Submitted:
08 August 2025
Posted:
08 August 2025
You are already at the latest version
Abstract
Background/Objectives: Regular physical activity helps prevent and treat non-communicable chronic diseases. Physical inactivity is one of the main risk factors for mortality due to non-communicable diseases, meaning that the risk of death increases by 20% to 30% compared to individuals who reach a sufficient level of physical activity. The aim was to explore the perceptions and practices of physicians in a secondary level hospital in Nuevo León, Mexico, regarding the prescription of exercise to treat non-communicable chronic diseases. Methods: A validated questionnaire was applied to 127 physicians affiliated with the hospital, assessing two dimensions: Advice on physical exercise (factor 1) and Application of physical exercise (factor 2). Results: It was found that, although 63.8% of physicians frequently inquire about their patients' levels of physical activity and 60.6% discuss its importance, only 44.9% conduct formal evaluations through physical tests. Additionally, while 85% recognize the need to refer patients to exercise specialists, only 26.8% do so regularly. The reliability of the instrument was excellent (α = 0.857; ω = 0.852 factor 1 and ω = 0.798 factor 2), confirming its validity. Conclusions: Identified barriers include a lack of standardized protocols, insufficient resources, and limitations in medical training. These findings underscore the need for institutional policies that prioritize exercise prescription as an essential part of the treatment of non-communicable chronic diseases, aligning with WHO guidelines to improve population health.
Keywords:
Physical activity
; Exercise prescription
; Chronic non-communicable diseases
; Hospital care
; Clinical practice
1. Introduction
Physical inactivity is one of the main risk factors for mortality from non-communicable diseases, which means that individuals with insufficient levels of physical activity have a 20% to 30% higher risk of death compared to those who achieve sufficient levels of physical activity (WHO, 2020).
It has been proven that regular physical activity (PA) helps prevent and treat chronic non-communicable diseases (NCDs) such as heart disease, strokes, diabetes, and breast and colon cancer. Additionally, it helps to prevent hypertension, overweight, and obesity, while also improving mental health, quality of life, and well-being (WHO, 2020).
Increasing physical activity at the population level has become an essential component of major global initiatives aimed at improving health (WHO, 2018). Structured counseling on PA uses established behavioral strategies to change an individual’s lifestyle, which is why it is suggested that physical exercise should also be part of hospital services (Börjesson, 2013; Lundqvist et al., 2017).
To support healthcare professionals’ efforts and increase physical activity levels among their outpatient patients, an initiative called Exercise is Medicine (EIM) was created, launched in 2007 by the American College of Sports Medicine and the American Medical Association. EIM highlights three underlying principles: first, physical activity should be monitored as a vital sign; second, physical activity is an effective medical modality and should be prescribed; and third, the success of this vision requires collaboration among three key stakeholder groups: physicians, exercise professionals, and patients (Bowen et al., 2018).
There are initiatives for implementing EIM in primary care, but it has been suggested that EIM should also be part of the hospital care system (secondary and tertiary) regarding treatment and prescription. EIM has great potential due to the authority and significant role that physicians play (Krops et al., 2020).
The prescription of physical exercise by health professionals has been widely debated in the last ten years as an adjunct tool for preventing and treating NCDs in healthcare settings (Teferi et al., 2017).
Research shows that most patients listen to their physicians when they discuss topics related to a healthy lifestyle, good nutrition, and physical activity. Despite this, committing to following physical activity guidelines and finding the motivation to adhere to them are significant challenges faced by both patients and healthcare professionals (Noetel et al., 2024).
Currently, there is interest in understanding the reality, future, and medical expectations regarding the inclusion of exercise prescription in Nuevo León, Mexico. It is important to have knowledge of this to promote new structured projects based on scientific evidence for exercise prescription to improve the health system. Therefore, the objective of the present study is to explore the level of exercise prescription or recommendation by physicians for treating non-communicable diseases in a public secondary-level hospital.
2. Materials and Methods
Type of Study
This publication corresponds to an instrumental analysis for which a quantitative, descriptive, and cross-sectional study was conducted following the research methodology of Hernández et al. (2023). This method is appropriate for understanding medical consideration regarding the prescription of physical activity in a second-level hospital. The data collection period lasted for 2 months.
Sample Selection Criteria
Participants: The study population consisted of active physicians at the Metropolitan Hospital of Nuevo León, Mexico, totaling approximately 140 active physicians
Sample: The study sample was a non-probabilistic sample due to being a voluntary participation study involving 132 physicians, of which 7 were excluded for not meeting the participation criteria. Therefore, considering the 127 responses, it was sufficient to conduct the statistical analysis.
Participation Criteria: Physicians with voluntary participation, male or female, employed at the hospital in question, and of any age, who diagnose and treat patients with NCDs (Non-Communicable Diseases). Exclusion Criteria: Physicians without voluntary participation were excluded. Additionally, participants who did not complete the survey were removed from the sample.
Ethical Considerations: Before evaluation by the research and ethics committees, the instrument was validated by a panel of experts. Subsequently, a protocol was established in accordance with the guidelines set forth in the General Law of Health Research (latest reforms, 2014, Mexico). Once this phase was completed, the document was reviewed and approved by the Research Ethics Committee of the Metropolitan Hospital of Nuevo León, obtaining official registration DEISC-19-01-24-43.
Instrument
The questionnaire designed by Teferi et al. (2017) was used as a basis, to which our study added a new item: “Do you think it is necessary for specialized professionals to prescribe exercise to aid in the prevention or treatment of NCDs?” This retained the 5-point Likert format (1: Never to 5: Always) used by Teferi et al. (2017). It was translated from English to Spanish and from Spanish to English to maintain the intended meaning of each item, highlighting the need for linguistic and cultural equivalence between versions (Mostafa, 2016).
Expert Validation
The translated questionnaire was evaluated based on Delphi method validation criteria (Loo, 2002) to ensure its content validity. The process was guided by the following methodological principles: Selection of Experts. Participants were systematically chosen based on their experience and specialization in the study area. Anonymity and Independence. Responses were collected anonymously and without interaction among the experts, minimizing group influence bias. Process Control. The researcher supervised each stage to ensure compliance with the established protocol. Interactive Feedback. Two-way communication was facilitated between the researcher and the experts to clarify doubts during the evaluation rounds. Results Analysis. Conclusions were drawn based on the consensus reached by the panel, supporting the validity of the instrument. Additionally, a comprehensive statistical analysis was implemented to quantify the level of agreement among the experts through the use of the Delphi method. This systematic approach allowed for the assessment of the robustness of the scale across four critical dimensions, defined according to the validation criteria of Hernández et al. (2023) and adapted to the context of this research by Carranza-Bautista et al. (2024).
The evaluation was conducted using a standardized rating scale that examined: Conceptual Coherence. Evaluates how each item reflects the theoretical constructs of the study, ensuring that there are no ambiguities and that there is alignment with the research objectives, to guarantee that the data is relevant and capable of answering the posed questions or hypotheses. Linguistic Validity. Ensures that the items are uniformly understood by the participants, including syntactic and semantic analysis, clarity assessment to eliminate ambiguities, and consideration of the educational level and sociocultural context of the population. Relevance as an Indicator. Its formulation must accurately capture the construct and provide analytical value. Inclusion is justified through previous literature and coherence with the conceptual framework. Methodological Importance. It should be essential for covering the dimensions of the construct and generating actionable data that can test hypotheses, thereby avoiding measurement gaps.
The validation process was implemented through iterative evaluation rounds with a panel of nine experts (N=9), who rated each item on a 4-point Likert scale: None = 0, Slight = 1, Sufficient = 2, Much = 3. This multi-center approach served a dual purpose: first, it strengthened the content validity by ensuring that the items comprehensively reflected the theoretical constructs, and second, it generated empirical evidence regarding their representativeness.
The selection criteria for participants are based on teaching, research, professional experience, and areas of specialty: 3 PhDs in physical activity and sport sciences, 4 medical specialists (one in emergency medicine, one in cardiology, one in internal medicine, and one in sports medicine), and 2 with a master's degree.
Calculation of the Results
According to Pedrosa et al. (2014), to determine the validity index of the experts, the validity of the experts must first be calculated using the Total Content Validity Coefficient (CVCt) method (Hernández-Nieto, 2002). This method helps assess the degree of agreement among the experts. The author of this methodology suggests the participation of at least three to five judges or experts; for our validation, we convened 9 experts.
Figure 1.
Equation of the total content validity coefficient (CVCt). Note: extracted from Hernández-Nieto (2002, p. 72).
Figure 1.
Equation of the total content validity coefficient (CVCt). Note: extracted from Hernández-Nieto (2002, p. 72).
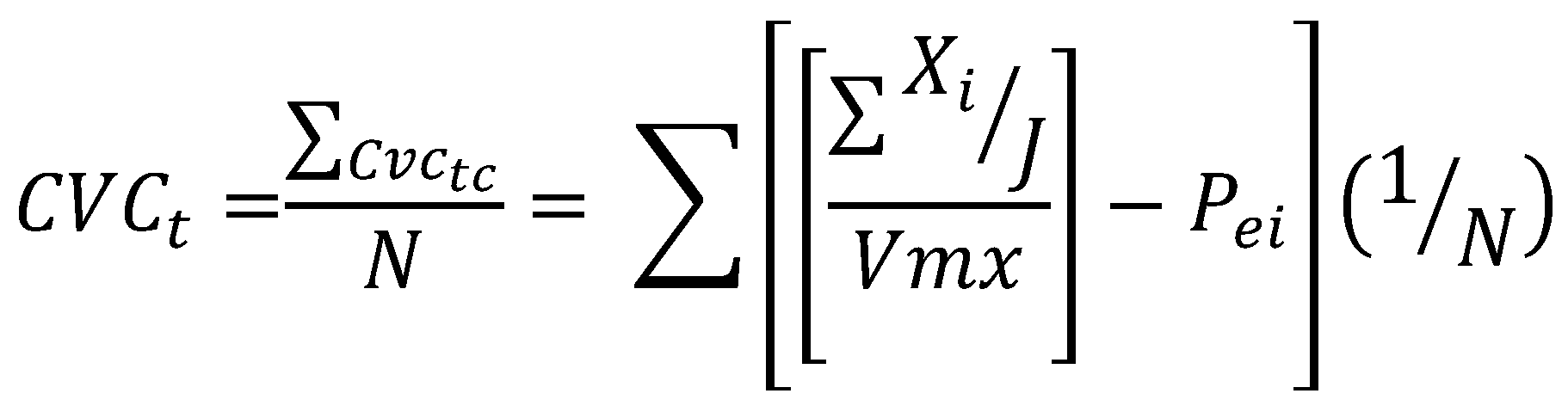
In Table 1, the assigned values from the 9 judges for each of the items in the ques-tionnaire are shown, along with the summation (∑xi); the maximum value (Mx); the Content Validity Coefficient obtained for each item (CVCi), the probability of error for each item (Pei), and finally the total Content Validity Coefficient (CVCt). Additionally, the average values for each of the dimensions are collected.
A comparison was made of the obtained data applied using a formula for each item with the interpretative estimation scale (Pedrosa et al., 2014). In the end, the translated instrument named "Prescription and Counseling of Physical Activity among Health Professionals in the Hospital Setting" (survey) has a validity and agreement index of .92 across the total items. Only two items have an average below 02.90 but above 0.85.

Table 2.
Estimated Scale for Interpreting Content Validity Coefficient.
| (a) Less than .60: Unacceptable validity and agreement. |
| (b) Equal to or greater than .60 and less than or equal to .70: Deficient validity and agreement. |
| (c) Greater than .71 and less than or equal to .80: Acceptable validity and agreement. |
| (d) Greater than .80 and less than .90: Good validity and agreement. |
| (e) Greater than .90: Excellent validity and agreement. |
(Pedrosa et al., 2014).
Procedure
Application of the Survey. To maintain the confidentiality of the participants, the questionnaire asked them to voluntarily and optionally include their name on the survey. Sample Collection. The survey was transferred to a Google Forms platform, a QR code was generated, and an invitation was sent to all departments of medicine at the metropolitan hospital, asking them to scan the QR code with their own mobile phones and complete the survey, which was estimated to take approximately 8 minutes to complete.
Data Analysis
The data analysis was based on descriptive statistics, conducted through a quantitative analysis using a data matrix analyzed via statistical programs like SPSS and EXCEL. The exploratory factor analysis was performed using the maximum likelihood method, KMO tests and Bartlett's sphere were conducted, and finally, reliability was calculated using Cronbach's alpha and McDonald's Omega, following the recommendations of Galindo-Domínguez (2020). Regarding the distribution of items by subscale, a minimum saturation criterion of .40 was considered (Lloret-Segura et al., 2014).
3. Results
Instrument Reliability
Global Cronbach's alpha: 0.857 (for 9 items), indicating that internal consistency is excellent (α > 0.8).
Table 3.
Reliability statistic.
| Cronbach's alpha | Elements |
|---|---|
| 0.857 | 9 |
The following table presents the reliability results for two factors of the instrument, calculated using McDonald's Omega (ω), a robust index that complements Cronbach's alpha, especially useful when items do not meet the assumption of unequal variances.
Table 4.
Exploratory Factor Analysis.
| KMO and Bartlett's Test | ||
|---|---|---|
| Kaiser-Meyer-Olkin Measure of Sampling Adequacy | 0.844 | |
| Bartlett's Test of Sphericity | Approx. Chi-square | 480.107 |
| gl | 36 | |
| Sig. | 0.001 | |
KMO = 0.844, this means it is "very good" for factorization. Bartlett's Test (p < 0.001) confirms sufficient correlations among all items.
Table 5.
Reliability by factors.
| Factor 1 Advice on Physical Exercise | McDonald's ω |
| Estimated | 0.852 |
| 95% CI lower limit | 0.810 |
| 95% CI upper limit | 0.894 |
| Factor 2 Application of Physical Exercise | |
| Estimated | 0.798 |
| 95% CI lower limit | 0.742 |
| 95% CI upper limit | 0.853 |
Factor 1: Advice on Physical Exercise
Point Omega (ω): 0.852, this result allows us to interpret internal consistency as excellent (ω > 0.8). The internal consistency was excellent (ω = 0.852; Dunn et al., 2014). The exploratory factor analysis confirmed two dimensions, CI 95% (0.810, 0.894): this means that the true value of ω in the population has a 95% probability of falling within this range (Watkins, 2018). This implies that the precision of the estimator is high.
Factor 2: Application of Physical Exercise
The reliability analysis of this factor revealed a point Omega (ω) of 0.798, which can be interpreted as good internal consistency. However, the confidence interval showed a wider range compared to Factor 1, suggesting a higher degree of uncertainty in the estimation of internal consistency (Watkins, 2018).
Table 6.
Factor loadings of clinical practices related to the prescription and evaluation of physical exercise.
Table 6.
Factor loadings of clinical practices related to the prescription and evaluation of physical exercise.
| Factor 1 | Factor 2 | |
|---|---|---|
| ¿Aconsejas ejercicio físico (verbal o escrita) para prevenir enfermedades no transmisibles? | 0.820 | |
| ¿Aconsejas ejercicio físico (verbal o escrita) para tratar enfermedades no transmisibles? | 0.784 | |
| ¿Hablas de ejercicio físico con tus pacientes? | 0.702 | |
| ¿Con qué frecuencia preguntas a tus pacientes sobre su nivel de AF? | 0.606 | |
| ¿Crees necesaria la prescripción del ejercicio por profesionales especializados para apoyar en la prevención o tratamiento de ECNT? | ||
| ¿Proporcionas instrucciones escritas sobre algún programa de ejercicio físico a tus pacientes? | 0.799 | |
| ¿Con qué frecuencia refieres a tus pacientes con personal especializado para que realicen una valoración de aptitud física? | 0.695 | |
| ¿Proporcionas instrucciones verbales sobre algún programa de ejercicio físico a tus pacientes? | 0.677 | |
| ¿Consideras importante evaluar la AF a través de un test físico como parte de tus exámenes clínicos? | 0.460 |
The table presents the structure of two main factors derived from exploratory factor analysis, which group the clinical practices related to the promotion of physical activity in patients. The item where no factor loading is observed has a factor loading lower than 0.40, as recommended. Finding by item. (Lloret-Segura et al., 2014).
Table 7.
Finding by ítem.
| ítem | Percentages | Description |
|---|---|---|
| 1) ¿Con qué frecuencia preguntas a tus pacientes sobre su nivel de AF? | - 63.8% Frequently or Very Frequently - Only 4.7% Never.. |
Finding: Most physicians actively inquire about physical activity. |
| 2) ¿Consideras importante evaluar la AF a través de un test físico como parte de tus exámenes clínicos? | - 44.9% Frequently or more. | Almost half of the physicians hysicians do not prioritize formal assessments of physical activity. |
| 3) ¿Con qué frecuencia refieres a tus pacientes con personal especializado para que realicen una valoración de aptitud física? | - 48.8% Never or Very Rarely - Only 26.8% Frequently or more. |
Low integration with specialized physical exercise professionals. |
| 4) ¿Proporcionas instrucciones verbales sobre algún programa de ejercicio físico a tus pacientes? | - 60.6% provide verbal instructions at least "occasionally," combining all the other options: Occasionally, Frequently, and Very Frequently.. - 29.1% do so Never or Very Rarely |
Although most physicians provide verbal instructions, about 30% of them rarely do, suggesting that these opportunities should be utilized to improve active communication. |
| 5) ¿Proporcionas instrucciones escritas sobre algún programa de ejercicio físico a tus pacientes? |
- 55.1% Never or Very Rarely. - Contrast: 60.6% give verbal instructions Occasionally or more. |
Oral communication predominates over written communication. |
| 6) ¿Aconsejas ejercicio físico (verbal o escrita) para prevenir enfermedades no transmisibles? | 70.9% do it frequently or very frequently (38.6% + 32.3%) Only 3.1% state they Never advise it, and another 9.4% do so Very Rarely. |
Most physicians recommend physical exercise as a strategy for the prevention of non-communicable diseases very frequently. |
| 7) ¿Aconsejas ejercicio físico (verbal o escrita) para tratar enfermedades no transmisibles? | 61.1% do so Frequently or Very Frequently (34.6% + 31.5%) The percentage of those who Never advise it rises to 7.1%, compared to 3.1% in prevention. |
Although recommendations also predominate, there is a slight decrease in the frequency with which physicians prescribe exercise as treatment. |
| 8) ¿Hablas de ejercicio físico con tus pacientes? | - 60.6% Frequently or Very Frequently - Only 0.8% Never |
Verbal communication is a very common practice between the physicians and the patient. |
| 9) ¿Crees necesaria la prescripción del ejercicio por profesionales especializados para apoyar en la prevención o tratamiento de ECNT? | - 85% of physicians consider it necessary or very necessary. Frequently-Very Frequently: 37.8% + 47.2% - Only 4.7% consider it Very Rarely necessary. |
There is a high recognition of the importance of the role of exercise specialists, but this contrasts with the low real frequency; they Never or Very Rarely make referrals. |
4. Discussion
Physical activity constitutes a cornerstone in the prevention and treatment of non-communicable chronic diseases (NCDs), as established by the World Health Organization (WHO, 2020). However, its effective implementation in daily clinical practice faces numerous challenges..
Detailed Analysis of Factor 1: Advice on Physical Exercise
This factor consistently grouped items related to active communication between physician and patient, highlighting a clear pattern in the responses. The high reliability of the construct (ω = 0.852), supported by significant factor loadings and elevated internal consistency, suggests that these items coherently measure a single underlying dimension: the quality of communication by the physician.
This finding aligns with recent research, such as the study by Kirk et al. (2023), which identifies physician-patient verbal interaction as a key predictor for adherence to physical activity. Nevertheless, there remains a concerning gap between discourse and clinical practice: only 44.9% of professionals assess PA through standardized physical tests. This discrepancy reveals a critical opportunity to strengthen the implementation of concrete tools that translate theoretical communication into tangible actions during consultations.
Detailed Analysis of Factor 2: Application of Physical Exercise
Despite the analyzed factor demonstrating acceptable reliability (ω = 0.798), its internal structure reveals certain aspects that warrant a critical review. Specifically, the low factor loading of the item related to the evaluation of physical activity through physical tests (0.460) suggests a weak integration with the underlying theoretical construct. Such discrepancies are not unusual in contexts where the application of standardized tools is affected by real clinical conditions. Recent research has indicated that the implementation of physical tests in clinical settings faces significant barriers, such as a lack of time, resources, or insufficient professional training in objective evaluation techniques (Piercy et al., 2018). In many cases, standardized physical tests require specific equipment, adequate spaces, and trained personnel, which are not always available in clinical settings, especially in primary care or centers with logistical constraints (Silsbury, Goldsmith & Rushton, 2015). This situation can generate considerable variability in the way these assessments are implemented and, consequently, bias in the obtaining of results, which, in turn, affects their structural validity within broader or more specific measurement scales or models. Furthermore, it has been shown that health professionals' perception of the applicability of these tests can influence their use, which introduces another level of variability (Pedersen, 2019). Therefore, these findings not only highlight structural limitations in measuring the construct but also point to the need for strategic interventions aimed at improving the capacity of clinical environments to apply physical evaluations systematically and objectively. This may involve both methodological reformulation of the items and strengthening clinical competencies through continuous training and access to adequate resources (WHO, 2020). In summary, although the factor manages to capture relevant dimensions, its heterogeneous operationalization opens an important pathway to refine its measurement and increase its applicability in other real-world scenarios.
Comparative Analysis Between Factors
The comparative study between the two factors reveals notable differences in their consistency and stability. Firstly, Factor 1 demonstrated greater reliability (ω = 0.852) compared to Factor 2 (ω = 0.798), indicating that its items measure the underlying construct with greater accuracy. However, both factors exhibit reliability above the acceptable level (Lloret-Segura et al., 2014). Factor 2 presented a wider confidence interval, suggesting greater variability in its measurements and, consequently, lower stability in its results.
Comparative Analysis Between Factors
The comparative study between the two factors reveals notable differences in their consistency and stability. Firstly, Factor 1 demonstrated greater reliability (ω = 0.852) compared to Factor 2 (ω = 0.798), indicating that its items measure the underlying construct with greater accuracy. However, both factors exhibit reliability above the acceptable level (Lloret-Segura et al., 2014). Factor 2 presented a wider confidence interval, suggesting greater variability in its measurements and, consequently, lower stability in its results.
Finally, it should be noted that all items showed adequate factor saturations (Lloret-Segura et al., 2014) except for the item "Do you think it is necessary for exercise to be prescribed by specialized professionals to support the prevention or treatment of NCDs?" indicating that all of this corresponds to an identified dimension.
This marked difference between verbal communication and documented communication is particularly relevant in light of research such as that of Wolner-Strohmeyer et al. (2021), who demonstrated that written guidance significantly improves long-term adherence to physical exercise in patients adherence to physical exercise in patients.
In the realm of clinical evaluation, the data present a revealing paradox: although 44.9% of professionals recognize the utility of standardized physical tests for evaluating physical activity, more than half (55.1%) rarely or never provide documented instructions. This apparent contradiction reflects, as noted by Van der Wardt et al. (2021), the structural limitations faced by health systems, including time constraints, insufficient resources, and gaps in specialized training.
The situation revealed is very concerning when analyzing referral processes. There is overwhelming consensus (85%) on the necessity for specialists in physical activity to prescribe exercise programs; however, in actual clinical practice, nearly half of the physicians (48.8%) almost never make these referrals. These limitations, indirectly highlighted in the call for a 'multisectoral approach' in the WHO's Global Action Plan (Foster et al., 2017), reflect challenges both globally and locally, where theory does not always translate into practice due to failings in those who manage health systems as well as those who operate within them.
Detailed Clinical Implications
The findings of this study present important challenges and opportunities for optimizing clinical practice in promoting physical exercise. First, improving evaluation processes requires the systematic implementation of validated and quickly applicable tools in clinical contexts. Recent research highlights the usefulness of standardized questionnaires such as the International Physical Activity Questionnaire (IPAQ) and the Physical Activity Readiness Questionnaire (PAR-Q) (Bull et al., 2020), as well as brief functional tests like the sit-to-stand test (Coletta & Phillips), which allow for objective assessment without consuming valuable consultation time.
Second, optimizing physicians-patient communication demands multifaceted interventions. Recent studies emphasize that standardized tools, such as digital forms for exercise prescription or infographics tailored to different literacy levels, significantly improve the clarity and follow-up of recommendations (Howes et al., 2024; Mbanda et al., 2021). Additionally, integrating practical workshops on empathetic communication and establishing collaborative goals has been shown to increase adherence even in reluctant patients, addressing not only educational barriers but also psychosocial ones (Bos-van den Hoek et al., 2018).
Finally, strengthening referral systems requires coordinated and concrete institutional actions. The creation of standardized protocols, such as those proposed by Pedersen et al. (2015), along with established shared responsibility agreements between interdisciplinary networks that include physicians, physical therapists, and exercise science specialists, could resolve the current paradox between theoretical assessment and actual practice for patient referral. The review by Cattuzzo et al. (2016) provides evidence that motor competence and physical fitness are interconnected, but their assessment and intervention lack uniformity. In conclusion, creating joint training programs, based on findings such as those of this review, will optimize the referral and treatment of patients in the specific hospital.
In summary, the effective transformation of these clinical practices will require: first, the adoption of brief but scientific assessment instruments; second, the implementation of standardized communication resources; and third, the institutionalization of evidence-based referral systems. As the WHO (2020) guidelines emphasize, only through this multidimensional approach can the gap between current knowledge and its application in daily patient care be overcome
Evidence-Based Intervention Proposals
The findings of this study suggest the need to implement multilevel interventions to improve the promotion of exercise prescription in clinical settings. At the individual level, it is recommended to conduct practical workshops aimed at healthcare professionals, focused on three key competencies: first, rapid evaluation of physical exercise using validated tools (for example, the Rapid Assessment of Physical Activity (RAPA) questionnaire adapted to clinical contexts (Pérez et al., 2015); second, effective communication techniques based on motivational interviewing enhanced with self-determination strategies (Martins et al., 2019); and third, basic principles of exercise prescription adapted to different populations, including approaches for older adults and chronic patients (Anderson & Durstine, 2019).
At the institutional level, interventions should aim to create support systems for clinical practice. This includes the development of standardized flowcharts for referring patients, clinical record systems that include metrics for physical exercise, and strategic partnerships with community exercise centers (Pedersen & Saltin, 2015). As suggested by the evidence from Cattuzzo et al. (2016), the disconnection between scientific research and practice in motor competence and physical fitness reflects multisystemic barriers. The creation of interdisciplinary networks could overcome these limitations, ensuring more effective patient follow-up.
In terms of public policy, it is proposed to systematically integrate physical exercise into national clinical guidelines for various chronic conditions, following the model of the WHO guidelines (Bull et al., 2020). Concurrently, the creation of professional incentives (both financial and for curriculum development) for those who demonstrate adherence to these protocols, along with funding for accessible community programs, could bridge the gap between medical recommendations and actual access to exercise programs (King et al., 2019).
These interventions, implemented in a coordinated manner, could transform the current fragmented approach into a comprehensive system where the prescription of physical activity is as systematic as any other medical treatment. As highlighted by international recommendations, this multilevel approach is essential for achieving significant impacts on population health (WHO, 2020).
Instrument Reliability and Construct Validity
The instrument used demonstrated some of the highest psychometric properties, evidenced by a Cronbach's alpha of 0.857, along with a McDonald's Omega value of 0.852 for factor 1 (Communication-Counseling) and for factor 2 (Referral-Evaluation). These values significantly exceed the thresholds recommended by Taber (2018), confirming the reliability of the questionnaire for evaluating these dimensions.
Limitations and Future Research
While this study provides valuable evidence regarding clinical practices related to the promotion of physical activity in a secondary-level hospital, it is important to recognize certain methodological limitations that could affect the generalization of the obtained results. First, the research was conducted with a sample confined to a specific geographic and sociocultural context, which limits the possibility of extrapolating the findings to other environments (Rio & Saligan, 2023). This aspect aligns with the literature highlighting how beliefs, cultural norms, and socioeconomic conditions—such as those related to gender roles, religion, or access to public spaces—can vary significantly between communities, impacting the generalization of physical activity interventions (Rio & Saligan, 2023). Additionally, the data collected through questionnaires could be subject to social desirability bias, where participants may have provided responses they deemed more acceptable rather than faithfully reflecting their actual clinical practice (Bispo Júnior, 2022). A third important limitation lies in the reliance on self-reports instead of direct observations or objective measurements, which could affect the validity of the collected data (Liu et al., 2016).
These limitations open up important opportunities for future research in this field. It would be particularly valuable to develop longitudinal studies that assess the medium- and long-term impact of different interventions designed to improve exercise prescription in clinical settings. Additionally, qualitative research like that of Ioannou et al. (2024) provides a deep understanding of the perceived barriers faced by healthcare professionals in promoting physical activity after gestational diabetes, highlighting both institutional factors (e.g., lack of continuity in postnatal care) and personal beliefs (e.g., perceptions of inconvenience or lack of training). These findings further emphasize the need for specific interventions that address not only the structural limitations of the healthcare system but also the attitudes and skills of health personnel to facilitate effective conversations about healthy lifestyles.
Finally, in recent years, it has been recognized that healthcare systems are imple-menting the use of technology. Therefore, it is a priority to evaluate the potential and use of digital tools (such as mobile apps or telemedicine platforms) to overcome some of the limitations identified in this study. For example, recent systematic reviews like that of Bi et al. (2024) demonstrate that digital interventions such as mobile apps, wearables, and smart messaging are effective in significantly increasing daily step counts in university populations (SMD = 0.64; p < 0.001), a key indicator of physical activity. However, the same study reveals that these tools still face challenges in im-pacting higher-intensity activities or reducing sedentary behavior, suggesting the need to complement them with personalized strategies or human support. These findings reinforce the importance of integrating technological solutions with a design centered on the specific gaps identified.
5. Conclusions
The results of this exploratory study reveal a dual landscape in the practices of promoting prescribed physical exercise among the participating physicians. On one hand, effective verbal communication during consultations is identified, where professionals convey recommendations for physical activity in a clear and motivating manner. However, this approach contrasts with critical gaps in the formal assessment of patients' physical activity levels, as well as a notable discrepancy between the theoretical valuation of the importance of physical activity and its translation into concrete referrals to specialized programs.
To close these gaps, the study suggests a multifocal action plan: first, strengthen practical training with assessment and prescription tools for physical exercise during medical education; second, develop standardized protocols that facilitate the systematic and objective integration of physical exercise into patient records; third, establish collaborative networks between primary and secondary care with exercise sciences; and finally, implement institutional policies that prioritize physical exercise as an indicator of quality care. Adopting these measures could catalyze a structural transformation in the management of non-communicable chronic diseases, aligning clinical practice with WHO guidelines (2020) and enhancing the impact of prescribed physical exercise on public health. This approach would not only improve adherence to international recommendations but also reduce the gap between theoretical knowledge and its application in real-world public secondary healthcare settings.
Author Contributions
design, implementation, drafting, methodological development, J. M. H._R. and B. R. R._C.; execution and obtaining results, E. B._J.; statistical analysis M. V_ F.; Design and methodological development D. C._B. All authors have read and agreed to the published version of the manuscript.
Funding
The following work was self-funded
Informed Consent Statement
All participants were verbally informed of the following three points: They we're clearly explained the objectives of the study, the voluntary nature of their participation, and the confidentiality and anonymity of their responses.
Data Availability Statement
Data are available upon request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest in the design, data collection, analysis, interpretation, or writing or this manuscript.
References
- Anderson, E.; Durstine, J.L. Physical activity, exercise, and chronic diseases: A brief review. Sports medicine and health science 2019, 1, 3–10. [Google Scholar] [CrossRef]
- Bi, S.; Yuan, J.; Wang, Y.; Zhang, W.; Zhang, L.; Zhang, Y.; Zhu, R.; Luo, L. Effectiveness of digital health interventions in promoting physical activity among college students: Systematic review and meta-analysis. Journal of Medical Internet Research 2024, 26, e51714. [Google Scholar] [CrossRef]
- Bispo Júnior, J.P. Social desirability bias in qualitative health research. Revista de Saúde Pública 2022, 56, 101. [Google Scholar] [CrossRef]
- Börjesson, M. (2013). Förderung körperlicher aktivität im Krankenhaus. In Deutsche Zeitschrift fur Sportmedizin (Vol. 64, Issue 6, pp. 162–165). Dynamic Media Sales Verlag. [CrossRef]
- Bos-van den Hoek, D.W.; Visser, L.N.C.; Brown, R.F.; Smets, E.M.A.; Henselmans, I. Communication skills training for healthcare professionals in oncology over the past decade: a systematic review of reviews. Current opinion in supportive and palliative care 2019, 13, 33–45. [Google Scholar] [CrossRef]
- Bowen, Pamela & Mankowski, Robert & Harper, Sara & Buford, Thomas. Exercise Is Medicine as a Vital Sign: Challenges and Opportunities. Translational journal of the American College of Sports Medicine 2019, 4, 1–7. [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G. Willumsen, J.F. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. British Journal of Sports Medicine 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Carranza-Bautista, D.; Janeth, F.; Mendoza, M.; Javier, F.; Farias, M.; Nava, R.R. (2024). Diseño y validación de un modelo de gestión de actividad física y del deporte universitario Design and validation of a management model for physical activity and university sports. In Retos (Vol. 57). [CrossRef]
- Cattuzzo, M.T.; Dos Santos Henrique, R.; Ré, A.H.; de Oliveira, I.S.; Melo, B.M.; de Sousa Moura, M.; de Araújo, R.C.; Stodden, D. Motor competence and health related physical fitness in youth: A systematic review. Journal of science and medicine in sport 2016, 19, 123–129. [Google Scholar] [CrossRef] [PubMed]
- Dunn, T.J.; Baguley, T.; Brunsden, V. From alpha to omega: A practical solution to the pervasive problem of internal consistency estimation. British Journal of Psychology 2014, 105, 399–412. [Google Scholar] [CrossRef]
- Foster, C.; Shilton, T.; Westerman, L.; Varney, J.; Bull, F. World Health Organisation to develop global action plan to promote physical activity: time for action. British journal of sports medicine 2017, 52, 484–485. [Google Scholar] [CrossRef]
- Galindo-Domínguez, H. (2020). Estadística para no estadísticos: una guía básica sobre la metodología cuantitativa de trabajos académicos (Vol. 59). 3ciencias.
- Hernández Sampieri,R.; Mendoza-Torres. (2023). Metodología de la investigación: Las rutas cuantitativa, cualitativa y mixta (2a ed.). McGraw-Hill.
- Hernández-Nieto, R. (2002). Contributions to Statistical Analysis. Universidad de los Andes file:///E:/Articulos%20cientificos/Coeficiente%20de%20Validez%20de%20contenido.pdf.
- Howes, S.; Stephenson, A.; Grimmett, C.; Argent, R.; Clarkson, P.; Khan, A.; Lait, E.; McDonough, L.R.; Tanner, G.; McDonough, S.M. The effectiveness of digital tools to maintain physical activity among people with a long-term condition(s): A systematic review and meta-analysis. Digital health 2024, 10, 20552076241299864. [Google Scholar] [CrossRef] [PubMed]
- Ioannou, E.; Humphreys, H.; Homer, C.; Purvis, A. Barriers and system improvements for physical activity promotion after gestational diabetes: A qualitative exploration of the views of healthcare professionals. Diabetic medicine : a journal of the British Diabetic Association 2024, 41, e15426. [Google Scholar] [CrossRef]
- Coletta, G.; Phillips, S.M. An elusive consensus definition of sarcopenia impedes research and clinical treatment: A narrative review. Ageing Research Reviews 2023, 86, 101883. [Google Scholar] [CrossRef]
- King, A.C.; Whitt-Glover, M.C.; Marquez, D.X.; Buman, M.P.; Napolitano, M.A.; Jakicic, J.; Fulton, J.E.; Tennant, B.L. ; 2018 PHYSICAL ACTIVITY GUIDELINES ADVISORY COMMITTEE* Physical Activity Promotion: Highlights from the 2018 Physical Activity Guidelines Advisory Committee Systematic Review. Medicine and science in sports and exercise 2019, 51, 1340–1353. [Google Scholar] [CrossRef] [PubMed]
- Kirk, B.O.; Khan, R.; Davidov, D.; Sambamoorthi, U.; Misra, R. (2023). Exploring facilitators and barriers to patient-provider communication regarding diabetes self-management. PEC Innovation, 3. [CrossRef]
- Krops, L.A.; Bouma, A.J.; van Nassau, F.; Nauta, J.; van den Akker-Scheek, I.; Bossers, W.J.R.; Brügemann, J.; Buffart, L.M.; Diercks, R.L.; de Groot, V.; de Jong, J.; Kampshoff, C.S.; van der Leeden, M.; Leutscher, H.; Navis, G.J.; Scholtens, S.; Stevens, M.; Swertz, M.A.; van Twillert, S.; … Dekker, R. (2020). Implementing individually tailored prescription of physical activity in routine clinical care: Protocol of the physicians implement exercise = Medicine (PIE=M) development and implementation project. JMIR Research Protocols, 9. [CrossRef]
- Liu, S.H.; Eaton, C.B.; Driban, J.B.; McAlindon, T.E.; Lapane, K.L. Comparison of self-report and objective measures of physical activity in US adults with osteoarthritis. Rheumatology international 2016, 36, 1355–1364. [Google Scholar] [CrossRef]
- Lloret-Segura, S.; Ferreres-Traver, A.; Hernández-Baeza, A.; Tomás-Marco, I. El análisis factorial exploratorio de los ítems: una guía práctica, revisada y actualizada. Anales de Psicología 2014, 30, 1151–1169. [Google Scholar] [CrossRef]
- Loo, R. (2002), The Delphi method: a powerful tool for strategic management, Policing: An International Journal, Vol. 25 No. 4, pp. 762–769. [CrossRef]
- Lundqvist, S.; Boorjesson, M.; Larsson, M.E.H.; Hagberg, L.; Cider, A. Physical Activity on Prescription (PAP), in patients with metabolic risk factors. A 6- month follow-up study in primary health care. PLoS ONE 2017, 12. [CrossRef]
- Martins, J.; Costa, J.; Sarmento, H.; Marques, A.; Farias, C.; Onofre, M.; Valeiro, M.G. Adolescents’ Perspectives on the Barriers and Facilitators of Physical Activity: An Updated Systematic Review of Qualitative Studies. International Journal of Environmental Research and Public Health 2019, 18, 4954. [Google Scholar] [CrossRef]
- Mbanda, N.; Dada, S.; Bastable, K.; Ingalill, G.B.; Ralf, W.S. A scoping review of the use of visual aids in health education materials for persons with low-literacy levels. Patient education and counseling 2021, 104, 998–1017. [Google Scholar] [CrossRef]
- Mostafa, M.M. Post-materialism, Religiosity, Political Orientation, Locus of Control and Concern for Global Warming: A Multilevel Analysis Across 40 Nations. Social Indicators Research 2016, 128, 1273–1298. [Google Scholar] [CrossRef]
- Noetel, M.; Sanders, T.; Gallardo-Gómez, D.; Taylor, P.; Del Pozo Cruz, B.; Van Den Hoek, D.; Smith, J.J.; Mahoney, J.; Spathis, J.; Moresi, M.; Pagano, R.; Pagano, L.; Vasconcellos, R.; Arnott, H.; Varley, B.; Parker, P.; Biddle, S.; Lonsdale, C. (2024). Effect of exercise for depression: Systematic review and network meta-analysis of randomised controlled trials. BMJ. [CrossRef]
- Organizacion Mundial de la Salud. (2018). PERSONAS MÁS ACTIVAS PARA UN MUNDO MÁS SANO. Available online: https://www.paho.org/es/documentos/plan-accion-mundial-sobre-actividad-fisica-2018-2030-mas-personas-activas-para-mundo.
- Pedersen, B.K. The physiology of optimizing health with a focus on exercise as medicine. Annual review of physiology 2019, 81, 607–627. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Saltin, B. Exercise as medicine–evidence for prescribing exercise as therapy in 26 different chronic diseases. Scandinavian Journal of Medicine & Science in Sports 2015, 25, 1–72. [Google Scholar] [CrossRef]
- Pedrosa, I.; Suárez-Álvarez, J.; García-Cueto, E. Evidencias sobre la Validez de Contenido: Avances Teóricos y Métodos para su Estimación. Acción Psicológica 2014, 10, 3–18. [Google Scholar] [CrossRef]
- Pérez, JC, Bustamante, C.; Campos, S.; Sánchez, H.; Beltrán, A.; Medina, M. Validación de la Escala Rapid Assessment of Physical Activity (RAPA) en población chilena adulta consultore en Atención Primaria. Aquichán 2015, 15, 486–498. [CrossRef]
- Piercy, KL, Troiano, RP, Ballard, RM, et al. Guías de actividad física para estadounidenses. JAMA 2018, 320, 2020–2028. [CrossRef]
- Rio, C.J.; Saligan, L.N. Understanding physical activity from a cultural-contextual lens. Frontiers in public health 2023, 11, 1223919. [Google Scholar] [CrossRef] [PubMed]
- Silsbury, Z.; Goldsmith, R. y Rushton, A. Systematic review of the measurement properties of self-report physical activity questionnaires in healthy adult populations. BMJ Open 2015, 5, e008430. [Google Scholar] [CrossRef] [PubMed]
- Taber, K.S. The use of Cronbach's alpha when developing and reporting research instruments in science education. Research in Science Education 2018, 48, 1273–1296. [Google Scholar] [CrossRef]
- Teferi, G.; Kumar, H.; Singh, P. Physical Activity Prescription for Non-Communicable Diseases: Practices of Healthcare Professionals in Hospital Setting, Ethiopia. IOSR Journal of Sports and Physical Education 2017, 04, 54–60. [Google Scholar] [CrossRef]
- Van der Wardt, V.; di Lorito, C.; Viniol, A. Promoting physical activity in primary care: a systematic review and meta-analysis. The British journal of general practice : the journal of the Royal College of General Practitioners 2021, 71, e399–e405. [Google Scholar] [CrossRef]
- Watkins, M.W. Exploratory Factor Analysis: A Guide to Best Practice. Journal of Black Psychology 2018, 44, 219–246. [Google Scholar] [CrossRef]
- Wolner-Strohmeyer, G.; Keilani, M.; Mähr, B.; Morawetz, E.; Zdravkovic, A.; Wagner, B.; Palma, S.; Mickel, M.; Jordakieva, G.; Crevenna, R. Can reminders improve adherence to regular physical activity and exercise recommendations in people over 60 years old?: A randomized controlled study. Wiener klinische Wochenschrift 2021, 33, 620–624. [Google Scholar] [CrossRef]
- World Health Organization. (2020). WHO guidelines on physical activity andsedentary behaviour. Available online: https://www.who.int/publications/i/item/9789240015128.
Table 1.
Assigned values from the 9 judges.
| Ítems | Judges | Formulas | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Judges 1 | Judges 2 | Judges 3 | Judges 4 | Judges 5 | Judges 6 | Judges 7 | Judges 8 | Judges 9 | Sx1 | Mx | CVCi | Pei | CVCtc | |
| item 1 | 9 | 11 | 11 | 12 | 12 | 12 | 7 | 12 | 8 | 94 | 7.83333333 | 0.87037037 | 2.58117E-09 | 0.87037037 |
| item 2 | 12 | 8 | 10 | 11 | 11 | 12 | 9 | 12 | 12 | 97 | 8.08333333 | 0.89814815 | 2.58117E-09 | 0.89814815 |
| item 3 | 10 | 9 | 12 | 9 | 12 | 12 | 11 | 12 | 12 | 99 | 8.25 | 0.91666667 | 2.58117E-09 | 0.91666666 |
| item 4 | 12 | 12 | 10 | 12 | 9 | 12 | 11 | 12 | 12 | 102 | 8.5 | 0.94444444 | 2.58117E-09 | 0.94444444 |
| item 5 | 12 | 7 | 12 | 9 | 12 | 12 | 11 | 12 | 12 | 99 | 8.25 | 0.91666667 | 2.58117E-09 | 0.91666666 |
| item 6 | 10 | 12 | 12 | 12 | 12 | 12 | 11 | 12 | 10 | 103 | 8.58333333 | 0.9537037 | 2.58117E-09 | 0.9537037 |
| item 7 | 12 | 12 | 12 | 12 | 12 | 12 | 11 | 11 | 10 | 104 | 8.66666667 | 0.96296296 | 2.58117E-09 | 0.96296296 |
| item 8 | 12 | 12 | 9 | 12 | 12 | 12 | 6 | 12 | 12 | 99 | 8.25 | 0.91666667 | 2.58117E-09 | 0.91666666 |
| item9 | 11 | 12 | 12 | 11 | 10 | 12 | 11 | 12 | 9 | 100 | 8.33333333 | 0.92592593 | 2.58117E-09 | 0.92592592 |
| Total sum of the CVCtc | 8.30555553 | |||||||||||||
| General average | 0.9228395 | |||||||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



