chamomilla, Sulphur, Calcarea Carbonica | Treatment vs placebo |
| Jacobs J et al., 2016 [34] | United States | High income | RCT | 261 | 2-5 years | URTI | Homeopathy | Allium Cepa, Hepar Sulphuris Calcareum, Natrum Muriaticum, Pulsatilla, Hydrastis, Extract of Glycyrrhiza | Treatment vs placebo |
| Kamin W et al., 2010 [41] | Ukraine | Upper -middle income | RCT | 200 | 1-18 years | Bronchitis | Phytotherapy | Pelargonium Sidoides | Treatment vs placebo |
| Kamin W et al., 2012 [39] | Russia | High income | RCT | 220 | 1-18 years | Bronchitis | Phytotherapy | Pelargonium Sidoides | Treatment vs placebo |
| Kubo T et al., 2007 [49] | Japan | High income | RCT | 49 | 5 months-13 years | Flu A | Phytotherapy | Ephedrae herba, Armenicae cortex, Cinnamon cortex, Glycyrrhizae radix | Anti-viral therapy + treatment or treatment or anti-viral treatment |
| Liu J et al., 2014 [48] | China | Upper -middle income | RCT | 399 | 1-7 years | HFMD | Phytotherapy | Salgae Tataricae Cornu, Fritillaria Usuriensis Maxim, Rheum Officiale Baill, Scutellaria Baicalensis Georgi,Sulfate minerals gypsum, Glycyrrhiza Glabra L. | Treatment vs placebo |
| Luo H et al., 2022 [27] | China | Upper -middle income | RCT | 138 | 2-14 years | URTI | Phytotherapy | Bambusae textilis McClure, Crocus sativus, Bovis calculus artifactus , Bergeniae rhizome, Aconitum tanguticum, Glycyrrhizae radix et rhizome, Radix solms-laubachiae, Lagotis brevituba maxim and Santali albi lignum | Treatment vs standard therapy |
| Malapane E et al., 2014 [33] | South Africa | Upper -middle income | RCT | 30 | 6-12 years | URTI | Homeopathy | Atropa belladonna, Calcarea Phosphoricum, Hepar Sulphuris, Kalium Bichromat, Mercurius protoiodid, and Mercurius biniodid Kalium Muriaticum | Treatment vs placebo |
| Matthys H et al., 2007 [42] | Germany | High income | Observational study | 2099 | Children and adults aged 0-93 years | Bronchitis | Phytotherapy | Pelargonium Sidoides | |
| Nishimura T et al., 2022 [25] | Japan | High income | RCT | 161 | 1-5 years | URTI | Phytotherapy | Acacia honey | Treatment vs placebo |
| Patiroglu T et al., 2012 [18] | Turkey | Upper -middle income | RCT | 28 | 1-5 years | URTI | Phytotherapy | Pelargonium Sidoides | Treatment vs placebo |
| Pedrero-Escalas MF, 2016 [45] | Spain | High income | RCT | 96 | 2 months-12 years | Otitis media | Homeopathy | Agraphis nutans, Thuya Occidentalis, Kalium Muriaticum and Arsenicum Iodatum | Treatment vs placebo |
| Peixoto Dm et al., 2016 [23] | Brazil | Upper -middle income | RCT | 60 | 2-15 years | URTI | Phytotherapy | Bromelin + honey | Treatment (bromelin+honey vs placebo (honey) |
| Popovych V et al., 2019 [37] | Ukraine | Upper -middle income | RCT | 238 | 6-18 years | URTI | Homeopathy | BNO 1030 extract | Treatment + standard therapy vs standard therapy |
| Popovych V et al., 2020 [26] | Ukraine | Upper -middle income | RCT | 292 | 6-11 years | URTI | Phytotherapy | Gentian root, Vervain herb, Sambuci flox, Rumex herba, primrose flowers | Treatment + standard therapy vs standard therapy |
| Sarrell EM et al., 2003 [47] | Israel | High income | RCT | 171 | 5-18 years | Otitis media | Homeopathy | Allium sativum, verbascum thapsus, calendula flores, hypercium perfoliatum, lavender, vitamin E | Treatment or treatment + topical anesthetic drops or treatment + antibiotic, or antibiotic + anesthetic drops. |
| Seçilmiş Y et al., 2020 [24] | Canada | High income | RCT | 104 | 5-12 years | URTI | Phytotherapy | Honey, royal jelly, propolis | Bacterial infection: treatment + antibiotic vs antibiotics Viral infection: Treatment vs placebo |
| Shadkam MN et al., 2010 [28] | Iran | Upper -middle income | RCT | 139 | 2-5 years | URTI | Phytotherapy | Honey | Treatment or standard therapy A or standard therapy B or control group |
| Sinha MN et al., 2012 [44] | India | Lower-middle income | RCT | 81 | 2-6 years | Otitis media | Homeopathy | Belladonna, Hepar sulphuris, Calcarea carbonica, Chamomilla, Mercurius solubilis | Treatment vs standard therapy |
| Spasov AA et al., 2004 [16] | Russia | High income | RCT | 133 | 4-11 years | URTI | Phytotherapy | Kan Jang or Echinacea Purpurea | Treatment A + standard therapy or treatment B + standard therapy or standard therapy |
| Taylor JA et al., 2003 [15] | United States | High income | RCT | 524 | 2-11 years | URTI | Phytotherapy | Echinacea Purpurea | Treatment vs placebo |
| Taylor J et al., 2011 [46] | United States | High income | RCT | 120 | 6 months-11 years | Otitis media | Homeopathy | Pulsatilla, Chamomilla, Belladonna, lycopodium | Treatment + standard therapy or standard therapy |
| Timen G et al., 2015 [31] | Ukraine | Upper -middle income | RCT | 78 | 6-10 years | URTI | Phytotherapy | Pelargonium Sidoides | Treatment vs placebo |
| Torbicka E et al., 1998 [32] | Poland | High income | RCT | 128 | Infants | URTI | Homeopathy | Vincetoxicum hirundinaria, sulfur | Treatment + standard therapy vs standard therapy |
| Van Haselen R et al., 2016 [36] | Ukraine and Germany | Upper -middle income and High income | RCT | 261 | 1-11 years | URTI | Homeopathy | Aconitum, Bryonia, Eupatorium Perfolatum, Gelsemium, Ipecuanha, Phosphorus | Treatment + standard therapy vs standard therapy |
| Voss HW et al., 2018 [35] | Ukraine | Upper -middle income | RCT | 180 | 7 months-12 years | URTI | Homeopathy | Drosera, Coccus cacti, Cuprum Sulfuricum, Ipecacuanha | Treatment vs placebo |
| Waris A et al., 2014 [22] | Kenya | Lower-middle income | RCT | 133 | 1-12 years | URTI | Phytotherapy | Honey | Treatment vs standard therapy vs placebo |
| Weishaupt R et al., 2020 [17] | Switzerland | High income | RCT | 79 | 4-12 years | URTI | Phytotherapy | Exctract of Echinacea purpurea | 5 tablets of treatment or 3 tablets of treatment |
References
- Alter, S.J.; Bennett, J.S.; Koranyi, K.; Kreppel, A.; Simon, R. Common Childhood Viral Infections. Curr. Probl. Pediatr. Adolesc. Heal. Care 2015, 45, 21–53. [Google Scholar] [CrossRef]
- Zha, M.; Usatine, R. Common Skin Conditions in Children and Adolescents: Atopic and Seborrheic Dermatitis. . 2024, 541, 27–38. [Google Scholar]
- Marsh, M.C.; Junquera, G.Y.; Stonebrook, E.; Spencer, J.D.; Watson, J.R. Urinary Tract Infections in Children. Pediatr. Rev. 2024, 45, 260–270. [Google Scholar] [CrossRef] [PubMed]
- Jain, N.; Lodha, R.; Kabra, S.K. Upper respiratory tract infections. Indian J. Pediatr. 2001, 68, 1135–1138. [Google Scholar] [CrossRef] [PubMed]
- Willis, G.A.; Preen, D.B.; Richmond, P.C.; Jacoby, P.; Effler, P.V.; Smith, D.W.; Robins, C.; Borland, M.L.; Levy, A.; Keil, A.D.; et al. The impact of influenza infection on young children, their family and the health care system. Influ. Other Respir. Viruses 2018, 13, 18–27. [Google Scholar] [CrossRef]
- Chow, M.Y.K.; Yin, J.K.; Heron, L.; Morrow, A.; Dierig, A.; Booy, R.; Leask, J. The impact of influenza-like illness in young children on their parents: a quality of life survey. Qual. Life Res. 2013, 23, 1651–1660. [Google Scholar] [CrossRef] [PubMed]
- Fashner, J.; Ericson, K.; Werner, S. Treatment of the common cold in children and adults. . 2012, 86, 153–9. [Google Scholar]
- Shehab, N.; Schaefer, M.K.; Budnitz, D.S.; Kegler, S.R. Adverse Events From Cough and Cold Medications After a Market Withdrawal of Products Labeled for Infants. Pediatrics 2010, 126, 1100–1107. [Google Scholar] [CrossRef]
- Zimmermann-Klemd, A.M.; Reinhardt, J.K.; Winker, M.; Gründemann, C. Phytotherapy in Integrative Oncology—An Update of Promising Treatment Options. Molecules 2022, 27, 3209. [Google Scholar] [CrossRef]
- Merrell, W.C.; Shalts, E. Homeopathy. Med Clin. North Am. 2002, 86, 47–62. [Google Scholar] [CrossRef]
- Levi, J.R.; Brody, R.M.; McKee-Cole, K.; Pribitkin, E.; O’rEilly, R. Complementary and alternative medicine for pediatric otitis media. Int. J. Pediatr. Otorhinolaryngol. 2013, 77, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Gori, A.; Brindisi, G.; Anania, C.; Spalice, A.; Zicari, A.M. Synergic Efficacy of a Multicomponent Nutraceutical Add-On Therapy in Seasonal Allergic Rhinitis in Children: A Prospective, Randomized, Parallel-Group Study. J. Clin. Med. 2025, 14, 1517. [Google Scholar] [CrossRef] [PubMed]
- Milani, G.P.; Alberti, I.; Abodi, M.; Lakoumentas, J.; Konstantinou, G.N.; Papadopoulos, N.G.; Pop, R.M.; Bocsan, I.C.; Cassimos, D.; Kull, I.; et al. A systematic review and meta-analysis on nutritional and dietary interventions for the treatment of acute respiratory infection in pediatric patients: An EAACI taskforce. Allergy 2024, 79, 1687–1707. [Google Scholar] [CrossRef] [PubMed]
- Bettocchi, S.; Comotti, A.; Elli, M.; De Cosmi, V.; Berti, C.; Alberti, I.; Mazzocchi, A.; Rosazza, C.; Agostoni, C.; Milani, G.P. Probiotics and Fever Duration in Children With Upper Respiratory Tract Infections. JAMA Netw. Open 2025, 8, e250669. [Google Scholar] [CrossRef]
- Cardinale, F.; Barattini, D.F.; Centi, A.; Giuntini, G.; Bordea, M.M.; Herteg, D.; Barattini, L.; Matei, C.R. Open, Randomised, Controlled Study to Evaluate the Role of a Dietary Supplement Containing Pelargonium sidoides Extract, Honey, Propolis, and Zinc as Adjuvant Treatment in Children with Acute Tonsillopharyngitis. Children 2025, 12, 345. [Google Scholar] [CrossRef]
- Cohen, H.A.; Hoshen, M.; Gur, S.; Bahir, A.; Laks, Y.; Blau, H. Efficacy and tolerability of a polysaccharide-resin-honey based cough syrup as compared to carbocysteine syrup for children with colds: a randomized, single-blinded, multicenter study. World J. Pediatr. 2016, 13, 27–33. [Google Scholar] [CrossRef]
- Cohen, H.A.; Rozen, J.; Kristal, H.; Laks, Y.; Berkovitch, M.; Uziel, Y.; Kozer, E.; Pomeranz, A.; Efrat, H. Effect of Honey on Nocturnal Cough and Sleep Quality: A Double-blind, Randomized, Placebo-Controlled Study. Pediatrics 2012, 130, 465–471. [Google Scholar] [CrossRef]
- Haidvogl, M.; Heger, M. Treatment effect and safety of EPs® 7630-solution in acute bronchitis in childhood: Report of a multicentre observational study. Phytomedicine 2007, 14, 60–64. [Google Scholar] [CrossRef]
- Jacobs, J.; Springer, D.A.; Crothers, D. Homeopathic treatment of acute otitis media in children: a preliminary randomized placebo-controlled trial. Pediatr. Infect. Dis. J. 2001, 20, 177–183. [Google Scholar] [CrossRef]
- Jacobs, J.; Taylor, J.A. A randomized controlled trial of a homeopathic syrup in the treatment of cold symptoms in young children. Complement. Ther. Med. 2016, 29, 229–234. [Google Scholar] [CrossRef]
- Kamin, W.; Ilyenko, L.I.; Malek, F.A.; Kieser, M. Treatment of acute bronchitis with EPs 7630: Randomized, controlled trial in children and adolescents. Pediatr. Int. 2012, 54, 219–226. [Google Scholar] [CrossRef] [PubMed]
- Kubo, T.; Nishimura, H. Antipyretic effect of Mao-to, a Japanese herbal medicine, for treatment of type A influenza infection in children. Phytomedicine 2007, 14, 96–101. [Google Scholar] [CrossRef] [PubMed]
- Matthys, H.; Kamin, W.; Funk, P.; Heger, M. Pelargonium sidoides preparation (EPs® 7630) in the treatment of acute bronchitis in adults and children. Phytomedicine 2007, 14, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Nishimura, T.; Muta, H.; Hosaka, T.; Ueda, M.; Kishida, K. ; the Honey and Coughs Study Group of the Society of Ambulatory and General Paediatrics of Japan Multicentre, randomised study found that honey had no pharmacological effect on nocturnal coughs and sleep quality at 1–5 years of age. Acta Paediatr. 2022, 111, 2157–2164. [Google Scholar] [CrossRef]
- Pedrero-Escalas, M.; Jimenez-Antolin, J.; Lassaletta, L.; Diaz-Saez, G.; Gavilán, J. Hospital clinical trial: Homeopathy (Agraphis nutans 5CH, Thuya occidentalis 5CH, Kalium muriaticum 9CH and Arsenicum iodatum 9CH) as adjuvant, in children with otitis media with effusion. Int. J. Pediatr. Otorhinolaryngol. 2016, 88, 217–223. [Google Scholar] [CrossRef] [PubMed]
- Sarrell, E.M.; Cohen, H.A.; Kahan, E. Naturopathic Treatment for Ear Pain in Children. Pediatrics 2003, 111, e574–e579. [Google Scholar] [CrossRef]
- Seçilmiş, Y.; Silici, S. Bee product efficacy in children with upper respiratory tract infections. Turk. J. Pediatr. 2020, 62, 634–640. [Google Scholar] [CrossRef]
- Spasov, A.A.; Ostrovskij, O.V.; Chernikov, M.V.; Wikman, G. Comparative controlled study of Andrographis paniculata fixed combination, Kan Jang® and an Echinacea preparation as adjuvant, in the treatment of uncomplicated respiratory disease in children. Phytotherapy Res. 2004, 18, 47–53. [Google Scholar] [CrossRef]
- Taylor, J.A.; Weber, W.; Standish, L.; Quinn, H.; Goesling, J.; McGann, M.; Calabrese, C. Efficacy and Safety of Echinacea in Treating Upper Respiratory Tract Infections in Children. JAMA 2003, 290, 2824–2830. [Google Scholar] [CrossRef] [PubMed]
- A Taylor, J.; Jacobs, J. Homeopathic ear drops as an adjunct to standard therapy in children with acute otitis media. Homeopathy 2011, 100, 109–115. [Google Scholar] [CrossRef]
- Torbicka E, Brzozowska-Binda A, Wilczynski J, Uzerowicz A. RSV infections in infants: therapy with a homeopathic preparation. Biomedical Therapy. 2: 1998;16(4), 1998.
- Weishaupt, R.; Bächler, A.; Feldhaus, S.; Lang, G.; Klein, P.; Schoop, R. Safety and Dose-Dependent Effects of Echinacea for the Treatment of Acute Cold Episodes in Children: A Multicenter, Randomized, Open-Label Clinical Trial. Children 2020, 7, 292. [Google Scholar] [CrossRef]
- Bereznoy VV, Heger M, Lehmacher W, Seifert G. Clinical efficacy and safety of liquid Pelargonium Sidoides preparation (eps 7630) in children with acute non-streptococcal tonsillopharyngitis. J Compr Pediatr. 2016;7(4). [CrossRef]
- Chen, H.-F.; Song, G.-H.; Zhao, G.; Zhai, W.-S.; Sun, M.-M.; Huang, Z.-J.; Zhang, B.-Q.; Li, H.; Tang, J.-Q. Efficacy and safety of Chinese herbal medicine children's Zibei Xuanfei syrup in treating acute trachea-bronchitis with wind-heat invading lung syndrome: A randomized, double-blind, multicentre, controlled trial. J. Ethnopharmacol. 2023, 309, 116207. [Google Scholar] [CrossRef]
- Gökçe, Ş.; Dörtkardeşler, B.E.; Yurtseven, A.; Kurugöl, Z. Effectiveness of Pelargonium sidoides in pediatric patients diagnosed with uncomplicated upper respiratory tract infection: a single-blind, randomized, placebo-controlled study. Eur. J. Pediatr. 2021, 180, 3019–3028. [Google Scholar] [CrossRef]
- Kamin, W.; Maydannik, V.; Malek, F.; Kieser, M. Efficacy and tolerability of EPs 7630 in children and adolescents with acute bronchitis – A randomized, double-blind, placebo-controlled multicenter trial with a herbal drug preparation from Pelargonium sidoides roots. Int. J. Clin. Pharmacol. Ther. 2010, 48, 184–191. [Google Scholar] [CrossRef]
- Liu, J.; Zhang, G.-L.; Huang, G.-Q.; Li, L.; Li, C.-P.; Wang, M.; Liang, X.-Y.; Xie, D.; Yang, C.-M.; Li, Y.; et al. Therapeutic Effect of Jinzhen Oral Liquid for Hand Foot and Mouth Disease: A Randomized, Multi-Center, Double-Blind, Placebo-Controlled Trial. PLOS ONE 2014, 9, e94466. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Song, G.-H.; Ma, X.-J.; Sun, M.-M.; Zhang, M.; Xie, J.-R.; Peng, S. Effect of Jiuwei Zhuhuang Powder on Cough Resolution in Children with Upper Respiratory Tract Infections: A Multicenter Randomized Controlled Trial. Chin. J. Integr. Med. 2021, 28, 387–393. [Google Scholar] [CrossRef]
- Malapane, E.; Solomon, E.M.; Pellow, J. Efficacy of a Homeopathic Complex on Acute Viral Tonsillitis. J. Altern. Complement. Med. 2014, 20, 868–873. [Google Scholar] [CrossRef]
- Patiroglu, T.; Tunc, A.; Gungor, H.E.; Unal, E. The efficacy of Pelargonium sidoides in the treatment of upper respiratory tract infections in children with transient hypogammaglobulinemia of infancy. Phytomedicine 2012, 19, 958–961. [Google Scholar] [CrossRef] [PubMed]
- Peixoto, D.M.; Rizzo, J.A.; Schor, D.; Silva, A.R.; de Oliveira, D.C.; Solé, D.; Sarinho, E. Use of honey associated with Ananas comosus (Bromelin) in the treatment of acute irritative cough. . 2016, 34, 412–417. [Google Scholar] [CrossRef]
- Popovych, V.; Koshel, I.; Malofiichuk, A.; Pyletska, L.; Semeniuk, A.; Filippova, O.; Orlovska, R. A randomized, open-label, multicenter, comparative study of therapeutic efficacy, safety and tolerability of BNO 1030 extract, containing marshmallow root, chamomile flowers, horsetail herb, walnut leaves, yarrow herb, oak bark, dandelion herb in the treatment of acute non-bacterial tonsillitis in children aged 6 to 18 years. Am. J. Otolaryngol. 2019, 40, 265–273. [Google Scholar] [CrossRef] [PubMed]
- Popovych, V.I.; Beketova, H.V.; Koshel, I.V.; Tsodikova, O.A.; Kriuchko, T.A.; Abaturov, A.E.; Vakulenko, L.I.; Gavrylenko, I.V. An open-label, multicentre, randomized comparative study of efficacy, safety and tolerability of the 5 plant - extract BNO 1012 in the Delayed Antibiotic Prescription Method in children, aged 6 to 11 years with acute viral and post-viral rhinosinusitis. Am. J. Otolaryngol. 2020, 41, 102564. [Google Scholar] [CrossRef]
- Shadkam, M.N.; Mozaffari-Khosravi, H.; Mozayan, M.R. A Comparison of the Effect of Honey, Dextromethorphan, and Diphenhydramine on Nightly Cough and Sleep Quality in Children and Their Parents. J. Altern. Complement. Med. 2010, 16, 787–793. [Google Scholar] [CrossRef]
- Timen G, Zabolotnyi D, Heger M, Lehmacher W. Eps 7630 is effective in children with acure, non-_-haemolytic streptococcal tonsillopharyngitis results of a double-blind, placebo-controlled, multicentre trial. Malay J Pediatr Child Health. 3: 2015; 21, 2015.
- van Haselen, R.; Thinesse-Mallwitz, M.; Maidannyk, V.; Buskin, S.L.; Weber, S.; Keller, T.; Burkart, J.; Klement, P. The Effectiveness and Safety of a Homeopathic Medicinal Product in Pediatric Upper Respiratory Tract Infections With Fever. Glob. Pediatr. Heal. 2016, 3. [Google Scholar] [CrossRef]
- Voß, H.W.; Michalsen, A.; Brünjes, R. Efficacy and tolerability of a complex homeopathic drug in children suffering from dry cough-A double-blind, placebo-controlled, clinical trial. Drug Res. 2018, 68, 444–449. [Google Scholar] [CrossRef]
- Sinha, M.; Siddiqui, V.; Nayak, C.; Singh, V.; Dixit, R.; Dewan, D.; Mishra, A. Randomized controlled pilot study to compare Homeopathy and Conventional therapy in Acute Otitis Media. Homeopathy 2012, 101, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Waris, A.; Macharia, M.; Njeru, E.K.; Essajee, F. RANDOMISED DOUBLE BLIND STUDY TO COMPARE EFFECTIVENESS OF HONEY, SALBUTAMOL AND PLACEBO IN TREATMENT OF COUGH IN CHILDREN WITH COMMON COLD. . 2014, 91, 50–6. [Google Scholar] [PubMed]
- https://datahelpdesk.worldbank.
- Cinatl, J.; Wass, M.N.; Michaelis, M. Multiple mechanisms enable broad-spectrum activity of the Pelargonium sidoides root extract EPs 7630 against acute respiratory tract infections. Front. Pharmacol. 2024, 15, 1455870. [Google Scholar] [CrossRef]
- Reina, B.D.; Malheiros, S.S.; Vieira, S.M.; de Andrade, P.F.; Dovigo, L.N. Unlocking the therapeutic potential of Pelargonium sidoides natural extract: A scoping review. Heliyon 2024, 10, e40554. [Google Scholar] [CrossRef]
- Barrett, B. Medicinal properties of Echinacea: A critical review. Phytomedicine 2003, 10, 66–86. [Google Scholar] [CrossRef] [PubMed]
- Molan, PC. The antibacterial activity of honey: the natura of the antibacterial activity. Bee World. 1992; ;73. [Google Scholar]
- Alvarez-Suarez, J.M.; Gasparrini, M.; Forbes-Hernández, T.Y.; Mazzoni, L.; Giampieri, F. The Composition and Biological Activity of Honey: A Focus on Manuka Honey. Foods 2014, 3, 420–432. [Google Scholar] [CrossRef] [PubMed]
- Mandal, M.D.; Mandal, S. Honey: its medicinal property and antibacterial activity. Asian Pac. J. Trop. Biomed. 2011, 1, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Kuitunen, I.; Renko, M. Honey for acute cough in children — a systematic review. Eur. J. Pediatr. 2023, 182, 3949–3956. [Google Scholar] [CrossRef] [PubMed]
- Oduwole, O.; E Udoh, E.; Oyo-Ita, A.; Meremikwu, M.M. ; Cochrane Acute Respiratory Infections Group Honey for acute cough in children. Cochrane Database Syst. Rev. 2018, 2018. [Google Scholar] [CrossRef]
Figure 1.
Literature review process.
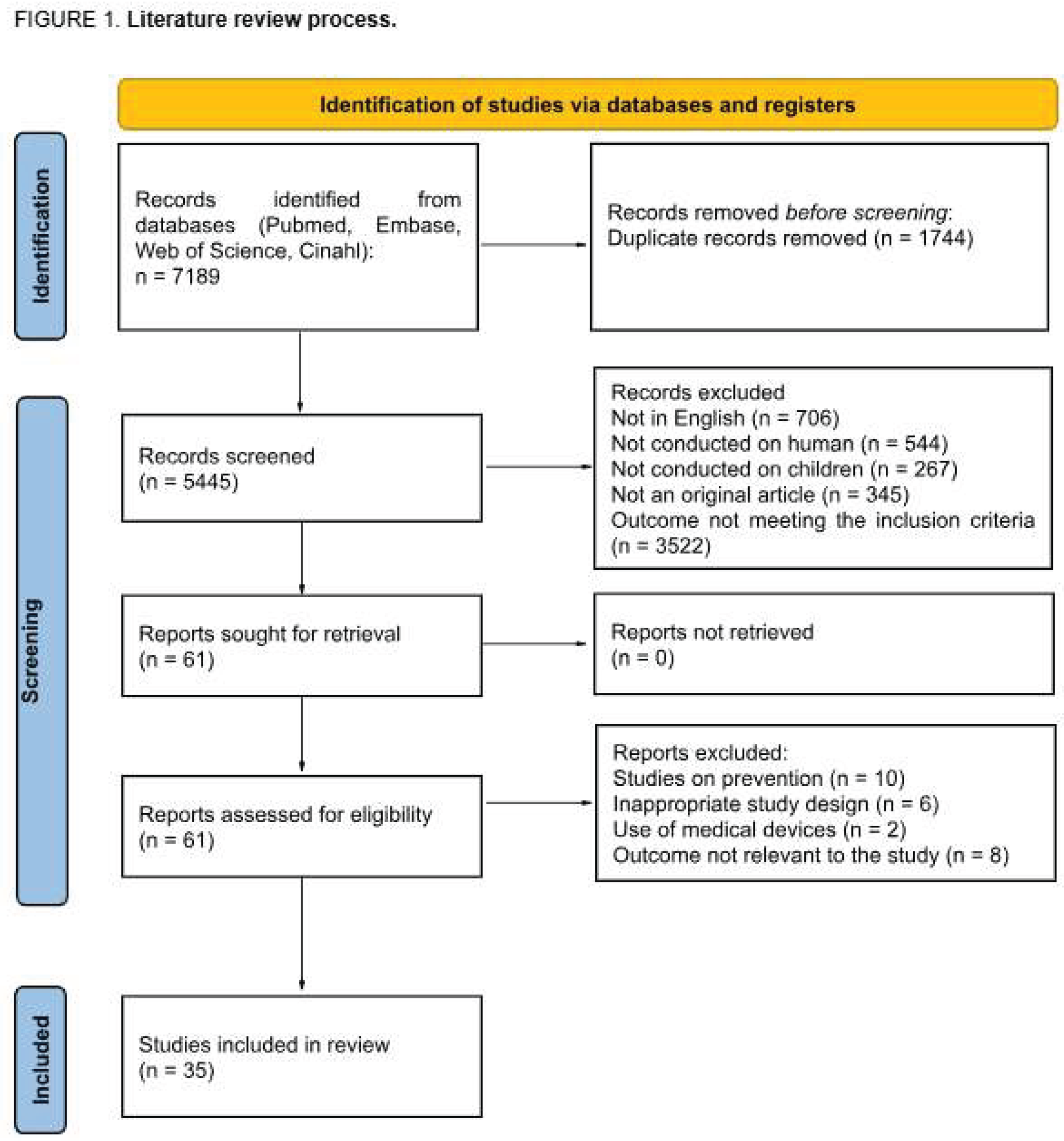
Table 1.
Clinical research and possible future studies on phytotherapeutic and homeopathic remedies in pediatric acute respiratory conditions.
Table 1.
Clinical research and possible future studies on phytotherapeutic and homeopathic remedies in pediatric acute respiratory conditions.
| Current areas of clinical research | Possible future studies |
|---|---|
|
Use of homeopathic remedies in pediatric respiratory infections by high quality studies |
Testing homeopathic treatments in acute respiratory infections like flu, bronchitis, and otitis media in children using well powered blinded RCT placebo vs interventions and employing validated scores for outcomes assessment |
|
Use of phytotherapeutic agents (e.g., Pelargonium sidoides) in school-age children |
Testing phytotherapeutics in infants and neonates under 1 year of age |
|
Isolated testing of phytotherapeutic treatments or phytotherapics and other approaches |
Studying combined use of more phytotherapeutics or phytotherapics with other potentially synergic compounds (e.g., probiotics) |
|
Single-agent studies of Pelargonium sidoides or honey |
Evaluating synergic combinations such as Pelargonium sidoides + honey or Pelargonium sidoides + probiotics |
|
Effectiveness and safety pf phytotherapeutic agents in young children |
Testing phytotherapeutic in infants and children < 1 year of age |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



