Submitted:
13 August 2025
Posted:
13 August 2025
You are already at the latest version
Abstract
HTLV-1/2 coinfection in people with HIV (PWH) has been little studied in the Peruvian Amazon, an endemic area for both viruses. We aimed to estimate its prevalence and describe the main clinical and epidemiological features of co-infected individuals. We conducted a prospective, cross-sectional study (October–December 2023) at the Divi-sion of Infectious Diseases and Tropical Medicine from the Regional Hospital of Loreto, in Iquitos. We performed a screening test (recombinant HTLV I+II ELISA) and confirm the results with INNO-LIA. Among 293 PWH analyzed, 14 (4.1%) were HTLV positive: 1 was HTLV-1 (0.3%; 95% CI: 0.06-0.9), 11 were HTLV-2 (3.8%; 95% CI: 2.1-6.8) and 2 were non-typeable (0.7%; 95% CI: 0.1-2.7). Compared with HIV-monoinfected indi-viduals, coinfected patients were older (55 vs. 39 years; p=0.001) and more often had low education (35.7% vs. 15.4%; p=0.05). In conclusion, HIV–HTLV-2 coinfection is relatively common (~4%) in the Peruvian Amazon, particularly among older, ru-ral-born individuals, underscoring the need for targeted screening and prevention strategies in endemic areas.
Keywords:
HTLV
; HTLV-2
; human T-cell lymphotropic virus
; human immunodeficiency virus
; HIV
; Peru
; Amazon
1. Introduction
Infection with Human T-Cell Lymphotropic Virus Types I and II (HTLV-1/2) represents an underestimated public health issue, with a heterogeneous geographic distribution and a significant burden in endemic areas of Latin America, particularly in Brazil and Peru. HTLV-1 affects millions of people worldwide and is associated with severe conditions such as adult T-cell leukemia/lymphoma and HTLV-1–associated myelopathy. In contrast, HTLV-2, which is considered less pathogenic, predominates among Indigenous populations and people who inject drugs [1,2,3,4,5,6,7].
HTLV-1/2 is primarily transmitted through sexual contact, vertical transmission (particularly via breastfeeding), blood transfusions, and, in certain regions, through exposure to contaminated blood through unsterile practices, such as scarification rituals or poorly hygienic procedures. These transmission routes are shared with the human immunodeficiency virus (HIV). HTLV/HIV coinfection may alter the natural history of both infections, potentially accelerating progression to AIDS and increasing susceptibility to opportunistic infections [1,3,8,9].
In Brazil, the prevalence of HTLV/HIV coinfection varies by region and risk group, with reported rates ranging from 1.3% to 7% among people living with HIV (PWH). HTLV-1a is the predominant subtype in the Amazon region, while a high endemicity of HTLV-2 has been observed among Indigenous populations and drug users. In Peru, although data are more limited, HTLV-1/2 infection has been documented in both urban and rural populations, with transmission hotspots in the Amazon region and evidence of circulation among Indigenous communities and individuals with similar risk factors to those reported in Brazil [4,5,6,8,10,11,12].
The Peruvian Amazon is a key area for HIV transmission, with the second-highest cohort of patients receiving antiretroviral treatment after Lima [13]. Some studies have also revealed very high rates in isolated indigenous populations, mainly due to sexual exposure without protection (including polygamy and homosexual practices), as there are little knowledge about the infection [14,15]. The absence of systematic screening programs in HIV and limited clinical awareness hinder detection and control of the infection, highlights the urgent need to strengthen epidemiological surveillance and research efforts in the region [1,2,3,4].
The aim of this study is to assess the prevalence of HTLV-1/2 infection in a pilot sample of PWH in the Peruvian Amazon, describe the clinical and epidemiological characteristics of coinfected individuals, and analyze differences compared to HIV-monoinfected patients.
2. Materials and Methods
2.1. Study Design and Setting
A prospective, cross-sectional study was conducted among PWH who were receiving care at the Division of Infectious Diseases and Tropical Medicine of Regional Hospital of Loreto “Felipe Santiago Arriola Iglesias”. The study period was from October 20, 2023, to December 31, 2023.
2.2. Study Population and Enrollment Procedures
Adults aged 18 years and older with confirmed HIV infection who were receiving outpatient care at the Regional Hospital of Loreto were eligible for inclusion. After providing informed consent, participants completed a semi-structured oral interview that collected data on demographics, clinical history and potential epidemiological risk factors. After that, a blood sample was obtain.
Blood serum samples were frozen at –20°C until serological testing could be performed. The presence of antibodies against HTLV-1/2 was initially screened using an ELISA assay (HTLV I+II ELISA recombinant v.4.0, Wiener Lab, Rosario, Argentina). A result was considered positive when the optical density value exceeded the negative control by 0.200, according to the manufacturer’s instructions. Serum samples from the 15 individuals who screened positive for HTLV were thawed and applied to Whatman filter paper for shipment to the HTLV reference laboratory in Madrid, Spain. Confirmatory testing was performed there using the INNO-LIA HTLV I/II score (Fujirebio, Japan). Besides, a serological testing for Strongyloides stercoralis was conducted using the Strongyloides IgG IVD-ELISA kit (DRG Instruments GmbH, Marburg, Germany).
Those who were positives for HTLV 1/2 were contacted again for conducting a more comprehensive interview on risk factors for transmission including the origin of their parents.
2.3. Data Analysis
Categorical variables were summarized as frequencies and percentages, while continuous variables were expressed as medians and interquartile ranges (IQRs). Ninety-five percent confidence intervals (95% CIs) were calculated using the Newcombe method. Comparisons between categorical variables were performed using the Chi-square test, and continuous variables were analyzed using the Mann–Whitney U test, given the non-normal distribution. Age was categorized into two groups: <P75 (15–49 years) and ≥P75 (≥50 years). Risk factors associated with HTLV positivity were explored using bivariate analysis, with odds ratios (ORs) used to quantify associations. Statistical analyses were performed via IBM SPSS Statistics version SPSS 22.0 (IBM, Armonk, EEUU).
2.4. Ethical Considerations
The study protocol was approved by the Ethics Committee of the Regional Hospital of Loreto in Iquitos, Peru (EXP: ID-018-CIEI-2023) and by the Ethics and Research Integrity Committee of Miguel Hernández University of Elche, Spain (DMC.JMRR.230908). Written informed consent was obtained from all participants. Confidentiality of data was strictly maintained, and results were only disclosed to each participant’s HIV care provider, who ensured appropriate follow-up and treatment.
3. Results
3.1. Overview of the Study Population
A total of 293 PWH were included in the study, of whom 66.9% were male, with a median age of 39 years (IQR: 29-47). Of the participants, 16.7% had no formal education or had only attended primary school, 20.4% had received a blood transfusion, 94.5% had been breastfed, and 89.9% acquired HIV through sexual transmission. The main characteristics of the population are described in Table 1.
3.2. HTLV Subtypes
15 patients tested positive for HTLV during screening. Of them, 14 (4.1%) were definitively confirmed: 1 was HTLV-1 (0.3% 95% CI 0.06-.9), 11 were HTLV-2 (3.8%, 95% CI 2.1-6.8) and 2 (0.7%, 95% CI 0.1-2.7) were non-typeable by INNO-LIA HTLV I/II score (Figure 1).
3.3. Description of Co-Infection HTLV-HIV
Of the 14 patients confirmed positive for HTLV, the medium age was 55 years (IQR: 52-61), and > 85% was older than 50 years. All but one were mestizos (92.9%), while one patient was of the Kukuma race, a tribe that lives on the Marañón River inside Pacaya Samiria National Reserve (Figure 2). The parents of 6 of 12 patients with information available (50%) came from the tributaries of Amazon River, in southern Iquitos, while the origin of one family was Pebas, in the part of the Amazon River that heads towards the border with Brazil, in northern Iquitos. 4 of the patients had parents from Iquitos and 2 had no recorded data on their origin due to loss to follow-up.
All but 1 (92.9%) had been breastfed. 3 (21.8%) had received a blood transfusion and only 1 (7.1%) referred scarification practices. 4 (28.6%) patients had non-heterosexual sexual practices or more than 5 sexual partners. The characteristics about HIV-HTLV coinfection is presented in Table 2.
3.4. Differences HTLV Positive vs. HTLV Negative
Table 1 presents the differences between PWH with positive and negative HTLV-1/2 serology. In the univariate analysis, the risk factors associated with HTLV-1/2 positivity in the screening were age ≥ 50 years (85.7% vs. 21.5%) (p=0.001) (OR: 21.9; 95%CI 4.77-100) and having no formal education or only attending primary school (35.7% vs. 15.4%) (p=0.05) (OR: 2.96 95%CI:0.95-9.27).
4. Discussion
This study confirms the relevance of HTLV-HIV coinfection in patients from the Peruvian Amazon, where HTLV-2 predominates, in contrast to other regions of South America and the world where HTLV-1 is more frequent. Two distinct epidemiological patterns of HTLV-2/HIV coinfection have been described: one primarily in Europe associated with people who inject drugs [16], and another in Latin America, especially in Brazil and Peru, where the prevalence of HTLV-2 among people with HIV is variable and can exceed 3% in certain cohorts [1,7,9,10,11,12,17,18,19], especially among indigenous populations in Amazonian areas of Brazil and Peru, even if it has also been found in urban populations.
In Peru, the Shipibo-Konibo ethnic group (from the Peruvian Amazon) has been reported to have a high prevalence of HTLV-1 (5.7%) and HTLV-2 (3.8%) [20]. In other indigenous communities of the Peruvian Amazon, seroprevalence rates of 4.54% for HTLV-1 and 2.38% for HTLV-2 have been documented [21]. Similarly, cross-sectional studies in the Brazilian Amazon have shown a higher prevalence of HTLV-2, with seroprevalence rates ranging from 0% to 40% [7]. In general, the overall prevalence of HTLV-2 infection in Brazil ranges from 5.7% [22] to 8.1% [5]. Abreu et al. reported a prevalence of HTLV-2 of 18.5% and HTLV-1 of 0.13% in 1,452 individuals from the Kayapó ethnic group, and found evidence of intrafamilial transmission in 42.7% of cases [5]. The variability in reported prevalence rates in the literature reflects differences in diagnostic methods, inclusion criteria, and the representativeness of the studied populations. In the Peruvian Amazon, the high proportion of indeterminate INNO-LIA HTLV I/II results underscores the need for confirmatory molecular testing and cautious interpretation of serological results, in line with the recommendations of the Infectious Diseases Society of America and the American Society for Microbiology [21,22]. Additionally, the lack of systematic screening and underreporting hinder precise estimation of disease burden and the identification of emerging risk factors [7,19,23].
The older age observed in patients with HTLV-HIV coinfection has been observed in previous studies [24]. This may be due to the transmission pattern of HTLV-2, which may be favored by certain practices that were more frequently practiced in indigenous or marginal urban communities some decades [25]. Besides, HTLV-2 has lower rates of sexual transmission than HTLV-1 and HIV, with a lower potential for spreading in highly mobile populations with risky sexual behavior, but greater for spreading in those with longer periods of exposure to cumulative risk factors [24].
Although at least half of the patient’s relatives came from rural areas from the Amazonian rivers, the most frequent origin was rural communities in the south of Iquitos (Marañón and Ucayali Rivers), with the Amazon River on its way to Brazil being less common, which could reinforce the idea of a persistent niche of contagion in the Peruvian Amazon [1,4,21].
The clinical course of HTLV-2/HIV coinfection is heterogeneous. Although HTLV-2 is associated with lower pathogenicity than HTLV-1, some studies suggest that coinfection may modulate HIV progression, with reports of “long-term non-progressor” phenotypes and lower HIV proviral load in individuals coinfected with HTLV-2, possibly mediated by increased CD8+ T cell cytotoxic activity. However, the evidence regarding the clinical impact of coinfection remains controversial and is limited by study heterogeneity and the lack of longitudinal follow-up [17,21].
One of the main strengths of this study is its focus on epidemiological surveillance strategies for HTLV and HIV coinfection, particularly in a region where such data are scarce. By addressing this neglected area, the study contributes valuable information for public health decision-making and future research planning in the Amazon region. However, the study has several limitations. First, the small sample size limits the generalizability of the findings. Second, confirmatory testing for HTLV infection were conducted using frozen serum samples applied to Whatman filter paper—a method that lacks full standardization and validation. Another limitation is the absence of molecular characterization of HTLV subtypes, which prevents a more detailed understanding of the virological features of the coinfection. Additionally, given the cross-sectional design, it was not possible to assess the longitudinal clinical impact of the coinfection, particularly the HTLV role in HIV disease progression and related complications.
In conclusion, our screening study in the Peruvian Amazon highlights a significant prevalence of HIV–HTLV coinfection, particularly with HTLV-2. Risk factors for coinfection include age over 50 years. However, awareness and identification of HTLV coinfection remain important, as they can guide appropriate patient follow-up and care strategies. Future multicenter studies with larger cohorts and long-term follow-up are needed to better define the clinical relevance of both HTLV-1 and HTLV-2 in people living with HIV, especially in endemic areas such as the Amazon region.
Author Contributions
Conceptualization, S.O.R., J.M.R.R. and M.C.M.; methodology, S.O.R., M.C.M., C.D.M., V.S., J.M.R.R.; software, S.O.R.; validation, S.O.R., J.M.R.R. and M.C.M.; formal analysis, S.O.R. and J.M.R.R.; investigation, S.O.R., S.M.C., and C.D.M.; resources, S.O.R.; data curation, S.O.R. and J.M.R.R.; writing—original draft preparation, S.O.R. and J.M.R.R.; writing—review and editing, S.O.R., M.C.M., C.D.M., V.P.C., S.M.C., V.S., E.M. and J.M.R.R.; visualization, J.M.R.R.; supervision, M.C.M., C.D.M, V.S and J.M.R.R.; project administration, S.O.R., M.C.M., V.P.C., E.M. and J.M.R.R.; funding acquisition, J.M.R.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Miguel Hernández University of Elche (UMH), grant number UMH-GVA 2022/0005; 11-134-4- 2023-0133, Alicante Health and Biomedical Research Institute (ISABIAL), grant number 2024-0181 and Instituto de Salud Carlos III (ISCIII), grant number CM23/00050.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Loreto Regional Hospital, Iquitos, Peru, protocol code ID-018-CIEI-2013, May 11, 2023.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The dataset used and/or analysed during the current study are available in Zenodo Repository, under the ORCID: 10.5281/zenodo.14864472.
Acknowledgments
We want to thank the medical staff of the Infectious Diseases Service in Loreto Regional Hospital and Iquitos Hospital, together with the laboratory staff of LIPNAA-CIRNA and Asociación Civil Selva Amazónica for the support on the field.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| HTLV | Human T-Cell Lymphotropic Virus |
| HIV | Human Immunodeficiency Virus |
| PWH | People with HIV |
| ELISA | Enzyme-Linked Immunosorbent Assay |
| IQRs | Interquartile Ranges |
| CIs | Confidence Intervals |
| ART | Anti-retroviral therapy. |
References
- Branda, F.; Romano, C.; Pavia, G.; Bilotta, V.; Locci, C.; Azzena, I.; Deplano, I.; Pascale, N.; Perra, M.; Giovanetti, M.; et al. Human T-Lymphotropic Virus (HTLV): Epidemiology, Genetic, Pathogenesis, and Future Challenges. Viruses 2025, 17, 664. [CrossRef]
- Legrand, N.; McGregor, S.; Bull, R.; Bajis, S.; Valencia, B.M.; Ronnachit, A.; Einsiedel, L.; Gessain, A.; Kaldor, J.; Martinello, M. Clinical and Public Health Implications of Human T-Lymphotropic Virus Type 1 Infection. Clin. Microbiol. Rev. 2022, 35, e0007821. [CrossRef]
- Solorzano-Salazar, D.M.; Hernández-Vásquez, A.; Visconti-Lopez, F.J.; Azañedo, D. Research on HTLV-1 and HTLV-2 in Latin America and the Caribbean over the last ten years. Heliyon 2023, 9, e13800. [CrossRef]
- Carneiro-Proietti, A.B.F.; Catalan-Soares, B.; Proietti, F.A. Human T Cell Lymphotropic Viruses (HTLV-I/II) in South America: Should It Be a Public Health Concern?. J. Biomed. Sci. 2002, 9, 587–595. [CrossRef]
- Abreu, I.N.; Lima, C.N.C.; Sacuena, E.R.P.; Lopes, F.T.; Torres, M.K.d.S.; dos Santos, B.C.; Freitas, V.d.O.; de Figueiredo, L.G.C.P.; Pereira, K.A.S.; de Lima, A.C.R.; et al. HTLV-1/2 in Indigenous Peoples of the Brazilian Amazon: Seroprevalence, Molecular Characterization and Sociobehavioral Factors Related to Risk of Infection. Viruses 2022, 15, 22. [CrossRef]
- Oliveira-Filho, A.B.; Araújo, A.P.S.; Souza, A.P.C.; Gomes, C.M.; Silva-Oliveira, G.C.; Martins, L.C.; Fischer, B.; Machado, L.F.A.; Vallinoto, A.C.R.; Ishak, R.; et al. Human T-lymphotropic virus 1 and 2 among people who used illicit drugs in the state of Pará, northern Brazil. Sci. Rep. 2019, 9, 1–10. [CrossRef]
- Ishak, R.; Ishak, M.d.O.G.; Azevedo, V.N.; Machado, L.F.A.; Vallinoto, I.M.C.; Queiroz, M.A.F.; Costa, G.d.L.C.; Guerreiro, J.F.; Vallinoto, A.C.R. HTLV in South America: Origins of a silent ancient human infection. Virus Evol. 2020, 6, veaa053. [CrossRef]
- Vieira, B.A.; Bidinotto, A.B.; Dartora, W.J.; Pedrotti, L.G.; de Oliveira, V.M.; Wendland, E.M. Prevalence of human T-lymphotropic virus type 1 and 2 (HTLV-1/-2) infection in pregnant women in Brazil: a systematic review and meta-analysis. Sci. Rep. 2021, 11, 1–10. [CrossRef]
- Galetto, L.R.; Lunge, V.R.; Béria, J.U.; Tietzmann, D.C.; Stein, A.T.; Simon, D. Short Communication: Prevalence and Risk Factors for Human T Cell Lymphotropic Virus Infection in Southern Brazilian HIV-Positive Patients. AIDS Res. Hum. Retroviruses 2014, 30, 907–911. [CrossRef]
- Alencar, S.P.; Souza, M.d.C.; Fonseca, R.R.d.S.; Menezes, C.R.; Azevedo, V.N.; Ribeiro, A.L.R.; Lima, S.S.; Laurentino, R.V.; Barbosa, M.d.A.d.A.P.; Freitas, F.B.; et al. Prevalence and Molecular Epidemiology of Human T-Lymphotropic Virus (HTLV) Infection in People Living With HIV/AIDS in the Pará State, Amazon Region of Brazil. Front. Microbiol. 2020, 11, 572381. [CrossRef]
- Etzel, A.; Shibata, G.Y.; Rozman, M.; Jorge, M.L.S.G.; Damas, C.D.; Segurado, A.A.C. HTLV-1 and HTLV-2 Infections in HIV-Infected Individuals From Santos, Brazil: Seroprevalence and Risk Factors. Am. J. Ther. 2001, 26, 185–190. [CrossRef]
- Caterino-De-Araujo, A.; Sacchi, C.T.; Gonçalves, M.G.; Campos, K.R.; Magri, M.C.; Alencar, W.K.; the Group of Surveillance and Diagnosis of HTLV of São Paulo (GSuDiHTLV-SP) Short Communication: Current Prevalence and Risk Factors Associated with Human T Lymphotropic Virus Type 1 and Human T Lymphotropic Virus Type 2 Infections Among HIV/AIDS Patients in São Paulo, Brazil. AIDS Res. Hum. Retroviruses 2015, 31, 543–549. [CrossRef]
- Tattsbridge, J.; Wiskin, C.; de Wildt, G.; Llavall, A.C.; Ramal-Asayag, C. HIV understanding, experiences and perceptions of HIV-positive men who have sex with men in Amazonian Peru: a qualitative study. BMC Public Heal. 2020, 20, 1–17. [CrossRef]
- Zavaleta, C.; Fernández, C.; Konda, K.; Valderrama, Y.; Vermund, S.H.; Gotuzzo, E. HIGH PREVALENCE OF HIV AND SYPHILIS IN A REMOTE NATIVE COMMUNITY OF THE PERUVIAN AMAZON. Am. J. Trop. Med. Hyg. 2007, 76, 703–705. [CrossRef]
- Bartlett, E.C.; Zavaleta, C.; Fernández, C.; Razuri, H.; Vilcarromero, S.; Vermund, S.H.; Gotuzzo, E. Expansion of HIV and syphilis into the Peruvian Amazon: a survey of four communities of an indigenous Amazonian ethnic group. Int. J. Infect. Dis. 2008, 12, e89–e94. [CrossRef]
- Quiros-Roldan, E.; Moretti, F.; Torti, C.; Casari, S.; Castelli, F.; Beltrame, A.; Carosi, G. HIV/HTLV Co-infection: Frequency and Epidemiological Characteristics among Patients Admitted to an Italian Hospital. Infection 2003, 31, 172–173. [CrossRef]
- Islam, N.; Mili, M.A.; Jahan, I.; Chakma, C.; Munalisa, R. Immunological and Neurological Signatures of the Co-Infection of HIV and HTLV: Current Insights and Future Perspectives. Viruses 2025, 17, 545. [CrossRef]
- Pereira, F.M.; Santos, F.L.N.; Silva, Â.A.O.; Nascimento, N.M.; Almeida, M.d.C.C.; Carreiro, R.P.; Galvão-Castro, B.; Grassi, M.F.R. Distribution of Human Immunodeficiency Virus and Human T-Leukemia Virus Co-infection in Bahia, Brazil. Front. Med. 2022, 8, 788176. [CrossRef]
- La Rosa, A.M.; Zunt, J.R.; Peinado, J.; Lama, J.R.; Ton, T.G.N.; Suarez, L.; Pun, M.; Cabezas, C.; Sanchez, J.; Peruvian HIV Sentinel Surveillance Working Group Retroviral Infection in Peruvian Men Who Have Sex with Men. Clin. Infect. Dis. 2009, 49, 112–117. [CrossRef]
- Abad-Fernández, M.; Hernández-Walias, F.J.; de León, M.J.R.; Vivancos, M.J.; Pérez-Elías, M.J.; Moreno, A.; Casado, J.L.; Quereda, C.; Dronda, F.; Moreno, S.; et al. HTLV-2 Enhances CD8+ T Cell-Mediated HIV-1 Inhibition and Reduces HIV-1 Integrated Proviral Load in People Living with HIV-1. Viruses 2022, 14, 2472. [CrossRef]
- Medeot, S.; Nates, S.; Recalde, A.; Gallego, S.; Maturano, E.; Giordano, M.; Serra, H.; Reategui, J.; Cabezas, C. Prevalence of antibody to human T cell lymphotropic virus types 1/2 among aboriginal groups inhabiting northern Argentina and the Amazon region of Peru.. Am. J. Trop. Med. Hyg. 1999, 60, 623–629. [CrossRef]
- Maloney, E.M.; Biggar, R.J.; Neel, J.V.; Taylor, M.E.; Hahn, B.H.; Shaw, G.M.; Blattner, W.A. Endemic Human T Cell Lymphotropic Virus Type II Infection among Isolated Brazilian Amerindians. J. Infect. Dis. 1992, 166, 100–107. [CrossRef]
- Fani, M.; Rezayi, M.; Meshkat, Z.; Rezaee, S.A.; Makvandi, M.; Abouzari-Lotf, E.; Ferns, G.A. Current approaches for detection of human T-lymphotropic virus Type 1: A systematic review. J. Cell. Physiol. 2019, 234, 12433–12441. [CrossRef]
- Campos, K.R.; Gonçalves, M.G.; Caterino-De-Araujo, A. Short Communication: Failures in Detecting HTLV-1 and HTLV-2 in Patients Infected with HIV-1. AIDS Res. Hum. Retroviruses 2017, 33, 382–385. [CrossRef]
- Hall, W.W.; Ishak, R.; Zhu, S.W.; Novoa, P.; Eiraku, N.; Takahashi, H.; Ferreira, M.d.C.; Azevedo, V.; Ishak, M.O.G.; Ferreira, O.d.C.; et al. Human T Lymphotropic Virus Type II (HTLV-II): Epidemiology, Molecular Properties, and Clinical Features of Infection. Am. J. Ther. 1996, 13, S204–S214. [CrossRef]
Figure 1.
Flow chart of study participant inclusion and HTLV subtypes.
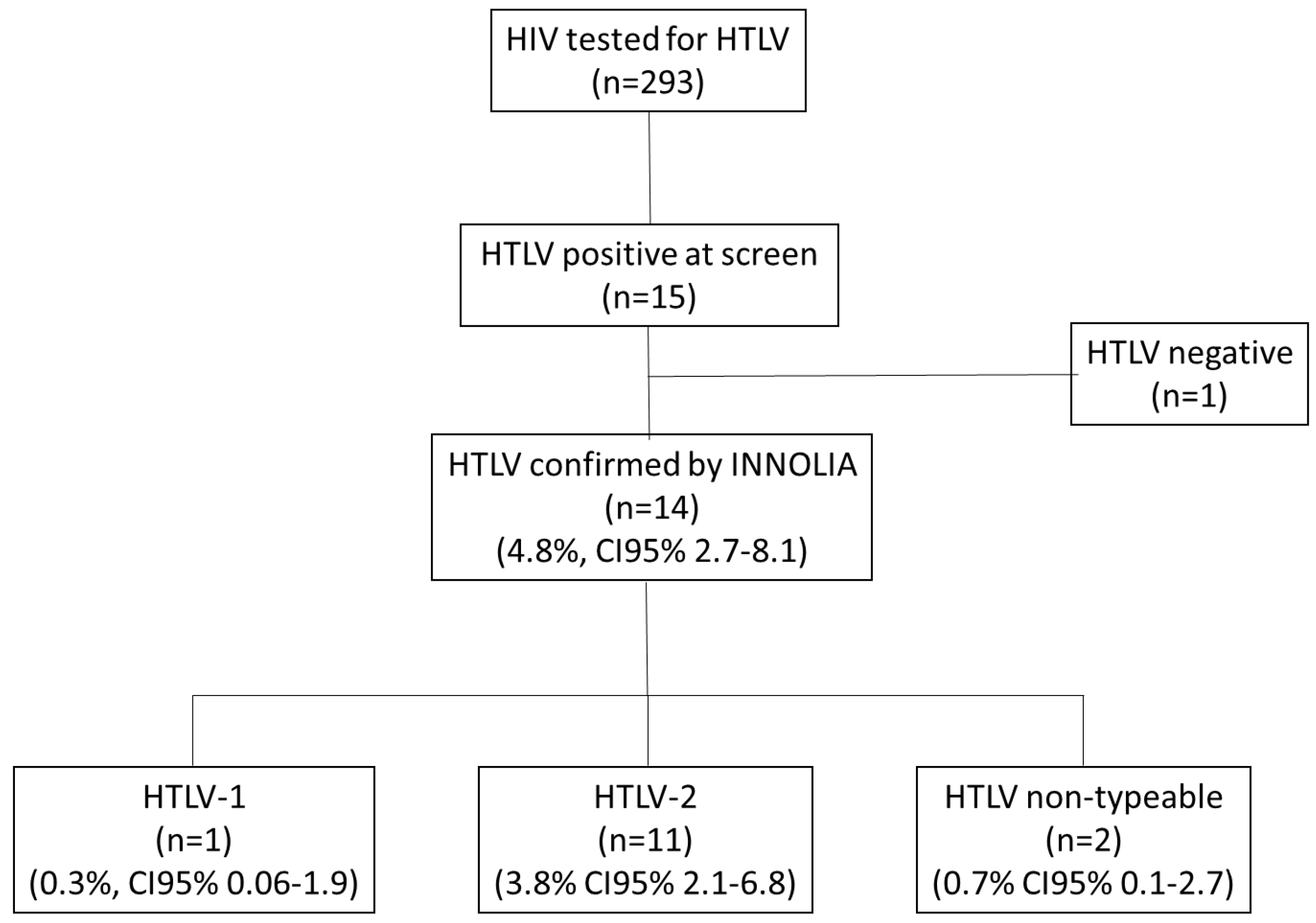

Table 1.
Epidemiological characteristics of study participants (N= 293) and by results of HTLV screening.
Table 1.
Epidemiological characteristics of study participants (N= 293) and by results of HTLV screening.
| Variables |
Overall (N=293) |
HTLV positive (N = 14) |
HTLV negative (N = 279) |
pvalue |
| Epidemiology | ||||
| Sex, male, n (%) | 196 (66.9%) | 9 (64.3) | 187 (66,9) | 0.789 |
| Age, median (IQR), years | 40 (30-49) | 55 (52-61) | 39 (29-47) | <0.001 |
| Age >50 years, n (%) | 72 (24.6) | 12 (85.7) | 60 (21.5) | <0.001 |
| Residence, n (%) | ||||
| Iquitos district | 97 (33.1) | 7 (50.0) | 90 (32.3) | 0.932 |
| Punchana district | 84 (28.7) | 4 (28.6) | 80 (28.7) | |
| San Juan district | 64 (21.8) | 64 (7.1) | 63 (22.6) | |
| Belen district | 33 (11.3) | 2 (14.3) | 31 (11.1) | |
| Outside of Iquitos city | 15 (5.1) | 0 (0.0) | 15 (5.3) | |
| Occupation, n (%) | ||||
| Unemployed or student | 111 (37.9) | 5 (35.7) | 106 (38.0) | 0.54 |
| Self-employment | 100 (34.1) | 5 (35.7) | 95 (34.1) | |
| Cattle, agriculture or construction | 47 (16.0) | 3 (21.4) | 44 (15.8) | |
| Intellectual work | 28 (9.8) | 0 (0.0) | 28 (10.7) | |
| Craft work | 7 (2.4) | 1 (7.1) | 6 (2.2) | |
| Education, n (%) | ||||
| None or only attended primary school | 49 (16.7) | 5 (35.7) | 44 (15.4) | 0.05 |
| Attended secondary school or university | 244 (83.3) | 9 (64.3) | 235 (84.2) | |
| Epidemiological risk factors, n (%) | ||||
| Breastfeeding | 277 (94.5) | 13 (92.9) | 264 (94.6) | 0.55 |
| Blood transfusion | 64 (21.8) | 3 (21.4) | 61 (21.9) | 1.0 |
| Comorbidity, n (%) | ||||
| Diabetes or high blood pressure | 21 (7.2) | 2 (14.3) | 19 (6.8) | 0.26 |
| Digestive disease | 12 (4.1) | 2 (14.39 | 10 (3.6) | 0.10 |
| Other cardiovascular disease | 10 (3.49 | 1 (7.1) | 9 (3.2) | 0.39 |
| Previous infections, n (%) | ||||
| Strongyloides serology positive | 167 (57.0) | 6 (42.9) | 161 (57.7) | 0.29 |
| Tuberculosis test positive | 55 (18.8) | 4 (28.6) | 51 (18.3) | 0.30 |
| Prior Gonorrhea | 33 (11.3) | 3 (21.4) | 30 (10.8) | 0.20 |
| Prior Syphilis | 41 (14.0) | 3 (21.3) | 38 (13.6) | 0.42 |
| Chronic hepatitis | 19 (6.5) | 2 (14.3) | 17 (6.7) | 0.23 |
| Prior Cerebral toxoplasmosis | 13 (4.4) | 0 (0.0) | 13 (4.7) | 0.41 |
| HIV acquisition, n (%) | ||||
| Sexual | 263 (89.9) | 12 (85.7) | 251 (90.0) | 0.71 |
| Vertical | 2 (1.0) | 0 (0.0) | 3 (1.1) | |
| Unknown | 27 (9.2) | 2 (14.39 | 25 (9.0) | |
| Virology, Immunology and Adherence of treatment | ||||
| Nadir CD4+/uL, median (IQR) | 228 (109-363) | 213 (123-360) | 230 (109-363) | 0.91 |
| Current CD4+, median (IQR) | 446 (303-597) | 455 (385-613) | 441 (299-593) | 0.47 |
| Current CD4+ < 200/mL n (%) | 22 (10.7) | 0 (0.0) | 22 (11.3) | 0.61 |
| Current undetectable HIV viral load (< 20 copies/ml), n (%) | 216 (76.3) | 12 (92.39 | 204 (75.6) | 0.31 |
| Poor ART adherence, ≤ 95%), n (%) | 22 (13.4) | 2 (15.4) | 30 (13.3) | 0.89 |
* Statistically significant differences shown in bold. Percentages may not total 100 due to rounding.
Table 2.
Characteristics of patients with HIV-HTLV coinfection.
| N |
Type of HTLV |
Age | Sex | Ethnicity |
Origin of parents |
Breast- feeding |
Sexual behavior/ number of sexual partners |
Non-sterilized proceduresa |
Transfusion |
Living in rural areab |
Chronic hepatitis |
ITS |
CD4 count nadir/last |
HIV viral load |
| 1 | HTLV-1 | 62 | M | Mestizo | Tarapoto | Yes | Transexual / < 5 | No | Yes | No | No | No | 479 / 677 | < 20 |
| 2 | HTLV-2 | 52 | M | Mestizo | Iquitos | Yes | Homosexual / < 5 | No | No | No | No | No | 218 / 674 | < 20 |
| 3 | HTLV-2 | 56 | M | Kukuma | Marañón River | Yes | Homosexual / < 5 | No | No | No | No | No | 287 / 684 | < 20 |
| 4 | HTLV-2 | 60 | F | Mestizo | Nauta | Yes | Heterosexual / >5 | No | No | No | No | No | 113 / 113 | < 20 |
| 5 | HTLV-2 | 61 | M | Mestizo | Requena | Yes | Heterosexual / >5 | No | Yes | No | No | No | 134 / 322 | < 20 |
| 6 | HTLV-2 | 53 | M | Mestizo | Cuzco | Yes | Bisexual / > 5 | No | Yes | No | Yes | Gonorrhea Syphilis |
52 / 371 | < 20 |
| 7 | HTLV-2 | 60 | M | Mestizo | LOF | Yes | Heterosexual / LOF | LOF | No | No | Yes | No | NA | < 20 |
| 8 | Non-typable HTLV |
43 | F | Mestizo | Pebas | Yes | Heterosexual / <5 | No | No | No | No | No | 261 / 261 | < 20 |
| 9 | Non-typable HTLV |
55 | M | Mestizo | Iquitos | Yes | Heterosexual / <5 | No | No | No | No | Gonorrhea Syphilis |
455 / 455 | < 20 |
| 10 | HTLV-2 | 54 | F | Mestizo | Marañón River | Yes | Heterosexual / >5 | Scarification | No | No | No | Syphilis | 76 / 525 | < 20 |
| 11 | HTLV-2 | 64 | M | Mestizo | LOF | Yes | Heterosexual / LOF | LOF | No | No | No | No | 171 / 399 | < 20 |
| 12 | HTLV-2 | 66 | F | Mestizo | Ucayali River | Yes | Heterosexual / <5 | No | No | No | No | No | 519 / 519 | < 20 |
| 13 | HTLV-2 | 45 | M | Mestizo | Iquitos | Yes | Heterosexual / <5 | No | No | No | No | No | 434 / 434 | < 20 |
| 14 | HTLV-2 | 50 | M | Mestizo | Iquitos | No | Heterosexual / <5 | No | No | No | No | Gonorrhea |
344 / 344 | < 20 |
a Non-sterilized procedures: Injection, scarification, tattoos, dental procedures, intravenous drugs. b Defined as absence of paved streets. LOF: not available due to loss to follow-up. NA: not available in the clinical history.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



