Submitted:
28 July 2025
Posted:
06 August 2025
You are already at the latest version
Abstract
Background : Human nasal myiasis, primarily is a rare zoonotic infection caused by Oestrus ovis, with a non-specific clinical presentation that can mimic more common conditions, such as allergic rhinitis. Objective : To report a series of nasal myiasis cases in immunocompetent individuals, emphasizing the clinical and paraclinical features that facilitate differential diagnosis from allergic rhinitis and enable early treatment. Methods : We conducted a retrospective study including cases of nasal myiasis diagnosed and managed at the ENT department of the Military Hospital of Tunis over 18-year period (2007–2025). Demographic, clinical, diagnostic, and therapeutic data were analyzed. Results : The mean patient age was 43.2 years (range: 18–70), with a female predominance (sex ratio 0.4). Six patients (43%) originated from rural areas. All presented with acute-onset rhinological symptoms (intense nasal pruritus, sneezing, obstruction, rhinorrhea, and headaches), initially suggestive of allergic rhinitis and partially responsive to antihistamines. Otalgia was noted in 3 cases (21%). Nasal endoscopy revealed live larvae in 11 patients (79%). Two patients consulted after spontaneous larval expulsion, and one had both expelled and retained larvae. Skin prick tests were negative in all cases. Facial CT scans (performed in 36%) were unremarkable. Parasitological analysis confirmed Oestrus ovis in 10 cases (71%). Treatment involved nasal irrigation with saline and an anthelmintic, along with corticosteroids and antihistamines, leading to symptom resolution within an average of 4 days. Conclusion : Nasal myiasis should be considered in cases of atypical or treatment-resistant rhinitis, even in immunocompetent individuals. Nasal endoscopy is crucial for diagnosis. Awareness of this condition is essential to prevent misdiagnosis and ensure prompt, effective management.

Keywords:
Introduction
Methods
Results
Demographic and Epidemiological Characteristics
Clinical Presentation and Initial Diagnosis
ENT Examination and Nasal Endoscopy
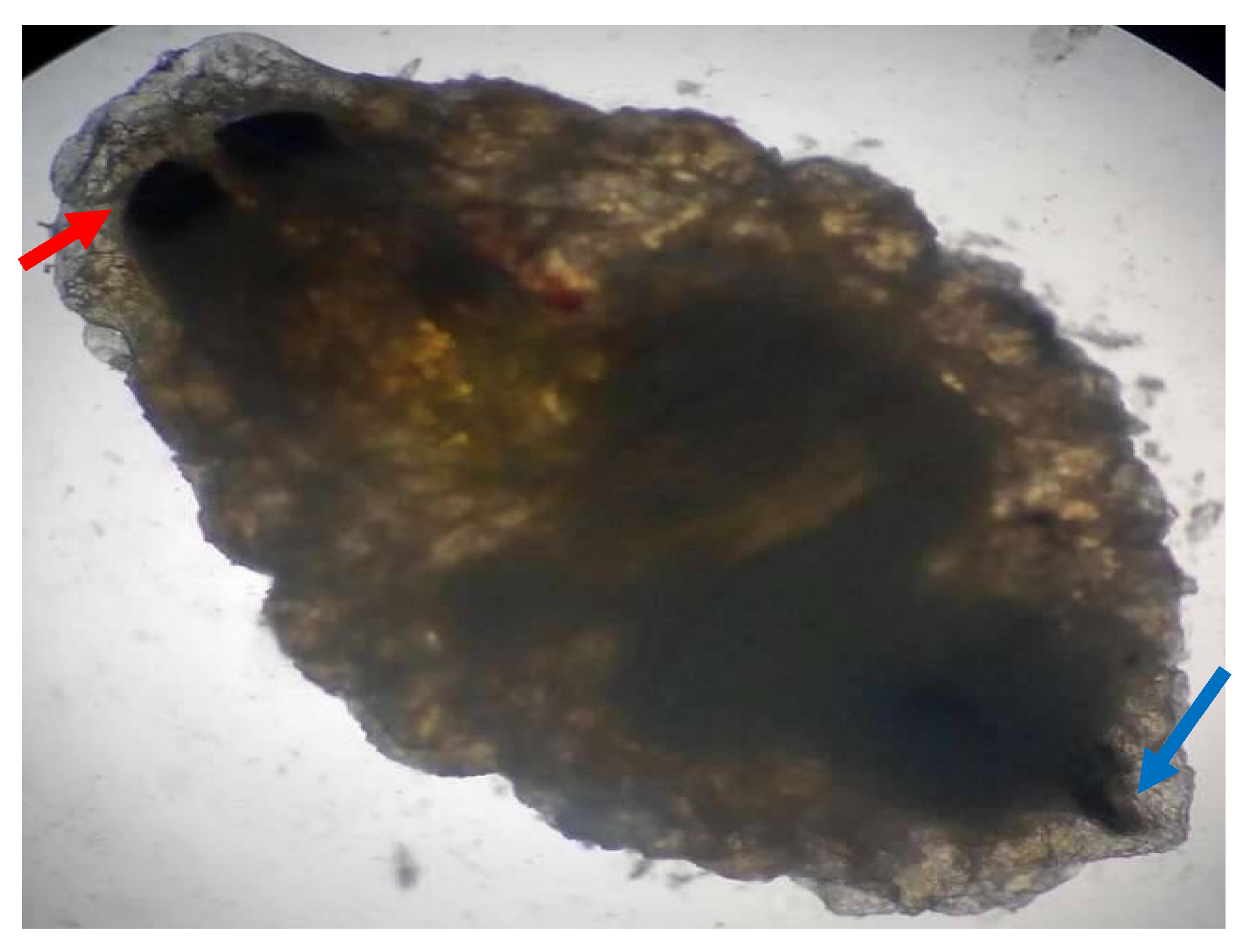
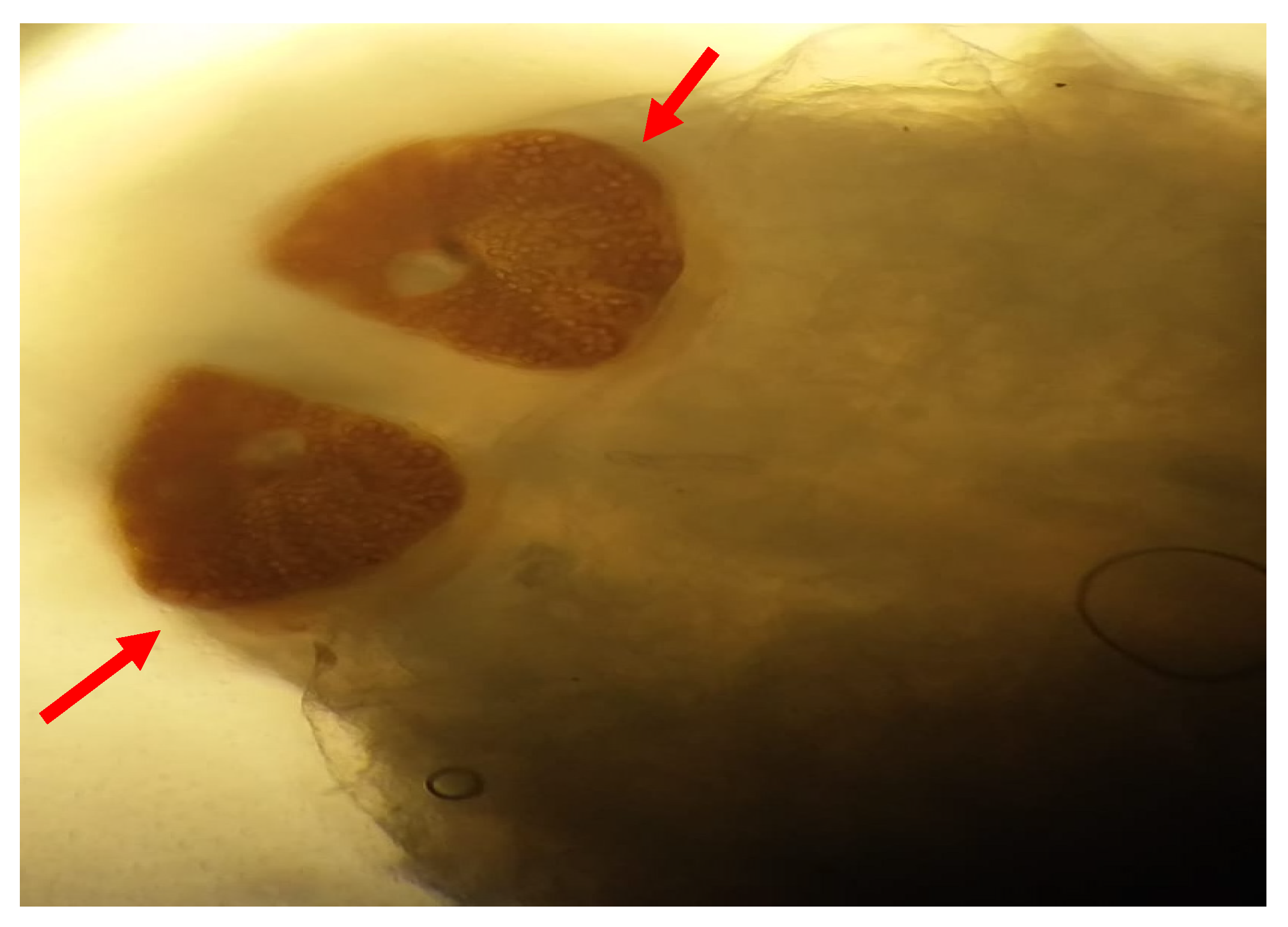
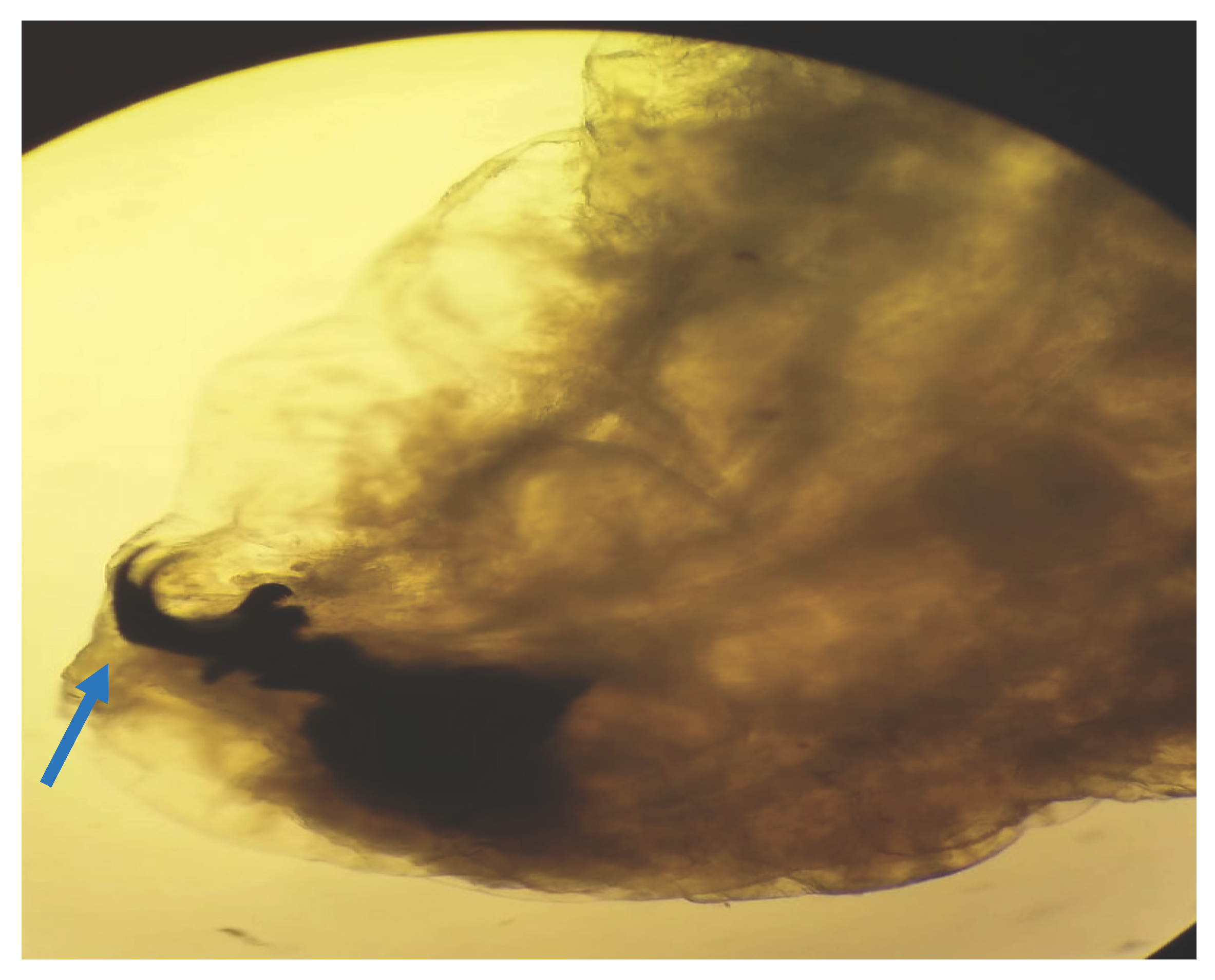
3.4. Complementary Examinations and Parasite Identification
Treatment and Outcome
Discussion
4.1. The Mimicry of Allergic Rhinitis: A Diagnostic Challenge
4.2. Clinical Clues and Diagnostic Modalities
4.3. Epidemiology and Predisposing Factors
4.4. Treatment and Outcomes
4.5. Limitations
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflict of interest statement
References
- Delhaes L, Bourel B, Pinatel F, Cailliez JC, Gosset D, Camus D, et al. Myiase nasale humaine à Œstrus ovis. Parasite. 1 déc 2001;8(4):289-96.
- Ravichandran K, Padmanabhan K, Thomas SK, S DP, Liji N. Unusual Presentation of Nasal Myiasis in Immunocompetent Young Individual: Case Report. Indian J Otolaryngol Head Neck Surg. févr 2025;77(2):1147-51. [CrossRef]
- Einer H, Ellegård E. Nasal myiasis by Oestrus ovis second stage larva in an immunocompetent man: case report and literature review. J Laryngol Otol. juill 2011;125(7):745-6. [CrossRef]
- Sante Fernández L, Hernández-Porto M, Tinguaro V, Lecuona Fernández M. Ophthalmomyiasis and nasal myiasis by Oestrus ovis in a patient from the Canary Islands with uncommon epidemiological characteristics. Enferm Infecc Microbiol Clin. 2017;35(7):461-2.
- Gupta SK, Nema HV. Rhino-orbital-myiasis. The Journal of Laryngology & Otology. avr 1970;84(4):453-5.
- Soni NK. Endoscopy in nasal myiasis. Trop Doct. oct 2000;30(4):225-7. [CrossRef]
- Tyagi AK, Suji PS, Kumar A, Varshney S, Mohanty A, Gupta P. First Report on Concomitant Infection of Nasal Myiasis and Trichosporonosis in an Uncontrolled Diabetic Patient: Case Report. Indian J Otolaryngol Head Neck Surg. oct 2022;74(Suppl 2):810-2. [CrossRef]
- Savaş N, Aykur M. Oral and Nasal Myiasis in Two Patients Hospitalized in the Intensive Care Unit: Diagnosis and Clinical Significance of Cases. Indian J Otolaryngol Head Neck Surg. oct 2024;76(5):4677-81. [CrossRef]
- Francesconi F, Lupi O. Myiasis. Clin Microbiol Rev. janv 2012;25(1):79-105.
- Sayeed A, Ahmed A, Sharma SC, Hasan SA. Ivermectin: A Novel Method of Treatment of Nasal and Nasopharyngeal Myiasis. Indian J Otolaryngol Head Neck Surg. nov 2019;71(Suppl 3):2019-24. [CrossRef]


| Patients | Age | gender | antecedents |
Origin | Job | Symptoms | Delay to consult | Initial treatment | Examination | Larva identification |
|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 24 | F | 0 | U | Ingeneer | Pruritus Rhinorrhea | 3 days | Irrigation corticoid anti histamine |
Larva moving | Oestrus Ovis |
| 2 | 69 | F | Gastric ulcer | U | 0 | Pruritus | 6 days | Irrigation Antibiotic | Larva moving | Oestrus Ovis |
| 3 | 52 | F | HTA | R | Factory | Rhinorrhea larva expulsion pharyngitis |
6 days | Irrigation Albendazole antihistamine |
Larva moving | Oestrus Ovis |
| 4 | 38 | F | Anti-synthetase syndrome immunosuppressive therapy and corticoids. |
U | Airport | Rhinorrhea larva expulsion |
3 days | Irrigation | Congestif rhinitis | Oestrus Ovis |
| 5 | 50 | F | 0 | Airport | Pharyngitis rhinorrhea larva expulsion |
10 days | Irrigation | Rhino-pharyngitis | Oestrus Ovis | |
| 6 | 43 | H | 0 | U | Compagny manager | Nasal obstruction Pruritus | 15 days | Irrigation Albendazole antihistamine |
Larva moving | Oestrus Ovis |
| 7 | 24 | H | 0 | R | Student | Nasal obstruction Pruritus | 10 days | Irrigation Zzole Antibiotic corticoid anti histamine |
Larva moving | - |
| 8 | 70 | F | Hypertension Diabetes | R | 0 | Nasal and pharyngeal Pruritus | 6 days | Irrigation Zzole antihistamine |
Larva moving | - |
| 9 | 57 | F | 0 | R | 0 | Nasal pruritus | 11 days | Irrigation Zzole | Larva moving | Oestrus Ovis |
| 10 | 44 | F | 0 | R | 0 | Pruritus | 5 days | Irrigation Zzole antihistamine |
Larva moving | Oestrus Ovis |
| 11 | 18 | F | 0 | U | Student | Pruritus Otitis |
8 days | Irrigation Zzole antibiotic corticoid antihistamine |
Larva moving | Oestrus Ovis |
| 12 | 29 | H | 0 | U | Restaurant agent | Pruritus Otitis Sinusitis |
6 days | Irrigation Corticoid Albendazole Antibiotic |
Larva moving | Oestrus Ovis |
| 13 | 52 | H | 0 | R | Farmer | Nasal obstruction Pruritus | 7 days | Irrigation Corticoid antibiotic antihistamine |
Larva moving | - |
| 14 | 36 | F | 0 | U | Esthetician | Pruritus Hyposmia | 15 days | Irrigation Corticoid Albendazole Antibiotic |
Larva moving | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



