Submitted:
21 August 2025
Posted:
22 August 2025
You are already at the latest version
Abstract
Introduction: Robotic-assisted thoracic surgery (RATS) has emerged as an innovative alternative to conventional video-assisted thoracoscopic surgery (VATS) in pediatric patients. Although individual case series have described its feasibility and safety, no systematic synthesis has previously addressed its role in children. Methods: We conducted a systematic review and meta-analysis in accordance with PRISMA guidelines, registered in PROSPERO (CRD420251091235). A comprehensive search of PubMed, CINAHL, Web of Science, and EMBASE was performed to identify studies reporting pediatric RATS. Quality and Risk of bias were assessed using the MINORS and ROBINS-I tools respectively. For the quantitative synthesis, random-effects models meta-analyses were applied with restricted maximum likelihood (REML) estimation, and confidence intervals were adjusted using either the Knapp–Hartung (HKSJ) or the modified Knapp–Hartung (mKH) methods to account for small-sample uncertainty. Results: Thirty-six studies encompassing 936 patients were included; 638 underwent RATS. Reported indications included tracheobronchial procedures, pulmonary resections, congenital diaphragmatic anomalies, mediastinal tumors and thymic disorders. Qualitative synthesis demonstrated high feasibility, versatility across pathologies, and favorable safety, with a 1.8% conversion rate and low complication rates (5.6%). Quantitative synthesis revealed longer operative times for RATS compared to VATS (mean difference 26.4 minutes, 95% CI: 3.26 to 49.47; p=0.04). However, RATS significantly reduced hospital stay (–0.70 days, 95% CI: –1.22 to –0.17; p=0.02) and showed a nonsignificant trend toward shorter chest tube duration. Complication rates did not differ significantly between groups (RR 1.16; 95% CI: 0.83 to 1.63; p=0.39). Conclusions: RATS may be considered as a safe and effective minimally invasive technique for selected pediatric thoracic conditions, offering enhanced precision and versatility. Current evidence, although very limited due to the low number of studies, presents a potentially beneficial profile for RATS, although larger prospective multicenter studies are needed to confirm long-term results and optimize patient selection.
Keywords:
robotic-assisted surgery
; robotic surgery
; thoracic surgery
; video-assisted thoracoscopic surgery
; children
; pediatric
Introduction
The earliest documented case of robot-assisted thoracic surgery (RATS) was a thoracoscopic sympathectomy performed with the da Vinci robotic system in 2002 [1]. This landmark report highlighted the feasibility and safety of integrating robotic technology into thoracic procedures and opened the door to more advanced operations [2]. Following its introduction in adults, RATS began to be adopted in pediatric populations. The first pediatric RATS report was published by Luebbe et al. in 2003 in two 10-year-old children with Morgagni congenital diaphragmatic hernia (CDH) and an infracarinal mediastinal mass [3]. Since then, clinical experience has progressively expanded, with single-center series reporting increasing numbers of patients and an increasingly broad range of indications, including mediastinal mass resections, diaphragmatic anomaly repairs, and tracheal procedures, among others [4,5,6]. In recent years, studies have also begun to compare the perioperative and postoperative outcomes of RATS with those of conventional thoracoscopic surgery, in order to determine whether the potential technical advantages of robotic platforms translate into measurable clinical benefits, such as reduced complication rates, improved operative precision, and shorter recovery times [7,8,9,10].
To date, no comprehensive qualitative or quantitative synthesis of the literature on pediatric RATS has been conducted. This systematic review and meta-analysis therefore aims to fill this gap by evaluating the current evidence, summarizing reported outcomes, and providing a critical appraisal of the role of RATS in pediatric patients.
Methods
Search Strategy
A systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines [11,12]. The research question was structured using the Population, Intervention, Comparator, Outcome (PICO) framework: “In pediatric patients undergoing thoracic surgery, does robot-assisted thoracic surgery (RATS), compared with video-assisted thoracoscopic surgery (VATS), result in improved perioperative and postoperative outcomes?”. A comprehensive literature search was performed across four electronic databases (PubMed, CINAHL, Web of Science and EMBASE), initially in July 2025 from inception, with an updated search conducted on August 11st, 2025 by two authors (CDM and JC). To identify relevant studies, the PubMed search employed the following MeSH terms: [“robotic-assisted” OR “robotic”] AND [“children” OR “pediatric”] AND [“thoracic” OR “thorax”]. The detailed search string applied for each database is provided in Supplementary Material S1. The primary outcome was to identify the main indications for robotic-assisted thoracic surgery, as well as to analyze the demographics, underlying pathology, operative time, intraoperative complications, conversion rate, long-term outcomes and need for reoperation. As secondary objectives, the review aimed to assess these outcomes in relation to VATS procedures and to integrate the findings through a quantitative synthesis (meta-analysis). The protocol of this systematic review was prospectively registered in the PROSPERO database (registration CRD420251091235).
Eligibility Criteria
Studies were considered eligible for inclusion if they involved patients under 18 years of age and addressed the use of robotic-assisted thoracic surgery. To qualify, publications needed to be full-text articles presenting original clinical data related to robotic-assisted thoracic surgery. Only studies conducted in human subjects and written in English were included.
Exclusion criteria comprised editorials, review articles lacking original clinical data, commentaries, conference abstracts, grey literature, studies involving animals or exclusively adult populations, and those unrelated to gastrointestinal surgery. Articles that included both pediatric and adult patients were retained only if sufficient data on the pediatric subgroup permitted independent analysis. Duplicate entries were removed, and remaining records were screened initially by title and abstract, removing those in which it was not specified that robotic-assisted thoracic surgery was used in pediatric patients. Full-text versions of potentially relevant studies were subsequently reviewed in detail to confirm compliance with inclusion criteria. Review articles were temporarily retained to allow manual screening of their reference lists, ensuring comprehensive literature coverage through a backward snowballing approach. This strategy enhanced the identification of all pertinent studies aligned with the predefined eligibility criteria.
Data Collection
Information on study characteristics, patient demographics, sample size, age at the time of surgery, underlying conditions, surgical techniques employed, operative time, conversion rate, postoperative complications, and clinical outcomes was extracted from each included publication. Data collection was independently carried out by two reviewers (CDM and JC) using a standardized Microsoft Excel™ (2007, Redmond, WA, USA) spreadsheet. The entire review process—comprising screening, eligibility assessment, and data extraction—was independently performed by both investigators. Additionally, relevant references cited within the selected studies were manually screened to identify further eligible articles. Any disagreements were resolved by discussion until a consensus was reached. A descriptive synthesis was performed to summarize the available evidence on outcomes of pediatric robotic-assisted thoracic surgery. Ethical approval was not required due to the nature of this systematic review.
Quality Appraisal and Risk of Bias
To evaluate the methodological quality of the included studies, the Methodological Index for Non-Randomized Studies (MINORS) was employed [13]. For nonrandomized comparative studies included in the quantitative analysis, the Risk of Bias in Non-randomized Studies of Interventions (ROBINS-I) tool [14] was applied. Two reviewers (CDM, JC) independently evaluated the risk of bias, and any disagreements were resolved through discussion with a third reviewer until consensus was achieved.
Data Synthesis
In the quantitative synthesis (meta-analysis), summary statistics presented as medians with interquartile ranges (IQR) were converted to means and standard deviations (SD) using the validated methods of Wan et al. and Luo et al. [15,16]. Skewness was evaluated following the approach described by Shi et al. [17], and when substantial skewness was detected, the Quantile Estimation (QE) method proposed by McGrath et al. was applied [18].
Data Analysis
Meta-analyses were performed using random-effects models for both dichotomous and continuous outcomes. For continuous variables, pooled estimates were calculated as mean differences with 95% confidence intervals (CIs). For dichotomous variables, pooled effect measures were expressed as risk ratios (RRs) or, when appropriate, as event rates per group according to the surgical approach. Between-study heterogeneity was assessed using the I2 statistic and Cochran’s Q test. Model selection was guided by the degree of heterogeneity, within-study variance, and the distribution of the outcome. Random-effects models were fitted by default using restricted maximum likelihood (REML). To account for uncertainty in estimating between-study variance, particularly in analyses with few studies, confidence intervals for pooled estimates were adjusted using either the Knapp–Hartung (HKSJ) or the modified Knapp–Hartung (mKH) method, in accordance with the Cochrane Handbook for Systematic Reviews of Interventions (version 6.5) [19]. When more than two studies were included and τ2 was non-zero, HKSJ adjustment was generally preferred for its favorable statistical properties. In borderline cases, sensitivity analyses compared HKSJ, mKH, and conventional Wald-type intervals, reporting the configuration that provided the most robust and interpretable results.
Given the limited number of studies in each meta-analysis, neither visual (e.g., funnel plots) nor statistical assessments of small-study effects were conducted, and meta-regression was not attempted due to insufficient power. A leave-one-out sensitivity analysis was performed to assess the influence of each individual study on the pooled estimates. Additionally, Baujat plots were generated in R version 4.1.5 (R Foundation for Statistical Computing, Vienna, Austria) using the meta package (version 8.1-0) to visually identify studies contributing most to heterogeneity and to the overall effect size. In these plots, the x-axis represents each study’s contribution to heterogeneity, while the y-axis reflects its influence on the pooled estimate, highlighting potential outliers or highly influential studies. All statistical analyses were conducted using Stata version 19.0 (StataCorp LLC, College Station, TX, USA) and R, as indicated.
GRADE Certainty of Evidence
The certainty of evidence for each outcome was assessed using the GRADE (Grading of Recommendations, Assessment, Development, and Evaluation) approach [20]. Each outcome was then evaluated across the standard GRADE domains (risk of bias, inconsistency, indirectness, imprecision, and publication bias) to determine whether further downgrading was warranted.
Results
A total of 436 records were initially retrieved from database searches. After screening, 36 studies met the eligibility criteria and were included in the qualitative synthesis of this systematic review. Of these, only 4 studies were suitable for quantitative analysis due to their comparative evaluation of robotic versus thoracoscopic approaches. The final dataset comprised 936 pediatric patients from publications spanning 2003 to 2025, of whom 638 underwent robotic surgery. Regarding study design, 19 (52.8%) were retrospective descriptive analyses, 11 (18.8%) were case reports, and 6 (31.3%) were retrospective comparative studies, as detailed in Table 1, Table 2 and Table 3. The article selection process and reasons for exclusion are presented in the PRISMA flow diagram (Figure 1).
Assessment with the MINORS tool indicated that retrospective studies and case reports generally scored between 12 and 14 points (low quality), while comparative studies achieved 20 points (high quality) (Supplementary Material: Table S2). The risk of bias assessment using the ROBINS-I tool across the four analyzed studies indicated an overall moderate risk of bias (Figure 2). This was primarily due to the lack of randomization and potential confounding, as patient allocation to intervention groups was non-random and, in some cases, influenced by parental choice or clinical criterio (Supplementary Material: Table S3). Nevertheless, the studies demonstrated strengths such as clear intervention classification, objective and consistent outcome measurement. No significant biases related to deviations from interventions or outcome reporting were identified. Therefore, while limitations exist, the evidence is moderately reliable for comparing robotic and thoracoscopic pediatric surgeries.
Qualitative Analysis
Tracheomalacia
Kamran et al. first described subsequent robotic-assisted tracheobronchopexy in 2018 in 6 patients (range 5-19 years) [21]. Patients were placed in a semi-prone lateral decubitus position with single-lung ventilation via a bronchial blocker, after which the azygos vein was ligated and partially resected for pledget material; the esophagus was mobilized laterally, and the anterior spinal ligament exposed by displacing fatty tissue and the thoracic duct to the left. Posterior tracheobronchopexy used pledgeted mattress sutures anchored to the anterior longitudinal ligament, with continuous bronchoscopic guidance ensuring optimal airway opening without distortion. All procedures were successfully completed robotically (duration range 4.5–10.5 hours) without postoperative complications, although three patients later required anterior aortopexy and tracheopexy via ministernotomy despite intact posterior repairs, as rigid bronchoscopy showed persistent dynamic anterior airway collapse needing additional support. Torre et al. reported two additional cases performed robotically within their series of six posterior tracheobronchopexies [22]. They positioned patients in a 90° left lateral decubitus position, followed by bed rotation, and they inserted four trocars which were placed differed slightly from thoracoscopic positioning, spaced at least 5 mm apart along a horizontal line in separate intercostal spaces. There were no complications or conversions in these patients.
Pulmonary Diseases
The first robotic lung resection experience was reported by Meehan et al. in 2008, involving 6 patients (2 CPAM, 2 intralobar sequestrations, 1 bronchiectasis, and 1 chronic granulomatous disease) [23]. For the first 4 cases, no robotic thermal device was available, so the surgeon dissected while the assistant sealed vessels with a 5-mm LigaSure, while last two cases were performed with the 8-mm robotic sealer Gyrus PK. Bronchi were divided and ligated with absorbable sutures in all lobectomies. No patient had intraoperative air leaks or significant blood loss. Fully robotic resections were completed in all but one patient (83%); one lobectomy was converted to open due to uncertain bronchus direction. Gao et al. published a 2022 series of 10 cases of intradiaphragmatic extralobar pulmonary sequestration (IDEPS), with 4 operated robotically without intra- or postoperative complications [24]. All IDEPS were entirely within the left diaphragm, with aberrant arteries supplying blood via small artery branches in two cases, the splenic artery in one case, and the abdominal aorta in one case. Jones et al. reported in 2024 a case of pulmonary arteriovenous malformation in a 14-year old girl causing hemoptysis, initially controlled by embolization that required, two years later, robotic ligation due to new bleedings, achieving definitive control of the hemorrhage [25]. The aberrant vessels forming the malformation were dissected, mobilized, skeletonized and multiple Hem-o-lok® clips were placed for ligation, and the vessels were divided.
Several series of robotic-assisted thoracic procedures have been published, such as the one reported in 2015 by Ballouhey et al., which included 4 mediastinal cysts and 2 congenital diaphragmatic hernias (CDH), as well as gastrointestinal cases such as 3 esophageal atresia, one esophagoplasty, and one esophageal myotomy [6]. One CDH case required conversion due to internal crowding. Navarrete-Arellano et al. (2020) described 11 thoracic procedures performed with the Da Vinci Si system, including four pulmonary resections (three congenital cystic adenomatoid malformations and one intralobar sequestration), four diaphragmatic plications (three right diaphragmatic paralysis and one eventration), and one case each of mediastinal teratoma, Ewing’s tumor of the fourth left rib, and pulmonary tuberculosis [5]. They reported one case of prolonged serous drainage after diaphragmatic plication and one conversion to open surgery for a right basal intralobar sequestration due to technical difficulties. In 2022, Soto et al. reported three thoracic cases—two subpleural resections for recurrent left pneumothorax and one extralobar sequestration—all completed robotically without postoperative complications [26].
More recently, Çeltik et al. published Turkey’s largest series of pediatric robot-assisted thoracic procedures to date, involving 30 patients aged 1–17 years [27]. Their cases included nine pulmonary resections (three pulmonary metastases, two bronchogenic cysts, one hydatid lung cyst, one abnormal pulmonary venous return, one CPAM, and one bronchiectasis), 12 thoracic tumors (10 neurogenic tumors, one Ewing sarcoma, and one mature cystic teratoma), and one Morgagni hernia. They also performed eight robotic procedures for esophageal pathologies (three corrosive strictures, two esophageal atresias, one achalasia, and one hiatal hernia). All procedures were completed robotically, with four postoperative complications: Horner’s syndrome after neurogenic tumor excision, atelectasis, pleural effusion, and prolonged air leak in a hydatid cyst case.
Congenital Diaphragmatic Defects
The first CDH repair was reported in 2003 by Luebbe et al. in a 10-year-old girl with Morgagni CDH using the Da Vinci S system. Subsequently, three additional cases of Morgagni CDH were successfully repaired robotically: two by Knight et al. (patients aged 23 months and 5 years) using the Zeus robot and four 5 mm robotic ports, and one by Anderberg et al., who operated on an 18-month-old patient in 145 minutes [2,28,29]. The largest series to date is that of Slater et al., including eight patients with diaphragmatic anomalies: five Bochdalek CDHs, one Morgagni CDH, and two cases of diaphragmatic eventration, all in patients under one year of age [30]. The initial attempts to repair Bockdalek -CDH and eventration were converted to thoracoscopy due to limited maneuverability of the robotic instruments in the confined space. The likely cause was suboptimal port placement—possibly one rib space too close to the target area—which was adjusted in subsequent cases. Delgado-Miguel et al. recently described three CDH repairs in 8-month-old infants: two left-sided Bochdalek CDH and one right-sided Morgagni CDH which were repaired robotically with hernia sac excision, Gore-Tex mesh closure, and a median operative time of 153 minutes, without conversions or complications [31]. Xu et al. compared 20 diaphragmatic eventration cases (9 RATS, 11 VATS) and found a significantly shorter suturing time in the RATS group (27.7±3.4 min vs 48.1±4.2 min; p < 0.001), with no reported complications or conversions [32]. More recently, Alzahrani et al. conducted a multicenter study involving 22 pediatric surgery departments to compare surgical outcomes of various techniques for diaphragmatic eventration [33]. Among 112 patients, 5 underwent RATS, 64 thoracoscopy, 15 thoracotomy, 16 laparoscopy, and 12 laparotomy. In the RATS cohort, plication was performed in four cases and resection–suturing in one, with a recurrence rate comparable to the thoracoscopic group, but showed a higher rate of symptom resolution (100% vs. 56.5%, p = 0.02) at a median follow-up of 48 months.
Thymic Disorders
Hartwich et al. reported in 2012 the first series of robot-assisted thymectomies in nine children with myasthenia gravis (MG), using a left-sided approach with three ports and only a Maryland grasper and hook cautery [34]. All procedures were completed robotically, and operative time gradually decreased from 190 to 136 minutes, with estimated blood loss below 25 mL and no need for transfusions. Grasso et al. reported a successful case of thymectomy in a 12-year-old child using the Da Vinci Xi system, while Hanke performed a robotic resection of a large 10 × 9 cm thymolipoma without complications [35,36]. More recently, Li et al. compared clinical outcomes in juvenile MG patients treated with robotic thymectomy (47 cases) versus those managed with medical therapy alone (20 cases) [37]. They observed that surgical group showed higher anti-acetylcholinesterase receptor antibody positivity (91.5% vs. 65%), shorter disease duration, and greater corticosteroid use at baseline, and Kaplan-Meier analysis revealed a significantly higher rate of complete stable remission after thymectomy.
Mediastinal Tumors
The first report of robotic resection of a mediastinal mass was published by Meehan et al. in 2008, involving five patients (ganglioneuroma, ganglioneuroblastoma, teratoma, germ cell tumor, and a large inflammatory mass of unknown origin) [38]. Procedures used 5-mm robotic instruments in lateral decubitus with three ports in two cases and four in three cases. Specimens were retrieved in an endobag via a trocar site, which was also used for chest tube placement. No conversions or postoperative complications occurred. In 2022, Blanc et al. reported 14 thoracic tumors among their first 100 pediatric robotic resections, including 4 neuroblastomas, 3 ganglioneuroblastomas, 3 ganglioneuromas, 3 thymic tumors, and 1 bronchial carcinoid treated with lobectomy [39]. Postoperative pneumothorax occurred in 2 cases, and 1 neuroblastoma required conversion to open surgery due to limited space. Later, Zeng et al. published the largest series to date with 149 patients (mean age 5.9 years, range 6 months–16 years 8 months), which included 99 neurogenic tumors (neuroblastoma, ganglioneuroblastoma and ganglioneuroma), 19 foregut cysts (bronchogenic and enterogenic cysts), 12 thymic (teratoma and thymic cysts), 9 angiolymphatic (lymphangioma and haemangioma), 6 lipogenic (lipoblastoma and lipoma) and 4 soft tissue sarcomas (rhabdomyosarcoma, Ewing sarcoma and infantile fibrosarcoma) [40]. Conversion was needed in 4 cases due to aortic or pericardial invasion (3 cases) and bleeding (1 case). All patients recovered well, with no tumor recurrence or mortality during 3–23 months of follow-up. More recently, Svetanoff et al. reported 17 thoracic neuroblastic tumors (8 ganglioneuroblastomas, 6 ganglioneuromas, 2 neuroblastomas, and 1 paraganglioma) resected with Si and Xi systems, with a median operative time of 124 minutes [41]. One chyle leak required interventional drainage and thoracostomy, and 2 cases were converted to open surgery due to poor visualization and limited working space. Furthermore, several cases reports of mediastinal tumors have been described in recent years. In 2014, Toker et al. successfully resected a bronchogenic cyst using Maryland and ProGrasp [42]. After opening the mediastinal pleura, the cyst was removed en bloc without bleeding or tissue damage, through an enlarged 2.5 cm right arm port. Nemoto et al. described a sympathetic trunk ganglioneuroma completely resected while preserving the trunk and the artery of Adamkiewicz, with an uneventful recovery and no neurological complications [43]. Yamaguchi et al. used point-of-care lung ultrasound to confirm lung isolation during one-lung ventilation for robotic resection of a right paraspinal mass in a 7-year-old [44]. Ochi et al. reported a 7 cm right posterior mediastinal neuroblastoma with bone and marrow metastases [45]. Chemotherapy aided tumor demarcation, and robotic visualization and articulation facilitated dissection from ribs, intercostal spaces, paravertebral region, and azygos vein. Histopathology confirmed an intact capsule and complete resection. Riccipetitoni et al. safely resected a paraspinal ganglioneuroblastoma with vessel encasement using RATS, without complications [46]. Prasad et al. reported a 6 × 4 cm posterior mediastinal ganglioneuroma, extending from T2 to the upper border of T6, successfully resected with the Xi system in 130 minutes [47]. Bahadır et al. reported a thoracic paraganglioma resected with the Si robotic system in an 11-year-old [48]. More recently, Kaneda et al. described the first thoracic procedure using the Single Port (SP) model for a ganglioneuroma via a 4.0-cm subcostal incision with a subcutaneous tunnel to the thoracic cavity, completed successfully in 250 minutes [49].
Quantitative Analysis
Operative Time
For the meta-analysis of operative time (minutes), four studies were included (223 patients in RATS; 224 in VATS), and a random-effects model was fitted using REML with mKH adjustments (Figure 3). The pooled mean difference favored the VATS group over the RATS group, indicating significantly shorter operative times in VATS: 26.37 minutes (95% CI: 3.26 to 49.47; model p = 0.04). Between-study heterogeneity was moderate (I2 = 48.8%), and Cochran’s Q test indicated significant heterogeneity (p = 0.01). Notably, the study by Durand et al. [10], despite its minimal weight (1.9%) due to small sample size, had a disproportionate influence on the pooled estimate. A leave-one-out sensitivity analysis revealed that excluding this study resulted in the largest change, decreasing the estimated benefit of VATS to 24.43 minutes (95% CI: 17.56 to 31.29; p < 0.0001).
Length of Hospital Stay
For the meta-analysis of length of hospital stay (days), four studies were included (223 patients in RATS; 224 in VATS). A random-effects model was fitted using REML with mKH adjustments (Figure 4). The pooled mean difference favored the RATS group, indicating a statistically significant reduction in hospital stay compared to VATS: –0.70 days (95% CI: –1.22 to –0.17; model p = 0.02). Between-study heterogeneity was low (I2 = 24.78%), and Cochran’s Q test was not significant (p = 0.28). Leave-one-out sensitivity analysis confirmed that statistical significance was preserved across all iterations. The exclusion that most attenuated the effect was Liang et al. [7], which reduced the pooled estimate to –0.57 days (95% CI: –0.87 to –0.26); however, the difference remained statistically significant. Statistical significance was preserved across all iterations, confirming the robustness of the result.
Chest Tube Duration
For the meta-analysis of chest tube duration (days), four studies were included (223 patients in RATS; 224 in VATS), and a random-effects model was fitted using REML with mKH adjustments (Figure 5). The pooled mean difference favored the RATS group but did not reach statistical significance: –0.70 days (95% CI: –1.81 to 0.42; model p = 0.14). Between-study heterogeneity was extremely high (I2 = 90.43%), and the Cochran’s Q test was significant (p < 0.001). Leave-one-out sensitivity analysis showed that statistical significance emerged only when Li et al. [9] was excluded, yielding a revised pooled estimate of –1.07 days (95% CI: –1.45 to –0.68; p < 0.001) in favor of shorter chest tube duration with RATS compared to VATS.
Conversion to Open Surgery
Regarding conversion to thoracotomy, meta-analytical modeling was not justified due to incomplete outcome reporting: one study reported no events in either group, and another presented zero events in one treatment arm. Under these conditions, pooled estimates would lack statistical validity and clinical interpretability.
Postoperative Complications
For the meta-analysis of overall complications (risk ratio), four studies were included (223 patients in RATS; 224 in VATS), and a random-effects model was fitted using REML with Wald-Type intervals (Figure 6). The pooled risk ratio was 1.16 (95% CI: 0.83 to 1.63; model p = 0.39), indicating no statistically significant difference between RATS and VATS. Between-study heterogeneity was negligible (I2 = 0%), and the Cochran’s Q test was not statistically significant (p = 0.15). Leave-one-out sensitivity analysis did not identify any exclusion that rendered the overall result statistically significant. However, omitting Li et al. [9] yielded a non-significant trend favoring RATS—that is, indicating fewer complications with robotic surgery—with a recalculated risk ratio of 1.27 (95% CI: 0.90 to 1.80; p = 0.17). This is consistent with their reported complication rates: 2 of 29 patients in the RATS group versus 12 of 42 in the VATS group. Conversely, Liang et al. [7] reported a higher complication rate in the RATS group (28 of 93) compared to VATS (16 of 77), and excluding this study shifted the model modestly in favor of VATS (RR = 0.77, 95% CI: 0.31 to 1.94; p = 0.58). Notably, none of these sensitivity analyses yielded statistically significant results.
Findings from Baujat Plots
The Baujat plots, derived from the REML with mKH adjustment, offer a two-dimensional visualization of each study’s influence on the meta-analytic model (Figure 7). The X-axis represents the study’s contribution to total heterogeneity (Cochran’s Q), while the Y-axis reflects its influence on the pooled effect. Importantly, the X-axis is not standardized across outcomes: it adapts to the magnitude of heterogeneity within each analysis. Therefore, contributions must be interpreted within the context of each outcome, not comparatively across plots. These visualizations complement formal sensitivity analyses by identifying potentially influential studies and clarifying their role in observed inconsistencies—whether stemming from clinical differences, sample size disparities, or reporting variability.
In the upper-left panel (operative time), Durand et al. [10] contributed most strongly to heterogeneity, likely due to their atypically prolonged operative times, but had virtually no impact on the overall effect—probably due to small sample size. In contrast, Liang et al. [7] had the most significant influence on the pooled estimate. This decoupling suggests that while Durand et al. introduced inconsistency across studies, Liang’s values shifted the overall result, despite making a minimal contribution to variance. In the upper-right panel (hospitalization days), Liang et al. appear in the upper-right corner, indicating a significant influence on both heterogeneity and the pooled effect. All other studies showed moderate contributions to heterogeneity, but only Li et al. [9] had moderate leverage on the overall estimate. Durand et al. had a negligible impact on the summary effect despite moderate heterogeneity contribution. In the lower-left panel (chest tube days), Li et al. emerged as an outlier with extreme influence, appearing in the upper-right quadrant of the plot. This pattern aligns with the leave-one-out analysis, where exclusion of this study altered the statistical significance of the pooled estimate. Liang et al. exhibited moderate contributions to both heterogeneity and overall effect, while Wei et al. had minimal influence on either dimension. Durand et al. contributed negligibly to both heterogeneity and the summary effect. In the lower-right panel (overall complications), Liang et al. exerted the highest influence on the pooled effect, with a small-to-moderate contribution to heterogeneity. Li et al. contributed notably to heterogeneity and moderately to the overall effect. Wei et al. and Durand et al. had no impact on either axis. It should be noted that Baujat plots are statistical visualization tools that are highly dependent on the number of studies and their power. Therefore, with only four observations, the interpretation of the findings should be approached with great caution and considered exploratory in nature.
Methodological Strengths and Limitations
This review is strengthened by the rigorous use of random-effects models fitted through REML, with confidence intervals adjusted using mKH methods, in line with current best-practice guidelines (Cochrane Handbook for Systematic Reviews of Interventions, version 6.5) [19]. In addition, the influence of individual studies was systematically explored through both leave-one-out analyses and Baujat plots, enabling a robust evaluation of heterogeneity sources. Nonetheless, the review is limited by the small sample sizes, the low number of included studies for each outcome, and the inability to perform meta-analytical modeling for some endpoints—such as conversion to thoracotomy—due to incomplete data structures. Furthermore, heterogeneity analysis (meta-regression models) could not be performed due to the low number of studies included in this review.
GRADE Certainty of Evidence
Using the GRADE framework, the certainty of evidence for the outcomes of RATS versus VATS in pediatric patients was assessed. Given that all included studies were retrospective comparative analyses, the starting level of certainty was rated as low. For operative time and length of hospital stay, the evidence was rated as low certainty due to the retrospective nature of all included studies, which introduces potential risk of bias, although effect estimates were consistent and statistically significant for these outcomes. For chest tube duration and postoperative complications, the evidence was downgraded to very low certainty owing to serious heterogeneity, imprecision, and inconsistency across studies, with results heavily influenced by individual study data. Overall, these limitations highlight the need for cautious interpretation of the findings.
Discussion
To our knowledge, this is the first systematic review and meta-analysis focused exclusively on robotic thoracic surgery in the pediatric population. Previous publications addressing this topic have been limited to narrative reviews or small single-center series, which lack the methodological rigor and quantitative synthesis provided in the present work [50]. Nonetheless, data on pediatric thoracic robotic surgery remain scarce. In a literature review, Saxena et al. found only seven pertinent publications between 2017 and 2022—four addressing thoracic procedures and three focusing on esophageal surgery—underscoring the limited evidence and few case series dedicated to this field in children [51]. By combining qualitative and quantitative analyses, our study offers a more comprehensive understanding of the current evidence base, highlighting both the potential advantages and the persisting limitations of robotic approaches in this highly selected patient group. Robotic assistance represents the latest advancement in pediatric thoracoscopic surgery, but its benefits still require comprehensive evaluation and validation. Its integration into clinical practice also demands adaptation of training protocols for pediatric thoracic surgeons [52]. The qualitative synthesis revealed a consistent trend toward feasibility and safety of robotic thoracic procedures across various pediatric indications, applied to a broad spectrum of pathologies, reflecting its versatility within this field.
In patients with tracheomalacia, aortopexy may be insufficient when collapse stems from posterior membranous intrusion. Posterior tracheobronchopexy directly corrects this, markedly improving respiratory status [21]. Intraoperative flexible bronchoscopy is essential to guide precise, well-oriented sutures while avoiding full-thickness placement. Robotic instruments provide superior articulation for complex angles and integrate real-time bronchoscopic views into the surgeon’s console, unlike standard thoracoscopy, which relies on separate monitors [22]. In addition, robotic surgery improves visualization, streamlines esophageal dissection, and enables more accurate, efficient pexy of the trachea and bronchi along their entire length. In congenital diaphragmatic anomalies, most cases were successfully completed robotically, with early conversions in initial attempts due to instrument crowding and one Bochdalek hernia recurrence, likely from excessive tension in a primary closure without mesh. Although some reports warn of higher recurrence with minimally invasive repair, no direct comparisons with thoracoscopy exist [53]. Only one recurrence has been documented, occurring 18 months after a Bochdalek CDH repair, while operative time has progressively decreased across reports—from 227 minutes of Knight et al. [28] to 140 minutes reported by Anderberg et al. [29] and 80 minutes in Slater et al. study [30]. Robotic articulation offers improved access to defects, and when mesh is required, intracorporeal suturing can provide greater precision and controlIn this setting, the robot’s enhanced optical magnification, 3D stereoscopic view, improved instrument flexibility, and superior ergonomics allowed robot-assisted thoracoscopic plication to overcome intercostal access constraints, enabling more accurate and efficient suturing and knot-tying in challenging areas such as the costophrenic and cardiophrenic angles [32,33].
Robotic surgery may be especially advantageous for thoracic masses, as articulating instruments can maneuver around rigid tumors more effectively than standard thoracoscopic tools, which often face suboptimal angles within the fixed chest cavity [40]. In addition, advances in one-lung ventilation anesthesia have broadened thoracoscopic lung and mediastinal tumor surgery in children with favorable results [54]. Still, limited instrument flexibility, longer operative times leading to hand tremor, and the reduced detail of 2D imaging compared to 3D make solid tumor navigation more challenging and potentially riskier. The cervicomediastinal area contains many vital vessels and nerves, making thoracoscopic and open surgery risky. Robotic instruments, being more flexible than thoracoscopic tools, allow easier navigation around the tumor and better identification of vessels, nerves, and tissues at the top of the thoracic cavity, enhancing surgical safety [40]. Children who are candidates for thoracoscopy are generally suitable for RATS, with mediastinal tumors under 8 cm often manageable minimally invasively [55,56]. The da Vinci single-port system, previously limited to pediatric urology and gastrointestinal surgery, has been used for thoracic tumor resection via a subcostal approach, as its 2.5 cm port is too large for intercostal placement. This technique, avoiding intercostal dissection, may help prevent future funnel chest and thoracic deformities [49]. In pediatric myasthenia gravis, robotic thymectomy is also safe and offers technical benefits without major increases in cost or operative time. Evidence from adults shows it achieves more complete resections than VATS, with higher rates of stable remission [57].
While robotic-assisted thoracic surgery has been performed in smaller neonates, it generally yields better results in patients over 6 months of age and weighing more than 8 kg, as this allows improved instrument handling and visualization [40]. For elective procedures on benign cystic lesions without symptoms, postponing surgery until this age and weight threshold can be beneficial [58]. In contrast, for solid tumors, surgery is often performed regardless of age due to the potential risk of malignancy [40]. Nonetheless, certain studies have concluded that body weight alone should not be viewed as an absolute barrier to performing robotic surgical procedures [59]. In pediatric patients undergoing lobectomy for congenital lung malformations, a large propensity-matched multicenter analysis demonstrated comparable short-term outcomes between VATS and open thoracotomy—while VATS significantly reduced hospital stay [60]. The quantitative analysis results in our study suggest certain advantages of RATS over VATS, such as a shorter length of hospital stay, although no statistically significant difference was observed in chest tube duration. Operative time was significantly longer for RATS, most likely reflecting both smaller sample sizes and the early stage of the learning curve for this technique. However, Li et al. shown that, when instrument exchange and docking times are excluded, the actual operative time does not differ significantly between the two groups [9]. Regarding postoperative complications, no significant differences were found; however, it is important to note that the definitions and reporting of complications varied considerably among studies. For instance, some events, such as postoperative fever, may represent mild or subjective findings, while others—like pneumothorax or pleural effusion—are more objective and clinically meaningful. In the study by Durant et al., the RATS group reported two complications, both Clavien–Dindo grade II (pleural effusion and lung infection), whereas the VATS group had one grade II event (pneumonitis) and three grade IIIa events (pneumothorax requiring percutaneous drainage) [10]. This heterogeneity in complication types and reporting standards limits the reliability and comparability of pooled complication rates across studies, making interpretation more complex. Postoperative complications in other pediatric robotic surgery series range from 0% to 15%, while intraoperative events remain rare [61]. In this systematic review, 36 complications (5.6%) and 12 conversions were recorded, primarily due to limited working space in smaller patients, resulting in a conversion rate of 1.8%, while previous studies of robot-assisted surgery procedures in pediatric children, reported conversion rates range from 2.5% to 6% [61,62]. Careful patient selection is essential, particularly during the learning curve, avoiding very young children, large thoracic lesions, or adhesions to vital vessels, as these conditions heighten the risk of conversion from poor exposure, prolonged operative time, or bleeding.
Our study has several limitations. First, as with any meta-analysis of retrospective comparisons, it inherits the biases of the included studies, none of which were randomized. Given the nature of the topic, opportunities for randomization or blinding are minimal. Nonetheless, well-designed observational studies can greatly improve validity, beyond simply increasing sample size. Second, procedural variables—such as differences in Da Vinci system generations, sutures, drugs, and surgeon experience—may have influenced outcomes. Moreover, none of the studies specified the number of surgeons involved or whether these RATS cases represented their initial experience with the technique.
Conclusion
This systematic review and meta-analysis provides the first comprehensive synthesis of RATS in pediatric patients. The evidence demonstrates that RATS may be considered as a safe and feasible approach across a wide spectrum of thoracic pathologies, including congenital diaphragmatic defects, mediastinal tumors, pulmonary resections, and tracheobronchial procedures. Qualitative analysis highlights the versatility of robotic platforms, offering enhanced visualization, superior instrument articulation, and improved precision in complex anatomical regions compared with conventional thoracoscopy. The meta-analytical findings suggest potential clinical advantages of RATS over VATS in selected perioperative outcomes. RATS was associated with shorter hospital stays and comparable complication rates relative to VATS, supporting its clinical effectiveness. While operative times are significantly longer for RATS, chest tube duration showed a nonsignificant trend favoring RATS. However, these conclusions must be interpreted with caution given multiple limitations, including the retrospective design of all included studies, a strong predominance of Chinese cohorts, the high degree of heterogeneity, and potential confounding from learning curve effects—such as in Durand et al., where only 7 and 11 patients were included per group, and where operative time and length of hospital stay were disproportionately high compared to other studies. Despite these caveats, this review provides a preliminary landscape of the currently scarce evidence base and offers a foundational framework to guide and justify future, more definitive investigations.
Supplementary Materials
The conversions performed and the data extracted from each article for the meta-analytic models are attached as Supplementary Material S4.
Funding
This research did not receive any funding for its development.
Conflicts of Interest
The authors declare no conflict of interest.
Registration and Protocol
This systematic review is registered in the PROSPERO database (https://www.crd.york.ac.uk/PROSPERO/view/CRD420251091235).
References
- Melfi FM, Menconi GF, Mariani AM, Angeletti CA. Early experience with robotic technology for thoracoscopic surgery. Eur J Cardiothorac Surg. 2002, 21, 864–868. [Google Scholar] [CrossRef]
- Schwartz G, Sancheti M, Blasberg J. Robotic Thoracic Surgery. Surg Clin North Am. 2020, 100, 237–248. [Google Scholar] [CrossRef]
- Luebbe B, Woo R, Wolf S, Irish M. Robotically assisted minimally invasive surgery in a pediatric population: initial experience, technical considerations, and description of the da Vinci Surgical System. Pediatr Endosurg Innov Tech. 2003, 7, 385–402. [Google Scholar] [CrossRef]
- Meehan, JJ. Robotic surgery in small children: is there room for this? J Laparoendosc Adv Surg Tech A. 2009, 19, 707–712. [Google Scholar] [CrossRef]
- Navarrete-Arellano, M. Thoracic surgery by minimally invasive robot-assisted in children: experience and current status. Mini-invasive Surg. 2020, 4, 9. [Google Scholar]
- Ballouhey Q, Villemagne T, Cros J, Vacquerie V, Bérenguer D, Braik K, Szwarc C, Longis B, Lardy H, Fourcade L. Assessment of paediatric thoracic robotic surgery. Interact Cardiovasc Thorac Surg. 2015, 20, 300–303. [Google Scholar] [CrossRef] [PubMed]
- Liang L, Tan Z, Huang T, Gao Y, Zhang J, Yu J, Xia J, Shu Q. Efficacy of robot-assisted thoracoscopic surgery in the treatment of pulmonary sequestration in children. World J Pediatr Surg. 2024, 7, e000748. [Google Scholar] [CrossRef]
- Wei S, Huang T, Liang L, Gao Y, Zhang J, Xia J, Yu L, Shu Q, Tan Z. Efficacy of Da Vinci Robot-assisted Thoracoscopic Surgery in Children With Congenital Cystic Adenomatiod Malformation. J Pediatr Surg. 2024, 59, 1458–1462. [Google Scholar] [CrossRef]
- Li S, Luo Z, Li K, Li Y, Yang D, Cao G, Zhang X, Zhou Y, Chi S, Tang S. Robotic approach for pediatric pulmonary resection: preliminary investigation and comparative study with thoracoscopic approach. J Thorac Dis. 2022, 14, 3854–3864. [Google Scholar] [CrossRef] [PubMed]
- Durand M, Musleh L, Vatta F, Orofino G, Querciagrossa S, Jugie M, Bustarret O, Delacourt C, Sarnacki S, Blanc T, Khen-Dunlop N. Robotic lobectomy in children with severe bronchiectasis: A worthwhile new technology. J Pediatr Surg. 2021, 56, 1606–1610. [Google Scholar] [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021, 372, n71. [Google Scholar]
- Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ. 2021, 372, n160. [Google Scholar]
- Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef] [PubMed]
- Sterne JAC, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomized studies of interventions. BMJ. 2016, 355, i4919. [Google Scholar]
- Wan X, Wang W, Liu J, Tong T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014, 14, 135. [Google Scholar]
- Luo D, Wan X, Liu J, Tong T. Optimally estimating the sample mean from the sample size, median, mid-range, and/or mid-quartile range. Stat Methods Med Res. 2018, 27, 1785–1805. [Google Scholar] [CrossRef]
- Shi J, Luo D, Wan X, Liu Y, Liu J, Bian Z, Tong T. Detecting the skewness of data from the sample size and the five-number summary. Stat Methods Med Res. 2023, 32, 1338–1360. [Google Scholar] [CrossRef]
- McGrath S, Zhao X, Steele R, Thombs BD, Benedetti A; DEPRESsion Screening Data (DEPRESSD) Collaboration. Estimating the sample mean and standard deviation from commonly reported quantiles in meta-analysis. Stat Methods Med Res. 2020, 29, 2520–2537. [Google Scholar] [CrossRef]
- Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA (editors). Cochrane Handbook for Systematic Reviews of Interventions version 6.5 (updated August 2024). Cochrane, 2024. Available from www.cochrane.org/handbook (access on: 01/08/2025).
- Newcombe RG, Bender R. Implementing GRADE: calculating the risk difference from the baseline risk and the relative risk. Evid Based Med. 2014, 19, 6–8. [Google Scholar] [CrossRef]
- Kamran A, Hamilton TE, Zendejas B, Nath B, Jennings RW, Smithers CJ. Minimally Invasive Surgical Approach for Posterior Tracheopexy to Treat Severe Tracheomalacia: Lessons Learned from Initial Case Series. J Laparoendosc Adv Surg Tech A. 2018, 28, 1525–1530. [Google Scholar] [CrossRef] [PubMed]
- Torre M, Guerriero V, Moscatelli A, Disma N, Lena F, Palo F, et al. Posterior tracheobronchopexy with thoracoscopic or robotic approach: technical details. J Pediatr Endosc Surg. 2020, 2, 169–174. [Google Scholar] [CrossRef]
- Meehan JJ, Phearman L, Sandler A. Robotic pulmonary resections in children: series report and introduction of a new robotic instrument. J Laparoendosc Adv Surg Tech A. 2008, 18, 293–295. [Google Scholar] [CrossRef] [PubMed]
- Gao Y, Han X, Jin J, Tan Z. Ten cases of intradiaphragmatic extralobar pulmonary sequestration: a single-center experience. World Jnl Ped Surgery 2022, 5, e000334. [Google Scholar] [CrossRef]
- Jones RE, Freedman-Weiss M, Ha J, Paranjape S, Garcia AV. Robotic ligation of a pulmonary arteriovenous malformation in a teenaged child: a case report. J Pediatr Surg Case Rep. 2024, 101, 102759. [Google Scholar] [CrossRef]
- Soto Beauregard C, Rodríguez de Alarcón García J, Domínguez Amillo EE, Gómez Cervantes M, Ávila Ramírez LF. Implementing a pediatric robotic surgery program: future perspectives. Cir Pediatr. 2022, 35, 187–195. [Google Scholar]
- Çeltik Ü, Şahutoğlu C, Dökümcü Z, Özcan C, Erdener A. Examining the potential of advanced robotic-assisted thoracic surgery in pediatric cases. J Pediatr Res. 2024, 11, 75–79. [Google Scholar]
- Knight CG, Gidell KM, Lanning D, Lorincz A, Langenburg SE, Klein MD. Laparoscopic Morgagni hernia repair in children using robotic instruments. J Laparoendosc Adv Surg Tech A. 2005, 15, 482–486. [Google Scholar] [CrossRef]
- Anderberg M, Kockum CC, Arnbjornsson E. Morgagni hernia repair in a small child using da Vinci robotic instruments--a case report. Eur J Pediatr Surg. 2009, 19, 110–112. [Google Scholar] [CrossRef]
- Slater BJ, Meehan JJ. Robotic repair of congenital diaphragmatic anomalies J Laparoendosc Adv Surg Tech A. 2009, 19 Suppl 1:S123-7.
- Delgado-Miguel C, Camps JI. Robotic surgery in newborns and infants under 12-months: Is it feasible? Asian J Surg. 2025 August 13 Online ahead of publish. [CrossRef]
- Xu PP, Chang XP, Tang ST, Li S, Cao GQ, Zhang X, et al. Robot-assisted thoracoscopic plication for diaphragmatic eventration. J Pediatr Surg. 2020, 55, 2787–2790. [Google Scholar] [CrossRef] [PubMed]
- Alzahrani K, Heng L, Khen-Dunlop N, Panait N, Hervieux E, Grynberg L, et al. Comparative Outcomes of Surgical Techniques for Congenital Diaphragmatic Eventration in Children: A Multicenter Retrospective Cohort Analysis. Eur J Pediatr Surg. 2025 Mar 18. Epub ahead of print.
- Hartwich J, Tyagi S, Margaron F, Oitcica C, Teasley J, Lanning D. Robot-assisted thoracoscopic thymectomy for treating myasthenia gravis in children. J Laparoend Adv Surg Tech 2012, 22, 925–929. [Google Scholar] [CrossRef] [PubMed]
- Grasso F, De Leonibus L, Bertozzi M, Sica M, Angotti R, Luzzi L, Molinaro F, Messina M, Paladini P. Robotic-assisted thoracoscopy thymectomy for juvenile myasthenia gravis. J Pediatr Surg Case Rep. 2020, 62, 101541. [Google Scholar] [CrossRef]
- Hanke R, Emr B, Taylor M, Fahy AS. Robotic resection of a giant thymolipoma in a pediatric patient. J Surg Case Rep. 2024, 2024, rjae691. [Google Scholar] [CrossRef]
- Li Z, Li F, Zhang H, Swierzy M, Ismail M, Meisel A, Rueckert JC. Outcomes of Juvenile Myasthenia Gravis: A Comparison of Robotic Thymectomy With Medication Treatment. Ann Thorac Surg. 2022, 113, 295–301. [Google Scholar] [CrossRef]
- Meehan JJ, Sandler AD. Robotic resection of mediastinal masses in children. J Laparoendosc Adv Surg Tech A. 2008, 18, 114–119. [Google Scholar] [CrossRef]
- Blanc T, Meignan P, Vinit N, Ballouhey Q, Pio L, Capito C, et al. Robotic Surgery in Pediatric Oncology: Lessons Learned from the First 100 Tumors-A Nationwide Experience. Ann Surg Oncol. 2022, 29, 1315–1326. [Google Scholar] [CrossRef]
- Zeng Q, Chen C, Zhang N, Yu J, Yan D, Xu C, Liu D, Zhang Q, Zhang X. Robot-assisted thoracoscopic surgery for mediastinal tumours in children: a single-centre retrospective study of 149 patients. Eur J Cardiothorac Surg. 2023, 64, ezad362.
- Svetanoff WJ, Carter M, Diefenbach KA, Michalsky M, DaJusta D, Gong E, Lautz TB, Aldrink JH. Robotic-assisted Pediatric Thoracic and Abdominal Tumor Resection: An Initial Multi-center Review. J Pediatr Surg. 2024, 59, 1619–1625. [Google Scholar] [CrossRef] [PubMed]
- Toker A, Ayalp K, Grusina-Ujumaza J, Kaba E. Resection of a bronchogenic cyst in the first decade of life with robotic surgery. Interact Cardiovasc Thorac Surg. 2014, 19, 321–323. [Google Scholar] [CrossRef] [PubMed]
- Nemoto Y, Kuroda K, Mori M, et al. Robot-assisted thoracoscopic resection of a posterior mediastinal tumor with preserving the artery of Adamkiewicz. Surg Case Rep.
- Yamaguchi Y, Moharir A, Burrier C, Tobias JD. Point-of-care lung ultrasound to evaluate lung isolation during one-lung ventilation in children: A case report. Saudi J Anaesth. 2019, 13, 243–245. [Google Scholar] [CrossRef] [PubMed]
- Ochi T, Koga H, Ueno H, Fujimura J, Kosaka S, Miyake Y, Yoshida S, Lane GJ, Suzuki K, Yamataka A. Successful all robotic-assisted excision of highly malignant mediastinal neuroblastoma in a toddler: A case report. Asian J Endosc Surg. 2023, 16, 542–545. [Google Scholar] [CrossRef] [PubMed]
- Riccipetitoni G, Bertozzi M, Gazzaneo M, Raffaele A, Vatta F. The role of video-assisted thoracoscopic surgery in pediatric oncology: single-center experience and review of the literature. Front Pediatr. 2021, 9, 721914. [Google Scholar] [CrossRef] [PubMed]
- Prasad A, Jain P, Narang R. Robotic assisted thoracoscopic surgery (RATS) for excision of posterior mediastinal mass. J Pediatr Endosc Surg. 2023, 5, 175–177. [Google Scholar] [CrossRef]
- Bahadır GB, Çalışkan MB, Ünlü Ballı SE, Atasever HE, Korkmaz G, Yıldırım İ, et al. Robotic Assisted Endoscopic Surgery Practices in Pediatric Surgery, Single Center Experience. Turkish J Pediatr Dis. 2023, 17, 147–153. [Google Scholar] [CrossRef]
- Kaneda S, Kawaguchi K, Ito A, Ito D, Kawaguchi T, Shimamoto A, Takao M. Subcostal approach using the single-port robotic system for a giant ganglioneuroma in a child. JTCVS Techniques. 2025, 32, 141–143. [Google Scholar] [CrossRef]
- Aithal S, Sinha A, Pathak M. Robotic assisted thoracoscopic surgery in children: a narrated review. J Pediatr Endosc Surg. 2024, 6, 107–114. [Google Scholar] [CrossRef]
- Saxena AK, Borgogni R, Escolino M, D’Auria D, Esposito C. Narrative review: robotic pediatric surgery-current status and future perspectives. Transl Pediatr 2023, 12, 1875–1886. [Google Scholar] [CrossRef]
- Lima, M. Editorial: Pediatric thoracic surgery. Front Pediatr. 2023, 11, 1132803. [Google Scholar] [CrossRef]
- Arca MJ, Barnhart DC, Lelli JL Jr, Greenfeld J, Harmon CM, Hirschl RB, Teitelbaum DH. Early experience with minimally invasive repair of congenital diaphragmatic hernias: results and lessons learned. J Pediatr Surg. 2003, 38, 1563–1568. [Google Scholar] [CrossRef]
- Li XF, Jin L, Yang JM, Luo QS, Liu HM, Yu H. Effect of ventilation mode on postoperative pulmonary complications following lung resection surgery: a randomised controlled trial. Anaesthesia. 2022, 77, 1219–1227. [Google Scholar] [CrossRef]
- Li XK, Cong ZZ, Xu Y, Zhou H, Wu WJ, Wang GM et al. Clinical efficacy of robot-assisted thoracoscopic surgery for posterior mediastinal neurogenic tumors. J Thorac Dis 2020, 12, 3065–3072. [Google Scholar] [CrossRef] [PubMed]
- Fraga JC, Rothenberg S, Kiely E, Pierro A. Video-assisted thoracic surgery resection for pediatric mediastinal neurogenic tumors. J Pediatr Surg 2012, 47, 1349–1353. [Google Scholar] [CrossRef]
- Ruckert JC, Swierzy M, Ismail M. Comparison of robotic and nonrobotic thorascopic thymectomy: A cohort study. J Thoracic Cardiovasc Surg 2011, 141, 673–677. [Google Scholar] [CrossRef] [PubMed]
- Fievet L, D’Journo XB, Guys JM, Thomas PA, De Lagausie P. Bronchogenic cyst: best time for surgery? Ann Thorac Surg 2012, 94, 1695–1699.
- Molinaro F, Angotti R, Bindi E, et al. Low weight child: can it be considered a limit of robotic surgery? Experience of two centers. J Laparoendosc Adv Surg Tech 2019, 29, 698e702. [Google Scholar]
- Raymond SL, Sacks MA, Hashmi A, Robertson JO, Moores D, Tagge EP, et al. Short-term outcomes of thoracoscopic versus open lobectomy for congenital lung malformations. Pediatr Surg Int. 2023, 39, 155. [Google Scholar] [CrossRef]
- Sinha SK, Haddad M. Robot-assisted surgery in children: current status. J Robotic Surg. 2008, 1, 243–246. [Google Scholar] [CrossRef]
- Najmaldin A, Antao B. Early experience of tele-robotic sugery in children. Int J Med Robot Comp Assist Surg. 2007, 3, 199–202. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flowchart.
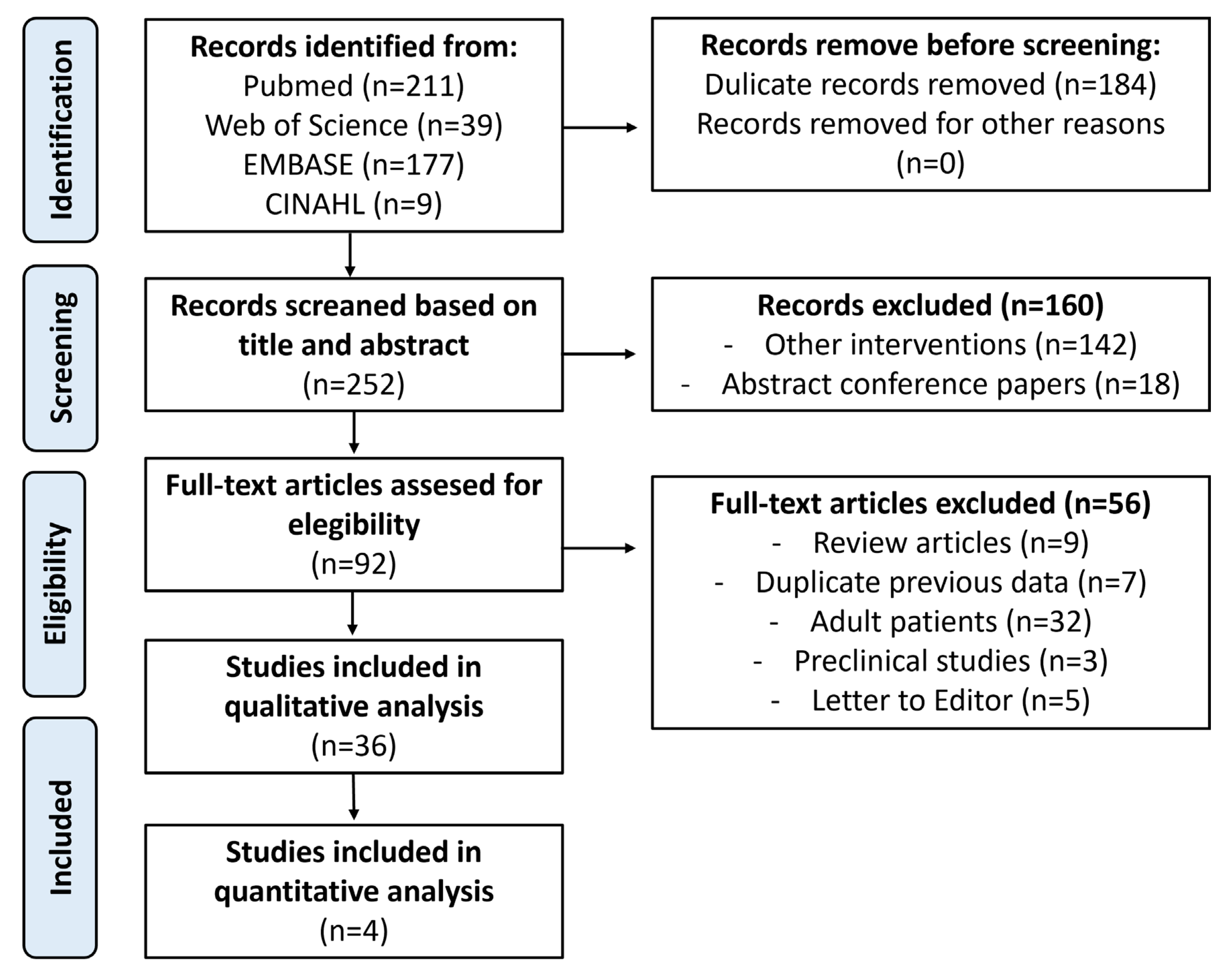
Figure 2.
Risk of bias of the included studies using ROBINS-I tool.
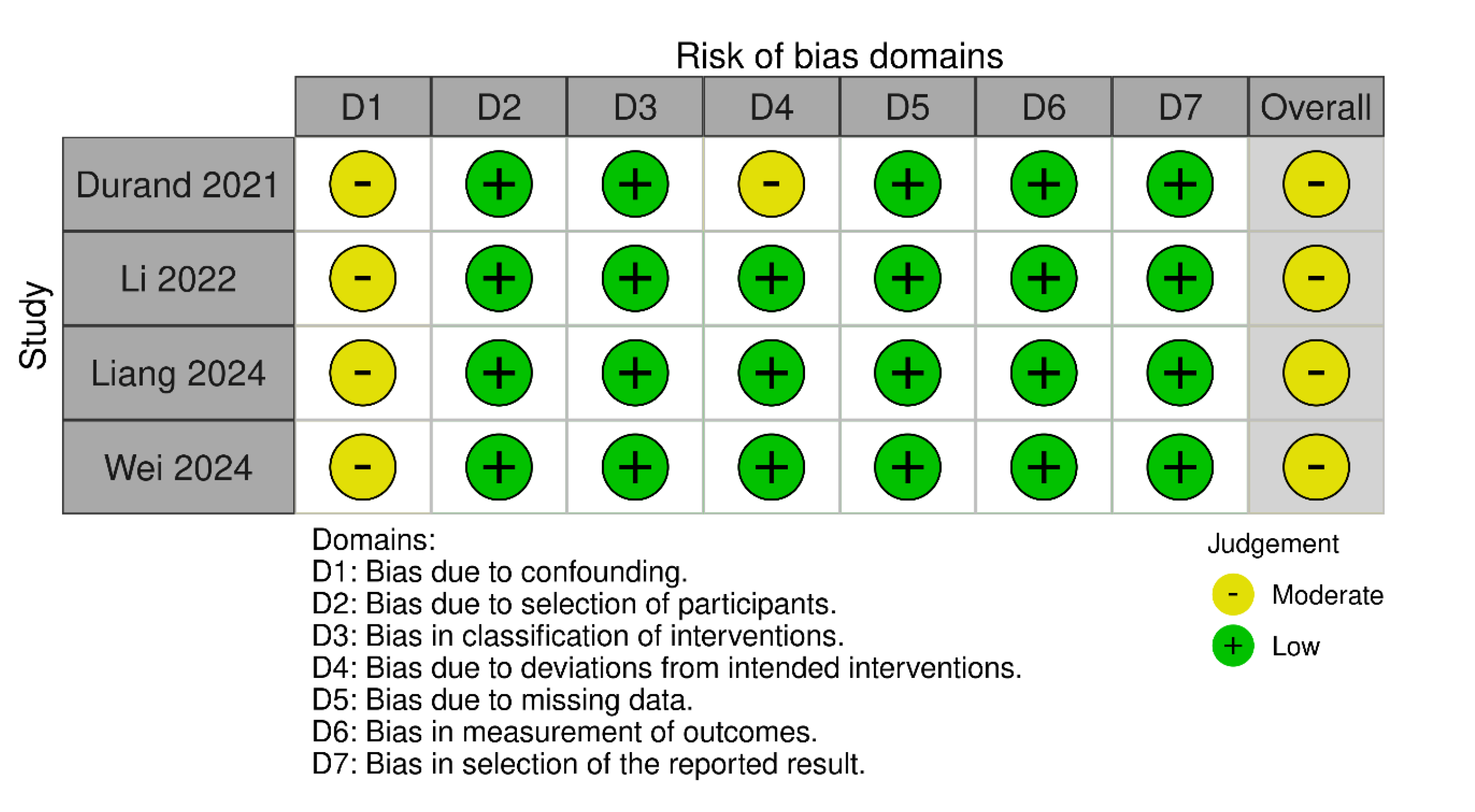
Figure 3.
Meta-analysis of operative time (in minutes).
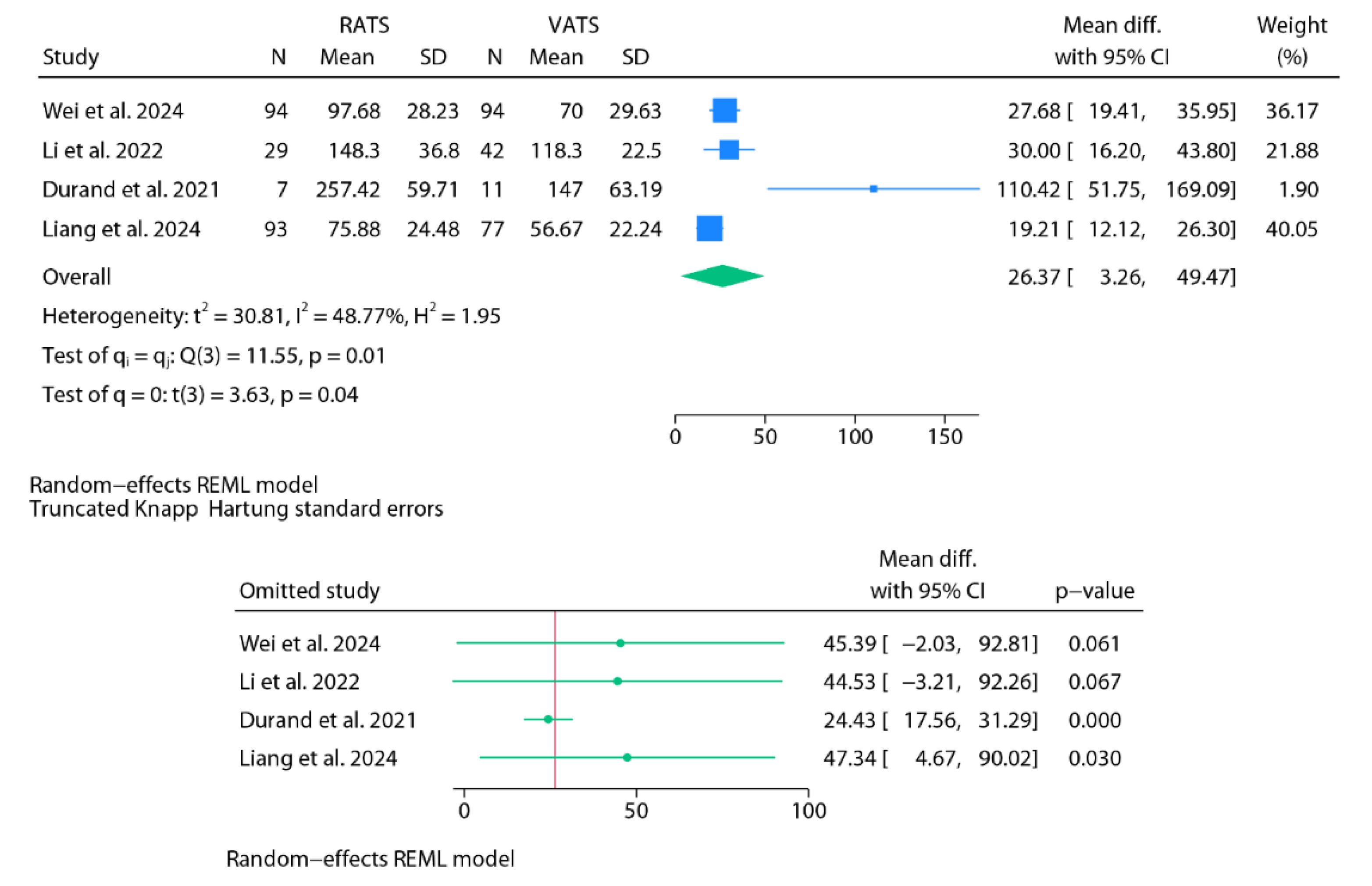
Figure 4.
Meta-analysis of hospital stay (in days).
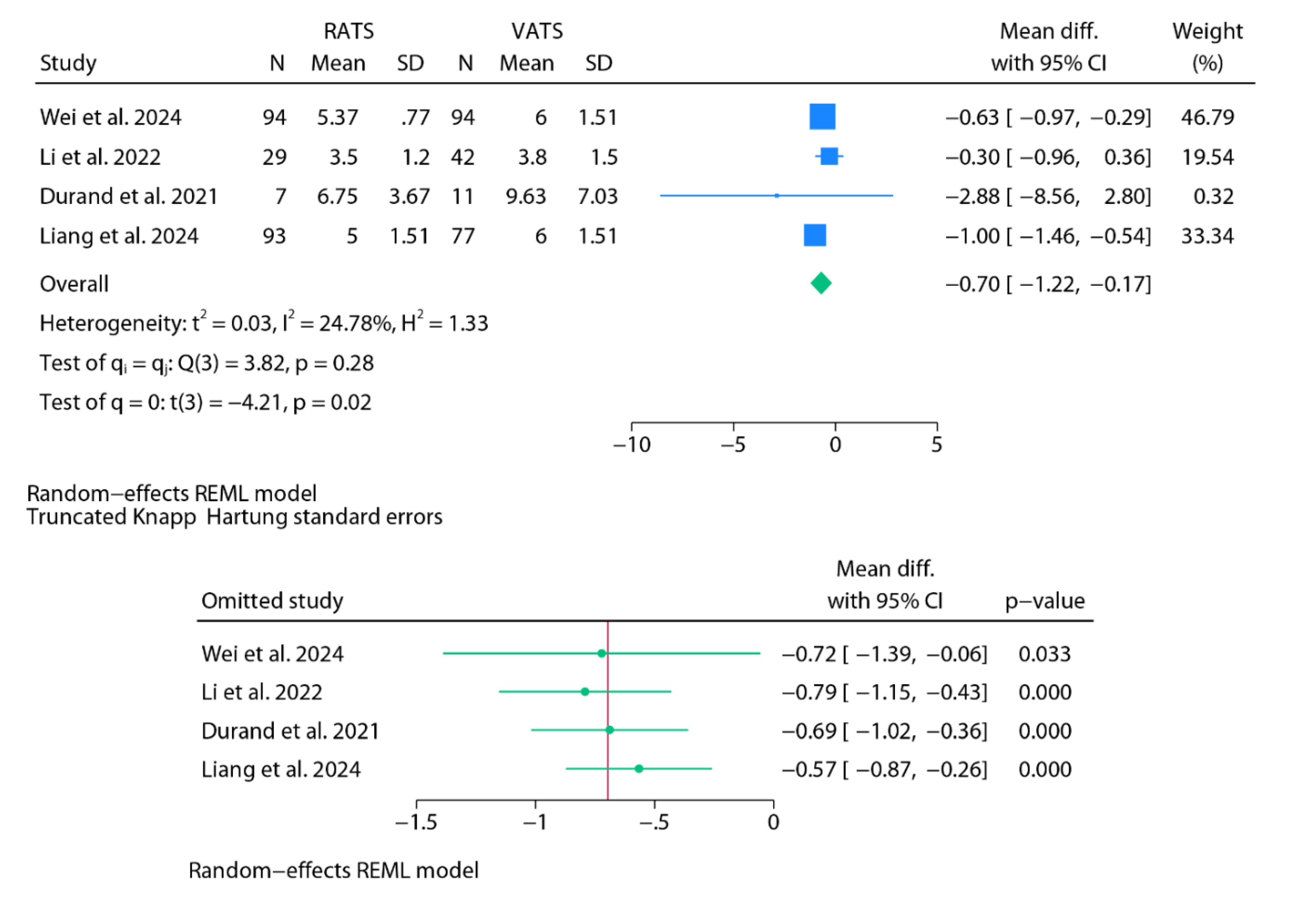
Figure 5.
Meta-analysis of chest tube duration (in days).
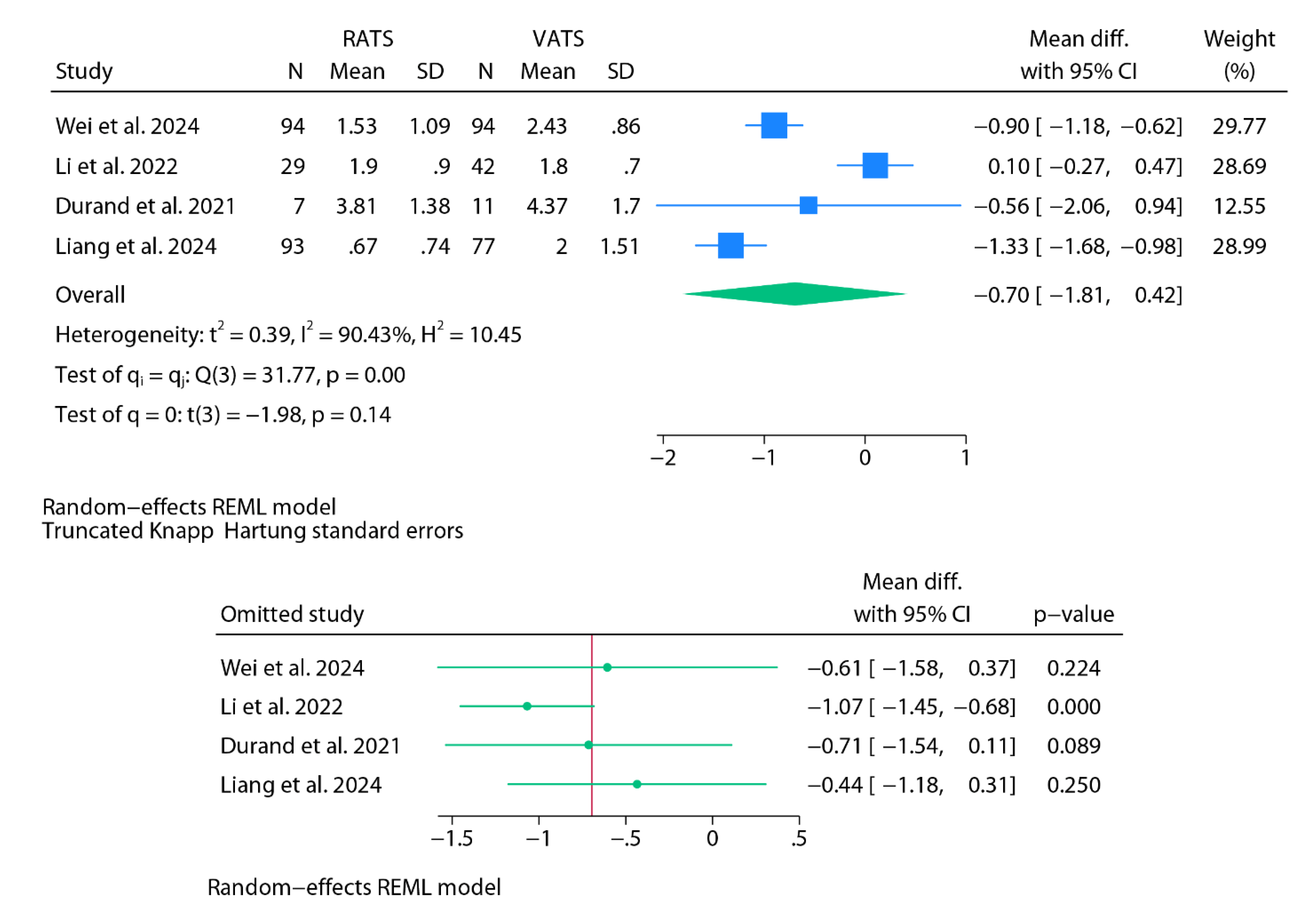
Figure 6.
Meta-analysis of postoperative complications.
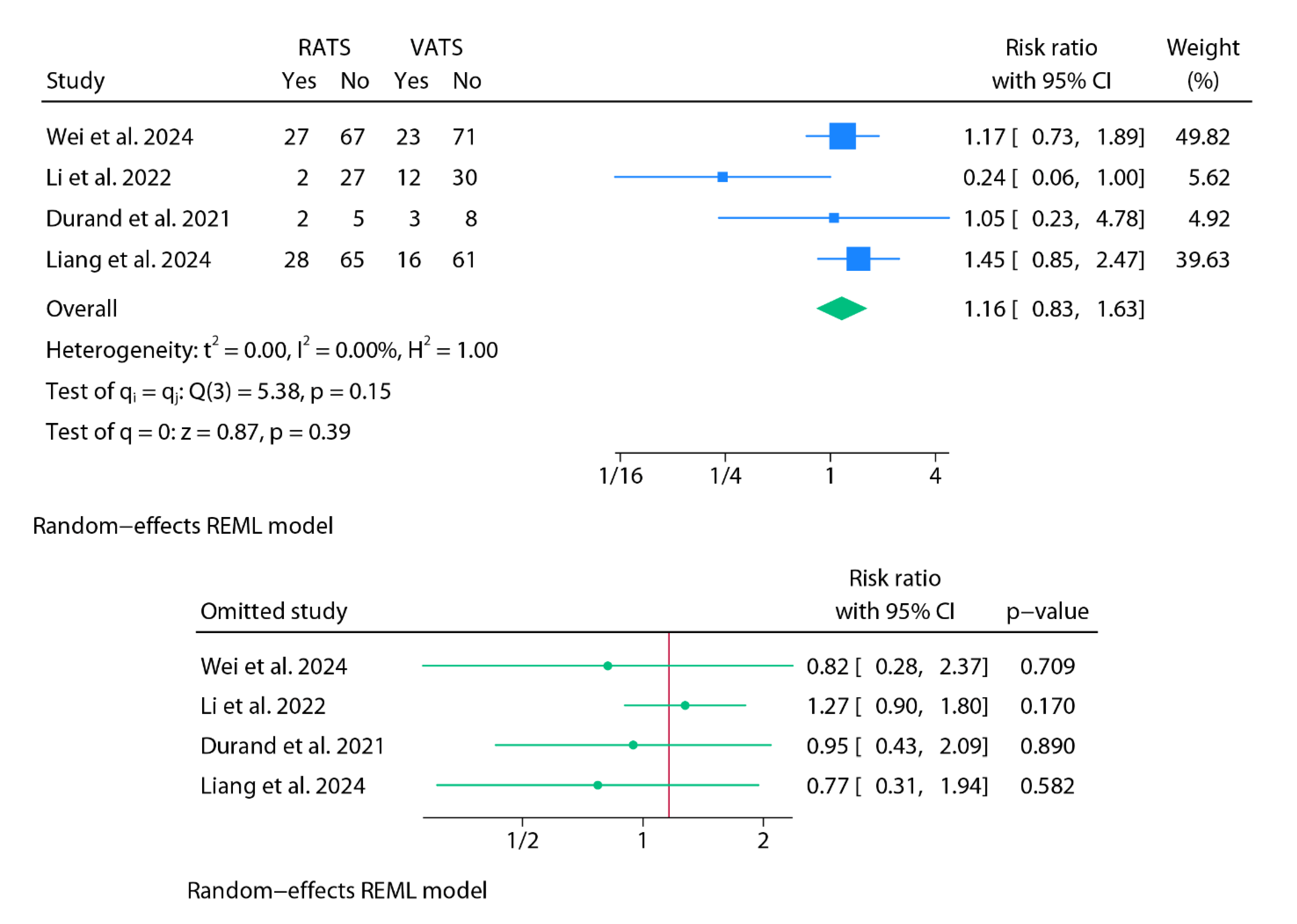
Figure 7.
Baujat plots.
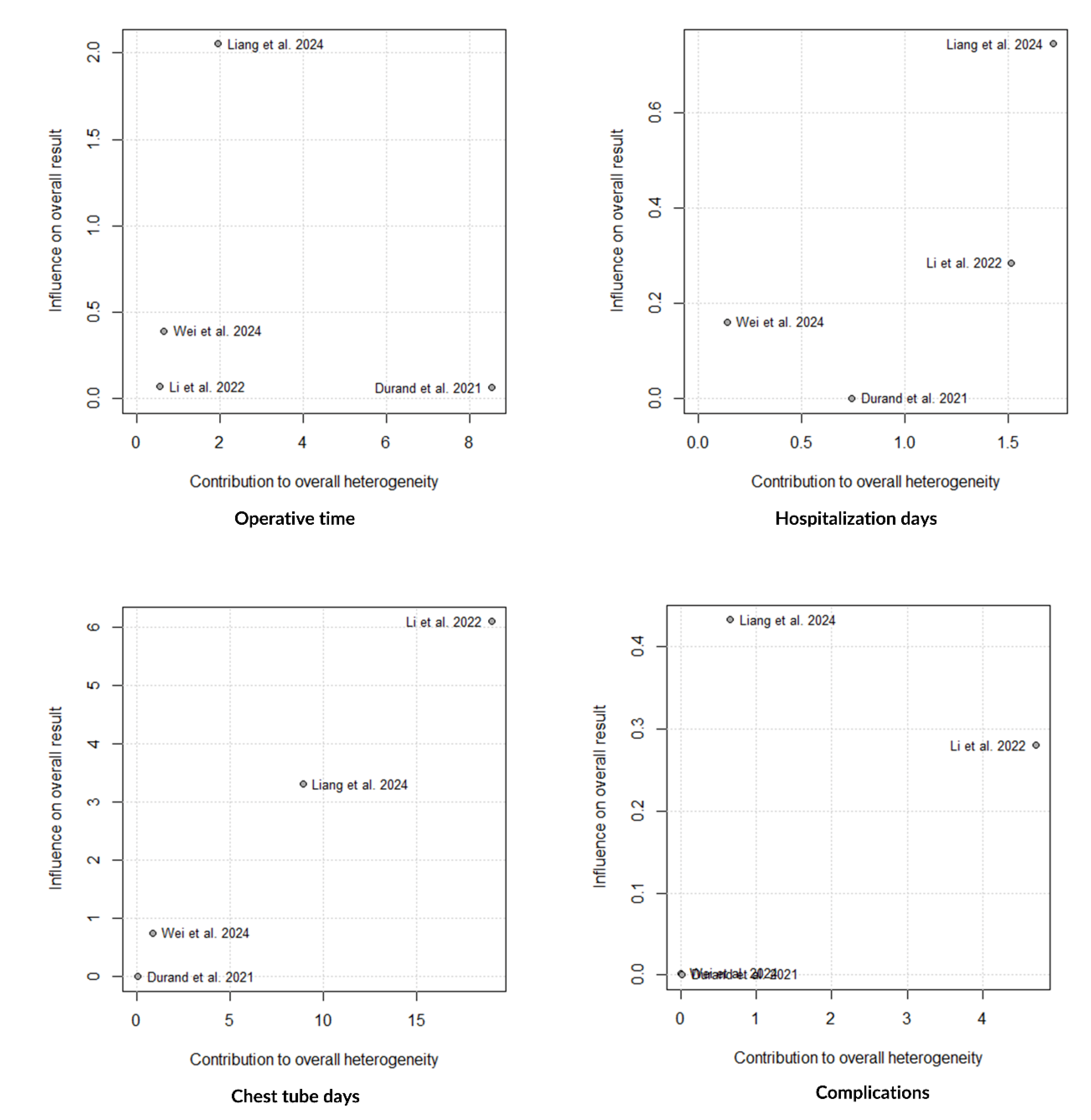

Table 1.
Robotic-assisted procedures in pediatric patients with tracheomalacia, congenital diaphragmatic pathology, and thoracic and pulmonary pathology.
Table 1.
Robotic-assisted procedures in pediatric patients with tracheomalacia, congenital diaphragmatic pathology, and thoracic and pulmonary pathology.
| References (country, year) | Procedure No. cases |
Study design | Age (range) | Robot model Ports |
Operating time (minutes) | Postoperative complications | Conversion to open | Chest tube (days) | Hospital stay (days) | Follow-up |
|---|---|---|---|---|---|---|---|---|---|---|
| Kamran et al. (USA, 2018) [21] | PT 6 RATS 4 VATS |
Retrospective descriptive | 11 yr (5- 19) | NS | 6.5 h (4.5-10.5) | None | None | NO | 3-7 | 6 mo (1-16) |
| Torre et al (Italia, 2020) [22] | PT 2 RATS 4 VATS |
Retrospective descriptive | 58 mo (8-162) | Xi 4 RB 8-mm |
150 (110-320) | None | None | YES NS |
5 (3-118) | NS |
| Meehan et al. (USA, 2008) [23] | Total: 6 2 CPAMs, 2 IS, 1 bronchiectasis, 1 chronic granulomatous disease |
Retrospective descriptive | 7 mo-14 yr | S 5-mm and 12-mm (camera) |
NS | None | 1 (LB) | 4 cases (1-3 days) |
1.8 (1-3) | 24 mo (2 mo-4 yr) |
| Gao et al. (China, 2022) [24] | 9 IEPS 4 RATS 5 VATS |
Retrospective descriptive | 9.5 mo | Xi 3 RP 8-mm |
RATS 80; VATS 48 | None | None | RATS 1.5 days; VATS 2.2 days | RATS 4.3; VATS 6.4 | NS |
| Jones et al. (USA, 2024) [25] | PAVM 1 |
Case report | 16 yr | Xi 4 RB 8-mm |
90 | None | None | YES 1 day |
2 | 4 mo |
| Ballouhey et al. (France, 2015) [6] | Total: 11 4 BC 2 CDH, 5 Esophageal procedures |
Retrospective descriptive | 72 mo (0-204) | Xi NS |
190 (120-310) | 1 dysphagia (BC) | 1 (CDH) | NS | 6.2 (3–20) | 26.9 mo (8-55) |
| Navarrete-Arellano (Mexico, 2020) [5] | Total: 11 3 CPAMs, 1 IS, 3 DE, 1 DP, 1 teratoma, 1 Ewing tumor, 1 pulmonary TBC |
Retrospective descriptive | 5.7 years (6 mo- 15 yr) | Si 3-4 RB 5-mm |
166.45 (25-314) | 1 serous prolonged drainage (DP) | 1 (IS) | NS | 3.6 (1-12) | NS |
| Soto et al. (Spain, 2022) [26] | Total: 3 2 pneumothorax, 1 ES |
Retrospective descriptive | 2.5-17 yr | Xi 3 RB 8-mm |
100 (81-108) | None | None | NO | 2 | NS |
| Çeltik et al. (Turkey, 2024) [27] | Total: 30 10 NT, 3 pulmonary metastasis, 2 BC, 1 Ewing tumor, 1 teratoma, 1 M-CDH, 1 CPAM, 1 hydatid cyst, 1 APVR, 1 bronchiectasis, 8 esophageal pathologies |
Retrospective descriptive | 8.4 yr (SD: 5.2) (1-17 yr) | NS | 165.6 (SD: 124.8) | 4: Horner syndrome, atelectasis, pleural effusion, prolonged air leakage | None | 20 cases 3 days (1-25) |
3.5 (1-30) | NS |
| Luebbe et al. (USA, 2003) [3] | M-CDH and mediastinal mass 2 |
Case series | 10 yr | S 8-mm RB + 12-mm camera |
NS | 1 pneumothorax | None | NO | NS | NS |
| Knight et al. (USA, 2005) [28] | M-CDH 2 |
Case series | 23 mo and 5 yr | Zeus 4 RB 5-mm |
227 | None | None | NO | 1-2 | NS |
| Anderberg et al. (Sweden, 2008) [29] | M-CDH 1 |
Case report | 18 mo | S 8-mm ports + 12-mm camera |
145 | None | None | NO | 3 | 1 yr |
| Slater et al. (USA, 2009) [30] | Total: 8 2 DE, 5 B-CDH, 1 M-CDH |
Retrospective descriptive | 3.9 mo (4 days-12 mo) | S 3 RB 5-mm |
80 | 1 recurrence (B-CDH) | 2 | NO | NS | NS |
| Delgado-Miguel et al. (USA, 2025) [31] | Total: 3 CDH 2 B-CDH 1 M-CDH |
Retrospective descriptive | 8 mo (7-10) |
Si 3-4 RP (12-mm camera + 2-3x5-mm) |
153 (IQR: 123-237) | None | None | NO | 3 (2-4) | 6.5 yr (IQR 3.8-9.4) |
| Xu et al (China, 2020) [32] | Total: 20 DE RATS: 9 VATS: 11 |
Retrospective comparative | RATS: 11.2 mo (SD: 2.1) VATS: 9.4 mo (SD: 2.3) |
Si 3 RP (12-mm camera + 2x8-mm) |
RATS; 103.6 (SD: 14.8) VATS: 102.4 (SD: 14.5) |
RATS: none VATS: 1 recurrence |
None | NO | RATS: 7.8 (SD: 0.6) VATS: 8.1 (SD: 0.9) |
NS |
| Alzahrani et al (France, 2025) [33] | Total: 112 DE RATS: 5 VATS: 64 Thoracotomy: 15 Abdominal: 28 |
Retrospective comparative | RATS: 29 mo (11.5-76.5) VATS: 13 mo (6–23.3) |
NS | NS | 3 RATS: 2 liver injuries, 1 recurrence 11 VATS: 4 pleural injuries. 1 tracheal tube dislodgement, 6 recurrences |
None | NO | RATS: 5 (4.3-6.5) VATS: 4 (3-5) |
RATS: 56 mo (10.5-65.0) VATS: 28.8 mo (11.3-52.8) |
PT, Posterior tracheopexy; CPAM, Congenital Pulmonary Airway Malformation; LB, lobectomy; BC, Bronchogenic cyst; IS, intralobar sequestration; ES, extralobar sequestration; DP, diaphragmatic paralysis; DE, diaphragmatic eventration; NT, Neurogenic tumors; B-CDH, Bockdalek congenital diaphragmatic hernia; M-CDH, Morgagni congenital diaphragmatic hernia; APVR, Abnormal pulmonary venous return; IEPS, Intradiaphragmatic extralobar pulmonary sequestration; TBC, tuberculosis; Pulmonary arteriovenous malformation; mo, months; yr, years; NS, non-specified; RP, robotic port; AP, auxiliary port; SD, standard deviation; IQR, interquartile range. All intervals between brackets refer to ranges.
Table 2.
Robotic-assisted procedures in thymic masses and mediastinal/thoracic tumors.
| References (country, year) | Procedure No. cases |
Study design | Age (range) | Robot model Ports |
Operating time (minutes) | Postoperative complications | Conversion to open | Chest tube (days) | Hospital stay (days) | Follow-up |
|---|---|---|---|---|---|---|---|---|---|---|
| Hartwich et al. (USA, 2012) [34] | Thymectomy 9 |
Retrospective descriptive | 9.4 yr (SD: 4.8) | S 3 RB: 8.5-mm camera + 2x5 mm |
160 (SD: 6) | 1 pneumothorax | None | 1 case | 1 (1-2) | 22 mo |
| Grasso et al. (Italy, 2020) [35] | Thymectomy 1 |
Case report | 12 yr | Xi 3 RB 8-mm |
90 | None | None | YES 2 days |
4 | 2 mo |
| Hanke et al. (USA, 2024) [36] | Giant thymolipoma 1 |
Case report | 10 yr | Xi 3 RB 8-mm + 2 AP (12-mm + 5-mm) |
NS | None | None | NO | 3 | 2 yr |
| Li et al. (Germany, 2022) [37] | Thymectomy 47 RATS 20 medical |
Retrospective descriptive | 13 yr (10-15) | Xi 3 RB 8-mm |
NS | 9 cases: 5 myasthenic symptoms, 2 pneumothorax, 2 chylothorax | None | NO | 4 (3-31) | 46 mo (30-94) |
| Meehan et al. (USA, 2008) [38] | Total: 5 1 GNB, 1 GN, 1 teratoma, 1 inflammatory mass, 1 germ cell tumor |
Retrospective descriptive | 9.8 yr (2-17) | S 3-4 RP 5-mm |
113 (44-156) | None | None | NS | NS | 26 mo (19-30) |
| Blanc et al. (France, 2022) [39] | Total: 14 4 NB, 3 GNB; 3 GN, 3 thymoma, 1 bronchial carcinoid |
Retrospective descriptive | NS | Xi NS |
NS | 2 pneumothorax | 1 (NB) | No | 3 (2–4) | 2.4 yr (1.5-3.4) |
| Zeng et al. (China, 2023) [40] | Total: 149 99 NT, 19 foregut cysts, 12 thymic tumors, 9 angiolymphatic tumours, 6 lipogenic tumors, 4 soft tissue tumours |
Retrospective descriptive | 5.9 yr (6 mo-16 yr) | Xi 4 RB 8-mm |
106.7 (25-260) | None | 4 | YES 2-3 days |
7.2 (4-14) | 3-23 mo |
| Svetanoff et al. (USA, 2024) [41] | Total: 17 8 GNB, 6 GN, 2 NB, 1 PG |
Retrospective descriptive | 6.1 yr (IQR 4.8-8.8) | Si and Xi 4 RB 8-mm |
124 (IQR:108-173) | 1 chyle leak | 2 | NS | 1.5 (IQR 1.1-3) | 13 mo (IQR 5.5-27.8) |
| Toker et al. (Turkey, 2014) [42] | BC 1 |
Case report | 8 yr | Si 3 RP 5-mm |
62 | None | None | YES 1 day |
2 | 6 mo |
| Nemoto et al. (Japan, 2022) [43] | GN 1 |
Case report | 15 yr | Xi 4 RP 8-mm |
NS | None | None | NO | NS | 18 mo |
| Yamaguchi et al. (USA, 2019) [44] | Paraspinal mass 1 |
Case report | 7 yr | Xi NS |
104 | None | None | NO | 1 | NS |
| Ochi et al. (Japan, 2023) [45] | NB 1 |
Case report | 28 mo | Xi 4 RB: 3x8-mm + 12-mm camera |
NS | None | None | YES 2 days |
NS | 7 mo |
| Riccipetitoni et al. (Italy, 2021) [46] | GNB 1 |
Case report | 7.6 yr | Xi 3 RB 2x8-mm + 12-mm camera |
290 | None | None | NO | 7 | 0.78 yr |
| Prasad et al. (India, 2023) [47] | GN 1 |
Case report | 9 yr | Xi 3 RB 8-mm + 1 AP 5-mm |
130 | None | None | YES 1 day |
2 | 1 yr |
| Bahadır et al (Turkey, 2023) [48] | PG 1 |
Case report | 11 yr | Si 3 RB (2x8-mm + 12-mm camera) + 1 AP 10-mm |
180 | None | None | NO | 4 | 44 mo |
| Kaneda et al (Japan, 2025) [49] | GN 1 |
Case report | 8 yr | SP | 250 | None | None | NO | 3 | 1 mo |
RATS, Robotic-Assisted Thoracic Surgery; BC, Bronchogenic cyst; NT, Neurogenic tumors; NB, neuroblastoma; GN, ganglioneuroma, GNB, ganglioneuroblastoma; PG, paraganglioma; PAVM, Pulmonary arteriovenous malformation; mo, months; yr, years; NS, non-specified; RP, robotic port; AP, auxiliary port; IQR, interquartile range. SP, single-port. All intervals between brackets refer to ranges.
Table 3.
Robotic-assisted pulmonary resections in pediatric patients.
| References (country, year) | Procedure No. cases |
Study design | Age (range) | Robot model Ports |
Operating time (minutes) | Postoperative complications | Conversion to open | Chest tube (days) | Hospital stay (days) | Follow-up |
|---|---|---|---|---|---|---|---|---|---|---|
| Durand et al (France, 2021) [20] | RATS: 7 VATS: 11 |
Retrospective comparative | RATS: 13.1 yr (9.65-13.5) VATS: 10.1 yr (6.8-13.2) |
Xi 3 RP 8-mm + AP 5-mm |
RATS: 268 (221.5-286.5) VATS: 131 (115.5-190) |
RATS: 2 VATS: 3 |
RATS: 0 VATS: 5 |
RATS: 4 (3-4.5) VATS: 4 (3.5-5.5) |
RATS: 6 (5-9) VATS: |
NS |
| Li et al (China, 2022) [21] | RATS: 29 VATS: 42 |
Retrospective comparative | RATS: 68.1±47.2 mo VATS: 64.6±45.1 mo |
Si 3·RP (12-mm camera + 2x8-mm) + AP 5-mm |
RATS: 148.3±36.8 VATS: 118.3±22.5 |
RATS: 2 VATS: 12 |
RATS: 1 VATS: 2 |
RATS: 1.9±0.9 VATS: 1.8±0.7 |
RATS: 3.5±1.2 VATS: 3.8±1.5 |
6-54 mo |
| Liang et al (China, 2024) [22] | RATS: 93 VATS: 77 |
Retrospective comparative | RATS: 10 mo (7- 25) VATS: 9.5 mo (7- 17.5) |
Xi 3·RP 8-mm + AP 5-mm |
RATS: 75 (60-92.5) VATS: 60 (40-70) |
RATS: 28 VATS: 16 |
RATS: 1 VATS: 1 |
RATS: 1 (0-1) VATS: 2 (1-3) |
RATS: 5 (4-6) VATS: 6 (5-7) |
NS |
| Wei et al (China, 2024) [23] | RATS: 94 VATS: 94 |
Retrospective comparative | RATS: 12 mo (8-44.7) VATS: 12 mo (7-45) |
Xi 3·RP 8-mm + AP 5-mm |
RATS: 97.5 (79.0-116.5) VATS: 70 (50-90) |
RATS: 27 VATS: 23 |
RATS: 0 VATS: 0 |
RATS: 1 (1-2) VATS: 2 (2-3) |
RATS: 5 (5-6) VATS: 6 (5-7) |
NS |
RATS, Robotic-Assisted Thoracic Surgery; VATS, Video-Assisted Thoracic Surgery; mo, months; yr, years; NS, non-specified; RP, robotic port; AP, auxiliary port; IQR, interquartile range. All intervals between brackets refer to interquartile ranges.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



