Submitted:
30 July 2025
Posted:
30 July 2025
You are already at the latest version
Abstract
Perioperative/neoadjuvant chemo-immunotherapy is a standard treatment for patients with resectable non-small cell lung cancer (NSCLC). However, several key clinical questions remain unresolved, including the monitoring of tumor response during neoadjuvant treatment, detection of residual disease after neoadjuvant treatment or after surgery, stratification of recurrence risk, and earlier detection of disease recurrence. Circulating tumor DNA (ctDNA) has emerged as a promising biomarker to ad-dress these challenges. Data from several recent clinical trials of perioperative/neoadjuvant chemo-immunotherapy demonstrated that ctDNA clearance before surgery was associated with higher rates of major pathological response. Additionally, landmark ctDNA positivity after surgery identified patients at high risk of disease recurrence, and longitudinal ctDNA monitoring enabled earlier detection of recurrence compared with radiographic surveillance. Several ongoing trials are incorporating ctDNA as a biomarker to guide treatment decisions, including optimizing the duration of neoadjuvant therapy, evaluating the need for surgery, and tailoring adjuvant strategies. These trials, together with further development of ctDNA detection technologies, will clarify the role of ctDNA analysis in refining perioperative treatment strategies and may ultimately enable individualized care in patients with resectable NSCLC. In this review, we discuss the current research data on ctDNA analysis in NSCLC in this era of perioperative chemo-immunotherapy.
Keywords:
circulating tumor DNA (ctDNA)
; liquid biopsy
; perioperative treatment
; neoadjuvant treatment
; non-small cell lung cancer (NSCLC)
; pathological response
; prognostic factor
1. Introduction
The clinical application of adjuvant immunotherapy [1,2] and neoadjuvant/perioperative chemo-immunotherapy [3,4,5] has expanded the treatment options for patients with resectable but locally-advanced non-small cell lung cancer (NSCLC). At present, there are no definite criteria to determine the appropriate treatment for each patient regarding upfront surgery followed by adjuvant immunotherapy or neoadjuvant chemo-immunotherapy before pulmonary resection. In general, neoadjuvant chemo-immunotherapy should be chosen for patients with more advanced disease who may have a higher risk of undetectable micro-metastases, with the purpose of inducing early systemic treatment. Furthermore, for patients with “marginally” resectable NSCLC, it is anticipated that the surgical time will be shortened and the likelihood of complete resection will increase if the tumor shrinks by neoadjuvant chemo-immunotherapy. Currently, neoadjuvant nivolumab plus chemotherapy (the Checkmate-816 regimen), neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab (the Keynote-671 regimen), and neoadjuvant durvalumab plus chemotherapy followed by adjuvant durvalumab (the AEGEAN regimen) are the available options in several countries. However, treatment response to neoadjuvant or perioperative agents varies among patients, and radiological evaluations sometimes do not correctly reflect tumor status. Therefore, there is a need for clinical examinations that more accurately reflect disease status. Furthermore, precise evaluation of recurrence risk over pathological stage will provide a personalized approach of post-operative care.
Circulating tumor DNA (ctDNA) is a potential groundbreaking biomarker with diagnostic and prognostic value for NSCLC [6,7,8,9]. ctDNA are small fragments of DNA that are released into the bloodstream by tumor cells. These fragments carry genetic and epigenetic alterations that are characteristic of the tumor, providing a unique molecular fingerprint that can be used to identify and quantify residual tumor cells [10,11,12,13]. Several studies reported that positive detection of post-operative ctDNA was a significant poor prognostic factor in patients with surgically resected NSCLC [6,14,15,16,17,18,19,20,21,22,23,24,25,26]. While current ctDNA analysis technology is not sufficiently sensitive to exclude patients who will be cured by surgery alone, some research has suggested the potential utility of ctDNA analysis as a tool to determine patients who will benefit from adjuvant treatment [27,28,29]. In this review, we discuss recent research data on the potential roles of ctDNA analysis in NSCLC patients in this era of perioperative and neoadjuvant chemo-immunotherapy.
2. Literature Search
We performed a systematic literature search using PubMed to identify relevant studies published between January 1st, 2020 and May 31st, 2025. The following keywords were used for the search: lung cancer [all fields] AND circulating tumor DNA [all fields] AND neoadjuvant [all fields]. Of the 51 articles initially identified, 32 were excluded because of article type (25 review articles, 2 study protocols, 1 perspective, 1 meta-analysis, 1 commentary, 1 case report, and 1 editorial). A further 6 studies were excluded because they focused only on NSCLC with epidermal growth factor receptor mutation (n=4) or other cancer types (n=2). Additionally, 7 studies were excluded for lacking neoadjuvant therapy (n=6) or surgical intervention (n=1). Three abstracts at American Society of Clinical Oncology (ASCO) 2025 and one at European Lung Cancer Conference (ELCC) 2025 described the results of ctDNA analysis from phase II or III clinical trials [30,31,32,33], therefore we included these data in this review (Figure 1). The details of these studies are summarized in Table 1. Ongoing clinical trials related to this topic were identified through www.clinicaltrials.gov.
3. Current Clinical Challenges of Perioperative/Neoadjuvant Chemo-Immunotherapy
While perioperative/neoadjuvant chemo-immunotherapy is now being widely used in clinical practice as a treatment for patients with resectable NSCLC, several important questions remain unresolved.
3.1. Need for Neoadjuvant Chemo-Immunotherapy
Some patients with clinical stage II–III disease are curable by surgical resection alone, and the application of neoadjuvant chemo-immunotherapy would be an over-treatment for these patients. Therefore, identifying patients with clinical stage II–III disease who can be treated with surgery alone is critical.
3.2. Adequate Treatment Courses of Neoadjuvant Chemo-Immunotherapy
Three cycles of neoadjuvant chemo-immunotherapy were applied in the Checkmate-816 trial and four cycles were applied in other studies including the Keynote-671 and AEGEAN trials. However, the number of adequate treatment courses of neoadjuvant chemo-immunotherapy remains unclear. We sometimes experience patients who show a dramatic response to neoadjuvant chemo-immunotherapy after only one course of treatment (Figure 2). Several studies evaluated the association between treatment cycles of neoadjuvant therapy and pathological response or ctDNA results and the results suggested that more treatment may be better [35,36,37]. The optimal number of treatment cycles may thus vary among individual patients.
3.3. Monitoring Tumor Response to Neoadjuvant Treatment
Clinical tumor response during neoadjuvant treatment is currently evaluated by radiological examination, mainly with computed tomography (CT). However, we sometimes observe a discordance between the radiological response and actual (pathological) tumor remission after chemo-immunotherapy, which may be because of the difficulty to distinguish true disease progression and inflammatory responses (Figure 3).
3.4. Recurrence Risk Stratification After Pulmonary Resection
As a result of the quite high efficacy of chemo-immunotherapy in some patients with metastatic NSCLC, as evidenced by the so-called “long tail effect” in survival curves, it is hypothesized that some patients may be cured by neoadjuvant treatment alone. These patients may not require adjuvant anti-PD-1/PD-L1 monotherapy and strict radiological follow-up after surgery or even not require pulmonary resection if we can precisely detect minimal residual disease (MRD) after neoadjuvant treatment. For patients with residual disease even after surgical resection, intensive adjuvant treatment, e.g., adding novel therapeutic agents to adjuvant anti-PD-1/PD-L1 monotherapy, may increase the possibility of cure or improve the event-free and overall survival.
4. Utility of ctDNA Analysis as a Tool to Solve the Above Clinical Questions
The use of ctDNA as a tool to evaluate tumor burden or detect MRD offers some advantages over traditional radiological examinations. ctDNA analysis is minimally invasive, requiring only small amount of blood sample (~ 20 ml), which allows repeated sampling over time. ctDNA can provide a comprehensive view of the tumor’s genetic landscape, capturing heterogeneity or therapy-resistant clones of residual disease [22,36,37,38]. Therefore, ctDNA analysis is emerging as a potential promising biomarker to refine clinical decision-making in the perioperative setting in NSCLC.
4.1. Utility of ctDNA Analysis Before and During Neoadjuvant Treatment
In the previous studies of MRD detection in patients who received upfront surgery for NSCLC, compared with post-surgical ctDNA analysis, pre-treatment ctDNA was associated with factors related to DNA shedding [38], such as larger tumor size, clinical stage (tumor burden), and squamous cell histology, and was less associated with patient outcomes [7,14,39]. ctDNA analysis may be beneficial to identify patients with a high tumor burden (candidates for neoadjuvant treatment rather than upfront surgery) or low tumor burden (candidates for limited surgical resection). However, currently, the use of pre-treatment ctDNA analysis for these applications has not been formally explored or demonstrated, and currently pre-treatment ctDNA testing is generally used to assess baseline values.
ctDNA analysis during neoadjuvant treatment may serve as a valuable tool for monitoring therapeutic response. We sometimes experience patients whose radiological response was inconsistent with pathological treatment efficacy as described above. The case described in Figure 3 illustrates the limitations of conventional imaging in assessing treatment response after chemo-immunotherapy. Furthermore, a potential discordance between radiographic and pathologic responses following neoadjuvant chemo-immunotherapy has been reported [40], underscoring the need for more reliable biomarkers for response, such as ctDNA, to accurately evaluate treatment efficacy and guide adequate perioperative management. Thus, ctDNA analysis is anticipated to provide useful information as to whether neoadjuvant treatment should be continued or if neoadjuvant treatment should be terminated and instead pulmonary resection should be performed because of progressive disease.
4.2. Utility of ctDNA Analysis Before Surgical Resection
Surgical strategies can be modified on the basis of the remaining tumor cells after neoadjuvant chemo-immunotherapy. However, the remaining tumor cells are usually assessed by pathological examination of resected tumor specimens. These pathological responses, specifically major pathological response (MPR) and/or complete pathological response, are promising surrogate endpoints for survival after pulmonary resection [41,42,43].
Xu et al. reported that ctDNA status before neoadjuvant immunotherapy did not correlate with patient outcome, as described above; however, patients who exhibited ctDNA clearance before surgery had significantly higher MPR rates compared with those with residual ctDNA (88.2% vs. 11.1%, P < 0.001) [44]. Other authors also reported the correlation between ctDNA clearance and complete pathological response [31] or MPR [45,46,47]. ctDNA negativity after neoadjuvant chemo-immunotherapy was also shown to be a biomarker to predict pathological response [48]. The detailed results of these studies are summarized in Figure 4 (3-1. Prediction for pCR and 3-2. Prediction for MPR).
Because ctDNA status after neoadjuvant chemo-immunotherapy was associated with pathological response and the pathological response is associated with survival outcome of patients, ctDNA status after neoadjuvant chemo-immunotherapy may reasonably predict patient outcome. Studies have reported that ctDNA negativity and ctDNA clearance were significantly associated with superior recurrence-free and overall survival (3-3. Prediction of survival, Figure 4) [30,49]. For example, Yue et al. reported that detected ctDNA after neoadjuvant therapy tended to be associated with worse recurrence-free survival, with a HR of 7.41 (95% CI: 0.91¬–60.22, P=0.03) [45].
4.3. Landmark ctDNA Status as a Tool for MRD Detection
Evaluation of ctDNA status after surgery is often referred to as “landmark analysis” and the detection of ctDNA at this landmark point is considered as MRD positive. Yue et al. performed ctDNA analysis using blood samples obtained between 3- and 8-days post-surgery. The authors found that 31.8% of patients had detectable ctDNA and positive MRD status was an independent risk factor for recurrence (HR, 5.37; 95% CI: 1.27–22.67; log-rank P=0.01) [45]. Another group examined ctDNA status at post-neoadjuvant and post-surgical resection time points and reported that patients who were ctDNA negative at both time points had an 18-month event-free survival rate of 93.8% compared with 47.3% for patients with ctDNA positive status at one of these two time points (HR: 0.15; 95% CI: 0.04–0.94; P=0.005) [48]. In the AEGEAN trial, 168 patients were included in the biomarker-evaluable population, and 10.1% were ctDNA-positive after surgery. Among these MRD-positive patients, 76.5% experienced disease recurrence or death within 12 months postoperatively compared with only 11.9% in the ctDNA-negative group (4-1. Prediction of survival, Figure 4) [32]. Whether ctDNA status at the landmark point will add further prognostic impact over pathological response remains controversial [32,46,49].
4.4. Longitudinal ctDNA Analysis for Early Detection of Disease Recurrence
Longitudinal ctDNA analysis is the serial measurement of ctDNA in plasma samples collected at multiple time points after pulmonary resection. The principal advantage of longitudinal ctDNA analysis lies in its capacity to detect molecular recurrence several months prior to radiographic recurrence [14,50]. Even in patients who received neoadjuvant treatment, post-operative longitudinal ctDNA analysis detected disease recurrence an average of 6.83 months earlier than conventional imaging [45].
5. Ongoing Clinical Trials Involving ctDNA During Perioperative Chemo-Immunotherapy
In numerous ongoing clinical trials of perioperative immunotherapy for NSCLC, ctDNA analysis is incorporated as part of the primary, secondary or exploratory endpoints. Many of these trials use ctDNA clearance (ctDNA resolution) after neoadjuvant immunotherapy or after surgery for the prediction of pathological response or prognostic classification purposes. Representative trials include NCT05382052 (REAL-NADIM), NCT05778253, NCT06111807, NCT06123754, and NCT06221462 (the PRIORITY trial).
ctDNA status is the primary endpoint in the phase II trial NCT04638582 comparing neoadjuvant pembrolizumab with or without chemotherapy in resectable early-stage NSCLC, which aims to evaluate ctDNA clearance after neoadjuvant immunotherapy and after surgery. The PROPHET trial (NCT06977074) is a phase II proof-of-concept study designed to evaluate the clinical utility of ctDNA testing to optimize the number of induction chemo-immunotherapy cycles in patients with resectable NSCLC. The SAVED LUNG trial (NCT06743555) is a study evaluating the feasibility of omitting surgery in NSCLC patients who achieve a clinical complete response after neoadjuvant therapy; ctDNA-based MRD assessment is also being performed in this trial. In some studies, such as ADOPT-LUNG (NCT06284317) and NCT06902272, the implications of adjuvant treatment in patients who received neoadjuvant treatment and surgical resection are being evaluated with an exploratory analysis of ctDNA status. These trials are summarized in Table 2.
6. Conclusions
Promising data have been published from clinical trials regarding the roles of ctDNA analysis in NSCLC treated with neoadjuvant/perioperative chemo-immunotherapy. Many ongoing studies are incorporating ctDNA as a biomarker to predict outcome and guide treatment decisions. These trials, together with the further development of ctDNA detection technologies, will clarify the role of ctDNA analysis in refining perioperative treatment strategies and may ultimately enable individualized care in patients with resectable NSCLC.
Author Contributions
Shuta Ohara: Methodology, Formal analysis, Investigation, Writing - Original Draft, Writing - Review & Editing, Visualization. Kenichi Suda: Conceptualization, Writing - Original Draft, Writing - Review & Editing, Visualization, Supervision, Project administration, Funding acquisition. Yasuhiro Tsutani: Validation, Writing - Review & Editing, Supervision.
Funding
This study was partly supported by grants-in-aid for scientific research from the Japan Society for the Promotion of Science (grants 24K10394 to Dr. Ohara / Dr. Suda and 22K07291 to Dr. Suda).
Data Availability Statement
This review article summarized published data and the data that support the findings of this study are available from the corresponding author (K.S.) upon reasonable request.
Acknowledgments
We thank Gabrielle White Wolf, PhD, from Edanz (https://jp.edanz.com/ac) for editing a draft of this manuscript.
Conflicts of Interest
Dr. Ohara has received honoraria from AstraZeneca. Dr. Suda has received research funding from AstraZeneca; has received honoraria from Chugai, MSD, Daiichi-Sankyo, and AstraZeneca; has undertaken an advisory board for Chugai and AstraZeneca outside of the submitted work. Dr. Tsutani has undertaken an advisory role for AstraZeneca and Chugai; received honoraria from AstraZeneca, Chugai, Eli Lilly Japan, Daiichi Sankyo, Novartis, Takeda, and Taiho; and has received research funding from Boehringer Ingelheim, Chugai, Daiichi Sankyo, Otsuka, and Taiho outside of the submitted work.
Abbreviations
The following abbreviations are used in this manuscript:
NSCLC: Non-small cell lung cancer, ctDNA: Circulating tumor DNA, MRD: Minimal residual disease, ASCO: American Society of Clinical Oncology, ELCC: European Lung Cancer Conference, MPR: Major pathological response, pCR: Pathological complete response, CT: Computed tomography, FDG-PET/CT: Fluorodeoxyglucose–positron emission tomography/computed tomography, PD-1: Programmed cell death protein 1, PD-L1: Programmed death-ligand 1, HR: Hazard ratio, RFS: Recurrence-free survival.
References
- Felip, E.; Altorki, N.; Zhou, C.; Vallières, E.; Martínez-Martí, A.; Rittmeyer, A.; Chella, A.; Reck, M.; Goloborodko, O.; Huang, M.; et al. Overall survival with adjuvant atezolizumab after chemotherapy in resected stage II-IIIA non-small-cell lung cancer (IMpower010): a randomised, multicentre, open-label, phase III trial. Ann. Oncol. 2023, 34, 907–919. [CrossRef]
- O’bRien, M.; Paz-Ares, L.; Marreaud, S.; Dafni, U.; Oselin, K.; Havel, L.; Esteban, E.; Isla, D.; Martinez-Marti, A.; Faehling, M.; et al. Pembrolizumab versus placebo as adjuvant therapy for completely resected stage IB–IIIA non-small-cell lung cancer (PEARLS/KEYNOTE-091): an interim analysis of a randomised, triple-blind, phase 3 trial. Lancet Oncol. 2022, 23, 1274–1286. [CrossRef]
- Forde PM, Spicer J, Lu S, Provencio M, Mitsudomi T, Awad MM, Felip E, Broderick SR, Brahmer JR, Swanson SJ et al. Neoadjuvant Nivolumab plus Chemotherapy in Resectable Lung Cancer. N Engl J Med 2022; 386: 1973-1985.
- Spicer, J.D.; Garassino, M.C.; Wakelee, H.; Liberman, M.; Kato, T.; Tsuboi, M.; Lee, S.-H.; Chen, K.-N.; Dooms, C.; Majem, M.; et al. Neoadjuvant pembrolizumab plus chemotherapy followed by adjuvant pembrolizumab compared with neoadjuvant chemotherapy alone in patients with early-stage non-small-cell lung cancer (KEYNOTE-671): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 2024, 404, 1240–1252. [CrossRef]
- Heymach, J.V.; Harpole, D.; Mitsudomi, T.; Taube, J.M.; Galffy, G.; Hochmair, M.; Winder, T.; Zukov, R.; Garbaos, G.; Gao, S.; et al. Perioperative Durvalumab for Resectable Non–Small-Cell Lung Cancer. New Engl. J. Med. 2023, 389, 1672–1684. [CrossRef]
- Abbosh, C.; Birkbak, N.J.; Wilson, G.A.; Jamal-Hanjani, M.; Constantin, T.; Salari, R.; Le Quesne, J.; Moore, D.A.; Veeriah, S.; Rosenthal, R.; et al. Phylogenetic ctDNA analysis depicts early-stage lung cancer evolution. Nature 2017, 545, 446–451. [CrossRef]
- Abbosh, C.; Hodgson, D.; Doherty, G.J.; Gale, D.; Black, J.R.; Horn, L.; Reis-Filho, J.S.; Swanton, C. Implementing circulating tumor DNA as a prognostic biomarker in resectable non-small cell lung cancer. Trends Cancer 2024, 10, 643–654. [CrossRef]
- Peng, Y.; Mei, W.; Ma, K.; Zeng, C. Circulating Tumor DNA and Minimal Residual Disease (MRD) in Solid Tumors: Current Horizons and Future Perspectives. Front. Oncol. 2021, 11. [CrossRef]
- Pellini, B.; Chaudhuri, A.A. Circulating Tumor DNA Minimal Residual Disease Detection of Non–Small-Cell Lung Cancer Treated With Curative Intent. J. Clin. Oncol. 2022, 40, 567–575. [CrossRef]
- Diehl, F.; Schmidt, K.; Choti, M.A.; Romans, K.; Goodman, S.; Li, M.; Thornton, K.; Agrawal, N.; Sokoll, L.; Szabo, S.A.; et al. Circulating mutant DNA to assess tumor dynamics. Nat. Med. 2008, 14, 985–990. [CrossRef]
- Qin, Z.; Ljubimov, V.A.; Zhou, C.; Tong, Y.; Liang, J. Cell-free circulating tumor DNA in cancer. Chin. J. Cancer 2016, 35, 1–9. [CrossRef]
- Burgener, J.M.; Rostami, A.; De Carvalho, D.D.; Bratman, S.V. Cell-free DNA as a post-treatment surveillance strategy: current status. Semin. Oncol. 2017, 44, 330–346. [CrossRef]
- Chakrabarti, S.; Kasi, A.K.; Parikh, A.R.; Mahipal, A. Finding Waldo: The Evolving Paradigm of Circulating Tumor DNA (ctDNA)—Guided Minimal Residual Disease (MRD) Assessment in Colorectal Cancer (CRC). Cancers 2022, 14, 3078. [CrossRef]
- Ohara, S.; Suda, K.; Sudhaman, S.; Hamada, A.; Chiba, M.; Shimoji, M.; Takemoto, T.; Kalashnikova, E.; Cheung, S.K.; Krainock, M.; et al. Clinical Significance of Perioperative Minimal Residual Disease Detected by Circulating Tumor DNA in Patients With Lung Cancer With a Long Follow-up Data: An Exploratory Study. JTO Clin. Res. Rep. 2024, 6, 100762. [CrossRef]
- Gale, D.; Heider, K.; Ruiz-Valdepenas, A.; Hackinger, S.; Perry, M.; Marsico, G.; Rundell, V.; Wulff, J.; Sharma, G.; Knock, H.; et al. Residual ctDNA after treatment predicts early relapse in patients with early-stage non-small cell lung cancer. Ann. Oncol. 2022, 33, 500–510. [CrossRef]
- Chen, K.; Zhao, H.; Shi, Y.; Yang, F.; Wang, L.T.; Kang, G.; Nie, Y.; Wang, J. Perioperative Dynamic Changes in Circulating Tumor DNA in Patients with Lung Cancer (DYNAMIC). Clin. Cancer Res. 2019, 25, 7058–7067. [CrossRef]
- Chen, K.; Yang, F.; Shen, H.; Wang, C.; Li, X.; Chervova, O.; Wu, S.; Qiu, F.; Peng, D.; Zhu, X.; et al. Individualized tumor-informed circulating tumor DNA analysis for postoperative monitoring of non-small cell lung cancer. Cancer Cell 2023, 41, 1749–1762.e6. [CrossRef]
- Chaudhuri, A.A.; Chabon, J.J.; Lovejoy, A.F.; Newman, A.M.; Stehr, H.; Azad, T.D.; Khodadoust, M.S.; Esfahani, M.S.; Liu, C.L.; Zhou, L.; et al. Early Detection of Molecular Residual Disease in Localized Lung Cancer by Circulating Tumor DNA Profiling. Cancer Discov. 2017, 7, 1394–1403. [CrossRef]
- Xia, L.; Pu, Q.; Kang, R.; Mei, J.; Li, L.; Yang, Y.; Deng, S.; Feng, G.; Ma, L.; Lin, F.; et al. Dynamic ctDNA to inform the precise management of resected NSCLC: LUNGCA-2 study.. J. Clin. Oncol. 2023, 41, 8528–8528. [CrossRef]
- Chin, R.-I.; Chen, K.; Usmani, A.; Chua, C.; Harris, P.K.; Binkley, M.S.; Azad, T.D.; Dudley, J.C.; Chaudhuri, A.A. Detection of Solid Tumor Molecular Residual Disease (MRD) Using Circulating Tumor DNA (ctDNA). Mol. Diagn. Ther. 2019, 23, 311–331. [CrossRef]
- Fu, R.; Huang, J.; Tian, X.; Liang, C.; Xiong, Y.; Zhang, J.; Jiang, B.; Dong, S.; Gong, Y.; Gao, W.; et al. Postoperative circulating tumor DNA can refine risk stratification in resectable lung cancer: results from a multicenter study. Mol. Oncol. 2023, 17, 825–838. [CrossRef]
- Li, N.; Wang, B.; Shao, Y.; Li, M.; Li, J.; Kuang, P.; Liu, Z.; Sun, T.; Wu, H.; Ou, W.; et al. Perioperative circulating tumor DNA as a potential prognostic marker for operable stage I to IIIA non–small cell lung cancer. Cancer 2021, 128, 708–718. [CrossRef]
- Tian, X.; Liu, X.; Wang, K.; Wang, R.; Li, Y.; Qian, K.; Wang, T.; Zhao, X.; Liu, L.; Zhang, P.L.; et al. Postoperative ctDNA in indicating the recurrence risk and monitoring the effect of adjuvant therapy in surgical non-small cell lung cancer. Thorac. Cancer 2024, 15, 797–807. [CrossRef]
- Tran, H.; Heeke, S.; Sujit, S.; Vokes, N.; Zhang, J.; Aminu, M.; Lam, V.; Vaporciyan, A.; Swisher, S.; Godoy, M.; et al. Circulating tumor DNA and radiological tumor volume identify patients at risk for relapse with resected, early-stage non-small-cell lung cancer. Ann. Oncol. 2023, 35, 183–189. [CrossRef]
- Waldeck, S.; Mitschke, J.; Wiesemann, S.; Rassner, M.; Andrieux, G.; Deuter, M.; Mutter, J.; Lüchtenborg, A.; Kottmann, D.; Titze, L.; et al. Early assessment of circulating tumor DNA after curative-intent resection predicts tumor recurrence in early-stage and locally advanced non-small-cell lung cancer. Mol. Oncol. 2021, 16, 527–537. [CrossRef]
- Wang, S.; Li, M.; Zhang, J.; Xing, P.; Wu, M.; Meng, F.; Jiang, F.; Wang, J.; Bao, H.; Huang, J.; et al. Circulating tumor DNA integrating tissue clonality detects minimal residual disease in resectable non-small-cell lung cancer. J. Hematol. Oncol. 2022, 15, 1–6. [CrossRef]
- Wakelee, H.; Reck, M.; Felip, E.; Altorki, N.; Vallieres, E.; Liersch, R.; Oizumi, S.; Tanaka, H.; Hamm, J.; McCune, S.; et al. 1211P IMpower010: ctDNA status and 5y DFS follow up in patients (pts) with resected NSCLC who received adjuvant chemotherapy (chemo) followed by atezolizumab (atezo) or best supportive care (BSC). Ann. Oncol. 2024, 35, S779–S780. [CrossRef]
- Qiu, B.; Guo, W.; Zhang, F.; Lv, F.; Ji, Y.; Peng, Y.; Chen, X.; Bao, H.; Xu, Y.; Shao, Y.; et al. Dynamic recurrence risk and adjuvant chemotherapy benefit prediction by ctDNA in resected NSCLC. Nat. Commun. 2021, 12, 1–11. [CrossRef]
- Wang, B.; Zou, B.; Xu, S.; Zhao, C.; Pei, J.; Wang, S.; Zhao, K.; Yu, J.; Liu, J. Postoperative ctDNA detection predicts relapse but has limited effects in guiding adjuvant therapy in resectable stage I NSCLC. Front. Oncol. 2023, 13, 1083417. [CrossRef]
- Forde, P.M.; Spicer, J.; Provencio, M.; Mitsudomi, T.; Awad, M.M.; Wang, C.; Lu, S.; Felip, E.; Broderick, S.; Swanson, S.; et al. Overall survival with neoadjuvant nivolumab (NIVO) + chemotherapy (chemo) in patients with resectable NSCLC in CheckMate 816.. J. Clin. Oncol. 2025, 43. [CrossRef]
- Cascone, T.; Awad, M.M.; Spicer, J.; He, J.; Lu, S.; Tanaka, F.; Cornelissen, R.; Petruzelka, L.B.; Ito, H.; Koch, L.D.O.; et al. Perioperative nivolumab (NIVO) vs placebo (PBO) in patients (pts) with resectable NSCLC: Updated survival and biomarker analyses from CheckMate 77T.. J. Clin. Oncol. 2025, 43. [CrossRef]
- Reck, M.; Gale, D.; Zhu, Z.; Harpole, D.H.; Taube, J.M.; Mitsudomi, T.; Van Luong, D.; Hochmair, M.; Lee, K.-Y.; Horio, Y.; et al. Association of post-surgical MRD status with neoadjuvant ctDNA dynamics, genomic mutations, and clinical outcomes in patients with resectable NSCLC (R-NSCLC) from the phase 3 AEGEAN trial.. J. Clin. Oncol. 2025, 43, 8009–8009. [CrossRef]
- Serna-Blasco, R.; Nadal, E.; Gonzalez-Larriba, J.; Martinez-Marti, A.; Caro, R.B.; Bosch-Barrera, J.; De Juan, V.C.; Molla, M.I.; Reguart, N.; Carpeño, J.d.C.; et al. 210P: Prognostic Value of minimal residual disease in the NADIM II trial. J. Thorac. Oncol. 2025, 20, S138–S139. [CrossRef]
- Forde PM, Spicer JD, Provencio M, Mitsudomi T, Awad MM, Wang C, Lu S, Felip E, Swanson SJ, Brahmer JR et al. Overall Survival with Neoadjuvant Nivolumab plus Chemotherapy in Lung Cancer. N Engl J Med 2025.
- Zhang, B.; Guo, X.; Jia, R.; Wang, Z.; Wu, J.; Chen, X.; Li, J.; Yang, D.; Li, X.; Wang, W.; et al. Neoadjuvant chemoimmunotherapy cycle number selection for non-small cell lung cancer and clinical outcomes: a real-world analysis. Front. Oncol. 2023, 13, 1200625. [CrossRef]
- Shao, M.; Yao, J.; Wang, Y.; Zhao, L.; Li, B.; Li, L.; Wu, Z.; Chen, Z.; Fan, J.; Qiu, F. Two vs three cycles of neoadjuvant sintilimab plus chemotherapy for resectable non-small-cell lung cancer: neoSCORE trial. Signal Transduct. Target. Ther. 2023, 8, 1–3. [CrossRef]
- Reck, M.; Gale, D.; Harpole, D.; Taube, J.; Mitsudomi, T.; Hochmair, M.; Winder, T.; Zhu, Z.; Lai, Z.; Stewart, R.; et al. LBA59 Associations of ctDNA clearance and pathological response with neoadjuvant treatment in patients with resectable NSCLC from the phase III AEGEAN trial. Ann. Oncol. 2023, 34, S1300–S1300. [CrossRef]
- Suda K. DNA shedding in non-small-cell lung cancer: useful to assess? Lancet Respir Med 2018; 6: 77-78.
- Zheng, J.; Qin, C.; Wang, Q.; Tian, D.; Chen, Z. Circulating tumour DNA-Based molecular residual disease detection in resectable cancers: a systematic review and meta-analysis. EBioMedicine 2024, 103, 105109. [CrossRef]
- Saw, S.P.L.; Ong, B.-H.; Chua, K.L.M.; Takano, A.; Tan, D.S.W. Revisiting neoadjuvant therapy in non-small-cell lung cancer. Lancet Oncol. 2021, 22, e501–e516. [CrossRef]
- Pataer, A.; Kalhor, N.; Correa, A.M.; Raso, M.G.; Erasmus, J.J.; Kim, E.S.; Behrens, C.; Lee, J.J.; Roth, J.A.; Stewart, D.J.; et al. Histopathologic Response Criteria Predict Survival of Patients with Resected Lung Cancer After Neoadjuvant Chemotherapy. J. Thorac. Oncol. 2012, 7, 825–832. [CrossRef]
- Cottrell, T.; Thompson, E.; Forde, P.; Stein, J.; Duffield, A.; Anagnostou, V.; Rekhtman, N.; Anders, R.; Cuda, J.; Illei, P.; et al. Pathologic features of response to neoadjuvant anti-PD-1 in resected non-small-cell lung carcinoma: a proposal for quantitative immune-related pathologic response criteria (irPRC). Ann. Oncol. 2018, 29, 1853–1860. [CrossRef]
- Travis, W.D.; Dacic, S.; Wistuba, I.; Sholl, L.; Adusumilli, P.; Bubendorf, L.; Bunn, P.; Cascone, T.; Chaft, J.; Chen, G.; et al. IASLC Multidisciplinary Recommendations for Pathologic Assessment of Lung Cancer Resection Specimens After Neoadjuvant Therapy. J. Thorac. Oncol. 2020, 15, 709–740. [CrossRef]
- Xu, L.; Si, H.; Zhuang, F.; Li, C.; Zhang, L.; Zhao, Y.; Chen, T.; Dong, Y.; Wang, T.; Hou, L.; et al. Predicting therapeutic response to neoadjuvant immunotherapy based on an integration model in resectable stage IIIA (N2) non–small cell lung cancer. J. Thorac. Cardiovasc. Surg. 2024, 169, 242–253.e4. [CrossRef]
- Yue, D.; Liu, W.; Chen, C.; Zhang, T.; Ma, Y.; Cui, L.; Gu, Y.; Bei, T.; Zhao, X.; Zhang, B.; et al. Circulating tumor DNA predicts neoadjuvant immunotherapy efficacy and recurrence-free survival in surgical non-small cell lung cancer patients. Transl. Lung Cancer Res. 2022, 11, 263–276. [CrossRef]
- Deutsch, J.S.; Cimino-Mathews, A.; Thompson, E.; Provencio, M.; Forde, P.M.; Spicer, J.; Girard, N.; Wang, D.; Anders, R.A.; Gabrielson, E.; et al. Association between pathologic response and survival after neoadjuvant therapy in lung cancer. Nat. Med. 2023, 30, 218–228. [CrossRef]
- Zhao, J.; Zhao, L.; Guo, W.; Wang, S.; Tao, X.; Li, L.; Mao, Y.; Tan, F.; Gao, Y.; Wu, N.; et al. Efficacy, Safety, and Biomarker Analysis of Neoadjuvant Camrelizumab and Apatinib in Patients With Resectable NSCLC: A Phase 2 Clinical Trial. J. Thorac. Oncol. 2023, 18, 780–791. [CrossRef]
- Dong, S.; Yang, X.-N.; Liao, R.-Q.; Jiang, B.-Y.; Wang, Q.; Ben, X.-S.; Qiao, G.-B.; Lin, J.-T.; Yan, H.-H.; Yan, L.-X.; et al. Neoadjuvant nivolumab with or without platinum-doublet chemotherapy based on PD-L1 expression in resectable NSCLC (CTONG1804): a multicenter open-label phase II study. Signal Transduct. Target. Ther. 2023, 8, 1–10. [CrossRef]
- Provencio, M.; Serna-Blasco, R.; Nadal, E.; Insa, A.; García-Campelo, M.R.; Rubio, J.C.; Dómine, M.; Majem, M.; Rodríguez-Abreu, D.; Martínez-Martí, A.; et al. Overall Survival and Biomarker Analysis of Neoadjuvant Nivolumab Plus Chemotherapy in Operable Stage IIIA Non–Small-Cell Lung Cancer (NADIM phase II trial). J. Clin. Oncol. 2022, 40, 2924–2933. [CrossRef]
- Abbosh, C.; Frankell, A.M.; Harrison, T.; Kisistok, J.; Garnett, A.; Johnson, L.; Veeriah, S.; Moreau, M.; Chesh, A.; Chaunzwa, T.L.; et al. Tracking early lung cancer metastatic dissemination in TRACERx using ctDNA. Nature 2023, 616, 553–562. [CrossRef]
Figure 1.
Flowchart of the selection of articles. From the 51 initially identified articles, 45 were excluded because of the reasons summarized in the figure. The 6 remaining articles were selected for the final review. Furthermore, 4 presentations were added from ASCO 2025 and ELCC 2025. The total 10 studies were summarized in this review. One ASCO presentation was replaced with the concurrent publication in The New England Journal of Medicine in 2025 [34].
Figure 1.
Flowchart of the selection of articles. From the 51 initially identified articles, 45 were excluded because of the reasons summarized in the figure. The 6 remaining articles were selected for the final review. Furthermore, 4 presentations were added from ASCO 2025 and ELCC 2025. The total 10 studies were summarized in this review. One ASCO presentation was replaced with the concurrent publication in The New England Journal of Medicine in 2025 [34].
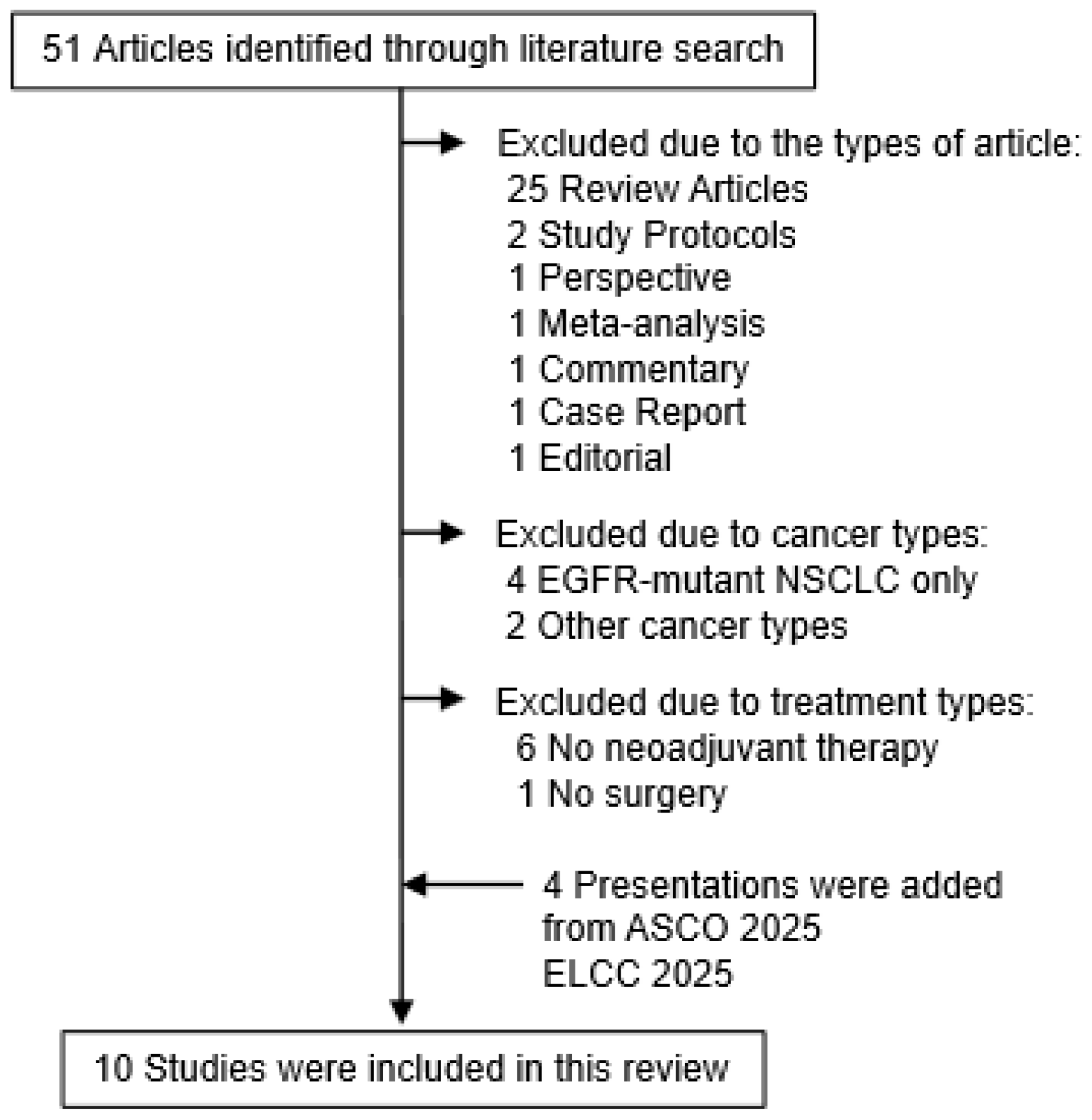
Figure 2.
Example of a patient with NSCLC who showed dramatic response to one course of neoadjuvant chemo-immunotherapy. (a) Chest X-ray before neoadjuvant treatment. (b) Chest X-ray after one course of neoadjuvant treatment.
Figure 2.
Example of a patient with NSCLC who showed dramatic response to one course of neoadjuvant chemo-immunotherapy. (a) Chest X-ray before neoadjuvant treatment. (b) Chest X-ray after one course of neoadjuvant treatment.
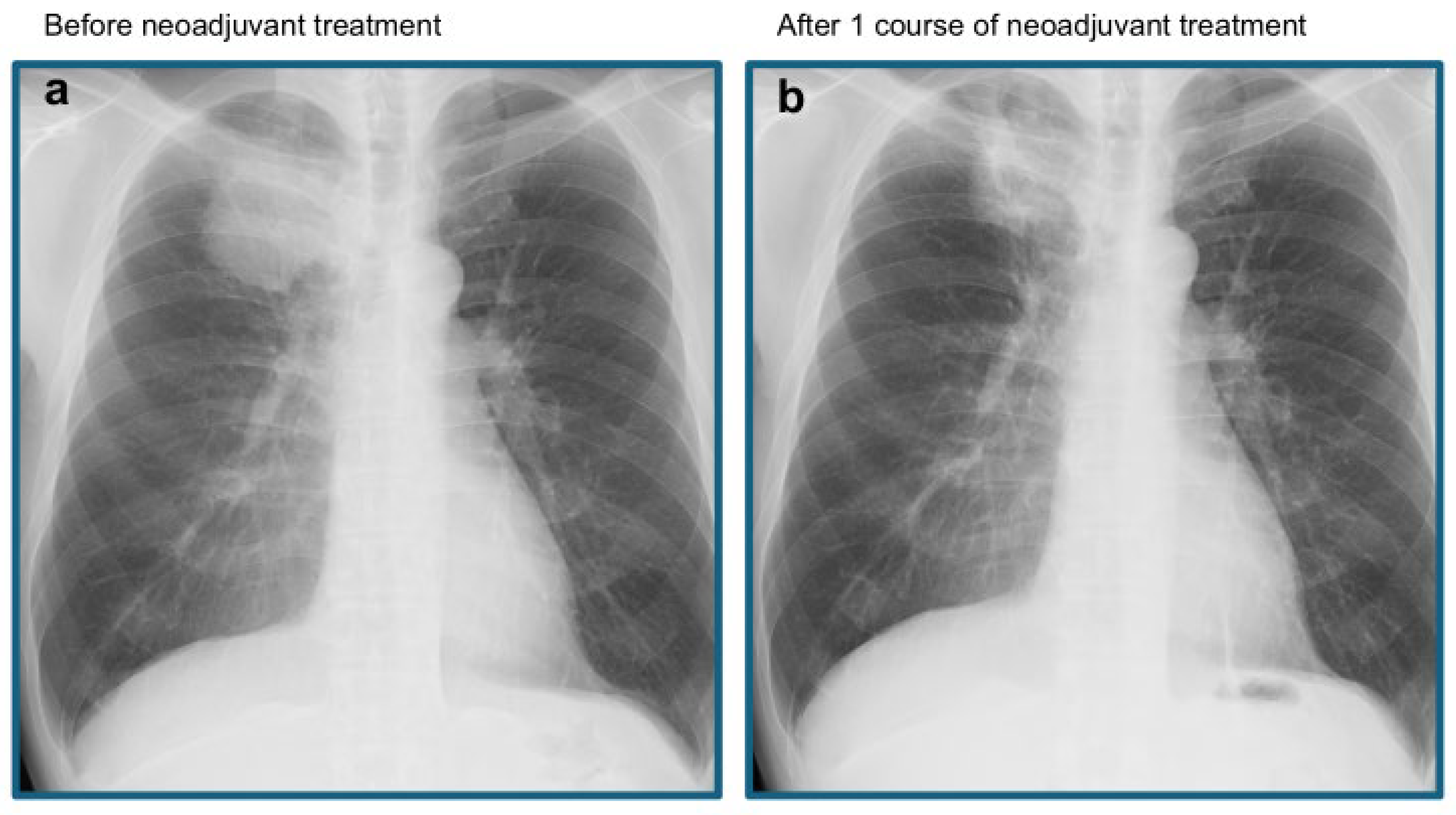
Figure 3.
Example of a patient with discordance between the radiologic response and pathological response to treatment. A 77-year-old female patient received neoadjuvant chemo-immunotherapy for clinical T2aN2M0 lung adenocarcinoma. (a–b) Chest CT (a) and FDG-PET/CT before treatment, and (c-d) chest CT (c) and FDG-PET/CR after two cycles of neoadjuvant chemo-immunotherapy treatment are shown. These radiological examinations suggested progressive disease; therefore, we decided to stop neoadjuvant treatment and performed pulmonary resection. (e) However, pathological examination of the resected tumor suggested partial efficacy of treatment rather than progressive disease.
Figure 3.
Example of a patient with discordance between the radiologic response and pathological response to treatment. A 77-year-old female patient received neoadjuvant chemo-immunotherapy for clinical T2aN2M0 lung adenocarcinoma. (a–b) Chest CT (a) and FDG-PET/CT before treatment, and (c-d) chest CT (c) and FDG-PET/CR after two cycles of neoadjuvant chemo-immunotherapy treatment are shown. These radiological examinations suggested progressive disease; therefore, we decided to stop neoadjuvant treatment and performed pulmonary resection. (e) However, pathological examination of the resected tumor suggested partial efficacy of treatment rather than progressive disease.
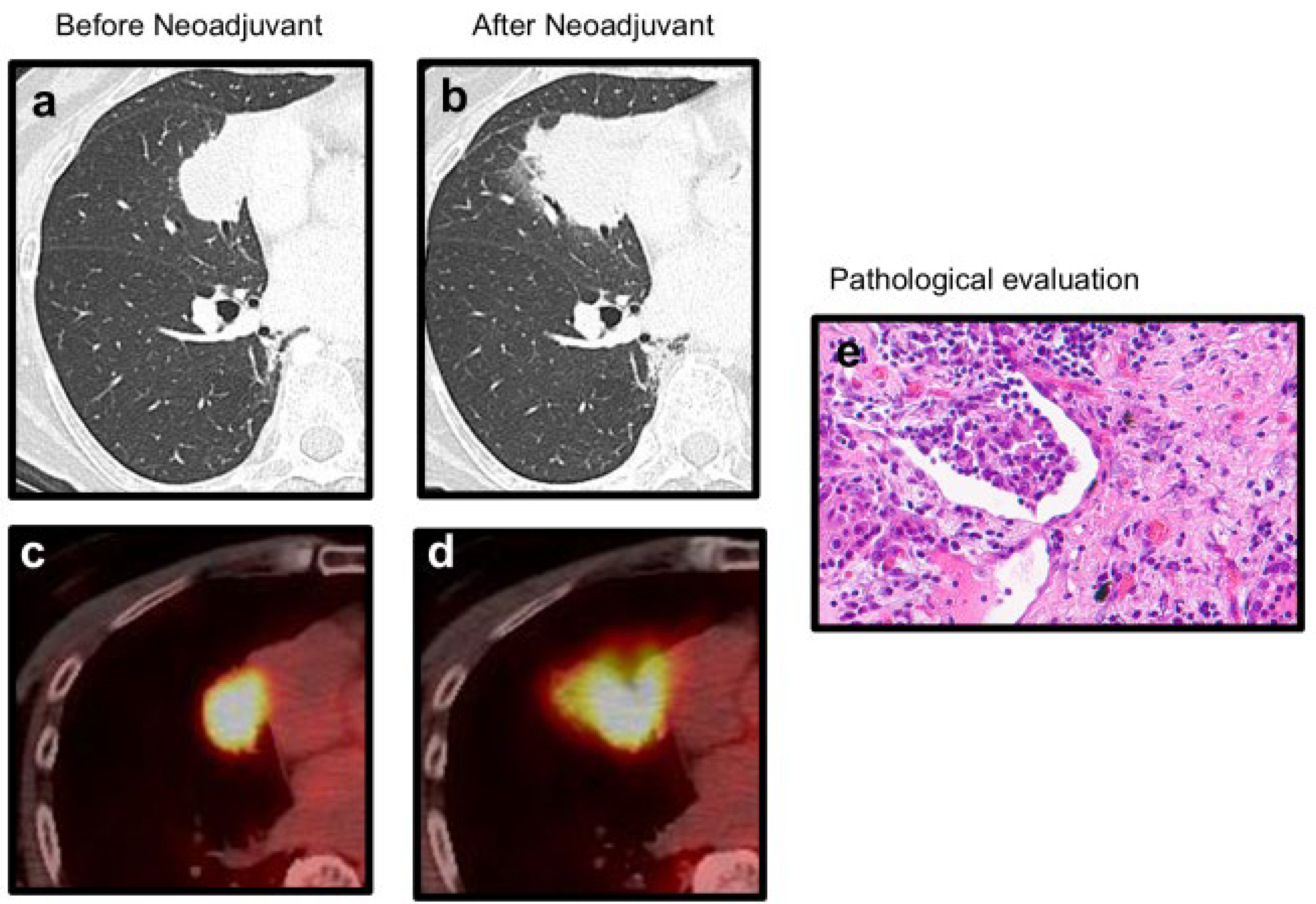
Figure 4.
Utility of ctDNA analysis at various time points for patients with NSCLC treated with perioperative chemo-immunotherapy.
Figure 4.
Utility of ctDNA analysis at various time points for patients with NSCLC treated with perioperative chemo-immunotherapy.
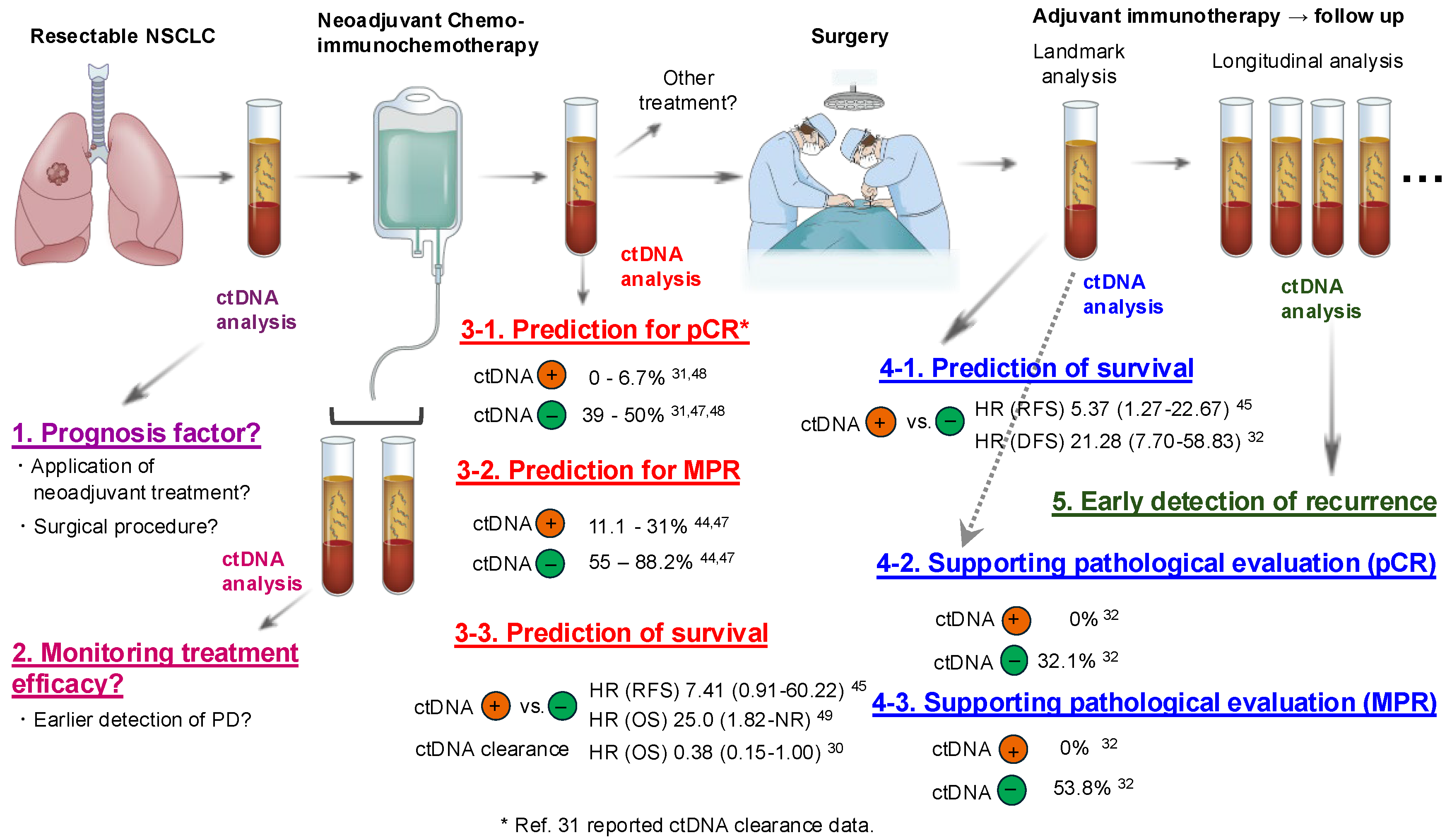

Table 1.
Summary of the clinical studies included in this review.
| Ref. # | Year | N | Neoadjuvant regimen | Adjuvant regimen |
| 45 | 2022 | 22 | ICI + CTx vs. ICI combo vs. CTx | - |
| 49 | 2022 | 46 | Nivo + CTx | Nivo vs. placebo |
| 46 | 2023 | 358 | Nivo + CTx vs. CTx | - |
| 48 | 2023 | 52 | Nivo + CTx vs. Nivo | - |
| 47 | 2023 | 78 | Camrelizumab + apatinib | - |
| 44 | 2025 | 45 | Sintilimab + CTx | - |
| 30 | 2025 | 358 | Nivo + CTx vs. CTx | - |
| 31 | 2025 | 461 | Nivo + CTx vs. CTx | Nivo vs. placebo |
| 32 | 2025 | 802 | Durval + CTx vs. CTx | Durval vs. placebo |
| 33 | 2025 | 86 | Nivo + CTx vs. CTx | Nivo vs. placebo |
Abbreviations: Ref: reference, ICI: Immune checkpoint inhibitor, CTx: Chemotherapy, Nivo: nivolumab, Durval: durvalmab.
Table 2.
ctDNA application in ongoing NSCLC neoadjuvant clinical studies.
| NCT # | Primary endpoints | Secondary endpoints | Exploratory analysis |
| NCT04638582 | ctDNA clearance (pre/post-surgery) |
MPR, pCR, radiologic response |
Correlation of ctDNA dynamics with DFS/OS |
| NCT05382052 | Association of ctDNA clearance with PFS |
DFS, OS | Longitudinal ctDNA monitoring feasibility |
| NCT05778253 | ctDNA clearance, AI-based prediction of pCR | MPR, ORR, DFS, OS, QoL, surgical outcomes | Correlation of AI pathology with clinical outcomes |
| NCT06111807 | Sensitivity/specificity of ctDNA assays | Association of ctDNA with recurrence/DFS | ctDNA-guided risk stratification |
| NCT06123754 | MPR (pre-op), EFS (post-op) |
pCR, DFS, OS, safety | Biomarker analysis, ctDNA dynamics |
| NCT06221462 | pCR/MPR, safety, surgical feasibility |
DFS, OS, AEs | ctDNA clearance, radiologic-pathologic correlation |
| NCT06284317 | DFS in non-pCR patients | DFS/OS in pCR group, safety, ctDNA analysis | Correlation of ctDNA with recurrence and survival |
| NCT06743555 | Feasibility and safety of surgery omission |
EFS, OS, recurrence rate | ctDNA monitoring for recurrence detection |
| NCT06902272 | Correlation between ctDNA and pCR/MPR |
DFS, OS, ctDNA kinetics | ctDNA MRD detection, longitudinal profiling |
| NCT06977074 | pCR, MPR, surgical eligibility |
DFS, OS, AEs | ctDNA-guided treatment optimization |
Abbreviations: ctDNA: circulating tumor DNA, pCR: pathological complete response, MPR: major pathological response, DFS: disease-free survival, OS: overall survival, EFS: event-free survival, PFS: progression-free survival, ORR: objective response rate, QoL: quality of life, AEs: adverse events, AI: artificial intelligence.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



