Submitted:
06 July 2025
Posted:
07 July 2025
You are already at the latest version
Abstract
Background/Objectives: Cancer represents a significant health challenge, with high mortality and morbidity rates. Such a diagnosis often triggers chronic stress, adversely affecting patient outcomes. Exercise has emerged as a complementary therapy, enhancing treatment adherence and mitigating the side effects of chemotherapy. This study examines the effects of mild exercise during chemotherapy on patient anxiety levels. Methods: This prospective paired cohort study was conducted at the General Oncology Hospital of Kifisia "Agioi Anargyroi" in Athens, Greece. Adult cancer patients undergoing chemotherapy participated, excluding those with cognitive, hearing, or motor impairments, side effects, or who declined consent. Anxiety was measured before and after a 20-minute exercise routine performed during chemotherapy, using the Greek-translated State-Trait Anxiety Inventory (STAI). The exercise regimen included warm-up, full-body stretching, and cool-down exercises. Pre- and post-exercise scores were analyzed using the Wilcoxon signed-rank test. Results: Forty-five patients (20 women, 25 men; mean age 69.02 ± 10.62 years) with various cancers participated. Pre-intervention anxiety levels were in the borderline "moderate" range, dropping post-exercise to the "low" range. Mean STAI scores decreased from 37.73 ± 13.33 to 32.00 ± 14.22 (p < 0.0001), with a medium-large effect size (Cohen's d for paired samples = -0.646). No significant correlation was found between age and anxiety scores. Conclusions: This study found a significant short-term reduction in anxiety, suggesting that incorporating mild exercise during chemotherapy may help alleviate patient stress. The medium-to-large effect size supports the potential for meaningful short-term benefits. These findings underscore the need for more comprehensive research in larger, more diverse populations to better understand the benefits of incorporating mild exercise into chemotherapy
Keywords:
exercise therapies
; chemotherapy
; anxiety
1. Introduction
In developed countries, it is estimated that approximately 20% of the population will receive a cancer diagnosis at some point in their lives [1]. The most prevalent types of cancer include breast cancer, prostate cancer, lung cancer, and colorectal cancers (2). Advancements in early diagnosis and treatment modalities have led to a significant improvement in survival rates, with some studies indicating an increase of up to 70%, thereby reclassifying cancer as a chronic disease in numerous cases [3,4]. Nonetheless, throughout the course of the disease and its associated treatment, patients frequently experience a range of physical symptoms—including pain, nausea, vomiting, motor disabilities—as well as emotional distress, all of which can profoundly impact their overall quality of life [QoL] [1,4].
A significant life event can elevate the risk of psychological distress and anxiety [5,6]. Anxiety is a normal, potentially adaptive reaction in situations perceived as threatening, but becomes pathological when it is persistent and its severity or duration exceed normal expectations [7,8]. A cancer diagnosis, due to its inherently threatening nature, understandably elicits considerable anxiety among patients who must confront this existential threat. However, this anxiety may escalate into a clinically significant condition requiring therapeutic intervention. Anxiety has been recognized as a critical factor influencing QOL among cancer patients [7]. Furthermore, elevated levels of anxiety may exacerbate the side effects associated with chemotherapy, thereby further compromising QOL.
Risk factors for anxiety in cancer populations include several clinical and psychosocial variables, with chemotherapy emerging as a particularly prominent contributor [9]. Advanced disease stage and prolonged illness duration are associated with increased anxiety. Other identified risk factors include unemployment, younger age, and a higher prevalence of physical symptoms. Impairments in social and cognitive functioning, alongside insecure attachment styles, may further elevate anxiety. Moreover, poor communication with healthcare providers can intensify feelings of uncertainty and fear, contributing to increased anxiety [10]. A thorough understanding of these risk factors, - especially those related to chemotherapy - is crucial for the development of targeted interventions aimed at supporting patients throughout their cancer care journey.
Exercise is a valuable adjunct therapy for cancer patients, as it has demonstrated the ability to mitigate many side effects and symptoms associated with both the disease and its treatment [11]. Research indicates that exercise significantly reduces cancer-related fatigue and psychosocial distress; it also enhances aerobic fitness, improves body composition and strength, and positively impacts various aspects of physical function as well as health-related QOL [12,13,14,15,16]. Moreover, regular physical activity may enhance relative dose intensity [RDI] by reducing chemotherapy-related toxicities, aiding recovery and overall health [17].
Current evidence regarding the benefits of exercise for cancer patients primarily focuses on exercise interventions conducted either during active treatment— excluding chemotherapy or radiotherapy—or after the completion of treatment. However, recent discussions have emphasized the potential value of engaging in physical exercise concurrently with chemotherapy infusions as a promising approach [18,19]. The aim of this prospective cohort study is to investigate the effects of mild exercise and stretching during chemotherapy on patients’ anxiety levels.
2. Materials and Methods
This prospective observational cohort study has received ethical approval from the Ethics Committee of the General Oncology Hospital of Kifissia “Agioi Anargyroi” in Athens, Greece [protocol number 779/15-1-2024]. The study was registered on ClinicalTrials.gov [Registration Number: NCT06943638].
The study population consisted of adult cancer patients aged ≥ 18 years undergoing chemotherapy. Prior to enrollment in the study, all participants provided informed consent after receiving a detailed printed guide outlining the nature of the intervention and their rights as research subjects. Patients were excluded if they declined participation, had cognitive or hearing impairments that could hinder their ability to participate, or if they were unable to mobilize independently.
Intervention
The intervention was systematically designed and implemented by a licensed physiotherapist. Each session lasted 20 minutes and included mild exercises and a stretching routine tailored to meet the individual capabilities of each participant, conducted in person. The exercise plan was developed and tailored with careful consideration of hospital constraints and the specific medical conditions of each patient.
The exercise plan is shown in Figure 1, Figure 2, Figure 3 and Figure 4 and the full program is explained in detail in Table 1.
We used the Spielberger State-Trait Anxiety Inventory [STAI], which is a psychological inventory consisting of 40 self-report items on a 4-point Likert scale [20]. The STAI measures two types of anxiety – state anxiety [STAI-Y1] and trait anxiety [STAI-Y2]. For the purposes of this study, the STAI-State scale [Form Y-1] was employed, which specifically measures the levels of anxiety experienced at a given moment, referred to as “state anxiety”. This contrasts with “trait anxiety,” which reflects an individual’s general tendency to experience anxiety as a personality characteristic. We utilized the Greek-translated version of the STAI, validated by Liakos and Giannitsis in 1984 [21].
The Y-1 form consists of 20 statements. For each statement, the subject must choose one of the 4 alternatives to indicate how they feel: absolutely not, a little, enough, and very much. The scoring for the Y-1 form of STAI-State scale ranges from 20 to 80, with higher scores indicating greater anxiety levels. Participants completed the STAI questionnaire both prior [baseline] and following the exercise program. Each participant served as their own control, allowing for a rigorous assessment of anxiety levels before and after the intervention. This design facilitates a thorough evaluation of the intervention’s effectiveness in alleviating anxiety within the study population.
Statistical Analysis
Sample size calculations, based on similar studies [19] determined a minimum of 45 participants to achieve adequate power [α = 0.01, β = 80%]. Due to the non-normal data distribution and paired nature of the measurements, the Wilcoxon signed-rank test was employed. Data differences Δ[After-Before] were normally distributed, and thus Cohen’s D for paired samples was used to determine effect size. Spearman’s rho was used to investigate possible correlations between gender, age, and the STAI scores, as well as their difference Δ[After-Before].
3. Results
The study included 45 patients [20 women, 25 men] aged 53–85 years [mean ± SD: 69.02 ± 10.62] with various cancer types [e.g., hematological malignancies, ovarian cancer]. Patients’ recruitment is presented in Figure 5 as a flowchart. Of the 211 patients initially invited to participate, 165 chose to decline due to concerns regarding potential injury or fatigue.
The most pronounced improvement was observed in an 83-year-old woman, whose anxiety score decreased by 25 points [from 46 to 21]. Conversely, some patients, such as a 61-year-old woman with high initial anxiety, reported an increase [from 64 to 79]. The mean anxiety score decreased significantly from 37.73 ± 13.33 to 32.00 ± 14.22, with a p-value < 0.0001. Cohen’s D for paired samples, was calculated to be d= -0.646, indicating a medium-large effect size. Anxiety scores before and after the intervention are summarized in Figure 6.
Spearman’s rho did not reveal any significant correlations between age, gender, and the STAI scale values. The only significant correlation was a strong positive correlation between the before and after values [rho= 0.738, P<0.001, 95% Confidence Interval [CI]: 0.5610-0.8502]. All other Spearman’s rho data, had large confidence intervals and do not permit definitive conclusions about the strength of the observed relationships. Spearman’s rho correlation analysis is summarized in Figure 7.
4. Discussion
This study demonstrated that a short program of mild exercise in cancer patients while receiving chemotherapy led to a reduction in state anxiety levels. Chemotherapy is an intense and cyclical treatment that, unlike surgery, has many side effects, including hair loss, nausea, vomiting, and diarrhea. Prolonged treatment periods, repeated hospitalizations, and the side effects of chemotherapy, along with the awareness of having cancer, can significantly impact the psychological well-being of patients [22]. It has been reported that physical and cognitive impairments through side effects of cancer treatment can significantly contribute to greater fear of cancer progression [23]. Furthermore, chemotherapy-induced fatigue and physical symptoms may remind patients of their cancer or be misinterpreted as signs of its possible relapse, leading to increased fears of recurrence [24]. In this context it seems reasonable that many studies report that coping with the effects of chemotherapy can be stressful, frustrating, and traumatic. Consequently, patients undergoing chemotherapy are at a higher risk of experiencing psychological and emotional difficulties, such as sleep problems, depression, and anxiety [22,23,24,25,26]. Among negative emotions, anxiety is the most experienced issue in cancer patients [22,26]; it is not just a normal reaction to a cancer diagnosis, but can also arise from treatment, fear of recurrence, or even after completing treatment due to fear of recurrence. It can manifest in four ways: situational anxiety, disease-related anxiety, treatment-related anxiety, and an exacerbation of pre-existing anxiety disorders [22].
Exercise has emerged as a promising supportive care strategy that can alleviate some of these adverse effects [27]. Many studies have shown that exercise may improve mood, enhance treatment tolerance and support immune system [28,29,30]. Furthermore, research consistently demonstrates that exercise can be highly effective in alleviating both acute and chronic side effects of cancer and chemotherapy [31]. The primary outcomes examined in these studies include cancer-related fatigue, depression, anxiety, sleep disturbances, cognitive function, self-esteem, nausea, cardiopulmonary function, muscular strength, flexibility, and body composition [32,33,34]. Despite these benefits, adherence to exercise guidelines among cancer patients remains low, largely due to treatment side effects, lack of guidance, and patient misconceptions [35]. A lack of information regarding exercise during treatment may cause patients to feel unsure about what they are allowed and able to do [35].
Exercise as an effective nonpharmacological therapy in cancer patients includes both aerobic and resistance training. Aerobic exercise is characterized by low intensity enabling prolonged periods of activity. It engages large muscle groups and is rhythmic in nature. Common forms of aerobic exercise include walking, running, cycling, and swimming. Resistance training regimens target improvements in muscle hypertrophy, bone mineral density, strength, functional mobility, and body composition [34].
However, before recommending exercise as non-pharmacological therapy in cancer patients, its feasibility and safety must be carefully considered. Thomas et al. investigated the safety of exercise during chemotherapy in a randomized crossover trial [36]. The study involved 10 adults aged 18 to 60 who were receiving non-vesicant chemotherapy agents. Participants engaged in 20 minutes of supervised low intensity cycling, during which no adverse events or treatment interferences were reported. Participants in the exercise group experienced significantly reduced boredom; however, there were no significant differences observed in other symptom experiences following the intervention. In a meta-analysis of 19 studies assessing the safety, feasibility, and effects of exercise in individuals with colorectal cancer, the authors concluded there was no difference in the risk of adverse events between the exercise intervention group and usual care [37].
Given that cancer patients often face a significant burden of symptoms and are frequently considered frail, it is reasonable to question whether all cancer patients are eligible to engage in exercise during chemotherapy and throughout the active phase of their illness. However, a recent review of physical activity recommendations for cancer patients indicates that the majority of assessed guidelines—eight out of eleven—support engaging in physical activity for the entire oncological population, across all stages of cancer treatment, both during and after therapy [38].
A related and equally important consideration involves the type and dosage of exercise recommended for cancer patients. Regarding the types of activities recommended, all guidelines advocate for a combination of aerobics and resistance training. Most guidelines suggested an average physical activity dosage of 150 minutes per week of moderate-intensity aerobic training [or 75 minutes of vigorous-intensity activity, which is considered equivalent] along with resistance training twice per week. However, detailed guidance regarding session duration, intensity measurement, and progression is often limited across all guidelines. Three recommendations, provided more comprehensive instructions, suggesting at least 3 sessions per week of aerobic training lasting 20–30 minutes, at moderate intensity, as well as 6–10 sets of resistance exercise performed at least 1–3 times per week with 1–4 sets of 8–15 repetitions at moderate intensity [at least 50–60 % of the one-maximal repetitions] [37,39,40].
The appropriate prescription of exercise for individuals living with and beyond cancer has yet to be clearly established, as there is still no consensus within the scientific community. Although the recently published exercise guidelines from the American College of Sports Medicine (ACSM) suggest that it is possible to tailor specific exercise prescriptions—such as frequency, intensity, time, and type of exercise—to improve various cancer-related health outcomes, the American Society of Clinical Oncology argues that current evidence is insufficient to provide specific exercise dosage recommendations [41].
This discrepancy in guidance likely contributes to the fact that many patients undergoing chemotherapy do not receive adequate information or individualized advice regarding exercise. Furthermore, most existing studies have focused on incorporating exercise protocols that patients can perform at home, either during or after the completion of chemotherapy regimens. Few studies have examined the feasibility of implementing exercise for patients with cancer directly within the chemotherapy infusion setting, under the supervision of a trained professional. Kerrigan et al. conducted a pilot study demonstrating that aerobic exercise during chemotherapy infusions is both safe and well tolerated [42]. In this study, ten breast cancer patients participating in the ExCITE [Exercise and Cancer Integrative Therapy and Education Program] trial at Henry Ford Hospital performed mild aerobic exercise on a portable leg ergometry machine [Monarck] while receiving chemotherapy. This activity was supplemented by a prescribed outpatient exercise program. During the infusion and simultaneous exercise, the patients’ heart rates were maintained at approximately 30-40% of heart rate reserve and all sessions were supervised by a clinical exercise physiologist. Across 55 chemotherapy infusions of those 10 patients, 18 sessions included exercise, while 37 did not, and no adverse events were reported.
The Exercise in All Chemotherapy trial further explored this model by embedding an exercise professional directly into the chemotherapy infusion suite as a method of making exercise a standard part of cancer care [18]. The exercise regimens provided to patients were individualized based on the results of brief baseline functional testing. This study concluded that this approach is both acceptable and feasible from the perspective of clinicians and patients, indicating strong potential for integration into routine oncology care. The same conclusion was supported by Schmitz et al., who provided a comprehensive analysis of the ENACT trial, demonstrating that exercise during chemotherapy is both feasible and beneficial [18]. In their study, patients received detailed exercise prescriptions—including frequency, intensity, and duration—and were encouraged to perform independently at home, between chemotherapy visits.
In our study, we observed that a 20-minute program of gentle exercise and stretching conducted during chemotherapy sessions, tailored to each patients’ physical status, had a positive impact on state anxiety levels. The clinical significance of this finding is very important, as high levels of anxiety can trigger physiological responses mediated by the autonomic nervous system, resulting in increased pain perception, nausea, and vomiting - factors that can subsequently further intensify distress. Moreover, anxiety can induce a state of behavioral paralysis and thus hinder the patient’s ability to cope with chemotherapy-related side effects [25]. As a result, anxiety may adversely affect compliance with treatment protocols [43].
A review of international studies revealed that clinically diagnosed anxiety disorders and anxiety symptoms were associated with increased cancer-specific mortality as well as poorer overall survival [44]. Anxiety and distress are both negative emotional states, but they differ in their nature and intensity. Anxiety is a characterized by an excessive sense of tension, worry or apprehension, relative to potential future threats [45]. In contrast, distress is a broader term that encompasses various unpleasant or uncomfortable emotional states, which can include anxiety, depression, and other negative feelings [46]. In this context, anxiety can be viewed as a specific manifestation of psychological distress.
Cancer-related distress is defined as “an unpleasant experience of psychological [cognitive, behavioral, emotional], physical, social, and/or spiritual nature that may interfere with the ability to cope effectively with cancer, its physical symptoms, and its treatment” [47]. This distress is multifactorial in cancer patients and often begins at the time of diagnosis. It tends to intensify over the course of the disease due to both the burden of cancer-related symptoms and toxicity associated with therapy [48].
The management of patients with cancer not only aims to achieve remission and enhance survival rates but also places significant emphasis on reducing psychological distress and enhancing patients’ QOL. This dual approach is essential, as an improved QOL fosters greater adherence to treatment protocols, encourages patients to complete therapy, and facilitates in the effective management of symptoms [49].
In our study, we used the Spielberger State-Trait Anxiety Inventory [STAI] to assess anxiety levels, specifically focusing on the STAI-Y1 scale, which measures state anxiety. While both state and trait anxiety are important concepts, they serve different purposes in understanding and addressing anxiety. State anxiety reflects a temporary emotional condition triggered by specific situations or stressors [50], making it particularly useful for evaluating patients’ immediate psychological responses to cancer treatment [45]. It reflects a transient condition rather than a pathological state, and it can fluctuate rapidly depending on the situation and the individual’s coping capacity.
In contrast, trait anxiety represents a stable predisposition to experience anxiety across a range of situations and is more relevant for understanding long-term emotional patterns and their influence on overall well-being. Trait anxiety is considered a more stable aspect of personality, as it is considered to be part of a broader spectrum of personality traits, and has been linked to various psychological conditions [50]. It represents a consistent individual tendency of a person to respond with worry, concern, and apprehension to various situations. Trait anxiety helps us understand individual variability in susceptibility to anxiety disorders and predict how individuals might react to stressful situations. It is relatively stable over time and across different situations. Individuals with higher trait anxiety often experience higher levels of state anxiety in response to stressors. While the two concepts are interrelated, some research suggests that trait and state anxiety may have partially distinct brain mapping [45]. This supports the value of assessing both to gain a comprehensive understanding of anxiety.
In our study, we chose to use only the STAI-Y1 [state anxiety] section of Spielberger’s State-Trait Anxiety Inventory to measure changes in state anxiety levels. This decision was based on the specific focus of our intervention: the acute anxiety experienced during chemotherapy sessions, often driven by fear of side effects and psychological distress. Additionally, limiting the time required to assess the STAI-Y1 helped reduce participant burden and limit dropout, as the shorter format required less time to complete. The significant number of patients that refused to participate in a short program of gentle physical activity strains out the fact that (a) patients should be informed of current recommendations regarding exercise and (b) it should be explained to them that exercise is a vital and feasible component in the management of their health-related quality of life [35].
Limitations
This study presents several limitations that should be acknowledged. First, the sample size was relatively small [n=45]. While it met the minimum threshold for statistical power, the limited number of participants may affect the generalizability of the findings. Second, the study population was drawn exclusively from a single hospital located in the northern region of Athens, specifically from its Day Care Unit, which may introduce selection bias and limit the applicability of the findings to broader cancer populations. Third, the intervention consisted only of a single 20-minute session, and the absence of a follow-up period restricts our ability to assess the sustained or long-term effects of the intervention on anxiety levels. Additionally, the inclusion of patients with different cancer types and treatment stages, without stratified analysis, introduces heterogeneity that may have impacted the consistency and interpretability of the findings.
From a methodological standpoint, the absence of a control group limits our ability to attribute changes in anxiety solely to the intervention, as other contextual factors may have influenced outcomes. The reliance on self-reported anxiety level introduces potential bias, including the tendency for participants to provide responses they perceive as socially acceptable or desirable.
Lastly, a significant number of eligible patients declined participation—often due to concerns about fatigue or injury—raising the possibility of selection bias, as those who participated may have been more physically or psychologically predisposed to engage in the program. It is also important to note that in Greece patients undergoing chemotherapy are not typically offered exercise as part of their care and may be unaware of its feasibility and safety. This unfamiliarity likely contributed to the reluctance of many patients to consent to participation in the study.
5. Conclusions
This study investigated the effects of mild exercise during chemotherapy sessions on patients’ state anxiety levels. The findings indicate that brief, patient-tailored exercise can lead to a short-term reduction in anxiety. These results suggest that incorporating mild exercise during chemotherapy may help alleviate anxiety and psychological burden. Further studies are warranted to determine the optimal type, intensity and duration of exercise across different types of cancer patients.
Author Contributions
Conceptualization, V.N.; methodology, C.M., V.N., G.S. and G.P.; formal analysis, G.P.; investigation, C.M. and A.K.; data curation, C.M. and A.K.; writing—original draft preparation, C.M., V.N., G.P., P.V., E.K., G.S.; writing—review and editing, G.S., A.P., V.N.; supervision, V.N.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the General Oncology Hospital of Kifissia “Agioi Anargyroi” in Athens, Greece (protocol code 779/15-1-2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available upon request from the first author.
Acknowledgments
Not Applicable
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| QoL | Quality of Life |
| STAI | State-Trait Anxiety Inventory |
| CI | Confidence Interval |
| ACSM | American College of Sports Medicine |
| ExCITE | Exercise and Cancer Integrative Therapy and Education Program |
References
- ‘Wang Y, Feng W. Cancer-related psychosocial challenges. Gen Psychiatr. 2022 Oct 6;35(5):e100871. PMID: 36311374; PMCID: PMC9540834.’. [CrossRef]
- ‘Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011;61:69–90.’.
- ‘Mayer RS, Engle J. Rehabilitation of ndividuals With Cancer. Ann Rehabil Med. 2022 Apr;46(2):60-70.’.
- ‘Brown M, Farquhar-Smith P. Pain in cancer survivors; filling in the gaps. Br J Anaesth. 2017 Oct 1;119(4):723-736.’. [CrossRef]
- ‘Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global Cancer Statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2021; 71:209-49.’. [CrossRef]
- ‘Hassanzadeh A, Heidari Z, Feizi A, Hassanzadeh Keshteli A, Roohafza H, Afshar H, Adibi P. Association of Stressful Life Events with Psychological Problems: A Large-Scale Community-Based Study Using Grouped Outcomes Latent Factor Regression with Latent Predictors. Comput Math Methods Med. 2017;2017:3457103. Epub 2017 Sep 19. Erratum in: Comput Math Methods Med. 2018 Feb 20;2018:8020962. doi: 10.1155/2018/8020962. PMID: 29312459; PMCID: PMC5625761. [CrossRef] [PubMed]
- ‘Grassi L, Caruso R, Riba MB, Lloyd-Williams M, Kissane D, Rodin G, McFarland D, Campos-Ródenas R, Zachariae R, Santini D, Ripamonti CI; ESMO Guidelines Committee. Electronic address: clinicalguidelines@esmo.org. Anxiety and depression in adult cancer patients: ESMO Clinical Practice Guideline. ESMO Open. 2023 Apr;8(2):101155. Epub 2023 Mar 14. PMID: 37087199; PMCID: PMC10163167.’. [CrossRef] [PubMed]
- Stark, D., House, A. Anxiety in cancer patients. Br J Cancer ,2000;83: 1261–1267’.
- ‘Mitchell AJ, Ferguson DW, Gill J, Paul J, Symonds P. Depression and anxiety in long-term cancer survivors compared with spouses and healthy controls: a systematic review and meta-analysis. Lancet Oncol. 2013 Jul;14(8):721-32. Epub 2013 Jun 5. PMID: 23759376. ’. [CrossRef]
- ‘Choudhury, A. Impact of Social Isolation, Physician-Patient Communication, and Self-perception on the Mental Health of Patients With Cancer and Cancer Survivors: National Survey Analysis. Interact J Med Res. 2023 Apr 7;12:e45382.’. [CrossRef]
- ‘Schmitz KH, Courneya KS, Matthews C, Demark-Wahnefried W, Galvão DA, Pinto BM, Irwin ML, Wolin KY, Segal RJ, Lucia A, Schneider CM, von Gruenigen VE, Schwartz AL; American College of Sports Medicine. American College of Sports Medicine roundtable on exercise guidelines for cancer survivors. Med Sci Sports Exerc. 2010 Jul;42(7):1409-26’. [CrossRef]
- ‘Mishra SI, Scherer RW, Snyder C, Geigle PM, Berlanstein DR, Topaloglu O. Exercise interventions on health-related quality of life for people with cancer during active treatment. Cochrane Database Syst Rev. 2012 Aug 15;2012(8):CD008465. PMID: 22895974; PMCID: PMC7389071.’. [CrossRef]
- ‘Meneses-Echávez JF, González-Jiménez E, Ramírez-Vélez R. Effects of Supervised Multimodal Exercise Interventions on Cancer-Related Fatigue: Systematic Review and Meta-Analysis of Randomized Controlled Trials. Biomed Res Int. 2015;2015:328636. Epub 2015 Jun 17. PMID: 26167483; PMCID: PMC4488083.’. [CrossRef]
- ‘Cormie P, Zopf EM, Zhang X, Schmitz KH. The Impact of Exercise on Cancer Mortality,Recurrence, and Treatment-Related Adverse Effects. Epidemiol Rev. 2017 Jan 1;39(1):71-92. PMID: 28453622.’. [CrossRef]
- ‘Gerritsen JK, Vincent AJ. Exercise improves quality of life in patients with cancer: a systematic review and meta-analysis of randomised controlled trials. Br J Sports Med. 2016 Jul;50(13):796-803. Epub 2015 Dec 30. PMID:26719503.’. [CrossRef]
- ‘Buffart LM, Kalter J, Sweegers MG, Courneya KS, Newton RU, Aaronson NK, Jacobsen PB, May AM, Galvão DA, Chinapaw MJ, Steindorf K, Irwin ML, Stuiver MM, Hayes S, Griffith KA, Lucia A, Mesters I, van Weert E, Knoop H, Goedendorp MM, Mutrie N, Daley AJ, McConnachie A, Bohus M, Thorsen L, Schulz KH, Short CE, James EL, Plotnikoff RC, Arbane G, Schmidt ME, Potthoff K, van Beurden M, Oldenburg HS, Sonke GS, van Harten WH, Garrod R, Schmitz KH, Winters-Stone KM, Velthuis MJ, Taaffe DR, van Mechelen W, Kersten MJ, Nollet F, Wenzel J, Wiskemann J, Verdonck-de Leeuw IM, Brug J. Effects and moderators of exercise on quality of life and physical function in patients with cancer: An individual patient data meta-analysis of 34 RCTs. Cancer Treat Rev. 2017 Jan;52:91-104.’. [CrossRef]
- ‘Grassi L, Caruso R, Riba MB, Lloyd-Williams M, Kissane D, Rodin G, McFarland D,Campos-Ródenas R, Zachariae R, Santini D, Ripamonti CI; ESMO Guidelines Committee. Electronic address: clinicalguidelines@esmo.org. Anxiety and depression in adult cancer patients: ESMO Clinical Practice Guideline. ESMO Open. 2023 Apr;8(2):101155.’. [CrossRef]
- ‘Schmitz KH, Potiaumpai M, Schleicher EA, Wolf LJ, Doerksen SE, Drabick JJ, Yee NS, Truica CI, Mohamed AA, Shaw BW, Farley DC. The exercise in all chemotherapy trial. Cancer. 2021 May 1;127(9):1507-1516. Epub 2020 Dec 17. PMID: 33332587.’. [CrossRef]
- ‘Moraes RF, Ferreira-Júnior JB, Marques VA, Vieira A, Lira CAB, Campos MH, Freitas-Junior R, Rahal RMS, Gentil P, Vieira CA. Resistance Training, Fatigue, Quality of Life,Anxiety in Breast Cancer Survivors. J Strength Cond Res. 2021 May 1;35(5):1350-1356.’.
- ‘Balsamo M, Cataldi F, Carlucci L, Fairfield B. Assessment of anxiety in older adults: a review of self-report measures. Clin Interv Aging. 2018 Apr 6;13:573-593. PMID: 29670342; PMCID: PMC5896683.’. [CrossRef]
- ‘Liakos, A., & Giannitsi, S. (1984). The Reliability and Validity of the Greek Version of Spielberger’s, State and Trait Anxiety Inventory. Encephalos, 21, 71-76.’.
- ‘Pandey, M., Sarita, G.P., Devi, N. et al. Distress, anxiety, and depression in cancer patients undergoing chemotherapy. World J Surg Onc 4, 68 (2006).’. [CrossRef]
- J. Dietrich, M. Prust, and J. Kaiser, ‘Chemotherapy, cognitive impairment and hippocampal toxicity’, Hippocampal Vulnerability Mol. Dis., vol. 309, pp. 224–232, Nov. 2015. [CrossRef]
- ‘Yang Y, Wen Y, Bedi C, Humphris G. The relationship between cancer patient’s fear of recurrence and chemotherapy: A systematic review and meta-analysis. J Psychosom Res. 2017 Jul;98:55-63. Epub 2017 May 3. PMID: 28554373.’. [CrossRef]
- ‘Mahdizadeh MJ, Tirgari B, Abadi O, Bahaadinbeigy K (2019) Guided imagery: reducing anxiety, depression, and selected side effects associated with chemotherapy. Clin J Oncol Nurs 23(5):87–92’.
- ‘Pitman A, Suleman S, Hyde N, Hodgkiss A. Depression and anxiety in patients with cancer. BMJ. 2018 Apr 25;361:k1415. PMID: 29695476.’. [CrossRef]
- ‘V. Bucciarelli, F. Bianco, A. Di Blasio, et al., “Cardiometabolic Profile, Physical Activity, and Quality of Life in Breast Cancer Survivors After Different Physical Exercise Protocols: A 34-Month Follow-Up Study,” Journal of Clinical Medicine 12, no. 14 (July 2023): 4795.’. [CrossRef]
- ‘Buffart LM, Kalter J, Sweegers MG, Courneya KS, Newton RU, Aaronson NK, Jacobsen PB, May AM, Galvão DA, Chinapaw MJ, Steindorf K, Irwin ML, Stuiver MM, Hayes S, Griffith KA, Lucia A, Mesters I, van Weert E, Knoop H, Goedendorp MM, Mutrie N, Daley AJ, McConnachie A, Bohus M, Thorsen L, Schulz KH, Short CE, James EL, Plotnikoff RC, Arbane G, Schmidt ME, Potthoff K, van Beurden M, Oldenburg HS, Sonke GS, van Harten WH, Garrod R, Schmitz KH, Winters-Stone KM, Velthuis MJ, Taaffe DR, van Mechelen W, Kersten MJ, Nollet F, Wenzel J, Wiskemann J, Verdonck-de Leeuw IM, Brug J. Effects and moderators of exercise on quality of life and physical function in patients with cancer: An individual patient data meta-analysis of 34 RCTs. Cancer Treat Rev. 2017 Jan;52:91-104. Epub 2016 Dec 5. PMID: 28006694.’. [CrossRef]
- ‘Ashcraft KA, Peace RM, Betof AS, Dewhirst MW, Jones LW. Efficacy and Mechanisms of Aerobic Exercise on Cancer Initiation, Progression, and Metastasis: A Critical Systematic Review of In Vivo Preclinical Data. Cancer research 2016, 76(14): 4032–4050’.
- ‘Nieman DC, Wentz LM. The compelling link between physical activity and the body’s defense system. J Sport Health Sci. 2019;8:201–17.’. [CrossRef]
- ‘Mustian KM, Sprod LK, Palesh OG, Peppone LJ, Janelsins MC, Mohile SG, Carroll J. Exercise for the management of side effects and quality of life among cancer survivors. Curr Sports Med Rep. 2009 Nov-Dec;8(6):325-30. PMID: 19904073; PMCID: PMC2875185.’. [CrossRef]
- ‘Scott JM, Zabor EC, Schwitzer E, Koelwyn GJ, Adams SC, Nilsen TS, Moskowitz CS, Matsoukas K, Iyengar NM, Dang CT, Jones LW. Efficacy of Exercise Therapy on Cardiorespiratory Fitness in Patients With Cancer: A Systematic Review and Meta-Analysis. J Clin Oncol. 2018 Aug 1;36(22):2297-2305. Epub 2018 Jun 12. PMID: 29894274; PMCID: PMC6804903.’. [CrossRef]
- ‘Loughney L, West MA, Kemp GJ, Grocott MP, Jack S. Exercise intervention in people with cancer undergoing neoadjuvant cancer treatment and surgery: A systematic review. European journal of surgical oncology : the journal of the European Society of Surgical Oncology and the British Association of Surgical Oncology 2016, 42(1): 28–38’.
- ‘Champ, C.E., Carpenter, D.J., Diaz, A.K. et al. Resistance Training for Patients with Cancer: A Conceptual Framework for Maximizing Strength, Power, Functional Mobility, and Body Composition to Optimize Health and Outcomes. Sports Med 53, 75–89 (2023).’. [CrossRef]
- ‘Henriksson A, Arving C, Johansson B, Igelström H, Nordin K. Perceived barriers to and facilitators of being physically active during adjuvant cancer treatment. Patient Educ Couns. 2016 Jul;99(7):1220-1226. Epub 2016 Jan 28. PMID: 26860549.’. [CrossRef]
- ‘Thomas, V.J., Seet-Lee, C., Marthick, M. et al. Aerobic exercise during chemotherapy infusion for cancer treatment: a novel randomised crossover safety and feasibility trial. Support Care Cancer 28, 625–632 (2020).’. [CrossRef]
- ‘Singh B, Hayes SC, Spence RR, Steele ML, Millet GY, Gergele L. Exercise and colorectal cancer: a systematic review and meta-analysis of exercise safety, feasibility and effectiveness. Int J Behav Nutr Phys Act. 2020 Sep 24;17(1):122. PMID: 32972439; PMCID: PMC7513291.’. [CrossRef]
- ‘Avancini A, Borsati A, Toniolo L, Ciurnelli C, Belluomini L, Budolfsen T, Lillelund C, Milella M, Quist M, Pilotto S. Physical activity guidelines in oncology: A systematic review of the current recommendations. Crit Rev Oncol Hematol. 2025 Jun;210:104718. Epub 2025 Apr 5. PMID: 40194715.’. [CrossRef]
- ‘Hayes, S.C., Spence, R.R., Galvao, D.A., Newton, R.U., 2009. Australian Association for Exercise and Sport Science position stand: optimising cancer outcomes through exercise. J. Sci. Med Sport 12 (4), 428–434’. [CrossRef]
- ‘Campbell, K.L., Winters-Stone, K.M., Wiskemann, J., May, A.M., Schwartz, A.L., Courneya, K.S., Zucker, D.S., Matthews, C.E., Ligibel, J.A., Gerber, L.H., Morris, G.S., Patel, A.V., Hue, T.F., Perna, F.M., Schmitz, K.H., 2019. Exercise Guidelines for Cancer Survivors: Consensus Statement from International Multidisciplinary Roundtable. Med Sci. Sports Exerc 51 (11), 2375–2390.’. [CrossRef]
- ‘Ligibel, J.A., Bohlke, K., May, A.M., Clinton, S.K., Demark-Wahnefried, W., Gilchrist, S. C., Irwin, M.L., Late, M., Mansfield, S., Marshall, T.F., Meyerhardt, J.A., Thomson, C. A., Wood, W.A., Alfano, C.M., 2022. Exercise, Diet, and Weight Management During Cancer Treatment: ASCO Guideline. J. Clin. Oncol. 40 (22), 2491–2507.’. [CrossRef]
- ‘D. Kerrigan, S. Keteyian, J. K. Ehrman, S. Brown, R. Filipiak, N. Martinez, D. Ihlenfeldt, J. Varga, E. M. Walker.A pilot study of aerobic exercise performed in breast cancer patients during chemotherapy infusion. Journal of Clinical Oncology 2010 28:15_suppl, e19527-e19527’. [CrossRef]
- ‘Housman B, Flores R, Lee DS (2021) Narrative review of anxiety and depression in patients with esophageal cancer: underappreciated and undertreated. J Thorac Dis 13(5):3160–3170’. [CrossRef]
- ‘Wang YH, Li JQ, Shi JF, Que JY, Liu JJ, Lappin JM, Leung J, Ravindran AV, Chen WQ, Qiao YL, Shi J, Lu L, Bao YP. Depression and anxiety in relation to cancer incidence and mortality: a systematic review and meta-analysis of cohort studies. Mol Psychiatry. 2020 Jul;25(7):1487-1499. Epub 2019 Nov 19. PMID: 31745237.’. [CrossRef]
- ‘Saviola, F., Pappaianni, E., Monti, A. et al. Trait and state anxiety are mapped differently in the human brain. Sci Rep 10, 11112 (2020). [CrossRef]
- ‘Battle DE. Diagnostic and Statistical Manual of Mental Disorders (DSM). Codas. 2013;25(2):191-2. PMID: 24413388. [CrossRef]
- ‘NCCN. Distress during cancer care. NCCN Guidelines for Patients, National Comprehensive Cancer Network. 2020. Available from https://www.nccn.org/patients/guidelines/content/PDF/distress-patient.pdf.
- ‘Üstündag, S., Zencirci, A.D. (2015) “Factors affecting the quality of life of cancer patients undergoing chemotherapy: A questionnaire study”, Asia-Pacific Journal of Oncology Nursing, 2(1), pp. 17–25. [CrossRef]
- ‘Committee on Improving the Quality of Cancer Care: Addressing the Challenges of an Aging Population; Board on Health Care Services; Institute of Medicine; Levit L, Balogh E, Nass S, et al., editors. Delivering High-Quality Cancer Care: Charting a New Course for a System in Crisis. Washington (DC): National Academies Press (US); 2013 Dec 27. 3, Patient-Centered Communication and Shared Decision Making. Available from: https://www.ncbi.nlm.nih.gov/books/NBK202146/’.
- ‘Spielberger, C. D., Gorsuch, R. L., Lushene, R., Vagg, P. R. & Jacobs, G. A. Manual for the state-trait anxiety inventory (Consulting Psychologists Press, Palo Alto, 1983).’.
Figure 1.
Warm up exercise. (a) Starting position; (b) dorsiflexion; (c) plantar flexion; (d) mid-range knee extension; (e) full knee extension and isometric contraction; (f) left knee lift; (g) right knee lift; (h) starting position for torso rotation; (i) right rotation; (j) left rotation.
Figure 1.
Warm up exercise. (a) Starting position; (b) dorsiflexion; (c) plantar flexion; (d) mid-range knee extension; (e) full knee extension and isometric contraction; (f) left knee lift; (g) right knee lift; (h) starting position for torso rotation; (i) right rotation; (j) left rotation.
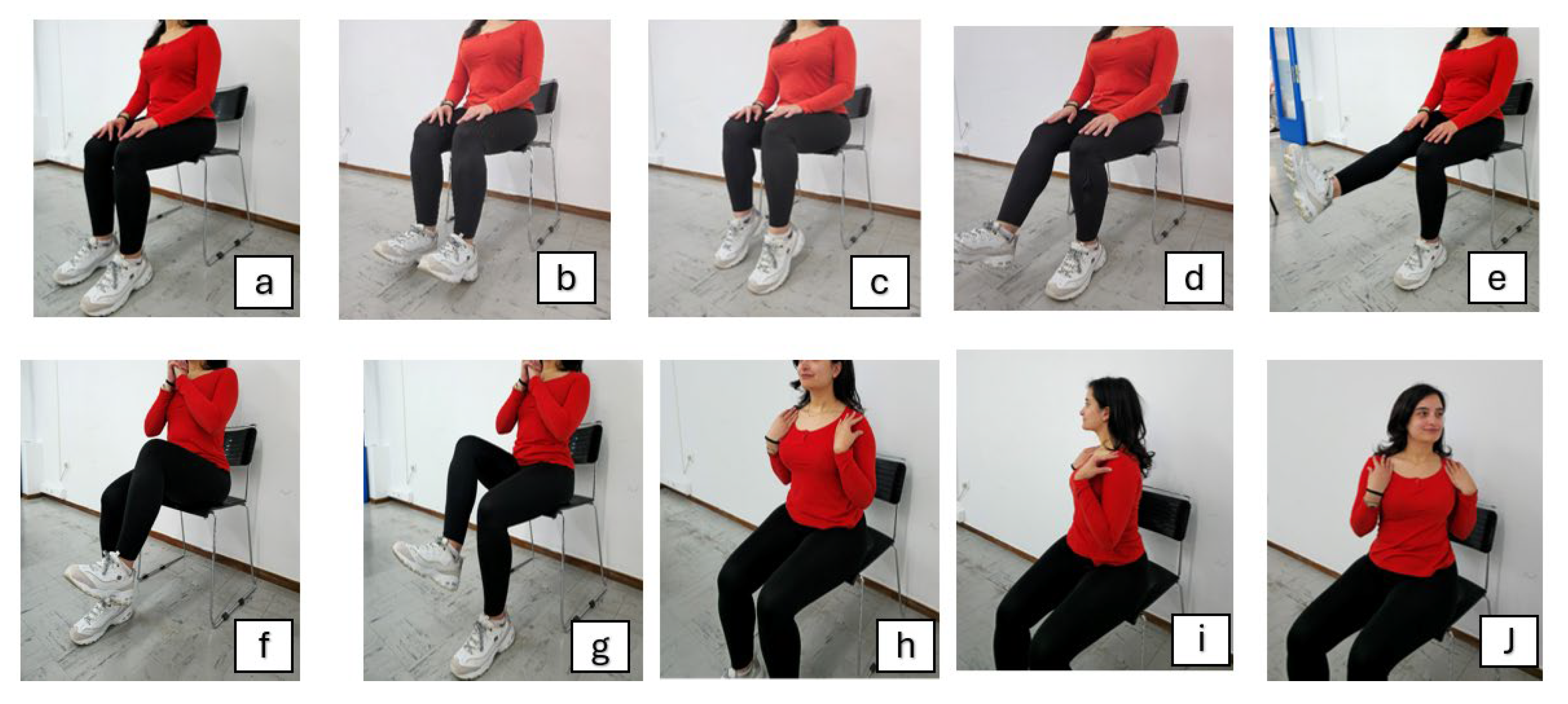
Figure 2.
Upper limb exercise. (a) Starting position for hand gripping; (b) final position of hand gripping; (c) forearm supination; (d) forearm pronation; (e) starting position of elbow flexion; (f) mid-range of elbow flexion; (g) end-range of elbow flexion; (h) starting position of shoulder flexion; (i) mid-position of shoulder flexion; (j) final position of shoulder flexion; (k) starting position of shoulder abduction; (l) mid-position of shoulder abduction; (m) final position of shoulder abduction.
Figure 2.
Upper limb exercise. (a) Starting position for hand gripping; (b) final position of hand gripping; (c) forearm supination; (d) forearm pronation; (e) starting position of elbow flexion; (f) mid-range of elbow flexion; (g) end-range of elbow flexion; (h) starting position of shoulder flexion; (i) mid-position of shoulder flexion; (j) final position of shoulder flexion; (k) starting position of shoulder abduction; (l) mid-position of shoulder abduction; (m) final position of shoulder abduction.
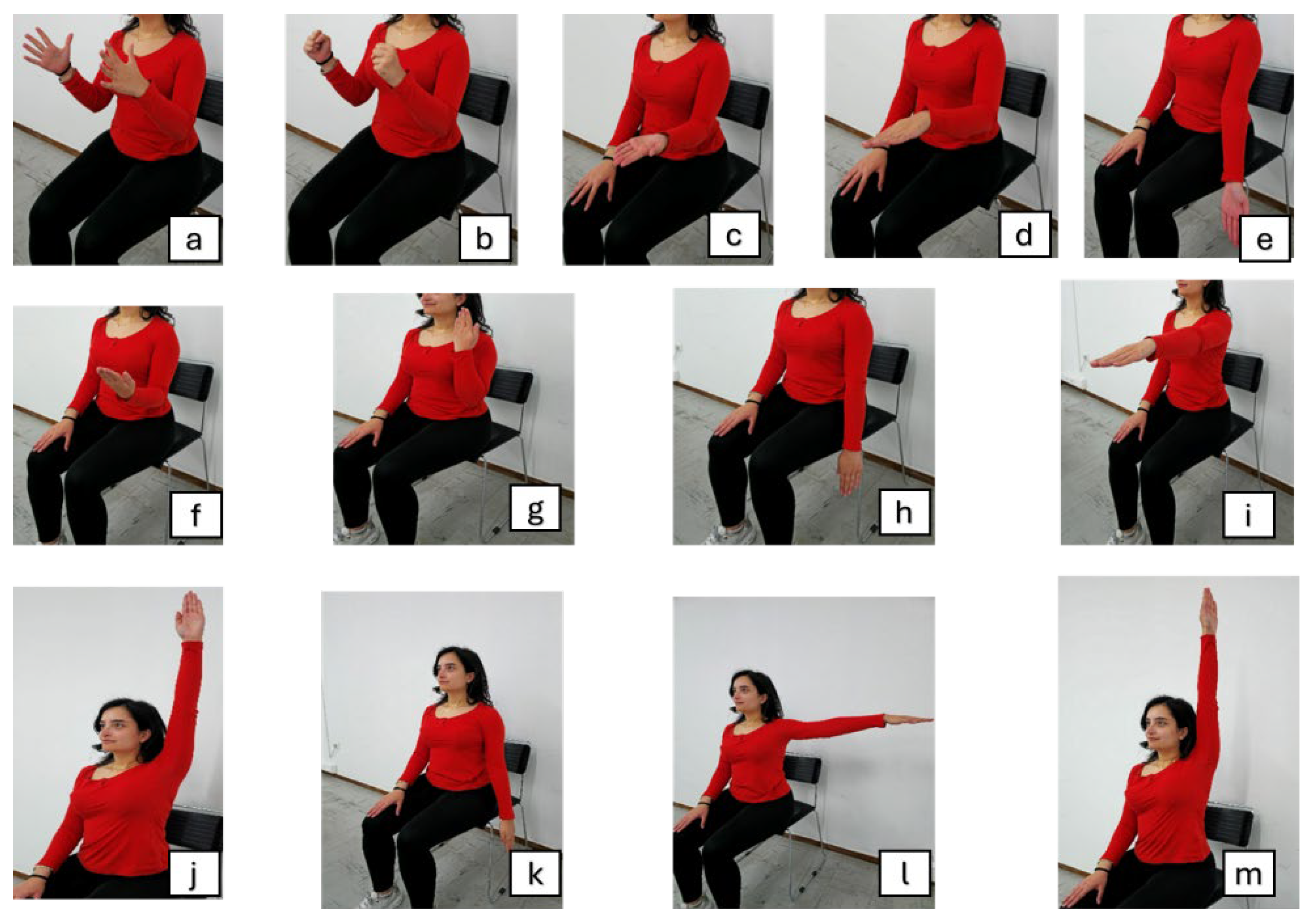
Figure 3.
Standing exercise. (a) Starting position; (b) left small on-the-spot step; (c) right small on-the-spot step; (d) left high-knee step; (e) right high-knee step; (f) left leg lunge; (g) right leg lunge; (h) position for torso rotation.
Figure 3.
Standing exercise. (a) Starting position; (b) left small on-the-spot step; (c) right small on-the-spot step; (d) left high-knee step; (e) right high-knee step; (f) left leg lunge; (g) right leg lunge; (h) position for torso rotation.
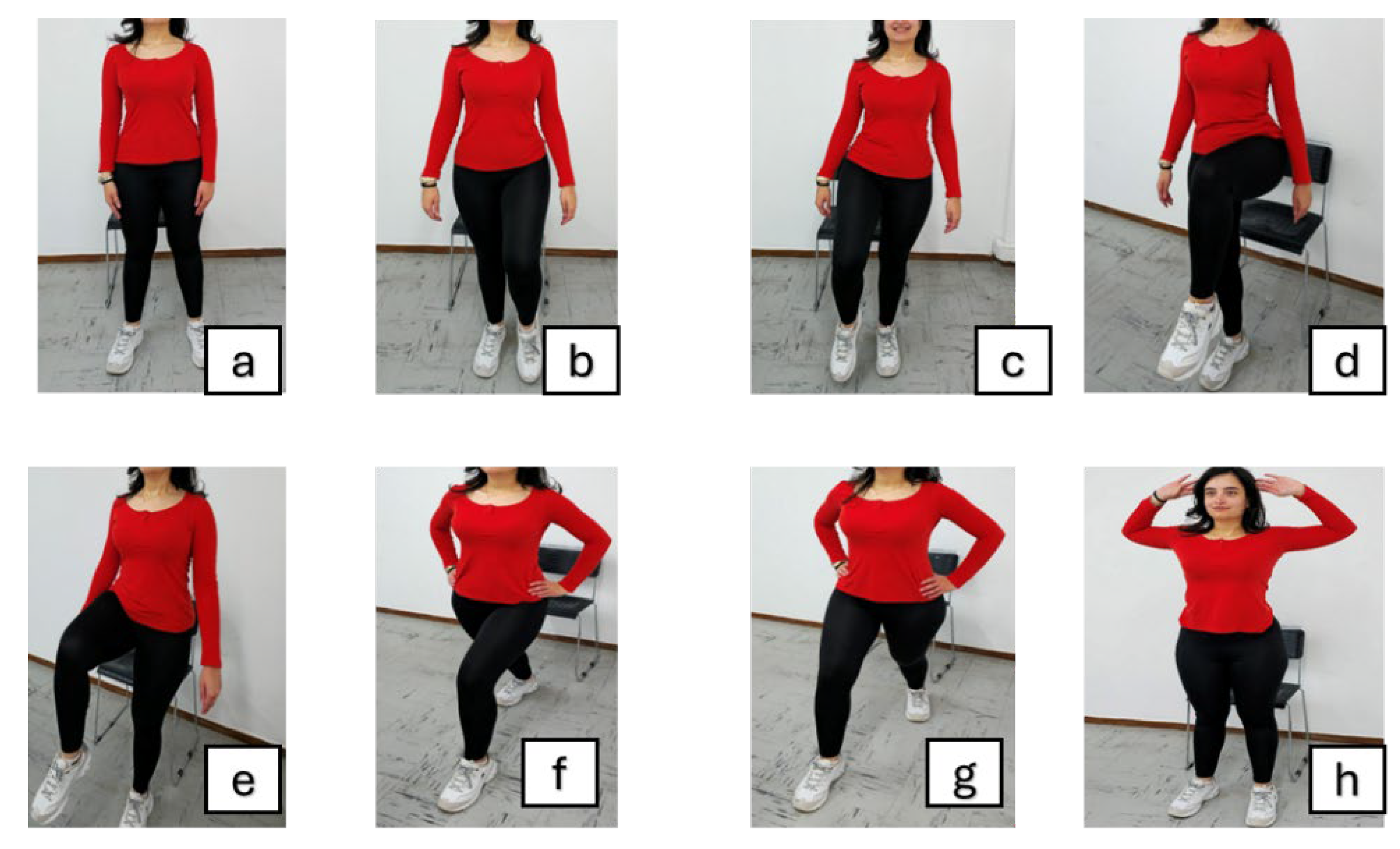
Figure 4.
Stretching. (a) Right torso bend; (b) left torso bend; (c) overhead arm stretch; (d) right seated hamstring stretch; (e) left seated hamstring stretch; (f) starting position for deep breath; (g) deep inhale; (h) exhale through the mouth.
Figure 4.
Stretching. (a) Right torso bend; (b) left torso bend; (c) overhead arm stretch; (d) right seated hamstring stretch; (e) left seated hamstring stretch; (f) starting position for deep breath; (g) deep inhale; (h) exhale through the mouth.
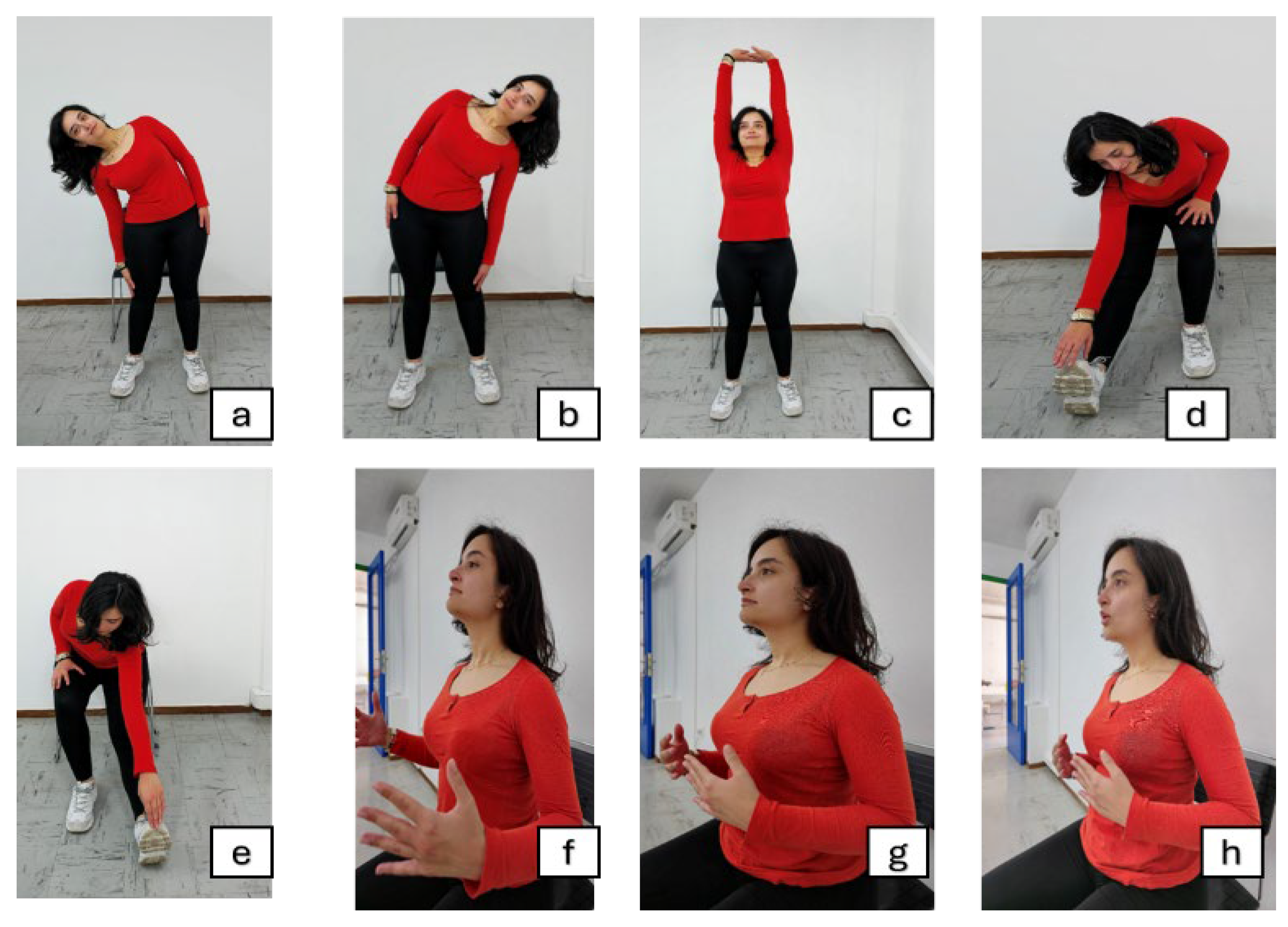
Figure 5.
Patient recruitment flow chart. Notably, most eligible patients refused participation due to fear of injury or fatigue.
Figure 5.
Patient recruitment flow chart. Notably, most eligible patients refused participation due to fear of injury or fatigue.
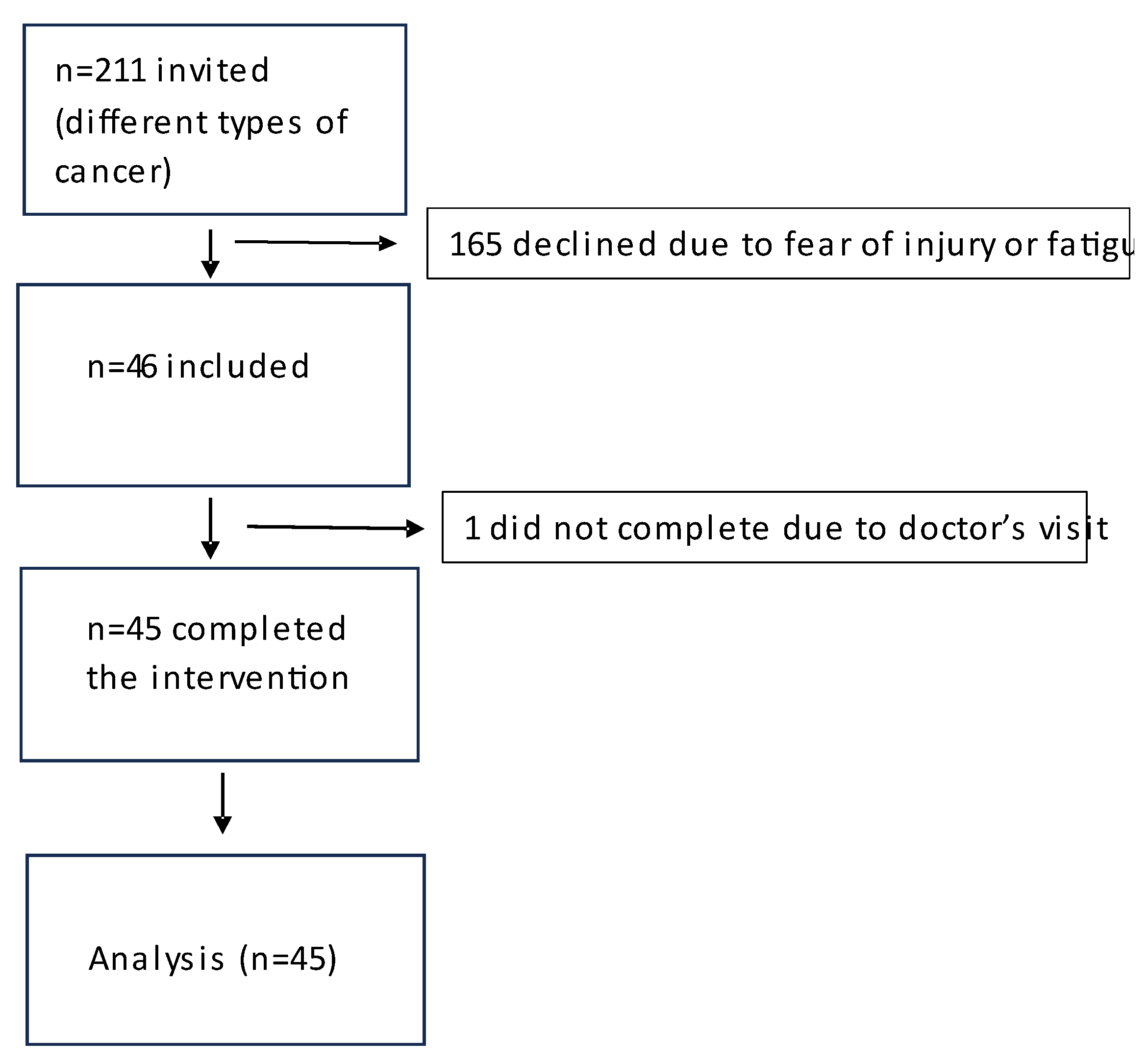
Figure 6.
Y-1 Form of STAI-State questionnaire answers before and after exercise. The median is symbolized by a continuous line, quartiles by dotted lines.
Figure 6.
Y-1 Form of STAI-State questionnaire answers before and after exercise. The median is symbolized by a continuous line, quartiles by dotted lines.
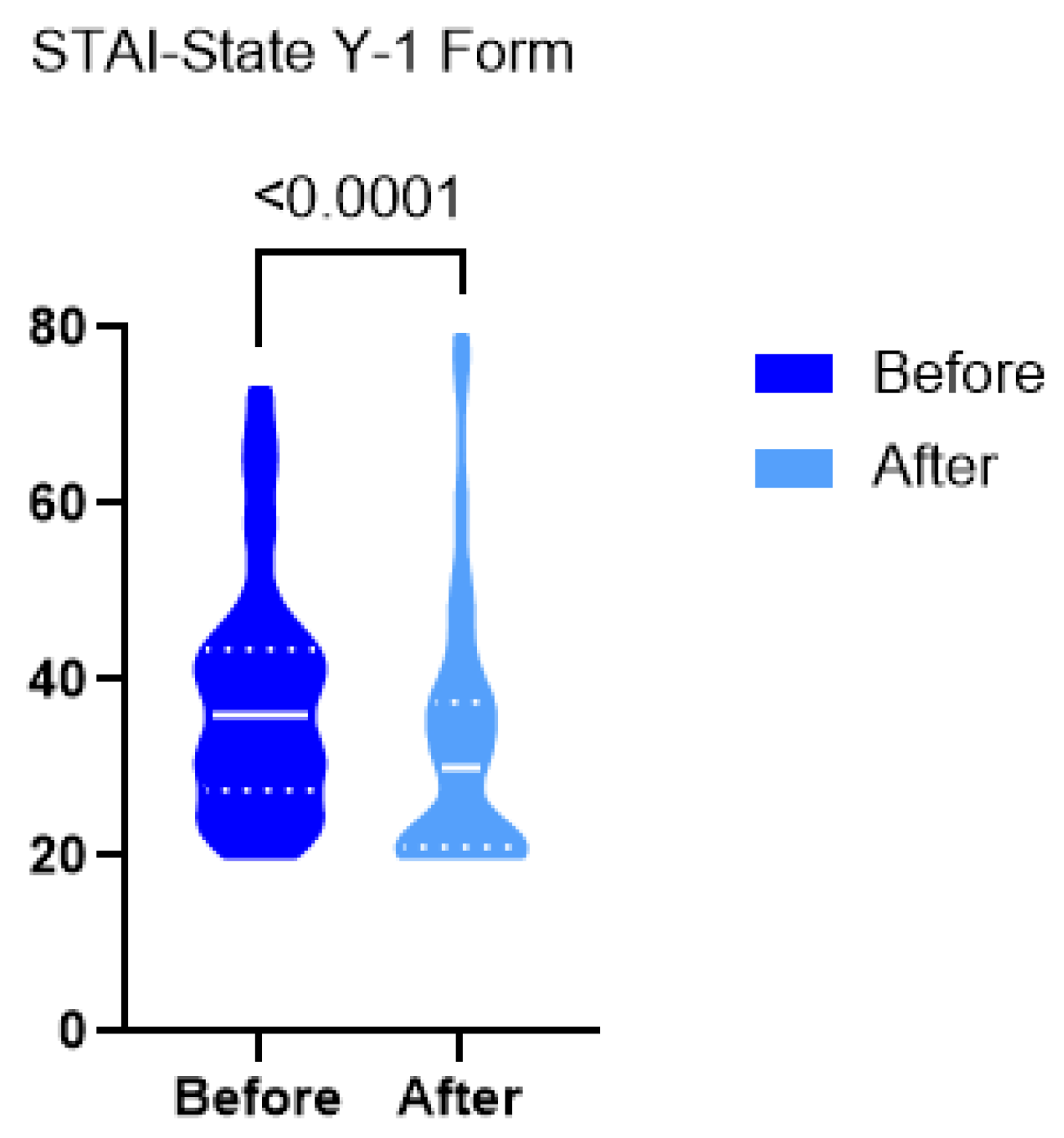
Figure 7.
Spearman’s rho correlation analysis.
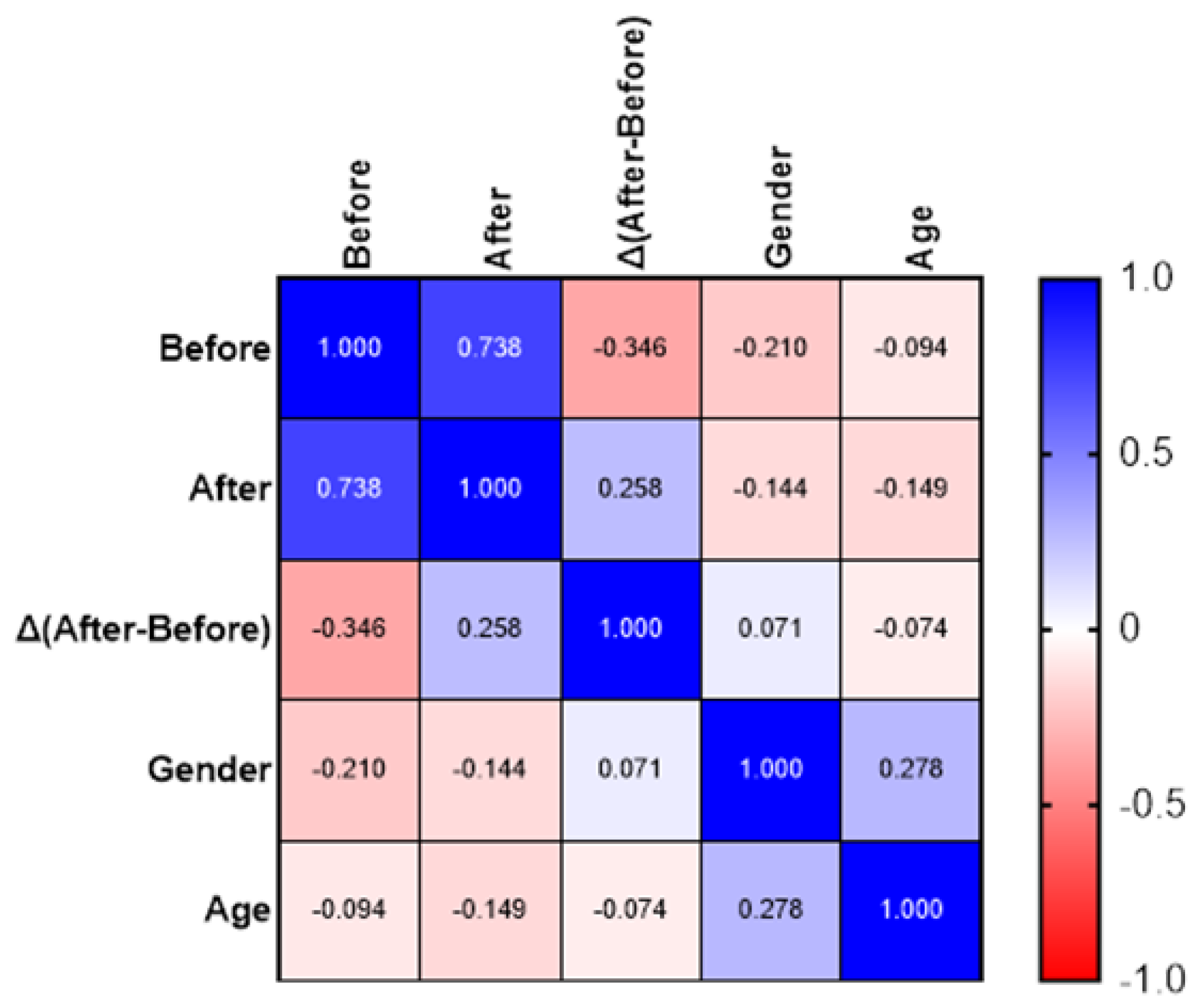

Table 1.
Program of mild exercise used in the study.
| Exercise stage | Included exercises |
|
Warm-Up [5 minutes]: |
|
| |
| |
|
Main Exercise [10 minutes]: |
|
| |
| |
| |
| |
|
Cool-Down [5 minutes]: |
|
| |
| |
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



