
Submitted:
01 August 2025
Posted:
04 August 2025
You are already at the latest version
Abstract
Background/Objectives: The Inhalable Microparticles (IMPs) is part of a currently invading field of medicine. In fact, the anatomical district of Rhinopharynx, represents a bed for many different pathology and infections, where the dimension of drug aerosol Microparticles (MP), represents a discriminating factor to success therapy. The aims of present work are three: 1) Demonstrate the efficacy of the Rinubes device and the aerosol reproducibility in the nebulization of suspensions or solutions to be deposited in the retropharynx; 2) Compare the performance of Rinubes to two other medical devices on the market and ascertain the production of a finer aerosol of the first compared to the latter; 3) Support the point 1 and 2 by reporting the data concerning a human experimentation using the medical device. Materials and Methods: The medical device Rinubes was used in order to demonstrate the reproducibility of aerosol MPs emission. Low Angle Laser Light Scattering (LALLS) method, was used to evaluate both the dimension and distribution of NPs by the medical device “Rinubes”. In the same way, six different API, used usually in Rhinopharynx pathology (N-acetylcysteine, budesonide, sobrerol, beclomethasone dipropionate, thiamphenicol glycinate acetylcysteinate and ipratropium bromide) were compared in order to investigate the dimension of NPs emission through 4 different devices , including Rinubes. The results of retrospective study including 74 subject treated with standard therapy (ST) and inhalation nebulized Sobrerol, were performed. Data regarding the persistance of clinical symptoms (i.e. cough and nasal constipation), were acquired. Results: No significant statistically differences among all the product tested (p>0.05) were addressed. However, only the cloud generated for the Beclomethasone dipropionate showed a significant finer cloud as indicated by a lower MMD value. The 90% of nanoparticles generated by Rinubes insufflator had a volume diameter less than 137 μm. All drugs tested with Rinubes showed a MMD between 52.1 and 69.7 μm. The lowest value of dimension was reported by beclomethasone dipropionate (52.1 μm). Rinubes demonstrated efficacy and robustness in fine nebulization of all pharmaceutical products analyzed indicating that the device is able to be efficient with all types of formulation tested, whether they are cortisone suspensions or solutions with different dosage strength and different composition of excipients. Rinubes, delivered an aerosol cloud with significantly lower MMD (66.3 µm) than Mad Nasal and Spray-sol (142.1 and 116.0 µm respectively), which would allow a higher fraction of drugs deposited in the retropharynx.
Keywords:
inhalation therapy
; micro-particles
; medical device
; low angle laser light scattering
; nasopharyngeal
1. Introduction
Respiratory tract disorders include asthma, chronic obstructive pulmonary disease (COPD), rhinitis due to infections, are a significant health problem worldwide. In 2019, it was estimated that a total of 450 million people suffered from chronic respiratory diseases worldwide causing 4 million deaths, making them the third leading cause of death [1].
The most important diseases affecting the upper airways are rhinitis, rhinosinusitis, otitis, and nasopharyngitis [2,3,4,5]. Acute nasopharyngitis may also include tonsillitis (pharyngotonsillitis) and adenoiditis. These diseases are commonly acute, and the cause is infectious, starting from the nose. Namely, the common cold includes nasopharynx involvement [6]. All these upper airway diseases have common or similar symptoms. Specifically, mucus hypersecretion and defective mucociliary clearance cause mucus accumulation, interfering with airflow passage [7]. Furthermore, chronic inflammation causes turbinate hypertrophy, leading to nasal obstruction [8]. Therefore, the persistence of mucus promotes extraordinary microbial growth, favoring the spread of infection to the paranasal sinuses and middle ear [9]. Posterior rhinorrhea that drips into the pharynx and larynx becomes the trigger for cough; this phenomenon is called postnasal drip and is the onset and cause of rhino-sinus-bronchial syndrome [10]. In particular, nasal function is impaired and significantly affects the lower airways, particularly influencing asthma and sleep [3,5,11]. Thus, the compromised nasal function significantly affects the lower airways [11]. Consequently, a non-patent and non-clean nose promotes, maintains and amplifies respiratory infections and inflammatory diseases [12]. Consequently, an ideal therapy should “open and clean” the nose to ensure the health of the respiratory tract [12]. Therefore, opening and cleaning the nose is the simplest and most useful remedy that can be pursued in daily practice and at all ages. However, the use of clinical treatments is indispensable. The various options include: physical, medical and surgical treatments can control upper airway diseases. Intranasal administration of products and active ingredients represents the safest and most effective way to quickly obtain normal nasal patency, regulate inflammation, fight pathogens and consequently reduce and alleviate nasopharyngeal symptoms [5]. In the opposite side, conventional therapies remain effective up to a certain point and often show limiting aspects, such as: systemic side effects, poor bioavailability of the active ingredient and non-optimal pharmacological targeting. Furthermore, these therapies often do not attain the specific anatomical site [13,14].
Typically, the methods of administering topical nasal treatments can be divided into three main groups which include: irrigation, nebulization and instillation of drops [15]. Specifically, the nebulization technique and the nebulizer medical device appear to have been originally developed to produce micrometric particles sized 2-10 µm, which can deposit within the nasal cavities. More recently, there has been growing interest in the nasal delivery of nanoparticles (NP) and in identifying systems capable of generating these particles [16,17].
Inhaled Nanoparticle therapy (INPT) is a very actual, but also, highly debated topic [14]. Recent technological developments have revolutionized the field of NPs by allowing them to be customized in size, in order to reach the specific anatomical site for the treatment of the pathology, while avoiding non-specific treatment [16,17,18]. Although, NPs conceived as drug carriers, have already been successful (e.g. in oncology) [19,20], the production other submicrometric particles (i.e. < 1 µm) , as well Inhalable Microparticles (IMPs) is part of a currently growing field of medicine [21,22,23,24]. In fact, the anatomical district of rhinopharynx, represents a bed for many different pathology and infections, where the dimension of drug aerosol microparticles (MP), represents a discriminating factor to success therapy [25,26,27,28,29,30,31]. Nasal nebulizers are devices designed to deliver microparticles into the upper airways, showing significant potential to improve airway symptoms.[32]. Current research focuses on the development of advanced formulations of microparticles or droplets containing nanoparticle for intranasal use, with the aim of overcoming biological barriers and improving drug bioavailability [33,34]. NPs, such as chitosan-based nanoparticles, preserve the active principles from degradation, promote their release and absorption, improving the efficacy of vaccines and drugs [35,36]. Furthermore, methodologies have been developed to evaluate the efficiency of NPs delivery by nebulizers, providing an important tool for the evaluation of micro/nanoflow systems in drug delivery [37]. However specific based-evidence seem to confirm that few option are available in order to combine nebulizers producing IMPs of drug production [21,38].
The present work has three main objectives: To demonstrate the efficacy of the Rinubes device (a nebulizer and Medical Device – MD) and its aerosol reproducibility in nebulizing suspensions or solutions targeted for deposition in the retropharynx; To compare the performance of Rinubes with two other medical devices available on the market, evaluating whether Rinubes produces a finer aerosol than the others; To support points 1 and 2 by presenting data from human trials conducted using the Rinubes device.
2. Materials and Methods
2.1. Medical Products
The assessment of particle size distribution by an aerosol of the following six different medicinal products, produced by ADL Farmaceutici nasal insufflator (Rinubes). The experiment included the formulation of the following compounds:
- N-acetylcysteine 300 mg/ 3ml(Fluimucil®, Zambon)
- Budesonide 0.5mg/ 2 ml, (Aircort®, Italchimici)
- Sobrerol 40 mg/ 3 ml (Sobrefluid®, Bayer)
- Beclomethasone dipropionate 0.8 mg / 2 ml (Clenil Aerosol®, Chiesi Farmaceutici)
- Thiamphenicol glycinate acetylcysteinate 0.5 mg/4 ml(Fluimucil antibiotico®, Zambon)
- Ipratropium bromide 0.5 mg / 2 ml (Atem®, Chiesi Farmaeutici)
In a second phase of the work, the assessment of the particle size distribution of an aerosol of Physiological Solution 0.9% Sodium Chloride aerosolized by:
- Rinubes, ADL Farmaceutici
- Mad Nasal, Sakura
- Spray-sol, Buona
- Rinowash, Air Liquide Medical Systems
2.2. Particles Size Assessments
Measurements were performed with a Malvern Instrument laser diffractometer, Spraytec, (Malvern, UK) validated with Duke Standard Uniform Polymer Microspheres 8.9 μm ± 0.4 (batch #248770, Thermo Scientific).
The FDA’s draft guidance recommends the use of laser diffraction to determine the droplet size produced for a given product. Laser diffraction systems, such as Malvern Spraytec, calculate the size of droplets by measuring the intensity of light scattered by particles as a function of angle. The applicable range according to ISO13320:2020 is 0.1 – 3000 μm. The analysis allows the determination of an aerosol particle size distribution directly by spraying the cloud through the laser beam. D[v,0.5] is the Volume Median Diameter (VMD) refers to the midpoint droplet size, where half of the volume of spray is in droplets smaller, and half of the volume is in droplets larger than the mean. The percentiles undersize D[v,0.1] and D[v,0.9], indicating the values of diameter corresponding respectively to 10% and 90% of the droplet population. For the assessment, 3 ml of each drug were introduced in a 5 ml syringe connected to the nasal insufflator. The Rinowash device was filled with 3 ml and connected to a pneumatic aerosol therapy apparatus as reported in the leaflet. A content of a few vials equal to 10 ml was mixed in a becker and 3 ml withdrawn for each analysis. In detail, the compressor employed was Pic AirFamily (Pic Solution). Three measurements were performed for one insufflator characterization for durations of 5 seconds. In the case of Rinowash the sampling period was of 30 s length.
The nasal device loaded with 3 ml of APIs or physiologic solution was positioned on a polystyrene support oriented at a 45°angle and actuated in front of laser. The distance between the orifice of the spray nozzle and the beam path was maintained at 5 cm, while the distance between the spray and the detector window was at 10 cm. Obscuration, a measure of the amount of light scattered by the sample, was in the range 11-16%.
All the data were analysed and used for the PSD curva calculation. Residual value, representing the deviation of the diffraction profile measured from the theoretical model, remained lower than 1% for a good correlation between the experimental data and the model applied for data analysis. Mie theory was employed for the data analysis. It describes the scattering of electromagnetic radiation by spherical particles. It’s a solution to Maxwell’s equations for scattering by a homogeneous sphere and provides a complete angular distribution of scattered light intensity as a function of particle size, refractive index, and the wavelength of incident light. Sample refractive index was 1.51 and for the air was 1.00.
Droplet size varies considerably during a spray event, so the Guidance for Industry – Bioavailability and Bioequivalence Studies for Nasal Aerosols and Nasal Sprays for Local Action (April 2, 2003) recommends the use of data from the fully developed phase to ensure statistically valid comparisons between different products. The fully developed phase can be defined in the data handling software, based on a time window in which all three size parameters (Dv10, Dv50 and Dv90) are stable (plateau of the measurement). Hence, for this reason, the measurements in this work were performed considering all the cloud profiles produced by the 3 ml nebulized.
2.3. Patients
This observational case study was conducted retrospectively through Extracting data previously described in the literature [39]. Inclusion criteria included recruiting subjects over 3 years of age, of either sex, with a history of recurrent respiratory infections. Each physician selected the patients they managed by prescribing Sobrerol. Additionally, each physician included a group of patients with upper respiratory tract infections (AURI) treated only with standard treatment for infections. Exclusion criteria included age under 36 months, epilepsy, severe respiratory insufficiency, uncontrolled asthma, or severe physical debilitation. The following data were harvested for each patient: age, gender, treatment, 4-day symptoms reduction, 7-day symptoms reduction and number of recurrence for patient.
2.4. Treatments
Two groups of patients (comprising a total of 74 subjects), were selected from a larger pool of 177 pharmacologically treated subjects [39]. These two groups included, on the one hand, subjects treated with standard therapy for acute viral infections (ST; 34 subjects). A second group, instead, was nebulized with Sobrerol via the medical device Rinubes (twice a day for 3 days). This treatment regimen was called the Nebulized Sobrerol (NS; 40 subject) group. This therapeutic regimen had to be repeated for each infectious episode.
2.5. Statistical Analyses
The software (GraphPad 8.0 version) for Apple Computer was used for statistical analysis (PRISM, San Diego, CA, USA). All the parameters measured in this study were evaluated by using the classical descriptive statistics of mean, SD, minimum and maximum (for quantitative variables), and frequencies (for qualitative variables). All statistical results were considered significant if the p-value was less than 0.05 (p < 0.05). The Shapiro–Wilk test was performed in order to determine whether the data were parametrically distributed. Both W- and p-values for the BMI data were calculated (W=0.980 and p=0.574). These values justified the implementation of parametric tests for the BMI analyses. Statistical analysis of variance (ANOVA) was performed to determine the significance (p-value) of particle size data among the curves, concerning the comparison among the product and the devices.
3. Results
3.1. Particle Size Distribution of Aerosol Produced by Six Different Drugs, with Rinubes Device
The results presented in Figure 1 show the median mass diameter (MMD) at D[v,0.5] and the percentiles undersize D[v,0.1] and oversized D[v,0.9] of the aerosol particles produced by nebulizing six formulations (six commercial liquid medicinal products) using four different medical devices, i.e. nebulizers. The analysis of particles indicated the values of diameter corresponding respectively to 10% and 90% of the droplet population. No significant statistically differences among all products tested (p>0.05) were evidenced, comparing the results concerning the following values: D[v,0.1], D[v,0.5] and D[v,0.9] (Figure 1). The 90% of droplets generated by Rinubes insufflator had a volume diameter less than 137 μm. All drugs tested with Rinubes showed a MMD between 52.1 and 69.7 μm. The lowest MMD value of dimension was reported by beclomethasone dipropionate (52.1 μm; Figure 1 and Figure 2). Rinubes demonstrated efficacy and robustness in fine nebulization of all pharmaceutical products analyzed indicating that the device is efficient with all types of formulation tested, whether they are cortisone suspensions or solutions with different dosage strength and different composition of excipients. The medical device showed a good reproducibility since the D(v,0.5) RSD was <3% and D(v,0.1) and D(v,0.9) RSD was <5%.
The global mean for all three parameters reported in Figure 1 revealed that Rinubes achieved a consistent production of droplets, as the DV50 differences among the compounds used were not statistically significant (ANOVA test; p > 0.05). In contrast, the differences between the undersized D[v,0.10] and oversized D[v,0.90] particles were statistically significant among products (ANOVA test; p < 0.0001). These data suggested that Rinubes produced a high number of particles with a size , for beclomethasone suitable for the treatment of nasopharyngeal site (Figure 2).
3.2. Particle Size Distribution of Aerosol Produced by Saline Solution, with Three Different Nasal Devices
In order to compare the four different nebulizing devices, saline solution was aerosolized using different nasal insufflators.
Three of them were constituted of a rubber nebulizer head attached to a syringe. They differed for the size and number of holes nebulizing the liquid. In parallel a nasal douche was tested since considered a mature and used technology.
The devices provided different performance in emitted droplet size. The 90% of microparticles had a volume diameter less than 284.8 μm when emitted from MadNasal, 130 μm from the Rinowash, 138.4 μm those emitted from Rinubes, 235.1 μm those emitted from Spray-sol and. The ANOVA test revealed that among all four devices the are statistical different (p<0.001) concerning the production of microparticles concerning the parameter D[v,0.50] (Figure 4).
The plume generated saline solution tested with Mad Nasal and Spray-sol showed a MMD of 142.1 μm and 116.0 μm, respectively. On the contrary, Rinubes produced a finer plume with MMD of 66.1 μm. Rinowash, which has a different mechanism of aerosol production reveled the lowest value of MMD (i.e., 30 μm: Figure 3). The dimension of areosol-particles of saline solution from four different devices are illustrated in Figure 3.
Rinowash is a nasal irrigation product that has to be connected a traditional pneumatic compressor for aerosol therapy with generated a air flow of 15-20 L/min and it allows a complete treatment of the upper airways in 1/3 minutes. It is reported that it generates particles with a diameter greater than 10 microns, it acts exclusively at the level of the upper airways and nebulizes 5 ml of solution in one minute. The generation of finer particles by this nasal shower is due to the more efficient thrust that the compressor imparts to the liquid compared to the force that is generated manually using a syringe with the nebulizer attached. On the other hand, this system is more sophisticated, requires electricity and a more detailed understanding of the procedure for using and cleaning the device
Finally, for all the manually activated devices (Mad Nasal, Spray-sol and Rinubes) there wasn’t a fraction of particle less than 10 microns. Hence, the data show that all the aerosol generated are of a size not suitable to be inhaled and reach the lungs. The plume produced is specifically useful for the treatment of the upper airways. Thus, the aerosol size distribution demonstrated to be suitable for a nasal deposition avoiding the penetration of droplets in the lungs. Rinowash, producing a finer cloud, generated about 9.5% of droplets < 10 µm, potentially capable to reach the lungs. It was specified in the introduction that the particles must be fine to reach the nasopharynx. For this reason we analyzed the portion of generated droplets between 10-30 µm because it is potentially more effective for the therapy. In this sense, the measured fraction corresponded to 0.34 and 2.14 % for Spray sol and Mad-nasal respectively while it reached 7.18 for Rinubes, indicating a more efficient generation of fine particles for this device. In line with what emerged from the MMD data, Rinowash showed a consistent fraction below 30 µm and equal to 51.6%. Among the manually activated devices, Rinubes showed the lowest MMD values indicating the higher probaibility of droplets to deposit in the rino pharingz portion. At the same time since no particles were generated with size < 10µm the risk of particles directed to the lungs is minimised.
3.3. Results of Patients Treated with ST and NS
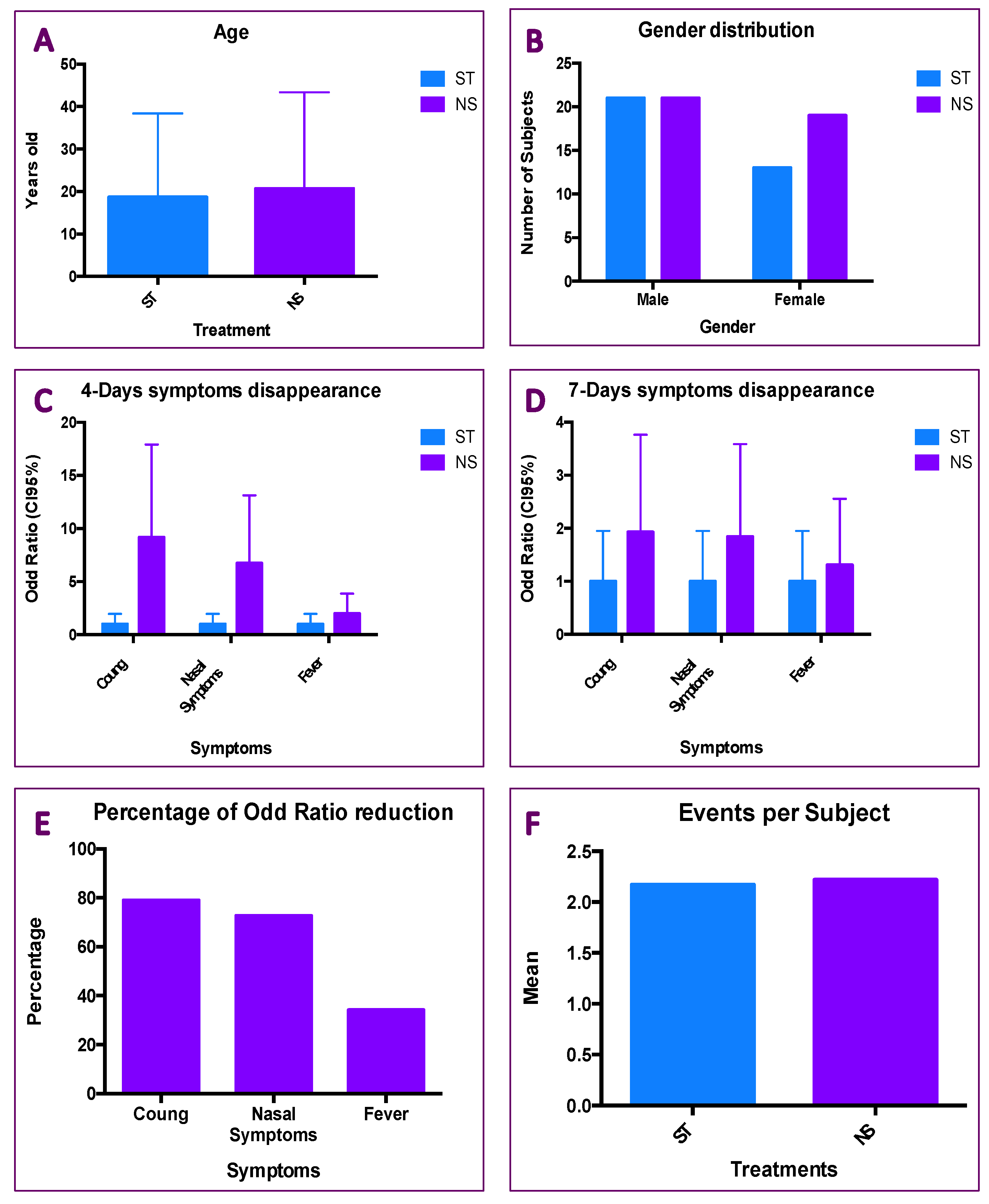
The two subgroups mentioned above, investigated in this retrospective study (ST vs NS) showed a similar distribution concerning the mean age and the gender distribution. In particular in ST group the mean age was equal to 18.70 ± 3.377, while, the NS showed a mean age equal to 20.70 ± 3.377 (Figure 5A). Nonetheless, the gender distribution revealed an equal distribution of M/F ratio among the treatment. Inside ST group there were 21 males out of 34 subjects, indeed in NS group there were 21 male out of 40 subjects (Figure 5B). The unpaired Student’s test (Figure 5A and the Fisher’s test (Figure 5B), revealed not statistical differences among the treatments (Figure 5A; p=o.6857 and Figure 5B; p=0.4847).
The ST group was considered as reference group, then the Odd Ratio (OR) concerning for three parameters (i.e. cough, nasal symptoms and fever) were calculated. The ORs for symptoms disappearance at 4 day were 9.18, 6.73 and 1.99 for the cough, nasal symptoms and fever, respectively (Figure 5C; p<0.0001). The ORs for symptoms disappearance at 7 day were 1.93, 1.94 and 1.31 (Figure 5D; p<0.0001), for the cough, nasal symptoms and fever, respectively. Comparing the ORs in NS group a significant reduction of them was observed for the cough (-78.98%), for the nasal symptoms (72.66), but not for the fever (-34.18%; Figure 5E). The results indicate that NS therapy effectively reduces cough and nasal symptoms as early as day four, with a significantly higher OR compared to the control treatment. The NS treatment also shows up to two times greater efficacy on cough compared to the control treatment four days after starting treatment (Figure 5C). By day seven, the OR values decrease by up to 78% (Figure 5D), but remain in line with the OR observed for fever and still maintain a high ratio compared to the control treatment (Figure 5E). Finally, no difference in terms of symptoms per patients, were observed (ST=2.17; NS=2.22). The data of NS treatment seem to indicate that the treatment affects the three symptoms invstigate in an independent manner. No association among the age, gender or events per patient, was found.
4. Discussion
Rhinosinusitis is a widespread disease worldwide, resulting in significant costs to society in terms of healthcare costs and lost productivity due to work absence [40]. Acute rhinosinusitis (ARS) has an annual prevalence of 6-15% and is usually the consequence of a viral common cold. ARS is usually a self-limiting disease, but serious complications have been described, leading to life-threatening situations and even death [41]. It is one of the most common causes of antibiotic prescription, and proper management is extremely important in the context of the global antibiotic resistance crisis. Chronic rhinosinusitis (CRS) is a significant health problem, affecting 5-12% of the general population [42]. All conditions affecting the upper airways (i.e. rhinitis, rhinosinusitis, otitis, and nasopharyngitis) are dangerus for the health [2,3,4,5]. So far, acute nasopharyngitis may also include tonsillitis (pharyngotonsillitis) and adenoiditis. All these conditions present themselves in acute trait. Indeed, they are located as nasopharynx involvements [6]. Symptoms of ARS or similar conditions, often last a few days, but no more than a week, but cough persists longer and can often lead to a reduction in quality of life [43]. In this regard, cough can be associated with two opposing situations: excessive mucus production or reduced mucus secretion. These two conditions essentially translate into a productive cough and a dry cough. Both types of cough require appropriate treatment. Mucus does indeed have protective and beneficial effects, but if overproduced, it has harmful effects [44] Therefore, a goal in managing patients with cough is to ensure adequate mucus production, meaning that it is neither excessive nor insufficient [45]. In this regard, Sobrerol is a mucoactive agent with additional activities that may be beneficial to patients with ARS.. Current clinical experience in primary care has shown some interesting results. Pharmacological, medical, and surgical treatments can certainly treat upper airway diseases (ARDs). Intranasal administration of active ingredients represents the fastest, safest, and most effective method to rapidly restore normal nasal space, reduce inflammation, fight pathogens, and ultimately alleviate symptoms [5]. Precisely, because of this ease of immediate treatment, from the outside in, not only have new pharmacological applications been developed [22,35], but the methods of administration have also grown enormously [14,17,32,34,36]. Focusing on this point carefully, inhaled nanoparticle therapy (INPT) is a very current, but also much debated topic [33]. However, it should be noted that confusion can arise when talking about inhaled particles based on their size [5,16,22,27]. It is important to underline for this reason that size makes a difference in reaching the target site for treatment [4,5]. For this reason, this work took into consideration the size of the particles in relation to the specific treatment site. Our results highlight that particle size is important for effectively treating ARS symptoms. Specifically, we compared four devices that demonstrated efficacy in producing the micron-sized particles needed for the specific treatment of these upper respiratory tract conditions [30,31,34]. Particle size must not be too small to enter the lungs [16,26] or too large to effectively noreach the retropharynx [11]. In particular, one of the devices used (i.e., Rinubes) has been shown to produce micrometric particles of the appropriate diameter. In particular, one of the devices used (i.e., Rinubes) produced micrometric particles of the appropriate diameter. The size of these particles produced by the Rinubes medical device is consistent with those used for pharmacological treatment through the nasal cavities [33]. Nonetheless, The above-mentioned pathological conditions are often accompanied by mucus overproduction or reduced mucus secretion. These two manifestations are two different situations: a productive cough and a dry cough, respectively. Both types of cough require appropriate treatment. Mucus does indeed have protective and beneficial effects, but if overproduced, it has harmful effects [39]. Therefore, a goal in managing patients with cough is to ensure adequate mucus production, meaning that it is neither excessive nor insufficient [45]. In this regard, Sobrerol is a mucoactive agent with additional activities that may be beneficial for patients with upper respiratory tract infections [46]. The results reported in Figure 5, showed the bigger effect of nebulizer Sobrerol (NS) in front of the standard treatment (ST). Nevertheless, the OR of NS group (against the cough), shower the highest value in disappearance of symptoms after 4 days (Figure 5C) and 7 days (Figure 5D). Finally, the two group of patients were homogenous looking for the Age, gender distribution and number of events per patients. Herein, the results seem not associated with the demographic data of patients.
5. Conclusions
Improved techniques for the administration of inhalable NPs (INPAD) and specially inhalable Micro Particles IMPs represent a significant progress in overcoming biological and anatomical barriers in controlling drug release at the specific site, as nasopharyngeal. The challenges of nasopharyngeal pathologies offer promising opportunities for the development of non-invasive drug delivery. The sub category of IMPs offers several advantages, including precise targeting of drugs in the nasal pharynx, improved drug absorption and bioavailability, and reduced systemic side effects. The results of patients reported in these analyses seem to validate the combination of medical device and drug Sobrerol, with respect to the control treatment. The medical device “Rinubes” seems to be able to be used for the diffusion of a wide range of pharmacological agents and consolidate a controlled and reproducible release of the drug, which is essential for achieving the therapeutic result.
6. Patents
- (1)
- Utility Model No. 202020000003820 IMPROVED NASAL NEBULIZER
- (2)
- Italian Patent for Industrial Invention No. 102020000015844 – USE OF SALT-BROMINE-IODINE WATERS FOR THE NASAL TREATMENT OF INFLAMMATION IN THE THREE AREAS OF THE UPPER AIRWAYS AND MEDICAL DEVICES ADAPTED FOR SUCH TREATMENT.
- (3)
- European Patent Application for Industrial Invention No. 21748658.8 – USE OF SALT-BROMINE-IODINE WATERS FOR THE NASAL TREATMENT OF THE INFLAMMATION OF THE THREE AREAS OF THE UPPER AIRWAYS AND MEDICAL DEVICES ADAPTED TO SUCH A TREATMENT.
Author Contributions
Conceptualization, E.Q.; F.B. and Prof. A.V.; methodology, E.Q.; F.B; software, I.L.M; Dr. A.V.; validation, E.Q.; L.G.; formal analysis, L.G.; E.Q.; N.F. and Prof. A.V. investigation, L.G.; Dr. A.V.; resources, I.L.M.; data curation, N.F.; Dr. A.V.; writing—original draft preparation, N.F.; F.B.; writing—review and editing, N.F.; E.Q.; F.B. and Prof. A.V.; visualization, Prof. A.V. and M.M. supervision, M.M.; project administration, M.M.; funding acquisition, Prof A.V. and I.L.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not Necessary. The study complies with the Declaration of Helsinki and was approved by the independent review committee of the Italian Upper Airway Association (AIVAS). The review committee stated that patient consent was not required for reviewing medical records, as the anonymity of the data and the confidentiality of data collection were guaranteed.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data included in this study will be made available upon request. The data owners are: Dr. Eride Quarta; Professors Francesca Buttini and Attilio Varricchio.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Momtazmanesh, S.; Moghaddam, S.S.; Ghamari, S.-H.; Rad, E.M.; Rezaei, N.; Shobeiri, P.; Aali, A.; Abbasi-Kangevari, M.; Abbasi-Kangevari, Z.; Abdelmasseh, M.; et al. Global Burden of Chronic Respiratory Diseases and Risk Factors, 1990–2019: An Update from the Global Burden of Disease Study 2019. eClinicalMedicine 2023, 59, 101936. [Google Scholar] [CrossRef]
- Wise, S.K.; Damask, C.; Greenhawt, M.; Oppenheimer, J.; Roland, L.T.; Shaker, M.S.; Wallace, D.V.; Lang, D.M. A Synopsis of Guidance for Allergic Rhinitis Diagnosis and Management From ICAR 2023. J. Allergy Clin. Immunol. Pract. 2023, 11, 773–796. [Google Scholar] [CrossRef]
- Ciprandi, G.; Tosca, M.A. Turbinate Hypertrophy, Allergic Rhinitis, and Otitis Media. Curr. Allergy Asthma Rep. 2021, 21, 44. [Google Scholar] [CrossRef]
- Fokkens, W.J.; Lund, V.J.; Hopkins, C.; Hellings, P.W.; Kern, R.; Reitsma, S.; Toppila-Salmi, S.; Bernal-Sprekelsen, M.; Mullol, J.; Alobid, I.; et al. European Position Paper on Rhinosinusitis and Nasal Polyps 2020. Rhinol. J. 2020, 0, 1–464. [Google Scholar] [CrossRef]
- Varricchio, A.; Presutti, L.; La Mantia, I.; Ciprandi, G. Inter-Societal Delphi Consensus on the Topical Nasal Treatments in Italy. Multidiscip. Respir. Med. 2024, 19, 2. [Google Scholar] [CrossRef]
- Eccles, R. Common Cold. Front. Allergy 2023, 4, 1224988. [Google Scholar] [CrossRef]
- Bansil, R.; Turner, B.S. The Biology of Mucus: Composition, Synthesis and Organization. Adv. Drug Deliv. Rev. 2018, 124, 3–15. [Google Scholar] [CrossRef]
- Karkouli, G.; Douros, K.; Moriki, D.; Moutsatsou, P.; Giannopoulou, I.; Maratou, E.; Koumpagioti, D. Dysfunctional Breathing in Children: A Literature Review. Children 2024, 11, 556. [Google Scholar] [CrossRef]
- Taherali, F.; Varum, F.; Basit, A.W. A Slippery Slope: On the Origin, Role and Physiology of Mucus. Adv. Drug Deliv. Rev. 2018, 124, 16–33. [Google Scholar] [CrossRef]
- Keicho, N.; Hijikata, M.; Miyabayashi, A.; Wakabayashi, K.; Yamada, H.; Ito, M.; Morimoto, K. Impact of Primary Ciliary Dyskinesia: Beyond Sinobronchial Syndrome in Japan. Respir. Investig. 2024, 62, 179–186. [Google Scholar] [CrossRef]
- Ciprandi, G.; Cirillo, I. The Lower Airway Pathology of Rhinitis. J. Allergy Clin. Immunol. 2006, 118, 1105–1109. [Google Scholar] [CrossRef]
- Ciprandi, G.; Gelardi, M. Open and Clean: The Healthy Nose. Acta Bio Medica Atenei Parm. 2019, 90. [Google Scholar] [CrossRef]
- Https://Www.Nobelprize.Org/Prizes/Chemistry/1925 /Summary/.
- Cojocaru, E.; Petriș, O.R.; Cojocaru, C. Nanoparticle-Based Drug Delivery Systems in Inhaled Therapy: Improving Respiratory Medicine. Pharmaceuticals 2024, 17, 1059. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Serrano, A.; Martínez-Campos, P.; Seijoso-González, L.; Ruiz-Rojo, H. Revisión narrativa de la técnica de los lavados nasales en pediatría. Enferm. Clínica 2021, 31, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Forest, V.; Pourchez, J. Nano-Delivery to the Lung - by Inhalation or Other Routes and Why Nano When Micro Is Largely Sufficient? Adv. Drug Deliv. Rev. 2022, 183, 114173. [Google Scholar] [CrossRef] [PubMed]
- Hami, Z. A Brief Review on Advantages of Nano-Based Drug Delivery Systems. Ann. Mil. Health Sci. Res. 2021, 19. [Google Scholar] [CrossRef]
- Jin, Z.; Gao, Q.; Wu, K.; Ouyang, J.; Guo, W.; Liang, X.-J. Harnessing Inhaled Nanoparticles to Overcome the Pulmonary Barrier for Respiratory Disease Therapy. Adv. Drug Deliv. Rev. 2023, 202, 115111. [Google Scholar] [CrossRef]
- Dinakar, Y.H.; Karole, A.; Parvez, S.; Jain, V.; Mudavath, S.L. Organ-Restricted Delivery through Stimuli-Responsive Nanocarriers for Lung Cancer Therapy. Life Sci. 2022, 310, 121133. [Google Scholar] [CrossRef]
- Leong, E.W.X.; Ge, R. Lipid Nanoparticles as Delivery Vehicles for Inhaled Therapeutics. Biomedicines 2022, 10, 2179. [Google Scholar] [CrossRef]
- Zhang, X.; Yan, S.; Wu, J.; Xi, Y.; Ma, J.; Wu, C.; Zhang, S.; Chen, X.D.; Wu, W.D. Enhancing Blending Efficiency and in Vitro Aerosol Performance of Low-Dose Inhalable Dry Powders with Spray Freeze Dried Microparticles. Eur. J. Pharm. Biopharm. 2025, 212, 114740. [Google Scholar] [CrossRef]
- Ullah, F.; Sabei, F.Y.; Shah, K.U.; Safhi, A.Y.; Bakkari, M.A.; Madkhali, O.A.; Albariqi, A.H.; Saeed, M.D.; Ramzan, M. Inhalable Microparticles Embedding Hyaluronic Acid–Coated Chitosan Nanoparticles: Fabrication and Evaluation for Preferential Accumulation of Montelukast in the Lung. J. Microencapsul. 2025, 1–12. [Google Scholar] [CrossRef]
- Kuntic, M.; Kuntic, I.; Cleppien, D.; Pozzer, A.; Nußbaum, D.; Oelze, M.; Junglas, T.; Strohm, L.; Ubbens, H.; Daub, S.; et al. Differential Inflammation, Oxidative Stress and Cardiovascular Damage Markers of Nano- and Micro-Particle Exposure in Mice: Implications for Human Disease Burden. Redox Biol. 2025, 83, 103644. [Google Scholar] [CrossRef]
- Liu, H.; Sun, Y.; Cai, S.; Zhao, C.; Xu, X.; Xu, A.; Zhou, H.; Yang, C.; Gu, X.; Ai, X. Formononetin-Loaded PLGA Large Porous Microparticles via Intratracheal Instillation for Bleomycin-Induced Pulmonary Fibrosis Treatment. AAPS PharmSciTech 2025, 26, 112. [Google Scholar] [CrossRef]
- Song, L.; Zhai, Z.; Ouyang, W.; Ding, J.; Wang, S.; Li, S.; Liang, M.; Xu, F.; Gao, C. Inhalation of Macrophage Membrane-Coated Hydrogel Microparticles for Inflammation Alleviation of Acute Lung Injury in Vivo. Acta Biomater. 2025, 192, 409–418. [Google Scholar] [CrossRef]
- Farnoud, A.; Tofighian, H.; Baumann, I.; Ahookhosh, K.; Pourmehran, O.; Cui, X.; Heuveline, V.; Song, C.; Vreugde, S.; Wormald, P.-J.; et al. Numerical and Machine Learning Analysis of the Parameters Affecting the Regionally Delivered Nasal Dose of Nano- and Micro-Sized Aerosolized Drugs. Pharmaceuticals 2023, 16, 81. [Google Scholar] [CrossRef]
- Biglarian, M.; MomeniLarimi, M.; Firoozabadi, B.; Inthavong, K.; Farnoud, A. Targeted Drug Delivery with Polydisperse Particle Transport and Deposition in Patient-Specific Upper Airway during Inhalation and Exhalation. Respir. Physiol. Neurobiol. 2023, 308, 103986. [Google Scholar] [CrossRef]
- Shang, Y.; Dong, J.; Inthavong, K.; Tu, J. Comparative Numerical Modeling of Inhaled Micron-Sized Particle Deposition in Human and Rat Nasal Cavities. Inhal. Toxicol. 2015, 27, 694–705. [Google Scholar] [CrossRef]
- Schroeter, J.D.; Tewksbury, E.W.; Wong, B.A.; Kimbell, J.S. Experimental Measurements and Computational Predictions of Regional Particle Deposition in a Sectional Nasal Model. J. Aerosol Med. Pulm. Drug Deliv. 2015, 28, 20–29. [Google Scholar] [CrossRef]
- Farhadi Ghalati, P.; Keshavarzian, E.; Abouali, O.; Faramarzi, A.; Tu, J.; Shakibafard, A. Numerical Analysis of Micro- and Nano-Particle Deposition in a Realistic Human Upper Airway. Comput. Biol. Med. 2012, 42, 39–49. [Google Scholar] [CrossRef]
- Heritage; Brook; Underdown; McDERMOTT Intranasal Immunization with Polymer-grafted Microparticles Activates the Nasal-associated Lymphoid Tissue and Draining Lymph Nodes. Immunology 1998, 93, 249–256. [CrossRef] [PubMed]
- Huang, Z.; Wu, H.; Yang, B.; Chen, L.; Huang, Y.; Quan, G.; Zhu, C.; Li, X.; Pan, X.; Wu, C. Anhydrous Reverse Micelle Nanoparticles: New Strategy to Overcome Sedimentation Instability of Peptide-Containing Pressurized Metered-Dose Inhalers. Drug Deliv. 2017, 24, 527–538. [Google Scholar] [CrossRef] [PubMed]
- Clementino, A.R.; Pellegrini, G.; Banella, S.; Colombo, G.; Cantù, L.; Sonvico, F.; Del Favero, E. Structure and Fate of Nanoparticles Designed for the Nasal Delivery of Poorly Soluble Drugs. Mol. Pharm. 2021, 18, 3132–3146. [Google Scholar] [CrossRef] [PubMed]
- Clementino, A.; Climani, G.; Bianchera, A.; Buttini, F.; Sonvico, F. Polysaccharides: New Frontiers for Nasal Administration of Medicines. Polysaccharides 2025, 6, 6. [Google Scholar] [CrossRef]
- Shim, S.; Yoo, H.S. The Application of Mucoadhesive Chitosan Nanoparticles in Nasal Drug Delivery. Mar. Drugs 2020, 18, 605. [Google Scholar] [CrossRef]
- Canelli, E.; Ferrari, L.; Borghetti, P.; Candela, F.; Abiakam, N.S.; Bianchera, A.; Buttini, F.; Magi, G.E.; Sonvico, F.; Martelli, P.; et al. Nano-Adjuvanted Dry Powder Vaccine for the Mucosal Immunization against Airways Pathogens. Front. Vet. Sci. 2023, 10, 1116722. [Google Scholar] [CrossRef]
- Komalla, V.; Wong, C.Y.J.; Sibum, I.; Muellinger, B.; Nijdam, W.; Chaugule, V.; Soria, J.; Ong, H.X.; Buchmann, N.A.; Traini, D. Advances in Soft Mist Inhalers. Expert Opin. Drug Deliv. 2023, 20, 1055–1070. [Google Scholar] [CrossRef]
- Reddy, K.P.; Naraharisetti, L.T.; Prasanna, V.S.; Babu, S.S.; Ehsan, I.; Godugu, C.; Datta, P. Excipient-Free Inhalable Combination Shell-Core Microparticles with Clofazimine as Shell for Extended Pulmonary Retention of Isoniazid in Core. Int. J. Pharm. 2025, 672, 125310. [Google Scholar] [CrossRef]
- Varricchio, A.; Ciprandi, G. Sobrerol in Managing Acute Respiratory Infections in Clinical Practice During the “Cold” Season: An Italian Primary Care Experience. Int. J. Gen. Med. 2024, Volume 17, 5471–5477. [Google Scholar] [CrossRef]
- Sidell, D.; Shapiro, N.L.; Bhattacharyya, N. Obesity and the Risk of Chronic Rhinosinusitis, Allergic Rhinitis, and Acute Otitis Media in School-age Children. The Laryngoscope 2013, 123, 2360–2363. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, M.J.; Chiu, E.J.; Landgraf, J.M.; Gliklich, R.E. The Health Impact of Chronic Recurrent Rhinosinusitis in Children. Arch. Otolaryngol. Neck Surg. 2000, 126, 1363. [Google Scholar] [CrossRef]
- Haruna, S.; Sawada, K.; Nakajima, T.; Moriyama, H. Relationship between Pediatric Sinusitis and Middle Turbinate Pneumatization—Ethmoidal Sinus Pyocele Thought to Be Caused by Middle Turbinate Pneumatization. Int. J. Pediatr. Otorhinolaryngol. 2005, 69, 375–379. [Google Scholar] [CrossRef]
- Lovie-Toon, Y.G.; Chang, A.B.; Newcombe, P.A.; Vagenas, D.; Anderson-James, S.; Drescher, B.J.; Otim, M.E.; O’Grady, K.-A.F. Longitudinal Study of Quality of Life among Children with Acute Respiratory Infection and Cough. Qual. Life Res. 2018, 27, 891–903. [Google Scholar] [CrossRef]
- Hill, D.B.; Button, B.; Rubinstein, M.; Boucher, R.C. Physiology and Pathophysiology of Human Airway Mucus. Physiol. Rev. 2022, 102, 1757–1836. [Google Scholar] [CrossRef] [PubMed]
- Volsko, T.A. Airway Clearance Therapy: Finding the Evidence. Respir. Care 2013, 58, 1669–1678. [Google Scholar] [CrossRef] [PubMed]
- Ciprandi, G.; Varriccchio, A. Sobrerol: New Perspectives to Manage Patients with Frequent Respiratory Infections. Children 2023, 10, 1210. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Analyses of Dimension of particles areosol-derived from Rinubes device. A) N-acetylcysteine ; B) Budesonide 0,5mg ; C) Sobrerol ; D) Beclomethasone dipropionate ; E) Thiamphenicol glycinate acetylcysteinate ; F) Ipratropium bromide .
Figure 1.
Analyses of Dimension of particles areosol-derived from Rinubes device. A) N-acetylcysteine ; B) Budesonide 0,5mg ; C) Sobrerol ; D) Beclomethasone dipropionate ; E) Thiamphenicol glycinate acetylcysteinate ; F) Ipratropium bromide .
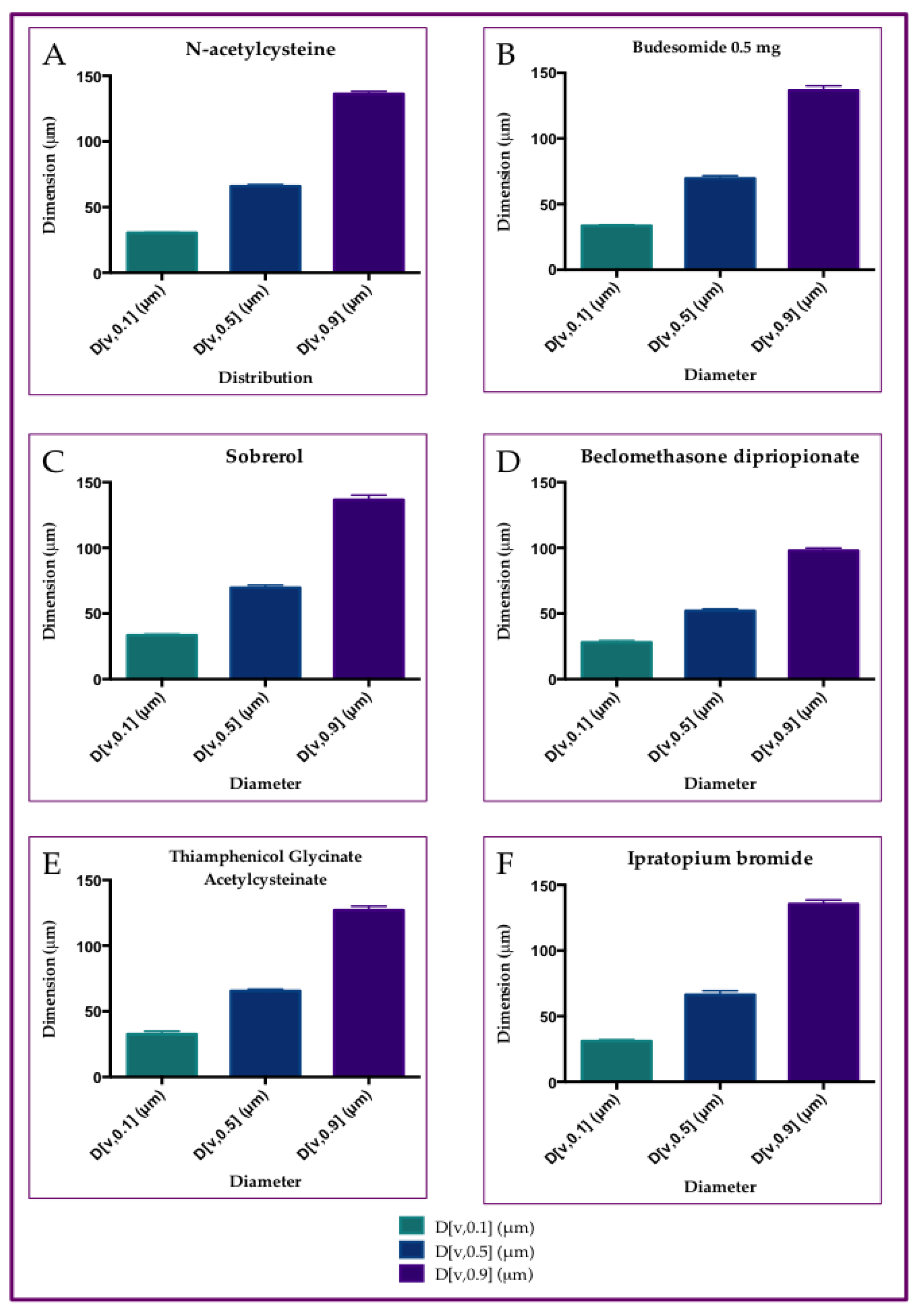
Figure 2.
Cumulative analyses concerning the six API tested. A) Average and standard deviation results of size distribution for the six tested drugs with Rinubes. B) ANOVA analyses of particle size distribution (PSD). No statistical difference was observed among the products (p>0.05, While, statistical difference wasobserved among the dimensions of size distribution.
Figure 2.
Cumulative analyses concerning the six API tested. A) Average and standard deviation results of size distribution for the six tested drugs with Rinubes. B) ANOVA analyses of particle size distribution (PSD). No statistical difference was observed among the products (p>0.05, While, statistical difference wasobserved among the dimensions of size distribution.
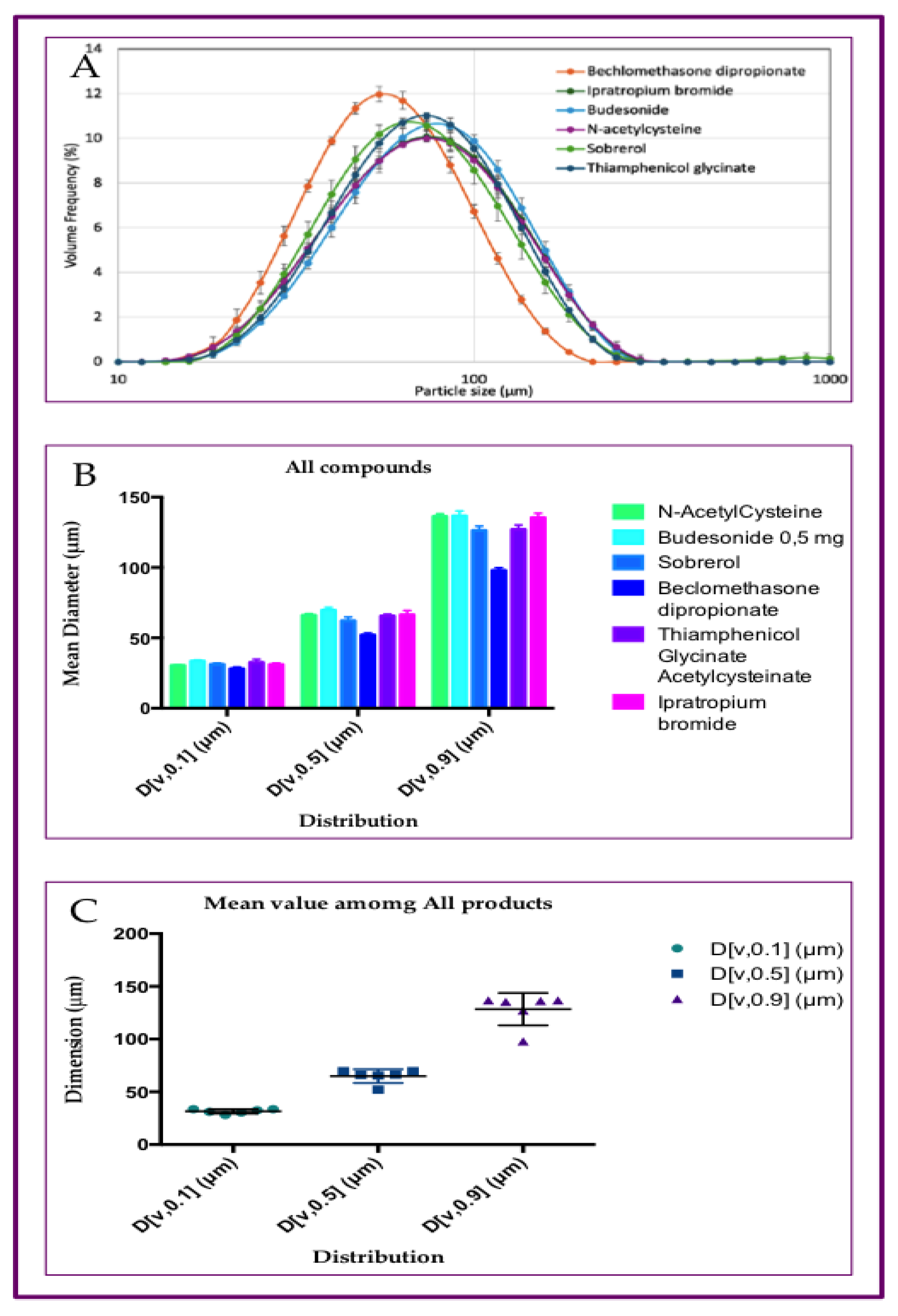
Figure 3.
Dimension of areosol- particles of saline solution from four different devices:. A) Mad Nasal; B)Rinowash; C) Rinubes; D) Spay-sol ;.
Figure 3.
Dimension of areosol- particles of saline solution from four different devices:. A) Mad Nasal; B)Rinowash; C) Rinubes; D) Spay-sol ;.

Figure 4.
Cumulative analyses concerning the four devices tested. A) Plotter concerning dimension and frequency of particles; B) ANOVA analyses of distribution.; C) mean value analyses among tested medical devices; Statistical difference were observed among the products (p<0.001) and the distribution of microparticles (p<0.001).
Figure 4.
Cumulative analyses concerning the four devices tested. A) Plotter concerning dimension and frequency of particles; B) ANOVA analyses of distribution.; C) mean value analyses among tested medical devices; Statistical difference were observed among the products (p<0.001) and the distribution of microparticles (p<0.001).
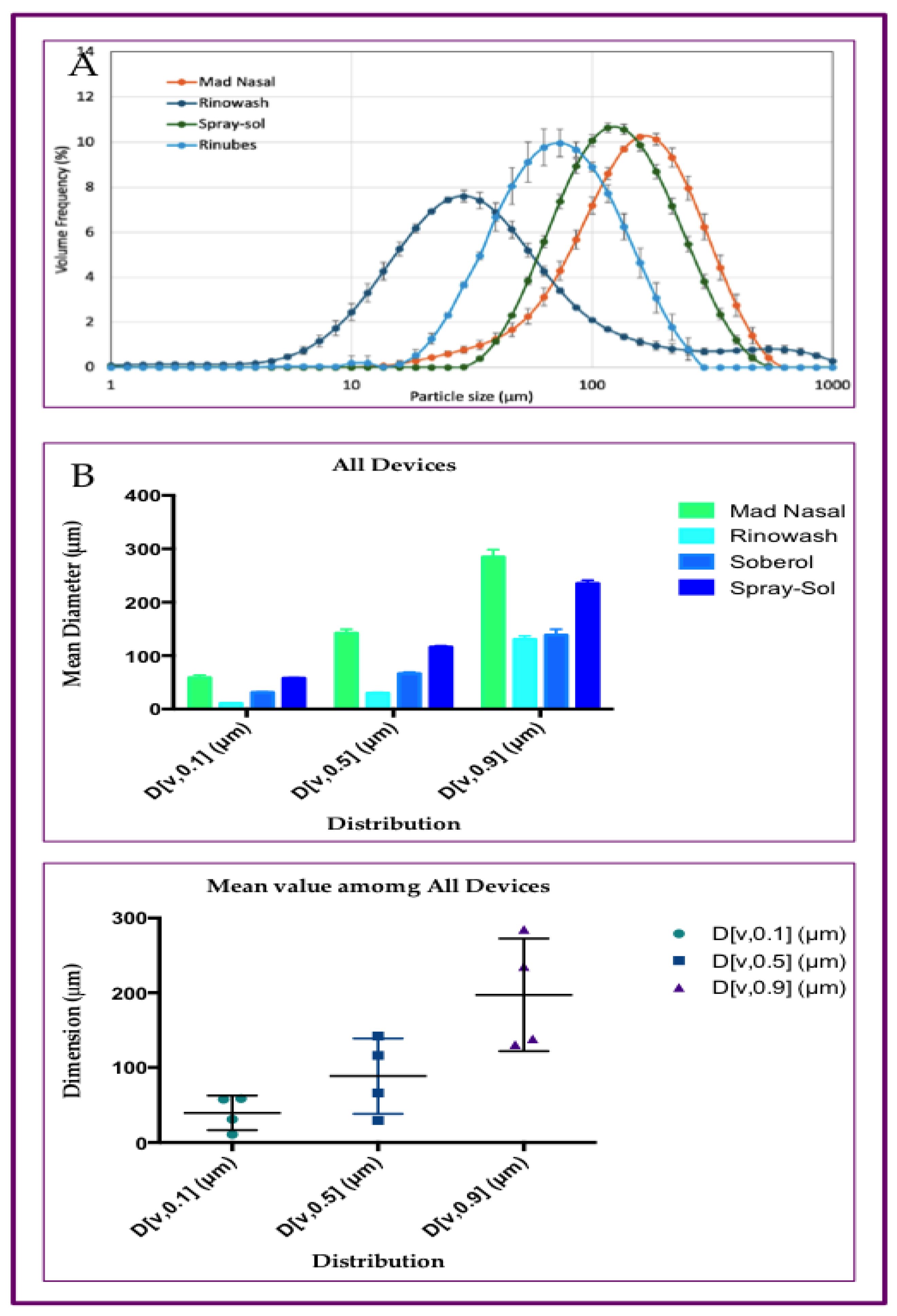
Figure 5.
Characteristics and analyses of cohort of patients. Among the subgroup previously published the focused analyses included 74 out of subject (41.80%) of treated patients. Thirty-four of them were treated with Standard Treatment (ST), while Forty subjects were treated with Nebulizer Sobrerol (NS). A) Age distribution: ST= Standard Therapy; NS=Nebulizer. No significant statistical differences were found by The Student’s Test application (p=0.6857). B) Gender distribution: ST= Standard Therapy; NS=Nebulizer; No significant statistical differences were found by Chi-square Test application (p=0.4847). C) Disappeared symptoms after 4 days: ST= Standard Therapy; NS=Nebulizer; Significant statistical differences were found by ANOVA Test application, concerning the differences among the treatment (p<0.0001) and the differences among the symptoms (p<0.001). D) Disappeared symptoms after 7 days: ST= Standard Therapy; NS=Nebulizer; Significant statistical differences were found by ANOVA Test application, concerning the differences among the treatment (p<0.0001), while not statistical difference were found among the symptoms (p<0.3302). E) Percentage of Odd Ratio (OR) reduction in symptoms (in percentage). The different of Odd Ratio (OR; CI 95%) expressed in percentage were calculate as (OR4Days-OR7Day)/ OR 4Days. Greater differences were evaluated for the cough and nasal symptoms, while the fever symptom report lowest percentage reduction. F) Number of infection recurrence (IR): Number of mean IR for subject; ST= Standard Therapy; NS=Nebulizer, No significant statistical differences (Ns) were found byThe Student’s Test application (p=Ns).
Figure 5.
Characteristics and analyses of cohort of patients. Among the subgroup previously published the focused analyses included 74 out of subject (41.80%) of treated patients. Thirty-four of them were treated with Standard Treatment (ST), while Forty subjects were treated with Nebulizer Sobrerol (NS). A) Age distribution: ST= Standard Therapy; NS=Nebulizer. No significant statistical differences were found by The Student’s Test application (p=0.6857). B) Gender distribution: ST= Standard Therapy; NS=Nebulizer; No significant statistical differences were found by Chi-square Test application (p=0.4847). C) Disappeared symptoms after 4 days: ST= Standard Therapy; NS=Nebulizer; Significant statistical differences were found by ANOVA Test application, concerning the differences among the treatment (p<0.0001) and the differences among the symptoms (p<0.001). D) Disappeared symptoms after 7 days: ST= Standard Therapy; NS=Nebulizer; Significant statistical differences were found by ANOVA Test application, concerning the differences among the treatment (p<0.0001), while not statistical difference were found among the symptoms (p<0.3302). E) Percentage of Odd Ratio (OR) reduction in symptoms (in percentage). The different of Odd Ratio (OR; CI 95%) expressed in percentage were calculate as (OR4Days-OR7Day)/ OR 4Days. Greater differences were evaluated for the cough and nasal symptoms, while the fever symptom report lowest percentage reduction. F) Number of infection recurrence (IR): Number of mean IR for subject; ST= Standard Therapy; NS=Nebulizer, No significant statistical differences (Ns) were found byThe Student’s Test application (p=Ns).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



