
Submitted:
01 August 2025
Posted:
01 August 2025
You are already at the latest version
Abstract
Background/Objectives: Caring-healing modalities (CHMs), i.e., non-pharmacological, nurse-led interventions rooted in caring science, have shown promise in reducing emotional distress while enhancing resilience. CHMs are heterogeneous, making it challenging to determine how they are formulated to build resilience, mitigate emotional distress, and explore their mechanisms of action. This scoping review mapped the literature on CHMs, including components, targeted outcomes, and measures. Methods: This review followed the JBI methodology and was guided by Watson’s theory of unitary human caring. Experimental studies, systematic reviews, opinion pieces, and gray literature on CHMs for emotional distress and resilience delivered to adults who underwent oncological treatment(s), written in English, were considered. No date or setting limits were applied. Eleven databases were searched. Two independent reviewers screened, selected, and extracted data. Results were interpreted using Watson’s theory. Results: We included 16 records (2016-2025), mostly from the United States (n = 4; 25%) and China (n = 6; 37.5%). CHMs mainly targeted persons with breast cancer. CHMs were categorized into four groups: Mindfulness-Based, Group-Based, Expressive, and Educational. Common active ingredients included peer support and group discussions. Dedicated healing spaces facilitated CHMs delivery; mode of delivery and dose varied widely. Conclusions: This review provides a foundational understanding of CHMs as a caring-based, holistic approach to cancer survivorship. Findings identify CHMs’ key components, including active ingredients, mode of delivery, and dose. Future studies should ensure diversity in terms of cancer type, as most existing studies focused on women with breast cancer.
Keywords:
Resilience psychological
; Emotional distress
; Anxiety
; Depression
; Cancer
; Complementary Therapies
1. Introduction
Cancer is one of the leading causes of death in U.S. and globally. In 2020, it was responsible for approximately 10 million deaths worldwide [1]. In the U.S. alone, more than 600,000 deaths from cancer are projected for 2025 [2]. Fortunately, the survival rates have been improving steadily due to early detection, advanced technology, and new treatment modalities. For example, the five-year relative survival from cancer increased from 49% (1975-1977) to 69% (2014-2020) [3]. As survivorship increases, growing attention has been paid to the persistent physical and psychological challenges faced by persons with cancer (PwC), including those individuals living with and beyond cancer. Many PwC experience various unpleasant symptoms and treatment-related adverse effects that negatively affect their emotional well-being and quality of life [4]. Moreover, they frequently do not express their emotions openly, resulting in internalized feelings of fear, anger, despair, bitterness, and ultimately the state of emotional distress [5].
Emotional distress is a syndrome characterized by anxiety (excessive worry and fear), depression (sadness and loss of interest in pleasurable activities) and/or intrusive thoughts about cancer [6,7]. Among PwC, emotional distress primarily manifests as depression and anxiety. These symptoms may affect approximately 30% of this population, making them two of the most predominant and challenging psychological issues faced during and after the oncological treatment. [8,9]. Risk factors for emotional distress include cancer type, stage of the illness, treatment-related factors, individual factors (e.g. personality traits, family psychiatric history), as well as social and interpersonal determinants (e.g. social support, socioeconomic status) [5]. Emotional distress is often accompanied by fear of dying, demoralization, and the inability to cope with the disease [5]. The toll of emotional distress among PwC is significant and translates into worse quality of life, decreased psychosocial functioning, increased suicide rates, and early death [4, 10).
Taking into account the substantial impact of emotional distress, recent research has increasingly focused on identifying personal abilities, strategies and resources that PwC can use to navigate difficult life circumstances [5]. Resilience is one such ability - or protective factor - often defined as an individual’s self-healing power to effectively restore balance in the face of adversity [6,11,12,13]. Higher levels of resilience have been associated with more effective management of cancer-related stress and treatment side effects [14], as well as lower rates of anxiety and depression [14,15,16]. As such, resilience may play a role in supporting emotional health and long-term health outcomes [15,16].
The psychological challenges experienced by PwC demonstrate the need for nurses and other healthcare professionals to expand their focus beyond physicality and disease management, moving towards the adoption of a whole-person approach and recognition of all human needs. This perspective aligns with Watson’s Theory of Unitary Human Caring which views caring as a heart-centered, relational, and moral ideal that transcends task-oriented practice [17]. Grounded in caring science, the theory supports the integration of the psychological, emotional, and existential dimensions of the person [18] and is operationalized through the ten Caritas Processes (CPs) and the theory’s main tenets (i.e., transpersonal caring relationship, caring moment/occasion, and caring/healing consciousness). This theory offers a framework for enhancing patient care through holistic practices and comprehensive, whole-person approaches. From Watson's perspective, Caring-Healing Arts/modalities, i.e., practices that honor the subjective experience of illness and support the individual’s innate healing capacity [19,20]. These modalities are nurse-led and may include complementary, alternative, or integrative therapies that foster emotional balance, spiritual well-being, and human connection [21].
Numerous studies have explored integrative and complementary health interventions to foster resilience and alleviate emotional distress. Yet, the literature is marked by substantial differences not only in terms of the conceptual and methodological aspects of studies but also concerning caring-healing modalities (CHMs) designs. This heterogeneity makes it challenging to determine how CHMs are structured and delivered, as well as which outcomes they aim to achieve. Thus, it remains unclear how CHMs are formulated to cultivate resilience and mitigate distress, and what specific or non-specific elements may contribute to their impact. A scoping review is thus needed to systematically explore the existing literature on CHMs aimed at enhancing resilience and reducing emotional distress in persons with cancer (PwC). By examining the active ingredients, delivery modalities, structure, dose, duration, measured outcomes, and evaluation instruments used across studies, this review will provide a comprehensive foundation for future research, practice, and CHM development. Moreover, understanding the application of CHMs that can decrease emotional distress and improve resilience will be an important milestone in the oncological nursing care to support PwC live beyond their cancer diagnosis.
A preliminary search of database/s (i.e., Cochrane Library, PubMed, and CINHAL (EBSCOhost)) yielded the identification of two related reviews. One is a systematic review that mapped the standardized measurement tools to evaluate psychosocial outcomes in patients with prostate cancer. However, our review goes beyond by including patients with all types of cancer and examining a wide range of CHM components, besides outcome assessment tools. [22]. The second systematic review identified major CHM components such as mode of delivery and duration of “talking” modalities in randomized controlled trials (RCTs) [23]. Our review differs from it since we included not only RCTs, but also systematic reviews, text, and opinion papers, in addition to considering all types of CHMs. Nevertheless, no reviews were found addressing emotional distress and resilience simultaneously.
The purpose of this scoping review was to assess the extent and nature of the literature regarding CHMs aimed at enhancing resilience and reducing emotional distress among PwC. More specifically, we were interested in exploring CHMs’ active ingredients that bring desired outcomes (increased resilience and reduced emotional distress), CHMs’ non-specific elements and their mode of delivery (medium and format), structure/approach of the identified CHMs and their components, dose/intensity of CHMs found in the literature, duration and frequency of implemented CHMs, primary and secondary outcomes that have been measured in the located CHMs, and finally instruments used to evaluate resilience, emotional distress, and other outcomes of the identified CHMs.
2. Materials and Methods
This theory-guided scoping review [24] was conducted by two independent reviewers, following the JBI methodology [25] and reported in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) [26]. An a priori protocol was developed and registered with the Open Science Framework (https://doi.org/10.17605/OSF.IO/HY2AX). During the preparation of this manuscript, the author(s) used ChatGPT AI, GPT-4-turbo model, to assist with language editing, phrasing suggestions, and structural clarity. The authors have reviewed the output and take full responsibility for the content of this publication.
Eligibility criteria followed the participants, concept, and context structure of a JBI scoping review in addition to types of sources.
Participants. This review considered studies that included PwC 18 years or older who underwent oncological treatment(s). Documents that included individuals on active surveillance were excluded because therapy-related side effects are believed to be associated with higher levels of depression and anxiety [11]. We also excluded sources that focused on individuals with a benign type of tumor, as they are generally non-cancerous and thus fall outside the scope of this review. Moreover, any source documents that included family members or partners of cancer survivors in their population of interest were excluded. The presence of a support system could introduce a potential bias and influence an individual’s emotional well-being and study outcomes [27,28].
Concept. This review considered records that explored CHMs addressing emotional distress (operationalized as anxiety and depression) and resilience simultaneously. To ensure comprehensive coverage of relevant interventions, we included complementary and alternative therapies not exclusively delivered by nurses, provided they fall within the scope of nursing practice as defined by professional standards and regulatory guidelines. We included studies in which these concepts were assessed using standardized measurement tools as well as numerical and verbal scales. We were interested in mapping CHMs that target both resilience and emotional distress. Thus, articles addressing only one of these concepts were excluded from this review.
Context. The context of this review remained open. Therefore, we included sources independently of the setting where the CHM was delivered.
Types of Sources. This scoping review considered published and unpublished experimental studies, systematic reviews, text, and opinion papers addressing PwC receiving CHMs to enhance resilience and decrease emotional distress (anxiety and depression). Retracted articles were excluded when there might be evidence of discrepancies in the description of the CHMs or the data of interest for this review. Furthermore, we did not apply any restrictions regarding publication period or geographical area and did not select specific racial or gender-based interests. However, the scope of source documents was restricted to the English language because this was the language in which all reviewers were proficient.
A three-step search strategy was utilized in this review. First, an initial limited search of PubMed and CINAHL (EBSCOhost) was undertaken to identify relevant records and map the keywords and controlled vocabulary terms present in their titles and abstracts. Next, a second search was performed in all databases included in this review using all identified keywords and controlled vocabulary terms. The search strategy was validated by an experienced librarian and adapted for each database. The databases searched in September 2024 and updated in April 2025 included PubMed, CINAHL, PsychInfo, Web of Science, Embase, Scopus, Lilacs, SciELO, and CUIDEN. Sources of unpublished studies and gray literature were searched in ProQuest Dissertations and Theses Global and DART-Europe. A comprehensive search strategy is provided in Figure 1. Lastly, the reference list of sources selected for full-text review was screened for additional sources that might not have been identified through the database searches.
Following the search, all identified records from each database were collected and uploaded into Covidence (Veritas Health Innovation, Melbourne, Australia) for the screening [29]. Upon review by two independent reviewers (JK and RG), source documents were selected based on the inclusion criteria. Potentially relevant records were retrieved in full and independently screened against the eligibility criteria by the same reviewers. Any disagreements that arose between the reviewers at each stage of the selection process were resolved through discussion or by a third reviewer (LH). A list of excluded sources, with reasons for exclusion, is provided in Figure 1.
Data were extracted by two independent reviewers (JK and RG) using a data extraction tool developed by the reviewers (JK and RG). The results of each extraction were verified by the reviewers, and any disagreements were resolved through discussion. The data of interest for this review included the characteristics of the articles and participants (author(s), year of publication, country of data collection, the purpose of the study, methodological design, type of cancer, sample size and its characteristics) and the characteristics of the CHMs (setting where the CHM was delivered, active ingredients and non-specific elements of the CHM, mode of delivery - medium and format -, structure/approach of the CHM, as well as the dose, intensity, duration, and frequency of the CHM), theoretical framework, outcomes and measurement tools.
Data analysis was guided by Watson’s Theory of Unitary Human Caring, particularly the CPs. Active ingredients, as well as other activities described in the CHM, were carefully considered. Then, CHMs were grouped by similarity. Next, CHM group characteristics were taken into account to determine group correspondence with the CPs. The results from the data analysis were presented narratively and in a tabular format. A diagrammatic representation of the findings was also presented.
Peer review during the screening process revealed that we should exclude retracted articles, source documents that do not describe the implemented CHM, and studies that tested approaches other than complementary and alternative modalities. These exclusion criteria were added during data extraction. Also, we added the theoretical framework as a variable of interest. Mapping the use (or absence) of theory across studies can help identify gaps in theoretical integration, reveal opportunities for advancing CHM science, and inform the development of more coherent and targeted CHMs in oncology.
3. Results
3.1. Source of Evidence Inclusion
The outcome of the literature searching strategy is shown in Figure 1. We identified 1,176 records across all databases (n = 1,174) and through backward reference chaining (n = 2). All retrieved records were uploaded to Covidence for deduplication. After removing duplicates (n = 145), 1,031 titles and abstracts were independently screened by two reviewers, and 934 records were excluded for not being relevant to the review question. As a result, the two independent reviewers assessed 97 full-text reports. From these, 81 were excluded due to the following reasons: duplicates (n = 2), not available in full text (n = 2), addressed wrong outcomes (i.e., missing resilience or anxiety and depression) (n = 39), wrong study design (n = 19), wrong patient population (n = 14), retracted article (n = 1), written in a language other than English (n = 1), did not address the testing of a CHM (n = 1), addressed benign type of tumor, not malignancy (n = 1), CHM components not described (n = 1). Therefore, 16 records were included in the final sample.
3.2. Characteristics of Included Sources of Evidence
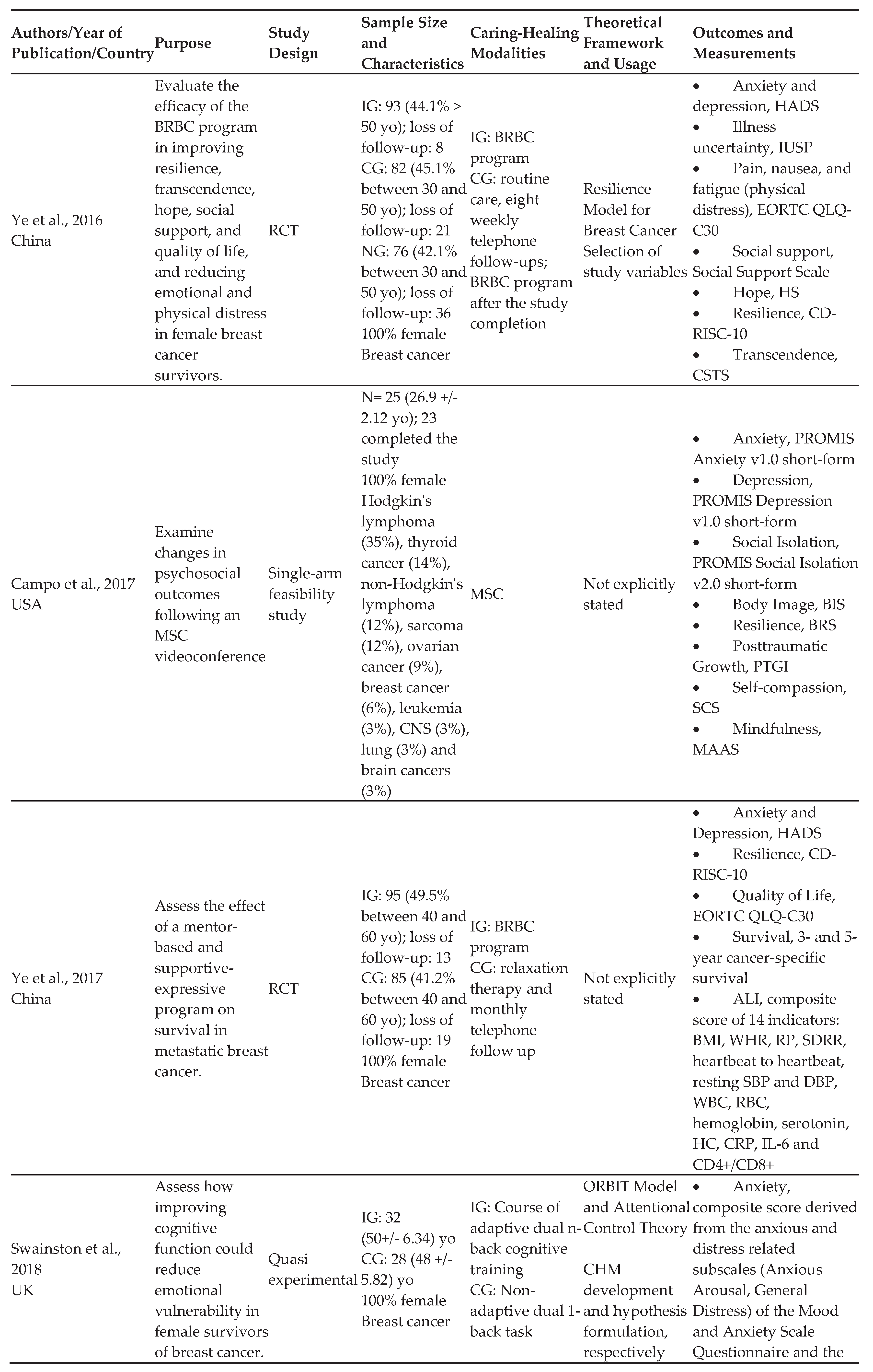
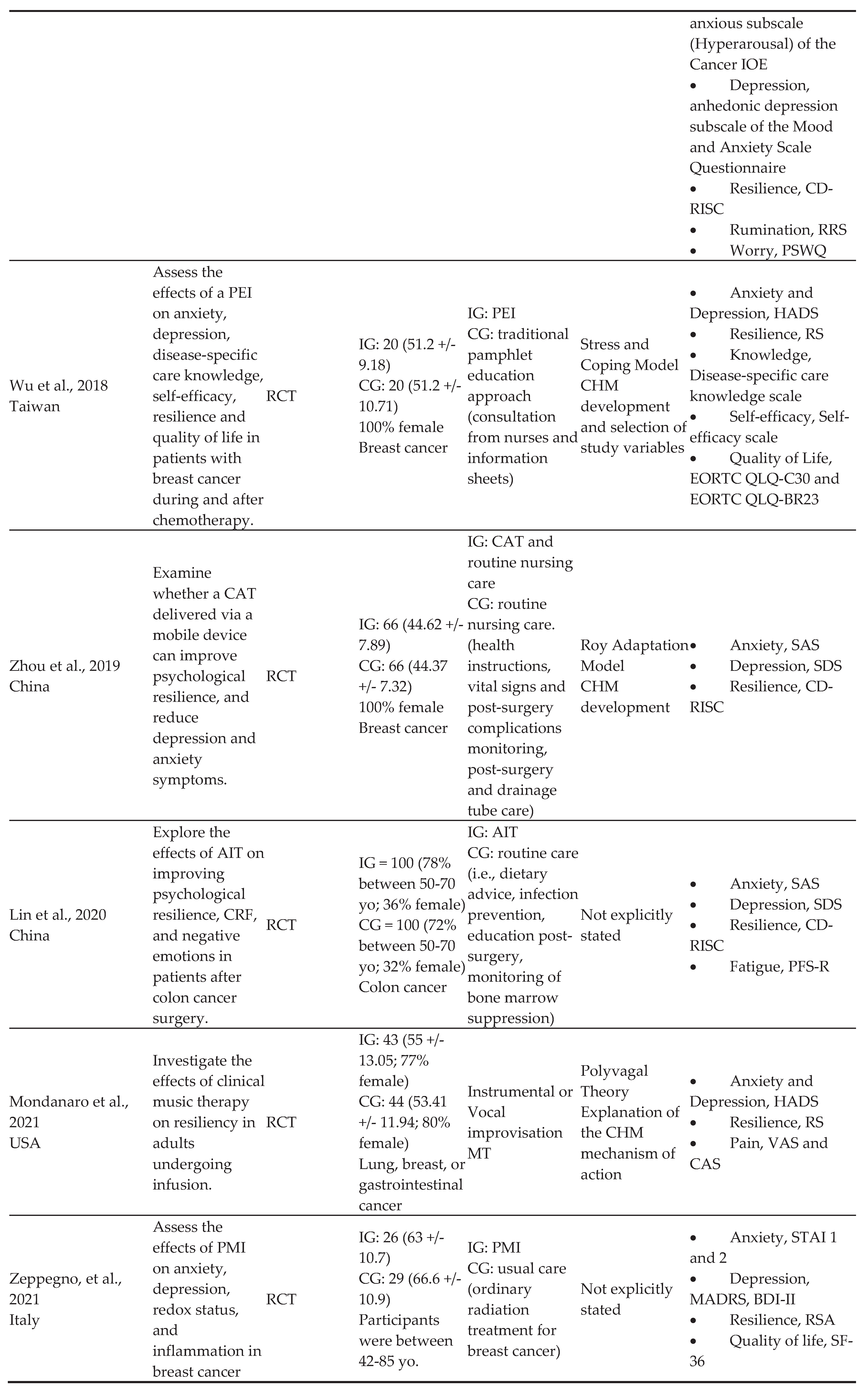
Of the 16 included records, the majority were from China (n = 6, 37.5%) and the United States (n = 4; 25%), with the remaining studies being from Taiwan (n = 1, 6.25%), United Kingdom (n = 1, 6.25%), Finland (n = 1, 6.25%), Germany (n = 1, 6.25%), Italy (n = 1, 6.25%), and Australia (n = 1, 6.25%). Although there were no restrictions regarding the year of publication, the included sources were published between 2016 and 2025. Of all the evidence sources, there were nine RCTs, two quasi-experimental studies, two retrospective studies, one single-arm feasibility study, one prospective longitudinal study, and one mixed-methods, uncontrolled study (Table 1).
3.3. Review Findings
The included records encompassed a total of 1,577 PwC, with an age range from under 30 to over 70 years, with seven studies [30,31,32,33,34,35,36] including 100% female population. Breast cancer survivors were predominantly represented in the sources of evidence (n = 9, 57%), but seven studies also focused on other types of cancer, including colon/colorectal cancer (n = 2) [37,38], acute myeloid leukemia (n = 1) [39], and various types of cancer (n = 4) [30,40,41,42]. CHMs took place in the outpatient setting (n = 3) [31,32,41], outpatient setting and home (n = 2) [33,38], home or private location (n = 3) [30,36,43], hospital (n = 4) [39,42,44,45], as well as hospital and home (n = 2) [34,37]. One CHM was tested in the Cancer Medical Center [35], whereas one source document did not clearly state the setting [40]. A summary of the review findings is presented in Table 2.
We found that CHMs described in the included records were closely aligned with four CPs (Figure 2): being authentically present, enabling faith-hope/belief, honoring subjective inner, life-world of self/others (CP #2), developing and sustaining loving, trusting-caring relationships (CP #4), allowing for expression of positive and negative feelings - authentically listening to another person's story (CP #5), and finally engaging in transpersonal teaching and learning within context of caring relationship; staying within other's frame of reference-shift toward coaching model for expanded health/wellness (CP #7) [19]. Therefore, CHMs were organized accordingly into the following categories: mindfulness-based, group-based, expressive, and educational. Notably, many CHMs incorporated components from more than one CP. When that happened, placement in one category was based on the most prominent CPs within each CHM and evaluation of how these CPs align with the activities and strategies integrated into the respective training programs.
3.3.1. Mindfulness-Based Caring Healing Modalities (Caritas Process #2)
Caritas Process 2 (being authentically present, enabling faith-hope/belief, honoring subjective inner, life-world of self/others) [19] emerged as a recurring theme across mindfulness-based CHMs, focusing on the breath and being fully aware/present in the caring moment. The CHMs grouped under this category include: Stress Management and Resiliency Training: Relaxation Response Resiliency Program (SMART-3RP) [40], Mindful Self-Compassion (MSC) [30], Attention and Interpretation Therapy (AIT) [37], and Mindfulness-Based Stress Reduction (MBSR) program [43]. The primary active ingredients of these CHMs consisted of teaching mindfulness skills and practicing various types of meditation [30,37,40,43]. Some CHMs also required formal and informal practices to be performed at home with daily records [43] and online home practice questionnaire [30], whereas other programs incorporated cognitive behavioral therapy [43], positive psychology [43], group discussions with a focus on self-kindness [30], and emotion training to regulate feelings and share experiences [37]. Non-specific elements of these CHMs included maintaining a quiet environment and minimizing distractions [30], ensuring privacy and providing technical support for the use of online platforms and Facebook [30], nurse supervision [37], incentives to encourage continuous practice [37], use of silent retreat diary [43], and audio recordings describing the nature and content of mindful practice [43]. The delivery was both verbal and written, using face-to-face [37,40,43] and distance formats such as videoconferencing [30,40], WeChat app [37], audio recordings [43], and Facebook [30]. The approach was standardized [30,43] and tailored [37,40] to specific needs of participants, with weekly sessions of 30 minutes to 2.5 hours, lasting between eight to ten weeks.
3.3.2. Group-Based Caring Healing Modalities (Caritas Process #4)
CHMs categorized group-based were most consistently aligned with Caritas Process 4 (developing and sustaining loving, trusting-caring relationships) [19], which served as a guiding framework for interpreting their common focus on sharing difficult-to-discuss experiences with other group members and gaining a sense of control. There were three CHMs in this category: the Interdisciplinary Integrative Oncology Group-Based Program [41], the Be Resilient to Breast Cancer (BRBC) program [31,32], and the Be Well Plan [33]. The main active ingredients of these CHMs consisted of group discussions addressing experiences and feelings [31,32,33,41], peer mentoring [31,32], interactive sessions on yoga, dance therapy, Qi Gong music therapy [41], and neurocognitive restructuring [41]. They also included educational components on a variety of topics, such as diet/nutrition, symptom control, posttreatment issues, sexuality, emotion management, traditional Chinese medicine, and Taichi [31,32]. Awareness of own mental well-being after taking a brief survey and having an option to include a support person in the program were non-specific elements in one of the trials [33]. In other studies, non-specific elements could not be identified. The CHMs were standardized [31,32,41] and adapted to meet the specific needs of participants [31,33], with curriculum tailored to mentor-mentee matching [31] and having an ability to develop own well-being plan from evidence-based activities (i.e., Cognitive Behavioral Therapy [CBT], Acceptance and Commitment Therapy [ACT], mindfulness, and positive psychology) [33]. The programs were primarily face-to-face [31,32,33,41], with one also using phone calls [31]. Most CHMs lasted between two to five hours per session and were conducted over a period ranging from five weeks to 12 months.
3.3.3. Expressive Caring Healing Modalities (Caritas Process #5)
CHMs in this category demonstrated a strong resonance with Caritas Process 5 (allowing for expression of positive and negative feelings - authentically listening to another person's story) [19], particularly through practices aimed at emotional release, employing various forms of expression. These CHMs included the Cyclic Adjustment Therapy (CAT) [34], music therapy [42], Managing Cancer and Living Meaningfully (CALM) [44], psychotherapy with music intervention [45], and expressive writing [39]. All of these CHMs focused on communication, verbal reflections, sharing, and discussions of feelings and experiences brought about by the disease [34,39,42,44,45]. The expression of emotions was facilitated by the use of creative activities or CHMs’ active ingredients, like reading, listening/playing music, singing songs, watching anti-cancer stories, and writing. Sessions were often followed by individual and/or group discussions focused on verbal and written expressions of feelings and experiences related to cancer diagnosis and treatment [34,42,45], verbalization of deepest emotions and thoughts [39], as well as communication of changes brought about the disease [44], relationships with friends and family [44], concerns about future, and understanding of death [44]. Multiple non-specific elements were identified, including providing routine nursing care to participants who received a CHM [34], supportive role of medical residents who joined the sessions and helped lead the program [45], quietness and privacy of the room [45], thorough instructions on the CHM prior to its implementation [39], and education regarding adverse effects of illness and treatment [44]. The approach was standardized for all CHMs, but one, where additional sessions were provided to participants still experiencing depression [44]. Delivery was primarily verbal, with face-to-face format [39,42,45], but also included distance formats, like WeChat [34], virtual reality (VR) [44], Zoom [39], and phone calls [39]. Additionally, writing was incorporated as a mode of delivery in two of CHMs, specifically mobile-based [34] and guided by writing prompts [39]. Sessions, delivered once or twice a week, lasted typically 30 minutes to one hour, with three to six sessions per CHM. Duration ranged from two to twelve weeks.
3.3.4. Educational Caring Healing Modalities (Caritas Process #7)
CHMs in this category reflected the essence of Caritas Process 7 (engaging in transpersonal teaching and learning within context of caring relationship; staying within other's frame of reference-shift toward coaching model for expanded health/wellness) [19], as they emphasized collaborative and person-centered learning experiences for patients to deal with cancer symptoms and treatment side effects. The CHMs include Psychoeducation Intervention (PEI) [35], adaptive dual n-back training [3/6], and psychological nursing with extended care [38]. The primary active ingredients included educational components covering a wide spectrum of knowledge, such as methods of self-care, dietary guidance, uses of alternative treatment, strategies for healthier lifestyles, and CHMs focused on emotional management [35,38]. Educational programs also provided life meaning therapy [38], psychological CHMs that helped cancer survivors to live with cancer and treatment side effects (i.e., stoma) [38], cognitive task to improve attention/working memory capacity and reduce anxiety-related symptoms [36], and finally self-assessment of learning to evaluate newly gained knowledge [35]. Non-specific elements of these CHMs included supervision by healthcare professionals throughout the program [35], the use of self-guided video materials [35], creation of personal file for participants [38], ongoing communication with CHM staff [38], and encouragement to ask questions [38]. Two CHMs followed a standardized approach, while one was tailored, allowing the psychological CHM to be delivered in various formats to accommodate individual participant needs [38]. The CHMs were delivered primarily face-to-face [35,38], with some also incorporating phone communication [35,38], an online platform for task delivery [36], WeChat app [38] and a written educational self-care manual [35]. The sessions lasted 30 minutes to an hour. The cognitive task was delivered over a two-week period, while the duration of other CHMs was not provided. The PEI consisted of six sessions, while psychological nursing with extended care was delivered once a week.
3.3.5. Other Outcomes Assessed in the Sources of Evidence and Measurement Tools
Other outcomes were also assessed beyond resilience, depression, and anxiety. Most often the other outcomes measured were self-compassion (n = 3, 18.75%) [30,33,43], mindfulness (n = 2, 12.5%) [30,43], quality of life (n = 7; 43.75%) [32,35,39,41,43,44,45], rumination (n = 2, 12.5%) [36,39], worry (n = 2, 12.5%) [36,40], and various blood biomarkers (n = 3, 18.75%) [32,43,45]. The tools used to assess outcomes in the included sources of evidence are described in Table 1.
4. Discussion
This is the first scoping review devoted to mapping CHMs aimed at enhancing resilience and decreasing emotional distress (i.e., depression and anxiety) among PwC. Our findings underscore the importance of a caring-based, holistic approach to cancer survivorship by providing a foundational understanding of these CHMs. Guided by Watson’s Theory of Human Caring, this review brings coherence to the findings and highlights the preservation of wholeness, healing, and human dignity [19]. The CHMs identified in this review advance disciplinary nursing knowledge and contribute meaningfully to caring science by fostering holistic care, compassion, acceptance, connection, and trust.
A total of 16 studies were included in this scoping review. The majority were RCTs and focused on persons with breast cancer. A significant number of studies were conducted in China and the United States. The investigators tested complementary and alternative modalities to manage emotional distress and enhance resilience among individuals surviving cancer, representing a range of CHM types, including mindfulness-based, group-based, expressive, and educational. These approaches were implemented in the hospital, outpatient setting, and participants’ homes.
Across the included studies, peer support and group discussions facilitating the expression of emotions and experiences were the most frequently used active ingredients. Although not all CHMs were classified as group-based, many of them incorporated dialogue with other individuals who survived cancer and exchange of feelings and insights regarding the cancer journey to foster the cultivation of appreciation, self-compassion, and loving kindness (CP #1). These active ingredients closely align with Watson’s full human radiant presence (CP #2) which is life giving and life receiving [19]. Caritas Presence restores well-being and human dignity [19]. Additionally, active ingredients correspond well with the caring-healing, trusting relationship with others (CP #7), listening to others’ stories with compassion and an open heart [19]. Connecting with the subjective world of others has the potential to touch the higher spiritual sense of self and the soul, allowing a person to gain a sense of inner harmony and hence, emotional stability [19]. These connections between these active ingredients and the CP are supported by the literature. Peer support and group discussions offer a safe space for mutual understanding and emotional expression, fostering interpersonal connection that normalizes emotional reactions and helps individuals express their needs, reduces isolation, and activates internal resources to cope with adversity [46,47].
When it comes to non-specific elements, CHMs included in this scoping review emphasized the importance of environmental quietness, control of distractions, and preservation of privacy – acts of healing for self and others [19]. This reflects the Watson’s healing environment at all levels (CP #8). A subtle environment for energetic, authentic caring practice creates a space for transformation and inner peace [19]. A growing body of evidence supports the critical role of the physical environment in improving patient outcomes. Environmental modifications, such as reduced lighting [48,49], minimized noise, optimal temperature, and enhanced privacy, have been shown to reduce anxiety and depression. Within Watson’s framework, such interventions create a healing space that fosters emotional and physiological restoration, reinforcing the therapeutic effects of nursing care. Moreover, trusting relationships and human connection are other common non-specific elements across CHMs which are congruent with caring practices. Transpersonal relationships and/or spirit-to-spirit connections have the potential to generate a self-healing process, affecting the life field of each person. Caring partnerships and healing bonds allow to recognize self in others, expand limits of openness, build one’s capacity for healing, and open to the dynamic expression of love [19].
For the delivery modes of CHMs, very common formats used were face-to-face and distance, with verbal and written media. These delivery approaches correspond with holistic and person-centered care values within Watson’s theory [19]. In-person sessions, especially, support authentic presence and meaningful human connection. Web-based platforms and phone applications, on the other hand, fulfill the integrated needs of mind, body, and spirit in diverse care settings. When it comes to structure of the CHMs, the majority used a standardized approach; however, six studies tailored their CHMs to the specific needs of participants. Honoring a person’s uniqueness and diverse needs respects the wholeness of the other, nurturing learning, growing, trusting and healing through love [19]. In terms of dose, duration, and frequency of CHMs, the range varied greatly, depending on the activities incorporated during a training program. Some CHMs lasted only 20-30 minutes, while others were as long as few hours per session. Also, the majority of CHMs were conducted over a period of few weeks with one CHM extended over 12 months. CHMs with shorter duration and manageable demands have important implications for clinical feasibility as they can be easily conduced in the practice setting. One systematic review reported that retention rates in psychosocial behavioral CHMs in the oncology setting are significantly influenced by the mode of delivery (with multiple modes of delivery being more effective) and the CHM duration (with CHMs over eight weeks being more effective than the CHMs taking longer than 16 weeks) [50]. Longer CHMs, on the other hand, are more consistent with Watson’s core values, supporting the development of sustained caring-healing relationships, fundamental to healing and inner harmony [19].
This scoping review primarily focused on resilience and emotional distress – anxiety and depression. Nevertheless, other outcomes were also measured in the included studies, with the most common being quality of life and self-compassion. Other primary and secondary outcomes were assessed, such as physical distress (i.e., fatigue, pain, insomnia), transcendence, posttraumatic growth, hope, worry, self-efficacy, among others. The outcomes were linked to CHMs’ goals and consistently defined. It is important to note that focusing on blood biomarkers [32,43,45] reflects a deepening of holistic inquiry and contributes to strengthening the role of nurses in interdisciplinary teams and advances data-informed patient care [51]. By honoring the embodied experience of persons while drawing on objective biological data, nurses can promote more precise and individualized caring modalities. This integration moves the profession closer to precision nursing that remains grounded in relational, transpersonal caring while embracing the possibilities of omics-informed insights into human harmony, healing, and wholeness.
A wide variety of tools were used to measure the each of the outcomes, particularly resilience, anxiety, and depression. The majority of studies assessed resilience by using the Connor-Davidson Resilience Scale (CD-RISC), whereas anxiety and depression were evaluated by Hospital Anxiety and Depression Scale (HADS), PROMIS short forms, Self-Rating Anxiety Scale (SAS) and Self-Rating Depression Scale (SDS), as well as Beck Anxiety Inventory (BAI) and Beck Depression Inventory (BDI), respectively. This variability suggests a lack of consensus on the best instruments to measure emotional distress outcomes, and it has important implications by limiting comparability across the studies. Furthermore, this becomes a challenge to synthesize CHM effectiveness. Few studies reported the psychometric properties of the instruments in the context of oncology or within the specific cultural settings in which they were used [30,34,36,37,40,41,43] This raises concerns about the appropriateness and sensitivity of the tools to capture changes in resilience and emotional distress among diverse populations of PwC. The wide range of measurement tools highlights the pressing need for standardization in the assessment of resilience and emotional distress in cancer research. Future studies may benefit from selecting validated, population-specific tools that are sensitive to change and aligned with the theoretical foundations of the CHM. Additionally, the development of tools grounded in Watson’s Theory of Human Caring to measure resilience and emotional distress is particularly important. Aligning instruments with theoretical frameworks ensures conceptual coherence, strengthens construct validity, and supports the development of CHMs consistent with this particular worldview. Although few measures are explicitly derived from Watson's theory beyond instruments like the Caring Factor Survey for caritas processes [52], resilience models informed by Unitary Caring Science illustrate how theory-driven frameworks unify caring concepts with psychological constructs [12].
The findings from this review have several important implications for nursing practice, future research, education, and policy. Clinical teams may benefit from being aware of these evolving approaches as they consider ways to integrate more humanized, caring-based strategies into psychosocial support services for PwC. In the context of research, CHMs should be tested in underrepresented cancer groups (i.e., individuals with prostate cancer). In terms of CHM development, the dose, duration, and frequency of CHMs need to be carefully considered in future studies to ensure consistency and clinical feasibility. Findings from this review support the demand for testing of CHMs grounded in caring science, particularly in Watson’s CPs, and possibly measuring caring as a health outcome. In education, findings of this review can be used to introduce and/or strengthen the content on integrative and holistic care, emotional distress, resilience, and caring science in general nursing and oncology. Also, this review demonstrates how Watson’s theory can be used to conceptualize and analyze review findings, serving as an example for nursing students to understand how a theoretical framework guides evidence-based care. Lastly, in terms of policy, the integration of CHMs into standard oncology care could play a vital role in addressing the emotional, mental, and spiritual needs of cancer survivors. However, the lack of reimbursement for complementary and alternative therapies, similar to that provided for conventional treatments, needs to be addressed to alleviate the financial burden experienced by those seeking care and support.
This review has several limitations. Although every effort was made to identify and include pertinent literature, relevant publications may have been missed due to the exclusion criteria, particularly the requirement that studies be published in English and measure both resilience and emotional distress. Moreover, further research is needed to evaluate the effectiveness of these CHMs not only in breast cancer survivors but also across diverse cancer populations. Additionally, considering both quantitative and qualitative methods in future reviews would be helpful to gain a deeper understanding of the phenomenon and the profound significance of CHMs for PwC.
5. Conclusions
In conclusion, this scoping review offers an overview of the current literature regarding CHMs aimed at enhancing resilience and reducing emotional distress among cancer survivors. These CHMs not only addressed physical symptoms, but also emotional, mental, and spiritual dimensions of care. Group-based CHMs were the most commonly implemented in included studies, and these involved peer mentoring, group discussions, and therapeutic dialogue. By examining different CHM components (i.e., active ingredients, non-specific elements, structure/approach, dose, intensity) through the lens of Waston’s theory and caring science, this review contributes to a deeper understanding of how emotional well-being is being addressed in the oncology setting. Also, measuring diverse outcomes in each study aligns with the overarching aim of caring science, which prioritizes the holistic needs of a person, extending beyond symptom relief and physicality. Nevertheless, continued exploration is needed to investigate practices that promote resilience and emotional well-being, ensuring that future care is both, evidence-based and human-centered.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author(s).
Public Involvement Statement
No public involvement in any aspect of this research.
Guidelines and Standards Statement
This manuscript was drafted against the JBI methodology and PRISMA-ScR guidelines for scoping review.
Use of Artificial Intelligence
ChatGPT AI, GPT-4-turbo model was used for text editing and revision purposes in all the sections of this manuscript.
Acknowledgments
During the preparation of this manuscript, the authors used ChatGPT AI, GPT-4-turbo model, for the purpose of text revision. The authors have reviewed and edited the output and take full responsibility for the content of this publication.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PwC | Persons with cancer |
| CHMs | Caring-healing modalities |
| CPs | Caritas Processes |
References
- Cancer. Available online: https://www.who.int/news-room/fact-sheets/detail/cancer (accessed on 26 May 2025).
- Cancer stat facts: Common cancer sites. Available online: https://seer.cancer.gov/statfacts/html/common.html (accessed on 26 May 2025).
- Corn, B. W., & Feldman, D. B. Cancer statistics, 2025: A hinge moment for optimism to morph into hope? A Cancer Journal for Clinicians 2025, 75, 7–9, . [CrossRef]
- Rodriguez-Gonzalez, A., Velasco-Durantez, V., Martin-Abreu, C., Cruz-Castellanos, P., Hernandez, R., Gil-Raga, M., Garcia-Torralba, E., Garcia-Garcia, T., Jimenez-Fonseca, P., & Calderon, C. Fatigue, emotional distress, and illness uncertainty in patients with metastatic cancer: Results from the prospective NEOETIC_SEOM study. Current Oncology 2022, 29, 9722–9732, . [CrossRef]
- Caldiroli, C. L., Sarandacchi, S., Tomasuolo, M., Diso, D., Castiglioni, M., & Procaccia, R. Resilience as a mediator of quality of life in cancer patients in healthcare services. Scientific Reports 2025, 15, 1-11, . [CrossRef]
- Martin, C. M., Schofield, E., Napolitano, S., Avildsen, I. K., Emanu, J. C., Tutino, R., Roth, A. J., & Nelson, C. J. African-centered coping, resilience, and psychological distress in Black prostate cancer patients. Psycho-Oncology 2022, 31, 622–630, . [CrossRef]
- Orom, H., Nelson, C. J., Underwood, W., 3rd, Homish, D. L., & Kapoor, D. A. Factors associated with emotional distress in newly diagnosed prostate cancer patients. Psycho-Oncology 2015, 24, 1416–1422, . [CrossRef]
- Shalata, W., Gothelf, I., Bernstine, T., Michlin, R., Tourkey, L., Shalata, S., & Yakobson, A. Mental health challenges in cancer patients: A cross-sectional analysis of depression and anxiety. Cancers 2024, 16, 1-14, . [CrossRef]
- Getie, A., Ayalneh, M., & Bimerew, M. Global prevalence and determinant factors of pain, depression, and anxiety among cancer patients: An umbrella review of systematic reviews and meta-analyses. BMC Psychiatry 2025, 25, 1-17, . [CrossRef]
- Wang, Y., & Feng, W. Cancer-related psychosocial challenges. General Psychiatry 2022, 35, 1-6. [CrossRef]
- Groarke, A., Curtis, R., Skelton, J., & Groarke, J. M. Quality of life and adjustment in men with prostate cancer: Interplay of stress, threat and resilience. PLoS ONE 2020, 15, 1–16, . [CrossRef]
- Wei, H., Hardin, S. R., & Watson., J. A Unitary Caring Science resilience-building model: Unifying the human caring theory and research-informed psychology and neuroscience evidence. International Journal of Nursing Sciences 2021, 8, 130-135, . [CrossRef]
- Zhou, Y., Shan, H., Wu, C., Chen, H., Shen, Y., Shi, W., Wang, L., & Li, Q. The mediating effect of self-efficacy on family functioning and psychological resilience in prostate cancer patients. Frontiers in Psychology 2024, 15, 1-10, . [CrossRef]
- Deshields, T. L., Asvat, Y., Tippey, A. R., & Vanderlan, J. R. Distress, depression, anxiety, and resilience in patients with cancer and caregivers. Health Psychology 2022, 41, 246–255, . [CrossRef]
- Zhu, H., Li, M., Wang, B., Yuan, X., Dong, B., Yin, H., & Yang, Y. The relationship among resilience, anxiety and depression in patients with prostate cancer in China: A cross-sectional study. Journal of Clinical Nursing in Practice 2023, 9, 102–110, . [CrossRef]
- Tan, W. S., Beatty, L., & Koczwara, B. Do cancer patients use the term resilience? A systematic review of qualitative studies. Supportive Care in Cancer 2019, 27, 43–56, . [CrossRef]
- Lukose, A. Developing a practice model for Watson’s Theory of Caring. Nursing Science Quarterly 2011, 24, 27-30, . [CrossRef]
- Gürcan, M., & Turan, S. A. Examining the expectations of healing care environment of hospitalized children with cancer based on Watson’s Theory of Human Caring. Journal of Advanced Nursing 2021, 77, 3472–3482, . [CrossRef]
- Watson, J. Metaphysics of Watson unitary caring science: A cosmology of love. University Press of Colorado: Louisville, United States, 2021, pp. 1-298.
- Sidani, S., & Braden, C. J. Nursing and Health Interventions. Design, Evaluation, and Implementation, 2nd ed.; John Wiley & Sons, Inc: Hoboken, United States, 2021; pp. 50-51.
- Watson, J. Nursing: The philosophy and science of caring. In Caring in Nursing Classics: An Essential Resource; M. C. Smith, M. C. Turkel, & Z. R. Wolf; Springer Publishing Company, LLC: New York, United States, 2013; pp. 243-263.
- Christie, D. R. H., Sharpley, C. F., & Bitsika, V. A systematic review of the association between psychological resilience and improved psychosocial outcomes in prostate cancer patients. Could resilience training have a potential role?. The World Journal of Men's Health 2024, 43, 1-11, . [CrossRef]
- Galway, K., Black, A., Cantwell, M. M., Cardwell, C. R., Mills, M., & Donnelly, M. Psychosocial interventions to improve quality of life and emotional wellbeing for recently diagnosed cancer patients. Cochrane Database of Systematic Reviews 2012, 11, 1-61, . [CrossRef]
- Opalinski, A. S., Martinez, L. A., Butcher, H., Bertulfo, T., Stewart, D., & Gengo, R. A theory-guided literature review: A knowledge synthesis methodology. The Journal of Nursing Education 2025, 64, 279–285, . [CrossRef]
- Aromataris, E., Lockwood, C., Porritt, K., Pilla, B., Jordan, Z. JBI manual for evidence synthesis. Available online: http://jbisumari.org/ (accessed on 20 April, 2025).
- Tricco, A. C., Lillie, E., Zarin, W., O'Brien, K. K., Colquhoun, H., Levac, D., Moher, D., Peters, M. D. J., Horsley, T., Weeks, L., Hempel, S., Akl, E. A., Chang, C., McGowan, J., Stewart, L., Hartling, L., Aldcroft, A., Wilson, M. G., Garritty, C., Lewin, S., … Straus, S. E. PRISMA extension for scoping reviews (PRISMA-ScR): Checklist and explanation. Annals of Internal Medicine 2018, 169, 467–473, . [CrossRef]
- Acoba E. F. Social support and mental health: The mediating role of perceived stress. Frontiers in Psychology 2024, 15, 1-12. [CrossRef]
- Amin, S. M., Khedr, M. A., Tawfik, A. F., Malek, M. G. N., E-Ashry, A. M. The mediating and moderating role of social support on the relationship between psychological well-being and burdensomeness among elderly with chronic illness: Community nursing perspective. BMC Nursing 2025, 24, 1-15. [CrossRef]
- Covidence [Reference Manager Software]. Available online: https://www.covidence.org/ (accessed on 26 April 2025).
- Campo, R. A., Bluth, K., Santacroce, S. J., Knapik, S., Tan, J., Gold, S., Philips, K., Gaylord, S., & Asher, G. N. A mindful self-compassion videoconference intervention for nationally recruited posttreatment young adult cancer survivors: Feasibility, acceptability, and psychosocial outcomes. Support Care Cancer 2017, 25, 1759–1768, . [CrossRef]
- Ye, Z. J., Liang, M. Z., Qiu, H. Z., Liu, M. L., Hu, G. Y., Zhu, Y. F., Zeng, Z., Zhao, J. J., & Quan, X. M. Effect of a multidiscipline mentor-based program, Be Resilient to Breast Cancer (BRBC), on female breast cancer survivors in mainland China - A randomized, controlled, theoretically-derived intervention trial. Breast Cancer Research and Treatment 2016, 158, 509–522, . [CrossRef]
- Ye, Z. J., Qiu, H. Z., Liang, M. Z., Liu, M. L., Li, P. F., Chen, P., Sun, Z., Yu, Y. L., Wang, S. N., Zhang, Z., Liao, K. L., Peng, C. F., Huang, H., Hu, G. Y., Zhu, Y. F., Zeng, Z., Hu, Q., & Zhao, J. J. Effect of a mentor-based, supportive-expressive program, Be Resilient to Breast Cancer, on survival in metastatic breast cancer: A randomised, controlled intervention trial. British Journal of Cancer 2017, 117, 1486–1494, . [CrossRef]
- Tuckey, N., van Agteren, J., Chur-Hansen, A., Ali, K., Fassnacht, D. B., Beatty, L., Bareham, M., Wardill, H., & Lasiello, M. Implementing a group-based online mental well-being program for women living with and beyond breast cancer – A mixed methods study. Asia-Pacific Journal of Clinical Oncology 2025, 21, 180-189, . [CrossRef]
- Zhou, K., Li, J., & Li, X. Effects of cyclic adjustment training delivered via a mobile device on psychological resilience, depression, and anxiety in Chinese post-surgical breast cancer patients. Breast Cancer Research and Treatment 2019, 178, 95–103, . [CrossRef]
- Wu, P. H., Chen, S. W., Huang, W. T., Chang, S. C., & Hsu, M. C. Effects of a psychoeducational intervention in patients with breast cancer undergoing chemotherapy. Journal of Nursing Research 2018, 26, 266–279, . [CrossRef]
- Swainston, J., & Derakshan, N. Training cognitive control to reduce emotional vulnerability in breast cancer. Psycho-Oncology 2018, 27, 1780-1786, . [CrossRef]
- Lin, C., Diao, Y., Dong, Z., Song, J., & Bao, C. The effect of attention and interpretation therapy on psychological resilience, cancer-related fatigue, and negative emotions of patients after colon cancer surgery. Annals of Cardiothoracic Surgery 2020, 9, 3261–3270, . [CrossRef]
- Liu, F., Yao, K., & Liu, X. Analysis on effect of psychological nursing combined with extended care for improving negative emotions and self-care ability in patients with colorectal cancer and enterostomy. A retrospective study. Medicine 2024, 103, 1-7, http://dx.doi.org/10.1097/MD.0000000000038165.
- Nakatani, M. M., Locke, S. C., Herring, K. W., Somers, T., & LeBlanc, T. W. Expressive writing to address distress in hospitalized adults with acute myeloid leukemia: A pilot randomized clinical trial. Journal of Psychosocial Oncology 2024, 42, 587–603, . [CrossRef]
- Finkelstein-Fox, L., Bliss, C. C., Rasmussen, A. W., Hall, D. L., El-Jawahri, A., & Perez, G. K. Do cancer curvivors and metavivors have distinct needs for stress management intervention? Retrospective analysis of a mind-body survivorship program. Supportive Care in Cancer 2023, 31, 1–11, http://www.springer.com/medicine/oncology/journal/520.
- Savaş, B. B., Märtens, B., Cramer, H., Voiss, P., Longolius, J., Weiser, A., Ziert, Y., Christiansen, H., & Steinmann, D. Effects of an interdisciplinary integrative oncology group-based program to strengthen resilience and improve quality of life in cancer patients: Results of a prospective longitudinal single-center study. Integrative Cancer Therapies 2022, 21, 1-11, . [CrossRef]
- Mondanaro, J. F., Sara, G. A., Thachil, R., Pranjić, M., Rossetti, A., EunHye Sim, G., Canga, B., Harrison, I. B., & Loewy, J. V. The effects of clinical music therapy on resiliency in adults undergoing infusion: A randomized, controlled trial. Journal of Pain and Symptom Management 2021, 61, 1099–1108, . [CrossRef]
- Sakki, S. E., Penttinen, H. M., Hilgert, O. M., Volanen, S.-M., Saarto, T., & Raevuori, A. Mindfulness is associated with improved psychological well-being but no change in stress biomarkers in breast cancer survivors with depression: A single group clinical pilot study. BMC Women’s Health 2022, 22, 1-12, . [CrossRef]
- Liu, S., Huang, R., Li, A., Yu, S., Yao, S., Xu, J., Tang, L., Li, W., Gan, C., & Cheng, H. Effects of the CALM intervention on resilience in Chinese patients with early breast cancer: A randomized trial. Journal of Cancer Research and Clinical Oncology 2023, 149, 18005–18021, . [CrossRef]
- Zeppegno, P., Krengli, M., Ferrante, D., Bagnati, M., Burgio, V., Farruggio, S., Rolla, R., Gramaglia, C., & Grossini, E. Psychotherapy with music intervention improves anxiety, depression and the redox status in breast cancer patients undergoing radiotherapy: A randomized controlled clinical trial. Cancers 2021, 13, 1-16, . [CrossRef]
- Lynex, C., Meehan, D., Whittaker, K., Buchanan, T., & Varlow, M. The need for improved integration of psychosocial and supportive care in cancer: A qualitative study of Australian patient perspectives. Supportive Care in Cancer: Official Journal of the Multinational Association of Supportive Care in Cancer 2025, 33, 1-9, . [CrossRef]
- Kiemen, A., Czornik, M., & Weis, J. How effective is peer-to-peer support in cancer patients and survivors? A systematic review. Journal of Cancer Research and Clinical Oncology 2023, 149, 9461–9485, . [CrossRef]
- Azizoğlu, H., Gürkan, Z., Bozkurt, Y., Demir, C., & Akaltun, H. The effect of an improved environment according to Watson's theory of human care on sleep, anxiety, and depression in patients undergoing open heart surgery: A randomized controlled trial. Healthcare 2025, 13, 1-16, . [CrossRef]
- Tian Y. A review on factors related to patient comfort experience in hospitals. Journal of Health, Population, and Nutrition 2023, 42, 1-19, . [CrossRef]
- Song, L., Qan'ir, Y., Guan, T., Guo, P., Xu, S., Jung, A., Idiagbonya, E., Song, F., & Kent, E. E. The challenges of enrollment and retention: A systematic review of psychosocial behavioral interventions for patients with cancer and their family caregivers. Journal of Pain and Symptom Management 2021, 62, e279–e304, . [CrossRef]
- Liu, Q., Wang, F., Wang, G., Liu, L. & Hu, X. Recent evidence and progress for developing precision nursing in symptomatology: A scoping review. International Nursing Review 2023, 70, 415–424, . [CrossRef]
- Nelson J. W. Using the profile of caring: Measuring nurses' caring for self and caring by their unit manager. Creative Nursing 2022, 28, 17–22, . [CrossRef]
Figure 1.
PRISMA flow diagram illustrating the identification, screening, and inclusion process of sources of evidence from this scoping review.
Figure 1.
PRISMA flow diagram illustrating the identification, screening, and inclusion process of sources of evidence from this scoping review.
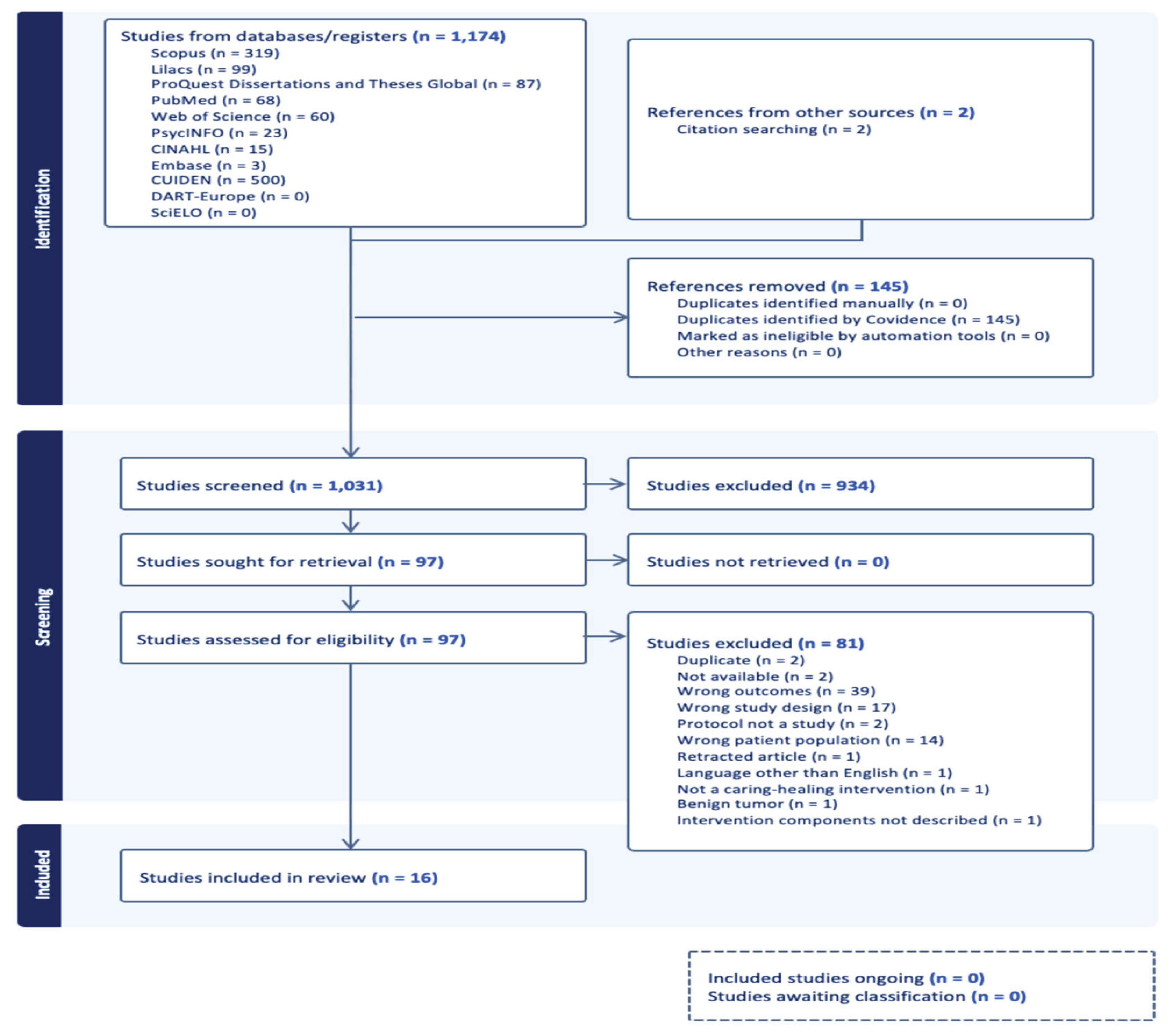
Figure 2.
Caring-healing modalities for enhancing resilience and reducing emotional distress grouped based on Watson’s Theory of Unitary Human Caring and the Caritas Processes.
Figure 2.
Caring-healing modalities for enhancing resilience and reducing emotional distress grouped based on Watson’s Theory of Unitary Human Caring and the Caritas Processes.
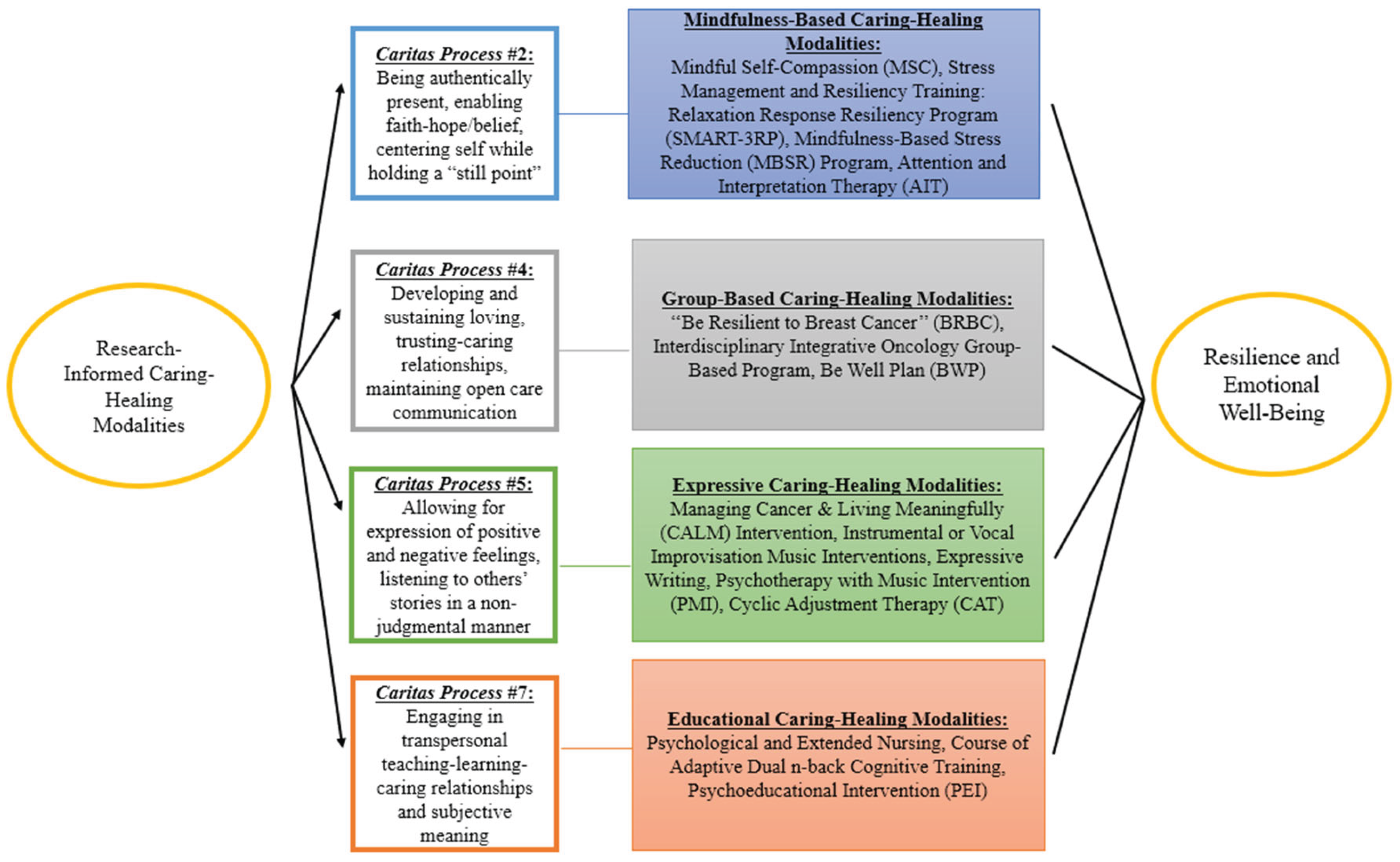

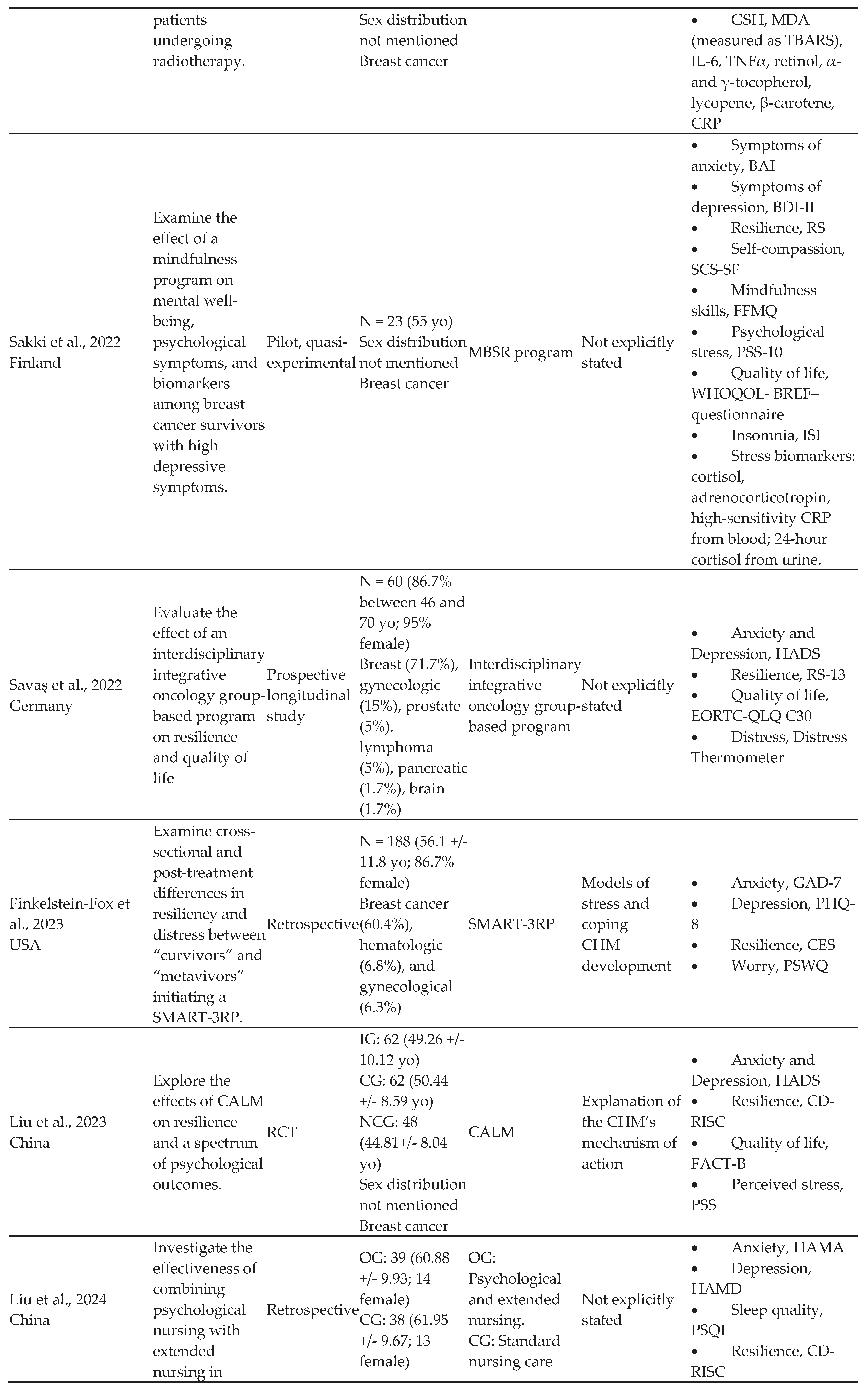
Table 1.
Characteristics of included sources of evidence.
 |
 |
 |
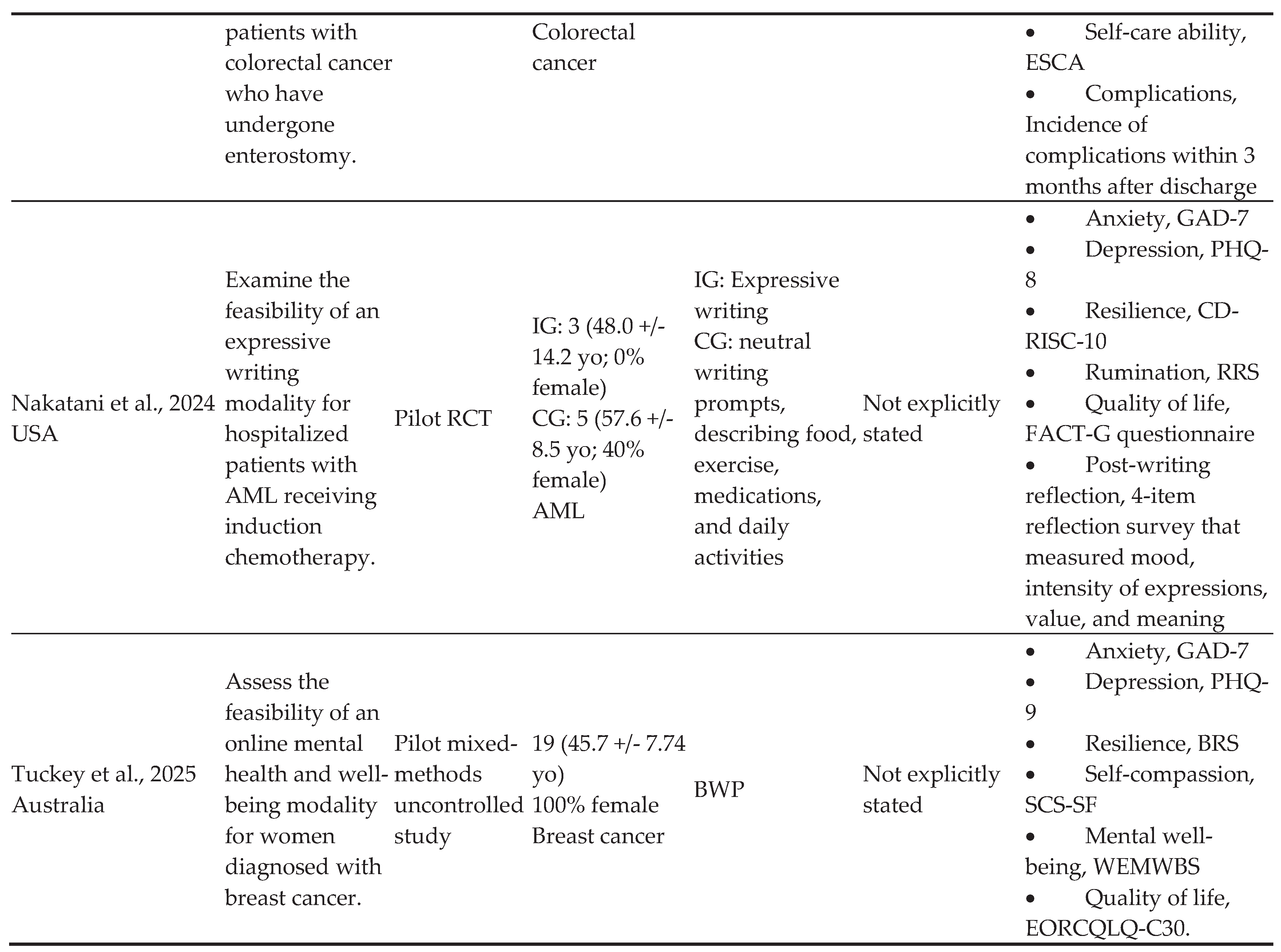 |
Note: BRBC, Be Resilient to Breast Cancer; RCT, randomized controlled trial; IG, intervention group; CG, control group; NG, norm group; yo, years old; HADS, Hospital Anxiety and Depression Scale; IUSP, Illness Uncertainty Scale for Patients; EORTC QLQ-C30, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire – Core 30; HS, the 8-item Hope Scale; CD-RISC-10, 10-item Connor-Davidson Resilience Scale; CSTS, Chinese version of Self-Transcendence Scale; MSC, Mindful Self-Compassion; BIS, Body Image Scale; BRS, Brief Resilience Scale; PTGI, Posttraumatic Growth Inventory; SCS, Self-Compassion Scale; MAAS, Mindful Attention Awareness Scale; ALI, Allostatic Load Index; BMI, body mass index; WHR, waist-hip ratio; RP, resting pulse; SDRR, standard deviation of R-R intervals; SBP, systolic blood pressure; DBP, diastolic blood pressure; WBC, white blood cell count; RBC, red blood cell count; HS, hormone cortisol; CRP, C-reactive protein; IL-6, interleukin-6; CD4+/CD8+, cluster of differentiation 4/cluster of differentiation 8; IOE, Impact of Events Scale; CD-RISC, Connor Davidson Resilience Scale; RRS, Ruminative Response Scale; PSWQ, Penn State Worry Questionnaire; PEI, psychoeducational intervention; RS, resilience scale; EORTC QLQ-BR23, European Organization for Research and Treatment of Cancer Quality of Life Questionnaire – Breast Cancer Module; CAT, cyclic adjustment training; SAS, Self-Rating Anxiety Scale; SDS, Self-Rating Depression Scale; AIT, attention and interpretation therapy; CRF, cancer-related fatigue; PFS-R, Revised Piper Fatigue Scale; MT, music intervention; RS, resilience scale; VAS, visual analog scale; CAS, body pain scale; PMI, psychotherapy with music intervention; STAI, State-Trait Anxiety Inventory; MADRS, Montgomery–Asberg Depression Rating Scale; BDI-II, Beck Depression Inventory II; RSA, Resilience Scale for Adults; SF-36, Short Form-36; GSH, Glutathione; MDA, malondialdehyde; IL-6, interleukin 6; TNF α, tumor necrosis factor α; MBSR, Mindfulness-Based Stress Reduction; BAI, Beck Anxiety Inventory; SCS-SF, Self-Compassion Scale Short Form; FFMQ, Five Facet Mindfulness Questionnaire; PSS-10, Perceived Stress Scale-10 item; WHOQOL-BREF, World Health Organization Quality of Life Questionnaire-BREF; ISI, Insomnia Severity Index; SMART-3RP, Stress Management and Resiliency Training: Relaxation Response Resiliency Program; GAD-7, Generalized Anxiety Disorder 7-item scale; PHQ-8, Patient Health Questionnaire 8-item; CES, Current Experiences Scale; NCG, Normal control group; Managing Cancer and Living Meaningfully; FACT-B, Functional Assessment of Cancer Therapy-Breast; PSS, Perceived Stress Scale; OG, observation group; HAMA, Hamilton Anxiety Rating Scale; HAMD, Hamilton Depression Rating Scale; PSQI, Pittsburgh Sleep Quality Index; ESCA, Studies of Self-Care Ability Scale; AML, acute myeloid leukemia; RRS, Rumination Response Scale; FACT-G, Functional Assessment of Cancer Therapy-General; BWP, Be Well Plan; PHQ-9, the 9-item Patient Health Questionnaire; BRS, Brief Resilience Scale; SCS-SF, Self-Compassion Scale - Short Form; WEMWBS, Warwick-Edinburgh Mental Well-Being Scale.
Table 2.
Characteristics of caring-healing modalities included in the sources of evidence analyzed in this scoping review.
Table 2.
Characteristics of caring-healing modalities included in the sources of evidence analyzed in this scoping review.
| Authors/ Year of Publication | Caring-Healing Modality Setting | Active ingredients | Non-specific Elements | Medium | Format | Structure/Approach | Dose | Duration and Frequency |
| Ye et al., 2016 | Outpatient setting | Education related to breast cancer (e.g. breast reconstruction, posttreatment issues, sexuality, anxiety, depression, uncertainty, diet and nutrition, music therapy, emotion management, positive mind therapy, traditional Chinese medicine, Taichi). Peer support Group discussions |
Not identified | Group-based and one-on-one; person-dependent Verbal/written |
In-person, phone calls Techniques included didactic lectures and group discussions on the following themes: surgery and treatment, physical therapy, emotional distress, nausea, diet and nutrition, traditional Chinese Medicine, Taichi practice, music and relaxation techniques, sexuality, restoration, to be better, and renewal. |
Standardized Curriculum with tailored mentor-mentee matching |
3 hours per session | 12 months; 8 weekly sessions in first 2 months, plus 3 follow-ups at 2, 6, and 12 months |
| Campo et al., 2017 | Participants’ homes or private location | MSC, self-esteem, gratitude, and self-appreciation | Quiet environment (headphones), control of distractions, protection of privacy, interaction among members on Facebook secret groups, assistance with technical issues while using online platform, reminders | Group-based, person dependent Verbal/written |
Online/remote (videoconference), including several techniques: didactic instruction, experiential activities (e.g., compassionate friend meditation, body scan, here-and-now stone, affectionate breathing meditation, loving kindness meditations, soften-soothe allow meditation, gratitude phone photos), introduction of different meditations and daily tools, group discussion, and interaction on Facebook | Standardized | 90-minute sessions | Once per week for 8 weeks |
| Ye et al., 2017 | Outpatient setting | Education related to breast cancer (e.g., surgery and treatment, physical therapy, emotional distress, nausea, diet and nutrition, traditional Chinese Medicine, Taichi practice, music and relaxation techniques, sexuality, restoration, to be better, and renewal) Peer support |
Not identified | Group-based Verbal/written |
In-person Techniques included didactic lectures and group discussions |
Standardized | 120 minutes per session | 12 months; weekly sessions |
| Swainston et al., 2018 | Home | Cognitive training | Not identified | Individual-based Verbal/written |
Online Techniques included adaptive dual n-back cognitive training tasks |
Standardized | 30 minutes per session | 12 days across 2-week period; daily sessions |
| Wu et al, 2018 | Cancer Medical Center | PEI consisting of an educational manual addressing depression, anxiety, disease-specific care knowledge, self-efficacy, and resilience, and a self-assessment of learning | Supervision by healthcare professionals, use of a self-directed videotape, educational information and materials | Individual-based Verbal/written |
In person; techniques included interaction between healthcare professionals and patients (telephone consultations), self-directed videotape, educational manual | Standardized CHM plan based on educational and support components | 1 hour per session | 6 sessions during five chemotherapy treatments |
| Zhou et al., 2019 | Hospital/home | Deep breath training, music listening, anti-cancer stories (reading/listening/watching), self-reflection, shared decision-making | Routine nursing care, health instruction, vital signs and post-surgery complications monitoring, post-surgery and drainage tube care | Group-based, person-dependent Verbal/written |
Online (via WeChat), in person (nurse-to-patient instruction) | Standardized | 30-60 minutes per session for nurse-to-patient instruction before surgery; 20 minutes per session for relaxed deep breath training before surgery; 10 minutes per session for relaxed deep breath training three times per day after surgery; 20-30 minutes per session for music listening and anti-cancer stories (reading/listening/watching) three times per day after surgery. | From hospital admission to 12 weeks follow-up; relaxed deep breath training three times per day and once before surgery; music listening and anti-cancer stories (reading/listening/watching) three times per day; re-introspect once per week |
| Lin et al., 2020 | Hospital and home | Transcendental meditation, emotional control, cultivation of appreciation, mindfulness, acceptance, support from peers, and commitment therapy | Nurse supervision and follow-up, personal file establishment, incentives for continuous practice (text message), maintaining peer connection, communication with interventionists | Group based person depended Verbal/written |
Face-to-face Techniques included didactic instruction, group meetings, emotional diaries, WeChat emotion management applet, video sharing, patient workshops |
Tailored according to the special needs of the patient | 30 minutes per session | Daily for 10 weeks |
| Mondanaro et al., 2021 | Hospital | Instrumental or vocal music | Not identified | Individual-based Verbal, auditory |
In-person Techniques included warm up, improvisation (melody, harmony, timbre, and rhythmic idioms), discussion of therapeutic goals and themes or issues identified in the music or self-disclosure |
Standardized | 20 minutes per session | 3 sessions over 1 to 3 months |
| Zeppegno, et al., 2021 | Quiet room at a hospital | Psychodynamic psychotherapy, MT, peer support | Supportive role of residents, quietness, privacy | Group-based Verbal/written |
In-person Techniques included music listening, song lyric analysis, sharing of emotions and memories, group discussions |
Standardized | 1 hour per session | 6 weeks; weekly sessions |
| Sakki et al., 2022 | Between- session practices done at home; group sessions not clearly stated | Mindfulness home practice, including body scan, breathing exercises, mindful movements and yoga practice, awareness | Silent retreat, diary, audio recordings describing nature and content of mindful practices | Group-based Verbal/written |
Informal home practices, group sessions, and diary of independent mindfulness practice | Standardized | 2.5 hours per session, 45 minutes for home practices | 8 weeks; weekly sessions, in addition to between-session practices and one day long silent retreat |
| Savaş et al., 2022 | Outpatient setting | Neurocognitive restructuring, recommendations for diet, exercise, stress management, relaxation, naturopathic self-help strategies, and psychosocial support | Not identified | Group-based Verbal, auditory, tactile |
In-person Music therapy, manual therapies |
Standardized | 5 hours per session, including a 2-hour break | 10 weeks; weekly sessions |
| Finkelstein-Fox et al., 2023 | Not clearly stated | Stress-awareness, stress-coping, and stress-buffering skills | Not clearly stated | Group-based Person-depended Verbal/written |
In-person, videoconferencing Program manual Mind-body techniques that elicit the RR (i.e., meditation, breath awareness), positive psychology (i.e., shifting focus to positive experiences), and cognitive behavioral therapy (i.e., re-structuring negative thoughts) |
Tailored | Not clearly stated | Once per week for 8 or 9 weeks |
| Liu et al., 2023 | Hospital | Guidance for symptom management, discussion of changes brought by the disease, psychotherapy to clarify the purpose and meaning of existence, discussion of concerns about the future and understanding of death | Trusting relationship, education regarding adverse effects of illness and treatment | Individual-based Visual/auditory, verbal |
In-person Techniques included dialogue, didactic instruction, virtual reality therapy |
Tailored to the participants’ needs | At least 30 minutes per session | 12 weeks; six sessions over 12 weeks |
| Liu et al., 2024 | Outpatient setting and home | Education, instillation of hope and confidence, meaning therapy, family association and peer support, emotional expression, and extended care (follow-up) | Personal file establishment, maintaining communication with interventionists, and encouragement to ask questions | Individual- and group- based, person-depended Verbal/written |
Face-to-face/in-person, telephone, and online Techniques included didactic instruction, group meetings, emotional expression, WeChat groups, video sharing |
Tailored to the participants’ needs | Not clearly stated | Once per week, not clearly stated for how long |
| Nakatani et al., 2024 | Hospital | Emotional expression Post writing reflections |
Instructions | Individual-based Verbal (coaching)/written |
In-person and remote (Zoom and phone) Techniques included writing prompts and coaching |
Standardized | 1-hour sessions | 4 sessions over 2 weeks |
| Tuckey et al., 2025 | Outpatient setting and home | Psychoeducation, self-reflection, and sharing | Awareness of participant’s mental health (survey); having a support person in the program | Group-based Verbal/written |
Online or face-to-face/in-person, mobile app | Tailored (developing own well-being plan) | 2 hours per session | 5 weeks; weekly sessions |
Note: MSC, Mindfulness, self-compassion; PEI, Psychoeducational intervention; MT, music intervention; RR, relaxation response; CALM, Managing Cancer and Living Meaningfully.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



