
Submitted:
27 July 2025
Posted:
28 July 2025
You are already at the latest version
Abstract
Chemotherapy-induced thrombocytopenia (CIT) is a common yet underrecognized complication of systemic chemotherapy, particularly in gastrointestinal (GI) cancers. Despite progress in targeted and immune-based therapies, platinum-based and fluoropyrimidine regimens, especially oxaliplatin-containing protocols, remain standard in GI cancer treatment and are linked to high rates of CIT. This complication often leads to treatment delays, dose reductions, and elevated bleeding risk. This review provides a comprehensive overview of the pathophysiology, clinical implications, and management strategies of CIT in GI malignancies.CIT arises from several mechanisms: direct cytotoxicity to megakaryocyte progenitors, disruption of the marrow microenvironment, thrombopoietin dysregulation, and immune-mediated platelet destruction. Platinum agents, antimetabolites, and immune checkpoint inhibitors can contribute to these effects. Oxaliplatin-induced CIT may occur acutely via immune mechanisms or chronically through marrow suppression. CIT affects 20–25% of solid tumor patients, with highest rates in those receiving gemcitabine (64%), carboplatin (58%), and oxaliplatin (50%). Within GI cancer regimens, FOLFOXIRI and S-1 plus oxaliplatin show higher CIT incidence compared to FOLFIRI and CAPIRI.Thrombocytopenia is graded by severity, from mild (Grade 1-2) to severe (Grade 3-4), and often necessitates treatment adjustments, transfusions, or supportive therapies. Current strategies include chemotherapy dose modification, platelet transfusion, and thrombopoietin receptor agonists (TPO-RAs) like romiplostim and eltrombopag. While platelet transfusions help in acute settings, TPO-RAs may preserve dose intensity and reduce bleeding. Emerging agents targeting megakaryopoiesis and marrow protection offer promising avenues for long-term management.
Keywords:
chemotherapy-induced thrombocytopenia
; gastrointestinal cancers
; FOLFOX
; FOLFIRINOX
; oxaliplatin
; gemcitabine
; platelet transfusion
; thrombopoietin receptor agonists
; romiplostim
; eltrombopag
1. Introduction
Cancer continues to be a major global health challenge, with an estimated 19.3 million new cases and 1 million cancer-related deaths reported annually [1]. Despite substantial advancements in cancer therapy, including immunotherapy and molecular-targeted treatments, systemic chemotherapy remains the cornerstone of treatment for Gastrointestinal malignancies. Among the standard chemotherapy regimens for gastrointestinal cancers, oxaliplatin-based protocols, such as S-1 plus oxaliplatin, oxaliplatin with capecitabine, and oxaliplatin combined with leucovorin and fluorouracil (FOLFOX), continue to be widely utilized. These regimens are frequently employed as first- and second-line therapies for gastrointestinal tract tumors, making their use nearly unavoidable. In pancreatic cancer, the FOLFIRINOX regimen, comprising oxaliplatin, irinotecan, leucovorin, and 5-fluorouracil, has emerged as an intensive first-line option, particularly for patients with good performance status, offering improved survival at the cost of increased toxicity [2].
A major complication of chemotherapy is chemotherapy-induced thrombocytopenia (CIT), which results from the suppression of bone marrow megakaryocytes, leading to a decline in peripheral platelet counts below 100 × 10⁹/L [3]. Among patients with solid tumors, CIT is most commonly observed in non-small cell lung cancer (25%), ovarian cancer (24%), and colorectal cancer (18%) [4]. A retrospective hospital-based study conducted in the Netherlands, which included over 600 adult patients receiving chemotherapy for solid tumors, reported that 22% of patients developed thrombocytopenia (platelet count < 100 × 10⁹/L) [5]. The highest incidence was observed in patients receiving carboplatin monotherapy (82%) and oxaliplatin monotherapy (50%). Additionally, combination regimens involving carboplatin (58%), gemcitabine (64%), and paclitaxel (59%) were also associated with an increased risk of thrombocytopenia [5].
CIT remains a frequent and clinically significant complication in cancer patients undergoing cytotoxic chemotherapy, affecting approximately 20–25% of individuals with solid tumors [4,6]. CIT’s incidence, severity, and duration vary widely based on the specific chemotherapeutic agents and their administered doses [4,6]. Notably, regimens containing gemcitabine and platinum-based compounds are associated with a particularly high risk of thrombocytopenia, defined as platelet counts dropping below 150 G/L. Reported thrombocytopenia rates in patients receiving gemcitabine-based therapy are as high as 64%, while those undergoing treatment with platinum-containing agents experience rates of 56% [4].
2. Pathophysiology
Outlined below are the distinct and interconnected pathophysiological processes that contribute to the development of chemotherapy-induced thrombocytopenia (CIT), reflecting its complex biological underpinnings (Figure 1).
2.1. Direct Cytotoxicity on Megakaryocytes and Progenitor Cells
Chemotherapeutic agents, particularly alkylating agents (e.g., cyclophosphamide), platinum-based drugs (e.g., oxaliplatin, cisplatin), and antimetabolites (e.g., 5-fluorouracil, methotrexate), are known to damage actively proliferating cells. Since HSPCs and megakaryocyte progenitors in the bone marrow undergo rapid division, they are particularly susceptible to chemotherapy-induced apoptosis and DNA damage, leading to platelet-producing cell depletion and thrombocytopenia [7].
A notable example is oxaliplatin-induced thrombocytopenia, which can occur acutely due to immune-mediated destruction or chronic marrow suppression. Oxaliplatin-based chemotherapy regimens, commonly used for gastrointestinal cancers, have been associated with acute thrombocytopenia, sometimes leading to treatment delays or dose reductions [8] Table 1.
2.2. Disruption of the Bone Marrow Microenvironment
The bone marrow niche supports hematopoietic stem cell (HSC) maintenance and differentiation and consists of stromal cells, endothelial cells, and cytokines that regulate hematopoiesis. Chemotherapy alters this microenvironment by:
Depleting supportive stromal cells, impairing their ability to secrete essential growth factors (e.g., TPO, interleukins).
Inducing oxidative stress and inflammation, disrupting normal HSC function.
Damaging endothelial cells, which are crucial for sustaining the BM niche and protecting stem cells from toxic insults [7].
As a result, megakaryopoiesis is severely compromised, leading to inadequate platelet production and a higher risk of bleeding complications. Furthermore, studies have shown that platinum-based chemotherapy and targeted therapies can cause long-term suppression of bone marrow progenitor cells, further worsening CIT in cancer patients [20] (Table 2).
2.3. TPO Dysregulation and Impaired Megakaryopoiesis
Thrombopoietin (TPO) is crucial for platelet production, as it stimulates the differentiation and maturation of megakaryocytes. Under normal conditions, when platelet levels drop, TPO levels rise to compensate. However, chemotherapy-induced myelosuppression disrupts this process in several ways:
TPO levels may be insufficiently elevated to compensate for platelet loss.
Megakaryocyte precursors may have reduced responsiveness to TPO signaling due to drug-induced cellular damage.
The liver, which produces TPO, may also be affected by chemotherapy, leading to suboptimal TPO production [21].
2.4. Immune-Mediated Platelet Destruction
Certain systemic therapy, particularly immune checkpoint inhibitors and targeted therapies, can inadvertently trigger an immune response against platelets or megakaryocytes, leading to their accelerated clearance from circulation. This is observed in some patients treated with immune checkpoint inhibitors (e.g., pembrolizumab, nivolumab), which can cause immune thrombocytopenia (ITP)-like syndromes in addition to myelosuppressive effects.
Furthermore, drug-associated thrombocytopenia has been linked to platelet-reactive antibodies, which accelerate platelet destruction in the spleen. Studies suggest that drug-induced thrombocytopenia can occur through immune-mediated pathways, particularly with certain chemotherapy drugs and monoclonal antibodies [23].

Table 4.
Immune-Mediated Platelet Destruction.
| Mechanism | Associated Chemotherapeutic Agents | Clinical Consequences | References |
|---|---|---|---|
| Immune checkpoint inhibitor-induced thrombocytopenia | Pembrolizumab, nivolumab | Increased platelet destruction, ITP-like syndrome | ASH, 2018 [23] |
| Drug-associated platelet-reactive antibodies | Monoclonal antibodies, targeted therapies | Accelerated platelet clearance in spleen, worsening thrombocytopenia | ASH, 2018 [23] |
| T-cell-mediated platelet destruction | Some targeted therapies and immune-based treatments | Increased risk of severe bleeding complications | ASH, 2018 [23] |
2.5. Gemcitabine Induced Thrombotic Microangiopathies (TMA)/Atypical HUS
Gemcitabine-induced thrombotic microangiopathy (GiTMA) is a rare but potentially life-threatening complication observed in patients receiving gemcitabine-based chemotherapy, particularly for pancreatic and other gastrointestinal cancers. The incidence of GiTMA is estimated to range between 0.015% and 0.31% of treated patients, though some single-center studies suggest higher rates in heavily pretreated populations [24]. The pathogenesis is thought to involve direct endothelial injury, resulting in platelet activation, microvascular thrombosis, and complement activation particularly through the alternative pathway, resembling atypical hemolytic uremic syndrome (aHUS) [25,26]. Clinically, patients present with the triad of microangiopathic hemolytic anemia, thrombocytopenia, and acute kidney injury, often accompanied by hypertension and proteinuria. Management includes prompt discontinuation of gemcitabine and supportive care, such as dialysis when indicated. While the role of plasma exchange remains unclear, eculizumab, a complement C5 inhibitor, has shown promise in select patients, particularly those with complement dysregulation [27].
3. Incidence of CIT-Induced Thrombocytopenia
According to the NCCN guidelines, CIT is defined as a platelet count of <100 × 10⁹/L persisting for ≥3 to 4 weeks after the last chemotherapy administration and/or causing delays in chemotherapy initiation due to thrombocytopenia. A threshold of <100 × 10⁹/L is clinically significant, as it correlates with higher risks of treatment modifications, including dose delays, reductions, or discontinuations, and an increased likelihood of recurrence in future chemotherapy cycles [28].
The Common Terminology Criteria for Adverse Events (CTCAE) categorizes thrombocytopenia into four grades based on platelet counts: Grade 1: 75–100 × 10⁹/L, Grade 2: 50–75 × 10⁹/L, Grade 3: 25–50 × 10⁹/L, and Grade 4: <25 × 10⁹/L. The clinical impact of thrombocytopenia aligns with these grades, ranging from mild, asymptomatic cases with petechiae to life-threatening hemorrhagic events, such as intracranial or gastrointestinal bleeding [29,30]. The grades are also clinically categorized based on bleeding severity. Grade 1 corresponds to petechiae, Grade 2 to mild blood loss, Grade 3 to gross blood loss, and Grade 4 to debilitating blood loss [31] (Table 5).
Although platelet count is a key predictor of bleeding risk, other factors significantly contribute to bleeding complications in CIT. Platelet function, the rate of platelet decline, infections, kidney insufficiency, underlying coagulopathies, and the concomitant use of antithrombotic agents all modulate the overall bleeding risk [15]. These factors may explain why some patients with moderate thrombocytopenia experience severe bleeding while others with very low platelet counts remain asymptomatic. Further research is needed to refine risk assessment models beyond platelet thresholds and incorporate functional platelet activity and patient-specific risk factors into CIT management strategies.
4. Discussion
Among solid tumors, gastrointestinal malignancies are particularly prone to CIT, due to both disease-related factors and the intensive chemotherapy regimens used for treatment, contributing to treatment delays, dose modifications, and increased bleeding risk. The incidence of CIT varies depending on tumor type, patient characteristics, and treatment regimen, with some studies reporting rates ranging between 13–40% in patients receiving chemotherapy for GI cancers [15,29]. The risk of thrombocytopenia is further exacerbated in patients with underlying liver dysfunction, which is common in GI cancers such as hepatocellular carcinoma and metastatic colorectal cancer. Additionally, thrombocytopenia in these patients is not only a consequence of myelosuppressive chemotherapy but also may be influenced by splenic sequestration and compromised thrombopoiesis due to liver disease [32].
Given the high incidence of chemotherapy-induced thrombocytopenia (CIT) in GI cancers, it is essential to evaluate which chemotherapy regimens contribute most significantly to this complication and how they impact treatment outcomes. Fluoropyrimidines (5-fluorouracil and capecitabine), gemcitabine, platinum-based agents (oxaliplatin and cisplatin), and irinotecan are among the most frequently used cytotoxic drugs in the treatment of GI malignancies, either as monotherapy or in combination regimens.
Multiple retrospective studies have investigated chemotherapy-induced thrombocytopenia (CIT) in solid tumors. In a large retrospective study by Shaw et al., 13% of patients with solid tumors developed thrombocytopenia, with the highest incidence observed in patients receiving gemcitabine and platinum-based therapies [29]. Similar findings were reported in a retrospective study of 47,159 patients, reinforcing the association between CIT and both platinum-based and gemcitabine-containing regimens [4].
In a recent meta-analysis on metastatic colorectal cancer by Zhan et al. (2024) [20], the Surface Under the Cumulative Ranking (SUCRA) values were used to assess the risk of chemotherapy-induced thrombocytopenia (CIT) across different regimens. The analysis found that CAPIRI + bevacizumab (capecitabine and irinotecan with bevacizumab), FOLFIRI + bevacizumab (5-fluorouracil, leucovorin, and irinotecan with bevacizumab), and CAPIRI + cetuximab (capecitabine and irinotecan with cetuximab) had the lowest risk of thrombocytopenia, ranking highest in safety. Conversely, S-1 + oxaliplatin, FUOX, FOLFOXIRI + bevacizumab, and IROX exhibited a higher risk of thrombocytopenia, as reflected by their lower SUCRA scores. Notably, the study also observed that platinum-containing regimens were more strongly associated with thrombocytopenia, highlighting the need for close platelet monitoring in patients receiving these treatments [20]. Among combination regimens, FOLFIRINOX has been linked to a higher incidence of Grade 3-4 thrombocytopenia compared to gemcitabine alone [2] (Table 6).
5. Management
The management of chemotherapy-induced thrombocytopenia (CIT) requires a comprehensive approach, considering the underlying cause, chemotherapy regimen, and treatment goals. Before initiating specific interventions, it is crucial to evaluate for secondary causes of thrombocytopenia, such as infection, coagulopathy, bone marrow suppression, or concurrent medications that may exacerbate platelet suppression [15]. In CIT, depending on chemotherapy regimen and risk of myelosuppression, platelet nadir and recovery varies. However, the depth of the platelet nadir may worsen with successive chemotherapy cycles, leading to an increased risk of bleeding and the need for treatment modifications [28].
One major strategy is to reduce the chemotherapy frequency or dosage. This is usually preferred if the therapy is not standard or not of curative intent [6]. A retrospective analysis evaluating irinotecan-based (FOLFIRI) and oxaliplatin-based (mFOLFOX6) regimens in metastatic colorectal cancer patients demonstrated that maintaining higher relative dose intensity (RDI) of irinotecan was significantly associated with improved outcomes (PFS: 9.9 vs. 5.6 months and OS: 26.7 vs. 12.9 months) [33]. These findings underscore the critical balance between managing CIT and preserving chemotherapy dose intensity to optimize patient outcomes.
Platelet transfusion is a key intervention in the management of chemotherapy-induced thrombocytopenia (CIT), particularly for patients at high risk of bleeding or those experiencing active hemorrhage. According to the American Society of Clinical Oncology (ASCO) guidelines, prophylactic platelet transfusions are recommended when platelet counts fall below 10 × 10⁹/L in solid tumors. A higher threshold can be used in case of bleeding or necrotic tumors [34]. A few studies mention <20 × 10⁹/L if the patient is febrile [15]. However, platelet transfusions have several limitations, making their use less ideal for long-term management. One of the main concerns is their short-lived effect—transfused platelets survive only 3-5 days [6,35]. Additionally, repeated transfusions can lead to alloimmunization, where patients develop HLA antibodies, making subsequent transfusions less effective and increasing the risk of platelet refractoriness. Patients who become refractory may require HLA-matched platelets [35]. Furthermore, platelet transfusions carry risks of transfusion-related reactions, infections, and thrombotic complications [36]. Given these limitations, platelet transfusions should be used judiciously, mainly for acute management of severe thrombocytopenia or active bleeding.
In patients with liver cirrhosis, splenic sequestration often contributes to persistent thrombocytopenia, which can complicate the administration of systemic chemotherapy. Partial splenic embolization (PSE) offers a minimally invasive strategy to mitigate hypersplenism by reducing splenic blood flow, thereby increasing circulating platelet counts. This approach has shown effectiveness in improving hematologic parameters, enabling safer delivery of chemotherapy in select cirrhotic patients. A prospective phase II study demonstrated that PSE enabled 94% of patients with gastrointestinal cancers to resume chemotherapy within a median of 14 days post-procedure, significantly improving platelet counts and minimal procedure-related morbidity [37]. Compared to splenectomy, PSE carries a lower procedural risk and can be tailored to minimize complications such as infarction or portal vein thrombosis [38].
Antifibrinolytic agents like ε-aminocaproic acid and tranexamic acid have been considered for managing bleeding in thrombocytopenic cancer patients when platelet transfusions are ineffective. However, their clinical benefit remains unproven, and their use may increase thrombotic risk, particularly in cancer patients [6,15].
Thrombopoietin receptor agonists (TPO-RAs) have emerged as a promising therapeutic option for managing chemotherapy-induced thrombocytopenia (CIT), particularly in patients with solid tumors. These agents, including romiplostim, eltrombopag, and avatrombopag, function by stimulating the thrombopoietin receptor, thereby enhancing megakaryocyte proliferation and increasing platelet production. Their use aims to maintain chemotherapy dose intensity, reduce the need for platelet transfusions, and mitigate bleeding risks associated with CIT.
Thrombopoietin receptor agonists (TPO-RAs) are a class of drugs that bind to and activate the TPO receptor (MPL), stimulating megakaryocyte proliferation, differentiation, and platelet production, without containing the peptide sequence of endogenous thrombopoietin [39]. There are currently four available TPO-RAs: romiplostim, a “peptibody” administered via weekly subcutaneous injection, and eltrombopag, avatrombopag, and lusutrombopag, which are oral small-molecule agents [40]. While TPO-RAs are FDA-approved for conditions such as immune thrombocytopenia (ITP), hepatitis C-associated thrombocytopenia, aplastic anemia, and periprocedural thrombocytopenia in chronic liver disease, their role in CIT remains under investigation. To date, only studies involving romiplostim have shown a significant benefit in CIT, whereas other agents require further evaluation [40].
Romiplostim, a subcutaneous TPO-RA, has demonstrated CIT, enabling chemotherapy continuation and reducing the need for platelet transfusions (Figure 2). In a retrospective study of 20 cancer patients with platelet counts <100 × 10⁹/L and prior chemotherapy dose delays or reductions, romiplostim increased platelet counts in all patients, with 19/20 achieving ≥100 × 10⁹/L and 15 resuming chemotherapy, of whom 14 completed at least two more cycles without modifications [41].
A phase II trial evaluated weekly romiplostim in CIT, where over half of the patients had primary gastrointestinal malignancies, and nearly 50% had primary or metastatic liver involvement. Romiplostim led to platelet recovery (≥100,000/μL) within 3 weeks in 93% (14/15) of treated patients, compared to only 12.5% (1/8) in the observation group. Mean platelet counts increased from 63,000/μL to 141,000/μL, allowing for safe chemotherapy resumption, and none of the romiplostim-treated patients required platelet transfusions. Due to the strong statistical significance (P < 0.001) and lack of spontaneous platelet recovery in the control group, the trial was converted into a single-arm, open-label study, where 85% (44/52) of patients achieved platelet correction within 3 weeks. Among those who resumed chemotherapy with romiplostim maintenance, 64% continued the same chemotherapy regimen, and 58% of those who previously required dose reductions were able to return to full or increased dosing. Only 6.8% (3/44) experienced CIT recurrence, leading to dose modifications. 10.2% of patients developed venous thromboembolism (VTE), but romiplostim was not discontinued due to VTE, and there was no observed increase in myocardial infarction or stroke risk. These findings reinforce romiplostim’s potential to restore platelet counts, sustain chemotherapy dose intensity, and minimize transfusion dependency while maintaining a stable safety profile [42].
In addition to romiplostim, several other TPO-RAs, including eltrombopag, avatrombopag, and lusutrombopag, have been explored for CIT. In a phase II study of solid tumors receiving gemcitabine monotherapy or gemcitabine with cisplatin/carboplatin, eltrombopag failed to show a significant improvement in platelet nadir compared to placebo [43]. Similarly, a randomised, double-blind, placebo-controlled, phase 3 study evaluating the use of avatrombopag in non-hematological malignancies showed no difference in CIT between avatrombopag and placebo group [44].
6. Conclusion
Chemotherapy-induced thrombocytopenia (CIT) remains a significant challenge in the treatment of gastrointestinal cancers, often leading to treatment delays, dose modifications, and increased bleeding risks. The complex pathophysiology of CIT involves direct bone marrow suppression, thrombopoietin dysregulation, immune-mediated destruction, and chemotherapy-induced microenvironmental changes. The incidence and severity of CIT vary among different chemotherapy regimens, with platinum-based and fluoropyrimidine-containing treatments showing a particularly high risk. Current management strategies include chemotherapy dose adjustments, platelet transfusions, and emerging thrombopoietin receptor agonists (TPO-RAs), which have shown promise in mitigating platelet depletion while preserving treatment efficacy. However, limitations such as transfusion-related complications and potential resistance to TPO-RAs necessitate further exploration of novel therapeutic options. A multidisciplinary approach incorporating early detection, individualized treatment strategies, and ongoing clinical research is essential to optimizing outcomes for patients with GI malignancies. Future studies should focus on refining risk stratification models and evaluating innovative agents that enhance platelet production while minimizing adverse effects, ultimately improving the quality of life and prognosis for affected patients.
Author Contributions
“Conceptualization, S.P. and R.I; methodology, S.P; software, A.D; validation, S.P. and R.I; formal analysis, K.T and S.P.; investigation, S.P and A.D.; resources, S.P; data curation, S.P and A.D; writing—original draft preparation, S.P.; writing—review and editing, S.P , A. D; visualization, S.P.; supervision, S.P , J.K , K.T.; project administration, J.K , S.P .; funding acquisition, R.I All authors have read and agreed to the published version of the manuscript.”.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
| MDPI | Multidisciplinary Digital Publishing Institute |
| DOAJ | Directory of open access journals |
| TLA | Three letter acronym |
| LD | Linear dichroism |
References
- Sung H, Ferlay J, Siegel RL, et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209-249. [CrossRef]
- Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus Gemcitabine for Metastatic Pancreatic Cancer. N Engl J Med. 2011;364(19):1817-1825. [CrossRef]
- Xu R, Shi Y, Feng J, et al. Consensus on the clinical diagnosis, treatment, and prevention of chemotherapy-induced thrombocytopenia in China (2019 version). Chin J Front Med Sci Electron Version. 2020;12(01):51-58.
- Wu Y, Aravind S, Ranganathan G, Martin A, Nalysnyk L. Anemia and thrombocytopenia in patients undergoing chemotherapy for solid tumors: A descriptive study of a large outpatient oncology practice database, 2000–2007. Clin Ther. 2009;31:2416-2432. [CrossRef]
- Ten Berg MJ, Van Den Bemt PMLA, Shantakumar S, et al. Thrombocytopenia in Adult Cancer Patients Receiving Cytotoxic Chemotherapy: Results from a Retrospective Hospital-Based Cohort Study. Drug Saf. 2011;34(12):1151-1160. [CrossRef]
- Kuter DJ. Managing thrombocytopenia associated with cancer chemotherapy. Oncol Williston Park N. 2015;29(4):282-294.
- Hoggatt J, Kfoury Y, Scadden DT. Hematopoietic Stem Cell Niche in Health and Disease. Annu Rev Pathol Mech Dis. 2016;11(1):555-581. [CrossRef]
- Erdem G, Dogan M, Demirci N, Zengin N. Oxaliplatin-induced acute thrombocytopenia. J Cancer Res Ther. 2016;12(2):509. [CrossRef]
- Li Q, Jin G, Jiang C, et al. Prophylactic administration of recombinant human thrombopoietin attenuates XELOX or SOX regimen-induced thrombocytopaenia. Arch Med Sci. 2021;17(5):1440-1446. [CrossRef]
- Jardim DL, Rodrigues CA, Novis YAS, Rocha VG, Hoff PM. Oxaliplatin-related thrombocytopenia. Ann Oncol. 2012;23(8):1937-1942. [CrossRef]
- Yeager AM, Levin J, Levin FC. The effects of 5-fluorouracil on hematopoiesis: studies of murine megakaryocyte-CFC, granulocyte-macrophage-CFC, and peripheral blood cell levels. Exp Hematol. 1983;11(10):944-952.
- Schutz FAB, Jardim DLF, Je Y, Choueiri TK. Haematologic toxicities associated with the addition of bevacizumab in cancer patients. Eur J Cancer. 2011;47(8):1161-1174. [CrossRef]
- Shu Y, Ding Y, He X, Liu Y, Wu P, Zhang Q. Hematological toxicities in PARP inhibitors: A real-world study using FDA adverse event reporting system (FAERS) database. Cancer Med. 2023;12(3):3365-3375. [CrossRef]
- Peck-Radosavljevic M. Thrombocytopenia in chronic liver disease. Liver Int. 2017;37(6):778-793. [CrossRef]
- Kuter DJ. Treatment of chemotherapy-induced thrombocytopenia in patients with non-hematologic malignancies. Haematologica. 2022;107(6):1243-1263. [CrossRef]
- Curtis BR, Kaliszewski J, Marques MB, et al. Immune-mediated thrombocytopenia resulting from sensitivity to oxaliplatin. Am J Hematol. 2006;81(3):199-201. [CrossRef]
- Mirtsching BC, George JN, Aster RH, Curtis BR. Irinotecan-induced immune thrombocytopenia. Am J Med Sci. 2014;347(2):167-169. [CrossRef]
- Kroll MH, Rojas-Hernandez C, Yee C. Hematologic complications of immune checkpoint inhibitors. Blood. 2022;139(25):3594-3604. [CrossRef]
- Jara Sánchez C, Olier Gárate C, García-Donas Jiménez J, Peñalver Párraga J. Drug-induced thrombocytopenia induced by trastuzumab: a special challenge in a curable disease. Ann Oncol. 2009;20(9):1607-1608. [CrossRef]
- Zhan Y, Cheng X, Mei P, Tan S, Feng W, Jiang H. Safety of first-line systemic therapy in patients with metastatic colorectal cancer: a network meta-analysis of randomized controlled trials. BMC Cancer. 2024;24(1):893. [CrossRef]
- Kaushansky K. Thrombopoietin and its receptor in normal and neoplastic hematopoiesis. Thromb J. 2016;14(S1):40. [CrossRef]
- De La Fouchardière C, Malka D, Cropet C, et al. Gemcitabine and Paclitaxel Versus Gemcitabine Alone After 5-Fluorouracil, Oxaliplatin, and Irinotecan in Metastatic Pancreatic Adenocarcinoma: A Randomized Phase III PRODIGE 65-UCGI 36-GEMPAX UNICANCER Study. J Clin Oncol. 2024;42(9):1055-1066. [CrossRef]
- Bakchoul T, Marini I. Drug-associated thrombocytopenia. Hematology. 2018;2018(1):576-583. [CrossRef]
- Humphreys BD, Sharman JP, Henderson JM, et al. Gemcitabine-associated thrombotic microangiopathy. Cancer. 2004;100(12):2664-2670. [CrossRef]
- Glezerman I, Kris MG, Miller V, Seshan S, Flombaum CD. Gemcitabine nephrotoxicity and hemolytic uremic syndrome: report of 29 cases from a single institution. Clin Nephrol. 2009;71(02):130-139. [CrossRef]
- Daviet F, Rouby F, Poullin P, et al. Thrombotic microangiopathy associated with gemcitabine use: Presentation and outcome in a national French retrospective cohort. Br J Clin Pharmacol. 2019;85(2):403-412. [CrossRef]
- Al Ustwani O, Lohr J, Dy G, et al. Eculizumab therapy for gemcitabine induced hemolytic uremic syndrome: case series and concise review. J Gastrointest Oncol. 2014;5(1):E30-33. [CrossRef]
- Soff GA, Al-Samkari H, Leader A, Eisen M, Saad H. Romiplostim in chemotherapy-induced thrombocytopenia: A review of the literature. Cancer Med. 2024;13(15):e7429. [CrossRef]
- Shaw JL, Nielson CM, Park JK, Marongiu A, Soff GA. The incidence of thrombocytopenia in adult patients receiving chemotherapy for solid tumors or hematologic malignancies. Eur J Haematol. 2021;106(5):662-672. [CrossRef]
- Cancer Therapy Evaluation Program, U.S. Department of Health and Human Services. Common Terminology Criteria for Adverse Events (CTCAE), Version 3.0. National Cancer Institute (NCI); 2006. http://ctep.cancer.gov.
- Miller AB, Hoogstraten B, Staquet M, Winkler A. Reporting results of cancer treatment. Cancer. 1981;47(1):207-214. [CrossRef]
- Gallo P, Terracciani F, Di Pasquale G, Esposito M, Picardi A, Vespasiani-Gentilucci U. Thrombocytopenia in chronic liver disease: Physiopathology and new therapeutic strategies before invasive procedures. World J Gastroenterol. 2022;28(30):4061-4074. [CrossRef]
- Nakayama G, Tanaka C, Uehara K, et al. The impact of dose/time modification in irinotecan- and oxaliplatin-based chemotherapies on outcomes in metastatic colorectal cancer. Cancer Chemother Pharmacol. 2014;73(4):847-855. [CrossRef]
- Schiffer CA, Bohlke K, Delaney M, et al. Platelet Transfusion for Patients With Cancer: American Society of Clinical Oncology Clinical Practice Guideline Update. J Clin Oncol. 2018;36(3):283-299. [CrossRef]
- Quillen K. Diagnosis and Management of Platelet Alloimmunization. The Hematologist. 2013;10(6). [CrossRef]
- Kiefel V. Reactions Induced by Platelet Transfusions. Transfus Med Hemotherapy Off Organ Dtsch Ges Transfusionsmedizin Immunhamatologie. 2008;35(5):354-358. [CrossRef]
- Luz JHM, Luz PM, Marchiori E, et al. Partial splenic embolization to permit continuation of systemic chemotherapy. Cancer Med. 2016;5(10):2715-2720. [CrossRef]
- Amin MA, El Gendy MM, Dawoud IE, Shoma A, Negm AM, Amer TA. Partial Splenic Embolization Versus Splenectomy for the Management of Hypersplenism in Cirrhotic Patients. World J Surg. 2009;33(8):1702-1710. [CrossRef]
- Kuter DJ. The biology of thrombopoietin and thrombopoietin receptor agonists. Int J Hematol. 2013;98(1):10-23. [CrossRef]
- Soff G, Leader A, Al-Samkari H, et al. Management of chemotherapy-induced thrombocytopenia: guidance from the ISTH Subcommittee on Hemostasis and Malignancy. J Thromb Haemost. 2024;22(1):53-60. [CrossRef]
- Parameswaran R, Lunning M, Mantha S, et al. Romiplostim for management of chemotherapy-induced thrombocytopenia. Support Care Cancer. 2014;22(5):1217-1222. [CrossRef]
- Soff GA, Miao Y, Bendheim G, et al. Romiplostim Treatment of Chemotherapy-Induced Thrombocytopenia. J Clin Oncol. 2019;37(31):2892-2898. [CrossRef]
- Winer ES, Safran H, Karaszewska B, et al. Eltrombopag for thrombocytopenia in patients with advanced solid tumors receiving gemcitabine-based chemotherapy: a randomized, placebo-controlled phase 2 study. Int J Hematol. 2017;106(6):765-776. [CrossRef]
- Al-Samkari H, Kolb-Sielecki J, Safina SZ, Xue X, Jamieson BD. Avatrombopag for chemotherapy-induced thrombocytopenia in patients with non-haematological malignancies: an international, randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Haematol. 2022;9(3):e179-e189. [CrossRef]
Figure 1.
illustrates the complex and multifactorial pathophysiological mechanisms underlying chemotherapy-induced thrombocytopenia (CIT) in gastrointestinal (GI) cancers. Key processes include disruption of the bone marrow microenvironment, where chemotherapeutic agents damage stromal and endothelial cells, alter cytokine signaling, and induce oxidative stress, ultimately impairing hematopoietic stem cell function and platelet production. Direct cytotoxicity to megakaryocytes and progenitor cells by agents such as alkylating compounds, platinum-based therapies, and antimetabolites further compromises thrombopoiesis. In addition, dysregulation of thrombopoietin (TPO) signaling—due to elevated levels with inadequate marrow responsiveness or suboptimal production—impairs megakaryopoiesis. Some patients also experience immune-mediated platelet destruction, where chemotherapy triggers the formation of platelet-reactive antibodies, accelerating platelet clearance via the spleen. Lastly, gemcitabine can induce thrombotic microangiopathy (TMA), characterized by endothelial injury and microvascular thrombosis, contributing to significant platelet consumption. These interconnected mechanisms underscore the clinical complexity of CIT in GI oncology.This figure was created with the assistance of BioRender.com.
Figure 1.
illustrates the complex and multifactorial pathophysiological mechanisms underlying chemotherapy-induced thrombocytopenia (CIT) in gastrointestinal (GI) cancers. Key processes include disruption of the bone marrow microenvironment, where chemotherapeutic agents damage stromal and endothelial cells, alter cytokine signaling, and induce oxidative stress, ultimately impairing hematopoietic stem cell function and platelet production. Direct cytotoxicity to megakaryocytes and progenitor cells by agents such as alkylating compounds, platinum-based therapies, and antimetabolites further compromises thrombopoiesis. In addition, dysregulation of thrombopoietin (TPO) signaling—due to elevated levels with inadequate marrow responsiveness or suboptimal production—impairs megakaryopoiesis. Some patients also experience immune-mediated platelet destruction, where chemotherapy triggers the formation of platelet-reactive antibodies, accelerating platelet clearance via the spleen. Lastly, gemcitabine can induce thrombotic microangiopathy (TMA), characterized by endothelial injury and microvascular thrombosis, contributing to significant platelet consumption. These interconnected mechanisms underscore the clinical complexity of CIT in GI oncology.This figure was created with the assistance of BioRender.com.
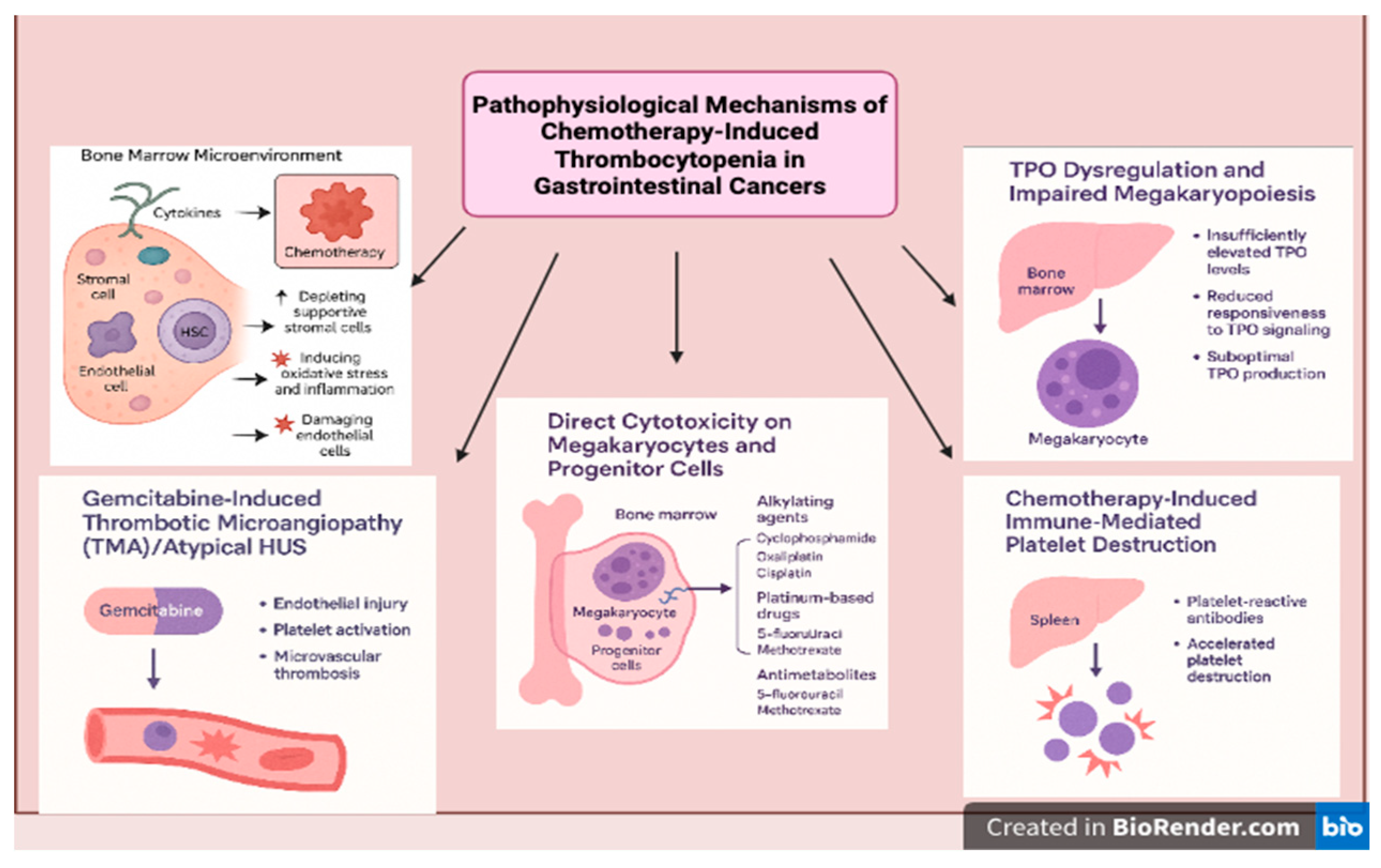
Figure 2.
The figure illustrates the molecular mechanism of thrombopoietin receptor activation and its role in promoting platelet production. Thrombopoietin (TPO) binds to its receptor, which consists of the HRD1 and HRD2 domains, leading to receptor dimerization and activation. Upon activation, the receptor recruits and phosphorylates JAK kinases, which phosphorylates downstream STAT proteins, leading to their dimerization and subsequent signal transduction for increased platelet production. Additionally, activation of the MAPK pathway via SHC, GRB2, and SOS triggers the RAS/RAF signaling cascade, promoting anti-apoptotic effects. The figure also highlights the pharmacological agents Romiplostim, Eltrombopag, Avatrombopag, Lusutrombopag, and Hetrombopag, which mimic TPO function by binding to and activating the thrombopoietin receptor, thereby enhancing platelet production. These therapeutic agents are clinically used to manage thrombocytopenia by stimulating megakaryopoiesis through JAK-STAT and MAPK signaling pathways.This figure was created with the assistance of BioRender.com.
Figure 2.
The figure illustrates the molecular mechanism of thrombopoietin receptor activation and its role in promoting platelet production. Thrombopoietin (TPO) binds to its receptor, which consists of the HRD1 and HRD2 domains, leading to receptor dimerization and activation. Upon activation, the receptor recruits and phosphorylates JAK kinases, which phosphorylates downstream STAT proteins, leading to their dimerization and subsequent signal transduction for increased platelet production. Additionally, activation of the MAPK pathway via SHC, GRB2, and SOS triggers the RAS/RAF signaling cascade, promoting anti-apoptotic effects. The figure also highlights the pharmacological agents Romiplostim, Eltrombopag, Avatrombopag, Lusutrombopag, and Hetrombopag, which mimic TPO function by binding to and activating the thrombopoietin receptor, thereby enhancing platelet production. These therapeutic agents are clinically used to manage thrombocytopenia by stimulating megakaryopoiesis through JAK-STAT and MAPK signaling pathways.This figure was created with the assistance of BioRender.com.
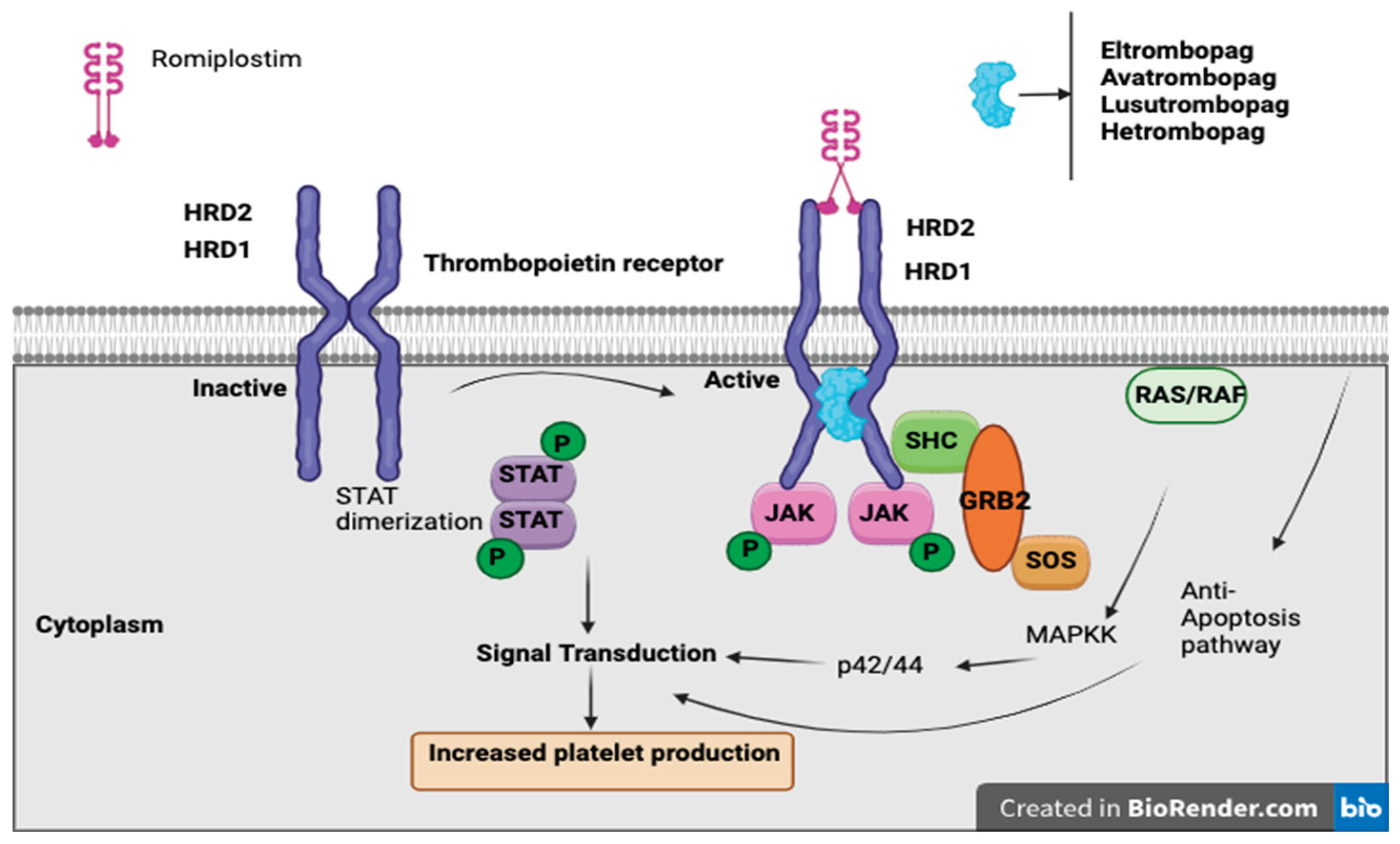
Table 1.
Pathophysiology of Chemotherapy-Induced Thrombocytopenia.
| Mechanism | Description | Chemotherapeutic Agents Involved |
|---|---|---|
| Direct Cytotoxicity on Megakaryocytes and Progenitor Cells | Chemotherapy damages actively proliferating hematopoietic stem and progenitor cells (HSPCs), leading to apoptosis and DNA damage in megakaryocyte precursors. | Alkylating agents (e.g., cyclophosphamide [9]), platinum-based drugs (e.g., oxaliplatin [10]), antimetabolites (e.g., 5-fluorouracil [11].) |
| Disruption of the Bone Marrow Microenvironment | Chemotherapy depletes stromal cells, induces oxidative stress, and damages endothelial cells, leading to impaired hematopoiesis and suppressed megakaryopoiesis. | Platinum-based chemotherapy (e.g., cisplatin, oxaliplatin [10]), targeted therapies (e.g., bevacizumab [12], olaparib [13]) |
| TPO Dysregulation and Impaired Megakaryopoiesis | Chemotherapy interferes with TPO production and megakaryocyte responsiveness, delaying platelet recovery. Liver dysfunction due to chemotherapy may further reduce TPO synthesis. | Chemotherapy agents, especially those affecting the liver [14] (e.g., high-dose alkylating agents, antimetabolites [15]) |
| Chemotherapy-Induced Immune-Mediated Platelet Destruction | Certain chemotherapies and immunotherapies trigger immune responses against platelets, causing their premature destruction via platelet-reactive antibodies or ITP-like mechanisms. | Chemotherapy (e.g., oxaliplatin [16], irinotecan [17]), Immune checkpoint inhibitors (e.g., ipilimumab, nivolumab [18]), and, targeted therapies (e.g., Trastuzumab [19]) |
Table 2.
Effects of Bone Marrow Microenvironment Disruption on CIT.
| Affected Component | Impact on Hematopoiesis | Consequence for CIT | References |
|---|---|---|---|
| Stromal Cells | Reduced secretion of essential growth factors like TPO and interleukins | Impaired megakaryocyte differentiation and platelet production | Hoggatt et al., 2016 [7] |
| Endothelial Cells | Increased oxidative stress and inflammation | Disrupted bone marrow protection for stem cells, leading to prolonged thrombocytopenia | BMC Cancer, 2024 [20] |
| Cytokine Regulation | Chemotherapy-induced alterations in cytokine balance | Inefficient platelet regeneration post-chemotherapy | Hoggatt et al., 2016 [7] |
Table 3.
TPO Dysregulation and Its Effects on CIT.
| Dysregulation Mechanism | Effect on Platelet Production | Chemotherapy Agents Implicated | References |
|---|---|---|---|
| Inadequate TPO elevation | TPO levels do not sufficiently increase to compensate for platelet loss | Alkylating agents, some antimetabolites | Kaushansky, 2016 [21] |
| Reduced Megakaryocyte Sensitivity to TPO | Megakaryocyte precursors fail to respond effectively to TPO stimulation | Platinum-based chemotherapy, targeted therapies | ASCO, 2023 [22] |
| Liver Dysfunction Affecting TPO Production | Impaired hepatic synthesis of TPO leads to prolonged thrombocytopenia | Chemotherapy drugs affecting liver function (e.g., methotrexate, high-dose cyclophosphamide) | Kaushansky, 2016 [21] |
Table 5.
Chemotherapy-Induced Thrombocytopenia (CIT) and Its Clinical Manifestations [30].
Table 5.
Chemotherapy-Induced Thrombocytopenia (CIT) and Its Clinical Manifestations [30].
| CIT Grade | Platelet Count (×10⁹/L) | Clinical Manifestations | Recommended Intervention |
|---|---|---|---|
| Grade 1–2 | 50–150 | Often asymptomatic or subtle signs such as petechiae, minimal bleeding | Mild thrombocytopenia, no intervention required |
| Grade 3 | 25–50 | Noticeable symptoms, including easy bruising, ecchymoses, and mucosal bleeding | Hold or reduce chemotherapy; consider platelet transfusion if bleeding occurs. |
| Grade 4 | <25 | High risk of major bleeding (GI tract, intracranial, retroperitoneal hemorrhages) | Immediate platelet transfusion; discontinue causative therapy if needed. |
Table 6.
Incidence of Chemotherapy-Induced Thrombocytopenia (CIT) in Gastrointestinal Cancers.
| Tumor Type | Chemotherapy Regimen | Incidence of CIT (%) | Severity & Risk Factors | Reference |
|---|---|---|---|---|
| Colorectal Cancer (CRC) | CAPIRI + bevacizumab (capecitabine, irinotecan, bevacizumab) | Low risk (SUCRA ranking highest in safety) | Lower thrombocytopenia risk compared to platinum-based regimens | Zhan et al., 2024 [20] |
| FOLFIRI + bevacizumab (5-FU, leucovorin, irinotecan, bevacizumab) | Low risk | Minimal platelet suppression | Zhan et al., 2024 [20] | |
| CAPIRI + cetuximab (capecitabine, irinotecan, cetuximab) | Low risk | Similar thrombocytopenia risk to FOLFIRI | Zhan et al., 2024 [20] | |
| S-1 + oxaliplatin (SOX) | High risk | Strong association with thrombocytopenia | Zhan et al., 2024 [20] | |
| FOLFOXIRI + bevacizumab (5-FU, leucovorin, oxaliplatin, irinotecan, bevacizumab) | High risk | Increased myelosuppression & platelet reduction | Zhan et al., 2024 [20] | |
| IROX (irinotecan + oxaliplatin) | High risk | Increased risk due to dual cytotoxic effects | Zhan et al., 2024 [20] | |
| Pancreatic Cancer | Gemcitabine-based regimens | 20-30% | High thrombocytopenia incidence, worsened by combination therapies | Wu et al., 2024 [4] |
| FOLFIRINOX (5-FU, leucovorin, oxaliplatin, irinotecan) | 20-25% (Grade 3-4 CIT) | Higher thrombocytopenia risk vs. gemcitabine alone | Shaw et al., 2024 [29] | |
| Gastric Cancer | FUOX (5-FU, oxaliplatin) | Moderate to High | Platinum-based agents contribute to thrombocytopenia | Zhan et al., 2024 [20] |
| Hepatocellular Carcinoma (HCC) | Platinum-based chemotherapy (cisplatin, oxaliplatin) | 30-40% | Liver dysfunction exacerbates platelet depletion | Shaw et al., 2024 [29] |
| Esophageal Cancer | 5-FU + Cisplatin | 13-25% | Increased thrombocytopenia risk with combination chemotherapy | Wu et al., 2024 [4] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



