Submitted:
28 July 2025
Posted:
29 July 2025
You are already at the latest version
Abstract
Aseptic loosening (AL) represents the leading cause of long-term failure in total joint arthroplasty, often necessitating revision surgery. This review explores the complex mechanisms underlying AL, which involve a multifaceted interaction between the implanted biomaterials and the host immune response. We outline the key inflammatory mechanisms triggered by wear debris from polyethylene, polymethylmethacrylate, metal, and ceramic materials. We also examine emerging biomarkers for early detection and differentiation between stable and loosened implants, including pro-inflammatory cytokines, bone metabolism markers, extracellular matrix degradation products, microRNAs, and genetic polymorphisms. Lastly, we discuss current and future strategies for prevention and treatment, ranging from surgical optimization and biomaterial selection to pharmacological interventions. A comprehensive understanding of these mechanisms may help reduce the incidence of AL and improve long-term outcomes in arthroplasty patients.
Keywords:
Aseptic loosening
; biomarker
; osteolysis
; total hip arthroplasty
1. Biology of Aseptic Loosening
Aseptic loosening (AL) refers to the detachment of an implant from the surrounding bone without any evidence of infection or injury [1]. It is still a critical issue in joint arthroplasty, standing as one of the main reasons for long-term implant failure and the need for revision procedures after primary total joint replacement [2,3]. The overall number of joint replacement procedures is increasing, and it is predicted that this will result in an increase in the revision surgery rate. Therefore, it is imperative to comprehend the underlying causes of aseptic loosening in order to mitigate its incidence [4]. AL is a complex process driven by biological mechanisms that gradually destabilize the implant. This multifactorial process involves intricate interactions between the implant, immune system cells, and bone cells [5,6,7].
1.1. Immune Response to Biomaterials
Orthopedic implant placement triggers an innate immune response, beginning with acute inflammation followed by chronic inflammation driven by wear particle phagocytosis [8]. This process promotes granulation tissue formation, periprosthetic fibrosis, and increased osteoclast activity, disrupting bone homeostasis and leading to osteolysis [8]. Concurrently, a distinct and persistent foreign body reaction (FBR) occurs in response to non-degradable particulate debris. The FBR is characterized by sustained macrophage activation, multinucleated foreign body giant cells (FBGCs) formation, and debris fibrotic encapsulation [6]. Importantly, the FBR depends on and is influenced by the chronic inflammatory environment demonstrating that these pathways are interconnected and mutually reinforcing [6,8]. Together, they amplify extracellular matrix remodeling and bone resorption, ultimately leading to AL. Figure 1 illustrates the process flowchart.
1.1.1. Acute Inflammation
The surgical introduction of biomaterials leads to inevitable tissue damage, triggering an acute inflammatory response, which occurs alongside the body's specific reaction to the biomaterial [5,9]. Upon implantation, biomaterials rapidly adsorb proteins from blood and interstitial fluid proteins, forming a layer that influences immune cell recruitment, inflammation, and matrix formation [9,10]. Among these adsorbed proteins, albumin, fibrinogen, fibronectin, and complement factors regulate cell adhesion and immune activation, shaping the host response [5]. Biomaterials can also trigger coagulation pathway through Factor XII (FXII) and tissue factor (TF). Surface contact activates FXII, leading to thrombin generation, while platelet adhesion amplifies coagulation and inflammation [11,12]. Fibrinogen adsorption on biomaterials promotes phagocyte activation, contributing to clot formation and immune responses [13]. Concurrently, complement system activation results in the formation of C3 convertase. This, in turn, generates the anaphylatoxins C3a and C5a, which trigger inflammation by activating immune cells, increasing vascular permeability, and promoting mast cell degranulation [5]. The complement and coagulation cascades interact and modulate each other’s activities [14]. Leukocytes exit blood vessels and migrate into perivascular tissues in response to the implant [5,15,16,17,18,19]. Their interaction with biomaterial surfaces is mediated by adsorbed proteins acting as ligands for integrins that are the key adhesion receptors on leukocytes [5,13,20]. Among these ligands are fibrinogen, factor X, iC3b, fibronectin, and vitronectin [18,19]. Initial phagocyte attachment and spreading are facilitated by β2 integrins, which later promote the expression of additional integrins [5,18]. Mast cell degranulation, with histamine release, directs polymorphonuclear leukocytes (PMNs) and monocytes to implants and modulates the immune response through IL-4 and IL-13 secretion [5,21,22]. PMNs secrete IL-8, which recruits additional neutrophils and enhances the immune response; with certain biomaterials like chitosan, this migration may persist due to ongoing IL-8 signaling [5,23,24,25,26]. Activated PMNs release monocyte chemotactic protein-1 (MCP-1/CCL2) and macrophage inflammatory protein-1 (MIP-1), which serves as strong chemoattractant and activation signals for monocytes, macrophages, immature dendritic cells, and lymphocytes [5,27,28]. This chemokine release shifts the immune response by limiting further neutrophil infiltration while promoting the recruitment of monocytes. Once at the implantation site, monocytes differentiate into macrophages, initially adopting a pro-inflammatory M1 phenotype [6,29,30,31,32]. These macrophages amplify inflammation by releasing cytokines and recruiting mesenchymal stem cells (MSCs) [6]. Additionally, these factors enhance the osteogenic differentiation of mesenchymal stem cells (MSCs) into osteoblasts and stimulate angiogenesis, both essential processes for bone repair [6,33,34,35]. Tissue injury causes damage to the bone microvasculature, resulting in a hematoma formation around the lesion [36,37]. The early inflammatory response promotes new blood vessel development, while macrophages and osteoclasts remove damaged bone tissue [37,38]. Newly formed blood vessels ensure oxygen and nutrient supply, essential for MSC differentiation and bone regeneration [37]. The transition from M1 to the anti-inflammatory M2 macrophage phenotype plays a crucial role in resolving the inflammation and supporting tissue remodeling [6]. As the inflammation subsides, PMNs undergo apoptosis due to the absence of further activation signals. Their clearance by macrophages via phagocytosis facilitates the M1-to-M2 transition, stabilizing new vascular networks and promoting long-term tissue healing [5]. Typically, PMNs are no longer present at the surgical site within the first 48 hours of biomaterial implantation [5,8].
1.1.2. Chronic Inflammation
Inflammation around the implant site represents the tissue's defense against multiple stressors, such as surgical intervention, trauma, infections, the implant, and its wear debris.To prevent tissue damage and persistent immune reactions, anti-inflammatory mechanisms are simultaneously activated to restore tissue homeostasis [39,40]. However, not all patients with joint prostheses achieve a stable state, and some stressors persist [6,41,42]. Ongoing inflammation at the bone-implant interface, driven by wear particles, results in periprosthetic osteolysis (PPOL) [43]. Excessive wear particle production can induce chronic inflammation, driven by cytokine release from macrophages and foreign body giant cells (FBGCs), resulting in a continuous cycle of inflammatory stress in the affected tissues [5]. The immune response to wear particles is influenced by multiple factors [5]. Size plays a crucial role, as particles between 0.1 and 1 µm are the most biologically active [44,45,46,47,48]. Smaller particles (<1 µm) are engulfed by macrophages through phagocytosis, while larger particles (>10 µm) are typically encased by multiple macrophages and FBGCs [49]. Material composition also plays a key role, as substances like polyethylene, PMMA, and metals tend to provoke a stronger inflammatory reaction. Shape and surface texture contribute as well, with irregular, rough particles triggering a more intense immune reaction [46,49]. The quantity of particles is another key factor, as exceeding a certain threshold can lead to periprosthetic osteolysis [45,46,50]. The inflammatory response is further influenced by factors such as surface charge and the capacity of periprosthetic tissues to clear debris [46]. The body’s ability to balance pro- and anti-inflammatory mechanisms further determines the severity of the response. Furthermore, surface charge and the efficiency of periprosthetic tissue clearance also affect the inflammatory process. The body's capacity to modulate pro- and anti-inflammatory mechanisms is a pivotal factor in determining the severity of the response [46]. Finally, genetic susceptibility, including particular single-nucleotide polymorphism (SNP) variations, may have the potential to render certain individuals more prone to an aggressive inflammatory response [46]. Although various cells respond to implant debris by initiating inflammation, the central role belongs to resident macrophages, whose particle-clearing activity drives the inflammatory processes around the implant [51,52]. Macrophage activation by wear particles is mediated through pattern recognition receptors (PRRs). PRRs differ by location, with Toll-like receptors (TLRs)—particularly TLR2 and TLR4—playing a central role in how macrophages detect implant particles [43,53]. Wear debris functions as alarmins, engaging PRRs either at the cell surface or after phagocytosis. This interaction leads to the secretion of pro-inflammatory cytokines such as tumor necrosis factor-α (TNF-α), IL-1β, IL-6, and prostaglandin E - 2 (PGE-2) [43,54]. Moreover, macrophages release growth factors like macrophage colony-stimulating factor 1 (M-CSF), osteoclast-activating signals including receptor activator of nuclear factor kappa B ligand (RANKL), and chemokines such as IL-8, macrophage inflammatory protein-1α (MIP-1α), and MCP-1 [43,54]. This process draws in more macrophages and osteoclast precursors, worsening inflammation and bone loss [54]. Wear particles activate the NLRP3 inflammasome, which through a two-step process involving NF-κB and ASC, leads to the release of IL-1β and IL-18 [55]. Macrophage phagocytosis of wear debris activates this inflammasome pathway, leading to the release of IL-1β, which plays a key role in osteolysis [56]. Macrophage release of TNF-α and IL-1β in response to wear particles induces osteoblasts and fibroblasts to increase RANKL expression and decrease osteoprotegerin (OPG) production [57,58] A decreased OPG/RANKL ratio has been associated with enhanced osteolysis [59]. When RANKL binds to RANK on osteoclast precursors, it activates signaling cascades including nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) and mitogen-activated protein kinase (MAPK), leading to osteoclast formation and enhanced bone resorption that contributes to implant loosening [60]. This process is summarized in Figure 2.
1.1.3. Granulation Tissue and Fibrosis
It has been observed that, during the chronic inflammation phase, the release of growth factors such as Platelet-Derived Growth Factor (PDGF), Fibroblast Growth Factor (FGF), Transforming Growth Factor-β (TGF-β), and Epidermal Growth Factor (EGF) from macrophages stimulates the formation of new blood vessels and connective tissue [61]. At the site of implantation, fibroblasts and vascular endothelial cells proliferate, forming granulation tissue, a key feature of the healing inflammatory response. This tissue, distinguished by its pink, granular appearance in healing wounds, is characterized by the growth of new blood vessels and fibroblast proliferation [8,61].
New blood vessels form by sprouting from existing ones, a process called neovascularization or angiogenesis, involving endothelial cell growth, maturation, and assembly into capillaries [61]. As granulation tissue develops, fibroblasts proliferate and synthesize collagen and proteoglycans, leading to fibrotic encapsulation. The consequence of this persistent immune response is the continuous production of an extracellular matrix around the implant. This, in turn, results in implant loosening and potential failure. [61].
1.1.4. Foreign Body Reaction
FBR refers to the body's response to small particles and debris from implanted medical devices, such as prostheses [6]. This response involves various immune cells, including monocytes, macrophages, fibroblasts, FBGCs, and osteoclasts [6]. However, FBR around implants differs from acute and chronic inflammation, progressing through three phases: tolerant, irritable, and intolerant [6].
Tolerant Phase
Biocompatibility is defined as the ability of these materials to not induce a significant adverse reaction in the body but instead activate a protective response that helps maintain the body's homeostasis [6]. When introduced into the body, wear particles are phagocytosed by macrophages and become embedded in the fibrous matrix of the forming pseudo-capsule. During this phase, no obvious granulomas are formed [6,62,63,64].
As particles accumulate, macrophages become overwhelmed and undergo apoptosis, resulting in the engulfment of debris by other macrophages or its embedding in the extracellular matrix [64]. When this immune response is insufficient, granulomas form around the pseudo-capsule, amplifying inflammation and triggering the shift from the tolerant to the irritable phase [6].
Irritable Phase
As wear particle accumulation exceeds the body's clearance capacity, chronic inflammation intensifies, leading to granuloma formation within the regenerating capsule [6].
This phase is characterized by an imbalance between the host's defense mechanisms (phagocytosis and fibrotic tissue formation) and the persistent influx of wear debris [6]. When macrophages cannot engulf large particles (>10μm), they fuse to form multinucleated FBGCs. These cells then attempt to degrade and isolate the debris but inadvertently prolong inflammation, exacerbating tissue damage [6,8,65,66,67]. Granulomas recruit additional macrophages, monocytes, lymphocytes, and mast cells, amplifying the inflammatory response. Excessive fibroblast activation results in the formation of a dense fibrous capsule around the particles, encapsulating them within a collagen-rich matrix [6,65]. While this process initially helps contain the debris, prolonged inflammation leads to tissue remodeling and extracellular matrix degradation, ultimately compromising implant stability [6,31,68]. The inflammatory microenvironment also promotes the release of cytokines (TNF-α, IL-1, IFN-γ), ROS, and growth factors, which further stimulate the innate immune response [6,31,46]. As inflammatory joint fluid infiltrates the implant-bone interface, mechanical stress and fluid pressure waves accelerate direct bone resorption [6,69]. Furthermore, the dissemination of wear particles throughout the body can trigger a systemic immune response, known as particle disease [6,70,71].
Intolerant Phase
As the immune response escalates beyond the host’s ability to control it, the foreign body reaction becomes increasingly destructive. Granulomas, primarily composed of activated macrophages, fibroblasts, endothelial cells, lymphocytes, and inflammatory mediators, expand, triggering osteoclast activation and excessive bone resorption at the bone-implant interface [6,70]. Mast cells have been shown to amplify the inflammatory response by releasing histamine, IL-3, and IL-4, thereby exacerbating tissue degradation [6,63,66,67]. The infiltration of inflammatory joint fluid, rich in cytokines and wear particles, has been demonstrated to accelerate extracellular matrix breakdown and disrupt bone homeostasis [6]. The resulting imbalance is known to favor osteoclast-mediated bone resorption, leading to progressive weakening of the peri-implant bone tissue [6,46]. Within an acidic microenvironment, the excessive release of proteolytic enzymes, particularly cathepsin K, drives aggressive extracellular matrix degradation [8]. As osteolysis progresses, a synovial-like lining forms around the implant, further compromising structural integrity. The persistent immune activation and bone loss ultimately lead to implant loosening and failure [6,8].
1.2. Inflammatory Response to Different Implant Materials
1.2.1. Polyethylene Wear Particles
Polyethylene (PE) is a material frequently utilized in joint implants, wherein a PE liner is affixed to a metallic acetabular shell and a metallic femoral head [59,72]. Wear particles are continuously generated over time due to joint movement, with volumetric wear being the primary factor influencing particle production. It has been demonstrated that larger femoral heads (for example, with a diameter of 36 mm) produce a greater number of particles than smaller ones (for example, with a diameter of 22 mm) [59,73]. Particles of PE, particularly those measuring between 0.1 and 1 μm, have been observed to trigger inflammatory responses, with those between 0.3 and 1 μm being the most potent in stimulating FBGCs. In contrast, particles smaller than 0.3 μm are generally eliminated via pinocytosis [6,59,74]. They can trigger the release of proinflammatory cytokines and promote bone resorption [6]. In vitro studies have investigated how cells respond to particles of different sizes and compositions. Smaller PE particles (0.24 μm) have been found to be highly effective in stimulating proinflammatory cytokine release and bone resorbing activity in murine peritoneal macrophages [45]. Ultra-high molecular weight polyethylene (UHMWPE) is the polymer most frequently used in joint implants, valued for its excellent performance when paired with metal or ceramic bearing surfaces. It exhibits exceptional biocompatibility and high resistance to corrosion. Because UHMWPE produces many wear particles, it has been modified into cross-linked polyethylene (XLPE), which releases significantly fewer particles [43,75]. This cross-linking involves irradiating UHMWPE, creating free radicals [76]. If these radicals stay trapped, they may react with oxygen over time, causing oxidative degradation, embrittlement, and eventual mechanical failure [76,77,78].
In order to overcome this problem, new XLPE products have been produced with the addition of Vitamin E, a powerful antioxidant, to neutralize these free radicals and prevent oxidation without compromising the material's mechanical properties [79,80]. Both UHMWPE and XLPE particles have the potential of triggering an inflammatory response by inducing the overexpression of TLR2 and TLR4, pathways previously described. In addition, there is a possibility that they may also activates the NLRP3 inflammasome [43,81,82]. These particles are recognized not only through TLRs but also via phagocytosis. Once internalized, they accumulate in phagosomes, where they are resistant to enzymatic degradation [59,83,84]. Both pathways ultimately activate NF-κB, triggering the release of proinflammatory cytokines and mediators that drive bone resorption [43,59,85,86,87]. Transcriptomic analyses of human macrophages reveal increased expression of inflammatory and bone resorption markers such as CCL2, CCL3, CCL4, CCL20, IL-8, IL-1β, IL-6, TNF-α, M-CSF, and MMPs [88].
1.2.2. Polymethylmethacrylate Wear Particles
Polymethylmethacrylate (PMMA) particles, resulting from bone cement, promote osteoclastogenesis and osteolysis, primarily through TLR activation, leading to IL-1β and TNF-α secretion and monocyte recruitment via MCP-1 signaling [43,89,90,91,92,93].
The MyD88-dependent pathways is the main signaling mechanism for most TLRs except TLR3. MyD88 activation leads to NF-κB and AP-1 signaling, which stimulates the production of inflammatory cytokines like TNF-α, IL-1, and IL-12 [94]. Studies in patient samples and animal models confirm that TLRs mediate the immune response to implant debris. Experiments show that blocking MyD88 in macrophages lowers inflammation caused by PMMA particles, while mice lacking MyD88 exhibit a reduced inflammatory reaction [91]. PMMA also activate the NALP3 inflammasome, driving caspase-1-mediated IL-1β release and exacerbating inflammation [43,95]. Additionally, PMMA particles upregulate the vascular endothelial growth factor (VEGF), promoting angiogenesis, which has been linked to osteolysis progression. Murine studies show that VEGF inhibition reduces TNF-α production, inflammation, and osteoclast formation, highlighting its role in PMMA-induced bone resorption [43,96].
1.2.3. Metallic Wear Debris
The response mechanism to metallic wear debris is still controversial. Metallic particles, especially cobalt (Co) and titanium (Ti), elicit strong immune responses [43,59]. The existing body of research on the subject indicates that the presence of cobalt alloy debris activates both TLR4 and the NLRP3 inflammasome, leading to an increase in the production of IL-1β and IL-18 [43,97,98]. However, other studies have suggested that cobalt primarily activates the inflammasome pathway [98]. The involvement of TLR signaling in macrophage responses to cobalt particles is still controversial.. Some recent research indicates that cobalt and nickel ions can activate TLR4 [99]. However, other studies suggest that cobalt alloy particles do not primarily trigger TLR4-driven inflammation compared to NLRP3 inflammasome activation (IL-1β) in vitro, and that blocking TLR4 does not reduce the inflammatory response [98]. Additionally, cobalt induces hypoxia-like responses, up-regulating HIF-1α, VEGF, TNF-α, and ROS production, further exacerbating osteolysis [98]. Titanium (Ti) particles similarly activate IL-1β, IL-6, and TNF-α via NLRP3 inflammasome, a process dependent on TNF-α priming [43]. Moreover, metal ions can act as haptens, triggering a Type IV hypersensitivity response, recruiting T-lymphocytes, and contributing to adverse reactions to metal debris (ARMD) and perivascular lymphocytic infiltrates [6,31,43].
1.2.3. Ceramic Wear Debris
Over the past decades, ceramic-on-ceramic (CoC) implants have become the most commonly used bearing surfaces. CoC implants generate minimal wear particles, have a reduced risk of osteolysis, and offer strong durability over time. These properties make it a favorable option for young and active patients [100]. Compared to polymeric particles, ceramic materials like alumina (Al₂O₃) and zirconia (ZrO₂) produce very little wear debris, show minimal immune system toxicity and provoke only a mild release of TNF-α and IL-1β [43,59,101]. Ceramic debris causes minimal macrophage death and has limited effect on RANKL, OPG, and TNF-α expression which of course increases in a concentration-dependent manner. [43,102]. However, zirconia has been found to activate TLR3, TLR7, and TLR10, though its influence on cytokine release is minimal [43,103]. Overall, ceramic-on-ceramic prostheses have been demonstrated to exhibit a reduced propensity for debris formation, osteolysis, loosening, and prosthetic failure, provided that they are implanted in a satisfactory manner. However, cases of squeaking and ceramic fracture have been reported [104,105].
2. Biomarkers
Implant loosening is a multifactorial process influenced by biomechanical forces and the balance between osteoblast and osteoclast activity [106]. This balance can be assessed through objective biomarkers, including serum and urinary markers, which offer a minimally invasive and easily accessible means of monitoring biological processes [107]. Several studies have explored the potential of these biomarkers in distinguishing between aseptically loosened and stable implants.
Among the most studied biomarkers are those related to inflammation, as this process plays a central role in AL. Elevated levels of TNF-α, IL-1β, IL-6, and IL-8 have been found in patients with AL, indicating an active immune response contributing to bone resorption [108,109,110,111,112,113]. A study by Wu et al. (2009) demonstrated that elevated TNF-α expression was associated with higher levels of CD14+CD16+ monocytes in the blood, suggesting that these monocytes could also serve as potential biomarkers for AL [110]. Additionally, several studies have reported elevated levels of the chemokine MCP-1 and the synovial fluid marker CCL18 in patients with AL, suggesting their involvement in mediating inflammatory pathways and promoting the recruitment of immune cells to the site of implant loosening [114,115]. Bone metabolism markers play a crucial role in assessing AL, as the condition disrupts the balance between bone formation and resorption. In particular, RANKL levels are elevated in patients with AL, contributing to enhanced osteoclastogenesis and subsequent bone resorption. This increase in RANKL promotes osteoclast activation, leading to excessive bone resorption and ultimately, the loosening of the implant [112,114]. Specifically, markers of bone resorption, such as CTX, NTX, TRAP5b, and ICTP (C-telopeptide of type I collagen) are elevated, indicating heightened osteoclastic activity [112,116,117,118,119,120]. In contrast, markers of bone formation, including osteocalcin and PiCP, show significant alterations, with PiCP levels notably reduced, suggesting a disruption in the bone formation process [116,120]. These changes reflect the abnormal bone remodeling characteristic of AL and underscore the potential of these markers in assessing the condition.
In addition to these markers, extracellular matrix degradation also plays a key role in AL. Hyaluronic acid, an important component of the joint matrix, was found to be upregulated in AL patients, suggesting damage to the joint environment [111]. Similarly, CHIT1, a marker involved in the degradation of bone and cartilage, is elevated both in blood and synovial fluid, further pointing to ongoing matrix breakdown [115]. Cell adhesion molecules, such as CD18, CD11b, and CD11c, are also found at increased levels, which may reflect enhanced cellular activation and migration to areas of bone resorption [121]. Emerging research into microRNAs has revealed their potential as biomarkers for AL [122]. Several miRNAs, including miR-21, miR-92a, miR-106b, miR-130, miR-135, and miR-155, are upregulated in AL patients, while miR-29 appears reduced, suggesting their involvement in regulating both inflammatory responses and bone remodeling [123]. Finally, several studies have explored genetic factors that may predispose individuals to AL, focusing on SNPs in key inflammatory and bone remodeling genes. López-Anglada et al. (2021) demonstrated that polymorphisms in exon 2 of NOS2 and the +3954C/T polymorphism (exon 5, rs11436434) of IL-1β are associated with an increased frequency of AL. Specifically, the AA genotype of NOS2 and the TT genotype of IL-1β appear to be linked to a higher risk of developing the condition [113]. Additionally, Malik et al. (2007) assessed SNPs in MMP1, revealing an association between these genetic variations and an elevated risk of AL. These findings suggest that genetic predisposition plays a significant role in the development of AL, highlighting the potential for using genetic markers to better identify individuals at higher risk [124].
Table 1 summarizes key biomarkers and genetic factors involved in AL, indicating their typical levels in patients, their biological roles, and the sample type for their detection.
Prevention and Treatment of Aseptic Loosening
At present, the only effective treatment for AL is implant revision arthroplasty. AL accounts for approximately 40% of all revision procedures, both for hip and knee arthroplasties [125]. Consequently, efforts must focus on prevention, which involves reducing patient-related risk factors and selecting an appropriate prosthetic implant. Additionally, ongoing research is being conducted to develop therapeutic protocols that prevent AL. In the context of prevention, we can adopt preoperative, intraoperative, and postoperative measures. About patient-related risk factors, a Body Mass Index (BMI) greater than 35 kg/m² has been demonstrated to be associated with a twofold increase in the incidence of aseptic loosening. Conversely, an excessively low BMI has been demonstrated to heighten the risk of implant component migration and delays in osseointegration. Consequently, preoperative planning should encompass the attainment of optimal body weight, in conjunction with appropriate nutritional therapy and physical activity [126]. Osteoporosis has been shown to impair implant osseointegration. This phenomenon can be attributed to the presence of estrogen deficiency, which has been shown to result in diminished osteoblast longevity, increased osteoclast activity, and impaired differentiation of mesenchymal stromal cells into osteoblasts. Therefore, osteoporosis diagnosis and careful management are advised to facilitate osseointegration. Smoking raises the risk of AL in both cemented and cementless joint replacements [128]. This is mainly due to nicotine’s narrowing of blood vessels and the reduced oxygen supply caused by higher levels of carboxyhemoglobin. These factors reduce blood flow to the local tissue, causing hypoxia that likely hinders osseointegration [129]. Kapadia et al. found no significant difference in AL rates between former smokers (those who quit at least 30 days before surgery) and current smokers over an average follow-up of four years. Consequently, smoking cessation 30 days before surgery does not appear to be associated with reduced implant loosening rates. Further studies are required to determine the optimal time for patients to cease smoking before and after surgery to achieve the best possible results [130].
The role of cardiovascular disease, cancer, and psychotic disorders regarding the risk of AL is still controversial. On the other hand, in the case of other comorbidities, including neurodegenerative diseases, diabetes mellitus, and pulmonary diseases, the survival rate of hip titanium implants seems to remain unaffected [131]. To summarize, preoperative optimization should include BMI adjustment, osteoporosis treatment, smoking cessation, and control of cardiovascular and psychiatric conditions [132].
To determine the optimal course of action before hip replacement surgery, selecting the implant is crucial to minimize the risk of AL. Material stiffness, measured by the Young's modulus, needs to be low enough (but not excessively) to avoid bone stress shielding. This occurs when a stiffness mismatch between the implant and bone causes improper load transfer, leading to increased bone resorption and impaired remodeling, which can ultimately result in AL [133]. Stress shielding increases bone resorption and inhibits remodeling, ultimately leading to AL. An ideal implant should have a Young's modulus similar to bone (10–30 GPa). For instance, Ti6Al4V titanium alloy has a modulus of 110 GPa, compared to stainless steel’s 180 GPa. Additionally, the implant's structure and elasticity influence its long-term survival. Elasticity, given by a low Young's modulus, results in an increased micromotion, which can lead to fibrous tissue formation at the bone–implant interface instead of bone ingrowth [134]. Extensive research has focused on treating titanium surfaces using methods such as plasma spraying, hydroxyapatite coating, acid etching, sandblasting, alkali heat treatment, ion implantation, and nanotechnology. The most commonly used coatings are hydroxyapatite and porous coatings. Observations have revealed better outcome and reduced incidence of AL in hydroxyapatite coated implants [135,136]. Future developments may involve coatings with silicatitanate or growth factors like bone morphogenetic protein (BMP). Porous surfaces on uncemented titanium implants help stimulate and secure bone growth. Specific pore shapes and sizes promote the optimal osseointegration. It has been established that a porosity level exceeding 40% is conducive to optimal bone growth [137].
A further pivotal element in selecting the implant to prevent AL is the size of itself, which is essential for ensuring a proper press fit and stability. Isaacson et al. observed that micromovements of up to 30 μm are beneficial, but those exceeding 150 μm compromise osseointegration. Furthermore, it is imperative to ensure that the acetabular cup is properly oriented; it should not be excessively horizontal (45°). It has been established that femoral head sizes greater than 32 mm are associated with an elevated rate of revision surgery due to AL, despite a concomitantly lower incidence of dislocation [138].
The selection of surgical approach may also impact the risk of AL, although this remains uncertain. McCormick et al. found no statistically significant difference in revision rate between patients treated with a posterolateral approach or an anterior approach (either direct anterior or anterior-based muscle sparing approach) [139]. Conversely, data from the Swedish Hip Arthroplasty Register show higher AL revision rates with the anterolateral approach, likely due to component malpositioning. Surgeon experience may influence this risk, making optimal joint exposure crucial when using the anterior approach. Moreover, it has been demonstrated that excessive drilling or rasping can lead to mechanical and thermal bone damage, thereby impairing osseointegration [140].
One promising approach to reduce arthroplasty failures from AL is using anti-inflammatory drug-releasing devices postoperatively, aiming to improve the 10-year revision rate of 10%, as reported by NICE guideline [125]. Anti-inflammatory agents reduce periprosthetic inflammation that leads to bone loss and subsequent AL. Among the most extensively studied is dexamethasone (DEX), a molecule rendered water-soluble via phosphate group binding. DEX release has been shown not to affect osteoblast and fibroblast proliferation while retaining anti-inflammatory activity. These drug-eluting systems appear promising in reducing prosthetic revision rates. In uncemented prostheses, DEX coatings are applied to the porous surface of the implant to prevent exposure to friction forces [125]. Conversely, the utilization of NSAIDs appears to be contraindicated [141]. Another promising pharmacological class includes bisphosphonates. Zoledronic acid has been demonstrated to reduce cortical osteopenia in the calcar region of the proximal femur, thus proving efficacious in the management of stress-shielding-induced osteopenia. The administration of bisphosphonate treatment has been demonstrated to mitigate the effects of stress shielding, thereby reducing the risk of wear-related AL by enhancing periprosthetic bone retention. It is conceivable that these pharmaceuticals could also play a role in the treatment of patients who are not candidates for revision surgery due to elevated surgical and anesthesiologic risks [142].
Finally, evidence-based strategies for reducing AL can be categorized into preoperative, intraoperative, and postoperative measures.
Preoperative: act on modifiable factors such as BMI and osteoporotic bone; selection of porous coatings such as tantalum or hydroxyapatite, pore size around 600 μm, porosity >70%, and the use of the right size of femoral stems.
Intraoperative: Minimize excessive drilling or rasping, ensure stable fixation, adequate bone coverage, and proper containment for long-term success.
Postoperative: Pharmacological management with risedronate or zoledronic acid to modulate bone metabolism; avoidance of NSAIDs.
3. Conclusions
In conclusion, biomarkers related to inflammation, bone metabolism, extracellular matrix degradation, microRNAs, and genetic factors show promise in improving the diagnosis and monitoring of AL. While these markers provide valuable insights into the mechanisms underlying AL, there are still inconsistent results across studies regarding the identification of the most reliable indicators for differentiating between stable and loosened implants, despite the broad range of biomarkers analyzed in both total hip and knee arthroplasties. In order to validate these biomarkers and to better understand their role in the early detection of AL, further larger, well-designed studies are required. These studies should also attempt to identify patterns that can be used to prevent and manage patients affected by AL without the need for revision surgery.
Author Contributions
Conceptualization: Gabriele Ricciardi, Lorenza Siracusano, Edoardo Micale, Biagio Zampogna, Maurizio Martini. Data Curation: Gabriele Ricciardi, Lorenza Siracusano, Edoardo Micale, Vito Addorisio. Project administration: Biagio Zampogna, Maurizio Martini, Danilo Leonetti Supervision: Biagio Zampogna, Maurizio Martini. Validation: Mariagiovanna Ballato, Domenico Donadio, Pietro Tralongo. Writing – original draft: Gabriele Ricciardi, Lorenza Siracusano, Edoardo Micale. Writing – review and editing: Gabriele Ricciardi, Lorenza Siracusano, Edoardo Micale, Pietro Tralongo, Domenico Donadio.
Funding
This review received no external founding.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare that they have no competing interests.
Abbreviations
| AL | Aseptic loosening; |
| FXII | Factor XII; |
| TF | tissue factor; |
| IL | interleukin; |
| MCP-1/CCL2 | monocyte chemotactic protein-1/Chemokine CC motif ligand 2; |
| MIP-1 | macrophage inflammatory protein-1; |
| PMN | polymorphonuclear leukocyte; |
| FBR | foreign body reaction; |
| MSC | mesenchymal stem cell; |
| PPOL | periprosthetic osteolysis; |
| FBGC | foreign body giant cell; |
| PRR | pattern recognition receptor; |
| TNF | tumor necrosis factor; |
| PGE | prostaglandin E; |
| RANKL | receptor activator of nuclear factor kappa B ligand; |
| MIP-1α | macrophage inflammatory protein-1α; |
| TLR | Toll-like receptors; |
| OPG | osteoprotegerin; |
| NF-κB | nuclear factor kappa-light-chain-enhancer of activated B cells; |
| MAPK | mitogen-activated protein kinase; |
| PDGF | Platelet-Derived Growth Factor; |
| FGF | Fibroblast Growth Factor; |
| TGF | Transforming Growth Factor; |
| EGF | Epidermal Growth Factor; |
| ROS | reactive oxygen species; |
| PE | polyethylene; |
| UHMWPE | ultra-high molecular weight polyethylene; |
| XLPE | cross-linked polyethylene; |
| PMMA | Polymethylmethacrylate; |
| ARMD | adverse reactions to metal debris; |
References
- C. Li, S. C. Li, S. Schmid, J. Mason, Effects of pre-cooling and pre-heating procedures on cement polymerization and thermal osteonecrosis in cemented hip replacements, Medical Engineering & Physics 25 (2003) 559–564. [CrossRef]
- P.F. Sharkey, P.M. P.F. Sharkey, P.M. Lichstein, C. Shen, A.T. Tokarski, J. Parvizi, Why are total knee arthroplasties failing today--has anything changed after 10 years?, J Arthroplasty 29 (2014) 1774–1778. [CrossRef]
- K. Thiele, C. K. Thiele, C. Perka, G. Matziolis, H.O. Mayr, M. Sostheim, R. Hube, Current failure mechanisms after knee arthroplasty have changed: polyethylene wear is less common in revision surgery, J Bone Joint Surg Am 97 (2015) 715–720. [CrossRef]
- T.J.M. van Otten, C.J.M. T.J.M. van Otten, C.J.M. van Loon, Early aseptic loosening of the tibial component at the cement-implant interface in total knee arthroplasty: a narrative overview of potentially associated factors, Acta Orthop Belg 88 (2022) 103–111. [CrossRef]
- Z. Yao, T.-H. Z. Yao, T.-H. Lin, J. Pajarinen, T. Sato, S. Goodman, Chapter 12 - Host Response to Orthopedic Implants (Metals and Plastics), in: S.F. Badylak (Ed.), Host Response to Biomaterials, Academic Press, Oxford, 2015: pp. 315–373. [CrossRef]
- E. Gibon, Y. E. Gibon, Y. Takakubo, S. Zwingenberger, J. Gallo, M. Takagi, S.B. Goodman, Friend or foe? Inflammation and the foreign body response to orthopedic biomaterials, J Biomed Mater Res A 112 (2024) 1172–1187. [CrossRef]
- Y. Cong, Y. Y. Cong, Y. Wang, T. Yuan, Z. Zhang, J. Ge, Q. Meng, Z. Li, S. Sun, Macrophages in aseptic loosening: Characteristics, functions, and mechanisms, Front Immunol 14 (2023) 1122057. [CrossRef]
- J.M. Anderson, A. J.M. Anderson, A. Rodriguez, D.T. Chang, FOREIGN BODY REACTION TO BIOMATERIALS, Semin Immunol 20 (2008) 86–100. [CrossRef]
- C.J. Wilson, R.E. C.J. Wilson, R.E. Clegg, D.I. Leavesley, M.J. Pearcy, Mediation of biomaterial-cell interactions by adsorbed proteins: a review, Tissue Eng 11 (2005) 1–18. [CrossRef]
- J. Andersson, K.N. J. Andersson, K.N. Ekdahl, R. Larsson, U.R. Nilsson, B. Nilsson, C3 adsorbed to a polymer surface can form an initiating alternative pathway convertase, J Immunol 168 (2002) 5786–5791. [CrossRef]
- C. Sperling, M. C. Sperling, M. Fischer, M.F. Maitz, C. Werner, Blood coagulation on biomaterials requires the combination of distinct activation processes, Biomaterials 30 (2009) 4447–4456. [CrossRef]
- M. Fischer, C. M. Fischer, C. Sperling, C. Werner, Synergistic effect of hydrophobic and anionic surface groups triggers blood coagulation in vitro, J Mater Sci Mater Med 21 (2010) 931–937. [CrossRef]
- W.J. Hu, J.W. W.J. Hu, J.W. Eaton, T.P. Ugarova, L. Tang, Molecular basis of biomaterial-mediated foreign body reactions, Blood 98 (2001) 1231–1238. [CrossRef]
- M. Fischer, C. M. Fischer, C. Sperling, P. Tengvall, C. Werner, The ability of surface characteristics of materials to trigger leukocyte tissue factor expression, Biomaterials 31 (2010) 2498–2507. [CrossRef]
- P.M. Henson, R.B. P.M. Henson, R.B. Johnston, Tissue injury in inflammation. Oxidants, proteinases, and cationic proteins, J Clin Invest 79 (1987) 669–674. [CrossRef]
- R.I. Lehrer, T. R.I. Lehrer, T. Ganz, M.E. Selsted, B.M. Babior, J.T. Curnutte, Neutrophils and host defense, Ann Intern Med 109 (1988) 127–142. [CrossRef]
- H.L. Malech, J.I. H.L. Malech, J.I. Gallin, Current concepts: immunology. Neutrophils in human diseases, N Engl J Med 317 (1987) 687–694. [CrossRef]
- R.O. Hynes, Integrins: bidirectional, allosteric signaling machines, Cell 110 (2002) 673–687. [CrossRef]
- C.A. Lowell, G. C.A. Lowell, G. Berton, Integrin signal transduction in myeloid leukocytes, J Leukoc Biol 65 (1999) 313–320. [CrossRef]
- A.K. McNally, J.M. A.K. McNally, J.M. Anderson, Complement C3 participation in monocyte adhesion to different surfaces., Proc Natl Acad Sci U S A 91 (1994) 10119–10123.
- L. Tang, Mechanisms of fibrinogen domains: biomaterial interactions, J Biomater Sci Polym Ed 9 (1998) 1257–1266. [CrossRef]
- J. Zdolsek, J.W. J. Zdolsek, J.W. Eaton, L. Tang, Histamine release and fibrinogen adsorption mediate acute inflammatory responses to biomaterial implants in humans, J Transl Med 5 (2007) 31. [CrossRef]
- P. Scapini, J.A. P. Scapini, J.A. Lapinet-Vera, S. Gasperini, F. Calzetti, F. Bazzoni, M.A. Cassatella, The neutrophil as a cellular source of chemokines, Immunol Rev 177 (2000) 195–203. [CrossRef]
- Y. Hidaka, M. Y. Hidaka, M. Ito, K. Mori, H. Yagasaki, A.H. Kafrawy, Histopathological and immunohistochemical studies of membranes of deacetylated chitin derivatives implanted over rat calvaria, J Biomed Mater Res 46 (1999) 418–423. [CrossRef]
- P.J. VandeVord, H.W.T. P.J. VandeVord, H.W.T. Matthew, S.P. DeSilva, L. Mayton, B. Wu, P.H. Wooley, Evaluation of the biocompatibility of a chitosan scaffold in mice, J Biomed Mater Res 59 (2002) 585–590. [CrossRef]
- C.J. Park, N.P. C.J. Park, N.P. Gabrielson, D.W. Pack, R.D. Jamison, A.J. Wagoner Johnson, The effect of chitosan on the migration of neutrophil-like HL60 cells, mediated by IL-8, Biomaterials 30 (2009) 436–444. [CrossRef]
- S.D. Kobayashi, J.M. S.D. Kobayashi, J.M. Voyich, C. Burlak, F.R. DeLeo, Neutrophils in the innate immune response, Arch Immunol Ther Exp (Warsz) 53 (2005) 505–517.
- S. Yamashiro, H. S. Yamashiro, H. Kamohara, J.M. Wang, D. Yang, W.H. Gong, T. Yoshimura, Phenotypic and functional change of cytokine-activated neutrophils: inflammatory neutrophils are heterogeneous and enhance adaptive immune responses, J Leukoc Biol 69 (2001) 698–704.
- D.W. Gilroy, T. D.W. Gilroy, T. Lawrence, M. Perretti, A.G. Rossi, Inflammatory resolution: new opportunities for drug discovery, Nat Rev Drug Discov 3 (2004) 401–416. [CrossRef]
- C. Schlundt, T. C. Schlundt, T. El Khassawna, A. Serra, A. Dienelt, S. Wendler, H. Schell, N. van Rooijen, A. Radbruch, R. Lucius, S. Hartmann, G.N. Duda, K. Schmidt-Bleek, Macrophages in bone fracture healing: Their essential role in endochondral ossification, Bone 106 (2018) 78–89. [CrossRef]
- S.B. Goodman, E. S.B. Goodman, E. Gibon, J. Gallo, M. Takagi, Macrophage Polarization and the Osteoimmunology of Periprosthetic Osteolysis, Curr Osteoporos Rep 20 (2022) 43–52. [CrossRef]
- P.J. Murray, Macrophage Polarization, Annu Rev Physiol 79 (2017) 541–566. [CrossRef]
- T. Kon, T.J. T. Kon, T.J. Cho, T. Aizawa, M. Yamazaki, N. Nooh, D. Graves, L.C. Gerstenfeld, T.A. Einhorn, Expression of osteoprotegerin, receptor activator of NF-kappaB ligand (osteoprotegerin ligand) and related proinflammatory cytokines during fracture healing, J Bone Miner Res 16 (2001) 1004–1014. [CrossRef]
- Z. Xing, C. Z. Xing, C. Lu, D. Hu, Y. Yu, X. Wang, C. Colnot, M. Nakamura, Y. Wu, T. Miclau, R.S. Marcucio, Multiple roles for CCR2 during fracture healing, Dis Model Mech 3 (2010) 451–458. [CrossRef]
- L.C. Gerstenfeld, D.M. L.C. Gerstenfeld, D.M. Cullinane, G.L. Barnes, D.T. Graves, T.A. Einhorn, Fracture healing as a post-natal developmental process: molecular, spatial, and temporal aspects of its regulation, J Cell Biochem 88 (2003) 873–884. [CrossRef]
- P. Kolar, K. P. Kolar, K. Schmidt-Bleek, H. Schell, T. Gaber, D. Toben, G. Schmidmaier, C. Perka, F. Buttgereit, G.N. Duda, The early fracture hematoma and its potential role in fracture healing, Tissue Eng Part B Rev 16 (2010) 427–434. [CrossRef]
- E.-J. Lee, M. E.-J. Lee, M. Jain, S. Alimperti, Bone Microvasculature: Stimulus for Tissue Function and Regeneration, Tissue Eng Part B Rev 27 (2021) 313–329. [CrossRef]
- F. Loi, L.A. F. Loi, L.A. Córdova, J. Pajarinen, T. Lin, Z. Yao, S.B. Goodman, Inflammation, fracture and bone repair, Bone 86 (2016) 119–130. [CrossRef]
- M.E. Kotas, R. M.E. Kotas, R. Medzhitov, Homeostasis, inflammation, and disease susceptibility, Cell 160 (2015) 816–827. [CrossRef]
- C. Kasikara, A.C. C. Kasikara, A.C. Doran, B. Cai, I. Tabas, The role of non-resolving inflammation in atherosclerosis, J Clin Invest 128 (2018) 2713–2723. [CrossRef]
- C. Nathan, A. C. Nathan, A. Ding, Nonresolving inflammation, Cell 140 (2010) 871–882. [CrossRef]
- Pezone, F. Olivieri, M.V. Napoli, A. Procopio, E.V. Avvedimento, A. Gabrielli, Inflammation and DNA damage: cause, effect or both, Nat Rev Rheumatol 19 (2023) 200–211. [CrossRef]
- M. Couto, D.P. M. Couto, D.P. Vasconcelos, D.M. Sousa, B. Sousa, F. Conceição, E. Neto, M. Lamghari, C.J. Alves, The Mechanisms Underlying the Biological Response to Wear Debris in Periprosthetic Inflammation, Front. Mater. 7 (2020). [CrossRef]
- T.R. Green, J. T.R. Green, J. Fisher, M. Stone, B.M. Wroblewski, E. Ingham, Polyethylene particles of a ‘critical size’ are necessary for the induction of cytokines by macrophages in vitro, Biomaterials 19 (1998) 2297–2302. [CrossRef]
- T.R. Green, J. T.R. Green, J. Fisher, J.B. Matthews, M.H. Stone, E. Ingham, Effect of size and dose on bone resorption activity of macrophages by in vitro clinically relevant ultra high molecular weight polyethylene particles, J Biomed Mater Res 53 (2000) 490–497. [CrossRef]
- S.B. Goodman, J. S.B. Goodman, J. Gallo, Periprosthetic Osteolysis: Mechanisms, Prevention and Treatment, J Clin Med 8 (2019) 2091. [CrossRef]
- Wang, A. Essner, C. Stark, J.H. Dumbleton, Comparison of the size and morphology of UHMWPE wear debris produced by a hip joint simulator under serum and water lubricated conditions, Biomaterials 17 (1996) 865–871. [CrossRef]
- N.J. Hallab, K. N.J. Hallab, K. McAllister, M. Brady, M. Jarman-Smith, Macrophage reactivity to different polymers demonstrates particle size- and material-specific reactivity: PEEK-OPTIMA(®) particles versus UHMWPE particles in the submicron, micron, and 10 micron size ranges, J Biomed Mater Res B Appl Biomater 100 (2012) 480–492. [CrossRef]
- E. Ingham, J. E. Ingham, J. Fisher, The role of macrophages in osteolysis of total joint replacement, Biomaterials 26 (2005) 1271–1286. [CrossRef]
- R. Chiu, T. R. Chiu, T. Ma, R.L. Smith, S.B. Goodman, Ultrahigh molecular weight polyethylene wear debris inhibits osteoprogenitor proliferation and differentiation in vitro, J Biomed Mater Res A 89 (2009) 242–247. [CrossRef]
- C. Nich, Y. C. Nich, Y. Takakubo, J. Pajarinen, M. Ainola, A. Salem, T. Sillat, A.J. Rao, M. Raska, Y. Tamaki, M. Takagi, Y.T. Konttinen, S.B. Goodman, J. Gallo, Macrophages-Key cells in the response to wear debris from joint replacements, J Biomed Mater Res A 101 (2013) 3033–3045. [CrossRef]
- N.A. Athanasou, The pathobiology and pathology of aseptic implant failure, Bone Joint Res 5 (2016) 162–168. [CrossRef]
- Q. Gu, Q. Q. Gu, Q. Shi, H. Yang, The role of TLR and chemokine in wear particle-induced aseptic loosening, J Biomed Biotechnol 2012 (2012) 596870. [CrossRef]
- S. Landgraeber, M. S. Landgraeber, M. Jäger, J.J. Jacobs, N.J. Hallab, The pathology of orthopedic implant failure is mediated by innate immune system cytokines, Mediators Inflamm 2014 (2014) 185150. [CrossRef]
- K. Schroder, J. K. Schroder, J. Tschopp, The inflammasomes, Cell 140 (2010) 821–832. [CrossRef]
- T. Shiratori, Y. T. Shiratori, Y. Kyumoto-Nakamura, A. Kukita, N. Uehara, J. Zhang, K. Koda, M. Kamiya, T. Badawy, E. Tomoda, X. Xu, T. Yamaza, Y. Urano, K. Koyano, T. Kukita, IL-1β Induces Pathologically Activated Osteoclasts Bearing Extremely High Levels of Resorbing Activity: A Possible Pathological Subpopulation of Osteoclasts, Accompanied by Suppressed Expression of Kindlin-3 and Talin-1, J Immunol 200 (2018) 218–228. [CrossRef]
- T. Lin, Y. T. Lin, Y. Tamaki, J. Pajarinen, H.A. Waters, D.K. Woo, Z. Yao, S.B. Goodman, Chronic inflammation in biomaterial induced periprosthetic osteolysis: NF-κB as a therapeutic target, Acta Biomater 10 (2014) 10.1016/j.actbio.2013.09.034. [CrossRef]
- A.M. Kandahari, X. A.M. Kandahari, X. Yang, K.A. Laroche, A.S. Dighe, D. Pan, Q. Cui, A review of UHMWPE wear-induced osteolysis: the role for early detection of the immune response, Bone Res 4 (2016) 1–13. [CrossRef]
- E. Sukur, Y.E. E. Sukur, Y.E. Akman, Y. Ozturkmen, F. Kucukdurmaz, Particle Disease: A Current Review of the Biological Mechanisms in Periprosthetic Osteolysis After Hip Arthroplasty, Open Orthop J 10 (2016) 241–251. [CrossRef]
- P.E. Purdue, P. P.E. Purdue, P. Koulouvaris, H.G. Potter, B.J. Nestor, T.P. Sculco, The cellular and molecular biology of periprosthetic osteolysis, Clin Orthop Relat Res 454 (2007) 251–261. [CrossRef]
- J.M. Anderson, Chapter II.2.2 - Inflammation, Wound Healing, and the Foreign-Body Response, in: B.D. Ratner, A.S. Hoffman, F.J. Schoen, J.E. Lemons (Eds.), Biomaterials Science (Third Edition), Academic Press, 2013: pp. 503–512. [CrossRef]
- M. Takagi, Neutral proteinases and their inhibitors in the loosening of total hip prostheses, Acta Orthop Scand Suppl 271 (1996) 3–29.
- F. Yang, W. F. Yang, W. Wu, L. Cao, Y. Huang, Z. Zhu, T. Tang, K. Dai, Pathways of macrophage apoptosis within the interface membrane in aseptic loosening of prostheses, Biomaterials 32 (2011) 9159–9167. [CrossRef]
- F. Renò, M. F. Renò, M. Sabbatini, A. Massè, M. Bosetti, M. Cannas, Fibroblast apoptosis and caspase-8 activation in aseptic loosening, Biomaterials 24 (2003) 3941–3946. [CrossRef]
- S. Santavirta, Y.T. S. Santavirta, Y.T. Konttinen, V. Bergroth, A. Eskola, K. Tallroth, T.S. Lindholm, Aggressive granulomatous lesions associated with hip arthroplasty. Immunopathological studies, J Bone Joint Surg Am 72 (1990) 252–258.
- S.A. Solovieva, A. S.A. Solovieva, A. Ceponis, Y.T. Konttinen, M. Takagi, A. Suda, K.K. Eklund, T. Sorsa, S. Santavirta, Mast cells in loosening of totally replaced hips, Clin Orthop Relat Res (1996) 158–165.
- Z. Sheikh, P.J. Z. Sheikh, P.J. Brooks, O. Barzilay, N. Fine, M. Glogauer, Macrophages, Foreign Body Giant Cells and Their Response to Implantable Biomaterials, Materials (Basel) 8 (2015) 5671–5701. [CrossRef]
- Y.-C. Lu, T.-K. Y.-C. Lu, T.-K. Chang, T.-C. Lin, S.-T. Yeh, H.-W. Fang, C.-H. Huang, C.-H. Huang, The potential role of herbal extract Wedelolactone for treating particle-induced osteolysis: an in vivo study, J Orthop Surg Res 17 (2022) 335. [CrossRef]
- P. Aspenberg, A. P. Aspenberg, A. Anttila, Y.T. Konttinen, R. Lappalainen, S.B. Goodman, L. Nordsletten, S. Santavirta, Benign response to particles of diamond and SiC: bone chamber studies of new joint replacement coating materials in rabbits, Biomaterials 17 (1996) 807–812. [CrossRef]
- T.P. Schmalzried, M. T.P. Schmalzried, M. Jasty, W.H. Harris, Periprosthetic bone loss in total hip arthroplasty. Polyethylene wear debris and the concept of the effective joint space, J Bone Joint Surg Am 74 (1992) 849–863.
- M.T. Manley, J.A. M.T. Manley, J.A. D’Antonio, W.N. Capello, A.A. Edidin, Osteolysis: a disease of access to fixation interfaces, Clin Orthop Relat Res (2002) 129–137. [CrossRef]
- G. Pap, A. G. Pap, A. Machner, T. Rinnert, D. Hörler, R.E. Gay, H. Schwarzberg, W. Neumann, B.A. Michel, S. Gay, T. Pap, Development and characteristics of a synovial-like interface membrane around cemented tibial hemiarthroplasties in a novel rat model of aseptic prosthesis loosening, Arthritis Rheum 44 (2001) 956–963. [CrossRef]
- S. Banerjee, R. S. Banerjee, R. Pivec, K. Issa, B.H. Kapadia, H.S. Khanuja, M.A. Mont, Large-diameter femoral heads in total hip arthroplasty: an evidence-based review, Am J Orthop (Belle Mead NJ) 43 (2014) 506–512.
- P.C. Oparaugo, I.C. P.C. Oparaugo, I.C. Clarke, H. Malchau, P. Herberts, Correlation of wear debris-induced osteolysis and revision with volumetric wear-rates of polyethylene: a survey of 8 reports in the literature, Acta Orthop Scand 72 (2001) 22–28. [CrossRef]
- J. Shi, W. J. Shi, W. Zhu, S. Liang, H. Li, S. Li, Cross-Linked Versus Conventional Polyethylene for Long-Term Clinical Outcomes After Total Hip Arthroplasty: A Systematic Review and Meta-Analysis, J Invest Surg 34 (2021) 307–317. [CrossRef]
- B. Lambert, D. B. Lambert, D. Neut, H.C. van der Veen, S.K. Bulstra, Effects of vitamin E incorporation in polyethylene on oxidative degradation, wear rates, immune response, and infections in total joint arthroplasty: a review of the current literature, Int Orthop 43 (2019) 1549–1557. [CrossRef]
- H. McKellop, F.W. H. McKellop, F.W. Shen, B. Lu, P. Campbell, R. Salovey, Effect of sterilization method and other modifications on the wear resistance of acetabular cups made of ultra-high molecular weight polyethylene. A hip-simulator study, J Bone Joint Surg Am 82 (2000) 1708–1725. [CrossRef]
- E. Gomez-Barrena, J.-A. E. Gomez-Barrena, J.-A. Puertolas, L. Munuera, Y.T. Konttinen, Update on UHMWPE research From the bench to the bedside, Acta Orthopaedica (2008) 832–840. [CrossRef]
- E. Oral, O.K. E. Oral, O.K. Muratoglu, Vitamin E diffused, highly crosslinked UHMWPE: a review, Int Orthop 35 (2011) 215–223. [CrossRef]
- E. Oral, S.L. E. Oral, S.L. Rowell, O.K. Muratoglu, The effect of α-tocopherol on the oxidation and free radical decay in irradiated UHMWPE, Biomaterials 27 (2006) 5580–5587. [CrossRef]
- R.D. Valladares, C. R.D. Valladares, C. Nich, S. Zwingenberger, C. Li, K.R. Swank, E. Gibon, A.J. Rao, Z. Yao, S.B. Goodman, Toll-like receptors-2 and 4 are overexpressed in an experimental model of particle-induced osteolysis, J Biomed Mater Res A 102 (2014) 3004–3011. [CrossRef]
- R. Maitra, C.C. R. Maitra, C.C. Clement, B. Scharf, G.M. Crisi, S. Chitta, D. Paget, P.E. Purdue, N. Cobelli, L. Santambrogio, Endosomal damage and TLR2 mediated inflammasome activation by alkane particles in the generation of aseptic osteolysis, Mol Immunol 47 (2009) 175–184. [CrossRef]
- C. Vermes, R. C. Vermes, R. Chandrasekaran, J.J. Jacobs, J.O. Galante, K.A. Roebuck, T.T. Glant, The effects of particulate wear debris, cytokines, and growth factors on the functions of MG-63 osteoblasts, J Bone Joint Surg Am 83 (2001) 201–211. [CrossRef]
- J.T. Hodrick, E.P. J.T. Hodrick, E.P. Severson, D.S. McAlister, B. Dahl, A.A. Hofmann, Highly crosslinked polyethylene is safe for use in total knee arthroplasty, Clin Orthop Relat Res 466 (2008) 2806–2812. [CrossRef]
- D.A. Bichara, E. D.A. Bichara, E. Malchau, N.H. Sillesen, S. Cakmak, G.P. Nielsen, O.K. Muratoglu, Vitamin E-diffused highly cross-linked UHMWPE particles induce less osteolysis compared to highly cross-linked virgin UHMWPE particles in vivo, J ARTHROPLASTY 29 (2014) 232–7. [CrossRef]
- W. Chen, D.A. W. Chen, D.A. Bichara, J. Suhardi, P. Sheng, O.K. Muratoglu, Effects of vitamin E-diffused highly cross-linked UHMWPE particles on inflammation, apoptosis and immune response against S. aureus, Biomaterials 143 (2017) 46–56. [CrossRef]
- F. Renò, P. F. Renò, P. Bracco, F. Lombardi, F. Boccafoschi, L. Costa, M. Cannas, The induction of MMP-9 release from granulocytes by vitamin E in UHMWPE, Biomaterials 25 (2004) 995–1001. [CrossRef]
- M.A. Terkawi, M. M.A. Terkawi, M. Hamasaki, D. Takahashi, M. Ota, K. Kadoya, T. Yutani, K. Uetsuki, T. Asano, T. Irie, R. Arai, T. Onodera, M. Takahata, N. Iwasaki, Transcriptional profile of human macrophages stimulated by ultra-high molecular weight polyethylene particulate debris of orthopedic implants uncovers a common gene expression signature of rheumatoid arthritis, Acta Biomater 65 (2018) 417–425. [CrossRef]
- J. Quinn, C. J. Quinn, C. Joyner, J.T. Triffitt, N.A. Athanasou, Polymethylmethacrylate-induced inflammatory macrophages resorb bone, The Journal of Bone & Joint Surgery British Volume 74-B (1992) 652–658. [CrossRef]
- Sabokbar, R. Pandey, J.M. Quinn, N.A. Athanasou, Osteoclastic differentiation by mononuclear phagocytes containing biomaterial particles, Arch Orthop Trauma Surg 117 (1998) 136–140. [CrossRef]
- J.I. Pearl, T. J.I. Pearl, T. Ma, A.R. Irani, Z. Huang, W.H. Robinson, R.L. Smith, S.B. Goodman, Role of the Toll-like receptor pathway in the recognition of orthopedic implant wear-debris particles, Biomaterials 32 (2011) 5535–5542. [CrossRef]
- J.K. Antonios, Z. J.K. Antonios, Z. Yao, C. Li, A.J. Rao, S.B. Goodman, Macrophage polarization in response to wear particles in vitro, Cell Mol Immunol 10 (2013) 471–482. [CrossRef]
- Z. Huang, T. Z. Huang, T. Ma, P.-G. Ren, R.L. Smith, S.B. Goodman, Effects of orthopedic polymer particles on chemotaxis of macrophages and mesenchymal stem cells, J Biomed Mater Res A 94 (2010) 1264–1269. [CrossRef]
- L.A.J. O’Neill, D. L.A.J. O’Neill, D. Golenbock, A.G. Bowie, The history of Toll-like receptors — redefining innate immunity, Nat Rev Immunol 13 (2013) 453–460. [CrossRef]
- L. Burton, D. L. Burton, D. Paget, N.B. Binder, K. Bohnert, B.J. Nestor, T.P. Sculco, L. Santambrogio, F.P. Ross, S.R. Goldring, P.E. Purdue, Orthopedic wear debris mediated inflammatory osteolysis is mediated in part by NALP3 inflammasome activation, J Orthop Res 31 (2013) 73–80. [CrossRef]
- Y. Abu-Amer, I. Y. Abu-Amer, I. Darwech, J.C. Clohisy, Aseptic loosening of total joint replacements: mechanisms underlying osteolysis and potential therapies, Arthritis Res Ther 9 Suppl 1 (2007) S6. [CrossRef]
- M.S. Caicedo, L. M.S. Caicedo, L. Samelko, K. McAllister, J.J. Jacobs, N.J. Hallab, Increasing both CoCrMo-alloy Particle Size and Surface Irregularity Induces Increased Macrophage Inflammasome Activation In vitro Potentially through Lysosomal Destabilization Mechanisms, J Orthop Res 31 (2013) 1633–1642. [CrossRef]
- L. Samelko, S. L. Samelko, S. Landgraeber, K. McAllister, J. Jacobs, N.J. Hallab, Cobalt Alloy Implant Debris Induces Inflammation and Bone Loss Primarily through Danger Signaling, Not TLR4 Activation: Implications for DAMP-ening Implant Related Inflammation, PLoS One 11 (2016) e0160141. [CrossRef]
- Oblak, J. Pohar, R. Jerala, MD-2 Determinants of Nickel and Cobalt-Mediated Activation of Human TLR4, PLOS ONE 10 (2015) e0120583. [CrossRef]
- S.M. Kurtz, D.T. S.M. Kurtz, D.T. Holyoak, R. Trebše, T.M. Randau, A.A. Porporati, R.L. Siskey, Ceramic Wear Particles: Can They Be Retrieved In Vivo and Duplicated In Vitro?, J Arthroplasty 38 (2023) 1869–1876. [CrossRef]
- Catelas, A. Petit, D.J. Zukor, R. Marchand, L. Yahia, O.L. Huk, Induction of macrophage apoptosis by ceramic and polyethylene particles in vitro, Biomaterials 20 (1999) 625–630. [CrossRef]
- D. Bylski, C. D. Bylski, C. Wedemeyer, J. Xu, T. Sterner, F. Löer, M. von Knoch, Alumina ceramic particles, in comparison with titanium particles, hardly affect the expression of RANK-, TNF-α-, and OPG-mRNA in the THP-1 human monocytic cell line, Journal of Biomedical Materials Research Part A 89A (2009) 707–716. [CrossRef]
- M. Lucarelli, A.M. M. Lucarelli, A.M. Gatti, G. Savarino, P. Quattroni, L. Martinelli, E. Monari, D. Boraschi, Innate defence functions of macrophages can be biased by nano-sized ceramic and metallic particles, Eur Cytokine Netw 15 (2004) 339–346.
- Y.-C. Ha, S.-Y. Y.-C. Ha, S.-Y. Kim, H.J. Kim, J.J. Yoo, K.-H. Koo, Ceramic liner fracture after cementless alumina-on-alumina total hip arthroplasty, Clin Orthop Relat Res 458 (2007) 106–110. [CrossRef]
- M.G. Zywiel, S.A. M.G. Zywiel, S.A. Sayeed, A.J. Johnson, T.P. Schmalzried, M.A. Mont, Survival of hard-on-hard bearings in total hip arthroplasty: a systematic review, Clin Orthop Relat Res 469 (2011) 1536–1546. [CrossRef]
- S. Hasan, P. S. Hasan, P. van Schie, B.L. Kaptein, J.W. Schoones, P.J. Marang-van de Mheen, R.G.H.H. Nelissen, Biomarkers to discriminate between aseptic loosened and stable total hip or knee arthroplasties: a systematic review, EFORT Open Rev 9 (2024) 25–39. [CrossRef]
- Biomarkers Definitions Working Group., Biomarkers and surrogate endpoints: preferred definitions and conceptual framework, Clin Pharmacol Ther 69 (2001) 89–95. [CrossRef]
- R.K. Chaganti, E. R.K. Chaganti, E. Purdue, T.P. Sculco, L.A. Mandl, Elevation of serum tumor necrosis factor α in patients with periprosthetic osteolysis: a case-control study, Clin Orthop Relat Res 472 (2014) 584–589. [CrossRef]
- Z. Hundrić-Haspl, M. Z. Hundrić-Haspl, M. Pecina, M. Haspl, M. Tomicic, I. Jukic, Plasma cytokines as markers of aseptic prosthesis loosening, Clin Orthop Relat Res 453 (2006) 299–304. [CrossRef]
- W. Wu, X. W. Wu, X. Zhang, C. Zhang, T. Tang, W. Ren, K. Dai, Expansion of CD14+CD16+ peripheral monocytes among patients with aseptic loosening, Inflamm Res 58 (2009) 561–570. [CrossRef]
- Moreschini, S. Fiorito, L. Magrini, F. Margheritini, L. Romanini, Markers of connective tissue activation in aseptic hip prosthetic loosening, J Arthroplasty 12 (1997) 695–703. [CrossRef]
- T. He, W. T. He, W. Wu, Y. Huang, X. Zhang, T. Tang, K. Dai, Multiple biomarkers analysis for the early detection of prosthetic aseptic loosening of hip arthroplasty, Int Orthop 37 (2013) 1025–1031. [CrossRef]
- E. López-Anglada, J. E. López-Anglada, J. Collazos, A.H. Montes, L. Pérez-Is, I. Pérez-Hevia, S. Jiménez-Tostado, T. Suárez-Zarracina, V. Alvarez, E. Valle-Garay, V. Asensi, IL-1 β gene (+3954 C/T, exon 5, rs1143634) and NOS2 (exon 22) polymorphisms associate with early aseptic loosening of arthroplasties, Sci Rep 12 (2022) 18382. [CrossRef]
- F. Tang, X. F. Tang, X. Liu, H. Jiang, H. Wu, S. Hu, J. Zheng, H. Guo, L. Yan, C. Xu, Y. Lin, J. Lin, J. Zhao, Biomarkers for early diagnosis of aseptic loosening after total hip replacement, (2016).
- S.K. Trehan, L. S.K. Trehan, L. Zambrana, J.E. Jo, E. Purdue, A. Karamitros, J.T. Nguyen, J.M. Lane, An Alternative Macrophage Activation Pathway Regulator, CHIT1, May Provide a Serum and Synovial Fluid Biomarker of Periprosthetic Osteolysis, HSS J 14 (2018) 148–152. [CrossRef]
- Morakis, S. Tournis, E. Papakitsou, I. Donta, G.P. Lyritis, Decreased tibial bone strength in postmenopausal women with aseptic loosening of cemented femoral implants measured by peripheral quantitative computed tomography (pQCT), J Long Term Eff Med Implants 21 (2011) 291–297. [CrossRef]
- J.M. Wilkinson, A.J. J.M. Wilkinson, A.J. Hamer, A. Rogers, I. Stockley, R. Eastell, Bone mineral density and biochemical markers of bone turnover in aseptic loosening after total hip arthroplasty, J Orthop Res 21 (2003) 691–696. [CrossRef]
- J. Antoniou, O. J. Antoniou, O. Huk, D. Zukor, D. Eyre, M. Alini, Collagen crosslinked N-telopeptides as markers for evaluating particulate osteolysis: a preliminary study, J Orthop Res 18 (2000) 64–67. [CrossRef]
- L. Savarino, S. L. Savarino, S. Avnet, M. Greco, A. Giunti, N. Baldini, Potential role of tartrate-resistant acid phosphatase 5b (TRACP 5b) as a surrogate marker of late loosening in patients with total hip arthroplasty: a cohort study, J Orthop Res 28 (2010) 887–892. [CrossRef]
- N.R. Lawrence, R.L. N.R. Lawrence, R.L. Jayasuriya, F. Gossiel, J.M. Wilkinson, Diagnostic accuracy of bone turnover markers as a screening tool for aseptic loosening after total hip arthroplasty, Hip Int 25 (2015) 525–530. [CrossRef]
- M. Ovrenovits, E.E. M. Ovrenovits, E.E. Pakos, G. Vartholomatos, N.K. Paschos, T.A. Xenakis, G.I. Mitsionis, Flow cytometry as a diagnostic tool for identifying total hip arthroplasty loosening and differentiating between septic and aseptic cases, Eur J Orthop Surg Traumatol 25 (2015) 1153–1159. [CrossRef]
- S. Papagiannis, I. S. Papagiannis, I. Tatani, G. Kyriakopoulos, Z. Kokkalis, P. Megas, C. Stathopoulos, K. Grafanaki, J. Lakoumentas, Alterations in Small Non-coding MicroRNAs (miRNAs) and the Potential Role in the Development of Aseptic Loosening After Total Hip Replacement: Study Protocol for an Observational, Cross-Sectional Study, Cureus 16 (2024) e72179. [CrossRef]
- R. Minaei Noshahr, F. R. Minaei Noshahr, F. Amouzadeh Omrani, A. Yadollahzadeh Chari, M. Salehpour Roudsari, F. Madadi, S. Shakeri Jousheghan, A. Manafi-Rasi, MicroRNAs in Aseptic Loosening of Prosthesis: Pathophysiology and Potential Therapeutic Approaches, Arch Bone Jt Surg 12 (2024) 612–621. [CrossRef]
- M.H.A. Malik, F. M.H.A. Malik, F. Jury, A. Bayat, W.E.R. Ollier, P.R. Kay, Genetic susceptibility to total hip arthroplasty failure: a preliminary study on the influence of matrix metalloproteinase 1, interleukin 6 polymorphisms and vitamin D receptor, Annals of the Rheumatic Diseases 66 (2007) 1116–1120. [CrossRef]
- H.F. Alotaibi, S. H.F. Alotaibi, S. Perni, P. Prokopovich, Nanoparticle-based model of anti-inflammatory drug releasing LbL coatings for uncemented prosthesis aseptic loosening prevention, Int J Nanomedicine 14 (2019) 7309–7322. [CrossRef]
- B.H. van Duren, A.M. B.H. van Duren, A.M. Firth, R. Berber, H.E. Matar, P.J. James, B.V. Bloch, Revision Rates for Aseptic Loosening in the Obese Patient: A Comparison Between Stemmed, Uncemented, and Unstemmed Tibial Total Knee Arthroplasty Components, Arthroplasty Today 32 (2025) 101621. [CrossRef]
- J.T. Layson, D. J.T. Layson, D. Hameed, J.A. Dubin, M.C. Moore, M. Mont, G.R. Scuderi, Patients with Osteoporosis Are at Higher Risk for Periprosthetic Femoral Fractures and Aseptic Loosening Following Total Hip Arthroplasty, Orthop Clin North Am 55 (2024) 311–321. [CrossRef]
- S.K. Patel, J.E. S.K. Patel, J.E. Dilley, A. Carlone, E.R. Deckard, R.M. Meneghini, K.A. Sonn, Effect of Tobacco Use on Radiolucent Lines in Modern Cementless Total Knee Arthroplasty Tibial Components, Arthroplasty Today 19 (2023). [CrossRef]
- S. Teng, C. S. Teng, C. Yi, C. Krettek, M. Jagodzinski, Smoking and Risk of Prosthesis-Related Complications after Total Hip Arthroplasty: A Meta-Analysis of Cohort Studies, PLOS ONE 10 (2015) e0125294. [CrossRef]
- B.H. Kapadia, K. B.H. Kapadia, K. Issa, R. Pivec, P.M. Bonutti, M.A. Mont, Tobacco use may be associated with increased revision and complication rates following total hip arthroplasty, J Arthroplasty 29 (2014) 777–780. [CrossRef]
- M. Khatod, G. M. Khatod, G. Cafri, R.S. Namba, M.C.S. Inacio, E.W. Paxton, Risk Factors for Total Hip Arthroplasty Aseptic Revision, The Journal of Arthroplasty 29 (2014) 1412–1417. [CrossRef]
- D. Apostu, O. D. Apostu, O. Lucaciu, C. Berce, D. Lucaciu, D. Cosma, Current methods of preventing aseptic loosening and improving osseointegration of titanium implants in cementless total hip arthroplasty: a review, J Int Med Res 46 (2018) 2104–2119. [CrossRef]
- S. Safavi, Y. S. Safavi, Y. Yu, D.L. Robinson, H.A. Gray, D.C. Ackland, P.V.S. Lee, Additively manufactured controlled porous orthopedic joint replacement designs to reduce bone stress shielding: a systematic review, Journal of Orthopaedic Surgery and Research 18 (2023) 42. [CrossRef]
- D. Apostu, O. D. Apostu, O. Lucaciu, C. Berce, D. Lucaciu, D. Cosma, Current methods of preventing aseptic loosening and improving osseointegration of titanium implants in cementless total hip arthroplasty: a review, J Int Med Res 46 (2018) 2104–2119. [CrossRef]
- F. De Meo, G. F. De Meo, G. Cacciola, V. Bellotti, A. Bruschetta, P. Cavaliere, Trabecular Titanium acetabular cups in hip revision surgery: mid-term clinical and radiological outcomes, Hip Int 28 (2018) 61–65. [CrossRef]
- G. Cacciola, F. G. Cacciola, F. Giustra, F. Bosco, F. De Meo, A. Bruschetta, I. De Martino, S. Risitano, L. Sabatini, A. Massè, P. Cavaliere, Trabecular titanium cups in hip revision surgery: a systematic review of the literature, Ann Jt 8 (2023) 36. [CrossRef]
- Y.-L. Chen, T. Y.-L. Chen, T. Lin, A. Liu, M.-M. Shi, B. Hu, Z. Shi, S.-G. Yan, Does hydroxyapatite coating have no advantage over porous coating in primary total hip arthroplasty? A meta-analysis, Journal of Orthopaedic Surgery and Research 10 (2015) 21. [CrossRef]
- B.M. Isaacson, S. B.M. Isaacson, S. Jeyapalina, Osseointegration: a review of the fundamentals for assuring cementless skeletal fixation, ORR 6 (2014) 55–65. [CrossRef]
- K.L. McCormick, M.A. K.L. McCormick, M.A. Mastroianni, N.L. Kolodychuk, C.L. Herndon, R.P. Shah, H.J. Cooper, N.O. Sarpong, Complications and Survivorship After Aseptic Revision Total Hip Arthroplasty: Is There a Difference by Surgical Approach?, J Arthroplasty 40 (2025) 203–207. [CrossRef]
- V. Lindgren, G. V. Lindgren, G. Garellick, J. Kärrholm, P. Wretenberg, The type of surgical approach influences the risk of revision in total hip arthroplasty: a study from the Swedish Hip Arthroplasty Register of 90,662 total hipreplacements with 3 different cemented prostheses, Acta Orthop 83 (2012) 559–565. [CrossRef]
- F. Birrell, S. F. Birrell, S. Lohmander, Non-steroidal anti-inflammatory drugs after hip replacement, BMJ 333 (2006) 507–508. [CrossRef]
- G. Friedl, R. G. Friedl, R. Radl, C. Stihsen, P. Rehak, R. Aigner, R. Windhager, The effect of a single infusion of zoledronic acid on early implant migration in total hip arthroplasty. A randomized, double-blind, controlled trial, J Bone Joint Surg Am 91 (2009) 274–281. [CrossRef]
Figure 1.
Inflammatory and Foreign Body Reactions Leading to Aseptic Loosening.
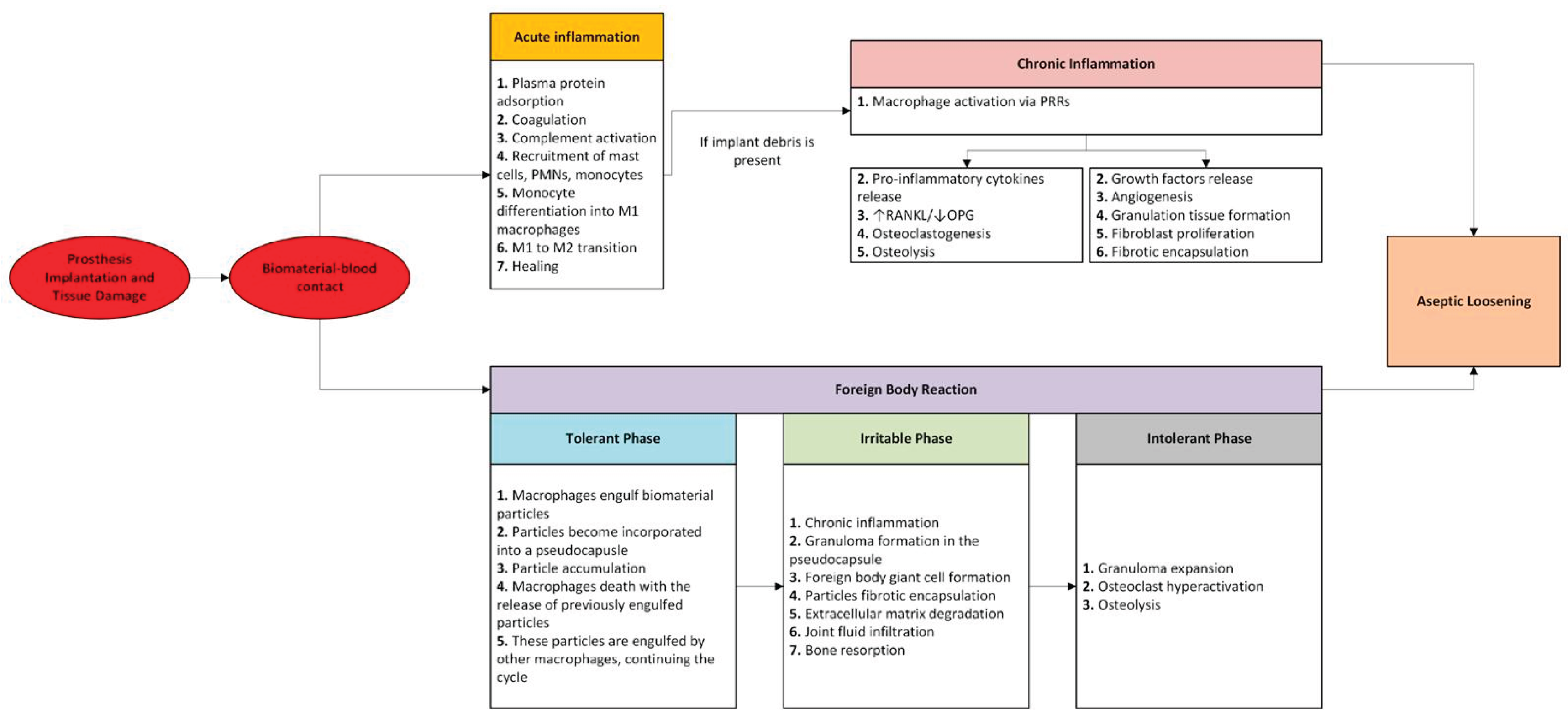
Figure 2.
Macrophages react to implant wear particles by engaging Toll-like receptors (TLRs) or internalizing debris via phagocytosis. This activates nuclear factor kappa B (NF-κB), triggering the release of pro-inflammatory cytokines (TNF-α, IL-1, IL-6, PGE-2), growth factors (M-CSF), osteoclast-promoting factors (RANKL), and chemokines (IL-8, MIP-1α, MCP-1). These signals recruit more macrophages and osteoclast precursors, driving inflammation, bone resorption, osteolysis and implant failure. This figure was created with Servier Medical Art (https://smart.servier.com) and NIH Bioart (https://bioart.niaid.nih.gov/).
Figure 2.
Macrophages react to implant wear particles by engaging Toll-like receptors (TLRs) or internalizing debris via phagocytosis. This activates nuclear factor kappa B (NF-κB), triggering the release of pro-inflammatory cytokines (TNF-α, IL-1, IL-6, PGE-2), growth factors (M-CSF), osteoclast-promoting factors (RANKL), and chemokines (IL-8, MIP-1α, MCP-1). These signals recruit more macrophages and osteoclast precursors, driving inflammation, bone resorption, osteolysis and implant failure. This figure was created with Servier Medical Art (https://smart.servier.com) and NIH Bioart (https://bioart.niaid.nih.gov/).
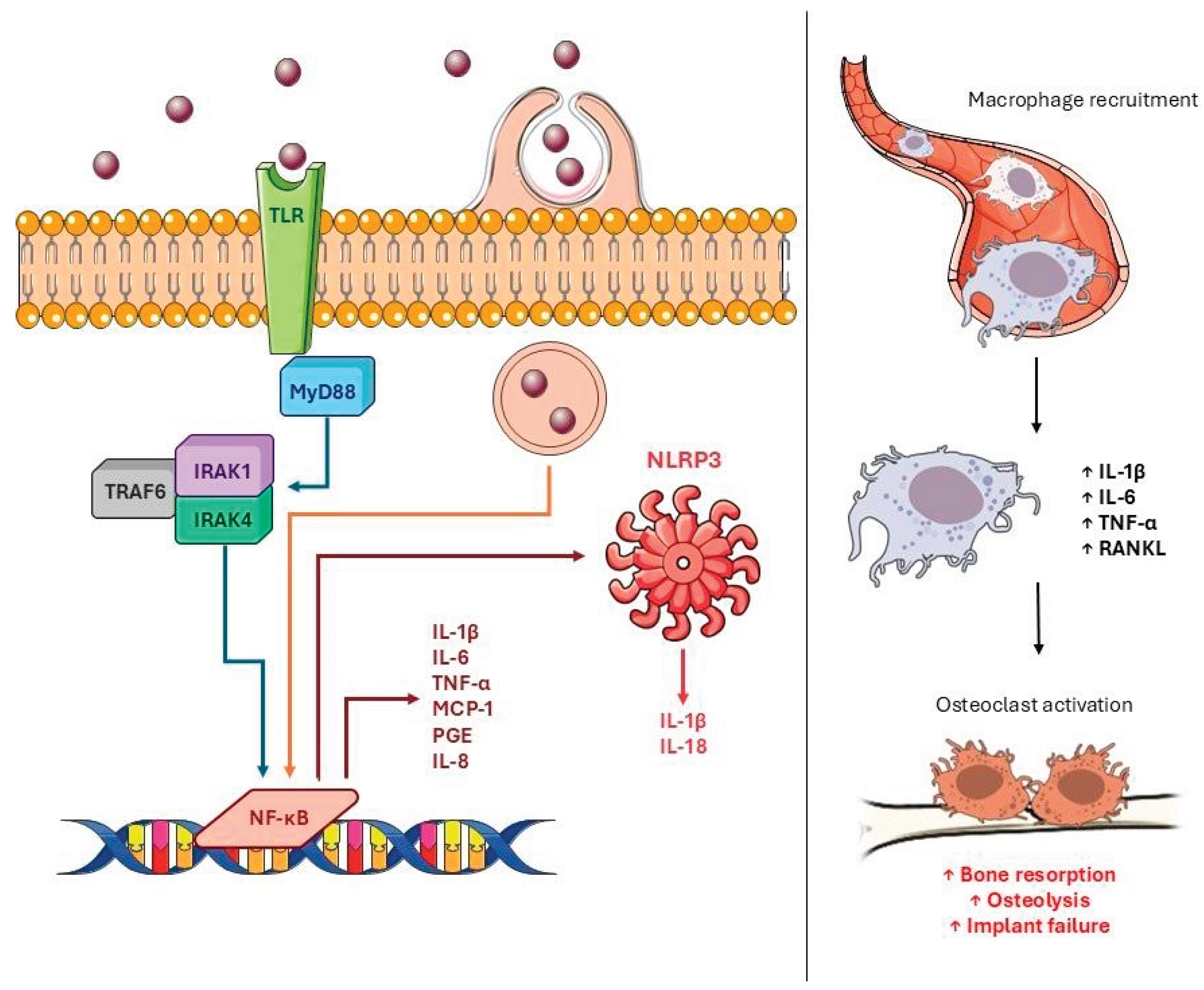

Table 1.
Biomarkers in Aseptic Loosening (AL).
| Category | Biomarkers | Levels in AL Patients | Role | Sample | References |
|---|---|---|---|---|---|
| Inflammatory Biomarkers | TNF-α, IL-1β, IL-6, IL-8, CD14+CD16+ monocytes, MCP-1, CCL18 | High | Indicative of an active inflammatory response that promotes the recruitment and activation of immune cells, contributing to bone destruction. | Blood, synovial fluid | [109,110,111,112,113,114,115,116] |
| Bone Metabolism | RANKL, CTX, NTX, TRAP5b, ICTP, | High | Represent the altered balance between bone formation and resorption; increased resorption and reduced bone formation, typical of AL | Blood, urine | [113,115,116,117,118,119,120,121] |
| Osteocalcin, PiCP | Low | ||||
| Matrix Degradation | Hyaluronic acid, CHIT1, CD18, CD11b, CD11c | High | Signals of extracellular matrix degradation and cellular activation, indicative of tissue damage and local immune response. | Blood, synovial fluid | [112,116,122] |
| MicroRNA | miR-21, miR-92a, miR-106b, miR-130, miR-135, miR-155 | High | Involved in the regulation of inflammatory processes and bone remodeling, contributing to the altered balance between osteoresorption and formation. | Blood | [123,124] |
| miR-29 | Low | ||||
| Genetic Factors | SNPs in NOS2 (AA genotype), IL-1β (TT genotype), and MMP1 | Associated with increased risk | Genetically predispose to the establishment of an accentuated inflammatory response and aberrant bone remodeling, favoring the development of AL | Blood | [114,125] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



