Submitted:
21 July 2025
Posted:
22 July 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background/Objectives: Although COVID-19 may cause cognitive impairments for up to six months, the long-term effects of mild cases remain unclear. Given their high exposure and critical role in public health, assessing this impact on healthcare workers is essential. Aim: This study examined the cognitive and emotional effects of mild COVID-19 in 92 healthcare workers one year after infection. Methods: Fifty had experienced mild COVID-19, while 42 had not been infected. Participants completed a neuropsychological assessment evaluating attention, memory, and executive functions, along with self-reported measures of anxiety, depression, post-traumatic stress, occupational stress, and burnout. Results: No significant cognitive differences were observed between groups. However, both exhibited moderate to severe psychological distress, with the COVID-19 group showing higher trait anxiety. Emotional symptoms were significantly associated with neuropsychological performance: higher burnout and stress correlated with more errors and slower responses on tasks such as the D2 variance index, TESEN, Rey-Osterrieth Figure, and Digit Span. Conclusions: These findings suggest no long-term cognitive impairment after mild COVID-19 but highlight the substantial emotional toll of the pandemic on healthcare workers. Future research should explore cognitive reserve as a protective factor.
Keywords:
mild COVID-19
; healthcare
; cognition
; neuropsychology
; long-term effects
1. Introduction
In the fourth year of the pandemic, substantial evidence underscores that the Coronavirus Disease 2019 (COVID-19) is a systemic illness frequently affecting the central nervous system. As of November 2024, data from World Health Organization confirmed 776,546,006 reported infections globally, including approximately 14 million cases in Spain [1]. The global investigation of this virus is unprecedented, with numerous emerging medical studies describing symptom profiles and treatment outcomes in COVID-19. Despite the extensive literature on COVID-19 and its effects on the brain, the long-term cognitive impact of the virus remains poorly understood. Addressing these issues is particularly critical for healthcare workers, who represent a population heavily exposed to the virus.
The virus responsible for COVID-19 is severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), a member of the Coronavirus (CoVs) family [2]. Common symptoms include fever, cough, headache, myalgia, respiratory and gastrointestinal issues, as well as metabolic and immune disturbances [3,4]. Neurological symptoms have also been described, including taste and smell dysfunction, encephalopathy, myelitis, seizures, ischemic stroke, and impaired consciousness [3]. The association between respiratory viral infections and neurological symptoms is not yet fully understood, and various hypotheses have been proposed [5]. The most widely accepted causes include cerebrovascular factors (ischemic strokes, intracranial hemorrhage, and cerebral microbleeds), neuroinflammation, dysregulation of the immune response, and direct viral invasion of the brain via the olfactory bulb [3,4,6]. Given its connections with the rest of the central nervous system, entry through the olfactory bulb could explain some neurological and cognitive symptoms [5,6].
Previous studies have signaled that individuals with acute SARS-CoV-2 infection frequently complain about cognitive issues, often described as `brain fog’ [7]. The most frequently observed symptoms include low energy, disorientation, attentional deficits, impairments in learning and memory retrieval, and executive dysfunction [3,4,8,9]. The prevalence and duration of self-reported cognitive symptoms post-COVID-19 are well-documented, although estimates vary significantly between studies [5]. Research indicates that these symptoms are relatively common, affecting 20–36% of individuals within the first three months post-infection, with attention and memory being the most affected domains [10]. In this vein, data derived from a large body of studies suggest that the short- and medium-term cognitive effects are relatively clear, with general cognitive decline observed up to six months post-infection [11,12]. Longitudinal studies have extended previous findings showing that working memory deficits, among other cognitive alterations, are noticeable in COVID-19 patients even one year after infection [13,14].
A key point to mention is that most of the studies included patients with acute COVID-19 who had been previously hospitalized or were still hospitalized during the evaluation period [5,7]. Cognitive disturbances have been consistently described in patients who have undergone prolonged hospitalizations or intensive care, as reported in previous studies [14,15]. Few studies have examined the effects of COVID-19 on cognition by distinguishing between participants who required hospitalization and those with milder symptoms [7,9,15]. These studies have found that cognitive deficits are significantly more pronounced in patients with severe infections compared to those experiencing mild or no symptoms. Although most of the population infected during these years has experienced mild infection [16], it remains unclear whether milder cases (i.e., those not requiring hospitalization) may also experience long-term cognitive deficits that could significantly impact their quality of life and emotional well-being.
Mood disturbances, such as anxiety, depression, and post-traumatic stress disorder have also been frequently reported by patients who have suffered from COVID-19, persisting for several months after the infection [14,17,18]. These emotional disturbances have been suggested to negatively impact cognitive processes such as attention, comprehension, and decision-making [14,19]. The risk of developing such symptoms is particularly pronounced among frontline healthcare workers involved in diagnosing, treating, and caring for infected patients [17,20]. At the same time, the healthcare environment has been characterized by high levels of occupational distress, including professional burnout and moral distress, even before the COVID-19 pandemic began. However, the prolonged duration of this situation has increased the risk of healthcare workers developing chronic occupational stress [21,22,23,24]. For this reason, exploring the potential effects of mild COVID-19 on cognition and distinguishing them from those linked to affective symptoms is of particular importance.
With this in mind, our study had two main objectives: 1) to assess the long-term effects (beyond one year after infection) of COVID-19 on cognitive functioning in healthcare workers using a comprehensive neuropsychological battery, and 2) to explore the potential relationships between cognitive functioning and emotional status (anxiety, depression, post-traumatic stress disorder, and occupational burnout) in healthcare professionals, considering their high exposure to the virus and the considerable pressure they face daily in their occupation.
2. Materials and Methods
2.1. Participants
Ninety-two right-handed healthcare professionals (78 women) from the University Hospital Alcorcon Foundation (HUFA), a large hospital within the public health network of the Community of Madrid, Spain, participated in this study. Participants were aged between 22– 61 years. The COVID-19 group (50 professionals) comprised patients who had received outpatient treatment after experiencing mild infection with clinical symptoms. At the time of their participation in the study, the mean time to symptom resolution was 13.26 months (SD = 3.33). The control group (42 participants) consisted of healthcare professionals who had not suffered from COVID-19, verified through bimonthly serological tests at HUFA to detect antibodies. Participants suffering from neurological diseases or disorders that impair cognitive function, psychosis, or substance abuse/dependence were excluded. The Rey Juan Carlos University Research Ethics Board (Number: 2212202001021) and the ethics committee of University Hospital Alcorcon Foundation (HUFA) approved the study in accordance with their respective requirements. After obtaining written informed consent for their participation, participants provided sociodemographic data (age, level of education, profession) as well as information on their COVID-19 symptoms and treatment. The sociodemographic characteristics of the participants are shown in Table 1, along with information about COVID-19 symptoms (only for the COVID-19 group).
2.2. Neuropsychological Assessments
Participants completed a comprehensive battery of neuropsychological tests to assess attention, memory, and executive functions. Attentional status was assessed by the Spanish version of the D2 Sustained Attention Test (D2 Test) [25], which assesses sustained attention, selective attention, and processing speed. The Test of the Paths (TESEN) [26], based on the Trail Making Test (TMT) [27], consists of four tests that evaluate alternating attention and flexibility. The Symbol Search and Number Key subtests of the Spanish version of the Wechsler Intelligence Scale for Adults-IV (WAIS-IV) [28] were also administered to assess processing speed.
To assess memory processing, several subtests of the Spanish version of the Wechsler Memory Scale III (WMS-III) [29,30] were applied, including Word List I and II, and Faces I and II. Additionally, the WAIS-IV vocabulary subtest was used to evaluate semantic memory. In addition, the Rey–Osterrieth Complex Figure Test [31] was used to evaluate visuospatial construction, memory retention, and the ability to recall and reproduce complex visual information.
Finally, executive functions were assessed by the Five Digit Test [32], consisting of four experimental conditions (i.e., reading, counting, select, and switch). Specifically, this test allowed us to assess numerical processing and processes of attentional control, interference, and flexibility. The Digit Span, Spatial Span, and Letters-Numbers Sequencing subtests of the WMS-III were applied to assess working memory. The Similarities subtest of the WAIS-IV was administered to measure verbal reasoning and abstraction capacity. Word fluency was assessed using the FAS Test, a subtest of the Neurosensory Center Comprehensive Examination for Aphasia [33]. In addition, the Key Search and Zoo subtests of the BADS Scale (Behavioral Assessment of the Dysexecutive Syndrome) [34] were administered to assess aspects related to planning.
2.3. Emotional Measures and Subjective Complaints
Participants’ mood and clinical variables, such as anxiety and depression, were assessed using the Patient Health Questionnaire-9 (PHQ-9) [35], the State-Trait Anxiety Inventory (STAI) [36], and the Symptom Checklist-90 (SCL-90) [37]. The SCL-90 evaluates the presence of 90 symptoms, interpreted in terms of nine primary (somatization, obsessions and compulsions, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism) and three global indices (global severity index, positive discomfort index, and total positive symptoms). Post-traumatic stress was assessed using the Post-traumatic Stress Checklist-Civilian Version (PCL) [38]. Finally, occupational burnout was measured using the Emotional Exhaustion Subscale of the Maslach’s Burnout Inventory (MBI) [39].
2.4. Procedure
The Occupational Health Service of HUFA was responsible for selecting healthcare professionals with and without a history of mild COVID-19 and invited them to participate in the study. Healthcare professionals who agreed to participate were subsequently contacted by Rey Juan Carlos University to verify that they met the inclusion criteria and to schedule appointments.
The neuropsychological assessment was conducted over two sessions: the first at HUFA, and the second at the Cognitive Neuroscience Laboratory of Rey Juan Carlos University. Each session lasted approximately 1.5 hours. Both centers had specially conditioned rooms, optimized for lighting, sound, and ventilation to ensure a conducive testing environment.
During the first session, participants were provided with an informed consent form and a questionnaire on COVID-19 symptoms and treatment characteristics (for the COVID group only). Next, attention, memory, and executive functions were assessed using the following battery of neuropsychological test: Word List I and II, Faces I and II, Letters-Numbers subtest, and Spatial Span from WMS-III. Additionally, the Five Digit Test, the FAS Test and the Symbol Search and Number Key tests of the WAIS-IV were administered. The second session, scheduled between two and four weeks after the first, included the following tests: the D2 Test, the TESEN, the Digits, Vocabulary and Similarities subtest of the WAIS-IV, the Rey–Osterrieth Complex Figure Test, and the Key Search and Zoo subtests. Self-reported emotional questionnaires were completed online in the interim between the two sessions.
2.5. Statistical Analysis
Prior to statistical analyses, the normality of both emotional measures and neuropsychological outcomes was assessed. All dependent variables followed a normal distribution, as determined by the Kolmogorov-Smirnov test (p > 0.05). To examine potential differences in age and education level between participants, independent samples t-tests and chi-squared (χ2) tests were conducted, respectively. No significant differences were found between groups for these variables (see Table 1).
A series of one-way ANOVAs were conducted to compare neuropsychological and emotional self-report measures between the COVID-19 and control groups. Emotional variables that showed significant differences between groups were included in the analyses as covariates.
Finally, bivariate correlations were conducted to examine the relationships between emotional test scores and neuropsychological performance. A one-tailed significance level of 0.05 was applied to all statistical analyses. All analyses were performed using SPSS v. 27.0 statistical software.
3. Results
3.1. Descriptive Analysis
The distribution of scores across each neuropsychological measure (see Figures 1, 2, and 3) was analyzed separately for the COVID-19 and control groups. In most tests, over 60% of the participants scored at or above average. However, a more detailed examination of these scores by cognitive domain is warranted. Regardless of the group, more than 50% of participants scored below average on tests assessing processing speed (Symbol Search and D2 Test), as shown in Figure 1. A similar pattern was observed in other cognitive domains, such as memory (Faces I subtest) and executive functions (Five Digits), where up to 60% of healthcare professionals scored below average (see Figure 2 and Figure 3).
Regarding emotional symptoms and subjective cognitive complaints assessed through self-reported questionnaires, moderate to severe levels were observed across both groups. Specifically, participants exhibited psychological stress (49.61%), post-traumatic stress (53.80%), depression (71.52%), trait anxiety (56.23%), state anxiety (77.87%), and memory failures (80,28%). Full details on the distribution of these scores by group are shown in Figure 4.
3.2. Analyses on Neuropsychological Measures
The mean scores for each neuropsychological test outcome, grouped by COVID-19 and control health professionals, are shown in Table 2. One-way ANOVAs comparing cognitive performance across tests revealed no significant differences between groups on any neuropsychological measure.
3.3. Analyses on Emotional Symptomatology and Subjective Complaints
The results of ANOVAs exploring potential differences between the COVID-19 and control groups on self-reported emotional scores are shown in Table 3. Although healthcare workers in the COVID-19 group generally scored higher on most emotional measures compared to the control group, significant differences were only observed for trait anxiety, with the COVID-19 group exhibiting higher scores than the control group [F(1,90) = 0.784, p = 0.032]. No other statistically significant differences were found in the remaining analyses.
3.4. Relationship Between Neuropsychological Tests and Emotional Symptomatology
As mentioned in the data analysis section, correlations were conducted to explore potential relationships between cognitive performance, as assessed through the neuropsychological tests, and the scores from the self-reported emotional questionnaires (see Table 4). The results revealed several correlations, both positive and negative, between cognitive outcomes (such as the D2 variance index, TESEN path 4 resolution time, Rey-Osterrieth Complex Figure recovery score, and forward amplitude in the Digit Span) and most emotional symptoms. A consistent pattern emerged, where higher levels of emotional symptomatology (e.g., anxiety, depression, post-traumatic stress disorder, work-related stress) were correlated with greater variability in cognitive performance and task resolution times, as well as reduced recall and accuracy scores.
4. Discussion
The main objective of this study was to explore the impact on cognition of mild COVID-19 in healthcare professionals one year post-infection. Additionally, we examined the potential relationships between emotional symptoms—such as anxiety, depression, post-traumatic stress disorder, and work-related stress—and cognitive functioning, as these clinical factors may also influence cognitive performance in patients suffering from COVID-19 [21,42].
Results derived from the present study indicate that, overall, healthcare workers affected by mild COVID-19 did not show significant cognitive impairments compared to those who were not infected. Thus, both groups were comparable, with over 60% of participants in each group scoring at or above average across the different cognitive domains (attention, memory, and executive functions) assessed by a comprehensive neuropsychological battery. Cognitive effects of COVID-19 infection have been extensively documented in patients with severe infection, short recovery periods (less than 7 months), or in those involved in ‘long COVID’ research [5]. This latter term refers to a range of symptoms, including fatigue, respiratory distress, and cognitive dysfunction, which appear three months after a coronavirus infection, persist for at least two months, impact daily life, and cannot be explained by other causes [1].
Longitudinal studies are beginning to emerge, providing data on the evolution and cognitive recovery following infection in patients who required inpatient treatment [13,43]. Blazhenets and coworkers [44] found that deficits in executive functions, visuoconstructional skills, and memory persisted six months after recovering from COVID-19, as assessed by the Montreal Cognitive Assessment (MoCA). However, in most of patients, there was a significant improvement in performance compared to the post-acute phase, suggesting that the potential effect on cognition is reversible over time. Similarly, it has been reported that 53% of patients who experienced critical symptoms of COVID-19 showed clear cognitive deficits in at least one cognitive domain within two months of recovery. However, this percentage dropped to 36% ten months after hospitalization [45]. Thus, the absence of cognitive deficits in our sample could be attributed to the fact that the COVID-19 symptomatology was less severe (it did not require hospitalization) and the time since recovery was longer, which is reassuring for the general population.
Nevertheless, alternative or complementary explanations can be considered. The observed limited impact of COVID-19 on the cognitive functioning of infected healthcare workers might, at least in part, be explained by factors related to cognitive reserve, which has been found to be higher in individuals with a high level of education and occupational activity [46]. Specifically, the concept of cognitive reserve refers to a set of factors and mentally stimulating activities developed throughout life, such as social stimulation and leisure activities, which may play a protective role in brain plasticity. In this context, the cognitive demands associated with healthcare employment, along with years of formal education, contribute to cognitive status that supports optimal daily functioning [47]. Hence, research by Panico and coworkers [48], one of the few studies to explore this issue throughout the pandemic, describes how higher levels of cognitive reserve are associated with lower levels of stress. This, in turn, may help mitigate the impact on cognition, suggesting the potential benefit of interventions aimed at enhancing cognitive reserve to reduce the risk of cognitive impairment during this period. Conversely, as noted by Vance and coworkers [47], the absence of work activities—an experience shared by the broader population confined at home during the early months of the pandemic—represents a factor that impacts cognitive reserve and, consequently, cognition. Thus, the results obtained in our sample of healthcare workers cannot be generalized to the entire population.
Regarding emotional symptomatology, self-reported measures of anxiety, depression, post-traumatic stress disorder, and occupational burnout were also collected, as these factors are known to impact cognitive performance [21,42,49]. As a result, healthcare workers in the COVID-19 group exhibited higher levels of trait anxiety compared to those in the control group. Additionally, both groups showed high levels of state anxiety, depression, and post-traumatic stress disorder. Although COVID-19 infection does not seem to be directly associated with the presence or absence of emotional disturbances, it has been suggested that prolonged exposure to the pandemic has had significant psychological effects on healthcare workers [50]. Several factors have been identified as contributing to emotional disturbances, such as working exclusively in healthcare roles, long shifts due to staff shortages, close and prolonged contact with infected patients, inadequate or insufficient use of personal protective equipment at the beginning of the pandemic, working in enclosed and crowded spaces, and poor or insufficient ventilation [20,24,50,51]. In this vein, previous research has documented a wide range of emotional health issues among healthcare workers during the pandemic, including depression, anxiety, post-traumatic stress disorder, and insomnia [18]. A recent meta-analysis [50], which examined 392 studies, confirmed that between 25 and 28.5% of healthcare workers exhibited symptoms of depression, anxiety, post-traumatic stress disorder, and substance abuse. Furthermore, the prevalence of these symptoms has been found higher among healthcare workers as compared to general population. This is unsurprising, given the increased workload, risk of infection, uncertainty, and heightened sense of threat experienced by health care population during the pandemic [20,24]. However, one of the few longitudinal studies conducted so far suggests that mental health problems tend to decrease as the COVID-19 pandemic progresses [50].
Following this line of reasoning, we observed several correlations between cognitive performance and emotional symptomatology. Higher levels of psychological stress, burnout symptoms, depression, and post-traumatic stress were associated with poorer performance on D2 variance index, TESEN path 4 resolution time, Rey-Osterrieth Complex Figure recovery score, and forward amplitude in the Digit Span Test (WAIS-IV). These findings suggest a relationship between certain cognitive processes, such as selective and sustained attention, working and visual memory, executive function, and the presence of emotional symptoms, which warrant further attention. This underscores the importance of further investigation into the role emotional disturbances may play in cognitive functioning, particularly in healthcare workers—a rarely addressed topic [52]—as it allows us to distinguish the effects of COVID-19 infection from the potential impact of these emotional variables on cognition. Several studies have identified cognitive dysfunction that may persist even during the remission phase of clinically significant symptoms [42,49], particularly in processes such as executive functions, attention, working memory, and episodic memory, in individuals with depression [49], post-traumatic stress [53], burnout [21,52], and high levels of stress in general [54].
Therefore, given the absence of cognitive differences between groups (COVID-19 infected and non-infected), the high prevalence of emotional disturbances, and their correlation with cognitive performance, it is critical to prioritize monitoring the emotional well-being of health professionals. Longitudinal findings from a limited number of studies [50] indicate that pre-existing health problems have contributed to an increased risk of mental health issues during the pandemic. Therefore, it is not only crucial to continue monitoring the emotional status of health professionals but also to develop long-term strategies to address the systemic challenges they face daily.
This study is not without limitations. First, measuring neuroinflammatory levels, which have previously been shown to play a role in the development, maintenance, and recovery of cognitive and psychological symptoms [18], would have been useful for better characterizing potential cognitive impairments in the participant sample. Additionally, the lack of cognitive and psychological data prior to COVID-19 limits our capability to estimate the exact impact of the disease on the healthcare professionals participating in our study. Longitudinal studies are needed to assess the cognitive and emotional effects of the pandemic several years after its onset
5. Conclusions
In summary, it appears that, fortunately, mild long-term COVID-19 infection does not significantly affect the cognitive functioning of COVID-19 patients, particularly in a sample of healthcare workers. However, regardless of their COVID-19 status, healthcare workers exhibited high levels of emotional symptoms, such as post-traumatic stress, depression, and burnout, which are linked to poorer cognitive performance. The risks faced by healthcare professionals, as the first line of defense against the virus, warrant special attention and care. These findings contribute to a better understanding of the cognitive associated with COVID-19 and highlight the need for further longitudinal studies. Although the pandemic was declared over in May 2023—without implying that the virus has been eradicated—the working conditions of healthcare professionals should continue to be studied to preserve the health of this population.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, I.P., S.P-A. and F.M.; methodology, I.P., D.M-I., R.F-M., S.P-A. and F.M.; software, D.M-I., A.G-R and D.S.; validation, I.P., R.F-M., ME.H. and AB.P.; formal analysis, I.P., D.M-I., A.G-R. and F.M.; investigation, I.P., R.F-N. and S.P-A.; resources, F.M.; data curation, ME.H., AB.P., A.G-R. and D.S.; writing—original draft preparation, I.P.; writing—review and editing, I.P., D.M-I., R.F-M. and F.M.; visualization, ME.H., AB.P., A.G-R. and D.S.; supervision, I.P and F.M.; project administration, I.P. All authors have read and agreed to the published version of the manuscript.”
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Rey Juan Carlos University (protocol code 2212202001021 and 07/04/2021 of approval).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
data are available at: https://osf.io/fd35j/?view_only=27f14638244340e3ae229ca318200944
Acknowledgments
The authors would like to thank all healthcare professionals who participated in this study.
Conflicts of Interest
The authors declare no conflicts of interest
Abbreviations
The following abbreviations are used in this manuscript:
| BADS | Behavioral Assessment of the Dysexecutive Syndrome |
| COVID-19 | Coronavirus Disease 2019 |
| CoVs | Coronavirus |
| HUFA | University Hospital Alcorcon Foundation |
| ISP-20 | Prefrontal Symptom Inventory |
| MBI | Maslach’s Burnout Inventory |
| MFE-30 | Failures in Everyday Life Questionnaire |
| MoCA | Montreal Cognitive Assessment |
| PCL | Post-traumatic Stress Checklist-Civilian |
| PHQ-9 | Patient Health Questionnaire-9 |
| SARS-CoV-2 | Severe acute respiratory syndrome coronavirus 2 |
| SCL-90 | Symptom Cheklist-90 |
| STAI | State-Trait Anxiety Inventory |
| TESEN | The Test of the Paths |
| TMT | Trail Making Test |
| WAIS-IV | Wechsler Intelligence Scale for Adults-IV |
| WMS-III | Wechsler Memory Scale III |
References
- World Health Organization. A clinical case definition of post COVID-19 condition by a Delphi consensus. Geneva: WHO; 2024.
- Hu, B. , Guo, H., Zhou, P., & Shi, Z. L. (2021). Characteristics of SARS-CoV-2 and COVID-19. Nature Reviews Microbiology, 19(3), 141–154. [CrossRef]
- Bailey EK, Steward KA, VandenBussche Jantz AB, Kamper JE, Mahoney EJ, Duchnick JJ. Neuropsychology of COVID 19: Anticipated cognitive and mental health outcomes. Neuropsychology. 2021;35(4):335–51. [CrossRef]
- Boldrini M, Canoll P, Klein RS. How COVID 19 affects the brain. JAMA Psychiatry. 2021;78(6):682–3. [CrossRef]
- Zhao S, Toniolo S, Hampshire A, Husain M. Effects of COVID 19 on cognition and brain health. Trends Cogn Sci. 2023;27(11):1053–67. [CrossRef]
- Maiese A, Manetti AC, Bosetti C, Del Duca F, La Russa R, Frati P, et al. SARS CoV 2 and the brain: A review of neuropathology in COVID 19. Brain Pathol. 2021;31(6):e13013. [CrossRef]
- Becker JH, Lin JJ, Doernberg M, Stone K, Navis A, Festa JR, et al. Assessment of Cognitive Function in Patients after COVID 19 Infection. JAMA Netw Open. 2021;4(10):e2130645. [CrossRef]
- Daroische R, Hemminghyth MS, Eilertsen TH, Breitve MH, Chwiszczuk LJ. Cognitive impairment after COVID 19 — a review on objective test data. Front Neurol. 2021;12:699582. [CrossRef]
- Hampshire A, Trender W, Chamberlain SR, Jolly AE, Grant JE, Patrick F, et al. Cognitive deficits in people who have recovered from COVID 19. EClinicalMedicine. 2021;39:101044. [CrossRef]
- Ceban F, Ling S, Lui LMW, Lee Y, Gill H, Teopiz KM, et al. Fatigue and cognitive impairment in Post COVID 19 syndrome: A systematic review and meta analysis. Brain Behav Immun. 2022;101:93–135. [CrossRef]
- Crivelli L, Palmer K, Calandri I, Guekht A, Beghi E, Carroll W, et al. Changes in cognitive functioning after COVID 19: A systematic review and meta analysis. Alzheimer’s Dement. 2022;18(5):1047–66. [CrossRef]
- Tavares Júnior JWL, de Souza ACC, Borges JWP, Oliveira DN, Siqueira Neto JI, Sobreira Neto MA, et al. COVID 19 associated cognitive impairment: A systematic review. Cortex. 2022;152:77–97. [CrossRef]
- Ferrucci R, Dini M, Rosci C, Capozza A, Groppo E, Reitano MR, et al. One year cognitive follow up of COVID 19 hospitalized patients. Eur J Neurol. 2022;29(7):2006–14. [CrossRef]
- Miskowiak KW, Johnsen S, Sattler SM, Nielsen S, Kunalan K, Rungby J, et al. Cognitive impairments four months after COVID 19 hospital discharge. Eur Neuropsychopharmacol. 2021;46:39–48. [CrossRef]
- Ollila H, Pihlaja R, Koskinen S, Tuulio Henriksson A, Salmela V, Tiainen M, et al. Long term cognitive functioning is impaired in ICU treated COVID 19 patients: A comprehensive neuropsychological study. Crit Care. 2022;26(1):92. [CrossRef]
- Román F, Calandri IL, Caridi A, Carosella MA, Palma PA, Llera JJ, et al. Consecuencias neurológicas y psiquiátricas a largo plazo (6 meses) en pacientes con COVID leve de la comunidad. J Appl Cogn Neurosci. 2022;3(1):e00264623. [CrossRef]
- Mattioli F, Stampatori C, Righetti F, Sala E, Tomasi C, De Palma G. Neurological and cognitive sequelae of Covid 19: a four month follow up. J Neurol. 2021;268(12):4422–6. [CrossRef]
- Mazza MG, Palladini M, De Lorenzo R, Magnaghi C, Poletti S, Furlan R, et al. Persistent psychopathology and neurocognitive impairment in COVID 19 survivors: Effect of inflammatory biomarkers at three month follow up. Brain Behav Immun. 2021;94:138–47. [CrossRef]
- García Iglesias JJ, Gómez Salgado J, Martín Pereira J, Fagundo Rivera J, Ayuso Murillo D, Martínez Riera JR, Ruiz Frutos C. Impacto del SARS CoV 2 en la salud mental de los profesionales sanitarios: una revisión sistemática. Rev Esp Salud Pública. 2020;94:e202004011.
- Lai J, Ma S, Wang Y, Cai Z, Hu J, Wei N, et al. Factors associated with mental health outcomes among health care workers exposed to coronavirus disease 2019. JAMA Netw Open. 2020;3(3):e203976. [CrossRef]
- Arnsten AFT, Shanafelt T. Physician distress and burnout: The neurobiological perspective. Mayo Clin Proc. 2021;96(3):763–9. [CrossRef]
- Batra K, Singh TP, Sharma M, Batra R, Schvaneveldt N. Investigating the psychological impact of COVID 19 among healthcare workers: A meta analysis. Int J Environ Res Public Health. 2020;17(23):9239. [CrossRef]
- Carmassi C, Dell’Oste V, Bui E, Foghi C, Bertelloni CA, Atti AR, et al. The interplay between acute post traumatic stress, depressive and anxiety symptoms among healthcare workers during the COVID 19 emergency. J Affect Disord. 2022;298:209–16. [CrossRef]
- García Gómez M, Gherasim AM, Roldán Romero JM, Montoya Martínez L, Oliva Domínguez J, Escalona López S. COVID 19 related temporary disability in healthcare workers in Spain during the four first pandemic waves. Prev Med Rep. 2024;43:102779. [CrossRef]
- Brickenkamp R, Zillmer E. Test de atención d2 (D2 Test). Madrid: TEA Ediciones; 2002.
- Portellano JA, Martínez-Arias R. TESEN. Test de los senderos para la evaluación de las funciones ejecutivas. Madrid: TEA Ediciones; n.d.
- Reitan, RM. Trail Making Test: manual for administration and scoring. Tucson (AZ): Reitan Neuropsychology Laboratory; 1992.
- Wechsler, D. WAIS-IV: escala de inteligencia de Wechsler para adultos-IV. Madrid: Pearson; 2012.
- Pereña J, Seisdedos N, Corral S, Arribas-Aguila D, Santamaría P, Sueiro M. WMS-III. Wechsler Memory Scale-III (Spanish adaptation). Madrid: Pearson; 2004.
- Wechsler, D. WMS-III: escala de memoria de Wechsler-III. Madrid: Pearson; 2004.
- Jerskey BA, Meyers JE. Rey complex figure test. In: Kreutzer JS, DeLuca J, Caplan B, editors. Encyclopedia of clinical neuropsychology. New York: Springer; 2011. p. 2176–9. [CrossRef]
- Sedó, MA. Five Digit Test (Test de los cinco dígitos). Madrid: TEA Ediciones; 2007.
- Patterson, J. F-A-S test. In: Kreutzer JS, DeLuca J, Caplan B, editors. Encyclopedia of clinical neuropsychology. New York: Springer; 2011.
- Norris G, Tate RL. The Behavioural Assessment of the Dysexecutive Syndrome (BADS): ecological, concurrent and construct validity. Neuropsychol Rehabil. 2000;10(1):33–45.
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–13. [CrossRef]
- Spielberger CD, Gorsuch RL, Lushene RE. Manual for the State-Trait Anxiety Inventory. Palo Alto (CA): Consulting Psychologists Press; 1970.
- Derogatis, LR. SCL-90-R: administration, scoring and procedures manual-II. Baltimore (MD): Clinical Psychometric Research; 1992.
- Weathers FW, Litz BT, Herman DS, Huska JA, Keane TM. The PTSD checklist (PCL). San Antonio (TX): National Center for PTSD; 1993.
- Seisdedos, N. Manual MBI, inventario burnout de Maslach. Madrid: TEA Ediciones; 1997.
- Carrasco PM, Peña MM, Sueiro MJ. The Memory Failures of Everyday Questionnaire (MFE-30): internal consistency and reliability. Span J Psychol. 2012;15(2):768–76. [CrossRef]
- Pedrero-Pérez EJ, Ruiz-Sánchez de León JM. Quejas subjetivas de memoria, personalidad y sintomatología prefrontal en adultos jóvenes. Rev Neurol. 2013;57(7):289–96.
- Czerwińska A, Pawłowski T. Cognitive dysfunctions in depression – significance, description and treatment prospects. Psychiatr Pol. 2020;54(3):453–66. [CrossRef]
- Diana L, Regazzoni R, Sozzi M, Piconi S, Borghesi L, Lazzaroni E, et al. Monitoring cognitive and psychological alterations in COVID-19 patients: A longitudinal neuropsychological study. J Neurol Sci. 2023;444:120511. [CrossRef]
- Blazhenets G, Schroeter N, Bormann T, Thurow J, Wagner D, Frings L, et al. Slow but evident recovery from neocortical dysfunction and cognitive impairment in a series of chronic COVID-19 patients. J Nucl Med. 2021;62(7):910–15. [CrossRef]
- Cecchetti G, Agosta F, Canu E, Basaia S, Barbieri A, Cardamone R, et al. Cognitive, EEG, and MRI features of COVID-19 survivors: a 10-month study. J Neurol. 2022;269(7):3400–12. [CrossRef]
- Nogueira J, Gerardo B, Santana I, Simões MR, Freitas S. The assessment of cognitive reserve: a systematic review of the most used quantitative measurement methods of cognitive reserve for aging. Front Psychol. 2022;13:847186. [CrossRef]
- Vance DE, Bail J, Enah C, Palmer J, Hoenig A. The impact of employment on cognition and cognitive reserve: implications across diseases and aging. Nurs Res Rev. 2016;6:61–71. [CrossRef]
- Panico F, Luciano SM, Sagliano L, Santangelo G, Trojano L, Vance DE, et al. Cognitive reserve and coping strategies predict the level of perceived stress during COVID-19 pandemic: a cross-sectional study. Pers Individ Dif. 2022;190:111703. [CrossRef]
- Rock PL, Roiser JP, Riedel WJ, Blackwell AD. Cognitive impairment in depression: a systematic review and meta-analysis. Psychol Med. 2014;44(10):2029–40. [CrossRef]
- Lee BEC, Ling M, Boyd L, Olsson C, Sheen J. The prevalence of probable mental health disorders among hospital healthcare workers during COVID-19: a systematic review and meta-analysis. J Affect Disord. 2023;330:329–45. [CrossRef]
- Bueno Ferrán M, Barrientos-Trigo S. Caring for the caregiver: the emotional impact of the coronavirus epidemic on nurses and other health professionals. Enferm Clin. 2021;31(Suppl 1):S35–S39. [CrossRef]
- Koutsimani P, Montgomery A. Burnout and cognitive functioning: are we underestimating the role of visuospatial functions? Front Psychiatry. 2022;13:775606. [CrossRef]
- Acheson DT, Gresack JE, Risbrough VB. Hippocampal dysfunction effects on context memory: possible etiology for posttraumatic stress disorder. Neuropharmacology. 2012;62(2):674–85. [CrossRef]
- Bakusic J, Schaufeli W, Claes S, Godderis L. Stress, burnout and depression: a systematic review on DNA methylation mechanisms. J Psychosom Res. 2017;92:34–44. [CrossRef]
Figure 1.
Distribution of scores on neuropsychological attention tests (in percentage) of both groups according to the intervals of each questionnaire. The classification was performed using standard scores. Abbreviations: D2 Sustained Attention Test (D2 test), Test of the Paths (TESEN).
Figure 1.
Distribution of scores on neuropsychological attention tests (in percentage) of both groups according to the intervals of each questionnaire. The classification was performed using standard scores. Abbreviations: D2 Sustained Attention Test (D2 test), Test of the Paths (TESEN).
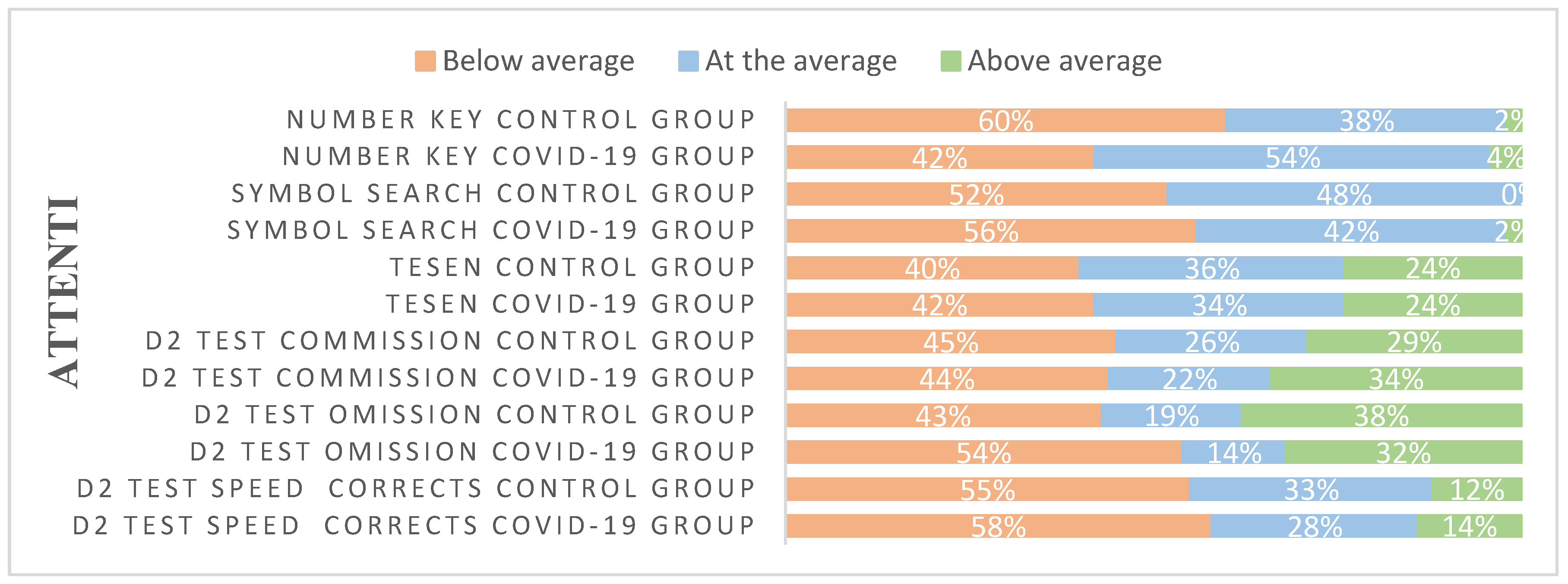
Figure 2.
Distribution of scores on neuropsychological memory tests (in percentage) of both groups according to the intervals of each questionnaire. The classification was performed using standard scores.
Figure 3.
Distribution of scores on neuropsychological executive functions tests (in percentage) of both groups according to the intervals of each questionnaire. The classification was performed using standard scores.
Figure 3.
Distribution of scores on neuropsychological executive functions tests (in percentage) of both groups according to the intervals of each questionnaire. The classification was performed using standard scores.
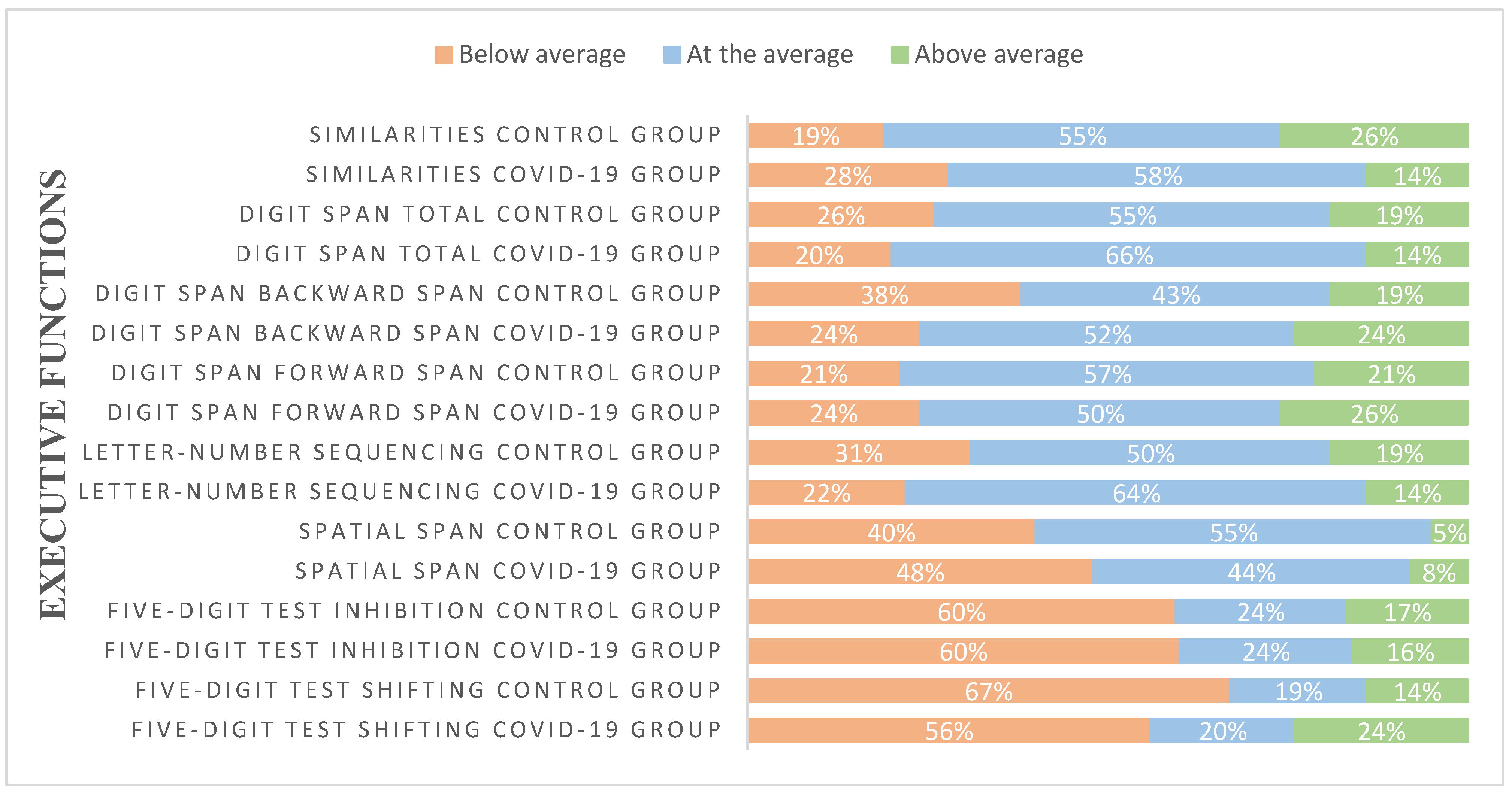
Figure 4.
Distribution of self-reported scores (in percentage) of both groups according to the intervals of each questionnaire. Abbreviations: Symptom cheklist-90 (SCL-90-R), Abbreviated Prefrontal Symptom Inventory (ISP-20), Failures in Everyday Life Questionnaire (MFE-30), Post-traumatic Stress Checklist-Civilian Version (PCL), Emotional Exhaustion Subscale of the Maslach’s Burnout Inventory (MBI), Patient Health Questionnaire-9 (PHQ-9), and State-Trait Anxiety Inventory (STAI).

Table 1.
Sociodemographic data and symptomatology (only for the COVID-19 group) are presented. Means, percentages, and standard deviations (in parentheses) are reported. Statistical details of group comparisons (Student’s-test or χ2-tests) are also displayed.
Table 1.
Sociodemographic data and symptomatology (only for the COVID-19 group) are presented. Means, percentages, and standard deviations (in parentheses) are reported. Statistical details of group comparisons (Student’s-test or χ2-tests) are also displayed.
| Variables | Percentage or Mean (SD) | Group effect | ||
| Control group | COVID-19 group | Statistic t or χ2 | p-value | |
| Age (years) | 44.24 (11.23) | 45.18 (10.49) | - 0.415 | 0.679 |
| Education | 0.393 | 0.822 | ||
| Intermediate Studies (%) | 33.3 | 32.0 | ||
| Advanced Vocational Qualification (%) | 4.8 | 8.0 | ||
| University studies (%) | 61.9 | 60.0 | ||
| Profession | 7.640 | 0.054 | ||
| Physician (%) | 16.7 | 6.0 | ||
| Nurse (%) | 54.8 | 80.0 | ||
| Physiotherapist (%) | 14.3 | 4.0 | ||
| Other (%) | 14.3 | 10.0 | ||
| Time since COVID-19 symptoms (months) | - | 13 (3.82) | ||
| COVID-19 Symptoms | ||||
| Fever (%) | - | 72.0 | ||
| Dry cough (%) | - | 66.0 | ||
| Tiredness (%) | - | 90.0 | ||
| Aches and pains (%) | - | 78.0 | ||
| Sore throat (%) | - | 52.0 | ||
| Diarrhoea (%) | - | 32.0 | ||
| Conjunctivitis (%) | - | 6.0 | ||
| Headache (%) | - | 84.0 | ||
| Loss of smell (%) | - | 70.0 | ||
| Loss of taste (%) | - | 64.0 | ||
| Dysgeusia (%) | - | 34.0 | ||
| Skin rash or loss of pain (%) | - | 14.0 | ||
| Difficulty breathing or feeling short of breath (%) | - | 48.0 | ||
| Chest pain or pressure (%) | - | 46.0 | ||
| Inability to speak or move (%) | - | 8.0 | ||
| Vomiting or nausea (%) | - | 22.0 | ||
| Itchy skin (%) | - | 12.0 | ||
| Feeling dizzy (%) | - | 32.0 | ||
| Syncope (%) | - | 4.0 | ||
| Confusion (%) | - | 10.0 | ||
Table 2.
Means and standard deviations (in parentheses) of neuropsychological scores, split by group. Raw scores are presented.
Table 2.
Means and standard deviations (in parentheses) of neuropsychological scores, split by group. Raw scores are presented.
| Neuropsychological tests | COVID-19 group | Control group | Statistics (df = 1,90) |
| ATTENTION | |||
| D2 test | |||
| Scanning speed | 432.38 (87.494) | 434.83 (81.874) | F=0.018, p=0.895 |
| Scanning accuracy | 170.10 (43.239) | 165.55 (38.952) | F=0.277, p=0.600 |
| Omission | 12.52 (10.300) | 17.31 (14.146) | F=3.516, p=0.064 |
| Commission | 7.90 (4.807) | 2.45 (4.915) | F=1.957, p=0.165 |
| Effectiveness index | 412.48 (82.240) | 406.93 (86.358) | F=0.099, p=0.753 |
| Concentration index | 162.18 (37.307) | 163.10 (40.975) | F=0.013, p=0.911 |
| Max | 36.96 (6.114) | 36.76 (5.656) | F=0.026, p=0.873 |
| Min | 25.14 (7.709) | 24.40 (6.950) | F=0.227, p=0.635 |
| Variation index | 12.04 (4.882) | 12.36 (5.093) | F=0.093, p=0.762 |
| TESEN | |||
| Path 1Execution | 27.01 (7.695) | 28.67 (5.549) | F=1.357, p=0.247 |
| Path 1 Speed | 92.88 (25.749) | 86.21 (20.290) | F=1.849, p=0.177 |
| Path 1 Accuracy | 98.59 (2.840) | 98.98 (2.473) | F=0.499, p=0.482 |
| Path 2Execution | 25.01 (6.653) | 26.56 (6.200) | F=1.305, p=0.256 |
| Path 2 Speed | 99.46 (25.565) | 94.36 (29.597) | F=0.787, p=0.377 |
| Path 2 Accuracy | 98.33 (3.039) | 98.23 (3.553) | F=0.018, p=0.893 |
| Path 3Execution | 18.31 (4.567) | 18.89 (4.371) | F=0.388, p=0.535 |
| Path 3 Speed | 106.54 (36.249) | 99.81 (25.072) | F=1.032, p=0.312 |
| Path 3 Accuracy | 95.96 (10.791) | 95.69 (7.221) | F=0.018, p=0.894 |
| Path 4Execution | 15.88 (19.016) | 14.39 (4.271) | F=0.250, p=0.619 |
| Path 4 Speed | 144.02 (3.759) | 139.19 (40.697) | F=0.027, p=0.555 |
| Path 4 Accuracy | 95.51 (13.201) | 98.04 (3.387) | F=1.468, p=0.229 |
| Total Execution | 19.57 (4.591) | 20.94 (4.24) | F=2.193, p=0.142 |
| Total Speed | 432.81 (128.36) | 418.62 (104.04) | F=0.331, p=0.567 |
| Total Accuracy | 97.54 (4.125) | 97.83 (2.846) | F=0.151, p=0.699 |
| Symbol search | 37.25 (8.411) | 37.78 (8.568) | F=0.084, p=0.773 |
| Number Key | 75.26 (14.151) | 79.36 (17.072) | F=1.585, p=0.211 |
| MEMORY | |||
| Word list I | |||
| Score 1º recall | 6.62 (1.398) | 6.67 (1.509) | F=0.024, p=0.878 |
| Total recall score | 35.80 (5.063) | 36.10 (4.674) | F=0.083, p=0.774 |
| Interference 1 | 0.92 (1.441) | 0.81 (2.027) | F=0.093, p=0.761 |
| Learning | 3.72 (1.371) | 3.95 (1.738) | F=0.514, p=0.475 |
| Interference 2 | 1.14 (1.552) | 1.21 (1.353) | F=0.059, p=0.809 |
| Word list II | |||
| Recall | 9.04 (2.466) | 9.02 (2.342) | F=0.001, p=0.974 |
| Recognition | 23.39 (1.169) | 23.17 (1.305) | F=0.726, p=0.396 |
| Faces I | 40.87 (3.512) | 40.60 (3.787) | F=0.128, p=0.721 |
| Faces II | 102.65 (15.806) | 100.55 (7.765) | F=0.619, p=0.433 |
| Vocabulary | 36.24 (9.317) | 34.00 (9.904) | F=1.246, p=0.267 |
| Rey-Osterrieth complex figure | |||
| Copy | 33.15 (4.136) | 32.77 (3.239) | F=0.229, p=0.633 |
| Copy time | 125.40 (38.970) | 137.52 (43.747) | F=1.975, p=0.163 |
| Recovery | 18.06 (5.985) | 18.45 (6.288) | F=0.094, p=0.760 |
| Recovery time | 109.84 (37.433) | 117.20 (43.584) | F=0.750, p=0.389 |
| EXECUTIVE FUNCTIONS | |||
| FAS Test | |||
| F (Words/min) | 18.04 (4.256) | 19.60 (3.749) | F=3.299, p=0.073 |
| A (Words/min) | 15.76 (4.461) | 16.31 (3.646) | F=0.408, p=0.525 |
| S (Words/min) | 15.18 (4.308) | 15.60 (3.722) | F=0.240, p=0.626 |
| Semantics (Words/min) | 63.18 (11.208) | 66.93 (10.778) | F=2.644, p=0.107 |
| Five-digit test | |||
| Reading | 20.14 (3.417) | 19.74 (3.507) | F=0.308, p=0.580 |
| Counting | 21.88 (3.409) | 21.19 (3.430) | F=0.929, p=0.338 |
| Choosing | 31.96 (5.525) | 30.52 (5.438) | F=1.565, p=0.214 |
| Shifting | 41.30 (8.812) | 39.07 (7.270) | F=1.709, p=0.194 |
| Inhibition | 11.82 (5.054) | 10.95 (5.860) | F=0.582, p=0.448 |
| Flexibility | 21.16 (7.950) | 19.26 (7.398) | F=1.385, p=0.242 |
| Spatial span | |||
| Forward | 8.60 (1.841) | 8.71 (1.672) | F=0.096, p=0.758 |
| Backward | 8.22 (1.962) | 7.95 (1.766) | F=0.465, p=0.497 |
| Total | 17.00 (3.812) | 16.62 (2.946) | F=0.279, p=0.599 |
| Letter-number sequencing | 19.12 (2.344) | 19.69 (2.552) | F=1.247, p=0.267 |
| Digit span | |||
| Forward | 9.00 (1.959) | 8.69 (2.089) | F=0.536, p=0.466 |
| Forward Span | 6.06 (1.168) | 5.93 (1.237) | F=0.274, p=0.602 |
| Backward | 8.28 (2.286) | 8.29 (1.798) | F=0.000, p=0.990 |
| Backward Span | 4.62 (1.244) | 4.67 (1.052) | F=0.037, p=0.848 |
| Increasing | 8.46 (2.279) | 8,79 (2.280) | F=0.466, p=0.496 |
| Increasing Span | 5.84 (1.695) | 6.29 (2.351) | F=1.111, p=0.295 |
| Total | 25.76 (5.286) | 25.76 (4.616) | F=0.000, p=0.999 |
| Similarities | 21.88 (4.914) | 19.93 (4.566) | F=3.838, p=0.053 |
| Key search | 10.80 (3.774) | 11.52 (3.487) | F=0.900, p=0.345 |
| Key search time | 60.42 (61.305) | 58.26 (57.274) | F=0.030, p=0.863 |
| Zoo test Total | 11.10 (3.898) | 11.40 (3.964) | F=0.137, p=0.712 |
Abbreviations: D2 Sustained Attention Test (D2 test), Test of the Paths (TESEN).
Table 3.
Means and standard deviations (in parentheses) of self-reported emotional scores by group. Raw scores are presented.
Table 3.
Means and standard deviations (in parentheses) of self-reported emotional scores by group. Raw scores are presented.
| Emotional measures | Covid-19 group | Control group | Statistics (df = 1,90) |
| STAI-State | 25.08 (4.923) | 24.67 (5.664) | F=0.113, p=0.738 |
| STAI-Trait | 26.52 (5.578) | 24.07 (5.110) | F=4.746, p=0.032 |
| PHQ-9 | 8.06 (5.482) | 7.71 (4.994) | F=1.748, p=0.190 |
| MBI | 11.32 (5.156) | 12.05 (6.231) | F=1.079, p=0.541 |
| PCL | 34.58 (11.500) | 34.55 (17.429) | F=0.639, p=0.426 |
| MFE-30 | 14.42 (8.442) | 13.76 (8.678) | F=1.303, p=0.992 |
| ISP-20 | 15.72 (11.644) | 14.76 (12.689) | F=0.057, p=0.812 |
| SCL-90-R | 78.32 (56.750) | 69.50 (64.569) | F=0.008, p=0.927 |
| Somatizations | 1.01 (0.783) | 1.70 (5.025) | F=0.245, p=0.622 |
| Obsessions and compulsions | 1.28 (0.868) | 2.45 (10.078) | F=0.097, p=0.756 |
| Interpersonal sensitivity | 0.84 (0.773) | 0.58 (0.556) | F=0.909, p=0.343 |
| Depression | 1.13 (0.881) | 0.81 (0.768) | F=0.822, p=0.367 |
| Anxiety | 0.69 (0.642) | 0.68 (0.782) | F=0.674, p=0.414 |
| Hostility | 0.68 (0.705) | 0.41 (0.671) | F=1.433, p=0.235 |
| Phobic anxiety | 0.27 (0.426) | 0.32 (0.535) | F=1.618, p=0.207 |
| Paranoid ideation | 0.66 (0.809) | 0.37 (0.562) | F=1.925, p=0.169 |
| Psychoticism | 0.42 (0.620) | 0.26 (0.362) | F=2.988, p=0.141 |
| Global severity index | 0.84 (0.647) | 0.67 (0.628) | F=0.176, p=0.676 |
| Positive discomfort index | 1.66 (0.575) | 1.76 (0.612) | F=3.672, p=0.059 |
| Total positive symptoms | 41.78 (21.076) | 34.02 (23.912) | F=0.856, p=0.357 |
Table 4.
Pearson correlations between neuropsychological measures and self-reported emotional scores for the entire sample of participants.
Table 4.
Pearson correlations between neuropsychological measures and self-reported emotional scores for the entire sample of participants.
| Emotional tests | STAI State | STAI Trait | PHQ-9 | MBI | PCL | MFE-30 | ISP20 | SCL-90-R |
| Neuropsychological tests | ||||||||
| ATTENTION | ||||||||
| D2 test | ||||||||
| Scanning speed | -,040 | -,023 | ,038 | -,105 | -,131 | ,037 | ,048 | -,086 |
| Scanning accuracy | ,001 | ,005 | ,028 | -,115 | -,080 | ,007 | ,009 | -,068 |
| Omission | -,084 | ,015 | ,005 | -,034 | -,015 | ,101 | ,126 | -,010 |
| Commission | ,002 | ,066 | -,057 | -,038 | ,017 | -,067 | -,044 | -,006 |
| Effectiveness index | ,000 | -,140 | ,061 | -,205* | -,133 | ,009 | ,033 | -,103 |
| Concentration index | ,000 | -,027 | ,057 | -,104 | -,093 | ,040 | ,030 | -,069 |
| Max | -,073 | ,058 | ,141 | -,104 | -,027 | ,113 | ,105 | ,002 |
| Min | -,104 | -,050 | -,101 | -,207* | -,201* | -,137 | -,006 | -,163 |
| Variation index | ,078 | ,137 | ,328** | ,199 | ,273** | ,328** | ,147 | ,249* |
| TESEN | ||||||||
| Sendero 1Execution | -,024 | -,057 | ,008 | -,179 | -,088 | -,123 | -,039 | -,125 |
| Send1 Speed | -,003 | ,086 | ,067 | ,177 | ,113 | ,110 | ,061 | ,132 |
| Send1 Accuracy | ,024 | ,059 | ,092 | ,024 | ,068 | ,013 | -,051 | -,085 |
| Sendero 2Execution | ,031 | -,152 | -,039 | -,188 | -,209* | -,237* | -,145 | -,182 |
| Send2 Speed | -,038 | ,125 | ,037 | ,215* | ,178 | ,176 | ,137 | ,146 |
| Send2 Accuracy | ,134 | -,112 | -,161 | 004 | -,001 | -,093 | -,087 | -,064 |
| Sendero 3Execution | ,027 | -,016 | ,134 | -,053 | ,053 | ,105 | ,018 | -,026 |
| Send3 Speed | -,089 | -,001 | -,091 | ,075 | -,049 | -,080 | ,004 | ,085 |
| Send3 Accuracy | -,038 | -,008 | ,028 | ,064 | ,074 | ,096 | ,079 | ,079 |
| Sendero 4Execution | ,100 | -,035 | ,189 | -,003 | ,151 | ,247* | ,135 | ,118 |
| Send4 Speed | ,046 | ,204* | ,039 | ,275** | ,176 | ,079 | ,169 | ,217* |
| Send4 Accuracy | ,055 | ,050 | ,015 | -,013 | ,010 | -,031 | -,044 | -,068 |
| Total Execution | -,022 | -,128 | ,022 | -,225* | -,124 | -,100 | -,104 | -,168 |
| Total Speed | -,013 | ,121 | ,037 | ,228* | ,133 | ,106 | ,104 | ,183 |
| Total Accuracy | ,031 | ,006 | -,033 | ,032 | ,046 | -,007 | -,042 | -,044 |
| Symbol search | ,121 | -,001 | ,049 | -,053 | -,012 | ,005 | ,051 | ,022 |
| Number Key | ,079 | ,059 | -,048 | ,016 | -,138 | -,076 | -,021 | -,056 |
| MEMORY | ||||||||
| Word list I | ||||||||
| Score 1º recall | -,044 | ,030 | -,043 | -,129 | -,077 | -,147 | -,091 | -,167 |
| Total recall score | -,087 | ,143 | ,078 | ,007 | ,003 | ,003 | ,022 | -,081 |
| Interference 1 | -,130 | -,047 | -,126 | -,175 | -,130 | -,164 | -,100 | -,095 |
| Learning | -,034 | ,126 | ,150 | ,177 | ,064 | ,155 | ,072 | ,097 |
| Interference 2 | -,082 | ,078 | ,112 | ,117 | ,192 | ,043 | ,014 | ,112 |
| Word list II | ||||||||
| Recall | -,010 | ,111 | ,020 | -,007 | -,096 | ,026 | -,026 | -,095 |
| Recognition | ,070 | ,141 | ,167 | ,078 | ,067 | ,184 | ,170 | ,101 |
| Faces I | -,013 | -,006 | ,011 | -,170 | -,112 | ,050 | -,005 | -,036 |
| Faces II | ,031 | ,104 | ,128 | ,130 | ,134 | ,031 | ,060 | ,094 |
| Vocabulary | -,022 | ,048 | -,225* | -,149 | -,183 | -,125 | -,091 | -,242* |
| Rey-Osterrieth complex figure | ||||||||
| Copy | -,179 | -,016 | -,041 | -,036 | -,161 | -,096 | -,110 | -,178 |
| Copy time | -,018 | ,023 | ,026 | ,261* | ,141 | ,064 | -,024 | ,098 |
| Recovery | -,161 | -,155 | -,046 | -,217* | -,294* | -,101 | -,167 | -,261* |
| Recovery time | ,039 | ,090 | -,035 | -,002 | -,016 | -,101 | -,196 | -,127 |
| EXECUTIVE FUNCTIONS | ||||||||
| F-A-S Test | ||||||||
| F (Words/min) | -,007 | -,016 | -,090 | -,042 | -,049 | -,073 | -,058 | -,063 |
| A (Words/min) | -,053 | -,104 | -,168 | -,022 | -,087 | -,012 | -,056 | -,094 |
| S (Words/min) | -,040 | -,092 | -,108 | -,157 | -,114 | -,073 | -,118 | -,170 |
| Semantics (Words/3min) | -,047 | -,098 | -,182 | -,127 | -,217* | -,065 | -,093 | -,209* |
| Five-digit test | ||||||||
| Reading | -,161 | ,043 | ,159 | -,053 | ,138 | -,020 | -,060 | ,047 |
| Counting | -,113 | ,071 | ,188 | -,021 | ,131 | -,029 | -,023 | ,074 |
| Choosing | -,059 | ,068 | ,067 | -,010 | ,065 | ,035 | ,123 | ,063 |
| Shifting | -,036 | -,053 | -,015 | ,056 | ,067 | ,027 | ,049 | ,105 |
| Inhibition | ,066 | ,064 | -,004 | ,067 | ,011 | ,072 | ,177 | ,064 |
| Flexibility | ,027 | -,083 | -,096 | ,070 | -,001 | ,030 | ,074 | ,081 |
| Spatial span | ||||||||
| Forward | -,029 | -,077 | ,030 | -,026 | -,020 | -,040 | ,017 | -,042 |
| Backward | -,064 | -,068 | -,027 | -,279** | -,167 | -,035 | -,114 | -,263* |
| Total | -,030 | -,039 | -,017 | -,186 | -,109 | -,069 | -,038 | -,179 |
| Letter-number sequencing | ,069 | -,092 | ,026 | -,101 | -,074 | ,043 | -,053 | -,116 |
| Digit span | ||||||||
| Forward | ,040 | -,106 | -,156 | -,257* | -,104 | -,098 | -,144 | -,198 |
| Forward Span | ,016 | -,124 | -,221* | -,279** | -,132 | -,132 | -,211* | -,235* |
| Backward | ,011 | -,111 | -,050 | -,110 | -,055 | -,059 | -,084 | -,102 |
| Backward Span | ,024 | -0,97 | -,020 | -,057 | -,047 | -,046 | -,111 | -,095 |
| Increasing | -,081 | -,274** | -,060 | -,159 | -,091 | ,010 | -,048 | -,147 |
| Increasing Span | ,035 | -,240* | -,004 | -,109 | -,017 | ,115 | -,062 | -,074 |
| Total | -,012 | -,209* | -,109 | -,224* | -,106 | -,061 | -,116 | -,190 |
| Similarities | ,071 | -,036 | -,148 | -,063 | -,141 | ,007 | ,047 | -,096 |
| Key search | ,091 | ,068 | -,019 | ,044 | -,108 | ,029 | ,070 | -,056 |
| Key search time | -,154 | -,120 | ,046 | ,056 | ,061 | ,044 | -,042 | ,021 |
| Zoo test Total | ,081 | ,177 | -,007 | ,163 | -,051 | -,125 | ,061 | -,022 |
* p < 0.05; ** p < 0.01. Abbreviations: State-Trait Anxiety Inventory (STAI), Patient Health Questionnaire-9 (PHQ-9), Emotional Exhaustion Subscale of the Maslach’s Burnout Inventory (MBI), Post-traumatic stress Checklist-Civilian Version (PCL), Failures in Everyday Life Questionnaire (MFE-30), Abbreviated Prefrontal Symptom Inventory (ISP-20), Symptom Checklist-90 (SCL-90-R). D2 Sustained Attention Test (D2 test), Test of the Paths (TESEND).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



