Submitted:
09 July 2025
Posted:
10 July 2025
You are already at the latest version
Abstract
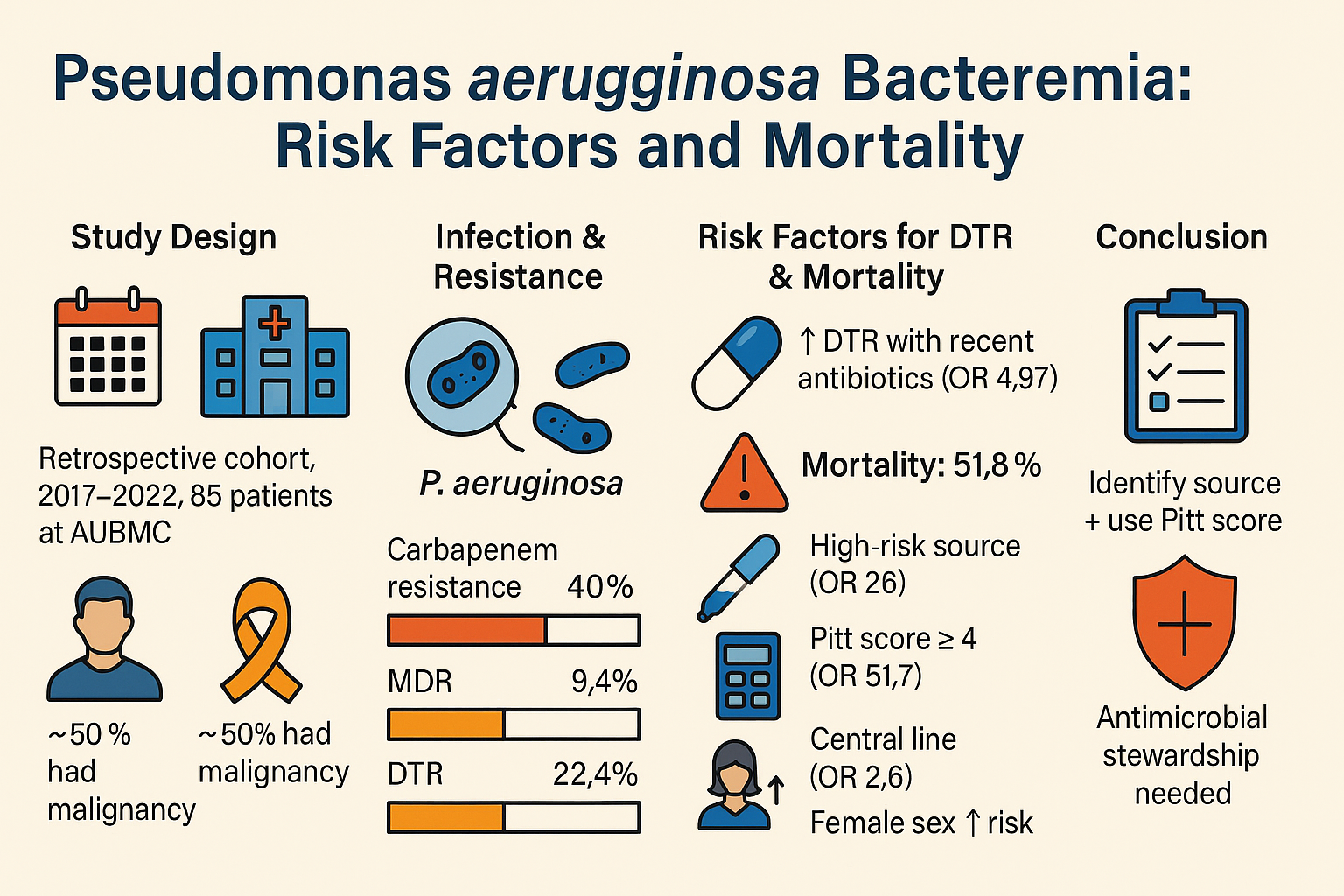
Pseudomonas aeruginosa bacteremia has become increasingly recognized as a major cause of morbidity and mortality and represents a challenge to the treating physician with the rise of multi-drug resistant (MDR) Pseudomonas. The purpose of this study is to evaluate the risk factors associated with Pseudomonas aeruginosa bacteremia and its clinical out-comes. A retrospective cohort study at the American University of Beirut Medical Center (AUBMC) was performed. It included 85 patients > 18 years of age who had confirmed Pseudomonas aeruginosa bacteremia during their hospital stay from 2017 to 2022. With regard to resistance patterns, 8 (9.4%) were considered multidrug-resistant (MDR) and 19 (22.4%) were considered difficult to treat (DTR). Antibiotic use in the month preceding the infection was associated with the risk of DTR Pseudomonas infections (odds ratio 4.97; p-value 0.026). The in-hospital mortality rate was 51.8%. Male sex was associated with decreased mortality (odds ratio 0.13; p-value 0.036). Recent central line placement and Pitt bacteremia score were associated with increased mortality (odds ratios 2.63; p-value 0.028 and 51.71; p-value < 0.001, respectively). Patients with high-risk primary sources of in-fection such as central line, gastrointestinal, and respiratory sources had increased mortality when compared to those with low-risk sources such as skin, abscess, and urinary sources (odds ratio of 25.96; p-value 0.001). In Pseudomonas aeruginosa bacteremia, in addition to prompt empirical treatment, identifying the primary source of infection is imperative as it can estimate the severity of the curent infection. Pitt bacteremia score can be an effective tool to evaluate patient outcome. Increasing antibiotic use has led to in-creasing rates of DTR Pseudomonas infections, which highlights the importance of an-timicrobial stewardship.
Keywords:
pseudomonas aeruginosa
; bacteremia
; difficult to treat infections
; mortality
1. Introduction
Bloodstream infections (BSI) carry significant implications on patient morbidity and mortality Pseudomonas aeruginosa (PA) is a challenging organism due to its virulence and high rate of emerging resistance [1]. It is a common nosocomial pathogen that is known to prolong the duration of hospitalization and exerts a substantial influence on both morbidity and mortality [2,3]. Its associated mortality is higher than other gram-negative organisms or Staphylococcus aureus even after accounting for patients’ characteristics and treatment [4]. The rate of in-hospital mortality from Pseudomonas aeruginosa bacteremia (PAB) ranges between 25.5% to 39% [5]. While PA is known to cause bacteremia in immunocompromised individuals, there have been several reports of community acquired bloodstream infection in immunocompetent individuals [2,3,6,7]. The importance of this pathogen and its increasing rate of resistance has led the World Health Organization (WHO) to classify carbapenem resistant PA as a pathogen of critical priority [8]. Therefore, it is imperative to study the risk factors associated with severe PAB. Immunocompromised patients and patients undergoing invasive procedures are particularly at risk [3]. Antibiotic resistance is another variable of interest that can alter the clinical course of PAB with recent antibiotic use or ICU admission as predictors for multi-drug resistant PA [9].
Due to the increasing ability of Pseudomonas aeruginosa to resist almost all currently available antipseudomonal antibiotics, notably aminoglycosides, quinolones and beta-lactams [10], therapeutic options can be limited. The excessive use of antibiotics is an important factor in the development of multidrug-resistant PA strains [10,11]. Antibiotic resistance is primarily through genetic alterations of the bacterium [12]. Antibiotic resistance can be divided into three classes: intrinsic, acquired and genetic resistance [13]. The intrinsic mechanisms of resistance can vary from enzymatic degradation of the drug, antibiotic target site modification, or an efflux pump [10,12,13,14,15]. In addition, the acquired resistance of PA involves mutational changes or horizontal transfer of genes [10,12,15]. Finally, the acquired resistance is achieved through the formation of a biofilm in the lungs which acts as a diffusion barrier limiting the access of antibiotics to the bacterial cells [10,16]. In the past few years, there has been a notable emphasis on the development of new antibiotic combinations to treat multi-drug resistant (MDR) PA infections [10,14,17]. Carbapenem-resistance is primarily associated with carbapenemase production as well as outer membrane permeability defect with the production of beta-lactamases with the presence of CTX-M variant [18]. MDR PA have been steadily increasing in Lebanon [19,20,21] where there is scarcity of research about PAB with its associated risk factors [20,21,22].
2. Materials and Methods
Definitions: Sources of infection were allocated to either high risk source or low risk source depending on their mortality rates. Central line and pulmonary infections were identified as high-risk while abscess, skin, and urinary infections were identified as low-risk sources of infection. Multi-drug resistance and difficult-to-treat resistance (DTR) were identified using 5 classes of antibiotics: antipseudomonal cephalosporins, antipseudomonal penicillin, fluoroquinolones, carbapenems, aminoglycosides. MDR was identified if PA was resistant to at least 3 classes of antibiotics. When resistant to all 5 classes of antibiotics, DTR PA was identified.
Study design: This is a retrospective cohort study involving hospitalized adult participants from 2017-2022 with positive blood cultures for PA. This study was approved and comes in accordance with the ethical standards of the Institutional Review Board (IRB) at AUBMC, a tertiary healthcare center in Lebanon. Demographic, clinical, and microbiology data were obtained by reviewing electronic medical records. Patients were classified based on route of acquisition into 3 categories: community acquired, hospital acquired, and healthcare associated. If there were multiple sources of infection or the primary source was never identified, then the source would be classified as unknown. The risk of critical illness and death was estimated using Pitt bacteremia score. We also estimated the risk of 10-year mortality using Charlson Comorbidity index.
Statistical analysis: Categorical and continuous variables were compared using the Chi-square test and the T-test, respectively. Multivariable logistic regression was performed to control for confounders and establish independent associations on variables with a cutoff p-value of < 0.2 on bivariable analysis. SPSS was used for data analysis in this study.
3. Results
The demographic and clinical characteristics of the patient population are shown in Table 1. There was a male predominance with 60 (70.6%) males and 25 (29.4%) females with a mean age of 64.5 years. Most patients had pre-existing medical conditions making them more susceptible to infection, aligning with data from other published studies. Approximately fifty percent of them had a cancer diagnosis. Patients admitted to the hospital prior to infection for more than 5 days were a majority consisting of 69 patients (81.2%) with 45 (53%) requiring at least 3-day ICU stay. Moreover, 67 (78.8%) patients had hospital acquired infection, while 6 (7.1%) and 12 (14.1%) had healthcare associated and community acquired PAB, respectively. Antibiotic use within 24 hours before the index infection was noted in 66 patients (77.6%) while 64 (75.3%) patients received an antibiotic course of at least 3 days during the month preceding the infection. The most commonly used antibiotics prior to infection were glycopeptides, aminoglycosides, and carbapenems.
We determined the source of bacteremia by reviewing physician notes in the medical record or contemporaneously cultured PA from a different location (such as sputum or urine). In our population, a primary source was identified in 88.2% of patients. The most common sources of bacteremia were pulmonary (29.4%), central line-associated (22.4%), urinary (16.5%). In 11.8% of cases, the source was deemed unknown (Figure 1).
Antibiotic susceptibility testing was performed in accordance with CLSI guidelines. The highest rates of resistance were to carbapenems in 34 patients (40%) followed by quinolones in 30 patients (35.3%). Out of 85 isolates, 8 were considered MDR and 19 DTR. Further susceptibility analysis was performed to ceftolozane-tazobactam in 9 cases (resistance 2/9) and to ceftazidime-avibactam in 16 cases (resistance 6/16). Antibiotic use within 30 days of PAB was significantly associated with DTR with an odds ratio of 4.97 (p-value 0.026).
The clinical course was complicated in most cases. Out of the 85 patients, 69 (81.2%) had sepsis, 54 (63.5%) required ICU admission, and 49 (57.6%) had septic shock (Table 2). The overall in-hospital mortality rate was 51.8% with an attributable mortality of 44.7%. The variables significantly associated with increased mortality were female sex, high risk source of infection, and Pitt Bacteremia Score ≥ 4 (Table 3). The use of combination therapy and antibiotic resistance of the isolate were not significantly associated with mortality).
4. Discussion
This retrospective analysis sheds light on key characteristics of PAB that can increase our understanding of the characteristics and prognosis of this infection. Historically, APACHE score, age and multidrug resistance were found to be significantly associated with PAB mortality [23]. In more recent years however, multiple variables were shown to be associated with PAB mortality with mixed results regarding risk factor associations.
In comparison with other contemporary analyses of PAB performed on different populations, some similarities and key differences can be examined. Most notably, the Pitt Bacteremia Score with a cutoff of ≥ 4 has been significantly associated with increased mortality in most studies [24,25].
The primary source of infection was proven to be an important prognostic factor as previously speculated in a study by Joo et al in 2011 [26]. Similar to the current study, the study done by Yoon et al in 2016 divided the primary sources of infection into high risk and low risk sources of infection with lower respiratory tract, abdomen, soft tissue, and sources of unknown origin as high-risk sources and pancreaticobiliary tract, intravenous catheters, and the urinary tract as low-risk sources which also showed a significant association with mortality. In line with observations reported in other published studies, we found that patients with central-line or pulmonary infections as the primary source of bacteremia had a higher rate of mortality [28]. Previous research has demonstrated that inadequate empiric therapy was an independent risk factor for mortality among patients whose infections originate from high-risk sites like the respiratory tract, as opposed to low-risk sites like the urinary tract [28]. This highlights the necessity of identifying patients with high-risk primary sites of infections at the outset to optimize empiric antibiotic treatment.
It has been observed that PAB tends to occur more frequently in males [27,29] , and in our study, 70% of the patients were male. We found that male sex was associated with decreased mortality. There has been previous description of increased mortality among women with PAB, although the underlying cause for this remains uncertain [30].
Carbapenems are broad spectrum antibiotics recommended for the management of critically ill patients. In suspected PAB, prompt empiric antibiotic administration is essential. Often, carbapenems are either used as monotherapy or in combination with another antipseudomonal agent. However, globally, the threat of carbapenem-resistant P. aeruginosa is on the rise. In our study, approximately 40% of the patients were infected with carbapenem-resistant P. aeruginosa. The prevalence of carbapenem-resistant PA in neighboring countries in the middle east and north Africa region ranges between 3% in Kuwait to 93% in Jordan [28]. Previous published data from Lebanon places the prevalence of carbapenem-resistant PA at 28% [28]. In our study, the isolate was least likely to be resistant to colistin (3.5%), amikacin (27.1%), and cefepime (23.5%). Yet a carbapenem was the most frequently used antipseudomonal agent empirically (32.9%). Thus, knowledge of epidemiology and resistance patterns within both the medical facility and the entire country is critical to guide empiric therapy.
We did not find antimicrobial resistance nor antipseudomonal monotherapy to be associated with increased mortality in our study. There are conflicting data in the literature regarding this issue. While some studies found that infection with resistant isolates leads to delay in appropriate antibiotic therapy and thus increase in mortality [29,31], other studies suggested that the impact of antimicrobial resistance could be contingent on the severity of pre-existing medical conditions and the initial site of infection [31,32].
Age, corticosteroid use, hospital acquired infection, inappropriate empiric therapy, previous hospital admission, and renal disease were predictors of increased mortality in some studies [26,27,28,29,30,31,32,33,34,35,36], but none of these factors remained associated with mortality after controlling for confounders. Overall, most studies had an overall PAB mortality rate ranging between 30-40% in comparison to our 51.8% mortality rate which was similar to the 90-day mortality rate reported in a study by Aviv et al [37].
The most important limitations to this study are the relatively limited sample size and the fact that the data come from a single center.
5. Conclusions
In the setting of PAB, in addition to prompt anti-pseudomonal empirical treatment, locating the primary source of infection is imperative as it can estimate the severity of the current infection. Increasing antibiotic use has led to increasing rates of DTR pseudomonas infections which warrants the use of more precautions with regards to antibiotic control and prescription. Future multi-centered studies are needed in the region to validate the results of this study.
Author Contributions
Conceptualization, Z.K.; methodology, Z.K.; software, H.I.; validation, Z.K.; formal analysis, Z.K. and H.I.; investigation, Z.K.; resources, Z.K.; data curation, H.I., L.K., M.M, J.A.; writing—original draft preparation, H.I., L.K., M.M, and J.A.; writing—review and editing, H.I. and Z.K.; visualization, Z.K.; supervision, Z.K.; project administration, H.I., L.K., M.M, and J.A.; funding acquisition, not applicable. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the American University of Beirut (protocol code BIO-2022-0065, 3 March 2022).
Informed Consent Statement
Since the study was observational and involved no more than minimal risk, informed consent was waived.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| AUBMC | American University of Beirut Medical Center |
| BMI | Body mass index |
| CLSI | Clinical and Laboratory Standards Institute |
| COPD | Chronic obstructive pulmonary disease |
| DTR | Difficult to treat |
| ICU | Intensive care unit |
| IRB | Institutional Review Board |
| MDR | Multidrug-resistant |
| OR | Odds ratio |
| PA | Pseudomonas aeruginosa |
| PAB | Pseudomonas aeruginosa bacteremia |
| SD | Standard deviation |
References
- Tam, V.H., Rogers, C.A., Chang, K.T., Weston, J.S., Caeiro J.P., Garey K.W. Impact of multidrug-resistant Pseudomonas aeruginosa bacteremia on patient outcomes. Antimicrob Agents Chemother 2010, 54, 3717-22. [CrossRef]
- Alhussain, F.A., Yenugadhati, N., Al Eidan, F.A., Al Johani, S., Badri, M. Risk factors, antimicrobial susceptibility pattern and patient outcomes of Pseudomonas aeruginosa infection: A matched case-control study. J Infect Public Health 2021, 14, 152-7. [CrossRef]
- Rojas, A., Palacios-Baena, Z.R., Lopez-Cortes L.E., Rodriguez-Bano, J. Rates, predictors and mortality of community-onset bloodstream infections due to Pseudomonas aeruginosa: systematic review and meta-analysis. Clin Microbiol Infect 2019, 25, 964-970. [CrossRef]
- Thaden, J.T., Park, L.P., Maskarinec S.A., Ruffin F., Fowler Jr, V.G., van Duin, D. Results from a 13-Year Prospective Cohort Study Show Increased Mortality Associated with Bloodstream Infections Caused by Pseudomonas aeruginosa Compared to Other Bacteria. Antimicrob Agents Chemother 2017, 61, e02671-16. [CrossRef]
- Lee, C.H., Su, T.Y., Ye, J.J., Hsu, P.C., Kuo A.J., Chia J.H., Lee, M.H. Risk factors and clinical significance of bacteremia caused by Pseudomonas aeruginosa resistant only to carbapenems. J Microbiol Immunol Infect 2017, 50, 677-83. [CrossRef]
- Migiyama, Y., Yanagihara, K., Kaku, N., Harada, Y., Yamada, K., Nagaoka, K., Morinaga, Y., Akamatsu, N., Matdusda, J., Izumikawa, K., Kohrogi, H., Kohno, S. Pseudomonas aeruginosa Bacteremia among Immunocompetent and Immunocompromised Patients: Relation to Initial Antibiotic Therapy and Survival. Jpn J Infect Dis 2016, 69, 91-6. [CrossRef]
- McCarthy, K.L., Paterson, D.L. Community-acquired Pseudomonas aeruginosa bloodstream infection: a classification that should not falsely reassure the clinician. Eur J Clin Microbiol Infect Dis 2017, 36, 703-11. [CrossRef]
- Tacconelli, E., Carrara, E., Savoldi, A., Harbarth, S., Mendelson, M., Monnet, D.L., Pulcini, C., et al. Discovery, research, and development of new antibiotics: the WHO priority list of antibiotic-resistant bacteria and tuberculosis. Lancet Infect Dis 2018, 18, 318-27. [CrossRef]
- Raman, G., Avendano, E.E., Chan, J., Merchant, S., Puzniak, L. Risk factors for hospitalized patients with resistant or multidrug-resistant Pseudomonas aeruginosa infections: a systematic review and meta-analysis. Antimicrob Resist Infect Control 2018, 7, 79. [CrossRef]
- Pang, Z., Raudonis, R., Glick, B.R., Lin, T.J., Cheng, Z. Antibiotic resistance in Pseudomonas aeruginosa: mechanisms and alternative therapeutic strategies. Biotechnol Adv 2019, 37, 177-92. [CrossRef]
- Meyer, E., Gastmeier, P., Deja, M., Schwab, F. Antibiotic consumption and resistance: data from Europe and Germany. Int J Med Microbiol 2013, 303, 388-95.
- Sindeldecker, D., Stoodley, P. The many antibiotic resistance and tolerance strategies of Pseudomonas aeruginosa. Biofilm 2021, 3, 100056. [CrossRef]
- Hancock, R.E. Resistance mechanisms in Pseudomonas aeruginosa and other nonfermentative gram-negative bacteria. Clin Infect Dis 1998, 27, S93-9. [CrossRef]
- Chatterjee, M., Anju, C.P., Biswas, L., Kumar, V.A., Mohan, C.G., Biswas, R. Antibiotic resistance in Pseudomonas aeruginosa and alternative therapeutic options. Int J Med Microbiol 2016, 306, 48-58. [CrossRef]
- Breidenstein, E.B., de la Fuente-Núñez, C., Hancock R.E. Pseudomonas aeruginosa: all roads lead to resistance. Trends Microbiol 2011, 19, 419-26. [CrossRef]
- Soares, A., Alexandre, K., Etienne, M. Tolerance and persistence of Pseudomonas aeruginosa in biofilms exposed to antibiotics: molecular mechanisms, antibiotic strategies and therapeutic perspectives. Front Microbiol 2020, 11, 2057. [CrossRef]
- Cigana, C., Bernardini, F., Facchini, M., Alcala-Franco, B., Riva, C., De Fino, I., Rossi, A., et al. Efficacy of the novel antibiotic POL7001 in preclinical models of Pseudomonas aeruginosa pneumonia. Antimicrob Agents Chemother 2016, 60, 4991-5000. [CrossRef]
- El-Herte, R.I., Kanj, S.S., Matar, G.M., Araj, G.F. The threat of carbapenem-resistant Enterobacteriaceae in Lebanon: an update on the regional and local epidemiology. J Infect Public Health 2012, 5, 233-43. [CrossRef]
- Abbara, A., Rawson, T.M., Karah, N., El-Amin W., Hatcher, J., Tajaldin, B.Dar, O., et al. Antimicrobial resistance in the context of the Syrian conflict: drivers before and after the onset of conflict and key recommendations. Int J Infect Dis 2018, 73, 1-6. [CrossRef]
- Osman, M., Halimeh, F.B., Rafei, R., Mallat, H., El Tom, J., Raad, E.B., Diene, S.M., et al. Investigation of an XDR-Acinetobacter baumannii ST2 outbreak in an intensive care unit of a Lebanese tertiary care hospital. Future Microbiol 2020, 15, 1535-42. [CrossRef]
- Dabbousi, A.A., Dabboussi, F., Hamze, M., Osman, M., Kassem, I.I. The emergence and dissemination of multidrug resistant Pseudomonas aeruginosa in Lebanon: current status and challenges during the economic crisis. Antibiotics (Basel) 2022, 11, 687. [CrossRef]
- Sakr, S., Ghaddar, A., Hamam, B., Sheet, I. Antibiotic use and resistance: An unprecedented assessment of university students’ knowledge, attitude and practices (KAP) in Lebanon. BMC Public Health 2020, 20, 535. [CrossRef]
- Hirsch, E.B., Cottreau, J.M., Chang, K.T., Caeiro, J.P., Johnson, M.L., Tam, V.H. A model to predict mortality following Pseudomonas aeruginosa bacteremia. Diagn Microbiol Infect Dis 2012, 72, 97-102. [CrossRef]
- Teelucksingh, K., Shaw., E. Clinical characteristics, appropriateness of empiric antibiotic therapy, and outcome of Pseudomonas aeruginosa bacteremia across multiple community hospitals. Eur J Clin Microbiol Infect Dis 2022, 41, 53-62. [CrossRef]
- Yoon, Y.K., Kim, H.A., Ryu, S.Y., Lee, E.J., Lee, M.S., Kim, J., Park, S.Y., et al. Tree-structured survival analysis of patients with Pseudomonas aeruginosa bacteremia: A multicenter observational cohort study. Diagn Microbiol Infect Dis 2017, 87, 180-7. [CrossRef]
- Joo, E.J., Kang, C.I., Ha, Y.E., Park, S.Y., Kang, S.J., Wi, Y.M., Lee, N.Y., et al. Impact of inappropriate empiric antimicrobial therapy on outcome in Pseudomonas aeruginosa bacteraemia: a stratified analysis according to sites of infection. Infection 2011, 39, 309-18. [CrossRef]
- Parkins, M.D., Gregson, D.B., Pitout, J.D., Ross, T., Laupland, K.B. Population-based study of the epidemiology and the risk factors for Pseudomonas aeruginosa bloodstream infection. Infection 2010, 38, 25-32. [CrossRef]
- Moghnieh, R.A., Kanafani, Z.A., Tabaja, H.Z., Sharara, S.L., Awad, L.S., Kanj, S.S. Epidemiology of common resistant bacterial pathogens in the countries of the Arab league. Lancet Infect Dis 2018, 18, e379-94. [CrossRef]
- Kang, C.I., Kim, S.H., Kim, H.B., Park, S.W., Choe, Y.J., Oh, M.D., Kim, E.C., et al. Pseudomonas aeruginosa bacteremia: risk factors for mortality and influence of delayed receipt of effective antimicrobial therapy on clinical outcome. Clin Infect Dis 2003, 37, 745-51. [CrossRef]
- Babich, T., Naucler, P., Valik, J.K., Giske, C.G., Benito, N., Cardona, R., Rivera, A., et al. Risk factors for mortality among patients with Pseudomonas aeruginosa bacteraemia: a retrospective multicentre study. Int J Antimicrob Agents 2020, 55, 105847. [CrossRef]
- Lodise, T.P. Jr, Patel, N., Kwa, A., Graves, J., Furuno, J. P., Graffunder, E., Lomaestro, B. et al. Predictors of 30-day mortality among patients with Pseudomonas aeruginosa bloodstream infections: impact of delayed appropriate antibiotic selection. Antimicrob Agents Chemother 2007, 51, 3510-5. [CrossRef]
- Furtado, G.H., Bergamasco, M.D., Menezes, F.G., Marques, D., Silva, A., Perdiz, L.B., Wey, S.B. et al. Imipenem-resistant Pseudomonas aeruginosa infection at a medical surgical intensive care unit: risk factors and mortality. J Crit Care 2009, 24, 625.e9-14. [CrossRef]
- Kang, C.I., Chung, D.R., Peck, K.R., Song, J.H. Clinical predictors of Pseudomonas aeruginosa or Acinetobacter baumannii bacteremia in patients admitted to the ED. Am J Emerg Med 2012, 30, 1169-75. [CrossRef]
- Hilf, M., Yu, V.L., Sharp, J., Zuravleff, J.J., Korvick, J.A., Muder, R.R. Antibiotic therapy for Pseudomonas aeruginosa bacteremia: outcome correlations in a prospective study of 200 patients. Am J Med 1989, 87, 540-6. [CrossRef]
- Zhang Y., Chen, X.L., Huang, A.W., Liu S.L., Liu, W.J., Zhang, N., Lu X.Z. Mortality attributable to carbapenem-resistant Pseudomonas aeruginosa bacteremia: a meta-analysis of cohort studies. Emerg Microbes Infect 2016, 5, e27. [CrossRef]
- Peña, C., Suarez, C., Ocampo-Sosa, A., Murillas, J., Almirante, B., Pomar, V., Aguilar, M. et al. Effect of adequate single-drug vs combination antimicrobial therapy on mortality in Pseudomonas aeruginosa bloodstream infections: a post Hoc analysis of a prospective cohort. Clin Infect Dis 2013, 57, 208-16. [CrossRef]
- Aviv, T., Lazarovitch, T., Katz, D., Zaidenstein, R., Dadon, M., Daniel, C., Tal-Jasper, R. et al. The epidemiological impact and significance of carbapenem resistance in Pseudomonas aeruginosa bloodstream infections: a matched case-case-control analysis. Infect Control Hospital Epidemiol 2018, 39, 1262-5. [CrossRef]
Figure 1.
Sources of infection in patients with P. aeruginosa bacteremia.
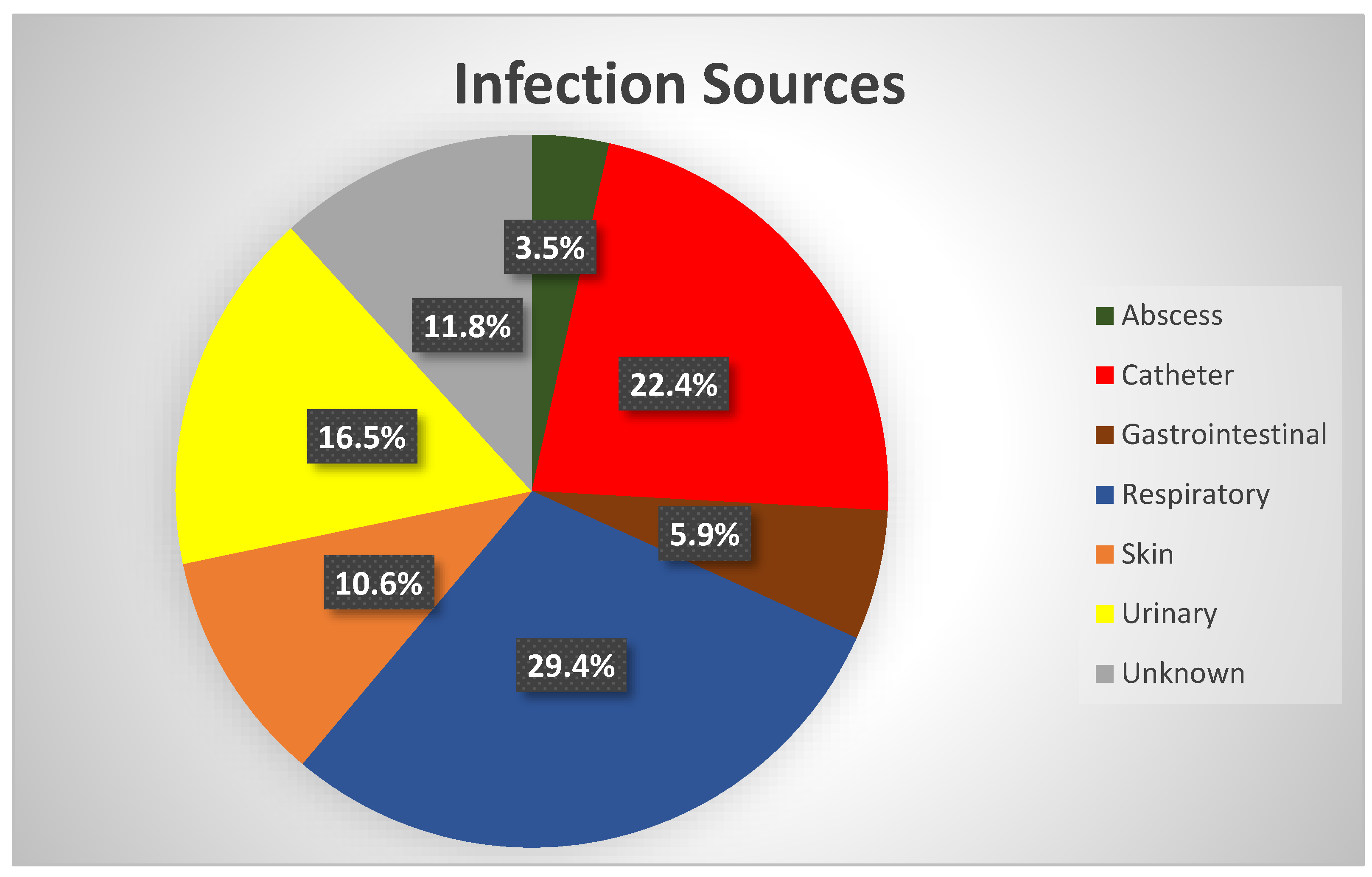

Table 1.
Demographic and clinical characteristics of patients with P. aeruginosa bacteremia.
| Characteristic | Value (N = 85) |
|---|---|
| Age, years (mean ± SD) | 64.5 ± 16.8 |
| Male sex | 60 (70.6) |
| BMI, kg/m2 (mean ± SD) | 27.6 ± 5.4 |
| Malignancy | 41 (48.2) |
| Solid | 23 (27.1) |
| Hematologic | 18 (21.2) |
| Diabetes | 27 (31.8) |
| Chronic kidney disease | 14 (16.5) |
| Hemodialysis | 6 (7.1) |
| COPD | 6 (7.1) |
| Burn injury | 3 (3.5) |
| HIV infection | 2 (2.4) |
| Hospital stay > 2 days* | 69 (81.2) |
| ICU stay > 2 days* | 45 (52.9) |
| Mechanical ventilation > 2 days* | 37 (43.5) |
| Central line > 2 days* | 56 (65.9) |
| Urinary catheter > 2 days* | 43 (50.6) |
| Nasogastric tube > 2 days* | 36 (42.4) |
| Steroid use* | 47 (55.3) |
| Surgery* | 21 (24.7) |
| Clean | 7 (8.2) |
| Clean-contaminated/contaminated | 14 (16.5) |
| Route of acquisition | |
| Hospital-acquired | 67 (78.8) |
| Community-acquired | 12 (14.1) |
| Healthcare-associated | 6 (7.1) |
| Pitt Bacteremia Score > 4 | 44 (51.8) |
All values represent n (%) except where otherwise indicated. * within 30 days prior to the infection. SD = standard deviation; BMI = body mass index; COPD = chronic obstructive pulmonary disease; ICU = intensive care unit.
Table 2.
Complications associated with P. aeruginosa bacteremia.
| Complications | Frequency (N = 85) |
|---|---|
| Sepsis | 69 (81.2) |
| ICU admission | 54 (63.5) |
| Septic shock | 49 (57.6) |
| Acute renal failure | 48 (56.5) |
| Hospital-acquired infection | 45 (52.9) |
| Mechanical ventilation | 43 (50.6) |
| Cardiovascular event | 30 (35.3) |
| Persistence/progression of the infection | 29 (34.1) |
| Recurrent infection | 19 (22.4) |
| Acute respiratory distress syndrome | 9 (10.6) |
| Persistent bacteremia | 6 (7.1) |
| Cerebrovascular event | 5 (5.9) |
| Systemic embolism | 1 (1.2) |
All values represent n (%). ICU = intensive care unit.
Table 3.
Predictors of mortality among patients with P. aeruginosa bacteremia.
| Variable | Unadjusted OR | p-Value | Adjusted OR | p-Value |
|---|---|---|---|---|
| Pitt bacteremia score ≥ 4 | 28.2 | < 0.01 | 51.7 | < 0.01 |
| High-risk source† | 24.3 | < 0.01 | 26.0 | < 0.01 |
| Central line* | 6.0 | 0.02 | 2.6 | 0.03 |
| Male sex | 3.7 | 0.05 | 0.1 | 0.04 |
| COPD | 6.0 | 0.01 | ||
| Steroid use* | 8.5 | < 0.01 | ||
| Hospital stay* | 8.6 | < 0.01 | ||
| ]ICU stay* | 8.7 | < 0.01 | ||
| Mechanical ventilation* | 7.9 | < 0.01 | ||
| Route of acquisition | 5.7 | 0.02 |
OR = odds ratio; COPD = chronic obstructive pulmonary disease; ICU = intensive care unit. †primary bacteremia or pneumonia. * within 30 days prior to the infection.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



