Submitted:
25 July 2025
Posted:
28 July 2025
You are already at the latest version
Abstract
A 45-year-old female with a history of livestock exposure presented to our tertiary care centre with progressive shortness of breath and dry cough for one year. There were no systemic signs of illness, and vitals were stable. Routine blood investigations were normal. Chest radiography showed a large, well-defined lesion in the left mid and lower lung zones with a characteristic acute angle to the pleura, suggestive of a pulmonary cyst. Cytological examination of the cyst fluid revealed numerous scolices, rostellum with hooklets, and calcific spherules. Histopathological analysis showed a lamellated, hyalinized cyst wall with fibrin and haemorrhage along with an inflamed pericyst. This case highlights a pulmonary hydatid cyst, managed successfully with a minimally invasive right posterolateral thoracotomy. The classical cytological characteristic features not only help confirm the diagnosis but also aid in differentiating it from other mimics.
Keywords:
Pulmonary hydatid cyst
; Echinococcus granulosus
; cytological diagnosis
; protoscolices
; albendazole therapy
; zoonotic parasitic infection
; differential diagnosis
Introduction
Hydatid disease, also known as echinococcosis, is a globally prevalent zoonotic infection caused by the larval stages of cestodes belonging to the genus Echinococcus [1]. The most common etiologic agent, Echinococcus granulosus, is responsible for cystic echinococcosis (CE), a parasitic disease that poses a significant public health concern in regions where animal husbandry and pastoral farming are commonly practiced under suboptimal hygienic conditions [2,3]. These endemic areas include parts of the Middle East, Africa, South America, Eastern Europe, Central Asia, and the Indian subcontinent. The disease is transmitted through a complex two-host life cycle, involving canids (typically dogs) as definitive hosts and ungulates, such as sheep, cattle, pigs, and goats, as intermediate hosts. Humans are accidental intermediate hosts who become infected through the ingestion of parasite eggs, usually via contaminated food, water, or direct contact with infected dogs [4,5].
Once ingested, the eggs hatch in the human duodenum, releasing oncospheres that penetrate the intestinal mucosa and enter the portal circulation. The liver serves as the primary filter, and the lungs serve as the secondary filter. Consequently, the liver and lungs are the most common sites of cyst development [6,7]. Pulmonary hydatid disease accounts for approximately 10–30% of cases and is more prevalent in younger individuals. The cysts grow slowly over several months to years, often remaining asymptomatic until they reach a size sufficient to exert pressure on adjacent structures. When symptoms do occur, they typically include cough, chest pain, dyspnea, and occasionally hemoptysis [8].
The diagnosis of pulmonary hydatid cysts relies heavily on imaging modalities such as chest radiography and computed tomography (CT), which can identify characteristic features, including well-defined, spherical lesions with smooth borders [9,10]. However, these imaging findings may not always be definitive, particularly in differentiating hydatid cysts from other pulmonary masses such as abscesses, neoplasms, or congenital bronchogenic cysts. In such cases, cytological analysis of aspirated cyst fluid or surgically excised specimens can provide critical diagnostic information. The presence of scolices, hooklets, and laminated membrane fragments is pathognomonic for hydatid disease and helps distinguish it from other parasitic or neoplastic lesions [11,12].
Although serological tests, such as ELISA and indirect hemagglutination assay, can support the diagnosis, they often lack sensitivity in cases of isolated pulmonary hydatid disease. Therefore, cytopathological confirmation remains a cornerstone in ambiguous cases or in regions where advanced serological testing is not readily available [13,14].
Management of hydatid disease is multifaceted and depends on the size, location, and number of cysts, as well as the patient’s clinical status. Albendazole is the drug of choice for medical therapy and is often administered pre- and post-operatively to reduce the risk of recurrence. Surgical resection remains the definitive treatment for large or symptomatic pulmonary cysts, with minimally invasive techniques now playing an increasing role in management [15,16,17].
This report presents a classic case of a large pulmonary hydatid cyst in a middle-aged woman with significant exposure to livestock. The diagnosis was confirmed through cytological and histopathological examination, highlighting the importance of recognizing the classical cytological features and differentiating them from mimics such as Taenia solium cysts. Through this case, we aim to underscore the role of cytology in establishing an accurate diagnosis and guiding appropriate management in resource-limited settings.
Case
A 45-year-old woman with a history of livestock exposure presented with progressive shortness of breath and a dry cough persisting for one year. She denied hemoptysis, fever, or other systemic symptoms. On examination, vital signs were stable, and there were no systemic signs of illness. Routine blood investigations were within normal limits.
Chest radiography revealed a large, well-circumscribed lesion in the left mid and lower lung zones, forming an acute angle with the pleura, suggestive of a pulmonary cyst (Figure 1). A contrast-enhanced CT scan of the thorax demonstrated a unilocular cystic lesion measuring 12.4 × 10.6 × 11 cm in the left upper lobe, causing mild compression of the adjacent bronchus with associated air trapping (Figure 2). There was no evidence of calcification or mediastinal lymphadenopathy.
The patient was admitted for planned surgical resection of a suspected pulmonary hydatid cyst. Preoperative management included albendazole 400 mg twice daily for cyst sterilization. She underwent surgical excision of the cyst via a left posterolateral thoracotomy.
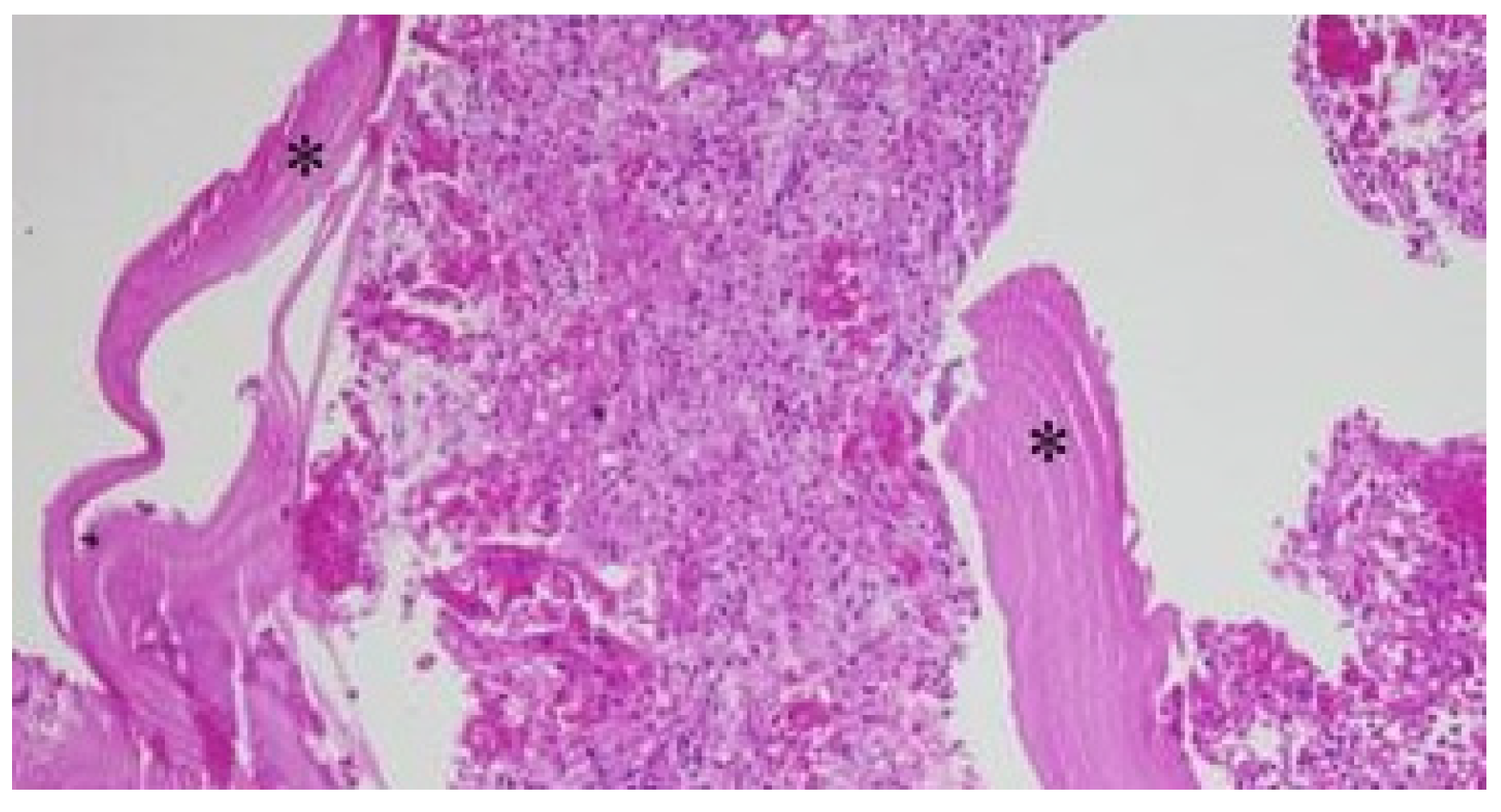
Cytological examination of the cyst fluid revealed numerous scolices, protoscolices with hooklets, and calcified spherules (Figure 3, Figure 4, Figure 5 and Figure 6). Histopathological analysis showed a lamellated, hyalinized cyst wall with areas of fibrin deposition and hemorrhage (Figure 7). The pericyst consisted of fibrocollagenous tissue with lymphocytic and plasmacytic infiltration.
Postoperative recovery was uneventful. The patient was extubated on the day of surgery and discharged in stable condition with instructions to continue albendazole therapy for three months.
Discussion
Hydatid cyst (HC) disease, or cystic echinococcosis (CE), is a chronic zoonotic infection caused primarily by the larval form of Echinococcus granulosus, a cestode of the family Taeniidae [18]. Less frequently, Echinococcus multilocularis, the causative agent of alveolar echinococcosis, can result in a more aggressive disease pattern, particularly affecting the liver and mimicking malignancy [2,19]. Hydatid disease remains a significant public health challenge in many developing and resource-limited regions, particularly in areas where livestock rearing and animal-human interactions occur without effective veterinary control measures. Countries in the Mediterranean basin, South America, Central Asia, Sub-Saharan Africa, and parts of India and China report some of the highest disease burdens globally [20,21].
The life cycle of Echinococcus granulosus involves two types of hosts: definitive and intermediate. The adult worm resides in the small intestine of definitive hosts—primarily dogs, but also other canids like wolves, foxes, and jackals [4,22]. These hosts excrete parasitic eggs through their feces, contaminating soil, water, and vegetation. Intermediate hosts, such as sheep, cattle, goats, and pigs, ingest these eggs while grazing. Humans become accidental intermediate hosts through the ingestion of contaminated food or water or via hand-to-mouth transmission following direct contact with infected dogs [23,24].
Once inside the human digestive tract, the eggs hatch in the duodenum, releasing oncospheres that penetrate the intestinal mucosa and enter the portal circulation [6,25]. The liver acts as the primary filter, trapping most larvae, which subsequently develop into cysts [7]. Those that bypass the hepatic filter may enter the pulmonary circulation—the secondary filter—leading to cyst formation in the lungs. Although hepatic hydatid cysts are more common overall, pulmonary hydatid disease is also frequently encountered, particularly in younger patients and in specific geographic locations [26,27].
Pulmonary hydatid cysts can remain asymptomatic for extended periods, sometimes even years, due to the slow growth of the cysts and the lungs’ ability to accommodate expanding masses without early signs of distress [7,28]. However, as the cyst enlarges, it can compress adjacent bronchovascular structures, resulting in symptoms such as a non-productive cough, chest pain, hemoptysis, and dyspnea. In rare cases, cyst rupture can lead to life-threatening complications such as anaphylaxis, bronchospasm, secondary bacterial infection, or dissemination into other organ systems [29].
Approximately 60% of pulmonary hydatid cysts are located in the right lung, with a predilection for the lower lobes, likely due to gravitational and anatomical factors. Bilateral involvement is observed in about 20% of cases. The size and number of cysts can vary, and multiple cysts may co-exist in both lungs or conjunction with hepatic cysts [30].
Radiological evaluation plays a pivotal role in the diagnosis of pulmonary hydatid disease. Plain chest radiography is often the initial diagnostic modality, revealing well-defined, spherical, homogenous opacities, often with smooth contours. Features such as the “water lily sign” or the “crescent sign” may indicate cyst rupture or partial collapse. However, chest radiography lacks specificity and sensitivity, particularly in distinguishing hydatid cysts from other cystic lesions or neoplasms [31].
High-resolution computed tomography (CT) provides superior diagnostic accuracy, especially for evaluating lesion morphology, cyst wall integrity, and potential complications such as rupture, infection, or daughter cyst formation. CT scans typically show well-circumscribed, hypoattenuating lesions with or without septations. In this case, CT imaging revealed a unilocular cyst measuring 12.4 × 10.6 × 11.0 cm in the left upper lobe, with mild compression of the left upper lobe bronchus and associated air trapping. No calcification or mediastinal lymphadenopathy was present, findings that further supported a diagnosis of an uncomplicated pulmonary hydatid cyst [32,33].
While imaging plays a central role, cytological analysis remains an indispensable diagnostic tool, particularly in distinguishing hydatid cysts from other mimics such as Taenia solium cysticercosis, congenital bronchogenic cysts, lung abscesses, and neoplastic lesions. Aspiration cytology, when performed under controlled conditions and in selected cases, can provide definitive evidence of hydatid disease by identifying key parasitological structures [34,35].
The classical cytological features include the presence of protoscolices, hooklets, and fragments of the laminated cyst wall. Protoscolices are small larval forms equipped with suckers and hooklets, which appear as birefringent refractile structures under microscopy. The rostellar hooklets are particularly diagnostic, forming a double row that can be visualized on high-power and oil immersion microscopy. In the presented case, cytological smears showed abundant scolices, hooklets, and calcified spherules, confirming the diagnosis of a hydatid cyst [11,36].
Histopathological examination of the excised cysts further supports the diagnosis and provides insight into the host’s inflammatory response. The typical hydatid cyst comprises three layers: the outer pericyst, formed by host tissue (fibrocollagenous), the middle laminated acellular layer, and the inner germinal layer where brood capsules and protoscolices develop. The pericyst may demonstrate chronic inflammatory infiltrates including lymphocytes, plasma cells, and occasionally eosinophils. In our case, the histology revealed a hyalinized, lamellated cyst wall with associated fibrin and hemorrhage, as well as a pericyst containing inflammatory cells—findings consistent with hydatid disease [37,38].
Differential diagnosis of pulmonary hydatid cysts is essential, particularly in endemic regions where other infections and malignancies are prevalent. Conditions that mimic hydatid cysts radiologically include lung abscesses, bronchogenic cysts, tuberculosis, metastatic tumors with cystic necrosis, and fungal infections such as aspergillosis. Cytological and histopathological examinations are invaluable in resolving such diagnostic dilemmas. Importantly, care must be taken during fine needle aspiration procedures, as puncturing a live hydatid cyst can lead to spillage of hydatid fluid and cause anaphylactic shock or secondary dissemination [39,40].
Serological tests such as ELISA, indirect hemagglutination, immunoblot, and latex agglutination are adjunctive tools in diagnosis, particularly in hepatic disease. However, their sensitivity for isolated pulmonary hydatid disease remains low (as low as 50–60%) due to reduced antigenic stimulus and lower systemic antibody levels. Thus, negative serology does not exclude pulmonary echinococcosis, reinforcing the need for correlation with radiological and cytological findings [13,41].
Therapeutic management of pulmonary hydatid disease involves a multidisciplinary approach integrating medical and surgical modalities. Albendazole remains the cornerstone of pharmacological therapy, often administered preoperatively for 1–4 weeks to sterilize the cyst, reduce intracystic pressure, and decrease the risk of spillage during surgery. Postoperative continuation of albendazole for 1–3 months helps reduce the risk of recurrence. In selected patients, mebendazole or praziquantel may be considered as alternative or adjunctive agents [42,43].
Surgical intervention is the definitive treatment for large, symptomatic, or complicated cysts. Procedures include cystotomy with or without capitonnage, pericystectomy, or segmental lung resection, depending on the cyst size, location, and presence of complications. Minimally invasive approaches such as video-assisted thoracoscopic surgery (VATS) are increasingly preferred due to reduced morbidity and faster recovery. In our case, the patient underwent successful excision via a left posterolateral thoracotomy, with an uneventful postoperative course [44,45].
Non-surgical options, such as percutaneous aspiration, instillation, and re-aspiration (PAIR), have shown promise in treating hepatic hydatid cysts but are generally avoided in pulmonary cases due to the risk of cyst rupture into the bronchial tree and resultant complications [46,47].
Public health interventions remain crucial for controlling and preventing hydatid disease. Strategies include regular deworming of dogs, proper disposal of livestock offal, public education regarding hygiene and food safety, improved meat inspection, and surveillance of infection in animal populations. Vaccination of intermediate hosts, such as sheep, using recombinant antigens (e.g., EG95) has shown promise in pilot studies and may become a future tool for control in endemic areas [48,49].
Pulmonary hydatid disease, while uncommon in many developed regions, remains an important differential diagnosis for cystic lung lesions in endemic areas. This case underscores the value of integrating clinical history, imaging, cytology, and histopathology in the diagnosis and management of pulmonary hydatid cysts. Cytological examination, in particular, plays a pivotal role in identifying classical parasitic features that confirm the diagnosis and help exclude mimics. Early recognition and appropriate intervention can prevent complications and ensure favorable outcomes. As global travel and migration increase, clinicians worldwide should remain vigilant for this neglected but significant parasitic disease [50,51].
Limitations
This case report highlights the classical cytological features of pulmonary hydatid disease; however, its single-patient scope limits generalizability. Although cytological and histopathological analyses confirmed the diagnosis, serological testing results were not included, which could have added diagnostic depth and comparative value. Furthermore, while imaging findings were suggestive, advanced imaging modalities such as MRI or PET-CT, which may aid in differentiating complex or recurrent cysts, were not utilized. The cytological sampling, although definitive in this case, carries a risk of cyst rupture and anaphylaxis, a concern not addressed in procedural detail. Follow-up data beyond the immediate postoperative period is also lacking, limiting insight into long-term outcomes or recurrence. Lastly, no molecular or genotypic analysis of the Echinococcus species was performed, which could have provided epidemiological relevance, especially in endemic settings. Future studies incorporating larger patient cohorts, serology, and molecular diagnostics are necessary to validate and expand upon these findings.
Conclusions
Pulmonary hydatid disease, though uncommon in many regions, remains a critical differential diagnosis for cystic lung lesions, particularly in endemic areas with ongoing zoonotic transmission. This case underscores the diagnostic value of integrating clinical history, imaging, cytopathology, and histopathology in identifying classical features of Echinococcus granulosus infection. Cytological examination, in particular, proved instrumental in confirming the diagnosis by revealing scolices, hooklets, and laminated membranes—hallmark findings that distinguish hydatid cysts from other parasitic or cystic pulmonary conditions. Early recognition and timely surgical intervention, complemented by albendazole therapy, ensured favorable clinical outcomes. Despite the success in this case, broader efforts in public health education, veterinary control, and preventive strategies remain essential for long-term disease control. Moreover, cytological expertise and access to diagnostic infrastructure are pivotal, especially in resource-limited settings. Continued documentation of such classical presentations can aid clinicians and pathologists in refining their diagnostic approach to pulmonary parasitic diseases.
Funding
The current article processing charges (publication fees) were funded by the Facultad de Ciencias Médicas (FCM) (2-03-01-01), Universidad Nacional Autonoma de Honduras (UNAH), Tegucigalpa, MDC, Honduras, Central America (granted to Zambrano).
Ethical statement
We confirm that the manuscript has been read and approved by all named authors and that no other persons have satisfied the criteria for authorship but are not listed. We further confirm that all have approved the order of authors listed in the manuscript. The material is original and is not under consideration for publication elsewhere. Written informed consent signed by the patient was obtained for the publication of this case.
Acknowledgements
This article has been registered in the Research Proposal Registration of the Coordination of Scientific Integrity and Surveillance of Universidad Cientifica del Sur, Lima, Peru.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
- Rodriguez-Morales, A.J.; Bolivar-Mejia, A.; Calvo-Betancourt, L.S.; Alarcón-Olave, C. Echinococcosis in Colombia — A Neglected Zoonosis? In Current Topics in Echinococcosis; Rodriguez-Morales, A.J., Ed.; IntechOpen: Rijeka, 2015. [Google Scholar] [CrossRef]
- Gessese, A.T. Review on Epidemiology and Public Health Significance of Hydatidosis. Vet Med Int 2020, 2020, 8859116. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Sarmiento, D.; Chiluisa-Utreras, V. First molecular identification of hydatid tapeworm Echinococcus granulosus sensu lato G6/G7 in Ecuador. J Helminthol 2019, 94, e100. [Google Scholar] [CrossRef] [PubMed]
- Hernández, F.; Verdugo, C.; Cárdenas, F.; Sandoval, R.; Morales, N.; Olmedo, P.; Bahamonde, A.; Aldridge, D.; Acosta-Jamett, G. Echinococcus Granulosus in the Endangered Patagonian Huemul (Hippocamelus bisulcus). J Wildl Dis 2019, 55, 694–698. [Google Scholar] [CrossRef]
- Shamsi, S.; McSpadden, K.; Baker, S.; Jenkins, D.J. Occurrence of tongue worm, Linguatula cf. serrata (Pentastomida: Linguatulidae) in wild canids and livestock in south-eastern Australia. Int J Parasitol Parasites Wildl 2017, 6, 271–277. [Google Scholar] [CrossRef]
- Aili, A.; Peng, L.; Zhang, J.; Liu, Y.; Peng, L.; Yi, Q.; Zhou, H. Hydatid Pulmonary Embolism: A Case Report and Literature Review. Am J Case Rep 2021, 22, e934157. [Google Scholar] [CrossRef]
- Almutairi, A.; Al Rajhi, S. Case Report of Hydatid Cyst in the Pulmonary Artery Uncommon Presentation: CT and MRI Findings. Case Rep Radiol 2018, 2018, 1301072. [Google Scholar] [CrossRef]
- Aydin, S.; Tek, C.; Dilek Gokharman, F.; Fatihoglu, E.; Nercis Kosar, P. Isolated hydatid cyst of thyroid: An unusual case. Ultrasound 2018, 26, 251–253. [Google Scholar] [CrossRef]
- Çobanoğlu, U.; Aşker, S.; Mergan, D.; Sayır, F.; Bilici, S.; Melek, M. Diagnostic Dilemma in Hydatid Cysts: Tumor-Mimicking Hydatid Cysts. Turk Thorac J 2015, 16, 180–184. [Google Scholar] [CrossRef]
- Mehta, P.; Prakash, M.; Khandelwal, N. Radiological manifestations of hydatid disease and its complications. Trop Parasitol 2016, 6, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Arora, V.K.; Chopra, N.; Singh, P.; Venugopal, V.K.; Narang, S. Hydatid cyst of parotid: Report of unusual cytological findings extending the cytomorphological spectrum. Diagn Cytopathol 2016, 44, 770–773. [Google Scholar] [CrossRef]
- Davakis, S.; Syllaios, A.; Kyros, E.; Garmpis, N.; Charalabopoulos, A. An extraordinary rare presentation of liver hydatidosis with hydatid cyst scolices. Clin Case Rep 2020, 8, 2298–2299. [Google Scholar] [CrossRef]
- Engström, E.L.S.; Salih, G.N.; Wiese, L. Seronegative, complicated hydatid cyst of the lung: A case report. Respir Med Case Rep 2017, 21, 96–98. [Google Scholar] [CrossRef] [PubMed]
- Khefacha, F.; Touati, M.D.; Bouzid, A.; Ayadi, R.; Landolsi, S.; Chebbi, F. A rare case report: Primary isolated hydatid cyst of the spleen- diagnosis and management. Int J Surg Case Rep 2024, 120, 109869. [Google Scholar] [CrossRef] [PubMed]
- Aydin, Y.; Ulas, A.B.; Ahmed, A.G.; Eroglu, A. Pulmonary Hydatid Cyst in Children and Adults: Diagnosis and Management. Eurasian J Med 2022, 54, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Koirala, D.P.; Yadav, M.; Shah, N.A.; Yadav, D.; Neupane, S.; Yadav, C. Giant isolated splenic hydatid cyst in a pediatric patient: A rare case report. Int J Surg Case Rep 2024, 120, 109768. [Google Scholar] [CrossRef]
- Zhu, A.; Tan, C.; Meredith, G.; Chard, R. Minimally invasive surgical resection of a large primary pulmonary hydatid cyst: A thoracoscopic approach. J Surg Case Rep 2023, 2023, rjad090. [Google Scholar] [CrossRef]
- Mirlohi, S.H.; Tajfirooz, S.; Raji, H.; Akhavan, S. Coexistence of kidney and lung hydatid cyst in a child: A case report. Respir Med Case Rep 2024, 52, 102138. [Google Scholar] [CrossRef]
- Khan, A.; Ahmed, H.; Simsek, S.; Liu, H.; Yin, J.; Wang, Y.; Shen, Y.; Cao, J. Molecular characterization of human Echinococcus isolates and the first report of E. canadensis (G6/G7) and E. multilocularis from the Punjab Province of Pakistan using sequence analysis. BMC Infect Dis 2020, 20, 262. [Google Scholar] [CrossRef]
- Sarkar, M.; Pathania, R.; Jhobta, A.; Thakur, B.R.; Chopra, R. Cystic pulmonary hydatidosis. Lung India 2016, 33, 179–191. [Google Scholar] [CrossRef]
- Zheng, X.; Zou, Y.; Yin, C. Rare presentation of multi-organ abdominal echinococcosis: Report of a case and review of literature. Int J Clin Exp Pathol 2015, 8, 11814–11818. [Google Scholar]
- Heidari, Z.; Sharbatkhori, M.; Mobedi, I.; Mirhendi, S.H.; Nikmanesh, B.; Sharifdini, M.; Mohebali, M.; Zarei, Z.; Arzamani, K.; Kia, E.B. Echinococcus multilocularis and Echinococcus granulosus in canines in North-Khorasan Province, northeastern Iran, identified using morphology and genetic characterization of mitochondrial DNA. Parasit Vectors 2019, 12, 606. [Google Scholar] [CrossRef] [PubMed]
- Nocerino, M.; Pepe, P.; Bosco, A.; Ciccone, E.; Maurelli, M.P.; Boué, F.; Umhang, G.; Pellegrini, J.; Lahmar, S.; Said, Y.; et al. An innovative strategy for deworming dogs in Mediterranean areas highly endemic for cystic echinococcosis. Parasit Vectors 2024, 17, 86. [Google Scholar] [CrossRef]
- Pipas, M.J.; Fowler, D.R.; Bardsley, K.D.; Bangoura, B. Survey of coyotes, red foxes and wolves from Wyoming, USA, for Echinococcus granulosus s. l. Parasitol Res 2021, 120, 1335–1340. [Google Scholar] [CrossRef]
- Arıbaş, E.T.; Metin, B.; Dumanlı, A.; Arıbaş, O.K. Concomitant Occurrence of Hepatopulmonary hydatid Cysts in Turkey. Iran J Parasitol 2021, 16, 506–511. [Google Scholar] [CrossRef]
- Alene, D.; Maru, M.; Demessie, Y.; Mulaw, A. Evaluating zoonotic metacestodes: Gross and histopathological alterations of beef in north-west Ethiopia one health approach for meat inspection and animal management. Front Vet Sci 2024, 11, 1411272. [Google Scholar] [CrossRef]
- Shrestha, A.; Shrestha, A.K.; Deo, A.; Sharma, G.R. Intramuscular hydatid cyst of paraspinal muscle: A diagnostic challenge. Clin Case Rep 2023, 11, e8105. [Google Scholar] [CrossRef] [PubMed]
- Pangeni, R.P.; Regmi, P.R.; Khadka, S.; Timilsina, B. Ruptured pulmonary hydatid cyst presenting as hemoptysis in TB endemic country: A case report. Ann Med Surg (Lond) 2022, 78, 103836. [Google Scholar] [CrossRef] [PubMed]
- Zayati, M.; Chaouch, M.A.; Mokni, S.; Maaref, M.; Gafsi, B.; Noomen, F. Peritoneal hydatidosis secondary to an asymptomatic liver hydatid cyst rupture: A case report. Int J Surg Case Rep 2024, 123, 110220. [Google Scholar] [CrossRef]
- Onal, O.; Demir, O.F. The relation between the location and the perforation rate of lung hydatid cysts in children. Asian J Surg 2018, 41, 422–426. [Google Scholar] [CrossRef]
- Sadashiva, N.; Shukla, D.; Devi, B.I. Rupture of Intraventricular Hydatid Cyst: Camalote Sign. World Neurosurg 2018, 110, 115–116. [Google Scholar] [CrossRef]
- Ichimura, H.; Ozawa, Y.; Shiigai, M.; Shiotani, S.; Kikuchi, K.; Sato, Y. Enlarged mediastinal air cyst in a patient with bronchial diverticula localized in the left main bronchus: A case report with surgical and bronchoscopic findings. Surg Case Rep 2017, 3, 1. [Google Scholar] [CrossRef] [PubMed]
- Pawar, P.A.; Deshmukh, P.P.; Deshpande, M.; Pusate, A.A. Asymptomatic Presentation of Large Cardiac Ball. J Assoc Physicians India 2016, 64, 96–97. [Google Scholar]
- Bhardwaj, S.; Rather, G. Fine Needle Aspiration Cytology of Cysticercosis: A Study of 30 Cases. J Cytol 2019, 36, 18–21. [Google Scholar] [CrossRef]
- Goyal, S.; Goyal, S. Cysticercosis: A case of missed diagnosis. Diagn Cytopathol 2022, 50, E214–e216. [Google Scholar] [CrossRef]
- Apte, O.; Bhartendu, B.; Panwar, V.K.; Prajapati, T.; Phulware, R.H. Cytomorphology of Renal Hydatid Cyst Mimicking as Simple Renal Cyst. Cytopathology 2025. [Google Scholar] [CrossRef] [PubMed]
- Beigh, A.B.; Darzi, M.M.; Bashir, S.; Kashani, B.; Shah, A.; Shah, S.A. Gross and histopathological alterations associated with cystic echinococcosis in small ruminants. J Parasit Dis 2017, 41, 1028–1033. [Google Scholar] [CrossRef]
- Hidalgo, C.; Stoore, C.; Strull, K.; Franco, C.; Corrêa, F.; Jiménez, M.; Hernández, M.; Lorenzatto, K.; Ferreira, H.B.; Galanti, N.; et al. New insights of the local immune response against both fertile and infertile hydatid cysts. PLoS ONE 2019, 14, e0211542. [Google Scholar] [CrossRef] [PubMed]
- Chhabria, B.A.; Agarwal, R.; Garg, M.; Gupta, N.; Bal, A.; Dhooria, S.; Sehgal, I.S. A rare cause of airway obstruction: Mediastinal cyst secondarily infected with Mycobacterium tuberculosis. Lung India 2018, 35, 421–424. [Google Scholar] [CrossRef]
- Kara, T.; Arpaci, R.B.; Vayisoğlu, Y.; Serinsöz, E.; Gürsoy, D.; Özgür, A.; Apaydin, D.; Özcan, C. Hydatid Cyst of Parotid Gland: An Unusual Case Diagnosed by Fine Needle Aspiration Biopsy. Turk Patoloji Derg 2017, 33, 171–174. [Google Scholar] [CrossRef]
- Parlak, E.; Kerget, F.; Demirdal, T.; Şen, P.; Ulaş, A.B.; Öztürk Durmaz, Ş.; Pekok, U.; Ertürk, A.; Akyol, D.; Kepenek Kurt, E.; et al. The Epidemiology, Clinical Manifestations, Radiology, Microbiology, Treatment, and Prognosis of Echinococcosis: Results of NENEHATUN Study. Vector Borne Zoonotic Dis 2021, 21, 948–954. [Google Scholar] [CrossRef]
- Gök, H.; Başkurt, O. Giant Primary Intracranial Hydatid Cyst in Child with Hemiparesis. World Neurosurg 2019, 129, 404–406. [Google Scholar] [CrossRef]
- Pavlidis, E.T.; Galanis, I.N.; Pavlidis, T.E. Current considerations for the management of liver echinococcosis. World J Gastroenterol 2025, 31, 103973. [Google Scholar] [CrossRef]
- Incekara, F.; Findik, G.; Turk, İ.; Erturk, H.; Aydogdu, K.; Apaydin, S.M.K.; Demiröz, S.M.; Demirag, F. Video-Assisted Thoracoscopic Treatment of Coelomic Cysts. J Laparoendosc Adv Surg Tech A 2020, 30, 553–557. [Google Scholar] [CrossRef]
- Li, M.; Yang, C.; Li, J.; Jia, D.; Wang, Y.; Xie, W.; Wang, J. A large pericardial cyst mimicking a unilateral pleural effusion: A case report. Medicine (Baltimore) 2023, 102, e33540. [Google Scholar] [CrossRef]
- Kalogeropoulu, S.K.; Schwierz, E.; Meyerhoff, M.; Ratjszczak, R.; Nadler, T.; Raphael, B.L. ULTRASOUND-GUIDED PERCUTANEOUS TREATMENT OF HEPATIC HYDATIDOSIS IN TWO RED-SHANKED DOUC LANGURS (PYGATHRIX NEMAEUS). J Zoo Wildl Med 2023, 54, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Peer, S.; Jabbal, H.S.; Singh, P.; M, P.S.; Kakkera, S.; Bhat, P. A case report of successful percutaneous aspiration, injection, and re-aspiration (PAIR) technique for treatment of retrovesical pelvic hydatid cyst. Radiol Case Rep 2023, 18, 331–334. [Google Scholar] [CrossRef]
- Gauci, C.G.; Jenkins, D.J.; Lightowlers, M.W. Protection against cystic echinococcosis in sheep using an Escherichia coli-expressed recombinant antigen (EG95) as a bacterin. Parasitology 2023, 150, 29–31. [Google Scholar] [CrossRef] [PubMed]
- Jazouli, M.; Lightowlers, M.W.; Bamouh, Z.; Gauci, C.G.; Tadlaoui, K.; Ennaji, M.M.; Elharrak, M. Immunological responses and potency of the EG95NC(-) recombinant sheep vaccine against cystic echinococcosis. Parasitol Int 2020, 78, 102149. [Google Scholar] [CrossRef]
- Essolaymany, Z.; Amara, B.; Khacha, A.; El Bouardi, N.; Haloua, M.; Alaoui Lamrani, M.Y.; Boubbou, M.; Serraj, M.; Maâroufi, M.; Alami, B. Hydatid pulmonary embolism underlying cardiac hydatid cysts - A case report. Respir Med Case Rep 2023, 44, 101856. [Google Scholar] [CrossRef] [PubMed]
- Kumar, M.; Harsh, V.; Prakash, A.; Sahay, C.B.; Kumar, A. Neglected Case of Primary Intraorbital Hydatid Cyst. Neurol India 2022, 70, 337–339. [Google Scholar] [CrossRef]
Figure 1.
CXR Large, well-defined lesion in the left mid and lower lung zones with an acute angle to the pleura.
Figure 1.
CXR Large, well-defined lesion in the left mid and lower lung zones with an acute angle to the pleura.
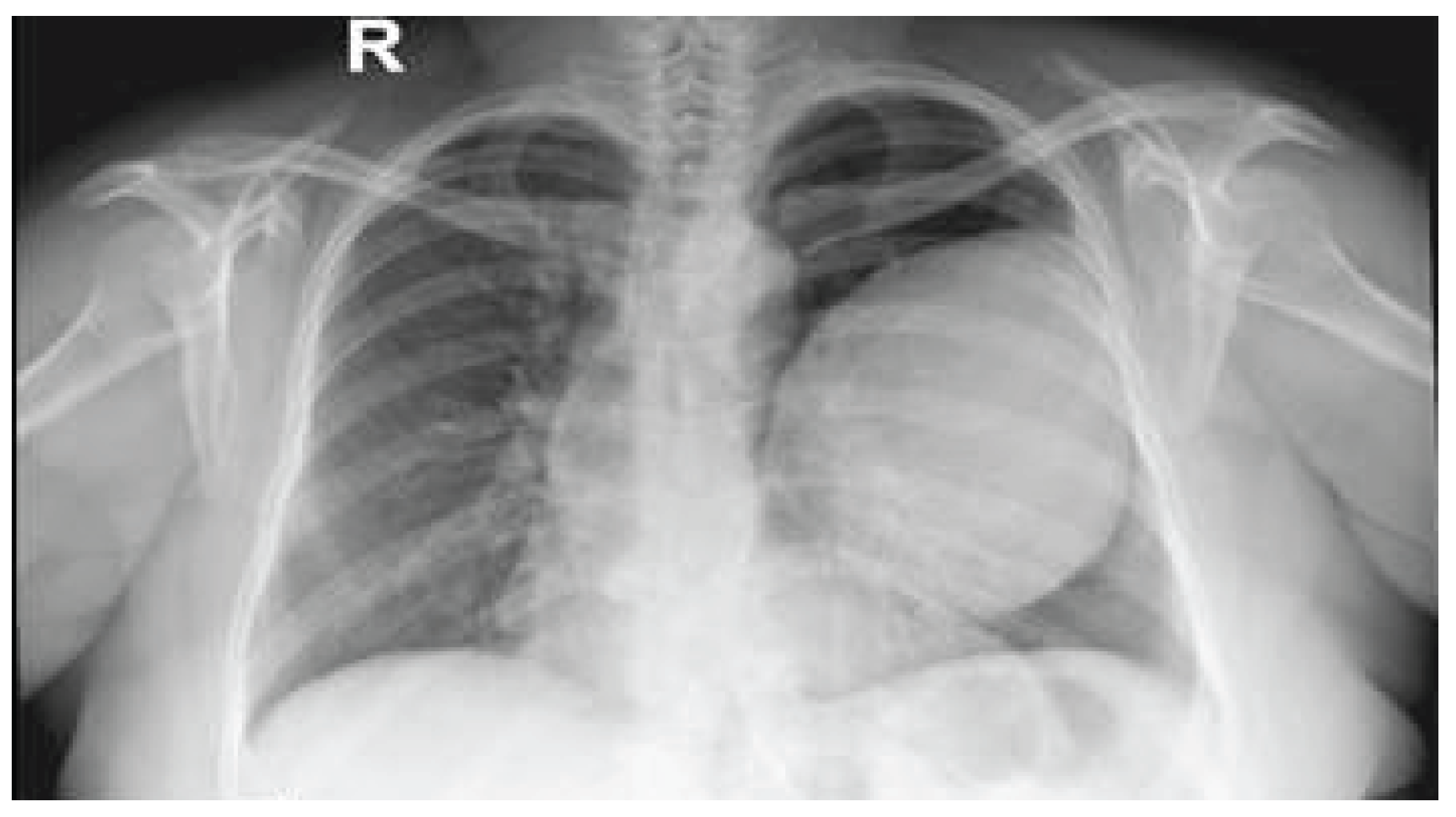
Figure 2.
CT scan showing a unilocular cystic lesion (12.4 × 10.6 × 11 cm) in the left upper lobe, with mild compression of the left upper lobe bronchus with air trapping.
Figure 2.
CT scan showing a unilocular cystic lesion (12.4 × 10.6 × 11 cm) in the left upper lobe, with mild compression of the left upper lobe bronchus with air trapping.

Figure 3.
Giemsa stain at low power (40×) showing abundant complete scolices.
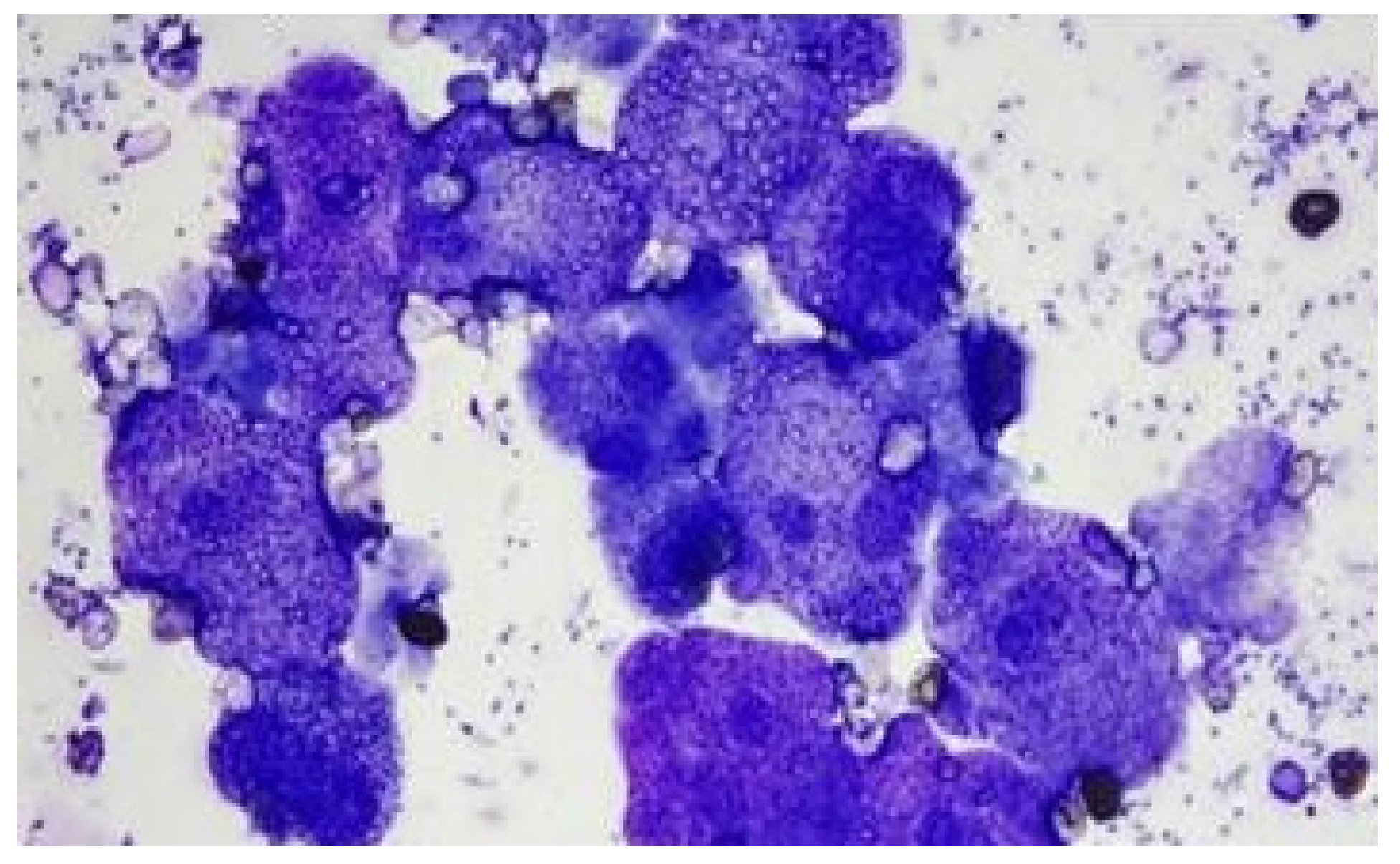
Figure 4.
Scolex showing suckers (red arrows) and rostellum (black arrow).
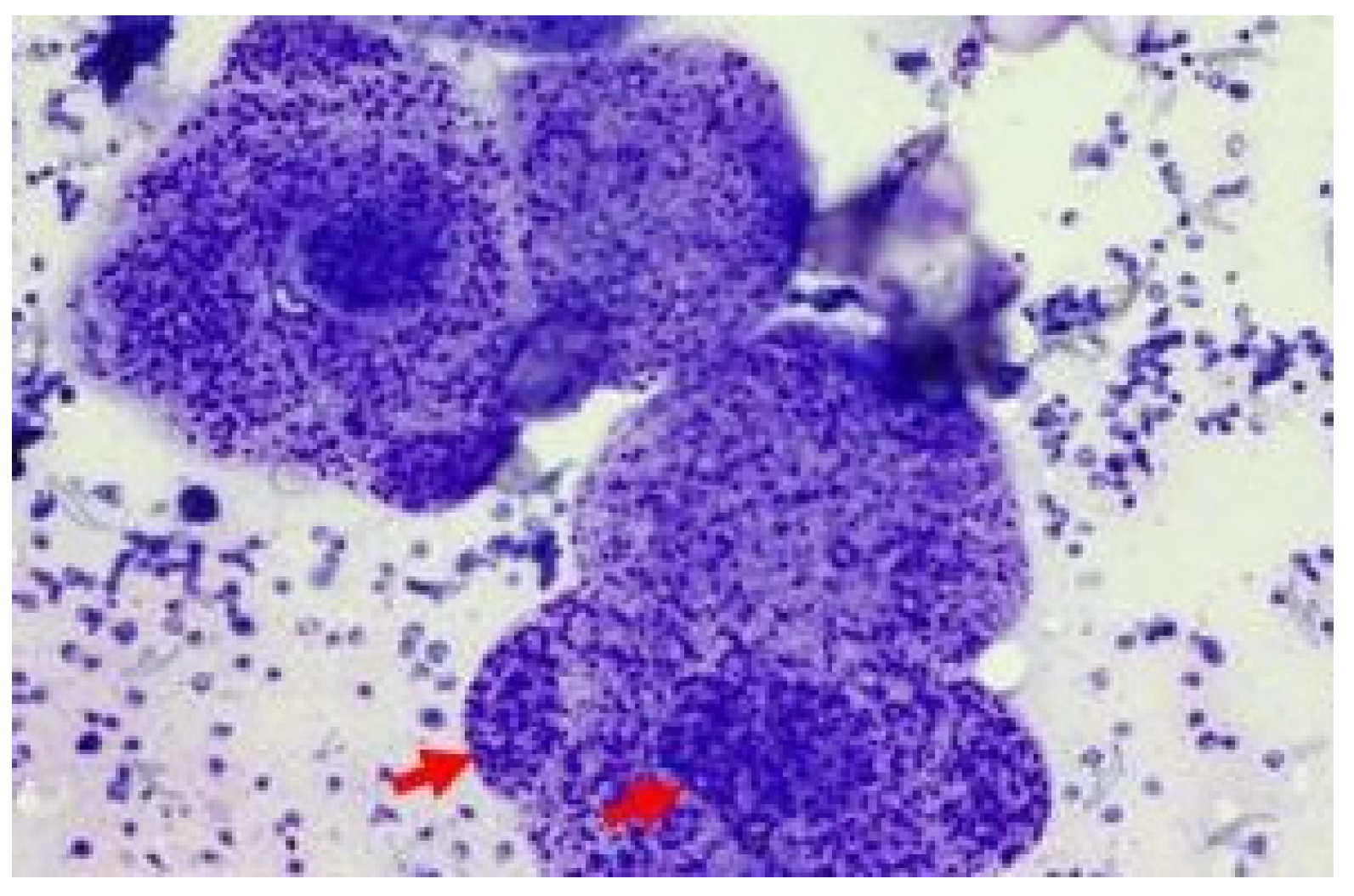
Figure 5.
High power (400×) & oil immersion view of rostellum showing double row of hooklets.
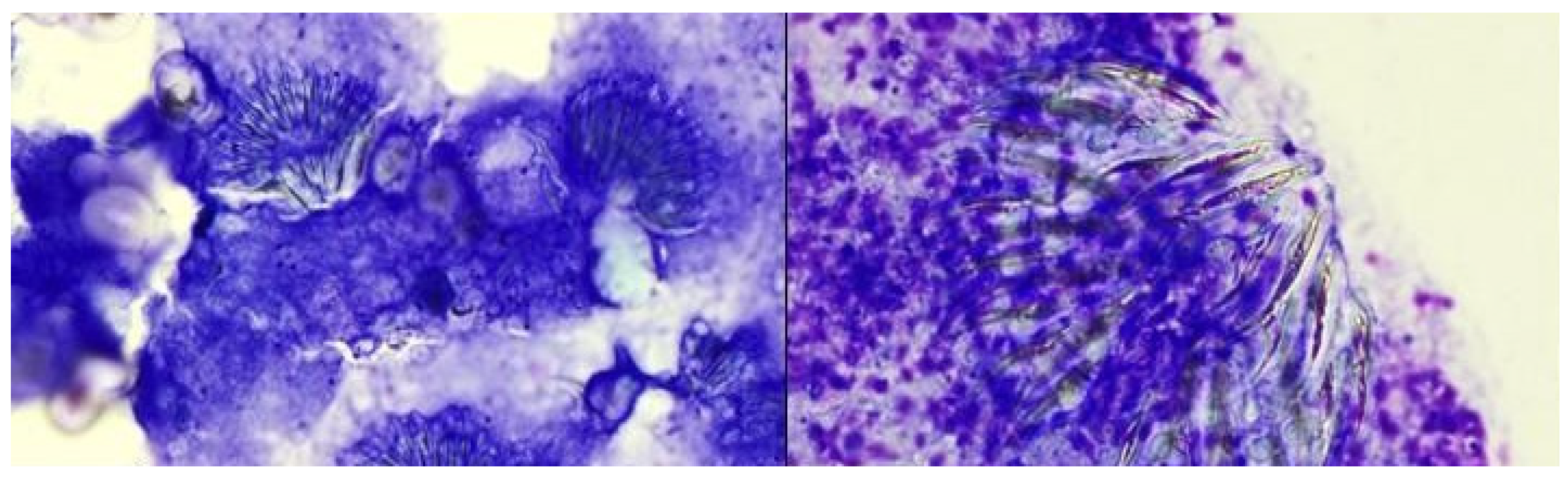
Figure 6.
Oil immersion view of hooklets (all the hooklets are of the same size).
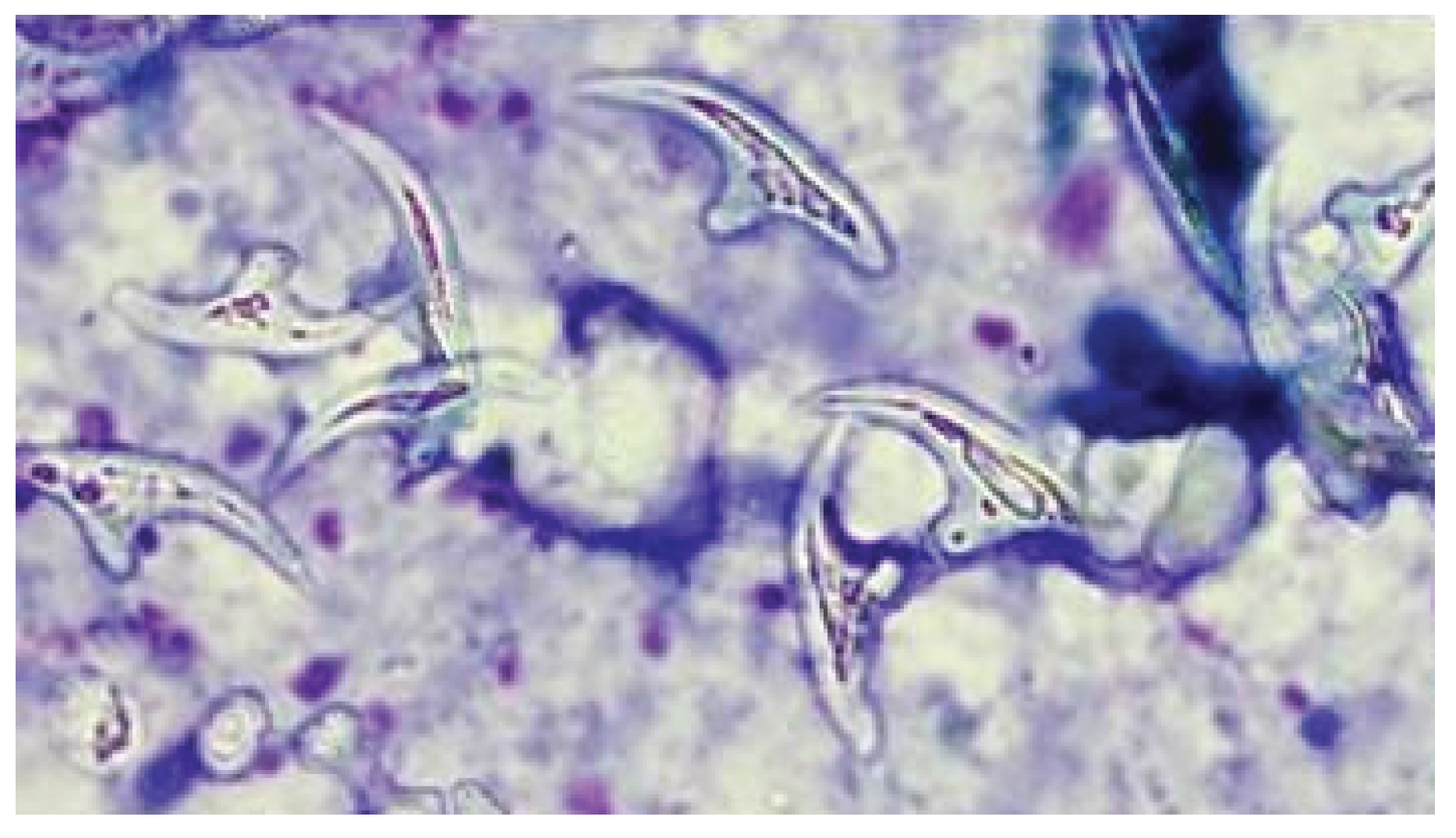
Figure 7.
Hematoxylin & eosin-stained section showing an acellular hyalinizing membrane with a pericyst containing a chronic inflammatory cell infiltrate.
Figure 7.
Hematoxylin & eosin-stained section showing an acellular hyalinizing membrane with a pericyst containing a chronic inflammatory cell infiltrate.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



