
Submitted:
09 July 2025
Posted:
10 July 2025
You are already at the latest version
Abstract
Background/Objectives: Self-adhesive flowable resins (SAFR) entered the market, eliminating the adhesive system application due to their self-adhesive technology. The aim was to conduct a systematic review of clinical studies to compare the clinical performance of Self Adhesive Flowable Resin (SAFRs) with conventional flowable resins used for direct restorations. Methods: The protocol of this systematic review was registered in the International Prospective Register of Systematic Reviews (CRD42023394297) and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guideline. A search of the scientific literature was performed by two independent reviewers using PubMed, Embase, Web of Science, Scopus, and Cochrane databases from commencement until July 2025. Investigations evaluating the clinical performance of SAFRs as direct restorative materials were included. The RevMan 5.4 program was used for meta-analysis, calculating the risk difference and 95% confidence interval (CI) of the dichotomous outcome (marginal adaptation, retention, post-operative sensitivity, marginal staining, smoothness, secondary caries, anatomical form and color match) using a random-effects model. Results: Nine studies were selected, comprising 493 analyzed restorations. The results revealed a comparable SARFs performance to conventional resins in terms of marginal adaptation, retention, post-operative sensitivity, marginal staining, smoothness, secondary caries, anatomical form and color match. Conclusions: SAFRs restorations exhibited comparable clinical performance when compared to conventional resins, specifically in the outcomes studied.
Keywords:
self-adhesive flowable composite
; dental restoration
; direct restoration
; resin composite
; systematic review
1. Introduction
Composite resins stand as the primary choice among clinicians for restorative materials. As a result, manufacturers persistently work towards enhancing the aesthetic and physical-mechanical properties of these materials. They function by replacing lost dental tissue due to caries or fractures, ensuring aesthetics and functionality for patients [1,2]. The restorative protocol for conventional composite resins involves acid conditioning and adhesive application to prepare the dental substrate. These additional steps make the technique more susceptible to errors and demand more clinical time [3]. Motivated by this, self-adhesive flowable resins (SAFR) entered the market, eliminating the adhesive system application due to their self-adhesive technology, a step prone to errors [4]
The self-adhesiveness of this new class of composite resin is conferred by the addition of the glycerol-phosphate molecule, which conditions the dental structure while also having an affinity for dental element calcium and methacrylate groups that copolymerize with other methacrylate monomers [5]. However, it is important to note that tissue demineralization is partial, meaning there is no complete removal of the smear layer, incorporating it into the adhesive interface, unlike the usually applied technique of total acid conditioning, where the smear layer is entirely removed [6].
SAFRs are indicated for direct restoration repair [7] direct restorative material [8], and as pit and fissure sealants [9]. However, in vitro studies indicate that SAFRs exhibit inferior marginal sealing ability and dentin bond strength values compared to other adhesive systems and conventional flowable resins [3,5]. These findings may be due to the finer resinous tags formed, presence of the smear layer, and high viscosity of SAFRs [4,10,11]. In contrast, other in vitro studies have demonstrated that SAFRs exhibit superior marginal sealing compared to all-in-one adhesive systems in class II cavities, and similar marginal adaptation to conventional flowable in class I cavities [12,13]. These results have been attributed to the lower hygroscopic expansion and polymerization shrinkage of SAFRs [13]. Clinical trials have revealed the potential use of SAFRs as restorative materials in Class I cavities, demonstrating notable clinical effectiveness regarding retention, secondary caries, and marginal discoloration [8]. However, there is a chance of suboptimal performance in terms of marginal adaptation and polishing [14]. In Non-Carious Cervical Lesions, the restorations exhibit a high failure rate [15]. Based on the available evidence from clinical and laboratory research, it is currently impossible to determine whether SAFRs possess favorable properties and clinical efficacy, thus casting doubt on their suitability for clinical use. Therefore, it is necessary to compile current scientific evidence on SAFRs performance.
There is a necessity to conduct an evidence synthesis study that examines data from multiple primary clinical studies. Such a study enables the generation of robust and dependable scientific evidence concerning the clinical suitability of this new material. This effort aims to offer stronger scientific evidence regarding the clinical performance of this new restorative material and to affirm or contest it’s for use. Therefore, the aim of this systematic review was to compare the clinical performance of SAFRs and conventional flowable resins for direct restoration.
2. Materials and Methods
2.1. Protocol and Registration
This systematic review was conducted following the guidelines of the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines (Supplementary Material Table S1) [16] and was structured as follows: (1) identification of the guiding question, (2) gathering of relevant studies, (3) determination of inclusion and exclusion criteria, (4) data extraction, and (5) synthesis of results [17]. Prior to commencement, the methodology of this study was registered in PROSPERO (International Prospective Register of Systematic Reviews) with the protocol number CRD42023394297.
2.2. Eligibility Criteria
The guiding question for this review was "Do SAFRs have clinical performance comparable to conventional flowable resins as direct restorative materials?" The Population/Problem, Intervention/Exposure, Comparison, and Outcome of the study were guided by the PICO strategy. The Population (P) consisted of patients with restorations in posterior teeth. The Intervention (I) analyzed was direct restoration with SAFRs, and the Comparator (C) was conventional flowable resin. The Outcomes (O) evaluated were marginal adaptation, retention, marginal staining, post-operative sensitivity, color stability, surface roughness, smoothness, secondary caries, and anatomical form.
Inclusion criteria for the studies were: (1) randomized clinical trials evaluating the clinical performance of SAFRs as direct restorative materials; (2) a follow-up period longer than 5 months. Exclusion criteria were: (1) Studies evaluating SAFRs only regarding post-operative sensitivity; (2) studies assessing the ability of SAFRs as sealing agents; (3) Studies that included experimental SAFRs; (4) unpublished information in the scientific literature; (5) studies with unavailable full text.
2.3. Information Sources and Search Strategy
PubMed, Embase, Web of Science, Scopus, and Cochrane were accessed on July 2, 2025, using a search strategy that did not limit a chronological period to find clinical studies evaluating the use of self-adhesive flowable composites as direct restorative materials. The following Medical Subject Headings (MESH) or text words were used: self-adhesive composite, self-adhering composite, self-adherent composite, permanent dental restorations, permanent dental restoration, permanent dental filling, flowable hybrid composite, flowable composite, and flowline. The following search was performed across all databases: [("Self adhering composite" OR "self adhesive composite" OR "self-adherent composite") AND ("restorations, permanent dental" OR "restoration permanent dental" OR "dental permanent filling")] AND ["flowable hybrid composite" OR "hybrid composite flowable" OR "flowline"] (Table 1).
2.4. Selection Process
Studies were saved and systematically organized using the online program Rayyan [18]. Duplicates were first removed, and then titles and abstracts were read to determine if the studies met the predefined criteria. The selection process was conducted independently by two authors (S.B.M. and C.F.C.L), previously calibrated, and discrepancies were discussed with a third author (G.L.d.M). The calibration process involved the two authors (S.B.M. and C.F.C.L.), initially reading and assessing a set of 10 articles together to ensure alignment in their understanding and application of the selection criteria. Through this collaborative review, they established a consistent approach to article selection based on the predetermined criteria. Subsequently, any disparities or discrepancies encountered during the independent selection process were addressed through discussion and consensus with the third author (G.L.d.M). Eligible articles were read in full, and their data were extracted.
2.5. Data Collection Process
Three authors (S.B.M. C.F.C.L and G.L.d.M.), previously calibrated, performed data extraction using a guiding table covering the main methodological characteristics of the studies. Key data included author, publication year, self-adhesive composite used, volunteers, number of restored teeth, type of restored tooth, cavity type, study design, follow-up period, analysis criteria, and conclusion.
2.6. Study Risk of Bias Assessment
Included studies underwent a risk of bias analysis by two authors (S.B.M and C.F.C.L.), previously calibrated. The Cochrane Risk of Bias for Randomized Trials version 2 (RoB 2) tool was used, structured into domains analyzing bias arising from randomization process, deviations from intended interventions, missing outcome data, measurement of outcome, and selection of reported results [19]. For each domain there are signaling questions, that are designed to offer a systematic method for extracting information pertinent to assessing the risk of bias and offer as answers: yes, probably yes, probably no, no, no information [20]. After response the signaling questions, the next step is to reach a risk-of-bias judgment, as follow: Low risk of bias, some concerns or high risk of bias [19]. The RoB 2 tool incorporates algorithms that link responses to signaling questions to a suggested risk-of-bias assessment for each domain [19]. In case of disagreement between the two assessors, a third assessor was consulted to reach a consensus (G.L.d.M).
2.7. Effect Measures and Synthesis Methods
Meta-analysis was performed using a random-effects model. Review Manager version 5.4 (Cochrane collaboration) was used to calculate the risk difference with a 95% confidence interval. For this analysis, data were dichotomized. The acceptable restorations were those that received the Alpha and Bravo scores. The unacceptable restorations were those that received the Charlie score in at least one clinical parameter of the USPHS (marginal adaptation, retention, sensitivity, color stability, smoothness, secondary caries, and anatomical form). The clinical parameters evaluated by the FDI criteria that coincide with the parameters assessed by the USPHS were also included. In this case, scores 4 and 5 were considered, comparable to the Charlie score, and these data were used in the meta-analysis. Table 2 outlines the USPHS assessment criteria and Table 3 outlines FDI assessment criteria.
2.8. Certainty Assessment
Certainty of evidence was assessed for each outcome using the Grading of Recommendations: Assessment, Development, and Evaluation (GRADE) tool (http://www.gradeworkinggroup.org/). This tool categorizes the study design and addresses risk of bias, imprecision, inconsistency, indirectness of evidence, and publication bias to possibly classify the quality of evidence. Each of these items is assessed as "no limitation," "serious limitations," and "very serious limitations" to categorize the evidence quality as high, moderate, low, or very low. Lower quality suggests that the estimate is far from the actual effect.
3. Results
3.1. Study Selection
A total of 155 studies were extracted from the databases in the search conducted in July 2025. After removing duplicates, 121 studies remained, and their titles and abstracts were analyzed according to the pre-defined inclusion and exclusion criteria. Full article reading was conducted on 13 studies considered potentially eligible, of which 9 met the selection criteria (Figure 1). One study was excluded for assessing only post-operative sensitivity criteria [20], another for evaluating effectiveness in teeth with previous hypersensitivity [21], for clinically evaluating self-adhesive resin as pit and fissure sealant [9], and the last due being a non-randomized clinical study [15].
3.2. Study Characteristics
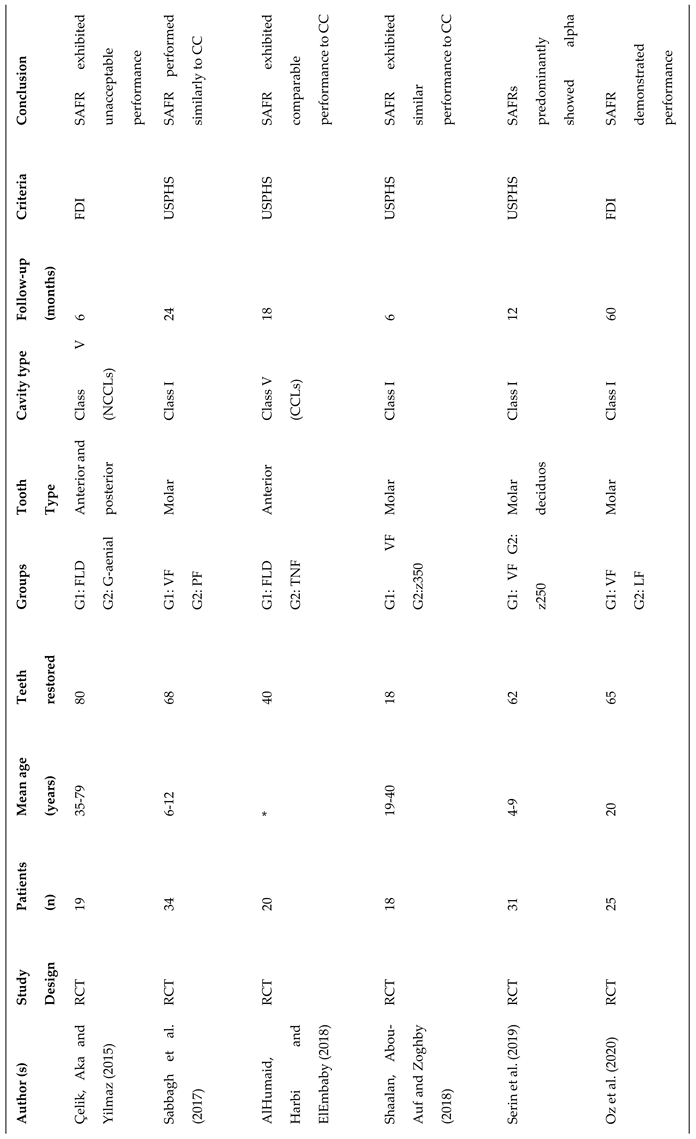
The characteristics of the studies are observed in Table 4.
The included articles were published between 2015 and 2022. The number of participants varied between 18 and 37. The ages of the study volunteers ranged from 4 to 79 years, with follow-up periods from 6 months to 5 years [8,14,22,23,24,25,26,27,28] The countries where the studies were conducted were Saudi Arabia [24], Poland [14], Turkey [22,26,27], Lebanon [23], Egypt [24,25] and India [8].
The total number of treated patients and restored teeth was 232 and 493, respectively. In seven studies, class I cavities were performed [8,14,23,25,26,27,28], and in two, class V cavities were performed [22,24], one non-carious cervical lesion [22] and other cervical carious lesion [24]. The restored dental elements included molars, incisors, canines, premolars, and deciduous molars. Of the selected studies, only Çelik, Aka, Yilmaz [23] and Oz et al. [27] used the FDI criteria, and the others used the USPHS. The SAFRs used were Vertise Flow [14,23,24,25,27,28], Fusion Liquid Dentin [8,22,24] The conventional flowable resins used were Premise Flowable [14,22,24], Tetric N Flow [8,24], Filtek z350 Xt [27,28], Filtek z250 [26, LuxaFlow27]. Almost all studies reported using absolute isolation, except for Maj et al. [14] and Oz et al. [27]. Çelik, Aka, Yilmaz [22] performed relative isolation. One study also evaluated the influence of using absolute isolation or cotton rolls [23].
For the meta-analysis, the studies that applied the United States Public Health Service (USPHS) criteria were extracted for the proportion of restorations considered with worse scores (Charlie) and studies that applied the World Dental Federation (FDI) were extracted the restorations with the equivalent worse scores (score 4 and 5), in the following criteria: adequate marginal adaptation, retention, sensitivity, marginal pigmentation, color match, surface roughness, polishing, recurrence of caries, and anatomical form (Table 5). Variables not analyzed were filled in the table with "not mentioned”.
3.3. Risk of Bias in Studies
The RoB 2 tool was used for the randomized clinical trials. Two studies did not describe the randomization process. Shaalan, Abou-Auf, and Zoghby [25] used a random sequence generator called "Randomness and Integrity Services," Oz et al. [27] used the "Research Randomized Program" tool, and Shalan and Abou-Auf [29] used the site "random.org." Four studies did not describe the method of patient allocation. Shaalan, Abou-Auf, and Zoghby [27] and Shalan and Abou-Auf [28] used sealed opaque envelopes. Two articles presented incomplete data on blinding of participants, examiners, and staff. [8,14] Two articles showed incomplete data on follow-up loss [4,8]. And, one study presented incomplete data on allocation knowledge by examiners and incomplete data on a pre-specified analysis plan [8] (Figure 2).
3.4. Results of Syntheses
The meta-analysis was conducted exclusively for Class I and II cavities because only one study evaluated carious lesions in Class V cavities, and another study assessed non-carious cervical lesions. As a result, it was impossible to include these studies in the same meta-analysis. The meta-analysis included the five studies selected in the systematic review. No significant differences were observed between conventional resin composites and SAFRs for the outcomes studied (p>0.05) (Figure 3, Figure 4, Figure 5, Figure 6, Figure 7, Figure 8, Figure 9 and Figure 10 ).
Descriptive analysis of the data not included in the systematic review [8,14,22,26] revealed a serious report on the lack of retention (27 out of 40 restorations) of SARFs in non-carious cervical lesions [22]. In Class V cavities (carious cervical lesions), no statistical difference was found with conventional resin used as a control [24]. In deciduous teeth, Serin et al. [26] reported no restoration failures in the evaluated clinical parameters (retention, post-operative sensitivity, marginal staining, and anatomical form). The number of restorations with alpha score (success) decreased over time, however, no performance difference was found between SARF and conventional flowable resin after 2 years of evaluation.
3.5. Certainty of Evidence
In Table 6, it is shown that the certainty of the evidence of marginal adaptation, retention, post-operative sensitivity, staining risk, smoothness, secondary caries, anatomic form, and marginal discoloration was rated as high for all follow-up periods.
4. Discussion
This systematic review and meta-analysis of clinical studies aimed to assess the clinical performance of SAFRs as direct restorative materials. The meta-analysis results revealed that SAFRs demonstrate clinically comparable results to conventional composite resins for the outcomes studied (anatomical form, secondary caries, marginal adaptation, color match, smoothness, retention, sensibility, and marginal staining). SAFRs combine features of both a restorative material and an adhesive system, providing advantages such as reduced clinical time by eliminating adhesive steps [30].
Most include studies of this systematic review and meta-analysis utilized Vertise Flow self-adhesive resin (n=5) [14,24,25,27,28], followed by Fusion Liquid Dentin (n=4) [8] (Table 4). Vertise Flow resin bond to the tooth through the affinity between the Glycerol Phosphate Dimethacrylate (GPDM) monomer and calcium ions in the tooth, as well as through micromechanical bonding between polymerized monomers and collagen fibers in dentin.31 Fusion Liquid Dentin resin contains the negatively charged 4-Methacryloxyethyl trimellitate anhydride (4-META) monomer, which links to tooth ions, incorporating into dentin and improving adhesion and sealing [32]. The clinical performance of SAFRs was evaluated in Class I (n=5) [8,14,25,27,28], Class V (n=1) [24] and Non-Carious Cervical Lesion (NCCL) (n=1) [22] cavities. Class V cavities and NCCL, compared to Class I, lack micromechanical retention in their cavity configuration, favoring analyses related to adhesion [15].
The most commonly used method for clinical evaluation of resins in the reviewed studies was USPHS, an event that proves to be a trend in clinical studies [26]. This criterion encompasses biological, aesthetic, and functional aspects of the investigated restorative materials through randomized clinical trials [33]. However, another criterion, known as the FDI criteria, is also utilized to monitor the longevity of restorative procedures in clinical trials. A study emphasizes that the variety of scores (1-5) enables a higher potential to detect differences in restorations, thereby enhancing the quality of the evaluation conducted [34]. For the meta-analysis, restorations that obtained the Charlie score (USPHS) or score 4 and 5 (FDI criteria) in the assessed parameters (anatomical form, secondary caries, marginal adaptation, color match, smoothness, retention, sensibility and, marginal staining) were counted. This score represents the category that considers the restorative procedure as unacceptable or unsuccessful [26,34]. Surface roughness was excluded from the meta-analysis due to the lack of comparative studies, as the analyses were conducted separately according to the type of dental cavity. Therefore, future clinical studies evaluating surface roughness are required.
Retention of SAFRs was comparable with conventional flowable resins in the meta-analysis of this study when compared in posterior teeth (Figure 3). For a restoration's performance to be considered successful, it needs to have longevity, thus confirming retention as one of the most important criteria [24]. This favorable performance may be related to the type of cavity that tends to be more retentive (Class I and II) [28]. Despite these results, in the study by Çelic, Aka, and Yılmaz [22], a failure rate of 67.5% was found in SARF retention. This event may be attributed to the hydrolytic degradation of the resin-dentin interface and lower conditioning capacity of SAFC [15,21,22]. More specifically, the poorer performance of Fusion Liquid Dentin may be related to the hydrolytic instability of 4-META. Additionally, this study evaluated the performance of SARF in NCCLs cavities that lack micromechanical retention, a factor that may reveal the true behavior of the material regarding adhesiveness and must be object of future studies. Alongside retention, marginal adaptation clarifies the sealing ability of restorative materials [22]. Following the same pattern, the marginal adaptation (Figure 4) of SAFRs was comparable to that of conventional flowable resins. The comparable performance of SARFs can be attributed to their chemical composition, including the presence of GPDM (for conditioning dentin and enamel), HEMA, amorphous silica, and nano-sized glass. Additionally, as the carboxylic acids of the material are neutralized and the monomers polymerize, they integrate into the dentin surface, enhancing its sealing capacity [24,35]. In regard to postoperative sensitivity SAFRs showed also comparable results to the control group (Figure 5).
The absence of postoperative sensitivity is related to the absence of acid conditioning and smear layer removal, keeping dentinal tubules sealed [36]. The literature highlights that eliminating the need for separate acid conditioning and adhesive application reduces the risk of excessive conditioning, excessive wetting, or excessive drying, factors that can cause the collapse of collagen fibers [15]. The success of a restorative procedure is also related to color stability over time [35]. Regarding discoloration of the restoration, SAFRs showed comparable performance when analyzing the resin color during the follow-up period of the studies included in the meta-analysis (Figure 6). The greater color change in conventional flowable resin may be related to the larger size of its particles, making it more susceptible to discoloration [24]. This fact may also justify the similar results regarding marginal discoloration (Figure 7).
A roughness surface texture may promote plaque accumulation and increase the risk of secondary caries, with this characteristic being influenced by the composition and size of the fillers present in composite resins. SARFs exhibit good surface finishing, possibly due to the presence of nano-sized silica and glass [24]. This characteristic justifies the comparable performance of SARFs to conventional resins in terms of surface smoothness and secondary caries occurrence (Figure 8 and Figure 9). Another factor influencing the recurrence of secondary caries is the interface stress between the resin material and the tooth. The literature mentions that stress between SARF and the tooth is insufficient to cause restoration separation and subsequent marginal infiltration, likely due to its low modulus of elasticity, thereby reducing the risk of secondary caries formation. Regarding anatomic form, SARF exhibit similar performance comparable to conventional resin (Figure 10). Azizi et al [37] found similar result. Fluid resins tend to exhibit good behavior regarding wear due to the presence of small particles and intra-particle spaces that protect the matrix [37]. There are few studies investigating the wear resistance of SARFs, making it difficult to gain a greater understanding of the compositions and characteristics of these resins.
Regarding the analysis of bias in the studies, most were classified as Low concerns [24,26,27], followed by some concerns [8,14] Studies with a low risk of bias reduce influences that could alter the results, making the findings more reliable and valid. The quality of evidence produced in the meta-analysis was classified as high, originating from RCTs that mostly presented a not serious risk of bias. A high level of evidence demonstrates robustness in the findings of the study and assists in evidence-based decision-making. The results should be interpreted with caution, and limitations should be taken into consideration.
Based on the findings of this study, SAFRs showed comparable clinical performance compared to conventional flowable resins in terms of retention, marginal adaptation, postoperative sensitivity, marginal discoloration, anatomic form, secondary caries, smoothness and color stability. This study had the limitation of including studies with a follow-up time between 6 months to 5 years; differences in the effectiveness of therapies can only be accurately measured after a period of 10 years, as restorative materials may exhibit different susceptibilities to failure over time [38]. Some studies included in the meta-analysis used the USPHS criterion, whose sensitivity is limited and may not definitively determine whether such a restorative procedure was successful or not [36]. The FDI criteria appear to be more sensitive and accurate than the USPHS criteria in detecting small differences in clinical studies [37]. Another limitation was the scarcity of studies in non-retentive cavities (Class V and NCCLs), as these are more ideal for studying the adhesive properties of a restorative material [22]. The findings of this systematic review and meta-analysis should be evaluated with caution due to the limited number of available clinical studies. We suggest conducting more randomized clinical studies to assess the clinical capability of these new flowable resins introduced to the market as direct restorative materials, particularly with a longer follow-up period, as the number of events tends to be lower in initial assessments.
5. Conclusions
Within the limitations of this systematic review and meta-analysis it was concluded that self-adhesive flowable resins exhibited comparable clinical performance to conventional flowable resins across various parameters, including retention, marginal adaptation, postoperative sensitivity, marginal discoloration, anatomic form, secondary caries, smoothness, and color stability. These findings were observed when these materials were evaluated as direct restorative materials over a follow-up period ranging from 6 months to 5 years.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Author Contributions: S.B.M., C.d.F.C.L and G.L.d.M. contributed to the study conception and design, and S.B.M. and R.B.W.e.L., for the material preparation and data collection. A.K.M.d.A. and G.L.d.M. performed the statistical analysis, R.B.W.e.L., A.K.M.d.A., R.B.E.L., and M.A.J.R.M. critically revised the manuscript and supervised the review process. The first draft of the manuscript was written by S.B.M. and C.d.F.C.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
All the data are available within the manuscript.
Acknowledgments
The authors acknowledge the Brazilian Federal Agency for Support and Evaluation of Graduate Education (CAPES).
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Miletic, V. Development of Dental Composites. Dental Composite Materials for Direct Restorations 2018, 1, 1–15. [Google Scholar]
- Neto, J.M.A.S.; da Silva, L.E.E.; Souza, C.C.B.; et al. Utilização de resinas compostas em dentes anteriores REAS 2021, 132, 1-7.
- David, C., Cardoso de Cardoso, G.; Isolan, C.P., Piva, E.; Moraes, R.R., Cuevas-Suarez, C.E. Bond strength of self-adhesive flowable composite resins to dental tissues: A systematic review and meta-analysis of in vitro studies. J Prosthet Dent 2022, 128, 876–885. [Google Scholar] [CrossRef] [PubMed]
- Peterson, J.; Rizk, M.; Hoch, M.; Wiegand, A. Bonding performance of self-adhesive flowable composites to enamel, dentin and a nano-hybrid composite. Odontology 2018, 106, 171–180. [Google Scholar] [CrossRef] [PubMed]
- Jordehi, A.Y.; Shahabi, M.S.; Akbari, A. Comparison of self-adhering flowable composite microleakage with several types of bonding agent in class V cavity restoration. Dent Res J (Isfahan) 2019, 16, 257–263. [Google Scholar] [CrossRef]
- Sachdeva, P.; Goswami, M.; Singh, D. Comparative evaluation of shear bond strength and nanoleakage of conventional and self-adhering flowable composites to primary teeth dentin Contemp Clin Dent 2016, 7, 326-331.
- Sismanoglu, S. Efficiency of self-adhering flowable resin composite and different surface treatments in composite repair using a universal adhesive Niger J Clin Pract 2019, 22, 1675-1679.
- Kalola, A.V.; Sreejith, S.U.; Kanodia, S.; Parmar, A.; Iyer, J.V.; Parmar, G.J. Comparative clinical evaluation of a self-adhering flowable composite with conventional flowable composite in Class I cavity: An in vivo study. J Conserv Dent 2022, 25, 156–160. [Google Scholar] [CrossRef] [PubMed]
- Wadhwa, S.; Nayak, U.; Kappadi, D.; Prajapati, D.; Sharma, R.; Pawar, A. Comparative Clinical Evaluation of Resin-based Pit and Fissure Sealant and Self-adhering Flowable Composite: An In Vivo Study Int J Clin Pediatr Dent 2018, 11, 430-434.
- Mine, A.; De Munck, J.; Van Ende, A.; Poitevin, A.; Matsumoto, M.; Yoshida, Y.; Kuboki, T.; Van Landuyt, K.L.; Yatani, H.; Van Meerbeek, B. Limited interaction of a self-adhesive flowable composite with dentin/enamel characterized by TEM. Dent Mater 2017, 33, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Brueckner, C.; Schneider, H.; Haak, R. Shear Bond Strength and Tooth-Composite Interaction With Self-Adhering Flowable Composites Oper Dent 2017, 42, 90-100.
- Gayatri, C.; Rambabu, T.; Sajjan, G.; Battina, P.; Priyadarshini, M.S.; Sowjanya, B.L. Evaluation of Marginal Adaptation of a Self-Adhering Flowable Composite Resin Liner: A Scanning Electron Microscopic Stud. Contemp Clin Dent 2013, 9, 1497–506. [Google Scholar] [CrossRef] [PubMed]
- Maj, A.; Trzcionka, A.; Twardawa, H.; Tanasiewicz, M. A comparative clinical study of the self-adhering flowable composite resin vertise flow and the traditional flowable composite resin premise flowable Coatings 2020, 10, 800.
- Abusamra, E.M.M.; Elsharkawy, M.M.; Mahmoud, E.M.; El Mahy, W.E.M. Clinical evaluation of self-adhering flowable composite in non-carious cervical lesion. Egypt 2016, 62, 757–764. [Google Scholar]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement PLoS Med 2009, 6, e1000097.
- Paolone, G.; Mazzitelli, C.; Josic, U.; Scotti, N.; Gherlone, E.; Cantatore, G.; Breschi, L. Modeling Liquids and Resin-Based Dental Composite Materials-A Scoping Review Materials (Basel) 2022, 15, 3759.
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan — a web and mobile app for systematic reviews Systematic Reviews 2016, 5, 210.
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Cochrane Training 2008. Available online: https://training.cochrane.
- de Oliveira, N.G.; Lima, A.S.L.C.; da Silveira, M.T.; de Souza Araújo, P.R.; Monteiro, G.Q.d.M; de Vasconcelos, M.C. Evaluation of postoperative sensitivity in restorations with self-adhesive resin: a randomized split-mouth design-controlled study Clin Oral Investig 2020, 24, 1829-1835.
- Pinna, R.; Bortone, A.; Sotgiu, G.; Dore, S.; Usai, P.; Milia, E. Clinical evaluation of the efficacy of one self-adhesive composite in dental hypersensitivity Clin Oral Investig 2015, 19, 1663-72.
- Çelik, E.U.; Aka, B.; Yilmaz, F. Six-month Clinical Evaluation of a Self-adhesive Flowable Composite in Noncarious Cervical Lesions J Adhes Dent 2015, 17, 361-8.
- Sabbagh, J.; Dagher, S.; El Osta, N.; Souhaid, P. Randomized Clinical Trial of a Self-Adhering Flowable Composite for Class I Restorations: 2-Year Results. Int J Dent 2017, 2017, 5041529. [Google Scholar]
- AlHumaid, J.; Al Harbi, F.A.; ElEmbaby, A.E. Performance of Self-adhering Flowable Composite in Class V Restorations: 18 Months Clinical Study J Contemp Dent Pract 2018, 19(7), 785-791.
- Shaalan, O.O.; Abou-Auf, E.; El Zoghby, A.F. Clinical evaluation of self-adhering flowable composite versus conventional flowable composite in conservative Class I cavities: Randomized controlled trial J Conserv Dent 2018, 21, 485-490.
- Serin, B.A.; Yazicioglu, I.; Deveci, C.; Dogan, M.C. Clinical evaluation of a self-adhering flowable composite as occlusal restorative material in primary molars: one-year results Eur Oral Res 2019, 53, 119-124.
- Oz, F.D.; Ergin, E.; Cakir, F.Y.; Gurgan, S. Clinical Evaluation of a Self-Adhering Flowable Resin Composite in Minimally Invasive Class I Cavities: 5-year Results of a Double Blind Randomized, Controlled Clinical Trial Acta Stomatol Croat 2020, 54, 10-21.
- Shaalan, O.O.; Abou-Auf, E. A 24-Month Evaluation of Self-Adhering Flowable Composite Compared to Conventional Flowable Composite in Conservative Simple Occlusal Restorations: A Randomized Clinical Trial Contemp Clin Dent 2021, 12, 368-375.
- Brueckner, C.; Schneider, H.; Haak, R. Shear Bond Strength and Tooth-Composite Interaction With Self-Adhering Flowable Composites Oper Dent 2017, 42, 90-100.
- Vertise Flow Instructions for Use Kerr. [(accessed on 06 December 2024)]. Available online: https://www.ultimatedental.com/uploads/KaVoKerr-VertiseFlowIFU.pdf.
- Fusion Liquid Dentin Instructions for Use Pentrol Clinical Technologies. [(accessed on 06 December 2024)]. Available online: https://docplayer.net/167674922-Liquid-dentin-a-fusion-of-composite-adhesive-technology.html.
- Hickel, R.; Roulet, J.F.; Bayne, S.; Heintze, S.D.; Mjör, I.A.; Peters, M.; Rousson, V.; Randall, R.; Schmalz, G.; Tyas, M.; Vanherle, G. Recommendations for conducting controlled clinical studies of dental restorative materials Clin Oral Investig 2007, 11, 5-33.
- Valizadeh, S.; Asiaie, Z.; Kiomarsi, N.; Kharazifard, M.J. Color stability of self-adhering composite resins in different solutions Dent Med Probl 2020, 57, 31-38.
- Marquillier, T.; Doméjean, S.; Le Clerc, J.; Chemla, F.; Gritsch, K.; Maurin, J. C.; Millet, P.; Pérard, M.; Grosgogeat, B.; Dursun, E. The use of FDI criteria in clinical trials on direct dental restorations: A scoping review. J Dent 2018, 68, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Elshinawy, F.M.; Abu, A.E.; Khallaf, Y.S. Evaluation Of Clinical Performance Of Self-Adhering Flowable Composite Vs Conventional Flowable Composite In Cervical Carious Lesions: A Randomized Clinical Trial ADJC 2023, 5, 186-194.
- Arbildo-Vega, H.I.; Lapinska, B.; Panda, S. Clinical Effectiveness of Bulk-Fill and Conventional Resin Composite Restorations: Systematic Review and Meta-Analysis. Polymers (Basel) 2020, 12, 1786. [Google Scholar] [CrossRef] [PubMed]
- Azizi, F.; Ezoji, F.; Khafri, S.; Esmaeili, B. Surface Micro-Hardness and Wear Resistance of a Self-Adhesive Flowable Composite in Comparison to Conventional Flowable Composites Front Dent 2023, 20, 10.
- Veloso, S.R.M.; Lemos, C.A.A.; de Moraes, S.L.D.; Vasconcelos, B.C.d.E.; Pellizzer, E.P.; Monteiro, G.Q.d.M. Clinical performance of bulk-fill and conventional resin composite restorations in posterior teeth: a systematic review and meta-analysis Clin Oral Investig 2019, 23, 221-233.
Figure 1.
Flow diagram of literature search and selection criteria.
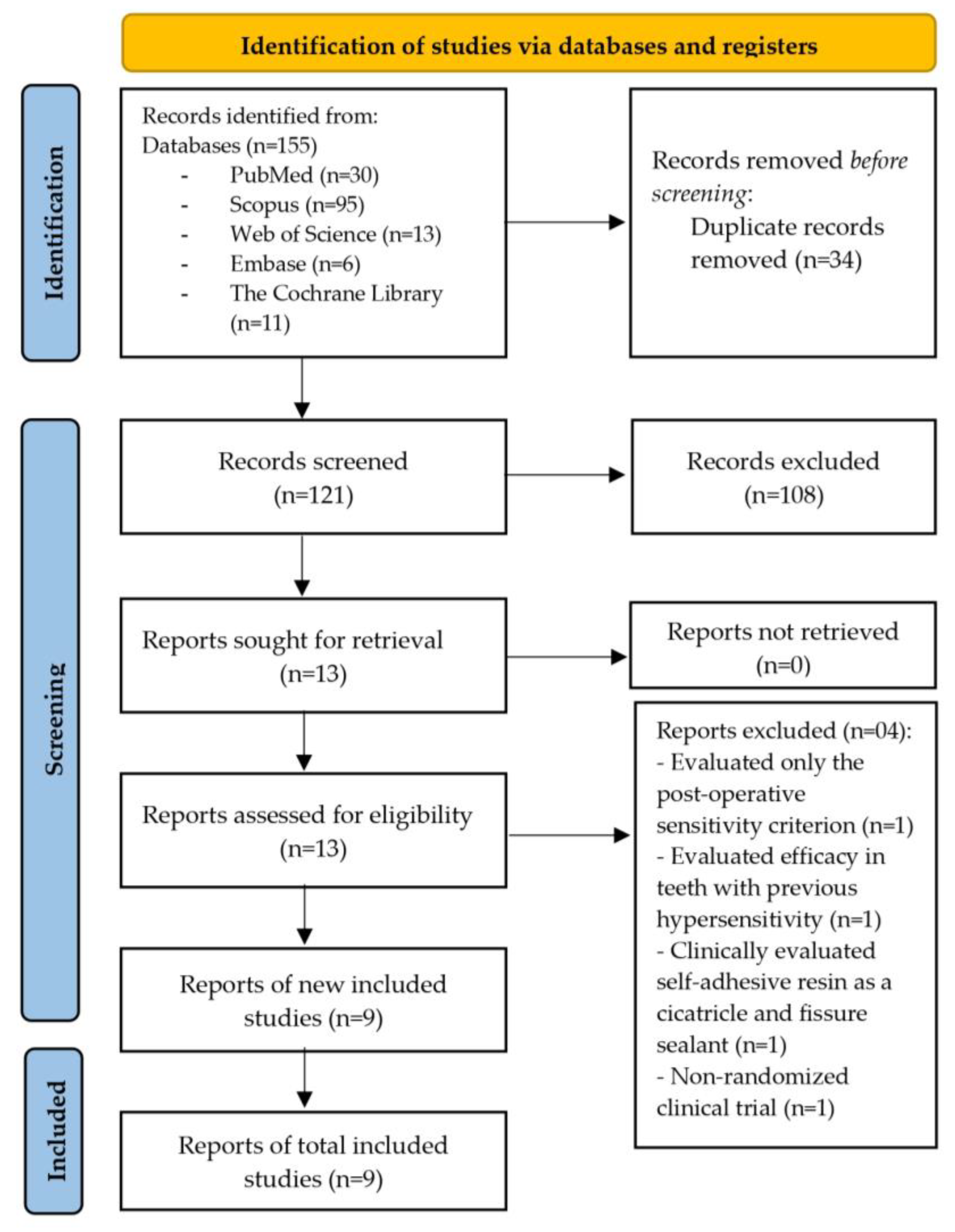
Figure 2.
Bias Risk Analysis for the randomized clinical trials.
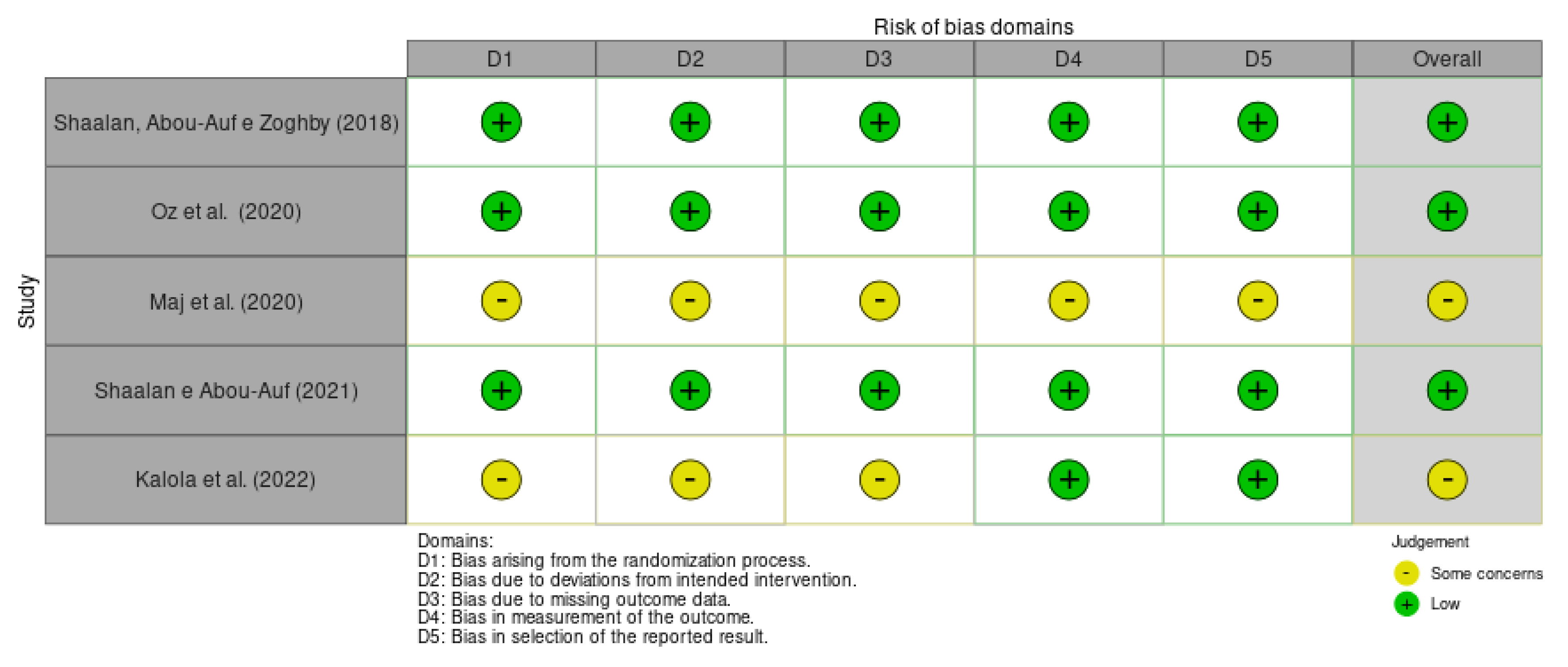
Figure 3.
Forest plot of retention.

Figure 4.
Forest plot of marginal adaptation.

Figure 5.
Forest plot of post-operative sensitivity.

Figure 6.
Forest plot of staining.

Figure 7.
Forest plot of marginal discoloration.

Figure 8.
Forest plot of smoothness.

Figure 9.
Forest plot of dental caries.

Figure 10.
Forest plot of anatomic form.


Table 1.
Search strategy.
| Database | Search strategy |
|---|---|
| PubMed | (Self-Adhesive Composite) OR (Self-Adhering Composite) OR (Self-Adherent Composite) AND (Restorations, Permanent Dental) OR (Restoration, Permanent Dental) OR (Dental Permanent Fillings) OR (Dental Permanent Filling) AND (Flowable hybrid composite) OR (flowable composite) OR (flowline) |
| Embase | ‘Self-Adhesive Composite’ OR ‘Self-Adhering Composite’ OR ‘Self-Adherent Composite’ AND ‘dental restorarion’/exp OR ‘dental restotarion’ OR ‘Restorations, Permanent Dental’ OR ‘Restoration, Permanent Dental’ OR ‘Dental Permanent Fillings’ OR ‘Dental Permanent Filling’ AND ‘Flowable hybrid composite’/exp ‘Flowable hybrid composite’ OR ‘flowable composite’ OR ‘flowline’ |
| Web of Science | TS= ((Self-Adhesive Composite) OR (Self-Adhering Composite) OR (Self-Adherent Composite)) AND TS= ((Restorations, Permanent Dental) OR (Restoration, Permanent Dental) OR (Dental Permanent Fillings) OR (Dental Permanent Filling)) AND TS= ((Flowable hybrid composite) OR (flowable composite) OR (flowline)) |
| The Cochrane Library | (Self-Adhesive Composite OR Self-Adhering Composite OR Self-Adherent Composite) AND (Restorations, Permanent Dental OR Restoration, Permanent Dental OR Dental Permanent Fillings OR Dental Permanent Filling) AND (Flowable hybrid composite OR Flowable composite OR flowline) |
| Scopus | ‘Restorations, AND permanent AND dental’ OR ‘restoration, AND permanent AND dental’ OR ‘dental AND permanent AND fillings’ OR ‘dental AND permanent AND filling' AND ‘self-adhesive AND composite’ OR ‘self-adhering’ AND composite’ OR ‘self-adherent AND composite' AND ‘Flowable hybrid composite’ OR ‘flowable composite’ OR ‘flowline’ |
Table 2.
USPHS criteria.
| The USPHS criteria |
|---|
|
Retention Alpha (A): Restoration is present. Delta (D): Restoration is partially or totally missing. Color match Alpha (A): The restoration matches the adjacent tooth tissue in color, shade, or translucency. Bravo (B): There is a slight mismatch in color, shade, or translucency, but within the normal range of adjacent tooth structure. Charlie (C): There is a slight mismatch in color, shade, or translucency, but outside of the normal range of adjacent tooth structure. |
|
Marginal discoloration Alpha (A): There is discoloration anywhere along the margin between the restoration and the adjacent tooth structure. Bravo (B): Discoloration is present, but has not penetrated along the margin in a pulpal direction. Charlie (C): Discoloration has penetrated along the margin in a pulpal direction. |
|
Recurrent caries Alpha (A): No caries are present at the margin of the restoration, as evidenced by softness, opacity, or etching at the margin. Bravo (B): There is evidence of caries at the margin of the restoration. |
|
Surface roughness Alpha (A): The restoration surface is as smooth as surrounding enamel. Bravo (B): The restoration surface is rougher than the surrounding enamel. Charlie (C): Surface pitting is sufficiently coarse to inhibit the continuous movement of an explorer across the surface. |
|
Marginal integrity Alpha (A): There is no visible evidence of a crevice along the margin into which the explorer penetrates. Bravo (B): There is visible evidence of a crevice along the margin into which the explorer penetrates or catches. Charlie (C): The explorer penetrates the crevice, and dentin or base is exposed. Delta (D): The restoration is mobile, or missing, either in part or total. |
|
Postoperative sensitivity Alpha (A): Normal reaction to cold spray compared with that of no restored teeth. Bravo (B): Increased cold sensitivity. Charlie (C): Spontaneous pain. Delta (D): Nonvital. |
Table 3.
FDI criteria.
| The FDI criteria |
|---|
|
Aesthetic properties
Surface gloss Score 1: Gloss similar to enamel. Score 2: Slightly opaque; Some isolated pores. Score 3: Opaque surface but acceptable if covered by saliva; Multiple pores in more than half of the surface. Score 4: Rough surface, where polishing is not sufficient. Score 5: Very rough surface, unacceptable. Staining Score 1: No superficial or marginal staining. Score 2: Minimal staining, easily removable. Score 3: Moderate staining, also present in other teeth and aesthetically acceptable. Score 4: Unacceptable staining in the restoration, intervention necessary. Score 5: Severe generalized or localized staining, without access for intervention. Color stability or translucency Score 1: Good coloration and translucency compared to neighboring teeth. Score 2: Minimal color and translucency deviation. Score 3: Clear deviation, but without affecting aesthetics. Score 4: Localized clinical deviation that can be corrected by repair. Score 5: Unacceptable, replacement necessary. Anatomic shape Score 1: Ideal shape. Score 2: Shape slightly deviates from normal. Score 3: Shape differs from normal but does not compromise aesthetics. Score 4: Shape is affected and aesthetically unacceptable. Intervention/correction is necessary. Score 5: Unacceptable or lost. Requires replacement. |
|
Functional properties
Fractures and retention Score 1: No fractures or cracks. Score 2: Small crack. Score 3: Cracks that do not affect marginal adaptation. Score 4: Chips that damage marginal adaptation or contact point. Score 5: Partial or total loss of the restoration. Marginal adaptation Score 1: Harmonious line without gaps or discoloration. Score 2: Small marginal fracture removable with polishing. Score 3: Gap less than 150µm, not removable; Several small fractures in enamel and dentin. Score 4: Gap larger than 250 µm or exposed dentin; Chips damage margin; Noticeable fracture in enamel or dentin. Score 5: Large gaps or widespread irregularities. Anatomic shape Score 1: Normal contact point (dental floss or 25 µm metal foil can pass through; Normal contour. Score 2: Slightly too strong contact but without disadvantage (dental floss or 25 µm metal foil can only pass with pressure); Slightly deficient contour. Score 3: Somewhat weak contact, no indication of damage to the tooth, gum, or periodontal structures; 50 µm metal foil can pass; Visibly deficient contour. Score 4: Too weak and possible damage due to food impaction; 100 µm metal foil can pass; Inadequate contour; Repair possible. Score 5: Too weak and/or clear damage due to food impaction and/or pain/gingivitis; Insufficient contour, requires replacement. |
|
Biological properties
Post-operative sensitivity Score 1: No hypersensitivity; normal vitality. Score 2: Low hypersensitivity for a short period of time; normal vitality. Score 3: Moderate hypersensitivity; Weak sensitivity that does not require treatment. Score 4: Intense hypersensitivity; Negative sensitivity; intervention necessary, but no replacement. Score 5: Very intense, pulpitis or non-vital. Endodontics necessary and restoration replacement. Caries recurrence Score 1: No secondary or primary caries. Score 2: Small and localized; Demineralization. Score 3: Larger areas of lesion without dentin exposure. Score 4: Caries with cavitation. Score 5: Deep secondary caries or exposed dentin, not accessible for repair or restoration |
Score 1: Clinically excellent; Score 2: Clinically good; Score 3: Clinically satisfactory; Score 4: Clinically unsatisfactory, but repairable; Score 5: Clinically poor, replacement is necessary.
Table 4.
Qualitative summary of the selected studies.
 |
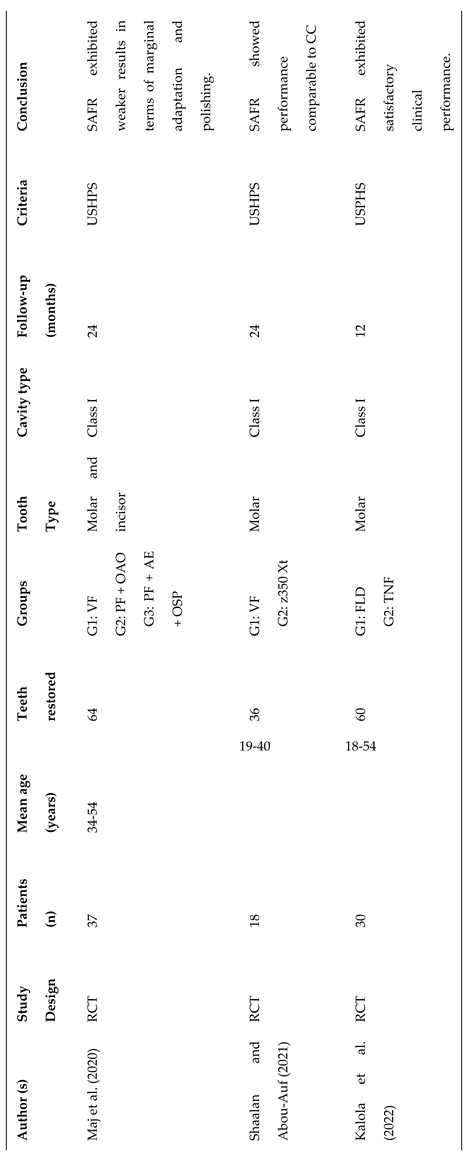 |
RCT: randomized clinical trial; G1: Group 1; G2: Group 2; G3: Group 3; VF: vertise flow; FLD: Fusion Liquid Dentin; TNF; LF: Luxaflow; PF: Premise Flowable; 350: Filtek Z350; 250: Filtek Z250; NCCLs: Non-carious Cervical Lesions; CCLs: Cervical Carious Lesions; * Not mentioned; OAO: Optibond All In One; AE: Acid Etching; OSP: OptiBond Solo Plus; SAFRs: self-adhering composite flow. CC: Conventional Composite; Part 2
Table 5.
USPHS and FDI data extracted from included studies.
| Author, year | Conventional resin composite | Self-Adhering Resin Flowable | ||
| Failure | Total | Failure | Total | |
| Çelik, Aka and Yilmaz (2015) | Marginal adaptation (n=0) Retention (n=0) Post-operative sensibility (n=0) Marginal staining (n=0) Color Match (n=0) Secondary caries (n=0) Anatomical Form (n=0) |
40 40 40 40 40 40 40 |
Marginal adaptation (n=0) Retention (n=27) Post-operative sensibility (n=0) Marginal staining (n=0) Color Match (n=0) Secondary caries (n=0) Anatomical Form (n=0) |
13 40 13 13 10 13 13 |
| Sabbagh et al. (2017) |
* | * | ||
| AlHumaid, Harbi and ElEmbaby (2018) | Marginal adaptation (n=3) Marginal staining (n=1) Color match (n=2) Surface roughness (n=1) |
20 20 20 20 |
Marginal adaptation (n=0) Marginal staining (n=0) Color match (n=0) Surface roughness (n=0) |
20 20 20 20 |
| Shaalan, Abou-Auf and Zoghby (2018) | Marginal adaptation (n=0) Retention (n=0) Post-operative sensibility (n=0) Marginal Staining (n=0) Color Match (n=0) |
18 18 18 18 |
Marginal adaptation (n=0) Retention (n=0) Post-operative sensibility (n=0) Marginal Staining (n=0) Color Match (n=0) |
18 18 18 18 |
| Serin et al. (2019) | Retention (n=0) Post-operative sensibility (n=0) Marginal Staining (n=0) Anatomical form (n=0) |
29 29 29 29 |
Retention (n=0) Post-operative sensibility (n=0) Marginal Staining (n=0) Anatomical form (n=0) |
29 29 29 29 |
| Maj et al. (2020) | Retention (n=0) Marginal Staining (n=0) Color Match (n=0) Proper Smoothness (n=0) Anatomical form (n=0) |
22 22 22 22 22 |
Retention (n=1) Marginal Staining (n=0) Color Match (n=1) Proper Smoothness (n=0) Anatomical form (n=0) |
22 22 22 22 22 |
| Oz et al. (2020) | Marginal adaptation (n=0) Retention (n=1) Post-operative sensibility (n=0) Marginal staining (n=0) Color Match (n=0) Proper Smoothness (n=0) Secondary caries (n=0) |
24 24 24 24 24 24 24 |
Marginal adaptation (n=0) Retention (n=0) Post-operative sensibility (n=0) Marginal staining (n=0) Color Match (n=0) Proper Smoothness (n=0) Secondary caries (n=0) |
22 22 22 22 22 22 22 |
| Shaalan e Abou-Auf (2021) | Marginal adaptation (n=0) Marginal staining (n=0) Color Match (n=0) Proper Smoothness (n=0) Secondary caries (n=0) Anatomical Form (n=0) |
18 18 18 18 18 |
Marginal adaptation (n=0) Marginal staining (n=0) Color Match (n=0) Proper Smoothness (n=0) Secondary caries (n=0) Anatomical Form (n=0) |
18 18 18 18 18 |
| Kalola et al. (2022) | Retention (n=0) Post-operative sensibility (n=0) Marginal staining (n=0) Color Match (n=0) Surface roughness (n=0) Secondary caries (n=0) Anatomical Form (n=0) |
30 30 30 30 30 30 30 |
Retention (n=0) Post-operative sensibility (n=2) Marginal staining (n=0) Color Match (n=0) Surface roughness (n=0) Secondary caries (n=0) Anatomical Form (n=0) |
30 30 30 30 30 30 30 |
*Not mentioned Charlie Score.
Table 6.
GRADE approach.
| Certainty assessment | № of patients | Effect | Certainty | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| № of studies | Study design | Risk of bias | Inconsistency | Indirectness | Imprecision | Other considerations | SARFs | CFR | Relative (95% CI) | Absolute (95% CI) | ||
| Marginal Adaptation (follow-up: range 6 months to 5 years) | ||||||||||||
| 5 | RCT | NSa | NSb | NSc | NSd | VSAe | 0/110 (0.0%) | 0/112 (0.0%) | RR 0.00 (-0.04 to 0.04) | -- per 1.000 (from 0 fewer to 0 fewer) | ⨁⨁⨁⨁ High | |
| Retention (follow-up: range 6 months to 5 years) | ||||||||||||
| 3 | RCT | NSe | NSb | NSc | NSd | VSAe | 0/70 (0.0%) | 1/72 (1.4%) | RR -0.01 (-0.06 to 0.04) | 14 fewer per 1.000 (from 15 fewer to 13 fewer) | ⨁⨁⨁⨁ High | |
| Post-operative sensibility (follow-up: range 6 months to 5 years) | ||||||||||||
| 3 | RCT | NSe | NSb | NSc | NSd | VSAe | 0/70 (0.0%) | 0/72 (0.0%) | RR 0.00 (-0.04 to 0.04) | -- per 1.000 (from 0 fewer to 0 fewer) | ⨁⨁⨁⨁ High | |
| Color match (follow-up: range 1 years to 5 years) | ||||||||||||
| 5 | RCT | NSa | NSb | NSc | NSd | VSAe | 1/110 (0.9%) | 0/112 (0.0%) | RR 0.00 (-0.03 to 0.04) | -- per 1.000 (from 0 fewer to 0 fewer) | ⨁⨁⨁⨁ High | |
| Marginal descoloration (follow-up: range 6 months to 5 years) | ||||||||||||
| 5 | RCT | NS | NS | NS | NS | VSAe | 0/110 (0.0%) | 0/112 (0.0%) | RR 0.00 (-0.04 to 0.04) | -- per 1.000 (from 0 fewer to 0 fewer) | ⨁⨁⨁⨁ High | |
| Anatomic Form (follow-up: range 1 years to 2 years) | ||||||||||||
| 3 | RCT | NS | NS | NS | NS | VSAe | 0/70 (0.0%) | 0/70 (0.0%) | RR 0.00 (-0.05 to 0.05) | -- per 1.000 (from 0 fewer to 0 fewer) | ⨁⨁⨁⨁ High | |
| Secondary caries (follow-up: range 1 years to 2 years) | ||||||||||||
| 3 | RCT | NS | NS | NS | NS | VSAe | 0/70 (0.0%) | 0/72 (0.0%) | RR 0.00 (-0.04 to 0.04) | -- per 1.000 (from 0 fewer to 0 fewer) | ⨁⨁⨁⨁ High | |
| Smoothness (follow-up: range 1 years to 2 years) | ||||||||||||
| 3 | RCT | NS | NS | NS | NS | VSAe | 0/62 (0.0%) | 0/63 (0.0%) | RR 0.00 (-0.05 to 0.05) | -- per 1.000 (from 0 fewer to 0 fewer) | ⨁⨁⨁⨁ High | |
Legend: CI- confidence interval; RR- risk ratio; RCT – randomized clinical trials; NS – Not serious; VSA- Very strong association; SARFs – Self Adhering Resin Flowable; CFR – conventional flowable resin. Explanations: a. All included studies presented low risk of bias and just two study some concerns for incomplete data on the allocation method, incomplete data on blinding of participants and staff and incomplete data about loss of follow-up; b. All included studies presented heterogeneity under <50%; c. Indirectness judge based on population, intervention, comparison, and outcome across studies; d. All included studies presented low CI; e. All studies presented RR<0,02.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



