
Submitted:
10 August 2025
Posted:
11 August 2025
You are already at the latest version
Abstract
Human papillomavirus (HPV) is common in both sexes and is also detected in male urine and semen. However, its exact origin and its etiological role in the male genital tract remain unclear. Formalin-fixed paraffin-embedded tissues from 157 prostate cancer patients were analyzed. HPV-DNA was detected using a nested PCR reaction, and HPV genotyping was performed using flow-through hybridization for positive cases. In situ hybridization (ISH) was used to localize HPV-DNA, whereas HPV-E6/E7 mRNA ISH and p16INK4a immunohistochemistry were conducted on high-risk (HR) HPV-positive samples. HPV-DNA was detected in 9.6% of prostate cancers and 0% of seminal vesicles. HR-HPV was observed in 4.5% of the samples, with HPV44 being the most common genotype. HPV prevalence was significantly higher in patients with high-grade groups (GG 4–5). Among 15 HPV-positive cases, HPV-DNA was found in 9 cancerous and 10 non-cancerous lesions. E6/E7 mRNA was expressed in 6 of 7 HR-HPV-positive cases, while p16INK4a expression was weak or absent in all cases. HPV can infect prostate tissue and may contribute to carcinogenesis in some cases, but p16INK4a may not be a consistent surrogate for E7 expression.
Keywords:
papillomavirus
; prostate cancer
; seminal vesicle
; p16
; E6/E7 mRNA
1. Introduction
Human papillomavirus (HPV) infection is a common sexually transmitted infection. It is equally prevalent in men and women [1]. In men, the most frequent infection sites are the external genitalia, such as the glans penis, penile shaft, coronal sulcus, and inner foreskin; however, it also occurs in the urinary tract, urine, and semen [2,3,4,5]. Recently, we demonstrated that HPV prevalence in semen among Japanese infertile men was 12.5% [5]; however, it remains unclear whether the origins of HPV, including seminal samples, are the urethra or genital tracts, such as the prostate and seminal vesicle.
Although HPV is a known causative agent of uterine cervical cancer, several studies indicate that HPV infection has a potential role in the development of other cancers, including skin, oropharyngeal, and penile cancers [6,7,8]. It has been associated with approximately 10% of all cancer cases [9]. Although the association between HPV infection and prostate cancer remains inconclusive, a meta-analysis involving 3,122 cases reported an HPV detection rate of 25.8% in prostate cancer patients, 17.4% in those with benign prostatic hyperplasia (BPH), and 9.2% in healthy controls [10]. Thus, HPV is detectable in prostate tissue, and HPV prevalence is likely significantly higher in prostate cancer patients compared with BPH and controls. Nonetheless, the etiological role of HPV infection in the development of prostate cancer remains unclear.
In this study, we examined the HPV-DNA prevalence and genotypes in prostate cancer and seminal vesicle samples among 157 Japanese patients with prostate cancer. In addition, the relationship between HPV infection and the clinical characteristics of prostate cancer was assessed. Moreover, for HPV-positive samples, we performed HPV-DNA in situ hybridization (ISH), and in cases positive for high-risk HPV, additional analyses, including HPV-E6/E7 mRNA ISH and immunohistochemistry (IHC) for p16INK4a expression, were performed to analyze the etiological role of HPV infection in the development of prostate cancer.
2. Materials and Methods
2.1. Subjects
Japanese prostate cancer patients who underwent robot-assisted radical prostatectomy or metastasectomy for prostate cancer at the Department of Urology, Kanazawa University Hospital, Kanazawa, Japan, between July 2017 and May 2019 were enrolled. The study was conducted following a protocol approved by the Ethics Committee of the Graduate School of Medical Sciences, Kanazawa University (Approval No. 2019-088). Information regarding the study was disclosed, and clinical data, such as patient background and tumor characteristics, were collected from the available medical records. Formalin-fixed paraffin-embedded (FFPE) prostate cancer samples were obtained for all cases; however, one case only had a metastatic lesion available, as the primary tumor could not be obtained. FFPE samples of the seminal vesicle were collected. In total, 157 prostate cancer specimens and 156 seminal vesicle specimens were analyzed.
2.2. HPV-DNA Test and Genotyping
FFPE blocks prepared with the prostate cancer and seminal vesicle specimens were sectioned at a thickness of 5 μm. After deparaffinizing, DNA was extracted from each sample using the Pinpoint Slide DNA Isolation System (Zymo Research, Orange, CA, USA). The quality of the DNA was assessed by confirming the amplification of the β-globin gene by the polymerase chain reaction (PCR). HPV-DNA was detected using nested PCR targeting the L1 gene, with MY09/MY11 as the outer primers and GP5+/GP6+ as the inner primers [11]. For HPV-positive samples, HPV genotyping was done using the 21-HPV GenoArray Diagnostic Kit (HybriBio, Hong Kong, China) [12], which uses the flow-through hybridization technique to identify a total of 21 HPV genotypes, including 15 high-risk HPV (HR-HPV) (16, 18, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, and 68) and 6 low-risk HPV (LR HPV) (6, 11, 42, 43, 44, and CP8304) types. Samples that tested positive by nested PCR, but yielded no detectable genotype using the GenoArray kit, were classified as having an unknown type.
2.3. HPV-DNA In Situ Hybridization
was used to confirm the localization of HPV-DNA in all of the HPV-positive samples. HPV-positive FFPE blocks were sectioned at 5-μm thickness, and hybridized with an HPV-DNA probe (Y1404; Dako, Carpinteria, CA, USA) based on the manufacturer’s protocol for the Dako GenPoint™ System [8]. This ISH analysis detects 13 HR-HPV genotypes (HPV types 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, and 68). As a negative control, some of the HPV-negative samples were processed simultaneously. The staining distribution of the ISH signals was scored as negative (₋; no staining), positive (+; visible only at high magnification), and strongly positive (2+; clearly visible at low magnification).
2.4. HPV-E6/E7 mRNA In Situ Hybridization
HPV is a nonenveloped icosahedral virus containing a double-stranded circular DNA genome. The viral genome encodes several genes, including E1, E2, E3, E4, E5, E6, E7, L1, and L2, among which E6 and E7 are key oncogenes [13]. When HPV-DNA was integrated into the host genome, E6 and E7 proteins were expressed. The E6 protein inhibits the tumor suppressor p53, thereby suppressing apoptosis, while the E7 protein promotes cellular proliferation by inactivating the retinoblastoma (Rb) protein [14]. In the present study, we performed HPV-E6/E7 mRNA ISH analysis to assess an etiological role for the development of prostate cancer in all HR-HPV-positive samples. E6/E7 mRNA expression was investigated using RNAscope® technology (Advanced Cell Diagnostics, Newark, CA, USA). This procedure was conducted with a specific probe (Code: 312591; Advanced Cell Diagnostics), targeting 18 HR-HPV genotypes (HPV types 16, 18, 26, 31, 33, 35, 39, 45, 51, 52, 53, 56, 58, 59, 66, 68, 73, and 82). As a negative control, E6/E7 mRNA expression was investigated in some of the HPV-negative samples. The staining distribution of the ISH signals was evaluated as described above; negative (−; no staining), positive (+; visible only at high magnification), and strongly positive (2+; visible clearly at low magnification).
2.5. Immunohistochemistry of p16INK4a, a Surrogate Marker of the E7 Protein
Under normal conditions, the cyclin-dependent kinase inhibitor p16INK4a activates Rb and halts cell proliferation. In HPV-associated tumors, however, Rb is inactivated by the E7 protein, which is expressed after HPV-DNA is integrated into the host genome. This results in a loss of negative feedback and overexpression of p16INK4a, which persists even during cell proliferation. Based on this mechanism, p16INK4a has been widely recognized as a surrogate marker for HPV-related malignancies [15]. We also evaluated p16INK4a expression in all HR-HPV-positive samples by IHC to determine whether it is a surrogate marker for E7 expression in prostate cancer with HR-HPV infection.
HPV-positive FFPE blocks were sectioned at 5-μm thickness, and antigen retrieval was performed by incubating the samples in 20 mM Tris-HCl (pH 9.0) at 95°C for 20 min, followed by cooling at room temperature for 20 min. The samples were incubated overnight with a mouse monoclonal p16INK4a antibody (ACR3231A; BIOCARE Medical, Pacheco, CA, USA) diluted 1:100. Next, the specimens were incubated with a peroxidase-labeled secondary antibody for 30 min. The expression of p16INK4a was observed following DAB staining (SK-4103; Vector LABORATORIES, Newark, CA, USA), and the slides were counterstained with hematoxylin. Some HPV-negative samples and HPV16-positive penile cancer samples [8] were available for IHC of p16INK4a as negative and positive controls, respectively. We assessed the IHC staining as follows: negative (−; no staining), positive (+; visible only at high magnification), and strongly positive (2+; clearly visible at low magnification).
2.6. Statistical Analysis
Patient background characteristics were compared using the Mann–Whitney U test or the Chi-squared test, as appropriate. Comparisons between the GG and HPV-positive and -negative cases were performed using the Chi-squared test. All statistical analyses were done using IBM SPSS Statistics version 29 (IBM Corp., Armonk, NY, USA), and a p-value of <0.05 was considered statistically significant.
3. Results
3.1. Patient Characteristics and HPV Prevalence
The median age and serum prostate-specific antigen levels of the 157 patients with prostate cancer were 68 years (range, 48–76 years) and 7.05 ng/ml (range, 2.42-74.2 ng/ml), respectively (Table 1). Nineteen (12.1%) cases were histologically GG1, 118 (75.2%) were GG2, and 20 (12.7%) were GG3 cancer. Many of the patients (87.9%) had localized prostate cancer (<T2).
HPV-DNA was detected in 15 cases (9.6%) of prostate cancer and 0 (0%) of the seminal vesicle samples (Table 2). HR-HPV was prevalent in 7 prostate cancer cases (4.5%). The most frequent HPV genotype was HPV44, followed by HPV31, 52, and 58. An unknown genotype, which was not determined by the flow-through hybridization of 21 types, was detected in 6 cases.
When patient backgrounds were stratified by HPV-DNA status, HPV prevalence in the patients with high GG (4–5) was significantly higher compared with those exhibiting low to intermediate GG (1–3) (p = 0.0214) (Table 1).
3.2. HPV-DNA In Situ Hybridization
In the 15 HPV-positive samples, HPV-DNA signals were observed in cancerous lesions in 9 (80%) cases. Positive signals were obtained in 2 cases, and 7 cases were strongly positive (Figure 1, Table 3). Strong ISH signals (strongly positive) were observed in 4 HR-HPV-positive cases, whereas weak signals (positive) were evident in one case. Moreover, ISH signals were also present in the cells of normal glandular tissue in non-cancerous lesions in 10 cases (Figure 1). HPV-DNA signals were even observed in samples that were positive for HPV genotypes (type 44, 66, and UK) not covered by the ISH probe. As a negative control, HPV-DNA signals were undetectable in the HPV-negative samples.
3.3. HPV-E6/E7 mRNA Expression
We performed HPV-E6/E7 mRNA ISH analysis to determine the etiological role for the development of prostate cancer in HR-HPV-positive samples. Strong signals were present in the nuclei of tumor cells among 6 of 7 HR-HPV-positive samples (Table 4, Figure 2). Among HR-HPV-positive samples with HPV-DNA ISH signals in cancerous lesions, 4 exhibited strong expression of E6/E7 mRNA. Furthermore, ISH signals of E6/E7 mRNA were also detected in two cases without HPV-DNA ISH signals. On the other hand, E6/E7 mRNA was not observed in one HR-HPV-positive sample and the HPV-negative samples.
3.4. p16INK4a Protein Expression
4. Discussion
We found that the prevalence of HPV-DNA was 9.6% (15/157 cases) among prostate cancer patients based on a PCR analysis. Numerous studies have demonstrated a wide range of HPV prevalence in prostate cancer patients, from 0% to 75% worldwide [10,16,17,18,19,20], and from 0% to 16% in Japan [18,19]. This variability may be the result of small cohorts, differences in HPV detection methods, and differences in the surveyed regions. The prevalence of HPV varies by region, particularly with East Asian populations, which generally show lower rates compared with the global average [20]. Although HPV prevalence in the present study was not considered high, it was consistent with the previous findings in Japan [18,19]. Moreover, the prostate was one of the HPV infectious sites in men; however, HPV-DNA was not detected in the seminal vesicle. To our knowledge, there are no previous reports examining HPV infection in the seminal vesicles. Currently, there is no evidence indicating that HPV can infect the seminal vesicles.
In the present study, the most frequent HPV genotype was the UK type, followed by type 44 (5 cases), and types 31, 52, and 58 (2 cases, respectively). A meta-analysis in 2019 involving 5,546 prostate cancer patients indicated that HPV16 was the most prevalent, followed by types 31 and 58 [21]. Therefore, the HPV type distribution was different from our results. Many studies included in this meta-analysis only evaluated HR-HPV types; thus, LR genotypes, such as HPV 44, may have been categorized as "unknown types." Indeed, a previous large population study including 803 Japanese patients evaluating HPV prevalence in urine samples demonstrated that HPV types 70, 71, 84, and 90, which are not covered by the HPV genotyping method used in the present study, were frequently detected [22]. Although the HPV type distribution between the urine and prostate specimens is not always consistent, the HPV genotypes detected in the prostate samples may also vary by region or country. Our results suggest that LR HPV infection, including UK types, may also be relatively common in the prostate. On the other hand, HPV16, which is the most common oncogenic type observed in many HPV-associated cancers, was not detected in the present study. However, the number of patients was small for an epidemiological study; thus, further studies including a large number of subjects are needed to clarify HPV prevalence in the prostate.
Prostate cancer is histologically classified into GG1–5. According to the National Comprehensive Cancer Network guidelines, GG1 corresponds to a low or very low-risk, GG2–3 is at intermediate risk, and GG4–5 represents high or very high-risk. In our analysis, all patients were grouped into GG1, GG2–3, and GG4–5 categories. The HPV detection rate was in higher the GG cases. A previous study including 95 prostate cancer cases revealed that a higher HPV prevalence was associated with cases exhibiting a high Gleason score [23]. Other studies have demonstrated an association between HPV infection and high Gleason score in prostate cancer [24,25]. HPV infection may also be correlated with tumor aggressiveness.
The localization of HPV-DNA in prostate tissue was determined by ISH analysis. Among the 15 HPV-positive samples, HPV-DNA signals were not only detected in the cancerous lesions of 9 cases, but also in non-cancerous lesions in 10 cases. Unexpectedly, HPV infection was also found in non-cancerous lesions in the prostate cancer samples. In particular, 2 HR-HPV-positive cases showed no signals in cancerous lesions, only in non-cancerous lesions. Overall, ISH signals were observed in 12 (80%) of 15 HPV-positive cases based on PCR analysis, and the signals were observed in all HR-HPV-positive specimens. These results confirm the presence of HPV-DNA in prostate tissue. On the other hand, HPV-DNA signals were even detected in some samples that were positive for HPV genotypes by PCR, which were not covered by the ISH probe. This may be due to cross-hybridization with the 44, 66, and unknown types because HPV-DNA signals were not observed in HPV-negative samples. The similar cross-reactions of HPV-DNA in the ISH procedure used in this study have been described previously [26].
In HPV-associated malignancies, such as penile cancer, oropharyngeal cancer, and anal cancer, persistent infection with HR-HPV results in the integration of HPV-DNA into the host genome, the expression of the E6 and E7 oncogenes, and an increased risk of carcinogenesis [27,28,29]. The association between HPV and cancer and the expression of the E6 and E7 genes has been evaluated to determine their etiological role in carcinogenesis [26,27,28]. In the present study, we found strong E6/E7 mRNA expression in 6 of 7 HR-HPV-positive samples, supporting a carcinogenic role for HR-HPV infection. In the remaining case (case 7, HPV58), HPV-DNA was detected in the cancerous lesions; however, E6/E7 mRNA was not expressed. This suggests that HPV58 may have been an episomal infection in this case. Only one study demonstrated that the E7 protein was expressed in all HR-HPV-positive samples by IHC [17]. Moreover, recent review proposed the potential involvement of the E6 and E7 proteins in the oncogenic mechanism of HPV infection [30]; however, studies examining E6/E7 expression in prostate cancer are currently limited. Therefore, further studies are needed to establish the oncogenic role of the E6/E7 protein in prostate cancer.
p16INK4a has been widely accepted as a surrogate marker of E7 expression, and this protein is markedly expressed in many HPV-associated cancers; however, our results indicate that p16INK4a overexpression is not absent in all cases. A noteworthy observation was the discordance between E6/E7 mRNA expression and p16INK4A expression. It has been well documented that some oropharyngeal cancers lack p16INK4A expression despite the functional inactivation of Rb by the E7 protein [31,32]. This may result from the difference in viral load and mutations or deletions in the p16INK4A gene (CDKN2A). In particular, CDKN2A is more frequently methylated in prostate cancer tissue compared with normal tissue [33], suggesting that p16INK4A expression may be epigenetically suppressed in malignant lesions. On the other hand, one study reported an HR-HPV prevalence of 19.6% in prostate cancer and observed p16INK4A overexpression in many HPV-positive samples [34], which differs from our results. Few studies have examined the relationship between HPV infection and p16 INK4a expression in prostate cancer. Although further studies are needed, our results suggest that p16 INK4a may not always be a surrogate marker for HPV-DNA integration in prostate cancer.
In the present study, the number of HR-HPV-positive samples was extremely limited, and E6/E7 mRNA and p16 INK4a expression were only evaluated in 7 cases. This is a limitation of the present study; however, we examined the carcinogenic role of HPV infection in prostate cancer using various molecular analyses, such as PCR, HPV-DNA ISH, E6/E7 mRNA ISH, and IHC, which is a strength.
5. Conclusions
HPV-DNA was detected in 9.6% of prostate cancer cases and 0% of the seminal vesicle specimens. ISH analysis revealed that HPV-DNA was present in the cancerous and/or non-cancerous lesions, suggesting that HPV may infect the prostate. In some cases of HR-HPV infection, HPV-E6/E7 mRNA was expressed in the cancer tissue. HPV infection occurs in the prostate, and it may play an etiological role in the development of prostate cancer, although this has only been tested in a limited number of cases to date.
Author Contributions
Conceptualization, Rei Shinzawa, Kazuyoshi Shigehara, Shohei Kawaguchi; methodology, Rei Shinzawa, Kazuyoshi Shigehara, Shohei Kawaguchi, Hiroki Nakata; validation, Rei Shinzawa Kazuyoshi Shigehara; formal analysis, Rei Shinzawa; investigation, Rei Shinzawa, Shohei Kawaguchi, Yuki Kato, Tomomi Nakagawa, Kotaro Fukukawa, Shingo Takada; resources, Kazuyoshi Shigehara, Kouji Izumi, Atsushi Mizokami; data curation, Rei Shinzawa, Yuki Kato; writing—original draft preparation, Rei Shinzawa; writing—review and editing, Kazuyoshi Shigehara; visualization, Rei Shinzawa, Kazuyoshi Shigehara; supervision, Kazuyoshi Shigehara, Kouji Izumi, Atsushi Mizokami; project administration, Rei Shinzawa, Kazuyoshi Shigehara, Shohei Kawaguchi. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the Kanazawa University Graduate School of Medical Science (No. 2019-088; approval date: 19 June 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
The authors used ChatGPT (GPT-4o mini, OpenAI) for preliminary English editing, followed by professional language editing services provided by Enago (www.enago.jp). All revisions were reviewed and approved by the authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Dunne, E.F.; Nielson, C.M.; Stone, K.M.; Markowitz, L.E.; Giuliano, A.R. Prevalence of HPV infection among men: A systematic review of the literature. J Infect Dis 2006, 194, 1044–1057. [Google Scholar] [CrossRef]
- Giuliano, A.R.; Nielson, C.M.; Flores, R.; et al. The optimal anatomic sites for sampling heterosexual men for human papillomavirus (HPV) detection: The HPV detection in men study. J Infect Dis 2007, 196, 1146–1152. [Google Scholar] [CrossRef] [PubMed]
- Shigehara, K.; Sasagawa, T.; Namiki, M. Human papillomavirus infection and pathogenesis in urothelial cells: A mini-review. J Infect Chemother 2014, 20, 741–747. [Google Scholar] [CrossRef] [PubMed]
- Laprise, C.; Trottier, H.; Monnier, P.; Coutlée, F.; Mayrand, M.H. Prevalence of human papillomaviruses in semen: A systematic review and meta-analysis. Hum Reprod 2014, 29, 640–651. [Google Scholar] [CrossRef]
- Kato, Y.; Shigehara, K.; Nakagawa, T.; et al. Human papillomavirus detected in sperm of Japanese infertile males affects reproductive parameters. Int J Infect Dis 2021, 112, 294–299. [Google Scholar] [CrossRef]
- Jenson, A.B.; Geyer, S.; Sundberg, J.P.; Ghim, S. Human papillomavirus and skin cancer. J Investig Dermatol Symp Proc 2001, 6, 203–206. [Google Scholar] [CrossRef]
- Fonsêca, T.C.; Jural, L.A.; Marañón-Vásquez, G.A.; et al. Global prevalence of human papillomavirus-related oral and oropharyngeal squamous cell carcinomas: A systematic review and meta-analysis. Clin Oral Investig 2023, 28, 62. [Google Scholar] [CrossRef]
- Sakamoto, J.; Shigehara, K.; Nakashima, K.; et al. Etiological role of human papillomavirus infection in the development of penile cancer. Int J Infect Dis 2019, 78, 148–154. [Google Scholar] [CrossRef]
- zur Hausen, H. Papillomaviruses and cancer: From basic studies to clinical application. Nat Rev Cancer 2002, 2, 342–350. [Google Scholar] [CrossRef] [PubMed]
- Tsydenova, I.A.; Ibragimova, M.K.; Tsyganov, M.M.; Litviakov, N.V. Human papillomavirus and prostate cancer: Systematic review and meta-analysis. Sci Rep 2023, 13, 16597. [Google Scholar] [CrossRef]
- de Roda Husman, A.M.; Walboomers, J.M.; van den Brule, A.J.; et al. The use of general primers GP5 and GP6 elongated at their 3′ ends with adjacent highly conserved sequences improves human papillomavirus detection by PCR. J Gen Virol 1995, 76, 1057–1062. [Google Scholar] [CrossRef]
- Shigehara, K.; Sasagawa, T.; Kawaguchi, S.; et al. Prevalence of human papillomavirus infection in the urinary tract of men with urethritis. Int J Urol 2010, 17, 563–568. [Google Scholar] [CrossRef]
- Nakagawa, S. ; Yoshikawa. H.; Yasugi, T.; et al. Ubiquitous presence of E6 and E7 transcripts in human papillomavirus-positive cervical carcinomas regardless of its type. J Med Virol 2000, 62, 251–258. [Google Scholar] [CrossRef]
- Schmitt, A.; Harry, J.B.; Rapp, B.; et al. Comparison of the properties of the E6 and E7 genes of low- and high-risk cutaneous papillomaviruses reveals strongly transforming and high Rb-binding activity for the E7 protein of the low-risk human papillomavirus type 1. J Virol 1994, 68, 7051–7059. [Google Scholar] [CrossRef] [PubMed]
- Darragh, T.M.; Colgan, T.J.; Thomas Cox, J.; et al. The Lower Anogenital Squamous Terminology Standardization project for HPV-associated lesions: Background and consensus recommendations. Int J Gynecol Pathol 2013, 32, 76–115. [Google Scholar] [CrossRef] [PubMed]
- Rotola, A.; Monini, P.; Di Luca, D.; et al. Presence and physical state of HPV DNA in prostate and urinary-tract tissues. Int J Cancer 1992, 52, 359–365. [Google Scholar] [CrossRef]
- Ahmed, M.Y.; Salman, N.A.; Sandhu, S.; et al. Detection of high-risk Human Papillomavirus in prostate cancer from a UK based population. Sci Rep 2023, 13, 7633. [Google Scholar] [CrossRef]
- Noda, T.; Sasagawa, T.; Dong, Y.; et al. Detection of human papillomavirus (HPV) DNA in archival specimens of benign prostatic hyperplasia and prostatic cancer using a highly sensitive nested PCR method. Urol Res 1998, 26, 165–169. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, H.; Komiya, A.; Aida, S.; et al. Detection of human papillomavirus DNA and p53 gene mutations in human prostate cancer. Prostate 1996, 28, 318–324. [Google Scholar] [CrossRef]
- Bruni, L.; Albero, G.; Rowley, J.; et al. Global and regional estimates of genital human papillomavirus prevalence among men: A systematic review and meta-analysis. Lancet Glob Health 2023, 11, e1345–e1362. [Google Scholar] [CrossRef]
- Moghoofei, M.; Keshavarz, M.; Ghorbani, S.; et al. Association between human papillomavirus infection and prostate cancer: A global systematic review and meta-analysis. Asia Pac J Clin Oncol 2019, 15, e59–e67. [Google Scholar] [CrossRef]
- Nakashima, K.; Shigehara, K.; Kitamura, T.; et al. Risk factors for human papillomavirus detection in urine samples of heterosexual men visiting urological clinics in Japan. J Infect Chemother 2018, 24, 713–717. [Google Scholar] [CrossRef]
- Singh, N.; Hussain, S.; Kakkar, N.; et al. Implication of high risk human papillomavirus (HR-HPV) infection in prostate cancer in Indian population: A pioneering case-control analysis. Sci Rep 2015, 5, 7822. [Google Scholar] [CrossRef]
- Pascale, M.; Pracella, D.; Barbazza, R.; et al. Is human papillomavirus associated with prostate cancer survival? Dis Markers 2013, 35, 607–613. [Google Scholar] [CrossRef]
- Shigehara, K.; Sasagawa, T.; Kawaguchi, S.; et al. Etiologic role of human papillomavirus infection in bladder carcinoma. Cancer 2011, 117, 2067–2076. [Google Scholar] [CrossRef] [PubMed]
- Abumsimir, B.; Mrabti, M.; Laraqui, A.; et al. Molecular characterization of human papillomavirus and mouse mammary tumor virus-like infections in prostate cancer tissue and relevance with tumor characteristics. Mol Clin Oncol. 2022, 16, 16. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.K.; Panaiyadiyan, S.; Kurra, S.; et al. Association of human papillomavirus in penile cancer: A single-center analysis. Indian J Urol 2022, 38, 210–215. [Google Scholar] [CrossRef]
- Yin, J.; Li, Y.; Song, C.; et al. Evaluation of an E6/E7 PCR-capillary electrophoresis fragment analysis in the genotyping of human papillomavirus in archival FFPE samples of oropharyngeal cancer. J Med Virol 2024, 96, e29716. [Google Scholar] [CrossRef]
- Phanuphak, N.; Teeratakulpisarn, N.; Keelawat, S.; et al. Use of human papillomavirus DNA, E6/E7 mRNA, and p16 immunocytochemistry to detect and predict anal high-grade squamous intraepithelial lesions in HIV-positive and HIV-negative men who have sex with men. PLoS ONE 2013, 8, e78291. [Google Scholar] [CrossRef] [PubMed]
- Bello, R.O.; Willis-Powell, L.; James, O.; et al. Does human papillomavirus play a causative role in prostate cancer? A systematic review using Bradford Hill's criteria. Cancers (Basel) 2023, 15, 3897. [Google Scholar] [CrossRef]
- Mehanna, H.; Taberna, M.; von Buchwald, C.; et al. Prognostic implications of p16 and HPV discordance in oropharyngeal cancer (HNCIG-EPIC-OPC): A multicentre, multinational, individual patient data analysis. Lancet Oncol 2023, 24, 239–251. [Google Scholar] [CrossRef] [PubMed]
- Zupancic, M.; Kostopoulou, O.N.; Holzhauser, S.; et al. Human papillomavirus (HPV) load is higher in HPV-DNA/p16 positive than in HPV-DNA positive/p16 negative oropharyngeal squamous cell carcinoma but does not differ significantly between various subsites or correlate to survival. Oral Oncol 2024, 151, 106749. [Google Scholar] [CrossRef] [PubMed]
- Murphy, T.M.; Sullivan, L.; Lane, C.; et al. In silico analysis and DHPLC screening strategy identifies novel apoptotic gene targets of aberrant promoter hypermethylation in prostate cancer. Prostate 2011, 71, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Medel-Flores, O.; Valenzuela-Rodríguez, V.A.; Ocadiz-Delgado, R.; et al. Association between HPV infection and prostate cancer in a Mexican population. Genet Mol Biol 2018, 41, 781–789. [Google Scholar] [CrossRef]
Figure 1.
HPV-DNA in situ hybridization. (a) Negative control x200 (b) Positive x200 (c) Strongly positive x100(d) HPV-DNA strongly positive normal prostate region.
Figure 1.
HPV-DNA in situ hybridization. (a) Negative control x200 (b) Positive x200 (c) Strongly positive x100(d) HPV-DNA strongly positive normal prostate region.
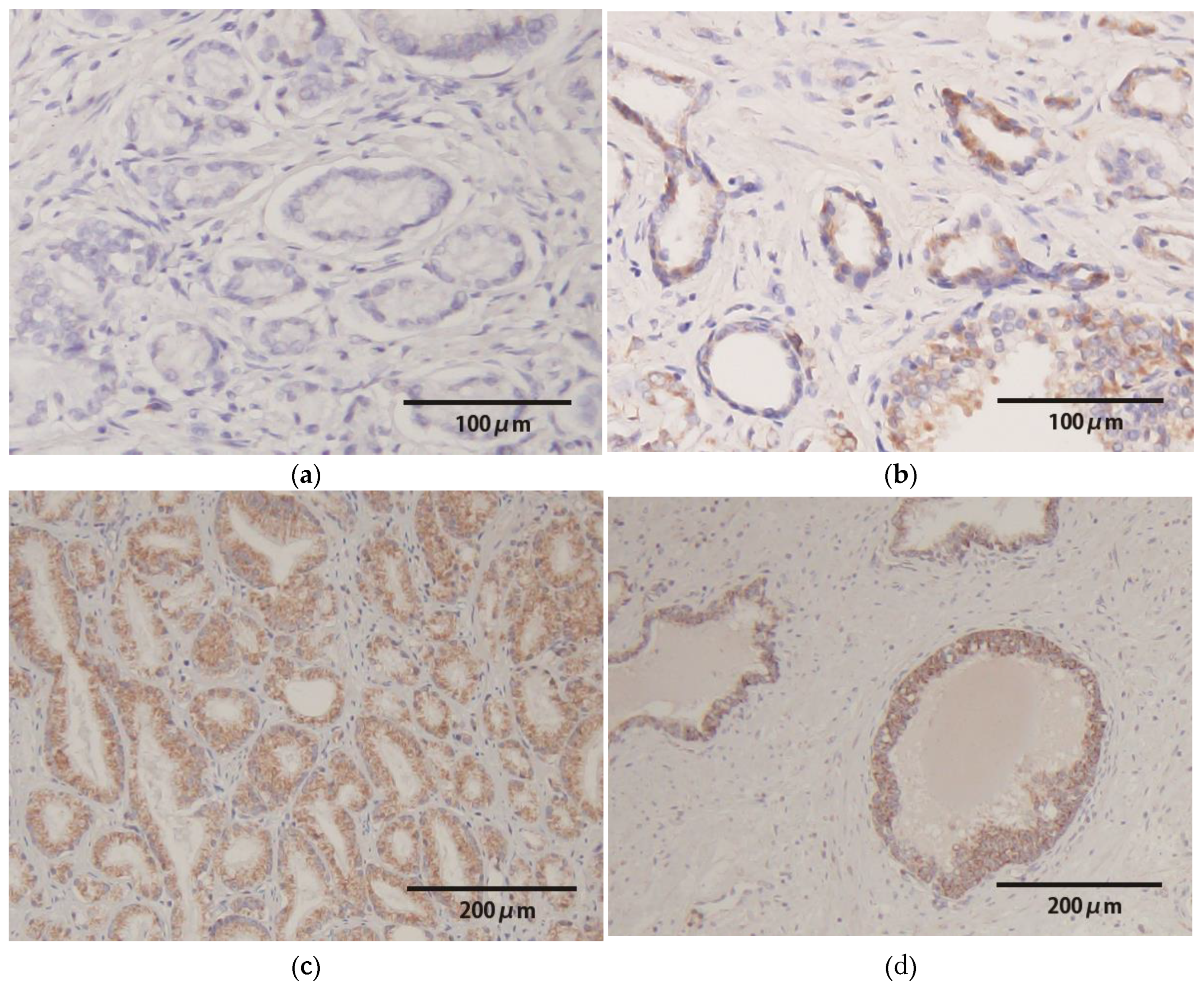
Figure 2.
E6/E7 mRNA in situ hybridization. (a) Negative control x200 (b) Positive x200 (c) Strongly positive x100.
Figure 2.
E6/E7 mRNA in situ hybridization. (a) Negative control x200 (b) Positive x200 (c) Strongly positive x100.
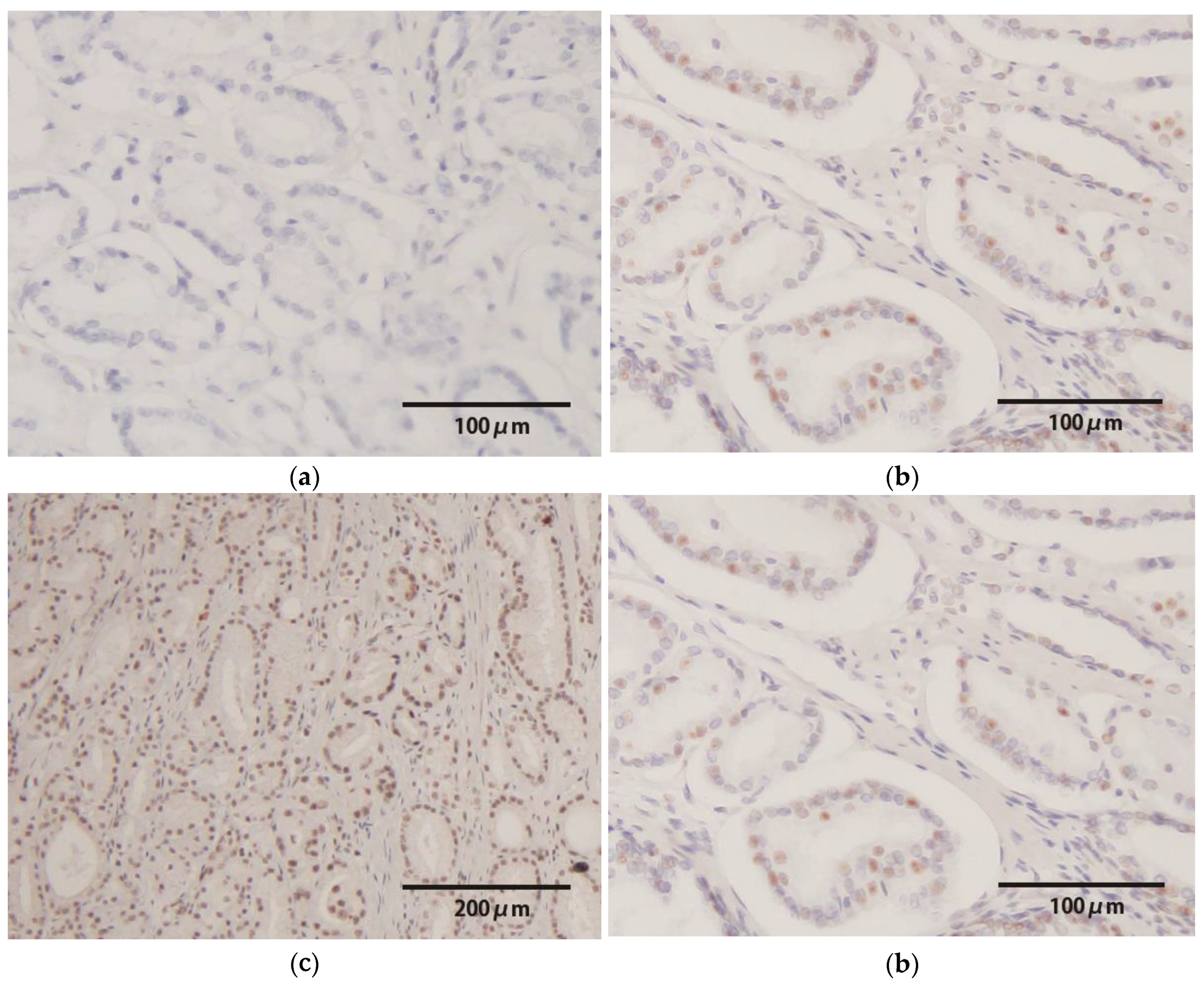
Figure 3.
p16INK4a immunohistochemistry. (a) Negative control x200 (b) Positive x200.
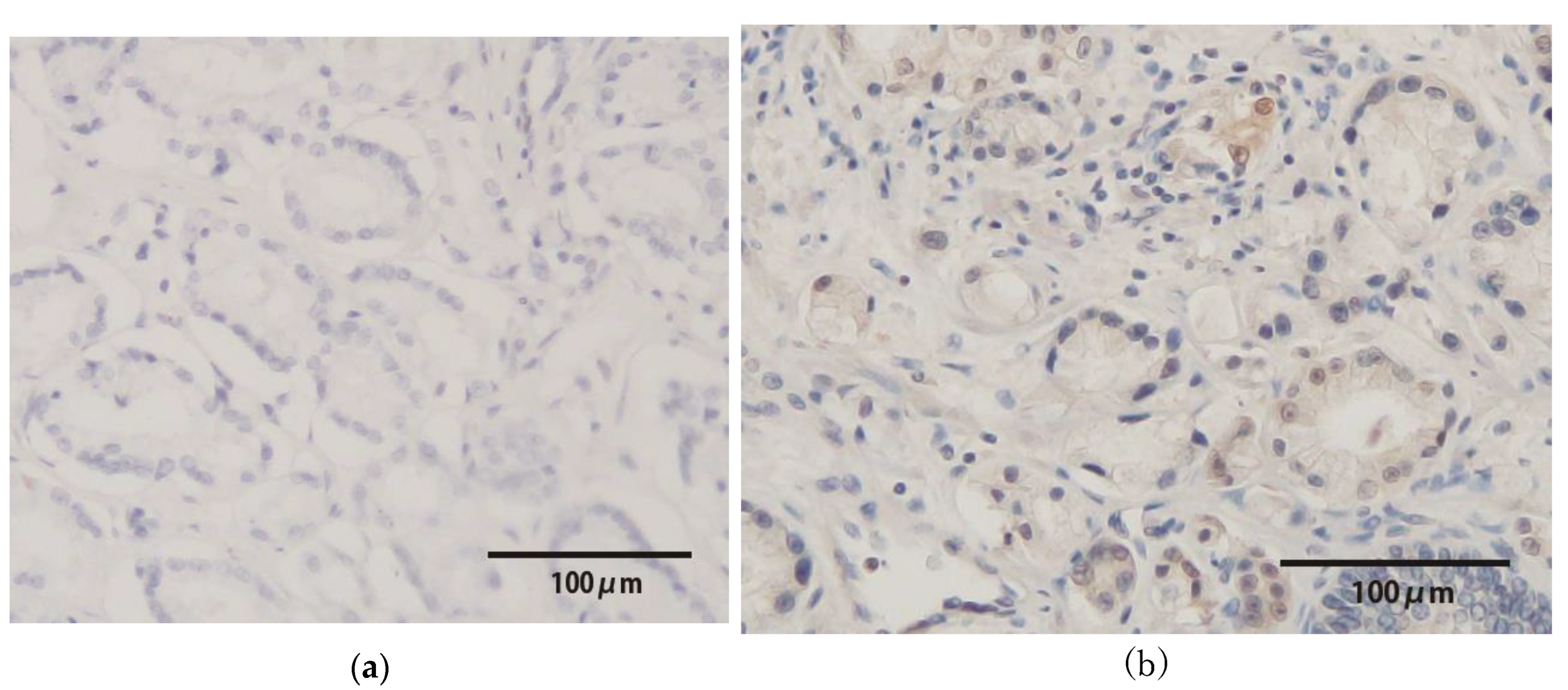

Table 1.
Patient backgrounds and tumor characteristics.
| Characteristics | n = 157 | HPV(+) (n = 15) | HPV(−) (n = 142) | p |
|---|---|---|---|---|
| Age (median, range) | 68 (48–76) | 70 (48–76) | 65 (56–76) | 0.981 |
| PSA, ng/ml (median, range) | 7.05 (2.42–74.2) | 6.24 (3.00–16.54) | 7.06 (2.42–74.2) | 0.375 |
| Grade Group (n, %) | ||||
| 1 | 19 (12.1%) | 0 (0%) | 19 (13.4%) | |
| 2–3 | 118 (75.2%) | 10 (66.7%) | 108 (76.1%) | |
| 4–5 | 20 (12.7%) | 5 (33.3%) | 15 (10.6%) | 0.0214 |
| T category (n, %) | ||||
| pT0 | 2 (1.3%) | 0 | 2 (1.4%) | |
| pT2 | 136 (86.6%) | 12 (80%) | 124 (87.3%) | 0.455 |
| pT3 | 15 (9.6%) | 3 (20%) | 12 (8.5%) | |
| pT4 | 4 (2.5%) | 0 | 4 (2.8%) |
HPV, human papillomavirus; PSA, prostate-specific antigen; T, tumor.
Table 2.
HPV-DNA prevalence and genotyping in prostate cancer specimens and seminal vesicle samples.
Table 2.
HPV-DNA prevalence and genotyping in prostate cancer specimens and seminal vesicle samples.
| PCR results. | Prostate Cancer Tissue | Seminal Vesicle Tissue |
| Any HPV | 15 (9.6%) | 0 (0%) |
| HR-HPV | 7 (4.5%) | 0 (0%) |
| The HPV genotype | N | |
| 31 | 2 | |
| 44 | 5 | |
| 52 | 2 | |
| 58 | 2 | |
| 66 | 1 | |
| Unknown 1 | 6 |
PCR, polymerase chain reaction; HPV, human papillomavirus; HR, high-risk. 1 Specimens that tested positive by nested PCR, but yielded no detectable genotype by the GenoArray kit, were classified as having an unknown type.
Table 3.
Summary of the HPV genotypes and HPV-DNA in situ hybridization in HPV−positive specimens.
| No | Age | GG | T | Genotype | HPV Risk | HPV-DNA ISH | |
| Normal Lesion | Cancer Lesion | ||||||
| 1 | 48 | 3 | 2c | 31 | HR | ++ | − |
| 2 | 63 | 2 | 3a | 31 | HR | ++ | ++ |
| 3 | 74 | 5 | 3b | 44 | LR | + | ++ |
| 4 | 59 | 2 | 2c | 44 | LR | ++ | ++ |
| 5 | 59 | 5 | 3b | 52 | HR | − | + |
| 6 | 71 | 2 | 2c | UK | Unknown | + | − |
| 7 | 72 | 4 | 2a | 58 | HR | ++ | ++ |
| 8 | 76 | 2 | 2c | 66 | HR | − | ++ |
| 9 | 72 | 3 | 2b | 52/44 | HR/LR | ++ | ++ |
| 10 | 63 | 4 | 2a | 58/44 | HR/LR | + | − |
| 11 | 64 | 4 | 2c | 44 | LR | − | − |
| 12 | 70 | 3 | 2c | UK | Unknown | ++ | ++ |
| 13 | 72 | 2 | 2c | UK | Unknown | − | − |
| 14 | 72 | 2 | 2b | UK | Unknown | + | + |
| 15 | 65 | 2 | 2c | UK | Unknown | − | − |
HPV, human papillomavirus; GG, Gleason grade; T, tumor; HR, high-risk. LR, low-risk; UK, unknown; ISH, in situ hybridization. Staining score; negative (c; no staining), positive (+; visible only at high magnification), and strongly positive (2+; visible clearly at low magnification).
Table 4.
Summary of HPV genotypes and HPV-E6/E7 expression in HR-HPV-positive specimens.
| No | Genotype | HPV risk | E6/E7 oncogenic protein | |
|---|---|---|---|---|
| E6/E7 mRNA ISH | p16INK4a protein | |||
| 1 | 31 | HR | ++ | + |
| 2 | 31 | HR | ++ | − |
| 5 | 52 | HR | ++ | − |
| 7 | 58 | HR | − | + |
| 8 | 66 | HR | ++ | + |
| 9 | 52/44 | HR/LR | ++ | + |
| 10 | 58/44 | HR/LR | ++ | − |
HPV, human papillomavirus; HR, high-risk; LR, low-risk; RNA, ribo nucleic acid, ISH, in situ hybridization, Staining score; negative (−; no staining), positive (+; visible only at high magnification), and strongly positive (2+; clearly visible at low magnification).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



