Submitted:
18 August 2025
Posted:
20 August 2025
You are already at the latest version
Abstract
Invasive lobular carcinoma (ILC) is the most common special type of breast carcinoma, accounting for 5-15% of all breast carcinoma cases. It exhibits several unique features in morphology, clinical behavior, radiological features, molecular characteristics, and metastatic pattern. The latter differs from that of invasive breast carcinoma of no special type with ILC metastases to the peritoneum, gastrointestinal tract, and female genital tract being more frequent. We herewith review the demographic, clinicopathological, and therapeutic aspects of ILC metastases to the female genital tract and discuss separately the differential diagnosis and prognosis for each anatomic location of the female genital tract.
Keywords:
breast carcinoma
; invasive lobular carcinoma
; female genital tract
; metastasis
; diagnosis
1. Introduction
Invasive lobular carcinoma (ILC) is the commonest special subtype of invasive breast carcinoma, accounting for 5-15% of breast carcinomas [1], thus being second in frequency only to invasive breast carcinoma of no special type (IBCNST) [2]. It was first described by Foote and Stewart in 1941 [2]. Its morphological, immunohistochemical, clinical, radiological, and molecular characteristics differ from those of IBCNST. It may remain undetectable or present as a palpable tumor [3]. In imaging studies, it may be detected with difficulty and tumor size may occasionally be underestimated, resulting in positive surgical margins [4]. The metastatic pattern also differs from that of IBC NST, with ILC metastases to the peritoneum, gastrointestinal tract, and female genital tract (FGT) being more frequent [5,6,7,8]. ILC lacks E-cadherin immunopositivity and displays an aberrant β-catenin immunostaining [9]. Its molecular profile is characterized by deleterious mutations in CDH1 paired with allelic loss of the remaining allele [4].
Histologically, ILC is characterized by small cells with a discohesive growth pattern forming single-cell files, and a minimal stromal response. Signet-ring-like cells may sometimes be found [4]. Apart from the classic variant, several histological variants have been described, including alveolar [10], tubulolobular [11], solid [12], trabecular [10], signet-ring [13], pleomorphic [14], and mixed [15]. Another three rare variants (ILC with extracellular mucin production, ILC with papillary features, and ILC with tubular elements) have recently been described [3].
ILC treatment usually includes hormonal therapy, since it is commonly positive for estrogen (ER) and progesterone receptors (PR) [3]. It displays a poor response to neoadjuvant chemotherapy when compared to IBCNST [3].
We herewith review case reports and case series describing ILC metastases to the FGT.
2. Materials and Methods
2.1. Search Strategy
A literature review was conducted using PubMed, Scopus, and Web of Science to identify all published cases in the English language of ILC metastasis to the FGT. The research utilized the following terms: “lobular carcinoma” AND “metastasis” AND “female genital tract OR ovary OR ovarian OR vulva OR vagina OR endometrium OR endometrial OR uterus OR uterine."We did not set any additional limitations while performing the search.
2.2. Inclusion and Exclusion Criteria
Two authors [MGS, KS] performed the literature review and collected data. Discrepancies were corrected in consensus. In cases where consensus could not be reached, the principal investigator (NK) resolved the discrepancy.
The timeline for the selected studies ranged from October 1993 to April 2024.
Both single case reports as well as case series (studies reporting at least two cases) on ILC metastasis to the FGT were included in the review. At the same time, we excluded narrative or systematic reviews, meta-analyses, opinion pieces, and other articles that did not present original research findings.
Papers available only as abstracts or those with text appearing too brief or noninformative were excluded from the present review.
The clinicopathological and treatment parameters analyzed included age (median and range), clinical presentation, primary tumor size, ER, PR, and HER-2 status both in primary focus and in the metastasis, tumor stage, location of metastatic involvement, metastases in organs or locations other than the FGT, surgical and neoadjuvant or adjuvant treatment, time interval to metastasis, median follow-up, outcome, and tumor grade (Tables 2–4).
In addition, cases with insufficient or too much aggregated data, as well as manuscripts in languages other than English, were excluded.
After applying inclusion and exclusion criteria, 54 manuscripts describing 61 cases of ILC with metastasis to the female genital tract [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69] remained for data extraction.
2.3. Statistical Analysis
As detailed patient characteristics were available in the studied case reports, it was feasible to perform statistical analysis. Specifically, the descriptive characteristics for the quantitative data that were expressed as median and Quartile 1 (Q1) to Quartile 3 (Q3), range and for completeness reasons via mean±standard deviation (SD), and for the qualitative data was reported the frequency of occurrence and the relevant percentage. It was also possible to evaluate overall survival (OS) via the Kaplan – Meier estimator and perform comparisons of OS with various characteristics via the log-rank method. The statistical analysis was performed using the R language for statistical analysis (version 4.4.0), and the significance level (p-value) was set to 0.05 when applicable tests were two-sided.The Materials and Methods should be described with sufficient details to allow others to replicate and build on the published results. Please note that the publication of your manuscript implicates that you must make all materials, data, computer code, and protocols associated with the publication available to readers. Please disclose at the submission stage any restrictions on the availability of materials or information. New methods and protocols should be described in detail while well-established methods can be briefly described and appropriately cited.
3. Results
3.1. Patients’ Characteristics
In total, 61 patients were reported in the studied case reports and case series. The mean patient age was 57.4±12.2 years (min: 32, max: 86). The detailed descriptive statistics for patient characteristics are depicted in Table 1.
3.2. Demographic and Clinicopathological Features
Metastasis of ILC to the female genital tract ILC metastasis to the FGT is uncommon. We were able to retrieve 54 manuscripts describing a total of 61 cases of ILC FGT secondaries. Primary tumor size was mentioned in 22/61 (36%) [17,18,21,22,23,25,28,32,34,36,39,40,41,43,50,53,58,59,63,65,66] cases. The mean tumor size was 36.5 mm (range 9–100 mm). The metastatic site was mentioned in all cases. Some of the patients had more than one FGT metastatic site. The most common metastatic site was the uterine corpus in 30/61 (49.2%) [20,24,27,28,30,35,36,38,39,40,41,43,44,45,46,47,49,50,51,53,54,55,56,59,61,62,64,65,66] patients, followed by the uterine cervix in 25/61 (41%) [21,22,24,27,28,30,31,32,34,35,39,44,46,50,53,54,58,59,62,65,66], and the ovary in 22/61 (36%) [28,29,30,35,36,38,42,44,48,51,53,54,57,63,65,66,67] patients. In 9/61 (14.7%) [16,20,26,27,52,60,68] cases, the metastatic site was an endometrial polyp; in 8/61 (13.1%) [17,23,27,33,37,38,44,45,52,59] a uterine leiomyoma, and in the vulva in 4/61 (6.5%) [18,25,37,42]. Less common metastatic sites were an ovarian granulosa cell tumor [19], the vagina [54], and an ovarian fibroma [69]. Metastases to sites other than the FGT were documented in 21/61 (34.4%) [18,20,21,23,36,37,38,40,41,42,43,44,45,46,49,57,59,62,63,64,66,67]. Metastatic spread to the bones was found in 12/21 (57.1%) [18,20,23,38,41,43,49,59,62,63,64,66] patients. Other metastatic sites were the pancreas [21], stomach [21,37,47,67], liver [36,38], pleura [37], peritoneum [37,42,43], lymph nodes [42,43,46], gallbladder [43], omentum [44], orbit [49], large bowel [57], and appendix [57].
Symptoms were mentioned in 60/61 (98.4%) [16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69] cases. Bleeding from the genitalia was the commonest symptom in 24/60 (40%) [17,20,21,24,26,28,33,35,37,41,43,44,49,52,53,54,55,56,58,60,61,64,65,68] cases followed by abdominal pain in 6/60 (10%) [19,22,57,59,60,69] patients, a mass in 5/60 (8.3%) [18,23,25,51] cases, abdominal distention in 3/60 (5%) [44,63,69] cases, abdominal discomfort in 3/60 (%) [39,67] patients. Less common symptoms included abdominal fullness [29], loss of appetite [29], urinary incontinence [38], polyuria [39], abdominal bloating [42,57], abdominal compression [45], postcoital bleeding [46], vaginal fullness and discomfort [51], altered bowel habits [57], and right shoulder pain [66] in 1/60 (1.7%) of patients each. Finally, 14/60 (23.3%) [16,27,30,31,32,34,36,40,47,48,49,50,51,62] patients were asymptomatic. In 42 cases, the FGT metastasis was metachronous, while in 12 cases, it was concomitant. The interval to metastasis ranged from 2 to 360 months (mean 65.6 months). The detailed demographic and clinicopathological features of the cases are shown in Table 2.
3.3. Histological Findings
3.4. Estrogen Receptors (ER) /Progesterone Receptors (PR) /HER-2 Status
Concerning hormonal and HER-2 status, 36/61 (59%) [18,20,21,23,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,50,54,55,56,58,59,63,65,66,68] cases reported ER and PR in the primary focus and 34/61 (55.7%) [18,19,20,21,23,26,27,28,29,32,35,37,39,40,41,42,44,45,46,47,48,50,52,56,57,58,59,62,63,64,66,68] in the metastatic setting. HER-2 status was reported in 24/61 (39.3%) [29,30,32,34,35,37,38,39,40,41,43,44,45,47,50,54,55,56,58,59,63,65,66,68] in the in the primary focus and 12/61 (19.7%) [28,29,32,35,46,47,52,58,62,64] in the metastatic location. ER, PR, and Her-2 status of the cases and the histological grade are shown in Table 3.
3.5. Treatment
Surgical treatment information was available in 51/61 (83.6%) [17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,52,54,55,56,57,58,59,61,62,63,64,65,66,67,68] cases. In 32/51 (62.7%) [17,20,21,22,23,25,26,27,28,29,30,31,35,39,40,42,44,47,49,54,55,56,57,58,61,62,65,66,67,68] cases, surgical treatment consisted of a modified radical mastectomy. Breast-conserving surgery was performed in 9/51 (17.6%) [18,32,34,36,41,45,46,48,53] cases, hysterectomy and bilateral salpingo-oophorectomy in 5/51 [23,36,39,59,63] (9.8%), breast biopsies in 3/51 (5.9%) [33,43,44]. Omentectomy was performed in 2/51 (3.9%) [36,63] cases. Endometrial and cervical biopsies were performed in 2/51 (3.9%) [34,49] cases, cervical biopsy in 1/51 (1.9%) [34], and partial vulvectomy in 1/51 (1.9%) [18] cases. Additionally, two manuscripts reported that surgical treatment was performed without any additional detail concerning the type of intervention [52,64]. In cases with metachronous FGT metastasis, second-line treatment was reported in 43/49 (87.7%) [16,19,20,21,22,23,25,27,28,29,30,31,32,33,35,37,38,40,41,42,44,45,46,47,48,49,52,53,54,55,56,57,58,60,61,62,64,65,66,68] cases. Surgical treatment consisted in hysterectomy and bilateral salpingo-oophorectomy in 22/43 (51.2%) [16,21,26,28,29,30,32,35,38,41,42,45,48,49,52,53,54,55,58,60,64,65,66,68] patients, bilateral oophorectomy in 2/43 (4.6%) [19,57], pancreatoduodenectomy in 1/43 (2.3%) [21], wide tumor excision in 1/43 (2.3%) [25], omentectomy in 4/43 (9.3%) [29,30,48,64], pelvic lymph node sampling in 1/43 (2.3%) [29], pelvic lymphadenectomy in 2/43 (4.6%) [30,32], excision of an endometrial polyps in 2/43 (4.6%) [33,37], appendectomy in 2/43 (4.6%) [42,57], endometrial biopsy in 1/43 (2.3%) [47], peritoneal biopsies in 2/43 (4.6%) [48,64], partial colectomy in 1/43 (2.3%) [52], anterior resection in 1/43 (2.3%) [57]. Biopsy of the metastatic lesion was performed in 5/43 (11.6%) cases [20,46,56,61,62].
Information regarding adjuvant treatment was provided in 50/61 (83.6%) [17,19,20,21,22,23,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,52,53,54,55,56,57,58,59,62,63,64,65,66,67,68] cases. Chemotherapy either in the adjuvant or neoadjuvant setting was offered in 43/50 (86%) [17,19,20,22,23,25,27,28,29,31,33,34,35,36,38,40,41,42,43,44,45,46,47,48,49,52,53,54,55,56,57,58,59,62,63,64,65,66,67,68] cases and radiotherapy in 27/50 (54%) [19,20,22,27,28,29,31,32,34,35,42,44,45,46,47,48,49,52,53,54,55,57,58,62,65,67,68] cases. In two cases, patients refused chemotherapy [30,50], and in another two, radiotherapy [30,66]. The most common regimen used consisted of cyclophosphamide, methotrexate, and 5-fluorouracil (CMF regimen). In contrast, the second most common regimen consisted of adriamycin, cyclophosphamide (AC regimen), and paclitaxel administered in four [20,25,31,42] and three cases [54,58,63], respectively. Hormonal treatment was provided to 48/50 (96%) [17,19,20,21,22,23,25,26,27,28,29,30,31,32,34,35,36,37,38,39,40,41,42,43,44,45,46,47,49,52,53,54,55,56,57,58,59,62,63,64,65,66,67,68] patients. Among 43 cases with metachronous metastasis, 13 received additional chemotherapy [21,25,30,32,40,42,44,46,47,48,54,56,66,67], one received targeted therapy [65], two received additional radiotherapy [23,41], and 13 received additional hormonal treatment [19,21,23,32,35,41,42,45,52,58,64,65,68].
3.6. Outcome
Follow-up information was available in 40/61 (65.6%) [17,18,19,21,22,23,25,28,30,31,32,34,35,36,37,38,39,40,41,42,43,45,47,48,50,51,52,53,54,58,60,62,63,64,66,67,68] cases. Briefly, 16/40 (40%) [17,19,32,35,36,37,38,39,45,48,52,53,58,60,64,67,68] patients were alive without evidence of disease, 9/40 (22.5%) [18,23,25,30,34,41,42,47,51] were alive with disease, and 10/40 (25%) [21,28,31,40,43,51,54,66] died of disease in a period of time that ranges from 1 to 308 months. In 2/40 (5%) [22,50] cases, patients were lost to follow-up. Treatment and follow-up data are shown in Table 4.
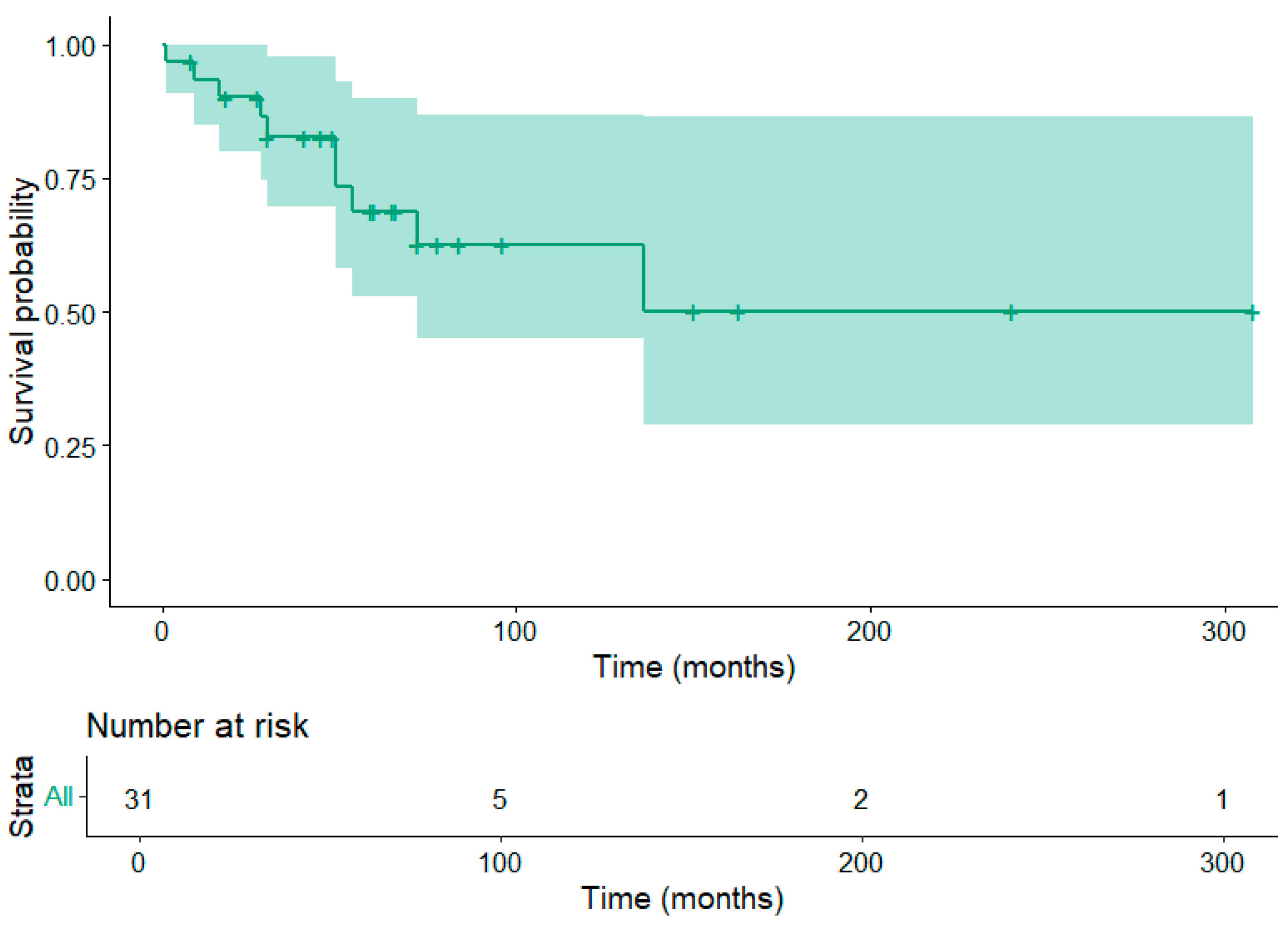
3.5. Patient Survival
Patient survival time information was available for 31 patients. Of these patients, 10 were deceased due to their disease; the restricted mean survival time was 186±30.7 months.
Figure 1.
Kaplan Meier estimator for the patient overall survival. The shaded area corresponds to the 95% confidence interval.
Figure 1.
Kaplan Meier estimator for the patient overall survival. The shaded area corresponds to the 95% confidence interval.
4. Discussion
Extragenital metastases to the FGT are relatively uncommon. Concernng specific locations of secondaries, One study reported that, among 149 metastatic neoplasms to the FGT from primary extragenital tumors reported in one study, the ovary (75.8%) and vagina (13.4%) were the most frequent locations, followed by the endometrium (4.7%) and cervix (3.4%) [72]. The majority of FGT metastases from breast cancer occurred in advanced cases during hormonal treatment or follow-up [53].
In the literature, the incidence of ILC metastasis to the FGT ranges from 2% to 5% in clinical series [5,73] and from 36% to 52% in autopsy series [74,75]. This difference is probably due to the fact that autopsy may discover clinically occult micrometastases. Adnexal involvement was reported in 21% of patients in a series [76].
The ovaries frequently receive metastases from primary malignant tumors both of genital and extragenital sites [77,78]. This can be explained by the fact that they provide an excellent environment for malignant cell implantation due to their rich vasculature and extensive lymphatic network, as well as due to a favorable pH and oxygen pressure in the ovarian stroma [31].
In a number of studies, the most common primary site varies between the gastrointestinal tract and the breast [79]. Ovarian metastasis from breast carcinoma constitutes 3–38% of all ovarian neoplasms, with a variable incidence depending on diagnostic methods, geographic distributions, and other variables [80,81,82]. Studies have shown that breast cancer patients have an incidence of ovarian metastases in 13–47% of cases, either in autopsy or surgical material [83,84,85].
ILC ovarian metastasis usually manifests as bilateral solid and cystic masses, the so-called Krukenberg tumor(s). Micrometastatic disease may remain undetected both on clinical examination and imaging studies [86].
Metastases in the ovaries may occasionally mimic clinical and histological characteristics of primary ovarian carcinomas [79]. The distinction of metastatic versus primary ovarian carcinoma is of paramount importance since their management differs [77,87,88,89]. To date, there are no clear guidelines concerning the management of carcinomas metastatic to the ovary. However, surgical resection may increase patient survival [79].
Some clinicopathologic factors of primary breast carcinoma have been identified to be related to increased risk for ovarian metastasis. ILC has an increased metastatic potential to the ovaries [5,74,75,90,91,92]. Also, young age and premenopausal status are factors related to increased risk [81,93,94,95,96]. Other factors related to the development of ovarian metastases are other co-existent metastatic sites [85], large primary tumor size [85,97], inflammatory breast cancer [85], positive lymph nodes [85,97], higher stage (III-IV)[97,98,99], and bilaterality [81].
The incidental finding of an ovarian mass in an asymptomatic patient may be the first sign of ovarian metastasis [77,98,99,100,101,102]. Usually, they are bilateral, small, and solid [81,82,87,103,104,105,106,107,108]. Other symptoms, including gastrointestinal symptoms, ascites, pelvic pain, and vaginal bleeding, can be observed in some patients [77,94]. However, none of these clinical manifestations is related to either breast metastasis or primary ovarian carcinoma [78,82,107]. In our review, only 3/20 (15%) [30,48,51] cases were asymptomatic.
Imaging examinations are also widely used for diagnosis, staging, and monitoring of curative effects.
The pathologic examination of a specimen includes gross, microscopic, and immunohistochemical testing. These are considered the ‘gold standard’ in the diagnosis of metastatic breast cancer to the ovaries [109].
On gross examination, bilateral involvement, small size, and a solid mass are clues related to metastatic breast carcinoma [81,82,87,98,103,105,106,108,109]. Metastases in the ovaries are usually located in the ovarian medulla and/or cortex [94]. On the other hand, primary tumors are typically located in the ovarian surface epithelium and superficial cortex [102].
Microscopically, ovarian metastases sometimes mimic histological features of primary ovarian carcinomas [103,110,111], which makes their distinction difficult. The characteristic pattern of ILC with small, discohesive cells forming single-cell files will usually allow to make the diagnosis on hematoxylin and eosin stains. In difficult cases, immunohistochemical analysis typically resolves any diagnostic problem. Immunostaining for GATA-3, GCDFP-15, and Mammaglobin is diagnostic for metastatic ILC, whereas PAX-8, WT-1 p53, and p16 are positive in primary ovarian carcinoma.
Concerning treatment options, most breast cancer patients have other non-FGT metastases at the time of ovarian metastasis. The treatment should be for systemic disease. The regimen should be tailored to the clinicopathological aspects of the metastatic site, the burden of disease and the eventual visceral crisis, the symptoms, and the performance status of the patient. Drug toxicity profile and patient preferences are of utmost importance [85,103].
The prognosis of patients with breast carcinoma ovarian metastases is poor since the median progression-free survival ranges from 9 to 30 months, the median overall survival is 16 to 38 months, and the 5-year survival rate is 6 to 26% [79].
Clinicopathologic factors that affect survival are age [103], time interval to ovarian metastasis [82], unilaterality [109], adenocarcinoma [112], and menstrual status [89].
Uterine metastases from extragenital cancers are much less common than ovarian metastases ones [52]. Metastases confined to the uterus, without ovarian involvement, are very rare and can occur through hematogenous spread [52]. The myometrium is the most commonly involved location within the corpus uteri that metastatic ILC involves, followed by the endometrium. The first manifestation of metastatic disease may be abnormal uterine bleeding [86].
ILC is, in most cases, ER-positive. Premenopausal patients regularly receive Tamoxifen as part of the adjuvant treatment, which, increases the risk for endometrioid carcinoma of the endometrium [86].
Differentiating metastatic ILC from a primary endometrial carcinoma can be difficult but is of huge importance since the treatment is different for these carcinomas.
Metastasis from breast carcinoma to the cervix uteri is very rare, with an estimated frequency of 0.8–1.7% [113]. This is possibly due to its small size, its reduced blood flow and distal circulation, and the presence of abundant fibrous tissue [114]. The true incidence of cervical metastasis from ILC remains unknown. Other distant metastases were found at the time of diagnosis of cervical metastasis in 67%–89% of the cases [115].
In our review, we found 22 cases of ILC metastatic to the cervix.
Differential diagnosis between a cervical primary and ILC cervical metastasis may occasionally prove difficult. Dedifferentiation of cervical adenocarcinoma and squamous cell carcinoma with acantholytic changes may result in the simulation of the morphology of ILC [116,117]. Again, the finding of the characteristic morphology of ILC, i.e., discohesive cells and the formation of single cell files within the cervical stroma, especially when the cervical epithelium is spared, should raise the suspicion of metastatic disease. Appropriate immunohistostaining with GATA3, mammaglobin, and GCDFP-15 will give the diagnostic solution in ambiguous cases.
Vaginal metastasis is second in frequency after ovarian involvement in the FGT. Treatment consists of surgical debulking chemotherapy and/or radiotherapy. For patients with vaginal metastasis from breast carcinoma, a very important prognostic feature is the finding of metastases in other sites [118]. A lot of times, when vaginal metastases occur, there are already metastases in other organs. Whenever this happens, the prognosis is poor [119].
Breast cancer metastasis to the vulva is very rare. In these cases, the differential diagnosis is done with primary breast carcinoma of the vulva [120]. The most important distinguishing feature is the previous history of breast cancer. Additionally, the histological similarity between the primary breast and the metastatic lesion, as well as the absence of an in situ element, will guide the pathologist in diagnosing a metastatic lesion [120].
5. Conclusions
In summary, we reviewed cases and case series of ILC metastasis to the FGT, describing the clinical, pathological, therapeutical, and follow-up data. We also discussed the current literature focusing on the differential diagnosis, treatment, and prognosis of ILC metastasis to the FGT.
Author Contributions
Conceptualization, N.I.K. and I.B.; methodology, G.B, R.C and M.Zi.; software, K.S., M.G.S. and A.Pou; validation, M.G.S, T.N. N.A. and A.Psy.; formal analysis, G.B., R.C. and M.Zi and ; investigation, I.S.P, D.G.; resources, K.S., T.N. and J.S.; data curation, A.P. , S.S. and M.Z.; writing—original draft preparation, N.I.K., A.Pou and J.S.; writing—review and editing, all authors; visualization, I.S.P and D.G..; supervision, N.A. A.Psy. and I.G.P.; project administration, S.S. I.B. and A.K.; funding acquisition, A.P., I.G.P. and M.Z.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. This study was partially supported by the Italian Ministry of Health - Ricerca Corrente Annual Program 2026.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ellis, I.; Galea, M.; Broughton, N.; Locker, A.; Blamey, R.; Elston, C.: Pathological prognostic factors in breast cancer. II. Histological type. Relationship with survival in a large study with long-term follow-up. Histopathology 1992, 20, 479-489. [CrossRef]
- Foote Jr, F.W.; Stewart, F.W.: Lobular carcinoma in situ: a rare form of mammary cancer. Am J Pathol. 1941, 17, 491. [CrossRef]
- Koufopoulos, N.; Pateras, I.S.; Gouloumis, A.R.; Ieronimaki,A.I.;, Zacharatou, A.; Spathis, A.; Leventakou, D.; Economopoulou, P.; Psyrri, A.; Arkadopoulos, N.; Panayiotides I.G.: Diagnostically Challenging Subtypes of Invasive Lobular Carcinomas: How to Avoid Potential Diagnostic Pitfalls. Diagnostics 2022, 12, 2658. [CrossRef]
- Reed, A.E.M.; Kutasovic, J.R.; Lakhani, S.R.; Simpson, P.T.: Invasive lobular carcinoma of the breast: morphology, biomarkers and’omics. Breast Cancer Res. 2015, 17, 1-11. [CrossRef]
- Arpino, G.; Bardou, V.J.; Clark, G.M.; Elledge, R.M.: Infiltrating lobular carcinoma of the breast: tumor characteristics and clinical outcome. Breast Cancer Res. 2004, 6, 1-8. [CrossRef]
- Mathew, A.; Rajagopal, P.S.; Villgran, V.; Sandhu, G.S.; Jankowitz, R.C.; Jacob, M.; Rosenzweig, M.; Oesterreich, S.; Brufsky, A.: Distinct pattern of metastases in patients with invasive lobular carcinoma of the breast. Geburtshilfe Frauenheilkund. 2017, 77, 660-666. [CrossRef]
- Inoue, M.; Nakagomi, H.; Nakada, H.; Furuya, K.; Ikegame, K.; Watanabe, H.; Omata, M.; Oyama, T.: Specific sites of metastases in invasive lobular carcinoma: a retrospective cohort study of metastatic breast cancer. Breast Cancer. 2017, 24, 667-672. [CrossRef]
- Kioleoglou, Z.; Georgaki, E.; Koufopoulos, N.; Kostek, O.; Volakakis, N.; Dimitriadou, A.; Kokkali, S.: Gastrointestinal metastases from lobular breast carcinoma: a literature review. Cureus. 2024, 16, e65852. [CrossRef]
- de Leeuw, W.J.; Berx, G.; Vos, C.B.; Peterse, J.L.; Van de Vijver, M.J.; Litvinov, S.; Van Roy, F.; Cornelisse, C.J.; Cleton-Jansen, A.M.: Simultaneous loss of E-cadherin and catenins in invasive lobular breast cancer and lobular carcinoma in situ. J Pathol. 1997, 183, 404-411. [CrossRef]
- Martinez, V.; Azzopardi, J.: Invasive lobular carcinoma of the breast: incidence and variants. Histopathology. 1979, 3, 467-488. [CrossRef]
- Fisher, E.R.; Gregorio, R.M.; Redmond, C.; Fisher, B.: Tubulolobular invasive breast cancer: a variant of lobular invasive cancer. Hum Pathol. 1977, 8, 679-683. [CrossRef]
- Fechner RE: Histologic variants of infiltrating lobular carcinoma of the breast. Hum Pathol. 1975, 6, 373-378. [CrossRef]
- Koufopoulos, N.I.; Boutas, I.; Pouliakis, A.; Samaras M.G.; Kotanidis, C.; Kontogeorgi, A.; Dimas, D.T.; Ieronimaki, A.I.; Leventakou, D.; Spathis, A.; Zanelli, M.; Palicelli, A.; Zizzo, M.; Goutas, D.; Pateras, I.S.; Panayiotides, I.G.: The “forgotten” subtypes of breast carcinoma: a systematic review of selected histological variants not included or not recognized as distinct entities in the current World Health Organization classification of breast tumors. Int J of Mol Sci. 2024, 25, 8382. [CrossRef]
- Eusebi, V.; Magalhaes, F.; Azzopardi, J.G.: Pleomorphic lobular carcinoma of the breast: an aggressive tumor showing apocrine differentiation. Hum Pathol. 1992, 23, 655-662. [CrossRef]
- Christgen, M.; Steinemann, D.; Kühnle, E.; Länger, F.; Gluz, O.; Harbeck, N.; Kreipe, H.: Lobular breast cancer: Clinical, molecular and morphological characteristics. Pathol Res Pract. 2016, 212, 583-597. [CrossRef]
- Aranda, F.I.; Laforga, J.B.; Martinez, M.A.: Metastasis from breast lobular carcinoma to an endometrial polyp Report of a case with immunohistochemical study. Acta Obstet Gynecol Scand. 1993, 72, 585-587. [CrossRef]
- Sugiyama, T.; Toyoda, N.; Nose, J.; Kihira, N.; Ando, Y.; Ishihara, A.: Breast cancer metastatic to uterine leiomyoma: A case report. J Obstet Gynaecol. 1995, 21, 349-355. [CrossRef]
- Menzin, A.W.; De Risi, D.; Smilari, T.F.; Kalish, P.E.; Vinciguerra, V.: Lobular breast carcinoma metastatic to the vulva: a case report and literature review. Gynecol Oncol. 1998, 69, 84-88. [CrossRef]
- Arnould, L.; Franco, N.; Soubeyrand, M.S.; Mege, F.; Belichard, C.; Lizard-Nacol, S.; Collin, F.: Breast carcinoma metastasis within granulosa cell tumor of the ovary: morphologic, immunohistologic, and molecular analyses of the two different tumor cell populations. Hum Pathol. 2002, 33, 445-448. [CrossRef]
- Alvarez, C.; Ortiz-Rey, J.; Estévez, F.; De La Fuente, A.: Metastatic lobular breast carcinoma to an endometrial polyp diagnosed by hysteroscopic biopsy. Obstet Gynecol. 2003, 102, 1149-1151.
- Ogino, A.; Nomizu, T.; Gonnda, K.; Okouchi, C.; Sakuma, T.; Yamada, M.; Katagata, N.; Watanabe, F.; Yamaguchi, Y.; Yoshida, T.: A case of breast cancer metastasizing to cervix after resection of pancreatic metastasis. Breast Cancer. 2003, 10, 284-288. [CrossRef]
- Rau, A.R.; Saldanha, P.; Raghuveer, C.: Metastatic lobular mammary carcinoma diagnosed in cervicovaginal smears: a case report. Diagn Cytopathol. 2003, 29, 300-302. [CrossRef]
- Blecharz, P.; Szpor, J.; Karolewski, K.; Ryś, J.: Breast cancer metastases to uterine leiomyomas-a clinical and patomorphological analysis of two cases. Nowotwory J Oncol. 2004, 54, 488-488.
- Famoriyo, A.; Sawant, S.; Banfield, P.J.: Abnormal uterine bleeding as a presentation of metastatic breast disease in a patient with advanced breast cancer on tamoxifen therapy. Arch Gynecol Obstet. 2004, 270, 192-193. [CrossRef]
- Sheen-Chen, S.M.; Eng, H.L.; Huang, C.C.: Breast cancer metastatic to the vulva. Gynecol Oncol. 2004, 94, 858-860. [CrossRef]
- Al-Brahim, N.; Elavathil, L.J.: Metastatic breast lobular carcinoma to tamoxifen-associated endometrial polyp: case report and literature review. Ann Diagn Pathol. 2005, 9, 166-168. [CrossRef]
- Lee, T.F.; Wang, Y.L.; Wei, T.S.; Chen, C.P.: Incidental detection of metastatic lobular breast carcinoma in the female internal genital organs 2 years following modified radical mastectomy. Taiwan J Obstet Gynecol. 2005, 44, 368-371. doi: 10.1016/S1028-4559(09)60175-3.
- Scopa, C.D.; Aletra, C.; Lifschitz-Mercer, B.; Czernobilsky, B.: Metastases of breast carcinoma to the uterus. Report of two cases, one harboring a primary endometrioid carcinoma, with review of the literature. Gynecol Oncol. 2005, 96, 543-547. [CrossRef]
- Chen, P.; Hu, W.M.; Wang, P.H.; Suen, J.H.: Recurrent breast cancer presents as a single solid ovarian mass and ascites. Taiwan J Obstet Gynecol. 2006, 45, 356-359. [CrossRef]
- Erkanli, S.; Kayaselcuk, F.; Kuscu, E.; Bolat, F.; Sakalli, H.; Haberal, A.: Lobular carcinoma of the breast metastatic to the uterus in a patient under adjuvant anastrozole therapy. Breast. 2006, 15, 558-561. [CrossRef]
- Perišić, D.; Jančić, S.; Kalinović, D.; Čekerevac, M.: Metastasis of lobular breast carcinoma to the cervix. J Obstet Gynaecol Res. 2007, 33, 578-580. [CrossRef]
- Manci, N.; Marchetti, C.; Esposito, F.; Graziano, M.; Tomao, F.; Pastore, M.; Bellati, F.; Panici, P.B.: Late breast cancer recurrence to the uterine cervix with a review of the literature. Int J Gynecol Pathol. 2008, 27, 113-117. [CrossRef]
- Manipadam, M.; Walter, N.; Selvamani, B.: Lobular carcinoma metastasis to endometrial polyp unrelated to tamoxifen: Report of a case and review of the literature. APMIS. 2008, 116, 538-540. [CrossRef]
- Bogliolo, S.; Morotti, M.; Valenzano Menada, M.; Fulcheri, E.; Musizzano, Y.; Casabona, F.: Breast cancer with synchronous massive metastasis in the uterine cervix: a case report and review of the literature. Arch Gynecol Obstet. 2010, 281, 769-773. [CrossRef]
- Ustaalioglu, B.B.; Bilici, A.; Seker, M.; Salman, T.; Gumus, M.; Barisik, N.O.; Salepci, T.; Yaylaci, M.: Metastasis of lobular breast carcinoma to the uterus in a patient under anastrozole therapy. Oncologie. 2009, 32, 424-426. [CrossRef]
- Engelstaedter, V.; Mylonas, I.: Lower genital tract metastases at time of first diagnosis of mammary invasive lobular carcinoma. Arch Gynecol Obstet. 2011, 283, 93-95. [CrossRef]
- Hooker, A.; Radder, C.; van De Wiel, B.; Geenen, M.: Metastasis from breast cancer to an endometrial polyp; treatment options and follow-up. Report of a case and review of the literature. Eur J Gynaecol Oncol. 2011, 32, 228-230.
- Işçi, H.; Güdücü, N.; Basgul, A.; Aydınlı, K.; Calay, Z.; Dünder, I.: Lobular carcinoma of the breast metastasızıng to leiomyoma in a patient under letrozole treatment. Eur J Gynaecol Oncol. 2011, 32, 560-562.
- Horikawa, M.; Mori, Y.; Nagai, S.; Tanaka, S.; Saito, S.; Okamoto, T.: Metastatic breast cancer to the uterine cervix mimicking a giant cervical leiomyoma. Nagoya J Med Sci. 2012, 74, 347.
- Komeda, S.; Furukawa, N.; Kasai, T.; Washida, A.; Kobayashi, H.: Uterine metastasis of lobular breast cancer during adjuvant letrozole therapy. J Obstet Gynaecol. 2013, 33, 100-101. [CrossRef]
- Vicioso, L.; Ortega, M.V.; Cívico, V.; López-Beltrán, A.: Synchronous metastasis from lobular carcinoma and primary carcinoma of the endometrium in a patient after tamoxifen therapy. Int J Gynecol Pathol. 2013, 32, 66-70. [CrossRef]
- Alligood-Percoco, N.R.; Kessler, M.S.; Willis, G.: Breast cancer metastasis to the vulva 20 years remote from initial diagnosis: a case report and literature review. Gynecol Oncol Rep. 2015, 13, 33-35. [CrossRef]
- Bezpalko, K.; Mohamed, M.A.; Mercer, L.; McCann, M.; Elghawy, K.; Wilson, K.: Concomitant endometrial and gallbladder metastasis in advanced multiple metastatic invasive lobular carcinoma of the breast: a rare case report. Int J Surg Case Rep. 2015, 14, 141-145. [CrossRef]
- Lokadasan, R.; Ratheesan, K.; Sukumaran, R.; Nair, S.P.: Metastatic lobular carcinoma of breast mimics primary cervix carcinoma: two case reports and a review of the literature. Ecancermedicalscience. 2015, 9. [CrossRef]
- Toyoshima, M.; Iwahashi, H.; Shima, T.; Hayasaka, A.; Kudo, T.; Makino, H.; Igeta, S.; Matsuura, R.; Ishigaki, N.; Akagi, K.; Sakurada, J.; Suzuki, H.; Yoshinaga, K.: Solitary uterine metastasis of invasive lobular carcinoma after adjuvant endocrine therapy: a case report. J Med Case Rep. 2015, 9, 1-4. [CrossRef]
- Waks, A.G.; Lennon, J.; Yadav, B.S.; Hwang, H.; dSchapirael Carmen, M.; Johnson, N.B.; Reynolds, K.; Schapira, L.; Gilman, P.B.; Overmoyer, B.: Metastasis to the Cervix Uteri 15 Years After Treatment of Lobular Carcinoma of the Breast. Semin Oncol. 2015 42, e81-94. [CrossRef]
- Lai, M.J.; Lai, C.L.; Huang, I.H.; Yu, J.C.; Lee, H.S.; Dai, M.S.: Synchronous endometrial and gastric metastases of invasive lobular breast carcinomas. Taiwan J Obstet Gynecol. 2016, 55, 131-134. [CrossRef]
- Makris, G.M.; Marinelis, A.; Battista, M.J.; Chrelias, C.; Papantoniou, N.: An ovarian mass after breast cancer: Metachronous carcinoma or metastasis? A case report. Int J Ssurg Case Rep. 2017, 31, 106-108. [CrossRef]
- Martinez, M.R.; Marazuela, M.A.; Vallejo, M.R.; Bernabeu, R.Á.; Medina, T.P.: Metastasis of lobular breast cancer to endometrial polyps with and without the presence of vaginal bleeding. Int J Gynecol Obstet. 2016, 134, 101-102. [CrossRef]
- Akhtar, A.; Ratra, A.; Puckett, Y.; Sheikh, A.B.; Ronaghan, C.A.: Synchronous uterine metastases from breast cancer: case study and literature review. Cureus. 2017, 9, e1840. [CrossRef]
- Bennett, J.A.; Young, R.H.; Chuang, A.Y.; Lerwill, M.F.: Ovarian metastases of breast cancers with signet ring cells: a report of 17 cases including 14 Krukenberg tumors. Int J Gynecol Pathol. 2018, 37, 507-515. [CrossRef]
- Razia, S.; Nakayama, K.; Tsukao, M.; Nakamura, K.; Ishikawa, M.; Ishibashi, T.; Ishikawa, N.; Sanuki, K.; Yamashita, H.; Ono, R.; Hossain, M.M.; Minamoto, T.; Kyo, S.: Metastasis of breast cancer to an endometrial polyp, the cervix and a leiomyoma: A case report and review of the literature. Oncol Lett. 2017, 14, 4585-4592. [CrossRef]
- Seo, S.O.; Shin, J.Y.; Ji, Y.I.: Metastatic uterine cancer looking as cervical fibroid in recurrent breast cancer woman: a case report. Obstet Gynecol Sci. 2017, 60, 481-484. [CrossRef]
- Aytekin, A.; Bilgetekin, I.; Ciltas, A.; Ogut, B.; Coskun, U.; Benekli, M.: Lobular breast cancer metastasis to uterus during adjuvant tamoxifen treatment: A case report and review of the literature. J Cancer Res Ther. 2018, 14, 1135-1137. [CrossRef]
- Briki, R.; Cherif, O.; Bannour, B.; Hidar, S.; Boughizane, S.; Khairi, H.: Uncommon metastases of invasive lobular breast cancer to the endometrium: a report of two cases and review of the literature. Pan Afr Med J. 2018, 30. [CrossRef]
- Franco-Márquez, R.; Torres-Gaytán, A.G.; Narro-Martinez, M.A.; Carrasco-Chapa, A.; Núñez, B.G.; Boland-Rodriguez, E.: Metastasis of Breast Lobular Carcinoma to Endometrium Presenting as Recurrent Abnormal Uterine Bleeding: A Case Report and Review of Literature. Case Rep Pathol. 2019, 2019, 5357194. [CrossRef]
- Kachi, A.; Nicolas, G.; Semaan, D.B.; Hashem, M.; Abou Sleiman, C.: Unusual pattern of invasive lobular carcinoma metastasis: a case report. Am J Case Rep. 2019, 20, 1659. [CrossRef]
- Fontinele, D.R.S.; Vieira, S.C.; da Silva Júnior, R.G.; Rodrigues, T.S.: Lobular carcinoma of the breast with metastasis to the uterine cervix. J Cancer Res Ther. 2019, 15, 1411-1414. [CrossRef]
- Abdallah, H.; Elwy, A.; Alsayed, A.; Rabea, A.; Magdy, N.: Metastatic breast lobular carcinoma to unusual sites: a report of three cases and review of literature. J Med Cases. 2020, 11, 292. [CrossRef]
- Arif, S.H.; Mohammed, A.A.; Mohammed, F.R.: Metastatic invasive lobular carcinoma of the breast to the endometrium presenting with abnormal uterine bleeding; Case report. Ann Med Surg. 2020, 51, 41-43. [CrossRef]
- Gomez, M.; Whitting, K.; Naous, R.: Lobular breast carcinoma metastatic to the endometrium in a patient under tamoxifen therapy: A case report. SAGE Open Med Case Rep. 2020, 8, 2050313X20907208. [CrossRef]
- Yuan, L.; Oshilaja, O.; Sierk, A.; et al.: Metastatic breast cancer diagnosed on cervical cytology. Cytopathology. 2021, 32, 127-131. [CrossRef]
- Akizawa, Y.; Kanno, T.; Horibe, Y.; Shimizu, Y.; Noguchi, E.; Yamamoto, T.; Okamoto, T.; Nagashima, Y.; Tabata, T.: Ovarian metastasis from breast cancer mimicking a primary ovarian neoplasm: a case report. Mol Clin Oncol. 2021, 15, 135. [CrossRef]
- Awazu, Y.; Fukuda, T.; Imai, K.; Yamauch, M.; Kasai, M.; Ichimura, T.; Yasui, T.; Sumi, T.: Uterine metastasis of lobular breast carcinoma under tamoxifen therapy: A case report. Mol Clin Oncol. 2021, 15, 266. [CrossRef]
- Lim, L.; Wang, T.Y.; Lam, H.B.; Chang, C.L.: Massive metastasis of breast cancer to female genital organs. Taiwan J Obstet Gynecol. 2021, 60, 563-566. [CrossRef]
- Kong, D.; Dong, X.; Qin, P.; Sun, D.; Zhang, Z.; Zhang, Y.; Hao, F.; Wang, M.: Asymptomatic uterine metastasis of breast cancer: Case report and literature review. Medicine. 2022, 101, e31061. [CrossRef]
- Li, T.; Jiang, X.; Zhang, Z.; Chen, X.; Wang, J.; Zhao, X.; Zhang, J.: Case Report: 68Ga-FAPI PET/CT, a more advantageous detection mean of gastric, peritoneal, and ovarian metastases from breast cancer. Front Oncol. 2022, 12, 1013066. [CrossRef]
- Benlghazi, A.; Messaoudi, H.; Benali, S.; Tazi, I.; Elhassani, M.M.; Kouach, J.: Lobular carcinoma metastasis to endometrial polyps: Insights from a case report and literature analysis. Int J Surg Case Rep. 2024, 124, 110463. [CrossRef]
- Faur, A.C.; Gurban, C.V.; Dăescu, E.; Tîrziu, R.V.; Lazăr, D.C.; Ghenciu, L.A.: Mucin-Producing Lobular Breast Carcinoma Metastasis to an Ovarian Fibroma: Histopathological and Immunohistochemical Analysis of a Rare Case and Literature Review. Diagnostics. 2024, 14, 953. [CrossRef]
- Cserni, G.; Floris, G.; Koufopoulos, N.; Kovács, A.; Nonni, A.; Regitnig, P.; Stahls, A.; Varga, Z.: Invasive lobular carcinoma with extracellular mucin production—a novel pattern of lobular carcinomas of the breast. Clinico-pathological description of eight cases. Virchows Arch. 2017, 471, 3-12. [CrossRef]
- Koufopoulos, N.; Antoniadou, F.; Kokkali, S.; Pigadioti, E.; Khaldi, L.: Invasive lobular carcinoma with extracellular mucin production: description of a case and review of the literature. Cureus. 2019, 11, e5550. [CrossRef]
- Mazur, M.T.; Hsueh, S.; Gersell, D.J.: Metastases to the female genital tract: analysis of 325 cases. Cancer. 1984, 53, 1978-1984. [CrossRef]
- Borst, M.J.; Ingold, J.A.: Metastatic patterns of invasive lobular versus invasive ductal carcinoma of the breast. Surgery. 1993, 114, 637-642.
- Harris, M.; Howell, A.; Chrissohou, M.; Swindell, R.; Hudson, M.; Sellwood, R.: A comparison of the metastatic pattern of infiltrating lobular carcinoma and infiltrating duct carcinoma of the breast. Br J Cancer. 1984, 50, 23-30. [CrossRef]
- Lamovec, J.; Bračkko, M.: Metastatic pattern of infiltrating lobular carcinoma of the breast: an autopsy study. J Surg Oncol. 1991, 48, 28-33. [CrossRef]
- Winston, C.B.; Hadar, O.; Teitcher, J.B.; et al.: Metastatic lobular carcinoma of the breast: patterns of spread in the chest, abdomen, and pelvis on CT. AJR Am J Roentgenol. 2000, 175, 795-800. [CrossRef]
- Ayhan, A.; Guvenal, T.; Salman, M.; Ozyuncu, O.; Sakinci, M.; Basaran, M.: The role of cytoreductive surgery in nongenital cancers metastatic to the ovaries. Gynecol Oncol. 2005, 98, 235-241. [CrossRef]
- Bruchim, I.; Ben-Harim, Z.; Piura, E.; Tepper, R.; Fishman, A.: Preoperative clinical and radiological features of metastatic ovarian tumors. Arch Gynecol Obstet. 2013, 288, 615-619. [CrossRef]
- Tian, W.; Zhou, Y.; Wu, M.; Yao, Y.; Deng, Y.: Ovarian metastasis from breast cancer: a comprehensive review. Clin Transl Oncol. 2019, 21, 819-827. [CrossRef]
- Demopoulos, R.I.; Touger, L.; Dubin, N.: Secondary ovarian carcinoma: a clinical and pathological evaluation. Int J Gynecol Pathol. 1987, 6, 166-175. [CrossRef]
- Bigorie, V.; Morice, P.; Duvillard, P.; Antoine, M.; Cortez, A.; Flejou, J.F.; Uzan, S.; Darai, E.; Barranger, E.: Ovarian metastases from breast cancer: report of 29 cases. Cancer: Interdisciplinary International Journal of the American Cancer Society. 2010, 116, 799-804. [CrossRef]
- Tserkezoglou, A.; Kontou, S.; Hadjieleftheriou, G.; Apostolikas, N.; Vassilomanolakis, M.; Sikiotis, K.; Salamalekis, E.; Tseke, P.; Magiakos, G.: Primary and metastatic ovarian cancer in patients with prior breast carcinoma. Pre-operative markers and treatment results. Anticancer Res. 2006, 26, 2339-2344.
- Rosendahl, M.; Wielenga, V.T.; Nedergaard, L.; Kristensen, S.G.; Ernst, E.; Rasmussen, P.E.; Anderson, M.; Schmidt, K.T.; Andersen, C.Y.: Cryopreservation of ovarian tissue for fertility preservation: no evidence of malignant cell contamination in ovarian tissue from patients with breast cancer. Fertil Steril. 2011, 95, 2158-2161. [CrossRef]
- Bastings, L.; Beerendonk, C.; Westphal, J.; Massuger, L.F.; Kaal, S.E.; van Leeuwen, F.E.; Braat, D.D.; Peek, R.: Autotransplantation of cryopreserved ovarian tissue in cancer survivors and the risk of reintroducing malignancy: a systematic review. Hum Reprod Update. 2013, 19, 483-506. [CrossRef]
- Peters, I.T.; van Zwet, E.W.; Smit, V.T.; Liefers, G.J.; Kuppen, P.J.; Hilders, C.G.; Trimbos, J.B.: Prevalence and risk factors of ovarian metastases in breast cancer patients< 41 years of age in the Netherlands: a nationwide retrospective cohort study. PLoS One. 2017, 12, e0168277. [CrossRef]
- He, H.; Gonzalez, A.; Robinson, E.; Yang, W.T.: Distant metastatic disease manifestations in infiltrating lobular carcinoma of the breast. AJR Am J Roentgenol. 2014, 202, 1140-1148. [CrossRef]
- Guerriero, S.; Alcazar, J.; Pascual, M.; Ajossa, S.; Olartecoechea, B.; Hereter, L.: Preoperative diagnosis of metastatic ovarian cancer is related to origin of primary tumor. Ultrasound Obstet Gynecol. 2012, 39, 581-586. [CrossRef]
- Boutas, I.; Kontogeorgi, A.; Koufopoulos, N.; Dimas, D.T.; Sitara, K.; Kalantaridou, S.N.; Dimitrakakis, K.: Breast cancer and fertility preservation in young female patients: a systematic review of the literature. Clinics and Practice. 2023, 13, 1413-1426. [CrossRef]
- Webb, M.J.; Decker, D.G.; Mussey, E.: Cancer metastatic to the ovary: factors influencing survival. Obstet Gynecol. 1975, 45, 391-396.
- Bumpers, H.L.; Hassett, J.M.; Penetrante, R.B.; Hoover, E.L.; Holyoke, E.D.: Endocrine organ metastases in subjects with lobular carcinoma of the breast. Arch Surg. 1993, 128, 1344-1347. [CrossRef]
- Ferlicot, S.; Vincent-Salomon, A.; Medioni, J.; Genin, P.; Rosty, C.; Sigal-Zafrani, B.; Fréneaux, P.; Jouve, M.; Thiery, J.P.; Sastre-Garau, X.: Wide metastatic spreading in infiltrating lobular carcinoma of the breast. Eur J Cancer. 2004, 40, 336-341. [CrossRef]
- Weigelt, B.; Peterse, J.L.; Van't Veer, L.J.: Breast cancer metastasis: markers and models. Nat Rev Cancer. 2005, 5, 591-602. [CrossRef]
- Fujiwara, K.; Ohishi, Y.; Koike, H.; Sawada, S.; Moriya, T.; Kohno, I.: Clinical implications of metastases to the ovary. Gynecol Oncol. 1995, 59, 124-128. [CrossRef]
- Moore, E.; Roylance, R.; Rosenthal, A.: Breast cancer metastasising to the pelvis and abdomen: what the gynaecologist needs to know. BJOG. 2012, 119, 788-794. [CrossRef]
- Nandy, S.B.; Gangwani, L.; Nahleh, Z.; Subramani, R.; Arumugam, A.; de la Rosa, J.M.; Lakshmanaswamy, R.: Recurrence and metastasis of breast cancer is influenced by ovarian hormone’s effect on breast cancer stem cells. Future Oncology. 2015, 11, 983-995. [CrossRef]
- de la Monte, S.M.; Hutchins, G.M.; Moore, G.W.: Influence of age on the metastatic behavior of breast carcinoma. Hum Pathol. 1988, 19, 529-534. [CrossRef]
- Pimentel, C.; Becquet, M.; Lavoué, V.; Hénno, S.; Lévêque, J.; Ouldamer, L.: Ovarian metastases from breast cancer: a series of 28 cases. Anticancer Res. 2016, 36, 4195-4200.
- Hann, L.E.; Lui, D.M.; Shi, W.; Bach, A.M.; Selland, D.L.; Castiel, M.: Adnexal masses in women with breast cancer: US findings with clinical and histopathologic correlation. Radiology. 2000, 216, 242-247. [CrossRef]
- Abd El hafez, A.; Monir, A.: Diagnostic spectrum of ovarian masses in women with breast cancer; magnetic resonance imaging: histopathology correlation. Ann Diagn Pathol. 2013, 17, 441-447. [CrossRef]
- Curtin, J.P.; Barakat, R.R.; Hoskins, W.J.: Ovarian disease in women with breast cancer. Obstet Gynecol. 1994, 84, 449-452.
- Abu-Rustum, N.R.; Aghajanian, C.A.; Venkatraman, E.S.; Feroz, F.; Barakat, R.R.: Metastatic breast carcinoma to the abdomen and pelvis. Gynecol Oncol. 1997, 66, 41-44. [CrossRef]
- Rabban, J.T.; Barnes, M.; Chen, L.M.; Powell, C.B.; Crawford, B.; Zaloudek, C.J.: Ovarian pathology in risk-reducing salpingo-oophorectomies from women with BRCA mutations, emphasizing the differential diagnosis of occult primary and metastatic carcinoma. Amer J Surg Pathol. 2009, 33, 1125-1136. [CrossRef]
- Gagnon, Y.; Tětu, B.: Ovarian metastases of breast carcinoma. A clinicopathologic study of 59 cases. Cancer. 1989, 64, 892-898. [CrossRef]
- De Waal, Y.R.; Thomas, C.M.; Oei, A.L.; Sweep, F.C.; Massuger, L.F.: Secondary ovarian malignancies: frequency, origin, and characteristics. Int J Gynecol Cancer. 2009, 19, 1160-1165. [CrossRef]
- Kondi-Pafiti, A.; Kairi-Vasilatou, E.; Iavazzo, C.; Dastamani, C.; Bakalianou, K.; Liapis, A.; Hassiakos, D.; Fotiou, S.: Metastatic neoplasms of the ovaries: a clinicopathological study of 97 cases. Arch Gynecol Obstet. 2011, 284, 1283-1288. [CrossRef]
- Perrotin, F.; Marret, H.; Bouquin, R.; Fischer-Perrotin, N.; Lansac, J.; Body, G.: Incidence, diagnosis and prognosis of ovarian metastasis in breast cancer. Gynecol Obstetr Fertil. 2001, 29, 308-315. [CrossRef]
- Antila, R.; Jalkanen, J.; Heikinheimo, O.: Comparison of secondary and primary ovarian malignancies reveals differences in their pre-and perioperative characteristics. Gynecol Oncol. 2006, 101, 97-101. [CrossRef]
- Bruls, J.; Simons, M.; Overbeek, L.I.; Bulten, J.; Massuger, L.F.; Nagtegaal, I.D.: A national population-based study provides insight in the origin of malignancies metastatic to the ovary. Virchows Arch 2015, 467, 79-86. [CrossRef]
- Kubeček, O.; Laco, J.; Špaček, J.; Petera, J.; Kopecký, J.; Kubečková, A.; Filip, S.: The pathogenesis, diagnosis, and management of metastatic tumors to the ovary: a comprehensive review. Clin Exp Metastasis. 2017, 34, 295-307. [CrossRef]
- Yadav, B.S.; Sharma, S.; Robin, T.P.; Sams, S.; Elias, A.D.; Kaklamani, V.; Kelly Marcom, P.; Schaefer, S.; Morris, G.J.: Synchronous primary carcinoma of breast and ovary versus ovarian metastases. Semin Oncol. 2015, 42, e13-e24. [CrossRef]
- Tamás, J.; Vereczkey, I.; Tóth, E.: Metastatic tumors in the ovary, difficulties of histologic diagnosis. Magy Onkol. 2015, 59, 205-213.
- Sal, V.; Demirkiran, F.; Topuz, S.; Kahramanoglu, I.; Yalcin, I.; Bese, T.; Sozen, H.; Tokgozoglu, N.; Salihoglu, Y.; Turan, H.; Iyibozkurt, C.; Kolomuc, T.; Sofiyeva, N.; Berkman, S.; Arvas, M.: Surgical treatment of metastatic ovarian tumors from extragenital primary sites. Int J Gynecol Cancer. 2016, 26, 688-696. [CrossRef]
- Pauer, H.U.; Viereck, V.; Burfeind, P.; Emons, G.; Krauss, T.: Uterine cervical metastasis of breast cancer: a rare complication that may be overlooked. Oncologie. 2003, 26, 58-60. [CrossRef]
- Pérez-Montiel, D.; Serrano-Olvera, A.; Salazar, L.C.; Cetina-Pérez, L.; Candelaria, M.; Coronel, J.; Montalvo, L.A.; de León, D.C.: Adenocarcinoma metastatic to the uterine cervix: a case series. J Obstet Gynaecol Res. 2012, 38, 541-549. [CrossRef]
- Abell, M.R.; Gosling, J.R.: Gland cell carcinoma (adenocarcinoma) of the uterine cervix. Am J Obstet Gynecol. 1962, 83, 729-755. [CrossRef]
- Scott, K.; Bryson, G.; Jamison, J.; Coutts, M.; McCluggage, W.G.: Cervical squamous carcinomas with prominent acantholysis and areas resembling breast lobular carcinoma: an aggressive form of dedifferentation. Int J Gynecol Pathol. 2018, 37, 74-81. [CrossRef]
- Mansor, S.; McCluggage, W.G.: Cervical adenocarcinoma resembling breast lobular carcinoma: a hitherto undescribed variant of primary cervical adenocarcinoma. Int J Gynecol Pathol. 2010, 29, 594-599. [CrossRef]
- Hermi, A.; Chakroun, M.; Saadi, A.; Saidani, B.; Kacem, L.B.; Chebil, M.: Upper urinary tract urothelial carcinoma diagnosis by biopsy of a vaginal metastasis. Urol Case Rep. 2022, 43, 102114. [CrossRef]
- Yan, Y.; Guo, T.; Zhang, M.; Cui, G.: Vaginal metastasis from breast cancer: A case report. Open Life Sci. 2023, 18, 20220623. [CrossRef]
- Gandhi, A.K.; Roy, S.; Mridha, A.R.; Sharma, D.N.: Vulvar metastasis from carcinoma breast unveiling distant metastasis: Exploring an unusual metastatic pattern. J Egypt Natl Canc Inst. 2015, 27, 243-246. [CrossRef]
Figure 2.
Kaplan Meier curves for overall survival in relation to ER status of the secondary tumor.
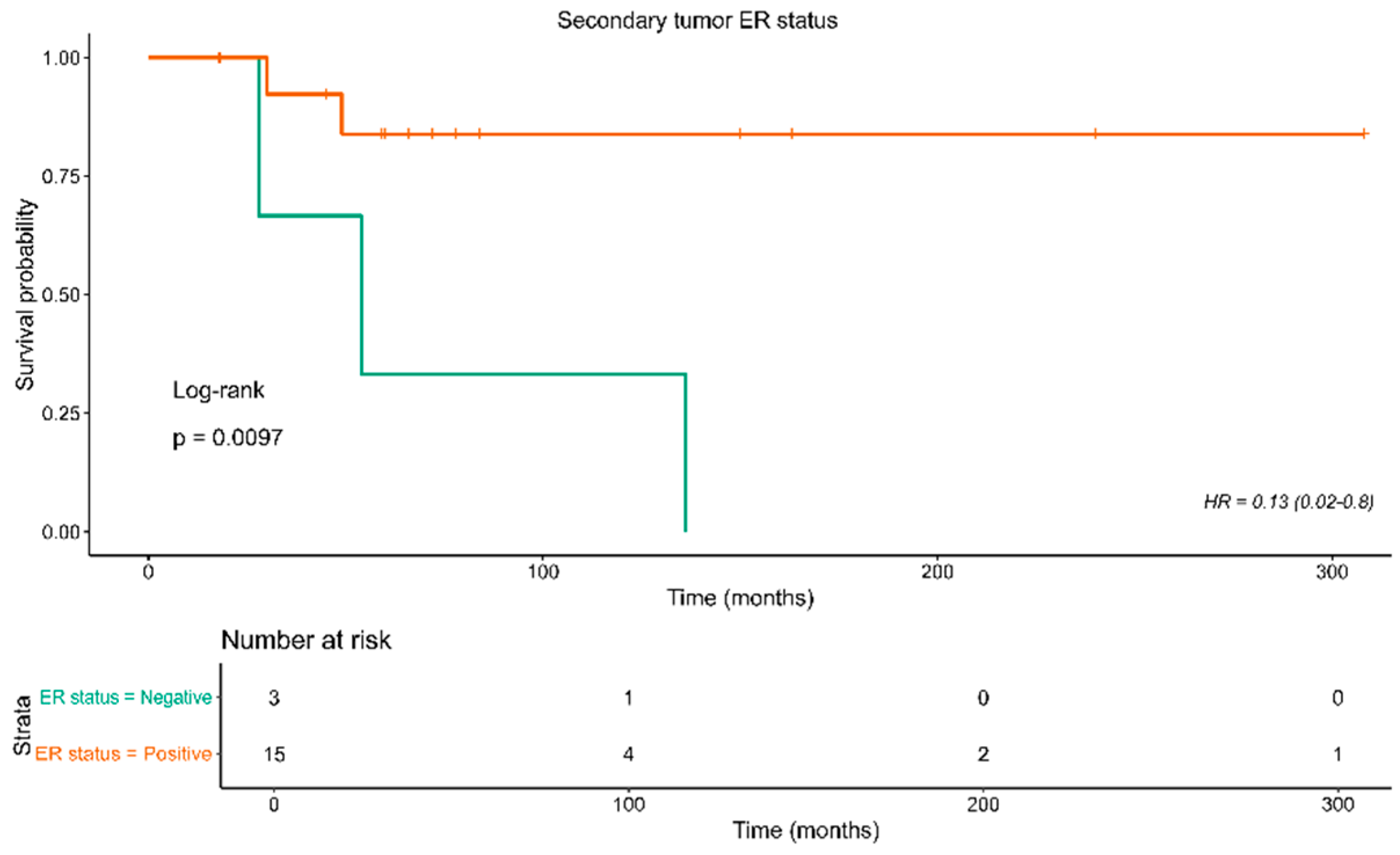

Table 1.
Descriptive characteristics of the reported cases in the studied case reports. ANED: Alive, no evidence of disease, AWD: Alive with the disease, DOD: died of disease, SD: Standard deviation.
Table 1.
Descriptive characteristics of the reported cases in the studied case reports. ANED: Alive, no evidence of disease, AWD: Alive with the disease, DOD: died of disease, SD: Standard deviation.
| Characteristic | Measure |
| Number of cases | 61 |
| Age | |
| Mean±SD | 57.4±12.2 |
| Median [Min, Max] | 56.0 [32.0, 86.0] |
| Tumor Size (cm) | |
| Mean±SD | 3.65±2.11 |
| Median [Min, Max] | 3.65 [0.900, 10.0] |
| Missing | 39 (63.9%) |
| Primary tumor ER status | |
| Negative | 2 (3.3%) |
| Positive | 34 (55.7%) |
| Missing | 25 (41.0%) |
| Primary tumor PR status | |
| Negative | 2 (3.3%) |
| Positive | 34 (55.7%) |
| Missing | 25 (41.0%) |
| HER-2/Cc-erbB-2 status | |
| Negative | 21 (34.4%) |
| Positive | 3 (4.9%) |
| Missing | 37 (60.7%) |
| Secondary tumor ER status | |
| Negative | 3 (4.9%) |
| Positive | 31 (50.8%) |
| Missing | 27 (44.3%) |
| Secondary tumor PR status | |
| Negative | 6 (9.8%) |
| Positive | 24 (39.3%) |
| Missing | 31 (50.8%) |
| HER-2 status | |
| Negative | 9 (14.8%) |
| Positive | 3 (4.9%) |
| Missing | 49 (80.3%) |
| Stage pT component | |
| pT1 | 1 (1.6%) |
| pT1b | 1 (1.6%) |
| pT1c | 6 (9.8%) |
| pT2 | 15 (24.6%) |
| pT3 | 6 (9.8%) |
| pT4 | 1 (1.6%) |
| Missing | 31 (50.8%) |
| Stage pN component | |
| N0 | 8 (13.1%) |
| N1 | 10 (16.4%) |
| N2 | 5 (8.2%) |
| N3 | 9 (14.7%) |
| Missing | 29 (47.5%) |
| Stage pM component | |
| M0 | 22 (36.1%) |
| M1 | 6 (9.8%) |
| Missing | 33 (54.1%) |
| Radiotherapy | |
| No | 24 (39.3%) |
| Yes | 27 (44.3%) |
| Missing | 10 (16.4%) |
| Interval to Met (in months) | |
| Mean±SD | 65.6±70.0 |
| Median [Min, Max] | 48.0 [2.00, 360] |
| Missing | 20 (32.8%) |
| Last, follow up (in months) | |
| Mean±SD | 71.1±67.6 |
| Median [Min, Max] | 54.0 [1.00, 308] |
| Missing | 30 (49.2%) |
| Last, follow up status | |
| ANED | 19 (31.1%) |
| AWD | 9 (14.8%) |
| DOD | 10 (16.4%) |
| Missing | 23 (37.7%) |
| Tumor grade | |
| Grade II | 10 (16.4%) |
| Grade III | 2 (3.3%) |
| Missing | 49 (80.3%) |
Table 2.
Demographic and clinicopathological features of the reported cases.
| Authors | Year | Age | Clinical Presentation | Tumor Size (cm) | Stage | Site of metastasis FGT[16–69 | Other metastatic sites |
| Aranda et al. | 1993 | 76 | Asymptomatic | NM | pTx, N0 | Endometrial polyps | - |
| Sugiyama et al. | 1995 | 51 | Hypermenorrhea | 4 | pT2, N1, M1 | Uterine leiomyoma | - |
| Menzin et al. | 1998 | 53 | Vulvar tumor | 2,5 | pT2, N0, M1 | Vulva | Vertebrae and pelvic bones. |
| Arnould et al. | 2002 | 59 | Abdominal and pelvic pain | - | - | Ovarian granulosa cell tumor | - |
| Alvarez et al. | 2003 | 69 | Metrorrhagia | - | pT2, N1, M0 | Endometrial polyps and uterus | Skull and spine. |
| Ogino et al. | 2003 | 49 | Abnormal genital bleeding | 3.5 | pT2, N0, M0 | Cervix | Pancreas, stomach |
| Rau et al. | 2003 | 55 | Abdominal pain | 5 | pT4, N1, M0 | Cervix | - |
| Blecharz et al. | 2004 | 46 | Enlarged uterus | 1 | pT1c, N2 | Uterine leiomyoma | Bone |
| Famoriyo et al. | 2004 | 78 | Postmenstrual bleeding | - | NM | Uterus and cervix | - |
| Sheen-Chen et al. | 2004 | 32 | Vulvar tumor | 3 | pT2, N0, M0 | Vulva | - |
| Al-brachim et al. | 2005 | 53 | Vaginal bleeding | NM | pTxN1 | Endometrial polyps | - |
| Lee et al. | 2005 | 76 | Asymptomatic | NM | NM | Uterine leiomyoma, myometrium, endometrial polyps, cervical stroma and soft tissue adjacent to the uterus and the cervix |
- |
| Scopa et al. | 2005 | 50 | Vaginal bleeding | 6 | pT3N3 | Endometrium, endocervix, ovaries, and fallopian tubes. | - |
| Scopa et al. | 2005 | 81 | Vaginal bleeding | 1,6 | pT1c, N3 | Endometrium | - |
| Chen et al. | 2006 | 47 | Poor appetite and abdominal fullness | pT3, N0, M0 | Ovary | - | |
| Erkanli et al. | 2006 | 63 | Asymptomatic | NM | pT2, N3, M0 | Endometrium, cervix, and ovaries. | - |
| Perisic et al. | 2007 | 65 | Asymptomatic | NM | pT2, N1, M0 | Cervix | - |
| Manci et al. | 2008 | 41 | Asymptomatic | 1 | pT1c, N0, M0 | Cervix | - |
| Manipadan et al. | 2008 | 70 | Vaginal bleeding | NM | NM | Endometrial polyps | - |
| Bogliolo et al. | 2009 | 78 | Asymptomatic | 0,9 | pT1b, N2, M1 | Cervix | - |
| Ustaalioglu et al. | 2009 | 56 | Vaginal bleeding | NM | pT2, N2, M0 | Endometrium, myometrium, cervix, left uterine tube and left ovary. | - |
| Engelstaedter et al. | 2011 | 64 | Asymptomatic | 4 | pT3, N3, M1 | uterus, adnexa | Liver |
| Hooker et al. | 2011 | 83 | Postmenopausal uterine bleeding | NM | NM | Endometrial polyps, vulva | Pleura, peritoneum, stomach |
| Isci et al. | 2011 | 48 | Increased abdominal girth urinary incontinence | NM | NM | Both the ovaries, tubes, abdominal washing fluid, myometrium, and the huge leiomyoma | Liver, bone |
| Horikawa et al. | 2012 | 52 | abdominal discomfort, polyuria. | 5 | pT2, N3, M1 | Cervix, endometrium | - |
| Komeda et al. | 2012 | 59 | Asymptomatic | 3,8 | pT3, N2, M0 | Uterus | multiple metastases |
| Vicioso et al. | 2013 | 67 | Metrorrhagia | 3,2 | pT2, N2, M0 | Uterus | Left femur, calvarial skull, axial skeleton, and rib cage. |
| Alligood-Percoco et al. | 2015 | 36 | Abdominal bloating | NM | NM | Ovaries / vulva | Peritoneum, lymph nodes |
| Bezpalko et al. | 2015 | 47 | Vaginal bleeding | 1,8 | pT1c, Nx, M1 | Endometrium | gallbladder, bone marrow, lymph nodes, and peritoneum. |
| Lokadasan et al. | 2015 | 49 | Menorrhagia | NM | NM | Endometrium, myometrium, fibroid, cervix, bilateral ovaries. | - |
| Lokadasan et al. | 2015 | 49 | Abdominal distention, pain | NM | pT3, N3, M0 | Cervix, bilateral adnexa | Omentum |
| Toyoshima et al. | 2015 | 62 | Abdominal compression. | NM | pT2, N1, M0 | Uterine leiomyomata, myometrium | - |
| Waks et al. | 2015 | 53 | Postcoital bleeding | NM | pT2, N1, M0 | Cervix, corpus uteri | Pelvic and para-aortic lymph nodes |
| Lai et al. | 2016 | 54 | Asymptomatic | NM | pT3, N3, M0 | Endometrium | Stomach |
| Makris et al. | 2016 | 45 | Asymptomatic | NM | pT2, N1, M0 | Ovary | - |
| Martinez et al. | 2016 | 40 | Vaginal bleeding | NM | NM | Endometrium | Orbit, bone |
| Martinez et al. | 2016 | 48 | Asymptomatic | NM | NM | Endometrium, myometrium | - |
| Akhtar et al. | 2017 | 62 | Asymptomatic | 2,9 | NM | Endometrium, cervix | - |
| Bennett et al. | 2017 | 53 | Asymptomatic | NM | Bilateral ovaries | - | |
| Bennett et al. | 2017 | 64 | Vaginal fullness and discomfort | NM | Bilateral ovaries, uterus, fallopian tubes | - | |
| Bennett et al. | 2017 | 54 | Adnexal mass | NM | - | - | |
| Bennett et al. | 2017 | 41 | Adnexal mass | NM | Bilateral ovaries, fallopian tube | - | |
| Bennett et al. | 2017 | 48 | NM | NM | Left ovary, uterine serosa | - | |
| Razia et al. | 2017 | 58 | Abnormal uterine bleeding | NM | NM | Endometrial polyps, uterine leiomyoma, cervix | - |
| Seo et al. | 2017 | 46 | Vaginal bleeding | 4 | pT1, N0, M0 | Uterine corpus, endocervix, left ovary | - |
| Aytekin et al. | 2018 | 38 | Vaginal bleeding | NM | pT2, N3, M0 | Uterus, bilateral ovaries, vaginal cuff, cervix | - |
| Briki et al. | 2018 | 50 | Postmenopausal uterine bleeding | NM | pT2, N1, M0 | Endometrium | - |
| Franko-Marquez et al. | 2019 | 86 | Abnormal uterine bleeding. | NM | NM | Endometrium | - |
| Kachi et al. | 2019 | 58 | Altered bowel habits, abdominal pain, bloating. | NM | NM | Bilateral ovaries | large bowel, appendix |
| Fontinele et al. | 2019 | 57 | Abnormal uterine bleeding | 10 | ypT0, N0, M0 | Cervix | - |
| Abdallah et al. | 2020 | 59 | Lower abdominal pain | 5 | NM | Endometrium, myometrium, leiomyoma, cervix | Scapula |
| Arif et al. | 2020 | 55 | Vaginal bleeding, lower abdominal pain. | NM | NM | Endometrial polyp | - |
| Gomez et al. | 2020 | 69 | Post menopausal bleeding | NM | NM | Endometrium | - |
| Yuan et al. | 2020 | 64 | Asymptomatic | NM | NM | Endometrium, cervix | Bones |
| Akizawa et al. | 2021 | 49 | Abdominal distention | 5 | NM | Ovary | Bones |
| Awazu et al. | 2021 | 66 | Abnormal genital bleeding | NM | NM | Endometrium | Bones |
| Lim et al. | 2021 | 57 | Vaginal bleeding | 5,6 | NM | Uterus, cervix, bilateral ovaries, fallopian tubes | - |
| Kong et al. | 2022 | 64 | Right shoulder pain | 1,5 | pT1c, N3 M0 | Uterus, cervix, bilateral ovaries, fallopian tubes | Bones |
| Li et al. | 2022 | 61 | stomach discomfort | NM | pT1c, N1, M0 | Bilateral ovaries, peritoneum | Stomach |
| Benlghazi et al. | 2024 | 56 | abnormal uterine bleeding | NM | NM | Endometrial polyps | - |
| Faur et al. | 2024 | 82 | abdominal distension and pain | NM | NM | Ovarian fibroma | - |
Abbreviations: FGT: female genital tract; HBSO: hysterectomy and bilateral salpingo-oophorectomy; Met: metastasis; Mo: months; N: No; Neoadj.: neoadjuvant; NM: not mentioned; OM: omentectomy; RT: radiotherapy; Y: Yes.
Table 3.
ER, PR, and Her-2 status and histological grade of the reported cases.
| Authors | Primary tumor | Metastatic tumor | Tumor grade | ||||
| ER status | PR status | HER-2 status | ER status | PR status | HER-2 status | ||
| Aranda et al. | NM | NM | NM | NM | NM | NM | NM |
| Sugiyama et al. | NM | NM | NM | NM | NM | NM | NM |
| Menzin et al. | + | + | NM | + | + | NM | NM |
| Arnould et al. | NM | NM | NM | + | + | NM | NM |
| Alvarez et al. | + | + | NM | + | + | NM | NM |
| Ogino et al. | - | + | NM | - | + | NM | NM |
| Rau et al. | NM | NM | NM | NM | NM | NM | NM |
| Blecharz et al. | + | + | NM | + | - | NM | NM |
| Famoriyo et al. | NM | NM | NM | NM | NM | NM | NM |
| Sheen-Chen et al. | NM | NM | NM | NM | NM | NM | NM |
| Al-brachim et al. | NM | NM | NM | + | + | NM | NM |
| Lee et al. | NM | NM | NM | + | + | NM | Grade II |
| Scopa et al. | - | + | NM | - | + | + | NM |
| Scopa et al. | NM | NM | NM | + | + | NM | NM |
| Chen et al. | + | + | - | + | + | - | Grade III |
| Erkanli et al. | + | + | - | NM | NM | NM | - |
| Perisic et al. | + | + | NM | NM | NM | NM | Grade II |
| Manci et al. | + | + | - | + | + | + | NM |
| Manipadan et al. | Not done | Not done | Not done | NM | NM | NM | NM |
| Bogliolo et al. | + | + | - | NM | NM | NM | Grade II |
| Ustaalioglu et al. | + | + | - | + | + | - | NM |
| Engelstaedter et al. | + | + | Grade II | ||||
| Hooker et al. | + | + | - | + | - | NM | NM |
| Isci et al. | + | - | - | NM | NM | NM | NM |
| Horikawa et al. | + | + | - | + | NM | NM | NM |
| Komeda et al. | + | + | - | - | - | NM | NM |
| Vicioso et al. | + | + | - | + | - | Grade II | |
| Alligood-Percoco et al. | + | + | NM | + | NM | NM | NM |
| Bezpalko et al. | + | + | - | NM | NM | NM | Grade II |
| Lokadasan et al. | + | + | - | NM | NM | NM | NM |
| Lokadasan et al. | + | + | NM | + | + | NM | Grade II |
| Toyoshima et al. | + | + | + | + | - | NM | NM |
| Waks et al. | + | + | + | + | - | NM | |
| Lai et al. | + | + | - | + | + | - | Grade II |
| Makris et al. | + | + | NM | + | + | NM | NM |
| Martinez et al. | NM | NM | NM | NM | NM | NM | |
| Martinez et al. | NM | NM | NM | NM | NM | NM | NM |
| Akhtar et al. | + | + | - | + | + | NM | NM |
| Bennett et al. | NM | NM | NM | NM | NM | NM | NM |
| Bennett et al. | NM | NM | NM | NM | NM | NM | NM |
| Bennett et al. | NM | NM | NM | NM | NM | NM | NM |
| Bennett et al. | NM | NM | NM | NM | NM | NM | NM |
| Bennett et al. | NM | NM | NM | NM | NM | NM | NM |
| Razia et al. | NM | NM | NM | + | + | + | NM |
| Seo et al. | + | + | NM | + | + | NM | NM |
| Aytekin et al. | + | + | - | NM | NM | NM | NM |
| Briki et al. | + | + | - | NM | NM | NM | NM |
| Franko-Marquez et al. | + | + | + | + | NM | NM | NM |
| Kachi et al. | NM | NM | NM | + | + | NM | NM |
| Silva Fontinele et al. | + | + | - | + | + | - | Grade II |
| Abdallah et al. | + | + | - | + | + | NM | NM |
| Arif et al. | NM | NM | NM | NM | NM | NM | NM |
| Gomez et al. | NM | NM | NM | NM | NM | NM | Grade II |
| Yuan et al. | NM | NM | NM | + | + | - | NM |
| Akizawa et al. | + | + | - | + | NM | NM | NM |
| Awazu et al. | NM | NM | NM | + | + | - | NM |
| Lim et al. | + | + | + | NM | NM | NM | NM |
| Kong et al. | + | - | - | + | + | - | NM |
| Li et al. | NM | NM | NM | NM | NM | NM | NM |
| Benlghazi et al. | + | + | - | + | - | - | Grade III |
| Faur et al. | NM | NM | NM | NM | NM | NM | NM |
Abbreviations: ER: estrogen receptors; NM: not mentioned; PR: progesterone receptors.
Table 4.
Treatment and follow-up features of the reported cases.
| Authors | Surgery | CHT | RT | Hormonal therapy | Interval to Met (Mo) |
Second-Line Therapy |
Outcome |
| Aranda et al. | NM | NM | NM | NM | 36 | HBSO | NM |
| Sugiyama et al. | MRM | 5-FU, mitomycin C, and pirarubicin |
N | Tamoxifen | Concomitant | - | 48 ANED |
| Menzin et al. | Quadrantectomy, ALND, and partial vulvectomy. | NM | N | Tamoxifen | Concomitant | - | 18 AWD |
| Arnould et al. | NM | CHT | Y | Tamoxifen | 48 | Bilateral oophorectomy, letrozole | 60 ANED |
| Alvarez et al. | MRM | 6 x CMF | Y | Tamoxifen | 48 | Biopsy | NM |
| Ogino et al. | MRM | No | N | Tamoxifen | 128 | Pancreatoduodenectomy, HBSO, ADM-TXL CHT and anastrozole. | 136 DOD |
| Rau et al. | MRM | 6x CHT | Y | Tamoxifen | 48 | Patient refused | Lost to follow-up |
| Blecharz et al. | MRM, HBSO | 6 x ADR, CTX, 5-FU. | N | Tamoxifen | Concomitant | Aromatase inhibitors and biphosphonates and palliative radiotherapy of the thoracic and lumbar vertebrae. | 59 AWD |
| Famoriyo et al. | NM | NM | NM | Tamoxifen | NM | NM | NM |
| Sheen-Chen et al. | MRM | 6 x CMF | N | Tamoxifen | 40 | Wide excision of the tumor, cyclophosphamide, epirubicin, and 5-FU. | 40 AWD |
| Al-brachim et al. | MRM | No | N | Tamoxifen | 48 | NM | NM |
| Lee et al. | MRM | CHT | Y | Tamoxifen | 18 | HBSO | |
| Scopa et al. | MRM | 4 x epirubicin | Y | Tamoxifen and LH-RH agonist | 36 | HBSO | 54 DOD |
| Scopa et al. | MRM | 4 x cyclophosphamide and adriamycin. | N | Tamoxifen and LH-RH agonist | 24 | HBSO | 30 DOD |
| Chen et al. | MRM | 6 x CHT | Y | Tamoxifen | 56 | HBSO, partial OM, and pelvic lymph node sampling |
NM |
| Erkanli et al. | MRM | Patient refused CHT | Patient refused RT | - | 8 | HBSO, omentectomy, and pelvic lymphadenectomy. Cyclophosphamide, epirubicin, and 5-FU | 8 AWD |
| Perisic et al. | MRM | 6 x CMF | Y | Tamoxifen | 52 | The patient refused CHT | 72 DOD |
| Manci et al. | quadrentectomy | No | Y | Tamoxifen | 130 | HBSO, pelvic lymphadenectomy, CHT, Femara. | 150 ANED |
| Manipadan et al. | Biopsy | 6 x docetaxel and zoledronic acid | N | No | 2 | Polypectomy | NM |
| Bogliolo et al. | Quadrantectomy, SLNB, endometrial and cervical biopsy. | 6 x 5-FU, epirubicin, cyclophosphamide, and docetaxel | Y | Letrozole | Concomitant | - | 30 AWD |
| Ustaalioglu et al. | MRM | 4 x doxorubicine, cyclophosphamide / 4 x docetaxel | Y | Anastrozole | 36 | HBSO, exemestane | 45 ANED |
| Engelstaedter et al. | HBSO, OM, lumpectomy, ALND. | Navelbine. | N | Tamoxifen | Concomitant | - | 65 ANED |
| Hooker et al. | No | No | N | Letrozole, Tamoxifen, Fulvestrant | 60 | Polypectomy | 72 ANED |
| Isci et al. | No | CHT | N | Letrozole and ibandronate. | 15 | HBSO, CHT | 27 ANED |
| Horikawa et al. | HBSO, MRM | No | N | Anastrozole, S-1 | Concomitant | - | 84 ANED |
| Komeda et al. | MRM | 4 x doxorubicin, cyclophosphamide/ 6 x paclitaxel | N | Letrozole | 15 | The patient refused HBSO, doxorubicin, and cyclophosphamide. | 28 DOD |
| Vicioso et al. | Quadrantectomy, ALND. | 6 x taxotere, adriamycin, and cyclophosphamide. | N | Tamoxifen | 72 | HBSO, letrozole, RT. | 163 AWD |
| Alligood-Percoco et al. | MRM | 4 x doxorubicin, 8 x CMF. | Y | Tamoxifen | 116 / 240 | HBSO, appendectomy, debulking, Taxotere, and Xeloda / Arimidex | 240 AWD |
| Bezpalko et al. | Biopsy | CHT | N | Hormonal therapy | Concomitant | - | 1 DOD |
| Lokadasan et al. | Biopsy | 5-FU, epirubicin, cyclophosphamide | N | Hormonal therapy | Concomitant | - | NM |
| Lokadasan et al. | MRM | 3 x 5-FU, adriamycin, cyclophosphamide / 3 x docetaxel | Y | Tamoxifen | 48 | Carboplatin, gemcitabine. | NM |
| Toyoshima et al. | Breast conserving surgery | 6 x 5-FU, epirubicin, cyclophosphamide. | Y | Anastrozole | 84 | HBSO, exemestane | ANED |
| Waks et al. | Breast conserving surgery, ALND | methotrexate, cyclophosphamide, 5-FU | Y | Tamoxifen | 180 | Biopsy, CHT | NM |
| Lai et al. | MRM | CHT | Y | Tamoxifen / anastrozole / exemestane | 84 | endometrial biopsy, CHT | AWD |
| Makris et al. | Lumpectomy, ALND | 6 x docetaxel, doxorubicin, cyclophosphamide | Y | No | 24 | HBSO, omentectomy, peritoneal biopsies, 6 x carboplatin, paclitaxel | 18 ANED |
| Martinez et al. | MRM, endometrial biopsy | CHT | N | Tamoxifen | Concomitant | - | |
| Martinez et al. | MRM | CHT | Y | Tamoxifen | 18 | HBSO | NM |
| Akhtar et al. | Biopsy | Patient refused CHT | N | N | Concomitant | - | Lost to follow-up |
| Bennett et al. | NM | NM | NM | NM | NM | ΝΜ | 49 DOD |
| Bennett et al. | NM | NM | NM | NM | NM | ΝΜ | 84 AWD |
| Bennett et al. | NM | NM | NM | NM | NM | ΝΜ | 9 DOD |
| Bennett et al. | NM | NM | NM | NM | NM | ΝΜ | NM |
| Bennett et al. | NM | NM | NM | NM | NM | ΝΜ | NM |
| Razia et al. | Surgery | doxifluridine, cyclophosphamide, docetaxel | Y | Goserelin acetate, Tamoxifen, toremifene citrate | 108 | HBSO, a partial colectomy, an aromatase inhibitor | ANED |
| Seo et al. | Breast conserving surgery, ALND | 2 x neoadj. Cyclophosphamide, adriamycin 4 x adj. cyclophosphamide, adriamycin |
Y | Goserelin, TamoxifenTamoxifenTamoxifen | 24 | HBSO | ANED |
| Aytekin et al. | MRM | 4 x adriamycin, cyclophosphamide / 12 x paclitaxel | Y | tamoxifen and luteinizing hormone-releasing hormone analog | 10 | HBSO, CHT | 16 DOD |
| Briki et al. | MRM | CHT | Y | Tamoxifen | 24 | HBSO | NM |
| Franko-Marquez et al. | MRM | CHT | N | NM | 360 | Biopsy, CHT | NM |
| Kachi et al. | MRM | 9 x CHT | Y | Tamoxifen | 60 | Anterior resection, BO, appendectomy | NM |
| Silva Fontinele et al. | MRM | Neoadj. 4x doxorubicin, cyclophosphamide/ 12 x paclitaxel | Y | Tamoxifen | 39 | HBSO, anastrozole | 66 ANED |
| Abdallah et al. | HBSO | 6 x cycolphosphamide, epirubicin 5-FU | N | Hormonal therapy | Concomitant | - | NM |
| Arif et al. | NM | NM | N | Tamoxifen | 84 | HBSO | 96 ANED |
| Gomez et al. | MRM | NM | NM | Tamoxifen | 60 | Biopsy | NM |
| Yuan et al. | MRM | CHT | Y | Hormonal therapy | 132 | Biopsy | ANED |
| Akizawa et al. | HBSO, OM | Palbociclib, denosumab | N | Letrozole | Concomitant | - | ANED |
| Awazu et al. | Surgery | CHT | NM | aromatase inhibitors/tamoxifen | 276 | HBSO, partial OM, a biopsy of the peritoneum, fulvestrant, toremifene citrate, and tegafur | 308 ANED |
| Lim et al. | MRM | 4 x cyclophosphamide, adriamycin, 5-FU/ 4 x taxotere | Y | Tamoxifen | 30 | HBSO, fulvestrant, ribociclib | NM |
| Kong et al. | MRM | 4 x epirubicin, cyclophosphamide / 4 x paclitaxel | patient refused RT | Letrozole | 29 | Radiotherapy, zoledronate / HBSO, 6 x paclitaxel, capecitabine, radiotherapy, zoledronate / 2 x gemcitabine, cisplatin | 49 DOD |
| Li et al. | MRM | 6 x docetaxel, doxorubicin, cyclophosphamide | Y | Anastrozole | 36 | hyperthermic perfusion chemotherapy (paclitaxel) | ANED |
| Benlghazi et al. | MRM | 3 x Epirubicine, cyclophosphamide, 5FU / 3 x Docetaxel | Y | Tamoxifen | 60 | HBSO, hormonal treatment | 78 ANED |
| Faur et al. | NM | NM | NM | NM | NM | NM | NM |
Abbreviations: Adj.: Adjuvant; Adriamycin-Cyclophosphamide (AC), ADR: Adriamycin; ADM-TXL: doxorubicin (ADM), paclitaxel (TXL); ANED: Alive no evidence of disease; AWD: Alive with disease; BO: Bilateral oophorectomy; Cyclophosphamide-adriamycin-5-Fluorouracil (CAF); Cyclophosphamide- Methotrexate- 5 Fluorouracil (CMF); CHT: chemotherapy (not specified); CTX: Cyclophosphamide; Docetaxel-doxorubicin- cyclophosphamide (TAC); DOD: Died of disease; Epirubicin-Cyclophosphamide (EC); Epirubicin-cyclophosphamide-5FU (FEC); FGT: female genital tract; 5-FU: 5 Fluorouracil; HBSO: hysterectomy and bilateral salpingo-oophorectomy; Met: metastasis; Mo: months; N: No; Neoadj.: neoadjuvant; NM: not mentioned; OM: omentectomy; RT: radiotherapy; Y: Yes.
Table 5.
Role of the study variables in patient overall survival. HR: Hazard Ratio, CI: Confidence interval, N: Number of valid cases.
Table 5.
Role of the study variables in patient overall survival. HR: Hazard Ratio, CI: Confidence interval, N: Number of valid cases.
| Characteristic | HR and 95% CI | p-value | N |
| Primary tumor ER status | 0.41 (0.08-2.18) | 0.283 | 22 |
| Primary tumor PR status | 0.27 (0.03-2.6) | 0.223 | 22 |
| Secondary tumor ER status | 0.13 (0.02-0.8) | 0.01 | 18 |
| Secondary tumor PR status | 2.04 (0.23-18.39) | 0.518 | 16 |
| HER-2 status | 1.73 (0.11-27.89) | 0.695 | 7 |
| Stage pN | 4.91 (0.2-118.15) | 0.31 | 20 |
| Stage pM | 0.64 (0.07-5.76) | 0.686 | 18 |
| Other metastasis | 0.82 (0.22-3.03) | 0.76 | 31 |
| RT | 0.72 (0.17-3.02) | 0.65 | 27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



