
Submitted:
21 August 2025
Posted:
22 August 2025
You are already at the latest version
Abstract
Chronic kidney disease is closely associated with an increased risk of cardiovas-cular disease. Although kidney transplantation represents the treatment of choice for patients with end-stage chronic kidney disease, it is also linked to significant cardio-vascular risk. This study aimed to evaluate the relationship between cardiovascular pathology and oxidative status in kidney transplant recipients, while also assessing the influence of disease etiology and humoral immune response on oxidative imbalance. A cross-sectional analysis was conducted in thirty-six individuals with advanced chronic kidney disease and forty kidney transplant recipients. The enzymatic activities of xan-thine oxidase, superoxide dismutase, and glutathione peroxidase, levels of lipid perox-idation products, oxidized glutathione, and reduced glutathione, were measured by spectrophotometry in plasma and mononuclear and polymorphonuclear leukocytes isolated using Ficoll density gradients. Individual oxidative status was evaluated using an OXYSCORE. Kidney transplantation was associated with a higher incidence of car-diovascular disease and increased levels of both pro-oxidant and antioxidant bi-omarkers. Elevated OXYSCORE values were observed particularly in patients with nephroangiosclerosis, diabetic kidney disease, polycystic kidney disease, and cardio-vascular comorbidities. Additionally, the presence of anti-graft antibodies correlated with higher oxidative scores. These findings suggest that redox status may serve as a potential biomarker for cardiovascular risk in kidney transplant recipients.
Keywords:
cardiovascular disease
; chronic kidney disease
; kidney transplantation
; leukocytes
; oxidative stress
; OXYSCORE
1. Introduction
Cardiovascular diseases (CVD) represent the leading cause of mortality among patients with chronic kidney disease (CKD). These events are typically preceded by subclinical endothelial dysfunction and are closely associated with an altered REDOX status [1]. The principal etiologies of CKD include nephroangiosclerosis (NAS), which is frequently linked to arterial hypertension (AH), and diabetic nephropathy (DN) [2]. Other significant causes encompass autosomal dominant polycystic kidney disease (ADPKD), interstitial nephritis (IN), and glomerulonephritis (GN) [3]. CKD stages 4 and 5, defined by an estimated glomerular filtration rate (eGFR) below 30 mL/min/1.73 m², are categorized as advanced chronic kidney disease (ACKD). When eGFR falls below 15 mL/min/1.73 m², renal replacement therapy, either hemodialysis (HD) or peritoneal dialysis (PD), becomes necessary [2]. Kidney transplantation (TX) remains the preferred therapeutic modality, as it markedly improves both survival and quality of life. Nonetheless, transplantation remains associated with complications such as CVD, graft rejection, the emergence of donor-specific anti-HLA antibodies, and adverse effects related to immunosuppressive therapy [4].
CKD is characterized by a disrupted REDOX homeostasis, marked by increased production of reactive oxygen species (ROS). Vida et al. 2021 demonstrated increased activity of pro-oxidant enzymes, as well as reduced antioxidant enzymes activity, elevated levels of lipid peroxidation products, and disruptions in the glutathione cycle in ACKD, HD, and PD. These alterations were observed in plasma, mononuclear leukocytes (MN), and polymorphonuclear leukocytes (PMN) [5]. (Valera-Arévalo et al. 2025) further confirmed an altered individual REDOX status in ACKD and HD patients compared to healthy subjects (HS), using the OXY-SCORE proposed by previous authors [6]. This REDOX imbalance has been corroborated by other studies and is attributed to the accumulation of uremic toxins, chronic systemic inflammation, and underlying pathophysiological conditions of CKD, such as AH and DN [7,8]. Some studies have reported increased pro-oxidant enzymes activity, such as xanthine oxidase (XO), in platelet-poor plasma following TX compared to pre-transplantation levels [9]. Despite this increase, higher concentrations of plasma lipid peroxidation products have been observed in non-transplanted patients compared to post-TX [10]. Additionally, elevated levels of lipid peroxidation markers, such as malondialdehyde (MDA), have been associated with a higher incidence of CVD following TX [10]. In terms of antioxidant defense, previous studies have demonstrated greater antioxidant capacity in TX [11], as evidenced by increased glutathione peroxidase (GPx) activity compared to individuals undergoing HD. However, conflicting findings have been reported, with some authors reporting greater superoxide dismutase (SOD) activity in HD compared to TX [12].
We hypothesized that the high incidence of CVD following TX may be related to the patients´ oxidative status, which is influenced by the underlying etiology of CKD and the production of anti-graft antibodies.
2. Materials and Methods
2.1. Study Design and Participants
This cross-sectional study included 36 individuals with ACKD and 40 TX. 18 HS were incorporated to establish reference values. TX participants had been transplanted at least six months prior to sample collection. Individuals with malignancies, active infections, autoimmune or inflammatory diseases, or CKD of unrelated etiology were excluded. Participants were recruited from the Nephrology Department at Hospital Universitario 12 de Octubre in Madrid, Spain. The study was conducted according to the ethical guidelines outlined by The Transplantation Society. The study was conducted following the principles of the Declaration of Helsinki and the Declaration of Istanbul on Organ Trafficking and Transplant Tourism. The research protocol was approved by the Ethics Committee of the Hospital 12 de Octubre Research Institute (Approval No. 17/407). Written informed consent was obtained from all participants prior to enrollment. Clinical characteristics of the study population are summarized in Table 1.
2.2. Blood Collection and Preparation
Peripheral blood samples were collected via venipuncture in EDTA tubes at the Nephrology Department of the Hospital Universitario 12 de Octubre, Madrid (Spain) during routine clinical analyses. Samples were transported to the Animal Physiology Unit of the Faculty of Biological Sciences, Complutense University of Madrid, Spain, within 24 hours for processing. Platelet-free plasma for oxidative stress assays was isolated by centrifugation at 1250xg for 20 min and stored at -80 ºC until analysis.
2.3. Leukocytes Density Gradient Separation
PMN and MN were isolated using Ficoll density gradient centrifugation. The samples were transferred to a 50 ml tube, mixed with an equal volume of phosphatebuffered saline (PBS), and underlaid with HistopaqueR 1.119 g/ml and 1.077 g/ml (Sigma-Aldrich, Madrid, Spain) before centrifugation at 800×g for 30 min with brake off. Leukocyte layers were washed three times with PBS at 1250×g for 20 min (Eppendorf Benchtop Refrigerated centrifuge 5403 with rotor 16F24-11, Eppendorf, Hamburg, Germany), adjusted to 1x106 cells/ml, and stored at -80 ºC until analysis.
2.4. Oxidative Stress Parameters
Oxidative stress parameters were measured in plasma, PMN, and MN.
2.4.1. Xanthine Oxidoreductase Activity
XO activity was quantified in plasma (40 μl), PMN, and MN (1x106 cells/ml) using the commercial AmplexR Red Xanthine/Xanthine Oxidase Assay Kit A-22182 (Molecular Probes, Paisley, UK). The aliquots of PMN and MN (1x106 cells/ml) were lysed and centrifuged at 10.000×g, at 4 ◦C for 20 min to obtain soluble fractions (Eppendorf Benchtop Refrigerated centrifuge 5403 with rotor 16F24-11, Eppendorf, Hamburg, Germany). XO catalyzes the oxidation of hypoxanthine to uric acid and superoxide. Superoxide spontaneously degrades to hydrogen peroxide (H2O2), which reacts with the AmplexR Red reagent to render resofurin, whose absorption was measured at 560 nm. XO activity was expressed as mU XO/mg protein or mU/ml.
2.4.2. Glutathione Peroxidase Activity
GPx activity was measured in plasma (10 μl), PMN, and MN (1x106 cells/ml) by colorimetry using the commercial EnzyChrom™ Glutathione Peroxidase Assay Kit EGPX-100 (BioAssay Systems, Hayward, CA, USA). The aliquots of PMN and MN (1x106 cells/ml) were resuspended in lysis buffer, sonicated, and centrifuged at 11.000×g, at 4 ◦C for 10 min to obtain the intracellular fraction (Eppendorf Benchtop Refrigerated centrifuge 5403 with rotor 16F24-11, Eppendorf, Hamburg, Germany). Absorbance was measured at 340 nm (t0; T4). Activity was expressed as units (U) of GPx/mg protein or U/L.
2.4.3. Lipid Peroxidation Assay
Lipid peroxidation was determined using the thiobarbituric acid reactive substance (TBA) assay, which measures MDA as a product of lipid peroxidation. Determination is performed in 300 μL of plasma and in aliquots of PMN and MN (1x106 cells/ml) using the commercial MDA Assay Kit (BioVision Inc., Milpitas, CA, USA). Lipid peroxidation was calculated using linear regression derived from an MDA standard curve and expressed as nmol MDA/mg protein or thiobarbituric acid reactive substance (TBARS)/ml.
2.4.4. Glutathione Content Assay
Glutathione analysis was carried out on plasma (10 μl), PMN, and MN (1x106 cells/ml). The aliquots of PMN and MN were sonicated for 10s (three times) and centrifuged at 11.000×g for 10 min at 4 ◦C to obtain the intracellular fraction (Eppendorf Benchtop Refrigerated centrifuge 5403 with rotor 16F24-11, Eppendorf, Hamburg, Germany). The supernatants were used to quantify oxidized glutathione (GSSG) and reduced glutathione (GSH) from the reaction with o-phthalaldehyde (OPT) (G4251-5G, G4376-500 MG, 79760-5G, respectively, Sigma Aldrich, Spain) at a pH between 8-12, resulting in a measurable product at 420 nm. GSH and GSSG concentrations were expressed in nmol/mg protein or nmol/ml.
2.4.5. Superoxide Dismutase Activity
SOD activity was determined by colorimetry using a commercial EnzyChromTM ESOD-100 kit (BioAssay Systems, Hayward, CA, USA). The assay was carried out in plasma (20 μl), PMN, and MN. The aliquots of PMN and MN (1x106 cells/ml) were sonicated with a lysis buffer, and centrifugation at 1500xg for 10 min at 4◦C was performed to obtain the intracellular fraction (Eppendorf Benchtop Refrigerated centrifuge 5403 with rotor 16F24-11, Eppendorf, Hamburg, Germany). The absorbance of formazan was measured at 438–460 nm. The results were expressed as U of SOD/mg protein or U of SOD/ml.
2.4.6. Protein Content Assay
The protein content of PMN and MN was determined using the bicinchoninic acid (BCA) protein assay kit protocol (Sigma-Aldrich, Madrid, Spain), according to the manufacturer´s instructions.
2.4.7. OXY-SCORE Index Determination
The study of patients´ oxidative status was completed by calculating the OXY-SCORE proposed by Veglia et al., 2010, based on pro-oxidant and antioxidant parameters measured in our study. A logarithmic transformation of the parameters that did not follow a normal distribution was performed, favoring a more symmetrical distribution. The variables were standardized by applying the formula: Zij = (xij − mj)/sj, where Zij (standardized value of variable j for subject); xij (raw measure (possibly log transformed) of variable j for subject i); mj (mean of variable j); sj (standard deviation of variable j) are related. Subsequently, individual scores were added to obtain the overall score.
2.5. Metabolic Syndrome Diagnosis
Metabolic syndrome was defined as the presence of three or more of the following criteria: body mass index (BMI)>30 kg/m2, triglycerides (TG)>150 mg/dL, low-density lipoprotein (LDL) <40 mg/dl for males and <50 mg/dl for females, AH diagnosis or fasting glucose >100 mg/dl.
2.6. Statistics
Data are presented as mean ± standard deviation (SD). Normality was assessed using the Kolmogorov–Smirnov test. Parametric variables were analyzed by one-way ANOVA followed by Tukey’s post hoc test; non-parametric data were analyzed using the Kruskal–Wallis test. Categorical variables were evaluated with the chi-square test. Statistical analyses were performed using SPSS 21.0 and GraphPad Prism 8.02 software. Significance was set at P<0.05.
3. Results
3.1. Study Population Baseline Characteristics
Clinical characteristics of study subjects are shown in Table 1. ACKD and TX had similar incidences of CVD (63.9% and 50%), ischemic heart disease (44.4% and 40%), and AH (88.9% and 97.5%). Vasculopathy was more frequent in TX (45%) than in ACKD (11.1%). In TX, 52.5% produced anti-graft antibodies. Immunosuppressive treatment included corticosteroids (90%), tacrolimus (95%), mycophenolate (80%), and everolimus (12.5%). 42.5% had less than 5 years post-transplant, and 57.5% more than 5 years post-transplant. CKD etiology in TX included NAS (15%), DN (20%), ADPKD (20%), IN (17.5%), GN (10%), or unrelated causes. The mortality rate was lower in TX than in ACKD (36.1% and 7.5%, respectively). No differences were observed in age and gender. No statistically significant differences were observed between groups regarding the incidence of acute cardiovascular events (ACVA) and chronic cardiac insufficiency (CCI).
3.2. Cardiovascular Disease Incidence Was Influenced by Etiology
In our cohort, patients with ACKD and TX due to NAS, DN, ADPKD, and GN showed an increased incidence of CVD compared to HS. TX patients with DN showed a higher CVD incidence compared to ACKD (Figure 1a). Ischemic cardiopathy was more frequent in ACKD and TX with NAS, DN, and ADPKD compared to HS, and higher in TX with DN and ADPKD versus ACKD (Figure 1b). ACVA was more frequent in TX with ADPKD compared to HS, while no cases were reported in TX with GN (Figure 1c). Vasculopathy was more common in TX with NAS, DN and ADPKD versus HS, and higher in TX with DN compared to ACKD. TX with GN showed a lower vasculopathy incidence compared to TX with DN, yet higher compared to TX with IN (Figure 1d). No significant differences were observed regarding the incidence of CCI (Figure 1e). None of the TX with IN suffered from CVD.
3.3. Alterations in Oxidative Stress Markers Were Detected in Plasma and Immune Cell Populations
Plasma XO activity was increased in TX compared to HS and ACKD (Figure 2a). Plasma TBARS levels in ACKD and TX were elevated compared to HS (Figure 2b). Plasma SOD activity increased in ACKD compared to HS and also in TX compared to HS and ACKD (Figure 2c). Plasma GPx activity in TX was increased relative to ACKD (Figure 2d). Plasma GSH levels were similar in ACKD and TX to HS (Figure 2e).
XO activity in MN increased in TX compared to HS (Figure 3a). MDA levels in MN were elevated in TX compared to HS and ACKD (Figure 3a). SOD activity in MN in TX was higher compared to ACKD patients, in which levels were lower compared to HS (Figure 3c). GPx activity in MN increased in TX compared to HS and ACKD (Figure 3d). GSSG levels in MN were increased compared to HS and ACKD (Figure 3e). GSH levels in TX were increased compared to ACKD, whose levels were lower concerning HS (Figure 3f). The GSSG/GSH ratio in MN in TX was similar to HS and ACKD (Figure 3g).
XO activity in PMN in TX patients was lower compared to ACKD, whose activity showed a trend of higher activity compared to HS (Figure 4a). MDA levels in PMN in TX were similar to HS and ACKD (Figure 4b). SOD activity in PMN was higher in TX compared to HS and ACKD (Figure 4c). GPx activity in PMN was higher in TX compared to HS (Figure 4d). GSSG levels in PMN were higher in ACKD compared to HS and were higher in TX compared to HS and ACKD (Figure 4e). GSH levels in PMN were similar in TX to HS and ACKD (Figure 4f). GSSG/GSH ratio in PMN was higher in TX compared to HS, as was the case in ACKD (Figure 4g).
No differences in REDOX parameters levels were observed relative to the etiology (Table A1, Table A2 and Table A3).
No differences in REDOX parameters levels were observed relative to the different immunosuppressive drugs combinations (Table A4, Table A5 and Table A6).
OXYSCORE in ACKD and TX was higher compared to HS (Figure 5a). TX with ADPKD had a higher OXYSCORE compared to HS, showing DN and NAS a trend of a higher OXYSCORE compared to HS. TX with IN had a lower OXYSCORE compared to TX patients with ADPKD (Figure 5b). A higher OXYSCORE was observed in TX with associated CVD compared to HS, and these differences were not observed in patients without CVD (Figure 5c). OXYSCORE in TX patients who had produced anti-graft antibodies was higher compared to those who had not, whose OXYSCORE was similar to HS (Figure 6a). No differences were observed depending on the length of time since transplantation (Figure 6b).
4. Discussion
This study hypothesized that oxidative stress—modulated by disease etiology and humoral immune response—is associated with CVD in CKD patients post-TX. Our study showed an altered REDOX status in TX subjects with DN, NAS, and ADPKD. Moreover, this altered oxidative status was associated with CVD and anti-graft antibodies. Although CKD is linked to a higher incidence of CVD, early diagnosis remains challenging due to the lack of reliable biomarkers.
In our study, TX subjects with NAS, DN, and ADPKD, as well as patients with ACKD showed a higher CVD incidence. These outcomes may be influenced by immunosuppressive therapy, comorbidities such as DM, dyslipidemia, AH, and graft dysfunction [13]. ADPKD is commonly associated with AH, often driven by activation of the renin-angiotensin-aldosterone system (RAAS) [14]. In our cohort, patients with GN also showed increased CVD incidence, consistent with prior studies that highlighted the role of systemic inflammation and dysregulation of RAAS in the CVD pathogenesis in this population [15].
Oxidative stress has been proposed as a trigger for endothelial dysfunction and subsequent CVD [4]. In this study, a higher XO activity was observed in TX in plasma and MN compared to HS and ACKD. XO, a purine-metabolizing enzyme, generates superoxide (O₂⁻) and hydrogen peroxide (H₂O₂), promoting endothelial damage, vascular inflammation, and atherosclerosis development [16,17]. Additionally, elevated plasma uric acid—XO's end-product—can be internalized by endothelial cells, inducing ROS production and apoptosis [18]. In TX, increased plasma XO activity has been linked to carotid atherosclerosis [19]. The lack of elevated XO activity in PMN in TX in our study may reflect reduced systemic inflammation following resolution of uremia or the absence of dialysis-related activation of immune system caused by bioincompatible materials [20]. Immunosuppressants such as everolimus or tacrolimus modulate lymphocyte activity, which potentially contributes to the increased XO activity observed in MN [3,21].
Elevated levels of lipid peroxidation products (TBARS and MDA) were observed in plasma and MN. Lipids are essential for maintaining membrane integrity, regulating protein trafficking and activity, and facilitating endocytosis. ROS-induced oxidation disrupts these processes [22]. Under physiological conditions, antioxidant enzymes counteract lipid oxidation, which may be altered under pathological conditions [23]. Previous studies have reported elevated MDA levels two weeks post-TX compared to pre-TX levels, reflecting oxidative stress resulting from surgical trauma and intense immunosuppressive therapy [24]. Lipid peroxidation products cause damage at the cellular, protein, and DNA level, and are implicated in the development of disorders such as atherosclerosis [25].
An increased SOD activity was observed in plasma, MN, and PMN. SOD catalyzes the dismutation of O₂⁻ into H2O2, which is subsequently reduced to H2O by catalase and GPx [26]. Despite the limited literature on this topic, this study is the first to explore the role of MN and PMN. Even though previous studies have not reported differences in plasmatic SOD activity in TX [27], our findings indicate elevated SOD activity as a compensatory response to increased XO activity and O₂⁻ production [16].
Increased GPx activity was also observed in plasma, MN, and PMN. GPx reduces H2O2 using GSH, generating GSSG [28]. Prior studies reported elevated GPx activity within 30 days post-TX, as a response to increased ROS and pro-oxidant activity [29]. High GPx activity has been linked to atherogenic markers detected by ultrasound [30]. This activity is accompanied by enhanced GSH synthesis due to its consumption. The GSSG/GSH ratio, which is an oxidative stress marker, was similar between TX and HS in MN but higher in PMN, suggesting distinct oxidative responses [31].
Despite the anticipated improvement in REDOX status following TX, a higher OXYSCORE was observed compared to HS, accompanied by considerable variability. ADPKD was associated with elevated OXYSCORE, with a similar trend in NAS and DN. OXYSCORE levels IN and GN were comparable to HS. These findings suggest that persistent systemic alterations may underlie the elevated OXYSCORE in NAS, DN, and ADPKD, which appear absent or less prominent in IN and GN.
NAS is characterized by arterial thickening, mainly due to AH, causing glomerular damage and reduced filtration [32]. DN involves oxidative stress and accumulation of advanced glycation products. Despite TX, systemic effects of AH and diabetes mellitus persist. NADPH oxidases contribute to ROS production under these conditions [33], and DN is linked to elevated lipid peroxidation and vascular complications [34]. Antioxidant enzymes activity remains controversial, with some previous studies reporting a higher plasmatic SOD activity [35], while others lower [36]. GSH levels have been reported to be reduced in DN compared to diabetics without nephropathy [37].
ADPKD, often linked to liver cysts, an organ with a crucial role in REDOX balance, may disrupt REDOX regulation [38]. Decreased SOD and GPx activity have been reported to contribute to the pathogenesis and severity of ADPKD [39].
The similarity in OXYSCORE levels between GN, IN, and HS supports the hypothesis of a primarily renal-level pathology, resolved following TX. GN is characterized by B/T lymphocyte and neutrophil infiltration [40], and IN involves tubular inflammation, which may be a consequence of drugs, infections, autoimmune disorders, or ischemia [41].
OXYSCORE was elevated in TX with CVD compared to HS, but not in those without CVD. Oxidative stress contributes to CVD development via endothelial dysfunction, cellular senescence, and pro-inflammatory signaling [42]. Elevated ROS reduces nitric oxide and prostaglandins bioavailability [43]. Low plasmatic SOD levels correlate with heart failure [44], while XO activity promotes uric acid-induced inflammation and endothelial damage [45]. Altered GSH and GSSG levels have been linked to AH [46], and impaired cardiac function [47].
OXYSCORE was unaffected by time since TX, highlighting CKD etiology and CVD as more relevant factors. Higher OXYSCORE in patients with anti-graft antibodies suggests a potential link with immune activation, requiring further investigation.
The limited sample size restricted detailed analysis of rejection types and history, thereby reducing the statistical power to detect meaningful associations. The potential bidirectional relationship between oxidative stress and endothelial damage could not be fully examined and requires further investigation. In vitro studies should be conducted to elucidate underlying mechanisms. Future research involving larger cohorts, longitudinal follow-up, and experimental models is essential to clarify these interactions and their relevance to graft outcomes.
5. Conclusions
TX is accompanied by a significantly altered oxidative status that reflects the complex interplay between underlying CKD etiology, CVD burden, and humoral immune responses. Our findings demonstrate that the OXYSCORE—a composite index of pro-oxidant and antioxidant markers—increased in patients with CVD, and also in those with diabetic nephropathy, nephroangiosclerosis, and autosomal dominant polycystic kidney disease. Importantly, the association between elevated OXYSCORE values and anti-graft antibody production highlights a potential mechanistic link between oxidative stress and immune-mediated graft injury, which may further exacerbate cardiovascular complications. These results position redox profiling not only as a valuable tool for early cardiovascular risk stratification in TX but also as a promising avenue for personalized therapeutic interventions aimed at modulating oxidative stress pathways. Integrating oxidative stress indicators like OXYSCORE into clinical practice could enhance predictive accuracy, enable earlier diagnosis of CVD, and inform tailored treatment strategies to improve long-term transplant outcomes.
Author Contributions
G.V.-A., E.M. and J.C. contributed in the conception and the design of the study; G.V.-A., M.d.M.R.-S.P., M.G.O.-D., C.Y., P.J.C., N.G.-P., R.R. and M.A. performed the research experiment and the acquisition of data. G.V.-A. and N.G.-P. performed the statistical analysis; C.Y. and P.J.C. provided the samples for the experimental study; C.Y., P.J.C. and E.M. made the clinical diagnosis of kidney transplantation patients and control’s selection; E.M. and J.C. acquired funding support; G.V.-A. wrote the manuscript; M.d.M.R.-S.P., M.G.O.-D ., P.J.C., C.Y., R.R., M.A., E.M., N.G.-P. and J.C. revised and completed the final draft of the article. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Instituto de Salud Carlos III through the project “PI17/01029”, “PI19/00240”, “PI20/01321” and “PI23/01109” co-funded by European Regional Development Fund “A way to make Europe”. This research was also funded by grants from the Instituto de Salud Carlos III (ISCIII) and cofounded by Fondos Europeos de Desarrollo Regional (FEDER): “EPU-INV-UAH/2022/001” from Universidad de Alcala (“Ayuda de la Linea de Actuacion Excelencia para el Profesorado Universitario de la UAH” to M.A. RICORS 2040. G.V.-A. was supported by imas12 contract “I+12-AY2OO414-1”, and M.d.M.R.-S.P. received FPU23/00347.
Institutional Review Board Statement
The study was conducted according to the ethical guidelines outlined by The Transplantation Society. The study was conducted following the principles of the Declaration of Helsinki and the Declaration of Istanbul on Organ Trafficking and Transplant Tourism. The research protocol was approved by the Ethics Committee of the Hospital 12 de Octubre Research Institute (Approval No. 17/407). Written informed consent was obtained from all participants prior to enrollment. Clinical characteristics of the study population are summarized in Table 1.
Informed Consent Statement
Written informed consent was obtained from all participants prior to enrollment.
Data Availability Statement
No data are available due to privacy or ethical restrictions.
Acknowledgments
We thank the nephrology service of the Hospital 12 de Octubre for their participation in the recruitment of study subjects and the provision of samples. We thank all patients and healthy subjects for their participation.
Conflicts of Interest
E.M received consulting fees from CSL Vifor, Otsuka, GSK, Samsung, AZ Alexion; payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing or educational events from CSL Vifor, Otsuka, GSK, Samsung, AZ Alexion; support for attending meetings and/or travel from CSL Vifor, Otsuka and participated on a Data Safety Monitoring Board or Advisory Board for CSL Vifor, Otsuka, AZ Alexion, Samsung.
Abbreviations
| ACKD | advanced chronic kidney disease |
| ACVA | acute cardiovascular accident |
| ADPKD | autosomal dominant polycystic kidney disease |
| AH | arterial hypertension |
| BCA | bicinchoninic acid |
| BI | body mass index |
| CCI | chronic cardiac insufficiency |
| CKD | chronic kidney disease |
| CVD | cardiovascular disease |
| DN | diabetic nephropathy |
| eGFR | estimated glomerular filtration rate |
| GPx | glutathione peroxidase |
| GSH | reduced glutathione |
| GSSG | glutathione disulfide |
| GN | glomerulonephritis |
| HD | haemodialysis |
| HS | healthy subjects |
| IN | interstitial nephritis |
| LDL | low density lipoprotein |
| MDA | malondialdehyde |
| MN | mononuclear leukocytes |
| NAS | nephroangioesclerosis |
| OPT | o-phtalaldehyde |
| PBS | phosphate buffered solution |
| PD | peritoneal dialysis |
| PMN | polymorphonuclear leukocytes |
| RAAS | renin-angiotensin-aldosterone system |
| ROS | reactive oxygen species |
| SD | standard deviation |
| SOD | superoxide dismutase |
| TBARS | thiobarbituric acid reactive substance |
| TG | triglicerides |
| TX | kidney transplantation |
| XO | xanthine oxidase |
Appendix A

Table A1.
Effect of the aetiology of chronic kidney disease on plasma prooxidant and antioxidant parameters in transplant recipients.
Table A1.
Effect of the aetiology of chronic kidney disease on plasma prooxidant and antioxidant parameters in transplant recipients.
| HS | TX (NAS) | TX (DN) | TX (ADPKD) | TX (IN) | TX (GN) | |
|---|---|---|---|---|---|---|
| XO Activity (mU/mL) | 0.04±0.012 | 0.29±0.39 | 0.17±0.15 | 0.6±0.1 | 0.44±0.44 | 1.8±0.06 |
| SOD Activity (U/mL) | 0.65±1.47 | 1.55±1.38 | 4.1±3.5 | 3.8±3.2 | 10.1±17.8 | 1.7±0.7 |
| GPx Activity (U/mL) | 60.2±15.6 | 701.8±1053.27 | 290.1±293.6 | 1075±1969 | 835±1073 | 342.9±141 |
| TBARS (nmol/mL) | 5.9±2.4 | 37±39 | 20.9±10.4 | 39.9±49.2 | 33.7±48.05 | 13.9±3.3 |
| GSH (umol/mL) | 1.7±0.53 | 1.6±0.8 | 1.4±0.5 | 1.7±0.5 | 2.1±1.33 | 1.8±0.9 |
HS, healthy subjects; TX, kidney transplantation; NAS, nephroangiesclerosis; DN, diabetic nephropathy; ADPKD, autosomal-dominant policystic kidney disease; IN, interstitial nephropaty; GN, glomerulonephritis; XO, xanthine oxidase; SOD, superoxide dismutase; GPx, glutathione peroxidase; TBARS, thiobarbituric acid reactive substance; GSH, reduced glutathione.
Table A2.
Effect of the aetiology of chronic kidney disease on mononuclear leukocytes prooxidant and antioxidant parameters in transplant recipients.
Table A2.
Effect of the aetiology of chronic kidney disease on mononuclear leukocytes prooxidant and antioxidant parameters in transplant recipients.
| HS | TX (NAS) | TX (DN) | TX (ADPKD) | TX (IN) | TX (GN) | |
|---|---|---|---|---|---|---|
| XO Activity (mU/mL) | 2.7±1.1 | 4. 8±1.3 | 2±0.5 | 5.1±3.4 | 6.4±2.8 | 0.80±0.014 |
| SOD Activity (U/mL) | 0.4±0.3 | 1.1±0.9 | 2.1±2 | 9.2±8.3 | 18±4 | 0.46 |
| GPx Activity (U/mL) | 0.8±1.1 | 1.7±1.6 | 8.7±1 | 5.4±7.7 | 1.5±1.3 | 0.12±0.08 |
| MDA (nmol/mL) | 3.5±2.9 | 6.73±1 | 42.3±33.8 | 15.7±15.4 | 6.4±3.6 | 8.037±2.016 |
| GSH (umol/mL) | 5.9±5.2 | 27±18.3 | 13.7±11.7 | 46.8±87.1 | 336±112 | 3.215±2.51 |
| GSSG (umol/mL) | 3.1±2.1 | 37.1±40.3 | 17±16.9 | 53.8±80.6 | - | - |
| GSSG/GSH | 0.9±0.9 | 2.9±4.3 | 2.8±2.5 | 2.1±2.1 | - | - |
HS, healthy subjects; TX, kidney transplantation; NAS, nephroangiosclerosis; DN, diabetic nephropathy; ADPKD, autosomal dominant polycystic kidney disease; IN, interstitial nephropathy; GN, glomerulonephritis; XO, xanthine oxidase; SOD, superoxide dismutase; GPx, glutathione peroxidase; MDA, malondialdehyde; GSH, reduced glutathione; GSSG, oxidized glutathione.
Table A3.
Effect of the aetiology of chronic kidney disease on polymorphonuclear leukocytes prooxidant and antioxidant parameters in transplant recipients.
Table A3.
Effect of the aetiology of chronic kidney disease on polymorphonuclear leukocytes prooxidant and antioxidant parameters in transplant recipients.
| HS | TX (NAS) | TX (DN) | TX (ADPKD) | TX (IN) | TX (GN) | |
| XO Activity (mU/mL) | 2.4±1.8 | 1.8±0.5 | 1.6±0.66 | 5.7±4.8 | 1.9±0.9 | - |
| SOD Activity (U/mL) | 0.5±0.8 | 2.2±2.1 | 3.1±1.7 | 9.5±12.7 | 8.2±1.2 | 2.1±1.18 |
| GPx Activity (U/mL) | 0.3±0.1 | 1±1.1 | 1.4±1.4 | 0.47±0.06 | 1.8±0.82 | 0.57±0.28 |
| MDA (nmol/mL) | 3.3±2.1 | 3.5±1 | 3.9±1 | 7.9±0.06 | 6.3±1.2 | - |
| GSH (umol/mL) | 1.3±2.4 | 3.7±1.8 | 9.6±16.1 | 15.6±15.4 | 3.3±1.1 | - |
| GSSG (umol/mL) | 0.2±0.07 | 7.6±5.7 | 7.2±3.9 | 17.8±9.9 | - | - |
| GSSG/GSH | 0.4±0.3 | 3.3±1.8 | 14.8±25.9 | 1.7±0.7 | - | - |
HS, healthy subjects; TX, kidney transplantation; NAS, nephroangiosclerosis; DN, diabetic nephropathy; ADPKD, autosomal dominant policystic kidney disease; IN, interstitial nephropaty; GN, glomerulonephritis; XO, xanthine oxidase; SOD, superoxide dismutase; GPx, glutathione peroxidase; MDA, malondialdehyde; GSH, reduced glutathione; GSSG, oxidized glutathione.
Table A4.
Effect of the immunosupressive drugs on plasma prooxidant and antioxidant parameters in transplant recipients.
Table A4.
Effect of the immunosupressive drugs on plasma prooxidant and antioxidant parameters in transplant recipients.
| HS | TX (corticoid+tacrolimus+mycophenolate) | TX (corticoid+tacrolimus+sirolimus) | TX (corticoid+mycophenolate+cyclosporin) | TX (corticoid+tacrolimus) | TX (tacrolimus+mycophenolate) | |
|---|---|---|---|---|---|---|
| XO Activity (mU/mL) | 0.04±0.01 | 0.4±0.6 | 0.79 | 0.97 | 0.09±0.02 | 0.1±0.1 |
| SOD Activity (U/mL) | 0.6±1.5 | 4.7±9.7 | 1.9 | 2.51 | 0.79±0.28 | 3.8±3 |
| GPx Activity (U/mL) | 60.2±15.6 | 810±1284 | 100.7 | 249.89 | 133.6±45.9 | 238.3±62.6 |
| TBARS (nmol/mL) | 6±2.5 | 25.2±32.4 | 104.4 | 39.84 | 33.12±44.63 | 20.6±14.7 |
| GSH (umol/mL) | 1.8±0.5 | 1.7±0.6 | 1.53 | 1.2 | 1.09±0.5 | 1.2±0.6 |
HS, healthy subjects; TX, kidney transplantation; XO, xanthine oxidase; SOD, superoxide dismutase; GPx, glutathione peroxidase; TBARS, thiobasbituric acid reactive substance; GSH, reduced glutathione.
Table A5.
Effect of the immunosupressive drugs on mononuclear leukocytes prooxidant and antioxidant parameters in transplant recipients.
Table A5.
Effect of the immunosupressive drugs on mononuclear leukocytes prooxidant and antioxidant parameters in transplant recipients.
| HS | TX (corticoid+tacrolimus+mycophenolate) | TX (corticoid+tacrolimus+sirolimus) | TX (corticoid+mycophenolate+cyclosporin) | TX (corticoid+tacrolimus) | TX (tacrolimus+mycophenolate) | |
| XO Activity (mU/mL) | 2.7±1.1 | 3.7±1.6 | 6.8 | - | 7.6±1.2 | 8.8 |
| SOD Activity (U/mL) | 0.4±0.3 | 2.6±3.9 | 1.4 | 0.42 | 2.7±2.9 | 10.9±12 |
| GPx Activity (U/mL) | 0.8±1.1 | 3.9±5.2 | 0.39 | 0.9 | 0.61 | 1.6 |
| MDA (nmol/mL) | 3.5±3 | 11.2±11.4 | 7.16 | - | 6.7 | 39.3±38.1 |
| GSH (umol/mL) | 6±5.2 | 33.5±67.5 | 7.2 | 3 | 19±12 | 9±6 |
| GSSG (umol/mL) | 3.2±2.1 | 30.4±58.5 | 43 | 11.31 | 44,8±54.7 | 34.7±15.7 |
| GSSG/GSH | 1±0.9 | 1.9±1.7 | 0.16 | 3.77 | 4.1±5.5 | 4.3±1.5 |
HS, healthy subjects; TX, kidney transplantation; XO, xanthine oxidase; SOD, superoxide dismutase; GPx, glutathione peroxidase; MDA, malondialdehyde; GSH, reduced glutathione; GSSG, oxidized glutathione.
Table A6.
Effect of immunosupressive drugs on polymorphonuclear leukocytes prooxidant and antioxidant parameters in transplant recipients.
Table A6.
Effect of immunosupressive drugs on polymorphonuclear leukocytes prooxidant and antioxidant parameters in transplant recipients.
| HS | TX (corticoid+tacrolimus+mycophenolate) | TX (corticoid+mycophenolate+cyclosporin) | TX (corticoid+tacrolimus) | TX (tacrolimus+mycophenolate) | TX (tacrolimus+mycophfenolate) | |
|---|---|---|---|---|---|---|
| XO Activity (mU/mL) | 2.4±1.8 | 1.6±0.7 | 9.2 | 2.52 | 1.8±0.8 | 1.1±0.5 |
| SOD Activity (U/mL) | 0.5±0.8 | 3.4±2.5 | 18.6 | 3.84 | 1.7±2.1 | 0.9 |
| GPx Activity (U/mL) | 0.3±0.1 | 0.7±0.5 | 0.4 | 0.5 | 2.4±0.1 | 0.4 |
| MDA (nmol/mL) | 3.3±2.1 | 4.4±3.4 | 7.9 | 6.04 | 3.5 | - |
| GSH (umol/mL) | 1.3±2.4 | 7.5±11.7 | 26.5 | - | 2.3±2.3 | 2.1±2.8 |
| GSSG (umol/mL) | 0.2±0.1 | 7.4±3.6 | 24.9 | 14.4 | 8.9±7.6 | 6.7±1.9 |
| GSSG/GSH | 0.4±0.3 | 3.9±4.7 | 0.9 | - | 3.1±0.8 | 53.8 |
HS, healthy subjects; TX, kidney transplantation; XO, xanthine oxidase; SOD, superoxide dismutase; GPx, glutathione peroxidase; MDA, malondialdehyde; GSH, reduced glutathione; GSSG, oxidized glutathione.
References
- House, A.A.; Wanner, C.; Sarnak, M.J.; et al. Heart failure in chronic kidney disease: Conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int. 2019, 95, 1304–1317. [Google Scholar] [CrossRef]
- Zijlstra, L.E.; Trompet, S.; Mooijaart, S.P.; et al. The association of kidney function and cognitive decline in older patients at risk of cardiovascular disease: A longitudinal data analysis. BMC Nephrol. 2020, 21, 81. [Google Scholar] [CrossRef]
- Priyadarshani, W.V.D.; de Namor, A.F.D.; Silva, S.R.P. Rising of a global silent killer: critical analysis of chronic kidney disease of uncertain aetiology (CKDu) worldwide and mitigation steps. Environmental Geochemistry and Health. 2023, 45, 2647–2662. [Google Scholar] [CrossRef]
- Cheung, C.Y.; Tang, S.C.W. Personalized immunosuppression after kidney transplantation. Nephrology. 2022, 27, 475–483. [Google Scholar] [CrossRef]
- Vida, C.; Oliva, C.; Yuste, C.; et al. Oxidative stress in patients with advanced ckd and renal replacement therapy: The key role of peripheral blood leukocytes. Antioxidants. 2021, 10, 1155. [Google Scholar] [CrossRef]
- Veglia, F.; Cavalca, V.; Tremoli, E. OXY-SCORE: a global index to improve evaluation of oxidative stress by combining pro- and antioxidant. 2010. [CrossRef]
- Cerqueira, A.; Quelhas-Santos, J.; Sampaio, S.; et al. Endothelial dysfunction is associated with cerebrovascular events in pre-dialysis CKD patients: a prospective study. Life. 2021, 11, 128. [Google Scholar] [CrossRef]
- Maraj, M.; Kusnierz-Cabala, B.; Dumnicka, P.; et al. Redox balance correlates with nutritional status among patients with end-stage renal disease treated with maintenance hemodialysis. Oxid Med Cell Longev. 2019, 2019, 1–10. [Google Scholar] [CrossRef]
- Cecerska-Heryć, E.; Heryć, R.; Dutkiewicz, G.; et al. Xanthine oxidoreductase activity in platelet-poor and rich plasma as an oxidative stress indicator in patients requiring renal replacement therapy. BMC Nephrol. 2022, 23, 1–14. [Google Scholar] [CrossRef]
- Cañas, L.; Iglesias, E.; Pastor, M.C.; et al. Inflammation and oxidation: do they improve after kidney transplantation? Relationship with mortality after transplantation. Int Urol Nephrol. 2017, 49, 533–540. [Google Scholar] [CrossRef]
- Yepes-Calderón, M.; Sotomayor, C.G.; Gans, R.O.B.; et al. Post-transplantation plasma malondialdehyde is associated with cardiovascular mortality in renal transplant recipients: a prospective cohort study. Nephrol Dial Transplant. 2020, 35, 512–519. [Google Scholar] [CrossRef]
- Soleymanian, T.; Hamid, G.; Arefi, M.; et al. Non-diabetic renal disease with or without diabetic nephropathy in type 2 diabetes: clinical predictors and outcome. Ren Fail. 2015, 37, 572–575. [Google Scholar] [CrossRef]
- Rangaswami, J.; Mathew, R.O.; Parasuraman, R.; et al. Cardiovascular disease in the kidney transplant recipient: epidemiology, diagnosis and management strategies. Nephrol Dial Transplant. 2019, 34, 760–773. [Google Scholar] [CrossRef]
- Klawitter, J.; Reed-Gitomer, B.Y.; McFann, K.; et al. Endothelial dysfunction and oxidative stress in polycystic kidney disease. Am J Physiol Renal Physiol. 2014, 307, F1198–F1206. [Google Scholar] [CrossRef]
- Qasim, M.T.; Mohammed, Z.I. The Impact of glomerulonephritis on cardiovascular disease: Exploring pathophysiological links and clinical implications. J Rare Cardiovasc Dis. 2025, 5, 3–8. [Google Scholar]
- Martinez-Hervas, S.; Real, J.T.; Ivorra, C.; et al. Increased plasma xanthine oxidase activity is related to nuclear factor kappa beta activation and inflammatory markers in familial combined hyperlipidemia. Nutr Metab Cardiovasc Dis. 2010, 20, 734–739. [Google Scholar] [CrossRef]
- Kushiyama, A.; Okubo, H.; Sakoda, H.; et al. Xanthine oxidoreductase is involved in macrophage foam cell formation and atherosclerosis development. Arterioscler Thromb Vasc Biol. 2012, 32, 291–298. [Google Scholar] [CrossRef]
- Yu, H.; Chen, X.; Guo, X.; Chen, D.; et al. The clinical value of serum xanthine oxidase levels in patients with acute ischemic stroke. Redox Biol. 2023, 60, 102623. [Google Scholar] [CrossRef]
- Oki, R.; Hamasaki, Y.; Komaru, Y.; et al. Plasma xanthine oxidoreductase is associated with carotid atherosclerosis in stable kidney transplant recipients. Nephrology. 2022, 27, 363–370. [Google Scholar] [CrossRef]
- Perez-Garcia, R.; Ramirez, R.; de Sequera, P.; et al. Citrate dialysate does not induce oxidative stress or inflammation in vitro as compared to acetate dialysate. Nefrologia. 2017, 37, 630–637. [Google Scholar] [CrossRef]
- Mamode, N.; Bestard, O.; Claas, F.; et al. European Guideline for the Management of Kidney Transplant Patients With HLA Antibodies: By the European Society for Organ Transplantation Working Group. Transplant Int. 2022, 35, 10511. [Google Scholar] [CrossRef]
- Ayala, A.; Muñoz, M.F.; Argüelles, S. Lipid Peroxidation: Production, Metabolism, and Signaling Mechanisms of Malondialdehyde and 4-Hydroxy-2-Nonenal. Oxid Med Cell Longev. 2014, 2014, 360438. [Google Scholar] [CrossRef]
- Andrade, F.; Darrah, E.; Rosen, A. Autoantibodies in Rheumatoid Arthritis. In: Firestein GS, Budd RC, Gabriel SE, McInnes IB, O’Dell JR, editors. Kelley and Firestein’s Textbook of Rheumatology. 10th ed. Amsterdam: Elsevier; 2017. p. 831–45. [CrossRef]
- Kumar, S.; Sharma, U.; Sharma, A.; et al. Evaluation of oxidant and antioxidant status in living donor renal allograft transplant recipients. Mol Cell Biochem. 2016, 413, 1–8. [Google Scholar] [CrossRef]
- Martín-Timón, I.; Sevillano-Collantes, C.; Segura-Galindo, A.; et al. Type 2 diabetes and cardiovascular disease: Have all risk factors the same strength? World J Diabetes. 2014, 5, 444–470. [Google Scholar] [CrossRef]
- Gutteridge, J.M.C.; Halliwell, B. Mini-Review: oxidative stress, redox stress or redox success? Biochem. Biophys. Res. Commun. 2018, 502, 183–186. [Google Scholar] [CrossRef]
- Moreno, J.M.; Ruiz, M.C.; Ruiz, N.; et al. Modulation factors of oxidative status in stable renal transplantation. Transplantation Proceedings. 2005, 37, 1428–1430. [Google Scholar] [CrossRef] [PubMed]
- Younus, H. Therapeutic potentials of superoxide dismutase. Int. J. Health Sci. 2018, 12, 88–93. [Google Scholar]
- Zachara, B.A.; Wlodarczyk, Z.; Andruszkiewicz, J.; et al. Glutathione and glutathione peroxidase activities in blood of patients in early stages following kidney transplantation. Renal Failure. 2005, 27, 751–755. [Google Scholar] [CrossRef]
- Ruiz, M.C.; Medina, A.; Moreno, J.M.; et al. Relationship between oxidative stress parameters and atherosclerotic signs in the carotid artery of stable renal transplant patients. Transplantation Proceedings. 2005, 37, 3796–3798. [Google Scholar] [CrossRef]
- Prasai, P.K.; Shrestha, B.; Orr, A.W.; et al. Decreases in GSH:GSSG activate vascular endothelial growth factor receptor 2 (VEGFR2) in human aortic endothelial cells. Redox Biology. 2018, 19, 22–27. [Google Scholar] [CrossRef]
- Heras Benito, M. Nephroangiosclerosis: an update. Hipertension y Riesgo Vascular. 2023, 40, 98–103. [Google Scholar] [CrossRef]
- Lassègue, B.; Griendling, K.K. NADPH oxidases: Functions and pathologies in the vasculature. Arteriosclerosis, Thrombosis, and Vascular Biology. 2010, 30, 653–661. [Google Scholar] [CrossRef]
- Bigagli, E.; Raimondi l Mannucci, E.; et al. Lipid and protein oxidation products, antioxidant status and vascular complications in poorly controlled type 2 diabetes. Br. J. Diabetes Vasc. Dis. 2012, 12, 33–39. [Google Scholar] [CrossRef]
- Bandeira, S.M.; Guedes, G.S.; da Fonseca, L.J.; et al. Characterization of blood oxidative stress in type 2 diabetes mellitus patients: Increase in lipid peroxidation and SOD activity. Oxid. Med. Cell. Longev. 2012, 819310. [Google Scholar] [CrossRef]
- Strom, A.; Kaul, K.; Brüggemann, J. , et al Lower serum extracellular superoxide dismutase levels are associated with polyneuropathy in recent-onset diabetes. Exp. Mol. Med. 2017, 49, e394. [Google Scholar] [CrossRef] [PubMed]
- Adeshara, K.A.; Diwan, A.G.; Jagtap, T.R.; et al. Relationship between plasma glycation with membrane modification, oxidative stress and expression of glucose trasporter-1 in type 2 diabetes patients with vascular complications. J. Diabetes Complicat. 2017, 31, 439–448. [Google Scholar] [CrossRef]
- Chapman, A.B.; Devuyst, O.; Eckardt, K.U.; et al. Autosomal-dominant polycystic kidney disease (ADPKD): Executive summary from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney International. 2015, 88, 17–27. [Google Scholar] [CrossRef]
- Maser, R.L.; Vassmer, D.; Magenheimer, B.S.; et al. Oxidant stress and reduced antioxidant enzyme protection in polycystic kidney disease. J. Am. Soc. Nephrol. 2002, 13, 991–999. [Google Scholar] [CrossRef]
- Angeletti, A.; Bruschi, M.; Kajana, X.; et al. Mechanisms Limiting Renal Tissue Protection and Repair in Glomerulonephritis. International Journal of Molecular Sciences. 2023, 24. [Google Scholar] [CrossRef]
- Praga, M.; Sevillano, A.; Gonzalez, E. Changes in the aetiology, clinical presentation and management of acute interstitial nephritis, an increasingly common cause of acute kidney injury. Nephrology Dialysis Transplantation. 2015, 30, 1472–1479. [Google Scholar] [CrossRef]
- Odegaard, A.O.; Jacobs, D.R.; Sanchez, O. A. Oxidative stress, inflammation, endothelial dysfunction and incidence of type 2 diabetes. Cardiovascular Diabetology. 2016, 15, 1–12. [Google Scholar] [CrossRef]
- Montiel, V.; Lobysheva, I.; Gérard, L.; et al. Oxidative stress-induced endothelial dysfunction and decreased vascular nitric oxide in COVID-19 patients. EbioMedicine. 2022, 77, 1–18. [Google Scholar] [CrossRef]
- Li, X.; Lin, Y.; Wang, S.; et al. Extracellular superoxide dismutase is associated with left ventricular geometry and heart failure in patients with cardiovascular disease. Journal of the American Heart Association. 2020, 9. [Google Scholar] [CrossRef]
- Zawada, A.M.; Carrero, J.J.; Wolf, M.; et al. Serum Uric Acid and Mortality Risk Among Hemodialysis Patients. Kidney International Reports, 2020, 5, 1196–1206. [Google Scholar] [CrossRef] [PubMed]
- Rybka, J.; Kupczyk, D.; Kedziora-Kornatowska, K.; et al. Glutathione-related antioxidant defense system in elderly patients treated for hypertension. Cardiovasc. Toxicol. 2011, 11, 1–9. [Google Scholar] [CrossRef]
- Damy, T.; Kirsch, M.; Khouzami, L.; et al. Glutathione deficiency in cardiac patients is related to the functional status and structural cardiac abnormalities. PLoS ONE. 2009, 4, e4871. [Google Scholar] [CrossRef]
Figure 1.
CVD incidence based on the etiology. (a) CVD, (b) ischemic cardiopathy, (c) ACVA, (d) vasculopathy, and (e) CCI incidence in HS, ACKD, and transplanted patients with nephroangioesclerosis, diabetic nephropathy, policystic kidney disease, interstitial nephropathy and glomerulopathy. CVD, cardiovascular disease; ACVA, acute cardiovascular accident; CCI, chronic cardiac insufficience; HS, healthy subjects; ACKD, advanced chronic kidney disease; NAS, nephroangioesclerosis; DN, diabetic nephropathy; ADPKD, autosomal dominant policystic kidney disease; IN, interstitial nephritis; GN, glomerulonephritis. **P<0.01 vs HS; ***P<0.001 vs HS; ##P<0.01 vs ACKD; ###P<0.001 vs ACKD; $$$P<0.001 vs NAS; &&&P<0.001 vs DN; +P<0.05 vs ADPKD; +++P<0.001 vs ADPKD; aP<0.05 vs IN; aaP<0.01 vs IN. Chi square.
Figure 1.
CVD incidence based on the etiology. (a) CVD, (b) ischemic cardiopathy, (c) ACVA, (d) vasculopathy, and (e) CCI incidence in HS, ACKD, and transplanted patients with nephroangioesclerosis, diabetic nephropathy, policystic kidney disease, interstitial nephropathy and glomerulopathy. CVD, cardiovascular disease; ACVA, acute cardiovascular accident; CCI, chronic cardiac insufficience; HS, healthy subjects; ACKD, advanced chronic kidney disease; NAS, nephroangioesclerosis; DN, diabetic nephropathy; ADPKD, autosomal dominant policystic kidney disease; IN, interstitial nephritis; GN, glomerulonephritis. **P<0.01 vs HS; ***P<0.001 vs HS; ##P<0.01 vs ACKD; ###P<0.001 vs ACKD; $$$P<0.001 vs NAS; &&&P<0.001 vs DN; +P<0.05 vs ADPKD; +++P<0.001 vs ADPKD; aP<0.05 vs IN; aaP<0.01 vs IN. Chi square.
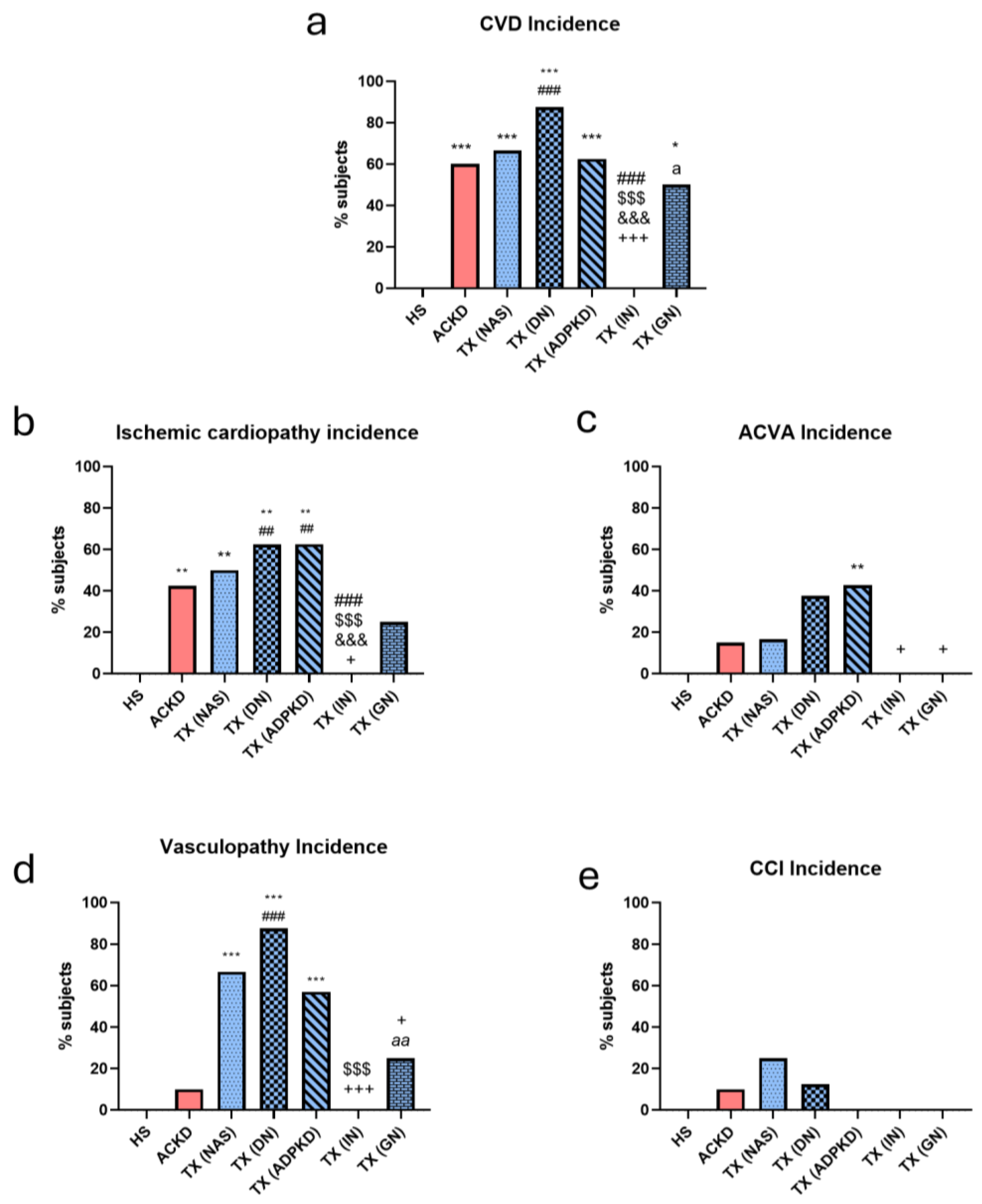
Figure 2.
Plasmatic prooxidant and antioxidant parameters. (a) Activity of XO, (b) levels of TBARS, (c) activity of SOD, (d) activity of GPx, and (e) levels of GSH in plasma and patients with ACKD, TX, and HS. XO, xanthine oxidase; TBARS, thiobarbituric acid reactive substance; SOD, superoxide dismutase; GPx, glutathion peroxidase; GSH, reduced glutathion; HS, healthy subjects; ACKD, advanced chronic kidney disease; TX, transplantation. *P<0.05 vs HS; **P<0.01 vs HS; ***P<0.001 vs HS; ###P<0.001 vs ACKD. ANOVA and Kruskal Wallis.
Figure 2.
Plasmatic prooxidant and antioxidant parameters. (a) Activity of XO, (b) levels of TBARS, (c) activity of SOD, (d) activity of GPx, and (e) levels of GSH in plasma and patients with ACKD, TX, and HS. XO, xanthine oxidase; TBARS, thiobarbituric acid reactive substance; SOD, superoxide dismutase; GPx, glutathion peroxidase; GSH, reduced glutathion; HS, healthy subjects; ACKD, advanced chronic kidney disease; TX, transplantation. *P<0.05 vs HS; **P<0.01 vs HS; ***P<0.001 vs HS; ###P<0.001 vs ACKD. ANOVA and Kruskal Wallis.
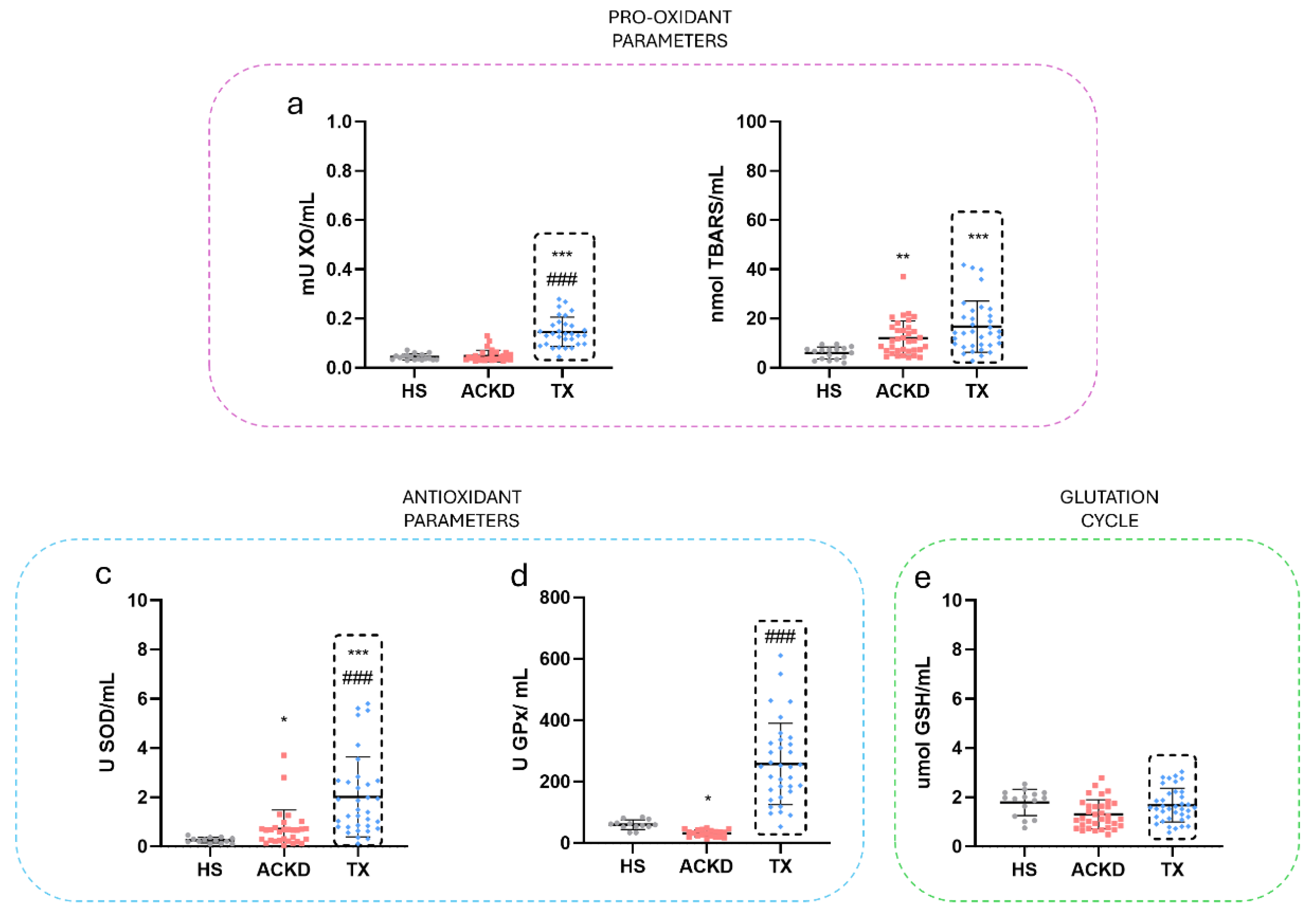
Figure 3.
Prooxidant and antioxidant parameters in mononuclear leukocytes. (a) Activity of XO, (b) levels of MDA, (c) activity of SOD, (d) activity of GPx, (e) levels of GSSG, (f) levels of GSH and (g) GSSG/GSH ratio in MN and patients with ACKD, TX, and HS. XO, xanthine oxidase; MDA, malondialdehyde; SOD, superoxide dismutase; GPx, glutathion peroxidase; GSSG, oxidized glutthion; GSH, reduced glutathion; HS, healthy subjects; ACKD, advanced chronic kidney disease; TX, transplantation. *P<0.05 vs HS; **P<0.01 vs HS; ***P<0.001 vs HS; ##P<0.01 vs ACKD; ###P<0.001 vs ACKD. ANOVA and Kruskal Wallis.
Figure 3.
Prooxidant and antioxidant parameters in mononuclear leukocytes. (a) Activity of XO, (b) levels of MDA, (c) activity of SOD, (d) activity of GPx, (e) levels of GSSG, (f) levels of GSH and (g) GSSG/GSH ratio in MN and patients with ACKD, TX, and HS. XO, xanthine oxidase; MDA, malondialdehyde; SOD, superoxide dismutase; GPx, glutathion peroxidase; GSSG, oxidized glutthion; GSH, reduced glutathion; HS, healthy subjects; ACKD, advanced chronic kidney disease; TX, transplantation. *P<0.05 vs HS; **P<0.01 vs HS; ***P<0.001 vs HS; ##P<0.01 vs ACKD; ###P<0.001 vs ACKD. ANOVA and Kruskal Wallis.
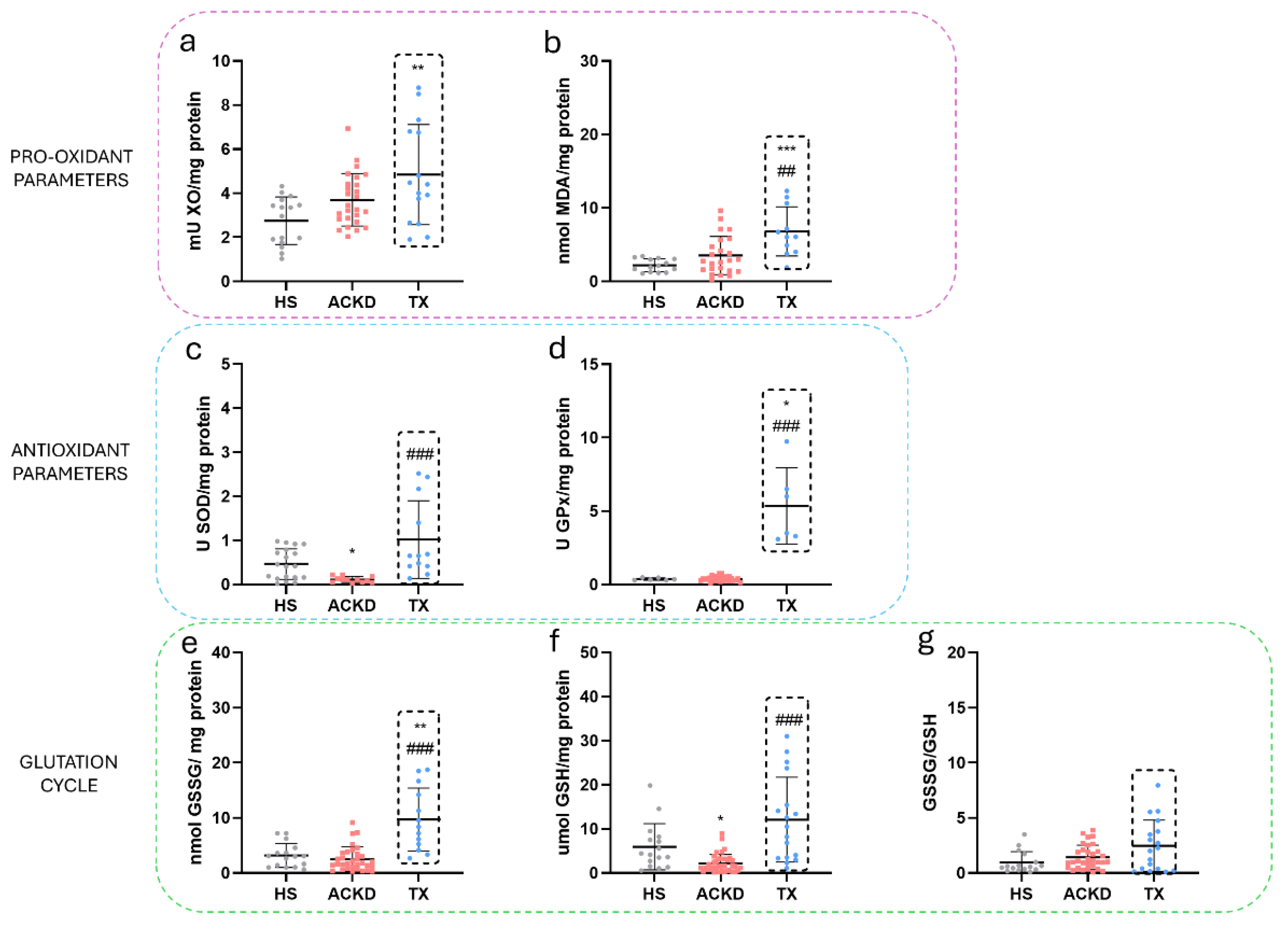
Figure 4.
Prooxidant and antioxidant parameters in polymorphonuclear leukocytes. (a) Activity of XO, (b) levels of MDA, (c) activity of SOD, (d) activity of GPx, (e) levels of GSSG, (f) levels of GSH and (g) GSSG/GSH ratio in PMN and patients with ACKD, TX, and HS. XO, xanthine oxidase; MDA, malondialdehyde; SOD, superoxide dismutase; GPx, glutathion peroxidase; GSSG, oxidized glutthion; GSH, reduced glutathion; HS, healthy subjects; ACKD, advanced chronic kidney disease; TX, transplantation. *P<0.05 vs HS; ***P<0.001 vs HS; ##P<0.01 vs ACKD; ###P<0.001 vs ACKD. ANOVA and Kruskal Wallis.
Figure 4.
Prooxidant and antioxidant parameters in polymorphonuclear leukocytes. (a) Activity of XO, (b) levels of MDA, (c) activity of SOD, (d) activity of GPx, (e) levels of GSSG, (f) levels of GSH and (g) GSSG/GSH ratio in PMN and patients with ACKD, TX, and HS. XO, xanthine oxidase; MDA, malondialdehyde; SOD, superoxide dismutase; GPx, glutathion peroxidase; GSSG, oxidized glutthion; GSH, reduced glutathion; HS, healthy subjects; ACKD, advanced chronic kidney disease; TX, transplantation. *P<0.05 vs HS; ***P<0.001 vs HS; ##P<0.01 vs ACKD; ###P<0.001 vs ACKD. ANOVA and Kruskal Wallis.
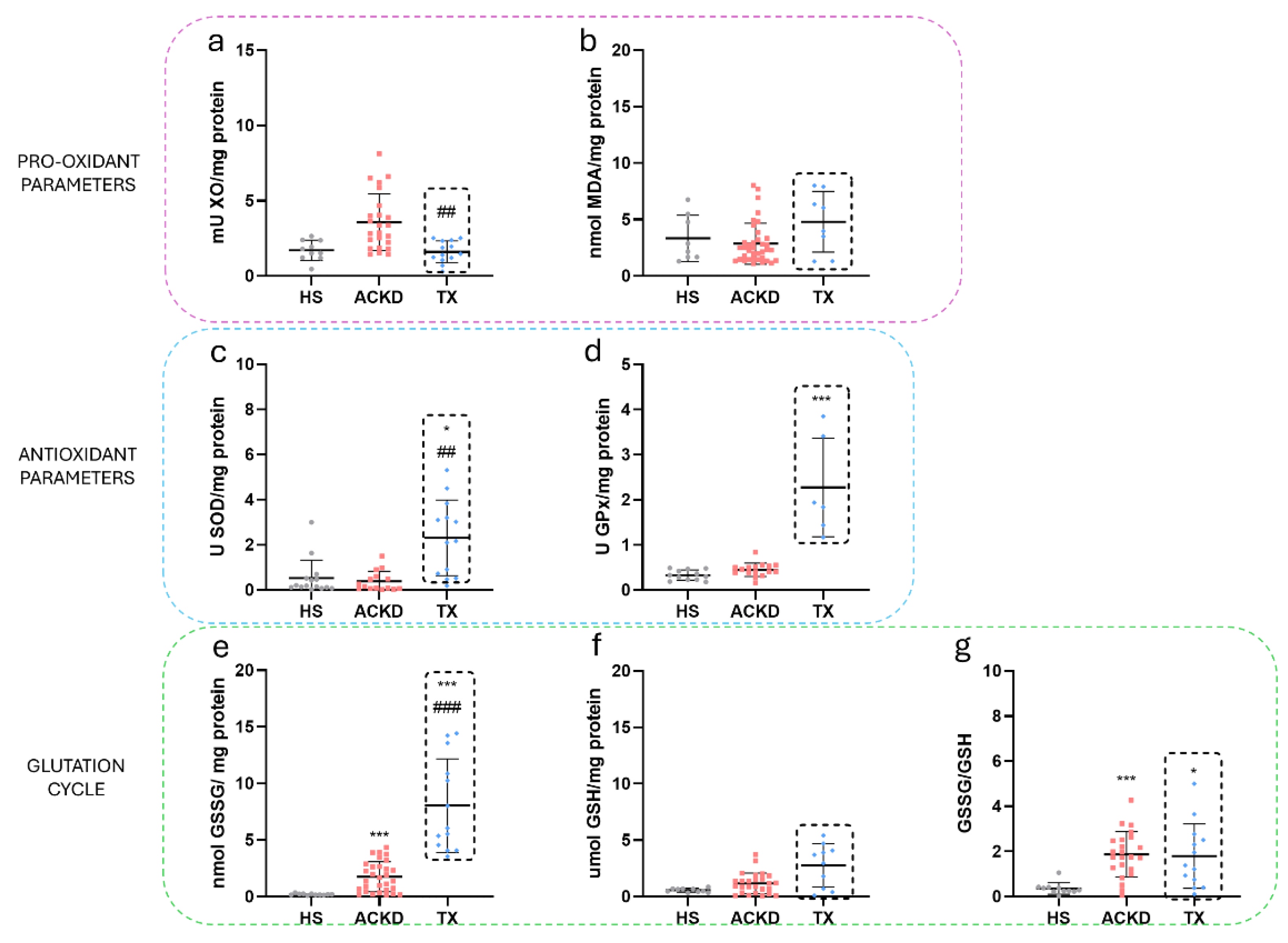
Figure 5.
OXYSCORE levels in TX based on etiology and CVD. (a) OXYSCORE levels in HS, ACKD and TX, (b) OXYSCORE levels in HS, ACKD and TX according to a systemic or localised kidney disease, (c) OXYSCORE levels in HS, ACKD and TX related to the presence cardiovascular disease. HS, healthy subjects; ACKD, advanced chronic kidney disease; TX, transplantation; NAS, nephroangioesclerosis; DN, diabetic nephropathy; ADPKD, autosomal dominant policystic kidney disease; IN, interstitial nephritis; GN, glomerulonephritis CVD, cardiovascular disease. *P<0.05 vs HS; **P<0.01 vs HS; ***P<0.001 vs HS; +P>0.05 vs ADPKD. Kruskal Wallis.
Figure 5.
OXYSCORE levels in TX based on etiology and CVD. (a) OXYSCORE levels in HS, ACKD and TX, (b) OXYSCORE levels in HS, ACKD and TX according to a systemic or localised kidney disease, (c) OXYSCORE levels in HS, ACKD and TX related to the presence cardiovascular disease. HS, healthy subjects; ACKD, advanced chronic kidney disease; TX, transplantation; NAS, nephroangioesclerosis; DN, diabetic nephropathy; ADPKD, autosomal dominant policystic kidney disease; IN, interstitial nephritis; GN, glomerulonephritis CVD, cardiovascular disease. *P<0.05 vs HS; **P<0.01 vs HS; ***P<0.001 vs HS; +P>0.05 vs ADPKD. Kruskal Wallis.
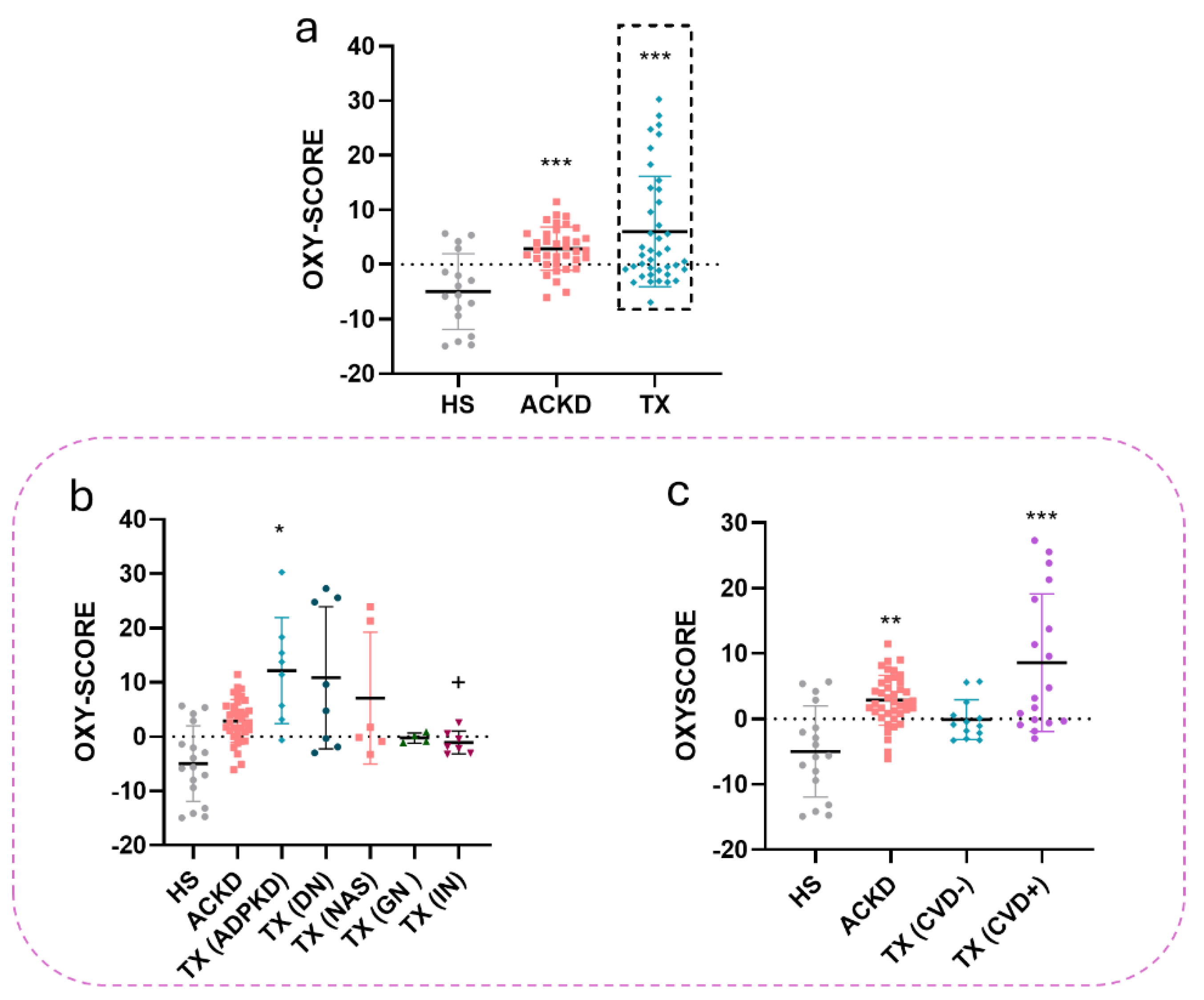
Figure 6.
OXYSCORE levels in TX based on anti-graft antibodies and time since transplantation. (a) OXYSCORE levels in patients with kidney transplantation and absence or presence of anti-graft antibodies, (b) OXYSCORE levels in patients with kidney transplantation for less or more than 5 years since transplantation. ***P<0.001 vs HS. Kruskal Wallis.
Figure 6.
OXYSCORE levels in TX based on anti-graft antibodies and time since transplantation. (a) OXYSCORE levels in patients with kidney transplantation and absence or presence of anti-graft antibodies, (b) OXYSCORE levels in patients with kidney transplantation for less or more than 5 years since transplantation. ***P<0.001 vs HS. Kruskal Wallis.
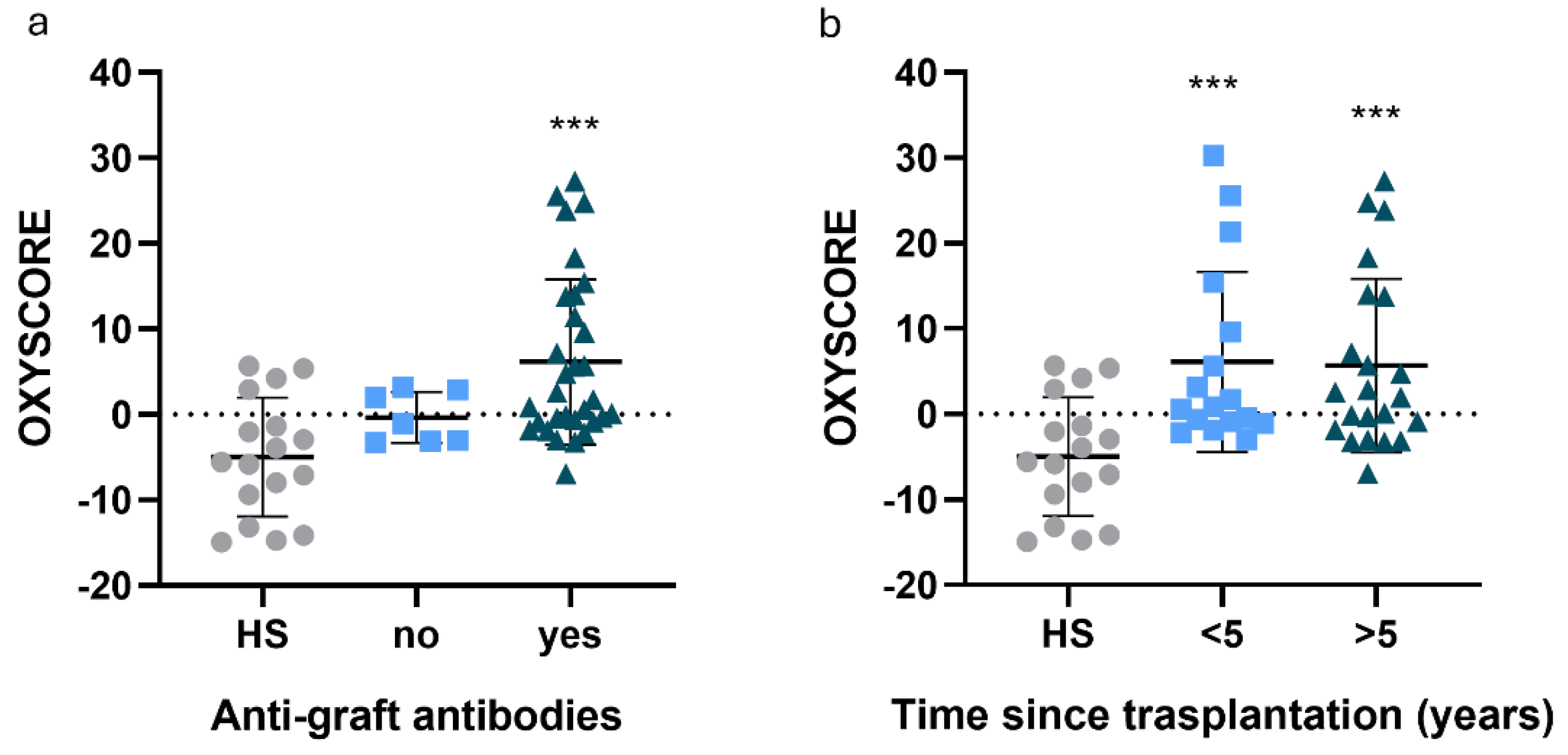
Table 1.
Demographic and clinical characteristics of the study population.
| Characteristics | HS (n=18) | ACKD (36) | TX (n=40) |
|---|---|---|---|
| Age (years±sd) | 54.83±16.25 | 61.16±16.48 | 56.22±13.55 |
| Gender (Women (%)) | 12 (52.2) | 14 (38.9) | 13 (32.5) |
| CVD (n (%)) | 0 (0) | 23 (63.9)** | 20 (50)** |
| Ischemic cardiopathy (n (%)) | 0 (0) | 16 (44.4)** | 16 (40)** |
| Acute cardiovascular accident (n (%)) | 0 (0) | 6 (16.7) | 9 (22.5) |
| Vasculopathy (n (%)) | 0 (0) | 4 (11.1) | 18 (45)** # |
| Chronic heart failure (n (%)) | 0 (0) | 3 (8.3) | 2 (5) |
| Arterial hypertension (n(%)) | 1 (5.8) | 32 (88.9)*** | 39 (97.5)*** |
| Beta-blockers (n(%)) | 0 (0) | 9 (25)* | 11 (27.5)* |
| Angiotensin II receptor blockers (n(%)) | 0 (0) | 3 (8.3) | 3 (7.5) |
| Calcium channel blockers (n(%)) | 0 (0) | 11 (30.6)* | 13 (32.5)* |
| Diuretics (n(%)) | 0 (0) | 4 (11.1) | 3 (7.5) |
| ACE inhibitors (n(%)) | 0 (0) | 3 (8.3) | 9 (22.5) |
| Dyslipidemia (n(%)) | 0 (0) | 27 (75)*** | 21 (52.5)*** |
| Statins (n(%)) | 0 (0) | 26 (72.2)*** | 17 (73.9)* |
| Diabetes mellitus (n(%)) | 1 (5.5) | 16 (44.4)** | 16 (40)** |
| Insulin (n(%)) | 1 (5.5) | 9 (25)* | 9 (22.5)** |
| SGLT2 inhibitors (n(%)) | 0 (0) | 14 (46.7)** | 1 (2.5) ## |
| Biguanide (n(%)) | 0 (0) | 2 (5.6) | 2 (5) |
| DPP-4 inhibitors (n(%)) | 0 (0) | 3 (10) | 1 (2.5) |
| Hyperuricemia (n(%)) | 0 (0) | 25 (69.4)*** | 8 (20)* # |
| Allopurinol (n(%)) | 0 (0) | 21 (58.3)** | 11 (27.5)** # |
| Erythropoietin (n(%)) | 0 (0) | 30 (100)*** | 8 (20)## |
| Metabolic syndrome (n(%)) | 0 (0) | 9 (25)* | 6 (15) |
| COPD (n(%)) | 0 (0) | 1 (2.8) | 7 (17.5)# |
| Liver disease (n(%)) | 0 (0) | 3 (8.3) | 8 (20) |
| Cancer (n(%)) | 0 (0) | 1 (2.8) | 11 (55)## |
| Antibodies against transplantation (n(%)) | - | - | 21 (52.5) |
| Immunosuppressive treatment (n(%)) | - | - | 36 Corticosteroid (90) 38 Tacrolimus (95) 32 Mycophenolate (80) 5 Everolimus (12.5) |
| Time since transplantation (n(%)) | - | - | 17 less than 5 years (42.5) 23 more than 5 years (57.5) |
| Aetiology of CKD (n(%)) | - | 7 NAS (19.4) 13 DN (36.4) 1 ADPKD (11.1) 6 IN (16.7) 6 GN (16.7) |
6 NAS (15) 8 DN (20) 8 ADPKD (20) 7 IN (17.5) 4 GN (10) 7 Others (17.5) |
| Tobacco (n(%)) | 4 (22.2) | 9 (25) | 10 (25) |
| Mortality rate (n(%)) | 0 (0) | 13 (36.1)* | 3 (7.5) |
HS, healthy subject; ACKD, advanced chronic kidney disease; TX, kidney transplantation; CVD, cardiovascular disease; ACE, angiotensin-converting Enzyme; SGLT2, sodium glucose co-transporter type 2 inhibitors; DPP-4, di-peptidyl peptidase-4; COPD, Chronic obstructive pulmonary disease; NAS, nephroangioesclerosis; DN, diabetic nephropathy; ADPKD, autosomal dominant polycystic kidney disease; IN, interstitial nephritis; GN, glomerulone-phritis; SD, standard deviation. *P<0.05 vs HS; **P<0.01 vs HS; ***P<0.01 vs HS; #P<0.05 vs. ACKD, ## P < 0.01 vs. ACKD. Chi-square test.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



