
Submitted:
25 July 2025
Posted:
29 July 2025
You are already at the latest version
Abstract
Background/Objectives: Urinary incontinence (UI) is increasingly reported among young nulliparous women, especially those engaged in high-impact sports. This may increase the risk of developing stress urinary incontinence (SUI) later in life. This scoping review aims to synthesize current evidence on UI in gymnasts, identify the gymnastics modalities with the highest prevalence of UI, and examine the outcomes measures and interventions considered for UI. Methods: A scoping review was conducted using the following databases: PubMed, Cochrane, Science Direct, Scielo, EBSCO, PEDro and NIH. Studies published in English or Portuguese between January 2012 and May 2023 were included. Review articles, qualitative studies and conferences abstracts were excluded. Results: Out of 169 identified studies, 4 were included. SUI emerged as the most prevalent type of UI, particularly in artistic and trampoline modalities. All the studies used the ICIQ-UI-SF to assess UI. Reported outcomes UI and SUI prevalence of, impact on quality of life and athletic performance, as well as knowledge about UI and pelvic floor. No studies investigated interventions for UI. Conclusions: The prevalence of SUI is high among gymnasts, especially in artistic and trampoline disciplines. Although there is outcome heterogeneity across studies, all used the ICIQ-UI-SF. There is a critical gap regarding interventions for UI in this population.
Keywords:
athletes
; exercise
; gymnastic
; pelvic floor dysfunction
; pelvic floor muscles
1. Introduction
Urinary incontinence (UI) is defined by the International Continence Society (ICS) in 2009 as the involuntary loss of urine [1]. Different types of UI have been described, the most prevalent being stress urinary incontinence (SUI), urge urinary incontinence (UUI) and mixed urinary incontinence (MUI). SUI is defined as the complaint of involuntary loss of urine with exertion or physical activity, including sporting activities or the act of sneezing or coughing [2]. In this case, the intravesical pressure exceeds the maximum urethral pressure in the absence of contraction of the detrusor muscle. UUI is associated with an urgent urge to urinate, where there are involuntary contractions of the detrusor muscle, which is responsible for the symptoms. Mixed urinary incontinence (MUI) combines the two types mentioned above, i.e. leakage associated with urgency and increased intra-abdominal pressure [3]. The condition occurs in both sexes, but is more common in women [4]. There are various repercussions for daily activities, social interactions and women's own perception of their health. Social and mental wellbeing, social isolation, low self-esteem and depression significantly affect quality of life, with psychological, physical, professional, sexual and social consequences [3]. In a systematic review of worldwide studies, the prevalence of UI ranges from 5% to 70%, with most studies reporting a prevalence of any type of UI of between 25% and 45% [5]. An epidemiological study carried out in the Portuguese population in adults over 40 in 2008 by the Faculty of Medicine of the University of Porto in conjunction with the Portuguese Association of Urology (APU) and the Portuguese Association of Neuro-Urogynecology (APNUG) found a prevalence of UI of 15.1% in the population, 21.4% in women and 7.6% in men [6,7]. This prevalence tends to increase with age [8]. However, this problem also affects young, physically active women, even in the absence of risk factors [9]. In fact, studies show an increase in the prevalence of UI in young, nulliparous women [10,11], especially when they practice high-impact sports [11,12,13,14]. The more frequent the impact associated with increased intra-abdominal pressure, the greater the need for containment and support of the pelvic organs by the pelvic floor muscles, which must be trained to preserve their function [15,16]. Prevalence varies not only with impact, but also with exercise intensity. In fact, scientific evidence shows that high-impact sports and participation in long-term competitions are associated with a higher prevalence of SUI in nulliparous women, especially trampolinists [15,17,18,19]. However, the majority of athletes leak urine during training and not during competitions (95.2% vs 51.2% respectively), probably due to the higher level of catecholamines, affecting the urethral alpha receptors, maintaining urethral closure during competitions [18,20]. In stressful situations, the sympathetic nervous system and the medulla of the adrenal gland release mediators: catecholamines (norepinephrine and epinephrine). This response to stressors can be modified by the characteristics of the stressor stimulus, and the ratio of epinephrine to norepinephrine varies depending on the nature of the stress. Mental stress mainly increases the level of epinephrine, while the combination of physical and mental exertion stimulates the production of norepinephrine, the main agonist of urethral alpha receptors [21,22]. Therefore, and based on what has been described, the aim of this scoping review was to summarise current evidence on the prevalence of UI among adolescent and adult female gymnasts, to identify which gymnastics disciplines have the highest prevalence of UI, and to describe the assessment instruments, reported outcomes, and any interventions studied. The following research questions guided this review: (1) Which gymnastics disciplines have the highest prevalence of UI in female athletes?; (2) What instruments and outcomes are used to assess UI in this population, and what interventions have been reported?
2. Materials and Methods
This scoping review was carried out in accordance with the guidelines Preferred Reporting Items for Systematic review and Meta-Analyses (PRISMA) [23] and the methodology proposed by Joanna Briggs Institute (JBI) Manual for evidence synthesis (2020) [24].
2.1. Eligibility Criteria
The eligibility criteria were established using the acronym PCC (Population, Concept and Context) in accordance with the JBI methodology [24].
- Population: adolescent and adult female gymnasts.
- Concept: evaluation of stress urinary incontinence in gymnasts.
- Context: to assess incontinence in a training environment, in a sports context.
2.2. Evidence Sources
Primary and secondary studies were considered in this scoping review. Review studies (literature and systematic), qualitative studies and abstracts of papers presented at congresses/conferences were excluded. Studies published in English and Portuguese were considered. Only studies published from 1 January 2012 to 31 May 2023 were included. The search for this information was carried out between April and May 2023.
2.3. Research Strategy
The search was carried out in the following databases: PubMed, Cochrane, Science Direct, Scielo, EBSCO, PEDro, NIH (ClinicalTrials.gov).based on the following research strategy: (“woman” OR “female” OR “athlete”) AND (“gymnastic” OR “trampoline” OR “acrobatic” OR “high impact sport”) AND (“urinary incontinence” OR “stress urinary incontinence” OR “pelvic floor disorders” OR “loss of urine” OR “urine leakage”) AND (“prevalence” OR “treatment” OR “knowledge” OR “impact” OR “quality of life” OR “prevention”). Depending on each database, adaptations were made to the research expression, as can be seen in Table 1.
2.4. Evidence Selection
The collection was carried out by just one reviewer (AH). After the initial database searches, grey literature was searched using Google Scholar. After the final selection, the principal investigator independently extracted the information from the articles eligible for data synthesis. The 2nd researcher (SL) was always present throughout the process, also analyzing independently and together whenever there were doubts about whether to include the articles. The most relevant data extraction included the author(s), the year of publication, the type of study, the objective(s) of the study, the characteristics of the participants, the instruments and outcomes. The extracted results were presented and analyzed using a table of the type “Data Charting” [24]. This selection process took account of the PCC and is detailed in the flowchart PRISMA-ScR (Figure 1). The results extracted are described in relation to the questions outlined in the context of the study's objective.
2.5. Analysis and Results Presentation
Results are summarized in tabular format, presenting systematically extracted data categories that address the study objectives and research questions. The data synthesis incorporates key characteristics from included studies to facilitate comprehensive analysis.
3. Results
3.1. Selection of Evidence Sources
The initial search strategy identified 169 potentially relevant studies (PubMed: 7 articles, Science Direct: 84 articles, PEDro: 6 articles, Cochrane: 10 articles, NIH: 23 articles, Scielo: 31 articles, ESBCO: 8 articles). After a search on Google Scholar, 2 additional studies were found. This was followed by the removal of 8 duplicate studies. A total of 101 studies were excluded because they were not available in full text (PubMed: 1, Science Direct: 73, Cochrane: 5, NIH: 20, ESBCO: 2) and 3 because they were not published in English or Portuguese (Scielo: 2, EBSCO: 1). A total of 59 references were assessed by title and abstract. Subsequently, 8 were excluded because they were not eligible in terms of the type of study (PubMed: 2, Science Direct: 1, PEDro: 3, Scielo; 2). 51 articles were eligible for full-text evaluation. Of these, 47 did not meet the PCC inclusion criteria; in fact, 23 studies were excluded in terms of population (PubMed: 1, Science Direct: 3, PEDro: 1, Cochrane: 2, NIH: 2, Scielo: 12, EBSCO: 2), 21 in terms of concept (PubMed: 1, Science Direct: 4, PEDro: 1, Scielo: 14, EBSCO: 1) and 3 in terms of context (Science Direct: 1, PEDro: 1, Scielo: 1). After selection, 4 studies were selected for this scoping review, in the PubMed (n = 2) [11,27], Science Direct and Google Scholar (n = 2) databases [25,26] respectively. After screening, four studies were selected for this scoping review, identified through the databases PubMed (n = 2) [11,27], ScienceDirect, and Google Scholar (n = 2) [25,26], respectively.
After extracting the data, a narrative synthesis was carried out to describe the articles included in terms of the type of study, intervention and the type of participants included in the study. Table 2 shows the characteristics of eligible studies.
3.2. Types of Study
After the study selection process (Table 2), four studies were included in the present scoping review: three cross-sectional studies [11,25,26] and one cohort study [27]. Regarding the year of publication, these studies were published between 2015 and 2022, with all having been published within the last 10 years. All studies were published in English.
3.3. Participant characteristics
The total sample across the four studies comprised 611 participants, all of whom were female. Two studies included exclusively gymnastics disciplines, namely 22 trampolinists [27] and 107 rhythmic gymnasts [25]. One study featured 9 artistic gymnasts and trampolinists within a group encompassing several sports: 23 volleyball players, 9 judokas, and 26 swimmers, in order to compare these disciplines with 96 non-athlete participants [11]. Another study included 68 artistic gymnasts, 116 team gymnasts, and 135 cheerleaders [26]. Overall, the athlete sample totalled 515 participants, with 322 gymnasts. The first study did not differentiate between the two gymnastics disciplines represented in the results (artistic gymnastics and trampoline) [11].
3.4. Intervention
Three studies [25,26,27] evaluated only gymnasts, all of whom were selected and assessed during national championships. However, Gram & Bø (2020) also collected data in a training context. One study [11] compared the prevalence of urinary incontinence (UI) between two groups: athletes (from four different sports disciplines) and non-athletes. This study was the only one to include an informational session on the pelvic floor and its training prior to administering the questionnaire. All studies assessed participants using self-administered questionnaires. However, for supervision, Almeida et al. (2016) made an investigator available, and Gram & Bø (2020) provided a physiotherapist. All questionnaires, designed by the researchers, included demographic data and UI assessment. One study [25] conducted a clinical assessment of benign joint hypermobility. This involved evaluating passive extension of each fifth finger beyond 90 degrees, passive opposition of each thumb to the forearm, hyperextension of each elbow beyond 190 degrees, hyperextension of each knee beyond 10 degrees, and trunk flexion.
3.5. Assessment tools
Regarding the assessment of urinary incontinence (UI), the International Consultation on Incontinence Questionnaire - Short Form (ICIQ-UI-SF or ICIQ-SF) was used in 100% of the studies. Questionnaires for the evaluation of anal incontinence were also identified [28,29]: the International Consultation on Incontinence Questionnaire Anal Incontinence Symptoms and Quality of Life Module (ICIQ-B) and the Fecal Incontinence Severity Index (FISI).For other symptoms, the following tools were observed: the Low Energy Availability in Females Questionnaire (LEAF-Q), the Low Energy Availability in Females Questionnaire - Short Form (LEAF-SF), the Triad-specific self-report questionnaire, and the Female Sexual Function Index (FSFI) for assessing the Female Athlete Triad [30,31]. The Beighton Score was used for assessing joint hypermobility [32], and the Rome III Criteria for functional gastrointestinal disorders (“Appendix B. The Rome III diagnostic criteria for functional gastrointestinal disorders,” 2012). Vaginal and sexual symptoms [33] were also assessed through the International Consultation on Incontinence Questionnaire - Vaginal Symptoms (ICIQ-VS) and the Female Sexual Function Index (FSFI).
3.6. Outcomes
The primary outcome assessed in all studies was the prevalence of urinary incontinence (UI). Subsequently, the occurrence of each type of UI [25,26], anal incontinence (AI) [11,26], and pelvic organ prolapse [11] was evaluated. One study [11] assessed the influence of the sports discipline on the occurrence of UI, while another [27] examined the association between UI severity and training volume. Two studies [11,27] evaluated the impact of UI on quality of life, and one [27] also analysed its impact on athletic performance. Two other studies [25,26] investigated the impact of UI on athletic performance and outcomes. One study [11] analysed athletes’ attitudes towards UI, one [25] assessed knowledge about pelvic floor muscles (PFM), and one [26] examined PFM training and UI.
4. Discussion
The aim of this scoping review was to summarize the current evidence on UI in adolescent and adult female gymnasts, to understand which gymnastics disciplines have the highest prevalence of UI, and which instruments and outcomes are used in the assessment and intervention of UI in athletes. This study showed that the prevalence of UI is high in all the gymnastics disciplines assessed, with a higher prevalence of SUI. The modalities with the highest recorded prevalence were artistic gymnastics and trampolining, with a rate of 88.9 per cent [11], and the lowest in rhythmic gymnastics, with a rate of 31.8 per cent [25]. As for the type of UI, two studies [25,26] evaluated the different types of UI and found a higher prevalence for SUI. The other two studies [11,27] only reported the prevalence of SUI, since it was the most prevalent type of UI. There was a lack of physiotherapy intervention as a tool in the prevention and intervention of UI in the studies included in this scoping review. The main methods for intervening in UI are physiotherapy, biofeedback, pharmacology and, in more serious cases, surgery [34,35]. Physiotherapy works to promote continence through pelvic floor muscle (PFM) training programs. This method is recommended as a first-line intervention, with no adverse effects and a level of evidence of 1A and is effective especially for SUI in the general female population [36]. The National Institute for Health and Care Excellence (NICE) guideline indicates that MPP training is as effective as or more effective than surgery for around half of women with SUI [37]. Training should be orientated baised on the deficits found and designed to develop specific function parameters for this muscle group. This is well documented as improving muscle strength, functionality and blood supply to muscle tissue [20]. However, to date, there have been few studies on the effect of MPP training on elite athletes and gymnasts [13]. Due to the nature of the studies included, no specific interventions were identified, so this information has not been incorporated into Table 2. However, in terms of the use of assessment instruments, the most prevalent was the ‘International Consultation on Incontinence Questionnaire - Urinary Incontinence-Short Form’ (ICIQ-UI-SF). This specific and brief questionnaire aims to identify the presence of UI, its type and frequency, as well as its impact on the athletes' quality of life [38,39]. This questionnaire is simple, quick to complete, has high levels of validity, reliability and sensitivity, and can be used in clinical practice and research [40]. The known risk factors for UI are pregnancy, eutocic labor, pelvic floor surgery, obesity and age [5]. However, as Gram et Bø (2020) point out, there is a lack of research into risk factors in young nulliparous women, and that a low BMI, hours of training and joint hypermobility are possible risk factors for UI. The advantage of the ICIQ-UI-SF self-completion questionnaire also lies in its assessment of quality of life, an outcome that was considered in all the studies. This allows us to raise some hypotheses about the repercussions of this condition on young athletes. Studies indicate that athletes report a negative impact on quality of life [11] and sports performance [25,26]. Although one study revealed that female athletes reported only a “slight” impact of UI on their quality of life, the interpretation of these results should be done with some caution, considering the sample limitation of only 22 athletes [27]. However, the authors suggest that shame and poor UI literacy may be additional factors contributing to the underreporting of actual symptoms [27]. The use of strategies to prevent episodes of UI has also been described, such as bladder emptying [11] or the use of pads [26]. In addition, the studies also emphasize the athletes' lack of knowledge about the anatomy of the pelvic floor [25,26]. However, they report an interest in training to prevent or intervene in UI [26]. This information shows that athletes are not aware of the options for preventing and intervening in UI. A pioneering study also found a significant association between athletic performance, training volume and UI severity, as well as a strong correlation between years of training and the ICIQ-UI-SF score, and years of training, frequency and amount of loss [27]. This extremely important information raises the debate about the lack of consensus among studies as to whether high-impact physical exercise, such as gymnastics, is a risk or protective factor for UI. There are two explanatory hypotheses about the effect of exercise on the pelvic floor: the first is that exercise strengthens the pelvic floor and reduces the risk of UI, and the second is that physical activity weakens the pelvic floor, increasing the risk of UI [12]. The increased risk of UI in high-impact sports is explained by the hypothesis of the high and repetitive increase in intra-abdominal pressure (IAP) [41], which explains the high prevalence of UI in gymnastics, involving the production of ground reaction forces during tumbling landings [43]. Based on these hypotheses, studies differ on the cause of the high prevalence of UI in gymnastics. Da Roza et al. (2015), defend the hypothesis that urine loss is not due to a morphological change or fatigue of the PFM, but is a consequence of the altered muscular response to a mechanical stimulus. The authors state that it could be speculated that the high stress on the MPP could have a negative impact on the intrafusal fibers, reducing their ability to respond to stretching, which could result in a delay in contraction. Other authors, Gram et Bø (2020), state that the high prevalence of UI seen in rhythmic gymnastics indicates that intense exercise does not protect against UI. For now, it can only be speculated whether high exposure to high-impact activities can cause UI or whether the condition is due to underlying genetic factors, such as a low position of the pelvic floor within the pelvis, a weakness of the PFM and/or connective tissue and/or a delayed neurophysiological response to increased intra-abdominal pressure. Finally, Skaug et al. (2022), state that PFM fatigue during exercise could be another possible mechanism of SUI in gymnasts and cheerleaders. However, the fact that UI doesn't seem to bother them during daily activities indicates that the impact during training isn't enough to induce incontinence and that the losses may be mainly related to sporting activities. This suggests that not only is there no consensus between the two hypotheses, but that high-impact sports such as gymnastics are a risk factor for the development of SUI in young nulliparous women. The studies underline the urgency of prioritizing the prevention and intervention of UI among the professionals who accompany these athletes, be they physiotherapists or others, as well as the athletes. It seems essential to us to promote pelvic floor literacy to the entire coaching staff and athletes, with the aim of fostering empowerment, knowledge and self-management of UI prevention. Health professionals, particularly physiotherapists, by raising awareness of MPP and providing appropriate exercise guidance. Opening the debate, in a training context, could draw the athletes' attention to the fact that there are means of prevention, but also of intervention in this condition. The physiotherapist's role is not only to rehabilitate, but also to communicate and educate the athletes, from a prevention and awareness perspective. This study has some limitations, namely the scarcity of bibliography, the small number of studies included, making it difficult to compare results and establish clear guidelines for intervention in this population. Another limitation is related to the lack of studies that carry out specific interventions, most of which on UI in athletes are observational. The uniformity of the assessment of UI in most studies, using questionnaires and other assessment instruments, also makes it difficult to compare them and can limit the robustness of their conclusions. These limitations could certainly represent a challenge for further studies, as well as contributing to the design of specific and effective preventive programs to improve this health condition in these athletes.
5. Conclusions
SUI was the most prevalent type of UI among female gymnasts, with the highest rates observed in artistic and trampoline disciplines . All included studies used the ICIQ-UI-SF to assess UI. Reported outcomes comprised the prevalence of UI and SUI, their impact on quality of life and athletic performance, and athletes’ knowledge about UI and the pelvic floor. None of the studies investigated or implemented any intervention strategies. Future research should prioritize the development of intervention studies, particularly experimental designs evaluating specific interventions, such as pelvic floor muscle training programs tailored to these athletes. It also seems important to increase athletes' knowledge about UI prevention and management, reducing the associated stigma and encouraging a holistic approach to women´s health in sport.
Author Contributions
Conceptualization, A.H.; methodology, A.H. and S.L.; validation, A.H. and S.L.; formal analysis, A.H. and S.L.; investigation, A.H. and S.L.; resources, A.H. and S.L.; data curation, A.H. and S.L.; writing—original draft preparation, A.H. and S.L.; writing—review and editing, A.H., S.L., A.C. and Á.V.; visualization, A.H.; supervision, S.L.; project administration, A.H. and S.L.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Haylen, BT., De Ridder, D., Freeman, R., Swift, S., Berghmans, B., Lee, JH., Monga, A., Petri, E., Rizk, DEE., Sand, PK., & Schaer, GN. An international urogynecological association (IUGA)/international continence society (ICS) joint report on the terminology for female pelvic floor dysfunction. Neurourology and Urodynamics 2011, 29(1): 4-20. [CrossRef]
- D’Ancona, CAL., Haylen, BT., Wein, AJ., Abranches-Monteiro, L., Arnold, EP., Goldman, H B., Hamid, R., Homma, Y., Marcelissen, T., Rademakers, K., Schizas, A., Singla, AK., Soto, I., Tse, V., De Wachter, S., Herschorn, S., & Dysfunction. The International Continence Society (ICS) report on the terminology for adult male lower urinary tract and pelvic floor symptoms and dysfunction. Neurourology and Urodynamics 2019, 38(2): 433 477. [CrossRef]
- Dedicação, AC., Haddad, M., Saldanha, M., & Driusso, P. Comparação da qualidade de vida nos diferentes tipos de incontinência urinária feminina. Revista Brasileira De Fisioterapia 2009, 13(2): 116 122. [CrossRef]
- Aoki, Y., Brown, HE., Brubaker, L., Cornu, J., Daly, JO. & Cartwright, R. Urinary incontinence in women. Nature Reviews Disease Primers 2017, 3(1): 17042. [CrossRef]
- Milsom, I., Altman, D., Cartwright, R., Lapitan, MC., Nelson, R., Sillén, U., & Tikkinen, K. Epidemiology of Urinary Incontinence (UI) and other Lower Urinary Tract Symptoms (LUTS), Pelvic Organ Prolapse (POP) and Anal Incontinence (AI). In: Incontinence: 5th International Consultation on Incontinence, Paris, P. Abrams, L. Cardozo, S. Khoury, & A. J. Wein (5th ed). 2013, ICUD-EAU, 15-107.
- Correia, S., Dinis, P., Rolo, F., & Lunet, N. Prevalence, treatment and known risk factors of urinary incontinence and overactive bladder in the non-institutionalized Portuguese population. International Urogynecology Journal 2009, 20(12): 1481-1489. [CrossRef]
- Preda, A. & Moreira, S. Incontinência Urinária de Esforço e Disfunção Sexual Feminina : O Papel da Reabilitação do Pavimento Pélvico. Acta Médica Portuguesa 2019, 32(11), 721-726. [CrossRef]
- Benício, CDAV., Luz, MHBA., De Oliveira Lopes, MV. & De Carvalho, NAR. Incontinência Urinária : Prevalência e Fatores de Risco em Mulheres em uma Unidade Básica de Saúde. Estima 2016, 14(4): 161-168. [CrossRef]
- De Oliveira Lopes, MV., & Higa, R. Restrições causadas pela incontinência urinária à vida da mulher. Revista Da Escola De Enfermagem Da Usp 2006, 40(1): 34-41. [CrossRef]
- Abrams, P., Cardozo, L., Fall, M., Griffiths, D., Rosier, PF., Ulmsten, U., Van Kerrebroeck, P., Victor, A. & Wein, A. J. The standardisation of terminology of lower urinary tract function : Report from the standardisation sub-committee of the international continence society. American Journal of Obstetrics and Gynecology 2002, 187(1): 116-126. [CrossRef]
- Almeida, M., Barra, AA., Saltiel, F., Silva-Filho, AL., Da Fonseca, AMRM. & Figueiredo, EM. Urinary incontinence and other pelvic floor dysfunctions in female athletes in Brazil : A cross-sectional study. Scandinavian Journal of Medicine & Science in Sports 2016, 26(9): 1109-1116. [CrossRef]
- Bø, K. Urinary Incontinence, Pelvic Floor Dysfunction, Exercise and Sport. Sports Medicine 2004, 34(7): 451-464. [CrossRef]
- Nygaard, I. & Shaw, JM. Physical activity and the pelvic floor. American Journal of Obstetrics and Gynecology 2016, 214(2), 164-171. [CrossRef]
- Shaw, JM. & Nygaard, I. Role of chronic exercise on pelvic floor support and function. Current Opinion in Urology 2017, 27(3): 257-261. [CrossRef]
- Nygaard, I., DeLancey, JO., Arnsdorf, L., & Murphy, E. Exercise and incontinence. International journal of gynaecology and obstetrics 1995, 33(4), 384. [CrossRef]
- Carls, C. The prevalence of stress urinary incontinence in high school and college-age female athletes in the midwest : implications for education and prevention. Urologic nursing 2007, 27(1): 21-24.
- Bø, K. & Borgen, JS. Prevalence of stress and urge urinary incontinence in elite athletes and controls. Medicine and Science in Sports and Exercise 2001, 33(11): 1797-1802, 2001. [CrossRef]
- Thyssen, HH., Clevin, L., Olesen, SS. & Lose, G. Urinary Incontinence in Elite Female Athletes and Dancers. International Urogynecology Journal 2002, 13(1): 15-17, 2002. [CrossRef]
- Eliasson, K., Larsson, TE. & Mattsson, E. Prevalence of stress incontinence in nulliparous elite trampolinists. Scan J Med Sci Sports 2002, 12(2): 106 110. [CrossRef]
- Joseph, CL., Srivastava, K., Ochuba, O., Ruo, SW., Alkayyali, T., Sandhu, JK., Waqar, A., Jain, A. & Poudel, S. Stress Urinary Incontinence Among Young Nulliparous Female Athletes. Cureus 2021, 13(9): e17986. [CrossRef]
- Tanno, AP. & Marcondes, FK. Estresse, ciclo reprodutivo e sensibilidade cardíaca às catecolaminas. Revista Brasileira De Ciencia Do Solo 2002, 38(3): 273-289. [CrossRef]
- Guezennec, C., Oliver, C., Lienhard, F., Seyfried, D., Huet, F. & Pesce, G. Hormonal and metabolic response to a pistol-shooting competition. Science & Sports 1992, 7(1): 27-32. [CrossRef]
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, Shamseer L, Tetzlaff JM, Akl EA, Brennan SE, Chou R, Glanville J, Grimshaw JM, Hróbjartsson A, Lalu MM, Li T, Loder EW, Mayo-Wilson E, McDonald S, McGuinness LA, Stewart LA, Thomas J, Tricco AC, Welch VA, Whiting P, Moher D. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021, 372(71). [CrossRef]
- Aromataris E, Lockwood C, Porritt K, Pilla B, Jordan Z, editors. JBI Manual for Evidence Synthesis 2020. [CrossRef]
- Gram, MCD., & Bø, K. High level rhythmic gymnasts and urinary incontinence : Prevalence, risk factors, and influence on performance. Scandinavian Journal of Medicine & Science in Sports 2020, 30(1): 159 165. [CrossRef]
- Skaug, KL., Engh, ME., Frawley, H. & Bø, K. Urinary and anal incontinence among female gymnasts and cheerleaders—bother and associated factors. A cross-sectional study. International Urogynecology Journal 2022, 33(4): 955-964. [CrossRef]
- Da Roza, T., Brandão, S., Mascarenhas, T., Jorge, RN. & Duarte, J. A. Volume of Training and the Ranking Level Are Associated With the Leakage of Urine in Young Female Trampolinists. Clinical Journal of Sport Medicine 2015, 25(3): 270 275. [CrossRef]
- Rockwood, T. H., Church, J. M., Fleshman, J. W., Kane, R. L., Mavrantonis, C., Thorson, A. G., Wexner, S. D., Bliss, R. N. D., & Lowry, A. C. Patient and surgeon ranking of the severity of symptoms associated with fecal incontinence. Diseases of The Colon & Rectum 1999, 42(12), 1525 1531. [CrossRef]
- Cotterill, N., Norton, C., Avery, K. N. L., Abrams, P., & Donovan, J. L. Psychometric Evaluation of a New Patient-Completed Questionnaire for Evaluating Anal Incontinence Symptoms and Impact on Quality of Life : The ICIQ-B. Diseases of The Colon & Rectum 2011, 54(10), 1235 1250. [CrossRef]
- De Maria, U. P., & Juzwiak, C. R. Cultural adaptation and validation of the low energy availability in females questionnaire (LEAF-Q). Bras Med Esporte 2021, 27(2). [CrossRef]
- De Souza, M. J., Nattiv, A., Joy, E. A., Misra, M., Williams, N. I., Mallinson, R. J., Gibbs, J. C., Olmsted, M. P., Goolsby, M., Matheson, G. O., & Panel, L. 2014 Female Athlete Triad Coalition Consensus Statement on Treatment and Return to Play of the Female Athlete Triad : 1st International Conference held in San Francisco, California, May 2012 and 2nd International Conference held in Indianapolis, Indiana, May 2013. British Journal of Sports Medicine 2014 48(4), 289. [CrossRef]
- Malek, S., Reinhold, E. J., & Pearce, G. The Beighton Score as a measure of generalised joint hypermobility. Rheumatology International 2021, 41(10), 1707-1716.
- Wiegel, M., Meston, C. M., & Rosen, R. C. The Female Sexual Function Index (FSFI) : Cross-Validation and Development of Clinical Cutoff Scores. Journal of Sex & Marital Therapy 2005, 31(1), 1-20. [CrossRef]
- Santos, KMD., Da Roza, T., Da Silva, LL., Wolpe, RE., Da Silva Honório, GJ., & Da Luz, SC. Female sexual function and urinary incontinence in nulliparous athletes : An exploratory study. Physical Therapy in Sport 2018, 33, 21-26. [CrossRef]
- Bø, K. Physiotherapy management of urinary incontinence in females. Journal of Physiotherapy 2020, 66(3): 147-154. [CrossRef]
- Dumoulin, C., Hay-Smith, J., & Mac Habée-Séguin, G. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. The Cochrane library 2014, 5: 1-94. [CrossRef]
- National Institute for Health and Care Excellence. Urinary incontinence and pelvic organ prolapse in women : management. NICE guideline 2019, No.123.
- Tamanini, JTN., Dambros, M., D’Ancona, CAL., Palma, P. & Netto, NR. Validação para o português do « International Consultation on Incontinence Questionnaire - Short Form » (ICIQ-SF). Revista De Saude Publica 2004, 38(3): 438-444. [CrossRef]
- Saboia, DM., Firmiano, MLV., De Castro Bezerra, K., Neto, JD., Oriá, MOB. & Vasconcelos, C TM. Impacto dos tipos de incontinência urinária na qualidade de vida de mulheres. Revista Da Escola De Enfermagem Da Usp 2017, 51(0): e03266. [CrossRef]
- Avery, KNL., Donovan, JL., Peters, TJ., Shaw, C., Gotoh, M., & Abrams, P. ICIQ : A brief and robust measure for evaluating the symptoms and impact of urinary incontinence. Neurourology and Urodynamics 2004, 23(4): 322-330. [CrossRef]
- Bø, K., & Nygaard, I. Is Physical Activity Good or Bad for the Female Pelvic Floor ? A Narrative Review. Sports Medicine 2020, 50(3): 471-484. [CrossRef]
- Seegmiller, JG. & McCaw, ST. Ground Reaction Forces Among Gymnasts and Recreational Athletes in Drop Landings. J Athl Train 2003, 38 (4): 311 314.
Figure 1.
Flowchart of the scoping review according to the PRISMA-ScR model.
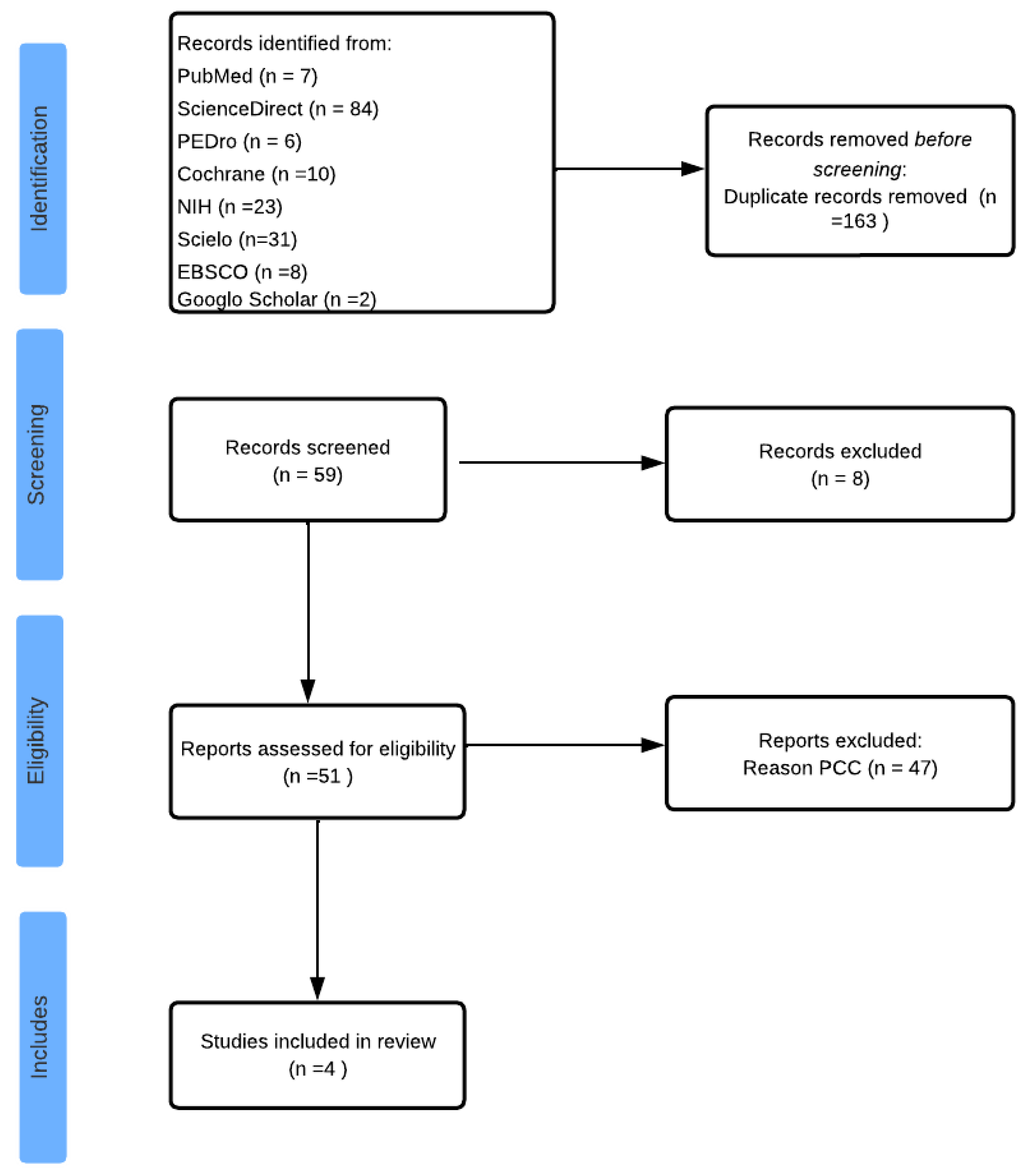

Table 1.
Search strategy according to database.
| Database | Search Strategy | Filters used |
|---|---|---|
| PubMed | (“woman” OR “female” OR “athlete”) AND (“gymnastic” OR “trampoline” OR “acrobatic” OR “high impact sport”) AND (“urinary incontinence” OR “stress urinary incontinence” OR “pelvic floor disorders” OR “loss of urine” OR “urine leakage”) AND (“prevalence” OR “treatment” OR “knowledge” OR “impact” OR “quality of life” OR “prevention”) | Published between 2012 and 2023 Full text available Study type: journal article, clinical trial, randomised controlled trial, books and documents Language: English, Portuguese Age: adolescents (13–18 years), young adults (19–24 years), adults (19–44 years) Sex: female |
| Cochrane | (“gymnastic” OR "trampolim" OR "acrobatic" OR "high impact sport") AND (“urinary incontinence” OR “stress urinary incontinence” OR “pelvic floor disorders”) | Published between 2012 and 2023 Language: English Publication type: Clinical trials |
| Science Direct | (“gymnastic” OR "trampolim" OR "acrobatic" OR "high impact sport") AND (“urinary incontinence” OR “stress urinary incontinence” OR “pelvic floor disorders”). | Published between 2012 and 2023 Publication type: research articles, book chapters Access: free access, open archive |
| Scielo | (“gymnastic” OR "trampolim" OR "acrobatic" OR "high impact sport") AND (“urinary incontinence” OR “stress urinary incontinence” OR “pelvic floor disorders”) | Published between 2012 and 2023 Language: English, Portuguese Type of literature: articles |
| EBSCO | (“gymnastic” OR "trampolim" OR "acrobatic" OR "high impact sport") AND (“urinary incontinence” OR “stress urinary incontinence” OR “pelvic floor disorders”) | Published between 2012 and 2023 References available Type of publication: academic journal articles, reports, books |
| PEDro | “incontinence. Subdisciplina: “sports” |
Published from 2012 onwards Method: clinical trial |
| NIH | “urinary incontinence”. Outros termos: “sport” |
Articles published from 2012 onwards Study type: clinical trial, observational study Status: completed and closed Expanded access: available Study with results Age: children and adults Sex: female |
Table 2.
Characteristics of eligible studies.
| Authors /Year |
Study | Objectives | Participants | Assessment tools |
Outcomes |
|---|---|---|---|---|---|
| Almeida et al. (2016) |
Cross-sectional study | To investigate the occurrence of pelvic floor dysfunction (PFD) symptoms among athletes and non-athletes. To investigate the influence of sport on the occurrence and severity of urinary dysfunction. |
n = 163 Athletes (n=67): artistic gymnastics and trampoline (n=9) Non-athletes (n=96) 15-29 years BMI athletes: 21.7 (± 2.6) BMI non-athletes: 20.9 (± 3.9) Nulliparous IU (gymnasts) : 88.9% IUE (gymnasts): 87.5% |
ICIQ-UI-SF FISI Criteria Rome III FSFI ICIQ-VS |
Pelvic floor dysfunctions Influence of modality Impact on quality of life Attitude towards UI |
| Da Roza et al. (2015) |
Cohort study | To investigate the association between UI severity and training volume and athletic performance in young female nulliparous trampolinists. | n = 22 Trampolinists/ National level 14-25 years BMI: 20.4 (± 1.3) Nulliparous SUI: 72.7% |
ICIQ-UI-SF |
Prevalence of pelvic floor dysfunction (PFD) Association between UI severity and training volume Impact on quality of life and athletic performance |
| Gram et Bø, (2020) |
Cross-sectional study | To investigate the prevalence and risk factors of UI in rhythmic gymnasts and the impact of UI on sports performance. Evaluate MPP knowledge and MPP training. |
n = 107 Rhythmic gymnastics International level 12-21 years BMI: 18.5 (± 5.3) Nulliparous 65.4% menarche UI: 31.8% SUI: 61.8% UI: 8.8% UI: 17.6% Other UI: 11.8% |
ICIQ-UI-SF "Triad-specific self- report questionnaire" LEAF-SF Beighton score |
UI prevalence Prevalence of type of UI Impact of UI on athletic performance Knowledge about MPP and its training |
| Skaug et al., (2022) |
Cross-sectional study | To investigate the prevalence and risk factors of UI and anal incontinence (AI) in high-performance female artistic gymnasts (GA), team gymnasts (GE) and female cheerleaders To investigate the impact of UI/IA on sports performance To assess the athletes' knowledge of MPP. |
n = 319 Artistic gymnastics (n=68), Team gymnastics (n=116),C Cheerleading (n=135) National and international level 12-36 years BMI: 21.7 (± 2. 7) Nulliparous 92.2% menarcas IU: GA 70.6%, GE 83.6% IUE: GA 70.6%, GE 80.2% IUU: GA 8.8%, GE 12.9% |
ICIQ-UI-SF ICIQ-B LEAF-Q |
Prevalence of UI and AI Prevalence of type of UI Impact on athletic performance Knowledge of UI |
GA - artistic gymnastics; GE - team gymnastics; AI - anal incontinence; ICIQ-B - International Consultation on Incontinence Questionnaire - Anal Incontinence Symptoms and Quality of Life Module; ICIQ-UI-SF - International Consultation on Incontinence Questionnaire-Short Form; BMI - body mass index; UI - urinary incontinence; SUI - stress urinary incontinence; MUI - mixed urinary incontinence; UUI - urge urinary incontinence; LEAF-Q - Low Energy Availability in Females Questionnaire - Short Form; MPP - pelvic floor muscles;.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



