
Submitted:
20 August 2025
Posted:
21 August 2025
You are already at the latest version
Abstract
It is imperative that futsal athletes enhance their functional performance to improve their performance and reduce the risk of injuries. This study aimed to determine whether futsal athletes have markers of biological individuality that can be used to identify a higher risk of anterior cruciate ligament injuries. Evaluated 85 former futsal athletes with ACL injuries and 127 without injuries. The protocol used to determine the markers of biological individuality was dermatoglyphics. There was a statistically significant association between the print pattern of the index finger of the left hand =and the little finger of the right hand. While the group with anterior cruciate ligament injuries had a greater number of spiral whorls print patterns in these two fingers, the group without injuries had a greater number of whorls print patterns in the little finger of the right hand. Specific markers of biological individuality can be used to identify higher risk of anterior cruciate ligament injuries in futsal athletes.
Keywords:
dermatoglyphics
; injuries
; anterior cruciate ligament
; sports career
; health
1. Introduction
Football is a sport that became a mass sport during the 20th century [1]. Futsal, a combination of the Spanish words: "fútbol" and "sala", refers to football played indoors [2]. Due to the special characteristics of the game, it has become a worldwide sport [3,4]. Recently, it has gained greater visibility in both educational and professional settings [5]. In the last two decades, it has gained popularity and become a sport that attracts a large audience [6,7]. It is characterized as a dynamic sport that requires various physical abilities to execute technical and tactical actions [8,9]. According to the Fédération Internationale de Football Association (FIFA), this sport is played by more than 270 million players [10]. These facts have led sports science to make an important contribution to this sport by developing more efficient training methods to achieve better performance and results [11]. It is essential that futsal athletes enhance their functional performance to improve their performance and reduce the risk of injuries [12].
Injuries are observed to occur because of the movement patterns required in this sport, such as jumps, short and long displacements, rapid changes of direction, technical actions, and frequent physical contact between players [13,14,15]. Factors, such as age, training load, level of play, tactical dynamics, and training patterns may contribute to the occurrence of injuries [16]. The most common injuries are those manifested by changes in muscles, nerves, tendons and ligaments, joints, and cartilage, including inflammatory and degenerative processes that affect the entire musculoskeletal system [17]. The main injuries are anterior cruciate ligament injuries (ACL), which account for approximately 79% of all joint injuries [18,19], regardless of whether the player is an amateur or professional player [20]. Ligament rupture is usually associated with changes in direction, jumping, or sudden deceleration [21,22]. The pathomechanics of the ACL is associated with hyperextension of the knee, alone or in combination with internal rotation of the tibia [23]. However, the most common mechanism of injuries is rotation of the femur on the tibia during excessive valgus motion (pivoting) [24]. Approximately 70% of all ACL injuries occur due to non-contact injuries mechanisms between players [25,26]. To recover, the athlete is usually out of action for six to nine months [27], which significantly affects their quality of life [20,28]. Professional players are those who suffer the most from this type of injuries [29]. They often give up this sport because of the cost and time spent outside their normal activities [30]. Approximately 47% of professional futsal players are forced to give up their career due to physical trauma [31]. ACL affects the athlete's performance and negatively impacts their physical and mental health; it increases the risk of physical disability and premature interruption of sports careers, as injured athletes may experience frustration, loss of identity, and sleep disorders [20,28,32].
Intrinsic and extrinsic factors are directly related to ACL injuries, and there is significant potential for genetic predisposition to these injuries [33]. The advent of modern biotechnology enabled the recognition of fingerprints through dermatoglyphics. Fingerprints are dermal representations of genetic traits [34,35]. The prints in the distal phalanx of each finger are individual identifiers that have been used in China since 300 BC [36]. The analyzed drawings have three basic shapes: arch (A), loop (L), and whorl (W) [37]. An arch is characterized by the absence of deltas or tri-radium and consists of ridges that cross the phalanx transversely. A loop is represented by a delta. It is a half-closed drawing, in which the ridges of the skin begin at one end of the finger and bend distally to the other, but without approaching the point where they begin. The whorl is represented by two deltas. It is a closed figure in which the center lines are around the center of the drawing [38].
In recent years, dermatoglyphics have been used for health prognosis [39,40,41]. In high performance sports, dermatoglyphics helps both in the physical preparation of athletes [42] and as a tool to recommend and guide talented young people [38,43]. The confirmation of the existence of dermatoglyphic markers in former futsal athletes who have been affected by ACL injuries could allow the development of predictive, preventive, and directional assessment parameters to help other athletes minimize the risk of being affected by these injuries. Our study aims to determine whether futsal athletes have markers of biological individuality that can be used to identify the risk of ACL injuries.
2. Materials and Methods
2.1. Design
This is an exploratory-analytical study of 212 former Brazilian, Spanish, and Italian male futsal athletes, 85 of whom had an ACL injury and 127 of whom had no ACL injuries. All of them have played in national and international leagues. Notably, 82.5% were white, 11.0% brown, and 6.5% black, and 77.9% were right-handed. The mean age of the athletes when they stopped playing professionally was 39.1 ± 9.0 years; and the overall mean age that they started specific futsal training was 9.4 ± 3.8 years.
2.2. Protocol
The protocol used to define the markers of biological individuality was dermatoglyphics [34]. To capture, process, and analyze the markers, we used the method validated for the Brazilian population [37,44]. We used the Watson Mini digital biometric reader to digitize the prints. After collecting the images, we determined the number of lines and the print pattern of all fingers of both hands [44,45]. The hands were coded as ME and MD, respectively; the fingers were coded between D1 and D5, where D1 represented the thumb, D2 the index finger, D3 the middle finger, D4 the ring finger, and D5 the little finger; TNLL and TNLR, in turn, represented the total number of lines of the fingers of both hands; TNL represented the total number of lines, and D10 represented the number of deltas of all fingers of both hands. The print patterns of arch, radial loop, ulnar loop, whorl, and spiral whorl were coded as A, LR, LU, W, and WS, respectively. Figure 1 shows the protocol used for fingerprint collection, finger coding, marking the points, and counting the number of lines on the fingers.
2.3. Statistical Analysis of Data
We used the Kolmogorov–Smirnov test to check the normality of the distribution. We checked the homoscedasticity of the variances using Levene's test. We used the Stuent's t-test to determine the differences in the mean number of lines and chi-square test to determine the association among the print patterns. We modeled the joint distribution of the categorical variables in a contingency table using log-linear regression. We used Jamovi (version 2.6) and R Language (version 4.4) to perform the statistical tests. A type I error probability (α) of 0.05 was considered in all the inferential analyses performed.
3. Results
Figure 2 shows the results of comparison of the age of athletes with and without ACL injuries when they stopped playing professionally.
The mean age of the athletes in the groups with and without ACL injuries when they stopped playing professionally showed a statistically significant difference (t = -2.660; p = 0.008). Table 1; Table 2 and Figure 3 show the results of the omnibus likelihood ratio test, the coefficients of the regression model, and the marginal means of the modeled categorical variables.
The log-linear model showed an association between the categorical variables of presence and absence of ACL injuries versus print patterns. Table 3 shows the results of comparing the number of lines per finger and hand for the presence and absence of ACL injuries.
The mean values of the number of lines did not show statistically significant differences (p > 0.05) for the groups with and without the injuries. Table 4 shows the results of the association between the print patterns per hand for the presence and absence of anterior cruciate ligament injuries.
There was a statistically significant association between the print pattern for both the left hand (χ² = 915.072; df = 4; p = 0.005) and the right hand (χ² = 18.015; df = 4; p = 0.001). There was also an association between the global analysis of hands and print pattern (χ² = 27.125; df = 4; p < 0.001). The radial print pattern of the left hand, the ulnar loop print pattern of the right hand, and the radial loop print pattern of the global analysis of hands were associated with the absence of injuries; the spiral whorl (WS) print pattern was associated with the presence of ACL injuries in the three comparisons performed (right hand, left hand, and global analysis of hands). Table 5 shows the results of the association between the print patterns per finger for the presence and absence of anterior cruciate ligament injuries.
There was a statistically significant association between the spiral whorl (WS) print pattern of the index finger of the left hand (MED2 | χ² = 9.875; df: 4; p = 0.043) in the group with ACL injuries. There was also an association for the whorl (W) print pattern and spiral whorl (WS) print pattern for the little finger of the right hand (MED5) (χ² = 11.978; df: 3; p = 0.007). The group with ACL injuries had a greater number of spiral whorl (WS) print patterns; the group without injuries had a greater number of whorl (W) print patterns. Table 6 shows the spiral whorl (WS) print pattern and the definite diagnosis for the presence and absence of anterior cruciate ligament injuries.
The sensitivity was 0.120, indicating whether the presence of the WS print pattern can be used to diagnose ACL injuries (disease/condition) in futsal athletes. The specificity was 0.937 and indicates whether the presence of the WS print pattern can be used to rule out ACL injuries (disease/condition) in futsal athletes. Figure 4 shows the cutoff values between the coefficients for specificity and sensitivity.
The accuracy (0.609) determined the proportion of all correct tests for the presence of WS print pattern versus the presence of ACL injuries and the absence of WS print pattern versus the absence of ACL injuries (true positives and true negatives) across all results obtained. A positive predictive value (PPV) of 0.560 indicated the probability that a futsal athlete with a positive test has ACL injuries. A negative predictive value (NPV) of 0.614 indicated the probability that a futsal athlete with a negative test does not have the condition. The likelihood ratio for a positive test was 1.905 and indicated the likelihood of a positive test in an athlete with ACL injuries compared to an athlete without ACL injuries. The likelihood of having a definitive diagnosis of ACL when the WS print pattern (102/80) is detected was 1.275; the likelihood of not having ACL when the WS print pattern (748/1,190) is detected was 0.629. The odds ratio (OR) for the presence of a definitive diagnosis of ACL versus its absence (1.275/0.629) was 2.028 (95% CI = (1.493; 2.756). Given that the 95% CI of OR does not include a value of 1, futsal athletes with clinical examination findings suggestive of a definitive diagnosis of ACL and that show a WS print pattern are approximately 1.5 to 2.8 times more likely to have ACL injuries than those that do not show a WS print pattern.
4. Discussion
We have divided this section into three subsections: a) diagnosis by dermatoglyphics, career time, and retirement age of the athlete; b) number of lines defined by dermatoglyphics; c) print standards. In all these subsections, we present a concise and precise description of the experimental results found, the interpretations we made on these results, and the experimental conclusions we drew from the results found.
4.1. Diagnosis by Dermatoglyphics, Career Time, and Retirement Age of the Athlete
The clinical diagnoses based on dermatoglyphics may provide a robust tool for prior observation of genetically predisposed diseases. Genetic studies can provide an additional method of prediction and help prevent potential health problems [38,41,46]. Each organism is unique and has an epigenetic trait inherited and generated during fetal development in the womb [47]. The definition of print patterns is closely related to the functioning of the central nervous system. The markers defined at this stage of development can be used as a simple and practical method for the prognosis of health conditions [48]. The markers of biological individuality can enable the discovery of the innate potential of the individual [37]. The combinations of genetic variants and markers of biological individuality identified by dermatoglyphic diagnosis can be used to evaluate the risk of ACL injuries. Our study aimed at identifying dermatoglyphic markers (lines and print patterns) that can be associated with the diagnosis of ACL injuries.
Athletes in most sports have a relatively short duration of career [49]. Career transition refers to the point in time when the athlete prepares to stop training and competing. The end of a sports career has an impact on the personal lifestyle of a former athlete [50]. The former athlete must adapt to new life conditions assuming different roles that are not necessarily related to the activity performed in the past [51]. Depending on the sport that the athlete practices, their athletic career can last between 15 and 25 years [52]. The end of the athlete's career occurs at 35.7 ± 3.83 years on mean [49]. The mean age determined in our study was higher and was 41.1 ± 7.7 years for the group with ACL and 38.0 ± 9.5 years for the group without ACL.
4.2. Number of Lines Defined by Dermatoglyphics
We did not find statistically significant differences between the number of lines in the groups with and without ACL injuries. This finding is comparable to the number of lines found by fingerprints in women with breast cancer [40]. The mean total number of lines (TNL) showed no statistically significant difference (t = 0.515; p = 0.581) between the group with ACL injuries (121.3 ± 35.9 total lines) and the group without ACL injuries (118.6 ± 38.8 total lines). These results are like the dermatoglyphic markers found in male high-level futsal athletes (124.6 ± 40.8 total lines) [53]. The results of our study are like the study that analyzed the number of lines in female high-level futsal athletes (121.7 ± 39.2 total lines) [45]. In these two studies, the mean number of lines was significantly different. However, the authors compared the mean number of lines in high-performance athletes with individuals who play the same sport but are not high-performance athletes.
Another study found a statistically different mean number of lines in the MESQL5 and MDSQL4 fingers [54]. The mean number of lines was higher in the group "high physical fitness level" than in the group "low physical fitness level". In a study that investigated the markers of biological individuality as a mechanism for the prognosis of heart diseases, the authors found that the mean number of lines on the MDSQL5 finger was significantly higher in the group with heart disease than in the control group [55]. In our study, the results showed no statistically significant differences (t = 0.943; p = 0.347) between the mean values of the number of lines in the group with ACL injuries (12.2 ± 4.8 lines) and in the group without ACL injuries (11.9 ± 4.7 lines). The results of our study are like those of a study analyzing the motor ability and speed in children and adolescents [56].
4.3. Print Patterns
We found statistically significant differences between the print patterns in the index finger of the left hand (MED2 | χ² = 9.875; df = 4; p = 0.043) and the little finger of the right hand (MED5 | χ² = 11.978; df: 3; p = 0.007). In both fingers (MED2 and MED5), the group with injuries showed a statistically significant association in the number of spiral whorl (WS) print patterns; in the group without ACL injuries, the whorl (W) print pattern was associated with the finger MED5. Considering the innate characteristics, the identification of fingerprint patterns that differ between the studied groups could be a determining factor for the prognosis of ACL injuries. In our study, regular practice, the number of games played, number of trips undertaken, and disciplined life of the athletes were observed in both groups. This shows that the phenotype behaves similarly in both groups. The identification of some specific markers of the genotype that are significantly different increases the likelihood that a futsal athlete will suffer an ACL injury.
In one study, a statistically significant association of the ulnar loop (LU) print pattern was found in all fingers of both hands in women diagnosed with breast cancer compared to the control group [41]. In our study, this pattern was more prevalent in the group of athletes without ACL injuries. The difference in the results, with one of the studies associating the marker with the group with the condition and our study indicating the absence of the condition, may suggest that there is a condition that we did not analyze and that potentiated the results found. However, it should be noted that the sample of the other study included only women, which could explain the difference in the association found.
The study that investigated the motor ability and speed in children and adolescents found a statistically significant association of the radial loop (LR) print pattern in the fingers of the left hand MED1 and MED5, and in the fingers of the right hand MDD1, MDD3, and MDD5 [56]. In our study, this print pattern showed no correlation between the analyzed groups.
5. Conclusions
The genetic markers presented by the dermatoglyphics can guide talented young futsal athletes and can be used for the prognosis of health conditions in futsal athletes in general. The results obtained in our study using the dermatoglyphic method can contribute to the early detection of ACL injuries. There are significantly different dermatoglyphic markers between the groups with and without ACL injuries. Our results suggest that there are different genetic markers associated with unique types of print patterns and on specific fingers in futsal athletes.
Future studies should be conducted with different ethnic groups. They should analyze different levels of performance, including intersex comparisons, balance or decompensation of anteroposterior and lateral muscle strength, "Q" angle, joint stability, obesity, joint hyperlaxity, dynamic valgus knees, to determine the characteristics by which the analyzed groups differ.
Author Contributions
“Conceptualization, B.H.S. and R.J.N.J.; methodology, B.H.S., R.J.N.J. and A.P.; software, B.H.S., R.J.N.J. and A.P.; validation, B.H.S. and R.J.N.J.; formal analysis, B.H.S., R.J.N.J. and A.P..; investigation, B.H.S.; resources, B.H.S., R.J.N.J. and A.P.; data curation, B.H.S and R.J.N.J. ; writing—original draft preparation, B.H.S.; writing—review and editing, B.H.S., R.J.N.J. and A.P.; visualization, B.H.S. and A.P.; supervision, R.J.N.J. and A.P.; project administration, B.H.S.; funding acquisition, A.P.. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Coordination for the Improvement of Higher Education Personnel - Brazil (CAPES) - Ordinance No. 155 CAPES (financial aid for an Educational and Research Project – AUXPE – Term of Application and Concession of Financial Support for a Project).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee the University of Passo Fundo, Brazil (protocol code 4.870.728, date of approval in 28 July 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The dataset analyzed or generated during the study can be accessed at https://sites.google.com/upf.br/data-for-marks-of-biological.
Acknowledgments
To the team at SALUS Dermatoglifia, Brazil, for supporting the development of the survey, but special thanks to Alexandre Heberle for organizing the data, and to Josiane A. de Jesus for supporting the generation of statistical results. To Daniele Ottoni, Guilherme Zanatta, Leonardo U. Nunes, Anderson S. da Rosa and Rodrigo V. Valiatti, who helped in scheduling, collecting, and organizing data with former futsal athletes. To the professors of the Physical Education and Physiotherapy Course at the University of Passo Fundo, Brazil, for their support for the development of the research.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Appendix A
Formulas
- Sensitivity (rate of true positives) = a/(a+c)
- Specificity (rate of true negatives) = d/(b+d)
- Accuracy = (a+d)/(a+b+c+d)
- Positive predictive value = a/(a+b)
- Negative predictive value = d/(c+d) fic
Appendix B
References
- Silvera, J.J.p. Loco Abreu: a autoconstrução de uma idolatria. Espo e Soc 2017, 30, 1–17. [Google Scholar]
- FIFA Futsal LOTG 2010/2011, Available from: http://www.fifa.com/mm/document/affederation/generic/51/44/50/spielregelnfutsal_2010_11_e.pdf, 2016.
- Moore, R.; Bullough, S.; Goldsmith, S.; Edmondson, L. A Systematic Review of Futsal Literature. Amer J. of Spor Scie and Med 2014, 3, 108–116. [Google Scholar] [CrossRef]
- Soares, B.; Nodari Junior, R.J.; Pasqualotti, A. Participação genética na lesão do ligamento cruzado anterior: revisão sistemática. In. Tópicos em Ciências da Saúde, 1ª ed.; Barros, R.N., Alves, G.S.B., Oliveira, E., Eds.; Editora: Paisson, Belo Horizonte, Brasil, 2022; Volume 28, pp. 98–107. [Google Scholar] [CrossRef]
- Kharisma, Y.; Mubarok, M.Z. Analisis Tingkat Daya Tahan Aerobik Pada Atlet Futsal Putri AFKAB Indramayu. Physical Activity Journal (PAJU), 2020, 2, 125–132. [Google Scholar] [CrossRef]
- Roxburgh, A. The technician futsal. Newsletter for coaches UEFA, 2008, Supplement 4, p. 1-12. Disponível online: https://www.uefa.com/newsfiles/649735.pdf (acessado em 23 de Novembro de 2022).
- Soares, B.H.; Pasqualotti, A.; Rocha, C.L.S.D.; Alberti, A.; Gomes, S.A. O impacto da pandemia covid-19 no futsal gaúcho. Rev Bras de Fut e Fut 2022, 54, 477–485. [Google Scholar]
- Kunze, A.; Schlosser, M. W.; Brancher, E.A. Análise das técnicas de goleiro mais utilizadas durante os jogos de Futsal masculino. Rev Bras de Fut e Fut 2016, 30, 228–234. [Google Scholar]
- Pestana, E.R.; Navarro, A.C.; Santos, Í.J.L.M.; Cunha, M.L.A.; Araújo, M.L.; Gomes de Carvalho, W.R. Análise dos gols e tendência com a equipe campeã em um campeonato de Futsal regional do Brasil. Rev Bras de Fut e Fut 2017, 34, 327–332. [Google Scholar]
- FIFA. Laws of the Game. Zurich: Fédération Internationale de Football Association (FIFA). 2020.
- Herman, I.; Hasan, M.F.; Hidayat, I.K.; Apriantono, T. Analysis of Speed and Acceleration on 60-Meters Running Test Between Women Soccer and Futsal Players. Advances in Health Sciences Research. International Conference on Sport Science, Health, and Physical Education 2019, 4, 345–347. [Google Scholar] [CrossRef]
- Mazurek, K. L.; Zmijewski, p.; Makaruk, H.; Mróz, A.; Lipnska, p. Effects of Short-Term Plyometric Training on Physical Performance in Male Handball Players. J. of Hum Kinet 2018, 63, 137–148. [Google Scholar] [CrossRef]
- Baldaço, F.; Cadó, V.; Souza, J.; Mota, C.; Lemos, J. Análise do treinamento proprioceptivo no equilíbrio de atletas de futsal feminino. Rev Fisio em Mov 2010, 2, 183–192. [Google Scholar] [CrossRef]
- Brunoro, J.C. Futebol 100% profissional, 15ª ed.; Editora Gente, Brasil - São Paulo, 2017. pp. 251.
- Fin, W.; Soares, B; Bona, C. C.; Vilasboas, R.; Matzenbacher, F. Potencia aeróbia em atletas de futsal de diferentes níveis competitivos. Rev Bras de Fut e Fut 2020, 49, 339–345. [Google Scholar]
- Pfirmann, D.; Herbst, M.; Ingelfinger, p.; Simon, p.; Tug, S. Analysis of injuries incidences in male professional adult and elite youth soccer players: a systematic review. J. of Athlet Train 2016, 5, 410–424. [Google Scholar] [CrossRef]
- Nunes Neto, J.S.; Andrade, C.; Girão, p.I.F.; Guimarães, D.F.; Bezerra, A.K.T.G.; Girão, M.V.D. Análises das faltas e lesões desportivas em atletas de futebol por meio de recursos audiovisuais de domínio público. Rev Bras de Fut e Fut 2020, 47, 31–38. [Google Scholar]
- Kraus, T.; Švehlík, M.; Singer, G.; Schalamon, J.; Zwick, E.; Linhart, W. The epidemiology of knee injuries in children and adolescents. Arch of Orthop and Trauma Sur 2012, 132, 773–779. [Google Scholar] [CrossRef]
- Rothenberg, p.; Grau, L.; Kaplan, L.; Baraga, M.G. Knee Injuries in American Football: An Epidemiological Review. Amer J. of Orthop 2016, 45, 368–373. [Google Scholar]
- Almeida, A.K.; De La Rosa Santana, J.D.; Santiesteban, L.L.E.; Peña, A.M.F.; Labrada, G.D. La articulación de la rodilla: lesión del ligamento cruzado anterior. Rev Cient 2 Dic 2020, 1, 1–6. [Google Scholar]
- Astur, D.C.; Batista, R.F.; Gustavo, A.; Cohen, M. Trends in treatment of anterior cruciate ligament injuries of the knee in the public and private health care systems of Brazil. São Paulo Med J 2013, 4, 257–263. [Google Scholar] [CrossRef]
- Brito, D.C.O.; Ordóñez, S.F.R.; Brito, p.R.F. Tratamiento funcional de la lesión de ligamento cruzado anterior de la rodilla: una revisión. La Cie al Serv de la Salud 2019, 2, 51–59. [Google Scholar] [CrossRef]
- Hewett, T.E.; Myer, G.D.; Ford, K.R.; Paterno, M.V; Quatman, C.E. Mechanisms, prediction, and prevention of ACL injuries: Cut risk with three sharpened and validated tools. J Orthop Res 2016, 11, 1843–1855. [Google Scholar] [CrossRef] [PubMed]
- Nessler, T.; Denney, L.; Y Sampley, J. ACL injuries prevention: what does research tell us? Curr Rev Musculoskelet Med. 2017, 3, 281–288. [Google Scholar] [CrossRef]
- Sutton, K.M.; Bullock, J.M. Anterior Cruciate Ligament Rupture: Differences between Males and Females. J. of the Amer Acade of Orthop Surg 2013, 1, 41–50. [Google Scholar] [CrossRef]
- Benis, R.; La Torre, A.; Bonato, M. Anterior cruciate ligament injuries profile in female elite Italian basketball league. The Amer Jour of Spo Med 2018, 3, 280–286. [Google Scholar] [CrossRef]
- Sanders, T.L.; Maradit Kremers, H.; Bryan, A.J. , Larson, D.R.; Dahm, D.L., Levy, B.A., Stuart, M.J., Eds.; Krych, A.J. Incidence of Anterior Cruciate Ligament Tears and Reconstruction: A 21-Year Population-Based Study. Am J Sports Med 2016, Volume 44, Number 06, p.1502-1507. [Google Scholar] [CrossRef]
- Von Rosen, p.; Kottorp, A.; Fridén, C.; Frohm, A.; Heijne,A. Young, talented and injured: Injuries perceptions, experiences and consequences in adolescent elite athletes. Euro J. of sport scien 2018, 5, 731–740. [Google Scholar] [CrossRef] [PubMed]
- Astur, D.C.; Xerez, M.; Rozas, J.; Vargas Debieux, p.; Franciozi, C.; Cohen, M. Anterior cruciate ligament and meniscus injuries in sports: incidence, time of practice until injuries, and limitations caused after trauma. Rev Bras de Ortop 2016, 51, 652–656. [Google Scholar] [CrossRef]
- Araújo, G.C.; Abreu, M.B.; Sandes, M.T.S.; Borges, M.R.; Silva, M.M. The effectiveness of electrochemistry in Acute treatment in football players. Rev de Ciên Hum, 2018, 2, 47–53. [Google Scholar]
- Meurer, M.C.; Silva, M.F.; Baroni, B.M. Strategies for injuries prevention in Brazilian football: Perceptions of physiotherapists and practices of premier league teams. Phys Ther Sport 2017, 28, 1–8. [Google Scholar] [CrossRef]
- Lohmander, L.S.; Englund, p.M.; Dahl, L.L.; Roos, E.M. The longterm consequence of anterior cruciate ligament and meniscus injuries: Osteoarthritis. Amer J. of Spo Medi. 2007, 10, 1756–1769. [Google Scholar] [CrossRef]
- Soares, B.; Vicensi, D.J.; Alves, M.A.R.; Ballesteros, M.A.M.; Gomes, S.A.; Ferreira, C.E.S.; Nodari Junior, R.J.; PaqualottI, A.; Voser, R.C. Análise da velocidade da bola no chute de jogadores de futsal em função do contato do peito do pé dos membros inferiores. Research, Soc and Dev 2022, 9, 1–8. [Google Scholar] [CrossRef]
- Cummins, H.; Midlo, C.H. Fingerprints, palms, and soles an introduction to dermatoglyphics. New York: Dover Publications; 1961. pp.333.
- Abramova, T.F.; Nikitina, T.M.; Izaak, S.I.; Kochetkova, N.I. Asimmetriia priznakov pal'tsevoĭ dermatoglifiki, fizicheskiĭ potentsial i fizicheskie kachestva cheloveka [Asymmetry of signs of finger dermatoglyphics, physical potential and physical qualities of a man]. Morfologiia. 2000, 5, 56–59. [Google Scholar]
- Barnes, J.G. The Fingerprint. U. S. Department of Justice Office of Justice Programs. National Institute of Justice; 2002.
- Nodari Junior, R.J. Heberle, A.; Ferreira-Emygdio, R.; Irany-Knackfuss, M. Impressões digitais para diagnóstico em saúde: validação de protótipo de escaneamento informatizado. Rev de Salud Púb 2008, 5, 767–776. [Google Scholar]
- Nodari Junior, R.J.; Fin, G. Dermatoglifia: impressões digitais como marca genética e de desenvolvimento fetal; Ed. Unoesc: Joaçaba, Brasil, 2016. [Google Scholar]
- Wertheim, K. The Fingerprint. U. S. Department of Justice Office of Justice Programs. National Institute of Justice, 2002.
- Baretta, E.; Sartori, G.; Fin, G.; Nodari Junior, R.J. Marcas Dermatoglíficas em mulheres com câncer de mama. Congresso Internacional De Atividade Física, Nutrição E Saúde, Volume 1. Recuperado de https://eventos.set.edu.br/CIAFIS/article/view/2856. 2016.
- Fin, G.; Jesus, J. A.; Benetti, M.; Nodari Júnior, R.J. La práctica de actividad física en mujeres con cáncer de mama: asociación entre factores motivacionales y características dermatoglíficas. Cuad de Psico del Dep 2022, 1, 176–189. [Google Scholar] [CrossRef]
- Silva, I.; Vianna, M.V.A.; Gomes, A.L.M.; Dantas, E.H.M. Diagnóstico do potencial genético físico e somatotipia de uma equipe de futebol profissional Fluminense. Rev Bras de Fut 2008, 1, 49–58. [Google Scholar]
- Dias, R.M.; Corrêa, D.A. Aspectos importantes no processo detecção e orientação de talentos esportivos e a contribuição da estatística Z neste contexto. Conexões 2015, 2, 166–184. [Google Scholar] [CrossRef]
- Nodari Junior, R.J. Heberle, A.; Ferreira-Emygdio, R.; Irany-Knackfuss, M. Dermatoglyphics: Correlation between software and traditional method in kineanthropometric application. Rev Andal Med Deporte 2014, 2, 60–65. [Google Scholar] [CrossRef]
- Alberti, A.; Fin, G.; Gomes de Souza, R.; Soares, B.; Nodari Junior, R.J. Dermatoglifia: as impressões digitais como marca característica dos atletas de futsal feminino de alto rendimento do Brasil. Rev Bras de Fut e Fute 2018, 37, 193–201. [Google Scholar]
- Kahn, H.S. , Graff, M., Stein, A. D., Lumey, L.H. A fingerprint marker from early gestation associated with diabetes in middle age: the Dutch Hunger Winter Families Study. Internat J. Epidem 2009, 1, 101–109. [Google Scholar] [CrossRef]
- Yohannes, S. Dermatoglyphic meta-analysis indicates early epigenetic outcomes & possible implications on genomic zygosity in type-2 diabetes. F1000Research 2015, 5, 1–5. [Google Scholar] [CrossRef]
- King, S.; Mancini-Marïe, A.; Brunet, A.; Walker, E.; Meaney, M.J.; Laplante, D.P. Prenatal maternal stress from a natural disaster predicts dermatoglyphic asymmetry in humans. Dev Psychopathol 2009, 2, 343–53. [Google Scholar] [CrossRef]
- Agresta, M.C.; Brandão, M.R.F.; Barros Neto, T.L. Impacto do término de carreira esportiva na situação econômica e profissional de jogadores de futebol profissional. R. Bras. C. e Mov 2008, 1, 29–38. [Google Scholar] [CrossRef]
- Rocha, H.p.A.D.; Miranda, I.S.; Silva, A.L.C.; Cos, F.R. A dupla carreira esportiva no Brasil: Um panorama na agenda das políticas públicas. Rev Com Censo 2020, 2, 52–59. [Google Scholar] [CrossRef]
- Mello, G.F.; Rubio, K. Mulheres atletas olímpicas brasileiras: início e final de carreira por modalidade esportiva. R. bras. Ci. e Mov 2017, 4, 104–116. [Google Scholar] [CrossRef]
- Wylleman, p.; Rosier, N. Holistic Perspective on the Development of Elite Athletes. In Sport and Exercise Psychology Research: From Theory to Practice, 1ª ed.; In: Raab, M., Seiler, R., Hatzigeorgiadis, A., Wylleman, p., Eds.; Elbe, A.M. Elsevier: Amsterdã, Holanda, 2016; Volume 1, pp. 269–288. [Google Scholar] [CrossRef]
- Nodari Junior, R.J.; Alberti, A.; Gomes de Souza, R.; Pinheiro, C.J. B.; Martinelli Comim, C.; Fin, G.; Dantas, E.H.M.; Soares, B.H. , Souza, R. Características dermatoglíficas de jogadores de futsal de alto desempenho. Rev Bras De Fut e Fut 2022, 57, 130–136. [Google Scholar]
- Baretta, E.; Pizzi, S.; Fin, G.; Fiedler, M.M.; Nodari Junior, R.J. Impressões digitais como marcadores genéticos de aptidão cardiorrespiratória. In: Anais do XXI Seminário de Iniciação Científica. E, VIII Seminário Integrado de Ensino, Pesquisa e Extensão. E, VI Mostra universitária, 2015, Videira. Pesquisa e Inovação: inserção social e científica na comunidade regional. Joaçaba: Unoesc, 2015, Volume 1, pp. 297-297.
- Stefanes, V.S.; Nodari Junior, R.J. impressão digital como marca Genética no prognóstico de Cardiopatias. Unoesc & Ciência 2015, 2, 203–208. [Google Scholar]
- Jesus, J.A.J; Zanoni, E.M.; Silva, H.L.; Baretta, E.; Souza, R.; Alberti, A.; Fin, G.; Nodari Júnior, R.J. Dermatoglyphics and its relationship with the speed motor capacity in children and adolescentes. Internat J. of Devel Research 2019, 3, 26430–26434. [Google Scholar]
- The jamovi project (2024). jamovi. (Version 2.6) [Computer Software]. Retrieved from https://www.jamovi.org.
- R Core Team (2024). R: A Language and environment for statistical computing. (Version 4.4) [Computer software]. Retrieved from https://cran.r-project.org. (R packages retrieved from CRAN snapshot 2024-08-07).
Figure 1.
Demonstration of fingerprint collection, finger coding, marking of the points, and counting of the number of lines on the fingers.
Figure 1.
Demonstration of fingerprint collection, finger coding, marking of the points, and counting of the number of lines on the fingers.
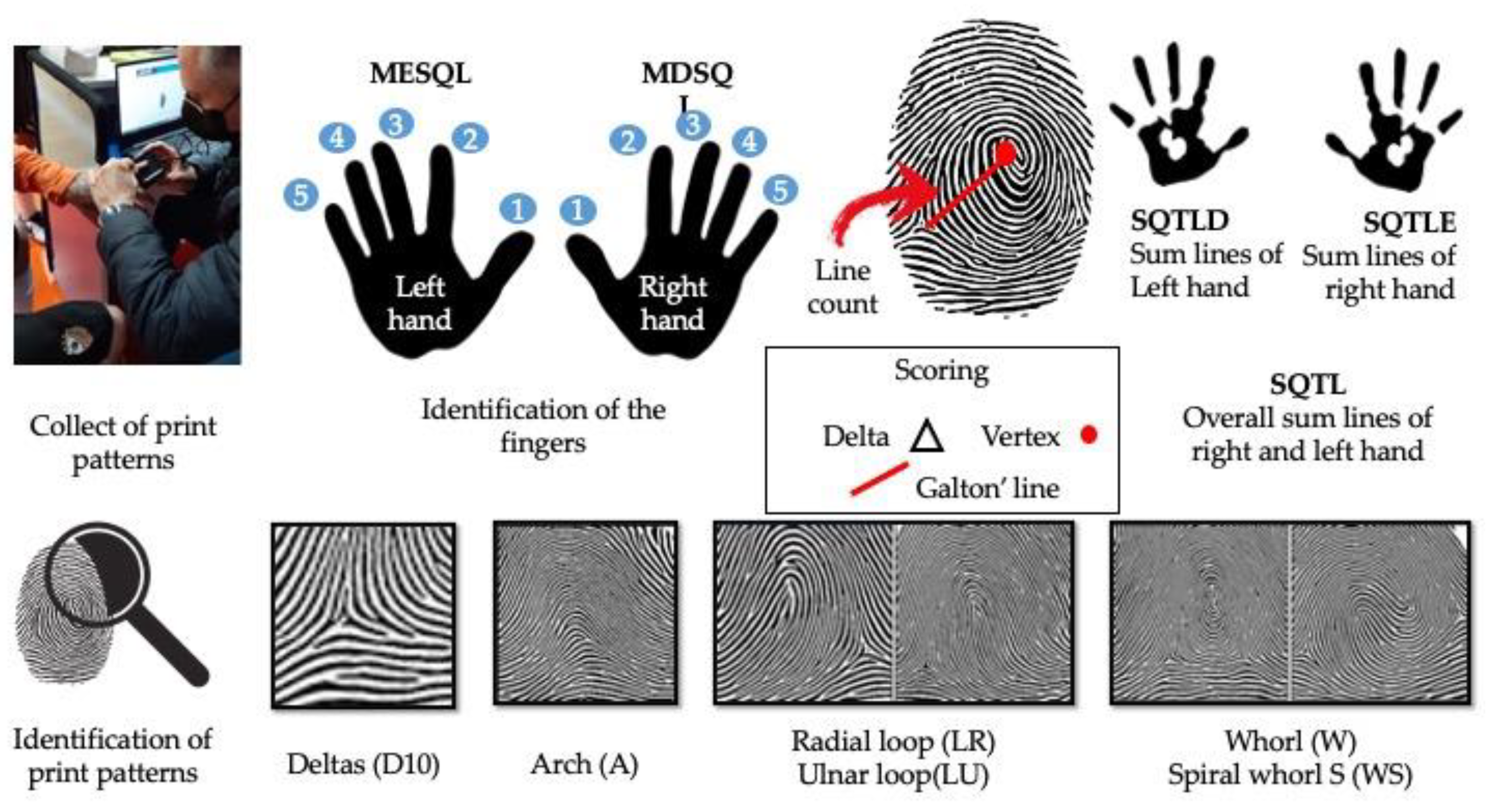
Figure 2.
Athletes with and without ACL. Student's t test; statistically significant difference for p < 0.05. (a) Density of age distribution. (b) Distribution of ages by group. (c) Mean and standard error of ages. (d)Mean, median, and 95% CI of ages.
Figure 2.
Athletes with and without ACL. Student's t test; statistically significant difference for p < 0.05. (a) Density of age distribution. (b) Distribution of ages by group. (c) Mean and standard error of ages. (d)Mean, median, and 95% CI of ages.
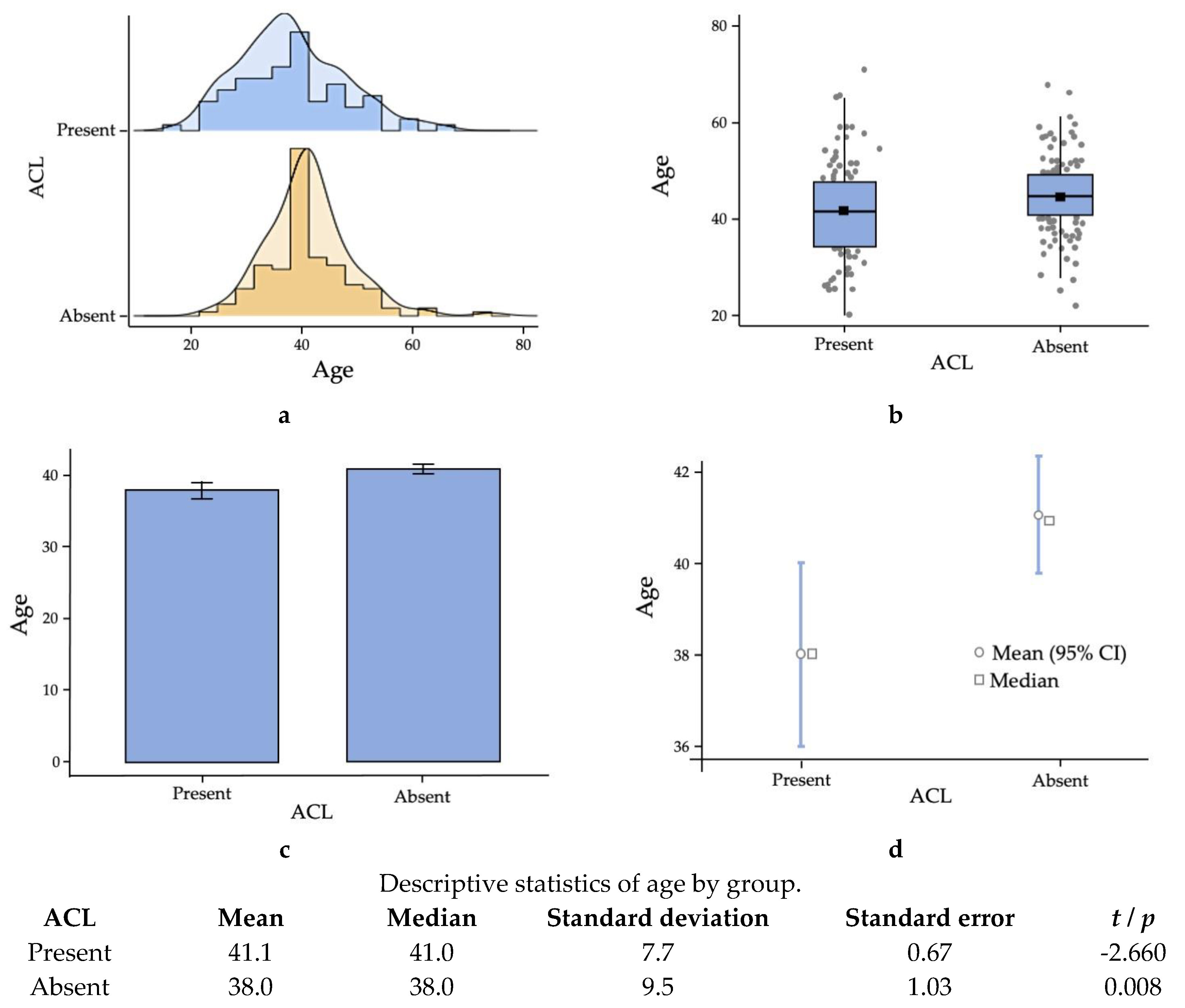
Figure 3.
Estimated marginal means of presence and absence of ACL injuries versus print patterns. Modeling of the categorical variables: presence and absence of ACL injuries and print patterns; log-linear regression; statistically significant difference for p < 0.05.
Figure 3.
Estimated marginal means of presence and absence of ACL injuries versus print patterns. Modeling of the categorical variables: presence and absence of ACL injuries and print patterns; log-linear regression; statistically significant difference for p < 0.05.

Figure 4.
Cut-Off Plot.
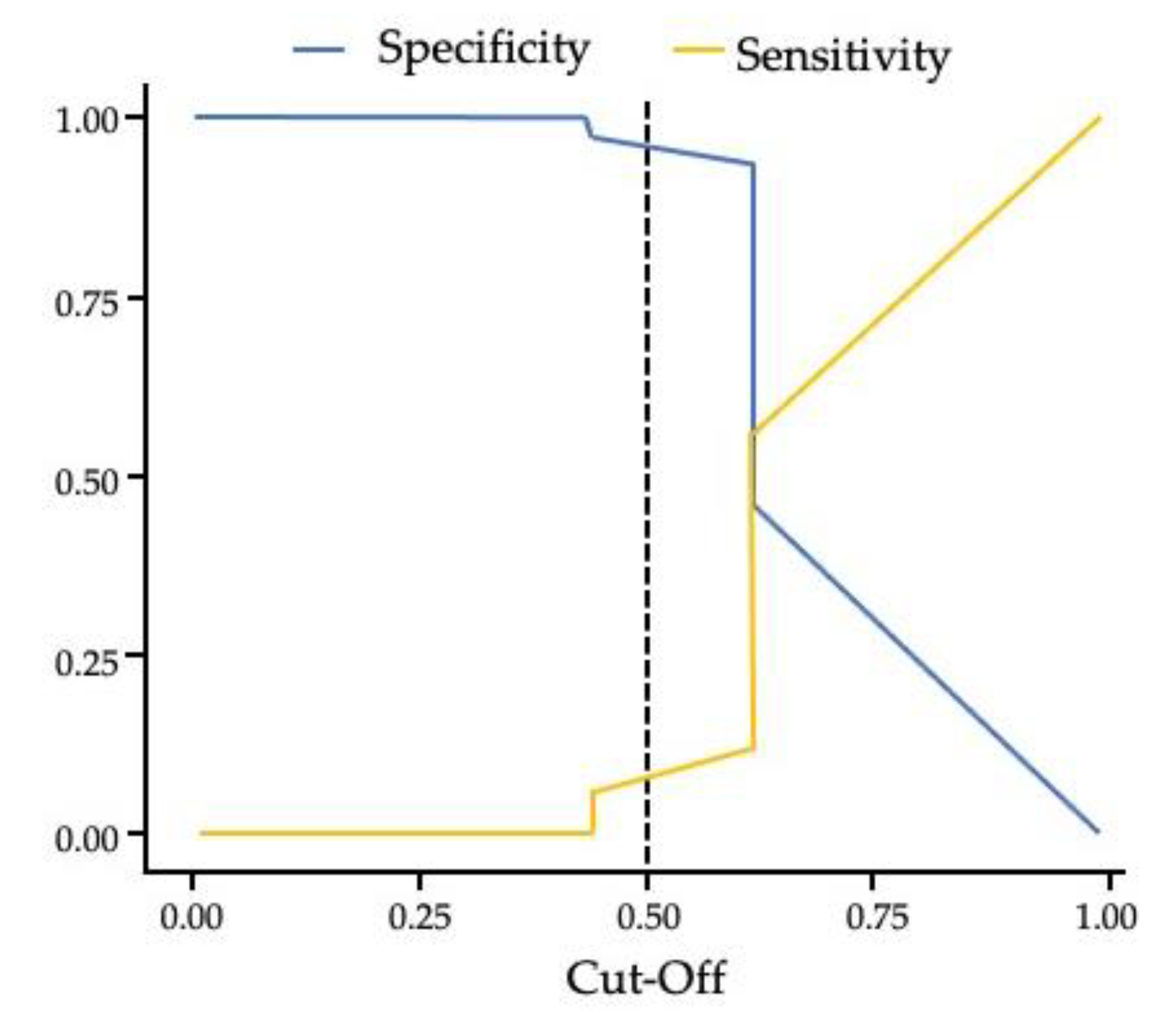

Table 1.
Omnibus likelihood ratio test.
| Predictor | χ² | df | p |
|---|---|---|---|
| ACL | 1.605 | 1 | 0.205 |
| Hands | 0.050 | 1 | 0.823 |
| Print patterns | 606.254 | 4 | < 0.001 |
| ACL ✻ Hands | 0.028 | 1 | 0.867 |
| Print patterns ✻ ACL | 18.188 | 4 | 0.001 |
| Hands ✻ Print patterns | 1.836 | 4 | 0.766 |
| ACL ✻ Hands ✻ Print patterns | 6.221 | 4 | 0.183 |
Modeling of the categorical variables: presence and absence of ACL injuries, print patterns and hands; log-linear regression; statistically significant difference for p < 0.05.
Table 2.
Coefficients of the Log-linear regression model.
| Predictor | Estimates | SE | Z | p |
|---|---|---|---|---|
| Intercept | 3.664 | 0.160 | 22.879 | < 0.001 |
| ACL: | ||||
| Present – Absent | 0.268 | 0.213 | 1.261 | 0.207 |
| Hands: | ||||
| Right hand – Left hand | 0.050 | 0.224 | 0.224 | 0.823 |
| Print patterns: | ||||
| A – WS | -0.445 | 0.256 | -1.736 | 0.083 |
| LR – WS | 0.187 | 0.217 | 0.861 | 0.389 |
| LU – WS | 2.282 | 0.168 | 13.574 | < 0.001 |
| W – WS | 1.292 | 0.181 | 7.148 | < 0.001 |
| ACL ✻ Hands: | ||||
| (Present – Absent) ✻ (Right hand – Left hand) | -0.050 | 0.299 | -0.167 | 0.867 |
| Print patterns ✻ ACL: | ||||
| (A – WS) ✻ (Present – Absent) | -1.408 | 0.459 | -3.070 | 0.002 |
| (LR – WS) ✻ (Present – Absent) | -1.228 | 0.349 | -3.515 | < 0.001 |
| (LU – WS) ✻ (Present – Absent) | -0.665 | 0.228 | -2.921 | 0.003 |
| (W – WS) ✻ (Present – Absent) | -0.713 | 0.252 | -2.835 | 0.005 |
| Hands ✻ Print patterns: | ||||
| (Right hand – Left hand) ✻ (A – WS) | -0.091 | 0.363 | -0.250 | 0.802 |
| (Right hand – Left hand) ✻ (LR – WS) | 0.070 | 0.300 | 0.234 | 0.815 |
| (Right hand – Left hand) ✻ (LU – WS) | -0.109 | 0.235 | -0.464 | 0.642 |
| (Right hand – Left hand) ✻ (W – WS) | 0.050 | 0.252 | 0.200 | 0.841 |
| ACL ✻ Hands ✻ Print patterns: | ||||
| (Present – Absent) ✻ (Right hand – Left hand) ✻ (A – WS) | 0.091 | 0.649 | 0.140 | 0.889 |
| (Present – Absent) ✻ (Right hand – Left hand) ✻ (LR – WS) | 0.777 | 0.457 | 1.701 | 0.089 |
| (Present – Absent) ✻ (Right hand – Left hand) ✻ (LU – WS) | -0.083 | 0.321 | -0.259 | 0.796 |
| (Present – Absent) ✻ (Right hand – Left hand) ✻ (W – WS) | 0.157 | 0.350 | 0.449 | 0.653 |
Modeling of the categorical variables: ACL, print patterns and hands; arch: A, radial loop: LR, ulnar loop: LU, whorl: W, spiral whorl: WS; Log-linear regression; statistically significant difference for p < 0.05.
Table 3.
Mean number of lines per finger and hand for the presence and absence of anterior cruciate ligament injuries.
Table 3.
Mean number of lines per finger and hand for the presence and absence of anterior cruciate ligament injuries.
| Number of lines | ACL | Mean | Standard deviation | Standard error | t /p |
|---|---|---|---|---|---|
| MESQL1 | Present | 13.9 | 5.5 | 0.6 | -0.914 |
| Absent | 14.6 | 5.1 | 0.46 | 0.362 | |
| MESQL2 | Present | 9.1 | 5.1 | 0.55 | 0.094 |
| Absent | 9.1 | 5.5 | 0.49 | 0.925 | |
| MESQL3* | Present | 10.9 | 4.5 | 0.49 | 0.519 |
| Absent | 10.5 | 5.5 | 0.49 | 0.604 | |
| MESQL4 | Present | 13.3 | 4.6 | 0.5 | 0.516 |
| Absent | 12.9 | 5.5 | 0.49 | 0.607 | |
| MESQL5 | Present | 12.3 | 4.5 | 0.49 | 1.650 |
| Absent | 11.3 | 4.7 | 0.42 | 0.101 | |
| MDSQL1 | Present | 15.9 | 5.2 | 0.56 | 0.442 |
| Absent | 16.4 | 4.5 | 0.40 | 0.659 | |
| MDSQL2 | Present | 9.9 | 5.4 | 0.59 | -0.796 |
| Absent | 8.9 | 5.9 | 0.52 | 0.427 | |
| MDSQL3 | Present | 10.7 | 4.6 | 0.49 | 1.161 |
| Absent | 10.5 | 5.0 | 0.45 | 0.247 | |
| MDSQL4* | Present | 13.2 | 4.6 | 0.50 | 0.199 |
| Absent | 12.5 | 5.5 | 0.49 | 0.843 | |
| MDSQL5 | Present | 12.2 | 4.8 | 0.52 | 0.943 |
| Absent | 11.9 | 4.7 | 0.42 | 0.347 | |
| SQTLE | Present | 59.5 | 18.5 | 2.00 | 0.455 |
| Absent | 58.3 | 20.1 | 1.79 | 0.650 | |
| SQTLD | Present | 61.8 | 18.9 | 2.05 | 0.553 |
| Absent | 60.3 | 19.9 | 1.77 | 0.581 | |
| SQTL | Present | 121.3 | 35.9 | 3.90 | 0.515 |
| Absent | 118.6 | 38.8 | 3.45 | 0.607 | |
| D10 | Present | 13.4 | 3.2 | 0.35 | 1.694 |
| Absent | 12.6 | 3.5 | 0.31 | 0.092 |
Student's t-test; statistically significant difference for p < 0.05. ᵃ Levene's test is significant (p < 0.05) indicating a violation of the assumption of homogeneity of variances.
Table 4.
Association between the print patterns per hand for the presence and absence of anterior cruciate ligament injuries.
Table 4.
Association between the print patterns per hand for the presence and absence of anterior cruciate ligament injuries.
| Hands | ACL | Print patterns | χ² | p | ||||
|---|---|---|---|---|---|---|---|
| A | LR | LU | W | WS | |||
| Left hand | Present | 8 (24.2 %) | 18 (27.7 %) | 257 (40.2 %) | 91 (39.1 %) | 51 (56.7 %) | 15.072 0.005 |
| Absent | 25 (75.8 %) | 47 (72.3 %) | 382 (59.8 %) | 142 (60.9 %) | 39 (43.3 %) | ||
| Right hand | Present | 8 (25.0 %) | 42 (44.2 %) | 212 (37.1 %) | 112 (41.6 %) | 51 (55.4 %) | 18.015 0.001 |
| Absent | 24 (75.0 %) | 53 (55.8 %) | 360 (62.9 %) | 157 (58.4 %) | 41 (44.6 %) | ||
| Overall | Present | 16 (24.6 %) | 60 (37.5 %) | 469 (38.8 %) | 203 (40.4 %) | 102 (56.0 %) | 27.125 < 0.001 |
| Absent | 49 (75.4 %) | 100 (62.5 %) | 742 (61.2 %) | 299 (59.6 %) | 80 (44.0 %) | ||
arch: A, radial loop: LR, ulnar loop: LU, whorl: W, spiral whorl: WS; Chi-square test; statistically significant difference for p < 0.05.
Table 5.
Association between the print patterns per finger for the presence and absence of anterior cruciate ligament injuries.
Table 5.
Association between the print patterns per finger for the presence and absence of anterior cruciate ligament injuries.
| Finger coding | ACL | Print patterns | p | ||||
| A | LR | LU | W | WS | |||
| MED1 | Present | 2 (33.3%) | 3 (42.9%) | 40 (38.1%) | 18 (35.3%) | 22 (51.2%) | 0.559 |
| Absent | 4 (66.7%) | 4 (57.1%) | 65 (61.9%) | 33 (64.7%) | 21 (48.8%) | ||
| MED2 | Present | 4 (30.8%) | 11 (26.8%) | 33 (41.3%) | 24 (40.7%) | 13 (68.4%) | 0.043 |
| Absent | 4 (66.7%) | 4 (57.1%) | 65 (61.9%) | 33 (64.7%) | 21 (48.8%) | ||
| MED3 | Present | 2 (22.2%) | 1 (9.1%) | 63 41.7%) | 14 (43.8%) | 5 (55.6%) | 0.145 |
| Absent | 7 (77.8%) | 10 (90.9%) | 88 (58.3%) | 18 (56.3%) | 4 (44.4%) | ||
| MED2 | Present | 0 (0.0%) | 1 (50.0%) | 49 (38.9%) | 28 (40.6%) | 7 (63.6%) | 0.250 |
| Absent | 4 (100.0%) | 1 (50.0%) | 77 (61.1%) | 41 (59.4%) | 4 (36.4%) | ||
| MED5 | Present | 0 (0.0%) | 2 (50.0%) | 72 (40.7%) | 7 (31.6%) | 4 (50.0%) | 0.770 |
| Absent | 1 (100.0%) | 2 (50.0%) | 105 (59.3%) | 15 (68.2%) | 4 (50.0%) | ||
| MDD1 | Present | 2 (66.7%) | 2 (66.7%) | 31 (32.3%) | 30 (43.5%) | 20 (48.8%) | 0.213 |
| Absent | 1 (33.3%) | 1 (33.3%) | 65 (66.7%) | 39 (56.5%) | 21 (51.2%) | ||
| MDD2 | Present | 2 (13.3%) | 27 (45.0%) | 23 (32.9%) | 23 (46.9%) | 10 (55.6%) | 0.053 |
| Absent | 13 (86.7%) | 33 (55.0%) | 47 (67.1%) | 26 (53.1%) | 8 (44.4%) | ||
| MDD3 | Present | 3 (30.0%) | 4 (33.3%) | 60 (39.2%) | 12 (41.4%) | 6 (75.0%) | 0.311 |
| Absent | 7 (70.0%) | 8 (66.7%) | 93 (60.8%) | 17 (58.6%) | 2 (25.0%) | ||
| MDD4 | Present | 1 (25.0%) | 4 (40.0%) | 33 (31.1%) | 40 (44.9%) | 7 (46.9%) | 0.646 |
| Absent | 3 (71.0%) | 6 (60.0%) | 61 (64.9%) | 49 (55.1%) | 8 (53.3%) | ||
| MDD5 | Present | 0 (0.0%) | 5 (50.0%) | 65 (40.9%) | 7 (21.2%) | 8 (80.0%) | 0.007 |
| Absent | 0 (0.0%) | 5 (50.0%) | 94 (59.1%) | 26 (78.8%) | 2 (20.0%) | ||
arch: A, radial loop: LR, ulnar loop: LU, whorl: W, spiral whorl: WS; Chi-square test; statistically significant difference for p < 0.05. *There are no records of arch pattern on this finger (df = 3).
Table 6.
Association between the spiral whorl (WS) print pattern and the final diagnosis for the presence and absence of anterior cruciate ligament injuries.
Table 6.
Association between the spiral whorl (WS) print pattern and the final diagnosis for the presence and absence of anterior cruciate ligament injuries.
| WS print pattern | Definitive diagnosis of ACL | Total | |
|---|---|---|---|
| Present | Absent | ||
| Present | 102 | 80 | 182 |
| Absent* | 748 | 1.190 | 1.938 |
| Total | 850 | 1.270 | 2.120 |
* Other patterns (A, LR, LU, W).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



