
Submitted:
10 July 2025
Posted:
11 July 2025
You are already at the latest version
Abstract
(1) Background: Physical activity (PA) is a key modifiable risk factor for chronic diseases, yet many adults do not meet PA guidelines. Just-in-time adaptive interventions (JITAIs), a type of mobile health (mHealth) intervention, offer tailored support based on an individual’s context to promote PA. Integrating behavior change techniques (BCTs) and theories is critical to the design of effective mHealth interventions. Understanding which BCTs and theories work best can inform future JITAI development. (2) Objective: To examine how behavior change theories and BCTs are implemented in mHealth PA JITAIs and assess their relationship to PA-related outcomes. (3) Methods: This scoping review followed the PRISMA-ScR guidelines. A total of 29 studies were included. (4) Results: The most commonly used BCTs include prompts/cues, goal setting (behavior), feedback on behavior, and self-determination theory and social cognitive theory are the most commonly used theory. However, there is insufficient evidence as to which theories and BCTs are most effective in eliciting effective PA behavior change. (5) Conclusion: Clearer re-porting and integration of BCTs and behavior change theories, along with optimized user interfaces, are needed to improve intervention quality, replicability, and long-term effectiveness of PA JITAIs.
Keywords:
physical activity
; digital health
; mobile health
; just-in-time adaptative interventions
1. Introduction
Chronic diseases, such as cardiovascular disease, chronic respiratory diseases, and diabetes are the leading causes of death worldwide, responsible for 39 million (72%) of all global deaths in 2021 [1]. Physical activity (PA) has been shown to be a key modifiable risk factor for many chronic conditions and can serve as a powerful lifestyle strategy for both management and prevention of chronic disease [2]. Despite these well-known benefits, almost one third of adults worldwide do not meet the recommendations of at least 150 minutes of moderate intensity PA, or 75 minutes of vigorous intensity PA per week [3]. While in-person PA interventions can be an effective option for combating inactivity, they often face challenges related to accessibility, cost, and scalability, particularly when targeting general populations [4,5]. In response, there is a growing need for innovative, scalable, and personalized approaches to support PA among adults not currently meeting PA guidelines.
The widespread adoption of smartphones has created new opportunities to deliver PA promotion interventions. In Canada and the United States, over 84% of the population now owns a smartphone, and an estimated 60% of the world owns a smartphone [6]. This increase in digital connectivity has supported the growth of mobile health (mHealth) interventions, which offer scalable and personalized solutions for promoting PA. Recent technological advancements of smartphones combined with wearable technology have also enabled a new type of mHealth intervention known as a just-in-time adaptive intervention, or JITAI. These interventions use real-time data from wearable sensors to adapt the timing and content of support based on an individual’s current context and state. This allows the intervention to be delivered at moments when the individual is both in need of support and most likely to respond positively [7]. JITAIs are a novel method of delivering mHealth interventions, which adapts the support provided based on the individual’s status and context to deliver the intervention not only when the individual needs it, but when they will be most receptive to the intervention [8]. Previous systematic reviews have already shown that JITAIs are more effective than non-JITAI interventions (g = 0.868, 95% CI = 0.41, 1.32) [9]. Although JITAIs show considerable promise, there is limited evidence on how behavior change theories and techniques have been applied in PA interventions.
Behavior change theories provide a conceptual framework for understanding behavior change. They help identify the mechanisms of action (e.g., motivation, self-efficacy, habit) that underpin behavior change [10]. JITAIs offer dynamic support by leveraging insights from traditional theoretical frameworks. For instance, JITAIs can foster autonomous motivation by delivering timely prompts that align with an individual’s goals, values, and sense of volition, which align with Ryan and Deci’s self-determination theory [11,12]. From a social cognitive perspective, JITAIs can enhance self-regulation by offering real-time feedback and support when individuals are most in need of reinforcement [13]. In turn, behavior change techniques (BCTs) are the observable components of interventions that translate theoretical constructs into practical strategies [14]. Examples of these practical strategies include goal setting, self-monitoring, or providing feedback, that can be implemented to change behavior. Overall, the behavior theories guide the selection of appropriate BCTs, which in turn operationalize those theories within behavior change interventions. Thus, understanding how behavior change theories and techniques have been used in PA JITAIs, as well as which theories and techniques are effective, can provide important information for the design of future PA JITAIs.
In addition, there is a lack of reviews on how adaptive algorithms are designed and implemented in JITAIs. These algorithms determine how interventions respond dynamically to user data by adjusting the timing, type, and content of support based on behavior theories and techniques. For example, some JITAIs tailor prompts based on real-time PA levels, user goals, time of day, or contextual features, such as weather [15]. Others incorporate features such as recommender systems based on user preferences [16], or artificial intelligence (AI)–driven chatbots that allow for conversational support [17]. While these approaches reflect increasing sophistication, the underlying logic, decision rules, and data inputs used to guide personalization are often poorly described. This lack of transparency hinders efforts to evaluate, replicate, and optimize JITAI design.
Therefore, the objectives of this review are 1) to describe the implementation of behavior change theories, techniques, and the JITAI personalization algorithms in JITAIs designed to promote PA, and 2) to explore whether the use of certain theories and techniques in JITAIs led to greater improvements in PA outcomes.
2. Materials and Methods
This scoping review was conducted following the Preferred Reporting Items for Systematic reviews and Meta-Analyses guidelines extension for Scoping Reviews (PRISMA-ScR) Checklist [18] and completed using Covidence software [19]. The completed PRISMA-ScR checklist is available in Appendix A. The review protocol was pre-registered on the Open Science Framework prior to publication [20]. Due to the nature of conducting a scoping review, ethics approval was not required for this work. We conducted an electronic literature search of Web of Science (EBSCO), MEDLINE (Ovid), PsycINFO (EBSCO), and SPORTDiscus (EBSCO). The search strategy consisted of three searches focusing on mHealth, JITAIs and PA, respectively, which were combined to provide our results. The mHealth search string consisted of terms such as “mobile health”, “Smartphones” and “Apple Watch”. The JITAI search string consisted of terms such as “just-in-time", “dynamic tailor” and “real time intervention”. An example search strategy and results for PsycINFO (EBSCO) is available in Appendix B. Additionally, reference lists were searched from relevant identified articles to detect any articles that were missed by our search strategy.
2.1. Eligibility Criteria
Studies deemed sufficient for further review from the search results had their titles and abstracts screened independently by the two authors (PC, AW) to make exclusions. Our search strategy was executed in November 2024. Studies were selected for full-text review if they met all the following criteria: published in a peer-reviewed journal, the study described or used a mobile-based PA JITAI, and published in English. There was no restraint in terms of the date range for studies included in our literature search. Types of studies that met the criteria include protocol studies, intervention studies, randomized controlled trials, rationale and design studies, micro-randomized trial studies, participatory development studies, pilot studies, experimental studies, and feasibility studies. Studies that met these criteria were then entered into the full-text review, where they were thoroughly analyzed to determine whether they would be included in the review. Discrepancies in included texts by each author were settled through discussion between PC and AW at both the title and abstract screening stage, and the full-text review stage. In all instances, consensus was reached through discussion, and there were no unresolved disagreements that required arbitration. As a result, a third reviewer was not needed.
2.2. Data Extraction
We extracted the following characteristics from the selected studies into a spreadsheet for further analysis: 1) BCTs stated (BCTs explicitly stated within a study by the author), 2) BCTs implied (Two authors (PC, AW) independently identified BCTs implied in studies by aligning if the author descriptions of intervention descriptors aligned with the BCT taxonomy [21]; both reviewers compared coding results and resolved discrepancies through discussion until consensus was reached), 3) behavior change theory, 4) JITAI decision tree or algorithm, 5) description of JITAI, 6) intervention length, 7) desired outcome, 8) findings, 9) PA description, and 10) comparator. All data extracted from the review is available in Appendix C.
2.3. Data Synthesis
We chose to do a scoping review rather than a systematic review or meta-analysis due to the variation of PA measurements and outcomes used by researchers. For our analysis, we initially identified and compiled a list of behavior change theories and techniques that had been implemented for JITAI PA interventions, their prevalence amongst the reviewed literature, and how these features had been delivered using mHealth tools. The behavior change technique taxonomy v1 from Michie and colleagues (2013) was used as our guide for BCTs.
To further explore the implementation of BCTs, we explored BCT combinations, analyzing how specific combinations of BCTs co-occur within interventions [22]. This approach recognizes that BCTs are often not applied in isolation, but in conjunction with others, potentially enhancing intervention effectiveness. Upon extracting individual BCTs from each study, we identified pairings through frequency counts where two BCTs were deliberately integrated to influence PA behavior. To assess the effectiveness of individual BCTs and their pairings, we examined their association with significant improvements in PA outcomes, such as increased PA time or step counts. This analysis aimed to identify which BCTs, and combinations thereof were linked to positive behavioral changes.
Furthermore, we conducted a descriptive analysis of the design and implementation of adaptive algorithms within JITAIs, which sought to determine how interventions respond dynamically to user data by adjusting the timing, type, and content of support based on behavior theories and BCTs. We extracted information of decision points, tailoring variables, intervention options, and decision rules from each study, where available.
3. Results
3.1. Study Selection
As shown in Figure 1, 1778 studies were imported for screening, 1761 from databases/registers and 17 from other sources. Of those 1778 studies, 29 met the entire inclusion criteria and were included in the final review.
3.2. Study and Participant Characteristics
Of the 29 studies included, 12 were from the United States, six were from the Netherlands, two were from Australia, two were from Germany, two were from Czech Republic and one each from Belgium, Lebanon, Singapore, Switzerland, and Qatar. In terms of study design, 12 studies were feasibility or pilot studies, six were study protocols, four studies were randomized controlled trials, four were development studies, three were quasi-experimental studies, and two were micro-randomized trials. Of the 29 studies, 14 reported PA outcomes, with eight employing within-person designs, and six with between-person designs. Studies that did not report PA outcome include study protocols, development studies, and some feasibility studies that did not report preliminary efficacy on behavioral outcomes. The average intervention length was 12.98 weeks (± 14.7 weeks), with intervention lengths ranging from 1 week to 12 months. Further study characteristics are available within Appendix C.
Of the studies that recruited participants (n=24/29, 82%), 13 recruited healthy but inactive adult participants, four studies recruited participants with diabetes, two studies recruited families, two studies recruited participants recovering from spinal cord injuries, two studies recruited older adults, one study recruited participants with hypertension, one study recruited participants with cardiovascular disease, and one study recruited participants with recovering from metastatic gastrointestinal cancer surgery. The average sample size was 55.83 participants (± 76.37 participants), with sample sizes ranging from 7 to 274 participants.
3.3. The Implementation of Behavior Change Theories and Techniques in PA JITAIs
Of the 29 papers included in the review, 16 explicitly stated a behavior change theory in which their JITAI was grounded. The most commonly stated behavior change theories were self-determination theory [11,12] (n=4, 14%) and social cognitive theory [23] (n=4, 14%). The next most common were Fogg’s behavior model [24] (n=3, 10%) and the capability, opportunity, motivation – behavior (COM-B) model [25] (n=3). Cialdini's 7 Principles of Influence [26] (n=1, 3%), the health action process approach [27] (n=1, 3%), learning theory [28] (n=1, 3%), Locke and Latham’s goal setting theory (n=1, 3%), Marlatt’s relapse prevention model [29] (n=1, 3%), the transtheoretical model [30] (n=1, 3%), Rothman’s theory [13,31] (n=1, 3%) and self-regulation theory [13] (n=1, 3%) were each stated once.
A total of 36 unique BCTs were used across the reviewed literature. Of the 36 total BCTs used, most (34/36, 94%) of the BCTs were stated by the authors of the papers. 13 of the 36 (36%) BCTs were implied, mapped on to the BCT taxonomy by the authors of this review (PC, AW). As shown in Figure 2, the most commonly used BCT that was used in all studies (n=29, 100%) was prompts/cues, due to the nature of PA JITAIs requiring prompts to perform activity. Other prominent BCTs include goal setting (behavior) (15/29, 52%), feedback on behavior (14/29, 48%), self-monitoring of behavior (14/29, 48%), and instruction on how to perform the behavior (10/29, 34%).
To gain a deeper understanding of how BCTs are implemented in PA JITAIs, we analyzed the various ways BCTs are combined within these interventions. The BCT prompts/cues was not included in the pair frequency counts as prompts serve as the trigger for delivering a JITAI, rather than a component paired with other techniques. The most paired BCTs were goal setting (behavior) with feedback on behavior (13 instances). For example, Carey and colleagues (2024) protocol for a JITAI among patients with spinal cord injury combine the use of behavioral goal setting and feedback on behavior through daily goal setting through a mobile app, combined with just-in-time tailored PA feedback messages framed within the COM-B model. Another instance of this pairing was in a PA and diet JITAI for blood pressure reduction [32]. 486 participants who self-reported having hypertension had the opportunity to set behavioral goals relating to choosing low salt foods and step goals. In response to these goals, participants received personalized, adaptive behavioral feedback relating to these goals [32]. For example, “The snow is not going to shovel itself! That is a lot of exercise right there, [Name]!” [32]. The second most prevalent BCT pairing was goal setting (behavior) with self-monitoring of behavior (11 instances). An example of this pairing was done through the app which included an artificial intelligence health coach that interacted with the user through a chat-like feature [33]. Participants were encouraged to set behavioral goals, such as exercise minutes, and through the chat feature, the app would share figures of daily exercise to promote self-monitoring. Another example of this pairing was in the VALENTINE study where participants used an app that allowed for goal setting and activity tracking [34]. Additionally, participants were encouraged to wear an Apple Watch or Fitbit, which enabled self-monitoring of PA [34].
Another BCT combination prevalent in the literature was feedback on behavior with self-monitoring of behavior (9 instances). Daryabeygi-Khotbehsara and colleagues (2023) reported delivering these BCTs through in-app notifications of their iMove app designed for adults with Type 2 Diabetes. Examples of notifications relating to these BCTs include “Congratulations! You achieved your daily physical activity goal [>= VALUE minutes] today. Keep up the good work!” to promote feedback on behavior [35]. An example of a self-monitoring of behavior notification developed for this app was “Check how much time you spent in physical activities yesterday.” [35]. Another example of the use of this BCT pairing was done by Hietbrink and colleagues (2023) who incorporated these BCTs to promote self-regulatory processes from the concept of negative feedback control. In their E-supporter 1.0 app, feedback on behavior notifications were tailored based on meeting or failing to meet a weekly step goal [36]. Self-monitoring was included in the app through self-reported activities and a digital food diary, along with a Fitbit [36].
Goal setting (behavior) with instruction to perform the behavior and self-monitoring of behavior with instruction to perform the behavior were each reported in combination in eight studies. In the ENERGISED app, participants were encouraged to set behavioral goals through phone counselling and received instructions on how to perform the behavior through educational leaflets [37]. The SNapp app is another example of this pairing where participant received messages encouraging users to set a daily step count goal for the upcoming week (i.e., “What’s your new goal, [NAME]? Set yourself an achievable walking goal for this week.” to promote behavioral goal setting [38]. Instruction to perform the behavior was encouraged through messages informing participants when they were near a green space to participate in PA (i.e., “Do you want to get some extra steps in today? You are close to a [green space type] where you can enjoy a nice walk.” [38]. Examples of the self-monitoring of behavior and instruction to perform the behavior pairing were displayed in the Ally app [39] and the PAUL app [40]. Kramer and colleagues (2019) designed self-monitoring prompts to remind participants of their daily step goal, compare the participants’ current step count to their daily goal, and provide an estimate of walking minutes necessary to reach the goal [39]. In addition to these self-monitoring prompts, participants would receive instruction on how to perform a walking behavior randomly between 10am and 6pm [39]. In the PAUL app, Sporrel and colleagues (2022) visually displayed the percentage of the PA goal that was met in the app to promote self-monitoring. Additionally in the app, participants received location-based exercise prompts with instructional videos in the direct environment of the user (i.e., if the participant was at the park, they would receive a video of how to do a push up in a park and using surroundings to modify the exercise) [40].
3.4. JITAI Adaptive Algorithms
While each intervention had its own unique JITAI personalization algorithms that were used, there were some similarities seen across the reviewed literature. Personalization was also seen within the content of notifications, with one paper tailoring notifications based on PA level, goal, time of day and weather [41]. Another prevalent feature was sedentary behavior interruption, with prompts encouraging movement to break up device-measured sedentary bouts [42,43]. Personalized coaching and content were amongst the most prevalent components seen across JITAIs. Coppens and colleagues (2024) implemented this by using a Recommender System algorithm, which automatically generated personalized suggestions based on users’ preferences. Activity tracking and self-monitoring was another commonly seen feature. Many JITAIs tracked measures such as steps, activity time or metabolic equivalents (METs), a quantification of metabolic activity to measure PA, and presented users with graphs and data to allow for self-monitoring of their behavior and goal-tracking. Finally, while less prevalent than the other features, a feature worth noting is the integration of generative AI chat bots by both Kramer and colleagues (2019) and Vandelanotte and colleagues (2023), which allowed participants to ask PA-related questions.
Despite these advancements, a significant concern is the insufficient reporting of the underlying algorithms that drive these personalization strategies. This lack of transparency limits the ability to assess the effectiveness of different algorithmic approaches and to guide the design of future interventions. Furthermore, many studies rely on static decision rules, such as if-then statements, without incorporating adaptive mechanisms that respond to changes in user behavior or context [44]. The absence of detailed reporting and adaptive algorithms reinforces the need for standardized guidelines to enhance the transparency and adaptability of JITAI designs.
3.5. Changes in PA-Related Outcomes for JITAIs
Only 14 of the 29 reviewed studies reported PA outcomes, due to many studies being protocol or feasibility studies, mainly reporting on outcomes other than behavior (i.e., recruitment, engagement, acceptability). Regarding specific PA outcomes, of six studies measuring steps, two demonstrated significant within-group improvements, but none showed between-group differences, relative to control. For light PA or MVPA time (n=4/14, 29%), only one study reported significant within-group increases, with no between-group effects. Among two studies measuring METs, one showed significant within-group improvement; none reported between-group differences. Two studies assessing minutes spent walking showed no significant changes within or between groups. Most studies (13/14, 93%) utilized device-based PA measurement, with only one relying on self-report. Table 1 displays PA outcome data.
Significant improvements in PA outcomes were observed in five of these 14 studies. We did not observe a clear pattern linking specific theories to improved PA outcomes; however, certain BCTs, particularly prompts/cues, self-monitoring, and goal setting, were common in interventions that elicited significant PA results. Of these five studies, only two studies reported the behaviour change theory used. These theories included learning theory, social cognitive theory, Fogg’s behavioral model [52], and self-determination theory [47]. In contrast, greater consistency was noted in the BCTs employed: prompts/cues [34,42,47,52,53], self-monitoring of behavior [34,52], behavioral goal setting [34,47], instruction on how to perform the behavior [47], and providing information about health consequences [47] were prevalent BCTs among effective studies.
Among the studies that did not report statistically significant improvements in PA outcomes (n=9, 64%), there was considerable variability in the use of theoretical frameworks, with no single theory used consistently across studies. Reported theories included Fogg’s behavioral model [40,46], goal setting theory [46], transtheoretical model [46], social cognitive theory [48], self-determination theory [54], and social influence strategies based on Cialdini's principles [43], while several studies did not report any guiding theory [45,49,50,51] Despite the lack of common theoretical grounding, a range of BCTs were applied. Prompts/cues (9/9, 100%) [40,43,45,46,48,49,50,51,54], goal setting (behavior) (6/9, 67%) [40,43,45,46,48,54], and self-monitoring of behavior (5/9, 56%) [40,48,49,50,54] were the most frequently used BCTs, followed by feedback on behavior (4/9, 44%) [40,45,48,54] and instruction on how to perform the behavior (3/9, 33%) [40,48,54]. Examples of additional techniques included material rewards [40,49], social support [43], and habit formation [43].
4. Discussion
This scoping review aimed to describe the implementation of behavior change theories, techniques, and personalization algorithms in JITAIs targeting PA and to evaluate the relationship between the use of theories and BCTs in improving PA outcomes. Our findings reveal considerable variability in how theories and techniques are reported and operationalized in mHealth-based JITAIs, and limited evidence to support the association of behavior change theories and techniques with significant PA improvements.
In addressing the first objective, our results suggested inconsistencies in the implementation and reporting of behavior change theories and techniques. Only 55% of studies referenced a theoretical framework, most commonly self-determination theory and social cognitive theory. However, these theories were often only mentioned without clearly informing the intervention design, tailoring strategies, or logic models. Similarly, only two-thirds of studies reported using BCTs, with prompts/cues, goal setting (behavior), and feedback on behavior being the most frequently applied. These BCTs are foundational in behavior change interventions but were seldom embedded in a broader, theory-informed strategy. Several well-established BCTs that support habit formation, motivation, and behavioral regulation, such as problem-solving or review of behavioral goals [55], were often not included.
The personalization algorithms central to JITAIs were also underreported. Only a subset of studies described their adaptation strategies in terms of tailoring variables and delivery conditions [16,17,32,34,38,41,45,47,50,51,52,56,57]. While some interventions detailed contextual inputs (e.g., location, time of day, or step count) or cited the use of decision rules ([32,34,36,38,41,46,47,50,51]) most did not comprehensively report the logic or algorithms guiding JITAI delivery. This gap limits the ability to replicate or evaluate the adaptiveness of interventions. The mHealth Evidence Reporting and Assessment (mERA) checklist developed by Agarwal et al. (2016) emphasizes the importance of transparent reporting of digital intervention components, including software platforms and adaptation protocols. Yet many studies in this review did not meet these standards.
The second objective of this review was to evaluate whether the presence of behavior change theories or techniques corresponded to improved PA outcomes. Of the 14 studies reporting PA outcomes, only five demonstrated statistically significant improvements. Among these, goal setting (behavior) and self-monitoring were each used in two of the five studies, and instruction on how to perform the behavior and information about health consequences were each used in one study. However, three of the five studies successful in improving PA outcomes did not report using a behavior change theory, while the others referenced self-determination theory, learning theory, or Fogg’s behavioral model. This reporting is consistent with Hardeman and colleagues (2019) systematic review which also reflected on the underreporting of behavior change theories among PA JITAIs.
There are several reasons that may explain the limited number of statistically significant PA studies. Most interventions had short durations, with 12 of the 14 studies that reported PA outcomes lasting less than 10 weeks. This may be insufficient for behavior change to consolidate into a habit, especially given that 10 weeks is often cited as the minimum threshold for habit formation [58]. Additionally, eight of the 14 studies had small sample sizes (n < 30), limiting statistical power and the generalizability of findings [59]. Many of the included studies were pilot or feasibility trials, which, while essential for early-stage testing, are not typically designed to assess intervention effectiveness [60]
Another concern was the underreporting of user interface design and user engagement strategies. While some studies such as Hietbrink et al. (2023) and Ismail & Al Thani (2022) described appealing and user-friendly apps, the majority did not provide visual documentation or discuss the usability of their platforms. User interface quality is a critical determinant of digital intervention success, and optimized interfaces improve user engagement, a key mechanism through which JITAIs may influence behavior [61,62]. In our review, there were only limited number of studies providing details on app design, and thus it remains unclear how interface design may have impacted study results.
Emerging work highlights the potential for AI to support more dynamic and scalable JITAIs. For example, Kramer et al. (2019) used the MobileCoach platform to develop a chatbot (Ally) that delivered prompts and incentives. Vandelanotte et al. (2023) used natural language processing and Google’s Dialogue Flow to create an interactive chatbot for answering PA-related questions. Willms & Liu (2024) explored using generative AI (ChatGPT) to rapidly generate PA JITAI content [63], while Haag et al. (2024) tested GPT-4 for adaptive decision-making within interventions [64]. These innovations represent promising directions for the field, although further research is needed to determine their long-term effectiveness, acceptability, and ethical implications.
Several implications for research and practice emerge from these findings. First, future JITAIs should be firmly grounded in behavior theory, with clear rationale for the selection and application of BCTs and BCT combinations. Reporting guidelines such as the BCT taxonomy [21] and the mERA checklist [65] should be routinely followed to enhance transparency and reproducibility. Second, adaptive mechanisms should be fully described, including the decision rules and contextual data that guide real-time content delivery. Third, app interface design deserves careful prioritization and optimization. Engaging, user-friendly, and intuitive platforms are critical for maintaining user retention and supporting intervention adherence over time. In this context, recent advances in “no-code” mHealth app development tools provide promising avenues to accelerate the design and testing of sophisticated JITAI. These tools allow researchers to build, evaluate and optimize JITAI aimed to promote PA [66,67]. Finally, researchers should design studies with sufficient duration and sample size to detect meaningful changes in PA, while accounting for the diverse populations and behavioral targets involved.
This review has limitations. The included studies were highly heterogeneous in their designs, target populations, and outcome measures, which limited comparability. Reporting gaps made it difficult to definitively assess the influence of specific theories or techniques on outcomes. Moreover, a standardized measure of PA was lacking across studies, and some interventions measured only walking rather than total PA. The inclusion of many early-phase studies also constrained the generalizability of the findings. Additionally, we did not conduct a formal quality assessment, as this review included study protocols and exploratory research, which are not always suitable for traditional appraisal tools.
5. Conclusions
In conclusion, the use of behavior change theories and techniques in JITAIs for PA remains inconsistent and often underreported. While a small number of studies demonstrated significant improvements in PA, there was no clear pattern linking specific BCTs or theories to effectiveness. Transparent reporting of adaptive features, careful integration of theory, and attention to app usability will be critical for the continued development of effective and scalable JITAIs. Advancing these areas will help ensure that JITAIs fulfill their potential as innovative tools for promoting sustained PA in diverse populations.
Author Contributions
Conceptualization, P.C, A.W., and S.L.; methodology, P.C. and A.W.; validation, P.C, A.W.; formal analysis, P.C, A.W.; writing—original draft preparation, P.C.; writing—review and editing, A.W. and S.L..; visualization, A.W.; supervision, S.L. All authors have read and agreed to the published version of the manuscript.
Funding
P.C. received funding from the Jamie Cassels Undergraduate Research Award; A.W. received funding from the Canadian Behavioral Intervention Trials Network and Michael Smith Health Research Foundation; S.L. received funding from the Michael Smith Health Research Foundation Scholar Award.
Institutional Review Board Statement
All included studies involving human participants were in accordance with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards and were reviewed and approved by the relevant Medical Ethics committee/Institutional Review Broads.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AI | Artificial intelligence |
| BCT | Behavior change technique |
| CI | Confidence interval |
| COM-B | Capability, Opportunity, Motivation – Behavior |
| JITAI | Just-in-time adaptive intervention |
| mERA | Mobile health evidence reporting and assessment |
| METs | Metabolic equivalents |
| mHealth | Mobile health |
| MVPA | Moderate-to-vigorous physical activty |
| PA | Physical activity |
Appendix A

Table A1.
PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation.
| SECTION | ITEM | PRISMA-ScR CHECKLIST ITEM | REPORTED ON PAGE # |
| TITLE | |||
| Title | 1 | Identify the report as a scoping review. | 1 |
| ABSTRACT | |||
| Structured summary | 2 | Provide a structured summary that includes (as applicable): background, objectives, eligibility criteria, sources of evidence, charting methods, results, and conclusions that relate to the review questions and objectives. | 1 |
| INTRODUCTION | |||
| Rationale | 3 | Describe the rationale for the review in the context of what is already known. Explain why the review questions/objectives lend themselves to a scoping review approach. | 1-2 |
| Objectives | 4 | Provide an explicit statement of the questions and objectives being addressed with reference to their key elements (e.g., population or participants, concepts, and context) or other relevant key elements used to conceptualize the review questions and/or objectives. | 2 |
| METHODS | |||
| Protocol and registration | 5 | Indicate whether a review protocol exists; state if and where it can be accessed (e.g., a Web address); and if available, provide registration information, including the registration number. | N/A |
| Eligibility criteria | 6 | Specify characteristics of the sources of evidence used as eligibility criteria (e.g., years considered, language, and publication status), and provide a rationale. | 3 |
| Information sources* | 7 | Describe all information sources in the search (e.g., databases with dates of coverage and contact with authors to identify additional sources), as well as the date the most recent search was executed. | 2-4 |
| Search | 8 | Present the full electronic search strategy for at least 1 database, including any limits used, such that it could be repeated. | Appendix B |
| Selection of sources of evidence† | 9 | State the process for selecting sources of evidence (i.e., screening and eligibility) included in the scoping review. | 2-4 |
| Data charting process‡ | 10 | Describe the methods of charting data from the included sources of evidence (e.g., calibrated forms or forms that have been tested by the team before their use, and whether data charting was done independently or in duplicate) and any processes for obtaining and confirming data from investigators. | N/A |
| Data items | 11 | List and define all variables for which data were sought and any assumptions and simplifications made. | 3 |
| Critical appraisal of individual sources of evidence§ | 12 | If done, provide a rationale for conducting a critical appraisal of included sources of evidence; describe the methods used and how this information was used in any data synthesis (if appropriate). | N/A |
| Synthesis of results | 13 | Describe the methods of handling and summarizing the data that were charted. | 3-4 |
| RESULTS | |||
| Selection of sources of evidence | 14 | Give numbers of sources of evidence screened, assessed for eligibility, and included in the review, with reasons for exclusions at each stage, ideally using a flow diagram. | 4 |
| Characteristics of sources of evidence | 15 | For each source of evidence, present characteristics for which data were charted and provide the citations. | 4-5 |
| Critical appraisal within sources of evidence | 16 | If done, present data on critical appraisal of included sources of evidence (see item 12). | N/A |
| Results of individual sources of evidence | 17 | For each included source of evidence, present the relevant data that were charted that relate to the review questions and objectives. | 5-10 |
| Synthesis of results | 18 | Summarize and/or present the charting results as they relate to the review questions and objectives. | 5-10 |
| DISCUSSION | |||
| Summary of evidence | 19 | Summarize the main results (including an overview of concepts, themes, and types of evidence available), link to the review questions and objectives, and consider the relevance to key groups. | 10-12 |
| Limitations | 20 | Discuss the limitations of the scoping review process. | 12 |
| Conclusions | 21 | Provide a general interpretation of the results with respect to the review questions and objectives, as well as potential implications and/or next steps. | 12 |
| FUNDING | |||
| Funding | 22 | Describe sources of funding for the included sources of evidence, as well as sources of funding for the scoping review. Describe the role of the funders of the scoping review. | 12 |
Appendix B
Table B1.
Search strategy for PsycINFO (EBSCO)
| Search | Terms | Results |
| S1 | DE "Digital Health Resources" OR DE "Digital Interventions" OR DE "Mobile Phones" OR DE "Smartphones" OR DE "Mobile Health Applications" OR DE "Mobile Applications" OR DE "Mobile Health" OR DE "Mobile Devices" OR DE "Mobile Technology" OR DE "Wearable Devices" | 19,129 |
| S2 | TI (mhealth OR ehealth OR "digital health" OR “electronic health”) OR AB (mhealth OR ehealth OR "digital health" OR “electronic health”) OR KW (mhealth OR ehealth OR "digital health" OR “electronic health”) | 9,367 |
| S3 | TI ( ((cyber OR digital OR remote* OR distance* OR phone* OR internet OR “smart phone*” OR smartphone* OR mobile* OR iPhone* OR Android*) N5 (based OR app OR apps OR application* OR health OR intervention* OR delivery)) ) OR AB ( ((cyber OR digital OR remote* OR distance* OR phone* OR internet OR “smart phone*” OR smartphone* OR mobile* OR iPhone* OR Android*) N5 (based OR app OR apps OR application* OR health OR intervention* OR delivery)) ) OR KW ( ((cyber OR digital OR remote* OR distance* OR phone* OR internet OR “smart phone*” OR smartphone* OR mobile* OR iPhone* OR Android*) N5 (based OR app OR apps OR application* OR health OR intervention* OR delivery)) ) | 37,861 |
| S4 | TI ( (("activit* track*" OR "fitness track*" OR Fitbit OR Garmin OR TomTom OR Jawbone OR Withings OR “Apple Watch” OR smartwatch OR “smart watch” OR Amazfit OR “Google Pixel” OR “Galaxy Watch”)) ) OR AB ( (("activit* track*" OR "fitness track*" OR Fitbit OR Garmin OR TomTom OR Jawbone OR Withings OR “Apple Watch” OR smartwatch OR “smart watch” OR Amazfit OR “Google Pixel” OR “Galaxy Watch”)) ) OR KW ( (("activit* track*" OR "fitness track*" OR Fitbit OR Garmin OR TomTom OR Jawbone OR Withings OR “Apple Watch” OR smartwatch OR “smart watch” OR Amazfit OR “Google Pixel” OR “Galaxy Watch”)) ) | 1,197 |
| S5 | S1 OR S2 OR S3 OR S4 | 53,154 |
| S6 | TI ( (("Just-in-time" OR “just in time” OR “just-in-time adaptive intervention*” OR JITAI OR “adaptive intervention*”) OR ("ecologic* momentary intervention*" OR EMI) OR (“experience sampling” OR “ambulatory assess*” OR “moment-to-moment measures” OR “daily diary” OR “repeat* assessment*” OR “ambulatory monitor*” OR “electronic diar*”) OR ("real time intervention*" OR "context* aware*" OR "context* trigger*" OR "context* tailor*" OR "dynamic tailor*" OR "real time tailor*" OR “real time intervention” OR “real time therapy” OR “real time tailor*” OR "sensor triggered" OR geofenc* OR "context* sens*" OR "real time context*" OR "persuasive technolog*" OR "sensing technolog*")) ) OR AB ( (("Just-in-time" OR “just in time” OR “just-in-time adaptive intervention*” OR JITAI OR “adaptive intervention*”) OR ("ecologic* momentary intervention*" OR EMI) OR (“experience sampling” OR “ambulatory assess*” OR “moment-to-moment measures” OR “daily diary” OR “repeat* assessment*” OR “ambulatory monitor*” OR “electronic diar*”) OR ("real time intervention*" OR "context* aware*" OR "context* trigger*" OR "context* tailor*" OR "dynamic tailor*" OR "real time tailor*" OR “real time intervention” OR “real time therapy” OR “real time tailor*” OR "sensor triggered" OR geofenc* OR "context* sens*" OR "real time context*" OR "persuasive technolog*" OR "sensing technolog*")) ) OR KW ( (("Just-in-time" OR “just in time” OR “just-in-time adaptive intervention*” OR JITAI OR “adaptive intervention*”) OR ("ecologic* momentary intervention*" OR EMI) OR (“experience sampling” OR “ambulatory assess*” OR “moment-to-moment measures” OR “daily diary” OR “repeat* assessment*” OR “ambulatory monitor*” OR “electronic diar*”) OR ("real time intervention*" OR "context* aware*" OR "context* trigger*" OR "context* tailor*" OR "real time tailor*" OR “real time intervention” OR “real time therapy” OR “real time tailor*” OR “dynamic tailor*” OR "sensor triggered" OR geofenc* OR "context* sens*" OR "real time context*" OR "persuasive technolog*" OR "sensing technolog*")) ) | 13,332 |
| S7 | TI ( ("daily life" or "real-time") N5 (intervention* OR aware* OR triggered OR tailor* OR sens* OR *measure* OR assessment* OR test* OR monitor*) ) OR AB (( ("daily life" or "real-time") N5 (intervention* OR aware* OR triggered OR tailor* OR sens* OR *measure* OR assessment* OR test* OR monitor*) ) OR KW ( ("daily life" or "real-time") N5 (intervention* OR aware* OR triggered OR tailor* OR sens* OR *measure* OR assessment* OR test* OR monitor*) ) | 4,540 |
| S8 | S6 OR S7 | 17,375 |
| S9 | DE "Physical Fitness" OR DE "Aerobic Exercise" OR DE "Running" OR DE "Walking" OR DE "Physical Activity" OR DE "Weightlifting" OR DE "Exercise" OR DE "Locomotion" OR DE “Active Living” | 78,438 |
| S10 | TI (“ physical activit*” OR "physical training" OR walk* OR exercis* OR fitness OR "physical fitness*" OR aerobics OR "aerobic* training" OR "aerobic* activit*" OR running OR jogging OR athletics OR cycling OR bike* OR biking OR bicycl* OR swim* OR hiking OR rollerblading OR roller-blading OR rollerskat* OR roller-skat* OR skating OR "physical exertion*" OR "active transport*" OR "circuit training" OR "strength training" OR calisthenics OR sport* OR "resistance training" OR "weight training" OR "endurance training" OR sport* OR pilates OR yoga) OR AB (“ physical activit*” OR "physical training" OR walk* OR exercis* OR fitness OR "physical fitness*" OR aerobics OR "aerobic* training" OR "aerobic* activit*" OR running OR jogging OR athletics OR cycling OR bike* OR biking OR bicycl* OR swim* OR hiking OR rollerblading OR roller-blading OR rollerskat* OR roller-skat* OR skating OR "physical exertion*" OR "active transport*" OR "circuit training" OR "strength training" OR calisthenics OR sport* OR "resistance training" OR "weight training" OR "endurance training" OR sport* OR pilates OR yoga) OR KW (“ physical activit*” OR "physical training" OR walk* OR exercis* OR fitness OR "physical fitness*" OR aerobics OR "aerobic* training" OR "aerobic* activit*" OR running OR jogging OR athletics OR cycling OR bike* OR biking OR bicycl* OR swim* OR hiking OR rollerblading OR roller-blading OR rollerskat* OR roller-skat* OR skating OR "physical exertion*" OR "active transport*" OR "circuit training" OR "strength training" OR calisthenics OR sport* OR "resistance training" OR "weight training" OR "endurance training" OR sport* OR pilates OR yoga) | 239,890 |
| S11 | S9 OR S10 | 249,104 |
| S12 | S5 AND S8 AND S11 | 222 |
Appendix C
Table C1.
Study Extraction Table
| Author and Year | Location | Design | Sample Size | Participant Characteristics | Behavior Change Theory | BCTs | JITAI Description |
| Bardus et al., 2018 [33] | Lebanon | Protocol | Recruitment has not commenced | Healthy adult employees of an Academic Institution | Not Stated | Self-monitoring of behavior*, Goal setting (behavior)*, Feedback on behavior*, Social reward*, Social support* | Mobile coach that provides interactive counselling and feedback based on several outcomes |
| Boerema et al., 2019 [45] | The Netherlands | Quasi-experimental | n=14 | 50+ year old office workers who spend 50% of their time or more at a computer | Not Stated | Prompts/cues, Goal setting (behavior), Feedback on behavior | Focuses on reducing sedentary behavior with periodic prompts |
| Carey et al., 2024 [68] | United States | Protocol | n=196 | 18-to-75-year-olds with a traumatic SCI injury at C5 and below who are 6 months+ post injury and use a wheelchair as their primary means of transportation | COM-B Model | Goal setting (behavior)*, Feedback on behavior*, Prompts/cues*, | Microrandomized feedback prompts and activity recommendations |
| Coppens et al., 2024 [13,56] | Belgium | Randomized Controlled Trial | n=25 | Healthy, inactive adults | Self-Determination Theory | Prompts/cues*, Instruction on how to perform the behavior | Uses machine learning for personalized activity suggestions |
| Daryabeygi-Khotbehsara et al., 2023 [56] | Australia | Protocol | Recruitment has not commenced | Adults between 35 and 65 years old with Type II Diabetes | Not Stated | Behavior substitution*, Social support*, Problem-solving*, Instruction on how to perform the behavior*, Information about health consequences*, Prompts/cues*, Goal setting (behavior), Self-monitoring of behavior, Feedback on behavior* | Notifications to encourage either sedentary interruption or movement. |
| Ding et al., 2016 [46] | United States | Feasibility Trial | Total n=16, Control n=7, Intervention n=9 |
College students | Fogg Behavior Model, Locke and Latham’s Goal Setting Theory, Trans-theoretical Model | Goal setting (behavior)*, Prompts/cues* | Reminders were sent when participants overused their smartphone, were sedentary for extended periods, were walking (to encourage more walking), or had just finished a meal |
| Fiedler et al., 2023 [47] | Germany | Randomized Controlled Trial | n=80 | Families including at least one parent and at least one child who was 10 years of age or older and who were living together in a common household | Self-Determination Theory | Goal setting (behavior)*, Prompts/cues*, Instruction on how to perform the behavior | Notifications to disrupt bouts of sedentary behavior (50/60 minutes of the last hour). |
| Golbus et al., 2024a [32] | United States | Development Study | n=108 | Adults 18 to 75 years old enrolled in cardiac rehabilitation | Not Stated | Goal setting (behavior), Self-monitoring of behavior, Prompts/cues | Physical activity notifications are designed to disrupt sedentary behavior (eg, to stand up or stretch) and to encourage lowlevel physical activity (eg, bouts of 250 to 500 steps). |
| Golbus et al., 2024b [34] | United States | Microrandomized Trial | Recruitment has not commenced | Adults with self-reported hypertension and no contradictions to PA or a low-sodium diet | Not Stated | Goal setting (behavior)*, Prompts/cues*, Visualizations*, Feedback on behavior* | Static component (e.g., a mobile application that allowed for goal setting and activity tracking) and a dynamic component that consisted of micro-randomized text messages. |
| Hietbrink et al., 2023 [36] | Netherlands | Development Study |
n=9 | Adults with Type II Diabetes | HAPA model, Rothman’s Theory, Marlatt’s Relapse Prevention Theory | Goal-setting (behavior)*, Problem solving*, Action planning*, Review behavior goal*, Feedback on behavior*, Self-monitoring of behavior*, Self-monitoring of outcomes of behavior*, social support*, Social support (practical)*, Instruction on how to perform the behavior*, Information about health consequences*, Information about emotional consequences*, Information about others’ approval*, Prompts/cues*, Habit formation*, Credible source*, Pros and cons*, Comparative imagining of future outcomes*, Reduce negative emotions*, Framing and reframing*, Verbal persuasion about capability*, Focus on past success* | 425 motivational messages, consisting of content for each of the tailoring variables. Decision points took place at 2 semirandom times per day. |
| Hiremath et al., 2019 [48] | United States | Pilot Study | n=16 | Adults 18 to 65 years old with an SCI who are 6 months+ post injury and use a wheelchair as their primary means of transportation | Social Cognitive Theory | Self-monitoring of behavior, Feedback on behavior, Goal setting (behavior), Instruction on how to perform the behavior | Provided proactive, near-real-time feedback via smartphone (audio/vibration, based on user preference) and smartwatch (vibration) when participants engaged in moderate or higher intensity physical activity |
| Hojjatnia et al., 2021 [69] | United States | Quasi-Experimental | n=45 | Insufficiently active emerging and young adults (18-29 years old) | Not stated | Prompts/cues | Messages were sourced from three libraries (move more, sit less, inspirational quotes). Smartphone location data were used to retrieve local weather at message delivery. System identification and simulations evaluated responses to each message type under varying conditions, with extracted features summarizing dynamic response patterns. |
| Ismail et al., 2022 [49] | Qatar | Quasi-Experimental | Total n=58, Control n=29, Intervention n=29 |
Sedentary adult employees aged 23 to 39 years old | Not Stated | Prompts/cues, Material reward (behavior), Self-monitoring (behavior) | Personalized prompts that include user information, user goals, daily routine, and the surrounding environment |
| Klasnja et al., 2019 [50] | United States | Microrandomized Trial | n=44 | 18- to 60-year-old adults with a. regular schedule outside the home (employed or a student) | Not Stated | Prompts/cues, Self-monitoring of behavior | Contextually tailored activity suggestions to walk (intended to encourage bouts of 500-1000 steps) and suggestions to disrupt sedentary behavior (to stand up, stretch, and/or move around). |
| Kramer et al., 2019 [39] | Switzerland | Protocol | n=274 | Healthy adults not working night shifts | Not Stated | Problem solving*, Action planning*, Discrepancy between current behavior and goal*, Feedback on behavior*, Instruction on how to perform the behavior*, Material reward (behavior)*, Nonspecific reward*, Self-monitoring of behavior*, Prompts/cues* | Sent out intervention and step goal–related notifications at random points in time but within prespecified time windows that guaranteed delivery at appropriate times |
| Low et al., 2023 [51] | United States | Pilot Study | Total n=26, Control n=13, Intervention n=13 |
Patients scheduled for surgery for metastatic gastrointestinal cancer | Not Stated | Prompts/cues | Real-time mobile intervention that detects prolonged sedentary behavior during the perioperative period and delivers walking prompts tailored to daily self-reported symptoms |
| Mair et al., 2023 [41] | Singapore | Feasibility Study | n=31 | Older adults who use a smartphone | COM-B Model | Goal setting (behavior)*, Action Planning*, Prompts/cues*, Self-monitoring of behavior*, Feedback on behavior* | Personalized PA messaging was delivered by the JitaBug app to encourage participants to meet their daily PA goal. Messages were tailored to participants’ context. |
| Novak et al., 2024 [70] | Czech Republic | Development | n=14 | Adults with prediabetes | Self-regulation theory | Prompts/cues*, Habit formation*, Behavior substitution*, Review behavior goal*, Discrepancy between current behavior and goal*, Feedback on behavior*, Social reward*, Action planning*, Information about health consequences* | "Walk faster" notifications while walking and "stand up" notifications after prolonged sitting |
| Park et al., 2023 [57] | United States | Protocol | n=48 | Inactive adults aged 25 years or older | Social Cognitive Theory | Prompts/cues*, Goal setting (beahvior)*, Feedback on behavior* | |
| Pellegrini et al., 2021 [42] | United States | Feasibility Study | n=8 | Adults aged 21 to 70 years old with Type II Diabetes | Not Stated | Prompts/cues* | Using an external accelerometer (Shimmer), when a person is sedentary for >= 20 mins, they received a prompt to engage in light behavior for 2 mins |
| Rabbi et al., 2015 [52] | United States | Randomized Controlled Trial | Total n=17, Control n=8, Intervention n=9 |
Low to moderately active adults | Learning theory, social cognitive theory, Fogg's behavioral model | Self-monitoring of behavior, Prompts/cues | Used auto/manual logging of activity, location, and food; analyzed logs to detect behavior patterns; applied multi-armed bandit algorithm to deliver personalized suggestions (continue, avoid, or modify behaviors) |
| Sporrel et al., 2022 [40] | The Netherlands | Feasibility Study | Total n=20, Basic Intervention n=9, Smart Intervention n=11 |
Adults aged 18 to 55 years old who would like to become more active | Fogg's Behavioral Model | Goal setting (behavior)*, Review behavioral goals*, Self-monitoring of behavior*, Instruction on how to perform the behavior*, Demonstration of the behavior*, Behavioral practice/rehearsal*, Graded tasks*, Situation-specific reward*, Prompts/cues | Compared two app versions: Basic PAUL (random-timed JIT prompts) vs. Smart PAUL (JIT adaptive prompts for walking/running). |
| Thomas & Bond, 2015 [53] | United States | Quasi-experimental | n=30 | Overweight or obese men and women aged 21 to 70 years old | None reported | Prompts/cues | Three conditions: (1) 3-min break after 30 min sedentary; (2) 6-min break after 60 min; (3) 12-min break after 120 min. |
| van Dantzig et al., 2013 [43] | The Netherlands | Pilot Study | Total n=86, Control n=46, Intervention n=40 |
Healthy adult office workers | Social influence strategies defined by Cialdini. | Prompts/cues*, Goal setting (behavior), Feedback on the behavior, Social support, Habit formation | Not stated |
| Vandelanotte et al., 2023 [14] | Australia | Development Study | Recruitment has not commenced | Adults interested in becoming more physically active | Self-Determination Theory | Social support (unspecified), Information about health consequences, Action planning, Habit formation, Restructuring the physical environment, Incentive (outcome), Framing/ reframing, Prompts/cues | (1) NLP-based conversations to increase activity knowledge; (2) reinforcement learning-driven nudge engine using real-time data (activity, GPS, GIS, weather, user input); (3) generative AI Q&A for physical activity support. |
| Vetrovsky et al., 2023 [37] | Czech Republic | Protocol | Recruitment has not commenced | Adults aged 18 or older with a diagnosis of Prediabetes or Type II Diabetes according to Czech guidelines | Not Stated | Credible source*, Instruction on how to perform the behavior*, Action planning*, Information about health consequences*, Graded tasks*, Goal setting (behavior)*, Self-monitoring of behavior*, Prompts/cues*, Habit formation*, Behavior substitution*, Review behavioral goals*, Discrepancy between current behavior and goal*, Feedback on behavior*, Social reward*, Information about health consequences*, Problem solving*, Social support (unspecified)*, Graded tasks* | Just-in-time prompts to increase walking pace were triggered when the patient is walking for 5 consecutive minutes with an average steps per minute ranging between 60-100. Just-in-time prompts to interrupt sitting were sent when the patient sits for more than 30 min. |
| Vos et al., 2023 [38] | The Netherlands | Pilot Study | n=11 | Adults aged 45 years or older | Social Cognitive Theory | Action planning*, Social reward*, Feedback on behavior*, Social comparison*, Information about health consequences*, Instruction on how to perform the behavior*, Goal setting (behavior)*, Self-monitoring of behavior*, Review of outcome goals*, Prompts/cues | Not stated |
| Wang et al., 2021 [71] | The Netherlands | Feasibility Study | n=7 | Adults struggling to maintaining a healthy activity level who would like to be more physically active |
Behavior change wheel | Prompts/cues* | The reinforcement learning model would track user data and take input from physical activity logs to determine if it was the right time to send a prompt |
| Wunsch et al., 2024 [54] | Germany | Randomized Controlled Trial | Total n=156, Control n=68, Intervention n=88 |
Households comprising at least 1 adult caregiver and 1 child aged >10 years residing together |
Not stated | Goal setting (behavior)*, Feedback on behavior*, Self-monitoring of behavior*, Instruction on how to perform the behavior, Social comparison*, Prompts/cues | Not stated |
1 BCTs = Behavior Change Techniques; PA = Physical activity; 2 BCTs denoted with a * were explicitly stated by the author
References
- World Health Organization, “Noncommunicable diseases,” World Health Organization. Accessed: May 28, 2025. [Online]. Available: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases.
- E. Anderson and J. L. Durstine, “Physical activity, exercise, and chronic diseases: A brief review,” Sports Medicine and Health Science, vol. 1, no. 1, pp. 3–10, Dec. 2019. [CrossRef]
- World Health Organization, “Nearly 1.8 billion adults at risk of disease from not doing enough physical activity,” World Health Organization. Accessed: May 28, 2025. [Online]. Available: https://www.who.int/news/item/26-06-2024-nearly-1.8-billion-adults-at-risk-of-disease-from-not-doing-enough-physical-activity.
- A. O’Regan et al., “How to improve recruitment, sustainability and scalability in physical activity programmes for adults aged 50 years and older: A qualitative study of key stakeholder perspectives,” PLoS One, vol. 15, no. 10, p. e0240974, Oct. 2020. [CrossRef]
- A. G. Gavarkovs, S. M. Burke, and R. J. Petrella, “The Physical Activity–Related Barriers and Facilitators Perceived by Men Living in Rural Communities,” Am J Mens Health, vol. 11, no. 4, pp. 1130–1132, Jul. 2017. [CrossRef]
- S. Gill, “How Many People Own Smartphones in the World? (2024-2029),” Priori Data.
- M. Zhang, W. Wang, M. Li, H. Sheng, and Y. Zhai, “Efficacy of Mobile Health Applications to Improve Physical Activity and Sedentary Behavior: A Systematic Review and Meta-Analysis for Physically Inactive Individuals,” Int J Environ Res Public Health, vol. 19, no. 8, p. 4905, Apr. 2022. [CrossRef]
- D. Spruijt-Metz et al., “Innovations in the Use of Interactive Technology to Support Weight Management,” Curr Obes Rep, vol. 4, no. 4, pp. 510–519, Dec. 2015. [CrossRef]
- L. Wang and L. C. Miller, “Just-in-the-Moment Adaptive Interventions (JITAI): A Meta-Analytical Review,” Health Commun, vol. 35, no. 12, pp. 1531–1544, Oct. 2020. [CrossRef]
- R. Davis, R. Campbell, Z. Hildon, L. Hobbs, and S. Michie, “Theories of behaviour and behaviour change across the social and behavioural sciences: a scoping review,” Health Psychol Rev, vol. 9, no. 3, pp. 323–344, Aug. 2015. [CrossRef]
- E. L. Deci and R. M. Ryan, “Intrinsic motivation and self-determination in human behavior. New York: Springer Science & Business Media,” 1985.
- R. M. Ryan and E. L. Deci, “Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being.,” American Psychologist, vol. 55, no. 1, pp. 68–78, 2000. [CrossRef]
- A. Bandura, “Social cognitive theory of self-regulation,” Organ Behav Hum Decis Process, vol. 50, no. 2, pp. 248–287, Dec. 1991. [CrossRef]
- S. Michie, C. Abraham, M. P. Eccles, J. J. Francis, W. Hardeman, and M. Johnston, “Strengthening evaluation and implementation by specifying components of behaviour change interventions: a study protocol,” Implementation Science, vol. 6, no. 1, p. 10, Dec. 2011. [CrossRef]
- W. Hardeman, J. Houghton, K. Lane, A. Jones, and F. Naughton, “A systematic review of just-in-time adaptive interventions (JITAIs) to promote physical activity,” International Journal of Behavioral Nutrition and Physical Activity, vol. 16, no. 1, p. 31, Dec. 2019. [CrossRef]
- I. Coppens, T. De Pessemier, and L. Martens, “Exploring the added effect of three recommender system techniques in mobile health interventions for physical activity: a longitudinal randomized controlled trial,” User Model User-adapt Interact, vol. 34, no. 5, pp. 1835–1890, Nov. 2024. [CrossRef]
- C. Vandelanotte et al., “Increasing physical activity using an just-in-time adaptive digital assistant supported by machine learning: A novel approach for hyper-personalised mHealth interventions,” J Biomed Inform, vol. 144, p. 104435, Aug. 2023. [CrossRef]
- J. McGowan et al., “Reporting scoping reviews—PRISMA ScR extension,” J Clin Epidemiol, vol. 123, pp. 177–179, Jul. 2020. [CrossRef]
- J. Babineau, “Product Review: Covidence (Systematic Review Software),” Journal of the Canadian Health Libraries Association / Journal de l’Association des bibliothèques de la santé du Canada, vol. 35, no. 2, p. 68, Aug. 2014. [CrossRef]
- P. Cotie, A. Willms, and S. Liu, “Implementation of Behavior Change Theories and Techniques for Physical Activity Just-in-Time Adaptive Interventions: A Scoping Review,” 2025.
- S. Michie et al., “The Behavior Change Technique Taxonomy (v1) of 93 Hierarchically Clustered Techniques: Building an International Consensus for the Reporting of Behavior Change Interventions,” Annals of Behavioral Medicine, vol. 46, no. 1, pp. 81–95, Aug. 2013. [CrossRef]
- L. C. Bohlen et al., “Do Combinations of Behavior Change Techniques That Occur Frequently in Interventions Reflect Underlying Theory?,” Ann Behav Med, vol. 54, no. 11, pp. 827–842, Nov. 2020. [CrossRef]
- A. Bandura, “Social foundations of thought and action,” Englewood Cliffs, NJ, vol. 1986, no. 23–28, p. 2, 1986.
- B. J. Fogg, “A behavior model for persuasive design,” in Proceedings of the 4th International Conference on Persuasive Technology, in Persuasive ’09. New York, NY, USA: Association for Computing Machinery, Apr. 2009, pp. 1–7. [CrossRef]
- S. Michie, M. M. Van Stralen, and R. West, “The behaviour change wheel: A new method for characterising and designing behaviour change interventions,” Implementation Science, vol. 6, no. 1, p. 42, Dec. 2011. [CrossRef]
- R. Cialdini, Pre-Suasion: A Revolutionary Way to Influence and Persuade. Simon & Schuster, 2016.
- R. Schwarzer, “Health Action Process Approach (HAPA) as a Theoretical Framework to Understand Behavior Change,” Actualidades en Psicología, vol. 30, no. 121, p. 119, Dec. 2016. [CrossRef]
- A. Bandura, Social learning theory. Oxford, England: Prentice-Hall, 1977.
- M. E. Larimer, R. S. Palmer, and G. A. Marlatt, “Relapse prevention. An overview of Marlatt’s cognitive-behavioral model.,” Alcohol Res Health, vol. 23, no. 2, pp. 151–60, 1999.
- J. O. Prochaska, C. A. Redding, and K. E. Evers, “The transtheoretical model and stages of change,” Health behavior and health education: Theory, research, and practice, vol. 4, pp. 97–121, 2008.
- A. J. Rothman, “Toward a theory-based analysis of behavioral maintenance.,” Health Psychology, vol. 19, no. 1, Suppl, pp. 64–69, Jan. 2000. [CrossRef]
- J. R. Golbus et al., “A Physical Activity and Diet Just-in-Time Adaptive Intervention to Reduce Blood Pressure: The myBPmyLife Study Rationale and Design,” J Am Heart Assoc, vol. 13, no. 2, Jan. 2024. [CrossRef]
- M. Bardus, G. Hamadeh, B. Hayek, and R. Al Kherfan, “A Self-Directed Mobile Intervention (WaznApp) to Promote Weight Control Among Employees at a Lebanese University: Protocol for a Feasibility Pilot Randomized Controlled Trial,” JMIR Res Protoc, vol. 7, no. 5, p. e133, May 2018. [CrossRef]
- J. R. Golbus et al., “Text Messages to Promote Physical Activity in Patients With Cardiovascular Disease: A Micro-Randomized Trial of a Just-In-Time Adaptive Intervention,” Circ Cardiovasc Qual Outcomes, vol. 17, no. 7, Jul. 2024. [CrossRef]
- R. Daryabeygi-Khotbehsara, D. W. Dunstan, S. M. S. Islam, Y. Zhang, M. Abdelrazek, and R. Maddison, “Just-In-Time Adaptive Intervention to Sit Less and Move More in People With Type 2 Diabetes: Protocol for a Microrandomized Trial,” JMIR Res Protoc, vol. 12, p. e41502, Sep. 2023. [CrossRef]
- E. A. G. Hietbrink et al., “A Digital Lifestyle Coach (E-Supporter 1.0) to Support People With Type 2 Diabetes: Participatory Development Study,” JMIR Hum Factors, vol. 10, p. e40017, Jan. 2023. [CrossRef]
- T. Vetrovsky et al., “mHealth intervention delivered in general practice to increase physical activity and reduce sedentary behaviour of patients with prediabetes and type 2 diabetes (ENERGISED): rationale and study protocol for a pragmatic randomised controlled trial,” BMC Public Health, vol. 23, no. 1, p. 613, Mar. 2023. [CrossRef]
- A. L. Vos, G.-J. de Bruijn, M. C. A. Klein, J. Lakerveld, S. C. Boerman, and E. G. Smit, “SNapp, a Tailored Smartphone App Intervention to Promote Walking in Adults of Low Socioeconomic Position: Development and Qualitative Pilot Study,” JMIR Form Res, vol. 7, p. e40851, Apr. 2023. [CrossRef]
- J.-N. Kramer et al., “Investigating Intervention Components and Exploring States of Receptivity for a Smartphone App to Promote Physical Activity: Protocol of a Microrandomized Trial,” JMIR Res Protoc, vol. 8, no. 1, p. e11540, Jan. 2019. [CrossRef]
- K. Sporrel et al., “Just-in-Time Prompts for Running, Walking, and Performing Strength Exercises in the Built Environment: 4-Week Randomized Feasibility Study,” JMIR Form Res, vol. 6, no. 8, p. e35268, Aug. 2022. [CrossRef]
- J. L. Mair, L. D. Hayes, A. K. Campbell, D. S. Buchan, C. Easton, and N. Sculthorpe, “A Personalized Smartphone-Delivered Just-in-time Adaptive Intervention (JitaBug) to Increase Physical Activity in Older Adults: Mixed Methods Feasibility Study,” JMIR Form Res, vol. 6, no. 4, p. e34662, Apr. 2022. [CrossRef]
- C. A. Pellegrini, S. A. Hoffman, E. R. Daly, M. Murillo, G. Iakovlev, and B. Spring, “Acceptability of smartphone technology to interrupt sedentary time in adults with diabetes,” Transl Behav Med, vol. 5, no. 3, pp. 307–314, Sep. 2015. [CrossRef]
- S. van Dantzig, G. Geleijnse, and A. T. van Halteren, “Toward a persuasive mobile application to reduce sedentary behavior,” Pers Ubiquitous Comput, vol. 17, no. 6, pp. 1237–1246, Aug. 2013. [CrossRef]
- T. C. Hsu, P. Whelan, J. Gandrup, C. J. Armitage, L. Cordingley, and J. McBeth, “Personalized interventions for behaviour change: A scoping review of just-in-time adaptive interventions,” Br J Health Psychol, vol. 30, no. 1, Feb. 2025. [CrossRef]
- S. Boerema, L. van Velsen, and H. Hermens, “An intervention study to assess potential effect and user experience of an mHealth intervention to reduce sedentary behaviour among older office workers,” BMJ Health Care Inform, vol. 26, no. 1, p. e100014, Nov. 2019. [CrossRef]
- X. Ding, J. Xu, H. Wang, G. Chen, H. Thind, and Y. Zhang, “WalkMore: promoting walking with just-in-time context-aware prompts,” in 2016 IEEE Wireless Health (WH), IEEE, Oct. 2016, pp. 1–8. [CrossRef]
- J. Fiedler, C. Seiferth, T. Eckert, A. Woll, and K. Wunsch, “A just-in-time adaptive intervention to enhance physical activity in the SMARTFAMILY2.0 trial.,” Sport Exerc Perform Psychol, vol. 12, no. 1, pp. 43–57, Feb. 2023. [CrossRef]
- S. V. Hiremath et al., “Mobile health-based physical activity intervention for individuals with spinal cord injury in the community: A pilot study,” PLoS One, vol. 14, no. 10, p. e0223762, Oct. 2019. [CrossRef]
- T. Ismail and D. Al Thani, “Design and Evaluation of a Just-in-Time Adaptive Intervention (JITAI) to Reduce Sedentary Behavior at Work: Experimental Study,” JMIR Form Res, vol. 6, no. 1, p. e34309, Jan. 2022. [CrossRef]
- P. Klasnja et al., “Efficacy of Contextually Tailored Suggestions for Physical Activity: A Micro-randomized Optimization Trial of HeartSteps,” Annals of Behavioral Medicine, vol. 53, no. 6, pp. 573–582, May 2019. [CrossRef]
- C. A. Low et al., “A Real-Time Mobile Intervention to Reduce Sedentary Behavior Before and After Cancer Surgery: Usability and Feasibility Study,” JMIR Perioper Med, vol. 3, no. 1, p. e17292, Mar. 2020. [CrossRef]
- M. Rabbi, A. Pfammatter, M. Zhang, B. Spring, and T. Choudhury, “Automated Personalized Feedback for Physical Activity and Dietary Behavior Change With Mobile Phones: A Randomized Controlled Trial on Adults,” JMIR Mhealth Uhealth, vol. 3, no. 2, p. e42, May 2015. [CrossRef]
- J. G. Thomas and D. S. Bond, “Behavioral response to a just-in-time adaptive intervention (JITAI) to reduce sedentary behavior in obese adults: Implications for JITAI optimization.,” Health Psychology, vol. 34, no. Suppl, pp. 1261–1267, Dec. 2015. [CrossRef]
- K. Wunsch, J. Fiedler, S. Hubenschmid, H. Reiterer, B. Renner, and A. Woll, “An mHealth Intervention Promoting Physical Activity and Healthy Eating in a Family Setting (SMARTFAMILY): Randomized Controlled Trial,” JMIR Mhealth Uhealth, vol. 12, p. e51201, Apr. 2024. [CrossRef]
- R. E. Rhodes, “Multi-Process Action Control in Physical Activity: A Primer,” Front Psychol, vol. 12, Dec. 2021. [CrossRef]
- R. Daryabeygi-Khotbehsara, D. W. Dunstan, S. M. S. Islam, Y. Zhang, M. Abdelrazek, and R. Maddison, “Just-In-Time Adaptive Intervention to Sit Less and Move More in People With Type 2 Diabetes: Protocol for a Microrandomized Trial,” JMIR Res Protoc, vol. 12, p. e41502, Sep. 2023. [CrossRef]
- J. Park et al., “Advancing Understanding of Just-in-Time States for Supporting Physical Activity (Project JustWalk JITAI): Protocol for a System ID Study of Just-in-Time Adaptive Interventions,” JMIR Res Protoc, vol. 12, p. e52161, Sep. 2023. [CrossRef]
- B. Gardner, P. Lally, and J. Wardle, “Making health habitual: the psychology of ‘habit-formation’ and general practice,” British Journal of General Practice, vol. 62, no. 605, pp. 664–666, Dec. 2012. [CrossRef]
- E. J. Mascha and T. R. Vetter, “Significance, Errors, Power, and Sample Size: The Blocking and Tackling of Statistics,” Anesth Analg, vol. 126, no. 2, pp. 691–698, Feb. 2018. [CrossRef]
- H. Hollman, S. Liu, M. Davenport, and R. E. Rhodes, “A critical review and user’s guide for conducting feasibility and pilot studies in the physical activity domain.,” Sport Exerc Perform Psychol, vol. 14, no. 1, pp. 40–56, Feb. 2025. [CrossRef]
- A. Willms, R. E. Rhodes, and S. Liu, “The Development of a Hypertension Prevention and Financial-Incentive mHealth Program Using a ‘No-Code’ Mobile App Builder: Development and Usability Study,” JMIR Form Res, vol. 7, p. e43823, Apr. 2023. [CrossRef]
- A. Willms, R. E. Rhodes, and S. Liu, “Effects of Mobile-Based Financial Incentive Interventions for Adults at Risk of Developing Hypertension: Feasibility Randomized Controlled Trial,” JMIR Form Res, vol. 7, p. e36562, Mar. 2023. [CrossRef]
- A. Willms and S. Liu, “Exploring the Feasibility of Using ChatGPT to Create Just-in-Time Adaptive Physical Activity mHealth Intervention Content: Case Study,” JMIR Med Educ, vol. 10, p. e51426, Feb. 2024. [CrossRef]
- D. Haag et al., “The Last JITAI? The Unreasonable Effectiveness of Large Language Models in Issuing Just-in-Time Adaptive Interventions: Fostering Physical Activity in a Prospective Cardiac Rehabilitation Setting,” Pre-Print, Apr. 2024. [CrossRef]
- S. Agarwal et al., “Guidelines for reporting of health interventions using mobile phones: mobile health (mHealth) evidence reporting and assessment (mERA) checklist,” BMJ, p. i1174, Mar. 2016. [CrossRef]
- S. Liu, H. La, A. Willms, and R. E. Rhodes, “A ‘No-Code’ App Design Platform for Mobile Health Research: Development and Usability Study,” JMIR Form Res, vol. 6, no. 8, p. e38737, 2022. [CrossRef]
- A. Willms, J. Rush, S. Hofer, R. E. Rhodes, and S. Liu, “Advancing physical activity research methods using real-time and adaptive technology: A scoping review of ‘no-code’ mobile health app research tools.,” Sport Exerc Perform Psychol, Sep. 2024. [CrossRef]
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses-Scoping Review Flowchart.
Figure 1.
Preferred Reporting Items for Systematic Reviews and Meta-Analyses-Scoping Review Flowchart.
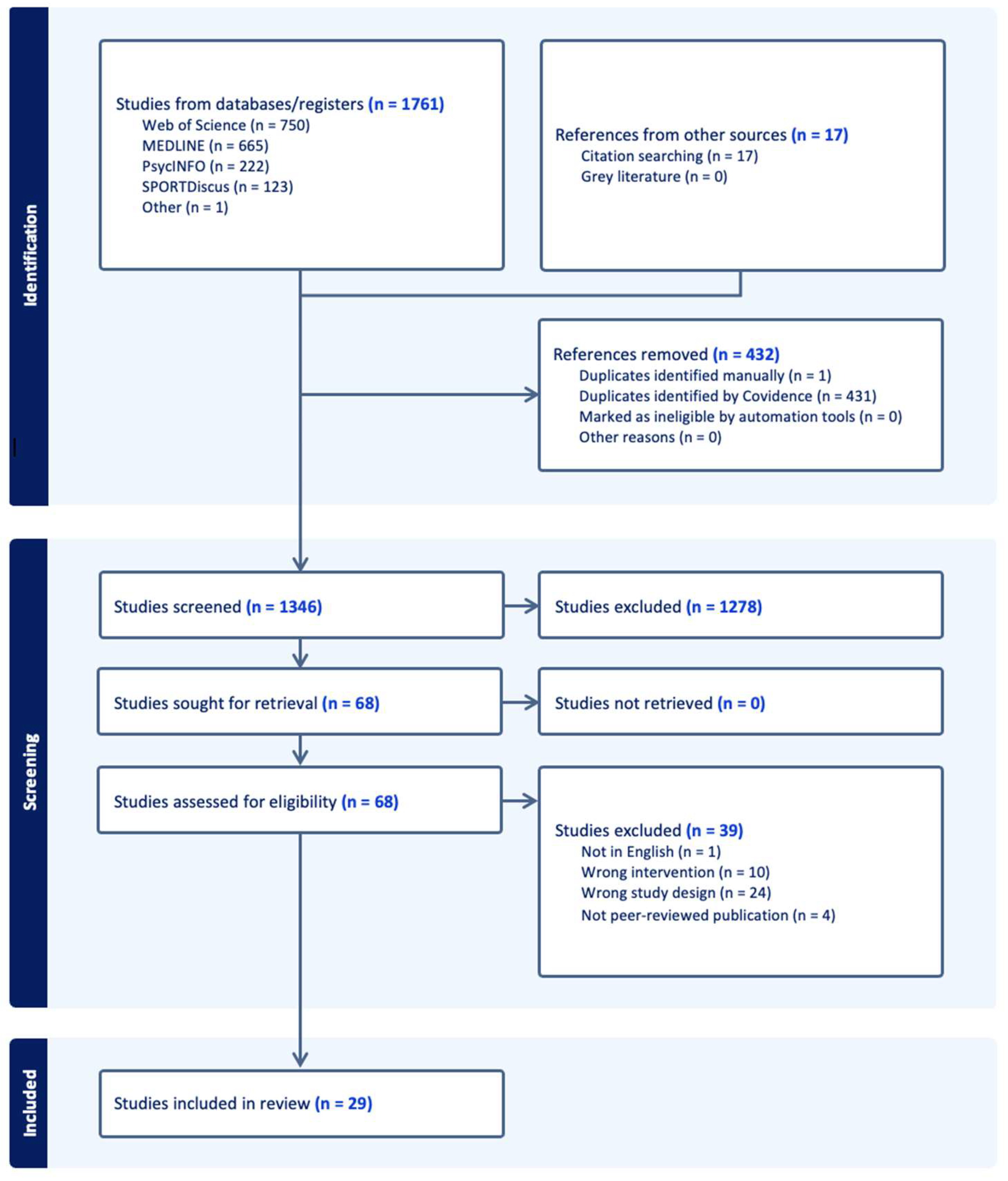
Figure 2.
Behavior Change Techniques (BCTs) and Their Inclusion Amongst Studies.
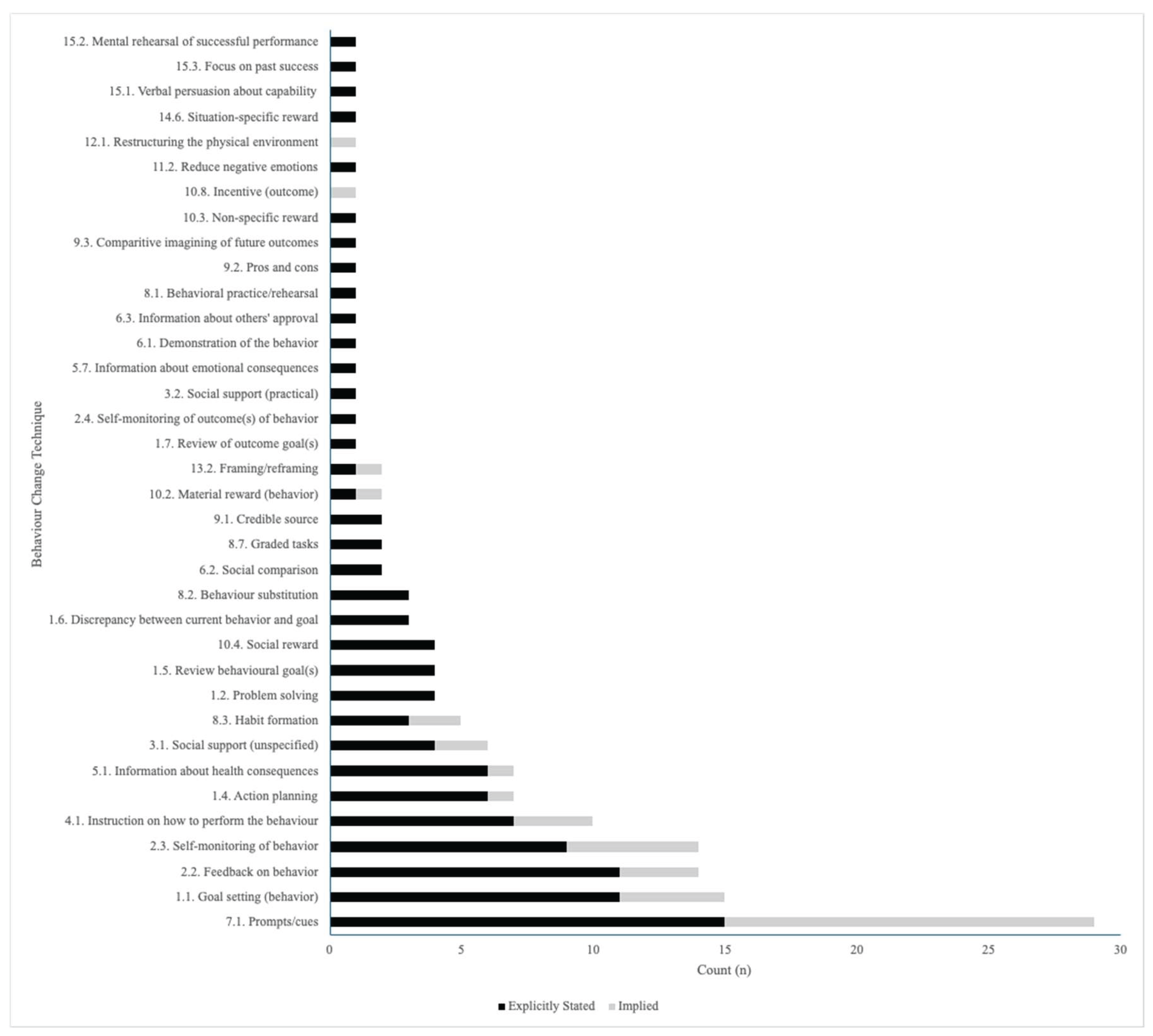
Table 1.
Reported Physical Activity Outcomes and Intervention Details.
| Author, Year | PA Outcome | PA Measurement Tool | Length | Significant Results | Comparator |
| Boerema et al., 2019 [45] | PA Intensity | ProMove 3D Activity Sensor | 1 week | No significant PA results | Baseline |
| Ding et al., 2016 [46] | Weekly Steps | Smartphone and Smartwatch Accelerometers | 3 weeks | No significant PA results | Between-Group |
| Fiedler et al., 2023 [47] | Step Count, METs | Move 3/Move 4, or Movisens GmbH Accelerometer | 3 weeks | Increased step count in “engaged” condition vs “not engaged” (Δ: +256 steps) | Within-Person |
| Golbus, Shi, et al., 2024 [34] | Step Count | iPhone or Android Phone and Apple Watch Series 4 or Fitbit Versa 2 | 6 months | Increased step count in Fitbit group during initiation phase only (Δ: +17%) | Within-Person |
| Hiremath et al., 2019 [48] | Energy Expenditure (kcal) and Light PA time, MVPA time | Nexus 5 or 5X Smartphone, LG-Urbane Smartwatch, PanoBike Wheel Rotation Monitor | 3 months | No significant PA results | Within-Person |
| Ismail et al., 2022 [49] | Step Count, METs | Android Smartphone | 66 days | No significant PA results | Between-Group |
| Klasnja et al., 2019 [50] | Steps | Android Smartphone, Jawbone Smartwatch | 6 weeks | No significant PA results | Within-Person |
| Low et al., 2023 [51] | Step Count | Fitbit Versa Smartwatch, Google Pixel 2 Smartphone | Varied based on surgery and discharge dates. | No significant PA results | Within-Person |
| Pellegrini et al., 2021 [42] | % of Time Doing Light PA or MVPA | Shimmer, Intervention Accelerometer | 1 month | Increased Light PA (Δ: +7.8%) | Within-Person |
| Rabbi et al., 2015 [52] | Minutes per Day Walking | Self-Report | 3 weeks | Increased MVPA (Δ: +10.4 mins/day) | Between-Group |
| Sporrel et al., 2022 [40,53] | Minutes of Behavior | Actigraph Accelerometer | 4 weeks | No significant PA results | Between-Group, then Within-Person |
| Thomas & Bond, 2015 [53] |
Walking Time | SenseWear Mini Armband | 3 weeks | 3-min condition (Δ: +31 min/day), had a greater increase in Light PA compared to 12-min (Δ: +15.3 min/day) | Between-Group |
| van Dantzig et al., 2013 - Study 2 [43] | Proportion of Active Minutes | Accelerometer | 6 weeks | No significant PA results | Between-Group |
| Wunsch et al., 2024 [54] | Steps/Week, MVPA Time/Week | Move 3, Move 4, or Movisens Accelerometer | 3 weeks | No significant PA results | Between-Group |
1 kcal = Kilocalories, MVPA = Moderate-to-Vigorous Physical Activity, METs = Metabolic Equivalents, PA = Physical activity.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



