Submitted:
04 August 2025
Posted:
05 August 2025
You are already at the latest version
Abstract
Human papillomavirus (HPV) is a major etiological factor in cervical, anal, and oro-pharyngeal cancers. Although prophylactic vaccines have substantially reduced infec-tion rates, effective therapeutic options for established HPV-associated malignancies remain limited. This review provides an up-to-date overview of emerging strategies to treat HPV-driven tumors. Key approaches include immune checkpoint inhibitors, therapeutic vaccines such as VGX‑3100 and PRGN‑2012, and gene-editing tools like CRISPR/Cas9. Epigenetic drugs, particularly histone deacetylase inhibitors, show promise in reactivating silenced tumor suppressor genes and enhancing antitumor immunity. In addition, natural bioactive compounds and plant-derived molecules are being explored as complementary anti-HPV agents, while drug repurposing and combination therapies offer cost-effective opportunities to broaden treatment options. We also highlight the role of patient-derived organoid models as powerful platforms for personalized drug screening and functional assessment. By integrating these therapeutic innovations with precision oncology approaches, this review outlines a multi-dimensional framework aimed at improving clinical outcomes and quality of life for patients with HPV-associated cancers.
Keywords:
HPV-associated cancers
; therapeutic vaccines
; immune checkpoint inhibitors
; CRISPR/Cas9
; epigenetic drugs
; natural compounds
; drug repurposing
; organoids
; precision oncology
1. Introduction
Human papillomavirus (HPV) is a small, double-stranded DNA virus of approximately 8 kilobases, encapsulated by the structural proteins L1 and L2. More than 200 HPV types have been identified, of which around a dozen, including HPV-16 and HPV-18, are classified as high-risk due to their strong association with cervical, anogenital, and oropharyngeal cancers [1]. HPV primarily infects epithelial cells and can integrate its DNA into the host genome. This integration often disrupts the viral E2 gene, leading to uncontrolled expression of the viral oncoproteins E6 and E7. E6 forms a complex with E6AP to mediate ubiquitin-dependent degradation of the tumor suppressor p53, while E7 inactivates pRb, releasing E2F transcription factors and driving uncontrolled cell proliferation. These molecular events promote genomic instability, a crucial step in malignant transformation [1] (Figure 1).
HPV has developed sophisticated immune evasion strategies to establish persistent infection. Early viral proteins suppress innate immune sensors and type I interferon signaling, thereby attenuating antiviral responses [2,3]. In addition, E6 and E7 downregulate MHC I expression, reducing recognition by cytotoxic T lymphocytes [4]. HPV further remodels the tumor microenvironment to promote immunosuppression by recruiting regulatory T cells and M2-polarized macrophages [5]. Although most HPV infections are transient and cleared within two years, approximately 10–30% persist. Chronic infection facilitates the long-term presence of viral DNA in epithelial tissues, creating a high risk of lesion formation and eventual malignant progression.
Prophylactic vaccines such as Gardasil and Cervarix induce neutralizing antibodies against the L1 capsid protein and are highly effective at preventing primary infection. However, they lack therapeutic activity against established infections or lesions [6]. Standard treatments—surgery, radiotherapy, and chemotherapy—primarily aim to remove or destroy tumor tissue but do not eradicate HPV DNA or reverse the virus-driven immune evasion mechanisms [7,8]. Consequently, recurrence rates remain high, especially in patients with advanced disease or immunocompromised conditions [9].
Given these limitations, novel therapeutic approaches are under active investigation. These include gene-editing technologies, epigenetic drugs, therapeutic vaccines, and natural bioactive compounds. In parallel, strategies such as drug repurposing, organoid-based drug screening, and precision oncology are gaining increasing attention. This review aims to provide a comprehensive overview of these emerging therapeutic strategies for HPV-associated cancers.
2. Therapeutic Approaches
The development of effective treatments for HPV-associated cancers requires strategies that directly target viral oncogenes, reverse immune evasion, and personalize therapy to individual tumor profiles. Several therapeutic modalities are under investigation, including genome editing, epigenetic drugs, therapeutic vaccines, natural compounds, drug repurposing, and organoid-based functional screening. An overview of these approaches and their key characteristics is provided in Table 1.
2.1. Genome Editing Approaches
Gene-editing technologies such as CRISPR/Cas9 and transcription activator-like effector nucleases (TALENs) directly target the viral oncogenes E6 and E7, which are essential for HPV-driven carcinogenesis. In vitro and in vivo studies have shown that disrupting these genes restores the function of the tumor suppressors p53 and pRb, leading to apoptosis, growth arrest, and tumor regression in mouse models [10,11].
CRISPR/Cas9 is currently the most extensively studied platform for genome editing in HPV-associated cancers. Proof-of-concept experiments have demonstrated that CRISPR-mediated knockout of E6 and E7 downregulates viral gene expression, restores p53 and Rb activity, and suppresses tumor growth [11,12,20]. These effects are illustrated in Figure 2.
A comparison of two representative CRISPR based studies is provided in Table 2.
Despite these promising findings, several barriers hinder clinical translation. Effective and safe delivery of genome-editing components remains a key challenge. Nanoparticles, liposomes, and viral vectors (e.g., AAVs) are under active investigation to improve delivery specificity and efficiency [10,11,12,13,14]. Although refined guide RNA designs and high-fidelity Cas9 variants have reduced off-target cleavage, the risk of unintended genomic alterations persists [15,21].
Other genome-targeting approaches include RNA interference (RNAi) using siRNA or antisense oligonucleotides, which can transiently suppress E6/E7 expression and partially restore p53 activity in preclinical models [14,15]. However, these strategies lack the durable effects of CRISPR and have yet to enter human clinical trials [11,12,13,14,15]. Overall, genome editing represents a highly promising strategy for directly eliminating the viral drivers of HPV-associated cancers. Future research must focus on improving delivery methods, minimizing off-target effects, and addressing ethical and regulatory concerns before clinical translation can be realized.
2.2. Epigenetic Drugs
High-risk HPV types, particularly HPV-16 and HPV-18, promote carcinogenesis not only through direct genetic disruption but also by extensively reprogramming the host cell epigenetic landscape. The viral oncoproteins E6 and E7 enhance DNA methylation and reduce histone acetylation, leading to the silencing of tumor suppressor genes such as p53 and RB, while simultaneously promoting immune evasion [22].
Epigenetic drugs have gained attention for their ability to reverse these oncogenic alterations. Histone deacetylase inhibitors (HDACi) including vorinostat, romidepsin, and belinostat can reactivate silenced genes, restore tumor suppressor function, and enhance tumor immunogenicity. In HPV-positive keratinocyte models, vorinostat treatment stabilized tumor suppressor proteins, induced apoptosis, and increased immune recognition of infected cells [22]. Early-phase clinical studies are investigating the combination of HDACi with immune checkpoint inhibitors or chemoradiotherapy, particularly in HPV-associated head and neck cancers [23].
DNA methyltransferase inhibitors (DNMTi) such as 5-azacytidine and decitabine can demethylate silenced tumor suppressor promoters, including p16 and E-cadherin. This reactivation of gene expression restores HPV antigen presentation, thereby enhancing T-cell recognition and sensitizing tumors to PD-1/PD-L1 checkpoint blockade. Robust preclinical evidence supports these effects, and early-phase clinical trials are evaluating DNMTi in combination with immunotherapies in HPV-positive cervical and oropharyngeal cancers [23].
Epigenetic therapy provides a dual mechanism of action by reversing HPV-driven gene silencing and creating a tumor microenvironment that is more responsive to immune attack. These features position epigenetic drugs as promising components of multimodal regimens for HPV-associated malignancies.
2.3. Therapeutic Vaccines
Therapeutic vaccines aim to stimulate the host immune system to selectively eliminate HPV-infected or transformed cells by targeting the viral oncoproteins E6 and E7, which are consistently expressed in HPV-associated malignancies. Unlike prophylactic vaccines such as Gardasil and Cervarix, which induce neutralizing antibodies against the L1 capsid protein to prevent infection, therapeutic vaccines are designed to elicit strong cytotoxic T-cell responses against established infections and lesions [24].
VGX-3100, a DNA-based vaccine encoding consensus sequences of HPV-16 and HPV-18 E6/E7 genes, has shown promising efficacy. Administered via intramuscular injection followed by electroporation, VGX-3100 induced robust antigen-specific CD8⁺ T-cell responses in women with cervical intraepithelial neoplasia grade 2 or 3 (CIN2/3). Phase I and II clinical trials demonstrated significant histologic regression and viral clearance, with durable immune responses lasting up to 24 weeks after vaccination [24,25]. The vaccine is currently undergoing phase III trials, as well as combination studies with immune adjuvants and checkpoint inhibitors [26].
PRGN-2012, a gorilla adenovirus–based vector vaccine, is designed to induce strong T-cell responses against HPV-6/11 and primarily targets recurrent respiratory papillomatosis (RRP). In a phase 1/2 trial in adult RRP patients, PRGN-2012 achieved a 55% complete response rate, with many patients avoiding surgical intervention for at least 12 months after treatment. The vaccine also significantly reduced lesion burden and improved vocal function, while demonstrating a favorable safety profile without serious adverse events [27]. It has since received Breakthrough Therapy and Orphan Drug designations, with ongoing phase 2 trials and regulatory submissions [27].
Despite encouraging results, several challenges remain, including optimization of antigen delivery methods, expansion of vaccine coverage beyond HPV-16/18 or 6/11, and overcoming immunosuppressive tumor microenvironments [13,14,17]. Combining therapeutic vaccines with checkpoint inhibitors, epigenetic drugs, or immune adjuvants is a promising strategy to enhance efficacy [6,17]. As ongoing clinical trials progress, therapeutic vaccines are poised to become an integral component of multimodal treatment regimens for HPV-driven diseases [17,25].
2.4. Natural Compounds & Phytochemicals
Plant-derived natural compounds have attracted considerable attention for their potential to suppress HPV infection and HPV-associated carcinogenesis. Among these, curcumin (from turmeric), epigallocatechin gallate (EGCG, from green tea), and resveratrol (a polyphenol found in grapes and berries) are the most extensively studied for their antiviral and anticancer effects [28,29,30]. These phytochemicals modulate multiple cellular pathways, including downregulation of HPV viral gene expression, induction of apoptosis, and immune modulation [30,31]. Evidence from in vitro and in vivo studies indicates that these compounds can slow HPV-driven cellular transformation and may reduce cancer progression risk [28,32].
Recent investigations have expanded the list of promising natural molecules. Withaferin A, a steroidal lactone from Withania somnifera, has been shown to downregulate E6/E7 expression and restore p53 activity in HPV-positive cervical cancer cells [33]. Berberine, an isoquinoline alkaloid, induces apoptosis and cell cycle arrest in HPV-transformed cervical cells via mitochondrial dysfunction and oxidative stress modulation [34]. Genistein, a soy-derived isoflavone, interferes with HPV oncoprotein activity while exerting immunomodulatory and antiproliferative effects [35].
A particularly noteworthy candidate is fig latex (Ficus carica), which has demonstrated selective inhibitory effects on HPV-positive cervical cancer cells. Our group has recently conducted a series of studies providing strong evidence of its multifaceted anti-HPV effects. We showed that fig latex suppresses proliferation, migration, and invasion of HPV16⁺ (CaSki) and HPV18⁺ (HeLa) cells while downregulating E6/E7 expression and reactivating p53 and Rb pathways [33]. Subsequent transcriptomic profiling revealed modulation of immunity-linked pathways, including antigen presentation and ubiquitination processes, suggesting enhanced tumor immunogenicity [34]. Furthermore, RNA-seq analysis demonstrated that fig latex induces cell cycle arrest at the sub-G1 phase and regulates key genes involved in nonsense-mediated decay (NMD), TP53 transcriptional regulation, and apoptosis [35]. Importantly, fig latex selectively targets HPV-positive cancer cells without cytotoxic effects on normal cervical keratinocytes, highlighting its potential as a safe therapeutic option [33,34,35].
Despite these promising findings, translation into clinical use remains limited by challenges such as extract standardization, variable bioavailability, and the absence of large-scale clinical trials. Further pharmacological optimization and rigorous clinical studies are essential to establish their therapeutic value [29,30,32,33,34,35].

Table 3.
Selected natural compounds with anti-HPV activity and their mechanisms of action.
| Compound | Natural Source | Mechanism of Action | HPV-related Effect |
|---|---|---|---|
| Curcumin | Turmeric (Curcuma longa) | Inhibits E6/E7 expression; induces apoptosis; modulates NF-κB signaling | Suppresses viral oncogene expression; anti-proliferative |
| EGCG | Green tea (Camellia sinensis) | Antioxidant activity; inhibition of DNA methylation; cell cycle arrest | Inhibits HPV-positive cell growth; sensitizes to therapy |
| Resveratrol | Grapes, berries | Downregulates E6/E7; induces autophagy and apoptosis | Inhibits HPV-driven transformation; enhances immune responses |
| Withaferin A | Withania somnifera | Downregulates E6/E7; restores p53 activity | Reduces HPV oncogene activity; promotes apoptosis |
| Berberine | Berberis species | Induces mitochondrial dysfunction; increases ROS; causes cell cycle arrest | Triggers apoptosis in HPV-transformed cervical cancer cells |
| Fig latex | Ficus carica | Downregulates HPV E6/E7; reactivates p53/Rb; induces cell cycle arrest and apoptosis; modulates immune-related gene expression | Selectively inhibits proliferation, migration, and invasion of HPV-positive cervical cancer cells; enhances antigen presentation and immune recognition |
3. Drug Repurposing & Combination Therapies
The development of entirely new drugs is often time-consuming and costly. Drug repurposing, which involves identifying new therapeutic uses for existing approved drugs, has therefore emerged as a promising strategy for the treatment of HPV-related cancers. Its key advantages include lower cost, shorter development timelines, and well-established safety profiles [36].
Several repurposed drugs have demonstrated activity against HPV-driven malignancies. Niclosamide, an anti-parasitic agent, has been shown to inhibit HPV oncoprotein activity and suppress proliferation of HPV-positive cancer cells [36]. Similarly, Lopinavir, an HIV protease inhibitor, exhibits cytotoxic effects on HPV-transformed cells and has been proposed as a topical or systemic therapy for HPV-associated lesions [37].
In parallel, combination therapies are gaining attention for their potential to enhance efficacy through multi-target approaches. Strategies under investigation include chemo-immunotherapy, the combination of epigenetic drugs with immune checkpoint inhibitors, and the integration of therapeutic vaccines with immunomodulatory agents [38]. Early-phase clinical studies have reported encouraging results, and several combinations are being evaluated in ongoing clinical trials (Table 4 and Table 5). However, further validation in larger patient cohorts is required to confirm efficacy and safety. These approaches hold promise for delivering more effective and personalized treatments for HPV-associated malignancies [38].
As ongoing trials mature, rational drug repurposing and synergistic combination regimens are likely to play an increasingly important role in the multimodal management of HPV-associated cancers.
4. Patient-Derived Organoids & Functional Screening
Organoids are three-dimensional (3D) mini-organ structures generated from stem cells or patient-derived tumor tissues. They closely recapitulate the architecture, cellular heterogeneity, and genetic features of the original tissue, making them powerful preclinical models for cancer research [39]. In HPV-associated malignancies, particularly cervical and oropharyngeal cancers, patient-derived organoids serve as a physiologically relevant platform to study viral oncogenesis and tumor biology in a patient-specific context [40,41].
These models enable the development of personalized therapies by accurately replicating individual tumor responses to various treatments [41]. Drug sensitivity assays performed on patient-derived organoids allow researchers to identify the most effective chemotherapeutic agents, targeted drugs, or immunotherapies for each patient. Compared with conventional two-dimensional cell line models, organoids provide superior predictive accuracy for preclinical drug testing [39,40]. When integrated with high-throughput pharmacogenomic platforms, organoid-based screening can systematically map drug responses across diverse HPV-positive tumor genotypes [41]. Such an approach holds significant promise for precision oncology, facilitating the discovery of patient-tailored treatment strategies and predictive biomarkers for therapy selection [39,41].
5. Integration with Precision Oncology
The treatment paradigm for HPV-related cancers is increasingly shifting toward precision oncology, where therapeutic decisions are guided by the molecular characteristics of each patient’s tumor [42]. This approach is facilitated by the integration of multi-omics data—genomics (DNA mutations), transcriptomics (gene expression profiles), and proteomics (protein activity and post-translational modifications)—to generate a comprehensive understanding of tumor biology [42,43]. Such datasets enable clinicians to design tailored treatment strategies and select the most effective drug combinations for individual patients.
Artificial intelligence (AI)-based tools are playing a pivotal role in analyzing these large and complex multi-omics datasets. Machine learning and deep learning algorithms can detect subtle molecular patterns, predict treatment responses, and identify novel therapeutic targets [44]. By combining genomic and clinical information, AI-driven platforms can assist in developing personalized treatment plans, simulating drug efficacy, and anticipating toxicity risks, thereby improving both treatment safety and clinical outcomes [44,45]. Some advanced systems even incorporate real-time clinical data to dynamically adjust therapy, further optimizing patient care and resource allocation.
The integration of patient-derived organoid models, multi-omics profiling, and AI-powered analytics represents a transformative step toward truly individualized treatment. By combining these approaches, precision oncology provides a pathway to highly effective, personalized, and safer therapies for patients with HPV-associated cancers.
6. Conclusions and Future Directions
Therapeutic strategies for HPV-related cancers have advanced considerably in recent years, expanding from foundational gene-editing approaches to include natural phytochemicals, drug repurposing, patient-derived organoid models, and AI-driven personalization. CRISPR/Cas9 systems targeting the viral oncogenes E6 and E7 have shown promising antitumor activity in preclinical studies [46,18]. By disrupting these oncogenes, multiple studies have demonstrated restoration of p53 and pRb tumor suppressor pathways, leading to apoptosis or cellular senescence in cervical cancer cells [47,48]. In vivo experiments confirmed these findings, with CRISPR-treated mice showing significant reductions in tumor burden and slower disease progression [11]. Efforts to enhance in vivo applicability include systemic delivery of CRISPR components via viral or nanoparticle-based vectors [14]. These findings highlight the therapeutic potential of gene-editing technologies in targeting viral oncogenesis at its source and lay the groundwork for highly specific, next-generation treatment options.
A phase I/II clinical trial is currently assessing the safety and feasibility of gene-editing tools such as CRISPR/Cas9 and TALENs in patients with persistent HPV infection and cervical intraepithelial neoplasia (CIN), marking an important step toward clinical translation [18]. In parallel, natural phytochemicals—including curcumin, epigallocatechin gallate (EGCG), resveratrol, and luteolin—have demonstrated potent antiviral and anticancer effects in both in vitro and in vivo HPV models. Curcumin suppresses E6/E7 oncogene expression, reactivates p53-dependent tumor suppressor pathways, and promotes apoptosis and DNA damage responses in HPV-positive cervical cancer cells [28]. Clinical studies with EGCG-rich green tea extracts have reported lesion regression in patients with cervical dysplasia [29,30]. Furthermore, combination formulations such as TriCurin, which includes curcumin, resveratrol, and EGCG, have shown synergistic antitumor activity and efficient inhibition of HPV transcripts in preclinical models [31]. Despite encouraging results, these compounds remain limited by poor bioavailability, variable dosing, and the absence of large-scale clinical trials [32].
Drug repurposing has also revealed promising candidates for HPV-related cancers. Niclosamide, originally developed as an antihelminthic, induces autophagic cell death and mitochondrial stress via mTOR pathway inhibition, supporting its potential repositioning for HPV-positive tumors [49]. Similarly, lopinavir, an antiretroviral protease inhibitor, has demonstrated cytotoxic effects in HPV-infected cervical cancer cell lines [37]. A topical intra-anal formulation of lopinavir/ritonavir is currently being evaluated in a phase I trial for preventing the progression of HPV-induced lesions, representing a novel localized therapeutic approach. In addition, AI- and network-based computational platforms are increasingly being used to accelerate drug discovery and repurposing, enabling rapid identification of candidate compounds and synergistic drug combinations by analyzing complex molecular interaction networks [50].
The development of patient-derived organoids offers a powerful tool for functional drug screening, enabling the assessment of therapeutic responses in a patient-specific context. While organoid research in HPV-related cancers remains in early stages, this approach is aligned with similar advances in other cancer types and holds strong potential for guiding precision-based treatments tailored to molecular and clinical profiles [51]. AI tools are being increasingly integrated with organoid platforms to enhance biomarker discovery and predict treatment outcomes. Predictive models trained on viral and host genomic, transcriptomic, and clinical data have begun identifying patient subgroups most likely to benefit from specific interventions [52]. However, the lack of validated, clinically actionable biomarkers for HPV-related malignancies continues to hinder the widespread implementation of these technologies.
Several clinical trials are currently investigating CRISPR-based interventions, therapeutic vaccines, immune checkpoint inhibitors, and repurposed drugs for HPV-related cancers. A summary of selected ongoing and completed clinical trials evaluating these approaches is provided in Table 6.
Despite significant progress, many of these strategies remain supported primarily by preclinical or early-phase clinical data, with relatively few advancing to phase II or III trials [53]. Natural compounds, while promising in vitro and in vivo, are limited by poor pharmacokinetics and variable pharmacodynamics. Likewise, organoid systems lack cross-laboratory standardization and require further validation for integration into clinical decision-making. Moreover, the scarcity of reliable biomarkers continues to hinder patient stratification and longitudinal monitoring of therapeutic efficacy.
To overcome these challenges, future progress will rely on multimodal precision strategies. An integrated approach combining gene-editing tools, immunotherapies, antiviral phytochemicals, repurposed pharmaceuticals, organoid-based functional screening, and AI-driven biomarker profiling could enable highly personalized and effective treatments. Clinical trial frameworks must also evolve to support this complexity, adopting adaptive, basket, and umbrella trial designs that reflect the dynamic nature of modern cancer therapy. Ultimately, the full potential of precision oncology in HPV-driven cancers will only be realized through the integration of diverse, patient-tailored therapeutic approaches.
References
- A, Kundu R. Human papillomavirus E6 and E7: The cervical cancer hallmarks and targets for therapy. Front Microbiol. 2020;10:3116. [CrossRef]
- Doorbar, J. The evolving immunobiology of human papillomavirus infection. Nat Rev Cancer. 2003, 3, B33–B44. [Google Scholar]
- Ronco, LV. HPV E6 proteins: Repertoire of functions from replication to immune modulation. Viruses. 2017, 9, 344. [Google Scholar]
- Pereira EM, et al. HPV E7 protein down-regulates MHC class I surface expression. PLoS One. 2015, 10, e0116775.
- Jaiswal R, Banerjee D. Tumor-associated inflammation and metastasis. Cancer Metastasis Rev. 2021, 40, 361–373.
- Teffera ZH, et al. Efficacy of a novel high-risk HPV-16/18 therapeutic vaccine in treating cervical intraepithelial neoplasia and cervical cancer in a clinical trial: A systematic review and meta-analysis. World Acad Sci J. 2024;6:52.
- Trimble, CL. Therapeutic HPV vaccines: Targeting the immune escape. Gynecol Oncol. 2010, 116, 486–490. [Google Scholar]
- Stanley, M. Immune responses to human papillomavirus. Vaccine. 2006;24(Suppl 1):S16–S22.
- Einstein MH, et al. Cervical cancer recurrence and immune status. Cancer Immunol Immunother. 2007, 56, 389–395.
- Zheng Y, Srisuttee R, Jiang Y, et al. Disruption of HPV16-E7 by CRISPR/Cas system induces apoptosis and growth inhibition in HPV16 positive human cervical cancer cells. Biomed Res Int. 2014;2014:612823. [CrossRef]
- Jubair L, Fallaha S, McMillan NAJ. Systemic delivery of CRISPR/Cas9 targeting HPV oncogenes is effective at eliminating established tumors. Mol Ther. 2019, 27, 2091–2099. [CrossRef]
- Xu Q, Chen Y, Jin Y, Wang Z, Dong H, Kaufmann AM, et al. Advanced nanomedicine for high-risk HPV-driven head and neck cancer. Viruses. 2022, 14, 2824. [CrossRef]
- Khairkhah N, Bolhassani A, Najafipour R. Current and future direction in treatment of HPV-related cervical disease. J Mol Med (Berl). 2022, 100, 829–845. [CrossRef]
- Lu Z, Haghollahi S, Afzal M. Potential therapeutic targets for the treatment of HPV-associated malignancies. Cancers (Basel). 2024, 16, 3474. [CrossRef]
- Zhen S, Qiang R, Lu J, Tuo X, Yang X, Li X. CRISPR/Cas9-HPV-liposome enhances antitumor immunity and treatment of HPV infection-associated cervical cancer. J Med Virol. 2023, 95, e28144. [CrossRef]
- Dadar M, Chakraborty S, Dhama K, et al. Advances in designing and developing vaccines, drugs and therapeutic approaches to counter human papilloma virus. Front Immunol. 2018;9:2478. [CrossRef]
- Huang Y, Wang J, Yang W, et al. Precision therapeutic targets for HPV-positive cancers: an overview and new insights. Infect Agents Cancer. 2025;20:17. [CrossRef]
- Wei Y, Zhao Z, Ma X. Description of CRISPR-Cas9 development and its prospects in human papillomavirus-driven cancer treatment. Front Immunol. 2022;13:1037124. [CrossRef]
- Kennedy EM, Kornepati AVR, Goldstein M, et al. Inactivation of the human papillomavirus E6 or E7 gene in cervical carcinoma cells using CRISPR/Cas9. J Virol. 2014, 88, 11965–11972. [CrossRef]
- Liu Y, Han X, Yuan J, et al. CRISPR/Cas9-mediated targeting of HPV oncogenes E6 and E7 induces apoptosis in cervical cancer cells. Biotechnol Lett. 2020, 42, 797–807.
- Zhang X-H, Tee LY, Wang X-G, Huang Q-S, Yang S-H. Off-target effects in CRISPR/Cas9-mediated genome engineering. Nat Rev Mol Cell Biol. 2021, 22, 467–484. [CrossRef]
- Autin P, Blanquart C, Fradin D. Epigenetic Drugs for Cancer and microRNAs: A Focus on Histone Deacetylase Inhibitors. Cancers. 2019;11:1530. [CrossRef]
- Burkitt K, Saloura V. Epigenetic modifiers as novel therapeutic targets and a systematic review of clinical studies investigating epigenetic inhibitors in head and neck cancer. Cancers (Basel). 2021, 13, 5241. [CrossRef]
- Bagarazzi ML, Yan J, Morrow MP, Shen X, Parker RL, Lee JC, et al. Immunotherapy against HPV16/18 generates potent TH1 and cytotoxic cellular immune responses. Sci Transl Med. 2012, 4, 155ra138. [Google Scholar] [CrossRef]
- Trimble CL, Morrow MP, Kraynyak KA, Shen X, Dallas M, Yan J, et al. Safety, efficacy, and immunogenicity of VGX-3100, a therapeutic synthetic DNA vaccine targeting human papillomavirus 16 and 18 E6 and E7 proteins for cervical intraepithelial neoplasia 2/3: a randomised, double-blind, placebo-controlled phase 2b trial. Lancet. 2015, 386, 2078–88. [Google Scholar] [CrossRef]
- Smalley Rumfield C, Roller N, Pellom ST, Schlom J, Jochems C. Therapeutic vaccines for HPV-associated malignancies. Immunotargets Ther. [CrossRef]
- Young MR, Rodriguez L, Hadden W, Ghosh S, Shrivastava S, Yang L, et al. PRGN-2012, a novel gorilla adenovirus-based immunotherapy, provides the first treatment that leads to complete and durable responses in recurrent respiratory papillomatosis patients. J Clin Oncol. 2024, 42(LBA6015). [CrossRef]
- Maher DM, et al. Curcumin inhibits human papillomavirus oncoproteins and induces apoptosis in cervical cancer cells. Gynecol Oncol. 2011, 123, 376–382.
- Musarra-Pizzo M, Pennisi R, Ben-Amor I, Mandalari G, Sciortino MT. Antiviral Activity Exerted by Natural Products against Human Viruses. Viruses. 2021, 13, 828. [CrossRef]
- Franconi R, Massa S, Paolini F, Vici P, Venuti A. Plant-Derived Natural Compounds in Genetic Vaccination and Therapy for HPV-Associated Cancers. Cancers. 2020, 12, 3101. [CrossRef]
- Einbond LS, Zhou J, Wu H, et al. A novel cancer preventative botanical mixture, TriCurin, inhibits viral transcripts and the growth of W12 cervical cells harbouring extrachromosomal or integrated HPV16 DNA. Br J Cancer. 2021;124:901–913. [CrossRef]
- Massa S, Pagliarello R, Paolini F, Venuti A. Natural Bioactives: Back to the Future in the Fight against Human Papillomavirus? A Narrative Review. J Clin Med. 2022, 11, 1465. [CrossRef]
- Ghanbari A, Le Gresley A, Naughton D, Kuhnert N, Sirbu D, Ashrafi GH. Biological activities of Ficus carica latex for potential therapeutics in Human Papillomavirus (HPV) related cervical cancers. Sci Rep. 2019, 9, 1013 Published 2019 Jan 31. [Google Scholar] [CrossRef]
- Cakir MO, Bilge U, Naughton D, Ashrafi GH. Ficus carica Latex Modulates Immunity-Linked Gene Expression in Human Papillomavirus Positive Cervical Cancer Cell Lines: Evidence from RNA Seq Transcriptome Analysis. Int J Mol Sci. 2023, 24, 13646. [CrossRef]
- Cakir MO, Bilge U, Ghanbari A, Ashrafi GH. Regulatory Effect of Ficus carica Latex on Cell Cycle Progression in Human Papillomavirus-Positive Cervical Cancer Cell Lines: Insights from Gene Expression Analysis. Pharmaceuticals (Basel). 2023, 16, 1723. [Google Scholar] [CrossRef]
- Xu M, Lee E, Choi J, Kim H. Repurposing anthelmintic drug niclosamide to treat HPV-positive cancers. Cancer Res. 2013, 73, 4777–4787.
- Hildebrand J, Smith A, Johnson L, Brown K. Lopinavir inhibits proliferation of HPV-positive cervical cancer cells. Gynecol Oncol. 2016, 141, 441–447. [CrossRef]
- Trimble CL, Morrow M, Kraynyak K, Amante D. Immunotherapy and combination strategies for HPV-associated cancers. Cancer Immunol Res. 2021, 9, 377–384.
- Sachs N, de Ligt J, Kopper O, Gogola E, Bounova G, Weeber F,... Clevers H. A living biobank of breast cancer organoids captures disease heterogeneity. Cell. 2018;172(1-2):373–386.e10. [CrossRef]
- Driehuis E, Kolders S, Spelier S, Lõhmussaar K, Willems SM, Devriese LA, de Bree R, de Ruiter EJ, Korving J, Begthel H, van Es JH, Clevers H, van Boxtel R. Human papillomavirus-associated oropharyngeal cancer organoids for drug screening and therapy development. Cancer Discov. 2019, 9, 852–871.
- Koppers C, Rinkes IHM, van den Brink GR. Patient-derived organoids from cervical cancer as a platform for precision medicine. Mol Oncol. 2022, 16, 661–676. [CrossRef]
- Cancer Genome Atlas Research Network. Integrated genomic and molecular characterization of cervical cancer. Nature. 2017, 543, 378–384. [CrossRef]
- Duffy MJ, et al. Precision oncology: Biomarkers, companion diagnostics and therapeutic targets. Mol Aspects Med. 2021;72:100832. [CrossRef]
- Topol, EJ. High-performance medicine: the convergence of human and artificial intelligence. Nat Med. 2019, 25, 44–56. [Google Scholar] [CrossRef] [PubMed]
- Esteva A, Robicquet A, Ramsundar B, et al. A guide to deep learning in healthcare. Nat Med. 2021, 27, 766–776. [CrossRef]
- Gao C, Wu P, Yu L, et al. The application of CRISPR/Cas9 system in cervical carcinogenesis. Cancer Gene Ther. 2022;29:466–474. [CrossRef]
- Inturi R, Jemth P. CRISPR/Cas9-based inactivation of human papillomavirus oncogenes E6 or E7 induces senescence in cervical cancer cells. Virology. 2021;562:92–102. [CrossRef]
- Kermanshahi AZ, Ebrahimi F, Taherpoor A, et al. HPV-driven cancers: a looming threat and the potential of CRISPR/Cas9 for targeted therapy. Virol J. 2025;22:156. [CrossRef]
- Kaushal JB, et al. Repurposing Niclosamide for Targeting Pancreatic Cancer by Inhibiting Hh/Gli Non-Canonical Axis of Gsk3β. Cancers. 2021, 13, 3105. [CrossRef]
- Ahmed F, Yang YJ, Samantasinghar A, Kim YW, Ko JB, Choi KH. Network-based drug repurposing for HPV-associated cervical cancer. Comput Struct Biotechnol J. 2023;21:5186–5200. [CrossRef]
- Zhao M, et al. Advances in organoid and CRISPR-based approaches for HPV-related cancer research. Front Oncol. 2019;9:1349. [CrossRef]
- Chakravarthy A, et al. Precision oncology for HPV-associated cancers: a roadmap toward personalized treatment. Lancet Oncol. 2020, 21, e428–e439.
- Bhatia S, et al. Emerging therapies in HPV-associated cancers: opportunities and challenges. J Clin Oncol. 2021, 39, 3359–3370.
Figure 1.
Mechanisms of HPV-induced carcinogenesis via E6 and E7 oncoproteins.Following infection of epithelial cells, high-risk human papillomavirus (HPV) integrates its DNA into the host genome, frequently disrupting the viral E2 gene. Loss of E2 function leads to uncontrolled expression of the viral oncoproteins E6 and E7. E6 promotes ubiquitin-mediated degradation of the tumor suppressor p53 via interaction with E6-associated protein (E6AP), whereas E7 binds and inactivates the retinoblastoma protein (pRb), releasing E2F transcription factors. These events drive continuous cell cycle progression, impair DNA damage responses, and promote genomic instability, ultimately leading to malignant transformation.
Figure 1.
Mechanisms of HPV-induced carcinogenesis via E6 and E7 oncoproteins.Following infection of epithelial cells, high-risk human papillomavirus (HPV) integrates its DNA into the host genome, frequently disrupting the viral E2 gene. Loss of E2 function leads to uncontrolled expression of the viral oncoproteins E6 and E7. E6 promotes ubiquitin-mediated degradation of the tumor suppressor p53 via interaction with E6-associated protein (E6AP), whereas E7 binds and inactivates the retinoblastoma protein (pRb), releasing E2F transcription factors. These events drive continuous cell cycle progression, impair DNA damage responses, and promote genomic instability, ultimately leading to malignant transformation.
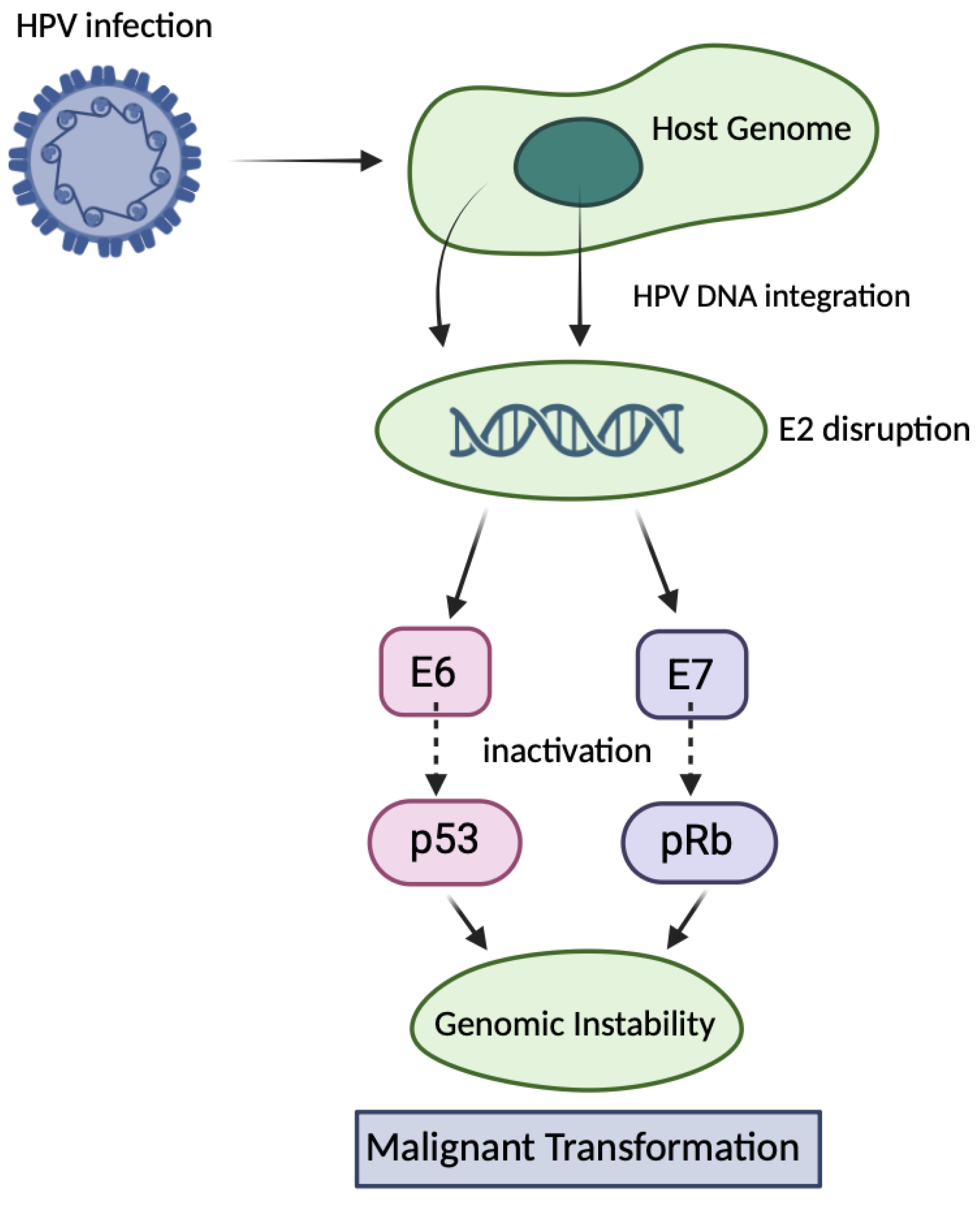
Figure 2.
Mechanism of CRISPR/Cas9-mediated therapeutic targeting of HPV oncogenes. CRISPR/Cas9 introduces double-strand breaks in the HPV genome, leading to disruption of the E6 and E7 genes. The loss of E6/E7 expression restores the activity of tumor suppressor proteins p53 and pRb, resulting in cell cycle arrest, apoptosis, and tumor regression in preclinical models of HPV-associated cancers.
Figure 2.
Mechanism of CRISPR/Cas9-mediated therapeutic targeting of HPV oncogenes. CRISPR/Cas9 introduces double-strand breaks in the HPV genome, leading to disruption of the E6 and E7 genes. The loss of E6/E7 expression restores the activity of tumor suppressor proteins p53 and pRb, resulting in cell cycle arrest, apoptosis, and tumor regression in preclinical models of HPV-associated cancers.
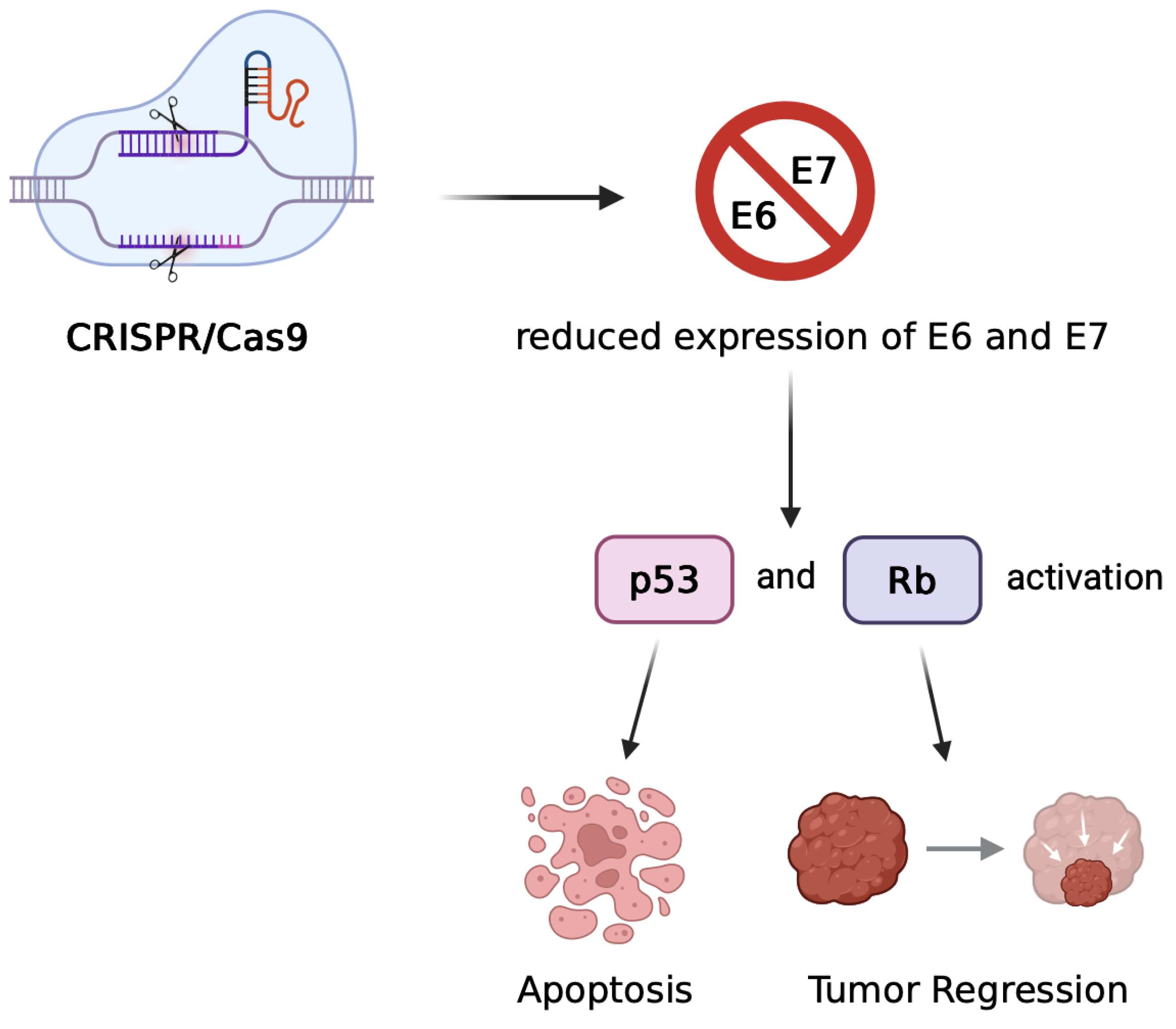
Table 1.
Overview of Therapeutic Strategies Targeting HPV-Driven Cancers.
| Approach | Mechanism | Advantages | Challenges | |
|---|---|---|---|---|
| CRISPR/TALEN | E6/E7 gene disruption → p53/pRb reactivation | Durable effect, tumor suppression | Vector delivery, off-target effects, safety concerns | |
| RNAi | Suppression of E6/E7 mRNA | Transient, no genomic alteration | Short-lived effects, delivery difficulties | |
| Therapeutic Vaccines | Induction of T cell immune response | Immune activation, long-term protection | Limited Phase III data | |
| Small Molecules | Inhibition of oncoprotein complexes | Targeted, direct molecular intervention | Potential off-target effects on normal cellular functions | |
| Nano-therapy | Targeted drug delivery | Increased efficacy, reduced toxicity | Complex manufacturing, safety uncertainties | |
| Organoids + AI | Personalized drug response modeling | Precision medicine, biomarker discovery | Lack of standardization, limited datasets |
Table 2.
Comparison of Representative CRISPR-Based Approaches Targeting HPV Oncogenes.
| Feature | Zheng et al. (2014) | Jubair et al. (2019/2021) |
|---|---|---|
| Model | In vitro (SiHa, CaSki cell lines) | In vivo (HPV16+ tumor-bearing mice) |
| Target | E7 oncogene only | Primarily E7, but also systems targeting both E6 and E7 |
| Delivery Method | Plasmid-based transfection | Systemic delivery via PEGylated liposomes |
| Outcome | Apoptosis induction, pRb restoration, growth arrest | Tumor regression, prolonged survival, efficient genome editing |
| Challenges | Limited to in vitro application | Need for metastatic targeting, off-target risks, vector optimization |
Table 4.
Overview of Investigational and Approved Therapies Targeting HPV Pathways.
| Drug/Therapy | Type | Target/Mechanism | Clinical Phase |
|---|---|---|---|
| Nivolumab | Immune Checkpoint Inhibitor | PD-1 | Approved |
| Decitabine | Epigenetic Drug | DNMT inhibition | Phase II |
| VGX-3100 | DNA Therapeutic Vaccine | E6/E7-specific immune response | Phase III |
| CRISPR-E7 (preclin) | Gene Editing | E7 knockout via Cas9 | Preclinical |
| Curcumin | Natural Compound | NF-κB inhibition, apoptosis induction | Preclinical |
Table 5.
Mechanisms of action of selected anti-HPV therapeutics.
| Drug | Mechanism of Action |
|---|---|
| VGX-3100 | Induces T-cell responses targeting E6/E7 oncoproteins (therapeutic vaccine) |
| Lopinavir/Ritonavir | Protease inhibitor disrupting viral protein function |
| Niclosamide | Downregulates E6/E7 expression; modulates cell signaling pathways |
| Cidofovir | Viral DNA polymerase inhibitor blocking DNA synthesis |
| PRGN-2012 | Induces cellular immune activation against E6/E7 proteins |
| GS-9191 | Topical nucleotide analogue inhibiting viral DNA synthesis |
Table 6.
Selected clinical trials in HPV-related cancers.
| Trial Name | Intervention | Cancer Type | Status |
|---|---|---|---|
| CheckMate-358 | Nivolumab (PD-1) | Cervical, HNSCC | Completed |
| NCT03162224 | CRISPR-Cas9 targeting E7 | Cervical | Recruiting |
| NCT03180684 | VGX-3100 therapeutic vaccine | Cervical lesions | Phase III |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



