Submitted:
30 July 2025
Posted:
30 July 2025
You are already at the latest version
Abstract
Men with high-risk localized prostate cancer (PCa) often experience unfavorable long-term outcomes, highlighting the need for improved neoadjuvant strategies beyond the current standard of care. Radioligand therapy with 177Lutetium-PSMA-617 (177Lu-PSMA-617) has emerged as a promising method to eliminate occult micrometastases while enhancing immune-mediated clearance of the primary tumor. Initial trials have affirmed the treatment's feasibility and safety, yet they consistently report a lack of pathologic complete responses.
This absence of profound initial tumor reduction necessitates further therapeutic advancements. The underlying rationale for future strategies is clear, as 177Lu-PSMA-617 promotes immunogenic cell death, potentially sensitizing immunologically "cold" tumors to checkpoint inhibitors. However, caution is warranted. The synergy observed between these therapies in advanced, metastatic castration-resistant PCa arises from a distinctly different biological context, and similar outcomes cannot be assumed in treatment-naïve, localized disease without dedicated validation.
Continued progress hinges on developing improved metrics for success and patient selection. Simple PSA reductions have shown minimal correlation with significant pathologic outcomes in this setting, underscoring the critical need for validated surrogate endpoints and predictive biomarkers. Ultimately, large-scale randomized trials are essential to determine whether this investigational approach impacts key clinical outcomes—namely, metastasis-free and overall survival. While the strategy is theoretically sound, its capacity to enhance cure rates for high-risk localized PCa remains an unverified proposition.
Keywords:
high-risk localized prostate cancer
; immunogenic cell death
; Lutetium-177
; neoadjuvant radioligand therapy
; PSMA
; radioimmunotherapy
; tumor immune microenvironment
1. Introduction
Prostate cancer (PCa) persists as the most prevalent non-dermatological malignancy among males and constitutes a significant factor in cancer-related mortality on a global scale [1]. In the year 2024, it is projected that approximately 299,010 novel cases will be identified in the United States, accompanied by an estimated 35,250 fatalities [1]. While the bulk of males get identified with localized disease that tend to be slow and treatable, a considerable fraction shows high-risk features that point to aggressive clinical patterns, metastatic developments, and ultimately, death related to the condition. In cases of high-risk localized PCa, standard localized therapies, while administered with the aim of curing, often do not meet the necessary standards for effective disease control [2].
This therapeutic limitation has engendered an acute and unmet clinical need for innovative strategies that can address the systemic characteristics of high-risk localized PCa from the initial stages. The elevated rates of disease recurrence following even optimally administered local therapies strongly imply that, in numerous instances, high-risk localized PCa is not merely a localized condition but rather an early systemic disease with latent micrometastases already present at the time of diagnosis [1]. This insight reframes the core therapeutic dilemma. The predicament we are dealing with is not fundamentally a shortage of local treatment tactics, like radical prostatectomy (RP) or radiation therapy (RT), but rather a limitation in a conceptual framework that believes the disease is confined to the prostate gland. The focus, therefore, transitions from exclusively enhancing local control to attaining early and effective systemic management [3].
The integration of systemic therapies into the neoadjuvant landscape, preceding the final local treatment, represents an optimistic framework aimed at improving long-term prognoses for this sensitive patient demographic [4]. In the realm of innovative systemic therapies, the 177Lutetium-PSMA-617 (177Lu-PSMA-617) radioligand therapy (RLT) focusing on the prostate-specific membrane antigen (PSMA) has surfaced as a notably captivating option [5]. This model employs a 'theranostic' framework, promoting the accurate administration of radiation focused on tumor cells found within the biological system. This review will investigate the landscape of high-risk localized PCa, elucidate the rationale for a neoadjuvant strategy, delineate the mechanism and evidence supporting 177Lu-PSMA-617 RLT, and scrutinize the emerging clinical data, immunomodulatory potential, and prospective hurdles associated with advancing this potent therapeutic modality into the curative-intent framework.
2. Defining the High-Risk Patient and the Limits of Standard of Care
2.1. A Heterogeneous Definition: Comparing International Guidelines
The contemporary method for managing PCa relies significantly on assessing risks, a tactical approach that influences the diagnosis, chosen therapies, and the advice for ongoing assistance [6]. Three essential global institutions—the National Comprehensive Cancer Network (NCCN) situated in the United States, the European Association of Urology (EAU), and the American Urological Association (AUA)—in conjunction with the American Society for Radiation Oncology (ASTRO) and the Society of Urologic Oncology (SUO)—supply protocols that are based on evidence for this method. Although these guidelines converge on a foundational framework that incorporates serum prostate-specific antigen (PSA) levels, Gleason score stratified by Grade Group, and clinical T-stage, their particular delineations of high-risk disease manifest subtle yet critical divergences, which are encapsulated in Table 1.
The 2025 NCCN guidelines [7] have been updated to differentiate advanced localized disease into two notable segments: high-risk and very high-risk. A disease is labeled high-risk when it has one or more of the following features: a clinical stage of cT3-cT4, Grade Group 4 or 5, or a PSA level that is above 20 ng/mL. The NCCN further designates a very high-risk subgroup for patients with at least two of the following: a clinical stage of cT3-cT4, Grade Group 4 or 5, or a PSA greater than 40 ng/mL. This granular stratification acknowledges the notably poor prognosis allied with particularly advanced local tumors or a confluence of detrimental clinical attributes.
The 2025 EAU guidelines [8] define high-risk localized PCa as having at least two of the following: cT3-4, Gleason Score 8-10, or PSA ≥40 ng/mL. Very high-risk PCa includes node-positive disease or, if node-negative, meeting the high-risk criteria mentioned above. The 2025 AUA/ASTRO/SUO guideline (last updated 2022 and still current in 2025) [9] continues to use a three tier risk system and designates localized prostate cancer as high risk when any one of the following is present: clinical stage cT3a, Grade Group 4 or 5 (Gleason 8–10), or a PSA level > 20 ng/mL. Unlike the NCCN, it does not create a separate “very high risk” category; tumors with seminal vesicle invasion (cT3b), adjacent organ involvement (cT4), multiple high risk features, or pelvic node positivity are classified as locally advanced disease and managed with intensified multimodality treatment rather than being labeled very high risk localized cancer.
The nuanced distinctions among these preeminent guidelines, particularly the explicit very high-risk classification posited by the NCCN, illuminate an aspect of clinical ambiguity. This absence of a singular, universally standardized definition may obfuscate the interpretation and comparison of clinical trial outcomes and could engender discrepancies in patient management across disparate healthcare systems. Also, it reveals a pivotal concern: clinical assessments on their own could struggle to convey the extensive biological diversity that exists in aggressive PCa. This incongruity underscores the pressing necessity for more sophisticated prognostic instruments, such as molecular biomarkers or the pathological response to neoadjuvant therapy, to more accurately identify patients necessitating treatment intensification [10].
2.2. The Sobering Reality of Recurrence and Mortality
For men diagnosed with high-risk localized PCa, the standard of care involves definitive local therapy, typically RP with extended pelvic lymph node dissection or external beam radiotherapy (EBRT) combined with long-term androgen deprivation therapy (ADT) [9]. While these treatments can be curative for some, a substantial proportion of patients experience disease recurrence, highlighting the limitations of a purely local approach for a disease that is often systemic at presentation.
The statistics on treatment failure are sobering. Across various studies, between 27% and 53% of all patients undergoing RP or RT will eventually develop a rising PSA, a condition known as biochemical recurrence (BCR) [9]. For patients with the most adverse disease features, the risk of recurrence and subsequent metastasis can exceed 50% [11]. This high rate of failure strongly suggests that at the time of initial diagnosis and treatment, occult micrometastatic disease has already spread beyond the prostate and pelvic region, rendering local therapy alone insufficient for cure. This leads to significant long-term mortality. Even with aggressive local treatment, the 10-year prostate cancer-specific mortality (PCSM) for men in the D'Amico high-risk group treated with RP is approximately 7.4% [8]. Other large series report 10-year PCSM rates for high-grade disease (Gleason score 8-10) ranging from 7% to as high as 15% after surgery [12]. For patients with clinical T3 disease, 10-year cancer-specific survival is approximately 85%, meaning 15% of these men will have died from their cancer within a decade of treatment [13].
2.3. The Rationale for a Neoadjuvant Approach
The neoadjuvant strategy, which involves administering systemic therapy before definitive local treatment, is a well-established paradigm in other solid tumors, such as breast, esophageal, and rectal cancers [14]. Its application in high-risk localized PCa is based on several compelling theoretical advantages. The primary goal is the eradication of micrometastatic disease. By delivering a potent systemic agent before surgery or radiation, there is an opportunity to eliminate the disseminated tumor cells that are responsible for future relapse and mortality. This approach addresses the fundamental limitation of local-only therapy.
Second, the neoadjuvant setting provides a unique "window of opportunity" for an in vivo assessment of treatment sensitivity. This concept is perhaps best illustrated by the experience in breast cancer, where the response of the primary tumor to neoadjuvant chemotherapy offers a powerful real-time biomarker of therapeutic efficacy [15]. A profound pathologic response, particularly a pathologic complete response (pCR) defined as the absence of any residual invasive tumor in the surgical specimen, is a strong surrogate for improved long-term survival [16]. The ability to observe this response transforms the primary tumor from a liability to be removed into a "living laboratory" for assessing drug efficacy. A poor response could identify patients at very high risk who may benefit from immediate adjuvant therapy or enrollment in clinical trials of novel agents, while a strong response could justify de-escalation of further treatment. This real-time biological feedback is a powerful tool for personalizing therapy and accelerating drug development, a principle that has been adopted by regulatory bodies like the U.S. Food and Drug Administration for expediting drug approvals in breast cancer [17].
Third, neoadjuvant therapy can induce tumor downstaging. By shrinking the primary tumor and treating locoregional lymph node involvement, the therapy may increase the probability of achieving negative surgical margins—a key predictor of recurrence-free survival (RFS)—and potentially facilitate nerve-sparing techniques, thereby improving functional outcomes [18].
Finally, this approach provides an invaluable platform for translational research. Analysis of pre-treatment biopsy tissue and post-treatment surgical tissue allows investigators to study the biological effects of a novel therapy on the tumor and its microenvironment, accelerating the discovery of predictive biomarkers and elucidating mechanisms of response and resistance. It is within this framework of addressing micrometastatic disease and gaining crucial biological insights that neoadjuvant 177Lu-PSMA-617 RLT is being explored as a transformative strategy for high-risk localized PCa [19,20].
Figure 1 provides a clear visual summary contrasting the standard treatment pathway with the proposed neoadjuvant RLT strategy, illustrating the latter's aim to systemically target both the primary tumor and occult micrometastases prior to definitive local therapy.
3. The Theranostic Foundation: PSMA-Targeted Radioligand Therapy
The advent of PSMA-targeted RLT signifies a substantial progression in the therapeutic management of PCa [21]. This technique hinges on the 'theranostic' concept—integrating both therapeutic and diagnostic processes—using one specific molecular target for imaging and treatments, thus allowing for a uniquely customized application of radionuclide therapy. The success of 177Lu-PSMA-617 in the most advanced stages of the disease has provided a robust foundation for its investigation in earlier, curative-intent settings.
3.1. Mechanism of Action of 177Lu-PSMA-617
The therapeutic effectiveness of 177Lu-PSMA-617 is contingent upon the intricate interaction of its three fundamental components: the target, the ligand, and the radionuclide [22]. The target, PSMA, is a transmembrane glycoprotein that is found to be overproduced by nearly 1000 times on the surface of PCa cells when compared to benign prostate tissue [23]. Notably, the expression of PSMA tends to escalate with the progression of the disease, attaining particularly high levels in poorly differentiated, metastatic, and castration-resistant tumors, thereby rendering it an optimal target for intervention in aggressive disease states.
The ligand known as PSMA-617 is a uniquely crafted small molecule designed to show remarkable affinity and precision towards the extracellular enzymatic site of the PSMA protein. Once the PSMA-ligand complex connects, the cancer cell swiftly internalizes it, thus isolating the corresponding radionuclide inside. The agent 177Lu serves therapeutically, noted for its radioisotopic nature and the decay process that includes beta particle (β-particle) emission [24]. The β-particles that are released, known as electrons, indicate an average distance of 0.67 mm, with a peak travel distance nearly hitting 2 mm in soft tissues [25]. When these pieces journey through organic entities, they produce energy, damaging the cellular arrangement, particularly influencing DNA. The 177Lu radiation mainly causes single-strand DNA breaks, which could arrest the cell cycle and eventually lead to apoptosis if they are sufficiently numerous or left unrepaired [26]. The millimeter-scale path length of these β-particles engenders a beneficial "cross-fire" effect, whereby radiation emanating from a targeted cell can also compromise adjacent tumor cells that may exhibit lower or absent PSMA expression, thereby aiding in the mitigation of tumor heterogeneity.
This therapeutic agent is one half of a theranostic pair. For patient selection, the diagnostic agent PSMA 11 is marked radioactively with Gallium 68 (68Ga), creating 68Ga PSMA 11. Subsequent to intravenous administration, PET/CT imaging corroborates adequate PSMA expression in the lesions of the patient, suggesting a propensity for these lesions to uptake the therapeutic radioligand 177Lu-PSMA-617. This imaging-centered selection approach guarantees that treatment is exclusively provided to patients most likely to reap therapeutic rewards [27].
3.2. Pivotal Evidence from the Metastatic Setting
The journey of 177Lu-PSMA-617 into clinical practice was solidified by two landmark clinical trials that established its efficacy in the most advanced and difficult-to-treat setting: metastatic castration-resistant prostate cancer (mCRPC) that has progressed after both novel hormonal agents and taxane-based chemotherapy [28]. These studies provide a high level of evidence for the efficacy of 177Lu-PSMA-617 in this patient population.
The VISION trial (NCT03511664) was a global, randomized, phase 3 study that enrolled 831 men with PSMA-positive mCRPC [29]. Patients were randomized 2:1 to receive 177Lu-PSMA-617 plus standard of care or standard of care alone. The results were practice-changing. The addition of 177Lu-PSMA-617 led to a significant improvement in the trial's two primary endpoints. Radiographic progression-free survival (rPFS) was more than doubled, with a median of 8.7 months in the RLT arm compared to 3.4 months in the control arm, corresponding to a hazard ratio (HR) of 0.40 (95% CI, 0.29–0.57; p<0.001). More importantly, 177Lu-PSMA-617 conferred a significant overall survival (OS) benefit, extending the median OS from 11.3 months to 15.3 months (HR 0.62; 95% CI, 0.52–0.74; p<0.001).
The TheraP trial (NCT03392428), a randomized phase 2 study conducted in Australia, provided further compelling evidence [30]. This trial compared 177Lu-PSMA-617 directly against an active comparator, the chemotherapy agent cabazitaxel, in men with mCRPC who had progressed after docetaxel. Patients were rigorously selected using both PSMA-PET and FDG-PET to ensure high PSMA expression and exclude tumors with FDG-avid but PSMA-negative disease. The trial met its primary endpoint, demonstrating a significantly higher PSA response rate (a decline of ≥50%) for 177Lu-PSMA-617 compared to cabazitaxel (66% vs. 37%). The RLT also resulted in a longer PFS (HR 0.63; 95% CI, 0.46–0.86). With longer follow-up, the OS was similar between the two arms. This result was heavily confounded by the high rate of patients in the cabazitaxel arm who crossed over to receive 177Lu-PSMA-617 upon progression, complicating the interpretation of the survival endpoint but not diminishing the clear evidence of superior activity and lower toxicity for the radioligand therapy [30].
The robust and consistent efficacy demonstrated in these trials, conducted in a patient population with very limited options and poor prognosis, provided unequivocal proof of the agent's potent anti-tumor activity. This success in the end-stage, palliative setting serves as the primary justification for investigating its use in earlier disease states. The logical hypothesis is that if 177Lu-PSMA-617 is effective against highly resistant, widespread disease, it may be even more effective, and potentially curative, when applied to the lower-volume, less-treated micrometastatic disease characteristic of the high-risk localized PCa setting [31,32].
3.3. The Radiobiological Imperative: Beta- versus Alpha-Emitters
The therapeutic effect of any RLT is dictated by the physical properties of the radionuclide it carries [33]. Understanding these properties is crucial for appreciating the current state of the field and its future direction, which increasingly involves the exploration of different types of radiation emitters. The two main classes of particles used in RLT are β-particles and α-particles, which have fundamentally different radiobiological characteristics, as detailed in Table 2.
Beta-emitters, such as 177Lu, are electrons or positrons. They are characterized by a relatively low Linear Energy Transfer (LET), which is a measure of the energy deposited per unit of distance traveled through tissue. For β-particles, the LET is approximately 0.2 keV/µm [34]. Because of this low energy deposition density, hundreds or even thousands of β-particle tracks, or "hits," are required to pass through a cell's nucleus to induce lethal damage. However, their longer path length in tissue (up to several millimeters for some beta emitters) provides the valuable cross-fire effect, allowing them to treat larger tumors and overcome some degree of target antigen heterogeneity [35].
Alpha-emitters, such as Actinium-225 (225Ac)andRadium−223(223Ra), are helium nuclei (two protons and two neutrons). They are vastly different from β-particles. They possess a very high LET, around 100 keV/µm, which is approximately 500 times greater than that of β-particles [36]. This dense ionization track is incredibly damaging to biological molecules. An alpha particle (α-particle) can cause complex, irreparable double-strand DNA breaks, which are highly cytotoxic [37]. Consequently, as few as one to ten α-particle traversals through a cell nucleus can be sufficient to kill the cell [38]. This high potency is coupled with an extremely short range in tissue—typically less than 100 µm, or the span of just a few cell diameters [39]. This short range minimizes damage to nearby healthy tissues but also eliminates any significant cross-fire effect.
This distinction creates a strategic trade-off in the design of radiopharmaceuticals. There is no single "best" radionuclide; rather, the choice depends on the clinical objective [40]. For the neoadjuvant goal of debulking a macroscopic primary tumor, which is likely to be heterogeneous in its PSMA expression, the longer range and cross-fire effect of a beta-emitter like 177Lu are advantageous [41]. However, for the goal of eradicating disseminated single tumor cells or microscopic clusters of cells—the definition of micrometastatic disease or minimal residual disease (MRD)—the extreme potency and short range of an alpha-emitter may be theoretically superior, delivering a lethal dose to isolated targets while maximally sparing surrounding normal tissue [42]. This understanding frames the evolution of RLT from a single-agent approach to a more sophisticated, tailored strategy where the choice of radionuclide could be matched to the volume of disease and the specific therapeutic intent.
4. Emerging Evidence for Neoadjuvant 177Lu-PSMA Radioligand Therapy
The transition of 177Lu-PSMA RLT from the palliative metastatic setting to the curative-intent neoadjuvant setting is a recent but rapidly advancing field [49]. While large-scale phase 3 data are not yet available, a foundation of preclinical work and a series of pioneering early-phase clinical trials are beginning to provide the first insights into the safety, feasibility, and potential efficacy of this approach.
4.1. Preclinical Rationale and Early Human Experience
The foundational rationale for the application of 177Lu-PSMA agents in the treatment of prostate cancer was predicated on extensive preclinical investigations. In controlled studies employing cellular models that express PSMA, we confirmed the significant binding strength of various PSMA-targeting compounds. Subsequent research utilizing murine xenograft models of prostate cancer revealed a specific and substantial accumulation of radiolabeled PSMA ligands within tumors, resulting in significant, dose-dependent inhibition of tumor growth and the induction of DNA damage [50]. These assessments highlighted the key evidence needed to validate the delivery system for PSMA-targeted radionuclides. The first human applications of 177Lu-PSMA radioligand therapy were initiated through compassionate use efforts, primarily in Germany and Australia [5]. Although these preliminary experiences were not performed under the stringent protocols of a formal clinical trial, they yielded critical initial data indicating that the therapy was generally well-tolerated and capable of eliciting significant PSA responses and tumor regression in patients who had undergone extensive prior treatment. This empirical evidence from real-world scenarios was pivotal in generating momentum and providing the safety justification necessary for the initiation of prospective clinical trials, which ultimately culminated in the landmark VISION and TheraP studies.
4.2. Initial Clinical Trial Data: The LuTectomy Study
The current landscape of neoadjuvant RLT is defined by a small number of innovative, investigator-initiated trials. The LuTectomy trial (NCT04430192) is a single-arm, phase 1/2 study conducted in Australia, designed as a first-in-human evaluation of neoadjuvant 177Lu-PSMA-617 [51]. The trial enrolled 20 men with high-risk localized PCa or locoregionally advanced PCa who were scheduled for RP and pelvic lymph node dissection. A key inclusion criterion was high PSMA avidity on a screening 68Ga-PSMA PET/CT scan. Participants were administered a solitary intravenous infusion of roughly 5 GBq of 177Lu-PSMA-617 six weeks in advance of their scheduled surgical intervention .
The first results, announced at the 2023 European Association of Urology yearly meeting, have delivered the pioneering prospective information concerning this method [52]. About safety, the treatment intervention was found to reflect a notable degree of tolerability. The characteristics of negative effects were in line with those noted in the metastatic setting, featuring mild xerostomia, temporary nausea, and fatigue as the chief toxicities. The surgeons affirmed that the RP performed afterward was both safe and uncomplicated, reporting no unforeseen intraoperative difficulties or escalated complications tied to the earlier RT. This represents a pivotal discovery, as it confirms the essential viability of the neoadjuvant RLT in conjunction with surgical intervention.
The primary endpoint of dosimetry confirmed that the therapy delivers a high and targeted radiation dose to the sites of disease. The median absorbed dose to the prostate was 19.6 Gy, and even higher to involved pelvic lymph nodes, at 37.9 Gy. While these doses are substantial, they are lower than the curative doses delivered with external beam radiation therapy (typically >70 Gy), and there was significant variability in dose delivery among patients.
The preliminary efficacy data were encouraging. The single cycle of RLT induced a median PSA decline of 49%, with 45% of patients achieving a PSA50 response (a decline of ≥50%). On post-treatment PSMA PET scans, 55% of patients had a partial response, defined as a decline in SUVmax of >30%, while 40% had stable disease. At a median follow-up of nearly 14 months, the biochemical RFS rate was 80%.
However, it was the most pivotal findings that arose from examining the prostatectomy specimens. A significant 80% of the subjects exhibited indications of a partial histologic response, which included aspects like stromal fibrosis, diminished tumor cell density, and cytoplasmic vacuolation, yet not a single patient in the trial accomplished a pathologic complete response (pCR). One individual (5%) was identified as possessing only MRD. This outcome, while indicating a distinct biological activity, holds considerable significance. It strongly implies that a solitary cycle of 177Lu-PSMA-617 monotherapy is inadequate for the complete eradication of macroscopic, high-risk PCa localized within the prostate. This 'negative' result is not indicative of a trial failure but is instead a valuable, hypothesis-generating insight. It delineates the lower threshold of efficacy for this therapeutic approach and offers a compelling rationale for the development of strategies designed to enhance the anti-tumor effect, such as the utilization of multiple RLT cycles, dose escalation, or integrative treatment modalities [51,53].
4.3. The Next Frontier in Trial Design: An Overview of Ongoing Studies
The findings from LuTectomy have directly informed the design of the next wave of clinical trials, which seek to build upon its initial observations. These studies, summarized in Table 3, represent the logical evolution of the research agenda in this space.
The NEPI trial (EudraCT 2021-004894-30) is a randomized phase 1/2 study being conducted in Germany, targeting patients with very high-risk PCa [54]. This trial takes the next logical step by evaluating a combination therapy strategy. It is designed as a direct response to the LuTectomy finding that monotherapy is insufficient for pCR. Patients are randomized to receive 12 weeks of neoadjuvant therapy consisting of ADT plus two cycles of 177Lu-PSMA-617, either with or without the addition of ipilimumab, an immune checkpoint inhibitor (ICI) that blocks CTLA-4. The co-primary endpoints are the feasibility of performing RP after this intensive neoadjuvant regimen and, critically, the rate of pCR.
While not a neoadjuvant trial in the strictest sense, the PSMA-DC trial is also highly relevant as it represents a move of RLT into an earlier, potentially curative disease space [55]. This international phase 3 trial is evaluating 177Lu-PSMA-617 versus observation in patients who have developed oligometastatic recurrence after initial definitive local therapy. The primary endpoint is metastasis-free survival (MFS). This study will provide valuable data on the ability of RLT to control low-volume metastatic disease and delay the need for systemic hormonal therapy, offering insights that are applicable to the goal of eradicating micrometastases in the neoadjuvant setting.
5. The Immunomodulatory Potential of Neoadjuvant Radioligand Therapy
Beyond direct cytotoxicity, RLT is shown to influence the tumor microenvironment and elicit systemic immune responses. This "in situ vaccine" effect suggests that targeted tumor cell destruction can transform non-responsive tumors into ones that the immune system actively targets. This effect that modulates immunity encourages the merging of RLT alongside immunotherapy [56].
5.1. Inducing an In Situ Vaccine Effect
Radiation, including radionuclide delivery, induces immunogenic cell death (ICD), which activates the immune response [57]. Unlike regular apoptosis, ICD signals the immune system regarding dying tumor cells. Notable aspects of ICD involve the emergence of Damage-Associated Molecular Patterns (DAMPs). Cardinal DAMPs in ICD involve calreticulin (CRT) translocation as an "eat me" signal for phagocytosis by dendritic cells (DCs) [58]. In addition, dying cells produce ATP, acting as a signal to draw DCs towards the tumor region [59]. Ultimately, the release of HMGB1 encourages the maturation process of DCs and the showcasing of tumor antigens to T-cells.
Dendritic cell activation within the tumor area can profoundly impact the local microenvironment and promote a widespread anti-tumor T-cell response. Mature DCs engage with naive T-cells in the lymph nodes by presenting tumor-associated antigens, thus priming cytotoxic CD8+ T-cells that are specific to the tumor. Activated T-cells can then journey back to the primary tumor and remote metastases to eliminate any lingering cancer cells. The concept of an in situ vaccine, where the treated tumor provides antigens for vaccination, is a primary objective in combining radiation with immunotherapy [56].
Figure 2 illustrates the detailed mechanistic cascade initiated by RLT, showing how targeted tumor destruction leads to immunogenic cell death, antigen presentation by dendritic cells, and the subsequent activation and trafficking of cytotoxic T cells to enact a systemic anti-tumor response.
5.2. A Hypothesis-Generating Biomarker: The PD-L2 Signature
Identifying which patients are most likely to mount an effective immune response to RLT is a critical step toward personalizing therapy. Recent research has uncovered promising biomarkers rooted in the interferon-gamma (IFN-γ) signaling pathway. A recent and potentially paradigm-shifting exploratory study analyzed the tumor immune microenvironment of patients with mCRPC undergoing 177Lu-PSMA-617 therapy [57,60]. The investigators correlated baseline tumor gene expression signatures from archival primary tumor tissue with clinical outcomes. The analysis revealed that a higher baseline expression signature for Programmed Death-Ligand 2 (PD-L2) was strongly and significantly associated with a better response to RLT [57]. Patients with a high PD-L2 signature had a much longer median overall survival compared to those with a low signature (17.2 months vs. 5.7 months), with a HR of 0.46. Furthermore, higher PD-L2 expression correlated with a greater PSA decline. Remarkably, the expression of the more widely studied immune checkpoint, PD-L1, showed no significant association with outcome.
It is critical to frame this finding with appropriate caution. This was a single-center, retrospective, exploratory analysis with a very small sample size for the transcriptomic analysis (n=23) and a long interval between biopsy and RLT. As such, these results are hypothesis-generating and require rigorous validation in larger, prospective cohorts before they can be considered for clinical use.
Nonetheless, the finding has profound implications. The discovery that the PD-L2 signature may be the dominant predictor of response to RLT suggests that radionuclide therapy could induce a distinct immunological phenotype within the tumor microenvironment, one that relies on a different axis of immune regulation than that targeted by most current immunotherapies [61-63]. This challenges the default assumption that anti-PD-1/L1 agents are the automatic choice for combination with RLT and provides a strong biological rationale for designing future clinical trials that incorporate agents targeting the PD-L2 pathway or other immune axes, such as the CTLA-4 pathway targeted by ipilimumab in the NEPI trial.
6. Optimizing Efficacy: Combination Strategies and Sequencing
The inadequacy of neoadjuvant 177Lu-PSMA-617 monotherapy for achieving high pCR rates has prompted the investigation of combinatorial approaches. By integrating RLT with agents exhibiting complementary mechanisms, synergistic anti-tumor effects and resistance mitigation may be attainable [56].
6.1. Synergy with Immunotherapy
The integration of RLT with ICIs represents a highly promising investigational strategy. The biological reasoning is solid: RLT operates as an 'in situ vaccine,' causing ICD, discharging tumor antigens, and prompting a T-cell response [56,64]. However, the activated T-cell response frequently encounters quick suppression by immune checkpoint pathways found in the tumor microenvironment. CTLA-4 inhibitors like ipilimumab and PD-1/PD-L1 inhibitors, part of the ICIs group, strive to 'remove the brakes' on T-cells, avoiding exhaustion and enhancing a more efficient and sustained systemic anti-cancer response. The NEPI trial, which assesses the combination of 177Lu-PSMA-617 and ipilimumab, is the inaugural clinical evaluation of this hypothesis in the neoadjuvant context for PCa [54].
6.2. Interplay with PARP Inhibitors: Evidence of Cross-Resistance
Poly(ADP-ribose) polymerase (PARP) inhibitors (PARPi) are another class of highly effective agents for a subset of men with mCRPC, specifically those whose tumors harbor mutations in DNA damage repair (DDR) genes, such as BRCA2 [65]. Since both RLT (via radiation) and PARPi (via enzymatic inhibition) ultimately exert their cytotoxic effects by inducing lethal DNA damage, there is a strong biological basis for both potential synergy and cross-resistance [66].
The question of how to best sequence these two potent therapies is a critical and unresolved clinical issue. A recent, important retrospective study investigated this question by comparing outcomes with 177Lu-PSMA-617 in men with DDR-mutated mCRPC who had either previously received a PARPi or were PARPi-naïve [67]. The results were notable. Prior exposure to a PARPi was associated with significantly worse outcomes on subsequent 177Lu-PSMA-617. This effect was most pronounced in the subgroup of patients with BRCA2 mutations. In this group, PARPi-naïve patients had a median PSA PFS of 14.0 months, compared to just 2.9 months for those who had previously been treated with a PARPi. The PSA50 response rate was also dramatically lower in the PARPi-exposed group (35% vs. 89%).
This clinical evidence strongly suggests the development of acquired cross-resistance. Treatment with a PARPi appears to exert a powerful selective pressure, enriching the tumor with clones that have developed mechanisms to more efficiently repair DNA damage. These same clones are then, in turn, resistant to the DNA damage induced by radiation from 177Lu-PSMA-617. This creates a crucial clinical dilemma: in a patient eligible for both therapies, which one should be used first? Using the PARPi first might effectively "burn the bridge" for RLT. This finding has immediate clinical implications for the sequencing of therapies in mCRPC and raises urgent questions for future research, including whether prior RLT induces resistance to subsequent PARPi therapy. Answering this will require prospective, randomized sequencing trials and will be essential for designing future neoadjuvant combination trials, as a significant proportion of men with high-risk localized PCa harbor germline DDR mutations [68].
6.3. Modulating the Target: The "PSMA Flare" Phenomenon
A third and highly sophisticated strategy for enhancing RLT efficacy involves manipulating the expression of the target itself. PSMA expression on the surface of PCa cells is not static; it is dynamically regulated by the androgen receptor (AR) signaling pathway. Paradoxically, inhibiting the AR with ADT or potent AR pathway inhibitors (ARPIs) such as enzalutamide has been shown to cause a transient upregulation of PSMA gene and protein expression [69,70].
This phenomenon, termed the "PSMA flare," has been demonstrated in both preclinical xenograft models and in clinical imaging studies [70]. In one notable case report, a patient with castration-sensitive PCa underwent a PSMA PET scan before and four weeks after starting ADT. The post-ADT scan revealed a 7-fold increase in PSMA uptake in known lesions, and, remarkably, 13 new metastatic lesions became visible on the scan that were not detected at baseline [71]. More recent work has shown that a short course of enzalutamide (9-14 days) can induce a significant increase (≥20%) in the SUVmax of existing tumor lesions in 56% of cases [69]. This biological insight transforms PSMA from a passive biomarker into a therapeutically modifiable target. It raises the possibility of using a short course of an ARPI to intentionally induce a PSMA flare immediately prior to PSMA-targeted therapy. This could theoretically increase the absorbed radiation dose delivered to tumors, improve the visualization of low-volume disease on diagnostic scans, and potentially convert patients with initially low PSMA expression into eligible candidates for RLT. Clinical trials are now underway to formally test this hypothesis.
8. Conclusion and Future Directions
8.1. Summary of the Potential for Neoadjuvant RLT to Reshape the Treatment Paradigm
Neoadjuvant 177Lu-PSMA-617 RLT represents a potential paradigm shift in the management of high-risk localized PCa. It challenges the traditional approach of relying solely on local therapies for a disease that is frequently systemic from its inception. By delivering a potent, targeted systemic therapy prior to definitive local treatment, this strategy offers the multifaceted potential to eradicate occult micrometastases, provide an in vivo readout of treatment sensitivity through pathological response, and prime a systemic anti-tumor immune response. The early data from trials like LuTectomy are encouraging, demonstrating that the approach is safe, feasible, and biologically active. While monotherapy appears insufficient to achieve complete tumor eradication, these initial findings have paved the way for more advanced combination strategies that hold the promise of significantly improving cure rates for men with the most aggressive forms of localized PCa.
8.2. Key Unanswered Questions and the Roadmap for Future Research
Despite the vast possibilities, the area of neoadjuvant RLT is still developing, and numerous critical questions remain. Future research must clarify these ambiguities through a series of meticulously designed, prospective trials.
First, the the optimal regimen for neoadjuvant RLT needs to be defined. This means investigating the most effective dosage, the treatment interval count, and the timing of administration tied to the surgical intervention. The LuTectomy trial implemented a singular cycle, whereas the NEPI trial is examining a two-cycle regimen, and subsequent studies may delve into further intensification strategies.
Second, the central question of whether a meaningful rate of pCR can be achieved should be addressed. This will likely necessitate transcending monotherapy approaches. The results of the NEPI research, melding RLT with immune treatment techniques, will signify an important preliminary progression. Future investigations should assess alternative combinations, such as those involving PARPi in patients with DDR mutations, or the incorporation of more efficacious alpha-emitting radionuclides like 225Ac-PSMA.
Third, establishing the optimal sequencing of RLT with other potent systemic agents, particularly PARPi, is essential. The preliminary evidence indicating cross-resistance underscores the pressing necessity for randomized trials to ascertain whether RLT should precede or follow PARPi in suitable patient populations to optimize cumulative therapeutic benefits.
Fourth, the role of biomarkers in personalizing neoadjuvant RLT needs to be solidified. This includes the validation of PSMA PET imaging parameters to forecast therapeutic response, the confirmation of the predictive value of immune signatures such as PD-L2 to appropriately select candidates for immunotherapeutic combinations, and the development of ctDNA-based MRD assays to inform post-operative adjuvant treatment decisions.
Finally, the long-term safety and quality-of-life impacts of neoadjuvant RLT in a curative-intent population should be carefully evaluated. While the immediate toxicity may be well-regulated, comprehensive long-term tracking is important to catch any delayed effects, especially concerning kidney and bone marrow function, particularly as more potent alpha-emitters are introduced.
In conclusion, neoadjuvant 177Lu-PSMA-617 RLT is one of the most exciting new frontiers in the treatment of high-risk localized PCa. It offers a scientifically robust strategy to address the fundamental challenge of micrometastatic disease. While the path to establishing this approach as a new standard of care is long and will require rigorous investigation, the potential to substantially increase the cure rate for these high-risk patients makes it a journey of paramount importance for the field of oncology. The success of this endeavor will hinge on the execution of well-designed, prospective, randomized clinical trials that leverage validated surrogate endpoints like MFS to deliver clear answers in a clinically relevant timeframe.
Author Contributions
Conceptualization, W.-A.K. and J.Y.J.; writing—original draft preparation, W.-A.K.; writing—review and editing, W.-A.K. and J.Y.J.; supervision, J.Y.J.; All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by grants from the National Cancer Center (No 2211880-3, and No 1941760-1).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Schaeffer, E.M.; Srinivas, S.; Adra, N.; An, Y.; Bitting, R.; Chapin, B.; Cheng, H.H.; D’Amico, A.V.; Desai, N.; Dorff, T.; et al. NCCN Guidelines® Insights: Prostate Cancer, Version 3.2024: Featured Updates to the NCCN Guidelines. Journal of the National Comprehensive Cancer Network 2024, 22, 140–150. [Google Scholar] [CrossRef]
- Berenguer, C.V.; Pereira, F.; Câmara, J.S.; Pereira, J.A.M. Underlying Features of Prostate Cancer-Statistics, Risk Factors, and Emerging Methods for Its Diagnosis. Curr Oncol 2023, 30, 2300–2321. [Google Scholar] [CrossRef] [PubMed]
- Gómez Rivas, J.; Ortega Polledo, L.E.; De La Parra Sánchez, I.; Gutiérrez Hidalgo, B.; Martín Monterrubio, J.; Marugán Álvarez, M.J.; Somani, B.K.; Enikeev, D.; Puente Vázquez, J.; Sanmamed Salgado, N. Current Status of Neoadjuvant Treatment Before Surgery in High-Risk Localized Prostate Cancer. Cancers 2024, 17, 99. [Google Scholar] [CrossRef] [PubMed]
- Kagawa, Y.; Smith, J.J.; Fokas, E.; Watanabe, J.; Cercek, A.; Greten, F.R.; Bando, H.; Shi, Q.; Garcia-Aguilar, J.; Romesser, P.B. Future direction of total neoadjuvant therapy for locally advanced rectal cancer. Nature Reviews Gastroenterology & Hepatology 2024, 21, 444–455. [Google Scholar] [CrossRef]
- Sallam, M.; Nguyen, N.T.; Sainsbury, F.; Kimizuka, N.; Muyldermans, S.; Benešová-Schäfer, M. PSMA-targeted radiotheranostics in modern nuclear medicine: then, now, and what of the future? Theranostics 2024, 14, 3043–3079. [Google Scholar] [CrossRef] [PubMed]
- Sekhoacha, M.; Riet, K.; Motloung, P.; Gumenku, L.; Adegoke, A.; Mashele, S. Prostate cancer review: genetics, diagnosis, treatment options, and alternative approaches. Molecules 2022, 27, 5730. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines®): Prostate Cancer Version 2.2025. Available online: https://www.nccn.org (accessed on 27 July 2025).
- EAU-EANM-ESTRO-ESUR-ISUP-SIOG Guidelines Panel on Prostate Cancer. EAU Guidelines on Prostate Cancer [Internet]. Arnhem, The Netherlands: EAU Guidelines Office; 2025 [cited 2025 Jul 26]. Available from: https://uroweb.org/guidelines/prostate-cancer.
- Eastham, J.A.; Auffenberg, G.B.; Barocas, D.A.; Chou, R.; Crispino, T.; Davis, J.W.; Eggener, S.; Horwitz, E.M.; Kane, C.J.; Kirkby, E. Clinically localized prostate cancer: AUA/ASTRO guideline, part I: introduction, risk assessment, staging, and risk-based management. The Journal of urology 2022, 208, 10–18. [Google Scholar] [CrossRef]
- Crocetto, F.; Musone, M.; Chianese, S.; Conforti, P.; Digitale Selvaggio, G.; Caputo, V.F.; Falabella, R.; Del Giudice, F.; Giulioni, C.; Cafarelli, A.; et al. Blood and urine-based biomarkers in prostate cancer: Current advances, clinical applications, and future directions. J Liq Biopsy 2025, 9, 100305. [Google Scholar] [CrossRef]
- Bhargava, P.; Ravizzini, G.; Chapin, B.F.; Kundra, V. Imaging Biochemical Recurrence After Prostatectomy: Where Are We Headed? American Journal of Roentgenology 2020, 214, 1248–1258. [Google Scholar] [CrossRef]
- Lewinshtein, D.; Teng, B.; Valencia, A.; Gibbons, R.; Porter, C.R. The long-term outcomes after radical prostatectomy of patients with pathologic Gleason 8–10 disease. Advances in urology 2012, 2012, 428098. [Google Scholar] [CrossRef]
- Hamdy, F.C.; Donovan, J.L.; Lane, J.A.; Mason, M.; Metcalfe, C.; Holding, P.; Davis, M.; Peters, T.J.; Turner, E.L.; Martin, R.M.; et al. 10-Year Outcomes after Monitoring, Surgery, or Radiotherapy for Localized Prostate Cancer. New England Journal of Medicine 2016, 375, 1415–1424. [Google Scholar] [CrossRef]
- Leichman, L. Neoadjuvant chemotherapy for disseminated colorectal cancer: changing the paradigm. 2006, 24, 3817-3818.
- Hirmas, N.; Holtschmidt, J.; Loibl, S. Shifting the paradigm: the transformative role of neoadjuvant therapy in early breast cancer. Cancers 2024, 16, 3236. [Google Scholar] [CrossRef]
- Häberle, L.; Erber, R.; Gass, P.; Hein, A.; Niklos, M.; Volz, B.; Hack, C.C.; Schulz-Wendtland, R.; Huebner, H.; Goossens, C. Prediction of pathological complete response after neoadjuvant chemotherapy for HER2-negative breast cancer patients with routine immunohistochemical markers. Breast Cancer Research 2025, 27, 13. [Google Scholar] [CrossRef]
- Howard, F.M.; He, G.; Peterson, J.R.; Pfeiffer, J.; Earnest, T.; Pearson, A.T.; Abe, H.; Cole, J.A.; Nanda, R. Highly accurate response prediction in high-risk early breast cancer patients using a biophysical simulation platform. Breast Cancer Research and Treatment 2022, 196, 57–66. [Google Scholar] [CrossRef]
- van Der Slot, M.A.; Remmers, S.; Kweldam, C.F.; den Bakker, M.A.; Nieboer, D.; Busstra, M.B.; Gan, M.; Klaver, S.; Rietbergen, J.B.; van Leenders, G.J. Biopsy prostate cancer perineural invasion and tumour load are associated with positive posterolateral margins at radical prostatectomy: implications for planning of nerve-sparing surgery. Histopathology 2023, 83, 348–356. [Google Scholar] [CrossRef] [PubMed]
- Aredo, J.V.; Jamali, A.; Zhu, J.; Heater, N.; Wakelee, H.A.; Vaklavas, C.; Anagnostou, V.; Lu, J. Liquid Biopsy Approaches for Cancer Characterization, Residual Disease Detection, and Therapy Monitoring. American Society of Clinical Oncology Educational Book 2025, 45, e481114. [Google Scholar] [CrossRef]
- Leslie SW, Soon-Sutton TL, Skelton WP. Prostate Cancer. [Updated 2024 Oct 4]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470550/.
- Wang, F.; Li, Z.; Feng, X.; Yang, D.; Lin, M. Advances in PSMA-targeted therapy for prostate cancer. Prostate Cancer and Prostatic Diseases 2022, 25, 11–26. [Google Scholar] [CrossRef]
- Jiang, Z.; Kadeerhan, G.; Zhang, J.; Guo, W.; Guo, H.; Wang, D. Advances in prostate-specific membrane antigen-targeted theranostics: from radionuclides to near-infrared fluorescence technology. Frontiers in Immunology 2025, 15, 1533532. [Google Scholar] [CrossRef] [PubMed]
- Corpetti, M.; Mueller, C.; Beltran, H.; de Bono, J.; Theurillat, J.-P. Prostate-specific membrane antigen–Targeted therapies for Prostate cancer: towards improving therapeutic outcomes. European urology 2024, 85, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Hennrich, U.; Eder, M. [177Lu] Lu-PSMA-617 (PluvictoTM): the first FDA-approved radiotherapeutical for treatment of prostate cancer. Pharmaceuticals 2022, 15, 1292. [Google Scholar] [CrossRef]
- Cross, W.; Wong, P.; Freedman, N. Dose distributions for electrons and beta rays incident normally on water. Radiation protection dosimetry 1991, 35, 77–91. [Google Scholar]
- Delbart, W.; Karabet, J.; Marin, G.; Penninckx, S.; Derrien, J.; Ghanem, G.E.; Flamen, P.; Wimana, Z. Understanding the radiobiological mechanisms induced by 177Lu-DOTATATE in comparison to external beam radiation therapy. International journal of molecular sciences 2022, 23, 12369. [Google Scholar] [CrossRef]
- Kuo, P.; Hesterman, J.; Rahbar, K.; Kendi, A.T.; Wei, X.X.; Fang, B.; Adra, N.; Armstrong, A.J.; Garje, R.; Michalski, J.M. [68Ga] Ga-PSMA-11 PET baseline imaging as a prognostic tool for clinical outcomes to [177Lu] Lu-PSMA-617 in patients with mCRPC: A VISION substudy. 2022.
- Ling, S.W.; de Lussanet de la Sablonière, Q.; Ananta, M.; de Blois, E.; Koolen, S.L.W.; Drexhage, R.C.; Hofland, J.; Robbrecht, D.G.J.; van der Veldt, A.A.M.; Verburg, F.A.; et al. First real-world clinical experience with [(177)Lu]Lu-PSMA-I&T in patients with metastatic castration-resistant prostate cancer beyond VISION and TheraP criteria. Eur J Nucl Med Mol Imaging 2025, 52, 2034–2040. [Google Scholar] [CrossRef]
- Sartor, O.; De Bono, J.; Chi, K.N.; Fizazi, K.; Herrmann, K.; Rahbar, K.; Tagawa, S.T.; Nordquist, L.T.; Vaishampayan, N.; El-Haddad, G. Lutetium-177–PSMA-617 for metastatic castration-resistant prostate cancer. New England Journal of Medicine 2021, 385, 1091–1103. [Google Scholar] [CrossRef]
- Hofman, M.S.; Emmett, L.; Sandhu, S.; Iravani, A.; Buteau, J.P.; Joshua, A.M.; Goh, J.C.; Pattison, D.A.; Tan, T.H.; Kirkwood, I.D. Overall survival with [177Lu] Lu-PSMA-617 versus cabazitaxel in metastatic castration-resistant prostate cancer (TheraP): secondary outcomes of a randomised, open-label, phase 2 trial. The Lancet Oncology 2024, 25, 99–107. [Google Scholar] [CrossRef]
- Almuradova, E.; Seyyar, M.; Arak, H.; Tamer, F.; Kefeli, U.; Koca, S.; Sen, E.; Telli, T.A.; Karatas, F.; Gokmen, I.; et al. The real-world outcomes of Lutetium-177 PSMA-617 radioligand therapy in metastatic castration-resistant prostate cancer: Turkish Oncology Group multicenter study. Int J Cancer 2024, 154, 692–700. [Google Scholar] [CrossRef] [PubMed]
- Hofman, M.S.; Violet, J.; Hicks, R.J.; Ferdinandus, J.; Thang, S.P.; Akhurst, T.; Iravani, A.; Kong, G.; Ravi Kumar, A.; Murphy, D.G.; et al. [(177)Lu]-PSMA-617 radionuclide treatment in patients with metastatic castration-resistant prostate cancer (LuPSMA trial): a single-centre, single-arm, phase 2 study. Lancet Oncol 2018, 19, 825–833. [Google Scholar] [CrossRef] [PubMed]
- Kassis, A.I. Therapeutic radionuclides: biophysical and radiobiologic principles. Semin Nucl Med 2008, 38, 358–366. [Google Scholar] [CrossRef]
- Russ, E.; Davis, C.M.; Slaven, J.E.; Bradfield, D.T.; Selwyn, R.G.; Day, R.M. Comparison of the medical uses and cellular effects of high and low linear energy transfer radiation. Toxics 2022, 10, 628. [Google Scholar] [CrossRef]
- Bertinetti, A.; Palmer, B.; Bradshaw, T.; Culberson, W. Investigation of a measurement-based dosimetry approach to beta particle-emitting radiopharmaceutical therapy nuclides across tissue interfaces. Physics in Medicine & Biology 2024, 69, 125008. [Google Scholar]
- Shi, M.; Jakobsson, V.; Greifenstein, L.; Khong, P.-L.; Chen, X.; Baum, R.P.; Zhang, J. Alpha-peptide receptor radionuclide therapy using actinium-225 labeled somatostatin receptor agonists and antagonists. Frontiers in medicine 2022, 9, 1034315. [Google Scholar] [CrossRef] [PubMed]
- Mavragani, I.V.; Nikitaki, Z.; Kalospyros, S.A.; Georgakilas, A.G. Ionizing radiation and complex DNA damage: from prediction to detection challenges and biological significance. Cancers 2019, 11, 1789. [Google Scholar] [CrossRef] [PubMed]
- King, A.P.; Lin, F.I.; Escorcia, F.E. Why bother with alpha particles? European Journal of Nuclear Medicine and Molecular Imaging 2021, 49, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Ballisat, L.; De Sio, C.; Beck, L.; Guatelli, S.; Sakata, D.; Shi, Y.; Duan, J.; Velthuis, J.; Rosenfeld, A. Dose and DNA damage modelling of diffusing alpha-emitters radiation therapy using Geant4. Physica Medica 2024, 121, 103367. [Google Scholar] [CrossRef]
- Lepareur, N.; Ramée, B.; Mougin-Degraef, M.; Bourgeois, M. Clinical Advances and Perspectives in Targeted Radionuclide Therapy. Pharmaceutics 2023, 15, 1733. [Google Scholar] [CrossRef]
- Tagawa, S.T.; Fung, E.; Niaz, M.O.; Bissassar, M.; Singh, S.; Patel, A.; Tan, A.; Zuloaga, J.M.; Castellanos, S.H.; Nauseef, J.T. Abstract CT143: Results of combined targeting of prostate-specific membrane antigen (PSMA) with alpha-radiolabeled antibody 225Ac-J591 and beta-radiolabeled ligand 177Lu-PSMA I&T: preclinical and initial phase 1 clinical data in patients with metastatic castration-resistant prostate cancer (mCRPC). Cancer Research 2022, 82, CT143–CT143. [Google Scholar]
- Bruchertseifer, F.; Kellerbauer, A.; Malmbeck, R.; Morgenstern, A. Targeted alpha therapy with bismuth-213 and actinium-225: meeting future demand. Journal of Labelled Compounds and Radiopharmaceuticals 2019, 62, 794–802. [Google Scholar] [CrossRef]
- Dash, A.; Pillai, M.R.; Knapp, F.F., Jr. Production of (177)Lu for Targeted Radionuclide Therapy: Available Options. Nucl Med Mol Imaging 2015, 49, 85–107. [Google Scholar] [CrossRef]
- Kouri, M.A.; Georgopoulos, A.; Manios, G.E.; Maratou, E.; Spathis, A.; Chatziioannou, S.; Platoni, K.; Efstathopoulos, E.P. Preliminary Study on Lutetium-177 and Gold Nanoparticles: Apoptosis and Radiation Enhancement in Hepatic Cancer Cell Line. Current Issues in Molecular Biology 2024, 46, 12244–12259. [Google Scholar] [CrossRef]
- Brans, B.; Mottaghy, F.M.; Kessels, A. 90Y/177Lu-DOTATATE therapy: survival of the fittest? European journal of nuclear medicine and molecular imaging 2011, 38, 1785–1787. [Google Scholar] [CrossRef]
- Henriksen, G.; Breistøl, K.; Bruland, Ø.S.; Fodstad, Ø.; Larsen, R.H. Significant antitumor effect from bone-seeking, α-particle-emitting 223Ra demonstrated in an experimental skeletal metastases model. Cancer research 2002, 62, 3120–3125. [Google Scholar] [PubMed]
- Miederer, M.; Scheinberg, D.A.; McDevitt, M.R. Realizing the potential of the Actinium-225 radionuclide generator in targeted alpha particle therapy applications. Advanced drug delivery reviews 2008, 60, 1371–1382. [Google Scholar] [CrossRef]
- Scheinberg, D.A.; McDevitt, M.R. Actinium-225 in targeted alpha-particle therapeutic applications. Curr Radiopharm 2011, 4, 306–320. [Google Scholar] [CrossRef]
- Parent, E.E.; Savir-Baruch, B.; Gayed, I.W.; Almaguel, F.; Chin, B.B.; Pantel, A.R.; Armstrong, E.; Morley, A.; Ippisch, R.C.; Flavell, R.R. 177Lu-PSMA therapy. Journal of nuclear medicine technology 2022, 50, 205–212. [Google Scholar] [CrossRef]
- Foxton, C.; Waldron, B.; Grønlund, R.V.; Simón, J.J.; Cornelissen, B.; O’Neill, E.; Stevens, D. Preclinical Evaluation of 177Lu-rhPSMA-10.1, a Radiopharmaceutical for Prostate Cancer: Biodistribution and Therapeutic Efficacy. Journal of Nuclear Medicine 2025, 66, 599–604. [Google Scholar] [CrossRef]
- Alghazo, O.; Eapen, R.; Dhiantravan, N.; Violet, J.A.; Jackson, P.; Scalzo, M.; Keam, S.P.; Mitchell, C.; Neeson, P.J.; Sandhu, S.K.; et al. Study of the dosimetry, safety, and potential benefit of 177Lu-PSMA-617 radionuclide therapy prior to radical prostatectomy in men with high-risk localized prostate cancer (LuTectomy study). Journal of Clinical Oncology 2021, 39, TPS264–TPS264. [Google Scholar] [CrossRef]
- Eapen, R.S.; Buteau, J.P.; Jackson, P.; Mitchell, C.; Oon, S.F.; Alghazo, O.; McIntosh, L.; Dhiantravan, N.; Scalzo, M.J.; O'Brien, J.; et al. Administering [(177)Lu]Lu-PSMA-617 Prior to Radical Prostatectomy in Men with High-risk Localised Prostate Cancer (LuTectomy): A Single-centre, Single-arm, Phase 1/2 Study. Eur Urol 2024, 85, 217–226. [Google Scholar] [CrossRef]
- Hoffmann, M.A.; Soydal, C.; Virgolini, I.; Tuncel, M.; Kairemo, K.; Kapp, D.S.; von Eyben, F.E. Management Based on Pretreatment PSMA PET of Patients with Localized High-Risk Prostate Cancer Part 2: Prediction of Recurrence—A Systematic Review and Meta-Analysis. Cancers 2025, 17, 841. [Google Scholar] [CrossRef]
- Krafft, U.; Grünwald, V.; Fendler, W.P.; Herrmann, K.; Reis, H.; Roghmann, F.; Rahbar, K.; Heidenreich, A.; Giesel, F.L.; Niegisch, G.; et al. A randomized phase I/II study of neoadjuvant treatment with 177-Lutetium-PSMA-617 with or without ipilimumab in patients with very high-risk prostate cancer who are candidates for radical prostatectomy (NEPI trial). Journal of Clinical Oncology 2024. [Google Scholar] [CrossRef]
- Sartor, A.O.; Kiess, A.P.; Feng, F.Y.; Hadaschik, B.A.; Herrmann, K.; Iagaru, A.; Matsubara, N.; Morris, M.J.; Nguyen, P.L.; Shore, N.D.; et al. PSMA-delay castration (DC): An open-label, multicenter, randomized phase 3 study of [<sup>177</sup>Lu]Lu-PSMA-617 versus observation in patients with metachronous PSMA-positive oligometastatic prostate cancer (OMPC). Journal of Clinical Oncology 2025, 43, TPS5127–TPS5127. [Google Scholar] [CrossRef]
- Zhang, Z.; Liu, X.; Chen, D.; Yu, J. Radiotherapy combined with immunotherapy: the dawn of cancer treatment. Signal Transduction and Targeted Therapy 2022, 7, 258. [Google Scholar] [CrossRef]
- Handke, A.; Kesch, C.; Fendler, W.P.; Telli, T.; Liu, Y.; Hakansson, A.; Davicioni, E.; Hughes, J.; Song, H.; Lueckerath, K.; et al. Analysing the tumor transcriptome of prostate cancer to predict efficacy of Lu-PSMA therapy. J Immunother Cancer 2023, 11. [Google Scholar] [CrossRef] [PubMed]
- Fucikova, J.; Kepp, O.; Kasikova, L.; Petroni, G.; Yamazaki, T.; Liu, P.; Zhao, L.; Spisek, R.; Kroemer, G.; Galluzzi, L. Detection of immunogenic cell death and its relevance for cancer therapy. Cell Death & Disease 2020, 11, 1013. [Google Scholar] [CrossRef]
- Barjij, I.; Meliani, M. Immunogenic Cell Death as a Target for Combination Therapies in Solid Tumors: A Systematic Review Toward a New Paradigm in Immuno-Oncology. Cureus 2025, 17, e85776. [Google Scholar] [CrossRef]
- Sandhu, S.; Subramaniam, S.; Hofman, M.S.; Stockler, M.R.; Martin, A.J.; Pokorski, I.; Goh, J.C.; Pattison, D.A.; Dhiantravan, N.; Gedye, C. Evolution: Phase II study of radionuclide 177Lu-PSMA-617 therapy versus 177Lu-PSMA-617 in combination with ipilimumab and nivolumab for men with metastatic castration-resistant prostate cancer (mCRPC; ANZUP 2001). 2023.
- Strati, A.; Adamopoulos, C.; Kotsantis, I.; Psyrri, A.; Lianidou, E.; Papavassiliou, A.G. Targeting the PD-1/PD-L1 signaling pathway for cancer therapy: focus on biomarkers. International Journal of Molecular Sciences 2025, 26, 1235. [Google Scholar] [CrossRef]
- Rozali, E.N.; Hato, S.V.; Robinson, B.W.; Lake, R.A.; Lesterhuis, W.J. Programmed death ligand 2 in cancer-induced immune suppression. Clin Dev Immunol 2012, 2012, 656340. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Qu, Y.; Yang, J.; Shao, T.; Kuang, J.; Liu, C.; Qi, Y.; Li, M.; Li, Y.; Zhang, S.; et al. PD-L2 act as an independent immune checkpoint in colorectal cancer beyond PD-L1. Front Immunol 2024, 15, 1486888. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wang, W.; Gu, R.; Chen, J.; Chen, Q.; Lin, T.; Wu, J.; Hu, Y.; Yuan, A. In Situ Vaccination with Mitochondria-Targeting Immunogenic Death Inducer Elicits CD8(+) T Cell-Dependent Antitumor Immunity to Boost Tumor Immunotherapy. Adv Sci (Weinh) 2023, 10, e2300286. [Google Scholar] [CrossRef]
- Bono, J.d.; Mateo, J.; Fizazi, K.; Saad, F.; Shore, N.; Sandhu, S.; Chi, K.N.; Sartor, O.; Agarwal, N.; Olmos, D.; et al. Olaparib for Metastatic Castration-Resistant Prostate Cancer. New England Journal of Medicine 2020, 382, 2091–2102. [Google Scholar] [CrossRef]
- Sun, C.; Chu, A.; Song, R.; Liu, S.; Chai, T.; Wang, X.; Liu, Z. PARP inhibitors combined with radiotherapy: are we ready? Front Pharmacol 2023, 14, 1234973. [Google Scholar] [CrossRef]
- Raychaudhuri, R.; Tuchayi, A.M.; Low, S.K.; Arafa, A.T.; Graham, L.S.; Gulati, R.; Pritchard, C.C.; Montgomery, R.B.; Haffner, M.C.; Nelson, P.S.; et al. Association of Prior PARP Inhibitor Exposure with Clinical Outcomes after (177)Lu-PSMA-617 in Men with Castration-resistant Prostate Cancer and Mutations in DNA Homologous Recombination Repair Genes. Eur Urol Oncol 2025. [Google Scholar] [CrossRef] [PubMed]
- Berchuck, J.E.; Zhang, Z.; Silver, R.; Kwak, L.; Xie, W.; Lee, G.-S.M.; Freedman, M.L.; Kibel, A.S.; Van Allen, E.M.; McKay, R.R.; et al. Impact of Pathogenic Germline DNA Damage Repair alterations on Response to Intense Neoadjuvant Androgen Deprivation Therapy in High-risk Localized Prostate Cancer. European Urology 2021, 80, 295–303. [Google Scholar] [CrossRef] [PubMed]
- van der Gaag, S.; Vis, A.N.; Bartelink, I.H.; Koppes, J.C.C.; Hodolic, M.; Hendrikse, H.; Oprea-Lager, D.E. Exploring the Flare Phenomenon in Patients with Castration-Resistant Prostate Cancer: Enzalutamide-Induced PSMA Upregulation Observed on PSMA PET. Journal of Nuclear Medicine 2025, jnumed.124.268340. [CrossRef]
- Mei, R.; Bracarda, S.; Emmett, L.; Farolfi, A.; Lambertini, A.; Fanti, S.; Castellucci, P. Androgen deprivation therapy and its modulation of PSMA expression in prostate cancer: mini review and case series of patients studied with sequential [68Ga]-Ga-PSMA-11 PET/CT. Clinical and Translational Imaging 2021, 9, 215–220. [Google Scholar] [CrossRef]
- Zacho, H.D.; Petersen, L.J. Bone flare to androgen deprivation therapy in metastatic, hormone-sensitive prostate cancer on 68Ga-prostate-specific membrane antigen PET/CT. Clinical Nuclear Medicine 2018, 43, e404–e406. [Google Scholar] [CrossRef]
- Stephenson, A.J.; Kattan, M.W.; Eastham, J.A.; Bianco, F.J., Jr.; Yossepowitch, O.; Vickers, A.J.; Klein, E.A.; Wood, D.P.; Scardino, P.T. Prostate cancer-specific mortality after radical prostatectomy for patients treated in the prostate-specific antigen era. J Clin Oncol 2009, 27, 4300–4305. [Google Scholar] [CrossRef] [PubMed]
- Xie, W.; Regan, M.M.; Buyse, M.; Halabi, S.; Kantoff, P.W.; Sartor, O.; Soule, H.; Clarke, N.W.; Collette, L.; Dignam, J.J.; et al. Metastasis-Free Survival Is a Strong Surrogate of Overall Survival in Localized Prostate Cancer. Journal of Clinical Oncology 2017, 35, 3097–3104. [Google Scholar] [CrossRef]
- Xie, W.; Ravi, P.; Buyse, M.; Halabi, S.; Kantoff, P.; Sartor, O.; Soule, H.; Clarke, N.; Dignam, J.; James, N.; et al. Validation of metastasis-free survival as a surrogate endpoint for overall survival in localized prostate cancer in the era of docetaxel for castration-resistant prostate cancer. Ann Oncol 2024, 35, 285–292. [Google Scholar] [CrossRef]
- Peng, Y.; Mei, W.; Ma, K.; Zeng, C. Circulating Tumor DNA and Minimal Residual Disease (MRD) in Solid Tumors: Current Horizons and Future Perspectives. Frontiers in Oncology 2021, Volume 11 - 2021. [CrossRef]
- Zang, P.D.; Lama, D.; Huang, Z.; Jaime-Casas, S.; Contente-Cuomo, T.; Stampar, M.; Marshall, A.; Dinwiddie, D.; Berens, M.E.; Pond, S.; et al. Feasibility of enriched amplicon circulating tumor DNA sequencing to detect minimal residual disease (MRD) after prostatectomy in localized prostate cancer. Journal of Clinical Oncology 2025, 43, 402–402. [Google Scholar] [CrossRef]
- Mehrens, D.; Kramer, K.K.M.; Unterrainer, L.M.; Beyer, L.; Bartenstein, P.; Froelich, M.F.; Tollens, F.; Ricke, J.; Rübenthaler, J.; Schmidt-Hegemann, N.-S.; et al. Cost-Effectiveness Analysis of 177Lu-PSMA-617 Radioligand Therapy in Metastatic Castration-Resistant Prostate Cancer. Journal of the National Comprehensive Cancer Network 2023, 21, 43–50.e42. [Google Scholar] [CrossRef]
Figure 1.
Comparative schematic of treatment strategies for high-risk localized prostate cancer.(a) Standard radical prostatectomy or radiation therapy alone frequently leaves occult micrometastases, leading to high biochemical-recurrence rates. (b) In the neoadjuvant paradigm, intravenous 177Lu-PSMA-617 radioligand selectively targets PSMA-expressing tumor foci in the prostate and potential micrometastatic deposits. β-particle emission induces direct DNA damage and cross-fire effects, debulking disease before surgery while initiating immunogenic cell death that may prime systemic anti-tumor immunity. Therapy is administered during the interval between diagnosis and planned radical prostatectomy. (Figure created with BioRender.com.).
Figure 1.
Comparative schematic of treatment strategies for high-risk localized prostate cancer.(a) Standard radical prostatectomy or radiation therapy alone frequently leaves occult micrometastases, leading to high biochemical-recurrence rates. (b) In the neoadjuvant paradigm, intravenous 177Lu-PSMA-617 radioligand selectively targets PSMA-expressing tumor foci in the prostate and potential micrometastatic deposits. β-particle emission induces direct DNA damage and cross-fire effects, debulking disease before surgery while initiating immunogenic cell death that may prime systemic anti-tumor immunity. Therapy is administered during the interval between diagnosis and planned radical prostatectomy. (Figure created with BioRender.com.).
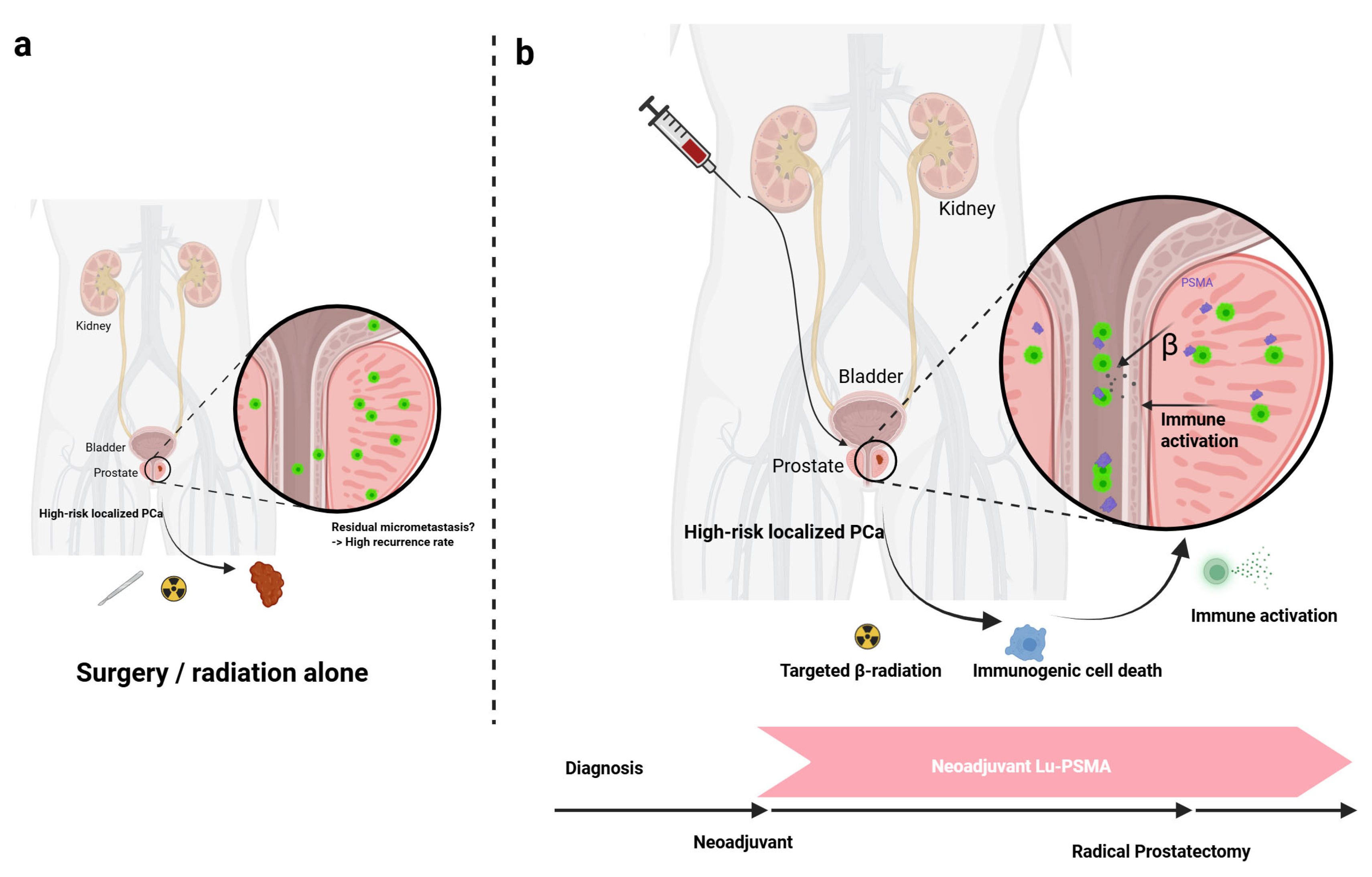
Figure 2.
Radio-immunologic modulation of the tumor immune microenvironment after 177Lu-PSMA-617 radioligand therapy. Targeted β-particle irradiation triggers apoptosis and necrosis of PSMA-expressing prostate-cancer cells, driving immunogenic cell death and the release of tumor-associated antigens and damage-associated molecular patterns. Immature dendritic cells capture these signals, mature under type-I-IFN influence and migrate to tumor-draining lymph nodes, where they prime naïve T cells. CXCL9–11-guided effector CD8⁺ T cells then home back to the tumor, release perforin and granzyme B, and secrete IFN-γ and TNF, collectively reshaping the tumor immune microenvironment toward effective cytotoxicity. (Figure created with BioRender.com.).
Figure 2.
Radio-immunologic modulation of the tumor immune microenvironment after 177Lu-PSMA-617 radioligand therapy. Targeted β-particle irradiation triggers apoptosis and necrosis of PSMA-expressing prostate-cancer cells, driving immunogenic cell death and the release of tumor-associated antigens and damage-associated molecular patterns. Immature dendritic cells capture these signals, mature under type-I-IFN influence and migrate to tumor-draining lymph nodes, where they prime naïve T cells. CXCL9–11-guided effector CD8⁺ T cells then home back to the tumor, release perforin and granzyme B, and secrete IFN-γ and TNF, collectively reshaping the tumor immune microenvironment toward effective cytotoxicity. (Figure created with BioRender.com.).
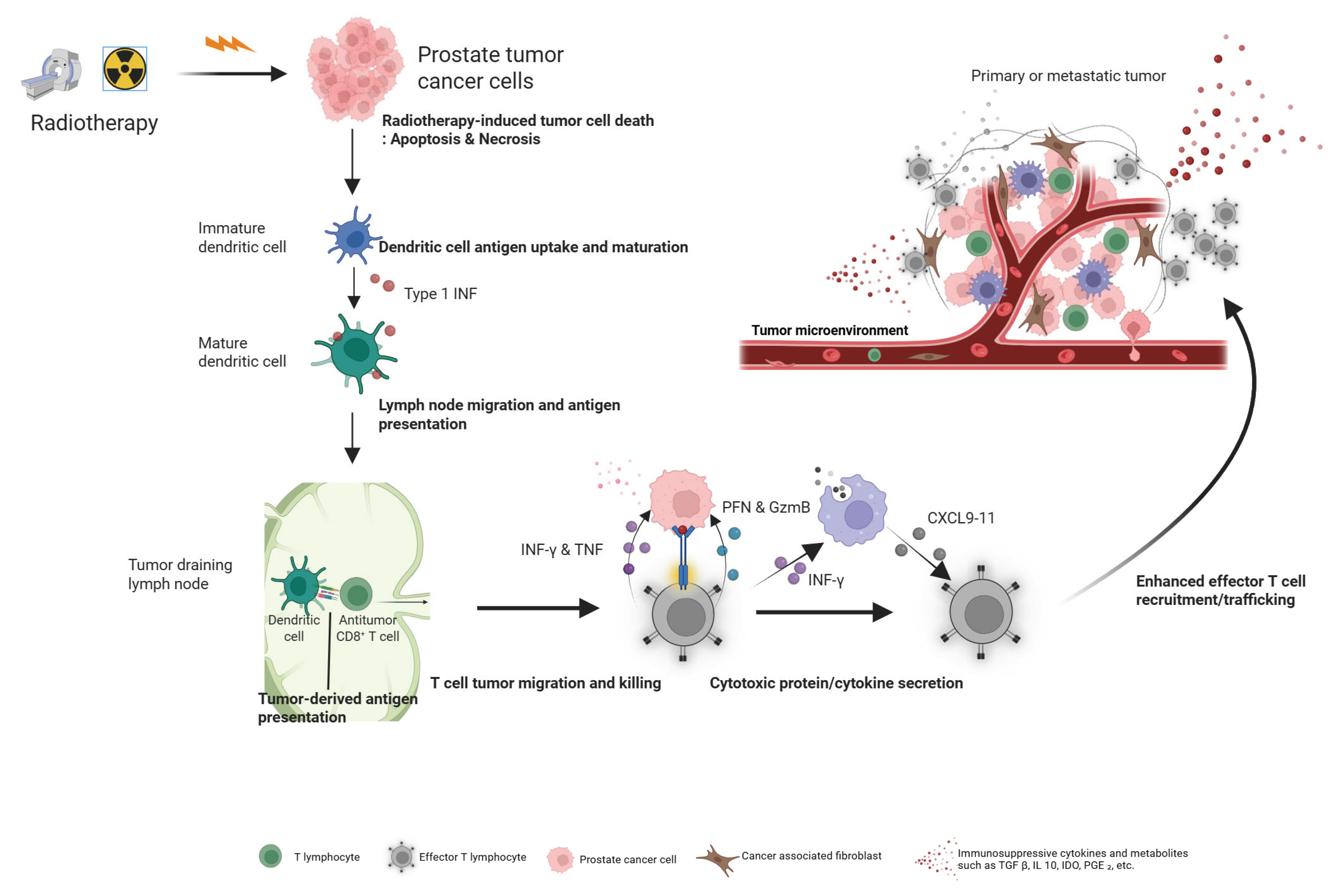

Table 1.
Comparison of International Guideline Definitions for High-Risk and Very High-Risk Localized Prostate Cancer.
Table 1.
Comparison of International Guideline Definitions for High-Risk and Very High-Risk Localized Prostate Cancer.
| Guideline | High-Risk Criteria | Very High-Risk Criteria | Key Features & Differences |
|---|---|---|---|
| NCCN (2025) [7] | One or more of the following: • Clinical stage cT3-cT4 • Grade Group 4 or 5 • PSA > 20 ng/mL |
Designated as Very High-Risk. Two or more of the following: • cT3-cT4 • Grade Group 4-5 • PSA > 40 ng/mL |
• Clearly defines separate "High-Risk" and "Very High-Risk" categories. • Uses a higher PSA threshold (40 ng/mL) for the Very High-Risk definition. |
| EAU (2025) [8] | Two or more of the following: • cT3-cT4 • Gleason Score 8-10 (GG 4-5) • PSA ≥ 40 ng/mL |
Designated as Very High-Risk. • Node-positive (N1) disease • Or meeting the high-risk criteria above (if node-negative) |
• The definition of "High-Risk" is much stricter than NCCN's, requiring 2 factors and a higher PSA threshold. • Explicitly includes N1 disease in the Very High-Risk category. |
| AUA/ASTRO/SUO (2022) [9] | One or more of the following: • cT3a • Grade Group 4-5 • PSA > 20 ng/mL |
No separate "Very High-Risk" category. Instead, these are classified as "Locally Advanced Disease": • cT3b-T4 (seminal vesicle invasion or beyond) • Presence of multiple high-risk features • Pelvic node positivity |
• Maintains a three-tier risk system and does not use the "Very High-Risk" terminology. • The High-Risk T-stage definition is more specific (cT3a). • The most advanced cases are managed as "Locally Advanced," emphasizing a multimodal approach. |
Abbreviations: ASTRO, American Society for Radiation Oncology; AUA, American Urological Association; cT, Clinical T-stage; EAU, European Association of Urology; GG, Grade Group; N1, Node-positive; NCCN, National Comprehensive Cancer Network; PSA, Prostate-Specific Antigen; SUO, Society of Urologic Oncology.
Table 2.
Radiobiological Properties of Clinically Relevant Radionuclides.
| Radionuclide | Particle Emitted | Half-life | Max Energy (MeV) | Max Range in Tissue | Typical LET (keV/µm) |
|---|---|---|---|---|---|
| 177Lu [43,44] | Beta (β) | 6.7 days | 0.497 | ~2 mm | ~0.2 |
| 90Y [45] | Beta (β) | 2.7 days | 2.3 | ~11 mm | ~0.2 |
| 223Ra [46] | Alpha (α) | 11.4 days | 5.0-7.5 | 40-100 µm | ~80 |
| 225Ac [47,48] | Alpha (α) | 9.9 days | 5.0-8.4 | 40-100 µm | ~100 |
Abbreviations: 177Lu, Lutetium-177; ²²³Ra, Radium-223; 225Ac, Actinium-225; ⁹⁰Y, Yttrium-90; keV, kilo-electron volt; LET, Linear Energy Transfer; MeV, Mega-electron Volt; µm, micrometer.
Table 3.
Summary of Key Ongoing Trials of Neoadjuvant PSMA-RLT.
| Trial Name (Identifier) | Phase | Patient Population | Intervention(s) | Primary Endpoint(s) | Key Secondary Endpoints |
|---|---|---|---|---|---|
| LuTectomy (NCT04430192) [51] | I/II | High-risk localized/locoregional PCa (n=20) | Single cycle of 177Lu-PSMA-617 prior to RP | Absorbed radiation dose (dosimetry) | Safety, surgical feasibility, PSA response, imaging response, pathological response |
| NEPI (EudraCT 2021-004894-30) [54] | I/II | Very high-risk localized PCa (n=46) | ADT + 2 cycles 177Lu-PSMA-617 +/- 4 cycles ipilimumab prior to RP | Feasibility of RP, pCR | Safety, DFS |
| PSMA-DC [55] | III | Oligometastatic (≤5 lesions) recurrence post-local therapy (n=~450) | SBRT to all lesions, then 177Lu-PSMA-617 vs. Observation | MFS | Time to next hormonal therapy, OS, safety |
Abbreviations: ADT, Androgen Deprivation Therapy; DFS, Disease-Free Survival; MFS, Metastasis-Free Survival; OS, Overall Survival; PCa, Prostate Cancer; pCR, pathologic Complete Response; PSA, Prostate-Specific Antigen; PSMA, Prostate-Specific Membrane Antigen; RP, Radical Prostatectomy; SBRT, Stereotactic Body Radiotherapy.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



