
Submitted:
31 July 2025
Posted:
31 July 2025
You are already at the latest version
Abstract
Hypoplastic Left Heart Syndrome (HLHS) is a severe congenital heart disease affecting 2-3 neonates every 10,000 live births. While prior research has highlighted potential genetic associations of HLHS, the precise pathophysiology remains elusive. Current standard of care involves three-staged surgical palliation that compensates for the underdeveloped left ventricle (LV) by redirecting systemic circulation via the right ventricle (RV). Despite surgical intervention, patients frequently experience complications of arrhythmias and right ventricular heart failure, culminating in the need for an eventual heart transplant. Scarcity of suitable donors combined with limited understanding of mechanisms of development highlights the need for further research into HLHS and alternative treatment options. Over the past decades, stem cell research has advanced our understanding of numerous cardiac conditions with significant implications for HLHS. This review outlines the emerging role of stem cell-based therapy with a focus on adult stem cells and pluripotent stem cells (PSC) in uncovering the pathophysiology of HLHS and optimizing future treatment directions. In addition, we will explore emerging directions of stem cell derived techniques such as cardiac organoids and bioengineering cardiac tissues and their utility for investigating disease mechanisms, drug screening, and novel therapy for HLHS.
Keywords:
Hypoplastic Left Heart Syndrome
; Congenital heart disease
; Stem cell
; Pluripotent stem cell
; Induced pluripotent stem cell
; Cardiac organoid
; Engineered cardiac tissue
; Stem cell therapy
; Drug screening
; 3D/4D bioprinting
1. Introduction
Hypoplastic left heart syndrome (HLHS) is a severe and complex congenital heart disease (CHD) affecting 1 in 3995 live births in the USA and constitutes roughly 2-3% of all CHDs [1]. It is characterised by underdevelopment of left-sided cardiac structures including left ventricle (LV), mitral valve, aortic valve and ascending aorta [2]. The resulting anatomical deficiency prevents effective systemic circulation and is incompatible with life without early surgical intervention [3].
Current standard of care for HLHS patients involves a series of staged surgical procedures aimed to overcome left sided cardiac deficiencies [2,4,5] (Figure 1). The initial Norwood procedure, usually performed in the first week of life, reconstructs the underdeveloped aorta with the pulmonary artery to form a neoaorta. This allows the right ventricle (RV) to supply the systemic circulation [6]. At the same time, a shunt is inserted from the RV to supply the pulmonary circulation and create an artificial connection between the right and left atrium to permit mixing of oxygenated and deoxygenated blood [7]. Subsequently, the bidirectional Glenn procedure, normally occurring at 4-6 months, connects the superior vena cava to the pulmonary arteries, thereby, bypassing the RV and resulting in a reduced RV workload [8]. Similarly, the final palliative stage termed the Fontan procedure, performed between 18 months and 3 years of age, redirects the inferior vena cava to the pulmonary artery, allowing all deoxygenated blood to enter the lungs directly [9]. Overall, these surgical palliation procedures allow HLHS patients to achieve a RV that is capable of supplying fully oxygenated blood to the systemic circulation. Although capable of extending patient life expectancy and improving quality of life [10], end outcomes of these surgical interventions remain inferior compared with healthy individuals [11]. Despite surgical advances enabling survival of an otherwise fatal condition, long-term complications such as arrhythmias [12,13] and eventual RV failure occur [14] in a significant proportion of patients. Even with successful staged palliation surgeries, many patients will eventually require heart transplantation [15] which is significantly limited by availability of suitable donors and comes with significant complications and risks of its own. These limitations combined with the poor regenerative capacity of the myocardium highlight the need for alternative therapeutic options.
The last two decades have seen notable progress towards addressing these limitations with the emergence of stem cell-based regenerative therapies. Multiple sources of viable adult stem cells have been identified from bone marrow, adipose tissue and umbilical cord blood [16,17,18]. These stem cells have shown translational potential within a wide range of pathologies including HLHS, with multiple published and ongoing trials investigating their potential use in HLHS [19]. Early clinical results have demonstrated feasibility and safety of stem cell application in HLHS patients such as in the ELPIS trials [20] laying the foundation for future later-phased efficacy trials.
Other than adult stem cells, pluripotent stem cells (PSCs) including induced PSCs (iPSCs) and embryonic stem cells (ESCs), offer an excellent alternative possibility. PSCs-derived cardiomyocytes (CMs) [21] have been used extensively to study disease modelling, pathogenesis and potential therapeutic applications [22,23,24,25]. More recently, the discovery of cardiac organoids and improvements in cardiac tissue engineering with the introduction of 3D bioprinting has led to some scientists incorporating these elements into the study of HLHS [26,27]. In this review, we aim to explore how recent stem cell technologies have redefined our understanding of HLHS and potentially provide innovative approaches to the treatment of HLHS beyond surgery.
2. Key Pathophysiological Basis and Signaling Molecules of HLHS
Cardiac development initially begins between day 15-17 of embryogenesis with the migration of mesoderm from the primitive streak to the two heart forming regions [28,29]. These regions then give rise to the first heart field (FHF) and the second heart field (SHF). The FHF contributes to the formation of the LV and atria whilst the SHF contributes to the development of the RV and outflow tract. These two structures then subsequently fuse to form the cardiac crescent and the primitive heart tube. The primitive heart tube undergoes looping which transforms the structure from that of a linear tube into a structure with distinct chambers. Subsequent migration of the neural crest cells contributes to the formation of the aorticopulmonary septum [30] whilst endocardial cushions give rise to the valves and septa [31].
Pathological studies have shown that the key pathogenesis of HLHS is attributed to a complex multifactorial disease secondary to cardiac developmental disruptions during early cardiogenesis [2,32]. A multitude of potential developmental and signaling pathways alongside growth and transcription factors have been proposed as contributory or even pathogenic components to HLHS [33] (Table 1). A foundational understanding of the finely balanced genetic and developmental signaling pathways is therefore the key to interpreting recent insights into HLHS pathogenesis.
2.1. Key Signaling Pathways for Heart Development and HLHS
The complex process of cardiogenesis relies on finely tuned spatial and temporal development of cardiac cell populations [86]. This is achieved via interactions between numerous transcription factors and signaling molecules as outlined extensively in Li et al’s review on molecular mechanisms of cardiac development [69]. Here we will highlight the important molecular pathways and transcription factors with relevance to HLHS(Table 1).
The WNT/β-catenin signaling cascade is a well-studied pathway for early cardiac development with direct implications in HLHS [87]. Activation of the canonical WNT pathway leads to an accumulation of β-catenin via frizzled receptors [88,89]. This triggers the development of mesoderm from the primitive streak, subsequently forming the FHF and the SHF. Evidence of the critical involvement of the canonical WNT pathway has been clearly demonstrated by the removal of Wnt 2 and Wnt 11 leading to a reduction in SHF progenitors [69]. Subsequently, the inhibition of the canonical WNT pathway and the activation of the non-canonical WNT/calcium pathway are required specifically for CM differentiation from stem cells. Overall, this highlights the importance of activation and inhibition of various WNT pathways at the correct time being crucial for early cardiogenesis and CMs generation from stem cells. Any genetic disruptions in either the canonical or non-canonical WNT pathways will likely result in cardiac developmental malformations including HLHS.
Another key signaling pathway implicated in the development of the heart is retinoic acid (RA). Under normal circumstances, RA produced by the retinaldehyde dehydrogenase enzymes acts as a morphogen which governs the development of tissue patterning and cardiac defects [90]. By exerting its effects on RA nuclear receptors, RA establish correct anterior-posterior (AP) axis patterns in cardiac mesoderm, which defines atrial and ventricular regions [91,92]. In addition, RA has been proven to prevent overgrowth of cardiac progenitor regions and regulate epithelial to mesenchymal transition [93]. Moreover, RA has been documented to interact with several key factors such as bone morphogenetic proteins (BMPs) and NKX2.5 implicated in HLHS pathogenesis [90], highlighting its role for HLHS aetiology.
Amongst the key cardiac developmental pathways, disruptions in NOTCH signaling remain one of the most extensively studied pathways with strong evidence supporting its role in HLHS pathogenesis. Normal function of the NOTCH pathway begins with Jagged and delta-like ligands binding to NOTCH 1-4 to facilitate activation of downstream genes via the notch intracellular domain (NICD) [34]. During cardiac development, activation of NOTCH signaling initially prevents expression of myocardial genes and inappropriate early cardiac differentiation [94], thereby keeping mesoderm in progenitor state. Subsequently, NOTCH signaling interacts with other pathways such as WNT and BMP, promoting SHF differentiation into outflow tracts (OFTs) and right heart structures. In addition, NOTCH also regulates key processes such as ventricular trabeculation, normal endocardial cushion placement, valve thickness and proper ventricular growth [95,96]. Defects in the NOTCH pathway have been associated with a variety of CHDs including ventricular septal defects (VSD), OFT malformations and HLHS [97].
BMP is a subset of growth factors within the much larger transforming growth factor beta (TGFβ) family. They act as signaling proteins that interact with many of the pathways such as FGF and WNT to ensure normal cardiac development. Different members of the BMP family are instrumental in different aspects of cardiac development. BMP2 and BMP4 working in tandem with WNT, FGF and other growth factors help to guide mesodermal cells to a cardiac fate [39]. These BMPs are required for the development and proliferation of endocardial cushions which eventually form the heart valves, structures that are underdeveloped in HLHS. In contrast, BMP10 is critical in trabeculation [98] and CM proliferation [99], with its absence in mice leading to ventricular wall underdevelopment and increased lethality rates during embryogenesis [100]. These findings highlight the multifaceted roles of members of the BMP family in cardiogenesis and its dysregulation serves as a potential source of pathogenesis for HLHS studies.
While this section does not aim to provide a comprehensive review on the topic of cardiac signaling pathways, the selected pathways offer helpful context for subsequent discussion on the use of stem cell technologies in uncovering HLHS mechanisms. Table 1 lists some key cardiac developmental signaling pathways discovered thus far including some yet to be associated with HLHS. Beyond signaling pathways, some transcription factors have also been investigated in the pathogenesis of HLHS with many of them thought to interact closely with cardiac development pathways.
2.2. Transcription Factors Underpinning Cardiac Development and HLHS
Part of the reason why HLHS etiology remains difficult to elucidate is the multitude of transcription factors, growth factors and signaling pathways involved in normal cardiac development (Table 1). They work synergistically with multiple molecules that must function in tandem [101,102,103]. A single factor can exert multiple permissive and inhibitory effects on other pathways in a precise time-dependent manner with dysregulation at any stage leading to downstream effects [101,104,105]. Key transcription factors implicated in normal cardiac function include HAND1/2 [106], NKX2.5 [62], GATA4 [107], MYRF [64], ISL1 [108], TBX1/5 [109], MEF2C [110] among others. This section focuses on transcription factors with the strongest evidence from literature supporting their involvement in HLHS. Other factors listed in Table 1 remain crucial for cardiogenesis although their roles in HLHS are currently less well-defined.
NKX2.5 is an essential homeobox transcription factor expressed in early cardiac progenitors and is responsible for heart tube formation, chamber specification and heart looping [111]. Studies have shown that interactions between NKX2.5 and other transcription factors promote CM differentiation [112], with NKX2.5 and HAND2 interactions crucial for ventricular identity [106]. NKX2.5 knockout mice [113] and zebrafish [114] exhibited severe cardiac defects including abnormal conduction system, impaired heart tube and ventricle development [115]. In patient cohort studies, NKX2.5 variants have been associated with various CHDs [116], however no strong association with HLHS was established [63]. As a result, patient-derived iPSCs are being used to further investigate the exact role of NKX2.5 in HLHS [61].
Similarly, HAND1, a basic helix-loop-helix (bHLH) transcription factor, interacts with transcription factors such as NKX2.5 and GATA4 [117] to regulate CM differentiation [118]. Crucially for HLHS, HAND1 plays a critical role in left heart development by specifying LV identity [119]. Genetic disruptions of HAND1 in animal models confirmed its critical role in cardiac development. Evidence by the removal of HAND1 leading to severe cardiac malformations including poorly formed or missing LV [119,120], resembling features seen in HLHS. In human studies, sequencing of patient cardiac tissue has identified a recurrent frameshift mutation (A126fs) leading to a truncated HAND1 protein [60]. However, follow-up studies using mouse models engineered with the same mutations were unable to replicate a hypoplastic LV [121]. Instead, mice with the mutation demonstrated increased embryonic lethality and structural abnormalities. These findings reinforce the importance of HAND1 in normal cardiac development although its specific role in HLHS appear more contributory rather than causative, consistent with current understanding of HLHS etiology.
Beyond transcription factors, some vital structural and regulatory proteins such as MYH6, LRP2, and GJA1 amongst others have also been proposed as contributing factors for HLHS [33]. In addition, multiple chromosomal syndromes such as Turner’s, Jacobsen’s, Digeorge, Holt-Oram and Edward’s syndrome have been associated with HLHS to various degrees [2,122], further highlighting the multifactorial etiology of HLHS and its complexity.
3. Application of Stem Cell in HLHS as an Adjunct Treatment
Unsurprisingly, no effective medication is currently available for HLHS patients due to its complicated and multifactorial etiology. Although early staged surgical intervention could extend life expectancy and improve quality of life for patients. Long-term efficacy remains poor, as evidenced by the very high 1-year mortality with the Norwood procedure (15 % to 60 %) [123]. This highlights the need for alternative therapeutic options such as stem cell therapy which may provide long-term benefits to HLHS patients. Stem cell research has advanced our understanding of human disease etiology and expanded our treatment options for a variety of CHDs including HLHS over the past few decades. Moreover, the recent advances of novel stem cell technologies, such as using patient-specific iPSC and organoids has enabled scientists to study HLHS from a precise perspective which may lead to therapeutic development.
Broadly speaking, stem cells can be classified into PSC and adult stem cells. Adult stem cells include hematopoietic stem cells, mesenchymal stem cells (MSCs) and fetal adult stem cells such as umbilical cord stem cells, placental stem cells among others. Whilst many types of stem cells have been applied to study HLHS, adult stem cells have received the most attention culminating in many small-scaled, early-phased clinical trials [19]. In this section, we review selected preclinical and clinical trials that investigate the role of adult stem cells in improving HLHS outcomes in addition to providing updated insights. (Table 2, Figure 1).
3.1. Umbilical Cord Derived Stem Cells
The umbilical cord is a readily available supply of stem cells, consisting of umbilical cord blood mononuclear cells (UCB-MNCs) isolated from blood and mesenchymal stem cells (UCB-MSCs) derived from Wharton’s jelly. UCB-MSCs exhibit a better proliferative capacity, superior mesodermal differentiation potential and higher level of secretion of growth factors compared to other sources of MSCs and other adult stem cells [129,130]. Preclinical investigation using UCB-MSCs in neonatal animal models of RV overload has demonstrated possible therapeutic benefits relevant to a HLHS overloaded state. Davies et al used neonatal ovine models receiving intramyocardial UCB-MSCs to demonstrate improvements in RV ejection fraction (RVEF), reduced fibrosis and increased recruitment of endogenous progenitors [131]. Notably, data from this preclinical study also suggest that the majority of benefits are attributed to the indirect effects of UCB-MSCs to enhance neovascularisation, reduce inflammation and ultimately adverse remodeling, rather than their direct differentiation into CMs [19].
Promising preclinical data have prompted translational efforts in applying UCB-MNCs in neonates with HLHS. Phase I trials investigating the safety of autologous umbilical cord blood-derived cells (NCT01883076) were conducted at Mayo Clinic with intramyocardial injection of UCB-MNCs during the Glenn procedure [126]. They were able to demonstrate that cord cell collection, processing and intramyocardial delivery were feasible and safe with no procedure-related serious adverse events. Echographic follow-up over 6 months, including measurements of RVEF, RV fractional area change, RV index of myocardial performance, demonstrated no evidence of adverse RV remodelling. These findings were supported by inflammatory biomarkers, which remained stable or downtrending, suggesting no evidence of long-term harm from the procedure [126].
Building on evidence from the Mayo clinic trials, Brizard et al [127] used a novel cardioplegia solution during Norwood operation to infuse UCB-MNCs. They reported 3 deaths which were considered unrelated to therapy, with remaining survivors demonstrating desired RV function at the time of stage II operation. Although preclinical studies giving us the mechanistic rationale of treatment and early clinical trials being promising, some UCB-MNC specific limitations remain. Most notably, challenges may arise when collecting viable umbilical cord blood in HLHS patients who are already at increased risk of hemodynamic instability [132]. Further optimisation of collection protocols and long-term follow-up data are urgently required before clinical translation can be implemented.
3.2. Bone Marrow Stem Cells
In addition to the umbilical cord, MSCs can also be sourced from bone marrow in the form of BM-MSCs [16]. BM-MSCs, much like their counterpart in the umbilical cord, is also a potential candidate for HLHS therapy. They exhibit multipotency, low immunogenicity and strong immunomodulatory effect [133] and can be easily isolated and collected with proven safety in vivo [134]. These properties are supported by extensive clinical, preclinical and translational data [135]. Although in vitro studies showed that BM-MSCs with manipulation are capable of differentiating into mesodermal lineages including endothelial cells [136] and CM-like cells [137], their primary therapeutic benefits do not derive direct cell replacement. Instead, BM-MSCs are thought to promote angiogenesis [138], reduce oxidative damage [139], inhibit tissue fibrosis, and prevent apoptosis [140] via paracrine signaling or through secretion of exosomes.
Using a porcine model, Wehman et al showed epicardial injection of BM-MSCs minimised cardiac hypertrophy, increased capillary density and preserved RVEF without any serious adverse events [141]. Building on these findings, Liufu et al simulated RV pressure overload in mouse models using pulmonary artery banding. They found that neonatal BM-MSCs exhibited age-dependent differences in vascular endothelial growth factor (VEGF) secretion and paracrine activity, resulting in improved RV function [142]. Although informative, this study also suggests that BM-MSCs provided meaningful benefits restricted to cells collected from very young donors, posing serious ethical challenges for their use in HLHS. Nonetheless, multiple research groups have conducted phase I/II clinical trials using BM-MSCs from adult volunteers with some promising results. The ELPIS trial was able to demonstrate safety and potential benefits of intramyocardial injection of allogeneic BM-MSCs (Lomocel-B) [20], which has seen progress into the phase IIb ELPIS II trial (NCT04925024). ELPIS II aims to recruit 38 patients for a blinded, randomised control trial to provide more rigorous evidence of efficacy compared to the open, non-randomised, single-arm ELPIS phase I.
A separate phase I/II randomised study investigated the benefits of mesenchymal precursor cells (MPCs) in patients with HLHS. The Mesoblast MPC trial (NCT03079401) [143] used rexlemestrocel-L, a highly purified population of STRO-3+ BM-MPCs derived from adult volunteers, to treat HLHS. 10 controls and 9 BM-MPC treated patients were followed up over a period of 24 months, with their cardiac parameters measured by 2D echocardiography, 3D echocardiography, cardiac MRI and catheterisation. When indexed for body surface area, the BM-MPC group demonstrated significant improvements in multiple 2D and 3D echocardiography parameters [143] including LV end diastolic volume and end systolic volume. However, such improvements were absent in cardiac MRI findings. Due to the conflicting results and underpowered nature of the study, no definitive conclusion should be made regarding the efficacy of BM-MPC in HLHS. Despite this, the feasibility and safety demonstrated by the study once again supports the rationale for future, more well-powered BM-MPC studies for HLHS. Interestingly, the authors also noted a higher rate of successful biventricular circulation, a procedure that significantly improves prognosis, with 5/5 BM-MPC patients having successfully completed the surgery compared to 4/7 for control [143]. Although limited by small sample sizes, these preliminary data raise the hypothesis that BM-MPC therapy may improve success rates of biventricular circulation in HLHS patients, which may warrant better-powered studies in the future.
In addition to BM-MSCs, bone marrow harbours other stem cell populations including endothelial progenitor cells and hematopoietic stem cells which have been studied extensively and widely used for many hematological conditions [144,145,146]. However, limited evidence exists which supports any potential benefit of non-mesenchymal bone marrow-derived stem cells in HLHS patients. To date, only one case report has described a 25 year old HLHS patient receiving intracoronary infusion of autologous BM-MNCs [147]. No serious adverse events were recorded and the patient saw significant improvement in RVEF most notably 3 months post infusion with an increase from 30% to 40%. This case suggests BM-MNCs may warrant further investigations following palliative surgery in HLHS.
3.3. Cardiac Stem and Cardiosphere-Derived Cells
Cardiac stem cell (CSC) is another source of stem cells that have been investigated as a potential therapy in HLHS. The concept of using CSCs for cardiac diseases has evolved significantly within the last two decades. Earlier efforts focused on a specific group of endogenous CSCs known as c-kit cells for the regeneration of new CMs following cardiac injury. However, multiple subsequent studies have failed to replicate c-kit cells’ cardiomyogenic potential [148,149]. As a result, the exact therapeutic potential of c-kit cells remains unclear, diverting research efforts into alternative CSC populations. Current CSC research primarily focuses on cardiosphere-derived cells (CDCs). These cells are derived from cardiospheres that comprise a heterogeneous population containing mesenchymal cells, c-kit cells and endothelial cells [150]. Preclinical studies using CDCs were able to demonstrate improved cardiac remodelling in infarcted myocardium of murine [151,152] and porcine [153,154] models. Specifically, compared with controls, CDCs reduced scar size, improved ventricular compliance and function [152] and enhanced neovascularisation [154]. Importantly, in models simulating RV overload similar to a post-surgical HLHS state, CDCs improved RVEF and reduced cardiac fibrosis, with the mechanism thought to be through paracrine effects [155].
Based on the promising outcome in pre-clinical studies with CDCs, the 2015 TICAP trial (Transcoronary Infusion of Cardiac Progenitor Cells in Patients With Single-Ventricle Physiology) was the first to utilise CDCs in the context of HLHS patients [124]. Fourteen infants due to undergo stage II and III palliative surgery were either given CDC intracoronary therapy or control. At 18 months, RVEF increased from 46.9±4.6% to 54.0±2.8% (p=0.0004) in the CDC group. Further functional improvements in heart failure status measured by the New York University Paediatric Heart Failure Index (NYUPHFI) [124] were observed.
The later, larger, phase II trial PERSEUS (Cardiac Progenitor Cell Infusion to Treat Univentricular Heart Disease) similarly evaluated the efficacy of intracoronary CDCs during stage II/III palliative surgery in 34 paediatric patients [125]. Analysis at three months post therapy demonstrated an improvement in RVEF of +6.4% in CDC group versus +1.3%; (p=0.003) in control. Subsequently, patients in the control group were given the option of receiving CDCs 4 months after surgery with all 17 patients electing to do so [125]. In these patients, RVEF improved to 38.8% from 34.8%; p<0.0001 following CDC infusion, corroborating with initial cohort response. Secondary outcomes including heart failure status, quality of life and somatic growth also improved. Follow-up analysis using combined data from TICAP and PERSEUS by Sano et al [156] compared controls to treatment and found significantly improved ventricular function with lower rates of complications and follow-up procedures. Similarly, Tauri et al [157] conducted a 3 year follow-up on TICAP patients and confirmed persistently improved RVEF (+8.0%vs +2.2%; p=0.03) with no serious long-term complications noted. Long-term follow-up analysis of TICAP/PERSEUS trials confirmed that CDC infusion was associated with lower hazards of late failure and adverse events, indicating durable clinical benefit of CDC therapy in patients with heart failure with reduced ejection fraction over 8 years [158]. Despite limitations of small sample size, heterogeneity in patient staging and lack of blinding analysis, early phase clinical trials provide sufficient evidence for more rigorous future studies that can validate therapeutic potential of CDCs in HLHS.
4. PSC Derived Cardiomyocytes for Studying HLHS
4.1. PSC-Derived Cardiomyocyte from HLHS Patients
Since the discovery of iPSCs by Yamanaka et al in 2006 [159], their application in CHD has yielded new insights into pathogenesis and novel therapeutics [160,161]. Briefly, iPSC are reprogrammed from somatic cells such as dermal fibroblasts harvested from a donor into a pluripotent state that closely resemble that of ESCs [162]. This reprogramming is achieved via the ectopic transduction of a combination of key transcription factors (OCT4, SOX2, KLF4 and c-MYC collectively known as OSKM) into dermal fibroblasts [162]. OSKM initiates the reversal of differentiation via epigenetic remodeling, silencing of somatic lineage gene enhancers and the activation of pluripotency associated gene enhancers. This reprogramming induces widespread changes resulting in cells with altered metabolism, signaling and nuclear architecture. Due to clonal competition and heterogeneity, the vast majority of cell colonies do not successfully transition into iPSCs [163]. Surviving and suitable iPSC colonies are selected and screened for future use by analysing their karyotype stability, pluripotency and trilineage differentiation potential in vitro and in vivo [163].
Once the iPSCs have been validated, the next step is directed differentiation into viable CMs. Currently, there is no universally accepted protocol for iPSC-CM derivation, though various protocols have been developed to generate chamber-specific CMs [21,164,165]. Multiple studies have shown that patient-specific iPSC-derived CMs could be a powerful tool to investigate HLHS pathogenesis and the causal effects of genetic variants on HLHS phenotypes or etiology (Table 3). In HLHS, the protocol of iPSC-CM generation for ventricular CMs remains the most clinically relevant and involves the manipulation of the Wnt/β-catenin signaling pathway [21]. During the first 24 hours, iPSCs are induced into mesoderm using a Wnt agonist, typically CHIR99021. Following mesoderm induction, inhibition of Wnt is achieved with IWP-2, IWP-4 or IWR-1 around day 3-4 of CM differentiation. By doing so, mesoderm is guided towards a cardiomyocyte lineage. Insulin can be added from day 7 onwards to support cell growth and survival [166], with spontaneous contracting clusters of CMs emerging at this stage [167]. Purity of the CM population is enhanced through the metabolic selection of cells by culturing them in glucose-free and lactate-rich medium. Lactate-rich medium promotes the preferential survival of CMs that is capable of utilising oxidative metabolism [168]. Final validation of iPSC-CMs is achieved through immunostaining or flow cytometry for cardiac markers such as cTnT, a-actinin, structural imaging to assess sarcomeres or electrophysiological assays [167].
4.2. Human iPSC-Derived Cardiomyocytes as Disease Modelling for HLHS
Advances in iPSC technology have enabled high-resolution disease modeling for CHDs such as HLHS. By reprogramming dermal fibroblasts or other cells from HLHS patients into iPSCs and subsequently differentiating them into CMs [178,179], researchers are able to more accurately model HLHS in-vitro.
Using the aforementioned techniques, several studies were able to demonstrate that HLHS patient-derived iPSC displayed impaired CM differentiation, decreased proliferation capacity, and altered expression levels of key cardiac markers. In addition, these iPSC-CMs exhibited downregulation of biological pathways related to cell cycle, DNA replication, and DNA repair, reduced capacity to form beating clusters, reduced oxygen consumption rate and ATP production, disorganized sarcomere structure, abnormal calcium transient patterns, and altered electrophysiological properties [72,80,170,173,176,180] (Table 3). Kobayashi et al showed that key transcription factors including HAND1/2, NKX2.5 and NOTCH-1 were significantly downregulated in HLHS iPSC-CMs [61]. Epigenetic modifications are thought to contribute to the downregulation of these genes in HLHS-CMs. Specifically, reduced H3K4 dimethylation and elevated H3K27 trimethylation at the NKX2.5 promoter were identified in HLHS iPSC-CMs. These changes align with the transcriptional silencing of NKX2.5 and downregulation of cardiac specific marker genes such as TNNT2 and NPPA [61]. In addition, HLHS iPSC-CMs showed reduced contractility and altered calcium handling signaling, suggesting an intrinsic CM defect as a key part of HLHS pathogenesis rather than solely as a consequence of abnormal blood flow during fetal development.
Later studies such as Yang et al derived iPSCs from 5 HLHS patients to further investigate NOTCH signaling pathway defects as a key driver of HLHS pathogenesis [72]. Exome sequencing using patient fibroblasts highlighted significant deletions in multiple aspects of the NOTCH pathway. HLHS-derived iPSCs displayed multiple abnormalities of NOTCH pathways. These include reduced NOTCH receptors and downstream target effects, diminished generation of cardiac progenitor cells, decreased CM contraction rate and an increased propensity towards smooth muscle relative to control iPSCs [72]. Reversal of defective NOTCH signaling using a Jagged-1 peptide, a NOTCH ligand, was able to restore normal CM functions by improving sarcomere organisation and beating frequency of HLHS iPSC-CMs [72]. These results support the role of dysfunctional NOTCH signaling as an important contributor to pathogenesis in HLHS.
More recently, Ye et al [171] employed CRISPR/Cas9 to generate NOTCH1-knockout iPSCs and demonstrated that NOTCH1 deficiency disrupts cardiac progenitor differentiation. NOTCH1-knockout iPSCs exhibited a significant preference towards atrial differentiation with disrupted ventricular lineage differentiation and suppressed proliferation of CMs via downregulation of NOTCH and WNT downstream effects. Single-cell RNA sequencing revealed that NOTCH1 plays a critical role in cardiac mesoderm transformation into FHF, which contributes to LV formation. This provides an additional mechanism for the ventricular hypoplasia observed in HLHS in addition to the “no flow no grow” model.
Studies using HLHS iPSC-CM models suggest that NOTCH pathway defects may be amplified by dysregulated nitric oxide (NO)-dependent signaling during early cardiogenesis [174]. HLHS iPSC-CMs consistently displayed lower levels of NO and decreased activation of NICD, contributing to defective early cardiac lineage differentiation. Such a linkage is further evidenced by the partial restoration of differentiation capability and CM maturation with the supplementation of NO.
Altogether, these iPSC-based studies provide compelling evidence that HLHS is driven by intrinsic defects in cardiogenesis and dysregulation of signaling pathways such as NOTCH1, NKX2-5 and HAND1 (Table 3). Patient-specific iPSC-CM models have expanded our understanding of HLHS beyond the previously dominant theory of hemodynamic compromise by identifying significant molecular and genetic contributions to disease. Improved understanding of disease modelling and etiology will inform future therapeutic development and may enable personalised treatment strategies.
4.3. HLHS iPSC-CMs: A Platform for Drug Discovery and Evaluating Drug Toxicity
Recent progress in identifying growth factors, transcription factors and signaling pathways critical to HLHS pathogenesis has also established potential therapeutic targets. Patient-specific iPSC-derived CMs have been used as a promising platform to identify and validate potential therapeutics for HLHS (Table 3). Beyond the use of NO [174] and Jagged-1 [34] to rescue NOTCH signaling defects, additional specific targets for HLHS have also been studied as a potential therapeutic option. Paige et al [176] used iPSCs from HLHS patients with the MYH6-R443P variant to show deficient contraction force and velocity of HLHS iPSC-CMs. Subsequent correction of the gene mutation effectively restored contraction and velocity in the HLHS iPSC-CMs. Xu et al [177] also reported an increase in apoptosis and oxidative stress in HLHS iPSC-CMs, features that are frequently observed with early-onset heart failure in clinical settings of HLHS. Treatment with Sildenafil and tauroursodeoxycholic acid reduced apoptosis and oxidative stress in HLHS iPSC-CMs. In addition, partial improvements in mitochondrial and contractile defects with improved sarcomere function were also noted. These findings highlight the possibility of utilising iPSCs in identifying potential cardioprotective compounds for HLHS.
Beyond identifying therapeutic targets, iPSCs have also been proposed as a tool for evaluating drug toxicity in many organs, in particular for the heart [181,182,183]. Compared to traditional animal models and other in vitro systems in drug testing and toxicity assessment, iPSCs offer several distinct advantages. Most notably, iPSCs are generated from human donors which allow for establishing in vitro human models that most accurately reflect human physiology and disease specific phenotypes, thereby enhancing the predictive value of preclinical testing. The scalability of iPSCs makes them highly compatible with high-throughput screening (HTS) technologies which allows for rapid drug evaluation with clearly quantifiable endpoints. Additional benefits with iPSC-CMs may also come from reduced ethical concerns and fewer regulatory barriers compared to animal models.
Currently, one area of cardiology which has seen a strong integration of iPSC-based drug testing and toxicity is the study of arrhythmogenic drugs. This is exemplified by the FDA and counterparts in Japan and Europe, who established the Comprehensive In vitro Proarrhythmia Assay (CiPA), which uses iPSC-CMs to study drugs with high risk of inducing torsades des pointes (tDP) [184,185,186]. The integration of iPSC-CMs into HTS has significantly advanced current and future candidate drug identification alongside toxicity screening. Briefly, HTS is a highly automated system that allows the rapid testing of hundreds to thousands of candidate compounds simultaneously. Miniature assays using iPSC-CMs can generate quantifiable readouts by measuring absorbance or fluorescence in response to compound exposure [187]. Compounds that elicit significant changes in fluorescence or absorbance are then validated in this high efficiency system to identify bioactive molecules or potential toxicity. Overall, HTS significantly accelerates early phase drug testing, especially with the integration of iPSC-CMs. For instance, Huang et al [188] generated iPSC-CMs from 13 HLA-super donors that could represent a significant proportion of the global population. Using HTS, they screened a wide range of compounds and identified dose-dependent toxicity amongst 5 previously known cardiotoxic drugs and a further 4 previously undescribed drugs. Subsequent electrophysiological studies and additional in-vivo studies were able to demonstrate a significant adverse effect on CMs caused by these drugs, thus demonstrating the utility of iPSC-CMs in identifying potential drug toxicities during the preclinical stage.
In the context of HLHS, iPSC-CMs from patients retain patient-specific genetic and epigenetic signatures that allow for study of drug toxicity in a precision medicine approach. Certain compounds tested may exacerbate or alleviate pathological features in some subsets of HLHS, whilst having minimal effect on others. HTS platforms employing HLHS-specific iPSC-CMs allow for rapid evaluation of candidate drugs by measuring their potential effects on endpoints such as electrophysiological stability, viability, and mitochondrial functions. Given the limited availability of non-surgical options and systemic complications arising from lifelong hemodynamics stress, novel medications discovered using HLHS-specific iPSC-based HTS could provide safe, effective and personalised pharmacological interventions to HLHS patients.
4.4. Limitations of iPSC-CMs 2D Model
Although the advent of iPSC-CMs has seen significant progress in elucidating the etiology and therapeutic target identification of HLHS, important limitations remain which must be acknowledged. One of the most frequently cited limitations is the immaturity of iPSC-CMs. Immature iPSC-CMs more closely resemble the fetal CMs with different organisation, calcium handling, electrophysiology and metabolism. This differs from the high pressure, post-natal physiology seen in HLHS patients [189,190,191]. This limitation is particularly relevant when assessing the translational potential of iPSC-CMs based techniques such as cardiac patches. Whilst preliminary data may be positive, more comprehensive analysis of clinical outcomes will be needed to ensure that iPSC-CMs based therapies can integrate effectively without significant adverse effects of arrhythmias, tumorigenesis or immune rejection.
The issue of iPSC-CM immaturity has been addressed by groups using numerous strategies. One possible way to achieve more mature CMs is to apply mechanical stretching alongside electrical stimulation to iPSC-CMs [192,193]. The resulting iPSC-CMs exhibited better calcium handling ability, increased mitochondrial density, improved sarcomere length and organization, and a gene expression profile more akin to adult CMs. Moreover, T-tubule formation alongside enhanced calcium release and improved excitation-contraction coupling were observed in iPSC-CMs treated with hormones such as triiodothyronine and dexamethasone [194]. Furthermore, metabolic strategies using fatty acid supplementation have also been shown to induce a shift from glycolysis to oxidative phosphorylation alongside improving sarcomere organization in iPSC-CMs [195]. Recent literature suggests combining multiple approaches of maturation including metabolic medium optimisation, electrostimulation and culturing in nano-patterned substrates can act synergistically to substantially improve maturation [196]. Collectively, these strategies for maturing iPSC-CMs can be used to generate more physiologically relevant cardiac models to complement existing iPSC-CM studies for HLHS and beyond.
A major challenge of HLHS research remains its complex multifactorial nature. Extensive genetic heterogeneity, copy number variants [197], chromosomal abnormalities and even maternal [198] and environmental impacts [199] have been attributed to risk factors for HLHS. However, many studies using iPSC-CMs fail to capture these complex interactions and focus more on specific genetic or signaling pathway defects. Current iPSC-CMs models often oversimplify the complex nature of cardiac development by predominantly focusing on CMs whilst neglecting the role of endothelial, valve and vascular smooth muscle cells in cardiogenesis. Recognition of these challenges and developing solutions to overcome them will be key to generating highly clinically relevant findings.
5. Implications of hiPSC-Derived 3D Cardiac Patches for Treating HLHS
3D cardiac patches or engineered heart tissues (EHTs) offer an alternative use of iPSCs for modelling HLHS and exploring potential therapies. Briefly, cardiac patches are generated initially using iPSC or other stem cells, they are then differentiated into the desired cell types such as CMs, endothelial cells and cardiac fibroblasts. These cells are seeded onto a biomaterial scaffold that supports growth and is designed to mimic the extracellular matrix (ECM) [200]. The scaffold can either be entirely synthetic made from polymers such as polyglycolic acid (PGA) and polycaprolactone (PCL) or from decellularised ECM [201]. Once seeded, the patch is cultured in a bioreactor to promote tissue maturation and form a functional cardiac patch (Figure 2).
Unlike 2D monolayers of iPSC-CMs which fail to replicate complex structural defects, 3D cardiac patches provide a more physiologically relevant model of HLHS [202]. Krane et al [173] used 3D heart patches derived from iPSCs to investigate deeper underlying intrinsic defects associated with HLHS (Figure 2). Corroborating evidence from 2D models, 3D cardiac patches generated from HLHS iPSCs were able to demonstrate a significant increase in MLC2a+ cells and a reduction in MLC2v+ cells representing atrial and ventricular cells respectively, thus indicating a poor maturation response to growth [173]. Importantly, HLHS iPSC-derived 3D cardiac patches were able to uncover additional evidence of DNA damage and CM apoptosis, with roughly 50 percent of CMs demonstrating three or more nuclei compared to roughly 5 percent in control cardiac patches. Analysis of cell cycle markers of Ki67, representing active cycling and PH3 representing mitosis, showed that although more HLHS cells initially entered the cell cycle, few cells completed mitosis, indicating a severe disruption within the cell cycle. Further analysis showed a strong association between multinucleated cells with increased apoptosis as indicated by the increased TUNEL+ and cleaved caspase-3 levels, both representing DNA damage and programmed cell death [173]. Together these results signify a strong genetic and cellular basis of HLHS occurring independently of hemodynamic factors. Furthermore, despite the heterogeneity of HLHS, this study was able to demonstrate a convergence of de novo mutations resulting in aberrant key pathways linked to cardiac development, chromatin organization, and cell cycle phases [173]. These findings highlight potential therapeutic targets that target common dysregulated pathways may be more effective than focusing on individual target mutations.
Conventional cardiac patches made from bovine pericardium or synthetic materials such as GoreTex or polyester are routinely used in clinical practice for the repair of many CHDs including HLHS [203,204]. Compared to conventional patches, cardiac patches derived from iPSC-CMs can integrate into native tissue, conduct impulses and revascularise damaged areas of the heart [205,206,207]. These patches are biodegradable, hence eliminating the need for multiple reinterventions and reducing the likelihood of fibrosis and calcification [208]. Many preclinical trials have investigated cardiac patches as a therapeutic option in cardiovascular disease, especially for ischemic heart disease and heart failure. Heart failure in particular is a highly relevant long-term complication of HLHS. Although surgical advances have improved survival for HLHS patients, the resulting single RV is poorly suited for its new role of long-term systemic circulation, often resulting in RV failure and the eventual need for transplantation. In fact, alongside arrhythmias, heart failure is the leading cause of morbidity amongst HLHS patients following surgical repair [209].
Recent studies in large and small animal models have demonstrated potential of iPSC-CM based cardiac patches in remuscularising infarcted myocardium. These patches are able to successfully integrate within the host structure and restore cardiac contractile and physiological functions in the animal models [205,206]. Building on these initial studies, Querdal et al established a dose-dependent relationship between cardiac patches size and functional recovery in guinea pig models, further validating their therapeutic potential [210]. Similar studies were able to confirm these benefits in their respective models with no significant adverse effects such as arrhythmias or tumorigenesis observed [208,211]. Given the likelihood of RV failure in HLHS, iPSC-CM patches may be used to support the overworked RV after surgical intervention and even as a tool to repair the hypoplastic LV.
Aside from preclinical trials, complete data from late-phased clinical trials on iPSC-CM patches have yet to be published to date. Nonetheless, relevant clinical trials such as in the bioVAT-HF phase 1/2 trial (NCT04396899) are actively recruiting participants. Following preclinical validation on rats and rhesus macaques, the trial aims to evaluate the efficacy of engineered heart muscle (EHM), a form of cardiac patches derived from stromal cells and iPSC-CMs, can be safely and effectively implemented to improve cardiac function in heart failure patients. So far, Zimmerman et al has been recruiting patients with advanced heart failure with an ejection fraction less than 35% and no realistic option of heart transplant. A recent update published by the group demonstrates a proof of concept for the use of EHM in humans. This is highlighted by the study of a patient’s heart with EHM implanted after the patient had received a successful heart transplant. The explanted heart contained viable human CMs that were vascularised indicating successful integration of the EHM with no signs of adverse outcomes such as tumour formation, immune rejection or arrhythmias [206]. Although wider implications of a significant therapeutic benefit cannot be derived from a single case, the evidence thus far supports the continuation of the broader clinical trial. This trial along with other isolated case reports in humans suggests the feasibility of using cardiac patches as a part of the larger HLHS therapy and in particular in the case of post-surgical RV failure. Further HLHS-specific preclinical studies will be required before clinical translation can be safely applied.
6. Future Directions
Despite substantial advances in HLHS mechanism and therapy that can be attributed to stem-cell based technologies, major limitations exist. Current models still fail to recapitulate the complexity of cardiac development with clinical applications limited to early-phase trials. Emerging tools such as 3D bioengineering and organoids [212,213] aim to further improve model fidelity and increase translational potential.
6.1. Cardiac Organoids: Better Model for HLHS?
HLHS consists of underdevelopment of multiple structures of the left heart including the LV, mitral valve, aortic valve, ascending aorta accompanied by genetic and cellular defects. While 2D iPSC derived models and traditional animal models have previously given us insight into HLHS pathogenesis, they fail to capture the complex and variable nature of HLHS. The emergence of cardiac organoids (COs) or cardioids has proven to be a better tool to model CHDs including HLHS. COs are self-organising 3D structures derived from PSCs (iPSCs and ESCs) [169,183]. Multiple experimental protocols have been reported to generate COs from human PSCs (Figure 3). They consist of CMs, endothelial cells and fibroblasts that aggregate together to resemble native cardiac tissue, architecture and functional dynamics [169,214]. Interestingly, some COs display properties of cardiac looping, polarity and even chamber formation similar to that of human embryonic heart development [215]. Once generated, these COs are capable of spontaneous rhythmic contractions with some studies even demonstrating the ability to derive vascularised and chambered COs [216]. Together, these properties make cardioids excellent platforms to study CHD such as HLHS.
Much like its 2D counterparts in iPSC-CMs, COs have been applied to model HLHS to uncover even more insights into underlying etiology. A landmark study by Hofbauer et al [169] highlights how 3D self-organising cardioid models can advance our understanding of pathogenesis beyond data provided by 2D iPSC models alone. Focusing on the role of HAND1, a transcription factor implicated in LV development, the study used CRISPR-Cas9 mediated knockout of HAND1 in iPSC to evaluate its role during cardioid formation. They were able to observe several key differences between HAND1-KO and control cardioids. Although HAND1-KO cardioids were still capable of specification into TNNT2+ CMs, they consistently failed to form cavities or formed significantly smaller and disorganised cavities. These findings indicate that HAND1 is essential for chamber morphogenesis but not for cardiac lineage commitment) [169].
Parallel NKX2.5-knockout cardioids were also conducted and did not show any cardiac cavity abnormalities or effect on HAND1 levels during the mesodermal stage. However, HAND1 levels in NKX2.5 KO cardioids were significantly reduced in the CM stage, suggesting that HAND1 operates downstream of NKX2.5 in a stage-specific manner during cardiac development [169]. Subsequently, the authors investigated the upstream regulation of HAND1 by manipulating levels of BMP to assess its impacts on downstream signaling pathways. Elevated BMP activity led to an increased HAND1 expression and improved cavity formation while BMP inhibition had the opposite effect [169]. This establishes the critical importance of the BMP-HAND1 axis in controlling chamber formation. Overall, the cardioid model in this study could unlock detailed understanding of gene regulation and signaling pathways during cardiogenesis beyond what a 2D iPSC-CMs model can provide. (Figure 3).
Alternative protocols for generating COs have also been used to study early human cardiogenesis. Drakhlis et al [215] used a protocol to generate COs from human PSCs embedded within Matrigel. The generated COs contained complex structures encompassing foregut endoderm tissue and vascular tissue alongside cardiac cells which they termed heart forming organoids (HFOs). HFOs with knockout of NKX2.5, a gene heavily implicated in HLHS, exhibited a much less compact cardiac tissue and a larger size alongside a greater proportion of disorganised sarcomeres [215]. In addition, NKX2.5-KO HFOs displayed an altered gene expression profile with an increase in markers for smooth muscle differentiation whilst genes associated with normal cardiac development such as IRX4 and NPPA were downregulated, indicating a deviation from normal cardiac cell fate [215]. Although not specifically tailored towards HLHS, the results confirm the possibility of using 3D CO models to study genes implicated in HLHS.
Beyond HLHS, COs have been employed for the study of congenital cardiac conditions. For instance, in the study by Lewis-Israeli et al [214], COs were used to investigate how maternal risk factors, such as pregestational diabetes may affect cardiogenesis and contribute to CHD risk. Other common cardiac conditions such myocardial infarcts have also been successfully replicated using Cos-based models, thus providing a robust alternative to animal models [217,218,219]. Aside from disease modelling, COs have been evaluated for their use in drug toxicity as well as screening therapeutic compounds [183,218]. It is reasonable to assume that HLHS-specific COs will be increasingly used to investigate HLHS pathogenesis and evaluate novel therapeutics for HLHS.
Although 3D cardiac patches and COs have shown promise, one possible future research direction would be to include the use of patient derived iPSC-COs to investigate HLHS associated genes. Whilst current 3D cardiac patches and COs are already more complex than 2D traditional models, moving beyond primitive heart modelling will require even more sophisticated organoids that incorporate anatomically accurate atria, ventricles, conduction systems, and immune components alongside neural crest integration (Figure 4A). Of note, a recent study showed that the addition of 2 μM CHIR99021 during the first 2 days of CO formation and transient 4-day addition of 3 μM DY131 combined with 10 μM MK8722 (days 24–28) significantly improved CO maturation, enabling complex disease modeling and drug discovery [220].
The creation of fully developed, matured, and chambered COs or cardiac patches that can capture salient features of HLHS will no doubt provide more physiologically relevant models. Integration of these highly accurate HLHS COs or cardiac patches into body-on-chip systems coupled with pumps to allow for high pressure microfluids can facilitate the study of hemodynamic challenges in HLHS. Beyond disease modelling, enhanced COs platforms and improved 3D cardiac patches can facilitate more applications for HLHS, such as high-throughput drug screening and the eventual development of personalised regenerative medicine strategies for individual HLHS patients (Figure 4B).
6.2. 3D/4D Bioprinting PSC-Derived Cardiac Tissues for Studying HLHS
3D bioprinting is another three-dimensional strategy which can provide high fidelity models for studying HLHS. 3D bioprinted tissues build on conventional 3D printing by replacing thermoplastic with cells, often derived from stem cells alongside biomaterials and growth factors to create functional 3D tissue constructs [221]. Currently multiple approaches have been validated for the creation of 3D bioprinted tissue structures [222]. Future research could prioritise systemic optimisation and standardisation of protocols to enhance reproducibility and to enable a more seamless transition into clinical applications. Compared to 2D models which require external maturation, 3D bioprinting using appropriate ECM-like hydrogel produces CMs capable of intrinsic maturation with the structure. 3D bioprinted cardiac tissues displayed spontaneous contractility with organised sarcomeres alongside increased expression of multiple cardiac-specific markers such as MYL2, MYH7, TNNI3, and KCNJ4 [26], supporting the use of 3D bioprinting in HLHS and beyond. To date, most research conducted using 3D bioprinting in HLHS comes from iPSCs derived from healthy volunteers. Once the protocol for generating 3D bioprinted cardiac structures becomes more reliably well-established, the next logical step would be to generate 3D bioprinted cardiac tissue constructs using HLHS-specific iPSCs. This would enable the investigation of HLHS-specific morphogenetic defects and facilitate targeted therapeutics. Although 3D bioprinting of the whole heart remains some way away, smaller tissue constructs such as valves, vessels and cardiac patches may be more precisely recreated than traditional seeding and scaffolding techniques.
Concurrently, recent advances in material sciences have inspired potential hypotheses about 4D bioprinting approaches [223]. Currently a 3D bioprinted tissue structure remains static and relatively unadaptable. The properties of some smart biomaterials allow them to change characteristics such as shape, size, and elasticity in response to a variety of stimuli such as pH, mechanical force, and electrical stimulation [224] (Figure 5). Engineering heart tissue with smart materials could eventually produce 4D bioprinted valves, cardiac patches, even whole hearts in the future that are capable of “growing” and adapting with changes to its environment. This technology would enhance integration into host tissue and reduce the need for surgical revisions that an unadaptable 3D bioprinted structure would likely require, thus representing an excellent option for pediatric conditions such as HLHS.
7. Conclusions
Surgical advances have greatly reduced mortality rates in HLHS, yet long-term complications remain prevalent. Despite extensive research, pathophysiology of HLHS remains incomplete with multiple factors implicated contributing to a highly heterogeneous clinical presentation. Stem cell-based techniques have provided an alternative avenue to study HLHS pathogenesis by uncovering complex, intrinsic molecular-level transcriptional defects in HLHS cardiomyocytes. Early-phase clinical trials using adult stem cell populations have demonstrated safety and feasibility with ongoing studies investigating potential therapeutic efficacy. Emerging stem cell techniques in the form of COs and multi-dimensional bioprinting tissue constructs have yielded ever more sophisticated, high-fidelity human models that replicate key disease features. These advances deepen our mechanistic understanding of HLHS and provide robust platforms which can be used in HTS drug screening and development of personalised regenerative medicine strategies.
Author Contributions
Conceptualization, R.X. and Q.X.; methodology, formal analysis, and investigation, R.X. and H.D.; Figure preparation, Q,X,; resources, Q.X.; writing—original draft preparation, R.X., and H.D.; writing—review and editing, Z,K. and Q.X.; supervision, Q.X.; project administration, Q.X.; funding acquisition, Q.X. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by British Heart Foundation (PG/15/11/31279, PG/15/86/31723, PG/20/10458, and PG/23/11371 to Q.X). This work forms part of the research portfolio for the National Institute for Health Research Biomedical Research Centre at Barts.
Institutional Review Board Statement
Not applicable for this review article.
Informed Consent Statement
Not applicable for this review article.
Data Availability Statement
Not applicable for this review article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HLHS | hypoplastic left heart syndrome |
| PSC | pluripotent stem cell |
| iPSC | induced pluripotent stem cell |
| CHD | congenital heart disease |
| CM | cardiomyocyte |
| RV | right ventricle |
| LV | left ventricle |
| FHF | first heart field |
| SHF | second heart field |
| EF | ejection fraction |
| BM-MSC | bone marrow-derived mesenchymal stem cell |
| BM-MNC | bone marrow-derived mononuclear cells |
| CDC | cardiosphere-derived cells |
| UCB-MSC | umbilical cord blood-derived mesenchymal stem cells |
| UCB-MNC | umbilical cord blood-derived mononuclear cells |
| NKX2 | NK homeobox 2 |
References
- Stallings, E.B.; Isenburg, J.L.; Rutkowski, R.E.; Kirby, R.S.; Nembhard, W.N.; Sandidge, T.; Villavicencio, S.; Nguyen, H.H.; McMahon, D.M.; Nestoridi, E. , et al. National population-based estimates for major birth defects, 2016-2020. Birth Defects Res 2024, 116, e2301. [Google Scholar] [CrossRef]
- Feinstein, J.A.; Benson, D.W.; Dubin, A.M.; Cohen, M.S.; Maxey, D.M.; Mahle, W.T.; Pahl, E.; Villafane, J.; Bhatt, A.B.; Peng, L.F. , et al. Hypoplastic left heart syndrome: current considerations and expectations. Journal of the American College of Cardiology 2012, 59, S1–42. [Google Scholar] [CrossRef] [PubMed]
- Hoshino, K.; Ogawa, K.; Hishitani, T.; Kitazawa, R.; Uehara, R. Hypoplastic left heart syndrome: duration of survival without surgical intervention. Am Heart J 1999, 137, 535–542. [Google Scholar] [CrossRef]
- Alphonso, N.; Angelini, A.; Barron, D.J.; Bellsham-Revell, H.; Blom, N.A.; Brown, K.; Davis, D.; Duncan, D.; Fedrigo, M.; Galletti, L. , et al. Guidelines for the management of neonates and infants with hypoplastic left heart syndrome: The European Association for Cardio-Thoracic Surgery (EACTS) and the Association for European Paediatric and Congenital Cardiology (AEPC) Hypoplastic Left Heart Syndrome Guidelines Task Force. Eur J Cardiothorac Surg 2020, 58, 416–499. [Google Scholar] [CrossRef]
- Ohye, R.G.; Schranz, D.; D'Udekem, Y. Current Therapy for Hypoplastic Left Heart Syndrome and Related Single Ventricle Lesions. Circulation 2016, 134, 1265–1279. [Google Scholar] [CrossRef]
- Norwood, W.I.; Lang, P.; Casteneda, A.R.; Campbell, D.N. Experience with operations for hypoplastic left heart syndrome. J Thorac Cardiovasc Surg 1981, 82, 511–519. [Google Scholar] [CrossRef]
- Lee, M.; Geoffrion, T.R. Norwood Procedure. In StatPearls, Treasure Island (FL) ineligible companies. Disclosure: Tracy Geoffrion declares no relevant financial relationships with ineligible companies., 2025.
- Glenn, W.W. Circulatory bypass of the right side of the heart. IV. Shunt between superior vena cava and distal right pulmonary artery; report of clinical application. The New England journal of medicine 1958, 259, 117–120. [Google Scholar] [CrossRef]
- Fontan, F.; Baudet, E. Surgical repair of tricuspid atresia. Thorax 1971, 26, 240–248. [Google Scholar] [CrossRef]
- Steele, M.M.; Zahr, R.A.; Kirshbom, P.M.; Kopf, G.S.; Karimi, M. Quality of Life for Historic Cavopulmonary Shunt Survivors. World J Pediatr Congenit Heart Surg 2016, 7, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Marshall, K.H.; D'Udekem, Y.; Sholler, G.F.; Opotowsky, A.R.; Costa, D.S.J.; Sharpe, L.; Celermajer, D.S.; Winlaw, D.S.; Newburger, J.W.; Kasparian, N.A. Health-Related Quality of Life in Children, Adolescents, and Adults With a Fontan Circulation: A Meta-Analysis. Journal of the American Heart Association 2020, 9, e014172. [Google Scholar] [CrossRef] [PubMed]
- Dib, N.; Poirier, N.; Samuel, M.; Hermann Honfo, S.; Zaidi, A.; Opotowsky, A.R.; Mongeon, F.P.; Mondesert, B.; Kay, J.; Ibrahim, R. , et al. Cardiovascular Outcomes Associated With Hypoplastic Left Heart Syndrome Versus Other Types of Single Right Ventricle: A Multicenter Study. Journal of the American Heart Association 2024, 13, e034757. [Google Scholar] [CrossRef] [PubMed]
- Yimer, M.A.; Tisma-Dupanovic, S.; Malloy-Walton, L.; Connelly, D.; Noel-Macdonnell, J.; J, O.B.; Papagiannis, J. Post-operative arrhythmias in patients with hypoplastic left heart syndrome and anatomic variants: incidence, type, and course. Cardiol Young 2021, 31, 1412–1418. [Google Scholar] [CrossRef] [PubMed]
- Poh, C.L.; d'Udekem, Y. Life After Surviving Fontan Surgery: A Meta-Analysis of the Incidence and Predictors of Late Death. Heart, lung & circulation 2018, 27, 552–559. [Google Scholar] [CrossRef]
- Chrisant, M.R.; Naftel, D.C.; Drummond-Webb, J.; Chinnock, R.; Canter, C.E.; Boucek, M.M.; Boucek, R.J.; Hallowell, S.C.; Kirklin, J.K.; Morrow, W.R. , et al. Fate of infants with hypoplastic left heart syndrome listed for cardiac transplantation: a multicenter study. The Journal of heart and lung transplantation : the official publication of the International Society for Heart Transplantation 2005, 24, 576–582. [Google Scholar] [CrossRef]
- Pittenger, M.F.; Mackay, A.M.; Beck, S.C.; Jaiswal, R.K.; Douglas, R.; Mosca, J.D.; Moorman, M.A.; Simonetti, D.W.; Craig, S.; Marshak, D.R. Multilineage potential of adult human mesenchymal stem cells. Science 1999, 284, 143–147. [Google Scholar] [CrossRef]
- Zuk, P.A.; Zhu, M.; Mizuno, H.; Huang, J.; Futrell, J.W.; Katz, A.J.; Benhaim, P.; Lorenz, H.P.; Hedrick, M.H. Multilineage cells from human adipose tissue: implications for cell-based therapies. Tissue Eng 2001, 7, 211–228. [Google Scholar] [CrossRef]
- Wang, H.S.; Hung, S.C.; Peng, S.T.; Huang, C.C.; Wei, H.M.; Guo, Y.J.; Fu, Y.S.; Lai, M.C.; Chen, C.C. Mesenchymal stem cells in the Wharton's jelly of the human umbilical cord. Stem cells 2004, 22, 1330–1337. [Google Scholar] [CrossRef]
- Bittle, G.J.; Morales, D.; Deatrick, K.B.; Parchment, N.; Saha, P.; Mishra, R.; Sharma, S.; Pietris, N.; Vasilenko, A.; Bor, C. , et al. Stem Cell Therapy for Hypoplastic Left Heart Syndrome: Mechanism, Clinical Application, and Future Directions. Circulation research 2018, 123, 288–300. [Google Scholar] [CrossRef]
- Kaushal, S.; Hare, J.M.; Hoffman, J.R.; Boyd, R.M.; Ramdas, K.N.; Pietris, N.; Kutty, S.; Tweddell, J.S.; Husain, S.A.; Menon, S.C. , et al. Intramyocardial cell-based therapy with Lomecel-B during bidirectional cavopulmonary anastomosis for hypoplastic left heart syndrome: the ELPIS phase I trial. Eur Heart J Open 2023, 3, oead002. [Google Scholar] [CrossRef]
- Lian, X.; Hsiao, C.; Wilson, G.; Zhu, K.; Hazeltine, L.B.; Azarin, S.M.; Raval, K.K.; Zhang, J.; Kamp, T.J.; Palecek, S.P. Robust cardiomyocyte differentiation from human pluripotent stem cells via temporal modulation of canonical Wnt signaling. Proceedings of the National Academy of Sciences of the United States of America 2012, 109, E1848–1857. [Google Scholar] [CrossRef]
- van Mil, A.; Balk, G.M.; Neef, K.; Buikema, J.W.; Asselbergs, F.W.; Wu, S.M.; Doevendans, P.A.; Sluijter, J.P.G. Modelling inherited cardiac disease using human induced pluripotent stem cell-derived cardiomyocytes: progress, pitfalls, and potential. Cardiovascular research 2018, 114, 1828–1842. [Google Scholar] [CrossRef] [PubMed]
- Caspi, O.; Huber, I.; Gepstein, A.; Arbel, G.; Maizels, L.; Boulos, M.; Gepstein, L. Modeling of arrhythmogenic right ventricular cardiomyopathy with human induced pluripotent stem cells. Circulation. Cardiovascular genetics 2013, 6, 557–568. [Google Scholar] [CrossRef]
- Yazawa, M.; Hsueh, B.; Jia, X.; Pasca, A.M.; Bernstein, J.A.; Hallmayer, J.; Dolmetsch, R.E. Using induced pluripotent stem cells to investigate cardiac phenotypes in Timothy syndrome. Nature 2011, 471, 230–234. [Google Scholar] [CrossRef]
- Lan, F.; Lee, A.S.; Liang, P.; Sanchez-Freire, V.; Nguyen, P.K.; Wang, L.; Han, L.; Yen, M.; Wang, Y.; Sun, N. , et al. Abnormal calcium handling properties underlie familial hypertrophic cardiomyopathy pathology in patient-specific induced pluripotent stem cells. Cell stem cell 2013, 12, 101–113. [Google Scholar] [CrossRef]
- Wolfe, J.T.; He, W.; Kim, M.S.; Liang, H.L.; Shradhanjali, A.; Jurkiewicz, H.; Freudinger, B.P.; Greene, A.S.; LaDisa, J.F., Jr.; Tayebi, L. , et al. 3D-bioprinting of patient-derived cardiac tissue models for studying congenital heart disease. Front Cardiovasc Med 2023, 10, 1162731. [Google Scholar] [CrossRef]
- Alonzo, M.; Contreras, J.; Bering, J.; Zhao, M.T. In Vivo and In Vitro Approaches to Modeling Hypoplastic Left Heart Syndrome. Curr Cardiol Rep 2024, 26, 1221–1229. [Google Scholar] [CrossRef] [PubMed]
- Van Vliet, P.; Wu, S.M.; Zaffran, S.; Puceat, M. Early cardiac development: a view from stem cells to embryos. Cardiovascular research 2012, 96, 352–362. [Google Scholar] [CrossRef]
- Brand, T. Heart development: molecular insights into cardiac specification and early morphogenesis. Dev Biol 2003, 258, 1–19. [Google Scholar] [CrossRef]
- Kirby, M.L.; Waldo, K.L. Neural crest and cardiovascular patterning. Circulation research 1995, 77, 211–215. [Google Scholar] [CrossRef]
- Gitler, A.D.; Lu, M.M.; Jiang, Y.Q.; Epstein, J.A.; Gruber, P.J. Molecular markers of cardiac endocardial cushion development. Developmental dynamics : an official publication of the American Association of Anatomists 2003, 228, 643–650. [Google Scholar] [CrossRef] [PubMed]
- Grossfeld, P.; Nie, S.; Lin, L.; Wang, L.; Anderson, R.H. Hypoplastic Left Heart Syndrome: A New Paradigm for an Old Disease? J Cardiovasc Dev Dis 2019, 6. [Google Scholar] [CrossRef]
- Datta, S.; Cao, W.; Skillman, M.; Wu, M. Hypoplastic Left Heart Syndrome: Signaling & Molecular Perspectives, and the Road Ahead. International journal of molecular sciences 2023, 24. [Google Scholar] [CrossRef]
- Niessen, K.; Karsan, A. Notch signaling in cardiac development. Circulation research 2008, 102, 1169–1181. [Google Scholar] [CrossRef]
- Kerstjens-Frederikse, W.S.; van de Laar, I.M.; Vos, Y.J.; Verhagen, J.M.; Berger, R.M.; Lichtenbelt, K.D.; Klein Wassink-Ruiter, J.S.; van der Zwaag, P.A.; du Marchie Sarvaas, G.J.; Bergman, K.A. , et al. Cardiovascular malformations caused by NOTCH1 mutations do not keep left: data on 428 probands with left-sided CHD and their families. Genet Med 2016, 18, 914–923. [Google Scholar] [CrossRef]
- McBride, K.L.; Riley, M.F.; Zender, G.A.; Fitzgerald-Butt, S.M.; Towbin, J.A.; Belmont, J.W.; Cole, S.E. NOTCH1 mutations in individuals with left ventricular outflow tract malformations reduce ligand-induced signaling. Human molecular genetics 2008, 17, 2886–2893. [Google Scholar] [CrossRef]
- Rahman, A.; DeYoung, T.; Cahill, L.S.; Yee, Y.; Debebe, S.K.; Botelho, O.; Seed, M.; Chaturvedi, R.R.; Sled, J.G. A mouse model of hypoplastic left heart syndrome demonstrating left heart hypoplasia and retrograde aortic arch flow. Dis Model Mech 2021, 14. [Google Scholar] [CrossRef] [PubMed]
- Durbin, M.D.; Cadar, A.G.; Williams, C.H.; Guo, Y.; Bichell, D.P.; Su, Y.R.; Hong, C.C. Hypoplastic Left Heart Syndrome Sequencing Reveals a Novel NOTCH1 Mutation in a Family with Single Ventricle Defects. Pediatric cardiology 2017, 38, 1232–1240. [Google Scholar] [CrossRef] [PubMed]
- Winnier, G.; Blessing, M.; Labosky, P.A.; Hogan, B.L. Bone morphogenetic protein-4 is required for mesoderm formation and patterning in the mouse. Genes & development 1995, 9, 2105–2116. [Google Scholar] [CrossRef]
- Beppu, H.; Kawabata, M.; Hamamoto, T.; Chytil, A.; Minowa, O.; Noda, T.; Miyazono, K. BMP type II receptor is required for gastrulation and early development of mouse embryos. Dev Biol 2000, 221, 249–258. [Google Scholar] [CrossRef] [PubMed]
- Jiao, K.; Kulessa, H.; Tompkins, K.; Zhou, Y.; Batts, L.; Baldwin, H.S.; Hogan, B.L. An essential role of Bmp4 in the atrioventricular septation of the mouse heart. Genes & development 2003, 17, 2362–2367. [Google Scholar] [CrossRef]
- Wang, J.; Greene, S.B.; Martin, J.F. BMP signaling in congenital heart disease: new developments and future directions. Birth Defects Res A Clin Mol Teratol 2011, 91, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Ricci, M.; Mohapatra, B.; Urbiztondo, A.; Birusingh, R.J.; Morgado, M.; Rodriguez, M.M.; Lincoln, J.; Vatta, M. Differential changes in TGF-beta/BMP signaling pathway in the right ventricular myocardium of newborns with hypoplastic left heart syndrome. J Card Fail 2010, 16, 628–634. [Google Scholar] [CrossRef] [PubMed]
- Stefanovic, S.; Zaffran, S. Mechanisms of retinoic acid signaling during cardiogenesis. Mechanisms of development 2017, 143, 9–19. [Google Scholar] [CrossRef]
- Vermot, J.; Niederreither, K.; Garnier, J.M.; Chambon, P.; Dolle, P. Decreased embryonic retinoic acid synthesis results in a DiGeorge syndrome phenotype in newborn mice. Proceedings of the National Academy of Sciences of the United States of America 2003, 100, 1763–1768. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Choudhary, B.; Merki, E.; Chien, K.R.; Maxson, R.E.; Sucov, H.M. Normal fate and altered function of the cardiac neural crest cell lineage in retinoic acid receptor mutant embryos. Mechanisms of development 2002, 117, 115–122. [Google Scholar] [CrossRef]
- Horitani, K.; Shiojima, I. Wnt signaling in cardiac development and heart diseases. In Vitro Cell Dev Biol Anim 2024, 60, 482–488. [Google Scholar] [CrossRef]
- Lorenzon, A.; Calore, M.; Poloni, G.; De Windt, L.J.; Braghetta, P.; Rampazzo, A. Wnt/beta-catenin pathway in arrhythmogenic cardiomyopathy. Oncotarget 2017, 8, 60640–60655. [Google Scholar] [CrossRef]
- Briggs, L.E.; Burns, T.A.; Lockhart, M.M.; Phelps, A.L.; Van den Hoff, M.J.; Wessels, A. Wnt/beta-catenin and sonic hedgehog pathways interact in the regulation of the development of the dorsal mesenchymal protrusion. Developmental dynamics : an official publication of the American Association of Anatomists 2016, 245, 103–113. [Google Scholar] [CrossRef]
- Washington Smoak, I.; Byrd, N.A.; Abu-Issa, R.; Goddeeris, M.M.; Anderson, R.; Morris, J.; Yamamura, K.; Klingensmith, J.; Meyers, E.N. Sonic hedgehog is required for cardiac outflow tract and neural crest cell development. Dev Biol 2005, 283, 357–372. [Google Scholar] [CrossRef]
- Nanni, L.; Ming, J.E.; Bocian, M.; Steinhaus, K.; Bianchi, D.W.; Die-Smulders, C.; Giannotti, A.; Imaizumi, K.; Jones, K.L.; Campo, M.D. , et al. The mutational spectrum of the sonic hedgehog gene in holoprosencephaly: SHH mutations cause a significant proportion of autosomal dominant holoprosencephaly. Human molecular genetics 1999, 8, 2479–2488. [Google Scholar] [CrossRef]
- Wang, J.; Liu, S.; Heallen, T.; Martin, J.F. The Hippo pathway in the heart: pivotal roles in development, disease, and regeneration. Nat Rev Cardiol 2018, 15, 672–684. [Google Scholar] [CrossRef]
- Zhou, Q.; Li, L.; Zhao, B.; Guan, K.L. The hippo pathway in heart development, regeneration, and diseases. Circulation research 2015, 116, 1431–1447. [Google Scholar] [CrossRef] [PubMed]
- Yagi, H.; Xu, X.; Gabriel, G.C.; Lo, C. Molecular Pathways and Animal Models of Hypoplastic Left Heart Syndrome. Advances in experimental medicine and biology 2024, 1441, 947–961. [Google Scholar] [CrossRef]
- Khosravi, F.; Ahmadvand, N.; Bellusci, S.; Sauer, H. The Multifunctional Contribution of FGF Signaling to Cardiac Development, Homeostasis, Disease and Repair. Front Cell Dev Biol 2021, 9, 672935. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Chang, J.Y.; Huang, Y.; Lin, X.; Luo, Y.; Schwartz, R.J.; Martin, J.F.; Wang, F. The FGF-BMP signaling axis regulates outflow tract valve primordium formation by promoting cushion neural crest cell differentiation. Circulation research 2010, 107, 1209–1219. [Google Scholar] [CrossRef]
- Reuter, M.S.; Sokolowski, D.J.; Javier Diaz-Mejia, J.; Keunen, J.; de Vrijer, B.; Chan, C.; Wang, L.; Ryan, G.; Chiasson, D.A.; Ketela, T. , et al. Decreased left heart flow in fetal lambs causes left heart hypoplasia and pro-fibrotic tissue remodeling. Commun Biol 2023, 6, 770. [Google Scholar] [CrossRef]
- Han, Z.; Yi, P.; Li, X.; Olson, E.N. Hand, an evolutionarily conserved bHLH transcription factor required for Drosophila cardiogenesis and hematopoiesis. Development 2006, 133, 1175–1182. [Google Scholar] [CrossRef] [PubMed]
- Riley, P.; Anson-Cartwright, L.; Cross, J.C. The Hand1 bHLH transcription factor is essential for placentation and cardiac morphogenesis. Nature genetics 1998, 18, 271–275. [Google Scholar] [CrossRef]
- Reamon-Buettner, S.M.; Ciribilli, Y.; Inga, A.; Borlak, J. A loss-of-function mutation in the binding domain of HAND1 predicts hypoplasia of the human hearts. Human molecular genetics 2008, 17, 1397–1405. [Google Scholar] [CrossRef]
- Kobayashi, J.; Yoshida, M.; Tarui, S.; Hirata, M.; Nagai, Y.; Kasahara, S.; Naruse, K.; Ito, H.; Sano, S.; Oh, H. Directed differentiation of patient-specific induced pluripotent stem cells identifies the transcriptional repression and epigenetic modification of NKX2-5, HAND1, and NOTCH1 in hypoplastic left heart syndrome. PloS one 2014, 9, e102796. [Google Scholar] [CrossRef]
- Akazawa, H.; Komuro, I. Cardiac transcription factor Csx/Nkx2-5: Its role in cardiac development and diseases. Pharmacology & therapeutics 2005, 107, 252–268. [Google Scholar] [CrossRef]
- Elliott, D.A.; Kirk, E.P.; Yeoh, T.; Chandar, S.; McKenzie, F.; Taylor, P.; Grossfeld, P.; Fatkin, D.; Jones, O.; Hayes, P. , et al. Cardiac homeobox gene NKX2-5 mutations and congenital heart disease: associations with atrial septal defect and hypoplastic left heart syndrome. Journal of the American College of Cardiology 2003, 41, 2072–2076. [Google Scholar] [CrossRef] [PubMed]
- Doering, L.; Cornean, A.; Thumberger, T.; Benjaminsen, J.; Wittbrodt, B.; Kellner, T.; Hammouda, O.T.; Gorenflo, M.; Wittbrodt, J.; Gierten, J. CRISPR-based knockout and base editing confirm the role of MYRF in heart development and congenital heart disease. Dis Model Mech 2023, 16. [Google Scholar] [CrossRef]
- Qi, H.; Yu, L.; Zhou, X.; Wynn, J.; Zhao, H.; Guo, Y.; Zhu, N.; Kitaygorodsky, A.; Hernan, R.; Aspelund, G. , et al. De novo variants in congenital diaphragmatic hernia identify MYRF as a new syndrome and reveal genetic overlaps with other developmental disorders. PLoS genetics 2018, 14, e1007822. [Google Scholar] [CrossRef] [PubMed]
- Watt, A.J.; Battle, M.A.; Li, J.; Duncan, S.A. GATA4 is essential for formation of the proepicardium and regulates cardiogenesis. Proceedings of the National Academy of Sciences of the United States of America 2004, 101, 12573–12578. [Google Scholar] [CrossRef]
- Misra, C.; Sachan, N.; McNally, C.R.; Koenig, S.N.; Nichols, H.A.; Guggilam, A.; Lucchesi, P.A.; Pu, W.T.; Srivastava, D.; Garg, V. Congenital heart disease-causing Gata4 mutation displays functional deficits in vivo. PLoS genetics 2012, 8, e1002690. [Google Scholar] [CrossRef]
- Ang, Y.S.; Rivas, R.N.; Ribeiro, A.J.S.; Srivas, R.; Rivera, J.; Stone, N.R.; Pratt, K.; Mohamed, T.M.A.; Fu, J.D.; Spencer, C.I. , et al. Disease Model of GATA4 Mutation Reveals Transcription Factor Cooperativity in Human Cardiogenesis. Cell 2016, 167, 1734–1749. [Google Scholar] [CrossRef]
- Li, Y.; Du, J.; Deng, S.; Liu, B.; Jing, X.; Yan, Y.; Liu, Y.; Wang, J.; Zhou, X.; She, Q. The molecular mechanisms of cardiac development and related diseases. Signal Transduct Target Ther 2024, 9, 368. [Google Scholar] [CrossRef]
- Patel, C.; Silcock, L.; McMullan, D.; Brueton, L.; Cox, H. TBX5 intragenic duplication: a family with an atypical Holt-Oram syndrome phenotype. Eur J Hum Genet 2012, 20, 863–869. [Google Scholar] [CrossRef] [PubMed]
- Bruneau, B.G.; Nemer, G.; Schmitt, J.P.; Charron, F.; Robitaille, L.; Caron, S.; Conner, D.A.; Gessler, M.; Nemer, M.; Seidman, C.E. , et al. A murine model of Holt-Oram syndrome defines roles of the T-box transcription factor Tbx5 in cardiogenesis and disease. Cell 2001, 106, 709–721. [Google Scholar] [CrossRef]
- Yang, C.; Xu, Y.; Yu, M.; Lee, D.; Alharti, S.; Hellen, N.; Ahmad Shaik, N.; Banaganapalli, B.; Sheikh Ali Mohamoud, H.; Elango, R. , et al. Induced pluripotent stem cell modelling of HLHS underlines the contribution of dysfunctional NOTCH signalling to impaired cardiogenesis. Human molecular genetics 2017, 26, 3031–3045. [Google Scholar] [CrossRef]
- von Gise, A.; Zhou, B.; Honor, L.B.; Ma, Q.; Petryk, A.; Pu, W.T. WT1 regulates epicardial epithelial to mesenchymal transition through beta-catenin and retinoic acid signaling pathways. Dev Biol 2011, 356, 421–431. [Google Scholar] [CrossRef]
- Crucean, A.; Alqahtani, A.; Barron, D.J.; Brawn, W.J.; Richardson, R.V.; O'Sullivan, J.; Anderson, R.H.; Henderson, D.J.; Chaudhry, B. Re-evaluation of hypoplastic left heart syndrome from a developmental and morphological perspective. Orphanet J Rare Dis 2017, 12, 138. [Google Scholar] [CrossRef]
- Qiao, X.H.; Wang, F.; Zhang, X.L.; Huang, R.T.; Xue, S.; Wang, J.; Qiu, X.B.; Liu, X.Y.; Yang, Y.Q. MEF2C loss-of-function mutation contributes to congenital heart defects. Int J Med Sci 2017, 14, 1143–1153. [Google Scholar] [CrossRef] [PubMed]
- Barnes, R.M.; Harris, I.S.; Jaehnig, E.J.; Sauls, K.; Sinha, T.; Rojas, A.; Schachterle, W.; McCulley, D.J.; Norris, R.A.; Black, B.L. MEF2C regulates outflow tract alignment and transcriptional control of Tdgf1. Development 2016, 143, 774–779. [Google Scholar] [CrossRef]
- Gao, R.; Liang, X.; Cheedipudi, S.; Cordero, J.; Jiang, X.; Zhang, Q.; Caputo, L.; Gunther, S.; Kuenne, C.; Ren, Y. , et al. Pioneering function of Isl1 in the epigenetic control of cardiomyocyte cell fate. Cell research 2019, 29, 486–501. [Google Scholar] [CrossRef]
- Stevens, K.N.; Hakonarson, H.; Kim, C.E.; Doevendans, P.A.; Koeleman, B.P.; Mital, S.; Raue, J.; Glessner, J.T.; Coles, J.G.; Moreno, V. , et al. Common variation in ISL1 confers genetic susceptibility for human congenital heart disease. PloS one 2010, 5, e10855. [Google Scholar] [CrossRef]
- Tomita-Mitchell, A.; Stamm, K.D.; Mahnke, D.K.; Kim, M.S.; Hidestrand, P.M.; Liang, H.L.; Goetsch, M.A.; Hidestrand, M.; Simpson, P.; Pelech, A.N. , et al. Impact of MYH6 variants in hypoplastic left heart syndrome. Physiological genomics 2016, 48, 912–921. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.S.; Fleres, B.; Lovett, J.; Anfinson, M.; Samudrala, S.S.K.; Kelly, L.J.; Teigen, L.E.; Cavanaugh, M.; Marquez, M.; Geurts, A.M. , et al. Contractility of Induced Pluripotent Stem Cell-Cardiomyocytes With an MYH6 Head Domain Variant Associated With Hypoplastic Left Heart Syndrome. Front Cell Dev Biol 2020, 8, 440. [Google Scholar] [CrossRef]
- Christ, A.; Christa, A.; Klippert, J.; Eule, J.C.; Bachmann, S.; Wallace, V.A.; Hammes, A.; Willnow, T.E. LRP2 Acts as SHH Clearance Receptor to Protect the Retinal Margin from Mitogenic Stimuli. Developmental cell 2015, 35, 36–48. [Google Scholar] [CrossRef] [PubMed]
- Kantarci, S.; Al-Gazali, L.; Hill, R.S.; Donnai, D.; Black, G.C.; Bieth, E.; Chassaing, N.; Lacombe, D.; Devriendt, K.; Teebi, A. , et al. Mutations in LRP2, which encodes the multiligand receptor megalin, cause Donnai-Barrow and facio-oculo-acoustico-renal syndromes. Nature genetics 2007, 39, 957–959. [Google Scholar] [CrossRef]
- Theis, J.L.; Vogler, G.; Missinato, M.A.; Li, X.; Nielsen, T.; Zeng, X.I.; Martinez-Fernandez, A.; Walls, S.M.; Kervadec, A.; Kezos, J.N. , et al. Patient-specific genomics and cross-species functional analysis implicate LRP2 in hypoplastic left heart syndrome. eLife 2020, 9. [Google Scholar] [CrossRef]
- Britz-Cunningham, S.H.; Shah, M.M.; Zuppan, C.W.; Fletcher, W.H. Mutations of the Connexin43 gap-junction gene in patients with heart malformations and defects of laterality. The New England journal of medicine 1995, 332, 1323–1329. [Google Scholar] [CrossRef]
- Dasgupta, C.; Martinez, A.M.; Zuppan, C.W.; Shah, M.M.; Bailey, L.L.; Fletcher, W.H. Identification of connexin43 (alpha1) gap junction gene mutations in patients with hypoplastic left heart syndrome by denaturing gradient gel electrophoresis (DGGE). Mutation research 2001, 479, 173–186. [Google Scholar] [CrossRef]
- Asp, M.; Giacomello, S.; Larsson, L.; Wu, C.; Furth, D.; Qian, X.; Wardell, E.; Custodio, J.; Reimegard, J.; Salmen, F. , et al. A Spatiotemporal Organ-Wide Gene Expression and Cell Atlas of the Developing Human Heart. Cell 2019, 179, 1647–1660. [Google Scholar] [CrossRef]
- Gessert, S.; Kuhl, M. The multiple phases and faces of wnt signaling during cardiac differentiation and development. Circulation research 2010, 107, 186–199. [Google Scholar] [CrossRef] [PubMed]
- Clevers, H. Wnt/beta-catenin signaling in development and disease. Cell 2006, 127, 469–480. [Google Scholar] [CrossRef] [PubMed]
- Tzahor, E. Wnt/beta-catenin signaling and cardiogenesis: timing does matter. Developmental cell 2007, 13, 10–13. [Google Scholar] [CrossRef] [PubMed]
- Ryckebusch, L.; Wang, Z.; Bertrand, N.; Lin, S.C.; Chi, X.; Schwartz, R.; Zaffran, S.; Niederreither, K. Retinoic acid deficiency alters second heart field formation. Proceedings of the National Academy of Sciences of the United States of America 2008, 105, 2913–2918. [Google Scholar] [CrossRef]
- Sirbu, I.O.; Zhao, X.; Duester, G. Retinoic acid controls heart anteroposterior patterning by down-regulating Isl1 through the Fgf8 pathway. Developmental dynamics : an official publication of the American Association of Anatomists 2008, 237, 1627–1635. [Google Scholar] [CrossRef]
- Ghyselinck, N.B.; Duester, G. Retinoic acid signaling pathways. Development 2019, 146. [Google Scholar] [CrossRef]
- Griffin, A.H.C.; Small, A.M.; Johnson, R.D.; Medina, A.M.; Kollar, K.T.; Nazir, R.A.; McGuire, A.M.; Schumacher, J.A. Retinoic acid promotes second heart field addition and regulates ventral aorta patterning in zebrafish. Dev Biol 2025, 522, 143–155. [Google Scholar] [CrossRef]
- Rones, M.S.; McLaughlin, K.A.; Raffin, M.; Mercola, M. Serrate and Notch specify cell fates in the heart field by suppressing cardiomyogenesis. Development 2000, 127, 3865–3876. [Google Scholar] [CrossRef] [PubMed]
- Grego-Bessa, J.; Luna-Zurita, L.; del Monte, G.; Bolos, V.; Melgar, P.; Arandilla, A.; Garratt, A.N.; Zang, H.; Mukouyama, Y.S.; Chen, H. , et al. Notch signaling is essential for ventricular chamber development. Developmental cell 2007, 12, 415–429. [Google Scholar] [CrossRef]
- Luxan, G.; D'Amato, G.; MacGrogan, D.; de la Pompa, J.L. Endocardial Notch Signaling in Cardiac Development and Disease. Circulation research 2016, 118, e1–e18. [Google Scholar] [CrossRef] [PubMed]
- MacGrogan, D.; Nus, M.; de la Pompa, J.L. Notch signaling in cardiac development and disease. Curr Top Dev Biol 2010, 92, 333–365. [Google Scholar] [CrossRef] [PubMed]
- McCulley, D.J.; Kang, J.O.; Martin, J.F.; Black, B.L. BMP4 is required in the anterior heart field and its derivatives for endocardial cushion remodeling, outflow tract septation, and semilunar valve development. Developmental dynamics : an official publication of the American Association of Anatomists 2008, 237, 3200–3209. [Google Scholar] [CrossRef]
- Chen, H.; Shi, S.; Acosta, L.; Li, W.; Lu, J.; Bao, S.; Chen, Z.; Yang, Z.; Schneider, M.D.; Chien, K.R. , et al. BMP10 is essential for maintaining cardiac growth during murine cardiogenesis. Development 2004, 131, 2219–2231. [Google Scholar] [CrossRef]
- Liu, W.; Selever, J.; Wang, D.; Lu, M.F.; Moses, K.A.; Schwartz, R.J.; Martin, J.F. Bmp4 signaling is required for outflow-tract septation and branchial-arch artery remodeling. Proceedings of the National Academy of Sciences of the United States of America 2004, 101, 4489–4494. [Google Scholar] [CrossRef]
- Luna-Zurita, L.; Stirnimann, C.U.; Glatt, S.; Kaynak, B.L.; Thomas, S.; Baudin, F.; Samee, M.A.; He, D.; Small, E.M.; Mileikovsky, M. , et al. Complex Interdependence Regulates Heterotypic Transcription Factor Distribution and Coordinates Cardiogenesis. Cell 2016, 164, 999–1014. [Google Scholar] [CrossRef]
- Fahed, A.C.; Gelb, B.D.; Seidman, J.G.; Seidman, C.E. Genetics of congenital heart disease: the glass half empty. Circulation research 2013, 112, 707–720. [Google Scholar] [CrossRef]
- Bruneau, B.G. Transcriptional regulation of vertebrate cardiac morphogenesis. Circulation research 2002, 90, 509–519. [Google Scholar] [CrossRef]
- Bruneau, B.G. The developmental genetics of congenital heart disease. Nature 2008, 451, 943–948. [Google Scholar] [CrossRef]
- Olson, E.N. Gene regulatory networks in the evolution and development of the heart. Science 2006, 313, 1922–1927. [Google Scholar] [CrossRef]
- McFadden, D.G.; Barbosa, A.C.; Richardson, J.A.; Schneider, M.D.; Srivastava, D.; Olson, E.N. The Hand1 and Hand2 transcription factors regulate expansion of the embryonic cardiac ventricles in a gene dosage-dependent manner. Development 2005, 132, 189–201. [Google Scholar] [CrossRef]
- Oka, T.; Maillet, M.; Watt, A.J.; Schwartz, R.J.; Aronow, B.J.; Duncan, S.A.; Molkentin, J.D. Cardiac-specific deletion of Gata4 reveals its requirement for hypertrophy, compensation, and myocyte viability. Circulation research 2006, 98, 837–845. [Google Scholar] [CrossRef]
- Cai, C.L.; Liang, X.; Shi, Y.; Chu, P.H.; Pfaff, S.L.; Chen, J.; Evans, S. Isl1 identifies a cardiac progenitor population that proliferates prior to differentiation and contributes a majority of cells to the heart. Developmental cell 2003, 5, 877–889. [Google Scholar] [CrossRef]
- Stennard, F.A.; Harvey, R.P. T-box transcription factors and their roles in regulatory hierarchies in the developing heart. Development 2005, 132, 4897–4910. [Google Scholar] [CrossRef]
- Lin, Q.; Schwarz, J.; Bucana, C.; Olson, E.N. Control of mouse cardiac morphogenesis and myogenesis by transcription factor MEF2C. Science 1997, 276, 1404–1407. [Google Scholar] [CrossRef]
- Tanaka, M.; Chen, Z.; Bartunkova, S.; Yamasaki, N.; Izumo, S. The cardiac homeobox gene Csx/Nkx2.5 lies genetically upstream of multiple genes essential for heart development. Development 1999, 126, 1269–1280. [Google Scholar] [CrossRef]
- Durocher, D.; Charron, F.; Warren, R.; Schwartz, R.J.; Nemer, M. The cardiac transcription factors Nkx2-5 and GATA-4 are mutual cofactors. The EMBO journal 1997, 16, 5687–5696. [Google Scholar] [CrossRef]
- Lyons, I.; Parsons, L.M.; Hartley, L.; Li, R.; Andrews, J.E.; Robb, L.; Harvey, R.P. Myogenic and morphogenetic defects in the heart tubes of murine embryos lacking the homeo box gene Nkx2-5. Genes & development 1995, 9, 1654–1666. [Google Scholar] [CrossRef]
- Targoff, K.L.; Colombo, S.; George, V.; Schell, T.; Kim, S.H.; Solnica-Krezel, L.; Yelon, D. Nkx genes are essential for maintenance of ventricular identity. Development 2013, 140, 4203–4213. [Google Scholar] [CrossRef]
- Pashmforoush, M.; Lu, J.T.; Chen, H.; Amand, T.S.; Kondo, R.; Pradervand, S.; Evans, S.M.; Clark, B.; Feramisco, J.R.; Giles, W. , et al. Nkx2-5 pathways and congenital heart disease; loss of ventricular myocyte lineage specification leads to progressive cardiomyopathy and complete heart block. Cell 2004, 117, 373–386. [Google Scholar] [CrossRef] [PubMed]
- Benson, D.W.; Silberbach, G.M.; Kavanaugh-McHugh, A.; Cottrill, C.; Zhang, Y.; Riggs, S.; Smalls, O.; Johnson, M.C.; Watson, M.S.; Seidman, J.G. , et al. Mutations in the cardiac transcription factor NKX2.5 affect diverse cardiac developmental pathways. The Journal of clinical investigation 1999, 104, 1567–1573. [Google Scholar] [CrossRef] [PubMed]
- Dai, Y.S.; Cserjesi, P.; Markham, B.E.; Molkentin, J.D. The transcription factors GATA4 and dHAND physically interact to synergistically activate cardiac gene expression through a p300-dependent mechanism. The Journal of biological chemistry 2002, 277, 24390–24398. [Google Scholar] [CrossRef]
- Risebro, C.A.; Smart, N.; Dupays, L.; Breckenridge, R.; Mohun, T.J.; Riley, P.R. Hand1 regulates cardiomyocyte proliferation versus differentiation in the developing heart. Development 2006, 133, 4595–4606. [Google Scholar] [CrossRef]
- Firulli, B.A.; George, R.M.; Harkin, J.; Toolan, K.P.; Gao, H.; Liu, Y.; Zhang, W.; Field, L.J.; Liu, Y.; Shou, W. , et al. HAND1 loss-of-function within the embryonic myocardium reveals survivable congenital cardiac defects and adult heart failure. Cardiovascular research 2020, 116, 605–618. [Google Scholar] [CrossRef] [PubMed]
- Vincentz, J.W.; Toolan, K.P.; Zhang, W.; Firulli, A.B. Hand factor ablation causes defective left ventricular chamber development and compromised adult cardiac function. PLoS genetics 2017, 13, e1006922. [Google Scholar] [CrossRef]
- Firulli, B.A.; Toolan, K.P.; Harkin, J.; Millar, H.; Pineda, S.; Firulli, A.B. The HAND1 frameshift A126FS mutation does not cause hypoplastic left heart syndrome in mice. Cardiovascular research 2017, 113, 1732–1742. [Google Scholar] [CrossRef]
- Pierpont, M.E.; Basson, C.T.; Benson, D.W., Jr.; Gelb, B.D.; Giglia, T.M.; Goldmuntz, E.; McGee, G.; Sable, C.A.; Srivastava, D.; Webb, C.L. , et al. Genetic basis for congenital heart defects: current knowledge: a scientific statement from the American Heart Association Congenital Cardiac Defects Committee, Council on Cardiovascular Disease in the Young: endorsed by the American Academy of Pediatrics. Circulation 2007, 115, 3015–3038. [Google Scholar] [CrossRef]
- Birla, A.K.; Brimmer, S.; Short, W.D.; Olutoye, O.O., 2nd; Shar, J.A.; Lalwani, S.; Sucosky, P.; Parthiban, A.; Keswani, S.G.; Caldarone, C.A. , et al. Current state of the art in hypoplastic left heart syndrome. Front Cardiovasc Med 2022, 9, 878266. [Google Scholar] [CrossRef]
- Ishigami, S.; Ohtsuki, S.; Tarui, S.; Ousaka, D.; Eitoku, T.; Kondo, M.; Okuyama, M.; Kobayashi, J.; Baba, K.; Arai, S. , et al. Intracoronary autologous cardiac progenitor cell transfer in patients with hypoplastic left heart syndrome: the TICAP prospective phase 1 controlled trial. Circulation research 2015, 116, 653–664. [Google Scholar] [CrossRef]
- Ishigami, S.; Ohtsuki, S.; Eitoku, T.; Ousaka, D.; Kondo, M.; Kurita, Y.; Hirai, K.; Fukushima, Y.; Baba, K.; Goto, T. , et al. Intracoronary Cardiac Progenitor Cells in Single Ventricle Physiology: The PERSEUS (Cardiac Progenitor Cell Infusion to Treat Univentricular Heart Disease) Randomized Phase 2 Trial. Circulation research 2017, 120, 1162–1173. [Google Scholar] [CrossRef]
- Burkhart, H.M.; Qureshi, M.Y.; Rossano, J.W.; Cantero Peral, S.; O'Leary, P.W.; Hathcock, M.; Kremers, W.; Nelson, T.J.; Wanek, H.C.C.P. Autologous stem cell therapy for hypoplastic left heart syndrome: Safety and feasibility of intraoperative intramyocardial injections. J Thorac Cardiovasc Surg 2019, 158, 1614–1623. [Google Scholar] [CrossRef] [PubMed]
- Brizard, C.P.; Elwood, N.J.; Kowalski, R.; Horton, S.B.; Jones, B.O.; Hutchinson, D.; Zannino, D.; Sheridan, B.J.; Butt, W.; Cheung, M.M.H. , et al. Safety and feasibility of adjunct autologous cord blood stem cell therapy during the Norwood heart operation. J Thorac Cardiovasc Surg 2023, 166, 1746–1755. [Google Scholar] [CrossRef] [PubMed]
- Gallego-Navarro, C.; Jaggers, J.; Burkhart, H.M.; Carlo, W.F.; Morales, D.L.; Qureshi, M.Y.; Rossano, J.W.; Hagen, C.E.; Seisler, D.K.; Peral, S.C. , et al. Autologous umbilical cord blood mononuclear cell therapy for hypoplastic left heart syndrome: a nonrandomized control trial of the efficacy and safety of intramyocardial injections. Stem Cell Res Ther 2025, 16, 215. [Google Scholar] [CrossRef]
- Ren, H.; Sang, Y.; Zhang, F.; Liu, Z.; Qi, N.; Chen, Y. Comparative Analysis of Human Mesenchymal Stem Cells from Umbilical Cord, Dental Pulp, and Menstrual Blood as Sources for Cell Therapy. Stem Cells Int 2016, 2016, 3516574. [Google Scholar] [CrossRef]
- Baksh, D.; Yao, R.; Tuan, R.S. Comparison of proliferative and multilineage differentiation potential of human mesenchymal stem cells derived from umbilical cord and bone marrow. Stem cells 2007, 25, 1384–1392. [Google Scholar] [CrossRef]
- Davies, B.; Elwood, N.J.; Li, S.; Cullinane, F.; Edwards, G.A.; Newgreen, D.F.; Brizard, C.P. Human cord blood stem cells enhance neonatal right ventricular function in an ovine model of right ventricular training. The Annals of thoracic surgery 2010, 89, 585-593, 593 e581-584. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.A.; Rajamarthandan, S.; Francis, B.; O'Leary-Kelly, M.K.; Sinha, P. Update on stem cell technologies in congenital heart disease. J Card Surg 2020, 35, 174–179. [Google Scholar] [CrossRef]
- Le Blanc, K.; Mougiakakos, D. Multipotent mesenchymal stromal cells and the innate immune system. Nature reviews. Immunology 2012, 12, 383–396. [Google Scholar] [CrossRef]
- Lalu, M.M.; McIntyre, L.; Pugliese, C.; Fergusson, D.; Winston, B.W.; Marshall, J.C.; Granton, J.; Stewart, D.J.; Canadian Critical Care Trials, G. Safety of cell therapy with mesenchymal stromal cells (SafeCell): a systematic review and meta-analysis of clinical trials. PloS one 2012, 7, e47559. [Google Scholar] [CrossRef]
- Ascheim, D.D.; Gelijns, A.C.; Goldstein, D.; Moye, L.A.; Smedira, N.; Lee, S.; Klodell, C.T.; Szady, A.; Parides, M.K.; Jeffries, N.O. , et al. Mesenchymal precursor cells as adjunctive therapy in recipients of contemporary left ventricular assist devices. Circulation 2014, 129, 2287–2296. [Google Scholar] [CrossRef]
- Oswald, J.; Boxberger, S.; Jorgensen, B.; Feldmann, S.; Ehninger, G.; Bornhauser, M.; Werner, C. Mesenchymal stem cells can be differentiated into endothelial cells in vitro. Stem cells 2004, 22, 377–384. [Google Scholar] [CrossRef]
- Toma, C.; Pittenger, M.F.; Cahill, K.S.; Byrne, B.J.; Kessler, P.D. Human mesenchymal stem cells differentiate to a cardiomyocyte phenotype in the adult murine heart. Circulation 2002, 105, 93–98. [Google Scholar] [CrossRef]
- Maacha, S.; Sidahmed, H.; Jacob, S.; Gentilcore, G.; Calzone, R.; Grivel, J.C.; Cugno, C. Paracrine Mechanisms of Mesenchymal Stromal Cells in Angiogenesis. Stem Cells Int 2020, 2020, 4356359. [Google Scholar] [CrossRef] [PubMed]
- Teng, X.; Chen, L.; Chen, W.; Yang, J.; Yang, Z.; Shen, Z. Mesenchymal Stem Cell-Derived Exosomes Improve the Microenvironment of Infarcted Myocardium Contributing to Angiogenesis and Anti-Inflammation. Cell Physiol Biochem 2015, 37, 2415–2424. [Google Scholar] [CrossRef] [PubMed]
- Pu, X.; Ma, S.; Gao, Y.; Xu, T.; Chang, P.; Dong, L. Mesenchymal Stem Cell-Derived Exosomes: Biological Function and Their Therapeutic Potential in Radiation Damage. Cells 2020, 10. [Google Scholar] [CrossRef]
- Wehman, B.; Sharma, S.; Pietris, N.; Mishra, R.; Siddiqui, O.T.; Bigham, G.; Li, T.; Aiello, E.; Murthi, S.; Pittenger, M. , et al. Mesenchymal stem cells preserve neonatal right ventricular function in a porcine model of pressure overload. American journal of physiology. Heart and circulatory physiology 2016, 310, H1816–1826. [Google Scholar] [CrossRef] [PubMed]
- Liufu, R.; Shi, G.; He, X.; Lv, J.; Liu, W.; Zhu, F.; Wen, C.; Zhu, Z.; Chen, H. The therapeutic impact of human neonatal BMSC in a right ventricular pressure overload model in mice. Stem Cell Res Ther 2020, 11, 96. [Google Scholar] [CrossRef]
- Wittenberg, R.E.; Gauvreau, K.; Leighton, J.; Moleon-Shea, M.; Borow, K.M.; Marx, G.R.; Emani, S.M. Prospective randomized controlled trial of the safety and feasibility of a novel mesenchymal precursor cell therapy in hypoplastic left heart syndrome. JTCVS Open 2023, 16, 656–672. [Google Scholar] [CrossRef]
- Thomas, E.D.; Lochte, H.L., Jr.; Lu, W.C.; Ferrebee, J.W. Intravenous infusion of bone marrow in patients receiving radiation and chemotherapy. The New England journal of medicine 1957, 257, 491–496. [Google Scholar] [CrossRef]
- Gratwohl, A.; Hermans, J.; Goldman, J.M.; Arcese, W.; Carreras, E.; Devergie, A.; Frassoni, F.; Gahrton, G.; Kolb, H.J.; Niederwieser, D. , et al. Risk assessment for patients with chronic myeloid leukaemia before allogeneic blood or marrow transplantation. Chronic Leukemia Working Party of the European Group for Blood and Marrow Transplantation. Lancet 1998, 352, 1087–1092. [Google Scholar] [CrossRef]
- Burnett, A.K.; Goldstone, A.H.; Stevens, R.M.; Hann, I.M.; Rees, J.K.; Gray, R.G.; Wheatley, K. Randomised comparison of addition of autologous bone-marrow transplantation to intensive chemotherapy for acute myeloid leukaemia in first remission: results of MRC AML 10 trial. UK Medical Research Council Adult and Children's Leukaemia Working Parties. Lancet 1998, 351, 700–708. [Google Scholar] [CrossRef]
- Qureshi, M.Y.; Cabalka, A.K.; Khan, S.P.; Hagler, D.J.; Haile, D.T.; Cannon, B.C.; Olson, T.M.; Cantero-Peral, S.; Dietz, A.B.; Radel, D.J. , et al. Cell-Based Therapy for Myocardial Dysfunction After Fontan Operation in Hypoplastic Left Heart Syndrome. Mayo Clin Proc Innov Qual Outcomes 2017, 1, 185–191. [Google Scholar] [CrossRef] [PubMed]
- van Berlo, J.H.; Kanisicak, O.; Maillet, M.; Vagnozzi, R.J.; Karch, J.; Lin, S.C.; Middleton, R.C.; Marban, E.; Molkentin, J.D. c-kit+ cells minimally contribute cardiomyocytes to the heart. Nature 2014, 509, 337–341. [Google Scholar] [CrossRef] [PubMed]
- Sultana, N.; Zhang, L.; Yan, J.; Chen, J.; Cai, W.; Razzaque, S.; Jeong, D.; Sheng, W.; Bu, L.; Xu, M. , et al. Resident c-kit(+) cells in the heart are not cardiac stem cells. Nature communications 2015, 6, 8701. [Google Scholar] [CrossRef]
- Messina, E.; De Angelis, L.; Frati, G.; Morrone, S.; Chimenti, S.; Fiordaliso, F.; Salio, M.; Battaglia, M.; Latronico, M.V.; Coletta, M. , et al. Isolation and expansion of adult cardiac stem cells from human and murine heart. Circulation research 2004, 95, 911–921. [Google Scholar] [CrossRef] [PubMed]
- Hasan, A.S.; Luo, L.; Yan, C.; Zhang, T.X.; Urata, Y.; Goto, S.; Mangoura, S.A.; Abdel-Raheem, M.H.; Zhang, S.; Li, T.S. Cardiosphere-Derived Cells Facilitate Heart Repair by Modulating M1/M2 Macrophage Polarization and Neutrophil Recruitment. PloS one 2016, 11, e0165255. [Google Scholar] [CrossRef]
- Carr, C.A.; Stuckey, D.J.; Tan, J.J.; Tan, S.C.; Gomes, R.S.; Camelliti, P.; Messina, E.; Giacomello, A.; Ellison, G.M.; Clarke, K. Cardiosphere-derived cells improve function in the infarcted rat heart for at least 16 weeks--an MRI study. PloS one 2011, 6, e25669. [Google Scholar] [CrossRef]
- Lee, S.T.; White, A.J.; Matsushita, S.; Malliaras, K.; Steenbergen, C.; Zhang, Y.; Li, T.S.; Terrovitis, J.; Yee, K.; Simsir, S. , et al. Intramyocardial injection of autologous cardiospheres or cardiosphere-derived cells preserves function and minimizes adverse ventricular remodeling in pigs with heart failure post-myocardial infarction. Journal of the American College of Cardiology 2011, 57, 455–465. [Google Scholar] [CrossRef]
- Gallet, R.; Dawkins, J.; Valle, J.; Simsolo, E.; de Couto, G.; Middleton, R.; Tseliou, E.; Luthringer, D.; Kreke, M.; Smith, R.R. , et al. Exosomes secreted by cardiosphere-derived cells reduce scarring, attenuate adverse remodelling, and improve function in acute and chronic porcine myocardial infarction. European heart journal 2017, 38, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Bittle, G.J.; Morales, D.; Pietris, N.; Parchment, N.; Parsell, D.; Peck, K.; Deatrick, K.B.; Rodriguez-Borlado, L.; Smith, R.R.; Marban, L. , et al. Exosomes isolated from human cardiosphere-derived cells attenuate pressure overload-induced right ventricular dysfunction. J Thorac Cardiovasc Surg 2021, 162, 975–986 e976. [Google Scholar] [CrossRef]
- Sano, T.; Ousaka, D.; Goto, T.; Ishigami, S.; Hirai, K.; Kasahara, S.; Ohtsuki, S.; Sano, S.; Oh, H. Impact of Cardiac Progenitor Cells on Heart Failure and Survival in Single Ventricle Congenital Heart Disease. Circulation research 2018, 122, 994–1005. [Google Scholar] [CrossRef]
- Tarui, S.; Ishigami, S.; Ousaka, D.; Kasahara, S.; Ohtsuki, S.; Sano, S.; Oh, H. Transcoronary infusion of cardiac progenitor cells in hypoplastic left heart syndrome: Three-year follow-up of the Transcoronary Infusion of Cardiac Progenitor Cells in Patients With Single-Ventricle Physiology (TICAP) trial. J Thorac Cardiovasc Surg 2015, 150, 1198–1207. [Google Scholar] [CrossRef]
- Hirai, K.; Sawada, R.; Hayashi, T.; Araki, T.; Nakagawa, N.; Kondo, M.; Yasuda, K.; Hirata, T.; Sato, T.; Nakatsuka, Y. , et al. Eight-Year Outcomes of Cardiosphere-Derived Cells in Single Ventricle Congenital Heart Disease. Journal of the American Heart Association 2024, 13, e038137. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, K.; Yamanaka, S. Induction of pluripotent stem cells from mouse embryonic and adult fibroblast cultures by defined factors. Cell 2006, 126, 663–676. [Google Scholar] [CrossRef]
- Ye, L.; Yu, Y.; Zhao, Z.A.; Zhao, D.; Ni, X.; Wang, Y.; Fang, X.; Yu, M.; Wang, Y.; Tang, J.M. , et al. Patient-specific iPSC-derived cardiomyocytes reveal abnormal regulation of FGF16 in a familial atrial septal defect. Cardiovascular research 2022, 118, 859–871. [Google Scholar] [CrossRef]
- Thareja, S.K.; Anfinson, M.; Cavanaugh, M.; Kim, M.S.; Lamberton, P.; Radandt, J.; Brown, R.; Liang, H.L.; Stamm, K.; Afzal, M.Z. , et al. Altered contractility, Ca(2+) transients, and cell morphology seen in a patient-specific iPSC-CM model of Ebstein's anomaly with left ventricular noncompaction. American journal of physiology. Heart and circulatory physiology 2023, 325, H149–H162. [Google Scholar] [CrossRef]
- Takahashi, K.; Tanabe, K.; Ohnuki, M.; Narita, M.; Ichisaka, T.; Tomoda, K.; Yamanaka, S. Induction of pluripotent stem cells from adult human fibroblasts by defined factors. Cell 2007, 131, 861–872. [Google Scholar] [CrossRef]
- Buganim, Y.; Faddah, D.A.; Cheng, A.W.; Itskovich, E.; Markoulaki, S.; Ganz, K.; Klemm, S.L.; van Oudenaarden, A.; Jaenisch, R. Single-cell expression analyses during cellular reprogramming reveal an early stochastic and a late hierarchic phase. Cell 2012, 150, 1209–1222. [Google Scholar] [CrossRef] [PubMed]
- Devalla, H.D.; Schwach, V.; Ford, J.W.; Milnes, J.T.; El-Haou, S.; Jackson, C.; Gkatzis, K.; Elliott, D.A.; Chuva de Sousa Lopes, S.M.; Mummery, C.L. , et al. Atrial-like cardiomyocytes from human pluripotent stem cells are a robust preclinical model for assessing atrial-selective pharmacology. EMBO Mol Med 2015, 7, 394–410. [Google Scholar] [CrossRef]
- Protze, S.I.; Liu, J.; Nussinovitch, U.; Ohana, L.; Backx, P.H.; Gepstein, L.; Keller, G.M. Sinoatrial node cardiomyocytes derived from human pluripotent cells function as a biological pacemaker. Nature biotechnology 2017, 35, 56–68. [Google Scholar] [CrossRef]
- Burridge, P.W.; Matsa, E.; Shukla, P.; Lin, Z.C.; Churko, J.M.; Ebert, A.D.; Lan, F.; Diecke, S.; Huber, B.; Mordwinkin, N.M. , et al. Chemically defined generation of human cardiomyocytes. Nat Methods 2014, 11, 855–860. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Pabon, L.; Murry, C.E. Engineering adolescence: maturation of human pluripotent stem cell-derived cardiomyocytes. Circulation research 2014, 114, 511–523. [Google Scholar] [CrossRef] [PubMed]
- Tohyama, S.; Hattori, F.; Sano, M.; Hishiki, T.; Nagahata, Y.; Matsuura, T.; Hashimoto, H.; Suzuki, T.; Yamashita, H.; Satoh, Y. , et al. Distinct metabolic flow enables large-scale purification of mouse and human pluripotent stem cell-derived cardiomyocytes. Cell stem cell 2013, 12, 127–137. [Google Scholar] [CrossRef]
- Hofbauer, P.; Jahnel, S.M.; Papai, N.; Giesshammer, M.; Deyett, A.; Schmidt, C.; Penc, M.; Tavernini, K.; Grdseloff, N.; Meledeth, C. , et al. Cardioids reveal self-organizing principles of human cardiogenesis. Cell 2021, 184, 3299–3317. [Google Scholar] [CrossRef]
- Jiang, Y.; Habibollah, S.; Tilgner, K.; Collin, J.; Barta, T.; Al-Aama, J.Y.; Tesarov, L.; Hussain, R.; Trafford, A.W.; Kirkwood, G. , et al. An induced pluripotent stem cell model of hypoplastic left heart syndrome (HLHS) reveals multiple expression and functional differences in HLHS-derived cardiac myocytes. Stem Cells Transl Med 2014, 3, 416–423. [Google Scholar] [CrossRef]
- Ye, S.; Wang, C.; Xu, Z.; Lin, H.; Wan, X.; Yu, Y.; Adhicary, S.; Zhang, J.Z.; Zhou, Y.; Liu, C. , et al. Impaired Human Cardiac Cell Development due to NOTCH1 Deficiency. Circulation research 2023, 132, 187–204. [Google Scholar] [CrossRef] [PubMed]
- Lewis J, L.T. , Schlegel B, Woods D, Rao K, Sentis A, Tan J, Jagannathan R, Javed Z, Boudreau AN, Nelson T, Moulik M, Hempel N, Chen BB, Shiva S, Rajasundaram D, Finkel T, Saraf A. Hypomorphic NOTCH1 Expression Alters Cardiomyocyte Cellular Architecture in Hypoplastic Left Heart Syndrome. bioRxiv, 2024; 10.1101/2024.09.30.615809. [Google Scholar] [CrossRef]
- Krane, M.; Dressen, M.; Santamaria, G.; My, I.; Schneider, C.M.; Dorn, T.; Laue, S.; Mastantuono, E.; Berutti, R.; Rawat, H. , et al. Sequential Defects in Cardiac Lineage Commitment and Maturation Cause Hypoplastic Left Heart Syndrome. Circulation 2021, 144, 1409–1428. [Google Scholar] [CrossRef]
- Hrstka, S.C.; Li, X.; Nelson, T.J.; Wanek Program Genetics Pipeline, G. NOTCH1-Dependent Nitric Oxide Signaling Deficiency in Hypoplastic Left Heart Syndrome Revealed Through Patient-Specific Phenotypes Detected in Bioengineered Cardiogenesis. Stem cells 2017, 35, 1106–1119. [Google Scholar] [CrossRef]
- Theis, J.L.; Hrstka, S.C.; Evans, J.M.; O'Byrne, M.M.; de Andrade, M.; O'Leary, P.W.; Nelson, T.J.; Olson, T.M. Compound heterozygous NOTCH1 mutations underlie impaired cardiogenesis in a patient with hypoplastic left heart syndrome. Hum Genet 2015, 134, 1003–1011. [Google Scholar] [CrossRef]
- Paige, S.L.; Galdos, F.X.; Lee, S.; Chin, E.T.; Ranjbarvaziri, S.; Feyen, D.A.M.; Darsha, A.K.; Xu, S.; Ryan, J.A.; Beck, A.L. , et al. Patient-Specific Induced Pluripotent Stem Cells Implicate Intrinsic Impaired Contractility in Hypoplastic Left Heart Syndrome. Circulation 2020, 142, 1605–1608. [Google Scholar] [CrossRef]
- Xu, X.; Jin, K.; Bais, A.S.; Zhu, W.; Yagi, H.; Feinstein, T.N.; Nguyen, P.K.; Criscione, J.D.; Liu, X.; Beutner, G. , et al. Uncompensated mitochondrial oxidative stress underlies heart failure in an iPSC-derived model of congenital heart disease. Cell stem cell 2022, 29, 840–855. [Google Scholar] [CrossRef] [PubMed]
- Alonzo, M.; Contreras, J.; Ye, S.; Lin, H.; Hernandez-Rosario, L.; McBride, K.L.; Texter, K.; Garg, V.; Zhao, M.T. Characterization of an iPSC line NCHi006-A from a patient with hypoplastic left heart syndrome (HLHS). Stem Cell Res 2022, 64, 102892. [Google Scholar] [CrossRef] [PubMed]
- Adhicary, S.; Ye, S.; Lin, H.; Texter, K.; Garg, V.; Zhao, M.T. Establishment of NCHi009-A, an iPSC line from a patient with hypoplastic left heart syndrome (HLHS) carrying a heterozygous NOTCH1 mutation. Stem Cell Res 2023, 66, 103013. [Google Scholar] [CrossRef]
- Yu, Y.; Wang, C.; Ye, S.; Qin, H.; Alonzo, M.; Onorato, A.; Argall, A.; Texter, K.; Ma, Q.; Garg, V. , et al. Common and divergent cellular aetiologies underlying hypoplastic left heart syndrome and hypoplastic right heart syndrome. European heart journal 2025, 46, 1946–1949. [Google Scholar] [CrossRef]
- Kussauer, S.; David, R.; Lemcke, H. hiPSCs Derived Cardiac Cells for Drug and Toxicity Screening and Disease Modeling: What Micro- Electrode-Array Analyses Can Tell Us. Cells 2019, 8. [Google Scholar] [CrossRef]
- Sinnecker, D.; Laugwitz, K.L.; Moretti, A. Induced pluripotent stem cell-derived cardiomyocytes for drug development and toxicity testing. Pharmacology & therapeutics 2014, 143, 246–252. [Google Scholar] [CrossRef]
- Liu, S.; Fang, C.; Zhong, C.; Li, J.; Xiao, Q. Recent advances in pluripotent stem cell-derived cardiac organoids and heart-on-chip applications for studying anti-cancer drug-induced cardiotoxicity. Cell Biol Toxicol 2023, 39, 2527–2549. [Google Scholar] [CrossRef]
- Colatsky, T.; Fermini, B.; Gintant, G.; Pierson, J.B.; Sager, P.; Sekino, Y.; Strauss, D.G.; Stockbridge, N. The Comprehensive in Vitro Proarrhythmia Assay (CiPA) initiative - Update on progress. J Pharmacol Toxicol Methods 2016, 81, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Pan, D.; Li, B.; Wang, S. Establishment and validation of a torsade de pointes prediction model based on human iPSC-derived cardiomyocytes. Exp Ther Med 2023, 25, 61. [Google Scholar] [CrossRef]
- Blinova, K.; Dang, Q.; Millard, D.; Smith, G.; Pierson, J.; Guo, L.; Brock, M.; Lu, H.R.; Kraushaar, U.; Zeng, H. , et al. International Multisite Study of Human-Induced Pluripotent Stem Cell-Derived Cardiomyocytes for Drug Proarrhythmic Potential Assessment. Cell reports 2018, 24, 3582–3592. [Google Scholar] [CrossRef] [PubMed]
- Bedut, S.; Seminatore-Nole, C.; Lamamy, V.; Caignard, S.; Boutin, J.A.; Nosjean, O.; Stephan, J.P.; Coge, F. High-throughput drug profiling with voltage- and calcium-sensitive fluorescent probes in human iPSC-derived cardiomyocytes. American journal of physiology. Heart and circulatory physiology 2016, 311, H44–53. [Google Scholar] [CrossRef]
- Huang, C.Y.; Nicholson, M.W.; Wang, J.Y.; Ting, C.Y.; Tsai, M.H.; Cheng, Y.C.; Liu, C.L.; Chan, D.Z.H.; Lee, Y.C.; Hsu, C.C. , et al. Population-based high-throughput toxicity screen of human iPSC-derived cardiomyocytes and neurons. Cell reports 2022, 39, 110643. [Google Scholar] [CrossRef]
- Goversen, B.; van der Heyden, M.A.G.; van Veen, T.A.B.; de Boer, T.P. The immature electrophysiological phenotype of iPSC-CMs still hampers in vitro drug screening: Special focus on I(K1). Pharmacology & therapeutics 2018, 183, 127–136. [Google Scholar] [CrossRef]
- Koivumaki, J.T.; Naumenko, N.; Tuomainen, T.; Takalo, J.; Oksanen, M.; Puttonen, K.A.; Lehtonen, S.; Kuusisto, J.; Laakso, M.; Koistinaho, J. , et al. Structural Immaturity of Human iPSC-Derived Cardiomyocytes: In Silico Investigation of Effects on Function and Disease Modeling. Front Physiol 2018, 9, 80. [Google Scholar] [CrossRef]
- Vuckovic, S.; Dinani, R.; Nollet, E.E.; Kuster, D.W.D.; Buikema, J.W.; Houtkooper, R.H.; Nabben, M.; van der Velden, J.; Goversen, B. Characterization of cardiac metabolism in iPSC-derived cardiomyocytes: lessons from maturation and disease modeling. Stem Cell Res Ther 2022, 13, 332. [Google Scholar] [CrossRef] [PubMed]
- Tu, C.; Chao, B.S.; Wu, J.C. Strategies for Improving the Maturity of Human Induced Pluripotent Stem Cell-Derived Cardiomyocytes. Circulation research 2018, 123, 512–514. [Google Scholar] [CrossRef]
- Ronaldson-Bouchard, K.; Ma, S.P.; Yeager, K.; Chen, T.; Song, L.; Sirabella, D.; Morikawa, K.; Teles, D.; Yazawa, M.; Vunjak-Novakovic, G. Advanced maturation of human cardiac tissue grown from pluripotent stem cells. Nature 2018, 556, 239–243. [Google Scholar] [CrossRef]
- Parikh, S.S.; Blackwell, D.J.; Gomez-Hurtado, N.; Frisk, M.; Wang, L.; Kim, K.; Dahl, C.P.; Fiane, A.; Tonnessen, T.; Kryshtal, D.O. , et al. Thyroid and Glucocorticoid Hormones Promote Functional T-Tubule Development in Human-Induced Pluripotent Stem Cell-Derived Cardiomyocytes. Circulation research 2017, 121, 1323–1330. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Rodriguez, M.L.; Leonard, A.; Sun, L.; Fischer, K.A.; Wang, Y.; Ritterhoff, J.; Zhao, L.; Kolwicz, S.C., Jr.; Pabon, L. , et al. Fatty Acids Enhance the Maturation of Cardiomyocytes Derived from Human Pluripotent Stem Cells. Stem cell reports 2019, 13, 657–668. [Google Scholar] [CrossRef]
- Li, W.; Luo, X.; Strano, A.; Arun, S.; Gamm, O.; Poetsch, M.S.; Hasse, M.; Steiner, R.P.; Fischer, K.; Poche, J. , et al. Comprehensive promotion of iPSC-CM maturation by integrating metabolic medium with nanopatterning and electrostimulation. Nature communications 2025, 16, 2785. [Google Scholar] [CrossRef] [PubMed]
- Carey, A.S.; Liang, L.; Edwards, J.; Brandt, T.; Mei, H.; Sharp, A.J.; Hsu, D.T.; Newburger, J.W.; Ohye, R.G.; Chung, W.K. , et al. Effect of copy number variants on outcomes for infants with single ventricle heart defects. Circulation. Cardiovascular genetics 2013, 6, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Mills, J.L.; Troendle, J.; Conley, M.R.; Carter, T.; Druschel, C.M. Maternal obesity and congenital heart defects: a population-based study. Am J Clin Nutr 2010, 91, 1543–1549. [Google Scholar] [CrossRef] [PubMed]
- Nicoll, R. Environmental Contaminants and Congenital Heart Defects: A Re-Evaluation of the Evidence. Int J Environ Res Public Health 2018, 15. [Google Scholar] [CrossRef]
- Roland, T.J.; Song, K. Advances in the Generation of Constructed Cardiac Tissue Derived from Induced Pluripotent Stem Cells for Disease Modeling and Therapeutic Discovery. Cells 2024, 13. [Google Scholar] [CrossRef]
- Liu, C.; Feng, X.; Li, G.; Gokulnath, P.; Xiao, J. Generating 3D human cardiac constructs from pluripotent stem cells. EBioMedicine 2022, 76, 103813. [Google Scholar] [CrossRef]
- Min, S.; Cho, S.W. Engineered human cardiac tissues for modeling heart diseases. BMB Rep 2023, 56, 32–42. [Google Scholar] [CrossRef] [PubMed]
- Minale, C.; Nikol, S.; Hollweg, G.; Mittermayer, C.; Messmer, B.J. Clinical experience with expanded polytetrafluoroethylene Gore-Tex surgical membrane for pericardial closure: a study of 110 cases. J Card Surg 1988, 3, 193–201. [Google Scholar] [CrossRef]
- Crawford, F.A., Jr.; Sade, R.M.; Spinale, F. Bovine pericardium for correction of congenital heart defects. The Annals of thoracic surgery 1986, 41, 602–605. [Google Scholar] [CrossRef]
- Gao, L.; Gregorich, Z.R.; Zhu, W.; Mattapally, S.; Oduk, Y.; Lou, X.; Kannappan, R.; Borovjagin, A.V.; Walcott, G.P.; Pollard, A.E. , et al. Large Cardiac Muscle Patches Engineered From Human Induced-Pluripotent Stem Cell-Derived Cardiac Cells Improve Recovery From Myocardial Infarction in Swine. Circulation 2018, 137, 1712–1730. [Google Scholar] [CrossRef] [PubMed]
- Jebran, A.F.; Seidler, T.; Tiburcy, M.; Daskalaki, M.; Kutschka, I.; Fujita, B.; Ensminger, S.; Bremmer, F.; Moussavi, A.; Yang, H. , et al. Engineered heart muscle allografts for heart repair in primates and humans. Nature 2025, 639, 503–511. [Google Scholar] [CrossRef]
- Yeung, E.; Fukunishi, T.; Bai, Y.; Bedja, D.; Pitaktong, I.; Mattson, G.; Jeyaram, A.; Lui, C.; Ong, C.S.; Inoue, T. , et al. Cardiac regeneration using human-induced pluripotent stem cell-derived biomaterial-free 3D-bioprinted cardiac patch in vivo. J Tissue Eng Regen Med 2019, 13, 2031–2039. [Google Scholar] [CrossRef] [PubMed]
- Miyagawa, S.; Kawamura, T.; Ito, E.; Takeda, M.; Iseoka, H.; Yokoyama, J.; Harada, A.; Mochizuki-Oda, N.; Imanishi-Ochi, Y.; Li, J. , et al. Pre-clinical evaluation of the efficacy and safety of human induced pluripotent stem cell-derived cardiomyocyte patch. Stem Cell Res Ther 2024, 15, 73. [Google Scholar] [CrossRef] [PubMed]
- Mahle, W.T.; Hu, C.; Trachtenberg, F.; Menteer, J.; Kindel, S.J.; Dipchand, A.I.; Richmond, M.E.; Daly, K.P.; Henderson, H.T.; Lin, K.Y. , et al. Heart failure after the Norwood procedure: An analysis of the Single Ventricle Reconstruction Trial. The Journal of heart and lung transplantation : the official publication of the International Society for Heart Transplantation 2018, 37, 879–885. [Google Scholar] [CrossRef]
- Querdel, E.; Reinsch, M.; Castro, L.; Kose, D.; Bahr, A.; Reich, S.; Geertz, B.; Ulmer, B.; Schulze, M.; Lemoine, M.D. , et al. Human Engineered Heart Tissue Patches Remuscularize the Injured Heart in a Dose-Dependent Manner. Circulation 2021, 143, 1991–2006. [Google Scholar] [CrossRef] [PubMed]
- Miyagawa, S.; Kainuma, S.; Kawamura, T.; Suzuki, K.; Ito, Y.; Iseoka, H.; Ito, E.; Takeda, M.; Sasai, M.; Mochizuki-Oda, N. , et al. Case report: Transplantation of human induced pluripotent stem cell-derived cardiomyocyte patches for ischemic cardiomyopathy. Front Cardiovasc Med 2022, 9, 950829. [Google Scholar] [CrossRef]
- Liu, C.; Niu, K.; Xiao, Q. Updated perspectives on vascular cell specification and pluripotent stem cell-derived vascular organoids for studying vasculopathies. Cardiovascular research 2022, 118, 97–114. [Google Scholar] [CrossRef]
- Cheruku, G.R.W., C. V. ; Raviendran, S.; Xiao, Q. Recent Advances and Future Perspectives in Vascular Organoids and Vessel-on-Chip Organoids 2024, 3, 203–246. [Google Scholar] [CrossRef]
- Lewis-Israeli, Y.R.; Wasserman, A.H.; Gabalski, M.A.; Volmert, B.D.; Ming, Y.; Ball, K.A.; Yang, W.; Zou, J.; Ni, G.; Pajares, N. , et al. Self-assembling human heart organoids for the modeling of cardiac development and congenital heart disease. Nature communications 2021, 12, 5142. [Google Scholar] [CrossRef]
- Drakhlis, L.; Biswanath, S.; Farr, C.M.; Lupanow, V.; Teske, J.; Ritzenhoff, K.; Franke, A.; Manstein, F.; Bolesani, E.; Kempf, H. , et al. Human heart-forming organoids recapitulate early heart and foregut development. Nature biotechnology 2021, 39, 737–746. [Google Scholar] [CrossRef]
- Yang, J.; Lei, W.; Xiao, Y.; Tan, S.; Yang, J.; Lin, Y.; Yang, Z.; Zhao, D.; Zhang, C.; Shen, Z. , et al. Generation of human vascularized and chambered cardiac organoids for cardiac disease modelling and drug evaluation. Cell Prolif 2024, 57, e13631. [Google Scholar] [CrossRef]
- Song, M.; Choi, D.B.; Im, J.S.; Song, Y.N.; Kim, J.H.; Lee, H.; An, J.; Kim, A.; Choi, H.; Kim, J.C. , et al. Modeling acute myocardial infarction and cardiac fibrosis using human induced pluripotent stem cell-derived multi-cellular heart organoids. Cell Death Dis 2024, 15, 308. [Google Scholar] [CrossRef] [PubMed]
- Richards, D.J.; Li, Y.; Kerr, C.M.; Yao, J.; Beeson, G.C.; Coyle, R.C.; Chen, X.; Jia, J.; Damon, B.; Wilson, R. , et al. Human cardiac organoids for the modelling of myocardial infarction and drug cardiotoxicity. Nat Biomed Eng 2020, 4, 446–462. [Google Scholar] [CrossRef]
- Sharma, P.; Liu Chung Ming, C.; Gentile, C. In vitro modeling of myocardial ischemia/reperfusion injury with murine or human 3D cardiac spheroids. STAR Protoc 2022, 3, 101751. [Google Scholar] [CrossRef] [PubMed]
- Pocock, M.W.; Reid, J.D.; Robinson, H.R.; Charitakis, N.; Krycer, J.R.; Foster, S.R.; Fitzsimmons, R.L.; Lor, M.; Devilee, L.A.C.; Batho, C.A.P. , et al. Maturation of human cardiac organoids enables complex disease modeling and drug discovery. Nat Cardiovasc Res 2025, 4, 821–840. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhao, G.; Ma, T.; Simmons, C.A.; Santerre, J.P. A critical review on advances and challenges of bioprinted cardiac patches. Acta Biomater 2024, 189, 1–24. [Google Scholar] [CrossRef]
- Lu, T.Y.; Xiang, Y.; Tang, M.; Chen, S. 3D Printing Approaches to Engineer Cardiac Tissue. Curr Cardiol Rep 2023, 25, 505–514. [Google Scholar] [CrossRef]
- Faber, L.; Yau, A.; Chen, Y. Translational biomaterials of four-dimensional bioprinting for tissue regeneration. Biofabrication 2023, 16. [Google Scholar] [CrossRef] [PubMed]
- Ashammakhi, N.; Ahadian, S.; Zengjie, F.; Suthiwanich, K.; Lorestani, F.; Orive, G.; Ostrovidov, S.; Khademhosseini, A. Advances and Future Perspectives in 4D Bioprinting. Biotechnol J 2018, 13, e1800148. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Cardiac developmental abnormalities, staged surgical procedures, and representative stem cell treatments in hypoplastic left heart syndrome (HLHS). The key cardiac developmental abnormalities of HLHS include ASD (atrial septal defect), PDA (patent ductus arteriosus), very small aorta (AO), significant under-developed LV (left ventricles), and under-developed MV (mitral valve) or closed MV, resulting in ineffective systemic circulation and early immature mortality. Multiple surgical interventions need to be conducted at early stages (Norwood at 1-2 weeks, Glenn at 3-6 months, and Fontan at 18-36 months) to establish and restore ineffective systemic circulation and prevent early immature death. Based on promising findings from pre-clinical studies using stem cell therapy in HLHS, a series of clinical trials were conducted to evaluate the feasibility, safety, and therapeutic potential of different adult stem cells in HLHS patients. Stem cells were administrated into patients at different stages of surgical procedures. Findings from most clinical studies have demonstrated good feasibility and safety of stem cell application in HLHS patients, with varied therapeutic effects being reported. AV, aortic valve; CDCs, cardiosphere-derived cells; IVC, inferior vena cava; LA, left atrium; MPCs, mesenchymal precursor cells; MSCs, mesenchymal stem cells; MV, mitral valve; PA, pulmonary artery; PV, pulmonary valve; RA, right atrium; RV, right ventricle; SVC, superior vena cava; TV, tricuspid valve; UCB-MNCs, umbilical cord blood mononuclear cells.
Figure 1.
Cardiac developmental abnormalities, staged surgical procedures, and representative stem cell treatments in hypoplastic left heart syndrome (HLHS). The key cardiac developmental abnormalities of HLHS include ASD (atrial septal defect), PDA (patent ductus arteriosus), very small aorta (AO), significant under-developed LV (left ventricles), and under-developed MV (mitral valve) or closed MV, resulting in ineffective systemic circulation and early immature mortality. Multiple surgical interventions need to be conducted at early stages (Norwood at 1-2 weeks, Glenn at 3-6 months, and Fontan at 18-36 months) to establish and restore ineffective systemic circulation and prevent early immature death. Based on promising findings from pre-clinical studies using stem cell therapy in HLHS, a series of clinical trials were conducted to evaluate the feasibility, safety, and therapeutic potential of different adult stem cells in HLHS patients. Stem cells were administrated into patients at different stages of surgical procedures. Findings from most clinical studies have demonstrated good feasibility and safety of stem cell application in HLHS patients, with varied therapeutic effects being reported. AV, aortic valve; CDCs, cardiosphere-derived cells; IVC, inferior vena cava; LA, left atrium; MPCs, mesenchymal precursor cells; MSCs, mesenchymal stem cells; MV, mitral valve; PA, pulmonary artery; PV, pulmonary valve; RA, right atrium; RV, right ventricle; SVC, superior vena cava; TV, tricuspid valve; UCB-MNCs, umbilical cord blood mononuclear cells.
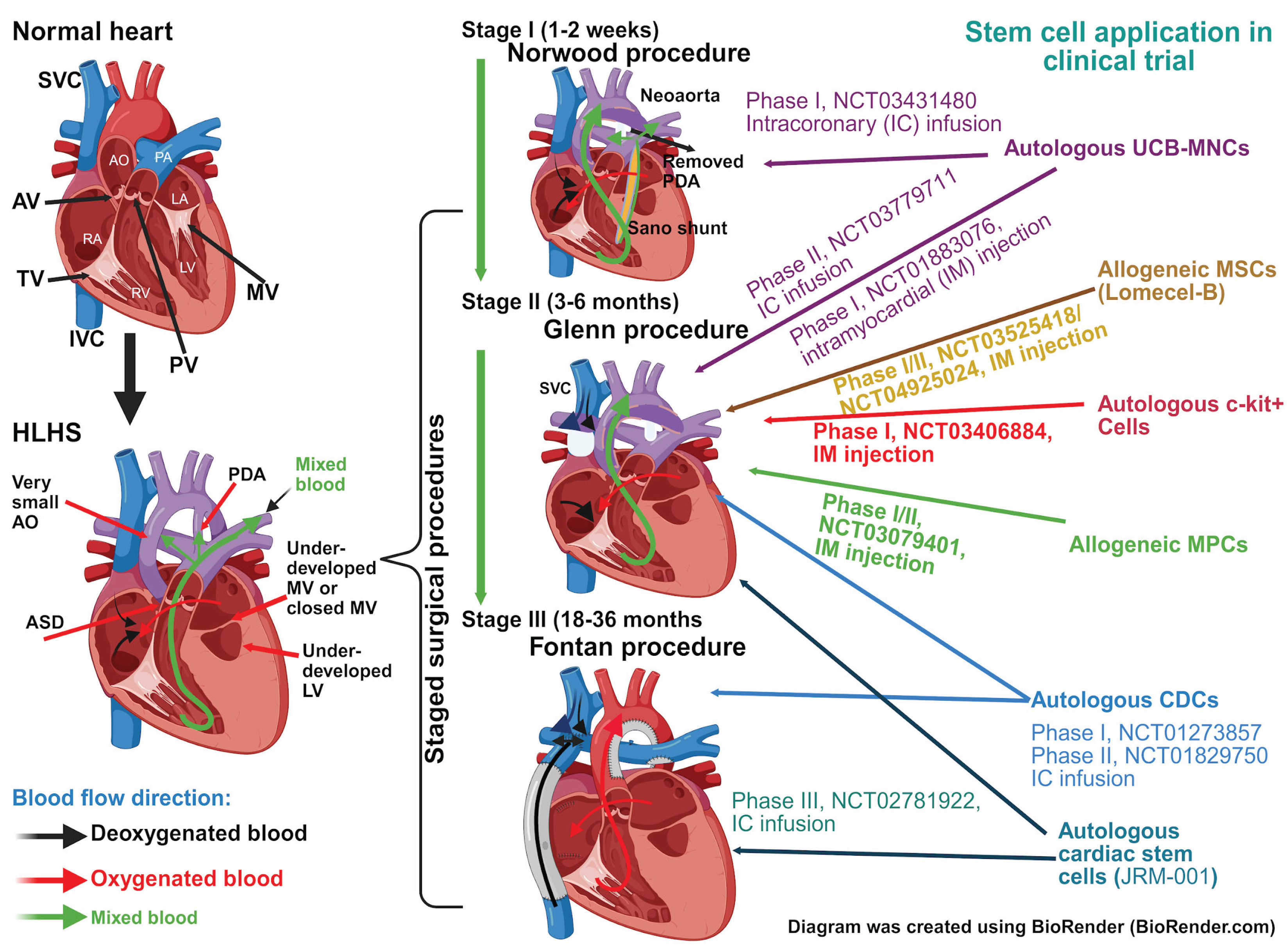
Figure 2.
Human iPSC-derived 3D cardiac patches and applications in HLHS. (A) Multiple types of 3D cardiac structures (cardiac strip, patches, ring and chamber) are generated from patients through several strategies by using cardiac cells (cardiomyocyte, smooth muscle cell, endothelial cell and cardiac fibroblast) either directly isolated from heart or differentiated from patient-specific iPSCs with different biomaterial and techniques (decellularized or 3D bio-printed cardiac tissue, hydrogel/collagen gel and polymer). (B) Krane et al [173] generated HLHS-specific 3D cardiac patches using HLHS iPSC-derived cardiomyocytes (CMs) and decellularized non-human primate’s left ventricular (LV) myocardium. They reported that these cardiac patches exhibited several HLHS-related functional abnormalities (impaired contractility and calcium handling and increased CM apoptosis), demonstrating that these cardiac patches are powerful platform to study HLHS pathogenesis and identify potential therapeutics for HLHS patients. .
Figure 2.
Human iPSC-derived 3D cardiac patches and applications in HLHS. (A) Multiple types of 3D cardiac structures (cardiac strip, patches, ring and chamber) are generated from patients through several strategies by using cardiac cells (cardiomyocyte, smooth muscle cell, endothelial cell and cardiac fibroblast) either directly isolated from heart or differentiated from patient-specific iPSCs with different biomaterial and techniques (decellularized or 3D bio-printed cardiac tissue, hydrogel/collagen gel and polymer). (B) Krane et al [173] generated HLHS-specific 3D cardiac patches using HLHS iPSC-derived cardiomyocytes (CMs) and decellularized non-human primate’s left ventricular (LV) myocardium. They reported that these cardiac patches exhibited several HLHS-related functional abnormalities (impaired contractility and calcium handling and increased CM apoptosis), demonstrating that these cardiac patches are powerful platform to study HLHS pathogenesis and identify potential therapeutics for HLHS patients. .
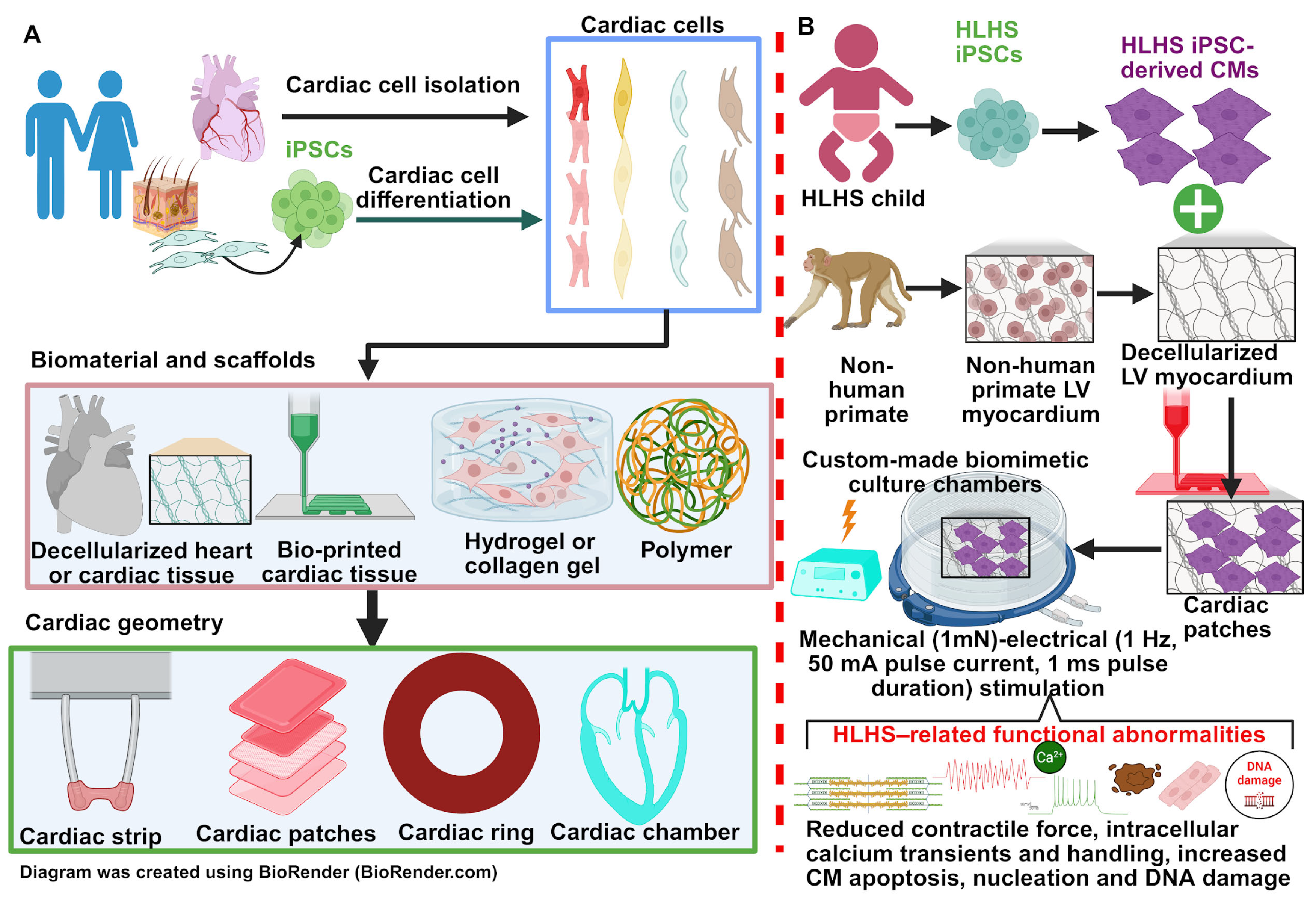
Figure 3.
Human iPSC-derived cardiac organoids (COs) and applications in HLHS. (A) Cardiac organoids (cardiomyocyte (CM) spheroid, self-organized COs, multi-cellular COs, heart-forming organoid (HFO) and cardioid) can be generated from induced pluripotent stem cells (iPSCs) using different strategies. Human iPSCs can be differentiated into different developmental stages with indicated protocol before CO generation, such as mesendoderm cells, mesoderm/cardiac mesoderm cells and cardiac cells (CM, cardiac fibroblast (CF), smooth muscle cell (SMC) and endothelial cell (EC)). Human iPSCs or their derivatives (CMs with or without CFs, SMCs and ECs) can be used to generate different COs through self-aggregation or embryoid body formation, 3D bioprinting or scaffolds with different material (agarose, gelatin/collagen hydrogel, Matrigel, PDMS micropillas and polystyrene). (B) Hofbauer et al [169] generated PSC-derived cardioids with different cellular composition using three experimental protocols (general cardioid, cardioids containing multiple cardiac cells, and epicardial cardioids). Combined with NKX2.5 or HAND1 gene knockout and BMP signaling inhibition, they demonstrated these cardioids could be used for studying cardiogenesis, and modeling left ventricular (LV) development, cardiac cavity defects and cardiac cryoinjury. .
Figure 3.
Human iPSC-derived cardiac organoids (COs) and applications in HLHS. (A) Cardiac organoids (cardiomyocyte (CM) spheroid, self-organized COs, multi-cellular COs, heart-forming organoid (HFO) and cardioid) can be generated from induced pluripotent stem cells (iPSCs) using different strategies. Human iPSCs can be differentiated into different developmental stages with indicated protocol before CO generation, such as mesendoderm cells, mesoderm/cardiac mesoderm cells and cardiac cells (CM, cardiac fibroblast (CF), smooth muscle cell (SMC) and endothelial cell (EC)). Human iPSCs or their derivatives (CMs with or without CFs, SMCs and ECs) can be used to generate different COs through self-aggregation or embryoid body formation, 3D bioprinting or scaffolds with different material (agarose, gelatin/collagen hydrogel, Matrigel, PDMS micropillas and polystyrene). (B) Hofbauer et al [169] generated PSC-derived cardioids with different cellular composition using three experimental protocols (general cardioid, cardioids containing multiple cardiac cells, and epicardial cardioids). Combined with NKX2.5 or HAND1 gene knockout and BMP signaling inhibition, they demonstrated these cardioids could be used for studying cardiogenesis, and modeling left ventricular (LV) development, cardiac cavity defects and cardiac cryoinjury. .
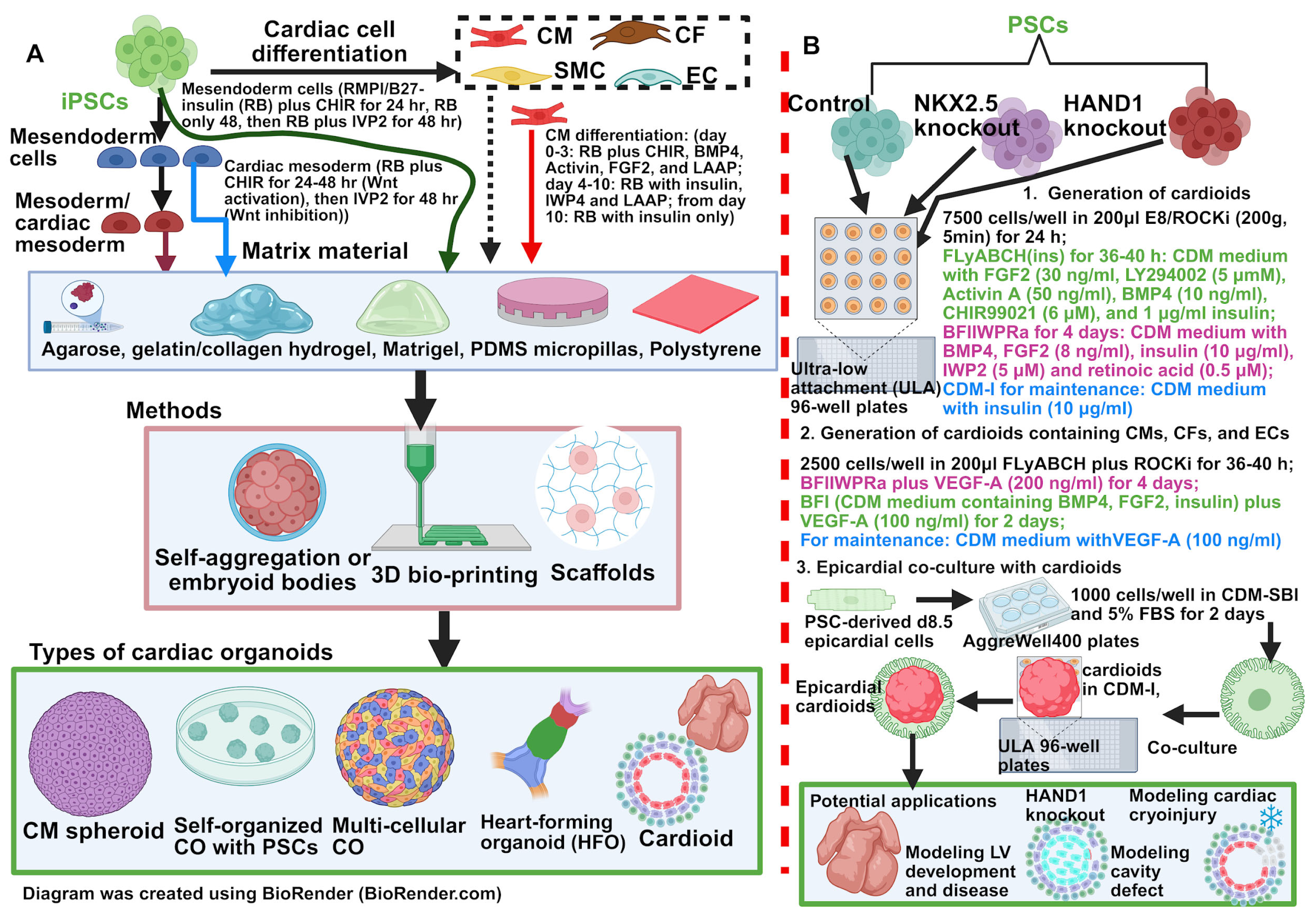
Figure 4.
Applications of cardiac organoids (COs) and potential improvements of COs and 3D engineered heart tissue (EHT). (A) Multiple strategies could be used to further improve CO and EHT maturation and functionalities, such as vascularization, cardiomyocyte (CM) maturation-promoting factors, generation of chamber-specific CMs and incorporation them into COs and EHTs, biomechanical and electrical stimulation, incorporation of non-CM cardiac cells including fibroblasts, pericytes, smooth muscle cells, endothelial cells, immune cells, mesenchymal stem cells and neural cells into COs and EHTs, as well as using different biomaterials and scaffolds. (B) Potential applications of PSC (pluripotent stem cell)-derived COs and EHTs. Increasing numbers of studies demonstrate a variety of promising applications for PSC-derived COs and EHTs, such as investigation of pathological causes of cardiac diseases, in vitro cardiac disease modeling, high-throughput drug screening and drug toxicity testing, creating human CO/EHT biobanks for regenerative medicine, multi-omics analysis to probe novel insights into signaling pathways underlying cardiac development and disease etiology, exploring key developmental events in human heart development, genetic engineering and editing for inherited cardiac disorders, and personalized and precision medicine for patients with cardiac diseases.
Figure 4.
Applications of cardiac organoids (COs) and potential improvements of COs and 3D engineered heart tissue (EHT). (A) Multiple strategies could be used to further improve CO and EHT maturation and functionalities, such as vascularization, cardiomyocyte (CM) maturation-promoting factors, generation of chamber-specific CMs and incorporation them into COs and EHTs, biomechanical and electrical stimulation, incorporation of non-CM cardiac cells including fibroblasts, pericytes, smooth muscle cells, endothelial cells, immune cells, mesenchymal stem cells and neural cells into COs and EHTs, as well as using different biomaterials and scaffolds. (B) Potential applications of PSC (pluripotent stem cell)-derived COs and EHTs. Increasing numbers of studies demonstrate a variety of promising applications for PSC-derived COs and EHTs, such as investigation of pathological causes of cardiac diseases, in vitro cardiac disease modeling, high-throughput drug screening and drug toxicity testing, creating human CO/EHT biobanks for regenerative medicine, multi-omics analysis to probe novel insights into signaling pathways underlying cardiac development and disease etiology, exploring key developmental events in human heart development, genetic engineering and editing for inherited cardiac disorders, and personalized and precision medicine for patients with cardiac diseases.
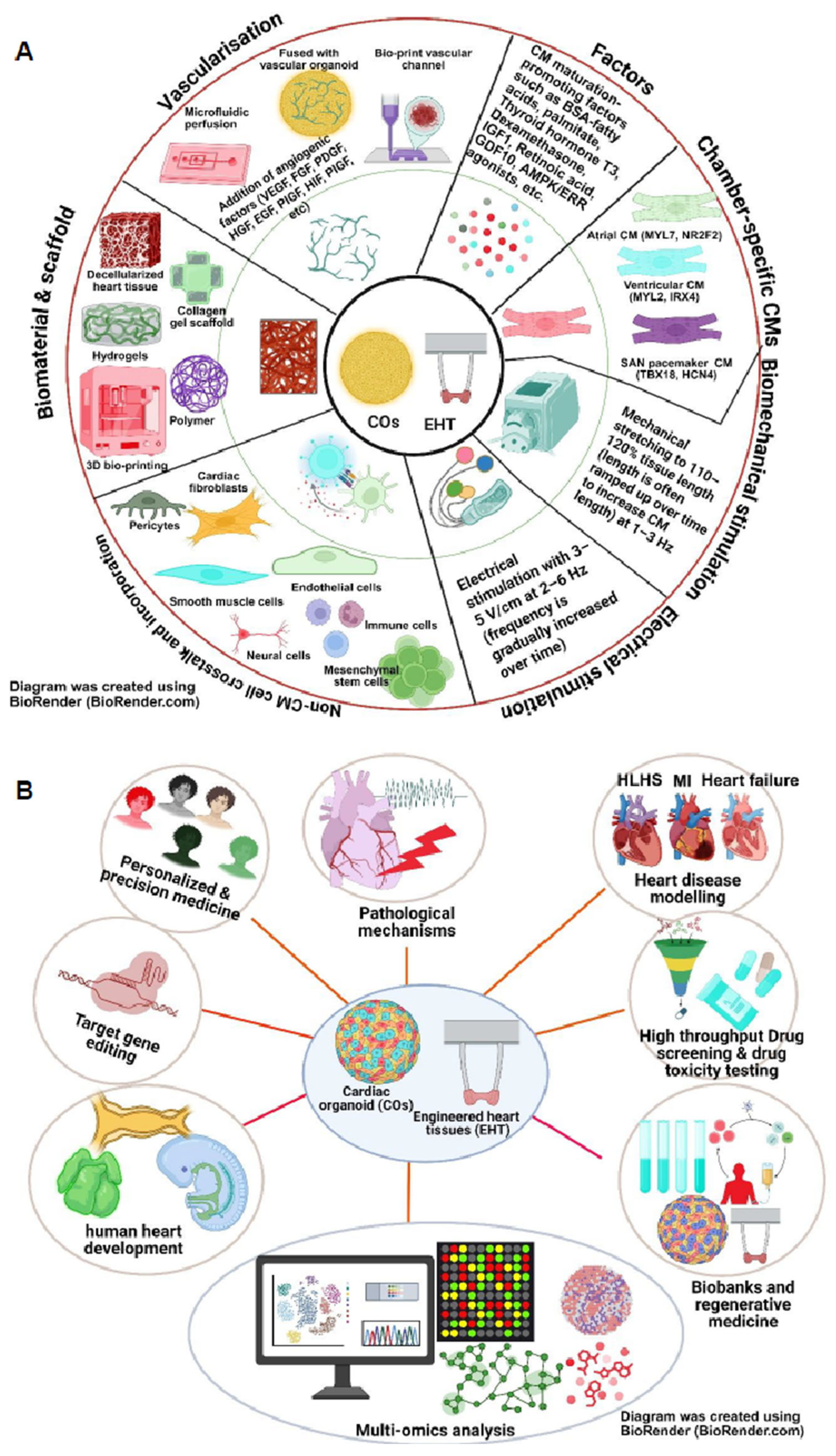
Figure 5.
Generation of functional cardiac patches or engineered heart tissue (EHT) with 3D and 4D bioprinting. Cardiac patches and EHT can be generated through 3D bio-printing technique using cardiac-specific bioink and patient-specific pluripotent stem cells (PSCs) or PSC-derived cardiac cells (cardiomyocytes, fibroblasts, endothelial cells, smooth muscle cells, immune cells, and neural cells). 3D bio-printed EHTs require further improvement to truly recapitulate the anatomical geometry and functionalities of their in vivo counterparts. In this aspect, one of the newly developed strategies, 4D bioprinting, which is mainly involved in integrating smart materials into a 3D bioprinting structure to acquire new shapes or functional properties, could be considered. After 3D bioprinting, EHT could be triggered by a stimulus (change of PH, CO2, O2 and temperature) that will self-reconfigure the structure into a functional cardiac tissue. .
Figure 5.
Generation of functional cardiac patches or engineered heart tissue (EHT) with 3D and 4D bioprinting. Cardiac patches and EHT can be generated through 3D bio-printing technique using cardiac-specific bioink and patient-specific pluripotent stem cells (PSCs) or PSC-derived cardiac cells (cardiomyocytes, fibroblasts, endothelial cells, smooth muscle cells, immune cells, and neural cells). 3D bio-printed EHTs require further improvement to truly recapitulate the anatomical geometry and functionalities of their in vivo counterparts. In this aspect, one of the newly developed strategies, 4D bioprinting, which is mainly involved in integrating smart materials into a 3D bioprinting structure to acquire new shapes or functional properties, could be considered. After 3D bioprinting, EHT could be triggered by a stimulus (change of PH, CO2, O2 and temperature) that will self-reconfigure the structure into a functional cardiac tissue. .
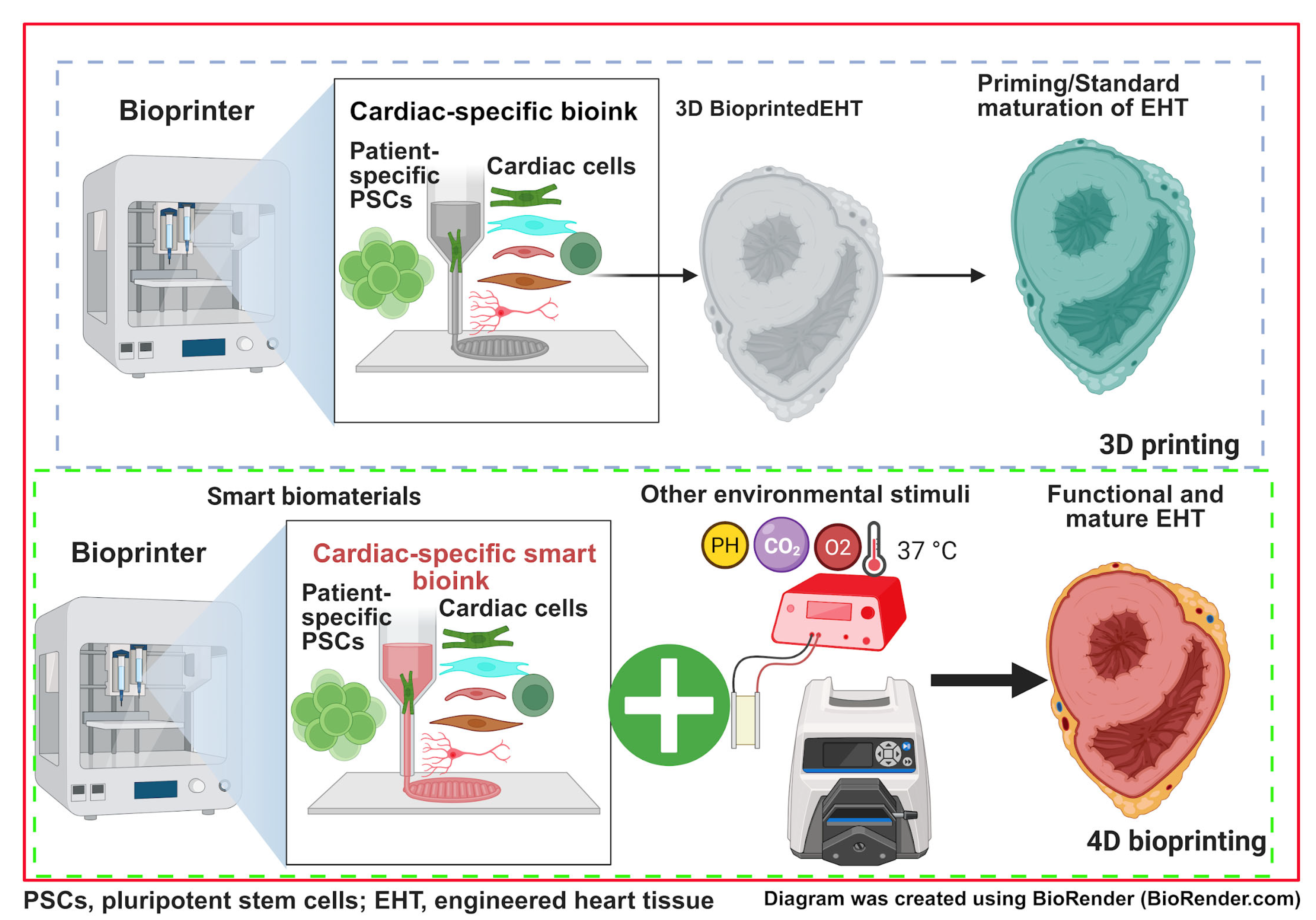

Table 1.
Key signaling molecules, transcriptional factors and regulatory proteins underpinning normal cardiac development and HLHS etiology.
Table 1.
Key signaling molecules, transcriptional factors and regulatory proteins underpinning normal cardiac development and HLHS etiology.
| Signaling Pathway | Normal Function | Disease secondary to defect | Association with HLHS |
|---|---|---|---|
| NOTCH1 | Valve formation; ventricular septation; Left-right patterning; Regulation of progenitor differentiation [34]; |
Bicuspid aortic valve; Right ventricular hypoplasia; VSD [35]; |
Strong–rare genetic variants (G661S,R1279H,A683T) and de novo mutations associated with HLHS found in patients and relatives [36]; Animal models with NOTCH 1 defects display HLHS associated ventricular hypoplasia and valve abnormalities [37,38] |
| Bone Morphogenetic Protein (BMP) | Mesoderm induction and regulation [39]; FHF formation; Proliferation of CMs; Development of cardiac cushion [40]; |
Pulmonary arterial Hypertension; AV canal defects [41]; |
Moderate–BMP2/4 knockouts in mouse models lead to ventricular hypoplasia [42]; Significant interactions with other pathways including Notch, HAND, Wnt, RA and SHH; BMP/TGF-beta dysregulation in human neonatal HLHS myocardial tissue [43]; |
| Retinoic Acid (RA) | Anterior-posterior patterning; FHF and SHF development; Mesoderm formation and induction [44]; |
DiGeorge Syndrome [45]; AV cushion defects; Truncus arteriosus [46] |
Emerging–biological plausibility due to critical role in anterior-posterior axis patterning, FHF and SHF development and chamber specification [44] |
| Wnt/Beta-catenin | Mesoderm induction; CM differentiation; SHF expansion and patterning [47] |
VSD; Truncus Arteriosus; ASD; Familial Exudative Vitreoretinopathy; Arrhythmogenic Cardiomyopathy [48,49] |
Moderate–dysregulated signaling of pathways in HLHS iPSC-CMs. |
| Sonic Hedgehog Pathway (SHH) | Heart tube development; SHF proliferation [50] |
OFT defects; Holoprosencephaly [51] |
Emerging–Essential for SHF and outflow tract development which contribute to normal development of LV [50]. |
| Hippo Pathway | Organ size; Regulates myocardial thickness [52] |
Abnormal heart size [53] | Emerging–Hippo-Yap signaling associated with HLHS iPSC-CMs [54] |
| Fibroblast growth factor (FGF) family | Mesoderm induction; Outflow tracts development; SHF proliferation [55] |
OFT defects; Overriding aorta [56] |
Moderate – pathway dysregulation observed in HLHS fetal lamb model [57] |
| Transcription Factors | Normal Function | Disease secondary to defect | Association with HLHS |
| HAND1 | Ventricle development; LV specification; Ventricular trabeculation [58,59]; |
LV defects; Endocardial cushion defects [60] |
Strong–mouse models with HAND1 deletion resulting in HLHS phenotype; iPSC models demonstrate reduced expression of HAND1 and downstream targets [61]; A126fs frameshift mutation seen in patient cardiac tissue [60] |
| NKX2-5 | Differentiation of CMs and ventricle formation; Purkinje fibre network, AV node and bundle branch development [62]; |
ASD, AV block, AVSD [62] | Moderate–cohort studies show genetic variant (T178M) in subset of HLHS [63]; iPSC studies show reduced expression of NKX2.5 [61] |
| MYRF | Ventricular formation, Transcriptional regulation [64] |
Congenital Diaphragmatic Hernia with CHD and Genitourinary anomalies; Hypomyelination disorders [64] |
Moderate–Associated with syndromic presentations of HLHS; Mutated MYRF in vertebrae models demonstrate HLHS phenotype [65] |
| GATA4 | Septation of chambers; CM differentiation; Valve formation [66] |
ASD, VSD, AVSD [67,68] | Moderate–GATA4 mutation leads to thin ventricular myocardium and CM proliferation [67]; significant synergism with TBX5 required for early cardiogenesis [68] |
| TBX1 [69] | Pharyngeal Arch development; OFT formation; SHF regulation of differentiation and proliferation |
DiGeorge syndrome/velocardiofacial syndrome, Conotruncal heart defects |
Emerging–biologically plausible given role in upstream SHF signaling and regulation |
| TBX5 | Cardiac septation; Conduction system; Chamber specification; |
Holt-Oram syndrome [70,71] |
Moderate – altered function and expression seen in HLHS iPSC studies [72] |
|
WT1 |
Epicardial-to-mesenchymal transition [73] | Wilms Tumor; Denys-Drash syndrome |
Emerging – biological plausibility |
| MEF2C | Heart tube looping; Ventricle formation [74] |
VSD, OFT defects [74,75] | Emerging– knockout animal models display RV and outflow tract defects [76] |
| ISL1 | SHF formation and regulation; Coronary development; |
RV defects, OFT defects, VSD [77] | Moderate– variations can increase susceptibility to CHD including HLHS [78] |
| Structural/Regulatory Proteins | Normal Function | Disease secondary to defect | Evidence for Association with HLHS |
| MYH6 | Encodes Alpha-myosin heavy chain; predominantly atrial contractile function | ASD, Late onset Hypertrophic cardiomyopathy | Moderate– multiple rare genetic variants (R443) found in HLHS cohorts [79]; HiPSC-CM models display reduced contractility [80] |
| LRP2 | Encodes endocytic receptors responsible for developmental signalling (SHH pathway) [81] | Neural tube defects, Donnai-Barrow Syndrome [82] |
Moderate–multiple rare genetic variants found in HLHS genomic and transcriptomic studies [83] |
| GJA1 (Connexin43) | Encodes gap junctions; facilitates electrical and metabolic communications between CMs | Arrhythmogenic Cardiomyopathy, Cardiac conduction disorders, Oculodentodigital Dysplasia [84] |
Emerging – altered expression of GJA1 in HLHS heart tissue [85] |
ASD, atrial septal defects; AV, atrioventricular; AVSD, atrioventricular septal defect; FHF, first heart field; LV, left ventricle; OFT, outflow tract; SHF, second heart field; VSD, ventricular septal defects.
Table 2.
Clinical trials of stem cell applications in HLHS patients.
| Study name (NCT number) | Stem cell type | Study timeline | Study stage | Enrolment: total (control/treatment) | Route and timing of administration | Key findings | Limitations | Status/reference(s) |
|---|---|---|---|---|---|---|---|---|
| Transcoronary Infusion of Cardiac Progenitor Cells in Patients With Single Ventricle Physiology (TICAP) (NCT01273857) | Autologous CDC | 2011-2013 | Phase I | 14 (7/7) | IC at stage II/III surgical palliation | ↑RV function over 18 month period; ↑HF status Safety and feasibility of CDCs; Long-standing benefits on follow-up analysis; |
Non-randomised; Open-Label; Small Sample Size; Variable timing of intervention; |
Completed; Ishigami et al [124] |
| Cardiac Progenitor Cell Infusion to Treat Univentricular Heart Disease (PERSEUS) (NCT01829750) |
Autologous CDC | 2013-2016 | Phase II | 34 (17/17) | IC at stage II/III surgical palliation | ↑RV function; ↑quality of life and somatic growth; Safety and feasibility of CDCs; Long-standing benefits on follow-up analysis |
Limited long term conclusion; Open label; Single Ventricle; Disease heterogeneity |
Completed; Ishigami et al [125] |
| Safety Study of Autologous Umbilical Cord Blood Cells for Treatment of Hypoplastic Left Heart Syndrome (NCT01883076) |
Autologous UCB-MNCs | 2013-2021 | Phase I |
Phase I: 10 (0/10) |
IM during Glenn Operation (Stage II) | Preserved RV; Safety and Feasibility; |
Single centre study; no control group; Short-term follow up; Heterogeneity of UCB-MNCs |
Completed; Burkhart et al [126]; |
| Safety of Autologous Cord Blood Cells in HLHS Patients During Norwood Heart Surgery (NCT03431480) | Autologous UCB-MNCs | 2018-2022 | Phase I | 10 (0/10) | IC during Norwood procedure | Preserved RV; Safety and Feasibility; |
Open label; no control group; Heterogeneity of UCB-MNCs |
Completed; Brizard et al [127] |
| Intramyocardial Injection of Autologous Umbilical Cord Blood Derived Mononuclear Cells During Surgical Repair of Hypoplastic Left Heart Syndrome (NCT03779711) | Autologous UCB-MNCs | 2019-2026 | Phase IIb | 95 (45/50) | IM at Stage II surgical repair | An unfavorable change in longitudinal cardiac strain and a greater incidence (20%) of at least one severe adverse event in treatment group; Failed to enhance cardiac functions |
Multicenter, open-label, nonrandomized study; Negative results. | Completed; Gallego-Navarro et al [128] |
| Cardiac Stem/Progenitor Cell Infusion in Univentricular Physiology (APOLLON) (NCT02781922) | Autologous cardiac stem cells | 2016-2023 | Phase III | 40 (NR/NR) | IC After stage II/III surgical palliation | NR | NR | NR |
| Lomecel-B Injection in Patients With Hypoplastic Left Heart Syndrome: A Phase I/II Study (ELPIS) (NCT03525418/ NCT04925024) |
Allogeneic MSCs (Lomecel-B) | 2018-2025 | Phase I Phase II |
Phase I: 10 (0/10) Phase II: 20 (10/10) |
IM during Glenn Operation | Phase I: Safety and feasibility; No alloimmune sensitisation Phase II: NR |
Phase I: Open Label; No control; Small sample size; Non-Randomised |
Phase I: Completed; Kaushal, et al [20]; Phase II: ongoing; |
| Autologous Cardiac Stem Cell Injection in Patients With Hypoplastic Left Heart Syndrome: An Open Label Pilot Study (CHILD Trial) (NCT03406884) | Autologous c-kit+ | 2019-2024 | Phase I/II | 10 (phase I); 22 (phase II) |
IM during Glenn Operation | NR | Open Label; |
Completed; Pending to report; |
| Mesoblast Stem Cell Therapy for Patients With Single Ventricle and Borderline Left Ventricle (NCT03079401) |
Allogeneic MPCs | 2017-2024 | Phase I Phase II |
19 (9/10) | IM during Glenn Operation | NR | NR | Completed; Pending to report; |
‘↑’, improved or increased; CDCs, cardiosphere-derived cells; IC, intracoronary; IM, intramyocardial; MPCs, mesenchymal precursor cells; MSCs, mesenchymal stem cells; NR, not reported; RV, right ventricle; UCB-MNCs, cord blood mononuclear cells. .
Table 3.
HLHS specific PSC-derived cardiomyocytes and functional characterizations.
| Cell source for iPSC reprogramming | Reprogramming system | Genetic mutations | Methodology (Medium, small molecular) | Key findings | Applications | Reference |
|---|---|---|---|---|---|---|
| H7/H9 ESCs; WTC iPSCs; 176/1 iPSC 176/5 iPSC 176/8 iPSC |
WiCell Research Institute; WiCell Research Institute; IMBA Stem Cell Core Facility |
HAND1 knockout or NKX2.5 knockout PSCs | Cardiac differentiation medium (CDM) with 30 ng/ml FGF2, 5 µM LY294002, 50 ng/ml Activin A, 10 ng/ml BMP4, and CHIR99021 (, 1-4 µM, Wnt-activation) for 36-40 hours; CDM with BMP4 (10ng/ml), FGF2 (8 ng/ml), insulin (10 µg/ml), IWP2 (5µM, Wnt inhibition) and retinoic acid (0.5 µM) for 4 days; CDM with BMP4 (10ng/ml), FGF2 (8 ng/ml) and insulin (10 µg/ml) for 2 days; Then CDM with insulin (10 µg/ml) for CM maintenance |
Main purpose: to screen for factors that are sufficient to stimulate intrinsic 3D cardiac structure formation and confirm that addition of laminins 521/511 before mesoderm induction resulted in intrinsic self-assembly of cells and the striking formation of hollow, beating 3D structures expressing the CM marker TNNT2 after 7 days of differentiation. Findings also confirm stage-specific regulation of HAND1 and NKX2.5 during cardiac development. | Cardioids generation, Molecular insights into cardiac cavity morphogenesis, disease modelling such as cryoinjury (mimicking myocardial infarcti) and HLHS |
Hofbauer et al [169] |
| Cardiac progenitor cells | Retroviruses to deliver OKSM factors | NR (not reported) | Matrigel-based monolayer: RPMI/B27 medium supplemented with 100 ng/ml activin A for 24 h, followed by incubation with 10 ng/ml BMP 4 for an additional 4 days. | Lower cardiomyogenic differentiation potential; decreased NKX2.5, TBX2, NOTCH/HEY signaling, and HAND1/2; reduced H3K4 dimethylation and histone H3 acetylation but increased H3K27 trimethylation. |
Provide molecular insights into complex transcriptional and epigenetic mechanisms underlying HLHS | Kobayashi et al [61] |
| Dermal fibroblasts | Polycistronic lentiviral system for OCT4, KLF4, SOX2, and MYC (OKSM) factors | NR | EB-based protocol: 1 mM ascorbic acid (AA), 4 × 10−4 M monothioglycerol (MTG), 10 ng/ml BMP4, 12.5 ng/ml bFGF, 6 ng/ml Activin A, 150ng/ml DKK1, 5 ng/ml VEGF, and 5.4 μM SB-431542. From day 7, EBs were plated on 0.1% gelatin-coated 12 well culture plates (20 EBs per well) and cultured in in StemPro-34 SFM media supplemented with VEGF and bFGF. |
Decreased number of beating clusters; myofibrillar disorganization, persistence of a fetal gene expression pattern, and changes in commitment to ventricular versus atrial lineages; different calcium transient patterns and electrophysiological responses |
NR | Jiang et al [170] |
| Peripheral blood mononuclear cells (PBMCs) | CytoTune-iPSC 2.0 Sendai Reprogramming Kit | Notch1 knockout | Matrigel-based monolayer (over 90% confluency): RPMI/B27 medium supplemented with 6 μM CHIR99021 for 48 h, RPMI/B27 medium for 24 h, RPMI/B27 medium plus 5 μM IWR-1 for 48 h, then maintain in RPMI/B27 untill use from day 7. Cell were incubated with RPMI1640 no glucose medium plus B27 supplement for 4 days to remove non-CMs. | Disruption of NOTCH1 blocks human ventricular-like CM differentiation but promotes atrial-like CM generation, defective CM proliferation; impaired cell cycle progression and mitosis; biased differentiation toward epicardial and second heart field progenitors at the expense of first heart field progenitors | Possibly modeling HLHS, gaining new insights into the comprehension of the mechanisms underlying HLHS etiology | Ye et al [171] |
| Fibroblast (ATCC) | Episomal plasmid (ND2.0, NIH CRM control iPSC line) | Isogenic hiPSC hypomorphic NOTCH1 clones | Matrigel-based monolayer (over 90% confluency): CM differentiation media A and B | Displayed abnormalities in pathways associated with mitochondrial function, actin cytoskeleton, and cardiomyocyte development; skew differentiation away from CMs and towards fibroblasts and smooth muscle cells; impaired cardiac cytoskeletal and mitochondrial architecture; decreased CM contractility and ATP production | Possibly modeling HLHS; high-throughput drug screen to identify potential HLHS drug such as auranofin. | Lewis et al [172] |
| Neonatal fibroblasts | Polycistronic vector encoding KLF4, OCT4, SOX2, as well as vectors encoding hc-Myc and hKlf4 |
Deleterious genetic variants of Notch1-4 | Embryoid body (EB) based protocol: StemPro-34 SFM (basal media) day 0-3 (10 ng/ml BMP4, 6 ng/ml Activin A, 5 ng/ml bFGF, 10 µM Y276321); day 3-5 (150 ng/ml DKK1, 10 ng/ml VEGF, 5.4 µM SB431542, 0.25 µM Droso, 10 µM Y276321); day 5-7 (150 ng/ml DKK1, 10 ng/ml VEGF, 10 µM Y276321) From day 7, EBs were plated on Matrigel-coated 12 well culture plates (20 EBs per well) and cultured in basal media plus 10 ng/ml VEGF and 5 ng/ml bFGF. |
Reduced ability to give rise to mesodermal, cardiac progenitors and mature CMs and an enhanced ability to differentiate to smooth muscle cells; lower beating rate, disorganised sarcomeres and sarcoplasmic reticulum; blunted response to isoprenaline | Possibly modeling HLHS; provide novel signalling and genetic insights into in HLHS pathogenesis | Yang et al [72] |
| Skin fibroblasts or PBMCs | CytoTune-iPSTM-iPS 2.0 Sendai Reprogramming Kit | heterozygous de-novo mutations in multiple genes including MYRF, BAI2, FGFR1, AIM1L, SYBU, MACF1, etc | Matrigel-based monolayer (over 90% confluency): Day 1: CDM3 (RPMI1640 supplemented with 500 μM/mL Oryza sativa-derived recombinant human albumin and 213 μg/mL L-ascorbic acid 2-phosphate) supplemented with 4-6 μM CHIR99021; Day 2-3: CDM3 plus 2 μM Wnt-C59; Fron day 4: CDM3 |
Unique aberrations in autophagy terms were present when directing HLHS iPSCs toward early cardiac progenitors (CPs), whereas apoptosis-associated pathways appeared solely affected in later CPs (day 6) and cardiomyocytes (day 8); dysregulated lineage-specific CM differentiation; disrupted both early CM subtype lineage specification and CM differentiation and maturation in HLHS |
Possibly modeling HLHS; provide novel signalling and genetic insights into in HLHS pathogenesis; use for 3D cardiax patches generation | Krane et al [173] |
| Dermal fibroblasts | Lentiviral transduction of OKSM factors | heterozygous NOTCH1(P1256L/P1964L) | Monolayer (over 90% confluency): Day 1: RPMI/B27 plus 40-100 ng/ml Activin A; Day 2-5: RPMI/B27 plus 5-20 ng/ml bFGF and BMP4; Fron day 5: RPMI/B27 |
Deficiency in Notch signaling pathway and a diminished capacity to generate CMs; impaired NO signaling | HLHS modeling; identification of small therapeutic molecules to compensate dysregulated NO signaling | Hrstka et al [174] Theis et al [175] |
| Dermal fibroblasts | Sendai reprogramming kits | MYH6-R443P variant | Geltrex-based monlayer: Day 0: mTeSR1 medium plus 5 μM ROCK inhibitor; Day 1-2: insulin-free RPMI/B27 plus 10 μM CHIR99021 and 10 ng/ml Activin-A; Day 3-6: insulin-free RPMI/B27 with 5 μM IWP; From day 7: RPMI/B27 with insulin |
MYH6-R443P variant CMs express beta myosin heavy chain expression (MYH7), with impaired contractility, relaxation, and CM differentiation, as well as sarcomere disorganization | HLHS modeling; study how genetic variants contribute to HLHS. | Kim et al [80]; Tomita-Mitchell et al [79] |
| NR | NR | NR | Small-molecule modulation of the canonical Wnt/β-catenin signaling pathway | Impaired contractility; upregulation in sarcomere and cytoskeletal genes and downregulation in genes involved in mitochondrial function and metabolism; reduced mitochondrial content, mitochondrial respiration and oxidative metabolism | HLHS modeling and drug screening | Paige et al [176] |
| Fibroblasts or lymphoblastoid cells | Episomal plasmids encoding OSKM | Pathogenic variants associated with mitochondrial metabolism | Matrigel-based monolayer (over 90% confluency): Day 1-2: basal CDM3 media (RPMI 1640, BSA, B27, 213 μg/ml Ascorbic acid) and 6 μM CHIR99021; Day 3-14: basal CDM3 media and 10 μM XAV939; Fro day 15: basal CDM3 media minus Ascorbic acid |
Impaired cardiomyocyte differentiation and contractile dysfunction; cell-cycle disturbance with metaphase arrest; incresed CM apoptosis; myofibrillar disarray; mitochondrial dysfunction and perturbation of mitochondrial dynamics; defects in YAP-regulated antioxidant response | Modelling of HLHS and early heart failure; drug screening; identification of potential therapeutics such as sildenafil and TUDCA | Xu et al [177] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



