
Submitted:
10 July 2025
Posted:
11 July 2025
You are already at the latest version
Abstract
Background: The presence of (1→3)-β-D-Glucan (BDG) in serum may be indicative of in-vasive fungal disease (IFD), but even without IFD elevated BDG can be associated with adverse patient outcomes. Methods: COVID-19 infected patients (n=125) who were screened for IFD with fungal biomarkers were evaluated to assess the prognostic value of BDG. BDG was correlated with patients’ mortality, while considering the influences of IFD and anti-fungal therapy (AFT). Results: A BDG concentration >31pg/mL was associated with significant mortality in the absence of documented IFD and without subsequent an-tifungal therapy (≤31pg/mL: 28% vs >31pg/mL: 91%; P = 0.0001). In patients without IFD but with a BDG >31pg/mL, mortality dropped to 50% when AFT was administered. In pa-tients with a BDG >31pg/mL, no IFD nor AFT then the average probability of death is 3.38-fold greater. Conclusions: Elevated serum BDG is associated with significant mortal-ity in COVID -19 infected patients without IFD, irrespective of AFT. A BDG associated proinflammatory response might be driving the high mortality. BDG serves as a prognos-tic marker in COVID -19 infected patients with or without IFD. When BDG is very low (≤31pg/mL) the likelihood of death remains consistent with the background morality rates for COVID-19 within the ICU.
Keywords:
(1→3)-β-D-Glucan
; mortality
; antifungals
; invasive fungal disease
Professor P. Lewis White, PHW Mycology Reference laboratory and Centre for trials research – division of infection and immunity, UHW, Cardiff, UK. Tel No: +44 (0)29 2027 6581
1. Introduction
COVID-19 can give rise to a wide spectrum of disease manifestations from asymptomatic infection to life threatening multi organ failure [1]. There is substantial risk of secondary invasive fungal disease (IFD) during COVID-19 infection due to immunosuppressive medications and virus-related immune dysregulation [2]. IFD can lead to deleterious effects in COVID-19 infected patients if not diagnosed and treated promptly. A considerable rise in mortality (48.5%) was observed in patients with secondary IFD during COVID-19 pandemic compared to baseline rates [2].
Determining a prognostic marker in COVID -19 is invaluable due to its unpredictable clinical course. Different blood-based biomarkers such as PCT, CD4+/CD8+ ratio, IL-6 etc have been evaluated in previous studies showing correlation with disease severity [1,3]. (1-3)-beta-D-glucan (BDG) is a polysaccharide in most pathogenic fungal cell walls, including Candida and Aspergillus species and is considered a broad fungal marker (excluding most cryptococci and zygomycetes) which is useful in early detection of IFD [4]. Apart from fungi, BDG is considered as a common component in the human diet, as well as in some bacteria, cereals (barley and oats) and seaweeds [5]. Therefore, interpretation of BDG may be challenging due to false positivity associated with translocation, clinical conditions and interventions [6].
Serial measurement of BDG has shown good prognostic value in ICU patients with proven invasive candidiasis (IC), where a decrease in BDG was associated with reduced mortality [7]. While BDG is commonly used to screen for IFD in susceptible patients using its negative predictive value to exclude disease, new evidence is emerging indicating that it generates profound proinflammatory responses with the involvement of TH-1 and TH-17 cells and is associated with poor prognosis, irrespective of the presence IFD [8,9].
As the majority of IFD in COVID-19 infected patients in the Western Hemisphere was caused by Aspergillus (21.5%) and Candida (21.5%) species [2], evaluating the value of BDG in COVID-19 infected patients may be beneficial for predicting mortality. During the COVID-19 pandemic, BDG testing formed part of the diagnostic strategy for IFD screening of high-risk critical-care patients in Wales [10]. The current study was designed to assess the prognostic value of BDG in COVID-19 infected patients with or without defined IFD and antifungal therapy (AFT).
2. Materials and Methods
Patients and Study Design
At the start of the COVD-19 pandemic and in recognition of the likely increased risk of IFD in the critical-care patient with severe respiratory viral infection, a diagnostic algorithm including BDG (amongst other mycological tests) was introduced [10]. The clinical performance and utility of this approach was previously described and demonstrated the significant negative impact of IFD in this cohort and the benefits of appropriate AFT. Given the emerging evidence indicating BDG positivity to be a poor prognostic marker, particularly when positivity is prolonged, it was decided to evaluate the impact of BDG positivity in the previously defined cohort.
All patients screened for BDG in serum/plasma (125 of the original 135 patients) during the first wave of the pandemic in Wales were included in the current study. Testing was performed, and all data was retrieved as part of routine diagnostic assessment. The current evaluation was undertaken as a retrospective, anonymous evaluation with no impact on patient management, subsequently not requiring ethical approval.
Detection of (1→3)-β-D-Glucan
BDG testing of serum or plasma samples was performed using Associates of Cape Cod Fungitell assay following the manufacturer’s instructions. Samples were tested in duplicate and the following thresholds were used to interpret results:Negative, ≤60 pg/ mL; Indeterminate, 60 –79 pg/mL; Positive, ≥80 pg/mL
Statistical Analysis
Receiver operator characteristic curve analysis was performed to determine an optimal threshold for correlating BDG concentration and prognosis. A value of >31 pg/ml was deemed optimal. For analytical purposes, the impact of a higher BDG value of ≥60 pg/mL was also evaluated. Logistic regression analysis was performed to determine any association between increasing BDG concentration and prognosis. An overall mortality rate for the entire cohort was determined, from which additional mortality rates were calculated dependent on the designated BDG threshold and subsequent diagnosis of IFD/fungal infection and/or the use of appropriate AFT (Table 1). AFT was considered appropriate if it correlated with guidelines for the management of a particular IFD or if it were deemed appropriate for the fungal species cultured. For proportional values, 95% confidence intervals (95% CI) were calculated, which were also used, along with the Fisher’s exact test to determine the significance of any differences between proportional values. When comparing means/medians the representative T-tests were performed. For all statistical comparisons a P value of ≤0.05 was considered significant
3. Results
Population
One hundred and twenty-five COVID-19 infected patients requiring critical care management were included in this study. The overall mortality was 38% (47/125; 95% CI: 29.6-46.3). The male/female ratio was 2.28/1, with an average age of 58 and 54 years for men and women respectively. There was a significant correlation between increasing age and mortality (Odds ratio: 1.0638 (95% CI: 1.0271-1.1018; P: 0.0006)) (Figure 1). There was no linear correlation between age and BDG concentration (Odds ratio: 1.0046 (95% CI: 0.9728-1.0374; P: 0.7802)). Mortality rate in men was 41% (36/87, 95% CI: 32-52), compared to 29% (11/38, 95% CI: 17-45) in women (P: 0.2303). There was no significant correlation between gender and mortality (Odds ratio: 1.7326 (95% CI: 0.7626-3.9366; P: 0.1819))
(1→3)-β-D-Glucan Concentration and Mortality
In 89/125 patients the highest recorded BDG concentration was ≤31 pg/mL (81% (63/78) of surviving patients compared to 55% (26/47) of deceased patients). Subsequently, the mortality rate was significantly greater when BDG concentrations were >31pg/ml (58%) compared to ≤31 pg/mL (29%) (Table 1, Figure 1 and Figure 2). Twenty-eight percent of patients who died (13/47) had a BDG concentration >60 pg/ml compared to 15% of patients who survived (12/78) (P: 0.1103). Nineteen percent of patients who died (9/47) had a BDG concentration >80 pg/ml compared to 14% of patients who survived (11/78) (P: 0.4617) and 11 percent of patients who died (5/47) had a BDG concentration >500 pg/ml compared to 8% of patients who survived (6/78) (P: 0.7459). Subsequently, there was no significant linear correlation between increasing BDG concentration and mortality.
Logistic regressions analysis confirmed a significant correlation between a BDG concentration >31 pg/mL and mortality (Odds ratio: 3.3923 (95% CI: 1.5169-7.5863; P: 0.0026)). Multivariable logistic regression analysis confirmed both increasing age and a BDG concentration >31 pg/mL to be significantly associated with mortality (Overall model fit P: <0.0001), where across the age range, the presence of a BDG concentration >31 pg/mL increased the probability of mortality by a mean of 2.35-fold (Figure 1).
There was a trend between a BDG concentration >60 pg/ml and mortality (Odds ratio: 2.1029 (95% CI: 0.8662-5.1057; P: 0.1008)) and the mortality of patients with a highest BDG concentration above this threshold was, on average, 1.73-fold greater (Figure 1).
Antifungal Therapy and Mortality
Thirty-four percent (42/125) of patients received AFT deemed appropriate for the management of their IFD. When not considering the BDG concentration, the mortality rate when AFT was administered was comparable to that in the absence of AFT (16/42: 38.1% vs 31/83: 37.4%, P: 1.0000). Mortality remained similar for patients receiving AFT, regardless of the calculated BDG concentration (Table 1). However, in patients not receiving AFT, the presence of a BDG concentration >31 pg/mL was associated with a significant increase in mortality (92%) compared to those with a BDG ≤31 pg/mL (33%). Using a higher BDG threshold of ≥60 pg/mL was associated with 100% mortality rate in patients not receiving AFT, significantly greater than in patients not receiving AFT but with a BDG concentration <60 pg/mL (33%, P: 0.0008).
Mortality Associated with Invasive Fungal Disease
Twenty-one percent (26/125) of patients were diagnosed with IFD or a fungal line infection. When not considering the BDG concentration, the mortality rate when IFD/line infection was diagnosed was comparable to that in the absence of IFD (11/26: 42.3% vs 36/99: 36.3%, P: 0.6511). Mortality remained similar for patients with IFD, regardless of the calculated BDG concentration (Table 1). However, in patients without IFD, the presence of a BDG concentration >31 pg/mL was associated with a significant increase in mortality (74%) compared to those with a BDG ≤31 pg/mL (28%). This was maintained when using a higher BDG threshold of ≥60 pg/mL, mortality being 83% mortality rate in patients without IFD, compared to 30% in patients without and with a BDG concentration <60 pg/mL (53%, P: 0.0006).
Mortality Associated with Invasive Fungal Disease and the Use of Antifungal Therapy
Eighty-eight percent (23/26) of patients with IFD/fungal line infection received appropriate AFT. The mortality rate in patients with IFD/fungal line infection receiving appropriate AFT when not considering the BDG concentration was 39% (9/23) compared to 67% (2/3) of patients with IFD/fungal line infection who did not receive AFT (P: 0.5558). There was no difference in mortality in patients with IFD/fungal line infection receiving appropriate AFT, regardless of the calculated BDG concentration (Table 1). In patients with IFD/fungal line infection not receiving appropriate AFT, 100% died when the BDG concentration was >31 pg/mL, compared to 0% when the BDG concentration was ≤31 pg/mL, although this did not reach statistical significance due to the limited number of patients (Table 1).
Nineteen percent (19/99) of patients without IFD/fungal line infection received AFT. The mortality rate in patients without IFD/fungal line infection receiving AFT when not considering the BDG concentration was 37% (7/19) compared to 36% (29/80) of patients without IFD/fungal line infection who did not receive AFT (P: 1.000). There was no difference in mortality in patients without IFD/fungal line infection receiving AFT, regardless of the calculated BDG concentration (Table 1). In patients without IFD/fungal line infection, not receiving AFT, 91% died when the BDG concentration was >31 pg/mL, compared to 28% when the BDG concentration was ≤31 pg/mL (P: 0.0001) (Table 1).
Multivariable logistic regression analysis confirmed that age and a combined variable where BDG was >31 pg/mL, but there was no IFD nor AFT were significantly associated with mortality (P <0.0001). While the association with age generated a significant, yet minimal odds ratio (1.0472, 95% CI: 1.0111-1.0846, P: 0.01), the combined variable generated a significant and substantial odds ratio (25.7889, 95% CI: 3.0357-219.0793, P: 0.0029) that equated to, on average a substantial, and 3.38-fold increase in the probability of death across all ages (Figure 1).
4. Discussion
COVID-19 infection can be complicated by IFD leading to increased mortality. Strategic mycological testing plays a major role directing appropriate antifungal therapy and survival of these patients [10]. BDG is a major cell wall component of many pathogenic fungi aiding the diagnosis of IFD through its detection in serum using validated and reproducible techniques [13]. Its high negative predictive value has made it suitable as a surrogate marker excluding IFD, stratifying antifungal treatment and the duration of empirical AFT [7,14,15].
BDG is a pathogen-associated molecular pattern (PAMPs) recognized by various immune receptors of immune cells such as monocytes, macrophages, natural killer cells and dendritic cells. C-type lectin receptors, mainly dectin-1, play a major role in the proinflammatory immune response associated with BDG with the involvement of T-helper 1 and T-helper 17 cells [8,9]. In sepsis, bacterial and fungal PAMPs can be translocated from the gut, including Endotoxins (LPS) from Gram-negative bacteria and BDG from fungi or other non-fungal sources causing a severe inflammatory response [16].
The prognostic value of high BDG concentrations leading to a worse clinical outcome likely being due a host proinflammatory innate immune response is an emerging concern [17] and studies have evaluated the value of BDG as a prognostic marker in different patient groups [7,9]. A significant morbidity and mortality were associated in patients following abdominal surgery who had persistent or increasing BDG in their circulation regardless of IC or antifungal treatment, highlighting its significance as a prognostic indicator [9]. The significance of BDG on the prognosis of critical care COVID-19 patients, where all-cause mortality rates are already substantial (approx. 30%) and who are susceptible to secondary IFD is less clear [18]. While studies have investigated the prognostic implications of the presence of serum/plasma BDG during COVID-19 infection, correlation with IFD (an obvious source of BDG) and its subsequent treatment have not been thoroughly investigated.
At that the start of the pandemic in March 2020, an algorithm for diagnosing IFD within the critical care COVID-19 patient was introduced across Wales and this involved BDG screening of serum. Data from the first wave of the pandemic was assessed to determine the prognostic value to BDG in COVID-19 infected patients, according to the presence of documented IFD and/or subsequent AFT. Predictably, increasing age was a demographic factor that correlated with mortality in critical care patients with COVID-19 (Figure 1). This has been documented previously, where the mortality rated was significantly greater in patients ≥65 years old (42%) compared to the younger cohort (11%), but age was not the sole factor in predicting mortality [19]. In the current study, mortality was 30% for patients <65 years old, rising to 58% for the older cohort. When an age threshold of 50 years was employed the mortality rate was 18% and 47%, respectively for the younger and older cohorts.
While there was no correlation between increasing age and BDG concentration, the presence of a BDG concentration >31 pg/mL further increased the probability of death across the age range and on average more than doubled the likelihood of death (Figure 1). The significance of this finding remained at higher BDG concentrations, more typically associated with IFD (e.g., >60 pg/mL). During COVID-19 infection, particularly post the acute phase, higher BDG concentrations have been associated with pro-inflammatory responses linked to increased levels of NF-κB signalling [20]. Given that both respiratory and gastro-intestinal inflammation are common symptoms during COVID-19 infection and increased membrane permeability has been shown associated with higher plasma levels of zonulin (a protein that regulates the permeability of intestinal membranes), translocation of BDG from commensal or colonizing fungi within these host environments appears a plausible source for BDG within the host’s circulation [21]. While it is convenient to apply existing BDG thresholds optimized for the diagnosis of IFD (>60 or >80 pg/ml) to this prognostic approach, it should be accepted that these thresholds will likely differ given the different goals. Indeed, during IFD fungal burdens and subsequent levels of BDG would typically be higher than when compared to BDG translocation sourced from commensal/colonizing fungi. In previous studies assessing the prognostic value of BDG testing, a threshold of >40 pg/ml was deemed optimal and is comparable to the optimal threshold identified in the current study (>31 pg/ml) [20,22]. Applying a BDG threshold of >40 pg/ml to determine patient prognosis in this current study remains significant (OR: 3.1034 95% CI: 1.3439-7.1667, P: 0.0073).
In patients receiving AFT, mortality was typically consistent regardless of the BDG concentration and generally compatible with the mortality rates associated with COVID-19 infection in the critical care patient without secondary IFD, albeit patient numbers are limited for some categories (Table 1). Conversely, in the absence of AFT and/or IFD mortality was significantly greater (at least 2.6-fold) when BDG was higher (>31 pg/mL) than when BDG was low (≤31 pg/mL), where mortality rates were typical of COVID-19 in critical care. In the final multi-logistic regression model, combining BDG >31 pg/mL in the absence of diagnosed IFD and subsequent AFT, the odds ratio associated with mortality was substantial (25.8), increasing the probability of death by, an average, of 3.4-fold over age alone across the age range.
Given the complexity of diagnosing IFD, particularly in cohorts lacking established host and clinical factors, the association with a BDG >31 pg/mL and increased mortality could be associated with undiagnosed IFD rather than a non-infective BDG driven proinflammatory response [15,16,17,18,19]. In patients with no evidence of IFD other than high serum BDG mortality was 91% when not treated with antifungals, falling to 50% when AFT was administered (P: 0.1108, Table 1). Sixty-five percent (17/26) of patients with documented IFD had a BDG >31 pg/mL, compared to 19% (19/99) of patients without documented IFD (P <0.0001). The median BDG concentration of patients with documented IFD and a BDG >31 pg/mL was 386 pg/mL, compared to 70 pg/mL in those without documented IFD and a BDG >31 pg/mL (Unpaired T test P: 0.0307). Thirteen of 17 patients (76%) with documented IFD and a BDG >31 pg/mL would have been considered positive for BDG using the Fungitell threshold of 80 pg/mL, compared to seven of 19 patients (37%) without documented IFD and a BDG >31 pg/mL (P: 0.0228). While indicating that in patients with documented IFD when BDG is present in serum, it is present in higher concentrations consistent with Fungitell thresholds, the response to AFT in the absence of documented IFD implies a degree of undiagnosed IFD is present and highlights the importance of diagnostic performance for detecting IFD and limiting missed diagnoses. When BDG is present >31 pg/mL, the difference in mortality in patients receiving AFT compared to those not receiving AFT highlights a potential trigger for initiating antifungal prophylaxis, when AFT for IFD has not already been administered. In this study only 15% (19/125) of patients would have received additional AFT over those with documented IFD and 64% (80/125) would not require AFT.
Unfortunately, the diagnosis of COVID-19 associated IFD is complicated, and no single test can be considered optimal, particularly when testing blood [23]. Diagnosis of IFD in COVID-19 infected patients might have been compromised due to the limited availability of deep respiratory specimens like bronchoalveolar lavage due to high risk of transmission of infection. In addition, with testing restricted to Aspergillus PCR, Candida PCR (detecting the six most common species), Pneumocystis PCR and Aspergillus antigen testing, the detection rates of IFD could have been increased if pan-fungal PCR testing was also performed. Further limitations include the number of alternative variables that could lead to a poor patient prognosis and could both contribute and conflict with the association of BDG and mortality. Unfortunately, our study lacked data on clinical status (e.g., disease severity score) and regularly documented clinical markers of inflammation (e.g., C-reactive protein, Procalcitonin), and evidence of cytokines/chemokines (IL-6, TNF-α) associated with pro-inflammatory innate immune response.
5. Conclusions
To conclude, 29% of COVID-19 critical care patients had BDG levels >31 pg/mL with mortality at 91% when not treated with antifungal drugs, even in the absence of documented IFD. Both undiagnosed IFD and a non-infective BDG pro-inflammatory response likely contribute to this poor prognosis. Overall, this indicates that high BDG serves as a prognostic marker in COVID - 19 infected patients probably due to the associated systemic inflammatory response irrespective of IFD. In patients with a BDG concentration ≤31 pg/mL, mortality is typically comparable with that for COVID-19 in the critical care patient. Further studies are warranted to evaluate more evidence for BDG associated mortality, its use as a prognostic marker and measures to be taken to minimize BDG levels in serum in critically ill patients with special attention to potential gut translocation of fungal and non-fungal PAMPs.
Author Contributions
Conceptualization, P.L.W.; methodology, P.L.W.; validation, P.L.W. and MB.; formal analysis, P.L.W. and U.W.; investigation, J.S.P and R.P.; resources, P.L.W.; data curation, P.L.W.; writing—U.W. and P.L.W, X.X.; writing—review and editing, M.B., J.S.P and R.P.; supervision, P.L.W.; project administration, J.S.P. All authors have read and agreed to the published version of the manuscript
Institutional Review Board Statement
“Ethical review and approval were waived for this study due to REASON as the study formed a retrospective, anonymous review of data collated during routine clinical practice with no impact on patient management.
Informed Consent Statement
Patient consent was waived as this study formed a retrospective, anonymous review of data collated during routine clinical practice with no impact on patient management.
Data Availability Statement
All data used for the calculations in this study are provided within the manuscript.
Conflicts of Interest
PLW: has performed diagnostic evaluations and received meeting sponsorship from Associates of Cape Cod, Bruker, Dynamiker, and Launch Diagnostics; speaker fees, expert advice fees, and meeting sponsorship from Gilead and Mundipharma; speaker and expert advice fees from Pfizer and expert advice fees from F2G.
All other authors: No conflicts disclosed.
Abbreviations
The following abbreviations are used in this manuscript:
| IFD | Invasive fungal disease |
| PCT | Procalcitonin |
| BDG | (1-3)-β-D-Glucan |
| AFT | Antifungal therapy |
| EORTC | European Organization for the research and treatment of Cancer |
| MSGERC | Mycoses Study group Educational and Research Consortium |
| ECMM | European Confederation of Medical Mycology |
| ISHAM | International Society for Human and Animal Mycoses |
| CAPA | COVID-19 Associated pulmonary aspergillosis |
| 95% CI | 95% confidence intervals |
| PAMPs | pathogen-associated molecular pattern |
| LPS | Lipopolysaccharide |
| IC | Invasive candidiasis |
References
- Arnold DT, Attwood M, Barratt S, Morley A, Elvers KT, McKernon J, et al. Predicting outcomes of COVID-19 from admission biomarkers: a prospective UK cohort study. Emerg Med J. 2021 Jul;38(7):543–8. [CrossRef]
- Gold JAW, Adjei S, Gundlapalli AV, Huang YLA, Chiller T, Benedict K, et al. Increased Hospitalizations Involving Fungal Infections during COVID-19 Pandemic, United States, January 2020–December 2021. Emerg Infect Dis [Internet]. 2023 Jul [cited 2025 May 14];29(7). Available from: https://wwwnc.cdc.gov/eid/article/29/7/22-1771_article.
- Mittal R, Chourasia N, Bharti VK, Singh S, Sarkar P, Agrawal A, et al. Blood-based biomarkers for diagnosis, prognosis, and severity prediction of COVID-19: Opportunities and challenges. Journal of Family Medicine and Primary Care. 2022 Aug;11(8):4330–41.
- Giacobbe DR, Esteves P, Bruzzi P, Mikulska M, Furfaro E, Mesini A, et al. Initial serum (1,3)-β-d-glucan as a predictor of mortality in proven candidaemia: findings from a retrospective study in two teaching hospitals in Italy and Brazil. Clinical Microbiology and Infection. 2015 Oct;21(10):954.e9-954.e17. [CrossRef]
- Singh RP, Bhardwaj A. β-glucans: a potential source for maintaining gut microbiota and the immune system. Front Nutr. 2023 May 5;10:1143682. [CrossRef]
- Yamamoto T, Oishi K, Suizu J, Murakawa K, Hisamoto Y, Fujii T, et al. False-positive Elevation of Beta-D-glucan and Aspergillus Galactomannan Levels Due to Mendelson’s Syndrome after Rice Aspiration. Intern Med. 2022 Oct 1;61(19):2935–9.
- Carelli S, Posteraro B, Torelli R, De Carolis E, Vallecoccia MS, Xhemalaj R, et al. Prognostic value of serial (1,3)-β-d-glucan measurements in ICU patients with invasive candidiasis. Crit Care. 2024 Jul 12;28(1):236.
- Hardison SE, Brown GD. C-type lectin receptors orchestrate antifungal immunity. Nat Immunol. 2012 Sep;13(9):817–22.
- White PL, Posso R, Parr C, Price JS, Finkelman M, Barnes RA. The Presence of (1→3)-β-D-Glucan as Prognostic Marker in Patients After Major Abdominal Surgery. Clinical Infectious Diseases. 2021 Oct 5;73(7):e1415–22. [CrossRef]
- White L, Dhillon R, Cordey A, Hughes H, Faggian F, Soni S, et al. A National Strategy to Diagnose COVID-19 Associated Invasive Fungal Disease in the ICU. SSRN Journal [Internet]. 2020 [cited 2025 May 14]; Available from: https://www.ssrn.com/abstract=3644400.
- Koehler P, Bassetti M, Chakrabarti A, Chen SCA, Colombo AL, Hoenigl M, et al. Defining and managing COVID-19-associated pulmonary aspergillosis: the 2020 ECMM/ISHAM consensus criteria for research and clinical guidance. The Lancet Infectious Diseases. 2021 Jun;21(6):e149–62.
- Donnelly JP, Chen SC, Kauffman CA, Steinbach WJ, Baddley JW, Verweij PE, et al. Revision and Update of the Consensus Definitions of Invasive Fungal Disease From the European Organization for Research and Treatment of Cancer and the Mycoses Study Group Education and Research Consortium. Clinical Infectious Diseases. 2020 Sep 12;71(6):1367–76.
- Carolis ED, Marchionni F, Torelli R, Posteraro P, Pascale GD, Carelli S, et al. Comparable Serum and Plasma 1,3--D-Glucan Values Obtained Using the Wako -Glucan Test in Patients with Probable or Proven Fungal Diseases. 2019;57(5).
- De Pascale G, Posteraro B, D’Arrigo S, Spinazzola G, Gaspari R, Bello G, et al. (1,3)-β-d-Glucan-based empirical antifungal interruption in suspected invasive candidiasis: a randomized trial. Crit Care. 2020 Dec;24(1):550.
- De Pascale G, Tumbarello M. Fungal infections in the ICU: advances in treatment and diagnosis. Current Opinion in Critical Care. 2015 Oct;21(5):421–9.
- Amornphimoltham P, Yuen PST, Star RA, Leelahavanichkul A. Gut Leakage of Fungal-Derived Inflammatory Mediators: Part of a Gut-Liver-Kidney Axis in Bacterial Sepsis. Digestive Diseases and Sciences. 2019 Sep 1;64(9):2416–28.
- Giacobbe DR, Esteves P, Bruzzi P, Mikulska M, Furfaro E, Mesini A, et al. Initial serum (1,3)-β-d-glucan as a predictor of mortality in proven candidaemia: findings from a retrospective study in two teaching hospitals in Italy and Brazil. Clinical Microbiology and Infection. 2015 Oct;21(10):954.e9-954.e17.
- Carbonell R, Urgelés S, Rodríguez A, Bodí M, Martín-Loeches I, Solé-Violán J, et al. Mortality comparison between the first and second/third waves among 3,795 critical COVID-19 patients with pneumonia admitted to the ICU: A multicentre retrospective cohort study. The Lancet Regional Health - Europe. 2021 Dec;11:100243.
- Bakakos A, Koukaki E, Ampelioti S, Ioannidou I, Papaioannou AI, Loverdos K, et al. The Real Impact of Age on Mortality in Critically Ill COVID-19 Patients. JPM. 2023 May 29;13(6):908.
- Giron LB, Peluso MJ, Ding J, Kenny G, Zilberstein NF, Koshy J et al. Markers of fungal translocation are elevated during post-acute sequelae of SARS-CoV-2 and induce NF-κB signaling. JCI Insight. 2022 Aug 8;7(15):e160989. [CrossRef]
- Fasano, A. Zonulin and Its Regulation of Intestinal Barrier Function: The Biological Door to Inflammation, Autoimmunity, and Cancer. Physiological Reviews. 2011 Jan;91(1):151–75.
- Kitsios GD, Kotok D, Yang H, Finkelman MA, Zhang Y, Britton N, et al. Plasma 1,3-β-d-glucan levels predict adverse clinical outcomes in critical illness. JCI Insight. 2021 Jul 22;6(14):e141277.
- Hurt W, Youngs J, Ball J, Edgeworth J, Hopkins P, Jenkins DR, et al. COVID-19-associated pulmonary aspergillosis in mechanically ventilated patients: a prospective, multicentre UK study. Thorax. 2024 Jan;79(1):75–82.
Figure 1.
The probability of death in COVID-19 critical care patients according to age, BDG concentration and the presence of invasive fungal disease and subsequent antifungal therapy.
Figure 1.
The probability of death in COVID-19 critical care patients according to age, BDG concentration and the presence of invasive fungal disease and subsequent antifungal therapy.
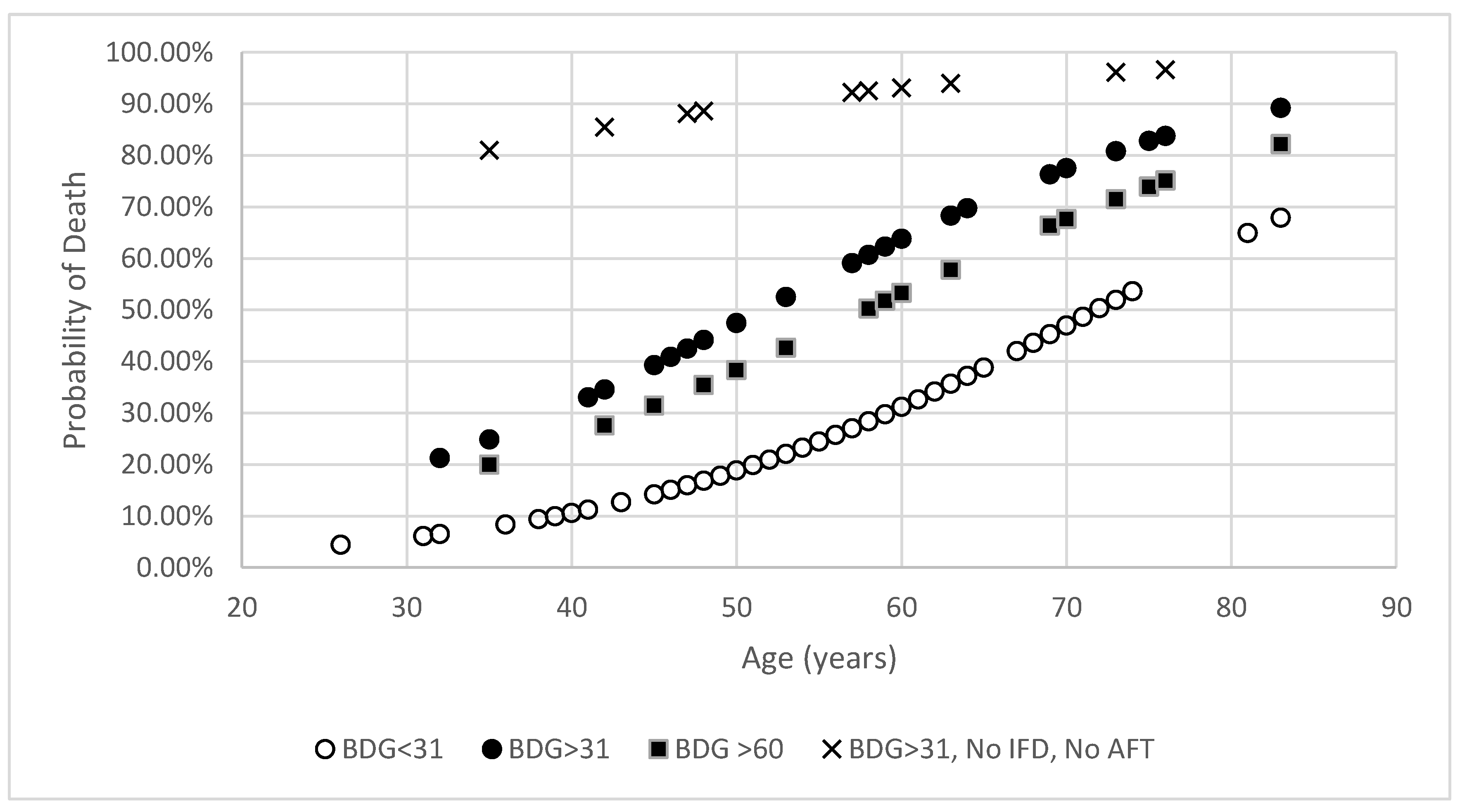
Figure 2.
The distribution of (1→3)-β-D-glucan concentrations among the 125 patients screened by the Associates of Cape Cod Fungitell assay, along with association with mortality with or without evidence of invasive fungal diseases and anti-fungal treatment.
Figure 2.
The distribution of (1→3)-β-D-glucan concentrations among the 125 patients screened by the Associates of Cape Cod Fungitell assay, along with association with mortality with or without evidence of invasive fungal diseases and anti-fungal treatment.
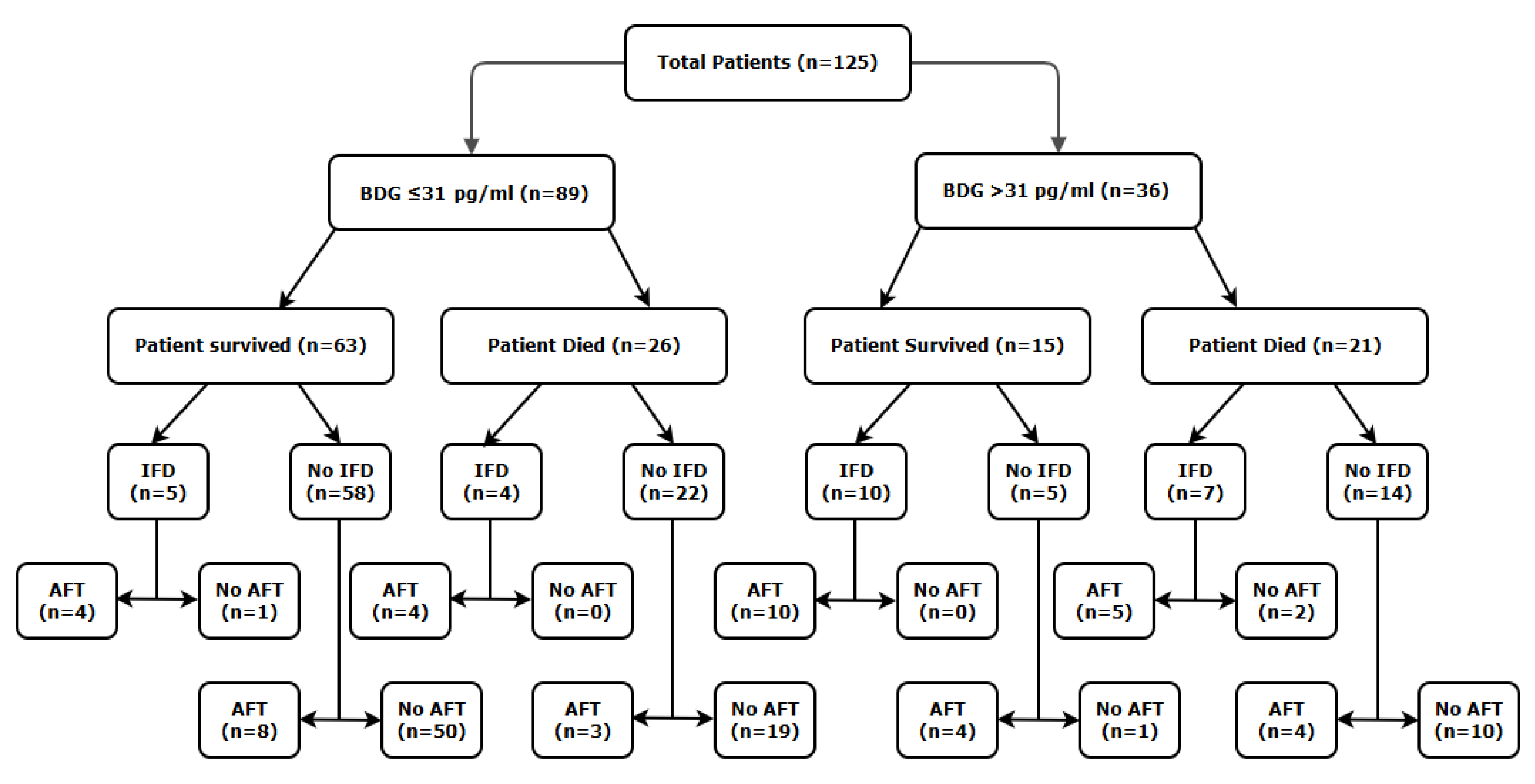

Table 1.
Mortality rate associated with (1→3)-β-D-Glucan concentration (Threshold: 31 pg/mL) and invasive fungal diseases with or without antifungal therapy. Significant differences are highlighted in bold text.
Table 1.
Mortality rate associated with (1→3)-β-D-Glucan concentration (Threshold: 31 pg/mL) and invasive fungal diseases with or without antifungal therapy. Significant differences are highlighted in bold text.
| Classification | Mortality rate (n/N, (%)) | |||
|---|---|---|---|---|
| BDG concentration | Difference in Mortality (95% CI) | Significance (P value) |
||
| ≤31 pg/mL | >31 pg/mL | |||
| Overall | 26/89 (29%) | 21/36 (58%) | 29% (10.0 to 45.9) | 0.0039 |
| AFT | 7/19 (37%) | 9/23 (39%) | 2% (29.1 to -25.6) | 1.0000 |
| No AFT | 19/70 (27%) | 12/13 (92%) | 65% (37.1 to 76.2) | <0.0001 |
| IFD | 4/9 (44%) | 7/17 (41%) | 3% (31.0 to -38.2) | 1.0000 |
| No IFD | 22/80 (28%) | 14/19 (74%) | 46% (21.3 to 63.0) | 0.0003 |
| IFD with AFT | 4/8 (50%) | 5/15 (33%) | 17% (21.2 to -50.4) | 0.6570 |
| IFD without AFT | 0/1 (0%) | 2/2 (100%) | 100% (30.5 to -100) | 0.3333 |
| No IFD with AFT | 3/11 (27%) | 4/8 (50%) | 23% (18.1 to -56.2) | 0.3765 |
| No IFD without AFT | 19/69 (28%) | 10/11 (91%) | 63% (32.5 to 75.2) | 0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



