
Submitted:
16 July 2025
Posted:
17 July 2025
You are already at the latest version
Abstract
Wolfram Syndrome is a rare neurodegenerative disorder primarily known for its multisystemic manifestations. Although classically associated with diabetes insipidus, diabetes mellitus, optic atrophy, and deafness, emerging evidence suggests a consistent pattern of executive dysfunction in many affected individuals. Based on findings from a scoping review and results obtained through the Dysexecutive Questionnaire in a Spanish patient cohort, we propose that WFS1 gene mutations—via chronic endoplasmic reticulum stress—disrupt serotonergic and cholinergic neurotransmission, leading to impairments in planning, inhibition, and emotional regulation. Importantly, recent studies have highlighted the interplay between WFS1-related molecular dysfunction and circadian regulation. Given the role of the endoplasmic reticulum and mitochondrial signaling in circadian homeostasis, and the frequent sleep disturbances observed in patients with Wolfram Syndrome, we hypothesize that circadian dysregulation may contribute to the neurobehavioral phenotype. This essay explores both the molecular and neuropsychological foundations of executive dysfunction in WS, suggesting it may be a primary feature and advocating for its inclusion in routine clinical care. Furthermore, the potential involvement of circadian mechanisms opens new avenues for future research and therapeutic approaches.
Keywords:
literature review
; wolfram syndrome
; circadian rhythms
; dysexecutive questionnaire
; DEX
; neuropsychological aspects
Introduction
Wolfram syndrome (WS), also known as DIDMOAD (diabetes insipidus, diabetes mellitus, optic atrophy, and deafness), represents a paradigmatic example of rare neurodegenerative diseases. Its prevalence is estimated to range from 1 in 55,000 to 1 in 770,000 individuals [1,2]; in the United Kingdom, it is reported as 1 in 770,000, and in Spain, only 47 cases have been documented [2,3,4]. Although the hallmark clinical features of WS, such as optic atrophy and neurogenic bladder, are well established, its cognitive and behavioral manifestations remain underexplored [5]. Over several decades, patients often progress from functional independence to total dependency, confronting blindness, hearing loss, and central nervous system involvement [6]. During this progression, many individuals experience symptoms suggestive of executive dysfunction, including impulsivity, emotional dysregulation, apathy, and impaired planning. These features may not merely represent reactions to chronic illness but rather reflect underlying neurobiological mechanisms.
In clinical settings, such symptoms are frequently overlooked or misattributed to psychosocial stressors. However, accumulating anecdotal evidence and early systematic research suggest the existence of a nonpsychotic frontal syndrome with a potential neuropathological basis [7,8]. If validated, this would substantially alter the current understanding and management of WS’s neuropsychiatric dimensions.
Accordingly, we propose a novel neuropsychological hypothesis linking molecular pathology to behavioral outcomes in WS. Drawing on existing literature and data obtained using the Dysexecutive Questionnaire (DEX) [9] in a Spanish patient cohort, we hypothesize that mutations in the WFS1 gene lead to chronic endoplasmic reticulum (ER) stress, disrupting critical neurotransmitter systems—particularly serotonergic and cholinergic circuits—essential for prefrontal executive functioning. [10]
Importantly, WFS1 is increasingly recognized as a gene involved in the regulation of mitochondrial and ER homeostasis, both of which are tightly linked to circadian biology [11]. Recent findings have also associated WFS1 mutations with altered sleep patterns and circadian rhythm disruptions, which may contribute to the behavioral and emotional symptoms observed in WS patients [12]. These alterations could affect the timing and amplitude of neurochemical activity that modulates executive functioning. Therefore, we further hypothesize that circadian dysregulation may act as a contributing factor to the executive dysfunction profile in WS.
This expanded perspective encourages interdisciplinary research combining neuropsychological, molecular, and chronobiological approaches, and supports incorporating both executive and circadian assessments into the routine clinical evaluation of individuals with WS.
Materials and Methods
First Stage: Scoping Review
This research employs a meticulous and methodologically rigorous scoping review designed to comprehensively examine the available literature on the selected topic. Rather than aiming to conduct a systematic meta-analysis or statistical synthesis, the primary objective was to identify recurring psychological patterns associated with Wolfram syndrome (WS) that may suggest shared neurobiological mechanisms.
This approach was deliberately selected not only for its breadth in mapping the field, but also because it aligns with the exploratory, hypothesis-generating nature of this study. The scoping review thus provides a foundational overview of the current literature concerning the psychological dimensions of WS, serving both as a springboard for future research and as the conceptual basis for the theoretical model proposed in this article.
Second Stage – Evaluation of Executive Functions Using DEX
In parallel with the scoping review, a complementary exploratory study was conducted to empirically assess executive functioning in individuals with Wolfram syndrome (WS). For this purpose, the Dysexecutive Questionnaire (DEX), part of the Behavioral Assessment of the Dysexecutive Syndrome (BADS), was administered.
The sample consisted of Spanish patients with a genetically and clinically confirmed diagnosis of WS due to WFS1 mutation, aged 16 years or older, recruited through specialized clinical units and patient associations. All participants—or their legal guardians—provided written informed consent prior to participation. Inclusion criteria required sufficient cognitive capacity to complete the instrument, with caregiver assistance provided when necessary.
The DEX is a 20-item self-report or informant-report questionnaire that assesses executive function difficulties encountered in everyday life [13]. These domains include impulse control, planning, working memory, inhibition, emotional regulation, and decision-making. The instrument was selected not only for its clinical utility, but also for its conceptual alignment with the central hypothesis: identifying behavioral indicators of prefrontal dysfunction potentially related to WFS1 mutation–induced neurobiological disruption. The version employed was the Spanish adaptation of the original scale, translated using a parallel back-translation process to ensure conceptual and linguistic equivalence.
The sample assessed with the DEX questionnaire included 28 individuals with a genetically and clinically confirmed diagnosis of Wolfram Syndrome (46.4% female), all aged 16 or older, with a mean age of 24.4 years (SD = 9.7). All participants met the cognitive requirements to complete the questionnaire, either independently or with caregiver assistance [14].
Rationale for Methodology: Unlike traditional hypothesis-driven studies, this research integrates qualitative synthesis and exploratory data to formulate a biologically plausible hypothesis. The scoping review was not intended for statistical inference but rather to identify psychological patterns and recurrent psychiatric features indicative of a shared neurobiological mechanism in Wolfram syndrome (WS).Within this framework, the Dysexecutive Questionnaire (DEX) was not employed as a diagnostic instrument per se, but rather as a conceptual probe—a means to evaluate whether the behaviors observed in WS are consistent with established patterns of prefrontal-executive dysfunction. Given the hypothesis that WFS1 mutations induce endoplasmic reticulum (ER) stress, resulting in neurotransmitter dysregulation, the DEX offers an indirect yet meaningful behavioral measure [15].
Thus, this methodological combination supports the theoretical framework proposed in this study, effectively bridging molecular hypotheses with real-world psychological profiles.
Search Strategy: A systematic search strategy was developed and applied across several major international databases and other sources, including peer-reviewed journals, technical reports, and academic books. This strategy was not only intended to retrieve a comprehensive range of sources, but also to determine whether a coherent psychological or psychiatric profile of Wolfram syndrome (WS) emerges from the existing literature [16].
The following Boolean search query was used:
(“Wolfram syndrome” OR “DIDMOAD syndrome”) AND (“cognitive” OR “cognition” OR “cognitive function” OR “neuropsychological assessment” OR “cognitive impairment” OR “executive function” OR “psychological” OR “psychiatric” OR “mental health” OR “behavioral health” OR “depression” OR “anxiety” OR “mood disorder” OR “emotional dysfunction”).This query was implemented in the following international databases: Scopus, Web of Science (WoS), Dialnet, PsycInfo, PsicoDoc, and ScienceDirect.
The sample assessed with the DEX questionnaire included 28 individuals with a genetically and clinically confirmed diagnosis of Wolfram Syndrome (46.4% female), with a mean age of 24.4 years (SD = 9.7). All participants met the cognitive requirements to complete the questionnaire, either independently or with caregiver assistance [14].
Rationale for methodological selection: In contrast to traditional hypothesis-driven research, this study integrates qualitative synthesis with exploratory empirical data to construct a biologically plausible hypothesis. The scoping review was not intended to generate statistical inferences, but rather to identify psychological patterns and recurring psychiatric manifestations that may indicate a shared neurobiological mechanism in Wolfram syndrome (WS).
Within this framework, the Dysexecutive Questionnaire (DEX) was not employed as a diagnostic instrument per se, but rather as a conceptual probe—a means to evaluate whether the behaviors observed in WS are consistent with established patterns of prefrontal-executive dysfunction. Given the hypothesis that WFS1 mutations induce endoplasmic reticulum (ER) stress, resulting in neurotransmitter dysregulation, the DEX offers an indirect yet meaningful behavioral measure [15].
Thus, this methodological combination supports the theoretical framework proposed in this study, effectively bridging molecular hypotheses with real-world psychological profiles.
Search Strategy: A systematic search strategy was developed and applied across several major international databases and other sources, including peer-reviewed journals, technical reports, and academic books. This strategy was not only intended to retrieve a comprehensive range of sources, but also to determine whether a coherent psychological or psychiatric profile of Wolfram syndrome (WS) emerges from the existing literature [16].The following Boolean search query was used: (“Wolfram syndrome” OR “DIDMOAD syndrome”) AND (“cognitive” OR “cognition” OR “cognitive function” OR “neuropsychological assessment” OR “cognitive impairment” OR “executive function” OR “psychological” OR “psychiatric” OR “mental health” OR “behavioral health” OR “depression” OR “anxiety” OR “mood disorder” OR “emotional dysfunction”).This query was implemented in the following international databases: Scopus, Web of Science (WoS), Dialnet, PsycInfo, PsicoDoc, and ScienceDirect.
Inclusion and Exclusion Criteria: Inclusion and Exclusion Criteria: Studies were included if the term Wolfram syndrome appeared in the title, abstract, or keywords; addressed cognitive, psychological, or psychiatric aspects of the condition; and were peer-reviewed journal articles, books, conference papers, or proceedings published in English, Spanish, or Portuguese. Animal-model studies and studies focused solely on caregivers rather than patients were excluded.
For the empirical component, participants were included if they had a genetically and clinically confirmed diagnosis of Wolfram syndrome (WFS1 mutation), were 12 years of age or older, had sufficient cognitive capacity to complete the DEX (with caregiver assistance if needed), and provided written informed consent. Participants who did not meet these criteria—specifically those under 12 years of age, those without genetic confirmation of WS, or those lacking the cognitive ability to complete the questionnaire—were excluded from the study.
The selection process for the scoping review was conducted in two phases. First, titles and abstracts were screened. Then, full-text evaluations were performed for potentially eligible articles. The total number of studies selected after applying these criteria is summarized in Table 1 [16].
For the empirical component, participants were included if they had a genetically and clinically confirmed diagnosis of Wolfram syndrome (WFS1 mutation), were 16 years of age or older, had sufficient cognitive capacity to complete the DEX (with caregiver assistance if needed), and provided written informed consent. Participants who did not meet these criteria—specifically those under 16 years of age, those without genetic confirmation of WS, or those lacking the cognitive ability to complete the questionnaire—were excluded from the study.
A standardized data extraction form was developed using Microsoft Excel to systematically collect relevant information from the selected studies. Extracted data included study design, sample characteristics, main findings, and conclusions. The aim was not to enable statistical meta-analysis, but rather to identify conceptually consistent patterns supporting the study’s central hypothesis [16].
Following data extraction, a descriptive and analytical synthesis was performed. Information was then organized coherently to enhance interpretability. Rather than focusing on methodological quality or effect sizes, the emphasis was placed on conceptual patterns relevant to the cognitive and psychiatric dimensions of Wolfram syndrome (WS). This strategy enabled a systematic exploration of psychological conditions in WS, aiming to identify thematic categories that support a neuropsychological interpretation—particularly regarding executive dysfunction and emotional dysregulation. This led to the identification of several conceptual categories summarizing key patterns in the reviewed literature (see Table 2).
Quality Assessment: Although scoping reviews do not typically include formal methodological quality assessments, the relevance and consistency of findings were evaluated in relation to the research question. Instead of standardized checklists, study selection prioritized conceptual coherence with the central hypothesis concerning frontal-executive involvement in Wolfram syndrome (WS). This approach ensured that the synthesized results were both conceptually meaningful and aligned with the study objectives.
Instrument Characteristics: Dysexecutive Questionnaire (DEX)
The Dysexecutive Questionnaire (DEX) [15] is a 20-item instrument used to supplement the primary tests of the Behavioral Assessment of the Dysexecutive Syndrome (BADS). It evaluates various dimensions of executive function, including abstract thinking deficits, impulsivity, confabulation, planning difficulties, euphoria, temporal sequencing problems, lack of insight, apathy, disinhibition, impulse control issues, superficial emotional responses, aggression, social disengagement, perseveration, restlessness, failure to inhibit responses, dissociation between knowledge and behavior, distractibility, poor decision-making, and disregard for social norms.Each item is rated on a 5-point Likert scale ranging from “never” to “very frequently.” Original factor analysis identified five orthogonal dimensions: inhibition, intentionality, executive memory, and two related to affective and personality changes, labeled as positive affect and negative affect. The first three were correlated with scores from other neuropsychological assessments, while the latter two showed no such association. Nonetheless, certain relevant neurocognitive aspects may not be fully captured by executive performance tasks [18].
The selection of the DEX in this study is based not only on its psychometric robustness but also on its theoretical relevance to prefrontal dysfunction linked to WFS1 mutations. Its emphasis on real-world executive deficits makes it particularly valuable for examining behavioral expressions of deeper neurobiological impairments. A validated Spanish version of the DEX was previously published by Pedrero et al. [19,37]. Although the adult version of the DEX is commonly used from age 15 onward, in this study it was administered to participants aged 12 years and older, with minor linguistic adaptations to facilitate comprehension where needed. All responses were evaluated using the standard adult scoring criteria.
Ethics considerations: The study adhered to the ethical standards set forth in the Declaration of Helsinki. Approval was obtained from the Research Ethics Committee of the Province of Almería (approval number AP-0009-2020-C1-F2, internal code 2/2021). Written informed consent was obtained from all participants or, when applicable, their legal guardians, prior to inclusion. Participant anonymity and data confidentiality were strictly maintained during all phases of data collection and analysis. These safeguards were particularly critical given the vulnerable nature of the clinical population and the exploratory design of the psychological hypothesis.
Conflict of interest statement: The authors declare that they have no conflicts of interest related to this study.
Results
The review of available studies was conducted to identify patterns of psychological and psychiatric disturbances associated with Wolfram Syndrome (WS), rather than to provide exhaustive epidemiological representation. The objective was to delineate dysfunctions potentially supportive of the central neuropsychological hypothesis.
The analysis led to the development of several functional categories (Table 3), grouped according to altered functional domains. These categories were conceptually organized based on domains likely modulated by prefrontal cortex activity and associated neurotransmitter systems.
Symptoms such as apathy, impulsivity, and emotional dysregulation appeared consistently across studies, reinforcing their potential centrality to the WS cognitive-behavioral phenotype. This overlap suggests that certain symptoms may reflect both psychological and psychiatric dimensions, justifying their inclusion in multiple categories. These findings provide a synthesis of current evidence and serve as a foundation for articulating new mechanistic hypotheses.
A total of 27 articles were included in the analysis. While some adopted a multidisciplinary approach, few provided conclusive insights into the quality of life of patients and caregivers. Notably, none demonstrated a direct causal relationship between WS and specific psychological or psychiatric disorders [16].
Nevertheless, a consistent pattern of associations emerged linking WFS1 gene mutations to a broad spectrum of psychological and psychiatric manifestations—among them depression, anxiety, suicidal behavior, behavioral alterations (such as chronic fatigue syndrome, hypersomnolence, impulse control deficits, and aggression), and severe psychiatric conditions including psychosis and bipolar disorder [6,7,8,9,11,14,16,20,24] (Figure 1).
Despite their varied presentation, these symptoms appear to converge on a common neuropsychological substrate, likely reflecting disruption of executive and affective regulation circuits. This supports the central hypothesis of a frontal-executive syndrome rooted in WFS1-mediated molecular pathology.
Mutations in the WFS1 gene are known to disrupt numerous cellular processes, including cytokine regulation, neurotransmitter synthesis—particularly serotonin—acetylcholinesterase activity, and hormonal signaling pathways. These molecular alterations converge in the endoplasmic reticulum (ER), where WFS1 dysfunction leads to calcium imbalance and sustained ER stress, ultimately triggering apoptosis in vulnerable cell populations. This cascade results in the clinical constellation observed in Wolfram Syndrome (WS), which includes diabetes mellitus, optic atrophy, deafness, hypogonadism, and notably, neuropsychiatric symptoms.
Particularly relevant is the impact on the central nervous system, where ER stress, serotonergic dysregulation, and impaired cholinergic signaling collectively compromise mood and cognitive control. Serotonin depletion, exacerbated by altered tryptophan metabolism, has been associated with symptoms of depression and anxiety [11,12,21]. Similarly, degeneration of acetylcholine pathways contributes to cognitive and behavioral impairments such as irritability, inattention, and memory deficits [25,28].
This biochemical triad—ER stress, serotonin imbalance, and cholinergic dysfunction—may constitute the neurobiological foundation of the behavioral phenotype observed in WS.
Functional Category 1 – Anxiety and Depression Disorders
Wolfram Syndrome (WS) is associated with a wide range of psychiatric symptoms, particularly among carriers of WFS1 mutations. Clinical studies consistently report anxiety, depression, hypersomnolence, and suicidal tendencies. Sequeira et al. identified a strong correlation between WFS1 mutations and depressive states [22], while Rosanio et al. observed panic attacks and severe depression exclusive to individuals with WFS1 mutations, but not those with WFS2 [27]. Similar psychiatric symptoms have also been documented in heterozygous carriers [11,12].
The biological underpinnings appear to involve disruptions in tryptophan metabolism and acetylcholinesterase activity—both critical to emotional regulation and executive functioning [25,28]. Additionally, the chronic somatic symptoms inherent to WS further contribute to the overall psychological burden [5].
These findings support the hypothesis that the psychiatric manifestations of WS are not incidental, but instead represent neurobiologically embedded outcomes of WFS1-driven cellular dysfunction (Figure 2).
Functional Category 2 - Suicidal and Aggressive Behaviors
Wolfram Syndrome (WS) has been associated with an increased prevalence of suicidal and aggressive behaviors, likely due to a complex interplay between genetic predisposition and neuropsychiatric vulnerability. Several studies have reported a marked increase in suicide attempts and psychiatric hospitalizations among individuals with WS, with Bischoff et al. highlighting the severity of these complications [5,24,26,38]
Swift et al. observed a higher frequency of suicide attempts in heterozygous WFS1 mutation carriers, suggesting that even partial gene expression may confer neuropsychiatric risk [11]. Nanko et al. later reported that psychiatric disturbances appeared even more frequently in homozygous individuals [23].
Regarding aggressive behavior, Swift et al. documented recurrent episodes of verbal and physical aggression, particularly among homozygous patients, many of whom were also diagnosed with psychiatric comorbidities such as antisocial personality disorder and psychosis [12]. Deficits in impulse control were especially prominent in this group.
Building on these findings, Rosanio et al. confirmed that individuals with homozygous WFS1 mutations not only exhibited a heightened propensity for aggression but also experienced more severe episodes [27]. These behavioral patterns have been associated with dysregulation of neurotransmitters such as dopamine and serotonin, further reinforcing the hypothesis of a neurochemical basis rooted in WFS1-related dysfunction.
Taken together, these findings support the notion that WFS1 mutations may increase susceptibility to suicidal and aggressive behaviors, particularly in interaction with environmental and psychological stressors. This aligns with the broader hypothesis that executive and emotional dysregulation in WS arises from a distinct neurobiological substrate (Figure 3).
Functional category 3 - Severe Psychological and Psychiatric Disorders
Mutations in the WFS1 gene have been associated with the emergence of psychotic and schizophrenia-like symptoms, suggesting a direct link between genetic dysfunction and severe neuropsychiatric alterations [22,27]. In bipolar disorder, symptom onset has been linked to both endocrine and cognitive dysfunction, including disruption of the hypothalamic-pituitary-adrenal (HPA) axis and impaired synaptic plasticity—processes that may be exacerbated by the loss of function in wolframin, the protein encoded by WFS1 [21].
From a biochemical perspective, WFS1 plays a critical role in maintaining endoplasmic reticulum (ER) homeostasis and regulating cellular stress responses. Its dysfunction results in sustained activation of the unfolded protein response (UPR), particularly through the PERK–eIF2α–ATF4 pathway, which promotes neuronal apoptosis [32].
Neurochemically, decreased acetylcholinesterase (AChE) activity has been observed, potentially disrupting cholinergic signaling pathways essential for cognitive integrity and emotional regulation—two domains commonly impaired in psychosis and mood disorders [28]. In addition, ER stress–related mitochondrial dysfunction may contribute to neuroinflammation and progressive neuronal loss, particularly in limbic structures, thereby increasing psychiatric vulnerability in individuals with WS. [39]
Taken together, the clinical severity, neurofunctional implications, and biologically grounded etiology of these disturbances support classifying WS within the domain of Severe Psychological and Psychiatric Disorders, particularly in clinical contexts where cognitive and emotional function is central to patient management (Figure 4).
Functional Category 4 – Chronic Fatigue Syndrome
Wolfram Syndrome (WS) has been associated with elevated levels of inflammatory cytokines in the bloodstream of affected individuals [33]. Cytokines such as interleukin-6 (IL-6) and tumor necrosis factor-alpha (TNF-α), which regulate immune and inflammatory responses, appear to play a key role in the pathophysiology of the syndrome [32].
In WS, increased levels of these pro-inflammatory markers have been linked to chronic inflammation, cellular stress, and accelerated neuronal apoptosis. Wang et al. observed that heightened immune activation in these patients may contribute directly to neurodegeneration, likely through cytokine-mediated neuronal toxicity and sustained glial activation [29].
Panfili et al. further emphasized the role of WFS1 in modulating apoptotic and stress-response pathways, proposing that its dysfunction initiates a cascade of inflammatory signaling that disrupts cellular homeostasis across multiple systems [32]. [40]
This chronic systemic inflammation may represent the biological substrate of fatigue-like symptoms frequently reported by WS patients. The overlap with fatigue syndromes observed in post-viral conditions such as long COVID supports the hypothesis that cytokine dysregulation and neuroimmune activation constitute a shared mechanistic axis [34,35]. [41]
Collectively, these findings suggest that WS may include a chronic fatigue component rooted in neuroinflammatory and metabolic dysfunction, expanding its clinical phenotype and reinforcing the need for immune-targeted therapeutic strategies (Figure 5).
Impact of Hypogonadism
Endocrine dysfunction represents another key factor contributing to the psychological burden observed in Wolfram Syndrome (WS) [36]. Hypogonadism, commonly reported in these patients, results from impaired hormonal signaling within the hypothalamic-pituitary-gonadal axis, causing decreased levels of sex hormones, including testosterone and estrogen [34].
These hormonal deficiencies negatively affect mood, energy levels, and motivation, exacerbating symptoms such as depression, apathy, and fatigue. Importantly, such endocrine imbalances may intensify preexisting neurotransmitter dysregulation, further amplifying affective and cognitive symptoms.
Additionally, extensive neurodegeneration—particularly affecting regions such as the cerebellum (involved in motor coordination) and the prefrontal cortex (essential for emotional regulation and executive functioning)—further compromises emotional stability. This structural deterioration, combined with oxidative stress and neuronal apoptosis, likely impairs the brain’s capacity for emotional modulation, frequently resulting in irritability, anxiety, and emotional dysregulation [13].
Collectively, the interplay among hormonal deficits, neurotransmitter imbalances, and structural brain alterations may account for a substantial portion of the psychiatric phenotype in WS. Thus, careful consideration of neuroendocrine interactions is crucial for understanding and treating the psychological manifestations of this syndrome.
Results and interpretation of data DEX: In the cohort of patients with Wolfram Syndrome (WS) included in this analysis, 46.4% were women (13 individuals) and 53.6% men (15 individuals), with a mean age of 24.4 years (SD = 9.7). Regarding cognitive functioning, 46.4% had a high IQ, 32.1% fell within the normal range, 14.3% were classified as low-average, 3.6% were also classified as low-average (possibly a duplication that should be clarified), and 3.6% showed signs of intellectual disability. Overall, 10.7% of the sample exhibited symptoms of cognitive impairment.
In terms of educational level, 32.1% had completed higher education, another 32.1% had basic education, 10.7% had middle-level studies, 14.3% were at an age-appropriate educational level, 7.1% had medium-level education, and 3.6% were reported to be one academic year behind.
The results from the Dysexecutive Questionnaire (DEX) administered to individuals with WS demonstrated a consistent pattern of executive dysfunction, with impairments observed across multiple domains. These findings highlight significant neuropsychological difficulties that notably affect everyday behavior and functioning, as summarized in Table 4 and Table 5.
Most notably, there was a pronounced disruption in inhibitory control, as evidenced by elevated scores on DEX items such as acting without thinking (item 2), difficulty stopping repetitive behaviors or speech (item 14), and inability to inhibit inappropriate actions despite awareness of their inappropriateness (item 16). This profile of impulsivity is classically associated with dysfunction in prefrontal brain regions, particularly the orbitofrontal cortex, which is essential for behavioral flexibility and social appropriateness.
Difficulties in emotional regulation were also prevalent, illustrated by inappropriate emotional expressions (item 11) and over-reactivity to minor stimuli (item 12). These symptoms may compromise social integration and likely reflect dysregulation of frontal-limbic circuitry.
Additionally, deficits in planning and decision-making (items 4 and 19) were observed, indicating a reduced capacity to anticipate outcomes, organize actions, and formulate effective strategies—all of which are core components of goal-directed behavior. These impairments can significantly limit autonomy and adaptive functioning.
Attention-related deficits (item 18) were also notable, particularly regarding sustained attentional focus, suggesting possible dysfunction in the dorsolateral prefrontal cortex or its attentional network connections. High scores on lack of motivation (item 8), often interpreted as apathy, may reflect executive initiation deficits rather than primary affective disorders.
Collectively, these findings point to a global impairment of executive functioning consistent with a frontal-executive syndrome driven by progressive neurodegeneration in WS [5]. This constellation of deficits provides empirical support for the hypothesis that WFS1 dysfunction compromises higher-order cognitive and emotional regulation via prefrontal network disruption.
Importantly, despite significant impairments in domains such as impulse control, planning, emotional regulation, and sustained attention, core capacities related to social awareness and reality monitoring remained relatively preserved in most individuals. Participants with WS generally retained the ability to recognize social norms, understand interpersonal consequences, and distinguish real experiences from delusions or hallucinations.
This preservation of social judgment and reality orientation stands in contrast to the cognitive disorganization typically observed in psychotic disorders. There was no evidence of severely disorganized thinking or behavior, nor of profound global cognitive dysfunction.
Therefore, the executive profile observed in this cohort does not align with a psychotic or diffusely disorganized syndrome, but rather reflects a moderate dysexecutive syndrome, consistent with focal frontal dysfunction in the absence of a global collapse of reasoning or perceptual coherence.
Based on DEX questionnaire responses, behavior frequency was categorized as “rarely,” “hardly ever,” and “sometimes.” While participants acknowledged some difficulties in attention, inhibition, and emotional control, these were mostly reported as infrequent. This is reflected in low average scores and narrow standard deviations (see Table 4). The overall frequency pattern is summarized in Figure 6, indicating that most executive impairments were reported as occurring “rarely.” These findings support the notion that, although Wolfram Syndrome (WS) compromises executive function, it does not uniformly impair self-awareness or behavioral regulation. Instead, the data point to a selective frontal-executive impairment, rather than a pervasive neuropsychiatric disorder—a profile previously described by Bischoff et al. [5] and Reiersen et al. [7].
These observations, however, should be interpreted with caution. Although the pattern suggests relatively preserved social reasoning and behavioral coherence, intermittent executive lapses—particularly under cognitively demanding conditions—should not be underestimated. Even subclinical impairments, when compounded by environmental stressors or disease progression, may significantly impact functional capacity in academic, occupational, or social contexts [8,29]. Such subtle deficits often remain undetected in standard evaluations, yet may impose a cumulative burden over time. Given the progressive neurodegenerative course of WS, ongoing monitoring of executive and emotional functions is essential. Longitudinal assessment may facilitate early detection of functional decline and the timely implementation of targeted cognitive or behavioral interventions before more disabling symptoms emerge.
Discussion
The findings of this study support the hypothesis that Wolfram syndrome (WS) imposes a substantial psychological and neurocognitive burden that exceeds the multisystemic organic deterioration traditionally associated with the disease. The executive dysfunction pattern identified through the Dysexecutive Questionnaire (DEX) indicates a selective disruption of frontal lobe circuitry, impairing core cognitive domains such as planning, impulse control, emotional regulation, and sustained attention—features reminiscent of those observed in Huntington disease [43]. A similar executive profile has also been described in mental disorders such as schizophrenia [44]. Although initially subclinical, these deficits tend to intensify as the neurodegenerative process advances. [45]
The scoping review further corroborates the consistent presence of psychiatric symptoms—including anxiety, depression, apathy, and behavioral dysregulation—associated with WFS1 mutations. This link is supported by both molecular mechanisms (e.g., endoplasmic reticulum [] stress, serotonin pathway dysregulation) and empirical clinical evidence [5,46].
Psychological manifestations in WS overlap with those found in other rare genetic and neurodegenerative conditions, including Prader–Willi syndrome and cystic fibrosis. For example, a systematic review and meta-analysis reported a prevalence of depression and anxiety in adults with cystic fibrosis of 27.2% and 28.4%, respectively, indicating a significant psychological burden [47]. In Prader–Willi syndrome, cognitive and behavioral impairments—such as attentional deficits, compulsive behaviors, and mood disorders—are also common [48]. However, WS appears to involve a more complex and multifactorial etiology, characterized by the convergence of genetic, neuroendocrine, and psychosocial factors. A defining feature of WS is the direct interaction between WFS1 mutations and critical neurotransmitter systems, including serotonin and acetylcholine, which may account for the high prevalence of mood disturbances and impulse control deficits in these individuals [49].
Importantly, recent research has also suggested that WFS1 dysfunction may affect circadian rhythms, particularly sleep regulation and the temporal organization of cognitive and emotional processes. Caruso and Rigoli [46] emphasized that WFS1 is implicated in sleep disorders and possibly in melatonin signaling disruption. These findings open the door to a circadian interpretation of emotional dysregulation and fatigue-like symptoms observed in WS. Given that many executive functions—such as attention and impulse control—follow diurnal fluctuations, alterations in the circadian system could exacerbate cognitive and affective impairments in this population.
Given the executive profile identified—particularly impairments in inhibition, planning, and attentional control—these findings may inform the development of targeted therapeutic strategies. Metacognitive training programs aimed at enhancing self-regulation and strategic planning may serve as cognitive scaffolding [50,52], while psychoeducational support for caregivers could mitigate the family burden during phases of functional decline [51]. These strategies, already implemented in other clinical contexts, may also benefit individuals with WS; however, this remains an area in need of further development.
Routine neuropsychological screening using instruments such as the DEX should become a standard component of clinical follow-up. Ideally, it should be complemented by performance-based assessments, such as the Wisconsin Card Sorting Test (WCST) or the Stroop Test, alongside structured clinical interviews targeting executive function (e.g., the D-KEFS battery), to provide a comprehensive cognitive profile.
Although some studies mention the emotional burden experienced by families, no research to date has specifically examined the mental health of primary caregivers of individuals with WS. Nor have family-based intervention models been developed or evaluated for efficacy in this population. Given the high levels of functional dependence typically observed in advanced stages of the disease, this gap is notable, as caregiver overload poses substantial risks to both caregiver well-being and patient outcomes [53].
This study has limitations, including its small sample size and reliance on the DEX, a self-report instrument that, while informative, remains inherently subjective. Furthermore, many of the included studies lack methodological consistency and often report psychological findings as secondary outcomes. The absence of longitudinal data also limits the ability to monitor the progression of executive dysfunction over time.
Future research should adopt a biopsychosocial framework that integrates the neurobiological substrates of WS with psychological resilience and family system dynamics. There is a critical need to evaluate structured psychological interventions—such as cognitive behavioral therapy or mindfulness-based approaches—tailored to the cognitive profile observed in this population. Additionally, grounding these interventions in theoretical models such as Barkley’s executive self-regulation theory or the frontal systems theory of Stuss and Benson may help define more precise rehabilitation targets and improve clinical outcomes. These frameworks offer valuable tools to better understand the spectrum of executive dysfunction in WS and to inform the design of more personalized and effective treatment plans.
Conclusions
The findings of this exploratory study suggest that most individuals with Wolfram Syndrome (WS) exhibit stable behavioral and emotional regulation, characterized by low impulsivity, preserved communicative comprehension, realistic thought patterns, and a general sense of self-control. Mean scores and standard deviations on the Dysexecutive Questionnaire (DEX) indicate that significant executive dysfunction is not predominant in this sample. When difficulties are reported, they tend to be sporadic—typically involving attentional lapses or arousal regulation issues—and are perceived as occasional rather than persistent or debilitating.
Nonetheless, these results should be interpreted cautiously given persistent gaps in the literature regarding the psychological and neurocognitive profile of WS. Most existing studies prioritize biological and physiological aspects, often treating psychological findings as secondary. Furthermore, while the genetic and cellular basis of WS is relatively well established—especially WFS1-related ER stress and neurodegeneration—the downstream pathways leading to psychiatric symptoms remain poorly understood. Notably, recent research suggests that WFS1 mutations may disrupt circadian regulation and sleep architecture, potentially exacerbating cognitive and emotional symptoms through chronobiological mechanisms [46].
Another key variable rarely addressed is the influence of caregiver dynamics and family systems, which may shape the trajectory of psychological resilience or vulnerability in WS. WS thus represents a valuable, though underutilized, model for exploring the neuropsychiatric dimensions of rare genetic syndromes—including how endocrine, circadian, and neurochemical disruptions converge on executive function and emotional regulation.
While most participants report a general sense of psychological well-being and only mild executive challenges, these findings highlight the need for more comprehensive, longitudinal, and interdisciplinary studies. Future research should define psychological phenotypes within WS, investigate the role of chronobiological and neuroendocrine factors, and validate interventions tailored to the cognitive and emotional needs of these individuals. Addressing these gaps may not only enhance clinical care for WS but also inform broader models of brain–behavior relationships in rare neurogenetic disorders.
Visual and cognitive deterioration tend to progress concurrently in WS, with optic neuropathy representing one of the earliest markers of neurological decline [54].
Funding
This article is part of the project “Evaluation of the effectiveness of a biopsychosocial intervention plan applied through ICTs to improve the quality of life of people affected by rare diseases (AP-0009-2020-C1-F2)”, funded by the Andalusian Public Health System (Conv. FPS 2020).
Author information
Conceptualization, G.E.-B., and A.J.S; methodology, G.E.-B., A.J.S., J.L.F-M. and J.R.C.; data curation, G.E.-B., A.J.S., J.L.F-M. and J.R.C.; writing—original draft preparation, G.E.-B., A.J.S., J.L.F-M., E.F.V. and J.R.C.; writing—review and editing, G.E.-B., A.J.S., J.L.F-M., E.F.V. and J.R.C.; project administration, G.E.-B.; funding acquisition, G.E.-B.
Ethical Standards
The study was conducted in accordance with the Declaration of Helsinki and was approved
by the Ethics Committee of Research Almería Center (protocol code wolfram15 on 29 April 2016).
Informed Consent Statement
Informed consent was obtained from all the subjects involved in the study.
Data Availability Statement
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request. Due to the sensitive nature of the data involving patients with rare diseases, access may be restricted to protect participant confidentiality.
Acknowledgements
The authors thank the Spanish Association for Research and Help to Wolfram Syndrome for its support in this research. We also express our deepest gratitude to the individuals and families affected by Wolfram Syndrome who participated in or supported this study.
Conflicts of Interest
The authors declare that they have no financial interest directly or indirectly related to the work submitted for publication.
References
- Esteban Bueno G, Fernández Martínez JL. Gonadal Dysfunction in Wolfram Syndrome: A Prospective Study. Diagnostics. 2025;15:1594. [CrossRef]
- Hardy C, Khanim F, Torres R, Scott-Brown M, Seller A, Poulton J, Collier D, Kirk J, Polymeropoulos M, Latif F, Barrett T. Clinical and molecular genetic analysis of 19 Wolfram syndrome kindreds demonstrating a wide spectrum of mutations in WFS1. Am J Hum Genet. 1999;65(5):1279–1290. [CrossRef]
- Bueno GE, Ruiz-Castañeda D, Martínez JR, Muñoz MR, Alascio PC. Natural history and clinical characteristics of 50 patients with Wolfram syndrome. Endocrine. 2018;61(3):440–446. [CrossRef]
- Esteban-Bueno G, Berenguel Hernández AM, Fernández Fernández N, Navarro Cabrero M, Coca JR. Neurosensory Affectation in Patients Affected by Wolfram Syndrome: Descriptive and Longitudinal Analysis. Healthcare. 2023;11(13):1888. [CrossRef]
- Bischoff AN, Reiersen AM, Buttlaire A, Al-Lozi A, Doty T, Marshall BA, Hershey T; Washington University Wolfram Syndrome Research Group. Selective cognitive and psychiatric manifestations in Wolfram Syndrome. Orphanet J Rare Dis. 2015;10:66. [CrossRef]
- Swift RG, Sadler DB, Swift M. Psychiatric findings in Wolfram syndrome homozygotes. Lancet. 1990;336(8721):667–669. [CrossRef]
- Reiersen AM, Noel JS, Doty T, Sinkre RA, Narayanan A, Hershey T. Psychiatric Diagnoses and Medications in Wolfram Syndrome. Scand J Child Adolesc Psychiatr Psychol. 2022;10(1):163–174. [CrossRef]
- Swift M, Gorman Swift R. Psychiatric disorders and mutations at the Wolfram syndrome locus. Biol Psychiatry. 2000;47(9):787–793. [CrossRef]
- Wilson BA, Alderman N, Burgess PW, Emslie H, Evans JJ. Behavioural Assessment of the Dysexecutive Syndrome. Thames Valley Test Company; 1996.
- Gerstorf D, Siedlecki KL, Tucker-Drob EM, et al. Executive dysfunctions across adulthood: Measurement properties and correlates of the DEX self-report questionnaire. Aging Neuropsychol Cogn. 2008;15(4):424–445. [CrossRef]
- Fonseca SG, Fukuma M, Lipson KL, Nguyen LX, Allen JR, Oka Y, Urano F. WFS1 is a novel component of the unfolded protein response and maintains homeostasis of the endoplasmic reticulum in pancreatic β-cells. J Biol Chem. 2005;280(47):39609–39615. [CrossRef]
- Hao X, Zhou Y, Park D, et al. Wolfram syndrome 1 regulates sleep in dopamine receptor neurons via ER-mediated calcium homeostasis. PLoS Genet. 2023;19(3):e1010827. [CrossRef]
- Ferreras C, Gorito V, Pedro J, et al. Wolfram syndrome: Portuguese research. Endokrynol Pol. 2021;72(4):353–356. [CrossRef]
- Uhlenbusch N, Löwe B, Depping MK. Correlates of depression and anxiety in patients with different rare diseases. J Psychosom Res. 2018;109:142. [CrossRef]
- Uhlenbusch N, Löwe B, Härter M, Schramm C, Weiler-Normann C, Depping MK, et al. Depression and anxiety in patients with different rare chronic diseases: a cross-sectional study. PLoS One. 2019;14(2):e0211343. [CrossRef]
- Silva P, Cedres L, Vomero A, et al. Síndrome de Wolfram. Rev Esp Endocrinol Pediatr. 2019;10(2):74–80. [CrossRef]
- Pedrero Pérez EJ, Olivar Arroyo L, Morales Alonso S, et al. Versión española del Cuestionario de Disfunción Ejecutiva (DEX-Sp): propiedades psicométricas en población clínica. Rev Neurol. 2009;48(4):193–198. [CrossRef]
- Welschen D, Peralta C, Estela M, et al. Síndrome de Wolfram: reporte de casos. Oftalmol Clin Exp. 2015;8(1):29–38.
- Ferreira VFS, Campos CR, Furtado AM, et al. Wolfram syndrome: A case report. Res Soc Dev. 2021;10(6):e52410616116. [CrossRef]
- Nanko S, Yokoyama H, Hoshino Y, et al. Organic mood syndrome in two siblings with Wolfram syndrome. Br J Psychiatry. [CrossRef]
- Swift RG, Perkins DO, Chase CL, et al. Psychiatric disorders in 36 families with Wolfram syndrome. Am J Psychiatry. [CrossRef]
- Xavier J, Bourvis N, Tanet A, et al. Bipolar Disorder Type 1 in a 17-Year-Old Girl with Wolfram Syndrome. J Child Adolesc Psychopharmacol. [CrossRef]
- Chatterjee SS, Mitra S, Pal SK. Mania in Wolfram’s disease: From bedside to bench. Clin Psychopharmacol Neurosci. [CrossRef]
- Sequeira A, Kim C, Seguin M, et al. Wolfram syndrome and suicide: Evidence for a role of WFS1 in suicidal and impulsive behavior. Am J Med Genet B Neuropsychiatr Genet. 2003;119B(1):108–113. [CrossRef]
- Nickl-Jockschat T, Kunert HJ, Herpertz-Dahlmann B, et al. Psychiatric symptoms in a patient with Wolfram syndrome caused by a combination of thalamic deficit and endocrinological pathologies. Neurocase. [CrossRef]
- Swift M, Gorman Swift R. Wolframin mutations and hospitalization for psychiatric illness. Mol Psychiatry. [CrossRef]
- Owen, MJ. Psychiatric disorders in Wolfram syndrome heterozygotes. Mol Psychiatry. [CrossRef]
- Rigoli L, Caruso V, Aloi C, Salina A, Maghnie M, d'Annunzio G, et al. An Atypical Case of Late-Onset Wolfram Syndrome 1 without Diabetes Insipidus. Int J Environ Res Public Health. [CrossRef]
- Kitamura RA, Maxwell KG, Ye W, et al. Multidimensional analysis and therapeutic development using patient iPSC-derived disease models of Wolfram syndrome. JCI Insight. 2022;7(18):e156549. [CrossRef]
- Rosanio FM, Di Candia F, Occhiati L, et al. Wolfram Syndrome Type 2: A Systematic Review of a Not Easily Identifiable Clinical Spectrum. Int J Environ Res Public Health. 2022;19(2):1–12. [CrossRef]
- Cairns G, Burté F, Price R, O’Connor E, Toms M, Mishra R, Moosajee M, Pyle A, Sayer JA, Yu-Wai-Man P.A mutant wfs1 zebrafish model of Wolfram syndrome manifesting visual dysfunction and developmental delay. Sci Rep. [CrossRef]
- Wang Z, Wang X, Shi L, et al. Wolfram syndrome 1b mutation suppresses Mauthner-cell axon regeneration via ER stress signal pathway. Acta Neuropathol Commun. [CrossRef]
- Panfili E, Mondanelli G, Orabona C, Belladonna ML, Gargaro M, Fallarino F, et al. Novel mutations in the WFS1 gene are associated with Wolfram syndrome and systemic inflammation. Hum Mol Genet. 2021;30(3–4):265–276. [CrossRef]
- de Muijnck C, Brink JBT, Bergen AA, Verhagen M, van Genderen MM, van den Born LI, et al. Delineating Wolfram-like syndrome: A systematic review and discussion of the WFS1-associated disease spectrum. Surv Ophthalmol. [CrossRef]
- Salzano G, Rigoli L, Valenzise M. Clinical Peculiarities in a Cohort of Patients with Wolfram Syndrome 1. Int J Environ Res Public Health. [CrossRef]
- Reiersen AM, Noel JS, Doty T, Cox CL, Hershey T, Swift RG, et al. Psychiatric Diagnoses and Medications in Wolfram Syndrome. Scand J Child Adolesc Psychiatr Psychol. [CrossRef]
- Pedrero EJ, Ruiz JM, Rojo G, et al. Versión española del Cuestionario Disejecutivo (DEX-Sp): propiedades psicométricas en adictos y población no clínica. Adicciones.
- Hershey T, Lugar HM, Shimony JS, Nebes RD, Sadler B, Perantie DC, et al. Early brain vulnerability in Wolfram syndrome. PLoS One. 2012;7(7):e40604. [CrossRef]
- Shi G, Cui L, Chen R, Liang S, Wang C, Wu P, et al.. TT01001 attenuates oxidative stress and neuronal apoptosis by preventing mitoNEET-mediated mitochondrial dysfunction after subarachnoid hemorrhage in rats. Neuroreport. [CrossRef]
- Morikawa S, Blacher L, Onwumere C, Akeju Y, Merali S, Woldeyohannes L, et al. Loss of Function of WFS1 Causes ER Stress-Mediated Inflammation in Pancreatic Beta-Cells. Front Endocrinol. 2022;13:849204. [CrossRef]
- Low RN, Low RJ, Akrami A. A review of cytokine-based pathophysiology of Long COVID symptoms. Front Med. 2023;10:1011936. [CrossRef]
- Paulsen, JS. Cognitive impairment in Huntington disease: diagnosis and treatment. Curr Neurol Neurosci Rep. [CrossRef]
- Orellana G, Slachevsky A. Executive functioning in schizophrenia. Front Psychiatry. [CrossRef]
- Szablewski, L. Associations Between Diabetes Mellitus and Neurodegenerative Diseases. Int J Mol Sci. [CrossRef]
- Caruso V, Rigoli L. Beyond Wolfram Syndrome 1: The WFS1 Gene's Role in Alzheimer's Disease and Sleep Disorders. Biomolecules. 2024;14(11):1389. [CrossRef]
- Quittner AL, Goldbeck L, Abbott J, et al. Prevalence of depression and anxiety in patients with cystic fibrosis and parent caregivers. Thorax. 2014;69(12):1090–1097. [CrossRef]
- Cassidy SB, Schwartz S, Miller JL, Driscoll DJ, Butler MG, Hanchett JM, et al. Prader-Willi syndrome. Genet Med. [CrossRef]
- Visnapuu T, Raud S, Loomets M, Talvik T, Cheng L, Dierssen M, et al. Wfs1-deficient mice display altered function of serotonergic system and increased behavioral response to antidepressants. Front Neurosci. [CrossRef]
- Michalsky, T. Metacognitive scaffolding for preservice teachers' self-regulated design of higher order thinking tasks. Heliyon. 2024;10(2):e24280. [CrossRef]
- Mirhosseini S, Imani Parsa F, Moghadam-Roshtkhar H, Jafari P, Peivandi S, Lotfi M, et al. Support based on psychoeducation intervention to address quality of life and care burden among caregivers of patients with cancer. Front Psychol. [CrossRef]
- Pozuelos JP, Combita LM, Abundis A, Martínez MJ, Valero B, Soto N, et al. Metacognitive scaffolding boosts cognitive and neural benefits following executive attention training in children. Dev Sci. [CrossRef]
- Atkins JC, Padgett CR. Living with a Rare Disease: Psychosocial Impacts for Parents and Family Members – a Systematic Review. J Child Fam Stud. [CrossRef]
- Majander A, Jurkute N, Burté F, Brock K, João C, Huang H, Neveu MM, Chan CM, Duncan HJ, Kelly S, Burkitt-Wright E, Khoyratty F, Lai YT, Subash M, Chinnery PF, Bitner-Glindzicz M, Arno G, Webster AR, Moore AT, Michaelides M, Stockman A, Robson AG, Yu-Wai-Man P. WFS1-Associated Optic Neuropathy: Genotype-Phenotype Correlations and Disease Progression. Am J Ophthalmol. [CrossRef]
Figure 1.
Psychological and psychiatric manifestations associated with WFS1 mutation. Source: Author’s elaboration.
Figure 1.
Psychological and psychiatric manifestations associated with WFS1 mutation. Source: Author’s elaboration.
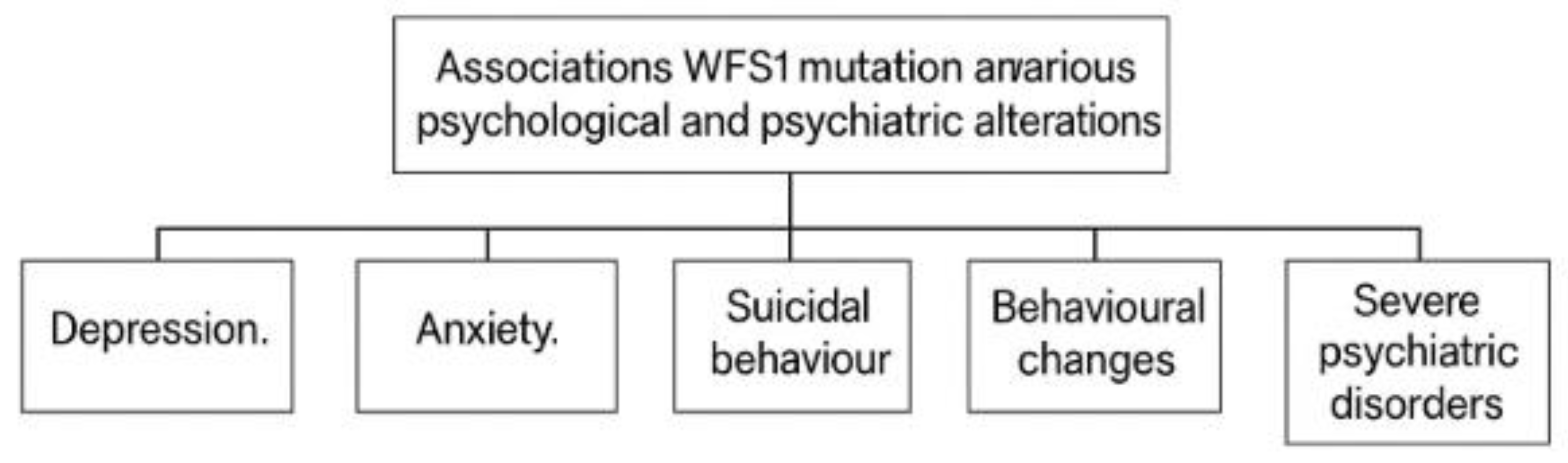
Figure 2.
Summary of functional category 1. Source: Author’s elaboration.
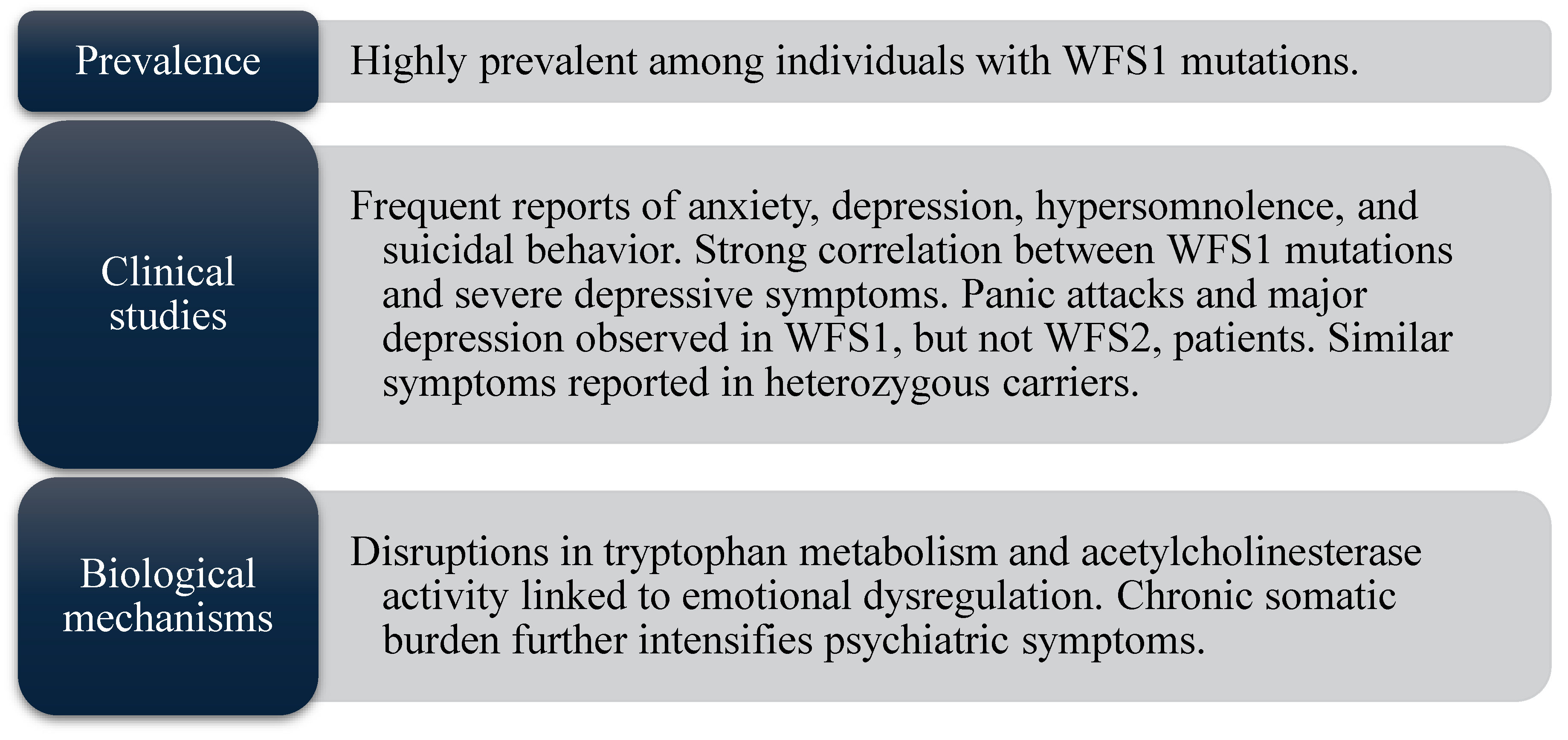
Figure 3.
Summary of functional category 2. Source: Author’s elaboration.
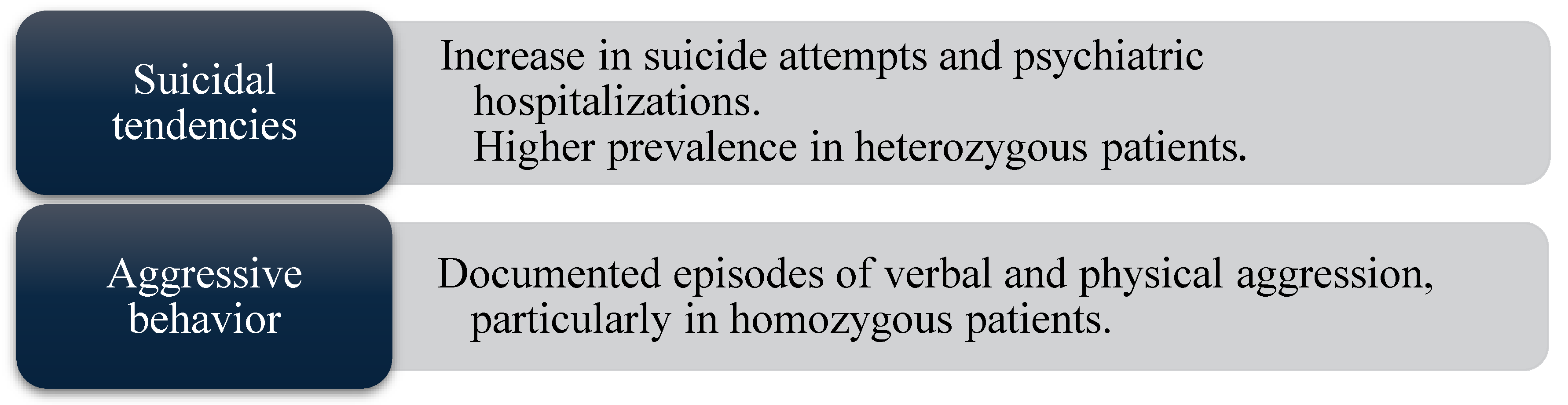
Figure 4.
Summary of functional category 3. Source: Author’s elaboration.
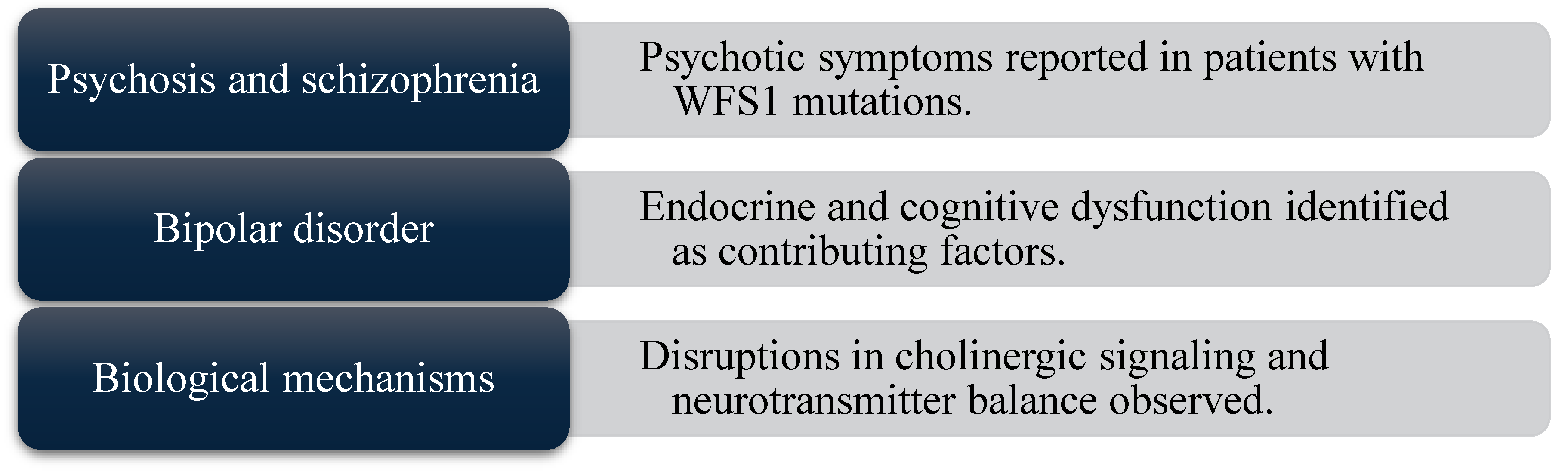
Figure 5.
Summary of functional category 4. Source: Author’s elaboration.
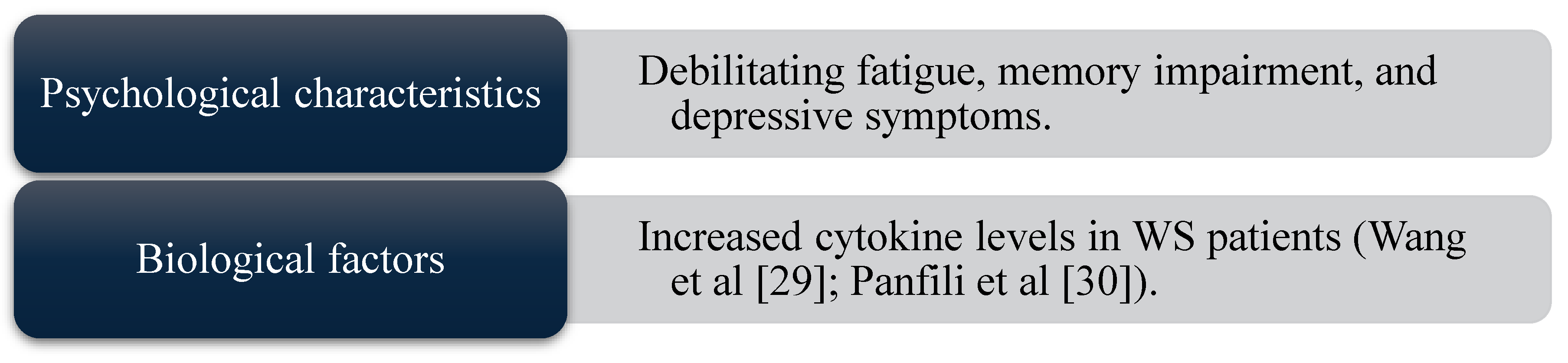
Figure 6.
Summary of main categorical findings on the DEX scale. Source: Data derived from DEX responses in the present study.
Figure 6.
Summary of main categorical findings on the DEX scale. Source: Data derived from DEX responses in the present study.
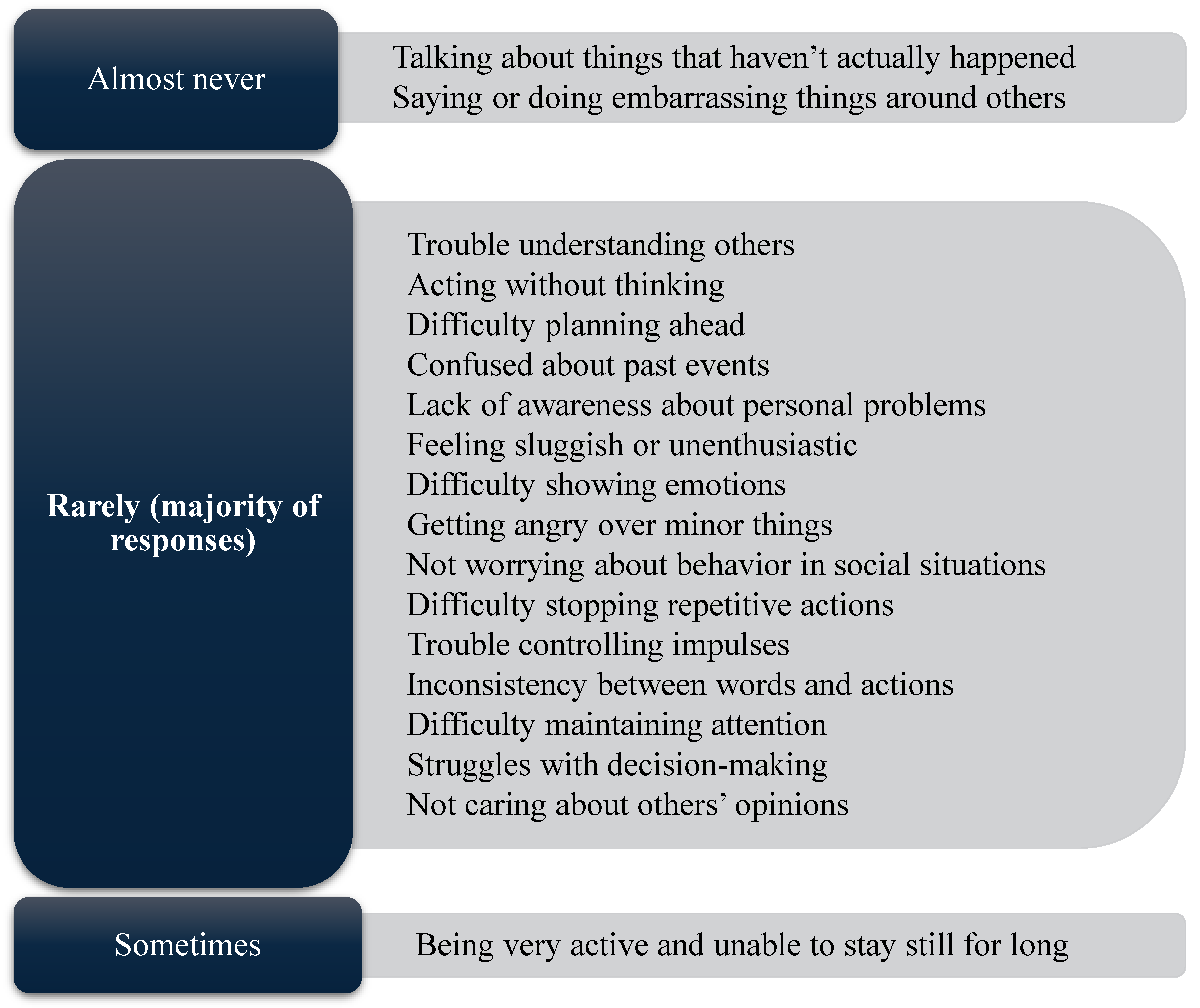

Table 1.
Documents retrieved from each database and studies meeting inclusion and exclusion criteria.
Table 1.
Documents retrieved from each database and studies meeting inclusion and exclusion criteria.
| Database | Documents Retrieved | Meeting Inclusion and Exclusion Criteria |
| Scopus | 843 | 8 |
| Web of Science | 672 | 6 |
| Dialnet | 116 | 5 |
| PsycInfo | 36 | 2 |
| PsicoDoc | 29 | 1 |
| ScienceDirect | 125 | 5 |
| Total | 1821 | 27 |
Source: Author’s elaboration.
Table 2.
References analyzed.
| TITLE | AUTHORS AND YEAR |
| Selective cognitive and psychiatric manifestations in Wolfram Syndrome | Bischoff, A.N.; Reiersen, A.M.; Butterfire, A. et al. (2015) [5] |
| Psychiatric diagnoses and treatment in Wolfram Syndrome | Reiersen, A.M.; Narayanan, A.; Sinkre, R.A. et al. (2019) [7] |
| Psychiatric findings in Wolfram syndrome homozygotes | Swift, R.G.; Sadler, D.B.; Swift M. (1990) [11] |
| Psychiatric Disorders and Mutations at the Wolfram Syndrome Locus | Swift, M.; Gorman Swift, R. (2000) [8] |
| Depression and anxiety in patients with different rare chronic diseases: A cross-sectional study | Uhlemusch, N.; Löwe, B.; Harter, M. et al. (2019) [15] |
| Correlates of depression and anxiety in patients with different rare diseases | Uhlemusch, N.; Löwe, B.; Depping, M.K. (2018) [14] |
| Síndrome de Wolfram | Silva, P., Cedres, L., Vomero, A., et al. (2019). [16] |
| Síndrome de Wolfram: reporte de casos | Welschen, D.; Peralta, C.; et al. (2015) [18] |
| Síndrome de Wolfram - Relato de caso | Ferreira, V. F. S., Campos, C. R., Furtado, A. M., et al. (2021). [19] |
| Organic mood syndrome in two siblings with Wolfram syndrome | Nanko, S., Yokoyama, H., Hoshino, Y., et al. (1992). [20] |
| Psychiatric disorders in 36 families with Wolfram syndrome | Swift, R. G., Perkins, D. O., Chase, C. L., Sadler, D. B., & Swift, M. (1991). [21] |
| Bipolar Disorder Type 1 in a -Year-Old Girl with Wolfram Syndrome | Xavier, J., Bourvis, N., Tanet, A. et al. (2016) [22] |
| Mania in wolfram’s disease: From bedside to bench | Chatterjee, S. S., Mitra, S., & Pal, S. K. (2017). [23] |
| Wolfram Syndrome and Suicide: Evidence for a Role of WFS1 in Suicidal and Impulsive Behavior | Sequeira, A., Kim, C., Seguin, M., et al. (2003). [24] |
| Psychiatric symptoms in a patient with Wolfram syndrome caused by a combination of thalamic deficit and endocrinological pathologies | Nickl-Jockschat, T., Kunert, H. J., Herpertz-Dahlmann, B., et al. (2009). [25] |
| Wolframin mutations and hospitalization for psychiatric illness | Swift, M., & Gorman Swift, R. (2005). [26] |
| Psychiatric disorders in Wolfram syndrome heterozygotes | Owen, M. J. (1998). [27] |
| An Atypical Case of Late-Onset Wolfram Syndrome 1 without Diabetes Insipidus | Rigoli, L., Caruso, V., Aloi, C., et al. (2022). [28] |
| Multidimensional analysis and therapeutic development using patient iPSC–derived disease models of Wolfram syndrome | Kitamura, R. A., Maxwell, K. G., Ye, W., et al. (2022). [29] |
| Wolfram Syndrome Type 2: A Systematic Review of a Not Easily Identifiable Clinical Spectrum | Rosanio, F. M., Di Candia, F., Occhiati, L., et al. (2022) [30] |
| A mutant wfs1 zebrafish model of Wolfram syndrome manifesting visual dysfunction and developmental delay | Cairns, G., Burté, F., Price, R., et al. (2021) [31] |
| Wolfram syndrome 1b mutation suppresses Mauthner-cell axon regeneration via ER stress signal pathway | Wang, Z., Wang, X., Shi, L., et al. (2022) [32] |
| Novel mutations in the WFS1 gene are associated with Wolfram syndrome and systemic inf lammation | Panfili, E., Mondanelli, G., Orabona, C., et al. (2021). [33] |
| Delineating Wolfram-like syndrome: A systematic review and discussion of the WFS1 -associated disease spectrum | de Muijnck, C., Brink, J. B. T., Bergen, A. A., et al. (2023). [34] |
| Clinical Peculiarities in a Cohort of Patients with Wolfram Syndrome 1 | Salzano, G., Rigoli, L., Valenzise, M. (2022). [35] |
| Psychiatric Diagnoses and Medications in Wolfram Syndrome | Reiersen, A.M., Noel, J.S., Doty, T., et al. (2022). [36] |
| Wolfram syndrome: Portuguese research | Ferreras, C., Gorito, V., Pedro, J., et al. (2021). [13] |
Source: Author’s elaboration.
Table 3.
Categories.
| CATEGORY | SUMMARY | REFERENCES |
| Associated psychiatric disorders | Includes the presence of psychiatric conditions such as depression, anxiety, and bipolar disorder. These studies examine potential biological, genetic, and neurological links. | [5,6,7,8,27,36] |
| Mood and behavioral disorders | Covers mood disturbances (e.g., major depression, bipolar disorder) and behavioral symptoms (e.g., impulsivity, suicidal behavior), and their relation to clinical or neurological features. | [20,22,23,24] |
| Cognitive and neurological aspects | Addresses cognitive deficits, neurodegeneration, and neuropsychiatric changes in WS, and their impact on daily function and disease progression. | [24,26] |
| Anxiety and depression disorders | Examines anxiety and depressive disorders in individuals with Wolfram Syndrome and other rare diseases, focusing on the psychological burden of chronic progressive conditions. | [13,14] |
Source: Author’s elaboration.
Table 4.
Highest scoring DEX items in patients with WS: mean and range [min, max].
| Question | Executive dimension | Mean | Range |
| 15 | Hyperactivity and restlessness | 2.8 | [2.29-3.57] |
| 18 | Difficulties in maintaining attention | 2.27 | [1.71-3.29] |
| 2 | Impulsivity (acting without thinking) | 2.05 | [1.57-2.86] |
| 8 | Lack of enthusiasm/apathy | 2.03 | [1.36-2.82] |
| 17 | Inconsistency between what is said and what is done | 1.99 | [1.57-2.57] |
| 11, 12, 14, 19 | Difficulty in showing emotions, anger, repetitive behaviors, indecisiveness | ≈1.98 | [1.36-2.45] |
Source: Data from present study.
Table 5.
Lowest scoring DEX items in patients with WS: mean and range [min, max].
| Question | Executive dimension | Mean | Range |
| 9 | Embarrassing behavior towards others | 1.3 | [1.00-1.82] |
| 3 | Confusion with reality (false memories) | 1.49 | [1.27-1.88] |
| 4 | Future planning | 1.69 | [1.29-2.00] |
| 6 | Confusion between events | 1.72 | [1.21-2.55] |
Source: Data from present study.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



