Submitted:
06 August 2025
Posted:
07 August 2025
You are already at the latest version
Abstract
Objective: The efficiency of the vegetarian diet on the health state highlighted through the monitoring of the biochemical parameters to persons of different ages and therapeutic approach variants in the treatment of the metabolic syndrome and premature aging. Material and method: The patient group consisting of 150 patients diagnosed with metabolic syndrome has followed a vegetarian diet (approximately 2100 calories/day), designed to prevent and fight the cholesterol level in the serum, the level of glucose in the serum and the level of uric acid in the serum. The group was subjected to an intensive program that has included, besides the vegetarian diet and physical activity (physical therapy), an anti-stress program, a smoke-quitting program, weight controlling, blood pressure management, diabetes management, psychological counseling and group therapy. Results: The patient group which has taken part into the study has followed a vegetarian diet which included 65% carbohydrates, mostly complex, 52.4 g dietary fibers, ≤ 23% lipids with a 2.24/1 ratio between polyunsaturated fats and saturated fats; 3.8 mg essential linoleic fatty acid and 0 mg cholesterol and 15% proteins, with an intake of 2100 calories/day. This diet has been designed taking into consideration the recommendations of the American Dietetic Association, the Institute of Medicine of the National Academy of Sciences and of the American Diabetes Association, which recommend that the total energy intake should consist of 45-65% carbohydrates, 20-35% lipids and 10-35% proteins. Conclusions: We could identify a series of major factors in the people’s lifestyle which are important for maintaining a good health state, but diet and physical activity are ranking on the first two places. 10 days after the start of the therapies we have observed the following: the level of total serum cholesterol has decreased in average by 41.21 mg/dL; serum triglycerides dropped in average with 72.86 mg/dL; LDL cholesterol dropped with 26.24 mg/dL in average; Glycemia dropped by 30.4mg/dL in average; body mass dropped by 2.99 kg in average; systolic blood pressure dropped by 10.82 mmHg in average, and the diastolic blood pressure dropped by 6.44 mmHg in average. In conclusion, through the results of this study, we can say that the total vegetarian diet has a positive impact on patients with metabolic syndrome in particular, but also on the human health and on the premature aging in general.
Keywords:
diet
; premature aging
; metabolic syndrome
; vegan diet
; health
1. Introduction
Based on their effects on the metabolism function, nutritive substances are classified in 5 groups: proteins, carbohydrates, minerals and vitamins. Each of these should represent a specific percent of a daily diet: 11-13% - proteins, 55-65% - carbohydrates, 20-30% - lipids. Essential nutrients which cannot be synthesised by the human body must be obtained from a balanced diet. These are represented by water, fatty acids (alfa linolenic and linolenic acid), amino-acids (leucine, isoleucine, lysine, methionine, phenylalanine, threonine, tryptophane, valine), some minerals and vitamins (1).
In order to get most of a good nutrition, we must follow the 8 principles of a healthy diet, promoted by Dr. Colin Campbell, director of the China-Oxford-Cornell Project, mentioned in his book named “China Project” (2).
Over the past decades, many doctors, nutritionists and researchers invented different types of diets, each having a different goal, objective and results. Below we refer to the most popular and well researched diets, published in articles such as: Medical News Today and U.S. News (3,4). Some kinds of known diets are represented by: Atkins, Zone, Keto, Vegetarian diet, Vegan diet, raw vegan diet, South Beach, Weight Watchers diet, Mediterranean diet, traditional and Western diets.
Other than its positive effects, the vegetarian diet has multiple metabolic benefits: the increase of butyrate in intestinal microbiota which induces incretin secretion and improves glucose metabolism (same effect as plant-based polyphenols), boosting β-pancreatic cells functions (while saturated fats rich meats cause β-pancreatic cells while, omega-3 fatty acids found in fish decrease insulin secretion and post-prandial GLP-1 levels. This diet significantly improves mental health and life quality (5-8). These benefits are demonstrated in relatively small population groups, known for their longevity and good health condition (Okinawa Island inhabitants, Hunza Tribe from Central Asia, Sherpa people from Nepal, Otomi Indians and inhabitants of Vilcabamba Valley from South America) (9).
Metabolic syndrome (insulin resistance, X syndrome) represents an important risk factor for cardiovascular diseases, type 2 diabetes and hepatic steatosis comprehending a large group metabolic disorders: abdominal obesity, arterial hypertension, dyslipidemia and endothelium dysfunction (10,11). Its causes are complex, involving a series of interactions between genetic, metabolic, environmental and hormonal risk factors, which in the end lead to metabolic syndrome characteristics: obesity/overweight, sedentary lifestyle, frailty and lipodystrophy. Insulin resistance is the central factor in metabolic syndrome development. Intracellular excess of fatty acids metabolites contributes to changes in intracellular signaling pathways leading to insulin resistance and triglycerides conglomerates within skeletal, heart muscles and liver as well as an increase in hepatic glucose production. Adipose tissue excess is followed by proinflammatory cytokines over-synthesis (11,12).
According to a consensus published in 2009 by American Heart Association and National Heart, Lung and Blood Institute, metabolic syndrome diagnosis is made on 3 or more of the 5 main criteria: central obesity, hypertriglyceridemia, low levels of HDL, high blood pressure and fasting blood sugar (10,12). In regard with its management, the following treatment scheme should be followed: bariatric surgery, lifestyle changes and drug therapy.
2. Materials and Methods
Plant based diets are known for having a major impact on chronic disorders prevention and treatment. The observed lot had 150 patients, diagnosed with metabolic syndrome that had an exclusive vegetarian diet, diversified according to physiological needs. Its calorie count was about 2100 calories/day, formulated in order to target:
Normalising cholesterol plasmatic levels, lipids providing 23% of total daily caloric intake (5% saturated lipids, 5% mono-non-saturated fats, 13% poli-non-saturated fats, 3,8g of linoleic acid);
Normalising blood sugar levels, carbohydrates providing 66% of total daily caloric intake (mostly complex carbohydrates from whole wheat bread and cereals which provide 52,4 g of fibres);
Normalising uric acid serum levels, proteins providing 12% of total daily caloric intake (only plant-based proteins) (13).
Our lot underwent an intensive procedure that included plenty of protective factors, besides the vegetarian diet, a physical programme, antistress and psychological counselling, support for quitting smoking, body weight control, blood pressure management and group therapy (11). The key aspects of this programme are physical activity and diet.
2.1. Exclusive Vegetarian Diet
This diet does not consist of cholesterol, is rich in vitamins (beta carotene, folic acids, B1, B3, B6, C, E), minerals (Mg, Fe, K, Se) and phytochemicals. It was made after vegetarian diet pyramid, elaborated by dr. Ella Haddad from university of medicine of Loma Linda (2008 version) – Figure 1 (13).
Figure 1.
Vegetarian Diet Pyramid (adapted from 2008 version).
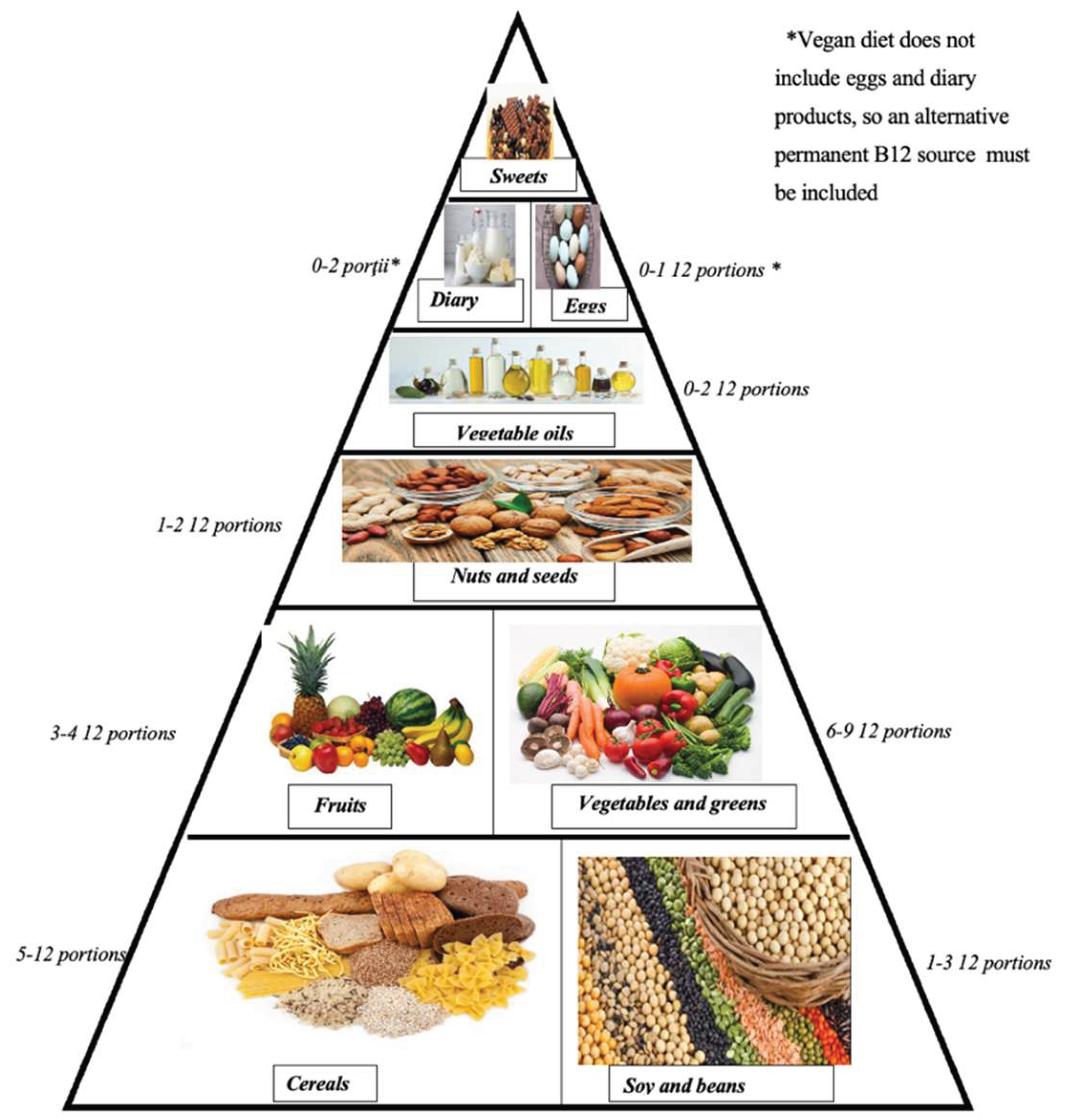
The vegetarian diet pyramid includes the main food groups: those from the top are necessary in a small quantity, while at the base most important foods as nutritional intake are necessary in a higher amount (13). As a result, in designing the daily menu, we considered these nutritional groups, but with less portions from each category.
Additionally, the following principles were respected in planning the menu:
- (1)
-
The quality principle:
- Choose foods from the above list (Figure 1);
- Avoid refined or fibre lacking foods;
- Fibre rich foods are: whole grain cereals, vegetables, fruits;
- Foods with less amounts of fibre: refined foods: white flour, sugar, meat, milk, eggs.
- (2)
-
The quantity principle:
- Breakfast represents the most important meal of the day and it should be composed by whole grain cereals, nuts, milk and fruits;
- Lunch is an important meal as well and int needs to satisfy the need of nutriments for the rest of the day. It should have a product rich in proteins;
- Dinner should be the lightest meal of the day, composed mainly of fruits. It is indicated that elderly individuals and sedentary people abstain from it.
- (3)
-
Time principle:
- Respect an organised and regular food schedule, have the last meal at 19:00, the latest;
- Keep a 5-6 hours interval between meals in which no snack is allowed;
- Allocate at least 30 minutes for each meal.
- (4)
-
Diversity principle:
- Each day the foods should vary;
- Eat a maximum of 2-3 types of dishes at each meal.
- (5)
-
The cooking principle:
- Keep the natural taste of food and avoid salt and irritant spices (pepper, chilli) excess;
- Avoid frying and boil, steam or bake the food;
- Decrease salt and rich in salt foods consumption: pickles, cheese, canned foods.
Each patient’s menu included:
- 1)
-
Breakfast: 40-50% of total daily calories intake
- Boiled cereals (oat flakes, wheat, groats), granola, musli, cornflakes;
- Whole grain bread;
- Fruits: apples, pears, bananas, apricots, citrus, forest fruits, other seasonal fruits;
- Spreadable creams, fruit jam, peanut butter, avocado, soy pate;
- Nuts or seeds;
- Soy/rice/coconut/almond/sesame milk (13).
- 2)
-
Lunch
- Main dish: meat/veggie balls, veggie-burgers, vegetables, nutty and seed derivates;
- Side dishes made from raw or boiled vegetables;
- Raw salads, fish with dressings or salads;
- Whole grain bread;
- Desserts (13).
- 3)
-
Evening Dinner
- Soups or salads;
- Fruits, fruit crisps, fruit salads;
- Smoothies;
- Whole grain bread, biscuits, whole grain cereals, popcorn (13).
6 o’clock tea – for patients that want to lose weight (in order to balance their metabolic disorders in conditions such as type 2 diabetes).
2.2. Physical Activity (Kinesiotherapy)
Physical activity, the second key element of the programme was represented by any movements produced by muscular-skeletal activity which leads to a substantial increase in energy production above resting levels. There are over 640 muscles in the human body, representing 30-45% of total body weight, consuming 25% of the energy used while resting. It is known that moderate physical activity: running, power walking, swimming regularly practiced at least 30 minutes per day lowers the blood pressure by 4-9 mmHg compared to first measurements (14). The most important outcomes that must be kept in mind are: decreased insulin secretion before meals and higher insulin sensitivity that reduces cardiovascular risk factors and weight loss (15).
Our lot underwent a physical 2,5 hours activity program with an intensity varying from 2 to 6 METs in regard with their chronic disease.
- A.
- Patient educational workshops: health, nutrition and healthy cooking classes.
- B.
- Other therapies
- Hydrotherapy (15).
- Swedish massage for relaxation and posture (50 minutes);
- Clay and paraffin packing;
- Charcoal and plant patches;
- Phytotherapy
- Psychological counselling
- C.
- Blood tests parameters
- Optimal value of total cholesterol <200 mg/dL;
- HDL cholesterol optimal value of ≥50 mg/dL (females) and ≥ 40mg/dL (males);
- LDL cholesterol optimal value of <100 mg/dL;
- Serum triglycerides levels <150 mg/dL;
- Fasting blood sugar level between 65-110 mg/dL;
- Based on BMI value, patients can be classified as:
*under-weight < 18,5 kg/m²;
* Normal range - 18,5-24,9 kg/m²;
* Over-weight: 25-29,9 kg/m²;
* Obese ≥ 30 kg/m².
-Other routine investigated parameters included: uric acid, urea, creatinine, atherogenic coefficient, calcium, magnesium.
- D.
- Blood pressure monitoring
Blood pressure in healthy adults is classified as below:
- ideal blood pressure: 110/60 mmHg;
- optimal blood pressure: <120/80 mmHg;
- normal blood pressure: <130/85 mmHg;
- borderline blood pressure: <140/90 mmHg;
Patients with a value of 140/90mmHg or higher are diagnosed with arterial hypertension, which can be classified in class I, class II– mild, class III – severe (14)
- E.
- Patient index
150 patients were involved in our study (82 females and 68 males), from 36 to 80 years old, with an average age of 61.45 years old:
* Between 35 & 45 years old: 7 patients
* Between 46 & 55 years old: 31 patients
* Between 56 & 65 years old: 65 patients
* Between 66 &75 years old: 36 patients
* Over 75 years old: 11 patients
- F.
- Blood tests
We analysed venous blood samples to evaluate metabolism and different parameters.
2. Results and Discussion
The patient lot that underwent our study followed a 100% vegetarian diet with a 65% carbo hydrates, mostly complex, 52,4g fibres, ≤ 23% fats with a 2.24/1 ratio of polyunsaturated fats and saturated, 3.8 mg of essential linolenic acid, 0 mg of cholesterol and 15% proteins with a daily caloric intake of 2100 calories/day. This diet was planned according to the guidelines issued by the Academy of Nutrition and Dietetics, the American Diabetes Association and the Medical Institute of American Academy of Science that recommend distributing the energy intake from various sources: 45-65% carbohydrates, 20-35% lipids and 10-35% from proteins (16)
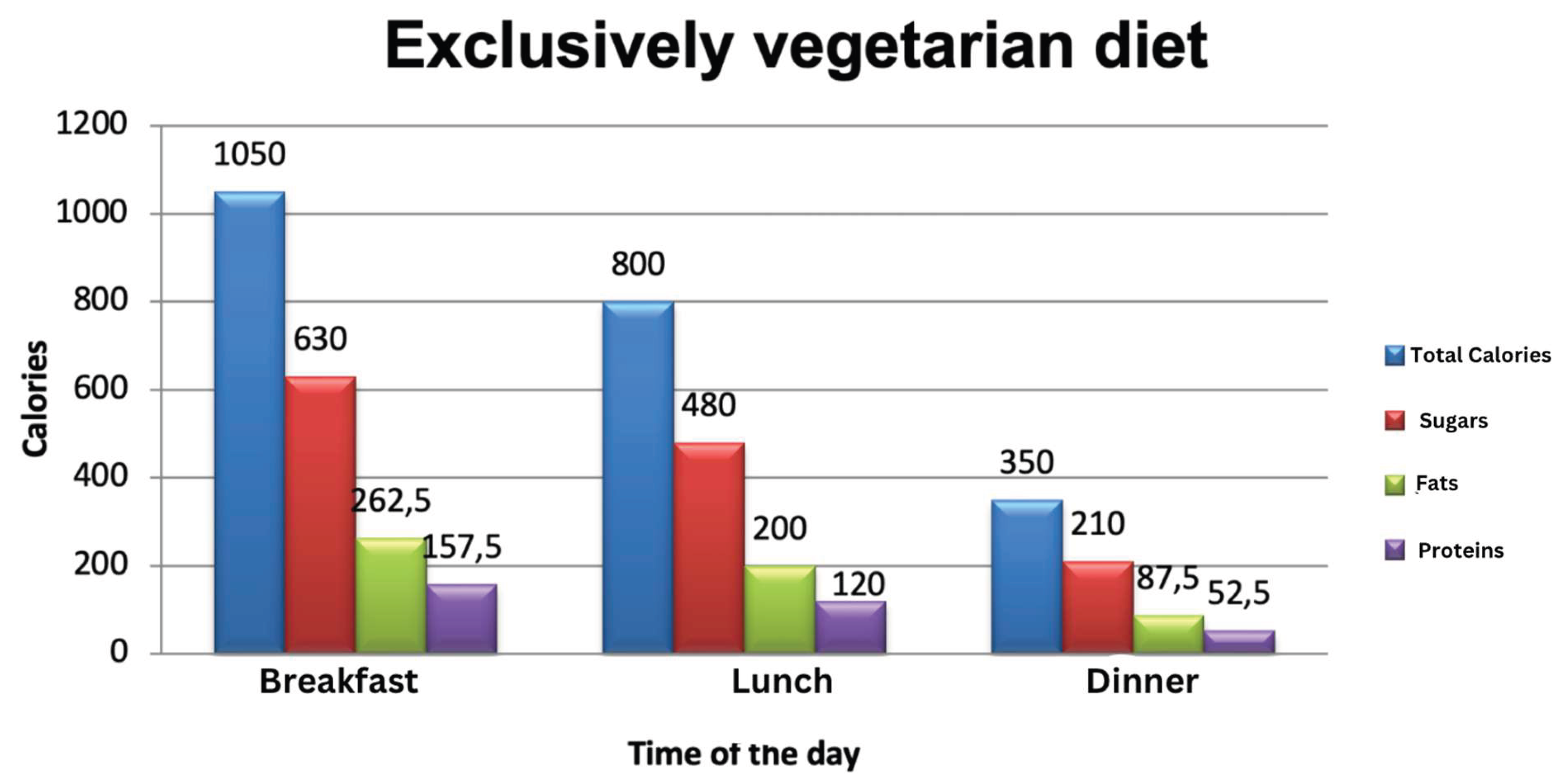
The first graphic shows the overall calories consumption, calories from sugar, fats and proteins according to different times of the day, with a more calories intake during breakfast and lunch with a gastro-protective and hypocaloric dinner.
Graph 1.
Total calories intake of our study lot (adapted after Nicolae D. and Valentina D.).
A comparative analysis of blood tests parameters before and after 10 days of lifestyle changes is shown in Figure 2 to Figure 16. The results are statistically significant.
Our findings shown the following:
- Serum Cholesterol levels:
Figure 2.
Cholesterol level evolution in males at admission & at the end of the programme (in 10 days).
Figure 2.
Cholesterol level evolution in males at admission & at the end of the programme (in 10 days).
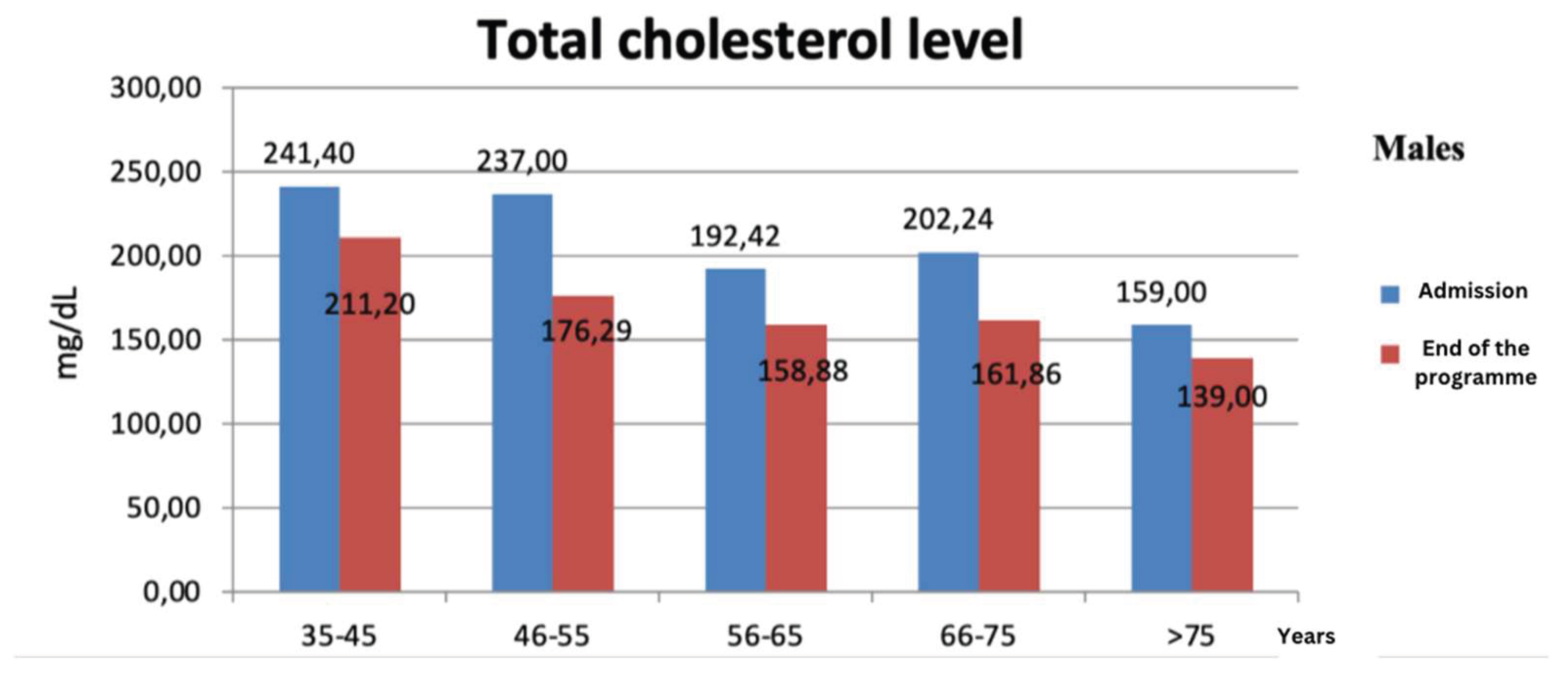
From 150 patients, 83 presented on admission over 200 mg/dl cholesterol, and after 10 days, only 29 patients registered values higher than normal.
On average, in males cholesterol level decreased with 36.98 mg/dl, while the best results were in patients aged between 46-55 years where the average value decreased with 60.71 mg/dl following this programme (Figure 2).
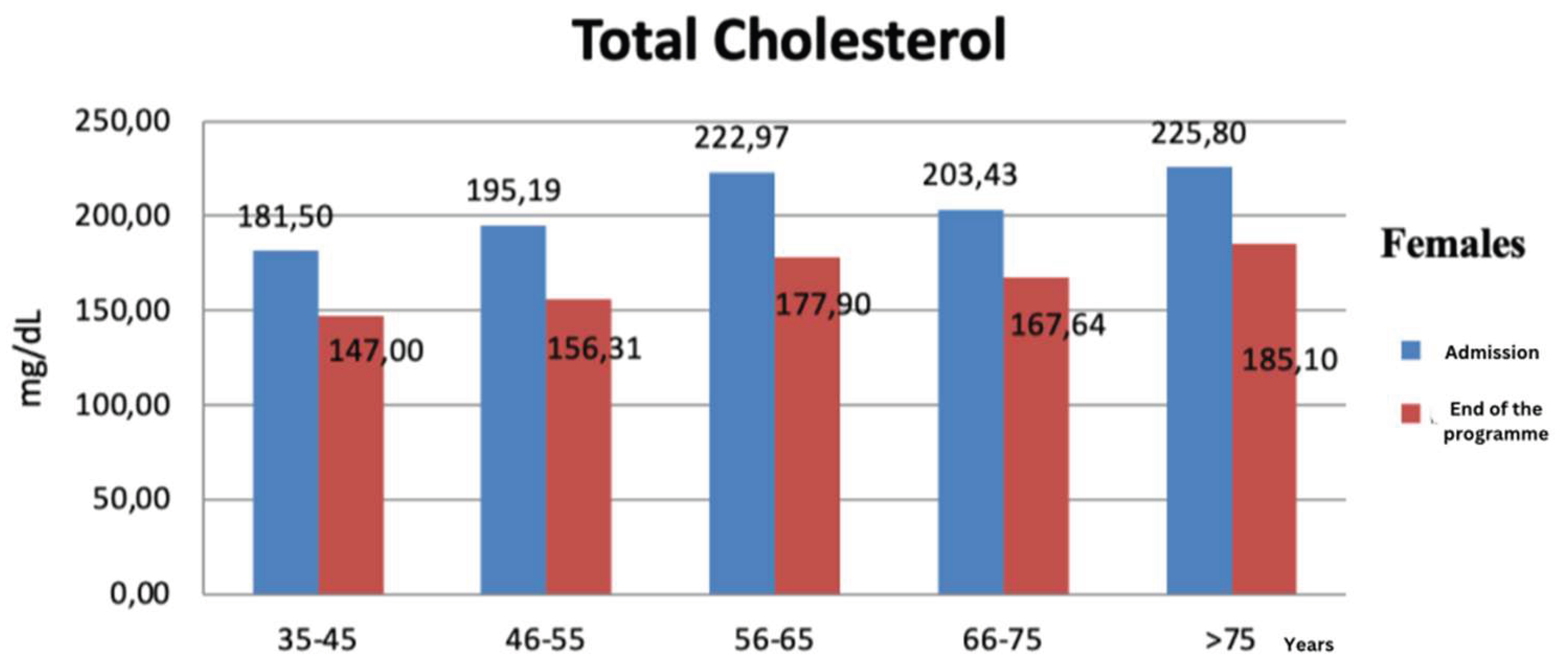
In the female group, the cholesterol levels decreased on average with 39.07 mg/dl, but most significant results were observed in the age group between 56-65 years old in which the average value decreased with 45.07 mg/dl (Figure 3).
Figure 2.
Cholesterol level evolution in females at admission & at the end of the programme (in 10 days).
Figure 2.
Cholesterol level evolution in females at admission & at the end of the programme (in 10 days).
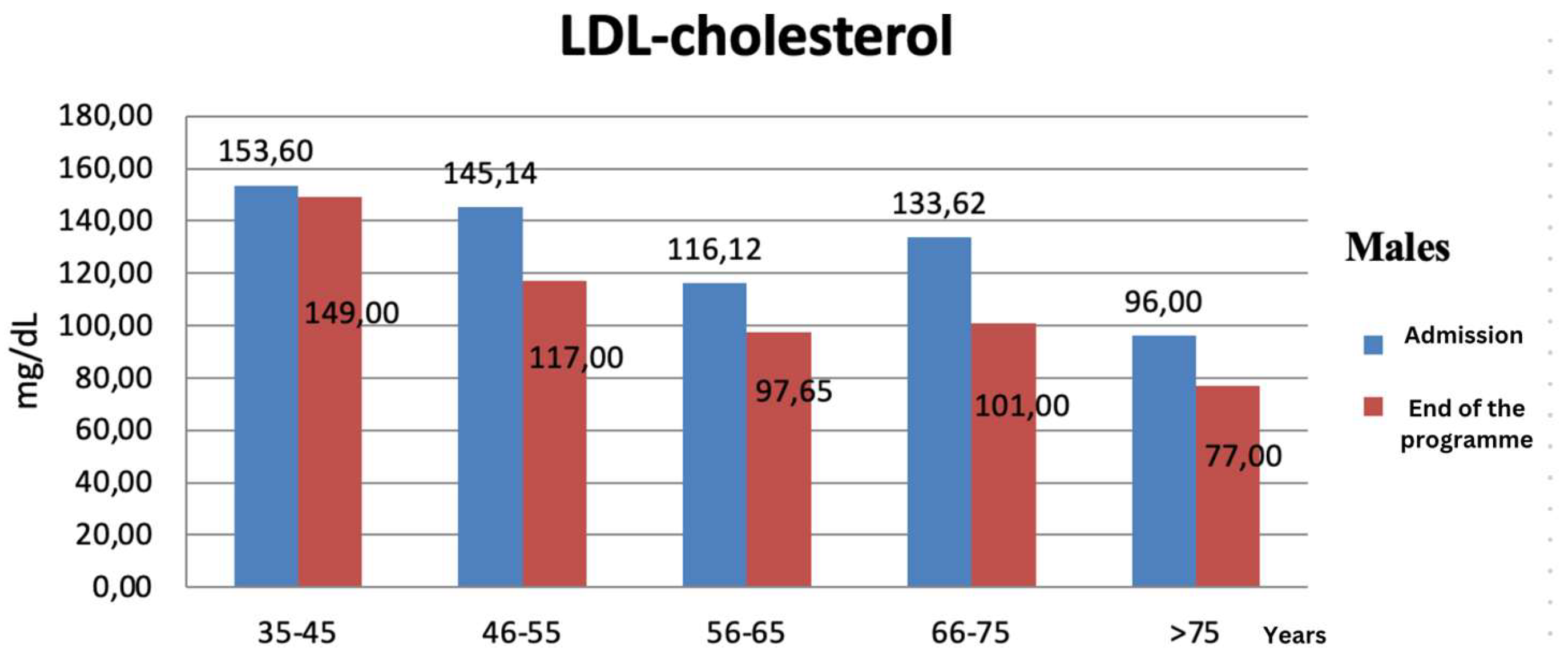
- LDL- Cholesterol:
From all 150 patients, on admission, 114 had LDL-cholesterol value over 100 mg/dl compared with only 72 patients that had higher LDL-cholesterol levels after 10 days. In males, LDL decreased on average with 20.57 mg/dl, but the best results were observed in males aged between 66-75 years old in which the average value decreased with 32.62 mg/dl (Figure 4).
Figure 3.
LDL- cholesterol evolution in males at admission & at the end of the programme (in 10 days).
Figure 3.
LDL- cholesterol evolution in males at admission & at the end of the programme (in 10 days).
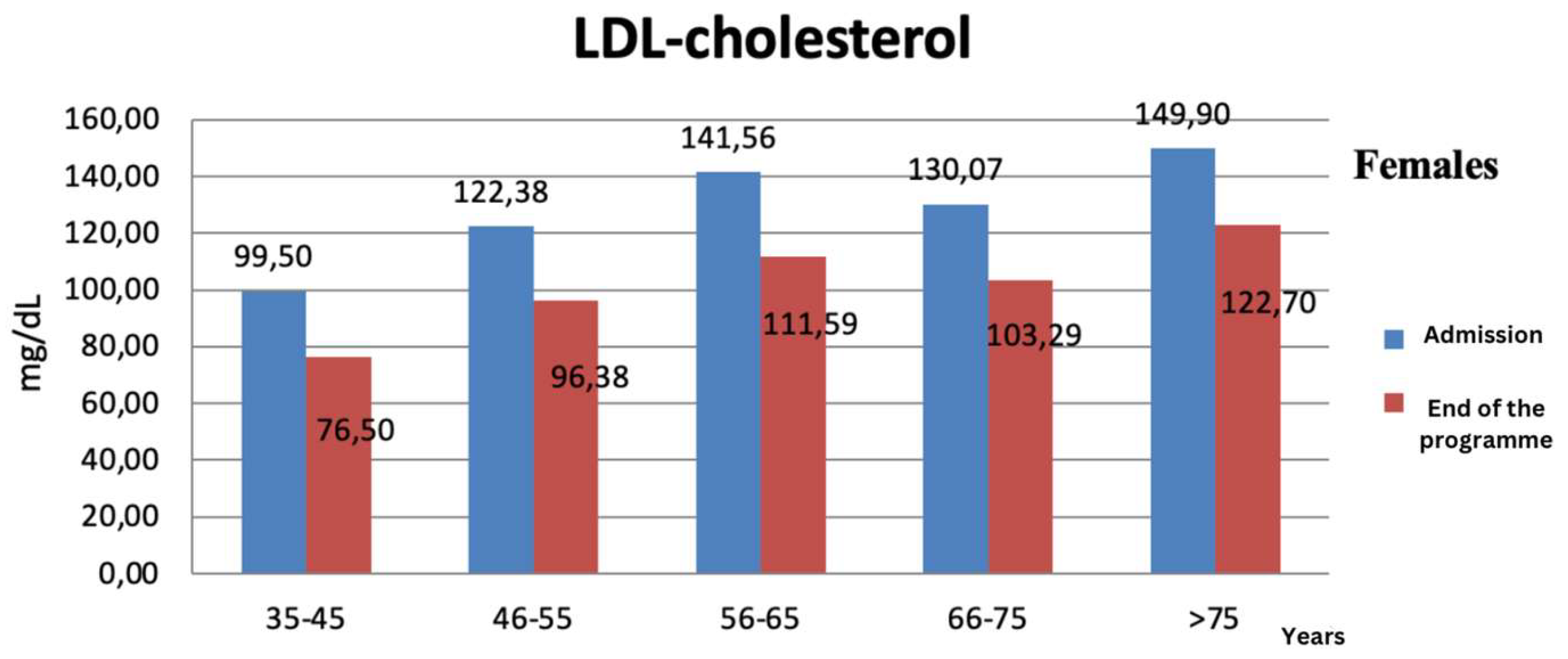
In females, LDL decreased on average with 26.65 mg/dl, but the best results were observed in females aged between 56-65 years old in which the average value decreased with 29.97 mg/dl (Figure 5).
Figure 4.
LDL- cholesterol evolution in males at admission & at the end of the programme (in 10 days).
Figure 4.
LDL- cholesterol evolution in males at admission & at the end of the programme (in 10 days).
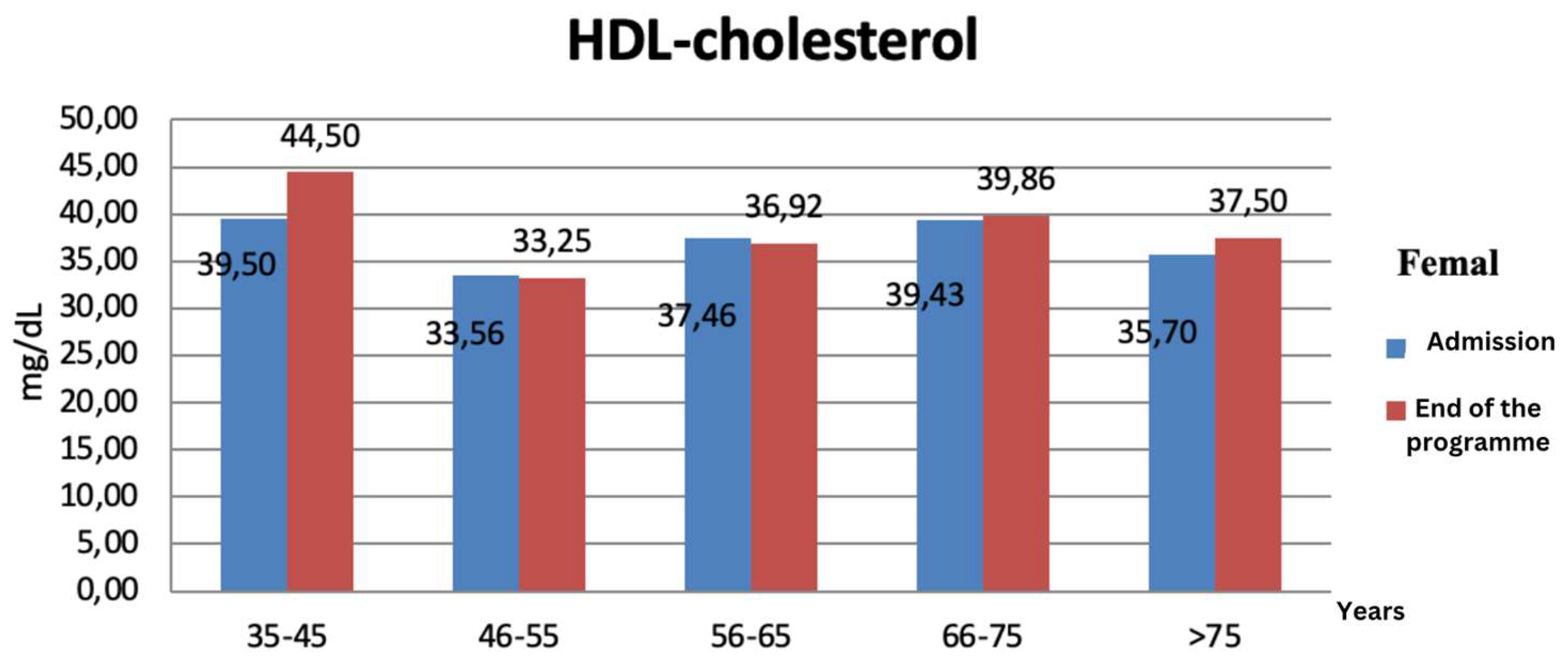
- HDL- Cholesterol:
On the first day at admission, 60 males had HDL levels below 40 mg/dl, 70 females had HDL levels below 50 mg/dl. After the 10 days programme, the best results were registered in patients aged between 35-45 years old in which HDL increased on average with 0.8 (Figure 6) in males and with 5 mg/dl in females (Figure 7).
Figure 5.
HDL cholesterol evolution in males at admission & at the end of the programme (in 10 days).
Figure 5.
HDL cholesterol evolution in males at admission & at the end of the programme (in 10 days).
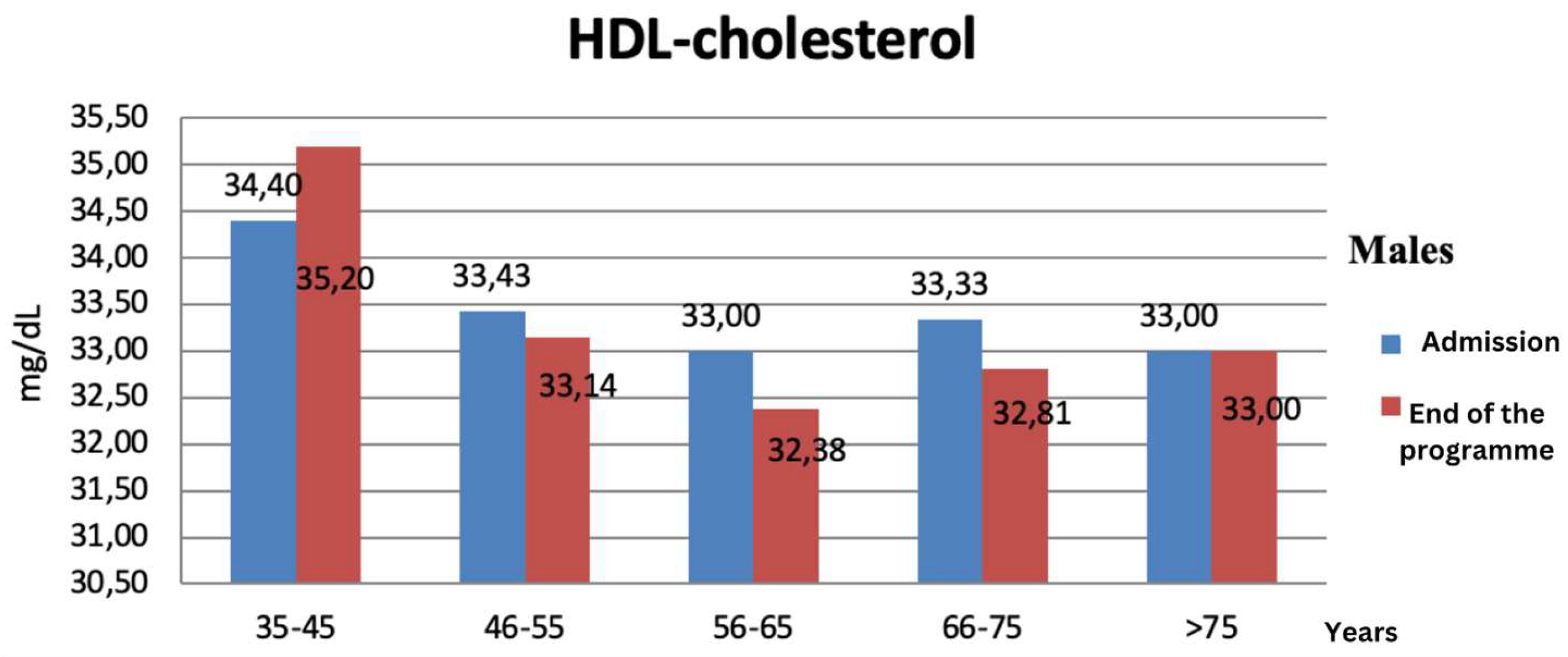
Figure 6.
HDL cholesterol evolution in males at admission & at the end of the programme (in 10 days).
Figure 6.
HDL cholesterol evolution in males at admission & at the end of the programme (in 10 days).
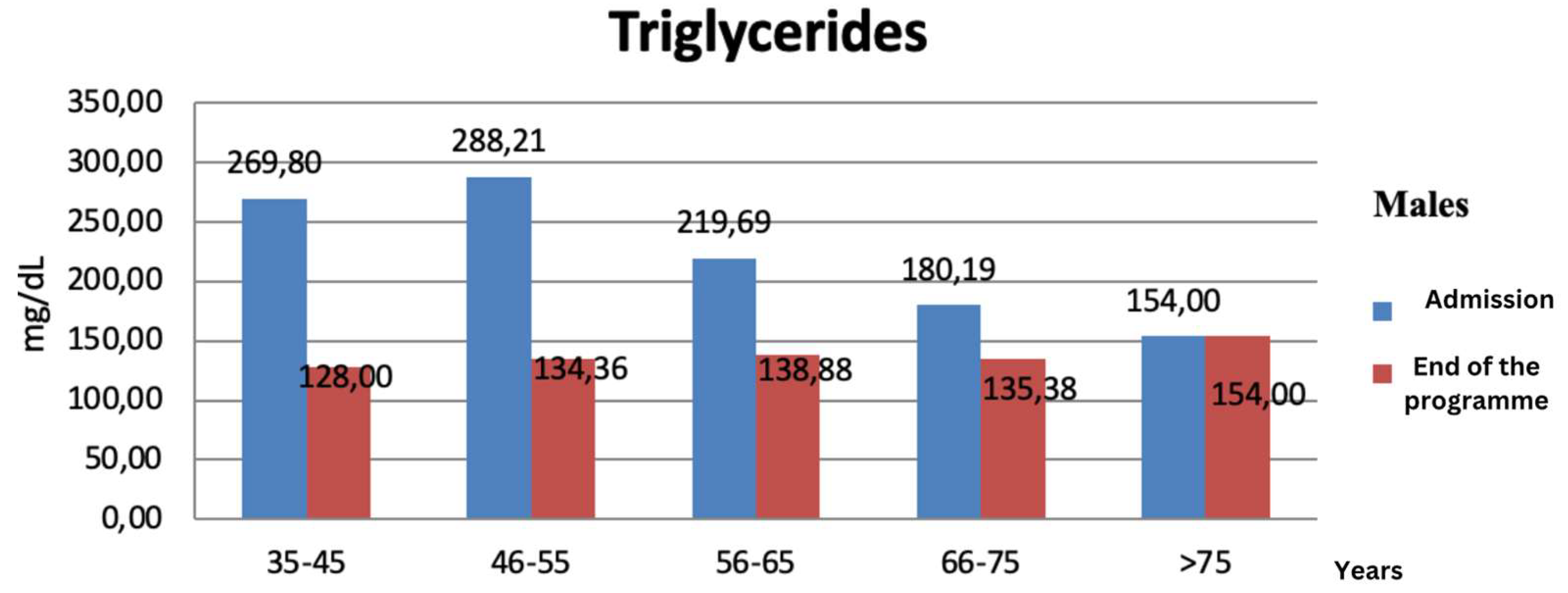
- Serum triglycerides
On the first day at admission, 108 patients had serum triglycerides over 150 mg/dl, while at the end of the programme, only 42 patients, less than a third had serum triglycerides over normal. In males, serum triglycerides decreased on average with 84.26 mg/dl, but the best results were observed in males aged between 46-55 years old in which the average value decreased with 153.85 mg/dl (with 53,38%) after the programme (Figure 8).
Figure 7.
triglycerides evolution in males at admission & at the end of the programme (in 10 days).
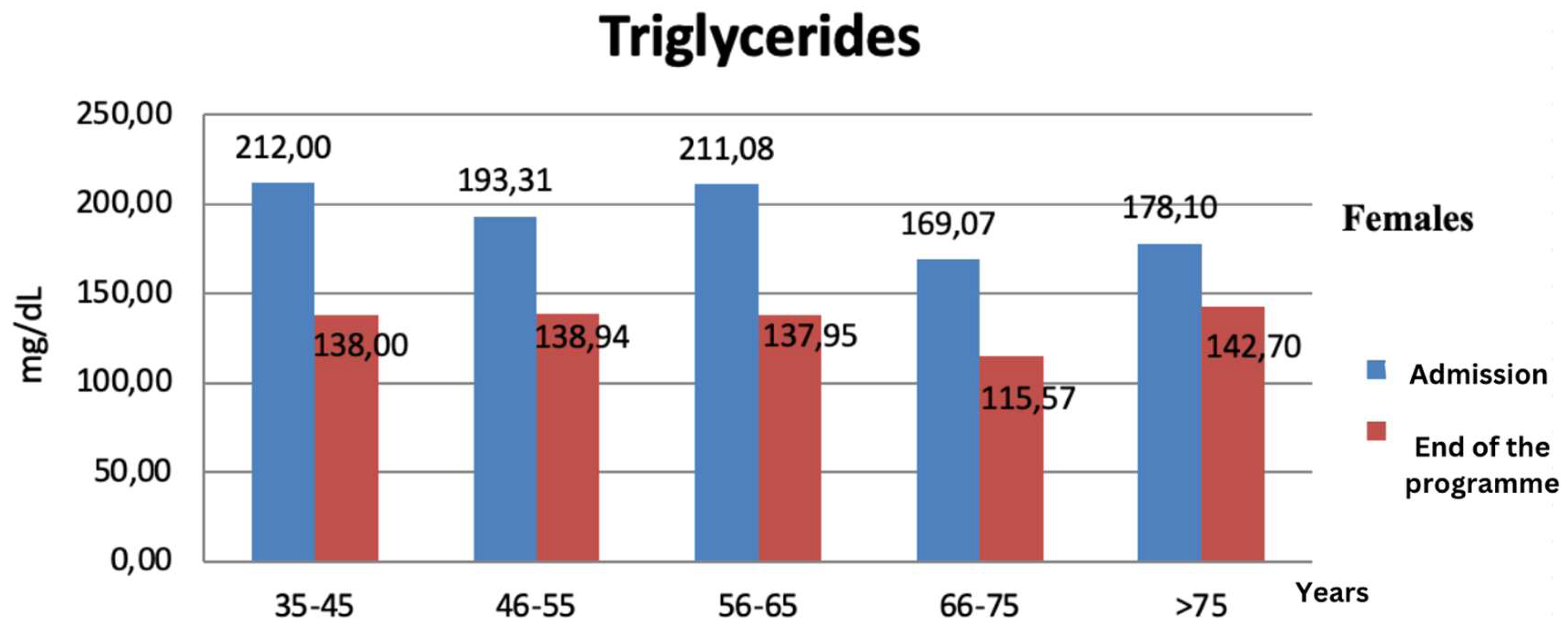
In females, serum triglycerides decreased on average with 57.03 mg/dl, but the best results were observed in males aged between 35-45 years old in which the average value decreased with 74 mg/dl after the programme (Figure 9).
Figure 8.
triglycerides evolution in females at admission & at the end of the programme (in 10 days).
Figure 8.
triglycerides evolution in females at admission & at the end of the programme (in 10 days).
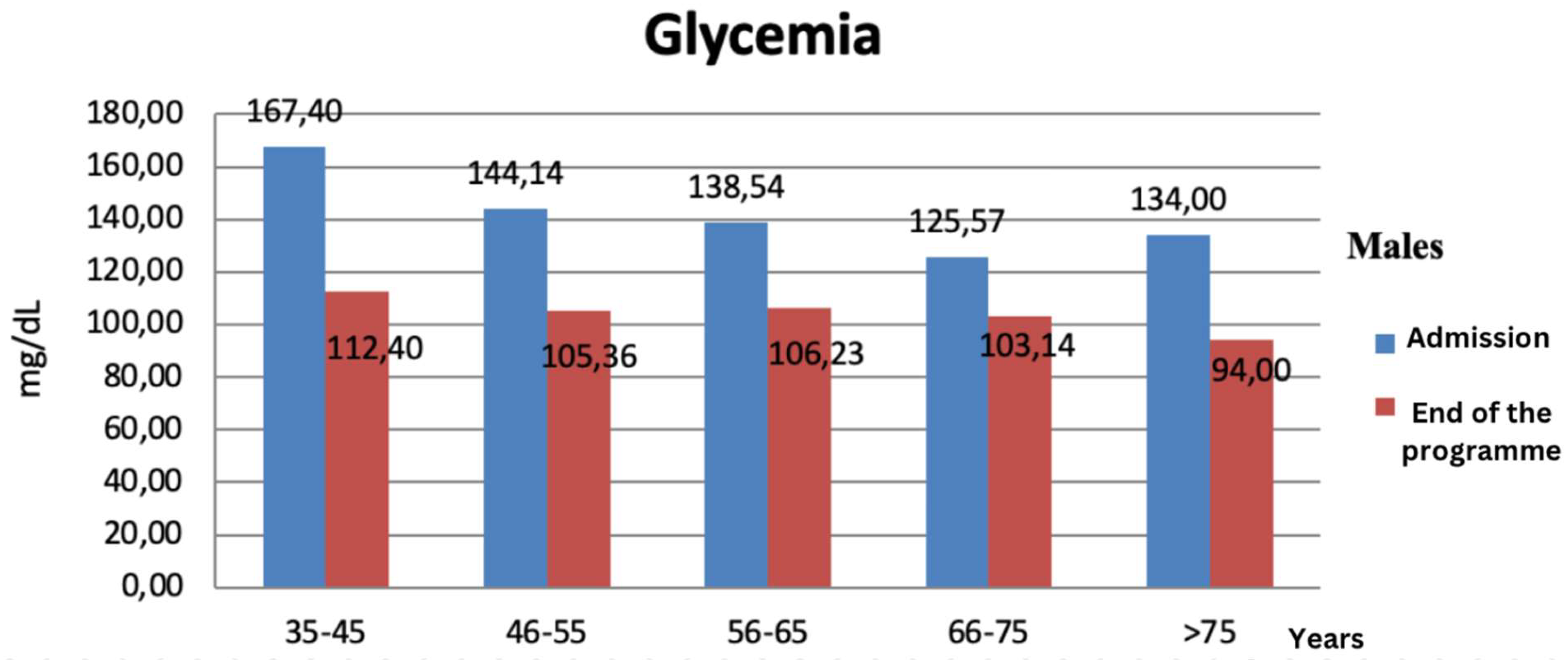
- Glycemia
Fasting glycemia measured on admission measured over 110 mg/dl in 125 patients, while after the programme its level decreased to 82 mg/dl.
In males, glycemia decreased on average with 37.7 mg/dl, but the best results were observed in females aged between 35-45 years old in which the average value decreased with 55 mg/dl (with 32%) after 10 days of treatment (Figure 10).
Figure 9.
Glycemia evolution in males at admission & at the end of the programme (in 10 days).
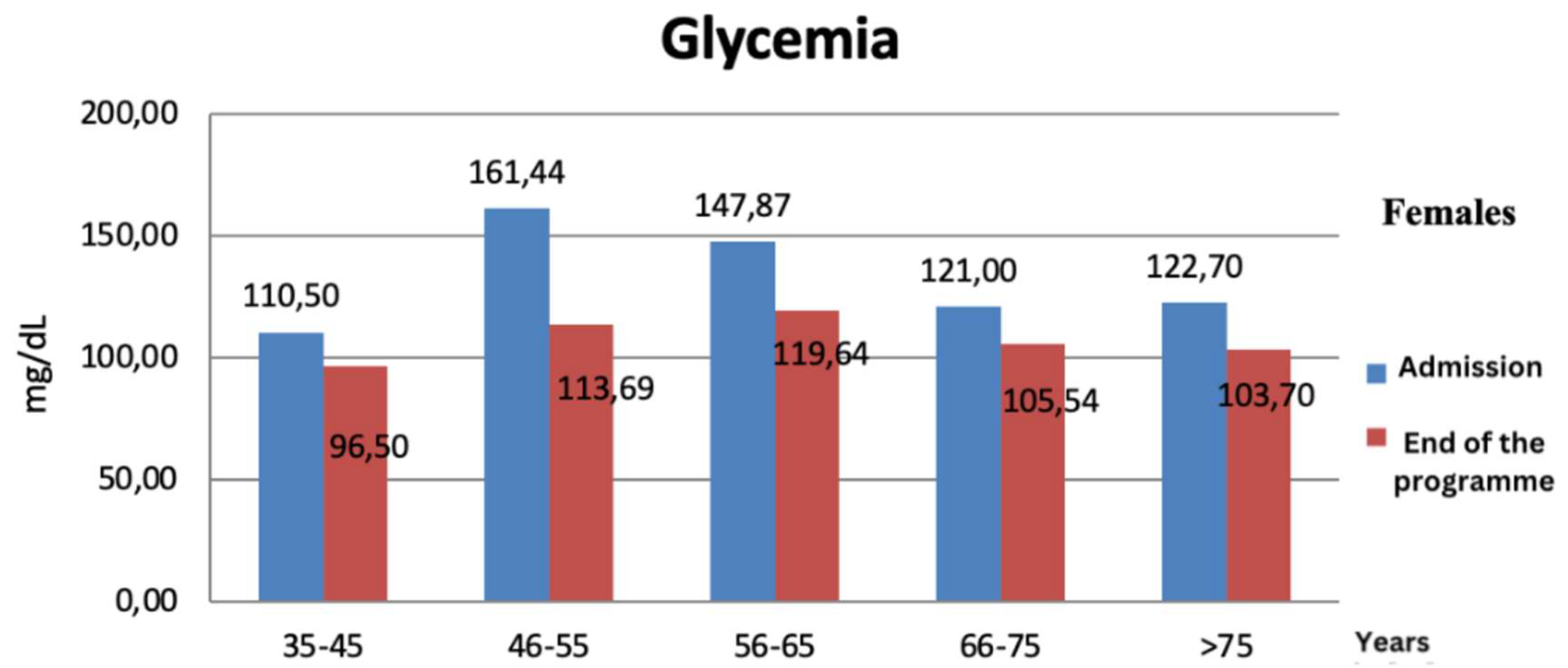
In females, glycemia decreased on average with 25.5 mg/dl, but the best results were observed in males aged between 46-55 years old in which the average value decreased with 47.75 mg/dl (with 29%) after the 10 days programme (Figure 11).
Figure 10.
Glycemia evolution in females at admission & at the end of the programme (in 10 days).
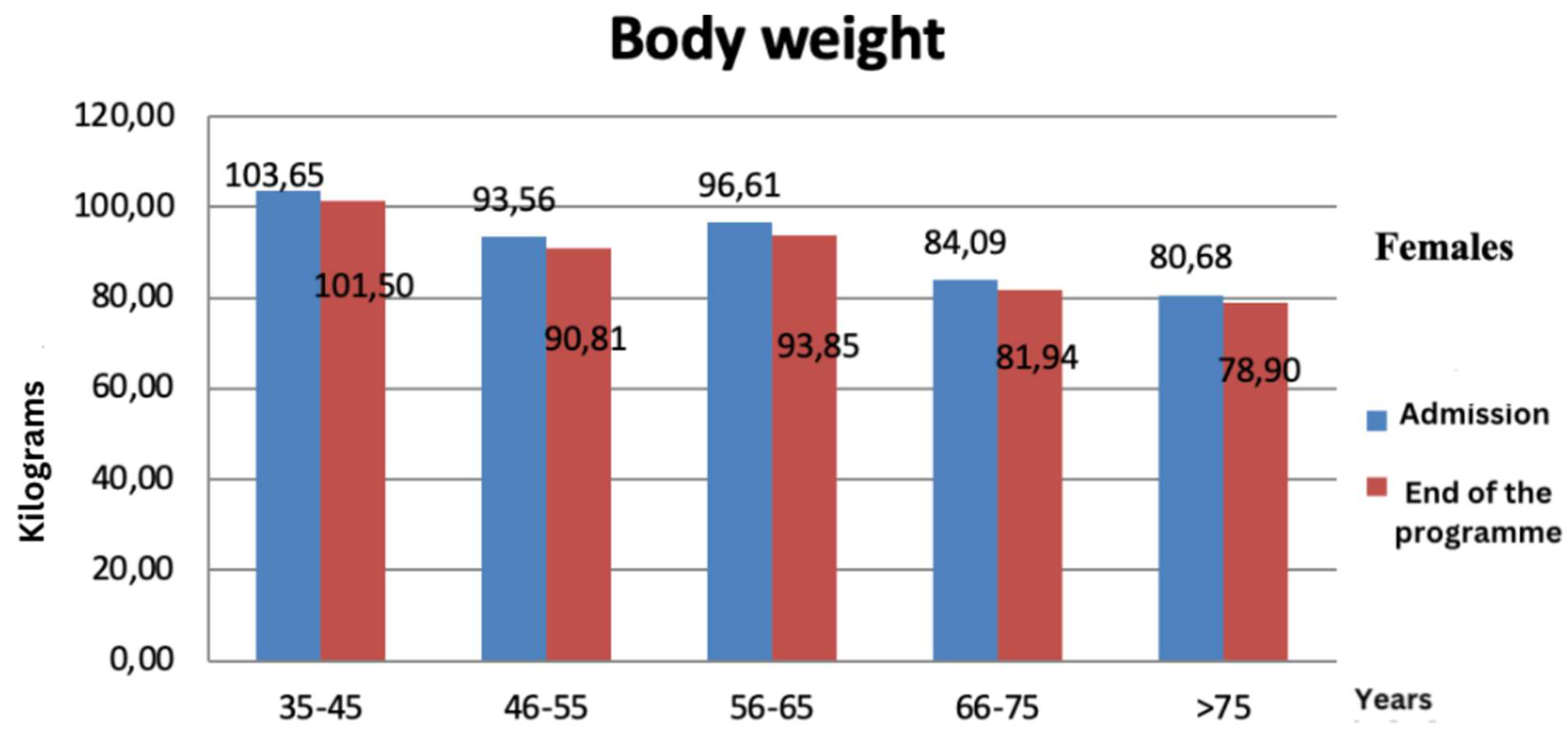
- Body weight
We followed the fat percentage evolution in correlation to body weight at our 150 patients, from which males managed to loss on average 3.25 kg, more than females that lost only 2.33 kg on average. The best results were observed in the age group 56-65 years old, where the average weight loss decreased on average with 3.95 kg in males and with 2.76 kg in females (Figure 12 and Figure 13).
Figure 11.
Body weight evolution in males at admission & at the end of the programme (in 10 days).
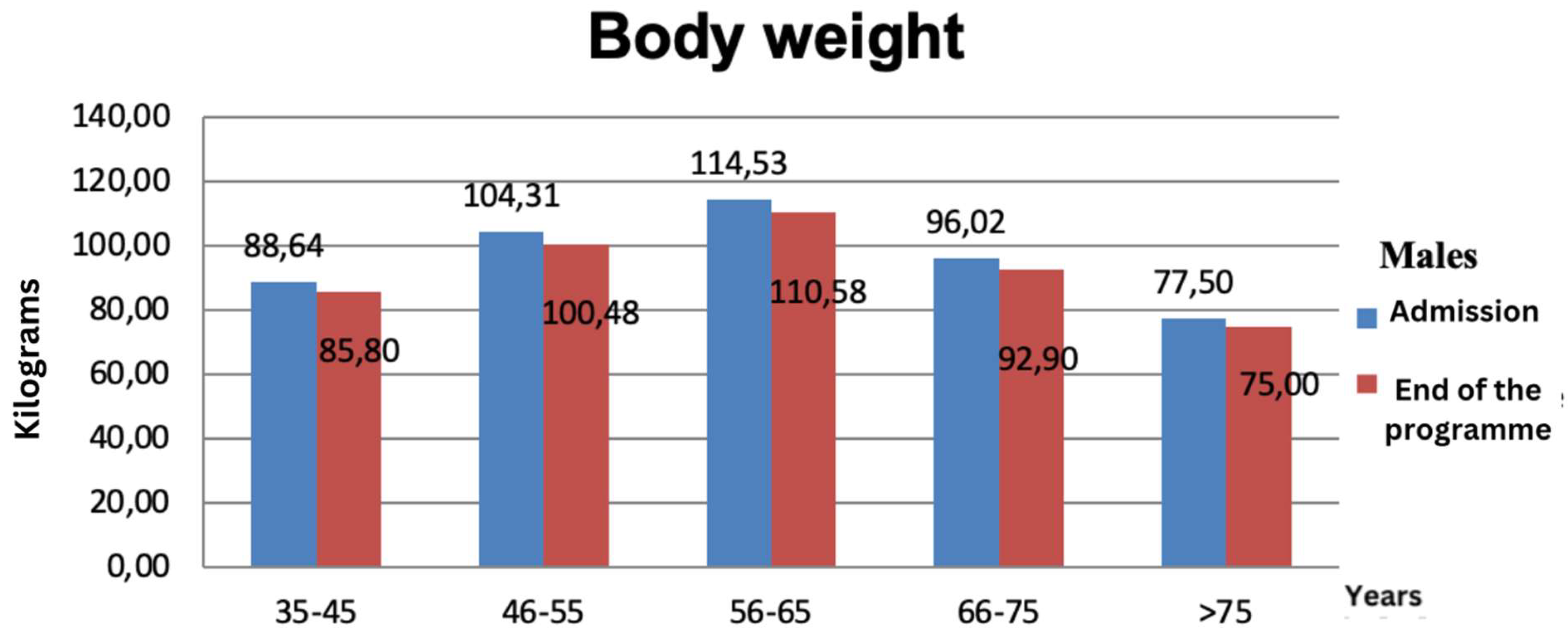
Figure 13.
Body weight evolution in males at admission & at the end of the programme (in 10 days).
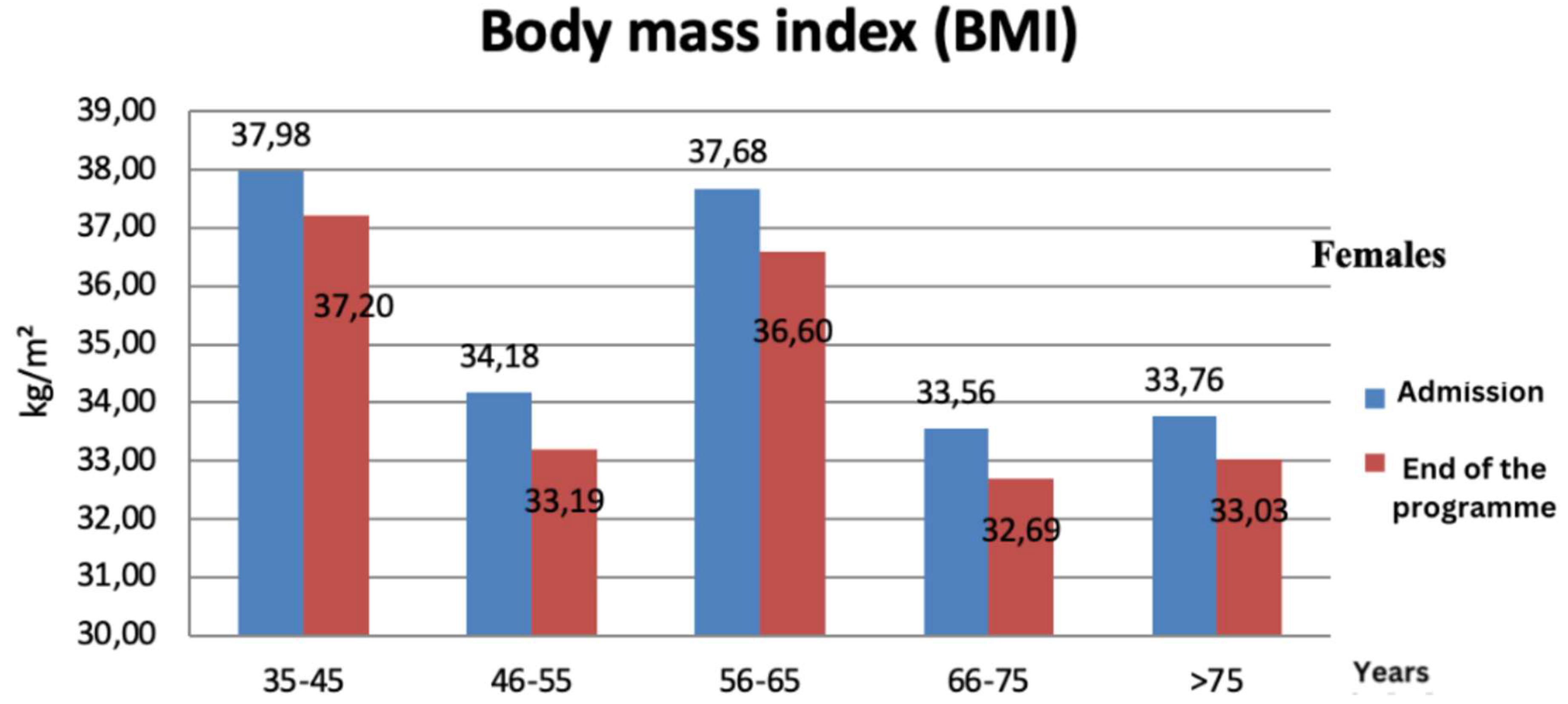
- Body mass index (BMI)
On the first day at admission, 119 patients registered a BMI of 30 kg/m², while at the end of the programme, only 8 patients managed to lower their BMI. The best results were observed in the age group 56-65 years old, where the average BMI decreased with 1,29 kg/m² in males and with 1,08 kg/m² in females (Figure 14 and Figure 15).
Figure 12.
Body mass index evolution in males at admission & at the end of the programme (in 10 days).
Figure 12.
Body mass index evolution in males at admission & at the end of the programme (in 10 days).
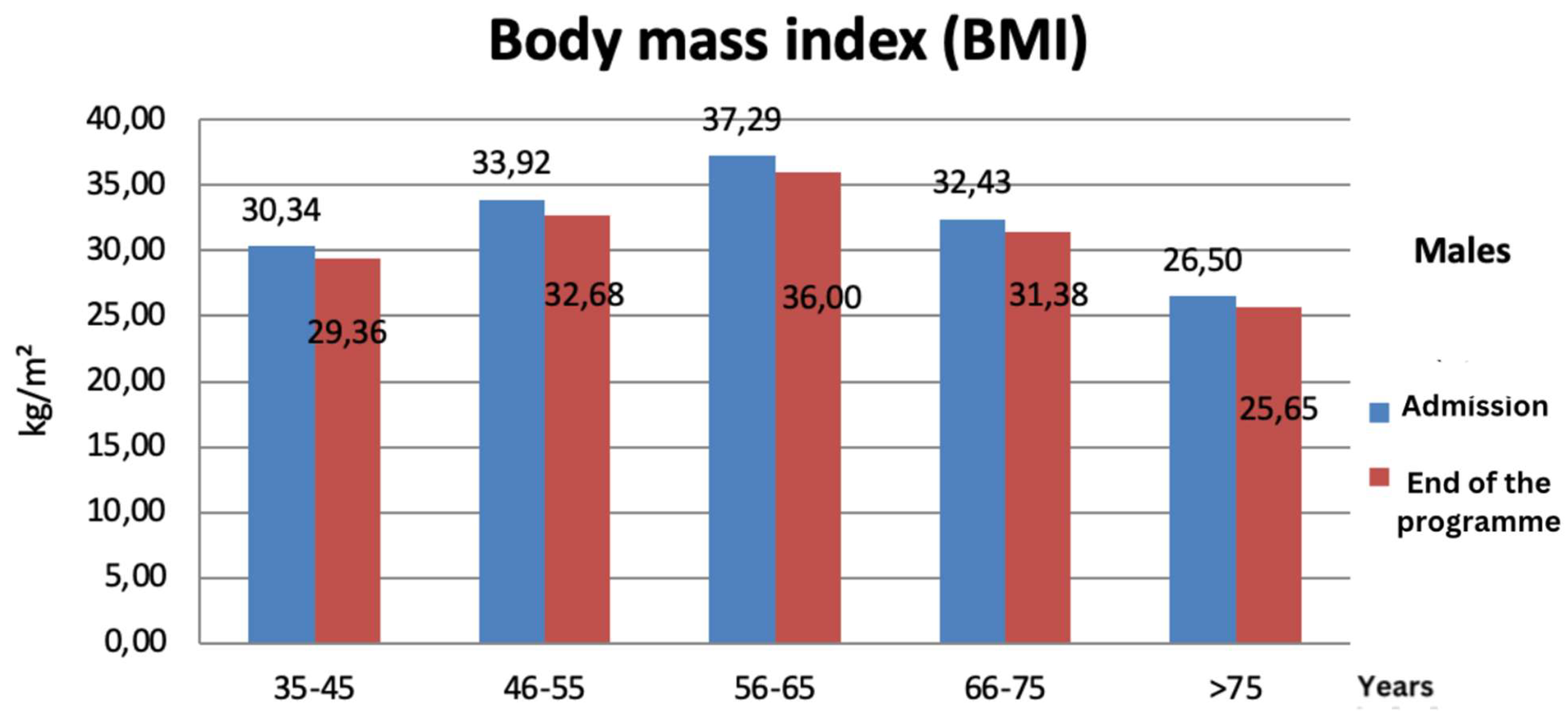
Figure 13.
Body mass index evolution in females at admission & at the end of the programme (in 10 days).
Figure 13.
Body mass index evolution in females at admission & at the end of the programme (in 10 days).
- Systolic and diastolic blood pressure
From all 150 patients involved in this study, 99 registered on admission systolic blood pressure over 130 mmHg, while 69 had diastolic blood pressure over 85 mmHg.
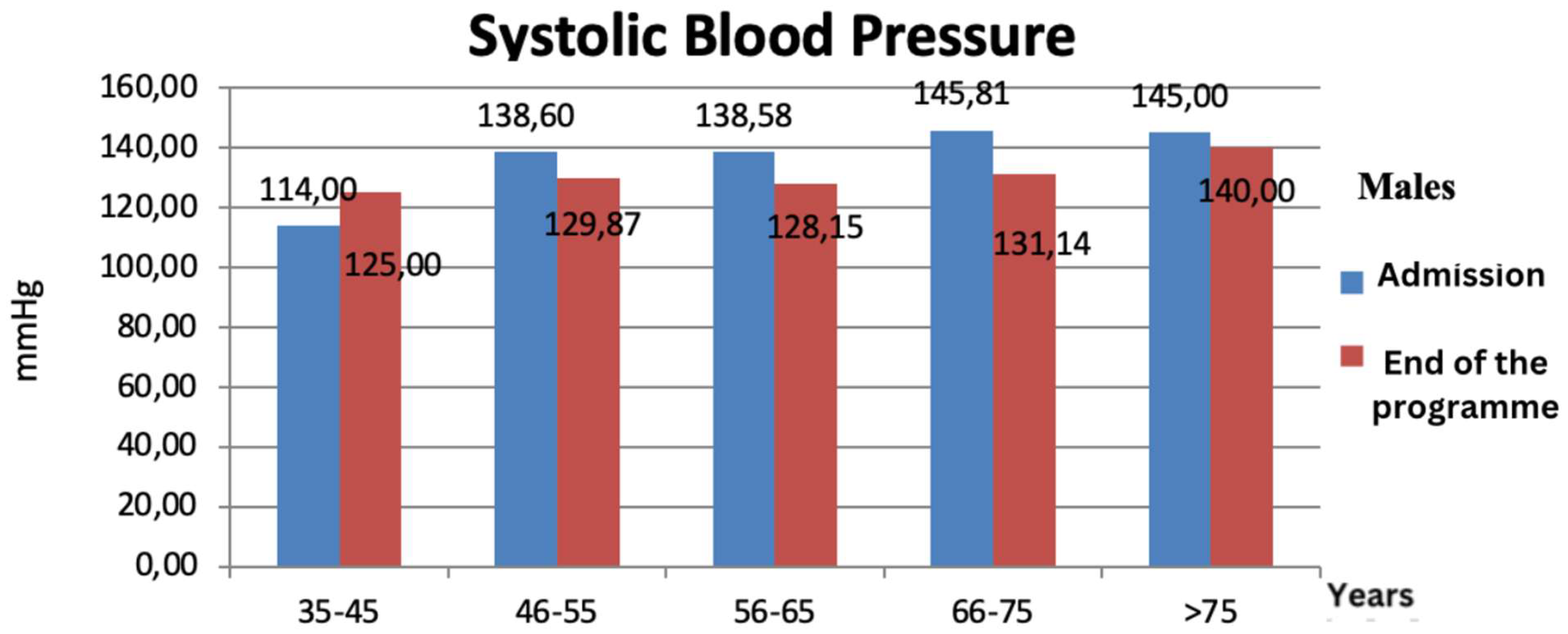
After 10 days of lifestyle changes, systolic blood pressure decreased with 5.57 mmHg in males while in females the systolic blood pressure decreased 2 times more comparing to males, on average with 11.84 mmHg. The best results were observed in males aged between 66-75 years old in which the systolic blood pressure decreased with 14.67 mmHg (Figure 16) and in females aged 35-45 years old of which systolic blood pressure decreased with 19.5 mmHg (Figure 17).
Figure 14.
Systolic blood pressure variation in females at admission & at the end of the programme (in 10 days).
Figure 14.
Systolic blood pressure variation in females at admission & at the end of the programme (in 10 days).
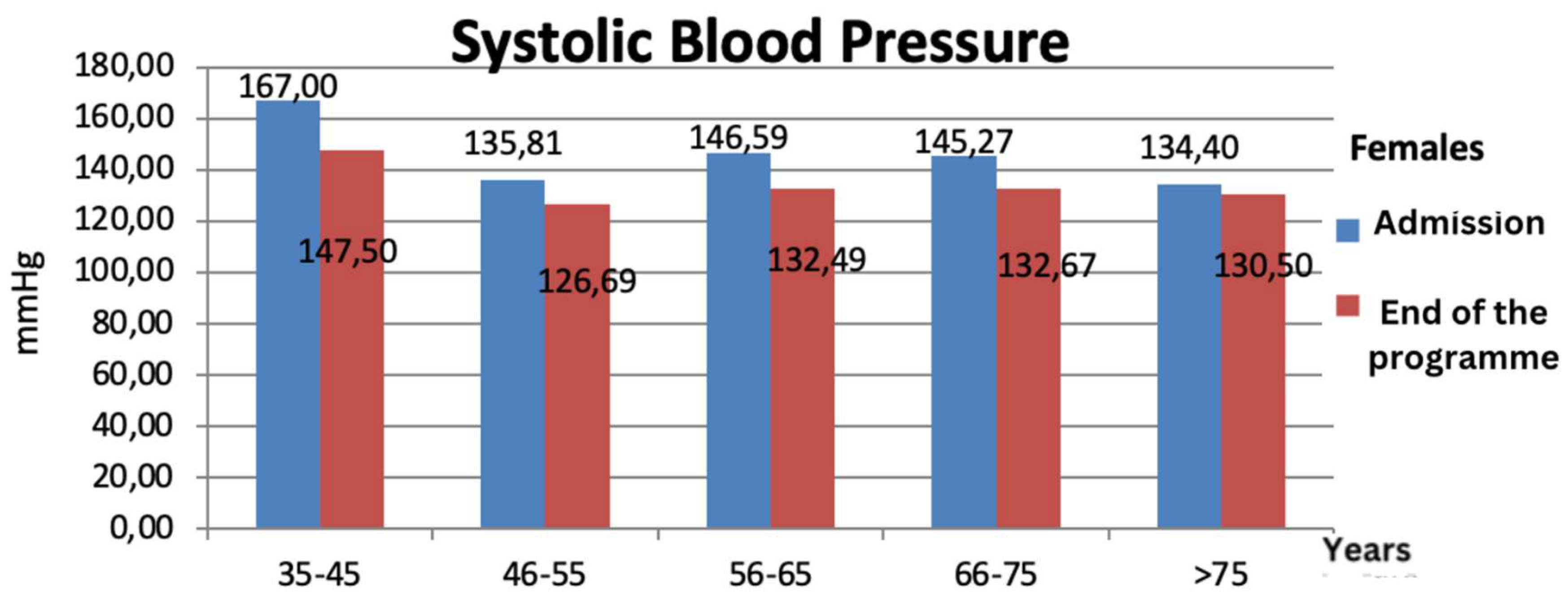
Figure 17.
Systolic blood pressure variation in males at admission & at the end of the programme (in 10 days).
Figure 17.
Systolic blood pressure variation in males at admission & at the end of the programme (in 10 days).
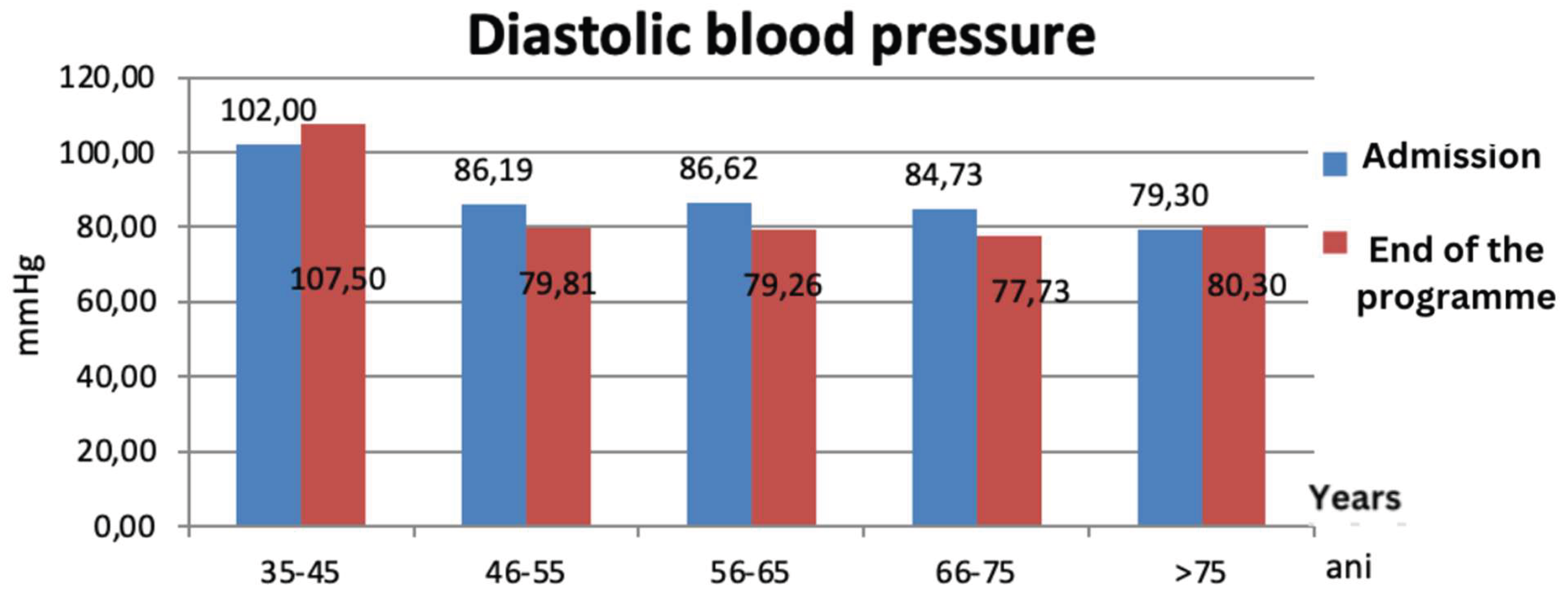
After 10 days of lifestyle changes, diastolic blood pressure decreased on average with 9.39 mmHg in males, while females registered a slight decrease on average, with only 2.85 mmHg. The best results were observed in males aged between 35-45 years old where the diastolic blood pressure decreased with 14.2 mmHg (with 15% from initial measurement) (Figure 18) and in females aged between 56-65 years old whose diastolic blood pressure decreased with 7.36 mmHg (Figure 19).
Figure 18.
Diastolic blood pressure variation in females at admission & at the end of the programme(in 10 days).
Figure 18.
Diastolic blood pressure variation in females at admission & at the end of the programme(in 10 days).
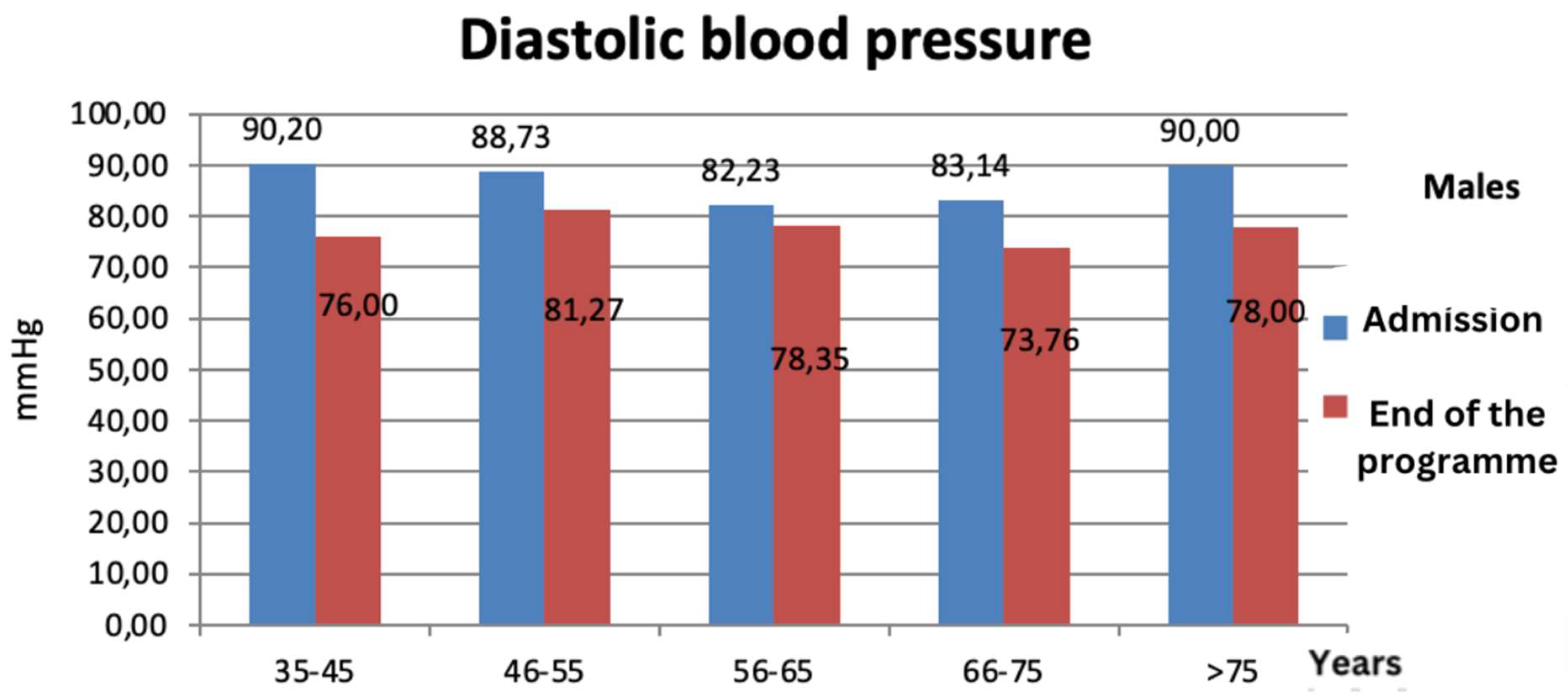
Figure 19.
Diastolic blood pressure variation in females at admission & at the end of the programme (in 10 days).
Figure 19.
Diastolic blood pressure variation in females at admission & at the end of the programme (in 10 days).
3. Conclusions
At the end of this study it is highlighted that lifestyle comprehend a series of factors that influence health, the most important pillars being represented by physical activity and diet.
This study was made on a 150 patients lot, all diagnosed with metabolic syndrome.
68 males, 82 females
Age range between 36-80 years old
After 10 days of treatment the following results were observed;
- Total serum cholesterol decreased on average with 41.21 mg/dl, with 19.54% less than the value registered on admission;
- Serum triglycerides decreased on average with 72.86 mg/dl, with 34.9% less than the value registered on admission;
- LDL- cholesterol decreased on average with 26.24 mg/dl, with 19.71% less than the value registered on admission;
- Glycemia decreased o average with 30.4 mg/dl, with 21.61% less than the value registered on admission;
- Body weight decreased on average with 2.99 kg, resulting in a 3% BMI reduction from initial value registered on admission;
- Systolic blood pressure decreased on average with 10.82 mmHg, but the diastolic blood pressure decreased with 6.44 mmHg, meaning a 7.6% reduction of blood pressure of initial value registered on admission.
High blood sugar levels, high blood pressure and obesity represent disorders that respond well to lifestyle changes such as: exclusive vegetarian diets correlated with physical activity, stress and burnout management, proving that this programme is recommended to all individuals suffering from metabolic syndrome, avoiding adverse effects of certain pharmaceutical treatments available. Our study states that an exclusive vegetarian diet has a positive impact on metabolic syndrome patients, but also on health and premature ageing.
Author Contributions
Conceptualization, Miloicov Bacean Oana Codruta; Data curation, Sitaru Georgiana Patricia; Investigation, Vacaru Gabriel Cristian, Simbrac Mihaela Cristina and Folescu Roxana; Methodology, Gurgus Daniela; Software, Borca Ciprian Ioan; Writing – original draft, Ursadan Mirabela Anca.
Ethical Issues
The research was conduced in accordance with the guidelines outlined in the Declaration of Helsinki. Ethical clearance obtained from “Victor Babes” University of Medicine and Pharmacy, Center for Studies in Preventive Medicine, Timisoara, Romania, Institutional Review Board, research support officers (1/07.04.2021 2021-04-07). The research’s objectives, benefit and risks were explained to the participants before data collection and obtained written informed consent from the study participants. The research participants were assured of the attainment of confidentiality, and the information they give us will not be used for any purpose other than the research.
References
- Mănescu, S.; Bedo, C.; Dumitrache, S.; et al. Tratat de igienă, vol.II, editura medical, Bucharest. 1985. [Google Scholar]
- Campbell, T.C.; Thomas, M. Campbell II: The China Study. The most comprehensive study of nutrition ever conducted and the startling implication for diet, weight loos and long-term health. Ed. BenBellaBooks, 2004.
- Christian Nordqvist. Nine most popular diets rated by experts 2017. Available online: https://www.medicalnewstoday.com/articles/5847.php (accessed on 17 July 2017).
- Search Best Diets for Weight-Loss, Heart Health and More, U.S.News. Available online: https://health.usnews.com/wellness/best-diet/search.
- Kahleova, H.; Tura, A.; Hill, M.; Holubkov, R.; Barnard, N.D. A plant-based dietary intervention improves beta-cell function and insulin resistance in overweight adults. A 16-week randomized clinical trial. Nutrients. Published online 9 February 2018.
- Chiu, T.H.T.; Pan, W.H.; Lin, M.N.; Lin, C.L. Vegetarian diet, change in dietary patterns, and diabetes risk: a prospective study. Nutr Diabetes. Published online 9 March 2018.
- Toumpanakis, A.; Turnbull, T.; Alba-Barba, I. BMJ Open Diab Res Care. 2018;6:e000534.
- Kyrø, C.; Tjønneland, A.; Overvad, K.; Olsen, A.; Landberg, R. Higher whole-grain intake is associated with lower risk of type 2 diabetes among middle-aged men and women: the Danish Diet, Cancer, and Health Cohort. J Nutr. 2018, 148, 1434–1444. [Google Scholar] [CrossRef] [PubMed]
- Marian Paraschiv Claudius, Tratat pentru alimentatia naturala a omului, editura Christalin, Bucharest, 2003; 317-333, 681-689.
- AMBOSS GmbH, Obesity and metabolic syndrome. Available online: https://next.amboss.com/us/article/4g03v2?q=metabolic+syndrome#Zc3983f79b8ec111f417e09fb2b300f00 (accessed on 14 march 2021).
- Dan L. Longo, Fauci, Kasper, Hauser, Jameson, Loscaldo: Harrison. Manual de medicină, Ediţia a 18-a. – Bucureşti: Editura ALL, 2014.
- Timar, R.; Vlad, A.; Sima, A.; et al. Noţiuni de diabet, nutriţie şi boli metabolice, editura EUROBIT. Timişoara 2014, 5, 163–173. [Google Scholar]
- Dan, V. Nicolae Dan: Cartea de bucate a Centrului Lifestyle Herghelia, Ediţia a 7-a. –Pantelimon : Viaţă şi Sănătate. 2016; 22, 27, 32, 34, 39-44, 57-58, 66-69, 72-79, 123-385. [Google Scholar]
- Stoica, V.; Scripcariu, V.; et al. Compendiu de specialităţi medico-chirurgicale, Vol.I, Ediţie revizuită - Bucureşti, Editura Medicală. 2018, 158, 163. [Google Scholar]
- Ramon, C. Gelabert: Diabetul: tratamente ştiinţifice şi naturale, Pantelimon: Viaţă şi sănătate. 2013; 64, 106-116. [Google Scholar]
- Trumbo, P.; Schlicker, S.; Yates, A.A.; et al. Dietary reference intakes for energy, carbohdrate, fiber, fat, fatty acids, cholesterol, protein and amino acids. American Dietetic Association. Journal of the American Dietetic Association; Chicago 2002, 102, 1621–30. Available online: https://search.proquest.com/openview/41e1233015fb62ff54f496de51364921/1?pq-origsite=gscholar&cbl=49142. [CrossRef] [PubMed]

Table 1.
An example of a 2000 kilocalories/day, during 11 days.
| Day | 1 | 2 | 3 | 4 | 5 |
| Breakfast (7:00 AM) |
Granola I Corn Flakes Sour cherry sauce Soy milk Apples Sunflower seeds Mushrooms Pate Whole grain bread |
Millet pudding II Pineapple sauce with forest fruits Almond milk Pumpkin seeds Nut butter Whole grain bread |
Apple crisp II Strawberry sauce Peanut milk Sunflower seeds Eggplant pate Whole grain bread |
Wheat pudding Carob sauce Millet milk Pumpkin seeds White beans pate Whole grain bread |
Whole grain nut pasta Blackberry Sauce Cashew milk Sunflower seeds Almond butter Whole grain bread |
| Lunch (13:00) | Baked French fries Veggie Burgers Dill pea stew Tomatoes Salad Lettuce Bran bread |
Baked celery Green peas pate Onion & cucumber salad Tomato salad Seed buns |
Barley with baked vegetables Tofu balls I Onion and pepper stew |
Spinach and tofu lasagna Boiled corn Chickpea shepherd’s pie Tomatoes, peppers and onion salad |
Vegetable cabbage rolls with sour cream Lentils pate Olives and tomatoes board Cupcakes with raisins and wheat germ |
| Dinner (18:00) |
Fruits board Filled rolls or cinnamon rolls |
Cream soup with olives and spiced croutons | Spinach soup with tofu Seed buns |
Fruits kompot Whole grains bread |
Mushrooms soup with millet Popcorn |
Table 2.
An example of a 2000 kilocalories/day, during 11 days.
| Day | 6 | 7 | 8 | 9 | 10 | 11 |
| Breakfast (7:00 AM) |
Baked apples Raspberry sauce Peanut milk Pumpkin seeds Olive pate Whole grain bread |
Oat flakes with fruits Fresh fruits sauce Milk Sunflower seeds Chickpeas pate Whole grain bread |
Rice pudding Blueberries sauce Soy milk Pumpkin seeds Cauliflower pate Whole grain bread |
Waffles I Apricot sauce Millet milk Sunflower seeds Veggie caviar Whole grain bread |
Cereal Flakes Rose hip paste Almond milk Pumpkin seeds Soy pate Whole grain bread |
Semolina with milk and granola Plum jam Cashew milk Sunflower seeds Green beans paste Whole grain bread |
| Lunch (13:00) | Polenta Garlic sauce Coriander and cabbage stew Mushrooms schnitzel Veggie salad |
Baked pasta with beans Mushrooms veggie balls Lettuce with celery and garlic |
Soy pizza Oriental Broccoli Green rice Lettuce |
Baked cauliflower Lentils shepherd’s pie I Spinach salad Tomatoes salad with peppers and cucumbers |
Baked potatoes Rosemary chickpeas stew Mediterranean salad Beet salad |
Baked rice with olives Zucchini stew Cucumber salad with onion |
| Dinner (18:00) |
Carrot cream soup Spiced croutons |
Country style soup Popcorn |
Beetroot soup Olives and pepper board |
Green peas soup Apple dessert |
Sweet cauliflower soup I Toast with garlic |
Fruits board Brioche |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



