
Submitted:
04 August 2025
Posted:
04 August 2025
You are already at the latest version
Abstract
Background: Early-life sensitization to house dust mites (HDMs) is a recognized risk factor for adverse respiratory allergic outcomes. Methods: We investigated the clinical characteristics of infants under two years of age who visited our allergy clinic for evaluation with detectable HDM-specific IgE (sIgE) and compared them to HDM-sIgE–negative infants. Results: Among 1,793 infants tested for HDM sIgE, 96 (5.4%) demonstrated sensitization. In the HDM-positive cohort, the prevalence of atopic dermatitis was 74.0% (90.9% among those <12 months), food allergy 57.3% (100% among those <12 months), egg white sensitization 71.9% (90.9% among those <12 months), and cow’s milk sensitization 56.3% (81.8% among those <12 months). Atopic dermatitis, food allergy, ≥4 wheezing episodes, physician-diagnosed asthma, allergic rhinitis, egg white sensitization, cow’s milk sensitization, and sensitization to three or more food allergens were significantly more common in the HDM-positive group compared with the HDM-negative group. Significant correlations were observed between HDM sIgE and total IgE levels, as well as between HDM sIgE and egg white sIgE levels. Overall, HDM sensitization in infants was most frequently accompanied by atopic dermatitis and egg white sensitization. Conclusions: These findings suggest that early HDM sensitization should be closely monitored, particularly in infants with atopic dermatitis and food allergies who exhibit elevated total IgE and egg white sIgE levels.
Keywords:
allergens
; house dust mites
; immunoglobulin E
; infants
1. Introduction
House dust mites (HDMs) were first implicated as a source of allergens in 1928 and have been recognized as a major etiological factor in allergic diseases since 1968 [1,2]. Among indoor allergens, HDMs are the most prevalent triggers of allergic sensitization, particularly in respiratory disorders. Two species, Dermatophagoides farinae (D. farinae) and Dermatophagoides pteronyssinus (D. pteronyssinus), collectively account for approximately 90% of the global HDM population. The relative distribution of these species varies geographically. In Korea, HDMs are predominantly composed of D. farinae (approximately 65%), followed by D. pteronyssinus (around 21%) [3]. Correspondingly, sensitization to D. farinae is generally more frequent than to D. pteronyssinus, with this disparity being particularly pronounced in pediatric populations, where sensitization to D. farinae typically precedes that to D. pteronyssinus [4,5,6].
Allergic diseases in children often follow a characteristic trajectory known as the “allergic march.” In this process, sensitization to food allergens typically precedes the onset of atopic dermatitis, followed by the manifestation of clinical food allergy symptoms. As children reach preschool age, sensitization to inhalant allergens, particularly HDMs, becomes more prominent than sensitization to food allergens and frequently leads to respiratory allergic diseases, including allergic rhinitis and asthma [7,8,9]. In Korea, the prevalence of HDM sensitization among patients with atopic dermatitis has been reported to range from 27.9% to 68.8%, while 40% to 60% of patients with respiratory allergies, allergic rhinitis, or asthma demonstrate HDM sensitivity [5]. More than half of asthmatic patients are sensitized to HDMs, and both the incidence and severity of asthma are strongly associated with HDM allergy [10,11,12].
Early-life exposure to HDMs plays a pivotal role in the development of HDM sensitization and infantile asthma [13,14]. Furthermore, early HDM sensitization has been linked to impaired lung function and is considered a significant risk factor for unfavorable respiratory allergic outcomes [15,16]. Young children with HDM sensitization and allergic diseases require timely diagnosis and early intervention to improve long-term prognosis. Therefore, understanding the clinical characteristics of infants with early HDM sensitization is crucial.
This study aimed to characterize infants under 24 months of age with documented HDM sensitization and to compare their clinical features with those of non-sensitized infants. The introduction should briefly place the study in a broad context and highlight why it is important. It should define the purpose of the work and its significance. The current state of the research field should be carefully reviewed and key publications cited. Please highlight controversial and diverging hypotheses when necessary. Finally, briefly mention the main aim of the work and highlight the principal conclusions. As far as possible, please keep the introduction comprehensible to scientists outside your particular field of research. References should be numbered in order of appearance and indicated by a numeral or numerals in square brackets—e.g., [1] or [2,3], or [4,5,6]. See the end of the document for further details on references.
2. Materials and Methods
2.1. Study Population
This study included infants under 24 months of age who visited our pediatric allergy clinic for evaluation of allergic diseases, including atopic dermatitis, allergic rhinitis, asthma, recurrent wheezing, and food allergies, and who underwent testing for HDM–specific immunoglobulin E (sIgE). Infants in the HDM-positive (HDM [+]) group were defined as those with a D. farinae sIgE level ≥0.35 kU/L, whereas the HDM-negative (HDM [–]) control group consisted of infants with negative D. farinae sIgE results. Controls were individually matched 1:1 to cases by age and sex. D. farinae was selected as the representative HDM allergen because it is the earliest and most frequently recognized HDM sensitizer among Korean children.
2.2. Methods
Data were collected retrospectively from electronic medical records. Information on physician-diagnosed allergic diseases was obtained, and results of the ImmunoCAP assay (Thermo Fisher Scientific, Uppsala, Sweden) were analyzed, including sIgE levels to D. farinae, egg white, and cow’s milk, as well as total IgE levels. We determined the proportion of infants sensitized to D. farinae among all participants under 24 months and among those under 12 months of age. Clinical characteristics and allergic disease patterns were assessed in the HDM (+) group. The HDM (–) control group was selected by 1:1 matching for age and sex, enabling comparative analyses between the two groups. ImmunoCAP results and clinical manifestations were compared across groups.
2.3. Statistical Analysis
Categorical variables were summarized as n (%), and continuous variables as mean ± standard deviation (SD). Differences between the HDM (+) and HDM (–) groups were evaluated using the Wilcoxon signed-rank test for continuous variables and McNemar’s test for categorical variables. Correlations between immunologic test results were analyzed using Spearman’s rank correlation coefficient. All P-values were two-sided, with statistical significance defined as P < 0.05. Analyses were performed using R version 4.5.0 (R Foundation for Statistical Computing, Vienna, Austria; https://www.R-project.org/).
Ethical Considerations
The present study protocol was approved by the Research Ethics Committee of Hallym University Dongtan Sacred Heart Hospital prior to the initiation of the study (approval no. 2021-08-008).
3. Results
3.1. Clinical Characteristics of Infants Sensitized to HDMs
Among 1,793 infants under 24 months of age included in the study, 96 (5.4%) demonstrated sensitization to house dust mites (HDMs). Of the 739 infants younger than 12 months, 11 (1.5%) were sensitized, whereas 85 (8.1%) of 1,054 children aged 12–24 months showed sensitization. Among infants with HDM sensitization, 74.0% had physician-diagnosed atopic dermatitis and 57.3% had documented food allergies. Additionally, 45.8% experienced recurrent wheezing episodes (≥4) at the time of examination. In a subset analysis of infants under 12 months, 90.9% had atopic dermatitis, all (100%) had food allergies, and 36.4% exhibited recurrent wheezing (Table 1).
3.2. Laboratory Findings in HDM-Sensitized Infants
Among HDM-sensitized infants under 24 months of age, 71.9% were co-sensitized to egg white, 56.3% to cow’s milk, and 50% to three or more food allergens. In the subgroup younger than 12 months, the rates of co-sensitization were 90.9% for egg white, 81.8% for cow’s milk, and 72.7% for multiple food allergens (Table 2). Three infants reached the maximum measurable D. farinae sIgE level of 100 kU/L. One of these patients, aged 10 months, had a strong family history of allergic diseases and presented with multiple allergic conditions, including atopic dermatitis, food allergy, infantile asthma, and allergic rhinitis.
3.3. Comparison Between the HDM (+) and HDM (–) Groups
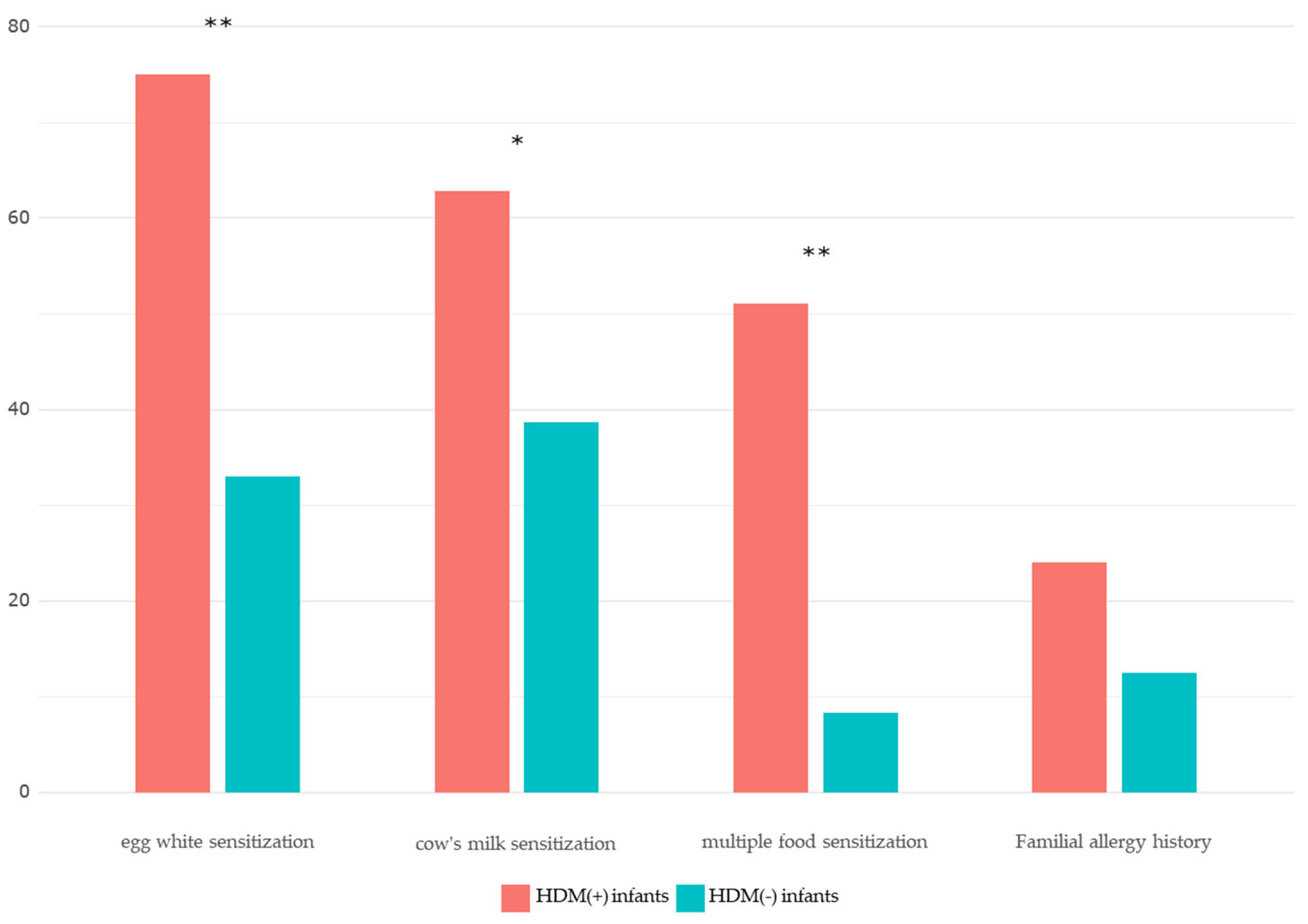
The prevalence of atopic dermatitis (74.0% vs. 21.9%, P<0.001) and food allergies (57.3% vs. 15.6%, P<0.001) was significantly higher in the HDM (+) group compared with the HDM (–) group. There was no statistically significant difference in the occurrence of anaphylaxis between the two groups (10.4% vs. 3.1%, P=0.096). Recurrent wheezing (≥4 episodes) (32.3% vs. 2.1%, P<0.001), physician-diagnosed asthma (24.2% vs. 1.0%, P<0.001), and allergic rhinitis (31.2% vs. 5.2%, P<0.001) were significantly more frequent among HDM-sensitized infants, whereas urticaria did not differ between groups. Egg white sensitization was observed in 75.0% of the HDM (+) group compared with 33.0% of the HDM (–) group (P<0.001), and cow’s milk sensitization was also significantly higher (62.8% vs. 38.7%, P=0.007). Multiple food sensitizations (≥3 allergens) were markedly more common in the HDM (+) group (51.1% vs. 8.3%, P<0.001) (Table 3).
Results of the Wilcoxon signed-rank test indicated significant differences in egg white and cow’s milk sIgE levels between groups. Total IgE values were log-transformed to approximate a normal distribution before analysis using paired t-tests, revealing significantly higher total IgE levels in HDM-sensitized infants. Mean egg white sIgE levels were 16.13 kU/L in the HDM (+) group versus 1.15 kU/L in the HDM (–) group, and mean cow’s milk sIgE levels were 6.08 kU/L versus 0.67 kU/L, respectively (Table 4). Within the HDM (+) group, D. farinae sIgE levels showed moderate positive correlations with total IgE (r=0.326, P=0.002) and egg white sIgE (r=0.312, P=0.002), and a weak but statistically significant correlation with cow’s milk sIgE (r=0.215, P=0.047) (Table 5).
Because the variables were not normally distributed, Spearman’s rank correlation test was used to assess relationships between HDM sIgE and total IgE, egg white sIgE, and cow’s milk sIgE. Correlation coefficients (ρ) and corresponding p-values are presented in this table.
Figure 1.
Comparison of allergic diseases between the HDM(+) and HDM(−) groups (**P < 0.01, ***P < 0.001).
Figure 1.
Comparison of allergic diseases between the HDM(+) and HDM(−) groups (**P < 0.01, ***P < 0.001).
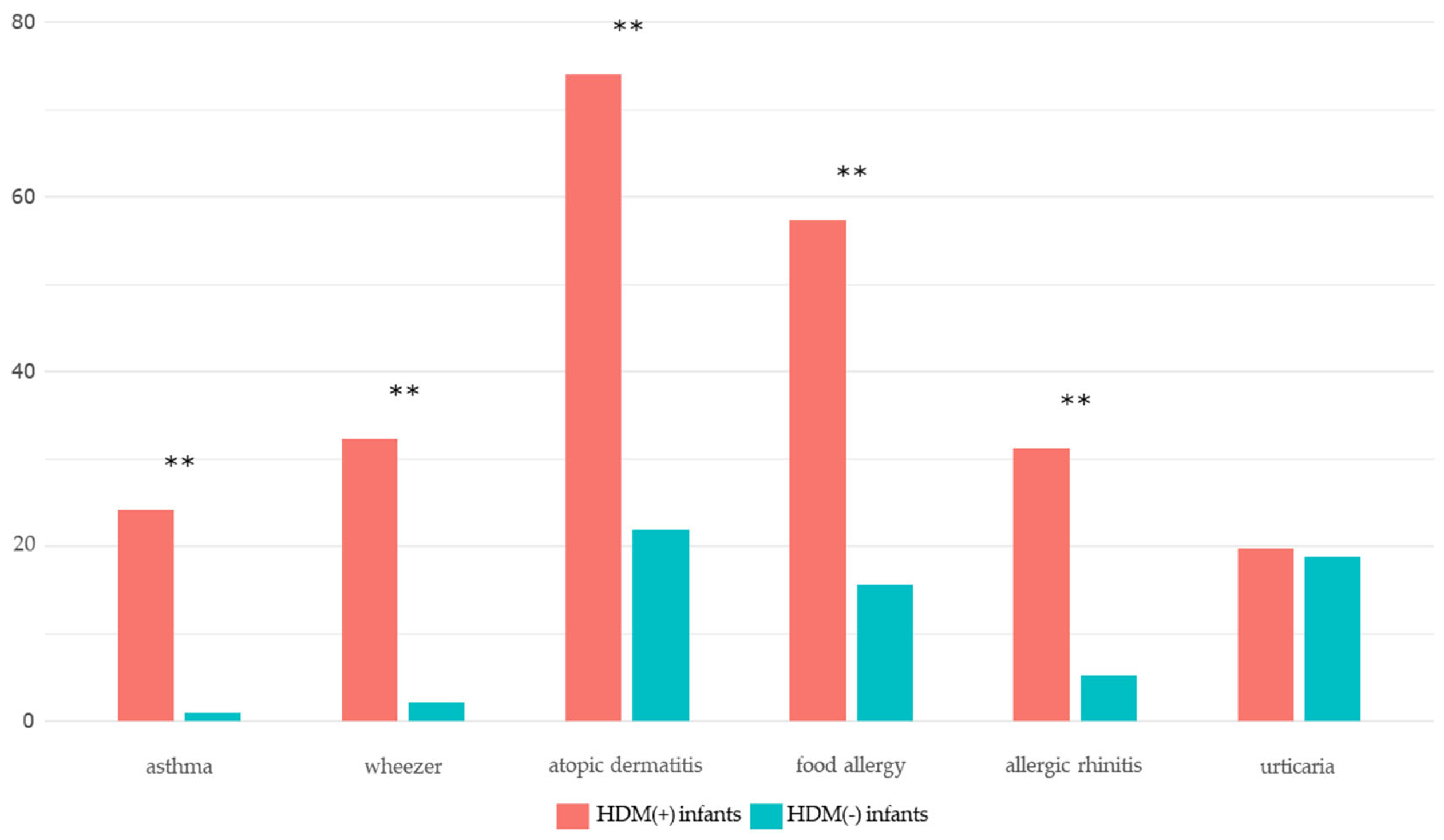
Figure 2.
Comparison of allergy test results and family history of allergic diseases between the HDM(+) and HDM(−) groups (**P < 0.01, ***P < 0.001).
Figure 2.
Comparison of allergy test results and family history of allergic diseases between the HDM(+) and HDM(−) groups (**P < 0.01, ***P < 0.001).
4. Discussion
In this study, the prevalence of HDM sensitization among infants under 2 years of age who visited our hospital’s allergy clinic was 5.4%. Sensitization to HDMs is generally considered uncommon in this age group. However, a Belgian study reported that up to 28% of infants under 2 years of age attending an asthma clinic were sensitized to aeroallergens, the majority of whom were sensitized to HDMs [1]. Similarly, a cohort study from Thailand found that approximately 30% of children aged 18–24 months were sensitized to HDMs, although two-thirds of these children were asymptomatic, a finding attributed to the region’s persistently humid climate [2].
Environmental conditions may explain regional differences in HDM sensitization rates. Korea’s traditional floor heating system (Ondol) and lower use of carpeting compared to Western countries have historically been thought to limit HDM exposure. Nonetheless, with progressive Westernization of living environments and lifestyle changes, the prevalence of HDM sensitization in Korea has risen [3]. Domestic data published in 2010 reported sensitization rates of 32.4% among elementary school students, 42.7% among middle school students, and 57.2% among children residing in metropolitan areas [4].
Although the relationship between early HDM exposure and subsequent respiratory allergic disease remains a subject of debate [5,6], multiple studies have demonstrated that early HDM sensitization is associated with impaired lung function and adverse respiratory outcomes later in childhood. In one birth cohort study, even asymptomatic toddlers with early HDM sensitization exhibited higher rates of asthma and allergic rhinitis at 7 years of age, increased exhaled nitric oxide levels, and a greater prevalence of airway hyperresponsiveness [2,7]. Given the retrospective nature of our study, it was not possible to assess long-term prognoses, such as respiratory disease severity or lung function in infants with early HDM sensitization. Nevertheless, we observed that 32.3% of sensitized infants experienced recurrent wheezing at the time of evaluation, and 22.9% had already been diagnosed with infantile asthma.
In the first year of life, IgE antibody responses are initially directed toward food allergens, followed later by responses to indoor and outdoor aeroallergens. Early onset of sensitization is clinically relevant, as it typically results in a longer duration of sensitization [1]. The harmful effects of exposure to indoor allergens, particularly when coupled with allergen sensitization, are most pronounced during the first three years of life. While adaptive immunity reaches maturity after approximately six years of age, the most critical period for establishing mature systemic immune responses occurs between one and two years of age [2].
There is growing evidence that impaired skin barrier function facilitates allergen sensitization. It is hypothesized that infants with disrupted skin barriers due to atopic dermatitis are more readily sensitized to food allergens, potentially initiating the “allergic march. [3,4,5]” Sensitization to HDMs via a damaged skin barrier has also been documented. A French study reported delayed sensitization to inhalant allergens in infants with atopic dermatitis and demonstrated that higher transepidermal water loss was associated with increased rates of sensitization to inhalant allergens [6]. In our study, 74% of infants under 24 months of age and 90.9% of those under 12 months with HDM sensitization had concomitant atopic dermatitis. These findings suggest that infants with severe atopic dermatitis may develop aeroallergen sensitization through a compromised skin barrier.
Among infants with HDM sensitization in our cohort, 71.9% were co-sensitized to egg white, 56.3% to cow’s milk, and 50% to three or more food allergens. In those younger than 12 months, the rates were even higher (90.9%, 81.8%, and 72.7%, respectively). Infants sensitized to HDMs also exhibited significantly elevated levels of egg white–specific IgE, cow’s milk–specific IgE, and total IgE compared to non-sensitized infants. These findings suggest that infants with atopic dermatitis who are already sensitized to egg, milk, or multiple foods may be at increased risk for HDM sensitization, warranting clinical evaluation for aeroallergen sensitization in this population.
Previous research has reported a positive correlation between egg white– and HDM-specific immune responses in infants with atopic dermatitis, supporting the hypothesis that food and indoor allergens may concurrently sensitize infants via the skin [7]. A Danish birth cohort study further demonstrated that early-life sensitization to hen’s eggs was associated with asthma and rhinoconjunctivitis at 14 years of age, while transient early HDM sensitization conferred an increased risk of asthma (adjusted odds ratio 3.80) at the same age [8]. In our cohort, infants sensitized to HDMs had a significantly higher prevalence of egg white sensitization compared to those without HDM sensitization, and HDM-specific IgE levels were significantly correlated with egg white–specific IgE levels.
In high-risk infants, HDM sensitization appears to negatively influence respiratory outcomes, emphasizing the need for early environmental interventions aimed at reducing HDM exposure to help prevent sensitization [9,10].
The primary limitation of this study is its retrospective design, which precluded assessment of long-term respiratory outcomes in infants with early HDM sensitization compared to non-sensitized infants. However, the matched case-control approach employed in this study, with 1:1 matching for age and sex, minimized confounding variables, improved statistical precision, enhanced efficiency despite a relatively small sample size, and allowed clearer interpretation of results. By analyzing the clinical characteristics of infants with early HDM sensitization, this study contributes to a better understanding of the risk profile for infants potentially predisposed to adverse respiratory allergic outcomes.
5. Conclusions
Early-life HDM sensitization in infants was frequently accompanied by multiple food sensitizations, particularly to egg white, and strongly associated with atopic dermatitis. Given these associations, clinicians should consider evaluating HDM sensitization in infants presenting with atopic dermatitis, food allergies, or elevated total and egg white–specific IgE levels to guide early intervention strategies.
Author Contributions
Conceptualization: Jeon YH. Data curation: Jung HI. Formal analysis: Jung HI. Investigation: Jung HI. Methodology: Jeon YH. Software: Jeon YH. Writing - original draft: Jung HI. Writing - review and editing: Jeon YH.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HDM | House dust mite |
| sIgE | Specific immunoglobulin E |
References
- Miyamoto, T.; Oshima, S.; Ishizaki, T.; Sato, S.H. Allergenic identity between the common floor mite (Dermatophagoides farinae Hughes, 1961) and house dust as a causative antigen in bronchial asthma. J Allergy 1968, 42, 14–28. [Google Scholar] [CrossRef] [PubMed]
- Sarsfield, J.K. Role of house-dust mites in childhood asthma. Arch Dis Child 1974, 49, 711–715. [Google Scholar] [CrossRef] [PubMed]
- Ree, H.I.; Jeon, S.H.; Lee, I.Y.; Hong, C.S.; Lee, D.K. Fauna and geographical distribution of house dust mites in Korea. Korean J Parasitol 1997, 35, 9–17. [Google Scholar] [CrossRef]
- Kim, J.; Hahm, M.I.; Lee, S.Y.; Kim, W.K.; Chae, Y.; Park, Y.M.; et al. Sensitization to aeroallergens in Korean children: a population-based study in 2010. J Korean Med Sci 2011, 26, 1165–1172. [Google Scholar] [CrossRef]
- Jeong, K.Y.; Park, J.W.; Hong, C.S. House dust mite allergy in Korea: the most important inhalant allergen in current and future. Allergy Asthma Immunol Res 2012, 4, 313–325. [Google Scholar] [CrossRef]
- Park, S.C.; Hwang, C.S.; Chung, H.J.; Purev, M.; Al Sharhan, S.S.; Cho, H.J.; et al. Geographic and demographic variations of inhalant allergen sensitization in Koreans and non-Koreans. Allergol Int 2019, 68, 68–76. [Google Scholar] [CrossRef]
- Dharmage, S.C.; Lowe, A.J.; Matheson, M.C.; Burgess, J.A.; Allen, K.J.; Abramson, M.J. Atopic dermatitis and the atopic march revisited. Allergy 2014, 69, 17–27. [Google Scholar] [CrossRef] [PubMed]
- Gabryszewski, S.J.; Hill, D.A. One march, many paths: Insights into allergic march trajectories. Ann Allergy Asthma Immunol 2021. [Google Scholar] [CrossRef]
- Eapen, A.A.; Kim, H. The Phenotype of the Food-Allergic Patient. Immunol Allergy Clin North Am 2021, 41, 165–75. [Google Scholar] [CrossRef]
- Calderón, M.A.; Linneberg, A.; Kleine-Tebbe, J.; De Blay, F.; Hernandez Fernandez de Rojas, D.; Virchow, J.C.; et al. Respiratory allergy caused by house dust mites: What do we really know? J Allergy Clin Immunol 2015, 136, 38–48. [Google Scholar] [CrossRef]
- Hammad, H.; Chieppa, M.; Perros, F.; Willart, M.A.; Germain, R.N.; Lambrecht, B.N. House dust mite allergen induces asthma via Toll-like receptor 4 triggering of airway structural cells. Nat Med 2009, 15, 410–416. [Google Scholar] [CrossRef] [PubMed]
- Sporik, R.; Holgate, S.T.; Platts-Mills, T.A.E.; Cogswell, J.J. Exposure to House-Dust Mite Allergen (Der p I) and the Development of Asthma in Childhood. 1990, 323, 502-7.
- Brussee, J.E.; Smit, H.A.; van Strien, R.T.; Corver, K.; Kerkhof, M.; Wijga, A.H.; et al. Allergen exposure in infancy and the development of sensitization, wheeze, and asthma at 4 years. J Allergy Clin Immunol 2005, 115, 946–952. [Google Scholar] [CrossRef]
- Celedón, J.C.; Milton, D.K.; Ramsey, C.D.; Litonjua, A.A.; Ryan, L.; Platts-Mills, T.A.; et al. Exposure to dust mite allergen and endotoxin in early life and asthma and atopy in childhood. J Allergy Clin Immunol 2007, 120, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Su, K.W.; Chiu, C.Y.; Tsai, M.H.; Liao, S.L.; Chen, L.C.; Hua, M.C.; et al. Asymptomatic toddlers with house dust mite sensitization at risk of asthma and abnormal lung functions at age 7 years. World Allergy Organ J 2019, 12, 100056. [Google Scholar] [CrossRef]
- Illi, S.; von Mutius, E.; Lau, S.; Niggemann, B.; Grüber, C.; Wahn, U. Perennial allergen sensitisation early in life and chronic asthma in children: a birth cohort study. Lancet 2006, 368, 763–770. [Google Scholar] [CrossRef]
- De Bilderling, G.; Mathot, M.; Agustsson, S.; Tuerlinckx, D.; Jamart, J.; Bodart, E. Early skin sensitization to aeroallergens. 2008, 38, 643-8.
- Casas, L.; Sunyer, J.; Tischer, C.; Gehring, U.; Wickman, M.; Garcia-Esteban, R.; et al. Early-life house dust mite allergens, childhood mite sensitization, and respiratory outcomes. Allergy 2015, 70, 820–827. [Google Scholar] [CrossRef] [PubMed]
- Lau, S.; Illi, S.; Sommerfeld, C.; Niggemann, B.; Bergmann, R.; von Mutius, E.; et al. Early exposure to house-dust mite and cat allergens and development of childhood asthma: a cohort study. The Lancet 2000, 356, 1392–1397. [Google Scholar] [CrossRef]
- Wahn, U.; Bergmann, R.; Kulig, M.; Forster, J.; Bauer, C.P. The natural course of sensitisation and atopic disease in infancy and childhood. Pediatr Allergy Immunol 1997, 8(10 Suppl), 16–20. [Google Scholar]
- Holt, P.G.; Jones, C.A. The development of the immune system during pregnancy and early life. Allergy 2000, 55, 688–697. [Google Scholar] [CrossRef] [PubMed]
- Brough, H.A.; Liu, A.H.; Sicherer, S.; Makinson, K.; Douiri, A.; Brown, S.J.; et al. Atopic dermatitis increases the effect of exposure to peanut antigen in dust on peanut sensitization and likely peanut allergy. J Allergy Clin Immunol 2015, 135, 164–170. [Google Scholar] [CrossRef]
- Tham, E.H.; Rajakulendran, M.; Lee, B.W.; Van Bever, H.P.S. Epicutaneous sensitization to food allergens in atopic dermatitis: What do we know? Pediatr Allergy Immunol 2020, 31, 7–18. [Google Scholar] [CrossRef]
- Brough, H.A.; Nadeau, K.C.; Sindher, S.B.; Alkotob, S.S.; Chan, S.; Bahnson, H.T.; et al. Epicutaneous sensitization in the development of food allergy: What is the evidence and how can this be prevented? Allergy 2020, 75, 2185–2205. [Google Scholar] [CrossRef]
- Boralevi, F.; Hubiche, T.; Léauté-Labrèze, C.; Saubusse, E.; Fayon, M.; Roul, S.; et al. Epicutaneous aeroallergen sensitization in atopic dermatitis infants - determining the role of epidermal barrier impairment. Allergy 2008, 63, 205–210. [Google Scholar] [CrossRef]
- Kimura, M.; Meguro, T.; Ito, Y.; Tokunaga, F.; Hashiguchi, A.; Seto, S. Close Positive Correlation between the Lymphocyte Response to Hen Egg White and House Dust Mites in Infants with Atopic Dermatitis. Int Arch Allergy Immunol 2015, 166, 161–169. [Google Scholar] [CrossRef]
- Christiansen, E.S.; Kjaer, H.F.; Eller, E.; Bindslev-Jensen, C.; Høst, A.; Mortz, C.G.; et al. Early-life sensitization to hen’s egg predicts asthma and rhinoconjunctivitis at 14 years of age. Pediatr Allergy Immunol 2017, 28, 776–783. [Google Scholar] [CrossRef] [PubMed]
- Yoo, Y.; Perzanowski, M.S. Allergic sensitization and the environment: latest update. Curr Allergy Asthma Rep 2014, 14, 465. [Google Scholar] [CrossRef] [PubMed]
- Jeon, Y.H.; Lee, Y.J.; Sohn, M.H.; Lee, H.R. Effects of Vacuuming Mattresses on Allergic Rhinitis Symptoms in Children. Allergy Asthma Immunol Res 2019, 11, 655–663. [Google Scholar] [CrossRef] [PubMed]

Table 1.
Demographic characteristics of infants with house dust mite sensitization.
| N (%) or mean ± SD | ||
|
Infants< 24 months (N=96) |
Infants< 12 months (N=11) |
|
| Age (months) | 17.2 ± 4.3 | 10.3 ± 0.9 |
| Male | 63 (64.6%) | 8 (72.7%) |
| Doctor-diagnosed allergic disease | ||
| Atopic dermatitis | 71 (74.0%) | 10 (90.9%) |
| Food allergy | 55 (57.3%) | 11 (100%) |
| Anaphylaxis | 10 (10.4%) | 2 (18.2%) |
| Recurrent wheezing (≥ 4 times) | 31 (32.3%) | 4 (36.4%) |
| Asthma | 23 (24.2%) | 3 (27.3%) |
| Allergic rhinitis | 30 (31.2%) | 2 (18.2%) |
Categorical variables are presented as n (%) and continuous variables as mean ± SD.
Table 2.
Allergy test results of infants with house dust mite sensitization.
| Characteristics | N (%) or mean ± SD | |
| Infants <24 months | Infants <12 months | |
| Total IgE* (kU/L) | 415.0 ± 674.1 | 368.2 ± 718.9 |
| HDM† sIgE‡ (kU/L) | 12.4 ± 23.6 | 13.3 ± 29.5 |
| Egg whitesensitization | 69 (75.0%) | 10 (90.9%) |
| Cow’s milk sIgEsensitization | 54 (62.8%) | 9 (81.8%) |
|
Multiple food sensitization (≥ 3 food allergens) |
48 (51.1%) | 8 (72.7%) |
*HDM, House dust mites; IgE, Immunoglobulin E; sIgE, Specific immunoglobulin E. Categorical variables are presented as n (%) and continuous variables as mean ± SD.
Table 3.
Comparison between the HDM (+) and HDM (−) groups of infants (<24 months).
| Variables | HDM (+) group | HDM (−) group | P-value |
| Atopic dermatitis | 71 (74.0) | 21 (21.9) | <0.001*** |
| Food allergy | 55 (57.3) | 15 (15.6) | <0.001*** |
| Anaphylaxis | 10 (10.4) | 3 (3.1) | 0.096 |
| Recurrent wheezing (≥ 4 times) | 31 (32.3) | 2 (2.1) | <0.001*** |
| Asthma | 23 (24.2) | 1 (1.0) | <0.001*** |
| Allergic rhinitis | 30 (31.2) | 5 (5.2) | <0.001*** |
| Urticaria | 19 (19.8) | 18 (18.8) | 1.000 |
| Egg whitesensitization | 69 (75.0) | 31 (33.0) | <0.001*** |
| Milk sIgEsensitization | 54 (62.8) | 36 (38.7) | 0.007** |
|
Multiple foodsensitization (≥ 3 food allergens) |
48 (51.1) | 8 (8.3) | <0.001*** |
*HDM, House dust mites; IgE, Immunoglobulin E; sIgE, Specific immunoglobulin E. HDM(+) versus HDM(–) infants were compared using McNemar’s test. *P < 0.05, **P < 0.01, ***P < 0.001.
Table 4.
Laboratory findings in the HDM (+) and HDM (−) groups of infants (<24 months).
| Variables |
HDM (+) group (mean ± SD) |
HDM (−) group (mean ± SD) |
P-value |
| Log(total IgE+1) | 2.17 ± 0.64 | 1.57 ± 0.66 | ≤ 0.001 |
| Egg white sIgE (kU/L) | 16.13 ± 29.65 | 1.15 ± 3.30 | ≤0.001 |
| Cow’s milk sIgE (kU/L) | 6.08 ± 16.20 | 0.67 ± 1.36 | 0.001 |
*HDM, House dust mites; IgE, Immunoglobulin E; sIgE, Specific immunoglobulin E. Values are expressed as mean ± SD. P-values for log-transformed total IgE were calculated using the paired t-test, whereas P-values for the remaining variables were calculated using the Wilcoxon signed-rank test.
Table 5.
Factors that are correlated with HDM levels.
|
Total IgE coefficient (P-value) |
Egg white sIgE coefficient (P-value) |
Cow’s milk sIgE coefficient (P-value) |
|
| HDM sIgE | 0.326 (0.002) | 0.312 (0.002) | 0.215 (0.047) |
*HDM, House dust mites; IgE, Immunoglobulin E; sIgE, Specific immunoglobulin E.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



