
Submitted:
15 July 2025
Posted:
16 July 2025
You are already at the latest version
Abstract
Despite growing recognition of gender disparities in health research and policy, young women’s subjective well-being (SWB) and physical activity (PA) remain insufficiently ad-dressed, particularly in socio-culturally diverse regions such as the Balkans. This study aims to evaluate the development, implementation, and outcomes of PA interventions conducted in five cities: Athens (Greece), Bucharest (Romania), Niš (Serbia), Štip (North Macedonia), and Plovdiv (Bulgaria), using a mixed-methods multiple-case study ap-proach. The target group consisted of 341 young women aged 18–30 who shifted their mobility behavior from non-active to active modes. Results indicate increased active mo-bility, improved self-reported health status, and positive changes in nutrition habits—especially in Serbia, North Macedonia, and Bulgaria. However, challenges such as partic-ipant motivation, ineffective digital communication, and socio-cultural norms limiting women’s participation were identified. The effectiveness of the interventions varied across countries, underscoring the importance of culturally responsive and flexible program de-sign. Lessons learned emphasize the value of targeted outreach, hybrid delivery formats, and sustained stakeholder collaboration. This study provides actionable recommenda-tions for the design and implementation of scalable, gender-sensitive health promotion in-itiatives in complex regional contexts.
Keywords:
physical activity
; well-being
; young women
; intervention
; Balkans region
1. Introduction
Despite progress in the health sector, women’s health is still not given enough attention due to entrenched gender inequalities in research, policy, and funding. Women are thus frequently misdiagnosed, not properly treated, and face health problems that could have been prevented. In recent years, subjective well—being (SWB) has gained increasing importance in public health discussions. Despite this progress, young women continue to face significant challenges regarding their physical and mental health. Social and cultural factors often exacerbate these difficulties. Despite advancements in global health, women‘s well—being remains underserved due to persistent gender inequalities in research, policy and resource allocation. Historically, clinical trials have predominantly focused on men, leading to misdiagnosis, inadequate treatment and preventable health issues for women [1,2]. For instance, while European women have a longer life expectancy than men, they experience extended periods of ill health, driven not by biology but by deficits in gender-sensitive research and policy [1]. The outcome is not an effect of biology but rather due to research and health policy deficit [1]. Chronic pain disorders, affecting 70% of female patients, are often understudied, with 80% of pain research targeting male-dominant conditions [1]. This continuous neglect affects women’s self-assessment of their health and results in lower confidence in healthcare systems, stopping them from receiving early medical care. Women are more likely than men to view themselves as not being healthy, and a lot of women fail to seek care since it is too expensive [2]. These drawbacks are particularly more prevalent among refugee, migrant, and minority women, who are faced with intensified disadvantages in income, housing, work, and culturally appropriate care availability [2]. The Balkan context of common socialist background, post-war recoveries, and strong traditional gender roles makes for a relevant setting in which challenges and potentialities of strategy to women’s wellbeing and physical activity (PA) are present. In the Balkans, these disparities are compounded by socio-cultural barriers, particularly for marginalized groups. All of these challenges erode women’s confidence in healthcare systems, contributing to lower self-reported health and delayed care-seeking, especially among refugee, migrant, and minority women [2].
Subjective well-being, encompassing life satisfaction, positive affect, and the absence of negative affect [3] (Diener, 1984), is a critical lens for addressing these disparities. In the Balkans, young women’s SWB is shaped by a unique socio-cultural landscape marked by a shared socialist history, post-war recovery, and entrenched gender norms [4]. A UNICEF study across Montenegro, North Macedonia, and Serbia found high SWB among women aged 15–49, with life satisfaction rates of 88.9%, 82.1%, and 83%, respectively, positively correlated with younger age, higher education, and wealth [5]. However, social inequalities and traditional roles continue to limit well-being, particularly for women in rural or marginalized communities. In order to reduce the gender gaps among men and women in healthcare and improve the well-being of women, increasing awareness, transforming the structures, and better usage of funding should be considered [1].
Physical activity (PA) offers a promising intervention to enhance SWB, promoting mental health, self-esteem, and social connectedness [6]. Yet, young women in the Balkans face significant barriers to PA participation. A cross-sectional study of 2,452 medical students from Slovenia, Croatia, Bosnia and Herzegovina, North Macedonia, and Serbia revealed that 39.1% of female students did not engage in regular daily PA, compared to 31.4% of males, with higher socio-economic status linked to greater activity [7]. Cultural norms prioritizing women’s caregiving roles, limited access to sports facilities, and perceptions that sports are “not for girls” further restrict participation, particularly in rural areas [8]. These barriers contribute to rising noncommunicable disease risks and poorer mental health outcomes among women [9].
Global and regional interventions highlight the potential of PA to address these challenges, aiming to improve health by modifying lifestyle and behaviour, focusing on physical activity, nutrition, and prevention. The North Karelia Project in Finland and the Diabetes Prevention Program in the United States demonstrated significant health improvements through lifestyle interventions, with PA reducing disease incidence by up to 58% [10,11]. Similarly in the Netherlands, the BeweegKuur lifestyle intervention tackled weight-associated health threats through diet and physical activity advice. One year of follow-up with 517 participants revealed statistically significant changes in reducing mean weight loss, waist circumference and blood glucose. Higher physical activity was strongly linked to treatment attendance, demonstrating the potential of real-life, supervised interventions in primary prevention [12].
Gender specific campaigns and interventions address some specific challenges related to PA levels, health and well-being of young females. Many of them were found effective for targeting girls and young women to support them in their efforts to improve their PA level, overall health and well—being. In relevant literature we identified many interventions that are school and university based due to possibility to access a large number of participants, provide possibilities for controlled actions within the interventions and possibilities for monitoring the progress [13]. For example, The “Girl Active Program” in UK, aims to increase participation in PA by improving the school environment and empowering girls as leaders, targeting secondary school girls ages 11–14 [14]. Another positive example is a FitSpirit program as a school-based intervention in Canada that promotes PA for girls aged 12–17 engaging them in a fun, inclusive, non-competitive way. The program includes fun runs and events, workshops, goal setting, team building activities that was confirmed to have a positive impact on self-esteem and interest in PA and greater enjoyment in group movement [15]. In the Balkan region, as a specific interest of our work, several positive examples were identified. In Niš, Serbia, twelve-week game-based school intervention on physical fitness in girls aged 12–14 years was implemented as after—school program. It included engagement in two 40-minute sessions weekly in small-sided games: football, basketball, handball, volleyball. The program showed a significant improvement in fitness performance of girls, measured with different fitness tests such as long jump, medicine-ball throw, sit-ups, bent-arm hang, endurance (Yo-Yo test) [16]. Another good practice example is a program that combines PA and nutrition. It is delivered in Niš, Serbia & Ljubljana, Slovenia, targeting overweight adolescent girls in Serbia and Slovenia. It included school-based exercise & nutrition program, combining structured exercise HIIT training sessions three days in a week and nutrition education sessions integrated during PE lessons and after school period. The outcomes suggested improvements of body composition, muscular and physical aerobic performance in overweighted adolescent girls after 8 weeks of participation [17].
On the other hand, different community-based programs were also found effective in empowering girls and young females health and wellbeing. One positive example is a UK campaign “This Girl Can”. It’s a large-scale media campaign promoting different community events in collaboration with fitness centres. The campaign targets women and girls aged 14+, aiming to reduce the gender gap in sport and PA by tackling fear of judgment and promoting body confidence by their engagement in different. The outcome is over 3 million women that became more active and increased self-reported confidence and activity of females [18]. Another interesting initiative comes from Ireland, named DARE—Dance for All in Rural Environments that aims to improve physical activity of young women in rural areas through culturally relevant dance and community building. The initiative is comprised of community dance sessions led by local leaders, performing Irish dance, hip-hop and creative movement. It’s a 24—month initiatives that supports participation in PA, enhanced social connection and emotional wellbeing [19]. Gender-specific interventions have also been tested in developing nations. In Iran, the Health Belief Model (HBM) was applied to promote conformity to national Food-Based Dietary Guidelines (IFBDGs) among urban dwelling women aged 26-54. The intervention received education in nutrition and cooking skills, and they lowered energy consumption and BMI considerably [20].
Similar experiences were identified among Balkan countries. Identified programs there are created as country specific or multiple country initiatives that are connecting only Balkan countries or Balkan and other EU counties. One example of such program is Nordic-Walking Intervention in Serbia aiming to support PA habits of middle-aged and older adult Serbian women by involving them in a structured Nordic-walking training program for a period of 12 weeks aiming to improve physical fitness parameters and PA habits [21]. The WISE initiative (Women’s Involvement in Steady Exercise) is another positive example that integrate digital HIIT intervention complemented by nutritional plans and other health-related advice.s It targeted young women aged between 15 and 24 years that have a sedentary lifestyle and do not comply with the WHO PA recommendations. The program was delivered in Serbia and two EU countries—Spain and Italy [22].
While outcomes and results from implementing different programs, interventions and campaigns were explicitly presented and shared, we could found limited examples of shared experiences and recommendation on how to approach when designing and implementing different health and well—being related programs for young women. These gap and the experiences that we had from the Balkan fit project were the invitation for this writing, Fit-Balkans project, is an initiative funded by Erasmus+ Sport, targeting young women’s SWB through PA, offering research, awareness campaigns, and online courses across five cities in Serbia, North Macedonia, Greece, Romania and Bulgaria, with a lead and integrated experiences from Germany
The presented study aims to identify effective strategies and address challenges to promote women’s health and empowerment in a region marked by unique socio-cultural dynamics.
The objective of this study is to examine the development, implementation, outcomes, and lessons learned from PA interventions aimed at improving the SWB of young women (aged 18–30) in five urban centers included in Fit-Balkans initiative. Through a comparative case study approach, the study seeks to identify effective strategies, contextual influences, and practical recommendations for designing and implementing culturally sensitive health and well-being programs targeting young women in socio-culturally diverse environments.
The study objective will be addressed by answering the following questions:
1) How were the physical activity interventions for young women developed and implemented across the five Balkan cities?
2) What were the reported effects of these interventions on participants’ physical activity levels, subjective well-being, and nutrition habits?
3) What contextual, cultural, and behavioral factors influenced the implementation and outcomes of these interventions?
4) What challenges did program designers and implementers face, and what lessons can be drawn to inform future health and well-being initiatives for young women in the region?
Research Design
The presented study aims to examine the development, implementation, effects and lessons learned from various interventions designed to enhance physical activity levels of young women aged 18 to 30 years old from five cities in five countries: Athens (Greece), Bucharest (Romania), Nis (Serbia), Plovdiv (Bulgaria), and Shtip (North Macedonia). The subject of research are the intervention programs implemented in each country within the scope of the FitBalkan Erasmus+ sport project, exploring their impact on participants’ physical activity levels and overall well-being. The study analyses the structure and objectives of each intervention, the methods of implementation, and the experiences of participants in integrating the programs into their everyday lives.
This study employed a mixed-methods multiple–case research approach, which combined qualitative and quantitative approaches, analysing qualitative data obtained through interviews and document analyses and statistical analysis of quantitative data collected via a questionnaire. The qualitative analysis focused on various intervention programs aimed to improve the physical activity and well-being of women aged 18 to 30 in Athens, Niš, Štip, Plovdiv, and Bucharest. The qualitative analyses focused on experiences of participants and outcomes from applied interventions. The study aimed to understand these programs’ structure, objectives, content, promotion, and implementation methods, as well as the challenges encountered, and lessons learned.
A multiple-case study approach was used to explore similarities and differences across the five intervention sites. Each program was treated as a separate case, allowing for in-depth contextual analysis while enabling cross-case comparisons. The study used a convergent mixed-methods strategy, where qualitative and quantitative data were collected and analyzed in parallel, and then integrated during interpretation to strengthen validity through triangulation.
The Research Study Phases
- Development of Standardized Questionnaires: Questionnaires were tailored to local contexts to collect data on the general well-being of women in the specified age group, levels of physical activity, and active mobility models.
- Online Data Collection: Participants filled out the questionnaires online, followed by data compilation and preparation of detailed reports.
- Design of Intervention Programs: Physical activity interventions were individually developed for each country to encourage increased activity among participants.
- Implementation of Intervention Programs: Programs were carried out as per the designed plans, promoting physical activities in alignment with the intervention goals.
- Post-Intervention Surveys: Participants were surveyed again following the intervention programs to evaluate their impact.
- Post—Intervention interviews: Project members responsible for designing the interventions and/or persons responsible for program delivery were engaged in post—intervention interview discussing the challenges, barriers, limitations and lessons learned from the implementation of intervention programs.
2. Materials and Methods
Sample ID
The qualitative study included 6 participants that were members of the Balkan- Fit project team, responsible for designing the interventions and/or persons responsible for program delivery. They were all engaged in semi—structured interview providing their answers in a written form to exclude language difficulties.
The sample included in the quantitative component of the study consisted of young women aged 18–30 who voluntarily participated in the Fit-Balkans interventions across the five Balkan cities: Athens, Bucharest, Niš, Plovdiv, and Štip. Participants were selected based on their willingness to engage regularly in project activities, complete both the pre- and post-intervention questionnaires, and provide valid responses that allowed for consistent comparative analysis. In total, data from 341 participants were included in the final quantitative analysis. This final number reflects participants who consistently participated and provided complete datasets from both questionnaire rounds. Selection criteria ensured reliability and comparability of data across intervention sites, aligning with similar methodologies used in related physical activity and subjective well-being studies [23,24]. Participants who provided incomplete data or dropped out during the intervention were excluded from quantitative analyses to ensure the accuracy and integrity of the findings.”
Data Collection
Data were gathered from multiple sources to capture both implementation processes and participant outcomes:
- Theoretical analyses: Included analysis of designed interventions exploring the type of intervention, its objectives and contents, specifics for its implementation and expected outcomes
- Semi-Structured Interviews: Conducted with key stakeholders in each country, including intervention designers and coordinators responsible for program delivery. These interviews explored rationale, objectives, implementation strategies, challenges faced, perceived impacts of the interventions and lessons learned.
- Standardized pre- and post-intervention questionnaire, specifically designed to capture changes in physical activity (PA) behaviors, subjective well-being (SWB), nutrition habits, neighborhood perceptions, and active mobility patterns.
The effectiveness of the interventions have been monitored throughout the procedure with frequent communication between the local teams and participants via the communication channels established by each partner. In addition, two questionnaires were distributed, one before and one after the intervention period. Questionnaires represent a commonly adopted tool in mixed-methods intervention research, given that they allow consistent and structured data collection across diverse populations and contexts [25,26]. The pre-intervention questionnaire was longer, exploring the different aspects that may affect the levels of physical activity and well-being of the young women in the Balkans. Specifically, the first questionnaire comprises a section about the spatial environment, well-being level, physical activity level, nutrition, health status and socio-economic characteristics. In the first section, the questions focused on the spatial characteristics and the mobility patterns of the respondents. The next section comprises the Warwick Edinburgh Wellbeing Questionnaire, a series of statements that reflect the well-being of the respondent. The following section focused on the current physical activity levels of the respondent, in terms of vigorous, moderate and walking activities. Moreover, the respondents were requested to log their sitting time and the time they usually spent in front of screens. In the next sections the respondents were asked about their eating habits and their perception of their health status. The final section of the questionnaire was dedicated to their socio-economic profile of each respondent. At the end of the first questionnaire, the respondents could also apply to participate in the interventions of the Fit-Balkans project. All should participate in the mobility intervention and optionally participate in one or more interventions focusing on sitting time, screen time, and nutrition.
After the completion of the intervention period, the women who followed one of the interventions of the project had to complete a follow-up questionnaire reflecting on their experience and the changes in physical activity and well-being. Following established practices in intervention research [23,24], the socioeconomic section was excluded from the post-intervention questionnaire, as these characteristics typically remain stable within short intervention periods. The second questionnaire comprises six sections. The first is the mobility section, where the respondents were asked if they changed their mobility patterns. Similarly to the first questionnaire, the next sections focused on the level of well-being, physical activity and nutrition post-intervention. Next, there were some questions regarding some biometrics and finally the respondents were asked to reflect on the interventions and to provide feedback for the intervention procedure and the project.
Additionally, semi-structured interviews served as a complementary qualitative instrument to enrich quantitative data, capturing stakeholders’ experiences, implementation challenges, and contextual nuances [27,28]. Combining these quantitative and qualitative instruments provided comprehensive insights and allowed effective triangulation of findings, aligning with methodological recommendations from similar physical activity and health interventions [29,30].
Ethical Considerations
Before the beginning of the interventions, the protection of personal data of the participants should be ensured. Therefore, in all participating countries together with the participation form a consent form was distributed ensuring the anonymity of each participant in every stage of the project. Ethical approval for the study was obtained from relevant institutional bodies in each participating country. Informed consent was secured from all participants prior to data collection. Anonymity and confidentiality were maintained throughout the research process.
Data Analysis
Qualitative Data Analysis
Interview transcripts were analyzed using thematic analysis to identify recurring themes related to the design, delivery, challenges and lessons learned from interventions. Coding was performed inductively, and emerging categories were refined through iterative comparison across cases. Key themes included program objectives, implementation facilitators and barriers, participant engagement, and sustainability.
Quantitative Data Analysis
In the first questionnaire, 1222 answers were collected in total from all participating countries. The project objective was to have at least 100 participants per country, allowing for a potential 20% dropout rate by the end of interventions. The highest number of respondents was collected in Romania, which comprises the 48.8% of the total sample. The lowest number of respondents was reported in Bulgaria, where 94 answers were collected.
After the end of the interventions, the second survey was conducted. Overall, 341 questionnaires were collected. Four out of five countries reached the target of 20% drop out rate, having 80 or more participants following the intervention until the end. Only in Greece, the majority of participant dropped with only 16 reaching the end of the intervention period and completing the post-intervention questionnaire.
The comparison of the pre- and post-intervention results for the different parameters is presented and analyzed thoroughly in the following section.
Integration of the Data
Findings from the qualitative and quantitative analyses were integrated through triangulation to identify convergences and divergences. Qualitative insights provided context and explanations for the quantitative trends observed, offering a more nuanced understanding of program impacts and implementation processes.
Balkan Fit Intervention Programs
The ultimate goal of the Fit-Balkans project was to enhance the subjective well-being of young women aged 18 to 30 in five Balkan cities through physical activity interventions. For this purpose, each country was responsible for designing different interventional programs that would promote different forms of physical activity and adoption of a healthy lifestyle and would contribute to enhancing physical activity level and well–being of young women. Based on initial needs analyses and identification of available resources, each country designed tailored interventions to promote physical activity and well-being. The interventions were developed with consideration of key factors such as needs of the target group, goals that should be achieved, as well as available location, timing, content, and overall objectives.
Different countries adopted diverse approaches and criteria when designing their interventions. The main criteria that leaded the design of the intervention included:
- The specific health needs of the target population;
- Most popular activities among young women;
- Addressing the characteristics of the target group—young women balancing studies, work, and/or family responsibilities.
- Focusing on young women (18–30 years), particularly those with lower levels of health-related behaviors according to self-reported data;
- Ensuring that all women who participated in the initial survey and expressed interest had access to the intervention;
- Encouraging engagement through elements of teamwork, innovation, and competition;
- Selecting interventions that were appealing to the target population while minimizing time constraints.
This flexible and context-sensitive approach allowed each country to design interventions that best fit the needs and lifestyles of the women in their respective regions. Following above mentioned criteria, it was understandable that the tailored intervention should be: accessible (easily available to all participants, including online formats, mobile-friendly content, and sessions in community spaces); affordable (cost-effective or free to ensure participation is not limited by financial constraints; ease of independent practice (activities that are simple, easy to follow and require minimal equipment); time-efficient (to fit easily into busy schedules, with short, flexible sessions); engaging and motivational (incorporate elements such as gamification, teamwork, competition, or social support to enhance commitment); personalized (offering different levels of difficulty or adaptable options); sustainable (participants can continue practicing the activities beyond the intervention period); focused on holistic well-being (addressing physical activity, mental health, stress management, changes in nutrition, and overall lifestyle); culturally relevant (to be aligned with local traditions, habits, and environmental factors); monitored and supported (available guidance, progress tracking, or peer-support mechanisms).
Following these key aspects and criteria, nine different program interventions were tailored and implemented in different countries. Table 1 presents the intervention programs that were practiced by participants included in pre and post intervention period. The interventions that were not properly followed or no participant followed them until the end are excluded from this list. Overall, five programs were indoor oriented, three were outdoor oriented and one (active breaks) could be practiced both indoor and outdoor. From the programs three can be practiced individually, three activities can be done both individually or in group and the rest are group activities in smaller or larger groups. In terms of content, the programs are mix of aerobic and anaerobic types of activities improving aerobic capacities, strength and overall fitness. The programs offer different level of difficulty and guidance for participants with different levels of engagement and experiences in different types of PA programs. The detailed description of each intervention program can be found at FitBalkan project web page.
3. Results
After the completion of the intervention period, which lasted six months, a second survey was conducted, this time only to the women participated to the interventions of the project, in order to assess the results and the effectiveness of the different approaches, followed by the project partners in the Balkan countries. The second survey was conducted within a two-month period. In total 341 responses were collected from the participating countries. North Macedonia, Romania, Serbia and Bulgaria collected on average 80 responses, while Greece reported the highest drop out with 16 respondents. The focus of the follow-up questionnaire was on factors linked to the different interventions the participants could choose. Specifically, all participants took part in the mobility intervention, which involved an increase in active mobility and they could choose also between changing their eating habits and decreasing screen and sitting time. In the following sections, the results obtained will be thoroughly presented and analyzed.
Mobility
In the second survey specific questions on the mobility habits were repeated, focusing on their dominant mode of transport for different travel purposes and the frequency of use of public transport. Table 2 shows the differences in use of the different modes pre- and post- intervention for non-commuting trips. Overall, it can be observed that the use of public transport modes and car decreased while active modes and ride hailing services show an increase in use. Analytically, the use of bicycle for non-commuting trips skyrocketed, showing an increase by 260%. The majority of participants claimed that they used more the bicycle, with the highest increase reported in Serbia. Greek participants didn’t show any change in bicycle use, something that can be explained by the lack of proper and sufficient infrastructure for cycling in Athens. However, Greeks shown the second highest increase in walking trips after Bulgaria. More than half of the participants of the interventions reduced car use for non-commuting trips in all countries apart from Greece where a 14.29% increase in car use is reported. Interestingly, the use of taxi and car sharing shown significant increase in Serbia, North Macedonia and Romania. Serbian participants increased the use of taxi by 1100%. Nis, the Serbian participating city, has limited mobility alternatives and respondents in both surveys reported that they rely on active modes, buses and taxis. Romanians also started using carsharing options for their non-commuting trips.
The participants were also asked about their dominant mode of transport for commuting trips. Table 3 summarizes the differences in use of each mode of transport pre- and post- intervention. When comparing the commuting with non-commuting trips, it can be observed that bicycle is preferred for trip purposes other than work. While for non-commuting trips, the use of bicycles increased, for work related trips the overall use of bicycle decreased by 37.85%. Only Bulgarian participants used bicycle more than before when commuting. On the other hand, Romania and North Macedonia shown a decrease in the use of bicycle. Compared to non-commuting trips and between active modes, participants chose walking for their commute. The highest increase in walking is reported in North Macedonia, followed by Greece and Serbia. Romanian participants reduced the use of active modes for their commute. Car use showed a 33.91% decrease pre- and post-intervention. Similarly to non-commuting trips both Serbian and North Macedonian participants increased drastically the use of taxi. Regarding the use of bus and urban rail, Greek participants used more the bus for commuting trips and Romanians the urban rail. It should be noted that only Athens, Greece and Bucharest, Romania have extended networks of public transport network, including buses and urban rail.
Figure 1 depicts the difference in frequency of use of public transport pre- and post-intervention. Overall, everyday use of public transport increased by 51.68%. This result is affected mostly by the sharp increase in Romania. Bulgarian also used more public transport for a few times per week and Serbians few times per month. Greek and North Macedonian participants rarely used public transport compared and reduced the use of public transport. Lastly, there is a significant increase of the participants that did not use public transport in the intervention period by 8.52%.
Health Status
The designed interventions aimed on increasing active mobility, walking and cycling, but also other actions that can help participants to adopt a healthier lifestyle. Therefore, in both surveys the participants were asked about their perception of their health status. It should be mentioned that in the first survey, respondents with health problems did not take part in the project’s interventions. Figure 2 1 depicts the change in perception of health status pre- and post- intervention. The most substantial improvement in health status can be observed at the North Macedonian participants. The share of participants that perceived their health status as good or very good shown a sharp increase. North Macedonia was the country that offered a wide range of social activities during the intervention period and potentially boosted the confidence of the participants. Serbia also reported a significant improvement in health status. In the remaining countries, the health status also improved with less people finding their health bad or very bad and changing their answer to a more positive status.
Nutrition
An additional category of interventions that accompanied the mobility interventions was nutrition. The participants that chose nutritional interventions could reduce the size of their portions, drink more water and change their mealtimes. Similarly to health status, the participants were asked about their perception of their eating habits. Table 4 shows the difference in eating habits perception pre- and post- intervention. In general, the participants, after the completion of the interventions, believed that they improved their eating habits. The only exception is Greece. Greek participants believed that their eating habits were healthier prior to the intervention period. A similar trend is reported in Romania with an increase of 42.96% in the “not really healthy” eating habits answer, but simultaneously there is a significant number of participants that believe that their eating habits are very healthy. The perception on the eating habits improved the most in Serbia, followed by Bulgaria and Romania. The North Macedonian participants are the most confident on their eating habits with an increase of “extremely healthy status by 13.24%.
One of the goals of the interventions was to increase daily water intake. Table 5 summarizes the change in water consumption pre- and post- intervention. It can be observed from the results that participants managed to increase their water intake and move closer to the suggested daily water intake. Analytically, participants increased their water intake to 5-7 glasses and to 8 or more glasses by 12.71% and 71.55% respectively. In all participating countries the low water intake was reduced drastically. In all countries participants claimed that they reached sufficient levels of hydration.
Physical Activity
Table 6 shows the average number of days the participants did vigorous activities, moderate activities or walked before and after the intervention period. The results reflect an overall positive impact of the intervention, with notable increases in all types of physical activity, especially moderate activity, which rose by 54.12% across all countries. Bulgarian participants shown remarkable gains in vigorous (133.58%) and moderate activities (208.70%), as well as in walking (58.50%), suggesting a successful example of the interventions. Serbia and North Macedonia also demonstrated positive outcomes, with Serbia showing steady improvements across all categories and North Macedonia recording a substantial increase in moderate activity, despite a decline in walking. Conversely, Greece and Romania presented a contrasting trend, with both countries experiencing declines in vigorous and moderate activities, though slight increases in walking were observed, indicating a possible shift towards lighter forms of exercise.
Table 7 shows the average minutes per day the participants did vigorous activities, moderate activities or walked before and after the intervention period. The results show a mixed picture of the intervention’s effectiveness across the different countries and types of physical activity. Overall, there were modest gains in vigorous (3.96%) and moderate activities (16.36%), but a notable decline in walking (-21.96%). Serbia shown substantial increases across both vigorous (61.64%) and moderate activity (72.74%), though it experienced a decline in walking (-24.06%). Bulgaria also showed positive results in vigorous activity (28.51%) and an impressive improvement in walking (32.91%), though moderate activity slightly declined (-0.98%). North Macedonia saw modest gains in moderate activity (24.00%) but slight declines in vigorous activity (-7.07%) and a substantial drop in walking (-37.04%). Conversely, Greece and Romania exhibited sharp decreases in vigorous and moderate activities, especially Greece, with declines of -67.82% in vigorous and -60.14% in moderate activity. Walking in Greece remained almost stable, showing a slight increase (3.76%), but Romania saw significant declines across the board, especially in walking (-39.72%).
Table 8 summarizes the results obtained on sedentary behavior of the participants. The results demonstrate a varied impact of the intervention across countries and categories. Overall, total sitting time decreased by 22.11%, indicating a positive shift towards reduced sedentary behavior, although Greece and North Macedonia deviated from this trend. Greece saw a slight increase in sitting time (5.39%), and North Macedonia experienced a substantial rise of 73.41%, suggesting that the intervention may have been less effective or faced specific challenges in these countries. Screen time on weekdays decreased modestly overall by 12.69%, with Romania showing a significant reduction of -52.55%, and Serbia also improving with a -13.64% drop. However, Greece notably saw an increase of 46.5% in weekday screen time, and Bulgaria also experienced a rise of 13.61%. Weekend screen time followed a more consistent positive trend, with an overall reduction of -15.51%. Romania and Serbia led with significant decreases of -38.28% and -56.71%, respectively, indicating strong behavioral changes. In contrast, Bulgaria’s weekend screen time increased sharply by 52.08%, and Greece saw a modest rise of 13.81%.
Intervention Assessment
The final section of the questionnaire was about the effectiveness of the interventions on well-being and physical activity. Table 9 summarizes the perceived effectiveness of the project’s interventions on well-being. The overall results show that the respondents have mixed perceptions on how their involvement affected their well-being. Almost the same share of respondents reported that the effect was weak and effective (summing both effective and very effective). The majority of North Macedonian respondents found that their involvement affected substantially their well-being. Greek respondents showcase similar trends. On the other hand, the highest share of weak effectiveness on well-being is reported at Bulgarian women with 58.54%, slightly higher than the Serbian share. In Romania, similar shares were reported between effectiveness and ineffectiveness of the interventions of the participants well-being.
The effectiveness of the interventions on physical activity was perceived in the same fashion as the effectiveness on well-being. Table 10 shows how the participants perceive the effectiveness of the intervention on their physical activity. The perceived effectiveness of the interventions in physical activity varied notably across countries, reflecting differing levels of impact and perhaps cultural or programmatic differences. Overall, the majority of participants rated the interventions as either “Weak” (48.09%) or “Very Effective” (27.27%), indicating a polarized perception of success. Greece had the highest percentage of participants rating the intervention as “Very Effective” at 43.75%, despite mixed objective outcomes in physical activity and sedentary behavior, suggesting that the intervention may have been well-received or subjectively appreciated regardless of measurable changes. Romania and Serbia also reported high levels of perceived effectiveness, with 35.8% and 35% respectively rating it as “Very Effective,” and none rating it as “Very Weak,” highlighting a generally positive reception in these countries. In contrast, Bulgaria stood out with a predominantly “Weak” perception (54.88%) and a low “Very Effective” score (4.88%), indicating potential dissatisfaction or challenges in the intervention’s design or implementation. North Macedonia showed a relatively balanced distribution, with 30.49% viewing the intervention as “Very Effective” and 45.12% as “Weak,” suggesting mixed feelings among participants. These perceptions align to some extent with the objective data, but also reveal the complexity of evaluating interventions, where subjective experiences and measurable outcomes may not always align.
The willingness to continue the interventions after the completion of the interventions was positive across all countries, with an overall willingness to continue of 88.86%. Serbia showed remarkable commitment, with a full 100% of participants indicating they would continue. Romania also demonstrated high enthusiasm, with 92.59% expressing intent to continue, reinforcing the earlier findings of favorable perceptions of effectiveness. North Macedonia (85.37%) and Greece (81.25%) maintained solid levels of commitment, despite more mixed views on intervention effectiveness, suggesting that participants still saw value in maintaining the behavior changes. Bulgaria, while slightly lower at 79.27%, still reflected a substantial majority willing to persist, even though perceptions of the intervention’s effectiveness were relatively modest. Overall, these figures underscore a positive outlook for the sustainability of the interventions, with participants largely inclined to integrate these activities into their daily routines beyond the project’s horizon.

Table 11.
Willingness to continue with the interventions.
| Yes | No | |
|---|---|---|
| Total | 88.86 | 11.14 |
| Greece | 81.25 | 18.75 |
| Bulgaria | 79.27 | 20.73 |
| Romania | 92.59 | 7.41 |
| Serbia | 100.00 | 0.00 |
| North Macedonia | 85.37 | 14.63 |
Results from Qualitative Analyses
Drawing from interview responses to eight open-ended questions, we conducted a thematic analysis to understand what worked, what didn’t, and how future interventions could be enhanced. Following the Braun & Clarke’s (2006) six-step approach included familiarization, coding, theme generation, review, definition, and reporting, six different themes were identified [31].They are following: Participant engagement challenges, Effective components of the interventions, Implementation barriers, Target group specificity, Lessons learned, Recommendations for future interventions.
Theme 1: Participant Engagement Challenges
A consistent issue across responses was the difficulty in maintaining participant motivation over the course of the intervention. One of participants quoted:
“The biggest challenge was helping people stay motivated and participate during the whole intervention.”
Sustained behavior change proved challenging, particularly over a six-month period. Digital platforms such as Facebook and email were used to engage participants, but they had limited success
“Only a few of them joined the Facebook group.”, with low participation in group activities and poor follow-through on communication (“Most respondents probably filled in the questionnaire without any real intention to engage.”).
Theme 2: Effective Components of the Interventions
Despite challenges, several positive intervention elements emerged, notably activities that were outdoors, enjoyable, and adaptable to participants’ lifestyles. Walking in parks, team-based activities like catchball, and HIIT sessions were particularly well received. This is notable from the following quotes from participants
“Walking time was the one aspect that worked best.”
“HIIT trainingsessions were well presented and fit the participants’ preference.”
These elements succeeded because they combined physical activity with enjoyment, accessibility, and social interaction. Nature and variety improve engagement as well as social elements of the activities are identified as important.
Theme 3: Implementation Barriers
The rollout of interventions faced both logistical and environmental barriers. Weather disruptions forced schedule changes for outdoor activities (“We had to change the schedule quite often due to weather.”), while other life events were the reasons why many participants were unable to adhere to strict routines and diets. In addition, the digital communication strategy was mismatched with participant preferences—Facebook was seen as outdated, especially for the younger participants
“Participants used different communication platforms… Facebook seemed outdated.”.
Location and having the activities only at one single place, was a big challenge, especially for bigger cities
“It was difficult to engage people who don’t know each other in a large city.”. These suggest that environmental and logistical constraints as well as technological mismatch with participants were identified as the biggest barriers for successful implementation of program interventions.
Theme 4: Target Group Specificity
Respondents emphasized that interventions aimed at homogenous groups (e.g., university students or workplace cohorts) were more likely to succeed
“Target groups which are homogeneous are easier to involve.” and
“Trying to engage people who do not know each other... is probably very difficult.”). In contrast, efforts to engage general, dispersed populations (such as residents of large cities) proved difficult. This was partly due to lack of shared identity and logistical constraints in organizing activities across distances and time zones.
Theme 5: Lessons Learned
Respondents reported that successful interventions require robust planning and coordination
“The key lesson was in organizing and managing all participants.”.
Flexibility in design, a gradual rollout, and collaborative team effort were key factors. Seasonality was also a factor: beginning interventions in spring especially for outdoor interventions or in stable weather conditions facilitated participation and continuity “Start the intervention in spring.”
Order of implementing interventions was also identified as very important “Do one month at a time, not all at once.”. Following these, what can be undelined as lessons learned is that pacing, planning and coordination across teams is essential.
Theme 6: Recommendations for Future Interventions
Recommendations are centered around flexibility, personalization, and modernization. Future interventions should:
- Use interactive and relevant platforms (e.g., Instagram, podcasts)
“Include podcasts, movies, fun challenges, mentors.”
- Build community identity by involving known figures or targeting closed groups
- Include supportive elements like mentors, personal feedback, and flexible scheduling
- Incorporate hybrid approaches combining online and in-person components
Respondents also suggested gamifying the experience through competitions and challenges and ensuring consistent feedback loops through participant data collection and reflection. The focus was also placed on personalization and motivation tools.
4. Discussion
The Fit-Balkans project, aimed at enhancing the subjective well-being of young women aged 18 to 30 in five Balkan cities through physical activity interventions, encountered numerous challenges throughout its implementation. While many risks were anticipated during the proposal submission period, additional unforeseen issues emerged due to specific circumstances that were difficult to predict during the planning phase. Similar to previous health interventions [32,33,34], the Fit-Balkans project demonstrated the importance of structured yet flexible implementation strategies to address evolving intervention programs dynamics.
The findings of the current study are in line with that study was conducted by Netz and Wu (2005) and confirm the positive impact of increasing physical activity on well-being of participants during the intervention [35]. The results of this study, showing an increase in the use of active mobility over non-active modes among young women in the Balkans, confirm the findings of Grydeland et al. (2013) [32], regarding the positive effect of interventions on increasing physical activity among adolescents. Also, the results of the current study are in line with a reviewed study on the impacts of intervention on physical activity and health status of girls, conducted by Vicki et al. (2016) [36].According to a mentioned reviewed study, the physical activity of girls increased after intervention in one of fifteen studies [37].
The intervention methods differ in several studies. Although the dominant intervention method in this study was increasing walking and cycling in commuting and non-commuting trips, the participants were encouraged to reduce sitting and screen time. The total sitting and screen time during the week and weekend was reduced by 22%, 12%, and 15%, respectively. This finding contradicts the results of another study on the impacts of intervention regarding increasing physical activity and reducing sitting time in workplaces [38]. However, the ineffectiveness of the intervention in that study was probably related to the impact of COVID-19 restrictions.
Twenty-five and twenty-two percent of participants in the intervention reported, respectively, very effective and effective impacts of the intervention on their total well-being, while only one percent of participants was not satisfied with the impacts of the intervention on well-being. This shows the same result as another study reviewing studies using a meta-analyses approach on the positive effect of physical activity on cognitive well-being. In addition, this study confirms another systematic review study conducted by Hale et al. (2021) [39]. Regarding the effectiveness of intervention in improving the well-being of young people, the effectiveness of physical activity interventions has been reported not only among youth but also among the elderly [40].
The findings of this paper are in line with several studies that have assessed the effectiveness of physical activity interventions on physical activity levels, health status, and well-being. In addition, the lessons and experiences gained from the intervention can support the findings of other studies and provide valuable insights for future research and policy-making.
Another related challenge was the project’s visibility and its ability to reach a broader audience. Despite efforts to promote the initiative through awareness-raising events, massive open online courses and other online resources, disseminating information to the target group and beyond required more intensive engagement strategies. While social media campaigns, newsletters, and the project’s website were initially chosen as primary methods to enhance visibility, the experience indicated that these strategies were in the end not optimally effective in reaching the intended target group. One key insight gained was that the target audience did not frequently engage with the types of media content or platforms utilized- with the exception of the Facebook group created by Corporate Games, possibly due to differing preferences for information consumption and the requirement for more engaging visuals or more dynamic formats, which would be easier to consume and interpret, in addition to potentially being conveyed by internet pages or personalities they are already following and with which they are familiar. Consequently, this highlighted the importance of adapting communication channels more closely to the specific behaviors and preferences of the target group. Future initiatives could benefit from assessing country-specific media consumption habits. For instance, similar efforts could benefit from teaming up with local influencers or from creating online challenges and community hashtags, as well as from involving newer social media platforms.This finding aligns with previous public health campaigns, such as Change4Life in the UK, which required sustained efforts to maintain engagement (Change4Life, n.d.) or the results of Silva et al. [42].
The need for localized and culturally adapted outreach strategies became apparent. Ensuring the sustainability of the project beyond its funded period remains another concern of the consortium, as maintaining long-term impact requires securing ongoing interest and support from stakeholders, including policymakers, community leaders, and the participants themselves. The project team organized workshops for local policymakers to encourage the continued promotion of physical activity among young women, as well as to extend efforts to more social groups. However, securing the commitment of policymakers remains a challenge, as shifting political priorities often divert attention away from long-term well-being initiatives [2]. The team from Goce Delčev University of Štip in North-Macedonia highlighted a potential formal as well as informal implementation of a sports program in the university in order to continue the efforts of the Fit-Balkans project even after the end of its funding.
The integration of each partner’s objectives and work processes presented some difficulties due to differing organizational structures and operational capacities across the participating countries. Some partners, particularly those with a grassroots community focus, struggled to adapt to the academic rigor required for data collection, leading to delays and miscommunications. Aligning the diverse objectives of academic and non-academic partners required ongoing negotiation and flexibility. Similar challenges have been observed in previous multi-partner initiatives [43] highlighting the complexity of coordinating diverse stakeholders in large-scale public health projects.
Keeping participants motivated and engaged over the course of the project was also difficult. Many faced socio-economic constraints, competing priorities, or lacked intrinsic motivation for sustained participation. To counteract these issues, the project introduced financial and reward-like incentives though some participants indicated that the incentives were not sufficient to overcome barriers such as work or childcare responsibilities. Tracking participant activity over time presented further difficulties, with a notable dropout rate by the final data collection phase. Many participants cited time constraints or a lack of immediate tangible knowledge.
Lastly, cultural and societal factors also significantly influenced participation levels, as varying perceptions of PA and well-being shaped how interventions were received and implemented in different locations. In some regions, cultural norms regarding women’s roles within the household limited their ability to participate in project activities. These results are similar to the ones discovered by Segar et al. [44] highlighting that women of various age groups, while attempting to increase their PA are confronted with issues of identity, lack of time and being deeply involved in their family’s needs. To address these culturally influenced barriers but also those that can be classified as more generic, and enhance accessibility of physical activities for women—particularly mothers—several adaptive strategies can be implemented.
In order to make physical activity more available to women in different age groups, but particularly in the cases of mothers, a solution identified by the NIH in 2018 was to use video exercise groups and to keep track of the physical activity using apps. Additionally, partaking into light exercise instead of focusing on heavy training frameworks proved helpful as well. Home workouts also made interventions easier and allowed participants to be more consistent. The feeling of guilt, which was also a relevant aspect in the analysis was also reduced by the fact that the participant maintained their proximity to the family members they have to care for and could adapt their exercise to the schedule of the children or the elderly in need of their presence.Some participants also reported feeling self-conscious about engaging in physical activity in public spaces, further reducing engagement levels. Addressing these culturally embedded attitudes required adaptive strategies to ensure relevance and resonance with the target group. These findings are consistent with previous studies that emphasize the importance of gender-sensitive health interventions [1]. Joseph et al. [45] highlighted the importance of understanding how sociocultural norms, values, and beliefs influence the physical activity behaviors of African-American women. Their study offers valuable guidance for researchers and practitioners in designing culturally responsive physical activity programs that effectively address the needs of diverse socioeconomic and cultural groups—an approach that strongly aligns with the goals and strategies adopted in the Fit-Balkans project.The findings and lessons from the implementation of intervention in the Fit-Balkans project is in the same line with that study and accepts the significant relationship between cultural norms and belief with the physical activity behaviors in different contexts. Following the experiences from our work, we suggest that cultural specifics should be considered in developing culturally relevant physical activity programs and intervention. Also the findings from the implementation of Fit-Balkans’ intervention on physical activity accept the finding of another research study on the psychological and cultural barriers on successful running of physical activity programs among Latin Men and Women in the U.S. [46].
Despite these challenges, the Fit-Balkans project provided valuable lessons for future initiatives. Tailoring approaches based on cultural contexts improved engagement and effectiveness, as recognizing and adapting to local customs, beliefs, and lifestyles made interventions more accessible. Adjusting intervention schedules to align with local religious holidays, for instance, significantly improved participation rates in one city. Maintaining participant motivation required fostering a sense of community and ensuring consistent communication. Participants who received regular personalized check-ins from project staff reported higher levels of motivation and adherence to the program. Developing effective strategies for increasing engagement also emerged as a critical factor, with interactive workshops and the use of social media groups helping to create a sense of community among participants and leading to higher engagement rates.
By integrating these lessons, future initiatives can more effectively address the challenges inherent in promoting physical activity and well-being among young women across varied socio-cultural landscapes.
5. Conclusions
Physical activity interventions developed within the Balkan Fit project successfully demonstrated the potential of culturally responsive interventions to enhance the subjective well-being of young women across diverse urban settings in the Balkans. Despite facing numerous implementation challenges—including sociocultural barriers, participant engagement issues, coordination difficulties among partners, and limitations in outreach strategies—the intervention yielded promising outcomes. Increases in physical activity, particularly through active mobility, alongside reductions in sedentary behavior and improved self-reported well-being, affirm the effectiveness of targeted, community-based approaches. The study underscores the importance of flexible yet structured implementation strategies, sustained stakeholder engagement, and the need to adapt interventions to local cultural contexts. Lessons from the project provide critical insights for future initiatives aiming to promote physical activity and well-being among young women, especially in regions marked by social and economic complexity. To ensure long-term impact, future programs should prioritize culturally sensitive planning, cross-sector collaboration, and strategies that address motivational and structural barriers to sustained participation.
Author Contributions
The authors confirm contributing to the paper as follows: conceptualization: all authors, methodology, B.P., S.JM., Mdz., GL.; analysis and interpretation of results: G.L., B.P; discussion M.M., L.P.; draft manuscript preparation: all authors. All authors reviewed the results and approved the final version of the manuscript.
Funding
The current study has been designed as a part of the project “Improving the Subjective Wellbeing of Young Women in Balkans through Interventions in their Physical Activity”-Fit-Balkans (Project number 101049997) funded by the ERASMUS+ program of the European Commission. The funders had no role in undertaking this review.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the Fit-Balkans study.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Acknowledgments
We acknowledge support by the Open Access Publication Fund of TU Berlin. The authors are grateful to the participants, and to diverse colleagues/collaborators who have contributed to the management of the survey by guiding participants about the questions, translating the questionnaires from English to local languages, and/or providing guidance/support to data collection/analysis related to accelerometry. The current study has been designed as a part of the project “Improving the Subjective Wellbeing of Young Women in Balkans through Interventions in their Physical Activity”-Fit-Balkans (Project number 101049997) funded by the ERASMUS+ program of the European Commission. The funders had no role in undertaking this review.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
Following abbreviations are used in this manuscript:
| SWB | Subjective well-being |
| PA | Physical activity |
References
- Khanna, D. Health and Healthcare Systems “Women’s health: Why is the health of at least half the global population so often overlooked?”. World Economic Forum, 2023, online article. Available online: https://www.weforum.org/stories/2023/01/women-health-gap-davos-2023/.
- Walsh, G. Women feel unheard and dismissed when it comes to health. Women’s Health Gap, 2021, Part I of a five-part series.
- Diener, E. Subjective well-being. Psychological Bulletin, 1984, 95, 542–575. [Google Scholar] [CrossRef] [PubMed]
- Brajša-Žganec, Andreja & Merkaš, Marina & Šverko, Iva. Quality of Life and Leisure Activities: How do Leisure Activities Contribute to Subjective Well-Being? Social Indicators Research. 2011, 102, 81–91. [Google Scholar] [CrossRef]
- Begovic-Mikanovic, V.; Wenzel, H. Data Mining Approach: What Determines the Well-being of Women in Montenegro, North Macedonia, and Serbia? Frontiers, 2022, 10, 873845. [Google Scholar] [CrossRef]
- Stuart, J.H. Biddle, Simone Ciaccioni, George Thomas, Ineke Vergeer, Physical activity and mental health in children and adolescents: An updated review of reviews and an analysis of causality. Psychology of Sport and Exercise 2019, 42, 146–155. [Google Scholar] [CrossRef]
- Grujičić, M.; Ilić, M.; Novaković, B.; Vrkatić, A.; Lozanov-Crvenković, Z. Prevalence and Associated Factors of Physical Activity among Medical Students from the Western Balkans. Int. J. Environ. Res. Public Health, 2022, 19, 7691. [Google Scholar] [CrossRef] [PubMed]
- Game Set Equality: Integrated Report on Current Conditions Related to Gender Equality in Sport, 2023: Sofia, Bulgaria: Sdruzenie Sporten Klub Dema, available on https://gamesetequality.eu/wp-content/uploads/2024/11/GAME-SET-EQUALITY-REPORT.
- World Health Organization. In Strategy on women’s health and well-being in the WHO European Region; WHO Regional Office for Europe: Copenhagen, Denmark, 2016.
- Puska, P.; Jaini, P. The North Karelia Project: Prevention of Cardiovascular Disease in Finland Through Population-Based Lifestyle Interventions. Am. J. Lifestyle Med., 2020, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Diabetes Prevention Program Coordinating Center. The Diabetes Prevention Program (DPP). Diabetes Care, 2002, 25, 2165–2171.
- Schutte, B.; Haveman-Nies, A.; Preller, L. One-Year Results of the BeweegKuur Lifestyle Intervention Implemented in Dutch Primary Healthcare Settings. Biomed Res. Int., 2015, 484823. [Google Scholar]
- Mok, M.; Chin, M.K.; Korcz, A.; Popeska, B.; Edgintoon, C.R.; Uzunoz, F.; Podnar, H.; Coetzee, D.; Georgescu, L.; Emeljanovas, A.; Pasic, M.; Balasekaran, G.; Anderson, E.; Durstin, J.L. Brain Breaks® Physical Activity Solutions in the Classroom and on Attitudes toward Physical Activity: A Randomized Controlled Trial among Primary Students from Eight Countries. Int. J. Environ. Res. Public Health, 2020, 17, 1666. [Google Scholar] [CrossRef] [PubMed]
- Harrington, D.M.; et al. Girls Active: a cluster randomised controlled trial of an intervention to increase physical activity among adolescent girls. Int. J. Behav. Nutr. Phys. Act., 2018, 15, 40. [Google Scholar] [CrossRef] [PubMed]
- Bélanger, M.; et al. FitSpirit: evaluation of a school-based program to promote physical activity among Canadian girls. Health Promot. Pract., 2019, 20, 106–114. [Google Scholar]
- Petrušic, T.; Trajkovic, N.; Bogataj, S. Twelve-Week Game-Based School Intervention Improves Physical Fitness in 12–14-Year-Old Girls. Front. Public Health, 2022, 10, 831424. [Google Scholar] [CrossRef] [PubMed]
- Bogataj, Š.; Trajković, N.; Cadenas-Sanches, C.; Sember, V. Effects of School-Based Exercise and Nutrition Intervention on Body Composition and Physical Fitness in Overweight Adolescent Girls. Nutrients, 2021, 13, 238. [Google Scholar] [CrossRef] [PubMed]
- Sport England. This Girl Can Campaign Evaluation; Sport England: UK, 2016; Available online: https://www.sportengland.org/ (accessed on 10 June 2025).
- www.cavanarts.ie.
- Shariatjafari, S.; Omidvar, N.; Shakibazadeh, E.; Majdzadeh, R.; Minaei, M.; Gholamzade, M. Effectiveness of Community-based Intervention to Promote Iran’s Food-based Dietary Guidelines. Int. J. Prev. Med., 2012, 249–261. [Google Scholar]
- https://www.isrctn.com/ISRCTN44310625.
- Ferrando-Terradez, I.; Dueñas, L.; Parčina, I.; Copić, N.; Petronijević, S.; Beltrami, G.; Pezzoni, F.; San Martín-Valenzuela, C.; Gijssel, M.; Moliterni, S.; et al. Women’s Involvement in Steady Exercise (WISE): Study Protocol for a Randomized Controlled Trial. Healthcare, 2023, 11, 1279. [Google Scholar] [CrossRef] [PubMed]
- Grydeland, M.; Bergh, I.H.; Bjelland, M.; et al. Intervention effects on physical activity: the HEIA study — a cluster randomized controlled trial. Int. J. Behav. Nutr. Phys. Act., 2013, 10, 17. [Google Scholar] [CrossRef] [PubMed]
- Schutte, B.; Haveman-Nies, A.; Preller, L. One-Year Results of the BeweegKuur Lifestyle Intervention Implemented in Dutch Primary Healthcare Settings. BioMed Research International, 2016, 84823. [Google Scholar] [CrossRef]
- Grujičić, M.; Ili’, M.; Novakovi’, B.; Vrkati’, A.; Lozanov-Crvenkovi’, Z. Prevalence and Associated Factors of Physical Activity among Medical Students from the Western Balkans. International Journal of Environmental Research and Public Health, 2022, 7691. [Google Scholar] [CrossRef] [PubMed]
- Voskuil, V.R.; Frambes, D.A.; Robbins, L.B. Effect of Physical Activity Interventions for Girls on Objectively Measured Outcomes: A Systematic Review of Randomized Controlled Trials. J. Pediatr. Health Care, 2017, 31, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Mayne, J. Challenges and Lessons in Implementing Results-Based Management. In Evaluation, 2007, 13, 87–109. [Google Scholar] [CrossRef]
- Netz, Y.; Wu, M.-J. Physical Activity and Psychological Well-Being in Advanced Age: A Meta-Analysis of Intervention Studies. Psychol. Aging, 2005, 20, 272–284. [Google Scholar] [PubMed]
- Ehlers, D.K.; Salerno, E.A.; Aguiñaga, S.; McAuley, E. Physical activity interventions: Effects on well-being outcomes in older adults. In Handbook of well-being; Diener, E., Oishi, S., Tay, L., Eds.; DEF Publishers: Salt Lake City, UT, 2018. [Google Scholar]
- Hale, G.E.; Colquhoun, L.; Lancastle, D.; Lewis, N.; Tyson, P.J. Review: Physical activity interventions for the mental health and well-being of adolescents—a systematic review. Child Adolesc. Ment. Health, 2021, 26, 357–368. [Google Scholar] [CrossRef] [PubMed]
- Braun, V.; Clarke, V. Using thematic analysis in psychology. Qualitative research in Psychology 2006, 3, 77–101. [Google Scholar] [CrossRef]
- Puska, P.; Jaini, P. The North Karelia Project: Prevention of Cardiovascular Disease in Finland Through Population-Based Lifestyle Interventions. Am. J. Lifestyle Med. 2020, 495–499. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A. D., Thiero, O., Whidden, C., Poudiougou, B., Diakité, D., Traoré, F., … Kayentao, K. Proactive community case management and child survival in periurban Mali. BMJ Glob Health 2018, e000634. [Google Scholar] [CrossRef]
- Wen, Li Ming & Thomas, Margaret & Jones, Helen & Orr, Neil & Moreton, Renee & King, Lesley & Hawe, Penny & Bindon, Jeni & Humphries, Jenni & Schicht, Karin & Corne, Shauna & Bauman, Adrian. Promoting physical activity in women: Evaluation of a 2-year community-based intervention in Sydney, Australia. Health promotion international 2002, 17, 127–137. [Google Scholar] [CrossRef]
- Yael Netz, M. Physical Activity and Psychological Well-Being in Advanced Age: A Meta-Analysis of Intervention Studies. Psychology and Aging, 2005, 20, 272–284. [Google Scholar] [CrossRef] [PubMed]
- Voskuil, V.R.; Frambes, D.A.; Robbins, L.B. Effect of Physical Activity Interventions for Girls on Objectively Measured Outcomes: A Systematic Review of Randomized Controlled Trials. J. Pediatr. Health Care, 2017, 31, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Voskuil, V.R.; Frambes, D.A.; Robbins, L.B. Effect of Physical Activity Interventions for Girls on Objectively Measured Outcomes: A Systematic Review of Randomized Controlled Trials. J Pediatr Health Care. 2017, 31, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Alec Gonzales, Jia-Hua Lin, Jackie S. Cha, A year-long case study of multicomponent interventions to promote physical activity in office workers: A randomized control trial, Applied Ergonomics, 2024, 120, 104333. [CrossRef]
- Hale, G.; Colquhoun, L.; Lancastle, D.; Lewis, N.; Tyson, P. Review: Physical activity interventions for the mental health and well-being of adolescents—a systematic review. Child and Adolescent Mental Health. 2021, 26. [Google Scholar] [CrossRef] [PubMed]
- Ehlers, D.K.; Salerno, E.A.; Aguiñaga, S.; McAuley, E. Physical Activity Interventions: Effects on Well-Being Outcomes in Older Adults. In Handbook of Well-Being; Diener, E., Oishi, S., Tay, L., Eds.; DEF Publishers: Salt Lake City, UT, 2018. [Google Scholar]
- Silva, K.L.; De Sena, R.R.; Belga, S.M.M.F.; Silva, P.M.; Rodrigues, A.T. Promoção da saúde: desafios revelados em práticas exitosas. Rev. Saúde Pública, 2014, 48, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Segar, M.; Jayaratne, T.; Hanlon, J.; Richardson, C.R. Fitting fitness into women’s lives: effects of a gender-tailored physical activity intervention. Womens Health Issues. 2002, 12, 338–347. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Joseph, R.P.; Keller, C.; Affuso, O.; et al. Designing Culturally Relevant Physical Activity Programs for African-American Women: A Framework for Intervention Development. J. Racial Ethn. Health Disparities, 2017, 4, 397–409. [Google Scholar] [CrossRef] [PubMed]
- European Commission, Directorate-General for Education, Youth, Sport and Culture; ECORYS; KEA. Mapping on healthy lifestyles—A report to the European Commission; Publications Office of the European Union: Luxembourg, 2023. [Google Scholar]
- Larsen, B.A.; Noble, M.L.; Murray, K.E.; Marcus, B.H. Physical Activity in Latino Men and Women: Facilitators, Barriers, and Interventions. Am. J. Lifestyle Med., 2014, 9, 4–30. [Google Scholar] [CrossRef]
Figure 1.
Change in public transport use frequency.
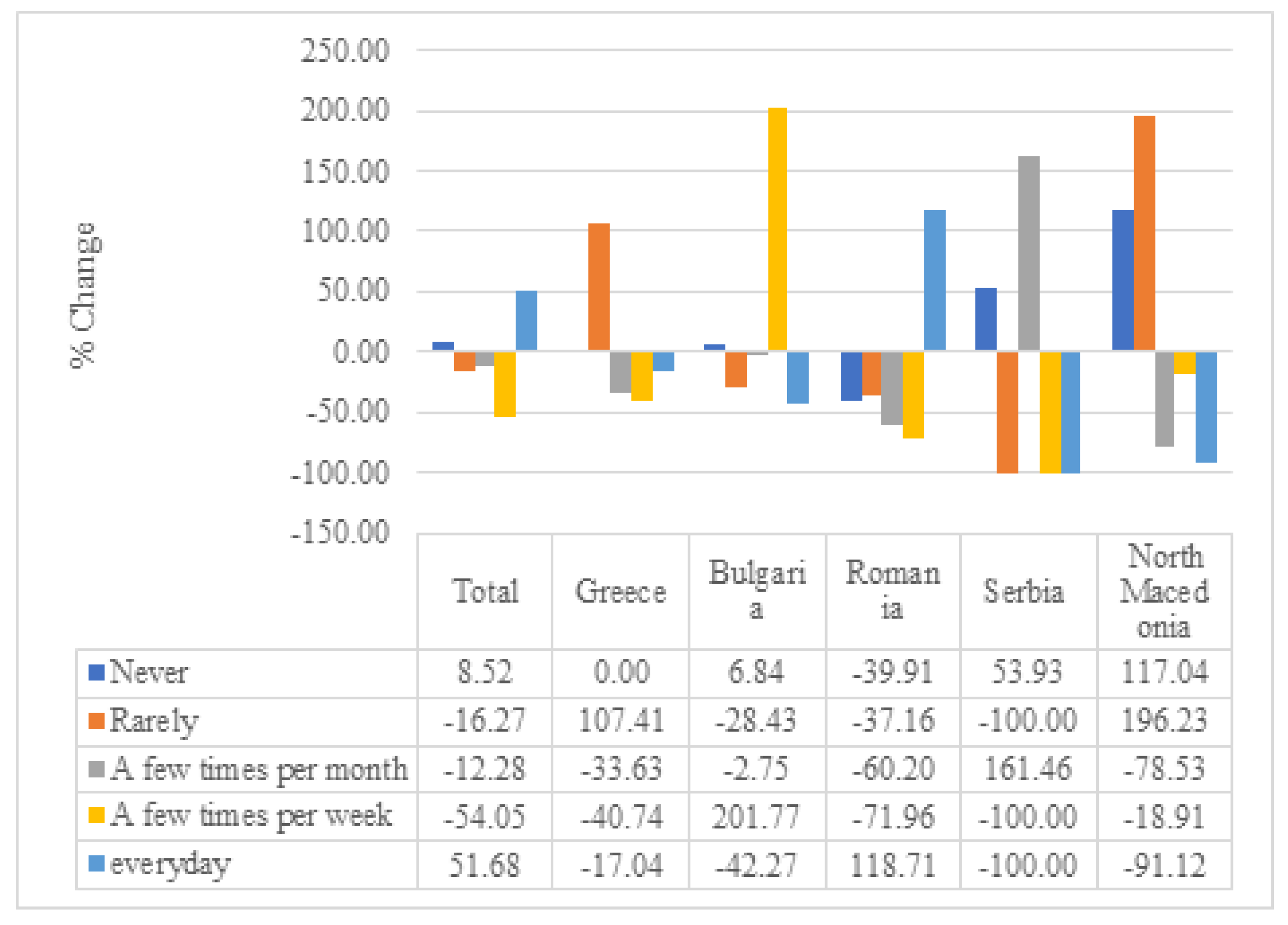
Figure 2.
Change in health status perception.
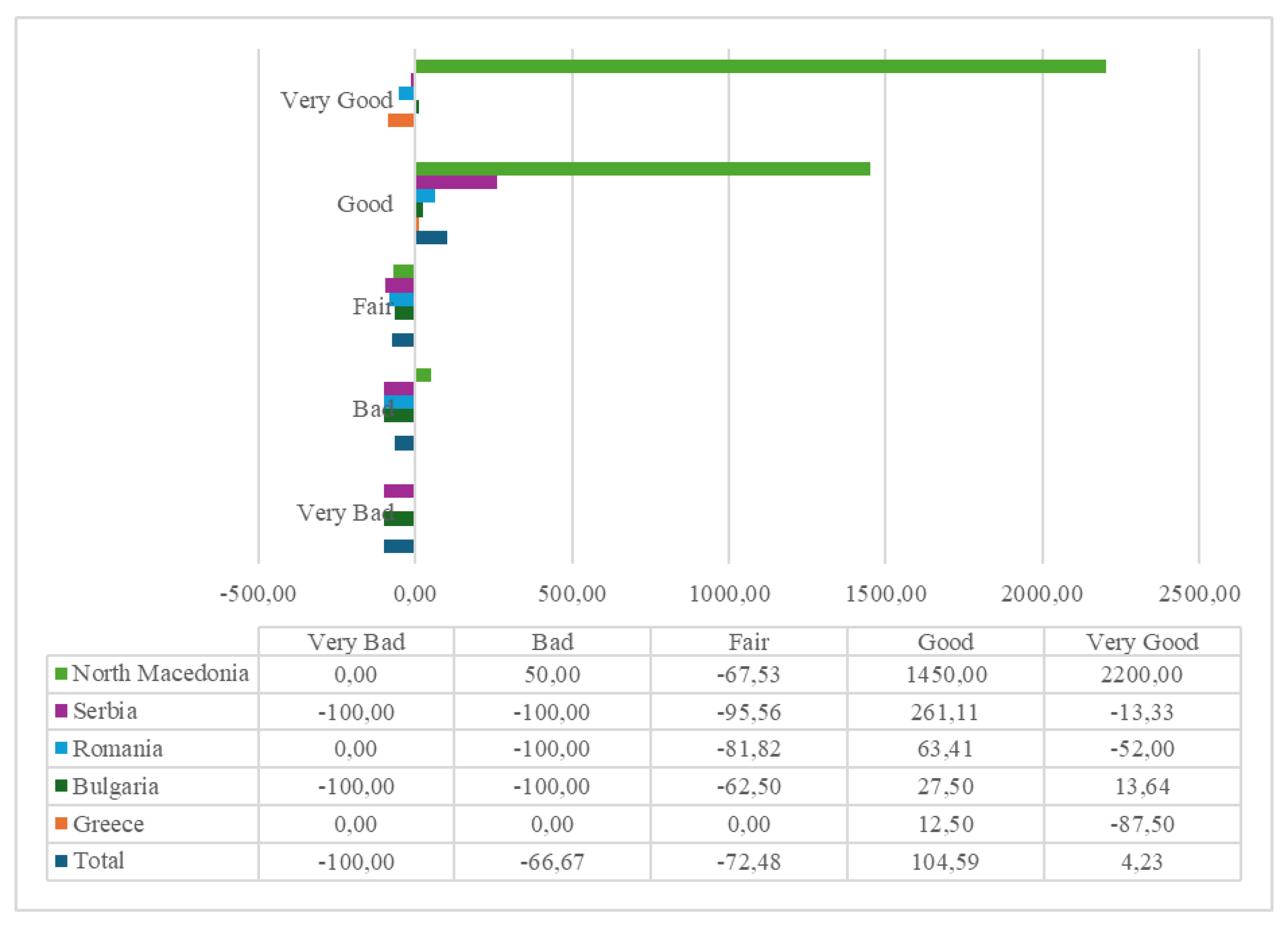
Table 1.
Overview of interventions.
| Name of the program | Enviornment | Type of participation | Facilities |
|---|---|---|---|
| Tabata | Indoor | Individual | Home, no specific facilities needed |
| Active breaks | Indoor and outdoor | Individual | Home/work office, no specific facilities needed |
| Outdoor activities | Outdoor | Individual and team | Any place in nature (Park or yard, nearby mountain, riverside path, recreational path, marked bike paths, hiking trails in the mountains, etc) |
| Partner crossfit | Indoor | Team | Sports hall |
| Pilates | Indoor | Group | Sports hall |
| Trail running | Outdoor | Individual and team | Near mountain or hill |
| Ftness challenge | Outdoor | Individual and team | Any place outdoor |
| Catch ball tournament | Indoor | Team | Volleyball courts |
| Nutrition video | Indoor | Individual | Home |
Table 2.
Change in mode use for non-commuting trips.
| Foot | Bicycle | Scooter | Motorcycle | Bus | Urban Rail | Car | Taxi | Carsharing | |
|---|---|---|---|---|---|---|---|---|---|
| Total | 10.62 | 260.57 | N/A | N/A | -26.02 | -37.00 | -43.85 | 241.79 | 192.96 |
| Greece | 66.67 | N/A | N/A | N/A | -100.00 | 50.00 | 14.29 | N/A | N/A |
| Bulgaria | 80.49 | 50.41 | N/A | N/A | -9.76 | -100.00 | -51.41 | -54.88 | N/A |
| Romania | -21.62 | 233.33 | N/A | N/A | 10.00 | 433.33 | -56.00 | -100.00 | 100.00 |
| Serbia | -18.92 | 1100.00 | N/A | N/A | -100.00 | -100.00 | -54.84 | 1100.00 | N/A |
| North Macedonia | 19.23 | 80.00 | N/A | N/A | 0.00 | -93.33 | -29.03 | 300.00 | N/A |
Table 3.
Change in mode use for commuting trips.
| Foot | Bicycle | Scooter | Motorcycle | Bus | Urban Rail | Car | Taxi | Carsharing | |
|---|---|---|---|---|---|---|---|---|---|
| Total | 20.49 | -37.85 | 63.14 | 35.95 | -10.83 | 39.90 | -33.91 | 296.21 | -56.49 |
| Greece | 101.48 | N/A | N/A | N/A | 208.15 | -26.52 | -26.26 | N/A | N/A |
| Bulgaria | 16.70 | 218.28 | N/A | N/A | 70.51 | -100.00 | -17.69 | 19.35 | N/A |
| Romania | -50.57 | -79.65 | N/A | N/A | -21.50 | 290.75 | -55.90 | -5.03 | -86.43 |
| Serbia | 96.19 | 15.61 | -100.00 | N/A | -100.00 | -100.00 | -30.63 | 927.64 | -100.00 |
| North Macedonia | 243.46 | -57.07 | N/A | N/A | -73.17 | -100.00 | 15.79 | 329.32 | N/A |
Table 4.
Change in perception of eating habits.
| Not healthy at all | Not really healthy | Somewhat healthy | Very healthy | Extremely healthy | |
|---|---|---|---|---|---|
| Total | -29.79 | -22.90 | 11.45 | 192.55 | -25.94 |
| Greece | 0.00 | 400.00 | -40.00 | 0.00 | -100.00 |
| Bulgaria | -82.71 | -25.91 | 67.80 | 332.20 | -50.61 |
| Romania | 0.00 | 42.96 | -62.03 | 127.85 | -9.81 |
| Serbia | -100.00 | -85.00 | 13.04 | 433.33 | -56.25 |
| North Macedonia | -71.69 | -38.24 | 96.27 | -24.51 | 13.24 |
Table 5.
Change in water consumption.
| Less than 2 glasses | 2-4 glasses | 5-7 glasses | 8 or more glasses | |
|---|---|---|---|---|
| Total | -70.19 | -43.75 | 12.71 | 71.55 |
| Greece | 0.00 | -66.67 | 266.67 | 0.00 |
| Bulgaria | -77.44 | -84.96 | 21.36 | 101.72 |
| Romania | 0.00 | 0.00 | -3.13 | 35.00 |
| Serbia | -100.00 | -85.59 | 38.45 | 43.39 |
| North Macedonia | -50.41 | -5.32 | -25.61 | 0.00 |
Table 6.
Average number of days of vigorous, moderate and walking activities pre and post intervention.
Table 6.
Average number of days of vigorous, moderate and walking activities pre and post intervention.
| Vigorous Activity | Moderate Activity | Walking | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre Intervention | Post Intervention | % Difference | Pre Intervention | Post Intervention | % Difference | Pre Intervention | Post Intervention | % Difference | |
| Total | 2.36 | 2.70 | 14.41 | 2.28 | 3.51 | 54.12 | 5.40 | 6.32 | 16.94 |
| Greece | 3.06 | 1.50 | -51.02 | 2.69 | 1.69 | -37.21 | 5.31 | 5.81 | 9.41 |
| Bulgaria | 1.67 | 3.90 | 133.58 | 1.96 | 6.06 | 208.70 | 4.88 | 7.73 | 58.50 |
| Romania | 2.62 | 1.64 | -37.26 | 2.77 | 2.25 | -18.75 | 5.99 | 6.54 | 9.28 |
| Serbia | 3.03 | 3.06 | 1.24 | 2.69 | 3.29 | 22.33 | 5.51 | 7.00 | 26.98 |
| North Macedonia | 2.01 | 2.43 | 20.61 | 1.62 | 2.77 | 70.68 | 5.26 | 4.11 | -21.81 |
Table 7.
Average minutes per day of vigorous, moderate and walking activities pre and post intervention.
Table 7.
Average minutes per day of vigorous, moderate and walking activities pre and post intervention.
| Vigorous Activity | Moderate Activity | Walking | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre Intervention | Post Intervention | % Difference | Pre Intervention | Post Intervention | % Difference | Pre Intervention | Post Intervention | % Difference | |
| Total | 42.19 | 43.86 | 3.96 | 36.29 | 42.22 | 16.36 | 62.91 | 49.10 | -21.96 |
| Greece | 55.94 | 18.00 | -67.82 | 46.25 | 18.44 | -60.14 | 38.25 | 39.69 | 3.76 |
| Bulgaria | 32.09 | 41.23 | 28.51 | 32.21 | 31.89 | -0.98 | 41.65 | 55.35 | 32.91 |
| Romania | 51.10 | 31.85 | -37.67 | 47.79 | 47.41 | -0.80 | 64.96 | 39.16 | -39.72 |
| Serbia | 44.78 | 72.38 | 61.64 | 33.25 | 57.44 | 72.74 | 71.03 | 53.94 | -24.06 |
| North Macedonia | 38.28 | 35.57 | -7.07 | 30.02 | 37.23 | 24.00 | 79.06 | 49.78 | -37.04 |
Table 8.
Average sitting and screen time pre and post intervention.
| Vigorous Activity | Moderate Activity | Walking | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre Intervention | Post Intervention | % Difference | Pre Intervention | Post Intervention | % Difference | Pre Intervention | Post Intervention | % Difference | |
| Total | 244.34 | 190.33 | -22.11 | 292.83 | 255.67 | -12.69 | 215.21 | 181.83 | -15.51 |
| Greece | 324.38 | 341.88 | 5.39 | 379.69 | 556.25 | 46.50 | 244.38 | 278.13 | 13.81 |
| Bulgaria | 322.10 | 321.38 | -0.22 | 318.15 | 361.44 | 13.61 | 205.73 | 312.88 | 52.08 |
| Romania | 322.77 | 106.35 | -67.05 | 324.86 | 154.14 | -52.55 | 229.81 | 141.84 | -38.28 |
| Serbia | 223.50 | 139.00 | -37.81 | 246.65 | 213.00 | -13.64 | 190.14 | 82.31 | -56.71 |
| North Macedonia | 93.84 | 162.73 | 73.41 | 263.99 | 233.17 | -11.67 | 229.05 | 168.60 | -26.39 |
Table 9.
Effectiveness of interventions on well being.
| Very weak | Weak | Fair | Effective | Very effective | |
|---|---|---|---|---|---|
| Total | 1.17 | 47.21 | 4.11 | 22.29 | 25.22 |
| Greece | 18.75 | 18.75 | 0.00 | 37.50 | 25.00 |
| Bulgaria | 1.22 | 58.54 | 13.41 | 21.95 | 4.88 |
| Romania | 0.00 | 44.44 | 1.23 | 14.81 | 39.51 |
| Serbia | 0.00 | 56.25 | 0.00 | 17.50 | 26.25 |
| North Macedonia | 0.00 | 35.37 | 2.44 | 31.71 | 30.49 |
Table 10.
Effectiveness of interventions on well being.
| Very weak | Weak | Fair | Effective | Very effective | |
|---|---|---|---|---|---|
| Total | 2.05 | 48.09 | 3.81 | 18.77 | 27.27 |
| Greece | 18.75 | 31.25 | 0.00 | 6.25 | 43.75 |
| Bulgaria | 3.66 | 54.88 | 12.20 | 24.39 | 4.88 |
| Romania | 0.00 | 48.15 | 0.00 | 16.05 | 35.80 |
| Serbia | 0.00 | 47.50 | 0.00 | 17.50 | 35.00 |
| North Macedonia | 1.22 | 45.12 | 3.66 | 19.51 | 30.49 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



