
Submitted:
03 July 2025
Posted:
04 July 2025
You are already at the latest version
Abstract
Background: Interstitial lung disease (ILD) is a frequent complication in rheumatoid arthritis (RA) where it represents the most common extra-articular involvement (with a prevalence of about 10-60%) and the second cause of mortality (after cardiovascular diseases). Spondyloarthritides (SpA) are chronic arthritides that share with RA both a similar disease burden and similar therapeutical approaches. ILD evaluation is challenging, given the low sensitivity of X-ray and pulmonary function tests, and radiation linked to repetitive HRCT. Lung Ultrasound (LUS) has shown potential in the evaluation of ILD in autoimmune diseases. Objectives: To assess the prevalence of ILD in a cohort of SpA patients (pts) using LUS with respect to healthy subjects (HS). Secondary aim is to assess possible correlations between ILD and clinical features in a cohort of SpA pts using LUS. Methods: Consecutive SpA out-patients were examined by LUS, applying the definition for pleural line irregularity (PLI) recently provided by the OMERACT taskforce for LUS in systemic sclerosis. Seventy-one intercostal spaces were studied (14 in the anterior chest, 27 lateral and 30 posterior) in all the pts/HS using an Esaote MyLab25 Gold US machine with a linear 7.5-10 MHz probe. A total pleural score was calculated. Each patient answered to Italian-validated PROs on respiratory function (Leicester and Saint-George), global health (SF-36) and dyspnea (mMRC scale). Clinical data on disease-duration, disease-onset, disease-activity (at the moment of the examination) and MTX/biologics treatment were collected from the medical records. Results: Seventy-three SpA pts (46 psoriatic arthritis -PsA- and 27 ankylosing spondylitis -AS-) and 56 HS were studied. No significant differences were demonstrated between groups (SpA vs HS and PsA vs AS) for age, sex, BMI and smoking habits. The total PLI score was significantly higher in SpA pts than in HS (p0.001). A positive correlation was found between total PLI score and PLI score from anterior, posterior and lateral chest. The posterior part of the chest showed a higher PLI score than the anterior and lateral one. No statistically significant differences were found between PsA and AS. MTX use was not a risk factor for PLI (no differences were found between SpA MTX+ and SpA MTX- patients). PROs (Leicester, Saint-George and SF-36) were not related to PLI total score. A significant correlation was found only between SF36 score and the presence of PLI in the anterior chest. PROs were instead related among them, showing a good concordance for absence/presence of symptoms. Disease activity, disease duration and age at disease-onset were not related to PLI total score. Smoking habit resulted to be predictive for a significant higher PLI score both in SpA patients and HS. Conclusions: LUS examination shows a higher amount of PLI in SpA with respect to HS. Smoking habit was the only clinical feature correlated to PLI on LUS examination in our population.
Keywords:
psoriatic arthritis
; interstitial lung disease
; lung ultrasound
; lung
; ultrasound
; ankylosing spondylitis
Introduction
Recent evidences from the literature underlined how the lung could be considered as a “target” organ in systemic autoimmune diseases, in particular systemic sclerosis (SSc), idiopathic inflammatory myopathies (IIM), primary Sjogren syndrome and rheumatoid arthritis (RA) [1,2]. It tends to manifest itself more frequently as an interstitial lung disease (ILD), that is an inflammatory involvement of the lung, with specific histologic and radiologic patterns, with different clinical presentation and prognosis. If, in the “non specific interstitial pneumonia” (NSIP) inflammatory cells infiltrates are the main characteristic, in the “usual interstitial pneumonia” (UIP) fibrosis is the predominant component [3]. ILD, usually presenting with a UIP pattern, is a frequent complication in rheumatoid arthritis (RA) [4] where it represents the most common extra-articular involvement (with a prevalence of about 10-60%), and the second cause of mortality (after cardiovascular diseases). Spondylarthritis (SpA) are chronic arthritis that share with RA both a similar burden of disease (i.e. peripheral arthritis, age of patients, impact on the quality of life etc…), some similar cytokines pathways (i.e. TNFa pathway) and similar therapeutical approaches (i.e. leflunomide, methotrexate, TNFa inhibitors). Lung involvement in SpA may occurr in every moment of the disease and it may present in ankylosing spondylitis (AS) patients as ILD, upper lobe fibrosis, emphysema, bronchiectasis, and functional ventilation defects, as already shown in 2007 by Sampaio-Barros et al, who found high resolution computer tomography (HRCT) abnormalities in 21/52 patients, mostly nonspecific linear parenchymal opacities (19%), lymphadenopathy (12%), emphysema (10%), bronchiectasis (8%), and pleural involvement (8%) [5]. Its prevalence in AS varies according to the diagnostic tool used, ranging from 8% using conventional radiology, to 40-80% using HRCT and 18-42% with pulmonary function tests (PFTs). El Maghraoui et al, in a recent systematic literature review (SLR), highlighted the discrepancy between the prevalence of symptomatic patients (5.9% out of 303) and the prevalence of ILD-related changes at the HRCT (61%) in a population of AS patients. The more common HRCT findings were pleural thickening (18%), parenchymal band (15%), interlobular thickening (11%) and ground glass areas (11%). A correlation between disease duration and the presence of HRCT findings was demonstrated only for the upper lobe fibrosis (in the 7% of patients) [6]. In psoriasis patients, an increased risk for chronic obstructive pulmonary disease (COPD) (RR 1,45) was demonstrated [7]. More recently, a significant link between psoriasis and ILD was noted [8,9]. ILD was identified in 8/392 psoriatic patients (2%) examined with HRCT during the screening for beginning a biologic DMARDs (bDMARD) treatment. Those patients were presenting more frequently bilateral ground-glass and/or irregular linear (reticular) opacity in the lower lung zone [8]. In another study, involving patients referring to an ILD clinic, psoriasis has been found in the 4.7% (21/447) of patients, presenting an usual interstitial pneumonia (UIP) HRCT pattern in 9 patients, a nonspecific interstitial pneumonia (NSIP) pattern in 6 patients, an organizing pneumonia pattern in 4 patients and an hypersensitivity pneumonitis pattern in 2 patients [9]. So, apparently, the most common HRCT pattern in psoriasis is the UIP pattern, just like what is the evidence for RA. Yue et al, recently provided genetic evidence supporting the hypotheis that PSA may be a contributory risk factor for ILD in psoriatic patients [10]. Considering that psoriasis is part of the broader concept of “psoriatic disease” we speculate that UIP pattern is the one we could find in PsA too, confirming the “similarity” between RA and psoriatic disease.
Peluso et al, demonstrated lung involvement in very few patients with axial psoriatic arthritis (PsA) [11]. Nodular or ground glass in the upper lobes and reticular pattern and honeycombing in the lower lobes were demonstrated by Bargagli et al as the predominant HRCT pattern in PsA patients [12], supporting the concept of UIP pattern in PsA. More recently, Schäfer et al demonstrated chest radiography pulmonary involvement in 37.0 % of a group of patients affected by RA and PsA (50% and 22.7% respectively, in RA and in PsA), with only the 35.3% of them symptomatic [13]. Similarly, Provan et al. noticed an ILD incidence per 1,000 person-years of 1.9, 0.6 and 0.2 in RA, PsA (with no previous ILD who initiated a first-ever treatment with a bDMARD) and control group, respectively, with PsA patients developping ILD being older, with higher levels of ESR and patient VAS at baseline with respect to the ones who did not present ILD [14]. Although those evidence, there is still a lack of data about lung involvement in SpA, particularly focusing on ILD.
ILD evaluation is challenging, given the low sensitivity of conventional radiology and PFTs, and radiation risk, which limits repetitive HRCT. Lung ultrasound (LUS), developed in the last 20 years, is a radiation-free imaging technique, not expensive, repeatable, and patient friendly. Since 2008, it has shown potential in the evaluation of ILD in autoimmune diseases [15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47]. LUS is based on the change in the alveolar air/tissue ratio, with an increment for solid tissue (i.e. fibrosis, blood, edema), that allow the creation of US artifacts. Most of time there is a thickening of interlobular septae (both for fibrosis or edema) that creates ultrasound findings (B-lines) and irregularities in the pleural line (PLI); these findings are the US demonstration of a change in the normal structure of the lung.
The most studied US finding is represented by the so-called B–lines, defined as a vertical hyperechoic reverberation artifact that arises from the pleural line, extends to the bottom of the screen without fading, and moves synchronously with lung sliding, by the Outcome Measure in Rheumatology (OMERACT) [27]. B-lines are well diffused in the cardiogenic lung edema and this the reason why LUS was primarily used by cardiologists and pneumologists. Anyway, in more recent years, LUS spreads also in the rheumatic field [15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47]. Pleural line evaluation (irregularity, thickening or fragmentation) for ILD assessment was initially described by Reißig & Kroegel [48] (together with B-lines and sub-pleural changes) and pleural line irregularity (PLI) is now defined as a loss of regularity that may be associated with an increase in thickness (either focal, diffuse, linear, or nodular) [27].
Recently, a SLR demonstrated face and content validity of LUS for the evaluation of ILD, as well as its feasibility, in systemic sclerosis, and by extension in other rheumatic musculoskeletal diseases which may present ILD as part of their clinical manifestation [26].
Considering the increasing role of LUS as a diagnostic tool for lung involvement in rheumatologic diseases, as well as its safety, we thought this technique might be used for the evaluation of pleural line irregularities (PLI) in patients with SpA. So, our primary aim was to assess, using LUS, the prevalence of ILD in a cohort of SpA patients with respect to healthy subjects (HS). Secondary aim is to assess possible correlations between ILD and clinical features in our cohort of SpA, as well as to assess it there are any differences between AS and PsA patients.
Materials and Methods
Patients
This is a cross-sectional study performed in the out-patients SpA Clinic of the Rheumatology Unit (Azienda Ospedaliero-Universitaria Pisana) between November 2019 and January 2022. The study was approved by the local Ethical Committee. Patients fulfilling ASAS or CASPAR classification criteria [49,50] were enrolled, in a consecutive way in two 3-months-time (without any previous selection) and compared to matched HS. Demographic and clinical data (sex, age, BMI, disease-duration, disease-onset, disease-activity at the moment of the examination -by using DAPSA and ASDAS score-, presence of psoriasis and treatment with synthetic DMARDs (sDMARDs) or bDMARDs were collected from the medical records, while smoking habits (presence/absence and the number of pack/year), the presence of respiratory symptoms (i.e. cough in the last 8 weeks) and their possible causes (i.e. COPD, asthma, gastroesophageal reflux or ACE-inhibitors treatment) were investigated, as well as previous exposition to pneumotoxic substances like asbestos, amiodarone or radiotherapy. The presence of respiratory symptoms already diagnosed as specific of a pulmonary disease different from ILD, or the exposition to respiratory toxic substances were considered exclusion criteria of the study.
Each patient filled-in the Italian-validated PROs on respiratory function, (Leicester Cough Questionnaire -LCQ- and Saint-George’s Respiratory Questionnaire – SGRQ-), global health (Short Form-36 Health Survey -SF-36-) and dyspnea (Modified British Medical Research Council Questionnaire -mMRC-). LCQ is used to evaluate how cough impacts on patients’ quality of life [51]; SGRQ investigate on the features and intensity of respiratory disorders, as well as their impact of patent’s life [52] and, mMRC assess the degree of physical effort that cause the symptom, being significantly correlated to respiratory function [53].
Lung Ultrasound Assessment
Seventy-two intercostal spaces scanning protocol was used (14 in the anterior, 27 in lateral and 30 in posterior chest; along parasternal, mid-clavear, anterior and posterior axillary, para-vertebral and scapular angle lines) in all the patients/HS, using Esaote MyLab25 Gold US machine with a linear 6-18 MHz probe set at a frequency of 10 MHz with a Gain set at 28%. Up to now, the scanning method is not standardised so, we used a scanning protocol we already used in previous studies; this was also used in another published paper where the scoring system we adopted was validated against HRCT [24].
Patients and HS were examined in a seated position for postero-lateral intercostal spaces and lying on the bed for the antero-lateral evaluation.
Lung examination was made assessing only PLI and applying the definition recently provided by the OMERACT taskforce for LUS [27]. We used the scoring system by Pinal-Fernandez et al [24], providing a score 0 if a normal pleural line was present, a score 1 if pleural irregularity was moderate and score 2 if it was severe as shown in Figure 1.
All the examinations were made by two different operators (C.E. and V.A.) who were previously trained by an expert utrasonographer (D.S.A.) with more than 10 years of experience in LUS. Before the beginning of the study, reproducibility intra- and inter- operators was tested on video clips, with the same methodology applied to the OMERACT validation process [27]. We used a set of 30 high-quality video-clips for pleural line irregularity obtained from systemic sclerosis patients, providing a balanced range of normal, low, medium and high lung disease involvement).
Statistical Analysis
Continuous variables were reported as mean and standard deviation in case of parametric distribution while, as median and interquartile range (IQR) for non-parametric distribution. Comparison between the means for the two groups was made with the non-parametric Mann Whitney test and, for comparison between three groups, with the Kriskal-Wallis test. Comparison of proportions was performed with Chi2. The correlation between continuous variables was done with Spearman's test. A p<0.05 was considered statistically significant. Fleiss kappa was used to assess the inter-rater agreement between the sonographer for scoring PLI [54]. Reliability data were interpreted as follows: 0–0.20 represent slight; 0.21–0.40 fair; 0.41–0.60 moderate; 0.61–0.80 good and >0.80 excellent reliability.
Results
Seventy-three SpA (46 with PsA and 27 with AS) patients and 56 HS were enrolled; demographic and clinical data are reported in Table 1. No significant differences were observed between groups (SpA vs HS and PsA vs AS) relative to sex, age, BMI (numerically higher in PsA) and smoking habits (also considering ex-smokers).
Disease activity, evaluated with ASDAS and DAPSA scores for AS and PsA, respectively, showed a higher diseases activity score in AS (mean ASDAS score was 2.2±1.4, indicating a high disease activity, while DAPSA score was 14.1±10.5 indicating a moderate disease activity).
Psoriasis (assessed by BSA) was present only in PsA group (42/46 patients, 22/42 with skin evidence of it at the moment of the LUS). All PsA patients with skin disease, presented low levels of psoriasis (BSA<5).
csDMARDs were significantly more prescribed in PsA than in AS (23/46 vs 7/27) being MTX the most frequently used (MTX in 18, luflunomide in 7, hydroxicloroquine in 3 and, sulfosalazine in 2 patients). MTX was mostly used in PsA patients but, few AS patients were also treated with MTX, for their pheripheral joint involvement.
bDMARDs were more frequently used in AS. TNFa inhibitors were significantly more used in AS, while biological treatments with other mechanisms, in PsA.
Ultrasound Results
Inter-reader reliability was good (k=0.77).
Mean PLI score in patients (AS+PsA) was 19.9±10.9 (range 0-51) with a statistically significant difference with respect to HS (10.3±7.7; range 0-36; p<0.001); this difference remained significant also when assessing anterior, posterior, or lateral chest areas alone (p<0.001) or between AS or PsA group and HS (p<0.001). No significant differences were found between PsA and AS groups (19.9±11.2; range 0-51; and 20±10.6; range 2-46; respectively). The posterior part of the chest showed a higher PLI score than the anterior and lateral one (with the latter resulting to be significantly lower than the posterior PLI score) (Figure 2). Single areas (anterior, posterior, or lateral chest) PLI scores were correlated with mean PLI score so (p<0.05 for all) so, we decided to use the mean value for evaluating the correlation between LUS and other parameters.
PLI Score Correlation with Demographic Data and PROs
We did not find any significant correlation between PLI score and sex, BMI (significantly higher in males), or age at the moment of the study.
Smokers were significantly more present in the patient’s group (67% vs 36%). A positive correlation between PLI score and smoke habits (yes/not, and also considering previous or actual smoking; p<0.003) or between PLI score and number of pack/years (p<0.05) was highlighted in both SpA patients and HS. Anterior chest resulted the mostly correlated to smoke (both for yes/not or pack/year) in both patients and HS. A positive correlation was also noted between dyspnea (assessed with mMRC) and smoke (p=0.05) and even stronger with pack/year (p=0.019).
PLI mean score was not correlated with PROs (LCQ, SGRQ, mMRC and SF-36); the only positive correlation was demonstrated for mMRC score and anterior chest PLI (p=0.05), as well as with SF-36 score. PROs were instead related among them (showing a good concordance for absence/presence of symptoms; p=0.001; r=0.500).
PLI Score Correlation with Clinical Data
Presence of crackles (even if in only 10 patients) was significantly related to PLI score (p<0.003).
Disease activity, disease duration, age at disease-onset (even when considering onset <40 years, onset between 40 and 65 years and onset >65 years groups) or presence of psoriasis were not related to PLI total score. Disease activity in AS group was significantly correlated to SGRQ single domains (activity and impact; p<0.05) and with all domains of SF-36 (p<0.05).
PLI Score Correlation with Treatments
We did not demonstrate any significant correlation between bDMARDs or csDMARDs and PLI score. When evaluating single treatments, we find a significant relationship between IL17 inhibitors and PLI score (p<0,0065 vs no bDMARDs) and a numerical difference in favor of TNFa inhibitors vs no bDMARDs: 18.4 and 21.7, respectively). When considering only MTX, patients treated with MTX presented numerically inferior PLI (both total and single areas) (Figure 3).
4. Discussion
ILD represents one of the most severe complications in different rheumatic diseases (systemic sclerosis, rheumatoid arthritis, other connective tissue diseases and vasculitis) being the first cause of mortality. ILD prevalence varies according to the method used to detect it, ranging between 10 and 60% (i.e. in RA it is between 10-70%) [54]. Little is known about the real prevalence of ILD in SpA: few data are available on AS showing about 60% of AS with different degrees of lung disease (pleural thickening in 18% and ground glass or interlobular thickening in about 11% of the patients), supporting the need of an early screening of patients [6]. Literature data in PsA are few and suggest that lung involvement is not common [10,13,14], with nodular or ground glass in the upper lobes or, honeycombing in the lower lobes [12].
The gold–standard imaging technique for ILD assessment is HRCT (usually using Warrick’s score). The radiation, necessary to complete a HRCT impose the need for other “less invasive” imaging techniques to be used for large screening programs. Lung ultrasound a “less invasive”, easy to perform and cheap technique, has recently shown potential for ILD evaluation by detecting two findings: B-lines and pleural irregularity. Those findings have demonstrated a direct correlation with HRCT score both in cardiology, pneumology and, more recently, rheumatology [6,18,32].
LUS standardization is still to come, and the OMERACT is working on it. Most of the paper in the literature are focusing on B-lines using different scanning protocols (ranges from 72 to 10 intercostal spaces) [20,21]. Less papers evaluate pleural line, both in terms of thickening (i.e. a thickening of more than 2.8 mm in at least two contiguous areas correlate with ILD on HRCT) [21,23] and pleural irregularity. Pinal Fernandez et al demonstrated a numerically higher sensitivity and specificity for pleural line irregularity with respect to B-lines [24]. Pleural line irregularity (in terms of fragmentation, thickening, interruption, or irregularity) has not been demonstrated in healthy subjects or in patients with congestive heart disease, apparently providing more specific results for ILD [25]. We know that the lower part of the lungs can present some isolated B-lines in healthy subjects too but, this was not yet described for PLI and, for more, applying the same scanning protocol to control group should eliminate changes due to anatomic-physical problems. Finally, we used pleural line irregularity evaluation and not B-lines because we consider its evaluation easier and faster than counting B-lines (especially if multiple). Feasibility is indeed really important, especially if you want to apply LUS on a large number of patients (like SpA) on a regular base, during the usual visiting time.
In the present work we aimed at examining a sample of our SpA cohort to understand if LUS could be a useful screening test for ILD to be used in asymptomatic subjects.
As reported in table 1, our SpA patients have quite a long disease duration (15.5±11.5 yrs) and they are not really young (57.8±11.9 yrs), this could be not the optimal population to apply our screening imaging tool (to screen younger/shorter disease duration patients could be more useful for choosing an appropriate therapy) but, up to now, there are no data so, we made a cross-sectional examination to evaluate if this approach could be feasible and useful.
We decided to use Pinal-Fernandez [24] scanning protocol and score system for the evaluation of pleural line irregularity. We made a separate evaluation for distinct areas (anterior, posterior, and lateral) and the posterior part of the chest showed a higher PLI score than the anterior and lateral one (with the latter resulting to be significantly lower than the posterior PLI score) but no significant difference in their correlation with other clinical data was shown. Our data demonstrate a significant higher pleural line irregularity score in SpA patients (19,9 in SpA group vs 10,3 in HS).
Interestingly, we did not find and correlation between therapies and pleural line irregularity (both for csDMARDs and bDMARDs) apart from IL17 inhibitors, but the low number of patients treated with IL17 (n=7) does not allow us to confirm the result as significant. Anyway, this aspect needs larger studies because IL17 could be one of the pro-inflammatory mediators (including IL-17, TNFα and TGF-β) involved in ILD development, as demonstrated in rat models, where both IL17 and TNFα (together with other cytokines) were increased (after bleomycin induction of ILD) in the lung tissue samples after hematoxylin-eosin staining [56]. The possible role of IL-17 in ILD is highlighted in systemic sclerosis patients by the significant increase levels for IL-17A in the patients with ILD compared to controls [57], as well as the positive effect on the fibrotic changes of lung tissues and the improved mechanical pulmonary functions in bleomycin-induced pulmonary fibrosis, that has been shown during the suppression of IL-17 production (through the inhibition of cytokines controlling Th17 differentiation) with theophylline [58]. So, IL17/23 pathway inhibitors could have potential anti-fibrotic effects as shown in some patients [8].
As reported in the more recent literature [59,60,61], and confirmed by Provan et al in a large population [14], we did not find any relationship between ILD and MTX exposure (in our study, MTX treated patients showed lower score with respect to the ones free of MTX, confirming MTX not as a risk factor for ILD).
A possible link between the use of anti-TNF drugs and the presence or progression of ILD was hypothesized and recent evidence have been published on the apparently TNFα inhibitors non-efficacy on controlling/reducing ILD progression with respect other treatment (i.e. abatacept, rituximab) [62,63]. Despite those data, we did not find any significant difference in patients treated with/without TNFα inhibitors, even if we are aware that the low number of subject enrolled does not allow any real conclusion.
Finally, we only had data on exposure and not on duration of the treatments: this could possibly affect the results. Prospective and larger studies (involving more patients) are needed to better evaluate the impact of different treatments on ILD development.
We did not find any correlation between disease duration and pleural line irregularity, confirming the results already reported in the literature for HRCT [6].
The absence of correlation between PROs (LCQ and SGRQ) and pleural line irregularity scores or between SF-36 and LUS is reflecting the possible subclinical phase of ILD in our patients (only few of them presented somewhere a score 2); this means that PROs cannot be used as a screening tool to detect a very early phase of ILD in SpA patients.
We did not notice any significant difference between pleural line irregularity score in AS and PsA so, we could speculate that results already known about ILD in AS can be applied also to PsA.
There was a positive trend in favor of a correlation between pleural line irregularity score and age at the moment of the study that would deserve further investigation.
A significant correlation was found for smoking habits and LUS results (both for actual or previous smoking and for pack/years). The prevalence of smokers resulted to be higher in the SpA groups with respect to HS (62% vs 36%) but, the positive relationship between smoking habits and PLI score was significant in both patients and HS (p<0,003). The strongest correlation between different areas of the lung and PLI irregularity was demonstrated, in both the groups, for anterior chest. Even if we do not have specific data on the impact of smoking on pleural line changes, it is well-known that smoking represents one of the major risk factors for the developing of ILD [64]. We also found a clear significant correlation between smoking habit and mMRC in terms of dyspnea presence (p=0,05) and pack/year (p=0,019).
The weakest point of our study is the low number of patients enrolled (27 AS and 46 PsA), a number that is not sufficient to completely explore such a low prevalence condition as symptomatic ILD in SpA. In addition, HRCT was not used as gold standard comparator because, being our patients and control subjects asymptomatic, there was not a clinical indication to request it. Finally, it would have not been ethical to perform HRCT examination only for scientific purposes. Anyway, as a sort of surrogate, we found a significant correlation between clinical examination (presence of crackles) and PLI score confirming the link between the presence of structural changes (producing crackles) and LUS findings.
Future Research Directions
In the light of the general results we obtained, our study is a proof of concept that demonstrate a possible high prevalence of asymptomatic ILD in SpA patients, suggesting the need of studies on larger groups to confirm our data. Moreover, prospective studies are needed to understand if LUS ILD will ever become symptomatic. Up to now, we already know the high prevalence of symptomatic ILD in RA, a form of chronic arthritis somehow similar to PsA.
LUS resulted to be feasible, not invasive, and potentially useful for screening larger groups of patients. According to the good reliability, between the two trained sonographers, multicenter studies might be possible.
Up to now, we still need a standardization of the technique (i.e. number of intercostal spaces to study, scoring system etc..) and more data on the applicability of LUS for screening purposes and, even more, for the follow-up of patients. The OMERACT is actually working on this topic [27].
Anyway, up to the small knowledge we have now, we still recommend confirming LUS positive result with more standardized techniques (i.e. pulmonary function tests) before sending the patient to the HRCT, which remain the gold standard for a complete assessment of ILD, showing important information on deeper lung structural changes and for the differentiation of specific pattern of ILD (i.e. NSIP or UIP).
Conclusions
This is the first study assessing ILD in SpA patients using LUS. It shows a higher amount of pleural line irregularity in SpA patients with respect to HS so, the real frequency of ILD in SpA could have been underestimated and we need larger studies (possibly prospective) to better understand the real prevalence of ILD in this population and the clinical relevance of it. Smoking habit was the only clinical feature correlated to pleural line irregularity on LUS examination in our population. Future application of LUS could be better addressed at the beginning of the disease then, repeating it on a regular base, in order to achieve a real personalization of SpA treatment according to the early recognition of ILD.
Institutional Review Board Statement
The study protocol has been approved by the local Ethics Committee.
References
- Joy GM, Arbiv OA, Wong CK, et al. Prevalence, imaging patterns and risk factors of interstitial lung disease in connective tissue disease: a systematic review and meta-analysis. Eur Respir Rev. 2023;32:220210. [CrossRef]
- Manfredi A, Sambataro G, Rai A, et al. Prevalence of Progressive Fibrosing Interstitial Lung Disease in Patients with Primary Sjogren Syndrome. J Pers Med. 2024;14(7):708. [CrossRef]
- Wittram C, Mark EJ, McLoud TC. CT-histologic correlation of the ATS/ERS 2002 classification of idiopathic interstitial pneumonias. Radiographics. 2003;23:1057-71. [CrossRef]
- Dai Y, Wang W, Yu Y, Hu S. Rheumatoid arthritis-associated interstitial lung disease: an overview of epidemiology, pathogenesis and management. Clin Rheumatol. 2021;40(4):1211-1220.
- Sampaio-Barros PD, Cerqueira EM, Rezende SM, et al. Pulmonary involvement in ankylosing spondylitis. Clin Rheumatol 2007;26:225-30. [CrossRef]
- El Maghraoui A, Dehhaoui M. Prevalence and Characteristics of Lung Involvement on High Resolution Computed Tomography in Patients with Ankylosing Spondylitis: A Systematic Review. Pulm Med 2012; 2012: 965956. [CrossRef]
- Li X, Kong L, Li F, et al. Association between Psoriasis and Chronic Obstructive Pulmonary Disease: A Systematic Review and Meta-analysis. PloS One 2015;10:e0145221. [CrossRef]
- Kawamoto H, Hara H, Minagawa S, et al. Interstitial Pneumonia in Psoriasis. Mayo Clin Proc Innov Qual Outcomes 2018;2:370-377.
- Ishikawa G, Dua S, Mathur A, et al. Concomitant Interstitial Lung Disease with Psoriasis. Can Respir J 2019;Aug 25;2019:5919304. [CrossRef]
- Peluso R, Iervolino S, Vitiello M, Bruner V, Lupoli G, Di Minno MND. Extra-articular manifestations in psoriatic arthritis patients. Clin Rheumatol 2015;34:745–53. [CrossRef]
- Yue L, Yan Y, Zhao S. A bidirectional two-sample Mendelian randomization study to evaluate the relationship between psoriasis and interstitial lung diseases. BMC Pulm Med 2024;24:330. [CrossRef]
- Bargagli E, Bellisai F, Mazzei MA, et al. Interstitial lung disease associated with psoriatic arthritis: a new disease entity? Intern Emerg Med 2021;16:229–31.
- Schäfer VS, Winter L, Skowasch D, et al. Exploring pulmonary involvement in newly diagnosed rheumatoid arthritis, and psoriatic arthritis: a single center study. Rheumatol Int 2024;44:1975-1986. [CrossRef]
- Provan SA, Ljung L, Kristianslund EK, et al. Interstitial lung disease in rheumatoid or psoriatic arthritis patients initiating biologics, and controls - data from five Nordic registries. J Rheumatol 2024 Sep 1:jrheum.2024-0252.
- Moazedi-Fuerst FC, Kielhauser S, Brickmann K, et al. Sonographic assessment of interstitial lung disease in patients with rheumatoid arthritis, systemic sclerosis and systemic lupus erythematosus. Clin Exp Rheumatol 2015;33:S87-91.
- Gargani L, Romei C, Bruni C, et al. Lung ultrasound B-lines in systemic sclerosis: cut-off values and methodological indications for interstitial lung disease screening. Rheumatol Oxf Engl 2022;61:SI56–64. [CrossRef]
- Foeldvari I, Klotsche J, Hinrichs B, et al. Underdetection of Interstitial Lung Disease in Juvenile Systemic Sclerosis. Arthritis Care Res 2022;74:364–70. [CrossRef]
- Mohammadi A, Oshnoei S, Ghasemi-rad M. Comparison of a new, modified lung ultrasonography technique with high-resolution CT in the diagnosis of the alveolo-interstitial syndrome of systemic scleroderma. Med Ultrason 2014;16:27–31.
- Barskova T, Gargani L, Guiducci S, et al. Lung ultrasound for the screening of interstitial lung disease in very early systemic sclerosis. Ann Rheum Dis 2013;72:390–5. [CrossRef]
- Gargani L, Doveri M, D’Errico L, et al. Ultrasound lung comets in systemic sclerosis: a chest sonography hallmark of pulmonary interstitial fibrosis. Rheumatol Oxf Engl 2009;48:1382–7. [CrossRef]
- Moazedi-Fuerst FC, Kielhauser SM, Scheidl S, et al. Ultrasound screening for interstitial lung disease in rheumatoid arthritis. Clin Exp Rheumatol 2014;32:199–203.
- Moazedi-Fuerst FC, Zechner PM, Tripolt NJ, et al. Pulmonary echography in systemic sclerosis. Clin Rheumatol 2012; 31:1621–5. [CrossRef]
- Sperandeo M, De Cata A, Molinaro F, et al. Ultrasound signs of pulmonary fibrosis in systemic sclerosis as timely indicators for chest computed tomography. Scand J Rheumatol 2015;44:389–98. [CrossRef]
- Pinal-Fernandez I, Pallisa-Nuñez E, Selva-O’Callaghan A, et al. Pleural irregularity, a new ultrasound sign for the study of interstitial lung disease in systemic sclerosis and antisynthetase syndrome. Clin Exp Rheumatol 2015;33:S136-141.
- Sferrazza Papa GF, Pellegrino GM, Volpicelli G, et al. Lung Ultrasound B Lines: Etiologies and Evolution with Age. Respir Int Rev Thorac Dis 2017;94:313–4. [CrossRef]
- Gutierrez M, Soto-Fajardo C, Pineda C, et al. Ultrasound in the Assessment of Interstitial Lung Disease in Systemic Sclerosis: A Systematic Literature Review by the OMERACT Ultrasound Group. J Rheumatol 2020;47:991–1000. [CrossRef]
- Delle Sedie A, Terslev L, Bruyn G.A.W., Cazenave T, Chrysidis S, Diaz M et al. Standardization of Interstitial Lung Disease Assessment by Ultrasound: Results from a Delphi Process and Web-reliability exercise by the OMERACT Ultrasound Working Group. Semin Arthritis Rheum. 2024;65:152406.
- Tardella M, Gutierrez M, Salaffi F, Carotti M, Ariani A, Bertolazzi C, et al. Ultrasound in the assessment of pulmonary fibrosis in connective tissue disorders: correlation with high-resolution computed tomography. J Rheumatol. 2012;39:1641-7. [CrossRef]
- Gutierrez M, Salaffi F, Carotti M, Tardella M, Pineda C, Bertolazzi C, et al. Utility of a simplified ultrasound assessment to assess interstitial pulmonary fibrosis in connective tissue disorders--preliminary results. Arthritis Res Ther. 2011;13:R134. [CrossRef]
- Di Carlo M, Tardella M, Filippucci E, Carotti M, Salaffi F. Lung ultrasound in patients with rheumatoid arthritis: definition of significant interstitial lung disease. Clin Exp Rheumatol. 2022;40:495-500. [CrossRef]
- Buda N, Piskunowicz M, Porzezińska M, Kosiak W, Zdrojewski Z. Lung ultrasonography in the evaluation of interstitial lung disease in systemic connective tissue diseases: criteria and severity of pulmonary fibrosis – analysis of 52 patients. Ultraschall Med. 2016;37:379–85. [CrossRef]
- Gigante A, Rossi Fanelli F, Lucci S, Barilaro G, Quarta S, Barbano B, et al. Lung ultrasound in systemic sclerosis: correlation with high-resolution computed tomography, pulmonary function tests and clinical variables of disease. Intern Emerg Med. 2016;11:213–17. [CrossRef]
- Delle Sedie A, Doveri M, Frassi F, Gargani L, D’Errico G, Pepe P, et al. Ultrasound lung comets in systemic sclerosis: a useful tool to detect lung interstitial fibrosis. Clin Exp Rheumatol. 2010;28:S54.
- Gutierrez J, Gutierrez M, Almaguer K, Gonzalez F, Camargo K, Soto C, et al. Ultrasound diagnostic and predictive value of interstitial lung disease in systemic sclerosis. Diagnostic and predictive value of ultrasound in the assessment of interstitial lung disease. Ann Rheum Dis. 2018;77:121. [CrossRef]
- Vicente-Rabaneda EF, Bong DA, Busquets-Pérez N, Möller I. Ultrasound evaluation of interstitial lung disease in rheumatoid arthritis and autoimmune diseases. Eur J Rheumatol. 2022 Aug 9. [CrossRef]
- Pinal Fernández I, Pallisa Núñez E, Selva-O'Callaghan A, Castella-Fierro E, Martínez-Gómez X, Vilardell-Tarrés M. Correlation of ultrasound B-lines with high-resolution computed tomography in antisynthetase syndrome. Clin Exp Rheumatol. 2014;32:404-7.
- Buda N, Masiak A, Zdrojewski Z. Utility of lung ultrasound in ANCA-associated vasculitis with lung involvement. PLoS One. 2019;14:e0222189. [CrossRef]
- Buda N, Wojteczek A, Masiak A, Piskunowicz M, Batko W, Zdrojewski Z. Lung Ultrasound in the Screening of Pulmonary Interstitial Involvement Secondary to Systemic Connective Tissue Disease: A Prospective Pilot Study Involving 180 Patients. J Clin Med. 2021;10:4114. [CrossRef]
- Gasperini ML, Gigante A, Iacolare A, Pellicano C, Lucci S, Rosato E. The predictive role of lung ultrasound in progression of scleroderma interstitial lung disease. Clin Rheumatol. 2020;39:119-123. [CrossRef]
- Gargani L, Bruni C, Romei C, Frumento P, Moreo A, Agoston G, et al. Prognostic Value of Lung Ultrasound B-Lines in Systemic Sclerosis. Chest. 2020;158:1515-1525. [CrossRef]
- Tardella M, Di Carlo M, Carotti M, Filippucci E, Grassi W, Salaffi F. Ultrasound B-lines in the evaluation of interstitial lung disease in patients with systemic sclerosis: Cut-off point definition for the presence of significant pulmonary fibrosis. Medicine (Baltimore). 2018;97:e0566. [CrossRef]
- Hassan RI, Lubertino LI, Barth MA, Quaglia MF, Montoya SF, Kerzberg E, et al. Lung Ultrasound as a Screening Method for Interstitial Lung Disease in Patients With Systemic Sclerosis. J Clin Rheumatol. 2019;25:304-307. [CrossRef]
- Bruni C, Mattolini L, Tofani L, Gargani L, Landini N, Roma N, et al. Lung Ultrasound B-Lines in the Evaluation of the Extent of Interstitial Lung Disease in Systemic Sclerosis. Diagnostics (Basel). 2022;12:1696. [CrossRef]
- Huang Y, Liu T, Huang S, Qiu L, Luo F, Yin G, et al. Screening value of lung ultrasound in connective tissue disease related interstitial lung disease. Heart Lung. 2023;57:110-116. [CrossRef]
- Reyes-Long S, Gutierrez M, Clavijo-Cornejo D, Alfaro-Rodríguez A, González-Sámano K, Cortes-Altamirano JL, et al. Subclinical Interstitial Lung Disease in Patients with Systemic Sclerosis. A Pilot Study on the Role of Ultrasound. Reumatol Clin (Engl Ed). 2021;17:144-149. [CrossRef]
- Wang Y, Chen S, Lin J, Xie X, Hu S, Lin Q, et al. Lung ultrasound B-lines and serum KL-6 correlate with the severity of idiopathic inflammatory myositis-associated interstitial lung disease. Rheumatology (Oxford). 2020;59:2024-2029. [CrossRef]
- Buda N, Piskunowicz M, Porzezińska M, Kosiak W, Zdrojewski Z. Lung Ultrasonography in the Evaluation of Interstitial Lung Disease in Systemic Connective Tissue Diseases: Criteria and Severity of Pulmonary Fibrosis – Analysis of 52 Patients Lungensonografie zur Bewertung von interstitiellen Lungenerkrankungenbei. Ultraschall der Medizin. 2016;37:379–85.
- Reissig A, Kroegel C. Transthoracic sonography of diffuse parenchymal lung disease: the role of comet tail artifacts. J Ultrasound Med. 2003;22:173–80.
- Rudwaleit M, van der Heijde D, Landewé R, et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part II): validation and final selection. Ann Rheum Dis. 2009;68:777–83. [CrossRef]
- Taylor W, Gladman D, Helliwell P, et al. Classification criteria for psoriatic arthritis: development of new criteria from a large international study. Arthritis Rheum. 2006;54: 2665–73. [CrossRef]
- Ward N. The Leicester Cough Questionnaire. J Physiother. 2016;62:53. [CrossRef]
- Jones PW, Quirk FH, Baveystock CM. The St George’s Respiratory Questionnaire. Respir Med. 1991;85 Suppl B:25–31; discussion 33-37.
- Mahler DA, Wells CK. Evaluation of clinical methods for rating dyspnea. Chest. 1988;93: 580–6. [CrossRef]
- Shrout P.E., Fleiss J.L. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979;86: 420-8.
- Fragoulis GE, Nikiphorou E, Larsen J, Korsten P, Conway R. Methotrexate-Associated Pneumonitis and Rheumatoid Arthritis-Interstitial Lung Disease: Current Concepts for the Diagnosis and Treatment. Front Med (Lausanne). 2019;6:238. [CrossRef]
- Feng Y, Dai L, Zhang Y, et al. Buyang Huanwu Decoction alleviates blood stasis, platelet activation, and inflammation and regulates the HMGB1/NF-κB pathway in rats with pulmonary fibrosis. J Ethnopharmacol. 2024;319:117088.
- Amira G, Akram D, Fadoua M, et al. Imbalance of TH17/TREG cells in Tunisian patients with systemic sclerosis. Presse Med. 2024;53:104221.
- Park SJ, Hahn HJ, Oh SR, Lee HJ. Theophylline Attenuates BLM-Induced Pulmonary Fibrosis by Inhibiting Th17 Differentiation. Int J Mol Sci. 2023;24:1019. [CrossRef]
- Kim JW, Chung SW, Pyo JY, et al. Methotrexate, leflunomide and tacrolimus use and the progression of rheumatoid arthritis-associated interstitial lung disease. Rheumatology (Oxford). 2023;62:2377-2385. [CrossRef]
- Kim K, Woo A, Park Y, et al. Protective effect of methotrexate on lung function and mortality in rheumatoid arthritis-related interstitial lung disease: a retrospective cohort study. Ther Adv Respir Dis. 2022;16:17534666221135314. [CrossRef]
- Dawson JK, Quah E, Earnshaw B, Amoasii C, Mudawi T, Spencer LG. Does methotrexate cause progressive fibrotic interstitial lung disease? A systematic review. Rheumatol Int. 2021;41:1055-1064. [CrossRef]
- Kelly CA, Nisar M, Arthanari S, et al. Rheumatoid arthritis related interstitial lung disease - improving outcomes over 25 years: a large multicentre UK study. Rheumatology (Oxford). 2021;60:1882-1890. [CrossRef]
- Carrasco Cubero C, Chamizo Carmona E, Vela Casasempere P. Systematic review of the impact of drugs on diffuse interstitial lung disease associated with rheumatoid arthritis. Reumatol Clin (Engl Ed). 2021;17:504-513.
- Margaritopoulos GA, Vasarmidi E, Jacob J, Wells AU, Antoniou KM. Smoking and interstitial lung diseases. Eur Respir Rev. 2015;24:428–35.
Figure 1.
PLI scoring system.
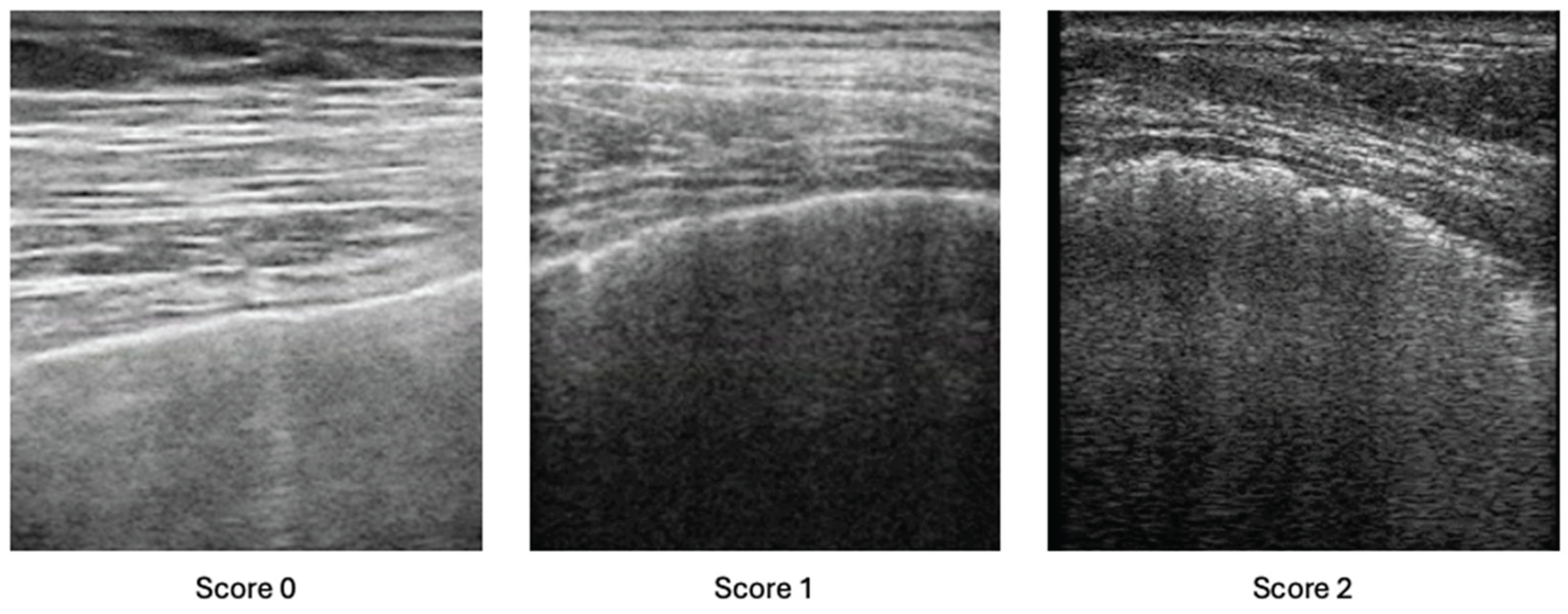
Figure 2.
PLI score for different areas in HS, PsA and AS groups.
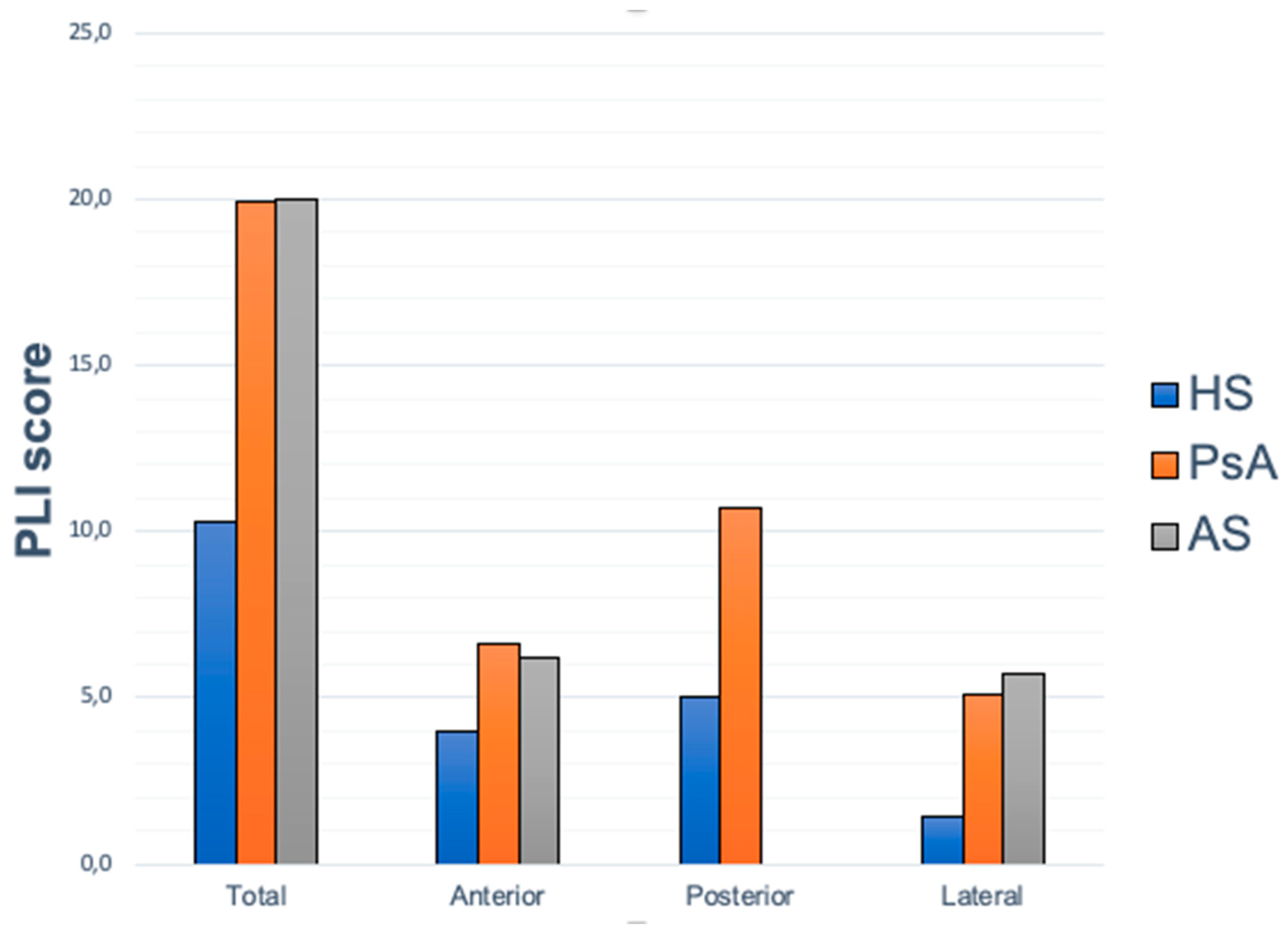
Figure 3.
PLI score in different areas, according to the exposition to MTX.
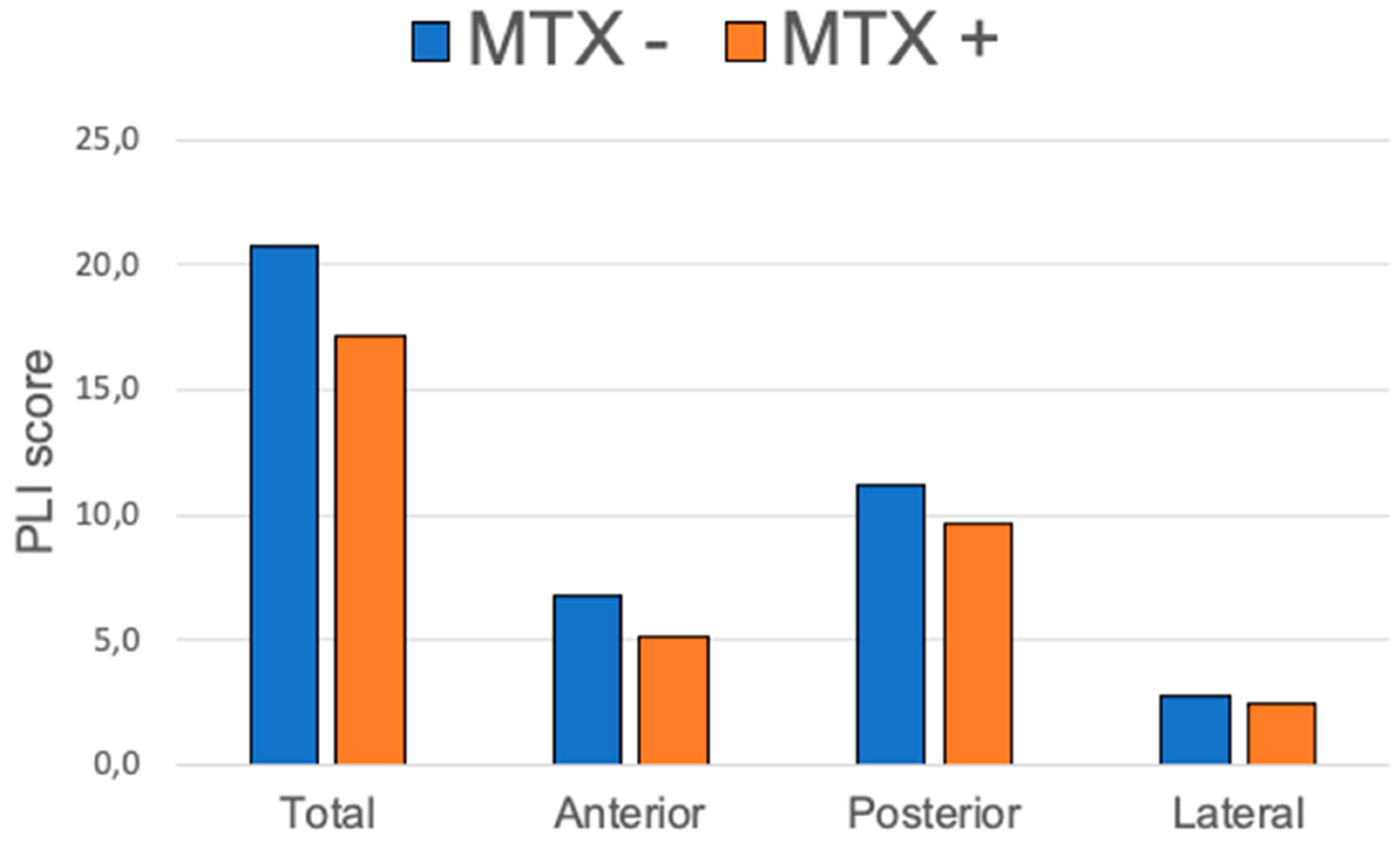

Table 1.
Demographic and clinical characteristics of subjects enrolled in the study.
| PsA+AS (n=73) | HS (n=56) | PsA (n=46) | AS (n=27) | |
| M | 38 (52.1%) | 30 | 25 (54.4%) | 14 (51.9%) |
| F | 35 (47.9%) | 26 | 21 (45.6%) | 13 (48.1%) |
| Age (±SD) | 57.8 (11.9) | 56 (15.6) | 58.8 (12.3) | 56.1 (11.4) |
| BMI (±SD) | 26.2 (4) | 24.4 (2.8) | 26.8 (4.1) | 24.7 (3.5) |
| Smoke habits (%) | 26 (35.6%) | 20 (35.7%) | 15 (32.6%) | 11 (40.7%) |
| Disease duration, yrs (±SD) | 15.5 (11.5) | ------- | 14.9 (10.6) | 16.4 (13.5) |
| ASDAS (±SD) | ------- | ------- | ------- | 2.2 (1.4) |
| DAPSA (±SD) | ------- | ------- | 14.1 (10.5) | ------- |
| Psoriasis | 42 | ------- | 42 | 0 |
| TNFa inhibitors, N (%) | 10 (13.7) | ------- | 23 (50) | 22 (81.5) |
| Other bDMARDs, N (%) | 10 (13.7) | ------- | 9 (19.6) | 1 (3.7%) |
| csDMARDs (all), N (%) | 30 (41.1) | ------- | 23 (50) | 7 (25.9) |
| csDMARDs (MTX), N (% csDMARDs) | 18 (60) | ------- | 14 (60.1) | 4 (57.1) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



