
Submitted:
06 August 2025
Posted:
07 August 2025
You are already at the latest version
Abstract
Background: Rheumatoid arthritis is the most common systemic inflammatory disease, manifesting mainly in the synovial tissue of small and large joints, but it can involve consequential extra-articular complications. Throughout the progression of this disease, all cardiac structures, including the conducting system, myocardium, endocardium, coronary arteries, and valves, may be affected, resulting in a higher incidence of cardiac arrhythmias. Methods: We performed a narrative review of the most recent studies that emphasise the epidemiology, pathophysiology, diagnosis and management of arrhythmias found in patients with rheumatoid arthritis. Additionally, the effects of disease-modifying antirheumatic drugs (DMARDs) as conventional synthetic DMARDs (csDMARDs), biologic DMARDs (bDMARDs) and targeted synthetic DMARDs (tsDMARDs), on cardiac electrophysiology were analysed. Results: The literature has revealed that cardiac immune cells may influence arrhythmogenesis through non-canonical and inflammatory mechanisms by modifying myocardial tissue architecture or by interacting with cardiomyocytes, potentially altering their electrical function. Conclusion: This review emphasises the essential role of a multidisciplinary approach involving, at least, rheumatologists and cardiologists in the screening and management of arrhythmias.
Keywords:
rheumatoid arthritis
; arrhythmias
; atrial fibrillation
; ventricular ectopic beats
; epidemiology
; csDMARDs
; bDMARDs
; tsDMARDs
1. Introduction
Rheumatoid arthritis (RA) is the most common systemic inflammatory rheumatic disease, manifesting mainly in the synovial tissue of small and large joints, mediated by interaction between T lymphocytes, B lymphocytes, and synovial fibroblasts. Throughout the progression of this disease, all cardiac structures, including the conducting system, myocardium, endocardium, coronary arteries, and valves, may be affected, resulting in a higher incidence of cardiac arrhythmias [1]. Lastly, preclinical and clinical data highlight the involvement of the immune system in the pathophysiology of arrhythmias. Recent studies have revealed that cardiac immune cells, through both inflammatory mechanisms and non-canonical functions, may contribute to arrhythmogenesis by modifying myocardial tissue architecture or by interacting with cardiomyocytes, potentially altering their electrical function [2].
In contemporary clinical practice, rheumatoid arthritis is recognized as a common and complex systemic disease with multisystem involvement. A multidisciplinary approach is required because, although it primarily targets the synovial tissue of both large and small joints, it can also result in significant extra-articular complications like abnormal cardiac rhythms.
This review aims to integrate essential insights from the literature to provide clinicians with a comprehensive understanding of arrhythmia management found in patients with rheumatoid arthritis. In addition to highlighting the vital role of interdisciplinary collaboration in improving patient outcomes, this paper covers topics ranging from epidemiology and pathophysiological mechanisms to diagnostic strategies and the cardiovascular effects of drugs used. Due to its systemic involvement, patients diagnosed with rheumatoid arthritis are frequently evaluated by internal medicine departments. Effective management requires close cooperation between rheumatologists, dermatologists, cardiologists, pulmonologists, gastroenterologists, general practitioners, and other specialists, depending on the extent of organ involvement. Such integrated care is essential for optimising prognosis and quality of life in individuals affected by rheumatoid arthritis.
2. Materials and Methods
This paper was designed as a narrative review, aiming to synthesize the latest scientific reports on the epidemiology, pathophysiology, diagnosis and management of arrhythmias found in patients with rheumatoid arthritis, including the cardiovascular effects of disease-modifying antirheumatic drugs (DMARDs) as conventional synthetic DMARDs (csDMARDs), biologic DMARDs (bDMARDs) and targeted synthetic DMARDs (tsDMARDs), on cardiac electrophysiology.
The literature search sources were filtered out through a structured query of PubMed and Google Scholar, using combinations of the following descriptors: “rheumatoid arthritis”, “arrhythmias”, “atrial fibrillation”, “ventricular ectopic beats”, “epidemiology, pathophysiology”, “autonomic nerve system”, “renin-angiotensin system”, “endothelial dysfunction”, “epicardial tissue adiposity”, “inflammation”, “csDMARDs, bDMARDs and tsDMARDs”. Articles published in the last five years (2020–2025) were prioritized to reflect the timeliness of data and clinical relevance of information. A limited selection of older sources was intentionally included when they provided foundational knowledge or established clinical guidelines critical to understanding the development of cardiovascular side effects noted over time.
3. Epidemiology of Arrhythmias in Rheumatoid Arthritis
3.1. General Prevalence of Arrhythmias in Rheumatoid Arthritis
Autoimmune diseases, such as RA,are linked to increased cardiovascular morbidity and mortality, with cardiovascular disease (CVD) accounting for more than 50% of premature deaths in affected individuals. Atrial fibrillation (AF) is 40% more common in patients with RAthan in the general population and can occur at any stage of the disease, sometimes even as the first symptom, according to a Danish cohort study of 4.182,335 participants, including 18.247 with RA. The pathophysiology of AFis closely associated with systemic inflammation, which leads to an increase in inflammatory proteins within the body. This effect is particularly pronounced in young females (<50 years) with sedimentation rates exceeding 60 mm/h or elevated levels of anti-TNF-α antibodies [3]. A 2024 study found that RA was associated with an increased risk of AF but Mendelian randomisation showed no causal link, suggesting the association may be due to shared risk factors [4]. Ventricular tachycardia (VT) is also observed, but it is associated with treatments like methotrexate (MTX) and infliximab [5].
A comprehensive analysis of the National Inpatient Sample Database (2015–2019) involving 9.370 patients with RA found that 25.7% had concomitant arrhythmias, more specifically, 12% had supraventricular tachycardia (SVT), 73.4% had AF 9.8% had atrial flutter (AFl) and 6.4% had VT. Based on this study, patients with RA have a 25.7% risk of developing arrhythmias [6].
Patients with RA have twice the risk of sudden cardiac death compared to healthy controls. It is often due to VT or ventricular fibrillation and occurs in about 0.2% of the general population annually [7].
3.2. Autoantibody-Associated Arrhythmias in Rheumatoid Arthritis
The principal features that distinguish RA from other inflammatory joint diseases are rheumatoid factor (RF) and anti-citrullinated protein antibodies (ACPA). These antibodies are found in the blood and the joint fluid of 60–70% of patients at an early stage, often years before symptoms appear. Seropositive RA is characterised by the presence of RF and/or ACPA and is now widely recognised as a distinct subtype, separate from seronegative RA [8]. Nevertheless, 20% of RA cases remain seronegative [9].
A 2021 study based on women with moderate to high activity seropositive RA identified arrhythmias in 56.25% of patients, most commonly sinus rhythm abnormalities (31.25%), including tachycardia (18.75%), bradycardia (6.25%), and sinus arrhythmia (6.25%). Premature supraventricular and ventricular beats were present in 12.5%, and left anterior bundle branch block in 12.5%. Myocardial repolarisation disturbances suggestive of silent ischaemia were observed in 18.75%, exclusively in patients with RA duration >10 years. These findings support the use of Holter ECG monitoring in seropositive RA to detect asymptomatic cardiovascular complications [10].
The RFis an autoantibody against the Fc region of immunoglobulin, with a sensitivity of 60–80% and a sensitivity of 85% [11]. It is routinely used for diagnostic purposes in patients with suspected RA [12]. The literature does not present data of correlation between RF and arrhythmia prevalence. However, based on the study of Kumar et al. the presence of RFhas a significant impact on cardiovascular involvement in patients with rheumatoid arthritis. The study found that the most common cardiovascular manifestations were ECG abnormalities, present in 58.3% of RA patients (82.9% RF-positive) [11].
Currently, ACPA, which target citrullinated peptides, are considered more specific serological markers for RAthan rheumatoid factor. ACPA testing has been incorporated into the 2010 revised RA classification criteria established by the American College of Rheumatology (ACR) and the European League Against Rheumatism (EULAR) [12]. According to the study published by Aiewruengsurat et al., ACPA may contribute to subclinical cardiac changes in patients with RAwho do not have clinically evident cardiovascular disease. Specifically, elevated ACPA levels were found to enhance the correlation between high-sensitivity troponin T and left ventricular mass index, indicating a potential role of these autoantibodies in myocardial remodelling.
No direct association has been described between ACPA and the prevalence of arrhythmias; however, current evidence supports the hypothesis that ACPA may contribute to subclinical cardiac injury and structural alterations of the heart [13]. In RA,some patients develop eccentric cardiac remodelling with reduced relative septal thickness, a change that correlates with elevated levels of ACPA and γ-globulin, suggesting a potential relationship with disease severity [7].
The potential triggers for ACPA production are known to be filaggrin, type II collagen, α-enolase, fibrinogen and vimentin [14]. In a cross-sectional study of 135 seropositive RApatients without a history of cardiovascular disease, plasma levels of anti-modified citrullinated vimentin (anti-MCV) antibodies were found to correlate inversely with left ventricular ejection fraction, with a stronger negative correlation (P < 0.001) than that observed for general ACPA (P = 0.019). These findings suggest that anti-MCV could serve as a promising biomarker for early screening of cardiac systolic dysfunction in RA [15].
Anti-Ro antibodies, present in 5–15% of RA patients, are linked to cardiac arrhythmias, including QTc prolongation in both neonates and adults. These antibodies downregulate L-type calcium channels, promoting conduction defects, but also inhibit the hERG/IKr current by binding to Kv11.1 channels, leading to prolonged repolarisation. Studies have found anti-Ro antibodies in 60% of patients with torsades de pointes or long QT syndrome, often without an associated connective tissue disease, suggesting a complex proarrhythmic role through multiple ion channel interactions [7]. Additionally, the literature suggests that anti-Ro antibodies (particularly the 52 kDa subtype) can contribute to long QT syndrome and ventricular arrhythmias [16]. The prevalence of arrhythmias correlated to RA antibodies is not fully explored. However, the literature suggests intriguing data for further investigation (Figure 1).
4. Pathophysiology
4.1. Atrial and Ventricular Remodeling
The immunological pathogenesis of rheumatoid arthritis-associated atrial fibrillation (RA-AF) appears to be driven by atrial fibrosis and structural remodelling, primarily mediated by the hyperactivation of resident cardiac macrophages and polymorphonuclear neutrophils (PMNs) [17]. More specifically, the structural and functional changes may be driven by chronic inflammation, particularly IL-6, and cardiomyocyte apoptosis, triggered by inflammation and oxidative stress, contributing to a pro-arrhythmic substrate. Extensive fibrosis disrupts normal atrial architecture and electrical conduction, increasing susceptibility to atrial fibrillation. Experimental models of collagen-induced arthritis show heightened AF inducibility and duration, supporting an inflammatory link [7].
In a 2021 study, Wang et al. examined the role of various inflammatory and immunological markers present in the peripheral blood of RA patients with and without atrial fibrillation. The research identified a significantly increased frequency of Th1, Th17, and Th1/Treg cells in patients with RA-AF. Th1 cells produce interferon-gamma (IFN-γ) and interleukin-2 (IL-2), which may contribute to atrial remodelling by stimulating proinflammatory cytokine secretion from macrophages. Additionally, elevated levels of interleukin-17A, secreted by Th17 cells, have been associated with the pathogenesis of AFthrough neutrophil-mediated inflammation and myocardial fibrosis [17]. The activation of complement locally leads to tissue damage, necrosis of myocytes and fibrosis, which triggers remodelling in the atrium. These changes in structure result in electrical activity changes in conduction patterns and varying refractory periods, often presenting as prolonged P wave duration and increased P wave dispersion (Pd) on an electrocardiogram [1].
The literature suggests that chronic inflammation in RA contributes to ventricular structural changes, such as fibrosis, which may also promote arrhythmias. Overt systolic dysfunction is uncommon, but subtle diastolic impairment is frequent and correlates with disease activity. Left ventricular (LV) remodelling is common in RA patients without clinical heart failure (HF). Proinflammatory cytokines such as TNFα and IL-1β have been shown to downregulate and disrupt connexin distribution in cardiomyocytes. Although ventricular connexin expression has not been directly studied in RA, evidence from Lazzerini et al. demonstrates an inverse association between atrial connexin levels and serum IL-6 in patients with inflammatory diseases. These findings suggest that chronic inflammation in RA may contribute to ventricular arrhythmogenesis via connexin downregulation [7]. In one study of 158 RA patients without clinical HF transthoracic echocardiography over 4–6 years showed an increase in LV remodelling, from 40% to 60%. Elevated IL-6 levels were associated with concentric remodelling and tocilizumab use correlated with increased relative wall thickness at baseline. These findings highlight IL-6 as a potential biomarker of LV remodelling in RA, warranting further prospective studies on its progression and modulation through IL-6 inhibition [18].
4.2. Autonomic Nervous System
Autonomic nervous system dysfunction in RA (evident in about 60% of patients) is linked to the neurotoxic impact of chronic systemic inflammation, as well as the side effects of certain therapeutic agents. The primary pattern involves disrupted cardiovascular reflexes and abnormal heart rate variability, reflecting decreased parasympathetic activity and increased sympathetic tone. This imbalance can lead to atrial ectopic beats, poor heart rate regulation and episodes of atrial tachycardia [5]. Arrhythmias can result from various electrophysiological disturbances, such as increased automaticity, delayed afterdepolarisations due to excess intracellular calcium, early afterdepolarisations caused by prolonged action potential duration, and the formation of reentrant circuits [7].
The regulation of cardiovascular, fluid, and energy balance relies on the coordinated interaction between the neuroendocrine and autonomic nervous systems, controlled by central neural networks. In the progression of HF these regulatory networks become impaired, leading to autonomic dysfunction. Recent evidence implicates chronic overactivation of G protein-coupled receptor kinase 2 (GRK2) in cardiac dysfunction and remodeling, primarily through β1-adrenergic receptor (β1AR) desensitisation. Prolonged exposure to high epinephrine levels induces GRK2-mediated β1AR phosphorylation, receptor internalisation, and reduced cardiomyocyte contractility. GRK2 inhibitors are thus proposed as potential therapeutic agents capable of mitigating arthritis-related inflammation, restoring β1AR sensitivity, and preventing cardiac dysfunction [19].
4.3. Renin Angiotensin System
RAS has been traditionally characterized as a hormonal cascade primarily responsible for regulating blood pressure and fluid-electrolyte homeostasis, playing a central role in cardiovascular and renal physiology through various mediators, receptors or intracellular signalling pathways. In patients with RA, elevated angiotensin-converting enzyme (ACE) levels have been detected in synovial fluid, implicating the classical RAS pathway in joint degradation [20]. Angiotensin II (Ang II) levels are significantly higher compared to the patients in remission, promoting AF by driving inflammation, epicardial fat accumulation, and electrical remodelling of the heart. RAS blockade therapy has been shown to reduce the relative risk of recurrent AF by 39% [21].
There have been a few studies that have explored the effects of biologic and targeted synthetic DMARDs on ACE and ACE 2 levels. Janus kinase (JAK) inhibition may lead to increased serum ACE levels and a temporary rise in ACE 2 activity in patients with RA, suggesting a redistribution and shedding of renin–angiotensin–aldosterone system (RAAS) components between the synovium and the bloodstream. Baseline levels of ACE and ACE 2 appear to be associated with disease activity, inflammatory markers such as ESR, and indicators of autoimmunity like RF. Moreover, baseline autoantibody levels (RF, ACPA) may be key determinants of how tofacitinib modulates the RAAS. These changes in ACE and ACE2 dynamics may partially explain the cardiovascular benefits observed with targeted synthetic DMARDs in RA patients [22].
4.4. Endothelial Dysfunction
The endothelium, a specialised epithelial layer lining blood vessels, lymphatics, and the heart, functions as a key endocrine organ in regulating vascular tone, coagulation, permeability and cell adhesion. Endothelial dysfunction disrupts these functions and contributes to disease pathogenesis. During inflammation, endothelial cells exhibit two activation types: a rapid, transient Type I and a delayed, sustained Type II. This increases permeability, stimulates cytokine and enzyme release, and promotes leukocyte adhesion via upregulated adhesion molecules [23].
Endothelial dysfunction is prevalent in RA,even in the absence of clinically apparent cardiovascular disease, and involves both macrovascular and microvascular compartments. Macrovascular dysfunction can be evaluated through flow-mediated dilation and biomarkers such as asymmetric dimethylarginine, matrix metalloproteinases, and toll-like receptors. Microvascular dysfunction is characterized by inflammatory activation, reduced capillary density, impaired vasodilation, and defective angiogenesis [24]. In inflammatory diseases like RA,high levels of pro-inflammatory molecules trigger endothelial activation and dysfunction, promoting leukocyte infiltration into heart tissue. Oxidative stress reduces nitric oxide availability, lowering cGMP and PKG levels in heart cells, which leads to cardiac hypertrophy and increased resting tension. Additionally, MHCII high macrophages, activated by IL-10, release osteopontin and TGF-β, stimulating fibroblast growth and collagen buildup. Together, these changes increase heart stiffness and contribute to diastolic dysfunction [25].
A 2022 study found that MTX can improve endothelial function in patients with early RA by reducing inflammation and supporting vascular repair. The mechanism involves lowering the activation of endothelial cells caused by TNF-α, specifically by regulating molecules like VCAM-1, ICAM-1 and E-selectin. MTX also prevents cell death, promotes healthy cell growth and reduces pro-inflammatory cytokines such as IL-6 and MCP-1. These positive effects become noticeable after three months of treatment and continue with long-term use [26].
4.5. Epicardial Tissue Adiposity and Inflammation
Obesity, characterized by a chronic low-grade systemic inflammatory state, leads to adipocyte hypertrophy and a hypoxic environment that triggers genetic mutations and alters the regulation of pro- and anti-inflammatory mediators. This inflammatory state is associated with an increased risk of atrial and ventricular arrhythmias, with a 65% higher risk of AF in individuals with a BMI >30 kg/m² compared to those with a normal BMI. This increased risk is linked to electrophysiological remodelling, including atrial volume expansion, conduction abnormalities, and upregulation of pro-fibrotic mediators, creating a proarrhythmogenic substrate [23].
Epicardial adipose tissue (EAT) is a fat layer located between the myocardium and the visceral pericardium, serving as a source of inflammatory mediators. Previous research has found that the thickness of EAT in patients with RA is greater than in the control population. In patients with RA and AF the LA diameter positively correlates with the EAT/BMI ratio, a relationship not observed in AF patients without RA. Previous reports have shown extensive atrial fibrosis in RA patients, which reduces LA compliance and leads to dilation. Additionally, RA patients have more pericardial adipose tissue around the LA compared to those without RA. Chahine demonstrated that LA epicardial adipose tissue is independently associated with LA volume and fibrosis, and suggested that EAT may promote atrial structural remodelling via paracrine inflammatory factors [24]. EAT thickness correlates with P-wave duration in morbidly obese patients and with LA diameter. In healthy individuals with normal atrial dimensions, the relationship between EAT and P-wave duration likely indicates slowed atrial conduction. However, in morbidly obese patients, P-wave prolongation is partly attributed to atrial enlargement. In patients with the largest EAT volumes, the PR interval was 10 to 16 milliseconds longer compared to those with the smallest EAT volumes. Observational studies have shown that a prolonged PR interval is associated with an increased incidence of AF HF and mortality. Additionally, high EAT volumes are linked to a higher incidence of AF. Prolonged QRS duration indicates slowed ventricular conduction and may result from hypertrophy. Increased BMI is linked to longer QRS duration. In a study of 3.087 healthy subjects, higher EAT volume was associated with a 6.7 millisecond increase in QRS duration for those above the 95th percentile compared to those below the 5th percentile, after adjusting for covariates. Research on the relationship between EAT volume and the QT interval, as well as its dispersion (QTd), is limited. One study reported a negative association between EAT volume and QTc. In the only available observational study on EAT and T peak-T end, a higher EAT volume was linked to increased QT dispersion, indicating greater repolarisation heterogeneity [25].
Higher adiponectin levels are independently associated with an increased risk of AF particularly in older individuals. Circulating adiponectin levels are significantly elevated in RA patients, where they contribute to the pro-inflammatory processes involved in the disease's pathogenesis. EAT thickness is positively correlated with the severity of RA [21].
Systemic inflammatory disorders can lead to injury in the coronary microcirculation, resulting in microvascular dysfunction and myocardial fibrosis. Since the epicardium and myocardium are interconnected through an unobstructed microcirculation, the release of proinflammatory adipocytokines (tumour necrosis factor-α, interleukin-1β, interleukin-6) can cause microcirculatory damage and fibrosis in the adjacent myocardium, particularly in the atrial myocardium, which contributes to AF [26].
5. Effects of Antirheumatic Drugs on Cardiac Rhythm
Ongoing advancements in drug design procedures and techniques have significantly enhanced pharmacological strategies for treating rheumatoid arthritis. These developments have led to therapies that effectively alleviate symptoms, slow disease progression, and reduce complications. According to the most recent ACR and EULAR guidelines, current RA management focuses on two main approaches: symptomatic treatment using nonsteroidal anti-inflammatory drugs (NSAIDs) and glucocorticoids (GCs), and disease-modifying therapy through the use of DMARDs. Initiating treatment at the earliest possible stage is essential. Due to their delayed onset of action, from 6 weeks to 6 months, disease-modifying antirheumatic drugs (DMARDs) should be introduced promptly. DMARDs are classified into three categories: conventional synthetic (csDMARDs), biologic (bDMARDs), and targeted synthetic (tsDMARDs) [27].
5.1. csDMARDs
In recent years, the management of RAhas emphasized early intervention with conventional synthetic disease-modifying antirheumatic drugs (csDMARDs). MTX (MTX) is used as the unequivocal first-line agent, to reduce inflammation, slow radiographic progression and improve long term outcomes. In cases of MTX intolerance or contraindication, leflunomide (LEF), hydroxychloroquine (HCQ) or sulfasalazine (SASP) may be substituted [28]. The cardiovascular effects and the possible correlations of arrhythmias with each csDMARDs are summarised in Figure 2.
5.1.1. Methotrexate
MTX, a folate antagonist, exerts anti-proliferative, anti-metabolic, and anti-inflammatory effects by reducing pro-inflammatory cytokines and limiting the infiltration of immune cells like neutrophils, monocytes, mast cells, Th cells, and B cells in the RA synovium [29].
Larger studies have shown that patients with RA have a higher risk of arrhythmias, particularly atrial fibrillation. A retrospective cross-sectional study investigated the potential association between MTX intermittent treatment and cardiovascular risk in RA patients. The analysis compared two groups: individuals who had ceased MTX therapy prior to enrolment (MTX 0) and those actively receiving the drug at the time of data collection (MTX 1). Findings revealed a higher incidence of arrhythmias in the MTX 0 group (9.0%) compared to the MTX 1 group (4.9%), indicating that discontinuation of MTX may be associated with a significantly elevated risk of cardiovascular complications [30].
Additionally, a retrospective case-control study involving 405 patients with RAfound that those who experienced cardiovascular events, including arrhythmias, were significantly less likely to have been treated with MTX compared to those without CVD (p = 0.003). The results suggest an inverse relationship between MTX use and the prevalence of arrhythmias. Despite the fact that the study design does not present definitive conclusions, the findings support the idea that MTX may have a protective cardiovascular effect, likely due to its anti-inflammatory properties [31].
5.1.2. Leflunomide
LEF is a non-biologic DMARD that inhibits dihydroorotate dehydrogenase, a key enzyme in pyrimidine synthesis. This suppresses activated T-cell proliferation, leading to reduced inflammation and joint damage [32].
A study of the 108.085 patients with seropositive RA evaluated whether DMARD treatment is associated with incident AF. LEF use was associated with a significantly increased risk of new-onset AF, exhibiting a 1.21 times higher risk of developing AF than non-LEF users. Noticeably, this effect was observed in a subgroup of patients aged 50 years and females [33]. In 2024, an experimental study by Jiang et al. suggested that LEF may improve cardiovascular outcomes by modulating lipid metabolism and endothelial function via the DHODH/AMPK pathway. However, its cardioprotective effects remain unclear due to limited clinical evidence [32].
5.1.3. Antimalarials
HCQ is commonly used to treat RA, as well as for malaria prevention, and has been associated with arrhythmias by slowing the rate of action potential firing in the sinoatrial node. This effect is thought to result from the structural similarity between HCQ and class IA anti-arrhythmic quinidine, which blocks sodium and potassium channels. This blockade can prolong the QT interval by increasing the risk of Torsade de Pointes, a potentially life-threatening arrhythmia [34].
The most recent studies focusing on the association between HCQ and arrhythmias in RA patients show contradictory data, but the majority emphasize a low risk. Table 1.
5.1.4. Sulfasalazine
SASP is chemically made up of 5-aminosalicylic acid and sulphapyridine, connected by azo bonds. While it is commonly used as an anti-inflammatory treatment for inflammatory arthritis and inflammatory bowel disease, sulphapyridine itself may also have therapeutic potential specifically for rheumatoid arthritis. However, the precise molecular mechanisms by which sulfasalazine exerts its effects in RA treatment are still not fully understood [39].
There are no specific studies on the involvement of sulfasalazine in the prevalence of arrhythmias. However, a 2022 study using an Ang II-induced cardiac remodelling mouse model treated with sulfasalazine evaluated blood pressure, cardiac function, and pathological changes, as well as Akt phosphorylation in vivo and in vitro. The results indicate that sulfasalazine, independent of its anti-inflammatory properties, exacerbates cardiac dysfunction, hypertrophy, and fibrosis by aggravating Ang II-induced cardiac remodelling through activation of the Akt signalling pathway. Despite these findings, the exact role of sulfasalazine in cardiac remodelling remains unclear [40].
5.2. bDMARDs and tsDMARDs
The 21st century brought a paradigm shift in RA treatment with the introduction of bDMARDs alongside tsDMARDs complementing conventional synthetic DMARDs (csDMARDs). These advances have made clinical remission achievable for most patients, enabling long-term prevention of joint damage and physical disability progression. The marketed biologics available for the treatment of RA include five TNF-targeting drugs, two IL-6 receptor-targeting drugs, one B cell antigen CD20-targeting antibody and one selective T cell costimulatory modulator [41]. The cardiovascular implications of these agents, along with their correlation with arrhythmic events, are presented in Table 2.
TNF inhibitors carry significant risks for patients with pre-existing heart failure. The 2021 ACR guidelines recommend using non-TNF biologics or targeted synthetic DMARDs in RA patients with HF (NYHA class II–IV or EF < 50%). These recommendations underscore the need for personalised treatment that includes cardiovascular risk assessment, QT interval evaluation, and consideration of existing cardiac conditions and CVD history to ensure safe and effective RA management [32].
Elevated interleukin-6 levels in systemic inflammation are linked to acquired long QT syndrome (LQTS) and increased risk of torsade de pointes. While the underlying mechanisms remain unclear, most cases of acquired LQTS involve dysfunction of the hERG channel, which mediates the rapid delayed rectifier K⁺ current (IKr) essential for cardiac repolarization [42]. However, interleukine-6 Inhibitors such as Tocilizumab suggests a potential antiarrhythmic effect, normalizing the QTc interval by dampening systemic inflammation [43].
CD20 is a transmembrane protein found on B lymphocytes, involved in their activation and differentiation. Rituximab targets CD20 and induces cell death through complement activation, antibody-dependent cytotoxicity, and apoptosis. After B-cell lysis, CD20 can redistribute to tissues such as cardiac myocytes, where its inhibition may disturb calcium handling and trigger early after depolarisations, potentially leading to arrhythmias like polymorphic VT or torsade de pointes, especially in patients with prolonged QT intervals. However, the exact mechanisms linking rituximab to arrhythmias are still not fully understood [44].
The main representative of selective T-cell co-stimulation inhibitors is abatacept. This biologic agent is blocking the co-stimulatory CD80/CD86:CD28 pathway, resulting in inhibiting full T cell activation and mitigating inflammatory processes in diseases such as RA [45]. Current cardiovascular evidence for abatacept predominantly addresses HF arterial stiffness, lipid metabolism, and major adverse cardiovascular events, with comparatively limited data on cardiac rhythm disturbances. The potential cardioprotective effects mediated by its anti-inflammatory activity appear to remain largely preserved [46].
Targeted synthetic DMARDs, such as the JAK inhibitors, represent an advanced class of oral therapies that inhibit JAK enzymes involved in immune signalling. By precisely modulating these pathways, they effectively reduce inflammation and provide alternatives for patients unresponsive or intolerant to conventional DMARDs or biologics. Due to their impact on critical signalling, JAK inhibitors require careful monitoring for potential infections and other adverse effects [47].
5.3. Complementary Therapies
5.3.1. Corticosteroids
GCS have demonstrated efficacy in improving the management of rheumatoid arthritis. However, difficulties with dose tapering lead to long-term use in up to one-third of patients. Notably, the 2021 American College of Rheumatology (ACR) guidelines did not recommend the use of GCS as short-term bridge therapy, contrasting with other guidelines that support or offer more nuanced recommendations regarding their use [61]. Steroid therapy may induce a range of arrhythmias through its direct effects on cardiac membrane potassium channels and the regulation of their expression [62].
The literature review conducted by Tisdale et al. analysed the most commonly used medications that may induce or exacerbate various types of arrhythmias. The article indicated that the incidence of AF and AFl associated with methylprednisolone is approximately 1.8%. However, the association between corticosteroid use and AF remains inconsistent, as arrhythmias are often secondary to the underlying medical condition rather than the medication itself. Atrioventricular nodal re-entrant tachycardia has also been reported in association with methylprednisolone use, although it is rare. The mechanism remains uncertain but is thought to involve intracellular electrolyte imbalances and repolarisation disturbances [63].
The most recent study that demonstrates the association between corticosteroids and arrhythmogenesis used male Sprague-Dawley rats. The glucocorticoid administration leads to significant alterations in the expression of key ion channel genes, including those encoding L-type calcium channels and T-type calcium channels, which are crucial for maintaining normal cardiac rhythm. These changes in gene expression result in disrupted calcium ion handling and increased susceptibility to atrial fibrillation. Furthermore, the research highlights the role of the glucocorticoid receptor in mediating these effects, suggesting that glucocorticoid-induced arrhythmogenesis is a receptor-dependent process. The findings underscore the importance of considering glucocorticoid therapy as a potential risk factor for atrial arrhythmias, particularly in patients with underlying cardiac conditions [64].
5.3.2. Sinomenine and Arrhythmias
Sinomenine, the main alkaloid from Sinomenium acutum, is a traditional Chinese medicine widely used in rheumatology and has shown cardioprotective and anti-arrhythmic effects. It modulates cardiac electrophysiology by prolonging action potential duration, enhancing repolarization, and reducing excitability through inhibition of key ion currents, including L-type calcium, delayed rectifier potassium, IK1, and fast sodium currents. These actions lower intracellular calcium, limit calcium overload, and reduce the risk of arrhythmias, highlighting sinomenine as a potential therapeutic option for cardiac rhythm disorders [65].
6. Diagnosis of Arrhythmias in RA
Early and accurate diagnosis of cardiac electrophysiology abnormalities in patients with RA is essential, because cardiac involvement may often be subclinical. An interdisciplinary evaluation by both rheumatologists and cardiologists is recommended for all RA patients to identify the risk of severe complications, including sudden cardiac death. Initial assessment includes clinical evaluation, laboratory tests, 12-lead ECG, and standard echocardiography, but the arrhythmias screening can be extended [5]. A visual representation of the diagnosis algorithm, which can be very useful in clinical practice, is presented in Figure 3.
RA has been linked to various subtle abnormalities on the 12-lead electrocardiogram. While a normal ECG reflects rapid and synchronous ventricular depolarization and repolarization, patients with RA may exhibit disturbances in both phases of the cardiac action potential. Although some studies report similar QTc durations but increased QT dispersion (QTd), indicating subclinical repolarisation abnormalities, the patients frequently show a corrected QT interval (QTc) prolonged by 10–20 ms in comparison to healthy controls. These discrepancies could be caused by small sample sizes or the impact of the severity and duration of the disease. One study observed elevated QTc over a 12-year period in RA patients, but no differences in QTc at diagnosis. Longer QTc durations have been linked to increased CRP levels and cytokine levels, especially IL-10 after age adjustment [7].
Gülkesen et al. identified new ECG indicators that may predict arrhythmia risk in patients with rheumatoid arthritis. The study compared P-wave dispersion (Pd), corrected QT (QTc) dispersion, Tp-e dispersion, and the Tp-e/QTc ratio between RA patients and healthy controls. P-wave dispersion (Pd) represents the difference between the longest (P max) and shortest (P min) P-wave duration on the ECG. Tp-e defines the interval from the T-wave peak to its end. In RA, local atrial complement activation leads to tissue injury, myocyte necrosis, and atrial fibrosis, resulting in structural remodelling. This creates electrical inhomogeneity, slower conduction, and variable refractory periods, which manifest as prolonged P waves and increased Pd, a known risk factor for paroxysmal and persistent atrial fibrillation. Corrected QT dispersion (QTc d) is defined as the difference between the maximum (QTc max) and minimum (QTc min) QT intervals. Increased QTc d reflects heterogeneous ventricular repolarization, which predisposes to ventricular instability, re-entry, and sudden cardiac death. The Tp-e interval, measured from the peak to the end of the T wave, reflects transmural dispersion of ventricular repolarization. Elevated Tp-e dispersion and Tp-e/QTc ratio indicate higher ventricular arrhythmia risk. The study concluded that RA patients showed significantly higher Pd, QTcd, Tp-ed, and Tp-e/QTc values compared with controls, suggesting an increased risk for both atrial and ventricular arrhythmias [1].
Twenty-four-hour Holter ECG offers a more detailed and prognostically meaningful assessment of QTc duration and arrhythmias, being a better option to complete the cardiovascular assessment of RA patients compared to short-term ECG recordings. A study that analysed 58 RA patients (22 males, 36 females) used both short ECG and 24-hour Holter monitoring, revealing significantly higher QTc values. The number of QRS complexes with QTc > 450 ms was strongly associated with ventricular ectopy and inflammation, proving that Holter monitoring provides a more accurate evaluation of QTc dynamics and arrhythmic risk in RA patients [66].
Both classic and advanced diagnostic tools are valuable for evaluating cardiac function and detecting myocardial involvement and coronary artery disease, key factors in arrhythmias in autoimmune rheumatic diseases. Advanced echocardiographic techniques like 2D/3D speckle-tracking and global longitudinal strain can detect early ventricular dysfunction, diastolic abnormalities, and valvular disease. However, normal echocardiography does not exclude cardiac involvement. PET and cardiac MRI offer superior tissue characterisation for detecting inflammation and fibrosis [5].
Cardiac magnetic resonance imaging (CMR) has revealed proarrhythmic substrates in RA, with 45% of asymptomatic patients showing abnormalities, mainly epicardial late gadolinium enhancement (LGE), indicative of myocardial fibrosis or myocarditis. Some also showed perfusion defects suggesting microvascular ischemia, possibly from vasculitis. LGE presence correlated with disease activity markers and brain-derived natriuretic peptide levels, indicating subclinical myocardial involvement. These findings, supported by other studies, suggest many RA patients may have undetected myocardial fibrosis, and some may benefit from intensive disease-modifying therapy to improve perfusion [7].
7. Management of Arrhythmias in RA
Contemporary strategies for managing cardiac arrhythmias adopt a multidisciplinary approach, aiming to optimize therapeutic outcomes by carefully balancing the potential benefits and associated risks of available interventions. The therapeutic plan involves tight control of RA activity using csDMARDs/bDMARDs, anti-arrhythmic drugs, autonomic modulation, implantable cardioverter–defibrillator (ICD) implantation, cardiac stereotactic body radiotherapy (SBRT) and catheter ablation [67].
The use of csDMARDs and bDMARDs in patients with autoimmune diseases such as RAhas raised questions about their cardiovascular safety, including the risk of cardiac arrhythmias. While traditional DMARDs (e.g., MTX, sulfasalazine) generally have a favourable cardiac safety profile, emerging data suggest that some bDMARDs may influence electrophysiological stability. Their use needs to be balanced with patient-associated comorbidities.
Anti-arrhythmic drugs are pharmacologic agents used to treat abnormal cardiac rhythms by modifying the electrical impulses within the myocardium. They are typically classified according to the Vaughan-Williams classification, which categorizes them based on their primary electrophysiological effect. However, considering the adverse effect profiles of anti-arrhythmic agents and the autoimmune nature of RA, therapeutic strategies must be approached with heightened clinical vigilance and tailored to the individual patient’s risk profile. The side effects of anti-arrhythmic drugs that can alter RA patients’ comorbidities are summarised in Table 3. Furthermore, drug-drug interactions between anti-arrhythmic agents and conventional, biologic or targeted synthetic DMARDs (e.g., MTX, LEF, tocilizumab, or JAK inhibitors) must be carefully monitored, especially with agents metabolized via hepatic cytochrome P450 pathways [68].
Alternative approaches are needed to modify arrhythmia substrates without damaging heart tissue. Reducing procedure-related inflammation through targeted therapies may lower arrhythmia recurrence. Cell-based molecular therapies show promise in restoring gene expression, protecting heart cells, regulating immune responses, and minimizing scarring to improve heart function.
Autonomic nerve remodelling, involving vagal stimulation that shortens the atrial refractory period, is a potential gene therapy target. Inhibiting components of the G-protein coupled autonomic pathway (like Gαi and Gαo) has effectively modulated atrial electrophysiology and reduced AF in animal studies. Gap junction remodelling, due to decreased or mislocalised connexins (Cx40, Cx43), disrupts electrical conduction and raises arrhythmia risk. Targeting these connexins improves conduction and lowers arrhythmia burden. Structural remodelling, characterized by fibrosis and increased TGF-β, is another key target; blocking TGF-β signalling can reduce fibrosis and related arrhythmias. For catecholaminergic polymorphic ventricular tachycardia (CPVT), gene-based strategies such as gene replacement, mutant gene silencing, CRISPR/Cas9 editing, and pathway suppression have shown promise in preclinical models [67].
8. Future Perspectives
Future perspectives for the management of arrhythmias in RA increasingly focus on gene-based therapies. These approaches aim to identify and mitigate the genetic mechanisms underlying atrial fibrillation. Two primary mechanisms driving AF are focal ectopic firing and reentry, both influenced by electrical and structural remodelling, autonomic nervous system alterations, and abnormalities in calcium handling.
Electrical remodelling is typically characterized by a shortening of the atrial action potential duration, which results from a reduction in the L-type calcium (Ca2+) current and an increase in the inward-rectifier potassium current (IK1). Furthermore, constitutive activation of the acetylcholine-induced potassium current (IKACh) may also contribute to this process. Abnormal calcium handling is another key contributor to ectopic activity, particularly due to calcium leak from the sarcoplasmic reticulum (SR) via the ryanodine receptor type 2 (RyR2). Targeting specific phosphorylation sites on RyR2 or employing modified forms of calmodulin (CaM) has demonstrated potential in attenuating SR calcium leak and reducing the susceptibility to AF [84].
9. Conclusions
RA is increasingly recognized not only as a joint-destructive autoimmune disease but also as a systemic inflammatory rheumatic disorder with significant cardiovascular implications. Epidemiological data consistently demonstrate an elevated incidence of cardiac arrhythmias, particularly AF and conduction abnormalities due to chronic inflammation, structural cardiac remodeling, and autonomic dysfunction. The presence of comorbidities such as interstitial lung disease, vasculitis, and ischemic heart disease further amplifies this risk.
Early identification of arrhythmias in RA is often complicated by overlapping symptoms (e.g., fatigue, dyspnea) and subclinical manifestations. Proactive cardiovascular screening, which includes echocardiography, Holter analysis, and ECG monitoring, is therefore necessary, particularly for patients who have a history of heart disease, a high disease activity, or history of cardiac involvement. A multidisciplinary approach is required for the therapeutic management of arrhythmias in RA, customizing to each patient's risk profile while accounting for drug-drug interactions with biologics or DMARDs.
Ultimately, optimal arrhythmia management in RA hinges not only on cardiologic intervention but also on effective control of systemic inflammation. Emerging evidence suggests that certain biologic DMARDs may indirectly reduce arrhythmic burden by attenuating inflammatory pathways implicated in atrial and ventricular remodeling. Further research is essential to define the precise interplay between immunomodulation and cardiac electrophysiology in this population.
Author Contributions
Conceptualization, V.U.; D.E.C., M.C.D., C.A. and M.F.; methodology, V.U.; A.O. and D.E.F; software, X.X.; validation, V.U., C.A. and M.F.; formal analysis, D.E.C., M.C.D., S.M.S., G.L.B. and M.M.G; investigation, V.U.; D.E.C. and M.C.D.; resources, D.T.M.; D.M.T. and A.K.; data curation, A.O.; writing—original draft preparation, V.U., P.C.M., A.F.O., M.M.G. and M.F.; writing—review and editing, V.U., M.F., D.E.F., D.M.T., A.K., C.A., S.M.S. and G.L.B.; visualization, V.U., D.E.C., M.C.D. and M.F.; supervision, A.O., C.A., and A.K..; project administration, D.E.C., M.C.D., D.M.T., D.E.F. and S.M.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| β1AR | β1-adrenergic receptor |
| ACE | Angiotensin-Converting Enzyme |
| ACE 2 | Angiotensin-Converting Enzyme 2 |
| ACPA | Anti-Citrullinated Protein Antibodies |
| AF | Atrial Fibrillation |
| AFl | Atrial Flutter |
| Ang II | Angiotensin II |
| anti-MCV | Anti-Modified Citrullinated Vimentin Antibodies |
| bDMARDs | Biologic Disease-Modifying Antirheumatic Drugs |
| cGMP | Cyclic Guanosine Monophosphate |
| csDMARDs | Conventional Synthetic Disease-Modifying Antirheumatic Drugs |
| CV | cardiovascular |
| CVD | Cardiovascular Disease |
| DILE | Drug-induced lupus erythematosus |
| EAT | Epicardial Adipose Tissue |
| ELISA | enzyme-linked immunosorbent assay |
| E-selectin | Endothelial Selectin |
| ESR | Erythrocyte Sedimentation Rate. |
| GCs | Glucocorticoids |
| GRK2 | G protein-coupled receptor kinase 2 |
| HCQ | Hydroxychloroquine |
| HF | Heart Failure |
| ICAM-1 | Intercellular Adhesion Molecule-1 |
| ICD | Implantable Cardioverter–Defibrillator |
| IKr | Rectifier K⁺ Current |
| JAK | Janus kinase |
| LA | Left Atrial |
| LEF | Leflunomide |
| LGE | Epicardial Late Gadolinium Enhancement |
| LQTS | Long QT Syndrome |
| LV | Left Ventricular |
| MCP-1 | Monocyte Chemoattractant Protein-1 |
| MHCII | Major Histocompatibility Complex Class Ii |
| MTX | Methotrexate |
| NETs | Neutrophil extracellular traps |
| NSAIDs | Nonsteroidal Anti-Inflammatory Drugs |
| Pd | P-Wave Dispersion |
| PKG | Protein Kinase G |
| PSVT/SVT | Paroxysmal Supraventricular Tachycardia/Supraventricular Tachycardia |
| QTcd | Corrected QT Dispersion |
| QTd | QT Dispersion |
| RA | Rheumatoid Arthritis |
| RA-AF | Rheumatoid Arthritis Associated with Atrial Fibrillation |
| RAAS | Renin–Angiotensin–Aldosterone System |
| RAS | The Renin-Angiotensin System |
| RF | Rheumatoid Factor |
| SASP | Sulfasalazine |
| SBRT | Cardiac Stereotactic Body Radiotherapy |
| tsDMARDs | Targeted Synthetic Disease-Modifying Antirheumatic Drugs |
| VCAM-1 | Vascular Cell Adhesion Molecule-1 |
| VT | Ventricular Tachycardia |
| WPW | Wolff-Parkinson-White syndrome |
References
- Gülkesen, A.; Yıldırım Uslu, E.; Akgöl, G.; Alkan, G.; Kobat, M.A.; Gelen, M.A.; Uslu, M.F. Is the Development of Arrhythmia Predictable in Rheumatoid Arthritis? Arch Rheumatol 2024, 39, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Grune, J.; Yamazoe, M.; Nahrendorf, M. Electroimmunology and Cardiac Arrhythmia. Nat Rev Cardiol 2021, 18, 547–564. [Google Scholar] [CrossRef]
- Hannawi, S.M.; Hannawi, H.; Al Salmi, I. Cardiovascular Risk in Rheumatoid Arthritis: Literature Review. Oman Med J 2021, 36, e262. [Google Scholar] [CrossRef]
- Song, Q.; Shang, L.; Zhang, Y.; Cui, Y.; Du, J.; Hou, Y. Rheumatoid Arthritis and Risk of Atrial Fibrillation: Results from Pooled Cohort Studies and Mendelian Randomization Analysis. Cardiovascular Innovations and Applications 2024, 9, 976. [Google Scholar] [CrossRef]
- Plastiras, S.C.; Moutsopoulos, H.M. Arrhythmias and Conduction Disturbances in Autoimmune Rheumatic Disorders. Arrhythm Electrophysiol Rev 2021, 10, 17–25. [Google Scholar] [CrossRef] [PubMed]
- Khalid, Y.; Dasu, K.; Gabriel, N.; Roy, T.; Umrani, R.; Lee, M.; Dasu, N.R. Prevalence and Outcomes of Arrhythmias in Patients with Rheumatoid Arthritis. Heart Rhythm 2023, 20, S181. [Google Scholar] [CrossRef]
- Patel, K.H.K.; Jones, T.N.; Sattler, S.; Mason, J.C.; Ng, F.S. Proarrhythmic Electrophysiological and Structural Remodeling in Rheumatoid Arthritis. American Journal of Physiology-Heart and Circulatory Physiology 2020, 319, H1008–H1020. [Google Scholar] [CrossRef] [PubMed]
- Steiner, G.; Toes, R.E.M. Autoantibodies in Rheumatoid Arthritis – Rheumatoid Factor, Anticitrullinated Protein Antibodies and Beyond. Current Opinion in Rheumatology 2024, 36, 217. [Google Scholar] [CrossRef]
- Salma, K.; Nessrine, A.; Krystel, E.; Khaoula, E.K.; Noura, N.; Khadija, E.; Taoufik, H. Rheumatoid Arthritis: Seropositivity versus Seronegativity; A Comparative Cross-Sectional Study Arising from Moroccan Context. Curr Rheumatol Rev 2020, 16, 143–148. [Google Scholar] [CrossRef]
- Spitsina, S.; Mozgovaya, E.; Trofimenko, A.; Bedina, S.; Mamus, M. Electrocardiographic Manifestations in Patients with Seropositive Rheumatoid Arthritis. Annals of the Rheumatic Diseases 2021, 80, 1108. [Google Scholar] [CrossRef]
- Kumar, A.; Vasdev, V.; Patnaik, S.K.; Bhatt, S.; Singh, R.; Bhayana, A.; Hegde, A.; Kumar, A. The Diagnostic Utility of Rheumatoid Factor and Anticitrullinated Protein Antibody for Rheumatoid Arthritis in the Indian Population. Med J Armed Forces India 2022, 78, S69–S74. [Google Scholar] [CrossRef] [PubMed]
- Iyengar, K.P.; Vaish, A.; Nune, A. Anti-Cyclic Citrullinated Peptide Antibody (ACPA) and Rheumatoid Arthritis: Clinical Relevance. J Clin Orthop Trauma 2022, 24, 101729. [Google Scholar] [CrossRef]
- Aiewruengsurat, D.; Phongnarudech, T.; Liabsuetrakul, T.; Nilmoje, T. Correlation of Rheumatoid and Cardiac Biomarkers with Cardiac Anatomy and Function in Rheumatoid Arthritis Patients without Clinically Overt Cardiovascular Diseases: A Cross-Sectional Study. Int J Cardiol Heart Vasc 2022, 44, 101161. [Google Scholar] [CrossRef] [PubMed]
- Van Steendam, K.; Tilleman, K.; Deforce, D. The Relevance of Citrullinated Vimentin in the Production of Antibodies against Citrullinated Proteins and the Pathogenesis of Rheumatoid Arthritis. Rheumatology (Oxford) 2011, 50, 830–837. [Google Scholar] [CrossRef]
- Norouzi, S.; Javinani, A.; Aminorroaya, A.; Masoumi, M. Anti-Modified Citrullinated Vimentin Antibody: A Novel Biomarker Associated with Cardiac Systolic Dysfunction in Patients with Rheumatoid Arthritis. BMC Cardiovasc Disord 2020, 20, 390. [Google Scholar] [CrossRef] [PubMed]
- Lazzerini, P.E.; Acampa, M.; Hammoud, M.; Maffei, S.; Capecchi, P.L.; Selvi, E.; Bisogno, S.; Guideri, F.; Galeazzi, M.; Pasini, F.L. Arrhythmic Risk during Acute Infusion of Infliximab: A Prospective, Single-Blind, Placebo-Controlled, Crossover Study in Patients with Chronic Arthritis. J Rheumatol 2008, 35, 1958–1965. [Google Scholar]
- Wang, X.; Fan, H.; Wang, Y.; Yin, X.; Liu, G.; Gao, C.; Li, X.; Liang, B. Elevated Peripheral T Helper Cells Are Associated With Atrial Fibrillation in Patients With Rheumatoid Arthritis. Front. Immunol. 2021, 12, 744254. [Google Scholar] [CrossRef]
- Park, E.; Ito, K.; Depender, C.; Giles, J.T.; Bathon, J. Left Ventricular Remodeling in Rheumatoid Arthritis Patients without Clinical Heart Failure. Arthritis Res Ther 2023, 25, 124. [Google Scholar] [CrossRef]
- Zhang, M.; Wang, M.; Tai, Y.; Tao, J.; Zhou, W.; Han, Y.; Wei Wei; Wang, Q. Triggers of Cardiovascular Diseases in Rheumatoid Arthritis. Current Problems in Cardiology 2022, 47, 100853. [Google Scholar] [CrossRef]
- Braz, N.F.T.; Pinto, M.R.C.; Vieira, É.L.M.; Souza, A.J.; Teixeira, A.L.; Simões-e-Silva, A.C.; Kakehasi, A.M. Renin–Angiotensin System Molecules Are Associated with Subclinical Atherosclerosis and Disease Activity in Rheumatoid Arthritis. Modern Rheumatology 2021, 31, 119–126. [Google Scholar] [CrossRef]
- Qian, Y.; Fei, Z.; Nian, F. The Association Between Rheumatoid Arthritis and Atrial Fibrillation: Epidemiology, Pathophysiology and Management. IJGM 2023, Volume 16, 1899–1908. [Google Scholar] [CrossRef]
- Kacsándi, D.; Fagyas, M.; Horváth, Á.; Végh, E.; Pusztai, A.; Czókolyová, M.; Soós, B.; Szabó, A.Á.; Hamar, A.; Pethő, Z.; et al. Effect of Tofacitinib Therapy on Angiotensin Converting Enzyme Activity in Rheumatoid Arthritis. Front Med (Lausanne) 2023, 10, 1226760. [Google Scholar] [CrossRef] [PubMed]
- Patel, K.H.K.; Hwang, T.; Se Liebers, C.; Ng, F.S. Epicardial Adipose Tissue as a Mediator of Cardiac Arrhythmias. American Journal of Physiology-Heart and Circulatory Physiology 2022, 322, H129–H144. [Google Scholar] [CrossRef] [PubMed]
- Yao, H.; Chen, J.; Li, X.; Zhang, X. Relationship between Epicardial Adipose Tissue Volume and Atrial Fibrillation in Patients with Rheumatoid Arthritis. Front. Cardiovasc. Med. 2025, 12. [Google Scholar] [CrossRef] [PubMed]
- Ernault, A.C.; Meijborg, V.M.F.; Coronel, R. Modulation of Cardiac Arrhythmogenesis by Epicardial Adipose Tissue. JACC 2021, 78, 1730–1745. [Google Scholar] [CrossRef] [PubMed]
- Packer, M. Characterization, Pathogenesis, and Clinical Implications of Inflammation-Related Atrial Myopathy as an Important Cause of Atrial Fibrillation. JAHA 2020, 9, e015343. [Google Scholar] [CrossRef] [PubMed]
- Radu, A.-F.; Bungau, S.G. Management of Rheumatoid Arthritis: An Overview. Cells 2021, 10, 2857. [Google Scholar] [CrossRef] [PubMed]
- Vassilopoulos, D.; Aslanidis, S.; Boumpas, D.; Kitas, G.; Nikas, S.N.; Patrikos, D.; Sfikakis, P.P.; Sidiropoulos, P. Updated Greek Rheumatology Society Guidelines for the Management of Rheumatoid Arthritis. Mediterr J Rheumatol 2020, 31, 163–171. [Google Scholar] [CrossRef]
- Zhao, Z.; Hua, Z.; Luo, X.; Li, Y.; Yu, L.; Li, M.; Lu, C.; Zhao, T.; Liu, Y. Application and Pharmacological Mechanism of Methotrexate in Rheumatoid Arthritis. Biomedicine & Pharmacotherapy 2022, 150, 113074. [Google Scholar] [CrossRef]
- Hloch, K.; Doseděl, M.; Duintjer Tebbens, J.; Žaloudková, L.; Medková, H.; Vlček, J.; Soukup, T.; Pávek, P. Higher Risk of Cardiovascular Diseases in Rheumatoid Arthritis Patients Without Methotrexate Treatment. Front Pharmacol 2021, 12, 703279. [Google Scholar] [CrossRef]
- Tekeoglu, S. Prevalence and Risk Factors of Cardiovascular Disease in Rheumatoid Arthritis Patients: A Comparative Analysis of Real-World Data. Int J Gen Med 2024, 17, 5859–5868. [Google Scholar] [CrossRef]
- Sunkara, P.; Garikipati, N.A.; Nimmagadda, R.; Cherukuri, A.M.K.; Anne, H.; Chakilam, R.; Yadav, D.; Sunkara, P.; Garikipati, N.A.; Nimmagadda, R.; et al. Cardiovascular Outcomes of Disease-Modifying Antirheumatic Drugs in Rheumatoid Arthritis: A Review of the Current Evidence. Cureus 2025, 17. [Google Scholar] [CrossRef]
- Kim, H.W.; Han, M.; Jung, I.; Ahn, S.S. New-Onset Atrial Fibrillation in Seropositive Rheumatoid Arthritis: Association with Disease-Modifying Anti-Rheumatic Drugs Treatment. Rheumatology 2024, 63, 630–638. [Google Scholar] [CrossRef]
- Farhat, H.; Kassab, C.J.; Tlaiss, Y.; Gutlapalli, S.D.; Ganipineni, V.D.P.; Paramsothy, J.; Tedesco, S.; Kailayanathan, T.; Abdulaal, R.; Otterbeck, P. Hydroxychloroquine and the Associated Risk of Arrhythmias. gcsp 2024, 2024. [Google Scholar] [CrossRef]
- Quiñones, M.E.; Joseph, J.K.; Dowell, S.; Moore, H.J.; Karasik, P.E.; Fonarow, G.C.; Fletcher, R.D.; Cheng, Y.; Zeng-Treitler, Q.; Arundel, C.; et al. Hydroxychloroquine and Risk of Long QT Syndrome in Rheumatoid Arthritis: A Veterans Cohort Study With Nineteen-Year Follow-Up. Arthritis Care Res (Hoboken) 2023, 75, 1571–1579. [Google Scholar] [CrossRef] [PubMed]
- Hoque, M.R.; Lu, L.; Daftarian, N.; Esdaile, J.M.; Xie, H.; Aviña-Zubieta, J.A. Risk of Arrhythmia Among New Users of Hydroxychloroquine in Rheumatoid Arthritis and Systemic Lupus Erythematosus: A Population-Based Study. Arthritis Rheumatol 2023, 75, 475–484. [Google Scholar] [CrossRef] [PubMed]
- Lo, C.-H.; Wei, J.C.-C.; Wang, Y.-H.; Tsai, C.-F.; Chan, K.-C.; Li, L.-C.; Lo, T.-H.; Su, C.-H. Hydroxychloroquine Does Not Increase the Risk of Cardiac Arrhythmia in Common Rheumatic Diseases: A Nationwide Population-Based Cohort Study. Front Immunol 2021, 12, 631869. [Google Scholar] [CrossRef]
- Eryavuz Onmaz, D.; Tezcan, D.; Abusoglu, S.; Yilmaz, S.; Yerlikaya, F.H.; Onmaz, M.; Abusoglu, G.; Unlu, A. Effects of Hydroxychloroquine and Its Metabolites in Patients with Connective Tissue Diseases. Inflammopharmacology 2021, 29, 1795–1805. [Google Scholar] [CrossRef]
- Zhao, C.; Yu, Y.; Yin, G.; Xu, C.; Wang, J.; Wang, L.; Zhao, G.; Ni, S.; Zhang, H.; Zhou, B.; et al. Sulfasalazine Promotes Ferroptosis through AKT-ERK1/2 and P53-SLC7A11 in Rheumatoid Arthritis. Inflammopharmacology 2024, 32, 1277–1294. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhang, X.; Zheng, C.; Gao, Z.; Jiang, X.; Bai, Y.; Meng, Y. Sulfasalazine Exacerbates Angiotensin II-Induced Cardiac Remodelling by Activating Akt Signal Pathway. Clin Exp Pharmacol Physiol 2022, 49, 776–783. [Google Scholar] [CrossRef]
- Tanaka, Y. Recent Progress in Treatments of Rheumatoid Arthritis: An Overview of Developments in Biologics and Small Molecules, and Remaining Unmet Needs. Rheumatology (Oxford) 2021, 60, vi12–vi20. [Google Scholar] [CrossRef] [PubMed]
- Aromolaran, A.S.; Srivastava, U.; Alí, A.; Chahine, M.; Lazaro, D.; El-Sherif, N.; Capecchi, P.L.; Laghi-Pasini, F.; Lazzerini, P.E.; Boutjdir, M. Interleukin-6 Inhibition of hERG Underlies Risk for Acquired Long QT in Cardiac and Systemic Inflammation. PLoS ONE 2018, 13, e0208321. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, H.; Kobayashi, Y.; Yokoe, I.; Kitamura, N.; Nishiwaki, A.; Takei, M.; Giles, J.T. Heart Rate–Corrected QT Interval Duration in Rheumatoid Arthritis and Its Reduction with Treatment with the Interleukin 6 Inhibitor Tocilizumab. The Journal of Rheumatology 2018, 45, 1620–1627. [Google Scholar] [CrossRef] [PubMed]
- Patil, V.B.; Lunge, S.B.; Doshi, B.R. Cardiac Side Effect of Rituximab. Indian Journal of Drugs in Dermatology 2020, 6, 49. [Google Scholar] [CrossRef]
- Dubois, E.A.; Cohen, A.F. Abatacept. Br J Clin Pharmacol 2009, 68, 480–481. [Google Scholar] [CrossRef]
- Yamada, Z.; Muraoka, S.; Kawazoe, M.; Hirose, W.; Kono, H.; Yasuda, S.; Sugihara, T.; Nanki, T. Long-Term Effects of Abatacept on Atherosclerosis and Arthritis in Older vs. Younger Patients with Rheumatoid Arthritis: 3-Year Results of a Prospective, Multicenter, Observational Study. Arthritis Research & Therapy 2024, 26, 87. [Google Scholar] [CrossRef]
- Sandra Deson Disease-Modifying Antirheumatic Drugs (Dmards): Revolutionizing Rheumatic Disease Management. International Journal of Clinical Rheumatology 2024, 19, 208–210.
- Manilall, A.; Mokotedi, L.; Gunter, S.; Le Roux, R.; Fourie, S.; Flanagan, C.A.; Millen, A.M.E. Inflammation-induced Left Ventricular Fibrosis Is Partially Mediated by Tumor Necrosis Factor-α. Physiological Reports 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Senel, S.; Cobankara, V.; Taskoylu, O.; Karasu, U.; Karapinar, H.; Erdis, E.; Evrengul, H.; Kaya, M.G. The Safety and Efficacy of Etanercept on Cardiac Functions and Lipid Profile in Patients with Active Rheumatoid Arthritis. J Investig Med 2012, 60, 62–65. [Google Scholar] [CrossRef]
- Ma, J.; Cai, J.; Chen, H.; Feng, Z.; Yang, G. Cardiovascular Adverse Events Associated with Tumor Necrosis Factor-Alpha Inhibitors: A Real-World Pharmacovigilance Analysis. J Atheroscler Thromb 2024, 31, 1733–1747. [Google Scholar] [CrossRef]
- Talotta, R.; Atzeni, F.; Batticciotto, A.; Ventura, D.; Sarzi-Puttini, P. Possible Relationship between Certolizumab Pegol and Arrhythmias: Report of Two Cases. Reumatismo 2016, 68, 104–108. [Google Scholar] [CrossRef]
- Weinblatt, M.E.; Westhovens, R.; Mendelsohn, A.M.; Kim, L.; Lo, K.H.; Sheng, S.; Noonan, L.; Lu, J.; Xu, Z.; Leu, J.; et al. Radiographic Benefit and Maintenance of Clinical Benefit with Intravenous Golimumab Therapy in Patients with Active Rheumatoid Arthritis despite Methotrexate Therapy: Results up to 1 Year of the Phase 3, Randomised, Multicentre, Double Blind, Placebo Controlled GO-FURTHER Trial. Annals of the Rheumatic Diseases 2014, 73, 2152–2159. [Google Scholar] [CrossRef]
- Smolen, J.S.; Kay, J.; Landewé, R.B.M.; Matteson, E.L.; Gaylis, N.; Wollenhaupt, J.; Murphy, F.T.; Zhou, Y.; Hsia, E.C.; Doyle, M.K. Golimumab in Patients with Active Rheumatoid Arthritis Who Have Previous Experience with Tumour Necrosis Factor Inhibitors: Results of a Long-Term Extension of the Randomised, Double-Blind, Placebo-Controlled GO-AFTER Study through Week 160. Ann Rheum Dis 2012, 71, 1671–1679. [Google Scholar] [CrossRef] [PubMed]
- Dijkshoorn, B.; Raadsen, R.; Nurmohamed, M.T. Cardiovascular Disease Risk in Rheumatoid Arthritis Anno 2022. J Clin Med 2022, 11, 2704. [Google Scholar] [CrossRef]
- Zhong, X.; Luo, J.; Huang, Y.; Wang, S.; Huang, Y. Cardiovascular Safety of Janus Kinase Inhibitors: A Pharmacovigilance Study from 2012–2023. PLoS One 2025, 20, e0322849. [Google Scholar] [CrossRef] [PubMed]
- Khosrow-Khavar, F.; Kim, S.C.; Lee, H.; Lee, S.B.; Desai, R.J. Tofacitinib and Risk of Cardiovascular Outcomes: Results from the Safety of TofAcitinib in Routine Care Patients with Rheumatoid Arthritis (STAR-RA) Study. Ann Rheum Dis 2022, 81, 798–804. [Google Scholar] [CrossRef] [PubMed]
- Sommer, S.L.; Kontaridis, M.I. Cardio-Rheumatology: The Cardiovascular, Pharmacological, and Surgical Risks Associated with Rheumatological Diseases in Women. Can J Physiol Pharmacol 2024, 102, 511–522. [Google Scholar] [CrossRef]
- Conaghan, P.G.; Mysler, E.; Tanaka, Y.; Da Silva-Tillmann, B.; Shaw, T.; Liu, J.; Ferguson, R.; Enejosa, J.V.; Cohen, S.; Nash, P.; et al. Upadacitinib in Rheumatoid Arthritis: A Benefit–Risk Assessment Across a Phase III Program. Drug Saf 2021, 44, 515–530. [Google Scholar] [CrossRef]
- Mariette, X.; Borchmann, S.; Aspeslagh, S.; Szekanecz, Z.; Charles-Schoeman, C.; Schreiber, S.; Choy, E.H.; Peyrin-Biroulet, L.; Schmalzing, M.; Tanaka, Y.; et al. Major Adverse Cardiovascular, Thromboembolic and Malignancy Events in the Filgotinib Rheumatoid Arthritis and Ulcerative Colitis Clinical Development Programmes. RMD Open 2025, 11, e005033. [Google Scholar] [CrossRef]
- Anderson, K.; Xin, Y.; Zheng, H.; Yun, C.; Kwan, E.; Qin, A.; Namour, F.; Kearney, B.P.; Mathias, A. Filgotinib, a JAK1 Inhibitor, Has No Effect on QT Interval in Healthy Subjects. Clinical Pharm in Drug Dev 2020, 9, 32–40. [Google Scholar] [CrossRef]
- Coburn, B.W.; Baker, J.F.; Hsu, J.Y.; Wu, Q.; Xie, F.; Curtis, J.R.; George, M.D. Association of Cardiovascular Outcomes With Low-Dose Glucocorticoid Prescription in Patients With Rheumatoid Arthritis. Arthritis & Rheumatology 2024, 76, 1585–1593. [Google Scholar] [CrossRef]
- Gawałko, M.; Peller, M.; Balsam, P.; Grabowski, M.; Kosiuk, J. Management of Cardiac Arrhythmias in Patients with Autoimmune Disease—Insights from EHRA Young Electrophysiologists. Pacing Clinical Electrophis 2020, 43, 1194–1198. [Google Scholar] [CrossRef]
- Tisdale, J.E.; Chung, M.K.; Campbell, K.B.; Hammadah, M.; Joglar, J.A.; Leclerc, J.; Rajagopalan, B. ; On behalf of the American Heart Association Clinical Pharmacology Committee of the Council on Clinical Cardiology and Council on Cardiovascular and Stroke Nursing Drug-Induced Arrhythmias: A Scientific Statement From the American Heart Association. Circulation 2020, 142. [Google Scholar] [CrossRef]
- Iwasaki, Y.; Sekiguchi, A.; Kato, T.; Yamashita, T. Glucocorticoid Induces Atrial Arrhythmogenesis via Modification of Ion Channel Gene Expression in Rats: Molecular Evidence for Stress-Induced Atrial Fibrillation. Int. Heart J. 2022, 63, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.-W.; Wang, X.-H.; Shi, J.; Yu, J.-G. Sinomenine in Cardio-Cerebrovascular Diseases: Potential Therapeutic Effects and Pharmacological Evidences. Front. Cardiovasc. Med. 2021, 8, 749113. [Google Scholar] [CrossRef] [PubMed]
- Saramet, E.E.; Negru, R.D.; Oancea, A.; Constantin, M.M.L.; Ancuta, C. 24 h Holter ECG Monitoring of Patients with Rheumatoid Arthritis-A Potential Role for a Precise Evaluation of QT Interval Duration and Associated Arrhythmic Complications. Diagnostics (Basel) 2022, 12, 638. [Google Scholar] [CrossRef] [PubMed]
- Adams, C. Autoimmunity and Biological Therapies in Cardiac Arrhythmias. MRAJ 2024, 12. [Google Scholar] [CrossRef]
- Tc, T.; Pe, N. Antiarrhythmic Agents: Drug Interactions of Clinical Significance. Drug safety 2000, 23. [Google Scholar] [CrossRef]
- C, C.; Me, G. Drug-Induced Lupus Erythematosus: Incidence, Management and Prevention. Drug safety 2011, 34. [Google Scholar] [CrossRef]
- Irizarry-Caro, J.A.; Carmona-Rivera, C.; Schwartz, D.M.; Khaznadar, S.S.; Kaplan, M.J.; Grayson, P.C. Brief Report: Drugs Implicated in Systemic Autoimmunity Modulate Neutrophil Extracellular Trap Formation. Arthritis Rheumatol 2018, 70, 468–474. [Google Scholar] [CrossRef]
- Upadhyaya, S.; Agarwal, M.; Upadhyaya, A.; Pathania, M.; Dhar, M. Rhupus Syndrome: A Diagnostic Dilemma. Cureus 2022, 14, e29018. [Google Scholar] [CrossRef]
- Jovanović, M.; Kovačević, M.; Vezmar-Kovačević, S.; Palibrk, I.; Bjelanović, J.; Miljković, B.; Vučićević, K. Lidocaine Clearance as Pharmacokinetic Parameter of Metabolic Hepatic Activity in Patients with Impaired Liver. J Med Biochem 2023, 42, 304–310. [Google Scholar] [CrossRef] [PubMed]
- Alhourani, N.; Wolfes, J.; Könemann, H.; Ellermann, C.; Frommeyer, G.; Güner, F.; Lange, P.S.; Reinke, F.; Köbe, J.; Eckardt, L. Relevance of Mexiletine in the Era of Evolving Antiarrhythmic Therapy of Ventricular Arrhythmias. Clin Res Cardiol 2024, 113, 791–800. [Google Scholar] [CrossRef] [PubMed]
- Johri, M.; Stewart, C. FLECAINIDE AS A FATAL CAUSE OF DIFFUSE ALVEOLAR DAMAGE. CHEST 2023, 164, A3276–A3277. [Google Scholar] [CrossRef]
- Chang, C.; Gershwin, M.E. Drug-Induced Lupus Erythematosus: Incidence, Management and Prevention. Drug Saf 2011, 34, 357–374. [Google Scholar] [CrossRef]
- Abuhelwa, A.Y.; Foster, D.J.R.; Manning-Bennett, A.; Sorich, M.J.; Proudman, S.; Wiese, M.D.; Hopkins, A.M. Concomitant Beta-Blocker Use Is Associated with a Reduced Rate of Remission in Patients with Rheumatoid Arthritis Treated with Disease-Modifying Anti-Rheumatic Drugs: A Post Hoc Multicohort Analysis. Ther Adv Musculoskelet Dis 2021, 13, 1759720X211009020. [Google Scholar] [CrossRef]
- Sills, J.M.; Bosco, L. Arthralgia Associated with Beta-Adrenergic Blockade. JAMA 1986, 255, 198–199. [Google Scholar] [CrossRef]
- Tatu, A.L.; Elisei, A.M.; Chioncel, V.; Miulescu, M.; Nwabudike, L.C. Immunologic Adverse Reactions of β-Blockers and the Skin. Exp Ther Med 2019, 18, 955–959. [Google Scholar] [CrossRef]
- Assad, A.; Alkhaldi, M.; Abrahamian, A.; Yonel, B.; Assaly, R.; Altorok, N. Diffuse Alveolar Hemorrhage Synergistically Induced by Amiodarone and Rheumatoid Arthritis. J Investig Med High Impact Case Rep 2023, 11, 23247096231196698. [Google Scholar] [CrossRef]
- Shenasa, F.; Shenasa, M. Dofetilide: Electrophysiologic Effect, Efficacy, and Safety in Patients with Cardiac Arrhythmias. Cardiac Electrophysiology Clinics 2016, 8, 423–436. [Google Scholar] [CrossRef]
- Fravel, M.A.; Ernst, M. Drug Interactions with Antihypertensives. Curr Hypertens Rep 2021, 23, 14. [Google Scholar] [CrossRef]
- Ye, Z.; Xia, H.; Hu, J.; Liu, Y.-N.; Wang, A.; Cai, J.-P.; Hu, G.-X.; Xu, R.-A. CYP3A4 and CYP2C19 Genetic Polymorphisms and Myricetin Interaction on Tofacitinib Metabolism. Biomed Pharmacother 2024, 175, 116421. [Google Scholar] [CrossRef] [PubMed]
- El-Mahdy, N.A.; Tadros, M.G.; El-Masry, T.A.; Binsaleh, A.Y.; Alsubaie, N.; Alrossies, A.; Abd Elhamid, M.I.; Osman, E.Y.; Shalaby, H.M.; Saif, D.S. Efficacy of the Cardiac Glycoside Digoxin as an Adjunct to csDMARDs in Rheumatoid Arthritis Patients: A Randomized, Double-Blind, Placebo-Controlled Trial. Front Pharmacol 2024, 15, 1445708. [Google Scholar] [CrossRef] [PubMed]
- Yoo, S.; Geist, G.E.; Pfenniger, A.; Rottmann, M.; Arora, R. Recent Advances in Gene Therapy for Atrial Fibrillation. Cardiovasc electrophysiol 2021, 32, 2854–2864. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Illustration of arrhythmias in RA-patients based on antibody profiles.
Figure 2.
The summary of cardiovascular effects and a possible correlation of arrhythmias with each conventional synthetic disease-modifying antirheumatic drugs (csDMARDs). AF: atrial fibrillation.
Figure 2.
The summary of cardiovascular effects and a possible correlation of arrhythmias with each conventional synthetic disease-modifying antirheumatic drugs (csDMARDs). AF: atrial fibrillation.
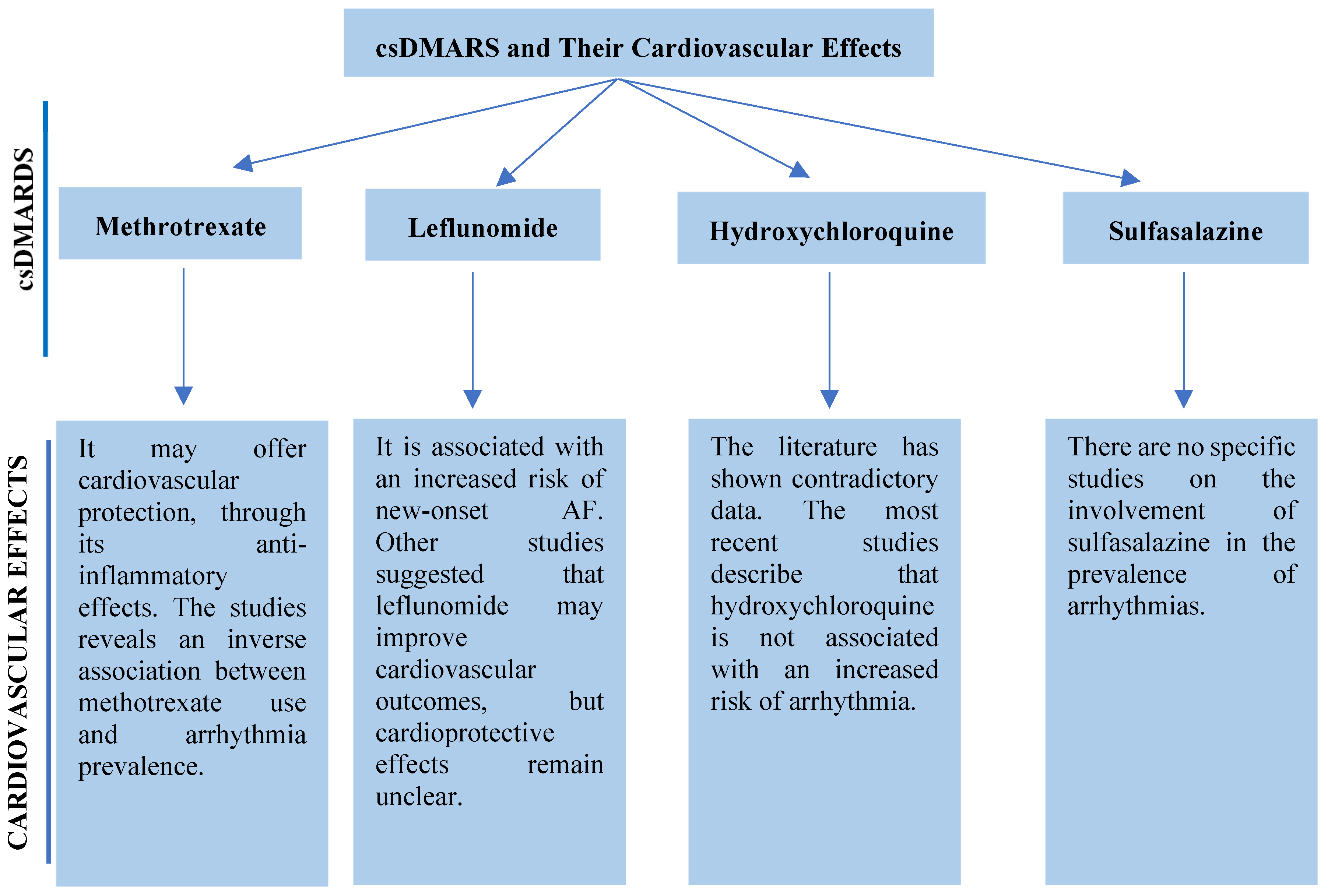
Figure 3.
A visual representation of the diagnosis algorithm for arrhythmias in RA. CRP: C reactive protein; ECG: electrocardiogram; ESR: erythrocyte sedimentation rate.
Figure 3.
A visual representation of the diagnosis algorithm for arrhythmias in RA. CRP: C reactive protein; ECG: electrocardiogram; ESR: erythrocyte sedimentation rate.
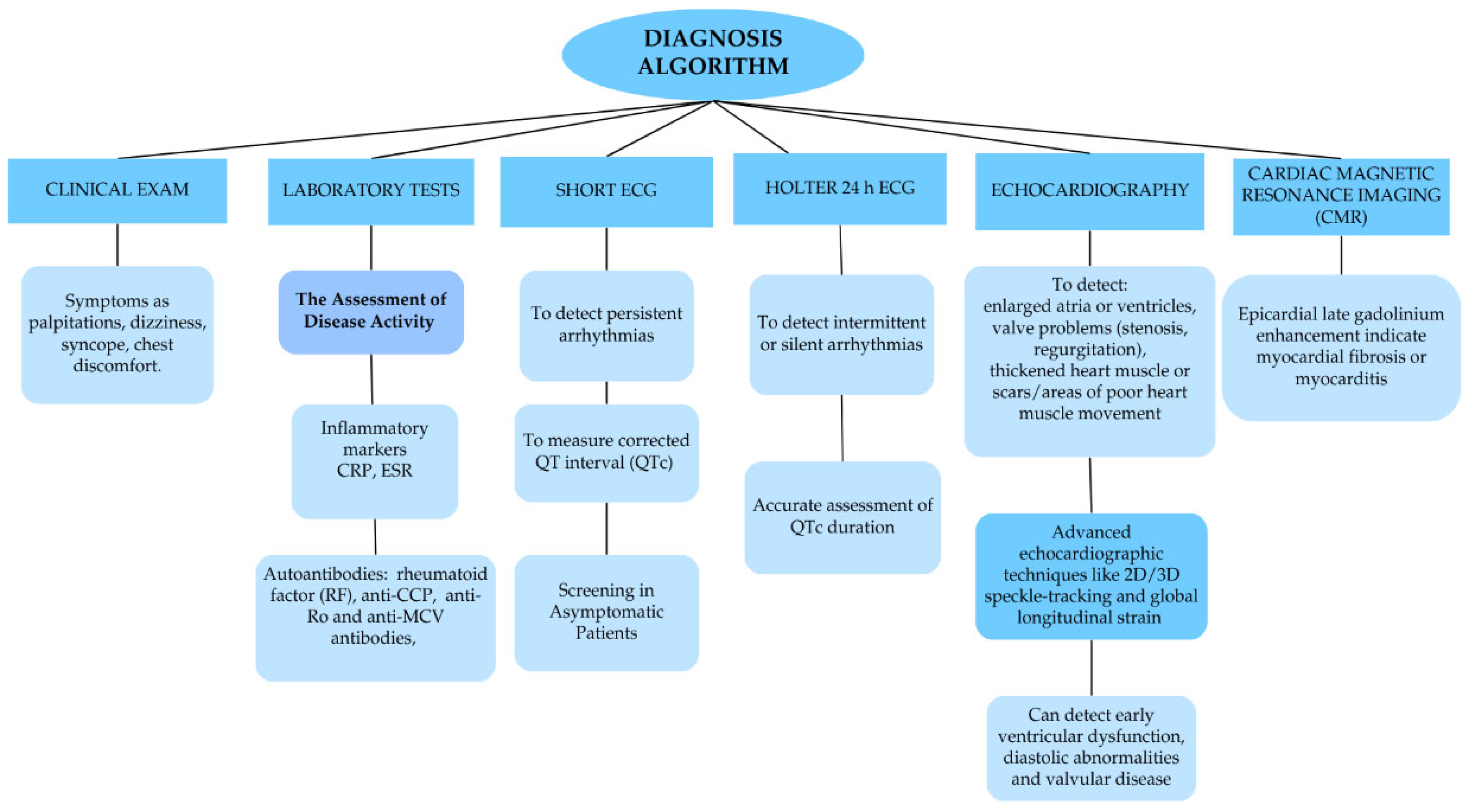

Table 1.
The most recent studies on the association between hydroxychloroquine (HCQ) and arrhythmias in patients with rheumatoid arthritis.
Table 1.
The most recent studies on the association between hydroxychloroquine (HCQ) and arrhythmias in patients with rheumatoid arthritis.
| Type of study | Year of publication | Number of patients |
Data and conclusions |
|---|---|---|---|
| Retrospective, propensity score–matched cohort safety study | 2023 | 8.852 | HCQ was not linked to an increased risk of long QT syndrome during the first two years of use. A higher risk emerged after five years, though the absolute risk remained low, with a minimal difference between those taking HCQ and those not. The risk decreased with longer follow-up, supporting HCQ's long-term safety in RA patients [35]. |
|
Retrospective cohort study |
2023 | 23.036 | Using data from 1996 to 2014, the cohort included 11.518 HCQ initiators and non-initiators. Over a follow-up of eight years, 1.610 arrhythmias occurred in the HCQ group and 1.646 in the non-HCQ group, with crude incidence rates of 17.5 and 18.1 per 1,000 person-years, respectively. HCQ initiation was not associated with an increased risk of arrhythmia [36]. |
|
Retrospective cohort study |
2021 | 3.575 | The use of HCQ was not associated with an increased risk of overall cardiac arrhythmia including ventricular arrhythmias, in patients with RA, systemic lupus erythematosus and Sjögren's syndrome, regardless of dose or treatment duration [37]. |
|
Observational, analytical study |
2021 | 70 | There was a positive correlation between blood HCQ and its metabolite levels with QTc interval, with average interval 390 ms [38]. |
Table 2.
The cardiovascular implications of these agents, along with their correlation with arrhythmic events. CV: cardiovascular; ELISA: enzyme-linked immunosorbent assay; HF: heart failure; JAK: Janus kinase; LV: left ventricular; MTX: methotrexate; PCR: protein chained reaction; RA: rheumatoid arthritis; TNF: tumor necrosis factor;.
Table 2.
The cardiovascular implications of these agents, along with their correlation with arrhythmic events. CV: cardiovascular; ELISA: enzyme-linked immunosorbent assay; HF: heart failure; JAK: Janus kinase; LV: left ventricular; MTX: methotrexate; PCR: protein chained reaction; RA: rheumatoid arthritis; TNF: tumor necrosis factor;.
| TNF-A inhibitors | Etanercept | Conclusions | Data and References |
| Cardioprotective in patients without HF. Reduce arterial stiffness, LV mass index, and overall CV morbidity in RA. | To investigate the effects of etanercept on cardiac functions were assigned seventy Sprague-Dawley rats with collagen-induced arthritis. Etanercept was administered for 6 weeks post-arthritis onset. LV structure and function were assessed by echocardiography, inflammatory markers by ELISA, and gene expression by quantitative PCR. The findings show that systemic inflammation contributes to LV fibrosis and extracellular matrix remodelling via increasing macrophage infiltration and local cardiac expression of pro-fibrotic genes. Etanercept partially inhibits collagen remodelling, but it does not stop diastolic dysfunction from starting, suggesting that other mechanisms besides TNF-α are involved [48]. Over the course of a 6-month follow-up with patients who had active disease, etanercept was demonstrated to be safe in terms of cardiac function and lipid profile and to be beneficial in improving RA parameters [49]. | ||
| Infliximab | The literature suggests that infliximab may be associated with life-threatening tachyarrhythmia and bradyarrhythmia. Improve arterial stiffness and vascular function in RA patients. | Infliximab and the risk of arrhythmias in RA have not been linked in any research published in the past five years. Older data and sporadic case reports without contemporary clinical study validation provide the only evidence of arrhythmogenicity. According to the literature, infliximab may be linked to bradyarrhythmia and tachyarrhythmia, which are potentially fatal. The total incidence of arrhythmias during infliximab infusion did not differ significantly from that of a placebo. Ventricular tachyarrhythmias with a recent onset, however, were more common and severe. Prolonged QT intervals and decreased heart rate variability were seen in affected patients, primarily those with RA [16]. | |
| Adalimumab | Inconclusive, one study showed increased thrombotic events, but no study data confirmed an arrhythmic risk. | A retrospective pharmacovigilance study revealed that adalimumab was the only TNF-α inhibitor associated with an elevated risk of cardiovascular adverse events (myocardial infarction, arterial thrombosis), whereas the other four TNF-α inhibitors did not show any risk effect [50]. | |
| Certolizumab pegol | Isolated cases report of arrhythmias, which may be associated with other CV risks. Favourable CV profile due to reduced systemic inflammation. | There are no specific studies or case reports in the last five years. A 2016 case report described two RA patients on certolizumab and MTX who developed serious arrhythmias: one with persistent AF resistant to cardioversion, and another with AFl managed by beta-blockers. Certolizumab pegol dosing intervals were extended, and MTX reduced in one case, without RA flare-ups [51]. | |
| Golimumab | Demonstrated cardioprotective effects in the GO-BEFORE and GO-FORWARD trials through improved cardiovascular markers. However, caution is advised in patients with HF. | A 2014 study evaluating intravenous golimumab (2 mg/kg) plus MTX over 52 weeks in active RA reported one case of AF between weeks 24 and 52 [52]. Across multiple long-term extension studies (GO-AFTER, GO-MORE, GO-FURTHER), no further increase in arrhythmia incidence was observed beyond the isolated cases previously reported [53]. | |
| Interleukine-6 Inhibitors | Tocilizumab | Suggest a potential antiarrhythmic effect, normalise the QTc interval by dampening systemic inflammation. | There are not recent data, a 2018 study of 94 RA and 42 non-RA controls patients, suggest a potential antiarrhythmic effect of IL-6 inhibition and reinforce the link between RA-related inflammation and elevated cardiovascular risk. The observed QTc normalisation with tocilizumab and its correlation with CRP reduction support the role of systemic inflammation in cardiac repolarisation abnormalities in RA [43]. |
| CD-20 monoclonal antibody | Rituximab | The literature suggests that Rituximab may be associated with arrhythmias. | Cardiovascular toxicity, including cardiac arrhythmias, has been reported in 8% of patients treated with rituximab. These arrhythmias encompass monomorphic and polymorphic ventricular tachycardia, supraventricular tachycardia, trigeminy, bradycardia, AF as well as nonspecific dysrhythmias and tachycardia. It is hypothesised that the CD20 antigen may influence calcium ion channel function [44]. |
| Selective T-cell co-stimulation inhibitor | Abatacept | Most available cardiovascular data pertain to HF arterial stiffness, lipid profiles, and major adverse cardiovascular events, rather than to cardiac rhythm disorders. | It may slow atherosclerosis progression and benefit high-risk patients [46]. Hypertension has been reported as a possible side effect in 1–10% of cases. However, the cardiovascular risk reduction associated with the anti-inflammatory effect of abatacept appears to remain unaffected [54]. |
| JAKinhibitors | Tofacitinib | FAERS data suggest JAK inhibitors may raise cardiovascular AE risk, particularly in older patients or those with pre-existing heart conditions. The literature does not provide evidence of a direct link between JAK inhibitors and specific arrhythmias. | Tofacitinib demonstrated signals for embolic/thrombotic events and hypertension [55]. The most recent study, STAR-RA, does not provide evidence of a direct link between tofacitinib and specific arrhythmias. The available data focus solely on major adverse cardiovascular events (including myocardial infarction and stroke), not on cardiac rhythm disturbances [56]. |
| Baricitinib | Baricitinib showed stronger associations with embolic and thrombotic events, torsade de pointes/QT prolongation pulmonary hypertension, ischemic heart disease, cardiac arrhythmias and cardiac failure [55]. Events of arrhythmia, HF and sudden cardiac death have been reported in post-marketing settings [57]. | ||
| Upadacitinib | Upadacitinib was associated with pulmonary hypertension, embolic and thrombotic events, ischemic heart disease, torsade de pointes/QT prolongation, HF,cardiac arrhythmias and cardiomyopathy [55]. It has shown an arrhythmia signal in spontaneous reporting systems, but clinical studies have not confirmed or quantified this risk [58]. | ||
| Filgotinib | Integrated analyses over >12.500 patient, with years of exposure confirm low rates of major adverse cardiovascular events and venous thromboembolism, with no evidence of rhythm-related cardiac events [59]. A 2019 study proved that there were no clinically relevant relationships between QTc interval and plasma concentrations of filgotinib or its major metabolite [60]. |
Table 3.
Side effects of anti-arrhythmic drugs and safety for RA patients. AF: atrial fibrillation; APD: action potential duration; AV: atrio-ventricular; JAK: Janus kinase; MI: myocardial infarction; PSVT: paroxysmal supraventricular tachycardia; SVT: supraventricular tachycardia; VF: ventricular fibrillation; VT: ventricular tachycardia; WPW syndrome: Wolf-Parkinson-White Syndrome;.
Table 3.
Side effects of anti-arrhythmic drugs and safety for RA patients. AF: atrial fibrillation; APD: action potential duration; AV: atrio-ventricular; JAK: Janus kinase; MI: myocardial infarction; PSVT: paroxysmal supraventricular tachycardia; SVT: supraventricular tachycardia; VF: ventricular fibrillation; VT: ventricular tachycardia; WPW syndrome: Wolf-Parkinson-White Syndrome;.
| Class | Mechanism of Action/ Indications | Examples | Drug safety for RA-patients | |
| Class I (Sodium (Na⁺) channels) | ||||
| Ia | Slows conduction, prolongs repolarization Used for AF, VT, WPW syndrome. |
Quinidine, Procainamide, Disopyramide |
Due to the potential of quinidine to cause a lupus-like syndrome, the use should be evaluated [69]. In 2018, Irizarry-Caro reported that procainamide is a lupus-inducing drug, promoting NET formation via neutrophil muscarinic receptor activation and calcium flux, highlighting innate immune involvement in DILE [70]. Rhupus syndrome, an overlap of RA and systemic lupus erythematosus, occurs in approximately 0.01–2% of rheumatic disease cases and the use of lupus-inducing drug need to be restricted [71]. The literature dose note provide data about autoimmunity induced by disopyramide or side effects that can alter the RA patient’s health status. | |
| Ib | Shortens repolarization. Used for VT (especially post-MI), not for atrial arrhythmias. |
Lidocaine, Mexiletine |
Lidocaine is metabolized in the liver. RA patients often use hepatotoxic drugs such as MTX, which can impair liver function and reduce lidocaine clearance, increasing the risk of toxicity [72]. Mexiletine can present diverse side effects, mostly related to the gastrointestinal tract and nervous system, but also hematological. The most prevalent symptoms are nausea, abdominal pain/discomfort, tremors, headaches, dizziness and thrombocytopenia, which can emphasise the existing health problems [73]. | |
| Ic | Slows conduction, no effect on repolarization. Used for AF, SVT. |
Flecainide, Propafenone | Patients with RA are at elevated risk for interstitial lung disease. Flecainide has been linked to potentially drug-induced interstitial pneumonitis or diffuse alveolar damage [74]. Propafenone is recognized as a very low-risk drug for inducing drug-induced lupus ,with < 0.1% incidence at clinically used doses [75]. | |
| Class II (β-adrenergic receptors) | ||||
| Beta-blockade → ↓ sympathetic tone, ↓ AV conduction. Used for AF (rate control), SVT, ventricular ectopy, post-MI. |
Metoprolol, Atenolol, Esmolol |
The literature presents beta-blocker use was independently associated with a lower likelihood of achieving remission [76]. In 1986, FDA reports described several cases of joint pain linked to metoprolol, which disappeared within a few days after the drug was stopped [77]. Atenolol can cause vasculitis and drug-induced lupus erythematosus [78]. There are no studies about Esmolol linked to negative effects on RA disease activity. | ||
| Class III (Potassium (K⁺) channels) | ||||
| Prolongs repolarization (↑ APD & QT interval), Used for AF, VT, VF |
Amiodarone, Sotalol, Dofetilide, Ibutilide |
Patients with preexisting pulmonary disease (RA-associated interstitial lung disease) are particularly vulnerable to amiodarone. The literature presents cases of diffuse alveolar hemorrhage syndrome induced [79]. Sotalol can induce vasculitis [78]. Dofetilide is primarily excreted through the kidneys, with about 80% eliminated renally, while approximately 20% to 30% is metabolized in the liver via the CYP3A4 enzyme pathway. Therefore, dose adjustments are necessary for RA patients with impaired kidney function [80]. There are no studies about Ibutilide linked to negative effects on RA disease activity. | ||
| Class IV (Calcium (Ca²⁺) channels) | ||||
| ↓ AV node conduction & automaticity. Used for AF (rate control), SVT. |
Verapamil, Diltiazem |
Calcium channel blockers, specifically diltiazem and verapamil, have been well established as strong inhibitors of CYP3A4, with most major drug interactions linked to these two medications [81]. Tofacitinib, a JAK inhibitor, is significantly metabolized by CYP3A4. In this case the association need to be evaluated [82]. | ||
| Others/ Various targets | ||||
| Mixed or unique mechanisms Used for PSVT (adenosine), rate control in AF (digoxin), sinus tachycardia. |
Adenosine, Digoxin, Ivabradine |
Digoxin was well tolerated in RA patients and demonstrated significant immunomodulatory and anti-inflammatory effects. Additionally, it may possess anti-angiogenic properties, suggesting that it could serve as an effective adjunct to csDMARDs in the treatment of RA [83]. There are no studies about Adenosine or Ivabradine linked to negative effects on RA disease activity. | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



