Submitted:
22 July 2025
Posted:
23 July 2025
You are already at the latest version
Abstract
Congenital heart defect (CHD), a life-threatening congenital pathology, is reported in about every one neonate among 100 live births, with severity ranged from mild to fatal. The prevalence of CHD is remarkably increasing over decades, most likely due to the evolved diagnostics and improved accessibility of healthcare worldwide. The ratio of severe CHDs, which need surgery urgently, to mild forms, which sometimes do not need surgery, is between 1:4 and 1:3. Therefore, every fourth or fifth newborn with CHD needs the immediate and effective surgical treatment. Furthermore, one out of 10 diagnoses is with multiple CHDs that requires complex surgical treatment and elevates the risk of peri- and post-operative mortality. In this review, we concern epidemiology of CHD, in particular, mostly diagnosed ventricular and atrial septal defects, and patent ductus arteriosus. Next, we focus solely on ventricular septal defects (VSD). We briefly discuss the historical background and current strategies for VSD treatment – open heart surgery, transcatheter surgery, and a mini-invasive hybrid surgery. The hybrid method is then comprehensively discussed including its success and complications rate compared to other two approaches, its implementation, typical delivery approaches, and most common occluder device types; we accompany with our own clinical experience. The advantages and limitations of the hybrid surgery are also highlighted in detail. We summarize that because CHDs need treating with mini-invasive, safe, and effective approach the perspectives for wider using of hybrid surgery are well prominent, especially due to its freedom from cardiopulmonary bypass – the cornerstone of open-heart surgery.
Keywords:
congenital heart disease
; ventricular septal defect
; pediatric patients
; hybrid approach
; hybrid surgery
; mini-invasive surgery
1. Introduction
Congenital heart disease (or congenital heart defects, CHD) encompasses a spectrum of cardiac defects that develop in prenatal period and present sustainably at the birth. CHDs are the leading part of birth defects, which are related to high morbidity, mortality, and excessive healthcare costs. The most common types of CHD include defects in ventricular or atrial septum, valves, and main vessels, and nearly in one of 10 CHD diagnoses there are multiple CHDs. While some types of CHD like tetralogy of Fallot or ventricular muscle defect are relatively frequent among all CHDs [1,2,3], other severe defects like single ventricle occur much rarely [4]. Nevertheless, high proportion of CHD requires urgent surgical correction and, if untreated, these CHDs are strongly life-threatening and mostly fatal. Moreover, the severity of CHD directly contributes to the pre-, peri- and post-operative mortality because it is often that a severe CHD is accompanied by other pathologies and malfunctions, many of them are congenital too. Also, nine out of ten of the world’s babies born with CHD live in locations with little or no care and where mortality remains high [5]. The wide spectrum of CHD brings great economic and social burden. For example, the cost of hospitalizations for individuals with CHDs only in the U.S. exceeded $9.8 billion in 2019 [6], highlighting the significant economic burden associated with CHD care. It is therefore clear that the need for safe and robust surgical treatments of CHD remains high.
In this review, we first describe the epidemiology of CHD, also in regards to regional variation in reported prevalence and mortality, and briefly concern the causation and outcomes of the congenital defects. Next, we summarize available data on most commonly diagnosed CHD – ventricular septal defects, atrial septal defects, and patent ductus arteriosus. We focus then solely on ventricular septal defects and, according to primary aim of the review, on one of the effective and mini-invasive surgical treatment of this category of defects – a hybrid method. We highlight definite advantages of the hybrid approach (applicable for low-weight patients, no need for cardiopulmonary bypass, little surgical scar) as well as some limitations. The comprehensive discussion about the hybrid method includes step-by-step description of its implementation, typical delivery approaches, and most common occluder device types, and is accompanied by the experience of our clinic. We conclude with the need for further research on the effectiveness and safety of the hybrid approach, especially in susceptible patients like neonates.
2. CHD epidemiology
2.1. Prevalence of CHD
The worldwide diagnosis rate for various CHDs at the birth is often reported between 8 and 10 per each 1000 live births, the value is steady enough over the last three decades [7,8,9,10,11]. However, the maximal reported CHD prevalence rate substantially exceeds 10 cases per 1000 births, e.g. over 20 in Central Vietnam [12] and 26.7 in sub-Saharan Africa [13] and some reported even much higher values up to 50 per 1000 newborns [14].
Certainly, there are numerous studies and reports about the rates of CHD prevalence, incidence and mortality. Due to the large amount of studies (and probably due to locally significant factors), the published rates show high variation that makes difficult to draw actual numbers. This includes both temporal variation, most easier to be explained by last advancements in diagnosis, and geographical, most easier explained by regional discrepancies in healthcare system. However, as we show below, even in a single geographical region the reported values may differ in several times. Other factors as well like race, ethnicity, socio-economic status, ecology, etc. may play in the variation. Meantime, all the reported values indicate that CHD is a serious health problem affecting many people worldwide – around 12 millions of people with CHD are living now globally that gives about 600,000 years of disability [5]. Here, we briefly give prevalence and mortality numbers that have been already published for different regions in the world.
The highest average rates are detected in Asian regions at ~9.3 cases per 1000 births [15,16,17]. On the other hand, highly different rates have been reported within the South and Central Asian regions. In China, the reported CHD prevalence rate at birth or in perinatal period displays remarkable inter-regional variability [18]. Thus, the reported values range from less than 3.0 in South China [19] to 3.6 and 3.9 in Liuyang and Jinan (cities in East China) [20,21] to 5.8 (averaged rate for 11 cities in East China) [22] to 7.6 (Northwestern China) [23] to 22.9 per 1000 infants (North China) [24], with overall prevalence at ~9 per 1000 live births in this country [25]. A ~15%-lower value for fetal CHD prevalence (7.4 per 1000 live births nationwide) was obtained by accumulating data from >90 clinical centers in China between 2011 and 2013 giving in total ~2.5 millions of pregnancies [26]. More recent Chinese data accumulated between 2015 and 2019 and based on the analysis of several millions of births showed even lower prevalence rate for CHD, approximately at 4.9 per 1000 newborns [18]. In India, the most populous country in the South Asia and in the world, the prevalence for CHD also greatly varies between country’s regions as well as between available reports. While most commonly accepted prevalence rates vary between 2 and 5 per 1000 live births [27], in North India the all-type CHD rate was reported at 8.07 per 1000 live births, with ventricular septal defects as a most frequent defect [28] and in North Central India the reported values were extremely higher, at the level of 19.14 per 1000 live births [29]. Surprisingly, in the regions of India with high natural level of radiation, the prevalence rate for CHD was found much lower compared to the normal level areas, and the total combined rate at 1.49 per 1000 live births was very low compared to other reported values [30]. In Central Vietnam, the rates remain extremely high over the last decade and range between 15 and 20 per 1000 live births [12,31]. Middle East region also has relatively higher prevalence rates, e.g. in Saudi Arabia the rate for mild plus severe CHD is 14.8 per 1000 live births while 3.2 per 1000 for severe CHD only [32].
Similar to Asian countries and regions, available reports and studies related to African region show varying values for prevalence of CHD. For example, it has been shown at 3.5 per 1000 newborn in Niger [33]. Pan-African data that combined over 1,600,000 pediatric patients from more than 40 clinical studies show population-based and hospital-based prevalence at 5.12 and 12.63 per 1000 live births, respectively [34]. It should be noted that the prevalence rate reported for African countries is typically lower compared to other regions [35,36,37] and there is a lack of systematic reports regarding this estimate. According to a systematic review and meta-analysis published more than a decade ago and spanned a period from 1970 to 2010, the prevalence of CHD in Africa was sustainably lower compared to all other geographical regions [15].
The variability in the reported values for CHD prevalence at birth shows very wide range in the Central and South America, with values of 1.24 per 1000 neonates in the most populous state in Brasil [38], 1.94 in Colombia [39], 7.1 in Equador [40], and 11.7 in French Guiana [41]. In North America, the U.S. nationwide estimates for all-type and all-severity CHD prevalence at birth have been reported at levels between 9 and 11 per 1000 live births, according to various studies [7,42,43,44]. However, one recent study showed, using pooled data taken from single-state (Colorado) pediatric care system between 2012 and 2019, that the actual prevalence rate for CHD in all-age children is much higher, comprising almost 2% of overall pediatric population, which is equivalent to approximately each 20 per 1000 children [45] – much higher rate than the reported values, e.g. for Asian regions.
The reported prevalence rates also vary significantly between European countries. According to registry-based data collected from 14 European countries for live births between 2008 and 2015, the overall prevalence rate for all-severity CHD was 6.02 per 1000 people [46]. For critical CHD, lower values were reported according to nationwide databases including European countries, with the highest prevalence found in Czech Republic, at 3.09 per 1000 neonates [47]. However, the all-type CHD prevalence in France was reported at the level of 10.7 per 1000 newborns [48], i.e. at the value exceeding the average rate in South Asian regions. In Sweden, the rate of CHD incidence in live births increased steadily during the last decades and now it has been reported even at higher level of 20 per 1000 live births (the estimate includes mild and severe CHDs of all types) [49]. In fact, the availability for proper diagnostic tools, the existence of nationwide prenatal screening programs, the severity of CHD (e.g. some studies provide numbers for severe CHD only while others report mild and severe CHD together), and other factors contribute to the great variability between the reported values on CHD-related early mortality.
In early childhood as well as in adolescence (4 to 18 years), the global prevalence of untreated CHD in 2010-2014 amounted to >4.8 per 1000 lives, and this estimate does not include children having genetic disorders associated with heart development impairment [50]. Another cross-sectional study performed in China found higher rate, 6.73 per 1000 children aged between 3 to 19 years and screened for CHD [51]. On the other hand, some recent meta-analyses report much lower global values in infant patients, e.g. ~3 case per 1000 infants [52]. In adults, the CHD prevalence is even much lower [29] most likely due to the following main contributions – the spontaneous closure of defects in survived and the proportion of deceased patients with CHD aged before adulthood.
The remarkable CHD prevalence, however, includes the range of defects that do not have critical influence on the heart contractility at least for some prolonged period, often to the adult age. For example, in 2010 in the US the number of currently living people with cardiac defects was estimated as ~2.4 millions, where adults amounted to around 60% of this cohort [7]. Moreover, more than 85% the neonates with CHD, if treated appropriately (but not interventionally or surgically), survive to adulthood [53].
It is now widely accepted that fetal echocardiography allows for early prenatal diagnosis improving outcomes by facilitating delivery planning at specialized centers and enabling immediate postnatal intervention. The increased availability for early prenatal screening in many countries worldwide is now the main contributor to the dramatic increase in the diagnosed fetal CHD over the last decades. For instance, one study reported the rise from 6.2% in 1991 to 82.8% in 2021 [54]. On average, 50-60% of CHD are detected now on fetal screening [55]. However, while screening programs and neonatal care have enhanced survival rates, implementation remains inconsistent in many low- and middle-income countries [56].
2.2. Mortality and morbidity in CHD
Many congenital cardiac defects are life-threatening at birth or become such during early development, at puberty, or in adulthood. For instance, critical congenital heart defects such as hypoplastic left heart syndrome or transposition of the great arteries can be fatal if not immediately corrected after birth [57]. Other examples include severe coarctation of the aorta, which can cause life-threatening complications like aortic rupture or heart failure if left untreated early in life [58]. According to a nationwide population-based study that encompassed several decades, the risk of myocardial infarction and the 30-day mortality in adult individuals with severe CHD are much higher compared to general population [59]. Moreover, the mortality risk in infants with severe forms of CHD during first year of life is 12 times higher vs. those with mild forms of CHD [14]. Another critical complication – heart failure – is developed during lifetime in each one of every 13 adult survivors with CHD [60]. A large meta-analysis based on 9 separate cohort studies (performed in Denmark, Sweden, UK, US, and China), which collectively included >80,000 CHD patients and >600,000 control individuals, revealed the following risks for CHD cohort: three-fold higher incidence of cardiovascular diseases, ~2.5 times more frequent chance of stroke, and about 6 times higher risk of heart failure [61].
In general, about 20-25% of CHD are considered seriously life-threatening conditions and therefore require urgent surgical treatment [44,62,63]. Additionally, nearly 10% of CHDs are multiple [64]. During adolescence, certain untreated congenital anomalies – such as severe ventricular septal defects – may lead to pulmonary hypertension or heart failure if not addressed timely. In adulthood, some conditions like Eisenmenger syndrome, which results from longstanding unrepaired congenital heart defects, can cause significant morbidity and can be life-threatening [65]. Additionally, acquired conditions like myocardial infarction (heart attack) or advanced heart failure can also be precipitated by congenital defects that were initially asymptomatic. Moreover, the implications of CHD were found in “essentially non-cardiac” diseases like the elevated risk of dementia and CNS infections [66,67] or type 2 diabetes mellitus [68] in the individuals with severe CHD. These pathologies may originate from the impaired/deficient metabolic status in CHD patients, as they correlate with patients’ underweight in early life [69]. Also, it has been revealed that about 23% of CHD-affected newborns have accompanying defects in the CNS [26] thus showing substantial parallelization of the malformations. Moreover, other accompanying malfunctions and abnormalities include gastrointestinal and urogenital organs [26]. These examples underscore the importance of early detection and management, as some defects pose immediate risks while others may threaten life at later stages if left unrecognized or untreated.
CHD-associated mortality and actual factors affecting its rate reveal distinct variation between reports as well as between geographical regions. In some African countries like Ethiopia, the mortality rate in neonates with CHD is reported at extremely high level of 9.9% [70] while other countries have nearly twice lower rates, e.g. Kenya and Tanzania (3.4-3.8%) [71]. The mortality of children aged before 5 years is somewhat higher in these two countries, about 4.5% [71]. Among countries in North Africa and Middle East, the reported mortality rate varies from 1.1 to 15.9 [37]. For African continent as a whole, the mortality rate is much higher compared to developed countries [36,37]. In some Asian countries the mortality rate during first year of life among neonates and infants born with CHD has been reported at very high levels like 15% in Malaysia [72] and 30% in China [20]. In Central Asian region, there are also different CHD-related mortality estimates for children born with CHD, i.e. ranging from 8% of neonatal mortality in Turkey [73] to 7.6% mortality in early age children (from birth to 4 years) in Kazakhstan [64]. In the Middle East countries, the mortality has been reported even at higher rate, e.g. around 17.4% in Saudi Arabia, but this rate was obtained for babies from birth to two years of life [32]. Comparable values are available from South and Central America, with 12% mortality in CHD neonates in Peru [74]. Data from the U.S. vary across available published sources, with mortality rate for CHD babies aged <1 year to be 0.3 per 1000 [75] and 4.1% mortality in neonates [43], during the comparable period of surveillance (from 1999 to 2016/2017). People born earlier, between 1980 and 1997, had elevated risk of mortality during first year of life which is reported at 7.2% [76]. In the UK, the mortality rate before age of 5 years in those with severe CHD was at the rate of 10.4% [77]. A very recent study that analyzed data provided by the European Congenital Heart Surgeons Association Congenital Cardiac Database (ECHSA-CCDB) for the period of 1999-2024 revealed the 10.28% in-hospital mortality rate in neonates with CHD [78]. Therefore, it might be concluded that the mortality rate in newborn and infants with CHD is nearly similar over the world.
According to the analysis of large sample of preterm live births the U.S., included over 1.8 million patients, the mortality rate in premature neonates with CHD was significantly higher vs. neonates without CHD, and accounted for 11.6% deaths [79,80]. Moreover, 1-year survival in those infants was significantly lower compared to norm-term neonates with CHD [81,82]. A large study collected very preterm birth clinical data obtained between 2007 and 2015 from 10 countries (including Australia, Canada, Japan, and several European countries) and similarly revealed that the mortality rate in neonates with CHD is two-fold more frequent compared to those without CHD [83]. On the other hand, some reports indicate that the mortality rate in neonates with diagnosed CHD may not differ between preterm and norm-term live births regardless if the compared groups are moderate CHD or severe CHD [84].
As many studies have reported the proportion of mortality in newborns with CHD to the total number of live births (i.e. irrespective to the presence of CHD or other pathology), direct comparison with reports for CHD-related deaths in CHD patient cohorts becomes tricky. In the countries of South America, 70.6 CHD-related fatal cases occurred during first year of life per 100,000 live births in Peru [85]. The rates are very high compared to the developed countries like the U.S. (0.29% for infants <1 year age and 0.12% for all-age cohort) [75] or the United Kingdom with reported value of 0.35% for children before 5 year in age [77]. Therefore, despite the overall global positive trends in CHD-related mortality in all-age cohort and below 5-year age cohort, the contribution of untreated CHD into overall mortality remains to be a critical challenge [86].
2.3. Causes and critical outcomes of CHD
The etiology of CHD is complex and multifactorial. Although the exact cause remains unknown in many cases, established risk factors include chromosomal abnormalities (e.g., trisomy 21 or Down syndrome), monogenic syndromes, maternal infections (e.g., rubella), pregestational diabetes, teratogenic drugs, alcohol, and other environmental exposures during pregnancy [87,88,89,90,91]. For example, the association between Down syndrome and congenital cardiac defects is generally reported at ~50% [92,93] but much greater association in ~75% has also been documented in patients with at least one cardiac defect [94] and in patients with complete atrioventricular septal defect [95]. Some may report lower association, e.g. only 12.8% of 1371 patients with CHD had Down syndrome according to a Tanzanian study, but it is still high enough to conclude that this association is important [96]. The trisomy 21 is so severe condition that among adult survivors only about 10% of those having severe CHD also have Down syndrome [91]. Other chromosomal aberrations, like trisomy 13 or trisomy 18, are accompanied by even higher co-incidence of CHD, at 60-80% [92,97]. Also, unequal prevalence of CHD in male and female neonates has been reported in several studies [70,91,96,98] while other studies did not reveal substantial sex disproportions [99,100]. It is interesting that greater overall frequency of CHD and the prevalence of moderate CHD are both higher in female neonates while the prevalence of severe CHD is higher in male neonates [25,101] thus explaining why male sex is a risk factor of mortality [64]. Specifically, females experience tetralogy of Fallot and atrial septal defects more frequently than males, but males are more predominant with stenosis/insufficiency of aortic valve as well as transposition of great arteries [102].
About one-third to 40% of CHD cases is related to genetic variants and the number of new such variants constantly increases [103,104]. Moreover, non-inherited de novo genetic variants are responsible for ~8% of CHD [105]. The most important variants include genes responsible for early stages of heart development, i.e. those that control normal cardiogenesis. The inherited predisposition to CHD is a greatly contributing factor because parents with CHD have substantially increased risk to give birth to offspring with CHD, and mothers have nearly twice higher such risk compared to fathers [106]. Because of high proportion of genetically conditioned CHDs, genetic screening and testing in prenatal stage is now considered one of the major contributors to further surviving of the affected people [97], along with constantly improved surgical approaches.
CHDs are typically classified as acyanotic or cyanotic defects, where the latter constitutes about 25-30% of all CHD [107,108]. Acyanotic forms, such as atrial septal defects, ventricular septal defects, and patent ductus arteriosus, often maintain hemodynamic stability for years. In contrast, cyanotic defects – including tetralogy of Fallot and truncus arteriosus – usually cause systemic hypoxemia, ischemic stroke, and affects neutrophil-to-lymphocyte ratio, and therefore require intervention urgently due to the risk of severe complications or death [55,107,109,110].
Despite the major advances in medical and surgical treatment of CHD, physical, psychosocial, and neurodevelopmental outcomes remain a major concern. In a large cohort of patients with CHD, aged between 19 and 38 years, about 40% reported at least one disability type among several types like troubles in hearing, vision, mobility, cognition, self-care, etc. [111]. Children with CHD – particularly those undergoing repeated surgeries or prolonged hospitalizations – are at increased risk for cognitive and motor delays, as well as attention, learning, and behavioral difficulties [112,113]; this is partly related to the same genetic mutations that were the background of CHD development [114]. Moreover, adult females with CHD are at elevated risk for complications of cardiovascular system during pregnancy as compared to their healthy counterparts [115]. Altogether contributes to a high proportion of people who are restrained in their everyday activity or even critically disabled life-long.
3. Most common types of CHD
In this section, we list most common types (with detailed description for ventricular septal defects only) of congenital heart defects, which can be successfully treated surgically or interventionally. We do not describe here the molecular and cellular mechanisms that commence pathophysiology of early heart development, which results in the defective heart structures. Another recent review paper covers these aspects in much detail [116]. However, we briefly mention here the most critical hemodynamic and functional consequences related to a certain type of defects.
3.1. Ventricular septal defect
Ventricular septal defect (VSD) is an opening in the interventricular septum that permits abnormal blood flow between left and right ventricles. This abnormal “shunting” increases pulmonary blood flow and without treatment it generally leads to congestive heart failure.
According to most studies, perimembraneous VSDs constitute the largest part of the VSD, often reported between 60 and 80% [117,118,119]. Muscular VSDs are usually reported in 10-15% cases [120]. A recent study performed in Malaysia also reported greater proportion of perimembraneous (55%) vs. muscular (30%) VSDs, with virtually similar occurrence of small and moderate sizes (42 and 46%, respectively) [121]. On the other hand, a study involved 25,000 newborn in Denmark revealed totally opposite distribution between main types of VSD, with ~93% of muscular and only 7% of perimembraneous [122]. Congenital VSDs constitute a vast majority of postnatally diagnosed VSD, and acquired VSDs in newborn, children, adolescent or adult people were reported as relatively rare events [123]. However, under certain conditions like trauma, ischemic episode, or infectious myocarditis, the development of acquired cardiac defects in childhood and in adulthood can occur [123,124,125,126]. The acquired defects often are VSDs in the form of ventricular septal rupture, and in some circumstances and conditions they can be repaired by the hybrid approach [127,128].
The size of the ventricular septal defect may vary significantly. It is generally accepted that the defects below 4 mm are small, between 4 and 6 mm are moderate, and above 6 mm are large [16,129] while standardized size-based classification is not currently introduced [116,130]. Indeed, the nominal size of VSD as measured by echocardiogram provides little information about its actual functional role until the size of the heart is known. This is why another classification may be used, where the small-moderate-large scale for VSD size is determined according to the diameter of aorta, i.e. by the ratio between VSD size and aortic root dimeter [131]. According to this approach, an alternative to the above classification for small, moderate, and large VSDs can be proposed, e.g. those VSDs with sizes of ≤1/3, >1/3 to ≤2/3, and >2/3 of the diameter of aorta, respectively [132].
Small perimembraneous and muscular defects may close spontaneously either in prenatal period or during the first year of life, often with much higher closure rate for muscular vs. perimembraneous VSD [118,122,133]. In younger patients aged <1-2 years, the rate of spontaneous closure of perimembranous or muscular VSDs may vary in a large range: from 30% [133,134] to 55% [121] to 83.5% [122] within one or two years of observation. In longer observation periods, the spontaneous closure rates may be as high as 97% for 7-year follow-up period [129]. A substantial proportion of prenatally discovered VSD was found to close successfully in uterus [135]. Much higher spontaneous closure occurrence after birth was reported for muscular VSD compared to perimembraneous VSD [122,129,133]; the difference between muscular and perimembraneous VSDs is especially remarkable for sizes ≥4 mm [136]. Of note, the larger chance for isolated muscular VSDs to close spontaneously correlates in some extent with reportedly much lower frequency for observation of chromosomal aberrations in these defects (0.4%) as compared to isolated perimembraneous VSDs (4.8%) [133]. It is also not surprising that the smaller size of VSD appears to be one of the factors contributing to its spontaneous closure [122] as well as the larger VSD is a risk factor for post-operative complications and longer in-hospital stay [117].
In contrast, moderate-size VSDs often necessitate surgical or catheter-based intervention, and large and very large VSDs always require on-time surgery [137]. Moreover, the severity of VSD-related heart malfunction generally depends not only on both nominal size of the VSD but also the age of the patient (i.e. therefore the size of patient’s heart). One study reported the results of successful VSD closure surgeries in infants aged between 4.2 and 6.5 months – among the VSDs, there were some with very large sizes of ~12-14 mm, according to the published data [138]. In another study, two infant patients aged 3.5 and 3.9 months had even larger muscular VSD sized in 14 and 16 mm, respectively [139]. Note that these VSD sizes are comparable with reported VSD sizes in adult patients [124,140].
3.2. Atrial septal defect
Atrial septal defect (ASD) is a communication between the left and right atria that may lead to right heart dilation, atrial arrhythmias, increased stroke risk, and also increased liver stiffness [141]. The congenital pathology often needs urgent treatment and presents a great challenge in cardiac surgery [142].
Moderate to large defects typically necessitate closure via catheter-based device or surgery [143,144]. The success rate for closure of ASD at the ostium secundum via percutaneous approach is high and reported typically between 94 and 99% [145,146,147]. It is interesting that among functional characteristics for evaluation of success in ASD occluder device closure in follow-up, liver stiffness was recently proposed as a high correlate to the ASD occlusion [148].
The size of ASD may vary substantially with age and size of the heart as well as between available reports. One study reported absolute values for ASD size between 15 and 40 mm in patients aged between 4 and 58 years [149]. Other studies that included only adult patients reported much different ranges, e.g. from 2 to 47 mm in [150] and from 17 to 26 mm in [151]. In general, the most often reported ASD size ranges in 10 to 30 mm in all-age cohort of patients [146].
Due to the thinner wall, one of the important challenges of ASD device closure is the wall erosion. It has been reported as a rare but serious complication of percutaneous transcatheter device deployment [152,153,154]. Novel ASD closure devices were developed providing good success rate of closure without reported lesions at the deployment site [155]; on the other hand, relatively high incidence rate for new onset arrhythmia has also been reported between <4 to 12% of cases [146,156,157].
3.3. Patent ductus arteriosus
Patent ductus arteriosus (PDA) is a persistent fetal connection between the aorta and pulmonary artery, causing left-sided volume overload. Treatment varies by age and defect size, from medical therapy in neonates to transcatheter closure in older infants [158,159,160]. Despite nearly half of the PDA-diagnosed neonates are not surgically treated [158,159], the size of the defect plays ultimate role in the choosing the surgical treatment. This defect may range in size between 2 to >5 mm in low-weight preterm neonates, according to available reports [161,162]. The success rate for transcatheter device closure of PDA was reported at high level of 95-100% [161,162,163]. In addition, the post-operative mortality and even major/significant complications are very rarely observed in such surgical treatments, including transcatheter closure. Also, it has been reported that in nearly a half of patients with PDA, the defect is spontaneously closing later postnatally, but this is dependent on the gestational age and the chance for spontaneous closure decreased with the age [159].
Despite high success rate for closure and minimized post-treatment mortality, the PDA, if untreated, is strongly associated with increased mortality, in particular in preterm neonates and in neonates with low weight [164]. Also, in neonates with hemodynamically significant PDA, the mortality is several times higher vs. those with hemodynamically non-significant PDA [165]. On the other hand, in surgically treated PDA patients, the risk of mortality is also higher compared to those treated conservatively, e.g. by medication [158]. Therefore, this type of CHD is a very critical and life-threatening pathology, and the proper strategy should be done in a patient-specific mode. Still, the in-hospital mortality rate can be decreased if early echocardiography screening for PDA is performed in neonates as soon as possible after the birth [166].
3.4. Prevalence of the three most common types of CHD
There is clearly regional and inter-institutional variation in the reported proportions for various types of CHD. For example, more than two-fold prevalence of VSD over ASD is reported by European network of population-based registries for the epidemiological surveillance of congenital anomalies in 2025 [167]. In Southern Africa, the prevalence for VSD is two-fold higher vs. ASD, and the two types are predominant among other CHDs [168]. In the East Africa, the reported prevalence of VSD is almost three-fold higher vs. that of ASD [35]. Another study reported 4-fold higher prevalence of VSD over ASD (~40 vs. ~11%, respectively) as well as ~18.5% for the prevalence of PDA among all types of CHD [169]. The meta-analysis based on data accumulated in Africa globally from 1992 through 2022 and presented in >40 clinical population-based and hospital-based studies concluded with 2-to-3 times more frequent detection of VSD vs. ASD [34]. Similarly, more than two-fold prevalence in VSD (25%) vs. ASD (10%) as well as vs. aortic valve disorders and coarctation of the aorta (16% together) was reported in Australia based on multicenter data encompassing over 68,000 CHD patients [170]. Less dissimilar but still two-fold prevalence of VSD over ASD was reported in other clinical studies, e.g. from China and India [29,171]. In a multicenter analysis of data obtained by six Ethiopian cardiovascular clinical centers with 6275 CHD patients in total, the ratio of VSD to ASD in these cohort was ~1.64 [172]. However, another group that analyzed nearly 235,000 live births in Colombia reported much smaller (but still presenting) prevalence of VSD over ADS, i.e. 13.7% vs. 10.1% among all cardiac defects [173].
Alike, the variability is found among reports from the same region. For example, a multicenter study that encompassed several African countries revealed non-uniform distribution in the VSD-to-ASD proportions, from much greater prevalence of VSD in Ghana and Central Cameroon through nearly similar proportions in Nigeria to much greater prevalence of ASD in Eastern Uganda, Northern Egypt and Southern region of South Africa [174]. On the other hand, the analysis of CHD types in 2559 pediatric patients in a Tanzanian heart disease screening center revealed comparable diagnosis rate for VSD and PDA (19.3% and 19.1%, respectively) and just a bit lower rate for ASD (15.1%) [100]. Essentially similar proportions were also reported in other studies performed in African region: a Ugandan study reported 27.2%, 22%, and 9.4% for VSD, PDA, and ASD, respectively (n = 3526 pediatric patients) [98] while a Tanzanian study reported 26.1% for VSD and 23.2% for PDA, but only 7.1% for ASD (n = 1371) [96]. In contrast, much smaller cohort of 199 CHD patients studied in an Ethiopian institution revealed totally opposite proportions: 41.2% for ASD, 26.6% for VSD, and only 9.5% for PDA [175]. In China, the reported proportion between diagnosed VSD to ASD varies greatly, from approximately 2:1 in [20,25,26] to the essentially opposite situation where ASD were detected three times more frequently compared to VSD [21,51]. These regional discrepancies may reflect both genuine epidemiological differences and unequal access to diagnostic tools or varying practices in clinical reporting. In resource-limited settings, underdiagnosis of mild forms of CHD (such as small ASDs) could artificially elevate the relative frequency of more symptomatic types like VSD.
Of note, the rate of CHD detection (of any type) increases steadily over decades virtually in all world regions but it is unlikely it reflects increasing susceptibility of the fetus to the pathological remodeling. Rather, the advancement of various diagnostic tools as well as running of local and national programs of early screening for prenatal development defects contributed to rapidly elevating number of CHD diagnoses [18,90]. Indeed, numerous studies report the dramatic increase in the diagnostic rate of major CHD in prenatal period and in neonates [18,54,62].
Whether congenital or acquired, timely diagnosis and treatment of structural heart defects are essential to prevent complications such as pulmonary hypertension, heart failure, arrhythmias, or irreversible myocardial damage. As surgical and interventional outcomes improve, early detection becomes increasingly vital.
4. Conventional, transcatheter, and hybrid approaches for correction of ventricular septal defects
4.1. General Considerations on Prognostic Implications and Risk Stratification
Although many VSDs have a favorable prognosis, the clinical course is strongly influenced by defect size, subtype, and hemodynamic burden (Table 1). Large perimembranous or outlet defects are associated with progressive cardiac dysfunction, increased risk of endocarditis, and early development of pulmonary hypertension if untreated [130,176]. Conversely, small muscular defects are typically benign and often resolve spontaneously. Despite the predominance of perimembranous VSDs among diagnosed cases, muscular VSDs may account for a disproportionately higher part of interventional procedures due to their multiplicity or complexity. Furthermore, many perimembranous defects are hemodynamically insignificant and may not require intervention.
Management decisions are guided by comprehensive risk stratification, incorporating defect size, location, shunt magnitude, and clinical symptoms [177,178]. Defects resulting in significant left-to-right shunting, chamber dilation, or pulmonary overcirculation require closure. However, small asymptomatic VSDs with negligible shunting may be safely monitored without surgical correction. Surgical or transcatheter closure may be contraindicated or technically infeasible in certain complex anatomies, such as multiple muscular VSDs or single ventricle [179]. Moreover, in younger patients, the surgical treatment of any type is accompanied by increased rate of intraoperative cardiac arrest [180]. It underscores the importance of individualized, anatomy-specific and hemodynamics-related treatment planning. It is also important to mention that according to a large retrospective study of fetal congenital defects involving >2,450,000 pregnancies, congenital VSDs are the type of defects which displays highest co-incidence with congenital defects in other organs and systems, including CNS, gastrointestinal, urogenital, and skeletal systems as the most often affected [26].
4.2. Surgical approaches to treat VSD
In this subsection, we discuss the following surgical modalities that remain in use for VSD management [181,182,183]: a) conventional surgical repair utilizing cardiopulmonary bypass, b) endovascular (percutaneous) closure techniques, and c) hybrid VSD repair without the use of a heart-lung machine. All these modalities differ with their basics and implementation but we are not tasked to discuss thoroughly the features of each modality. However, we mention briefly the historical evolution of the modalities.
4.2.1. Conventional surgical repair of VSD utilizing cardiopulmonary bypass
In 1948, Gordon Murray was the first who performed VSD closure on a beating heart. To close the defect, he used a needle carrying a flap of fascia lata to occlude the defect with fascial tissue. This series included four patients, the youngest being 1 year and 5 months old. Three of the operated patients survived, while one died due to respiratory failure caused by atelectasis [184]. In 1952, Charles Bailey employed a similar method for VSD closure, using a pedicled autologous pericardial patch [185]. Later in 1954, Kay and Zimmerman were the first to perform VSD closure under hypothermic conditions [186]. Also in 1954, at the University of Minnesota, Lillehei with colleagues performed the first VSD closure using cross-circulation. The technique involved cannulation of the internal jugular vein for venous drainage and the common carotid artery for the return of oxygen-rich arterial blood. The "donor" of oxygenated blood, via femoral artery and great saphenous vein cannulas, was the patient’s father. Using this method, eight patients were operated on. Five were under one year of age, and three were between four and five years old. Two patients died but the mortality rate is likely reflecting the complexity of the procedure and not its technical inadequacy [187]. Essentially the same approach was implemented by the same surgeons’ team later between 1954 and 1955 on 45 patients, with great proportion of out-hospital survivors: despite eight patients died in-hospital, only two died during the next 30 years of follow-up [188].
In 1955, at the Mayo Clinic, large VSDs were closed under normothermic conditions using a mechanical pump-oxygenator with 20% mortality, which was considered a relatively low for that time [189]. In 1957, Lillehei and colleagues reported the feasibility of VSD closure via atrial access [190]. Subsequently, Okamoto et al. introduced a method involving hypothermic circulatory arrest with rewarming using a pump-oxygenator for neonates with VSD [191]. Successful one-stage repair of VSDs in infants was proposed in the late 1950s by Kirklin et al. at the University of Michigan [192,193]. However, morbidity and mortality associated with cardiopulmonary bypass in young children remained relatively high. One-stage repair gained wider acceptance following the introduction of deep hypothermic circulatory arrest by Barratt-Boyes at Green Lane Hospital in Auckland, New Zealand, in 1969 [194,195]. However, normothermic CPB is still widely used; moreover, a recent meta-analysis provided good evidence that normothermic CPB in pediatric patients can be considered as safe (or even safer) as hypothermic CPB [196].
Currently, there are numerous surgical open-heart techniques available for the correction of VSD. Open-heart surgery using cardiopulmonary bypass (CPB) was previously considered the gold standard for VSD repair [197,198,199]. This method is effective indeed; however, it carries potential risks associated with the use of CPB as well as cosmetic-related issues. The sudden cardiac arrest in patients subjected to another widely used open-heart surgery, coronary artery bypass grafting (CABG), is also an important issue. For example, a recent study reported that in a large cohort of 41,450 those patients, 231 suffered the cardiac arrest immediately post-surgery in the ICU or in the ward conditions, and 41.3% of them died within 30-day interval after the surgery [200].
Technical advancements in last decades significantly improved patient compatibility with CPB. Nevertheless, the risk of systemic inflammatory response – manifested through edema, encephalopathy, thrombosis, or air embolism – is still persisting [201]. The post-operative infections are another critical complication after CPB in pediatric patients, with some reports showing that nearly half of the patients may develop secondary infection [202]. Next, research indicates that CPB procedure may impact neurodevelopment, especially motor skills and especially in infants – most likely due to the systemic stress induced by deeper and/or longer anesthesia [203,204]. The incidence of neurological outcomes in pediatric patients after CPB may be as high as 25% [205]. Also, the presence of genetic anomaly is a risk factor for the negative neurodevelopmental outcomes, as it has been shown in infants aged <9 months at the time of CPB [203]. In addition, postoperative pain due to full sternotomy and subsequent scar formation remains a significant concern [206,207]. It therefore has been concluded that the use of CPB in children and in particular in infant patients is a challenging procedure affecting many physiological systems [205,208].
Vertical right axillary and right anterior mini-thoracotomy (ministernotomy) are approaches mainly used as a standard approach for closure of ASD while they can also be successfully and safely utilized for VSD and atrioventricular septal defects [209,210,211,212]. The implementation of these approaches, however, also requires using of cardiopulmonary bypass, so their use in treating VSD brings increased risks for post-surgery complications. In addition, as discussed in the following section, these approaches almost always require larger surgical incision compared to hybrid approach thus making issues related to the cosmetic outcomes of the surgery.
These consequences, which affect patients' quality of life, have prompted researchers to pursue innovations aimed at improvement. As a result, efforts were initiated to develop interventional (percutaneous) methods for closing ventricular septal defects.
4.2.2. Percutaneous (transcatheter) approach for VSD closure
Transcatheter approach for closure of VSD is utilized since 1988 when Lock and colleagues reported the first percutaneous closure of a ventricular septal defect (VSD) in six patients, three of whom had post-infarction VSDs and three with congenital VSDs. At the time, this approach was considered an alternative treatment for selected patients [213]. However, the endovascular method had its own limitations, including various types of arrhythmias, device embolization, and vascular complications. Nevertheless, with advancements in VSD closure devices, the first percutaneous closure of a VSD using the Amplatzer occluder was performed in animal models in 1997, followed by successful application in patients with muscular VSDs since 1998 [214,215].
The percutaneous transcatheter closure was shown to be effective in several clinical studies. For example, it was feasible in closure of moderate and large perimembraneous VSD, with success rate of 91.4% in 35 pediatric patients aged approximately 2 years and weighed below 10 kg [216]. Similar was found in children with weight deficiency where the success rate was reported at 85.7% for the transcatheter closure of large or moderate perimembraneous VSD; the procedure did not result in mortality or any major complications during median 20-month follow-up period [217]. The transcatheter approach using modified Amplatzer Duct Occluder II for closure of small perimembraneous VSD was 100% effective and free from major complications in another study, which involved 49 patients aged between 1.9 and 25 years [218]. A single-center retrospective study that accumulated long-term data for 75 pediatric patients aged 46-96 months and treated by percutaneous device closure with different types of devices (Amplatzer, Occlutech, Hyperion, etc.) showed pooled 95.7% success rate for defect closure within 1 year after the treatment [219]. Another single-center study retrospectively analyzed long-term outcomes for 149 patients, both children and adults, diagnosed with muscular or perimembraneous VSD and treated by transcatheter device closure; again, the devices were different in brands and types [140]. The reported closure rate was 86.2% for median 6-year follow-up period, with only one patient died in the period due to the treatment procedure. Transcatheter closure was also shown effective in outlet-type VSD, with 100% success closure and no incidence of complete atrioventricular block (cAVB) [220], and in post-myocardial infarction ventricular septal rupture [221]. In general, according to systemic reviews on the effectiveness of transcatheter VSD closure, perimembraneous VSD can be successfully closed percutaneously in selected patients with limited reports about major negative outcomes like regurgitation or heart block for at least one month post-treatment [222,223,224]. Technical and procedural advancements allow for successful implementation of the transcatheter approach in low-weight infants, mostly with perimembraneous VSD [225]. According to a large meta-analysis collecting data from three randomized controlled studies and 24 observational studies (6421 patients in total), comparison between open-heart surgery, transcatheter closure, and mini-invasive repair of perimembraneous VSD indicates the superiority of the transcatheter closure regarding the total duration of procedure, major complications, ICU stay, and in-hospital stay [223].
It is important to note that the entire procedure is performed under continuous fluoroscopic guidance, and the long-term effects of radiation exposure on various organs of the body remain insufficiently studied [226,227]. There are still numerous criteria that significantly limit the selection of suitable patients for this method (while mostly those who have ASD) [118,143,179]. Additionally, complications such as injury to and regurgitation of the aortic and tricuspid valves have been reported [228,229,230], along with a high incidence of atrioventricular block or arrhythmias [224,231,232,233,234]. Further advancements in the approach like a single transradial arterial access may partially overcome these challenges [235,236]. Also, using softer material for the device decreases the risk of conduction block issues, e.g. cAVB [178]. However, the feasibility of routine use of percutaneous VSD closure in small patients (newborns and infants) is still debated – currently it is advised to apply the method only for selected pediatric patients [227,237,238]. Therefore, despite the numerous reports on utilization of the method for surgical correction of VSD, some limitations and challenges of the treatment remain to be present, e.g. in the correction of perimembraneous VSD [239].
4.2.3. Hybrid approach for VSD correction
An alternative approach proposed was the hybrid procedure, known as transventricular or perivenrticular closure of ventricular septal defect. The term “hybrid procedure,” now commonly used in cardiology and cardiac surgery, refers to the combination of surgical and interventional techniques aimed at optimizing the treatment of congenital and acquired heart defects while minimizing their limitations. It is important to understand the rationale behind the term “hybrid”: this technique combines some features characteristic for open-heart surgery (e.g. making an incision in thoracic region while without the use of CPB) and catheter-based surgery to implant an occluder device.
The initial attempts at hybrid VSD closure did involve the direct use of CPB and employed the Rashkind double-umbrella occluder. However, the outcomes of these early procedures were suboptimal, with failure rates ranging from 20 to 40% and mortality rates between 14 and 25% [240,241,242,243]. The first successful implantation of an occluder on a beating heart without CPB was performed in 1998 by Dr. Amin and his colleagues [244]. In animal-based experimental studies, muscular VSDs were artificially created in pigs and dogs to advance the technique of VSD closure on a beating heart without CPB [244,245,246,247].
As technology evolved, self-centering implants became popular, allowing for more flexible devices to be used. Furthermore, the use of transesophageal or epicardial echocardiography significantly improved the accuracy of diagnosis and treatment. The first promising studies on hybrid VSD closure began emerging since the first half of 2000s [248,249]. Moreover, researchers sought alternative incision techniques for VSD closure. In 2003, Bacha and colleagues reported a case utilizing a subxiphoid incision, marking the first instance of a muscular VSD being closed without CPB via this approach [250]. Later, perimembranous VSD closure without CPB was successfully applied in over 400 patients, aged between 5 months and 15 years, with overall success rate of 96.3% and ~3% of minor adverse effects like tricuspid valve regurgitation and incomplete right bundle branch block [251]. Other studies reported success closure rates between 90 and 100% in infants and children with low weight [252,253,254,255]. Of note, the success closure may be below 100% immediately after the surgery but can eventually achieve this rate, e.g. 6 month later [253].
Based on available published data and our own gathered experience, the average mortality rate associated with the hybrid approach appears to be lower than that observed with conventional surgical correction using CPB or with percutaneous transcatheter approach. Often available reports indicate no mortality within short- and medium-term periods. For example, in a small cohort of 30 pediatric patients (all with non-muscular VSDs, aged <3 years or weighed <15 kg), no peri- or post-mortality was observed during a 6-month period [252]. The hybrid approach was applied to another small cohort of infants aged <1 year with large apical muscular VSD of mean size 8.5 mm – no fatal cases during 36-month follow-up were reported as well [256]. In fact, many other case reports, case-series reports, and large retrospective analyzes also provide data indicating no mortality in hybrid method for VSD closure, in patients of different ages – from neonates to adults [254,257,258,259]. In patients with post-myocardial infarction VSDs, the early mortality was substantially higher in open-heart surgery group with CPB; however, the 1-year mortality was similar in these groups [260]. Our own data accumulated on 500 pediatric patients subjected either to hybrid or conventional open-heart surgery – 250 in each group – indicated much lower in-hospital mortality for hybrid approach (0.43% for all-age mixed data) vs. traditional open-heart surgery with CPB (1.5%) [261]. However, there is still the need to accumulate long-term results for survival rates and, in particular, for any delayed unfavorable effects including neurological and developmental disorders.
Indeed, it is well known that the left ventricular (LV) function in most cases is compromised immediately after VSD repair as well as in short-term period [262,263]. Moreover, in middle- or long-term periods, the LV function may restore incompletely yet. For instance, a clinical study involving infants younger or slightly older than 6 months (in total 104 patients) showed that the post-operative LV dysfunction was observed in 38% of the patients and that the recovery of LV contractility requires ~9 months [264]. Similar estimates were obtained in another study, where pediatric patients with pre-operative LV dilation and aged below one year needed approximately 12 months to recover their LV function to the pre-surgery baseline [265]. It has also been found that the elevated pre-operative internal dimension of the LV is a risk factor for either the post-operative LV dysfunction occurrence or the prolonged recovery in LV contractility [263]. The negative post-surgery outcomes may relate not only to the LV ejection fraction (LVEF, used as a standardized functional measure of pumping function of the ventricle) but also its mechanical deformability measures even in the case of normal LVEF values [266]. On the other hand, these reports mostly concern the patients treated by conventional surgery with CPB, with in general much longer anesthesia and operation time. Yet, comparing the conventional open-heart surgery and transcatheter device closure within a single study revealed eventual recovery of LV function in both groups despite more pronounced decrease in LV function was detected in those subjected to open-heart surgery [267]. Of note, substantial decrease in LV function is of especial issue in small children despite if are treated for small defects [268].
Additionally, right ventricular dysfunction after surgical repair was reported with a variable frequency [269,270], whereas no right ventricular dysfunction was observed following the hybrid procedure [271,272]. Although long-term studies on the hybrid method are still lacking and some show single cases of serious adverse effects like cAVB [178,273], short-term data indicate that serious postoperative functional complications are rare. Furthermore, when treatment is conducted in early childhood, the patients appears to have normal LV function, i.e. comparable to that of healthy individuals [274].
Perventricular VSD device closure is mostly used in patients with muscular VSD [252,253]. Also, it has been validated as a safe approach in complex muscular VSD in infants [Karimi et al. 2012]. Moreover, perventricular approach has been reported as a successful approach for closure of perimembranous or doubly committed VSDs [199,254,276,277]. In infants and patients with low weight, a subxiphoid perventricular approach via small incision was found a successful treatment in ~90% of patients (n=17), including the closure of muscular and perimembraneous VSD [278]. In another study with 21 individuals including seven neonates, no post-operative mortality, morbidity, need for reoperation, and functional consequences were reported after perventricular hybrid approach [279]. A larger cohort of 59 patients, mostly with perimembraneous VSD, was treated by periventricular approach with the overall success closure of 97% and only one post-operative major complication [254]. Others report similar very good outcomes for perimembraneous, muscular, and subaortic VSD in infants, with no observed late rhythm disturbances or other complications [199]. Small infants with large defects and patients with insufficient venous access are the selected patients for perventricular hybrid approach, including muscular VSDs [276,280]. In addition, hybrid perventricular transcatheter approach may be successfully performed in patients with apical VSD developed after myocardial infarction, with much better in-hospital survival compared to traditional surgery [260].
Besides in general better values for mortality and post-surgery complications, the hybrid approach also has advantages in its shorter in-operation duration and overall cost-effectiveness. Many reports show that the procedural duration is nearly twice shorter in hybrid vs. traditional surgery [208,257,261,277,281]. Mini-invasive surgical treatments in pediatric patients, in particular with congenital heart defects, continue developing, and further assessments in safety, outcomes, and long-term efficacy (evaluated by care-related costs, everyday activity, etc.) will be accumulated [282].
5. Procedural and technical aspects of hybrid approach in treating ventricular septal defects
The hybrid approach to ventricular septal defect closure integrates surgical exposure with interventional devices on a beating heart, eliminating the need for cardiopulmonary bypass. The procedure is conducted under general anesthesia with continuous transesophageal echocardiographic (TEE) guidance. The primary procedural steps are outlined below and illustrated in Figures 1–7.
5.1. Surgical Steps of the Hybrid Ventricular Septal Defect Closure Technique
Although many VSDs have a favorable prognosis, the clinical course is strongly influenced by defect size, subtype, and hemodynamic burden (Table 1). Large perimembranous or outlet defects are associated with progressive cardiac dysfunction, increased risk of endocarditis, and early development of pulmonary hypertension if untreated [130,176]. Conversely, small muscular defects are typically benign and often resolve spontaneously. Despite the predominance of perimembranous VSDs among diagnosed cases, muscular VSDs may account for a disproportionately higher part of interventional procedures due to their multiplicity or complexity. Furthermore, many perimembranous defects are hemodynamically insignificant and may not require intervention.
Step 1: Preoperative Assessment
Preoperative TEE is essential for accurate assessment of VSD size, location, and morphology, with special attention to any associated valvular abnormalities (Figure 1). Based on this evaluation, an appropriate occluder device is selected – typically symmetric, asymmetric, eccentric, or muscular types – tailored to the defect anatomy.
Step 2: Surgical Access
A 2–4 cm inferior median sternotomy is performed, followed by a pericardiotomy to expose the anterior free wall of the right ventricle (RV). For subarterial VSDs, an anterior parasternal incision may be used as an alternative approach (Figure 2).
Step 3: Right Ventricular Puncture
Under real-time TEE monitoring, the optimal puncture site on the RV free wall is identified (Figure 3A,B). A purse-string suture is placed around the selected site, and a trocar or 6F needle is utilized to puncture the RV wall.
Step 4: Guidewire and Sheath Insertion
A 0.035-inch guidewire is introduced into the RV and passed across the VSD into the left ventricle (LV). The trocar is then removed, and a delivery sheath is advanced over the guidewire into the LV cavity (Figure 4).
Step 5: Device Deployment
With the heart beating and under continuous TEE guidance, the occluder device is delivered through the loading sheath (Figure 5). The left ventricular disc is deployed first against the interventricular septum, followed by deployment of the right ventricular disc, achieving secure closure of the VSD.
Step 6: Post-deployment Assessment
After successful device release, intraoperative TEE is used to evaluate for residual shunts, device position, and potential complications such as aortic or tricuspid regurgitation (Figure 6). Special attention is given to detecting conduction abnormalities such as atrioventricular block. If significant residual shunting (>2 mm), new-onset valve dysfunction, or conduction disturbances are observed, conversion to conventional on-pump surgery may be required. The delivery system is detached only after favorable transesophageal echocardiography (TEE) findings – no residual shunt across the ventricular septum, preserved aortic and tricuspid valve function, and absence of rhythm or conduction disturbances. A safety suture remains in place and is exteriorized through the purse-string suture. After securing the purse-string, TEE is repeated to reassess the heart. The safety suture is then shortened, the knot is tied, and the sternotomy is closed (Figure 7A,B). Hemostasis is verified, and protamine sulfate is administered if needed. In primary procedures, stainless steel wires are not used for sternal closure, whereas in reoperations, they are applied. If indicated, epicardial pacing wires are placed. Standard pericardial drainage is maintained for 24 hours (Figure 7С,D).
This algorithm provides the optimal level of automation and control of unnecessary movements, which allows minimizing trauma and reducing the total duration of the surgical procedure. This sequence of actions is based on our eight years of experience and vision of the operation, which, in turn, has demonstrated high efficiency.
5.2. Device delivery approaches
An occluding device can be delivered either directly to the ventricle via a small incision on the heart’s chamber or via a large vessel like femoral vein using catheter-based delivery system.
The system consists of: i) the VSD occluder, designed to connect to the delivery cable via a screw mechanism, ii) the guidewire, used to advance the devices into the desired position (Figure 8B), iii) the dilator, which facilitates penetration through tissue and the vessel wall, iv) the hemostatic valve, which minimizes bleeding, and includes a side port with a flexible extension tube and a stopcock used for flushing the system (Figure 8A), v) the loading sheath (loader), which is used to introduce the occluder, attached to the delivery cable, into the introducer (Figure 8D), and vi) the delivery sheath with plastic torque control (Figure 8C). The delivery sheath is used to advance the occluder through the introducer and hold it in place while the introducer is retracted to deploy the occluder or retrieve it if its size, position, or deployment is deemed unsatisfactory. The plastic torque device, screwed onto the proximal end of the delivery cable, facilitates directional control and serves as a handle for detaching the delivery system from the occluder.
5.3. The types of device used to close VSD
The occluder devices used for VSD closure may have different shapes and sizes (Figure 9). The most common types of occluder used in VSD closure are concentric and eccentric. Generally, the former type is used more frequent compared to the latter. For example, the concentric type was used in >70% of devices while eccentric type was set up in just 25.6% cases of <1 year old infants with muscular and perimembraneous VSD [283]. Special types of occluder can also be used but its prevalence has been reported as low as 5% of total number of occluders [283]. Typically, the size of VSD occluder is 2-3 mm larger than the diameter of the VSD (the waist of the occluder corresponds to the VSD diameter) [284]. Transcatheter implants have unique material properties, including shape memory. Therefore, the devices for the closure of VSD, ASD, and PDA are pre-shaped according to the individual anatomical features. Importantly, these devices can be compacted, delivered through catheters, and deployed intracardially, where they resume their intended shape.
According to many available reports, the most used VSD occluder in perventricular approach is Amplatzer Muscular VSD Occlude device [276]. This device is a self-expandable double-sided disc made of nitrinol wire mesh and polyester, which provides tight deployment at the site of defect as well as provides a space for surrounding tissue to grow inside the device. Older versions of Amplatzer closure devices for perimembraneous VSD are not used now in some countries like the U.S. due to the high risk of complete heart block; however, they are widely used in other countries [285]. Currently widely used essential analogues of Amplatzer occluders include Konar MFO [119,286,287,288] and MemoPart™ [199,281,289]. Moreover, the off-label use of different variants of Amplatzer or Amplatzer-like devices specifically in the closure of VSD was shown to be feasible in selected patients. The examples include closure of perimembraneous VSD [218,290,291,292] or subarterial VSD [293] by Amplatzer Duct occluders (ADO II and ADO I, generally used for PDA closure) and closure of perimembraneous VSD by Amplatzer Vascular Plug II [294,295]. Of importance, the off-label use of the occluder devices results in fair good success rate, according to these reports. In some reports, it has been shown that the use of duct occluders instead of original VSD occluder can bring more safety as it allows for avoiding cAVB [290]. In addition, compared to the conceptually different and widely used type of occluding device – Nit-Occlud Lê VSD Coil – the Amplatzer and Amplatzer-like duct occluders show somewhat better occlusion success rate [296,297]. For example, a comparative study showed that six month after the occlusion procedure, the complete occlusion was remarkably higher, although non-significantly, in the group with duct occluders compared to the coil group – 91.3% vs. 84.1%, respectively [296].
A novel transcatheter device occluder, LifeTech™ Multifunctional Occluder (also known as Konar-MFO), was introduced several years ago as a promising closure device for muscular VSD [258]. It has recently been evaluated for its safety in terms of avoiding intra- or post-operative atrioventricular blockage [288]. The meta-analysis thoroughly compared 19 studies which used this device and it was found that the overall success rate was >94%, with cAVB reported in only 2.3% of followed-up patients. In a recent clinical study, percutaneous closure of muscular or perimembraneous VSDs by Konar-MFO was implemented in 151 patients, with 98.7% of total success rate in the closure; however, in 3.3% of the patients there were observed rhythm disturbances [119]. Slightly lower success rate, 93% in 57 patients subjected to percutaneous VSD closure by Konar-MFO, was reported in another clinical study but no complications related to rhythm disturbance were observed within a 6-month follow-up [287]. Only one case of complete heart block was reported in a clinical study on 98 patients (mostly pediatric) with perimembraneous and muscular VSD subjected to Konar MFO device deployment, whereas the overall success of the procedure was 98% [285]. A smaller set of five patients with perimembraneous VSD and aged <12 months was surgically repaired by Konar-MFO, and no electric block of the heart was observed during 15-month follow up [2]. Importantly, the feasibility of Konar-MFO has recently been demonstrated in low-weight infants (below 10 kg), with procedural advancement where no arterial access and transesophageal echocardiographic guidance were necessary and only venous route was used for catheterization [225]. However, the lack of long-term follow-up observations still exists, and there are some reports about adverse events after using Konar-MFO as late as 20 months post-surgery; on the other hand, this case was about a transcatheter device closure of perimembraneous VSD [298].
The effectiveness of Konar-MFO was directly compared to the commonly used Amplatzer Duct Occluder II device: long-term outcomes for 33 vs. 44 patients were analyzed, respectively [286]. There was no reported permanently persisting heart conduction block or death in both groups, and the freedom from post-operative complications was high and comparable between these devices. On the other hand, some studies indicate that the Konar MFO device is more frequently used in larger VSD. According to available comparative studies for these two devices, the difference in average or median defect sizes may be as high as 2.5 mm [286,299]. There are several ongoing studies which continue accumulating data about the safety of Konar-MFO and long-term outcomes for post-treatment complications [178].
Another novel device – Cocoon Membranous VSD Occluder – has recently been introduced into clinical practice and it is currently utilized for correction of perimembraneous VSDs. This is a symmetric fabric-reinforced double-disc device made of nitrinol designed for compact closure of a defect [300]. Preliminary reports were concerning its feasibility in pediatric and/or adult patients with VSD [301] including post-operative defects [302]. In recent studies, the effectiveness and the prevalence in use of Cocoon duct occluder has been evaluated against other types of occluders. For example, it was revealed that Cocoon duct occlude is the most prevalently used device in India for closure of perimembraneous VSDs [292]. However, early reports show that the implanting by this type of device may be accompanied by adverse effects including leakage and incomplete conduction block [301]. It is therefore needed to gather additional data on the safety and effectiveness of Coccon devices in further studies.
In our center, we use the occluder CeraTM Occluder, LifeTech Scientific Co., China. It is a self-expandable, double-disc device crafted from nitinol wire mesh. The two discs are interconnected by a short cylindrical waist tailored to match the size of the VSD. Both the discs and the waist feature polytetrafluoroethylene (PTFE) membranes securely sewn to the device using nylon threads (Figure 10). It has been shown in early studies that CeraTM septal occluders are safe and give good alternative to the Amplatzer devices in treating ASD via transcatheter approach [303]. More recent study with >200 patients revealed that both CeraTM and CeraFlexTM occluders provide excellent ASD closure success with reliable safety and minimal occurrence of major/serious adverse complications [304]. The CeraTM occluders were found effective for PDA closure as well [305]. Nevertheless, similar to Cocoon occluder devices, there are ongoing studies needed for further verification of long-term safety of this type of device.
6. Advantages and limitations of hybrid approach for VSD closure
Here we describe most important advantages and limitations when using hybrid approach vs. traditional open heart surgery. Despite the prominently successful implementation of hybrid closure in most of reported studies, one should note that it is generally applicable with most success on selected patients.
Probably the most advantageous thing is that hybrid approach is performing on beating heart (also known as off-pump coronary artery bypass grafting), i.e. without the need for cardiopulmonary bypass [306]. Another important advantage of hybrid closure is its feasibility in very small patients, often weeks or even days old [118]. Indeed, the hybrid approach has demonstrated good applicability and feasibility in neonates and infants aged <1 year, according to several clinical studies [278,279]. Perventricular hybrid approach is especially effective in small infants with large defects or in those patients with insufficient access through vasculature [276,307]. Third, the overall duration of the hybrid treatment surgery is substantially shorter compared to conventional surgery. Thus, some studies reported two-to-three times shorter mean procedural duration as well as anesthesia duration for hybrid vs. conventional approaches [208,257,281]. Inevitably, this also results in shorter in-hospital stay [277].
In general, the success of hybrid approach to close the ventricular septal defect(s) has been confirmed high, giving the overall post-operative success rate at around 95% or more with 5% of complications or less [308]. For example, in a study embraced over 440 pediatric patients aged in average below 1 year, the success closure achieved >96% with no reported deaths or major complications [283]. Similarly, 96.6% of success closure was reported in total of 320 pediatric patients aged between 1 and 3 years and subjected to the perventricular device closure [281]. Even large muscular VSDs can be effectively closed by hybrid approach via percutaneous approach [309].
Within a 5-year period, the complete closure of the defect(s) occurred in 98.6% of the patients, according to a multi-center study [310]. In few cases where the initial percutaneous closure gave incomplete effect, the second hybrid approach can be effective [302]. However, some certain types of heart defects like Swiss cheese VSD may require alternative approaches if the percutaneous device closure has failed [311].
Better psychological outcome in patients subjected to mini-invasive hybrid approach, as compared to those treated by conventional surgical methods, is also a definitive advantage [312]. The minimization of cosmetic defects due to the diminished size of the surgical scar, as well as the unnecessity of cardiopulmonary bypass in the hybrid approach are the most important outcomes [306].
Among the limitations, fails in closure and rhythm disturbances are the main issues of hybrid approach. It has been shown that the failure rate is somewhat higher for muscular VSD than for perimembranous VSD, with major complications of 5.3% vs. 1.2%, respectively [127]. This study also reported 1.6% rate for occurrence of cAVB after hybrid approach. Another study, in which complications were counted in patients subjected to the hybrid approach (interventional VSD closure) between 1993 and 2015 in a single center, demonstrated even lower complication rate, with only 0.7% for cAVB [140]. Transcatheter closure of perimembraneous VSD may result in arrhythmias approximately in 25% cases, according to the study on 395 pediatric patients with median age of 4 years [313]. However, similar cohort (320 patients) in another study did not demonstrate any rhythm disturbances or impairments of conduction system [281]. The brand of the closure device is unlikely affects the outcomes. For example, nearly similar occurrence of cAVB in ~1-year old patients was reported in the case of Amplatzer Duct Occluder II (ADO II) and Konar MFO, where each subgroup contained one such case (4.5% and 3.3% of total number of patients, respectively) [299]. In another study on 77 pediatric patients with median age of 4.3 years, there were no occurrence of permanent conduction block in the heart or other surgery-related complications if the patients were treated either by ADO II or by Konar MFO [286]. In general, it might be concluded that the incidence of delayed cAVB is even lower in hybrid setting compared to transcatheter percutaneous closure, despite the inevitable risk of such complication [273].
It should also be noted that the limiting factor for wider use of hybrid approach is the lack of standardized protocols resulting in sometimes individualized decisions often based on the actual experience present in a clinic and patient-specific symptoms and anatomical findings [273,314]. Other issues include further need for analysis of long-term outcomes of the hybrid approaches, in particular in regard to the risk of cAVB [273] and especially in patients with neuropsychological comorbidities [315]. However, many large scale comparative studies did confirm that the hybrid approach is safer and more efficient compared to both traditional open-heart surgery and transcatheter percutaneous closure [277,316].
The annual (or, better, decade-based) rate of published papers concerning the hybrid approach remains high from 2000s, and the available data show that this approach is effective in the treatment of various VSD, mostly perimembranous and muscular [117,309]. However, regional discrepancies in the using this approach do exist. For example, in the U.S. there are no FDA-approved occluders for transmyocardial (perventricular) closure of VSD (while Amplatzer Septal Occluder is FDA-approved device for ASD closure). Accordingly, there are few reports from the U.S. about perventricular closure with hybrid approach, mostly reporting extending corrective measures in adult patients previously subjected to the VSD correction [317]. Similarly, limited reports are available from some other countries and regions including European countries [318,319] and Japan [260]; if applied there, it is mostly used in adult patients. In contrast, the VSD occluder device for perventricular closure in hybrid setting under video-assisting guidance (via TTE) is widely used in China, especially for pediatric patients with CHD and especially in recent years [117,208,257,273,316,320,321]. Several reports and case series were published which show that the hybrid approach is used for newborn, infant, and early childhood patients in Russia [281,289,322], Middle East [199], and Central East [65,261].
7. Future prospects in using hybrid approach for VSD closure
The hybrid approach to ventricular septal defect (VSD) closure continues to evolve as an effective strategy that bridges the gap between open-heart surgery and transcatheter interventions [178,276,323]. While current data demonstrate its feasibility and short-term safety in selected cases, future advancements and broader clinical integration depend on several key developments:
1) Refinement of patient selection criteria through evidence-based protocols will be crucial. Ongoing accumulation of clinical experience and real-world data will enable more precise stratification of patients based on anatomical characteristics, age, comorbidities, and risk factors, ensuring optimal outcomes and minimizing complications such as arrhythmias and device embolization. Also, the increasing interest to genotyping diagnosed CHD (in particular, VSD) may lead to better outcome of hybrid treatment in terms of better closure and diminished reopening, especially if preoperative genetic mapping would be available [324].
2) Technological advancements in occluder device design are expected to enhance procedural success and reduce device-related complications. Innovations aimed at improving anchoring mechanisms, biocompatibility, and retrievability may further increase the safety profile of the hybrid method, especially in infants and young children.
3) Integration of imaging technologies, including real-time 3D transesophageal echocardiography and intraoperative navigation systems, may improve accuracy in device placement, reduce intraoperative time, and further minimize myocardial trauma.
4) Developing standardized hybrid protocols and surgeon training programs will be vital for widespread adoption. Given the multidisciplinary nature of the procedure requiring both surgical and interventional expertise, centers of excellence with dedicated hybrid teams will play a pivotal role in training and outcome benchmarking.
5) Long-term follow-up studies and multicenter clinical trials are essential to assess durability, functional outcomes, and the incidence of late complications such as cAVB [178,273]. These data will provide the scientific foundation necessary for formal incorporation of the hybrid approach into VSD management guidelines.
The progression and evolution of surgical treatment for CHD over the time led to significant decline in overall mortality as well as to the improvement of quality of life of the survived patients [5,88,325]. However, the reported post-operative mortality rates for surgical treatment of pooled types of CHD remain significantly higher in the low- and middle-income countries compared to the high-income countries with well-developed healthcare programs [5,10,13,33,326,327]. (Note that this applies only for those countries/regions where the appropriate level of instrumental diagnostics and medical expertize are available, as the lack of diagnostic tools may result in the inadequately low prevalence rates as well as CHD-related mortality rates, for example, in some reports from South America and Africa [10,38,39].) This great challenge stimulates using more advanced but also less invasive surgical methods in the countries with insufficiently low reported mortality rates after CHD correction, as well as further global and national efforts in the development of pediatric healthcare system to reduce the burden of CHD [11]. Among other advancements, the hybrid technique holds considerable promise as a less invasive yet highly effective modality for VSD closure. With continued innovation and rigorous clinical validation, it may eventually become a standard of care for selected patients.
Author Contributions
Conceptualization, Sh.M., O.L., and Ak.A.; methodology, Sh.M., O.L., and Ak.A.; validation, Sh.M., B.N., A.K., Sa.M., B.T., R.D., R.M., As.A., E.K., Y.A., T.R., Ak.A.; formal analysis, Sh.M., B.N., A.K., Sa.M., B.T., R.D., R.M., As.A., E.K., Y.A., T.R., Ak.A.; investigation, O.L., Ak.A.; resources, Sh.M., O.L., Ak.A.; data curation, Sh.M., B.N., A.K.; writing—original draft preparation, O.L. and Ak.A.; writing—review and editing, Sh.M., O.L., B.N., A.K., Sa.M., B.T., R.D., R.M., As.A., E.K., Y.A., T.R., Ak.A.; visualization, Sh.M., B.N., R.D., As.A., E.K., Ak.A.; supervision, Sh.M. and A.K.; project administration, Sh.M.; funding acquisition, Sh.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research is funded by the Science Committee of the Ministry of Science and Higher Education of the Republic of Kazakhstan (Grant No. AP23488091).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created in this study.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ADO | Amplatzer Duct Occluder |
| ASD | Atrial Septal Defect |
| CABG | Coronary Artery Bypass Grafting |
| cAVB | complete Atrio-Ventricular Block |
| CHD | Congenital Heart Defect |
| CPB | CardioPulmonary Bypass |
| LV | Left Ventricle |
| LVEF | Left Ventricular Ejection Fraction |
| PDA | Patent Ductus Arteriosus |
| RV | Right Ventricle |
| TEE | Trans-Esophageal Echocardiographic (guidance) |
| VSD | Ventricular Septal Defect |
References
- Forman, J.; Beech, R.; Slugantz, L.; Donnellan, A. A Review of Tetralogy of Fallot and Postoperative Management. Crit Care Nurs Clin North Am 2019, 31, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Singhi, A.K.; Mukherji, A.; De, A. Perimembranous ventricular septal defect closure in infants with KONAR-MF occluder. Prog Pediatr Cardiol 2022, 65, 101489. [Google Scholar] [CrossRef]
- Nurkeyev, B.; Marassulov, S.; Aldabergenov, Y.; Adilbekova, A.; Murzabayeva, S.; Kuandykova, E.; Akhmoldaeva, A. A Clinical Case of Successful Surgical Correction of Tetralogy of Fallot by Using the Right Atrial Appendage as a Neopulmonary Valve. J Clin Med Kaz 2024, 21, 71–73. [Google Scholar] [CrossRef]
- Dalén, M.; Odermarsky, M.; Liuba, P.; Johansson Ramgren, J.; Synnergren, M.; Sunnegårdh, J. Long-Term Survival After Single-Ventricle Palliation: A Swedish Nationwide Cohort Study. J Am Heart Assoc 2024, 13, e031722. [Google Scholar] [CrossRef]
- GBD2017 Congenital Heart Disease Collaborators Global regional national burden of congenital heart disease 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017 Lancet Child Adolesc Health, 2.0.2.0.; 4; 185-200,,,, h.t.t.p.s.:././.d.o.i.o.r.g./.1.0.1.0.1.6./.S.2.3.5.2.-4.6.4.2.(.1.9.).3.0.4.0.2.-X. Erratum in: Lancet Child Adolesc Health 2020, 4, e6. [CrossRef]
- Swanson, J.; Ailes, E.C.; Cragan, J.D.; Grosse, S.D.; Tanner, J.P.; Kirby, R.S.; Waitzman, N.J.; Reefhuis, J.; Salemi, J.L. Inpatient Hospitalization Costs Associated with Birth Defects Among Persons Aged <65 Years - United States, 2019. MMWR Morb Mortal Wkly Rep 2023, 72, 739–745. [Google Scholar] [CrossRef]
- Gilboa, S.M.; Devine, O.J.; Kucik, J.E.; Oster, M.E.; Riehle-Colarusso, T.; Nembhard, W.N.; Xu, P.; Correa, A.; Jenkins, K.; Marelli, A.J. Congenital Heart Defects in the United States: Estimating the Magnitude of the Affected Population in 2010. Circulation 2016, 134, 101–9. [Google Scholar] [CrossRef]
- Bravo-Valenzuela, N.J.; Peixoto, A.B.; Araujo Júnior, E. Prenatal diagnosis of congenital heart disease: A review of current knowledge. Indian Heart J 2018, 70, 150–164. [Google Scholar] [CrossRef] [PubMed]
- Poulsen, C.B.; Damkjær, M. Trends in prescription of cardiovascular drugs to children in relation to prevalence of CHD from 1999 to 2016. Cardiol Young 2018, 28, 1136–1141. [Google Scholar] [CrossRef] [PubMed]
- Saxena, A. Status of Pediatric Cardiac Care in Developing Countries. Children (Basel) 2019, 6, 34. [Google Scholar] [CrossRef]
- Vervoort, D.; Jin, H.; Edwin, F.; Kumar, R.K.; Malik, M.; Tapaua, N.; Verstappen, A.; Hasan, B.S. Global Access to Comprehensive Care for Paediatric and Congenital Heart Disease. CJC Pediatr Congenit Heart Dis 2023, 2(6Part B), 453–463. [Google Scholar] [CrossRef]
- Giang, H.T.N.; Bechtold-Dalla Pozza, S.; Ulrich, S.; Linh, L.K.; Tran, H.T. Prevalence and Pattern of Congenital Anomalies in a Tertiary Hospital in Central Vietnam. J Trop Pediatr 2020, 66, 187–193. [Google Scholar] [CrossRef]
- Rossano, J.W. Congenital heart disease: a global public health concern. Lancet Child Adolesc Health 2020, 4, 168–169. [Google Scholar] [CrossRef]
- Tankeu, A.T.; Bigna, J.J.; Nansseu, J.R.; Aminde, L.N.; Danwang, C.; Temgoua, M.N.; Noubiap, J.J. Prevalence and patterns of congenital heart diseases in Africa: a systematic review and meta-analysis protocol. BMJ Open 2017, 7, e015633. [Google Scholar] [CrossRef] [PubMed]
- van der Linde, D.; Konings, E.E.; Slager, M.A.; Witsenburg, M.; Helbing, W.A.; Takkenberg, J.J.; Roos-Hesselink, J.W. Birth prevalence of congenital heart disease worldwide: a systematic review and meta-analysis. J Am Coll Cardiol 2011, 58, 2241–7. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.Y.; Chao, A.S.; Kao, C.C.; Lin, C.H.; Hsieh, C.C. The Outcome of Prenatally Diagnosed Isolated Fetal Ventricular Septal Defect. J Med Ultrasound 2017, 25, 71–75. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, S.; Zühlke, L.; Black, G.C.; Choy, M.K.; Li, N.; Keavney, B.D. Global birth prevalence of congenital heart defects 1970-2017: updated systematic review and meta-analysis of 260 studies. Int J Epidemiol 2019, 48, 455–463. [Google Scholar] [CrossRef]
- Zhao, L.; Chen, L.; Yang, T.; Wang, T.; Zhang, S.; Chen, L.; Ye, Z.; Luo, L.; Qin, J. Birth prevalence of congenital heart disease in China, 1980-2019: a systematic review and meta-analysis of 617 studies. Eur J Epidemiol 2020, 35, 631–642. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Wei, J.; Huang, X.; Chen, B.; Liang, L.; Feng, B.; Song, P.; He, J.; Que, T.; Lan, J.; Qin, J.; He, S.; Wei, Q. Epidemiology of Congenital Heart Defects in Perinatal Infants in Guangxi, China. Int J Gen Med 2024, 17, 5381–5396. [Google Scholar] [CrossRef]
- Xie, D.; Wang, H.; Liu, Z.; Fang, J.; Yang, T.; Zhou, S.; Wang, A.; Qin, J.; Xiong, L. Perinatal outcomes and congenital heart defect prognosis in 53313 non-selected perinatal infants. PLoS One 2017, 12, e0177229. [Google Scholar] [CrossRef]
- Zhang, L.; Liu, B.; Li, H.; Wang, C.; Yang, S.; Li, Z. Epidemiology of Congenital Heart Disease in Jinan, China From 2005 to 2020: A Time Trend Analysis. Front Cardiovasc Med 2022, 9, 815137. [Google Scholar] [CrossRef]
- Pan, F.; Li, J.; Lou, H.; Li, J.; Jin, Y.; Wu, T.; Pan, L.; An, J.; Xu, J.; Cheng, W.; Tao, L.; Lei, Y.; Huang, C.; Yin, F.; Chen, J.; Zhu, J.; Shu, Q.; Xu, W. Geographical and Socioeconomic Factors Influence the Birth Prevalence of Congenital Heart Disease: A Population-based Cross-sectional Study in Eastern China. Curr Probl Cardiol 2022, 47, 101341. [Google Scholar] [CrossRef]
- Pei, L.; Kang, Y.; Zhao, Y.; Yan, H. Prevalence and risk factors of congenital heart defects among live births: a population-based cross-sectional survey in Shaanxi province, Northwestern China. BMC Pediatr 2017, 17, 18. [Google Scholar] [CrossRef]
- Sun, P.F.; Ding, G.C.; Zhang, M.Y.; He, S.N.; Gao, Y.; Wang, J.H. Prevalence of Congenital Heart Disease among Infants from 2012 to 2014 in Langfang, China. Chin Med J (Engl) 2017, 130, 1069–1073. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Q.M.; Liu, F.; Wu, L.; Ma, X.J.; Niu, C.; Huang, G.Y. Prevalence of Congenital Heart Disease at Live Birth in China. J Pediatr 2019, 204, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Zhao, S.; Dong, X.; Liu, J.; Guo, Y.; Ju, W.; Chen, P.; Gao, Y.; Feng, Q.; Zhu, X.; Huang, H.; Lu, X.; Yang, X.; Yang, F.; Cheng, C.; Luo, X.; Cheng, L. Zhong, N; Chinese Consortium for Prenatal Ultrasound Screening of Congenital Heart Defects. Incidence, distribution, disease spectrum, and genetic deficits of congenital heart defects in China: implementation of prenatal ultrasound screening identified 18,171 affected fetuses from 2,452,249 pregnancies. Cell Biosci 2023, 13, 229. [Google Scholar] [CrossRef]
- Kumar, A.; Kumar, P. Echocardiographic Study of Ventricular Septal Defect in 1- to 12-Year-Old Children Visiting a Tertiary Care Center in Patna, India. Cureus 2023, 15, e46363. [Google Scholar] [CrossRef]
- Saxena, A.; Mehta, A.; Sharma, M.; Salhan, S.; Kalaivani, M.; Ramakrishnan, S.; Juneja, R. Birth prevalence of congenital heart disease: A cross-sectional observational study from North India. Ann Pediatr Cardiol 2016, 9, 205–9. [Google Scholar] [CrossRef]
- Dixit, R.; Rai, S.K.; Yadav, A.K.; Lakhotia, S.; Agrawal, D.; Kumar, A.; Mohapatra, B. Epidemiology of Congenital Heart Disease in India. Congenit Heart Dis 2015, 10, 437–46, Erratum in: Congenit Heart Dis 2019, 14, 1214. 10.1111/chd.12775. [Google Scholar] [CrossRef]
- Sudheer, K.R.; Mohammad Koya, P.K.; Prakash, A.J.; Prakash, A.M.; Manoj Kumar, R.; Shyni, S.; Jagadeesan, C.K.; Jaikrishan, G.; Das, B. Evaluation of risk due to chronic low dose ionizing radiation exposure on the birth prevalence of congenital heart diseases (CHD) among the newborns from high-level natural radiation areas of Kerala coast, India. Genes Environ 2022, 44, 1. [Google Scholar] [CrossRef]
- Giang, H.T.N.; Hai, T.T.; Nguyen, H.; Vuong, T.K.; Morton, L.W.; Culbertson, C.B. Elevated congenital heart disease birth prevalence rates found in Central Vietnam and dioxin TCDD residuals from the use of 2, 4, 5-T herbicides (Agent Orange) in the Da Nang region. PLOS Glob Public Health 2022, 2, e0001050. [Google Scholar] [CrossRef]
- Majeed-Saidan, M.A.; Atiyah, M.; Ammari, A.N.; AlHashem, A.M.; Rakaf, M.S.; Shoukri, M.M.; Garne, E.; Kurdi, A.M. Patterns, prevalence, risk factors, and survival of newborns with congenital heart defects in a Saudi population: a three-year, cohort case-control study. J Congenit Heart Dis 2019, 3, 2. [Google Scholar] [CrossRef]
- Zimmerman, M.; Sable, C. Congenital heart disease in low-and-middle-income countries: Focus on sub-Saharan Africa. Am J Med Genet C Semin Med Genet 2020, 184, 36–46. [Google Scholar] [CrossRef]
- Danso, K.A.; Appah, G.; Akuaku, R.S.; Karikari, Y.S.; Ansong, A.K.; Edwin, F.; Yao, N.A. Prevalence of Congenital Heart Disease in Children and Adolescents Under 18 in Africa: A Systematic Review and Meta-Analysis. World J Pediatr Congenit Heart Surg 2025, 16, 357–367. [Google Scholar] [CrossRef]
- Zikarg, Y.T.; Yirdaw, C.T.; Aragie, T.G. Prevalence of congenital septal defects among congenital heart defect patients in East Africa: A systematic review and meta-analysis. PLoS One 2021, 16, e0250006. [Google Scholar] [CrossRef]
- Rossouw, B. Congenital heart disease in Africa threatens Sustainable Development Goals. South Afr J Crit Care 2021, 37, 10. [Google Scholar] [CrossRef]
- Soleimani, H.; Bahiraie, P.; Tavakoli, K.; Hosseini Mohammadi, N.S.; Hajari, P.; Taheri, H.; Hosseini, K.; Ebrahimi, P. Burden of Congenital Heart Anomalies in North Africa and the Middle East, 1990 to 2021: A Systematic Analysis for the Global Burden of Disease Study 2021. J Am Heart Assoc 2025, 14, e037291. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, P.S.; Magalhães, L.R.; Pezzini, T.R.; de Sousa Santos, E.F.; Calderon, M.G. Congenital heart diseases trends in São Paulo State, Brazil: a national live birth data bank analysis. World J Pediatr 2022, 18, 472–481. [Google Scholar] [CrossRef]
- Portilla, R.E.; Harizanov, V.; Sarmiento, K.; Holguín, J.; Gracia, G.; Hurtado-Villa, P.; Zarante, I. Risk factors characterisation for CHD: a case-control study in Bogota and Cali, Colombia, 2002-2020. Cardiol Young 2024, 34, 178–182. [Google Scholar] [CrossRef] [PubMed]
- González-Andrade, F. High Altitude as a Cause of Congenital Heart Defects: A Medical Hypothesis Rediscovered in Ecuador. High Alt Med Biol 2020, 21, 126–134. [Google Scholar] [CrossRef]
- Lucron, H.; Brard, M.; d'Orazio, J.; Long, L.; Lambert, V.; Zedong-Assountsa, S.; Le Harivel de Gonneville, A.; Ahounkeng, P.; Tuttle, S.; Stamatelatou, M.; Grierson, R.; Inamo, J.; Cuttone, F.; Elenga, N.; Bonnet, D.; Banydeen, R. Infant congenital heart disease prevalence and mortality in French Guiana: a population-based study. Lancet Reg Health Am 2023, 29, 100649. [Google Scholar] [CrossRef]
- Egbe, A.; Uppu, S.; Lee, S.; Stroustrup, A.; Ho, D.; Srivastava, S. Temporal variation of birth prevalence of congenital heart disease in the United States. Congenit Heart Dis 2015, 10, 43–50. [Google Scholar] [CrossRef]
- Wilkes, J.K.; Whitehead, W.E.; Wang, Y.; Morris, S.A. Congenital Heart Disease and Myelomeningocele in the Newborn: Prevalence and Mortality. Pediatr Cardiol 2021, 42, 1026–1032. [Google Scholar] [CrossRef]
- Stallings, E.B.; Isenburg, J.L.; Aggarwal, D.; Lupo, P.J.; Oster, M.E.; Shephard, H.; Liberman, R.F.; Kirby, R.S.; Nestoridi, E.; Hansen, B.; Shan, X.; Navarro Sanchez, M.L.; Boyce, A.; Heinke, D. ; National Birth Defects Prevention Network Prevalence of critical congenital heart defects selected co-occurring congenital anomalies 2014-2018:,,,, A. U.S. population-based study. Birth Defects Res 2022, 114, 45–56. [Google Scholar] [CrossRef] [PubMed]
- Parker, D.M.; Stabler, M.E.; MacKenzie, T.A.; Zimmerman, M.S.; Shi, X.; Everett, A.D.; Bucholz, E.M.; Brown, J.R. Population-Based Estimates of the Prevalence of Children With Congenital Heart Disease and Associated Comorbidities in the United States. Circ Cardiovasc Qual Outcomes 2024, 17, e010657. [Google Scholar] [CrossRef] [PubMed]
- Mamasoula, C.; Addor, M.C.; Carbonell, C.C.; Dias, C.M.; Echevarría-González-de-Garibay, L.J.; Gatt, M.; Khoshnood, B.; Klungsoyr, K.; Randall, K.; Stoianova, S.; Haeusler, M.; Nelen, V.; Neville, A.J.; Perthus, I.; Pierini, A.; Bertaut-Nativel, B.; Rissmann, A.; Rouget, F.; Schaub, B.; Tucker, D.; Wellesley, D.; Zymak-Zakutnia, N.; Barisic, I.; de Walle, H.E.K.; Lanzoni, M.; Mullaney, C.; Pennington, L.; Rankin, J. Prevalence of congenital heart defects in Europe, 2008-2015: A registry-based study. Birth Defects Res 2022, 114, 1404–1416. [Google Scholar] [CrossRef]
- Bakker, M.K.; Bergman, J.E.H.; Krikov, S.; Amar, E.; Cocchi, G.; Cragan, J.; de Walle, H.E.K.; Gatt, M.; Groisman, B.; Liu, S.; Nembhard, W.N.; Pierini, A.; Rissmann, A.; Chidambarathanu, S. Sipek A,,,, J.r.; Szabova, E.; Tagliabue, G.; Tucker, D.; Mastroiacovo, P.; Botto, L.D. Prenatal diagnosis and prevalence of critical congenital heart defects: an international retrospective cohort study. BMJ Open 2019, 9, e028139. [Google Scholar] [CrossRef] [PubMed]
- Bourdon, G.; Lenne, X.; Godart, F.; Storme, L.; Theis, D.; Subtil, D.; Bruandet, A.; Rakza, T. Epidemiology of congenital heart defects in France from 2013 to 2022 using the PMSI-MCO (French Medical Information System Program in Medicine, Surgery, and Obstetrics) database. PLoS One 2024, 19, e0298234. [Google Scholar] [CrossRef]
- Giang, K.W.; Mandalenakis, Z.; Fedchenko, M.; Eriksson, P.; Rosengren, A.; Norman, M.; Hanséus, K.; Dellborg, M. Congenital heart disease: changes in recorded birth prevalence and cardiac interventions over the past half-century in Sweden. Eur J Prev Cardiol 2023, 30, 169–176. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, S.; Zühlke, L.; Babu-Narayan, S.V.; Black, G.C.; Choy, M.K.; Li, N.; Keavney, B.D. Global prevalence of congenital heart disease in school-age children: a meta-analysis and systematic review. BMC Cardiovasc Disord 2020, 20, 488. [Google Scholar] [CrossRef]
- He, S.; Zhao, F.; Liu, X.; Liu, F.; Xue, Y.; Liao, H.; Zhan, X.; Lin, W.; Zheng, M.; Jiang, J.; Li, H.; Ma, X.; Wu, S.; Deng, H. Prevalence of congenital heart disease among school children in Qinghai Province. BMC Pediatr 2022, 22, 331. [Google Scholar] [CrossRef]
- Salari, N.; Faryadras, F.; Shohaimi, S.; Jalili, F.; Hasheminezhad, R.; Babajani, F.; Mohammadi, M. Global prevalence of congenital heart diseases in infants: A systematic review and meta-analysis. J Neonatal Nurs 2024, 30, 570–575. [Google Scholar] [CrossRef]
- Gurvitz, M.; Dunn, J.E.; Bhatt, A.; Book, W.M.; Glidewell, J.; Hogue, C.; Lin, A.E.; Lui, G.; McGarry, C.; Raskind-Hood, C.; Van Zutphen, A.; Zaidi, A.; Jenkins, K.; Riehle-Colarusso, T. Characteristics of Adults With Congenital Heart Defects in the United States. J Am Coll Cardiol 2020, 76, 175–182. [Google Scholar] [CrossRef] [PubMed]
- Tomek, V. Jicínská,,,, H.; Pavlícek, J.; Kovanda, J.; Jehlicka, P.; Klásková,,,, E.; Mrázek, J.; Cutka, D.; Smetanová,,,, D.; Brešták, M.; Vlašín, P.; Pavlíková,,,, M.; Chaloupecký, V.; Janoušek, J.; Marek, J. Pregnancy Termination and Postnatal Major Congenital Heart Defect Prevalence After Introduction of Prenatal Cardiac Screening. JAMA Netw Open 2023, 6, e2334069. [Google Scholar] [CrossRef]
- Singh, Y.; Lakshminrusimha, S. Perinatal Cardiovascular Physiology and Recognition of Critical Congenital Heart Defects. Clin Perinatol 2021, 48, 573–594. [Google Scholar] [CrossRef] [PubMed]
- Rakha, S. Initiating a Fetal Cardiac Program from Scratch in Low- and Middle-Income Countries: Structure, Challenges, and Hopes for Solutions. Pediatr Cardiol 2025, 46, 257–266. [Google Scholar] [CrossRef]
- Feinstein, J.A.; Benson, D.W.; Dubin, A.M.; Cohen, M.S.; Maxey, D.M.; Mahle, W.T.; Pahl, E.; Villafañe, J.; Bhatt, A.B.; Peng, L.F.; Johnson, B.A.; Marsden, A.L.; Daniels, C.J.; Rudd, N.A.; Caldarone, C.A.; Mussatto, K.A.; Morales, D.L.; Ivy, D.D.; Gaynor, J.W.; Tweddell, J.S.; Deal, B.J.; Furck, A.K.; Rosenthal, G.L.; Ohye, R.G.; Ghanayem, N.S.; Cheatham, J.P.; Tworetzky, W.; Martin, G.R. Hypoplastic left heart syndrome: current considerations and expectations. J Am Coll Cardiol 2012, 59(1 Suppl), S1–42, Erratum in: J Am Coll Cardiol 2012, 59(5), 544. [Google Scholar] [CrossRef] [PubMed]
- Raza, S.; Aggarwal, S.; Jenkins, P.; Kharabish, A.; Anwer, S.; Cullington, D.; Jones, J.; Dua, J.; Papaioannou, V.; Ashrafi, R.; Moharem-Elgamal, S. Coarctation of the Aorta: Diagnosis and Management. Diagnostics (Basel) 2023, 13, 2189. [Google Scholar] [CrossRef]
- Olsen, M.; Marino, B.; Kaltman, J.; Laursen, H.; Jakobsen, L.; Mahle, W.; Pearson, G.; Madsen, N. Myocardial Infarction in Adults With Congenital Heart Disease. Am J Cardiol 2017, 120, 2272–2277. [Google Scholar] [CrossRef]
- Bergh, N.; Skoglund, K.; Fedchenko, M.; Bollano, E.; Eriksson, P.; Dellborg, M.; Wai Giang, K.; Mandalenakis, Z. Risk of Heart Failure in Congenital Heart Disease: A Nationwide Register-Based Cohort Study. Circulation 2023, 147, 982–984. [Google Scholar] [CrossRef]
- Wang, T.; Chen, L.; Yang, T.; Huang, P.; Wang, L.; Zhao, L.; Zhang, S.; Ye, Z.; Chen, L.; Zheng, Z.; Qin, J. Congenital Heart Disease and Risk of Cardiovascular Disease: A Meta-Analysis of Cohort Studies. J Am Heart Assoc 2019, 8, e012030. [Google Scholar] [CrossRef]
- Lytzen, R.; Vejlstrup, N.; Bjerre, J.; Petersen, O.B.; Leenskjold, S.; Dodd, J.K.; Jørgensen, F.S.; Søndergaard, L. Live-Born Major Congenital Heart Disease in Denmark: Incidence, Detection Rate, and Termination of Pregnancy Rate From 1996 to 2013. JAMA Cardiol 2018, 3, 829–837. [Google Scholar] [CrossRef]
- Ha, K.; Park, C.; Lee, J.; Shin, J.; Choi, E.; Choi, M.; Kim, J.; Shin, H.; Choi, B.; Kim, S.J. A Comparison for Infantile Mortality of Crucial Congenital Heart Defects in Korea over a Five-Year Period. J Clin Med 2024, 13, 6480. [Google Scholar] [CrossRef]
- Syssoyev, D.; Seitkamzin, A.; Lim, N.; Mussina, K.; Poddighe, D.; Gaipov, A.; Galiyeva, D. Epidemiology of Congenital Heart Disease in Kazakhstan: Data from the Unified National Electronic Healthcare System 2014-2021. J Clin Med Kaz 2024, 21, 49–55. [Google Scholar] [CrossRef]
- Adilbekova, A.; Nurkeev, B.; Marassulov, S.; Kozhakhmetov, S. Mid-Term Outcome of the Hybrid Method of Ventricular Septal Defect Closure in Children. J Clin Med Kaz 2024, 21, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Bagge, C.N.; Henderson, V.W.; Laursen, H.B.; Adelborg, K.; Olsen, M.; Madsen, N.L. Risk of Dementia in Adults With Congenital Heart Disease: Population-Based Cohort Study. Circulation 2018, 137, 1912–1920. [Google Scholar] [CrossRef] [PubMed]
- Bagge, C.N.; Smit, J.; Madsen, N.L.; Olsen, M. Congenital Heart Disease and Risk of Central Nervous System Infections: A Nationwide Cohort Study. Pediatr Cardiol 2020, 41, 869–876. [Google Scholar] [CrossRef]
- Madsen, N.L.; Marino, B.S.; Woo, J.G.; Thomsen, R.W.; Videbœk, J.; Laursen, H.B.; Olsen, M. Congenital Heart Disease With and Without Cyanotic Potential and the Long-term Risk of Diabetes Mellitus: A Population-Based Follow-up Study. J Am Heart Assoc 2016, 5, e003076. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, S.; Olsen, M.; Woo, J.G.; Madsen, N. Congenital heart disease and the prevalence of underweight and obesity from age 1 to 15 years: data on a nationwide sample of children. BMJ Paediatr Open 2017, 1, e000127. [Google Scholar] [CrossRef]
- Ayfokru, A.; Shewasinad, S.; Ahmed, F.; Tefera, M.; Nigussie, G.; Getaneh, E.; Mengstie, L.A.; Teklehaimanot, W.Z.; Seyoum, W.A.; Gebeyehu, M.T.; Alemnew, M.; Girma, B. Incidence and predictors of mortality among neonates with congenital heart disease in Ethiopia: a retrospective cohort study. BMC Pediatr 2024, 24, 559. [Google Scholar] [CrossRef]
- Jivanji, S.G.M.; Lubega, S.; Reel, B.; Qureshi, S.A. Congenital Heart Disease in East Africa. Front Pediatr 2019, 7, 250. [Google Scholar] [CrossRef]
- Mat Bah, M.N.; Kasim, A.S.; Sapian, M.H.; Alias, E.Y. Survival outcomes for congenital heart disease from Southern Malaysia: results from a congenital heart disease registry. Arch Dis Child 2024, 109, 363–369. [Google Scholar] [CrossRef]
- Çaylan, N.; Yalçin, S.S.; Tezel, B.; Üner, O.; Aydin, Ş.; Kara, F. Investigation of infant deaths associated with critical congenital heart diseases; 2018-2021, Türkiye. BMC Public Health 2024, 24, 441. [Google Scholar] [CrossRef]
- Lopes, S.A.V.D.A.; Guimarães, I.C.B.; Costa, S.F.O.; Acosta, A.X.; Sandes, K.A.; Mendes, C.M.C. Mortality for Critical Congenital Heart Diseases and Associated Risk Factors in Newborns. A Cohort Study. Arq Bras Cardiol 2018, 111, 666–673. [Google Scholar] [CrossRef]
- Lopez, K.N.; Morris, S.A.; Sexson Tejtel, S.K.; Espaillat, A.; Salemi, J.L. US Mortality Attributable to Congenital Heart Disease Across the Lifespan From 1999 Through 2017 Exposes Persistent Racial/Ethnic Disparities. Circulation 2020, 142, 1132–1147. [Google Scholar] [CrossRef]
- Downing, K.F.; Nembhard, W.N.; Rose, C.E.; Andrews, J.G.; Goudie, A.; Klewer, S.E.; Oster, M.E.; Farr, S.L. Survival From Birth Until Young Adulthood Among Individuals With Congenital Heart Defects: CH STRONG. Circulation 2023, 148, 575–588. [Google Scholar] [CrossRef]
- Gimeno, L.; Brown, K.; Harron, K.; Peppa, M.; Gilbert, R.; Blackburn, R. Trends in survival of children with severe congenital heart defects by gestational age at birth: A population-based study using administrative hospital data for England. Paediatr Perinat Epidemiol 2023, 37, 390–400. [Google Scholar] [CrossRef]
- Protopapas, E.; Padalino, M.; Tobota, Z.; Ebels, T.; Speggiorin, S.; Horer, J.; Kansy, A.; Jacobs, J.P.; Fragata, J.; Maruszewski, B.; Vida, V.; Sarris, G. The European Congenital Heart Surgeons Association congenital cardiac database: A 25-year summary of congenital heart surgery outcomes†. Eur J Cardiothorac Surg 2025, 67, ezaf119. [Google Scholar] [CrossRef] [PubMed]
- Steurer, M.A.; Baer, R.J.; Chambers, C.D.; Costello, J.; Franck, L.S.; McKenzie-Sampson, S.; Pacheco-Werner, T.L.; Rajagopal, S.; Rogers, E.E.; Rand, L.; Jelliffe-Pawlowski, L.L.; Peyvandi, S. Mortality and Major Neonatal Morbidity in Preterm Infants with Serious Congenital Heart Disease. J Pediatr 2021, 239, 110–116. [Google Scholar] [CrossRef] [PubMed]
- Aly, S.; Qattea, I.; Kattea, M.O.; Aly, H.Z. Neonatal outcomes in preterm infants with severe congenital heart disease: a national cohort analysis. Front Pediatr 2024, 12, 1326804. [Google Scholar] [CrossRef]
- Laas, E.; Lelong, N.; Ancel, P.Y.; Bonnet, D.; Houyel, L.; Magny, J.F.; Andrieu, T.; Goffinet, F. Khoshnood B; EPICARD study group. Impact of preterm birth on infant mortality for newborns with congenital heart defects: The EPICARD population-based cohort study. BMC Pediatr 2017, 17, 124. [Google Scholar] [CrossRef] [PubMed]
- Higgins, B.V.; Levy, P.T.; Ball, M.K.; Kim, M.; Peyvandi, S.; Steurer, M.A. Double Jeopardy: A Distinct Mortality Pattern Among Preterm Infants with Congenital Heart Disease. Pediatr Cardiol 2025, 46, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Norman, M.; Håkansson, S.; Kusuda, S.; Vento, M.; Lehtonen, L.; Reichman, B.; Darlow, B.A.; Adams, M.; Bassler, D.; Isayama, T.; Rusconi, F.; Lee, S.; Lui, K.; Yang, J.; Shah, P. S; International Network for Evaluation of Outcomes in Neonates (iNeo) Investigators* †. Neonatal Outcomes in Very Preterm Infants With Severe Congenital Heart Defects: An International Cohort Study. J Am Heart Assoc 2020, 9, e015369. [Google Scholar] [CrossRef]
- Palma, A.; Morais, S.; Silva, P.V.; Pires, A. Congenital heart defects and preterm birth: Outcomes from a referral center. Rev Port Cardiol 2023, 42, 403–410. [Google Scholar] [CrossRef]
- Arriola-Montenegro, J.; Coronado-Quispe, J.; Mego, J.C.; Luis-Ybáñez, O.; Tauma-Arrué, A.; Chavez-Saldivar, S.; Sierra-Pagan, J.E.; Pinto-Salinas, M.; Marquez, R.; Arboleda, M.; Niño de Guzman, I.; Vera, L.; Alvarez, C.; Bravo-Jaimes, K. Congenital heart disease-related mortality during the first year of life: The peruvian experience. Int J Cardiol Congenit Heart Dis 2024, 19, 100557. [Google Scholar] [CrossRef]
- Su, Z.; Zou, Z.; Hay, S.I.; Liu, Y.; Li, S.; Chen, H.; Naghavi, M.; Zimmerman, M.S.; Martin, G.R.; Wilner, L.B.; Sable, C.A.; Murray, C.J.L.; Kassebaum, N.J.; Patton, G.C.; Zhang, H. Global, regional, and national time trends in mortality for congenital heart disease, 1990-2019: An age-period-cohort analysis for the Global Burden of Disease 2019 study. EClinicalMedicine 2022, 43, 101249. [Google Scholar] [CrossRef] [PubMed]
- Suluba, E.; Shuwei, L.; Xia, Q.; Mwanga, A. Congenital heart diseases: genetics, non-inherited risk factors, and signaling pathways. Egypt J Med Hum Genet 2020, 21, 11. [Google Scholar] [CrossRef]
- Yasuhara, J.; Garg, V. Genetics of congenital heart disease: a narrative review of recent advances and clinical implications. Transl Pediatr 2021, 10, 2366–2386. [Google Scholar] [CrossRef]
- Ossa Galvis, M.M.; Bhakta, R.T.; Tarmahomed, A.; et al. Cyanotic Heart Disease. [Updated 2023 Jun 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available online: https://www.ncbi.nlm.nih.gov/books/NBK500001/.
- Zubrzycki, M.; Schramm, R.; Costard-Jäckle, A.; Grohmann, J.; Gummert, J.F.; Zubrzycka, M. Cardiac Development and Factors Influencing the Development of Congenital Heart Defects (CHDs): Part I. Int J Mol Sci 2024, 25, 7117. [Google Scholar] [CrossRef]
- Villamil, V.I.; Downing, K.F.; Oster, M.E.; Andrews, J.G.; Galindo, M.K.; Patel, J.; Klewer, S.E.; Nembhard, W.N.; Farr, S.L. Comorbidities and Healthcare Utilization Among Young Adults With Congenital Heart Defects by Down Syndrome Status-Congenital Heart Survey to Recognize Outcomes, Needs, and wellbeinG, 2016-2019. Birth Defects Res 2025, 117, e2439. [Google Scholar] [CrossRef]
- Saliba, A.; Figueiredo, A.C.V.; Baroneza, J.E.; Afiune, J.Y.; Pic-Taylor, A.; Oliveira, S.F.; Mazzeu, J.F. Genetic and genomics in congenital heart disease: a clinical review. J Pediatr (Rio J) 2020, 96, 279–288. [Google Scholar] [CrossRef]
- Dimopoulos, K.; Constantine, A.; Clift, P.; Condliffe, R.; Moledina, S.; Jansen, K.; Inuzuka, R.; Veldtman, G.R.; Cua, C.L.; Tay, E.L.W.; Opotowsky, A.R.; Giannakoulas, G.; Alonso-Gonzalez, R.; Cordina, R.; Capone, G.; Namuyonga, J.; Scott, C.H.; D'Alto, M.; Gamero, F.J.; Chicoine, B.; Gu, H.; Limsuwan, A.; Majekodunmi, T.; Budts, W.; Coghlan, G.; Broberg, C. S; for Down Syndrome International (DSi). Cardiovascular Complications of Down Syndrome: Scoping Review and Expert Consensus. Circulation 2023, 147, 425–441. [Google Scholar] [CrossRef] [PubMed]
- Geleta, B.E.; Seyoum, G. Prevalence and Patterns of Congenital Heart Defects and Other Major Non-Syndromic Congenital Anomalies Among Down Syndrome Patients: A Retrospective Study. Int J Gen Med 2024, 17, 1337–1347. [Google Scholar] [CrossRef] [PubMed]
- Dodge-Khatami, A.; Herger, S.; Rousson, V.; Comber, M.; Knirsch, W.; Bauersfeld, U.; Prêtre, R. Outcomes and reoperations after total correction of complete atrio-ventricular septal defect. Eur J Cardiothorac Surg 2008, 34, 745–50. [Google Scholar] [CrossRef]
- Zuechner, A.; Mhada, T.; Majani, N.G.; Sharau, G.G.; Mahalu, W.; Freund, M.W. Spectrum of heart diseases in children presenting to a paediatric cardiac echocardiography clinic in the Lake Zone of Tanzania: a 7 years overview. BMC Cardiovasc Disord 2019, 19, 291. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, S.; Brueckner, M. Genetics and Genomics of Congenital Heart Disease. Circ Res 2017, 120, 923–940. [Google Scholar] [CrossRef]
- Namuyonga, J.; Lubega, S.; Aliku, T.; Omagino, J.; Sable, C.; Lwabi, P. Pattern of congenital heart disease among children presenting to the Uganda Heart Institute, Mulago Hospital: a 7-year review. Afr Health Sci 2020, 20, 745–752. [Google Scholar] [CrossRef]
- Thomford, N.E.; Biney, R.P.; Okai, E.; Anyanful, A.; Nsiah, P.; Frimpong, P.G.; Boakye, D.O.; Adongo, C.A.; Kruszka, P.; Wonkam, A. Clinical Spectrum of congenital heart defects (CHD) detected at the child health Clinic in a Tertiary Health Facility in Ghana: a retrospective analysis. J Congenit Heart Dis 2020, 4, 3. [Google Scholar] [CrossRef]
- Majani, N.G.; Koster, J.R.; Kalezi, Z.E.; Letara, N.; Nkya, D.; Mongela, S.; Kubhoja, S.; Sharau, G.; Mlawi, V.; Grobbee, D.E.; Slieker, M.G.; Chillo, P.; Janabi, M.; Kisenge, P. Spectrum of Heart Diseases in Children in a National Cardiac Referral Center Tanzania, Eastern Africa: A Six-Year Overview. Glob Heart 2024, 19, 61. [Google Scholar] [CrossRef]
- Pugnaloni, F.; Felici, A.; Corno, A.F.; Marino, B.; Versacci, P.; Putotto, C. Gender differences in congenital heart defects: a narrative review. Transl Pediatr 2023, 12, 1753–1764. [Google Scholar] [CrossRef] [PubMed]
- Freilinger, S.; Andonian, C.; Beckmann, J.; Ewert, P.; Kaemmerer, H.; Lang, N.; Nagdyman, N.; Oberhoffer-Fritz, R.; Pieper, L.; Schelling, J.; von Scheidt, F.; Neidenbach, R. Differences in the experiences and perceptions of men and women with congenital heart defects: A call for gender-sensitive, specialized, and integrative care. Int J Cardiol Congenital Heart Dis 2021, 4, 100185. [Google Scholar] [CrossRef]
- Rachamadugu, S.I.; Miller, K.A.; Lee, I.H.; Zou, Y.S. Genetic detection of congenital heart disease. Gynecol Obstet Clin Med 2022, 2, 109–123. [Google Scholar] [CrossRef]
- Chhatwal, K.; Smith, J.J.; Bola, H.; Zahid, A.; Venkatakrishnan, A.; Brand, T. Uncovering the Genetic Basis of Congenital Heart Disease: Recent Advancements and Implications for Clinical Management. CJC Pediatr Congenit Heart Dis 2023, 2(6Part B), 464–480. [Google Scholar] [CrossRef] [PubMed]
- Sevim Bayrak, C.; Zhang, P.; Tristani-Firouzi, M.; Gelb, B.D.; Itan, Y. De novo variants in exomes of congenital heart disease patients identify risk genes and pathways. Genome Med 2020, 12, 9. [Google Scholar] [CrossRef]
- Øyen, N.; Boyd, H.A.; Carstensen, L.; Søndergaard, L.; Wohlfahrt, J.; Melbye, M. Risk of Congenital Heart Defects in Offspring of Affected Mothers and Fathers. Circ Genom Precis Med 2022, 15, e003533. [Google Scholar] [CrossRef]
- Patra, S.; Rama Sastry, U.M.; Mahimaiha, J.; Subramanian, A.P.; Shankarappa, R.K.; Nanjappa, M.C. Spectrum of cyanotic congenital heart disease diagnosed by echocardiographic evaluation in patients attending paediatric cardiology clinic of a tertiary cardiac care centre. Cardiol Young 2015, 25, 861–7. [Google Scholar] [CrossRef] [PubMed]
- Shahid, S.; Khurram, H.; Lim, A.; Shabbir, M.F.; Billah, B. Prediction of cyanotic and acyanotic congenital heart disease using machine learning models. World J Clin Pediatr 2024, 13, 98472. [Google Scholar] [CrossRef] [PubMed]
- Mohammad, M.; James, A.F.; Qureshi, R.S.; Saraf, S.; Ahluwalia, T.; Mukherji, J.D.; Kole, T. Acute ischemic stroke in a child with cyanotic congenital heart disease due to non-compliance of anticoagulation. World J Emerg Med 2012, 3, 154–6. [Google Scholar] [CrossRef]
- Manuel, V.; Miana, L.A.; Solla, D.J.F.; Fernandes, N.; Carrillo, G.; Jatene, M.B. Preoperative level of neutrophil-lymphocyte ratio: Comparison between cyanotic and acyanotic congenital heart disease. J Card Surg 2021, 36, 1376–1380. [Google Scholar] [CrossRef]
- Downing, K.F.; Oster, M.E.; Klewer, S.E.; Rose, C.E.; Nembhard, W.N.; Andrews, J.G.; Farr, S.L. Disability Among Young Adults With Congenital Heart Defects: Congenital Heart Survey to Recognize Outcomes, Needs, and Well-Being 2016-2019. J Am Heart Assoc 2021, 10, e022440. [Google Scholar] [CrossRef]
- Brosig, C.L.; Bear, L.; Allen, S.; Hoffmann, R.G.; Pan, A.; Frommelt, M.; Mussatto, K.A. Preschool Neurodevelopmental Outcomes in Children with Congenital Heart Disease. J Pediatr 2017, 183, 80–86. [Google Scholar] [CrossRef]
- Raj, M.; Chattopadhyay, A.; Gupta, S.K.; Jain, S.; Sastry, U.M.K.; Sudevan, R.; Sharma, M.; Pragya, P.; Shivashankar, R.; Sudhakar, A.; Radhakrishnan, A.; Parveen, S.; Patil, S.; Naik, S.; Das, S.; Kumar, R.K. Neurodevelopmental outcomes after infant heart surgery for congenital heart disease: a hospital-based multicentre prospective cohort study from India. BMJ Paediatr Open 2025, 9, e002943. [Google Scholar] [CrossRef]
- White, B.R.; Rogers, L.S.; Kirschen, M.P. Recent advances in our understanding of neurodevelopmental outcomes in congenital heart disease. Curr Opin Pediatr 2019, 31, 783–788. [Google Scholar] [CrossRef]
- Farr, S.L.; Downing, K.F.; Tepper, N.K.; Oster, M.E.; Glidewell, M.J.; Reefhuis, J. Reproductive Health of Women with Congenital Heart Defects. J Womens Health (Larchmt) 2023, 32, 132–137. [Google Scholar] [CrossRef]
- Meng, X.; Song, M.; Zhang, K.; Lu, W.; Li, Y.; Zhang, C.; Zhang, Y. Congenital heart disease: types, pathophysiology, diagnosis, and treatment options. MedComm (2020) 2024, 5, e631. [Google Scholar] [CrossRef]
- Ren, C.; Wu, C.; Pan, Z.; Li, Y. Minimally invasive closure of transthoracic ventricular septal defect: postoperative complications and risk factors. J Cardiothorac Surg 2021, 16, 30. [Google Scholar] [CrossRef]
- Turner, M.E.; Bouhout, I.; Petit, C.J.; Kalfa, D. Transcatheter Closure of Atrial and Ventricular Septal Defects: JACC Focus Seminar. J Am Coll Cardiol 2022, 79, 2247–2258. [Google Scholar] [CrossRef]
- Elafifi, A.; Kotit, S.; Shehata, M.; Deyaa, O.; Ramadan, A.; Tawfik, M. Early experience with transcatheter ventricular septal defects closure with the KONAR-MF multifunctional occluder. Front Pediatr 2025, 13, 1528490. [Google Scholar] [CrossRef]
- Diab, K.A.; Cao, Q.L.; Hijazi, Z.M. Perventricular closure of muscular ventricular septal defects: How do I do it? Ann Pediatr Cardiol 2008, 1, 27–33. [Google Scholar] [CrossRef]
- Bah, M.N.M.; Sapian, M.H.; Anuar, M.H.M.; Alias, E.Y. Survival and outcomes of isolated neonatal ventricular septal defects: A population-based study from a middle-income country. Ann Pediatr Cardiol 2023, 16, 322–330. [Google Scholar] [CrossRef]
- Pihl, C.; Sillesen, A.S.; Norsk, J.B.; Vøgg, R.O.B.; Vedel, C.; Boyd, H.A.; Vejlstrup, N.; Axelsson Raja, A.; Bundgaard, H.; Iversen, K.K. The Prevalence and Spontaneous Closure of Ventricular Septal Defects the First Year of Life. Neonatology 2024, 121, 742–751. [Google Scholar] [CrossRef]
- Durden, R.E.; Turek, J.W.; Reinking, B.E.; Bansal, M. Acquired ventricular septal defect due to infective endocarditis. Ann Pediatr Cardiol 2018, 11, 100–102. [Google Scholar] [CrossRef]
- Sabiniewicz, R.; Huczek, Z.; Zbroński, K.; Scisło, P.; Rymuza, B.; Kochman, J.; Marć, M.; Grygier, M.; Araszkiewicz, A.; Dziarmaga, M.; Leśniewicz, P.; Hiczkiewicz, J.; Kidawa, M.; Filipiak, K.J.; Opolski, G. Percutaneous Closure of Post-Infarction Ventricular Septal Defects-An Over Decade-long Experience. J Interv Cardiol 2017, 30, 63–71. [Google Scholar] [CrossRef]
- Khajali, Z.; Firouzi, A.; Jorfi, F.; Keshavarz Hedayati, M. Device closure of a traumatic VSD in a young man with a history of a stab wound to the chest. J Cardiol Cases 2020, 21, 217–219. [Google Scholar] [CrossRef]
- Zughaib, M.T.; LaVoie, J.; Multani, N.; Darda, S. An Incidental Case of a Rare Ventricular Septal Defect (VSD): Does Infective Endocarditis Ger-Bode Well? Cureus 2024, 16, e60677. [Google Scholar] [CrossRef]
- Cinteză, E.E.; Butera, G. Complex ventricular septal defects. Update on percutaneous closure. Rom J Morphol Embryol 2016, 57, 1195–1205. [Google Scholar]
- Mainzer, G.; Rosenthal, E.; Austin, C.; Morgan, G. Hybrid Approach for Recanalization and Stenting of Acquired Pulmonary Vein Occlusion. Pediatr Cardiol 2016, 37, 983–5. [Google Scholar] [CrossRef]
- Zhao, Q.M.; Niu, C.; Liu, F.; Wu, L.; Ma, X.J.; Huang, G.Y. Spontaneous Closure Rates of Ventricular Septal Defects (6,750 Consecutive Neonates). Am J Cardiol 2019, 124, 613–617, Erratum in: Am J Cardiol 2020, 125(2), 302. doi: 10.1016/j.amjcard.2019.10.003. [Google Scholar] [CrossRef]
- Lopez, L.; Houyel, L.; Colan, S.D.; Anderson, R.H.; Béland, M.J.; Aiello, V.D.; Bailliard, F.; Cohen, M.S.; Jacobs, J.P.; Kurosawa, H.; Sanders, S.P.; Walters, H.L. 3rd.; Weinberg P.M.; Boris J.R.; Cook A.C.; Crucean A.; Everett A.D.; Gaynor J.W.; Giroud J.; Guleserian K.J.; Hughes M.L.; Juraszek A.L.; Krogmann O.N.; Maruszewski B.J.; St Louis J.D.; Seslar S.P.; Spicer D.E.; Srivastava S.; Stellin G.; Tchervenkov C.I.; Wang L.; Franklin R.C.G. Classification of Ventricular Septal Defects for the Eleventh Iteration of the International Classification of Diseases-Striving for Consensus: A Report From the International Society for Nomenclature of Paediatric and Congenital Heart Disease. Ann Thorac Surg 2018, 106, 1578–1589. [Google Scholar] [CrossRef]
- Liu, J.X.; Wang, J.H.; Yang, S.R.; Liu, M.; Xu, Y.; Sun, J.H.; Yan, C.Y. Clinical utility of the ventricular septal defect diameter to aorta root diameter ratio to predict early childhood developmental defects or lung infections in patients with perimembranous ventricular septal defect. J Thorac Dis 2013, 5, 600–4. [Google Scholar] [CrossRef]
- Moradian, M.; Alizadehasl, A. Ventricular Septal Defect (VSD). In: Moradian, M., Alizadehasl, A. (eds) Atlas of Echocardiography in Pediatrics and Congenital Heart Diseases. Springer, Berlin, Heidelberg, 2021. [CrossRef]
- Mladenova, M.K.; Bakardzhiev, I.V.; Hadji Lega, M.; Lingman, G. Apparently isolated ventricular septal defect, prenatal diagnosis, association with chromosomal aberrations, spontaneous closure rate in utero and during the first year of life: a systematic review. Folia Med (Plovdiv) 2023, 65, 871–878. [Google Scholar] [CrossRef]
- Kim, A.Y.; Tchah, N.; Lin, C.Y.; Park, J.M.; Woo, W.; Kim, C.S.; Jung, S.Y.; Choi, J.Y.; Jung, J.W. Predictive Scoring System for Spontaneous Closure of Infant Ventricular Septal Defect: The P-VSD Score. Pediatr Cardiol 2025, 46, 401–408. [Google Scholar] [CrossRef]
- Chen, X.; Zhang, Q.; Lu, M.; Feng, Q.; Qin, L.; Liao, S. Prenatal finding of isolated ventricular septal defect: genetic association, outcomes and counseling. Front Genet 2024, 15, 1447216. [Google Scholar] [CrossRef]
- Bride, P.; Kaestner, M.; Radermacher, M.; Vitanova, K.; von Scheidt, F.; Scharnbeck, D.; Apitz, C. Spontaneous Closure of Perimembranous Ventricular Septal Defects: A Janus-Faced Condition. CASE (Phila) 2019, 4, 103–105. [Google Scholar] [CrossRef]
- Adilbekova, A.; Marasulov, S.; Nurkeyev, B.; Kozhakhmetov, S. Evolution of surgery of ventricular septal defect closure. J Clin Med Kaz 2022, 19, 4–8. [Google Scholar] [CrossRef]
- Gray, R.G.; Menon, S.C.; Johnson, J.T.; Armstrong, A.K.; Bingler, M.A.; Breinholt, J.P.; Kenny, D.; Lozier, J.; Murphy, J.J.; Sathanandam, S.K.; Taggart, N.W.; Trucco, S.M.; Goldstein, B.H.; Gordon, B.M. Acute and midterm results following perventricular device closure of muscular ventricular septal defects: A multicenter PICES investigation. Catheter Cardiovasc Interv 2017, 90, 281–289. [Google Scholar] [CrossRef]
- Kang, S.L.; Tometzki, A.; Caputo, M.; Morgan, G.; Parry, A.; Martin, R. Longer-term outcome of perventricular device closure of muscular ventricular septal defects in children. Catheter Cardiovasc Interv 2015, 85, 998–1005. [Google Scholar] [CrossRef]
- Bergmann, M.; Germann, C.P.; Nordmeyer, J.; Peters, B.; Berger, F.; Schubert, S. Short- and Long-term Outcome After Interventional VSD Closure: A Single-Center Experience in Pediatric and Adult Patients. Pediatr Cardiol 2021, 42, 78–88. [Google Scholar] [CrossRef]
- Küçükosmanoğlu, M.; Koç, A.S.; Sümbül, H.E.; Koca, H.; Çakır Pekoz, B.; Koç, M. Liver stiffness value obtained by point shear-wave elastography is significantly related with atrial septal defect size. Diagn Interv Radiol 2020, 26, 284–291. [Google Scholar] [CrossRef]
- Cinteza, E.; Vasile, C.M.; Busnatu, S.; Armat, I.; Spinu, A.D.; Vatasescu, R.; Duica, G.; Nicolescu, A. Can Artificial Intelligence Revolutionize the Diagnosis and Management of the Atrial Septal Defect in Children? Diagnostics (Basel) 2024, 14, 132. [Google Scholar] [CrossRef]
- Fraisse, A.; Latchman, M.; Sharma, S.R.; Bayburt, S.; Amedro, P.; di Salvo, G.; Baruteau, A.E. Atrial septal defect closure: indications and contra-indications. J Thorac Dis 2018, 10 (Suppl 24), S2874–S2881. [Google Scholar] [CrossRef]
- Menillo, A.M.; Alahmadi, M.H.; Pearson-Shaver, A.L. Atrial Septal Defect. [Updated 2025 Jan 21]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available online: https://www.ncbi.nlm.nih.gov/books/NBK535440/.
- Rodríguez Fernández, A.; Bethencourt González, A. Imaging Techniques in Percutaneous Cardiac Structural Interventions: Atrial Septal Defect Closure and Left Atrial Appendage Occlusion. Rev Esp Cardiol (Engl Ed) 2016, 69, 766–77. [Google Scholar] [CrossRef]
- Sommer, R.J.; Love, B.A.; Paolillo, J.A.; Gray, R.G.; Goldstein, B.H.; Morgan, G.J.; Gillespie, M. J; ASSURED Investigators. ASSURED clinical study: New GORE® CARDIOFORM ASD occluder for transcatheter closure of atrial septal defect. Catheter Cardiovasc Interv 2020, 95, 1285–1295. [Google Scholar] [CrossRef] [PubMed]
- Brancato, F.; Stephenson, N.; Rosenthal, E.; Hansen, J.H.; Jones, M.I.; Qureshi, S.; Austin, C.; Speggiorin, S.; Caner, S.; Butera, G. Transcatheter versus surgical treatment for isolated superior sinus venosus atrial septal defect. Catheter Cardiovasc Interv 2023, 101, 1098–1107. [Google Scholar] [CrossRef] [PubMed]
- Pekoz, B.C.; Koc, M.; Kucukosmanoglu, M.; Koc, A.S.; Koca, H.; Dönmez, Y.; Sumbul, H.E. Evaluation of Liver Stiffness After Atrial Septal Defect Closure. Ultrasound Q 2022, 38, 165–169. [Google Scholar] [CrossRef]
- Thingnam, S.K.S.; Mahajan, S.; Kumar, V. Surgical perspective of percutaneous device closure of atrial septal defect. Asian Cardiovasc Thorac Ann 2018, 26, 343–346. [Google Scholar] [CrossRef] [PubMed]
- Adhikari, C.M.; Bogati, A.; Prajapati, D.; Dhungel, S.; Najmy, S.; Acharya, K.; Shahi, R.; Subedi, C.; Adhikari, J.; Sharma, D. Atrial Septal Defect Size and Rims on Transesophageal Echocardiogram. Maedica (Bucur) 2019, 14, 81–85. [Google Scholar] [CrossRef]
- Bashir, F.; Hameed, M.; Hanif, B.; Aijaz, S. Outcomes and complications of percutaneous device closure in adults with secundum atrial septal defect. J Pak Med Assoc 2022, 72, 385–389. [Google Scholar] [CrossRef]
- Crawford, G.B.; Brindis, R.G.; Krucoff, M.W.; Mansalis, B.P.; Carroll, J.D. Percutaneous atrial septal occluder devices and cardiac erosion: a review of the literature. Catheter Cardiovasc Interv 2012, 80, 157–67. [Google Scholar] [CrossRef]
- Mendirichaga, R.; Smairat, R.A.; Sancassani, R. Late tissue erosion after transcatheter closure of an atrial septal defect. Catheter Cardiovasc Interv 2017, 89, 502–504. [Google Scholar] [CrossRef]
- Abe, T.; Tsukano, S.; Tosaka, Y. Pericardial tamponade due to erosion of a Figulla Flex II device after closure of an atrial septal defect. Catheter Cardiovasc Interv 2019, 94, 1003–1005. [Google Scholar] [CrossRef]
- Shrivastava, S.; Shrivastava, S.; Allu, S.V.V.; Schmidt, P. Transcatheter Closure of Atrial Septal Defect: A Review of Currently Used Devices. Cureus 2023, 15, e40132. [Google Scholar] [CrossRef]
- Hribernik, I.; Thomson, J.; Bhan, A.; Mullen, M.; Noonan, P.; Smith, B.; Walker, N.; Deri, A.; Bentham, J. A novel device for atrial septal defect occlusion (GORE CARDIOFORM). EuroIntervention 2023, 19, 782–788. [Google Scholar] [CrossRef]
- Qureshi, A.M.; Sommer, R.J.; Morgan, G.; Paolillo, J.A.; Gray, R.G.; Love, B.; Goldstein, B.H.; Sugeng, L.; Gillespie, M. J; GORE ASSURED Clinical Trial Investigators. Long-Term Results of the Atrial Septal Defect Occluder ASSURED Trial for Combined Pivotal/Continued Access Cohorts. JACC Cardiovasc Interv 2024, 17, 2274–2283. [Google Scholar] [CrossRef]
- Park, J.; Yoon, S.J.; Han, J.; Song, I.G.; Lim, J.; Shin, J.E.; Eun, H.S.; Park, K.I.; Park, M.S.; Lee, S.M. Patent ductus arteriosus treatment trends and associated morbidities in neonates. Sci Rep 2021, 11, 10689. [Google Scholar] [CrossRef]
- Khowaja, W.; Akhtar, S.; Jiwani, U.; Mohsin, M.; Shaheen, F.; Ariff, S. Outcomes of preterm neonates with patent ductus arteriosus: A retrospective review from a tertiary care hospital. J Pak Med Assoc 2022, 72, 2065–2068. [Google Scholar] [CrossRef]
- Gillam-Krakauer, M.; Mahajan, K. Patent Ductus Arteriosus. [Updated 2023 Aug 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available online: https://www.ncbi.nlm.nih.gov/books/NBK430758/.
- Morville, P.; Akhavi, A. Transcatheter closure of hemodynamic significant patent ductus arteriosus in 32 premature infants by amplatzer ductal occluder additional size-ADOIIAS. Catheter Cardiovasc Interv 2017, 90, 612–617. [Google Scholar] [CrossRef]
- Wang, J.N.; Lin, Y.C.; Hsieh, M.L.; Wei, Y.J.; Ju, Y.T.; Wu, J.M. Transcatheter Closure of Patent Ductus Arteriosus in Premature Infants With Very Low Birth Weight. Front Pediatr 2021, 8, 615919. [Google Scholar] [CrossRef] [PubMed]
- Tomasulo, C.E.; Gillespie, M.J.; Munson, D.; Demkin, T.; O'Byrne, M.L.; Dori, Y.; Smith, C.L.; Rome, J.J.; Glatz, A.C. Incidence and fate of device-related left pulmonary artery stenosis and aortic coarctation in small infants undergoing transcatheter patent ductus arteriosus closure. Catheter Cardiovasc Interv 2020, 96, 889–897. [Google Scholar] [CrossRef]
- Sellmer, A.; Bjerre, J.V.; Schmidt, M.R.; McNamara, P.J.; Hjortdal, V.E.; Høst, B.; Bech, B.H.; Henriksen, T.B. Morbidity and mortality in preterm neonates with patent ductus arteriosus on day 3. Arch Dis Child Fetal Neonatal Ed 2013, 98, F505–F510. [Google Scholar] [CrossRef] [PubMed]
- Terrin, G.; Di Chiara, M.; Boscarino, G.; Metrangolo, V.; Faccioli, F.; Onestà, E.; Giancotti, A.; Di Donato, V.; Cardilli, V.; De Curtis, M. Morbidity associated with patent ductus arteriosus in preterm newborns: a retrospective case-control study. Ital J Pediatr 2021, 47, 9. [Google Scholar] [CrossRef] [PubMed]
- Rozé, J.C.; Cambonie, G.; Marchand-Martin, L.; Gournay, V.; Durrmeyer, X.; Durox, M.; Storme, L.; Porcher, R.; Ancel, P. Y; Hemodynamic EPIPAGE 2 Study Group. Association Between Early Screening for Patent Ductus Arteriosus and In-Hospital Mortality Among Extremely Preterm Infants. JAMA 2015, 313, 2441–8. [Google Scholar] [CrossRef]
- European Commission EUROCAT Prevalence charts and tables. Last update in April 2025. Available online: https://eu-rd-platform.jrc.ec.europa.eu/eurocat/eurocat-data/prevalence_en (accessed on 11 June 2025).
- Aldersley, T.; Lawrenson, J.; Human, P.; Shaboodien, G.; Cupido, B.; Comitis, G.; De Decker, R.; Fourie, B.; Swanson, L.; Joachim, A.; Magadla, P.; Ngoepe, M.; Swanson, L.; Revell, A.; Ramesar, R.; Brooks, A.; Saacks, N.; De Koning, B.; Sliwa, K.; Anthony, J.; Osman, A.; Keavney, B.; Zühlke, L. PROTEA.; A Southern African Multicenter Congenital Heart Disease Registry and Biorepository: Rationale, Design, and Initial Results. Front Pediatr 2021, 9, 763060. [Google Scholar] [CrossRef]
- Abdulkadir, M.; Abdulkadir, Z. A systematic review of trends and patterns of congenital heart disease in children in Nigeria from 1964-2015. Afr Health Sci 2016, 16, 367–77. [Google Scholar] [CrossRef]
- Nicholson, C.; Strange, G.; Ayer, J.; Cheung, M.; Grigg, L.; Justo, R.; Maxwell, R.; Wheaton, G.; Disney, P.; Yim, D.; Stewart, S.; Cordina, R.; Celermajer, D.S. A national Australian Congenital Heart Disease registry; methods and initial results. Int J Cardiol Congenit Heart Dis 2024, 17, 100538. [Google Scholar] [CrossRef]
- An, G.; Zhang, H.; Zheng, S.; Wang, W.; Ma, L. Mid-term Outcomes of Common Congenital Heart Defects Corrected Through a Right Subaxillary Thoracotomy. Heart Lung Circ 2017, 26, 376–382. [Google Scholar] [CrossRef]
- Yadeta, D.; Guteta, S.; Alemayehu, B.; Mekonnen, D.; Gedlu, E.; Benti, H.; Tesfaye, H.; Berhane, S.; Hailu, A.; Luel, A.; Hailu, T.; Daniel, W.; Haileamlak, A.; Gudina, E.K.; Negeri, G.; Mekonnen, D.; Woubeshet, K.; Egeno, T.; Lemma, K.; Kshettry, V.R.; Tefera, E. Spectrum of cardiovascular diseases in six main referral hospitals of Ethiopia. Heart Asia 2017, 9, e010829. [Google Scholar] [CrossRef] [PubMed]
- Giraldo-Grueso, M.; Zarante, I.; Mejía-Grueso, A.; Gracia, A. Risk factors for congenital heart disease: A case-control study. Revista Colombiana de Cardiología 2020, 27, 324–329. [Google Scholar] [CrossRef]
- Edwin, F.; Zühlke, L.; Farouk, H.; Mocumbi, A.O.; Entsua-Mensah, K.; Delsol-Gyan, D.; Bode-Thomas, F.; Brooks, A.; Cupido, B.; Tettey, M.; Aniteye, E.; Tamatey, M.M.; Gyan, K.B.; Tchoumi, J.C.T.; Elgamal, M.A. Status and Challenges of Care in Africa for Adults With Congenital Heart Defects. World J Pediatr Congenit Heart Surg 2017, 8, 495–501. [Google Scholar] [CrossRef] [PubMed]
- Eshetu, M.A.; Goshu, D.Y.; Kebede, M.A.; Negate, H.M.; Habtezghi, A.B.; Gregory, P.M.; Wirtu, A.T.; Gemechu, J.M. Patterns and Complications of Congenital Heart Disease in Adolescents and Adults in Ethiopia. J Cardiovasc Dev Dis 2024, 11, 253. [Google Scholar] [CrossRef]
- Spicer, D.E.; Hsu, H.H.; Co-Vu, J.; Anderson, R.H.; Fricker, F.J. Ventricular septal defect. Orphanet J Rare Dis 2014, 9, 144. [Google Scholar] [CrossRef]
- Jacobs, M.L.; Jacobs, J.P. Operative Techniques for Repair of Muscular Ventricular Septal Defects. Oper Tech Thorac Cardiovasc Surg 2010, 15, 2–17. [Google Scholar] [CrossRef]
- Song, J. Percutaneous Transcatheter Closure of Congenital Ventricular Septal Defects. Korean Circ J 2023, 53, 134–150. [Google Scholar] [CrossRef]
- Alakhfash, A.A.; Jelly, A.; Almesned, A.; Alqwaiee, A.; Almutairi, M.; Salah, S.; Hasan, M.; Almuhaya, M.; Alnajjar, A.; Mofeed, M.; Nasser, B. Cardiac Catheterisation Interventions in Neonates and Infants Less Than Three Months. J Saudi Heart Assoc 2020, 32, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.L.; Staffa, S.J.; Adams, P.S.; Caplan, L.A.; Gleich, S.J.; Hernandez, J.L.; Richtsfeld, M.; Riegger, L.Q.; Vener, D.F. Intraoperative cardiac arrest in patients undergoing congenital cardiac surgery. JTCVS Open 2024, 22, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Minette, M.S.; Sahn, D.J. Ventricular septal defects. Circulation Erratum in: Circulation 2007, 115, e205. 2006, 114, 2190–7. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.H.; Spicer, D.E.; Giroud, J.M.; Mohun, T.J. Tetralogy of Fallot: nosological, morphological, and morphogenetic considerations. Cardiol Young 2013, 23, 858–66. [Google Scholar] [CrossRef]
- Morray, B.H. Ventricular Septal Defect Closure Devices, Techniques, and Outcomes. Interv Cardiol Clin 2019, 8, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Murray, G. Closure of Defects in Cardiac Septa. Ann Surg 1948, 128, 843–52. [Google Scholar] [CrossRef]
- Bailey, C.P.; Lacy, M.H.; Neptune, W.B.; Weller, R.; Arvanitis, C.S.; Karasic, J. Experimental and clinical attempts at correction of interventricular septal defects. Ann Surg 1952, 136, 919–36. [Google Scholar] [CrossRef]
- Kay, E.B.; Zimmerman, H.A. Surgical repair of intraventricular septal defects: report of a case. J Am Med Assoc 1954, 154, 986–7. [Google Scholar] [CrossRef]
- Lillehei, C.W.; Cohen, M.; Warden, H.E.; Ziegler, N.R.; Varco, R.L. The results of direct vision closure of ventricular septal defects in eight patients by means of controlled cross circulation. Surg Gynecol Obstet 1955, 101, 446–66. [Google Scholar] [PubMed]
- Lillehei, C.W.; Varco, R.L.; Cohen, M.; Warden, H.E.; Patton, C.; Moller, J.H. The first open-heart repairs of ventricular septal defect, atrioventricular communis, and tetralogy of Fallot using extracorporeal circulation by cross-circulation: a 30-year follow-up. Ann Thorac Surg 1986, 41, 4–21. [Google Scholar] [CrossRef]
- Clarkson, P.M.; Frye, R.L.; DuShane, J.W.; Burchell, H.B.; Wood, E.H.; Weidman, W.H. Prognosis for patients with ventricular septal defect and severe pulmonary vascular obstructive disease. Circulation 1968, 38, 129–35. [Google Scholar] [CrossRef] [PubMed]
- Stirling, G.R.; Stanley, P.H.; Lillehei, C.W. The effects of cardiac bypass and ventriculotomy upon right ventricular function; with report of successful closure of ventricular septal defect by use of atriotomy. Surg Forum 1957, 8, 433–438. [Google Scholar]
- Okamoto, Y. [Clinical studies on open heart surgery in infants with profound hypothermia]. Nihon Geka Hokan 1969, 38, 188–207. [Google Scholar] [PubMed]
- Kirklin, J.W.; Dushane, J.W. Repair of ventricular septal defect in infancy. Pediatrics 1961, 27, 961–966. [Google Scholar] [CrossRef]
- Sigmann, J.M.; Stern, A.M.; Sloan, H.E. Early surgical correction of large ventricular septal defects. Pediatrics 1967, 39, 4–13. [Google Scholar] [CrossRef]
- Barratt-Boyes, B.G.; Simpson, M.; Neutze, J.M. Intracardiac surgery in neonates and infants using deep hypothermia with surface cooling and limited cardiopulmonary bypass. Circulation 1971, 43(5 Suppl), I25–30. [Google Scholar] [CrossRef]
- Barratt-Boyes, B.G.; Neutze, J.M.; Clarkson, P.M.; Shardey, G.C.; Brandt, P.W. Repair of ventricular septal defect in the first two years of life using profound hypothermia-circulatory arrest techniques. Ann Surg 1976, 184, 376–90. [Google Scholar] [CrossRef]
- Xiong, T.; Pu, L.; Ma, Y.F.; Zhu, Y.L.; Cui, X.; Li, H.; Zhan, X.; Li, Y.X. Safety of Normothermic Cardiopulmonary Bypass in Pediatric Cardiac Surgery: A System Review and Meta-Analysis. Front Pediatr 2021, 9, 757551. [Google Scholar] [CrossRef]
- Xing, Q.; Wu, Q.; Pan, S.; Ren, Y.; Wan, H. Transthoracic device closure of ventricular septal defects without cardiopulmonary bypass: experience in infants weighting less than 8 kg. Eur J Cardiothorac Surg 2011, 40, 591–7. [Google Scholar] [CrossRef]
- Huang, J.S.; Huang, S.T.; Sun, K.P.; Hong, Z.N.; Chen, L.W.; Kuo, Y.R.; Chen, Q. Health-related quality of life in children and adolescents undergoing intraoperative device closure of isolated perimembranous ventricular septal defects in southeastern China. J Cardiothorac Surg 2019, 14, 218. [Google Scholar] [CrossRef]
- Omelchenko, A.; Jha, N.K.; Shah, N.; AbdelMassih, A.; Montiel, J.P.; Rajkumar, B.R. Perventricular device closure of the ventricular septal defects in children-first experience in the United Arab Emirates. J Cardiothorac Surg 2024, 19, 430. [Google Scholar] [CrossRef]
- Yang, T.; Tiemuerniyazi, X.; Hu, Z.; Feng, W.; Xu, F. Analysis of cardiac arrest after coronary artery bypass grafting. J Cardiothorac Surg 2024, 19, 451. [Google Scholar] [CrossRef]
- Squiccimarro, E.; Stasi, A.; Lorusso, R.; Paparella, D. Narrative review of the systemic inflammatory reaction to cardiac surgery and cardiopulmonary bypass. Artif Organs 2022, 46, 568–577. [Google Scholar] [CrossRef] [PubMed]
- Li, M.; Nie, Y.; Qiu, G.; Jiang, Y.; Muthialu, N.; Yang, Z. Risk factors for early secondary infections after cardiopulmonary bypass in children with congenital heart disease: a single-center analysis of 265 cases. Transl Pediatr 2025, 14, 104–112. [Google Scholar] [CrossRef]
- Gaynor, J.W.; Stopp, C.; Wypij, D.; Andropoulos, D.B.; Atallah, J.; Atz, A.M.; Beca, J.; Donofrio, M.T.; Duncan, K.; Ghanayem, N.S.; Goldberg, C.S.; Hövels-Gürich, H.; Ichida, F.; Jacobs, J.P.; Justo, R.; Latal, B.; Li, J.S.; Mahle, W.T.; McQuillen, P.S.; Menon, S.C.; Pemberton, V.L.; Pike, N.A.; Pizarro, C.; Shekerdemian, L.S.; Synnes, A.; Williams, I.; Bellinger, D.C.; Newburger, J. W; International Cardiac Collaborative on Neurodevelopment (ICCON) Investigators. Neurodevelopmental outcomes after cardiac surgery in infancy. Pediatrics 2015, 135, 816–25. [Google Scholar] [CrossRef]
- Naguib, A.N.; Winch, P.D.; Tobias, J.D.; Yeates, K.O.; Miao, Y.; Galantowicz, M.; Hoffman, T.M. Neurodevelopmental outcome after cardiac surgery utilizing cardiopulmonary bypass in children. Saudi J Anaesth 2015, 9, 12–8. [Google Scholar] [CrossRef] [PubMed]
- Whiting, D.; Yuki, K.; DiNardo, J.A. Cardiopulmonary bypass in the pediatric population. Best Pract Res Clin Anaesthesiol 2015, 29, 241–56. [Google Scholar] [CrossRef] [PubMed]
- Matsuda, M.; Takemura, H.; Yamashita, A.; Matsuoka, Y.; Sawa, T.; Amaya, F. Post-surgical chronic pain and quality of life in children operated for congenital heart disease. Acta Anaesthesiol Scand 2019, 63, 745–750. [Google Scholar] [CrossRef]
- de Hoogd, S.; Goulooze, S.C.; Valkenburg, A.J.; Krekels, E.H.J.; van Dijk, M.; Tibboel, D.; Knibbe, C.A.J. Postoperative breakthrough pain in paediatric cardiac surgery not reduced by increased morphine concentrations. Pediatr Res 2021, 90, 1201–1206. [Google Scholar] [CrossRef] [PubMed]
- Yuan, Y.; Pan, B.; Liang, X.; Lv, T.; Tian, J. Health-related quality of life in children with congenital heart disease following interventional closure versus minimally invasive closure. Front Cardiovasc Med 2022, 9, 974720. [Google Scholar] [CrossRef] [PubMed]
- Mishaly, D.; Ghosh, P.; Preisman, S. Minimally invasive congenital cardiac surgery through right anterior minithoracotomy approach. Ann Thorac Surg 2008, 85, 831–5. [Google Scholar] [CrossRef]
- Wang, Q.; Li, Q.; Zhang, J.; Wu, Z.; Zhou, Q.; Wang, D.J. Ventricular septal defects closure using a minimal right vertical infraaxillary thoracotomy: seven-year experience in 274 patients. Ann Thorac Surg 2010, 89, 552–5. [Google Scholar] [CrossRef]
- Vo, A.T.; Vu, T.T.; Nguyen, D.H. Ministernotomy for correction of ventricular septal defect. J Cardiothorac Surg 2016, 11, 71. [Google Scholar] [CrossRef]
- Heinisch, P.P.; Wildbolz, M.; Beck, M.J.; Bartkevics, M.; Gahl, B.; Eberle, B.; Erdoes, G.; Jenni, H.J.; Schoenhoff, F.; Pfammatter, J.P.; Carrel, T.; Kadner, A. Vertical Right Axillary Mini-Thoracotomy for Correction of Ventricular Septal Defects and Complete Atrioventricular Septal Defects. Ann Thorac Surg 2018, 106, 1220–1227. [Google Scholar] [CrossRef]
- Lock, J.E.; Block, P.C.; McKay, R.G.; Baim, D.S.; Keane, J.F. Transcatheter closure of ventricular septal defects. Circulation 1988, 78, 361–8. [Google Scholar] [CrossRef]
- Pedra, C.A.; Pedra, S.R.; Esteves, C.A.; Pontes, S.C. Jr.; Braga, S.L.; Arrieta, S.R.; Santana, M.V.; Fontes, V.F.; Masura, J. Percutaneous closure of perimembranous ventricular septal defects with the Amplatzer device: technical and morphological considerations. Catheter Cardiovasc Interv 2004, 61, 403–10. [Google Scholar] [CrossRef]
- Masura, J.; Gao, W.; Gavora, P.; Sun, K.; Zhou, A.Q.; Jiang, S.; Ting-Liang, L.; Wang, Y. Percutaneous closure of perimembranous ventricular septal defects with the eccentric Amplatzer device: multicenter follow-up study. Pediatr Cardiol 2005, 26, 216–9. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, S.; Mukherji, A.; Chattopadhyay, A. Percutaneous closure of moderate to large perimembranous ventricular septal defect in small children using left ventricular mid-cavity approach. Indian Heart J 2020, 72, 570–575. [Google Scholar] [CrossRef]
- Pillai, A.A.; Rangasamy, S.; Balasubramonian, V.R. Transcatheter Closure of Moderate to Large Perimembranous Ventricular Septal Defects in Children Weighing 10 kilograms or less. World J Pediatr Congenit Heart Surg 2019, 10, 278–285. [Google Scholar] [CrossRef]
- Wongwaitaweewong, K.; Promphan, W.; Roymanee, S.; Prachasilchai, P. Effect of transcatheter closure by AmplatzerTM Duct Occluder II in patients with small ventricular septal defect. Cardiovasc Interv Ther 2021, 36, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Elmarsafawy, H.; Hafez, M.; Alsawah, G.A.; Bakr, A.; Rakha, S. Long-term outcomes of percutaneous closure of ventricular septal defects in children using different devices: A single centre experience from Egypt. BMC Pediatr 2023, 23, 381. [Google Scholar] [CrossRef]
- Roymanee, S.; Su-angka, N.; Promphan, W.; Wongwaitaweewong, K.; Jarutach, J.; Buntharikpornpun, R.; Prachasilchai, P. Outcomes of Transcatheter Closure in Outlet-Type Ventricular Septal Defect after 1 Year. Congenit Heart Dis 2023, 18, 169–181. [Google Scholar] [CrossRef]
- Andersen, M.M.; Zhao, D.X.M. Percutaneous Post-Myocardial Infarction Ventricular Septal Rupture Closure: A Review. Structural Heart 2018, 2, 121–126. [Google Scholar] [CrossRef]
- Saurav, A.; Kaushik, M.; Mahesh Alla, V.; White, M.D.; Satpathy, R.; Lanspa, T.; Mooss, A.N.; DelCore, M.G. Comparison of percutaneous device closure versus surgical closure of peri-membranous ventricular septal defects: A systematic review and meta-analysis. Catheter Cardiovasc Interv 2015, 86, 1048–56. [Google Scholar] [CrossRef] [PubMed]
- Yi, K.; You, T.; Ding, Z.H.; Hou, X.D.; Liu, X.G.; Wang, X.K.; Tian, J.H. Comparison of transcatheter closure, mini-invasive closure, and open-heart surgical repair for treatment of perimembranous ventricular septal defects in children: A PRISMA-compliant network meta-analysis of randomized and observational studies. Medicine (Baltimore) 2018, 97, e12583. [Google Scholar] [CrossRef]
- Ha, N.C.; Viet, N.L.; Nguyen, H.L.T.; Hien, N.S.; Hung, N.D. Early and mid-term outcomes of transcatheter closure of perimembranous ventricular septal defects using double-disc occluders. Front Cardiovasc Med 2025, 12, 1540595. [Google Scholar] [CrossRef]
- Ece, İ.; Bağrul, D.; Kavurt, A.V.; Terin, H.; Torun, G.; Koca, S.; Gül, A.E.K. Transcatheter Ventricular Septal Defect Closure with Lifetech™ Konar-MF Occluder in Infants Under 10 kg with Only Using Venous Access. Pediatr Cardiol 2024, 45, 175–183. [Google Scholar] [CrossRef]
- Fu, Y.C. Transcatheter device closure of muscular ventricular septal defect. Pediatr Neonatol 2011, 52, 3–4. [Google Scholar] [CrossRef]
- Haddad, R.N.; Rizk, C.; Saliba, Z.; Farah, J. Percutaneous closure of ventricular septal defects in children: key parameters affecting patient radiation exposure. Am J Cardiovasc Dis 2021, 11, 65–72. [Google Scholar]
- Knauth, A.L.; Lock, J.E.; Perry, S.B.; McElhinney, D.B.; Gauvreau, K.; Landzberg, M.J.; Rome, J.J.; Hellenbrand, W.E.; Ruiz, C.E.; Jenkins, K.J. Transcatheter device closure of congenital and postoperative residual ventricular septal defects. Circulation 2004, 110, 501–7. [Google Scholar] [CrossRef]
- Yang, P.; Wu, Z.; Liu, Z.; Zhang, J.; Zhou, H.; Ji, X.; Yi, Q.; Li, M. Unplanned Surgery After Transcatheter Closure of Ventricular Septal Defect in Children: Causes and Risk Factors. Front Pediatr 2021, 9, 772138. [Google Scholar] [CrossRef]
- Haddad, R.N.; Sawan, E.B.; Saliba, Z. Word of caution: Severe aortic valve injury linked to retrograde closure of perimembranous ventricular septal defects. J Card Surg 2022, 37, 1753–1758. [Google Scholar] [CrossRef]
- Butera, G.; Carminati, M.; Chessa, M.; Piazza, L.; Abella, R.; Negura, D.G.; Giamberti, A.; Claudio, B.; Micheletti, A.; Tammam, Y.; Frigiola, A. Percutaneous closure of ventricular septal defects in children aged <12: early and mid-term results. Eur Heart J 2006, 27, 2889–95. [Google Scholar] [CrossRef]
- Butera, G.; Carminati, M.; Chessa, M.; Piazza, L.; Micheletti, A.; Negura, D.G.; Abella, R.; Giamberti, A.; Frigiola, A. Transcatheter closure of perimembranous ventricular septal defects: early and long-term results. J Am Coll Cardiol 2007, 50, 1189–95. [Google Scholar] [CrossRef]
- Sullivan, I.D. Transcatheter closure of perimembranous ventricular septal defect: is the risk of heart block too high a price? Heart 2007, 93, 284–6. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Zhao, X.X.; Zheng, X.; Qin, Y.W. Arrhythmias after transcatheter closure of perimembranous ventricular septal defects with a modified double-disk occluder: early and long-term results. Heart Vessels 2012, 27, 405–10. [Google Scholar] [CrossRef]
- Weeraman, D.; Hilling-Smith, R.; Dooley, M.; Hildick-Smith, D. Transradial and transfemoral percutaneous closure of iatrogenic perimembranous Ventricular Septal Defects using the Amplatzer AVP IV device. Int J Cardiol 2016, 224, 65–68. [Google Scholar] [CrossRef] [PubMed]
- Samaras, A.; Papadopoulos, K.; Giannakoulas, G.; Tzikas, A. First-in-man transradial percutaneous closure of ventricular septal defect with an Amplatzer Duct Occluder IΙ in an adult patient: a case report. Eur Heart J Case Rep 2023, 7, ytad189. [Google Scholar] [CrossRef] [PubMed]
- Oses, P.; Hugues, N.; Dahdah, N.; Vobecky, S.J.; Miro, J.; Pellerin, M.; Poirier, N.C. Treatment of isolated ventricular septal defects in children: Amplatzer versus surgical closure. Ann Thorac Surg 2010, 90, 1593–8. [Google Scholar] [CrossRef]
- Tejada García, J.; Lara Lezama, L.B.; de la Fuente Blanco, R.; Pérez de Prado, A.; Benavente Fernández, L.; Rico Santos, M.; Fernández Couto, M.D.; Naya Ríos, L.; Couso Pazó, I.; Alba, P.V.; Redondo-Robles, L.; López Mesonero, L.; Arias-Rivas, S.; Santamaría Cadavid, M.; Tejada Meza, H.; Horna Cañete, L.; Azkune Calle, I.; Pinedo Brochado, A.; García Sánchez, J.M.; Caballero Romero, I.; Freijo Guerrero, M.M.; Luna Rodríguez, A.; de Lera-Alfonso, M.; Arenillas Lara, J.F.; Pérez Lázaro, C.; Navarro Pérez, M.P.; Martínez Zabaleta, M. Selection of patients for percutaneous closure in nonlacunar cryptogenic stroke associated with patent foramen ovale. Data from the NORDICTUS cooperative registry. Neurologia (Engl Ed) 2025, 40, 139–149. [Google Scholar] [CrossRef]
- Haddad, R.N. Transcatheter treatment of perimembranous ventricular septal defects: challenges, controversies, and a paradigm shift. Future Cardiol 2025, 21, 551–553. [Google Scholar] [CrossRef]
- Fishberger, S.B.; Bridges, N.D.; Keane, J.F.; Hanley, F.L.; Jonas, R.A.; Mayer, J.E.; Castaneda, A.R.; Lock, J.E. Intraoperative device closure of ventricular septal defects. Circulation 1993, 88(5 Pt 2), II205–9. [Google Scholar]
- Murzi, B.; Bonanomi, G.L.; Giusti, S.; Luisi, V.S.; Bernabei, M.; Carminati, M.; Vanini, V. Surgical closure of muscular ventricular septal defects using double umbrella devices (intraoperative VSD device closure). Eur J Cardiothorac Surg 1997, 12, 450–454, discussion 454. [Google Scholar] [CrossRef]
- Okubo, M.; Benson, L.N.; Nykanen, D.; Azakie, A.; Van Arsdell, G.; Coles, J.; Williams, W.G. Outcomes of intraoperative device closure of muscular ventricular septal defects. Ann Thorac Surg 2001, 72, 416–423. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, R.R.; Shore, D.F.; Yacoub, M.; Redington, A.N. Intraoperative apical ventricular septal defect closure using a modified Rashkind double umbrella. Heart 1996, 76, 367–9. [Google Scholar] [CrossRef]
- Amin, Z.; Berry, J.M.; Foker, J.E.; Rocchini, A.P.; Bass, J.L. Intraoperative closure of muscular ventricular septal defect in a canine model and application of the technique in a baby. J Thorac Cardiovasc Surg 1998, 115, 1374–6. [Google Scholar] [CrossRef] [PubMed]
- Phillips, A.B.; Green, J.; Bergdall, V.; Yu, J.; Monreal, G.; Gerhardt, M.; Cheatham, J.P.; Galantowicz, M.; Holzer, R.J. Teaching the "hybrid approach": a novel swine model of muscular ventricular septal defect. Pediatr Cardiol 2009, 30, 114–8. [Google Scholar] [CrossRef] [PubMed]
- Ratnayaka, K.; Saikus, C.E.; Faranesh, A.Z.; Bell, J.A.; Barbash, I.M.; Kocaturk, O.; Reyes, C.A.; Sonmez, M.; Schenke, W.H.; Wright, V.J.; Hansen, M.S.; Slack, M.C.; Lederman, R.J. Closed-chest transthoracic magnetic resonance imaging-guided ventricular septal defect closure in swine. JACC Cardiovasc Interv 2011, 4, 1326–34. [Google Scholar] [CrossRef]
- Saunders, A.B.; Carlson, J.A.; Nelson, D.A.; Gordon, S.G.; Miller, M.W. Hybrid technique for ventricular septal defect closure in a dog using an Amplatzer® Duct Occluder II. J Vet Cardiol 2013, 15, 217–24. [Google Scholar] [CrossRef]
- Bacha, E.A.; Marshall, A.C.; McElhinney, D.B.; del Nido, P.J. Expanding the hybrid concept in congenital heart surgery. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu 2007, 146–150. [Google Scholar] [CrossRef]
- Crossland, D.S.; Wilkinson, J.L.; Cochrane, A.D.; d'Udekem, Y.; Brizard, C.P.; Lane, G.K. Initial results of primary device closure of large muscular ventricular septal defects in early infancy using perventricular access. Catheter Cardiovasc Interv 2008, 72, 386–391. [Google Scholar] [CrossRef] [PubMed]
- Bacha, E.A.; Cao, Q.L.; Starr, J.P.; Waight, D.; Ebeid, M.R.; Hijazi, Z.M. Perventricular device closure of muscular ventricular septal defects on the beating heart: technique and results. J Thorac Cardiovasc Surg 2003, 126, 1718–23. [Google Scholar] [CrossRef] [PubMed]
- Xing, Q.; Pan, S.; An, Q.; Zhang, Z.; Li, J.; Li, F.; Wu, Q.; Zhuang, Z. Minimally invasive perventricular device closure of perimembranous ventricular septal defect without cardiopulmonary bypass: multicenter experience and mid-term follow-up. J Thorac Cardiovasc Surg 2010, 139, 1409–15. [Google Scholar] [CrossRef]
- Gan, C.; An, Q.; Lin, K.; Tang, H.; Lui, R.C.; Tao, K.; Pan, W.; Shi, Y. Perventricular device closure of ventricular septal defects: six months results in 30 young children. Ann Thorac Surg 2008, 86, 142–146. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, B.; Patel, N.; Shah, S.; Poptani, V.; Madan, T.; Shah, C.; Shukla, A.; Prajapati, V. Perventricular device closure of isolated muscular ventricular septal defect in infants: a single centre experience. Indian Heart J 2012, 64, 559–67. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Tanidir, I.C.; Ye, D.; Zhang, X.; Li, B.; Zhu, D.; Deng, G.; Chen, H. Hybrid Transthoracic Periventricular Device Closure of Ventricular Septal Defects: Single- Center Experience. Braz J Cardiovasc Surg 2021, 36, 48–56. [Google Scholar] [CrossRef]
- Huang, L.L.; Chen, M.; Zeng, C.; Su, C.X.; Jiang, C.L.; Zheng, B.S.; Wu, J.; Li, S.K. Comparison of perventricular and percutaneous ultrasound-guided device closure of perimembranous ventricular septal defects. Front Cardiovasc Med 2023, 10, 1281860. [Google Scholar] [CrossRef]
- Changwe, G.J.; Hongxin, L.; Zhang, H.Z.; Wenbin, G.; Liang, F.; Cao, X.X.; Chen, S.L. Percardiac closure of large apical ventricular septal defects in infants: Novel modifications and mid-term results. J Card Surg 2021, 36, 928–938. [Google Scholar] [CrossRef]
- Huang, X.S.; Luo, Z.R.; Chen, Q.; Yu, L.S.; Cao, H.; Chen, L.W.; Zhang, G.C. A Comparative Study of Perventricular and Percutaneous Device Closure Treatments for Isolated Ventricular Septal Defect: A Chinese Single-Institution Experience. Braz J Cardiovasc Surg 2019, 34, 344–351. [Google Scholar] [CrossRef]
- Haddad, R.N.; Gaudin, R.; Bonnet, D.; Malekzadeh-Milani, S. Hybrid perventricular muscular ventricular septal defect closure using the new multi-functional occluder. Cardiol Young 2020, 30, 1517–1520. [Google Scholar] [CrossRef]
- Cleuziou, J.; Georgiev, S.; Heinisch, P.P.; Ewert, P.; Hörer, J. Transventricular ventricular septal defect closure with device as hybrid procedure in complex congenital cardiac surgery. JTCVS Tech 2024, 26, 79–81. [Google Scholar] [CrossRef] [PubMed]
- Ueyama, H.A.; Leshnower, B.G.; Inci, E.K.; Keeling, W.B.; Tully, A.; Guyton, R.A.; Xie, J.X.; Gleason, P.T.; Byku, I.; Devireddy, C.M.; Hanzel, G.S.; Block, P.C.; Lederman, R.J.; Greenbaum, A.B.; Babaliaros, V.C. Hybrid Closure of Postinfarction Apical Ventricular Septal Defect Using Septal Occluder Device and Right Ventricular Free Wall: The Apical BASSINET Concept. Circ Cardiovasc Interv 2023, 16, e013243. [Google Scholar] [CrossRef] [PubMed]
- Adilbekova, A.; Marassulov, S.; Baigenzhin, A.; Kozhakhmetov, S.; Nurkeyev, B.; Kerimkulov, A.; Murzabayeva, S.; Maiorov, R.; Kenzhebayeva, A. Hybrid versus traditional method closure of ventricular septal defects in children. JTCVS Tech 2024, 24, 137–144. [Google Scholar] [CrossRef]
- Cantinotti, M.; Marchese, P.; Scalese, M.; Medino, P.; Jani, V.; Franchi, E.; Vitali, P.; Santoro, G.; Viacava, C.; Assanta, N.; Kutty, S.; Koestenberger, M.; Giordano, R. Left Ventricular Systolic Impairment after Pediatric Cardiac Surgery Assessed by STE Analysis. Healthcare (Basel) 2021, 9, 1338. [Google Scholar] [CrossRef]
- Faraji, E.; Bolin, E.H.; Bond, E.G.; Thomas Collins, R. 2nd.; Greiten L.; Daily J.A. Left Ventricular Dysfunction Following Repair of Ventricular Septal Defects in Infants. Pediatr Cardiol 2025, 46, 296–304. [Google Scholar] [CrossRef] [PubMed]
- Adamson, G.T.; Arunamata, A.; Tacy, T.A.; Silverman, N.H.; Ma, M.; Maskatia, S.A.; Punn, R. Postoperative Recovery of Left Ventricular Function following Repair of Large Ventricular Septal Defects in Infants. J Am Soc Echocardiogr 2020, 33, 368–377. [Google Scholar] [CrossRef]
- Safa, R.; Dean, A.; Sanil, Y.; Thomas, R.; Singh, G.; Charaf Eddine, A. Effect of Preoperative Volume Overload on Left Ventricular Function Recovery After Ventricular Septal Defect Repair. Am J Cardiol 2023, 203, 253–258. [Google Scholar] [CrossRef]
- Hassan, M.A.; Al-Akhfash, A.; Bhat, Y.; Alqwaiee, A.; Abdulrashed, M.; Almarshud, S.S.; Almesned, A. Myocardial deformation in children post cardiac surgery, a cross-sectional prospective study. Egypt Heart J 2024, 76, 151. [Google Scholar] [CrossRef]
- Lasheen, S.S.; Ahmed, M.K.; Elgayar, M.M. Assessment of Left Ventricular Systolic Function after Surgical and Transcatheter Device Closure of Ventricular Septal Defect Using Speckle Tracking Imaging. Menoufia Medical Journal 2023, 36, Article 11. [Google Scholar] [CrossRef]
- Shin, H.J.; Jhang, W.K.; Park, J.J.; Yu, J.J.; Kim, Y.H.; Ko, J.K.; Park, I.S.; Seo, D.M. Left ventricular function after left ventriculotomy for surgical treatment of multiple muscular ventricular septal defects. Ann Thorac Surg 2011, 92, 1490–3. [Google Scholar] [CrossRef]
- Zhu, D.; Tao, K.; An, Q.; Luo, S.; Gan, C.; Lin, K. Perventricular device closure of residual muscular ventricular septal defects after repair of complex congenital heart defects in pediatric patients. Tex Heart Inst J 2013, 40, 534–40. [Google Scholar]
- Mattei, A.; Strumia, A.; Benedetto, M.; Nenna, A.; Schiavoni, L.; Barbato, R.; Mastroianni, C.; Giacinto, O.; Lusini, M.; Chello, M.; Carassiti, M. Perioperative Right Ventricular Dysfunction and Abnormalities of the Tricuspid Valve Apparatus in Patients Undergoing Cardiac Surgery. J Clin Med 2023, 12, 7152. [Google Scholar] [CrossRef]
- Li, G.; Wang, Q.; Liu, Y.L.; Xu, Y.L.; Guo, Y. Surgical closure of apical multiple muscular septal defects via right ventriculotomy using a single patch with intermediate fixings. Chin Med J (Engl) 2013, 126, 2866–70. [Google Scholar] [PubMed]
- Frandsen, E.L.; Schauer, J.S.; Morray, B.H.; Mauchley, D.C.; McMullan, D.M.; Friedland-Little, J.M.; Kemna, M.S. Applying the Hybrid Concept as a Bridge to Transplantation in Infants Without Hypoplastic Left Heart Syndrome. Pediatr Cardiol 2024, 45, 323–330. [Google Scholar] [CrossRef]
- Lu, J.; Lian, X.; Wen, P.; Liu, Y. Case report: Recovery of long-term delayed complete atrioventricular block after minimally invasive transthoracic closure of ventricular septal defect. Front Cardiovasc Med 2023, 10, 1226139. [Google Scholar] [CrossRef]
- Heiberg, J.; Ringgaard, S.; Schmidt, M.R.; Redington, A.; Hjortdal, V.E. Structural and functional alterations of the right ventricle are common in adults operated for ventricular septal defect as toddlers. Eur Heart J Cardiovasc Imaging 2015, 16, 483–9. [Google Scholar] [CrossRef] [PubMed]
- Karimi, M.; Hulsebus, E.; Murdison, K.; Wiles, H. A case of hybrid closure of a muscular ventricular septal defect: anatomical complexity and surgical management. Cardiol Young 2012, 22, 356–9. [Google Scholar] [CrossRef] [PubMed]
- Bearl, D.W.; Fleming, G.A. Utilizing Hybrid Techniques to Maximize Clinical Outcomes in Congenital Heart Disease. Curr Cardiol Rep 2017, 19, 72. [Google Scholar] [CrossRef]
- Lu, W.; Zhang, F.; Fan, T.; Zhao, T.; Han, Y.; Hu, X.; Li, Q.; Shi, H.; Pan, X. Minimally-invasive-perventricular-device-occlusion versus surgical-closure for treating perimembranous-ventricular-septal-defect: 3-year outcomes of a multicenter randomized clinical trial. J Thorac Dis 2021, 13, 2106–2115. [Google Scholar] [CrossRef]
- Ng, L.Y.; Al-Alawi, K.; Breatnach, C.; Nolke, L.; Redmond, M.; McCrossan, B.; Oslizlok, P.; Walsh, K.P.; McGuinness, J.; Kenny, D. Hybrid Subxiphoid Perventricular Approach as an Alternative Access in Neonates and Small Children Undergoing Complex Congenital Heart Interventions. Pediatr Cardiol 2021, 42, 526–532. [Google Scholar] [CrossRef]
- Kulyabin, Y.Y.; Voitov, A.V.; Nichay, N.R.; Soynov, I.A.; Zubritskiy, A.V.; Bogachev-Prokophiev, A.V. Single-stage off-pump repair of coarctation of the aorta and ventricular septal defects in children. Interact Cardiovasc Thorac Surg 2022, 35, ivac186. [Google Scholar] [CrossRef]
- Pedra, C.A.; Pedra, S.R.; Chaccur, P.; Jatene, M.; Costa, R.N.; Hijazi, Z.M.; Amin, Z. Perventricular device closure of congenital muscular ventricular septal defects. Expert Rev Cardiovasc Ther 2010, 8, 663–74. [Google Scholar] [CrossRef]
- Voitov, A.; Omelchenko, A.; Gorbatykh, Y.; Zaitsev, G.; Arkhipov, A.; Soynov, I.; Bogachev-Prokophiev, A.; Karaskov, A. Outcomes of perventricular off-pump versus conventional closure of ventricular septal defects: a prospective randomized study. Eur J Cardiothorac Surg 2017, 51, 980–986. [Google Scholar] [CrossRef] [PubMed]
- Dodge-Khatami, J.; Dodge-Khatami, A.; Nguyen, T.D.; Rüffer, A. Minimal invasive approaches for pediatric & congenital heart surgery: safe, reproducible, more cosmetic than through sternotomy, and here to stay. Transl Pediatr 2023, 12, 1744–1752. [Google Scholar] [CrossRef]
- Xing, Q.; Wu, Q.; Shi, L.; Xing, Y.; Yu, G. Minimally invasive transthoracic device closure of isolated ventricular septal defects without cardiopulmonary bypass: long-term follow-up results. J Thorac Cardiovasc Surg 2015, 149, 257–64. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.J.; Sun, S.Q.; Chen, X.F.; Ma, X.J.; Luo, Y.H.; Lim, Y.P.; Tao, L. Device closure of perimembranous ventricular septal defects with a minimally invasive technique in 12 patients. Ann Thorac Surg 2008, 85, 192–4. [Google Scholar] [CrossRef] [PubMed]
- Tanidir, I.C.; Baspinar, O.; Saygi, M.; Kervancioglu, M.; Guzeltas, A.; Odemis, E. Use of Lifetech™ Konar-MF, a device for both perimembranous and muscular ventricular septal defects: A multicentre study. Int J Cardiol 2020, 310, 43–50. [Google Scholar] [CrossRef]
- Haddad, R.N.; Saliba, Z.S. Comparative outcomes of two competitive devices for retrograde closure of perimembranous ventricular septal defects. Front Cardiovasc Med 2023, 10, 1215397. [Google Scholar] [CrossRef]
- Laha, S.; Gangopadhyay, D.; Roy, M.; Singh, A.; Nandi, D.; Dutta, J. Procedural outcomes of percutaneous closure of perimembranous and other ventricular septal defects using Konar-MF occluder and short-term follow-up. Ann Pediatr Cardiol 2024, 17, 101–108. [Google Scholar] [CrossRef]
- Kabadayı, B.; Eren, Z.B.; Odemis, E. Efficacy and Safety of the LifeTech™ Multifunctional Occluder (Konar-MFO) in Transcatheter Closure of Ventricular Septal Defects: A Systematic Review and Meta-Analysis. Catheter Cardiovasc Interv 2025. [CrossRef]
- Omelchenko, A.; Gorbatykh, Y.; Voitov, A.; Zaitsev, G.; Bogachev-Prokophiev, A.; Karaskov, A. Perventricular device closure of ventricular septal defects: results in patients less than 1 year of age. Interact Cardiovasc Thorac Surg 2016, 22, 53–6. [Google Scholar] [CrossRef]
- Fujii, T.; Higaki, T.; Tomita, H.; Nagaoka, K.; Yamaguchi, H.; Shimizu, T.; Oyama, N.; Sasaki, T.; Asada, D.; Hata, Y.; Tarui, S.; Miyahara, Y.; Ishino, K.; Soga, T.; Ota, M. Transcatheter closure of perimembranous ventricular septal defects with Amplatzer® duct occluder I; The first case report in Japan. J Cardiol Cases 2019, 20, 147–150. [Google Scholar] [CrossRef]
- Haddad, R.N.; Daou, L.; Saliba, Z. Device Closure of Perimembranous Ventricular Septal Defect: Choosing Between Amplatzer Occluders. Front Pediatr 2019, 7, 300. [Google Scholar] [CrossRef]
- Ghosh, B.; Sahai, I.; Agrawal, G.; Khadase, S.; Rao, T.; Lohakare, A.; Chaturvedi, A.; Gomase, S. Experience of Percutaneous Closure of Ventricular Septal Defects in 140 Patients With Different Duct Occluders in a Tertiary Care Rural Hospital in Central India. Cureus 2023, 15, e42591. [Google Scholar] [CrossRef]
- Shyu, T.C.; Lin, M.C.; Quek, Y.W.; Lin, S.J.; Saw, H.P.; Jan, S.L.; Fu, Y.C. Initial experience of transcatheter closure of subarterial VSD with the Amplatzer duct occluder. J Chin Med Assoc 2017, 80, 487–491. [Google Scholar] [CrossRef] [PubMed]
- Piccinelli, E.; Bautista-Rodriguez, C.; Fraisse, A. Transcatheter closure of large perimembranous ventricular septal defects with inlet to outlet extension with the Amplatzer Vascular Plug-II. Cardiol Young 2023, 33, 1018–1022. [Google Scholar] [CrossRef] [PubMed]
- Mijangos-Vázquez, R.; Hernández-Reyes, R. Closure of perimembranous ventricular septal defects using the Amplatzer vascular plug II: experience of a Mexican centre. Cardiol Young 2025, 35, 683–687. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H.L.; Phan, Q.T.; Dinh, L.H.; Tran, H.B.; Won, H.; Thottian, J.J.; Duc, D.D.; Quang, T.N.; Kim, S.W. Nit-Occlud Lê VSD coil versus Duct Occluders for percutaneous perimembranous ventricular septal defect closure. Congenit Heart Dis 2018, 13, 584–593. [Google Scholar] [CrossRef] [PubMed]
- Ghaderian, M.; Shahsanaei, F.; Behdad, S.; Mozafari, S. Long-term Consequences of Ventricular Septal Defect Closure Using Nit-Occlud Le VSD Coil Device: A Systematic Review and Meta-Analysis. Heart Views 2022, 23, 93–99. [Google Scholar] [CrossRef]
- Bichali, S.; Houeijeh, A.; Godart, F. Late complete atrioventricular block after transcatheter perimembranous ventricular septal defect closure with the KONAR-MF™ VSD occluder: a case report and systematic review. Cardiol Young 2024, 34, 2480–2483. [Google Scholar] [CrossRef]
- Yildiz, K.; Narin, N.; Oksuz, S.; Ozdemir, R.; Pamukcu, O.; Baykan, A.; Ozyurt, A.; Bagli, S.; Aktas, R.; Safak, I.N.; Atlan, M.A.; Bayam, Y.S.; Karadeniz, C. Safety and efficacy of Amplatzer duct occluder II and konar-MF™ VSD occluder in the closure of perimembranous ventricular septal defects in children weighing less than 10 kg. Front Cardiovasc Med 2023, 10, 1255808. [Google Scholar] [CrossRef]
- Singhi, A.K.; Mohapatra, S.K.; De, A. Transcatheter closure of perimembranous ventricular septal defect using the cocoon membranous VSD occluder. Prog Pediatr Cardiol 2024, 74, 101744. [Google Scholar] [CrossRef]
- Park, H.; Song, J.; Kim, E.S.; Huh, J.; Kang, I.S. Early Experiences Using Cocoon Occluders for Closure of a Ventricular Septal Defect. J Cardiovasc Imaging 2018, 26, 165–174. [Google Scholar] [CrossRef] [PubMed]
- Kouakou, N.Y.N.; Song, J.; Huh, J.; Kang, I.S. The experience of transcatheter closure of postoperative ventricular septal defect after total correction. J Cardiothorac Surg 2019, 14, 104. [Google Scholar] [CrossRef] [PubMed]
- Kaya, M.G.; Akpek, M.; Celebi, A.; Saritas, T.; Meric, M.; Soylu, K.; Karapinar, H.; Lam, Y.Y. A multicentre, comparative study of Cera septal occluder versus AMPLATZER Septal Occluder in transcatheter closure of secundum atrial septal defects. EuroIntervention 2014, 10, 626–31. [Google Scholar] [CrossRef]
- Apostolopoulou, S.C.; Tsoutsinos, A.; Laskari, C.; Kiaffas, M.; Rammos, S. Large single centre experience with the Cera™ and CeraFlex™ occluders for closure of interatrial communications: usefulness of the flexible rotation feature. Cardiovasc Interv Ther 2018, 33, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Epçaçan, S.; Bulut, M.O.; Yücel, İ.K.; Ceviz, N.; Çelebi, A. Preliminary results of the CeraflexTM PDA occluder and device behaviour during releasing. Cardiology in the Young 2019, 29, 519–523. [Google Scholar] [CrossRef]
- Gupta, A.; Amin, Z. Popular Hybrid Congenital Heart Procedures without Cardiopulmonary Bypass. Front Surg 2017, 4, 9. [Google Scholar] [CrossRef]
- Kang, S.-L.; Benson, L. Interventions in Congenital Heart Disease: A Review of Recent Developments: Part II. Structural Heart 2021, 5, 570–581. [Google Scholar] [CrossRef]
- Hong, Z.N.; Chen, Q.; Huang, L.Q.; Cao, H. A meta-analysis of perventricular device closure of perimembranous ventricular septal defect. J Cardiothorac Surg 2019, 14, 119. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.S.; Harris, A.D. Recent advances in managing septal defects: ventricular septal defects and atrioventricular septal defects. F1000Res 2018, 7, F1000 Faculty Rev–498. [Google Scholar] [CrossRef] [PubMed]
- Kozlik-Feldmann, R.; Lorber, A.; Sievert, H.; Ewert, P.; Jux, C.; Müller, G.C.; Dalla Pozza, R.; Yigitbasi, M.; Schranz, D.; Lindinger, A.; Galal, O.; Meinertz, T. Long-term outcome of perimembranous VSD closure using the Nit-Occlud® Lê VSD coil system. Clin Res Cardiol 2021, 110, 382–390. [Google Scholar] [CrossRef]
- Morse, A.K.; Dobrila, J.; LaPar, D.J.; Salazar, J.D. Occluder Device Removal and Total Septation of "Swiss-Cheese" Ventricular Septal Defects. Ann Thorac Surg Short Rep 2024, 2, 829–831. [Google Scholar] [CrossRef]
- Singab, H.; Elshahat, M.K.; Taha, A.S.; Ali, Y.A.; El-Emam, A.M.; Gamal, M.A. Transcatheter versus surgical closure of ventricular septal defect: a comparative study. Cardiothorac Surg 2023, 31, 8. [Google Scholar] [CrossRef]
- Zhao, L.J.; Han, B.; Zhang, J.J.; Yi, Y.C.; Jiang, D.D.; Lyu, J.L. Postprocedural Outcomes and Risk Factors for Arrhythmias Following Transcatheter Closure of Congenital Perimembranous Ventricular Septal Defect: A Single-center Retrospective Study. Chin Med J (Engl) 2017, 130, 516–521. [Google Scholar] [CrossRef]
- Sudaka, A.; Thambo, J.B.; Vaksmann, G.; Hadeed, K.; Houeijeh, A.; Khraiche, D.; Hery, E.; Vincenti, M.; Pangaud, N.; Benbrik, N.; Vastel, C.; Legendre, A.; Jalal, Z.; Laux, D.; Harchaoui, S.; Lambert, V.; Chalard, A.; Douchin, S.; Bouzguenda, I.; Denis, C.; Urbina-Hiel, B.; Bonnemains, L.; Mostefa-Kara, M.; Ansquer, H.; Léty, S.; Leborgne, A.S.; Cohen, L.; Lupoglazoff, J.M.; Guirgis, M.; Maragnes, P.; Moceri, P.; Bertail, C.; Lefort, B.; Ovaert, C.; Haddad, R.N.; Guirgis, L. ; Hascoet S; FRANCISCO investigators. Anatomical insights and management strategies for haemodynamically significant pressure-restrictive perimembranous ventricular septal defects: Findings from the French nationwide FRANCISCO cohort. Arch Cardiovasc Dis 2025, 118(6-7), 391-399. [CrossRef]
- Zampi, J.D.; Sower, C.T.; Lancaster, T.S.; Sood, V.; Romano, J.C. Hybrid Interventions in Congenital Heart Disease: A Review of Current Practice and Rationale for Use. Ann Thorac Surg 2024, 118, 329–337. [Google Scholar] [CrossRef]
- Li, D.; Zhou, X.; Li, M.; An, Q. Comparisons of perventricular device closure, conventional surgical repair, and transcatheter device closure in patients with perimembranous ventricular septal defects: a network meta-analysis. BMC Surg 2020, 20, 115. [Google Scholar] [CrossRef]
- Aboulhosn, J.; Levi, D.; Sopher, M.; Johnson, A.; Child, J.S.; Laks, H. Perventricular closure of a large ventricular septal defect in congenitally corrected transposition of the great arteries. Congenit Heart Dis 2010, 5, 60–5. [Google Scholar] [CrossRef]
- Prifti, E.; Baboci, A.; Dado, E.; Kajo, E. Perventricular device closure of a large residual perimembranous interventricular septal defect after previous surgical correction. J Cardiothorac Surg 2014, 9, 12. [Google Scholar] [CrossRef] [PubMed]
- Soquet, J.; Houeijeh, A.; Richardson, M.; Hebbar, E.; Vaksmann, G.; Baudelet, J.B.; Moussa, M.D.; Vincentelli, A. Hybrid closure of ventricular septal defect and implantation of systemic right ventricular assist device. ESC Heart Fail 2022, 9, 3636–3638. [Google Scholar] [CrossRef]
- Wang, S.; Zhuang, Z.; Zhang, H.; Zhen, J.; Lu, Y.; Liu, J.; Xu, Z. Perventricular closure of perimembranous ventricular septal defects using the concentric occluder device. Pediatr Cardiol 2014, 35, 580–6. [Google Scholar] [CrossRef]
- Wang, L.; Xie, L.; Ruan, W.; Li, T.; Gan, C.; Lin, K. Percutaneous-perventricular device closure of ventricular septal defect: mid-term follow-up. BMC Surg 2020, 20, 208. [Google Scholar] [CrossRef]
- Omelchenko, A.Y.; Zaitsev, G.S.; Gorbatykh, Y.N.; Khapaev, T.S.; Malakhova, O.Y.; Arkhipov, A.N.; Karaskov, A.M. Perventricular device closure of ventricular septal defect using a video-assisted thoracoscopic approach. Ann Thorac Surg 2014, 98, 350–2. [Google Scholar] [CrossRef]
- Salavitabar, A.; Armstrong, A.K.; Carrillo, S.A. Hybrid Interventions in Congenital Heart Disease. Interv Cardiol Clin 2024, 13, 399–408. [Google Scholar] [CrossRef] [PubMed]
- Frogoudaki, A.A. Congenital heart disease prevalence: what does the future hold? Eur J Prev Cardiol 2023, 30, 167–168. [Google Scholar] [CrossRef] [PubMed]
- Benziger, C.P.; Stout, K.; Zaragoza-Macias, E.; Bertozzi-Villa, A.; Flaxman, A.D. Projected growth of the adult congenital heart disease population in the United States to 2050: an integrative systems modeling approach. Popul Health Metr 2015, 13, 29. [Google Scholar] [CrossRef]
- Araujo, J.J.; Rodríguez-Monserrate, C.P.; Elizari, A.; Yáñez-Gutiérrez, L.; Mouratian, M.; Amaral, F.; Huertas-Quiñonez, M.; Rosario, M.; O'Connell, M.; Aguirre-Zurita, O.N.; Fernández, C.; Callau-Briceño, M.; Lorente-Coppola, M.M.; Garay, N. Position statement for the development of adult congenital heart disease units in Latin America and the Caribbean: Recommendations by the adult congenital heart disease chapter and pediatric cardiology council of the interamerican society of cardiology …. Int J Cardiol Congenit Heart Dis 2023, 13:100461. [CrossRef]
- Kadiyani, L.; Kalaivani, M.; Iyer, K.S.; Ramakrishnan, S. The outcome of surgery for congenital heart disease in India: A systematic review and metanalysis. Ann Pediatr Cardiol 2024, 17, 164–179. [Google Scholar] [CrossRef]
Figure 1.
Short-axis view of ventricular septal defect by transesophageal echocardiography (TEE). The arrow points to the ventricular septal defect and shows its approximate size.
Figure 1.
Short-axis view of ventricular septal defect by transesophageal echocardiography (TEE). The arrow points to the ventricular septal defect and shows its approximate size.
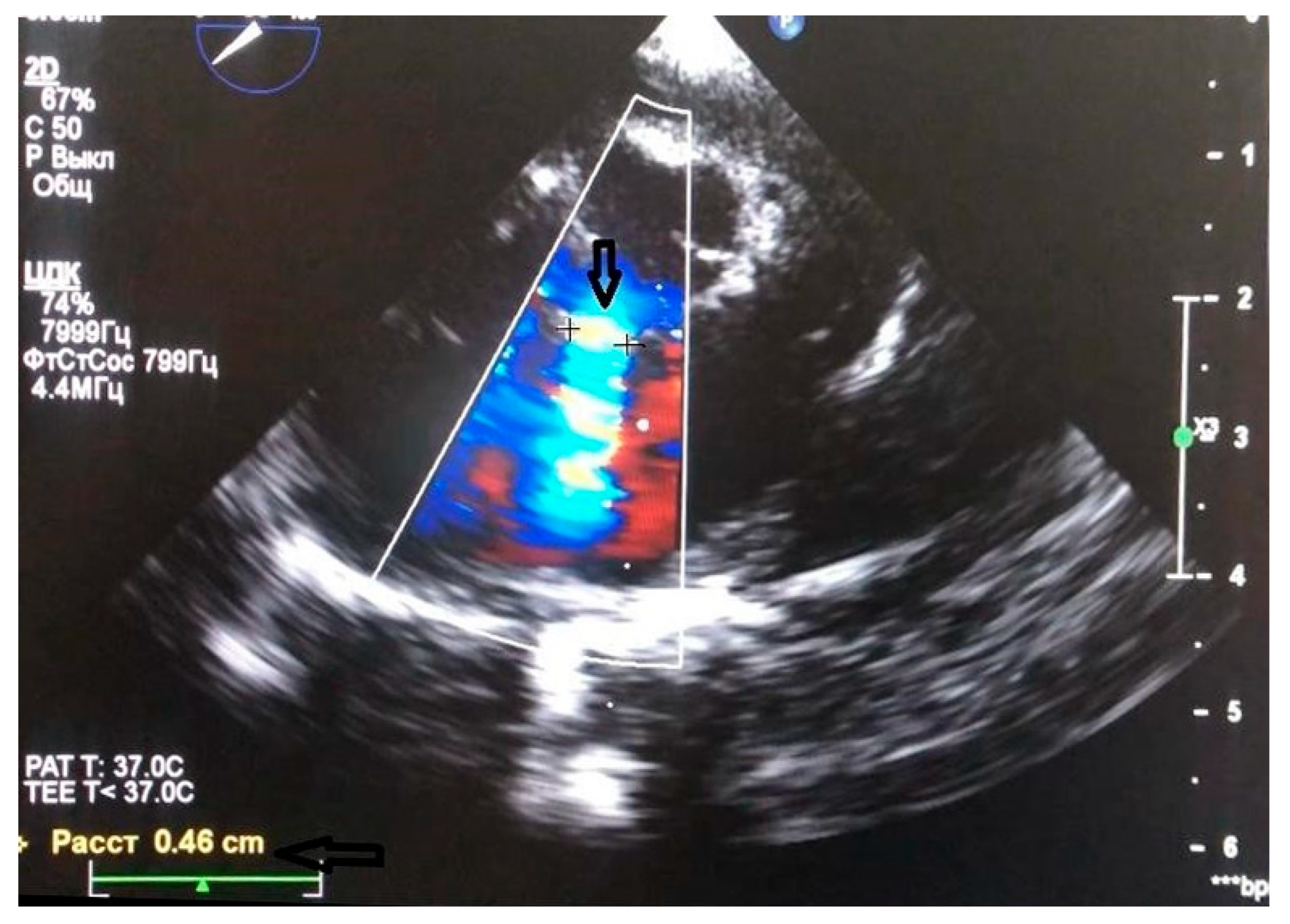
Figure 2.
Typical surgical wound size in the hybrid method.
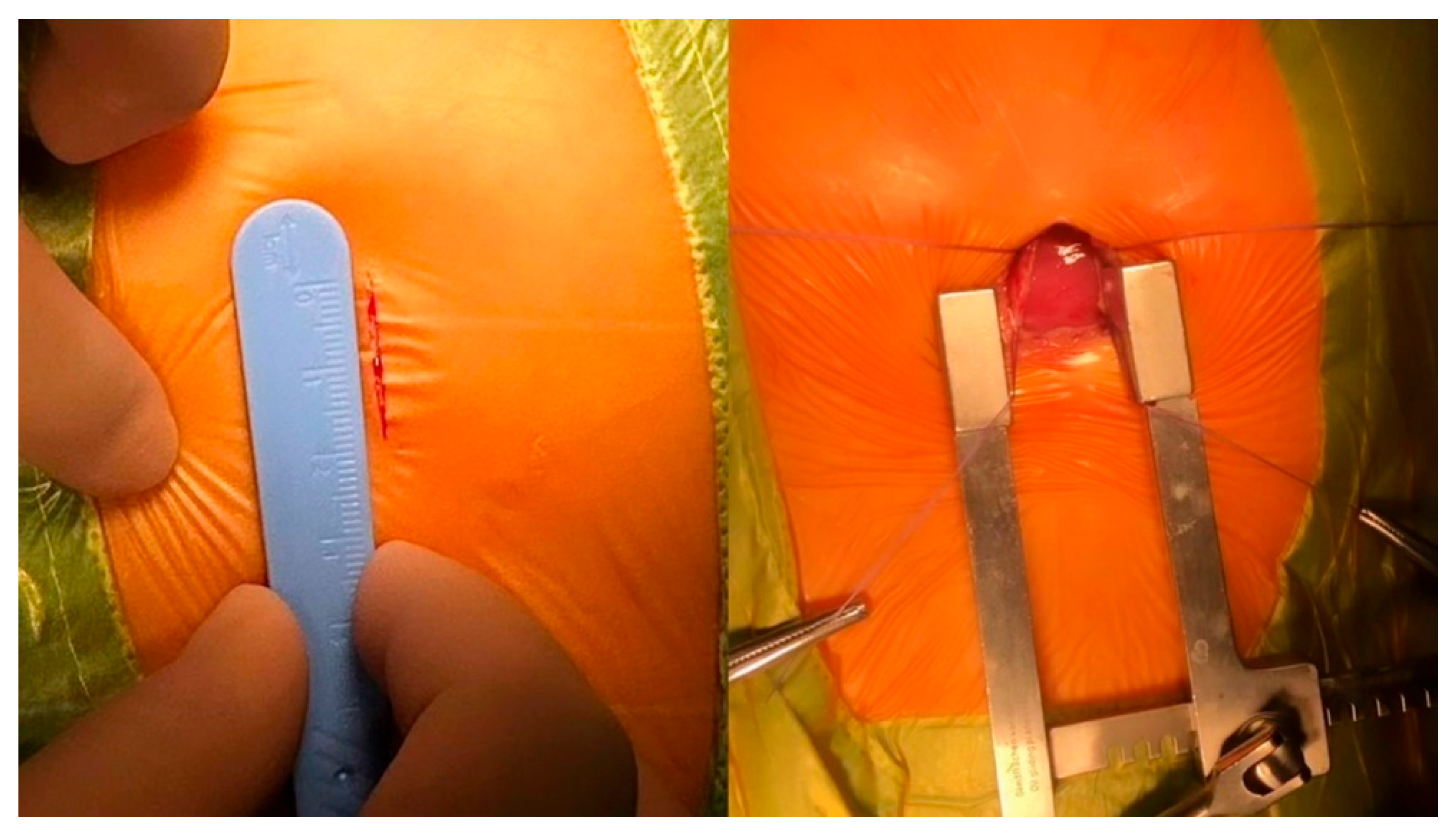
Figure 3.
Methods for determining the right location for right ventricular puncture. (A) Using the right index finger, the operator identifies the approximate puncture site under transesophageal echocardiographic (TEE) guidance. (B) With the left hand, the surgeon uses forceps to stabilize the right ventricular myocardium; with the right hand, forceps are used to identify the optimal puncture site and direction.
Figure 3.
Methods for determining the right location for right ventricular puncture. (A) Using the right index finger, the operator identifies the approximate puncture site under transesophageal echocardiographic (TEE) guidance. (B) With the left hand, the surgeon uses forceps to stabilize the right ventricular myocardium; with the right hand, forceps are used to identify the optimal puncture site and direction.
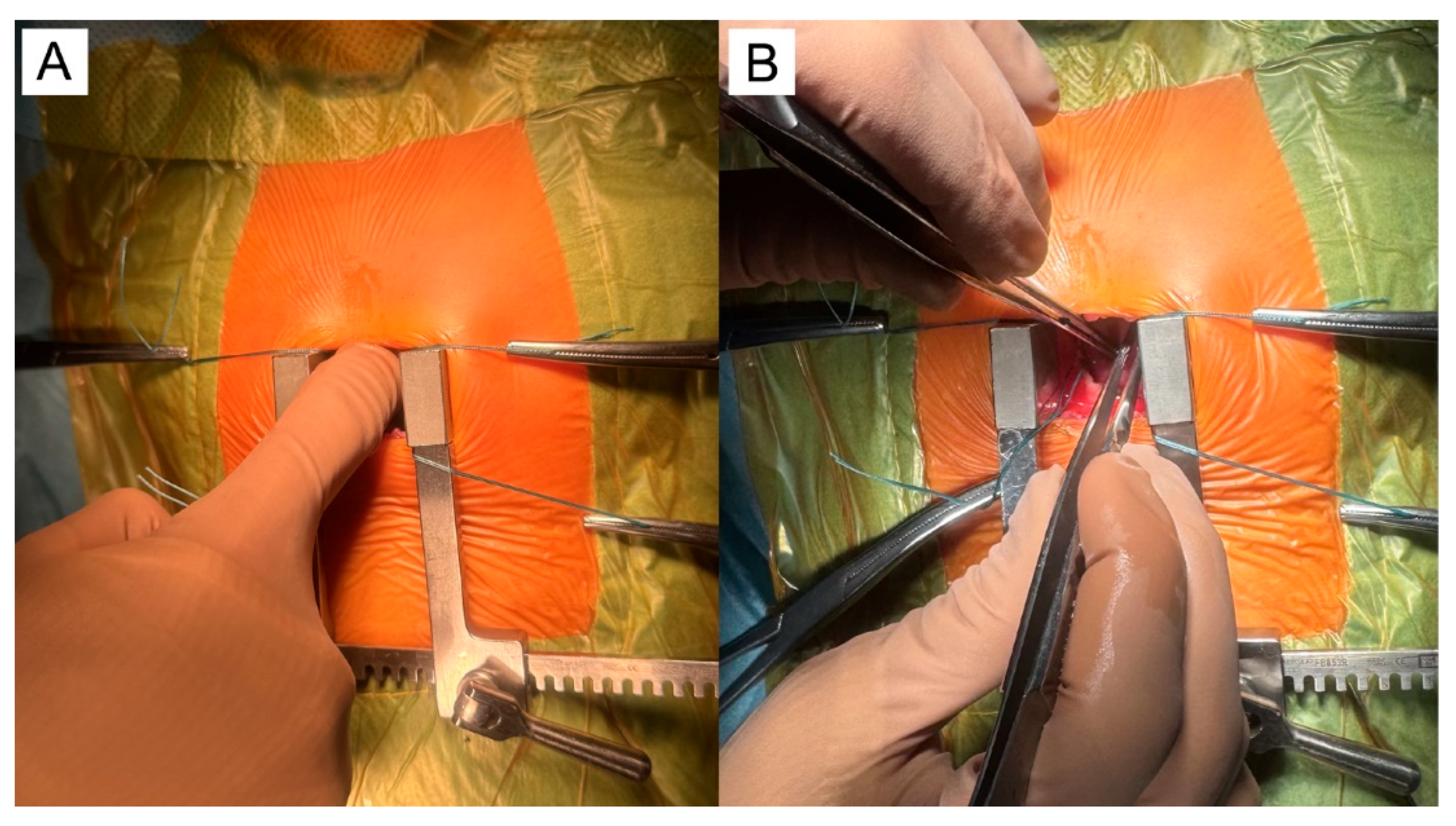
Figure 4.
Installation of a guidewire and dilator. (A) The surgeon advances the dilator with stylet over the guidewire, passing it through the anterior wall of the right ventricle (RV) and across the ventricular septal defect (VSD), while the assistant holds the myocardium near the purse-string suture to stabilize the area. (B) As soon as the dilator advances over the guidewire into the left ventricular (LV) cavity, the surgeon releases the myocardium and removes the stylet along with the guidewire, while the assistant maintains the same position.
Figure 4.
Installation of a guidewire and dilator. (A) The surgeon advances the dilator with stylet over the guidewire, passing it through the anterior wall of the right ventricle (RV) and across the ventricular septal defect (VSD), while the assistant holds the myocardium near the purse-string suture to stabilize the area. (B) As soon as the dilator advances over the guidewire into the left ventricular (LV) cavity, the surgeon releases the myocardium and removes the stylet along with the guidewire, while the assistant maintains the same position.

Figure 5.
The delivery system is connected to the loader (A-B), then the occluder is opened (C), and then the pusher is disconnected (D).
Figure 5.
The delivery system is connected to the loader (A-B), then the occluder is opened (C), and then the pusher is disconnected (D).
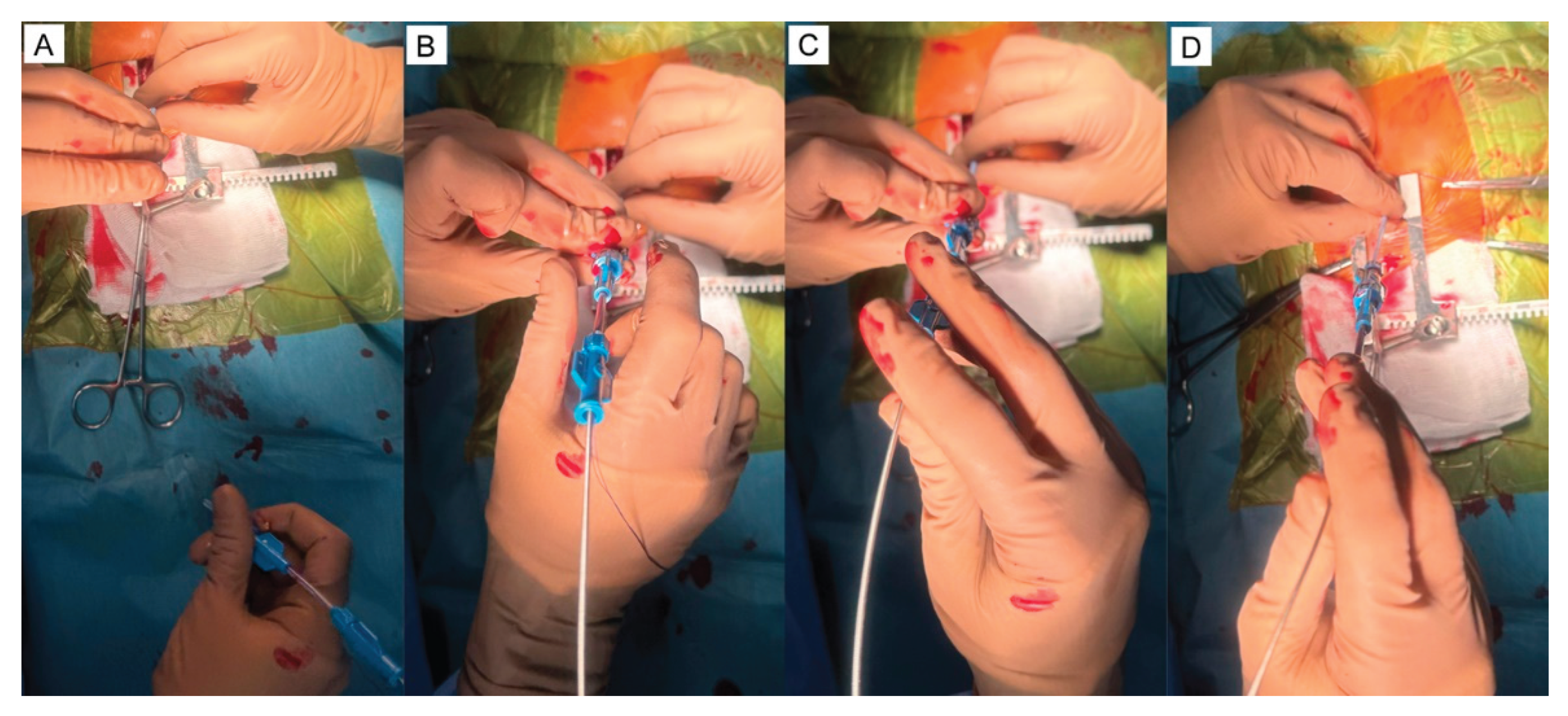
Figure 6.
Muscular occluder installed (B-long-axis view). The arrow shows the opening of the left and right occluder discs.
Figure 6.
Muscular occluder installed (B-long-axis view). The arrow shows the opening of the left and right occluder discs.
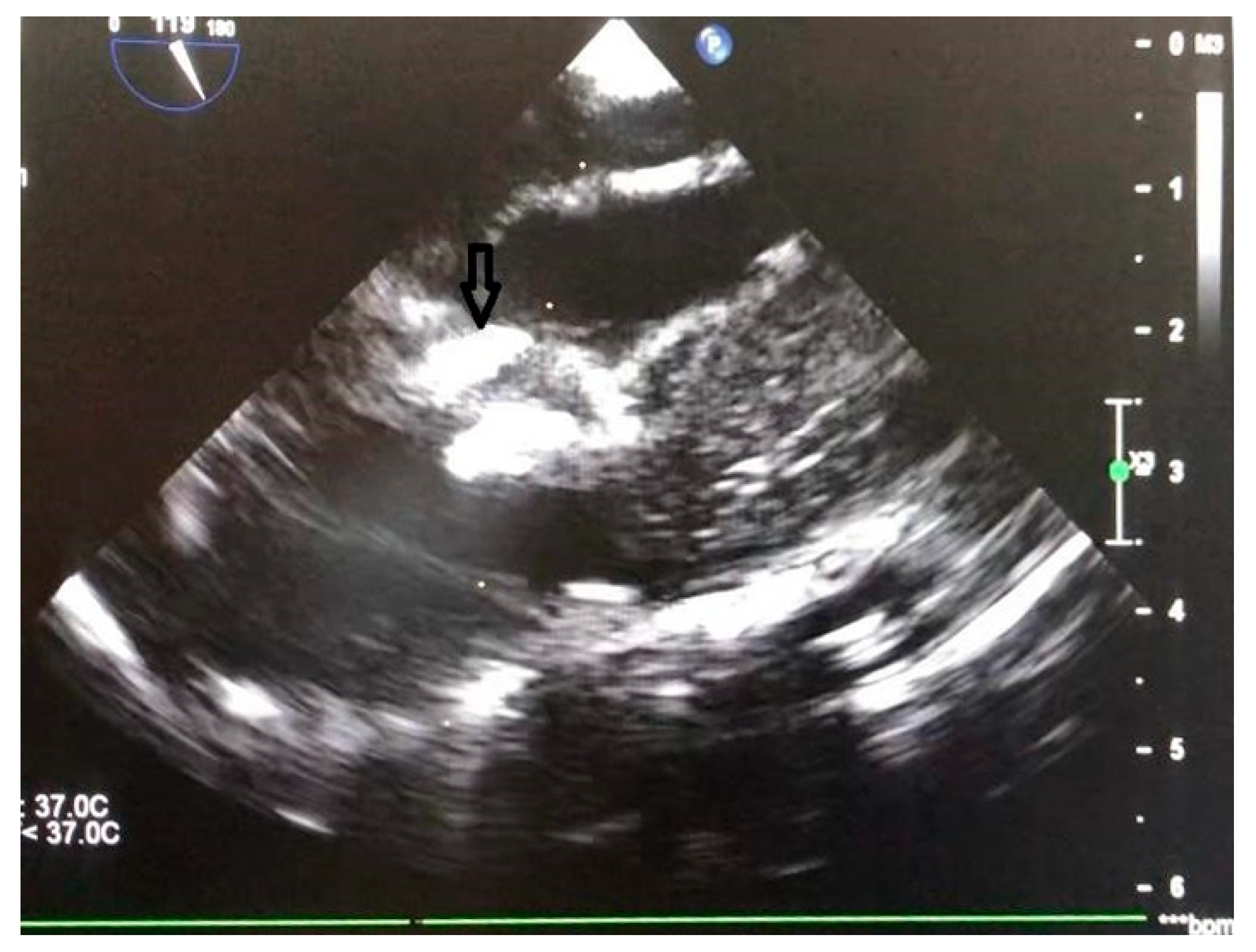
Figure 7.
Tying a purse-string suture (A), then removing the safety thread (B), and then draining and preparing the wound for suturing (C,D).
Figure 7.
Tying a purse-string suture (A), then removing the safety thread (B), and then draining and preparing the wound for suturing (C,D).
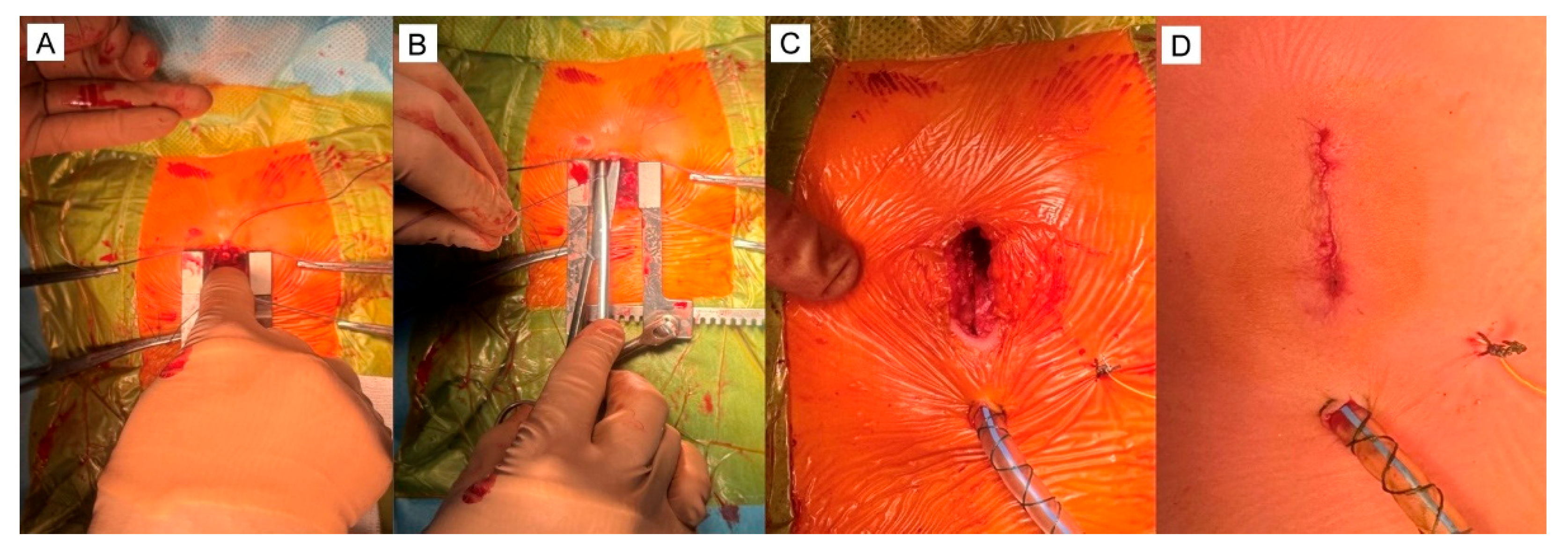
Figure 8.
Delivery system: a – trocar, b – guidewire, c – delivery sheath and dilator, d – loading sheath with a muscular occluder.
Figure 8.
Delivery system: a – trocar, b – guidewire, c – delivery sheath and dilator, d – loading sheath with a muscular occluder.
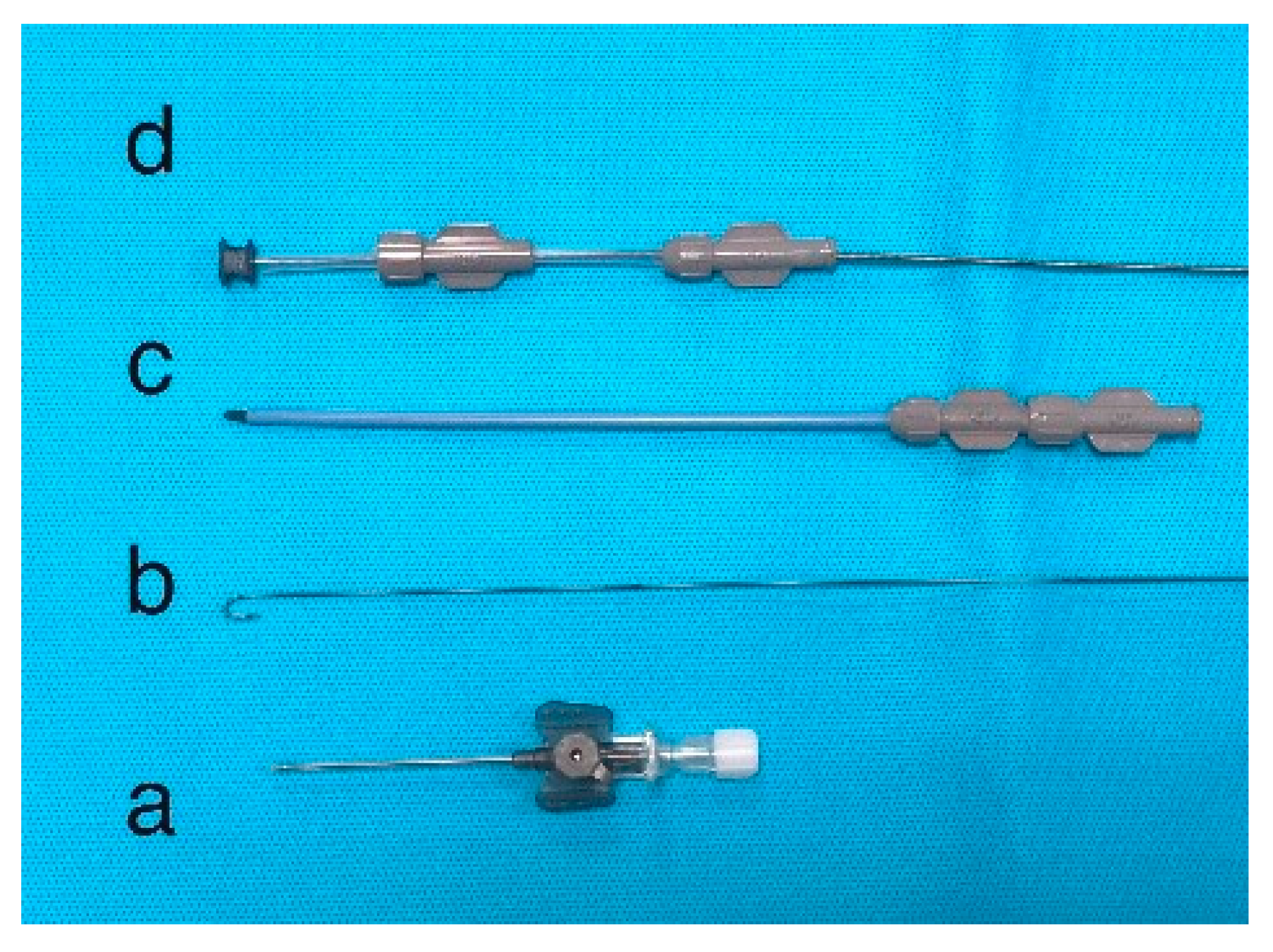
Figure 9.
Types of occluders used for VSD closure (Cera Occluders, LifeTech Scientific Co). (A) Muscular occluder. (B) Symmetric occluder. (C) Asymmetric occluder. (D) Eccentric occlude. (Adapted with permission from [260]).
Figure 9.
Types of occluders used for VSD closure (Cera Occluders, LifeTech Scientific Co). (A) Muscular occluder. (B) Symmetric occluder. (C) Asymmetric occluder. (D) Eccentric occlude. (Adapted with permission from [260]).
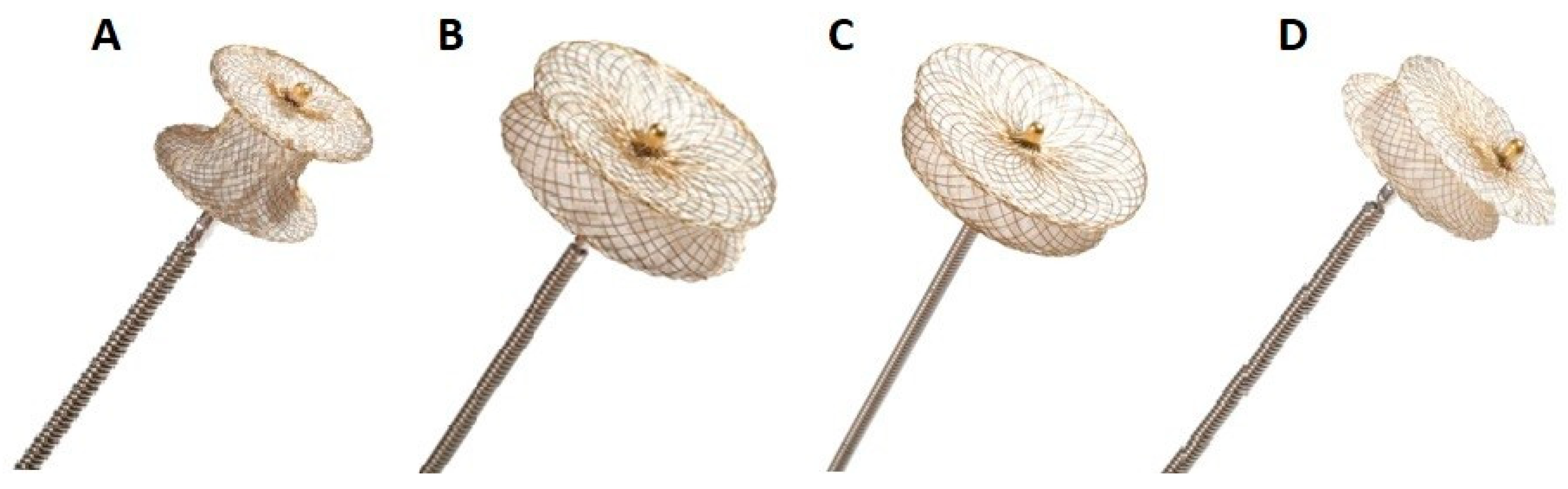
Figure 10.
Types of occluders and delivery system components. (A) Eccentric (asymmetric, a) and muscular (symmetric, b) occluders. (B) The identical delivery systems with attached asymmetric (top, a) or symmetric (bottom, b) occluder.
Figure 10.
Types of occluders and delivery system components. (A) Eccentric (asymmetric, a) and muscular (symmetric, b) occluders. (B) The identical delivery systems with attached asymmetric (top, a) or symmetric (bottom, b) occluder.
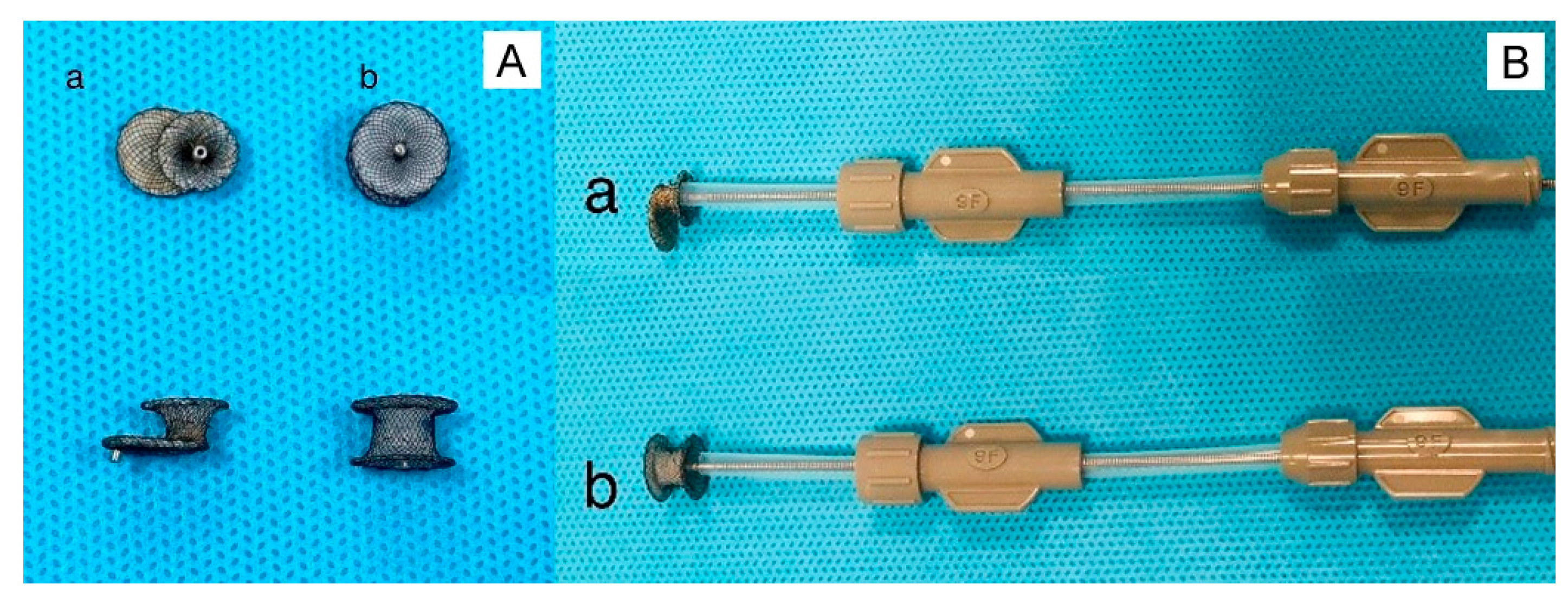

Table 1.
VSD Types: Prevalence, Spontaneous Closure, and Clinical Considerations.
| VSD Type | Prevalence | Spontaneous Closure | SurgicalIndication | Associated Risks |
|---|---|---|---|---|
| Perimembranous | 70–80% | Moderate | Common | Aortic regurgitation, heart block |
| Muscular | 5–20% | High | Rare (unless multiple) | Residual defects, arrhythmias |
| Inlet | 5–8% | Low | Common | AV valve involvement |
| Outlet | 5–7% | Low | Common | Aortic valve prolapse, regurgitation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



