Submitted:
02 July 2025
Posted:
03 July 2025
You are already at the latest version
Abstract
The trunk of Henle (TH) and the posterosuperior pancreaticoduodenal vein, also known as Belcher’s Vein (BV), are important anatomical landmarks within the portomesenteric vascular anatomy during robot-assisted pancreatoduodenectomy. A detailed understanding of these veins is necessary for the safe and effective resection in the robotic approach for oncological surgery of the pancreatic head and uncinate process. This technical note describes in detail the stepwise approach to use these veins as reference landmarks during robot-assisted pancreatoduodenectomy. This methodology may improve the dissection precision, reduce the vascular injury risk, and enhance the oncological outcomes.
Keywords:
gastrocolic trunk of henle
; robotic pancreaticoduodenectomy
; surgical vascular anatomy
Introduction
Robot-assisted pancreatoduodenectomy (RAPD) is a complex procedure because of the necessary dissection near major vascular structures and multiple reconstructions [1], which can lead to significant morbidity. Outcome of RAPD has improved in recent years despite a long learning curve without a negative effect on 90-day mortality [2]. However, the robotic approach has helped overcome some of the laparoscopic challenges by improving precision and exposure, but also because of the ability of wrist movements, improved 3-dimensional vision, and simplifying the instrument movements [1,2,3,4]. The superior mesenteric vein (SMV) and its arterial counterpart, the superior mesenteric artery (SMA), have complex three-dimensional anatomy with variable vascular patterns [5].
Accurate understanding of surgical anatomy and correct identification of blood vessels are important during RAPD. The trunk of Henle (TH) connects the right gastro-pancreato-colic vein and middle colic vein with the SMV [6].
Described by Cameron and Belcher as the posterosuperior pancreaticoduodenal vein (PSPDV), the Belcher’s Vein (BV) forms part of the venous drainage of the head of the pancreas and is a major tributary to the portal vein (PV), which highlights the importance of identification during the uncinate process dissection of a Whipple’s procedure. This vein was named after a Cameron’s assistant: “ironically due to its description of being short, fat, and always getting in the way” [7].
The TH and BV are reliable venous landmarks that assist surgeons during robotic procedures for safer navigation of the pancreas head and uncinate process region. Identifying and controlling these veins is essential for safe mobilization of the pancreatic head and uncinate process from the PV. This technical note describes a stepped methodology to perform the RAPD.
Surgical Resection Technique
Patient Selection and Positioning
Patient suitability for RPD during the learning curve of 80-100 procedures is considered with BMI<35 kg/m2 and signs of chronic and necrotizing pancreatitis and no vascular contact. The patient is placed 10º in reverse Trendelenburg position. The robot arm is docked from the right of the patient. Closed 12mmHg pneumoperitoneum is achieved through Veress needle at Palmer’s point. Trocar placement is shown in Figure 1, these are marked after insufflation is completed. T2, is marked 11.5cm from the costal margin at the gallbladder on a line ending 2cm on the patient right from the umbilicus. Hereafter, T2 and T4 trocars are marked following a horizontal line, T1 is place slightly more cranial. One or two laparoscopic ports for the table side surgeon are placed 7cm from T2, T3, and T4. The first trocar place is the patient right sided laparoscopic ports whereafter all trocars are place under direct vision.
Stepwise Dissection Approach
The dissection begins by dividing the gastrocolic ligament to access the lesser sac, proceeding laterally to the short gastric vessels on the left, and medially to expose the first part of the duodenum to the right. Alternatively, the first step is the Treitz dissection.
The right colonic flexure is widely mobilized to expose the duodenum, superior mesenteric vein (SMV), and the pancreatic head, following with a complete Kocher maneuver to detach the pancreatic head from the retroperitoneum, down to the left side of the aorta, and exposing the interaortocaval lymph nodes, the left renal vein and the origin of the SMA.
The proximal jejunum is exposed over the right side of the transverse colon and the first jejunal loop, divided with 60mm white reload robotic Endostapler, and dissected to the mesenteric root, taking the Treitz ligament as well. The specimen is then rotated 270º clockwise and uncrossed posteriorly to the mesenteric root, retrieving it from the right upper quadrant. This maneuver mobilizes the first jejunal loop and the third and fourth portions of the duodenum by transposing the duodenum and proximal jejunum to the right of the SMV–SMA axis in the coronal plane. This positioning is key for a safe and effective dissection of the uncinate process and the SMV.
Depending on the type of robotic approach, whether robotic-assisted or fully robotic [3] (defined as the complete use of the robotic technique for PD, including resection and reconstruction, without laparoscopic or hand-assisted techniques, but including the use of laparoscopic ports by a table side surgeon, which is regarded as standard), the hilar lymphadenectomy may be performed prior to the duodenal uncrossing or after to it. In both approaches, the final resective step during a RAPD is the uncinate process dissection from the SMV, once the specimen has been collected on the right upper quadrant, in order to take full control of the PV/SMV vascular axis, as a key milestone before starting to spare the uncinate process.
Once the minor omentum is opened above, the posterior wall of the stomach is dissected, and the right gastric artery an the right gastroepiploic vessels have been transected using locking clips and an energy device, the antrum of the stomach is divided with a 60mm blue reload robotic Endostapler just upstream to the pylorus to improve access to the pancreas and allow exposure of the suprapancreatic lymph nodes and hepatic hilum, taking the right gastric artery to its origin, and performing the lymphadenectomy from level 8A, upwards to the hilar plate.
The gastroduodenal artery (GDA) is dissected, vessel loop surrounded, clipped, and ligated with 2/0 silk prior to its mechanical transection with 30mm white reload robotic Endostapler for a secure vascular control, leading to the exposition of the common, proper, right and left hepatic arteries and bile duct.
Although not considered the default technique in RAPD, the pylorus-preserving PD (PPPD) has been also described. In this case, the right gastroepiploic arcade must be identified and preserved to maintain adequate blood supply to the pylorus [1].
Once the superior and inferior limits of the pancreas neck have been dissected, a tunnel is created between the posterior surface of the pancreatic neck and the anterior aspect of the PV. After hanging the pancreas neck with a loop, the neck is incised with monopolar curved scissors, identifying and dividing the main pancreatic duct with a ‘cold cut’ to prevent occlusion or stenosis of the pancreatic duct.
As the duodenum specimen is successfully right uncrossed, a slight countertraction using robot arm 1 next to the gastroepiploic locking clip on the specimen side facilitates a safe uncinate process dissection, by simplifying the torsional position between the duodenum and the SMA/SMV axis. In this step, it is essential to properly identify and manage the two major key venous landmarks.
Trunk of Henle (TH)
The TH is found in 86.9% of people [6]. It is usually found at the lower border of the pancreas, close to the pancreatic head, between the lower border of the pancreas and extends up to 20 mm downward along the front-right side of the superior mesenteric vein (SMV) [14]. The TH drains directly into the superior mesenteric vein (SMV). The most frequent branches from the pancreas and colon are the anterior superior pancreaticoduodenal vein (ASPDV), seen in 88.3% of patients, and the superior right colic vein (SRCV), seen in 82.5% of patients [6]. The average diameter of the trunk is 4.2 mm. (Figure 2). Identifying this structure and performing careful monopolar scissor dissection are important to obtain enough vascular buds before looping it and placing the 30mm white reload robotic Endowrist® mechanical stapler or locked clips to ensure good surgical results. This process is greatly facilitated by countertraction of arm 1 next to the locking clip of the gastroepiploic vessels as it creates some tension and allows for better visualization of the TH.
Belcher’s Vein (BV)
Identified during the pancreatic head dissection, this vein is a consistent tributary of the PV, becoming a major landmark during this step. A consistent tributary to the PV, the BV is present in 90% of patients [7,11,16]. It joins the right posterolateral wall of the PV, usually within 1 cm of the splenic vein–portal vein (SV–PV) confluence [7]. BV transection should be performed using a locked or metal clip (Figure 3), allowing safe exposure of the PV and SMV, thereby opening the posterior hilar portal confluence, and completing the 360º PV dissection, thus ending the pancreas head mobilization. Ideally, BV transection is postponed until all SMA branches have been transected to prevent venous congestion in the pancreatic head.
After completing the PV dissection, the common bile duct (CBD) is clamped proximally upstream to the cystic duct with a bulldog, before being transected with monopolar scissors. The gallbladder and the remaining surgical Whipple specimen are taken in-bloc, and removed in a specimen retrieval bag via Pfannenstiel incision.
Discussion
The uncinate process dissection is known to be the most technically challenging step in minimally invasive approach, due to the small and posterior collaterals arising from the SMV. During the uncinate process resection, the correct exposure of the SMV is essential [8]. The dissection proceeds from caudal to cranial, along the SMV-PV axis. Small venous branches from the PV, SMV, and SMA must be carefully identified, dissected, and divided, but the risk of bleeding from variant collaterals remains significant [9]. Especially for SMA branches clips are advised. Although which factors are related to the lower conversion rates to open in RAPD versus laparoscopic approach [10] remains unclear, it is reasonable to argue that the major advantage of the 7 degrees of movement of the robotic tooltips may be determinant to the successful vascular control and avoidance of bleeding-related not-programmed conversions.
This way, it is essential to know the anatomical variations of the SMA/SMV collaterals. A comprehensive description of these structures is essential for surgical planning and intraoperative navigation. Nevertheless, standard surgical textbooks often lack a detailed description of the tributaries of the SMV and PV [7,8] which are paramount for the safe planning and performance of the RAPD [7,8,11].
Several veins, particularly those draining the uncinate process and proximal jejunum, require careful dissection and ligation. In some cases, ligation may be required to achieve adequate exposure and control of the SMV and its tributaries, or to manage bleeding risks [12,13].
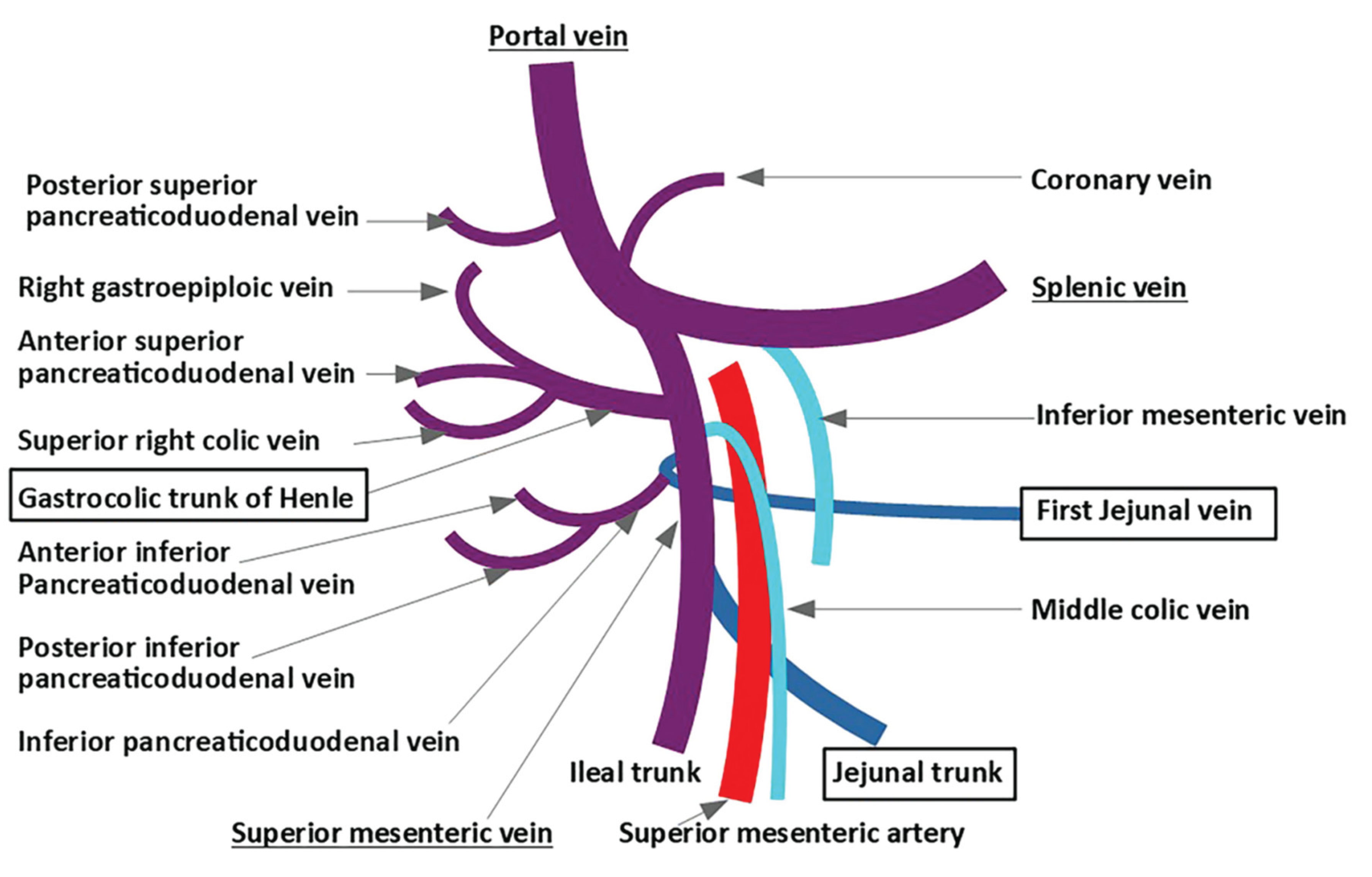
On one hand, TH must be differentiated from the first jejunal vein. Despite frequent anatomical variations in the venous outflow of the uppermost jejunum, a common configuration, known as the jejunal trunk (JT), may occur when a shared trunk arises from the confluence of the IPDV and the first jejunal vein (FJV), or the first jejunal trunk (FJT), when both FJV and the second jejunal vein (SJV) join to drain this territory [15]. The FJV is a major PV tributary draining the proximal jejunum, often receiving the inferior pancreaticoduodenal vein (IPDV). The FJV/JT is a major vein draining into the portal system, running close to the SMA [7]. It maintains venous drainage of the proximal jejunum and often lies posterior to it [5,15]. The FJV/JT typically receives tributaries from the IPDV, which serves as the primary drainage vein for the uncinate process [6]. Moreover, the FJV/JT may course either above or below the TH, and may vary its position relative to the SMA: anterior in 20-26% of cases and posterior in 71,8- 80% (5,6,10,11)(Figure 4). Since the jejunal vein itself should not be cut during a Whipple, it is crucial to differentiate it from the TH.
On the other hand, The BV is a valuable anatomical landmark during the final step of the uncinate process dissection. (Figure 3) Duodenojejunal uncrossing allows a safer and more direct access to key vascular structures, including TH, IPDV, and small pancreatic tributaries [17]. Thus, preserving the FJV/JT enables the safe dissection around the SMA/SMV axis from the mesenterium root [8,18].
As such, the TH and VB are key landmarks to obtain a safer resection plane and exposure of the SMV and PV [12,13]. Accurate identification and secure vascular control contribute to a standardized and reproducible dissection during robotic-assisted pancreaticoduodenectomy (RAPD). Importantly, the routine use of staplers is not mandatory; effective hemostasis can be achieved using a Hem-o-lok clip for Henle’s trunk and a metal clip for the vein of Belcher, in combination with energy devices.
As robotic surgery improves the augmented visualization and precision of dissection, the better handling of the TH, FJV/JT and BV can be achieved more precisely, leading to a more structured and systematized dissection, compared with open or laparoscopic approaches. These findings support those of previous anatomical studies and emphasize the importance of using these venous landmarks [19].
Conclusion
The TH and BV are critical anatomical landmarks during RAPD. Their identification and proper dissection is key for safe ligation, and to reduce the risk of bleeding and need for conversion. This approach will also be instrumental in improving an optimal oncological outcomes linked to the robotic assisted minimally invasive approach during pancreatic head and uncinate process resection.
References
- Giulianotti PC, Mangano A, Bustos RE, Gheza F, Fernandes E, Masrur MA, et al. Operative technique in robotic pancreaticoduodenectomy (RPD) at University of Illinois at Chicago (UIC): 17 steps standardized technique. Surg Endosc. 2018;32(10):4329–36.
- Jones LR, Zwart MJW, de Graaf N, Wei K, Qu L, Jiabin J, et al. Learning curve stratified outcomes after robotic pancreatoduodenectomy: International multicenter experience. Surgery. 2024 Dec;176(6):1721–9.
- Cugat Andorrà E, Cremades Perez M, Navinés López J, Matallana Azorín C, Zárate Pinedo A, Pardo Aranda F, et al. Challenge and future of liver and pancreatic robotic surgery. Analysis of 64 cases in a specialized unit. Cir Esp (Engl Ed). 2022 Mar;100(3):154–60.
- Giulianotti PC, Sbrana F, Bianco FM, Elli EF, Shah G, Addeo P, et al. Robot-assisted laparoscopic pancreatic surgery: single-surgeon experience. Surg Endosc. 2010 Jul 1;24(7):1646–57.
- Negoi I, Beuran M, Hostiuc S, Negoi RI, Inoue Y. Surgical Anatomy of the Superior Mesenteric Vessels Related to Pancreaticoduodenectomy: a Systematic Review and Meta-Analysis. J Gastrointest Surg. 2018 May;22(5):802–17.
- Stefura T, Kacprzyk A, Droś J, Pędziwiatr M, Major P, Hołda MK. The venous trunk of henle (gastrocolic trunk): A systematic review and meta-analysis of its prevalence, dimensions, and tributary variations. Clin Anat. 2018 Nov;31(8):1109–21.
- Negoi I, Beuran M, Hostiuc S, Negoi RI, Inoue Y. Response of the Authors to the Letter of the Editor Surgical Anatomy of the Superior Mesenteric Vessels Related to Pancreaticoduodenectomy: a Systematic Review and Meta-Analysis. J Gastrointest Surg. 2018 Aug 1;22(8):1457–1457.
- Katz MHG, Fleming JB, Pisters PWT, Lee JE, Evans DB. Anatomy of the Superior Mesenteric Vein With Special Reference to the Surgical Management of First-order Branch Involvement at Pancreaticoduodenectomy. Annals of Surgery. 2008 Dec;248(6):1098–102.
- Toya K, Tomimaru Y, Kobayashi S, Sasaki K, Iwagami Y, Yamada D, et al. Investigation of the variation of vessels around the pancreatic head based on the first jejunal vein anatomy at pancreaticoduodenectomy. Langenbecks Arch Surg. 2023 Aug 28;408(1):340.
- Klompmaker S, van Hilst J, Wellner UF, Busch OR, Coratti A, D’Hondt M, et al. Outcomes After Minimally-invasive Versus Open Pancreatoduodenectomy: A Pan-European Propensity Score Matched Study. Annals of Surgery. 2020 Feb;271(2):356.
- Pran L, Baijoo S, Dan D, Maharaj R. The Vein of Belcher: Revisited. J Gastrointest Surg. 2018 Jul 1;22(7):1303–4.
- AlMasri S, Kraftician J, Zureikat A, Paniccia A. Management of Intra-Operative Hemorrhage and Safe Venous Resection in Robotic-Assisted Pancreaticoduodenectomy: Techniques to Avoid Open Conversion. J Gastrointest Surg. 2023 Aug;27(8):1753–6.
- Bruna CL, Emmen AMLH, Wei K, Sutcliffe RP, Shen B, Fusai GK, et al. Effects of Pancreatic Fistula After Minimally Invasive and Open Pancreatoduodenectomy. JAMA Surg. 2025 Feb 1;160(2):190–8.
- Negoi I, Beuran M, Hostiuc S, Negoi RI, Inoue Y. Surgical Anatomy of the Superior Mesenteric Vessels Related to Colon and Pancreatic Surgery: A Systematic Review and Meta-Analysis. Sci Rep. 2018 Mar 8;8(1):4184.
- Desai G, Wagle PK. First jejunal vein, jejunal trunk, and pancreatico-duodenectomy: resolving the literature conundrum. Langenbecks Arch Surg. 2023 Feb 24;408(1):104.
- Cirocchi R, Matteucci M, Randolph J, Boselli C, Davies J, Scarselletti G, et al. Anatomical Variants of the Jejunal Veins and Their Technical Implications in Pancreaticoduodenectomy: A Systematic Review and Meta-Analysis. Dig Surg. 2024;41(5–6):245–55.
- Nagakawa Y, Hosokawa Y, Sahara Y, Takishita C, Hijikata Y, Osakabe H, et al. Approaching the superior mesenteric artery from the right side using the proximal-dorsal jejunal vein preisolation method during laparoscopic pancreaticoduodenectomy. Surg Endosc. 2018 Sep 1;32(9):4044–51.
- Kang MJ, Han SS, Park SJ, Park HM, Kim SW. Do jejunal veins matter during pancreaticoduodenectomy? Ann Hepatobiliary Pancreat Surg. 2022 Aug 31;26(3):229–34.
- Miyazawa M, Kawai M, Hirono S, Okada K ichi, Shimizu A, Kitahata Y, et al. Preoperative evaluation of the confluent drainage veins to the gastrocolic trunk of Henle: understanding the surgical vascular anatomy during pancreaticoduodenectomy. Journal of Hepato-Biliary-Pancreatic Sciences. 2015;22(5):386–91.
Figure 1.
Trocar placement during RAPD. T2 is marked 11.5 cm from the costal margin and 2 cm right of the umbilicus; T3 and T4 are aligned horizontally, with T1 placed slightly cranial. Assistant ports(A) are placed 7 cm from T2, T3, and T4 under direct vision.
Figure 1.
Trocar placement during RAPD. T2 is marked 11.5 cm from the costal margin and 2 cm right of the umbilicus; T3 and T4 are aligned horizontally, with T1 placed slightly cranial. Assistant ports(A) are placed 7 cm from T2, T3, and T4 under direct vision.
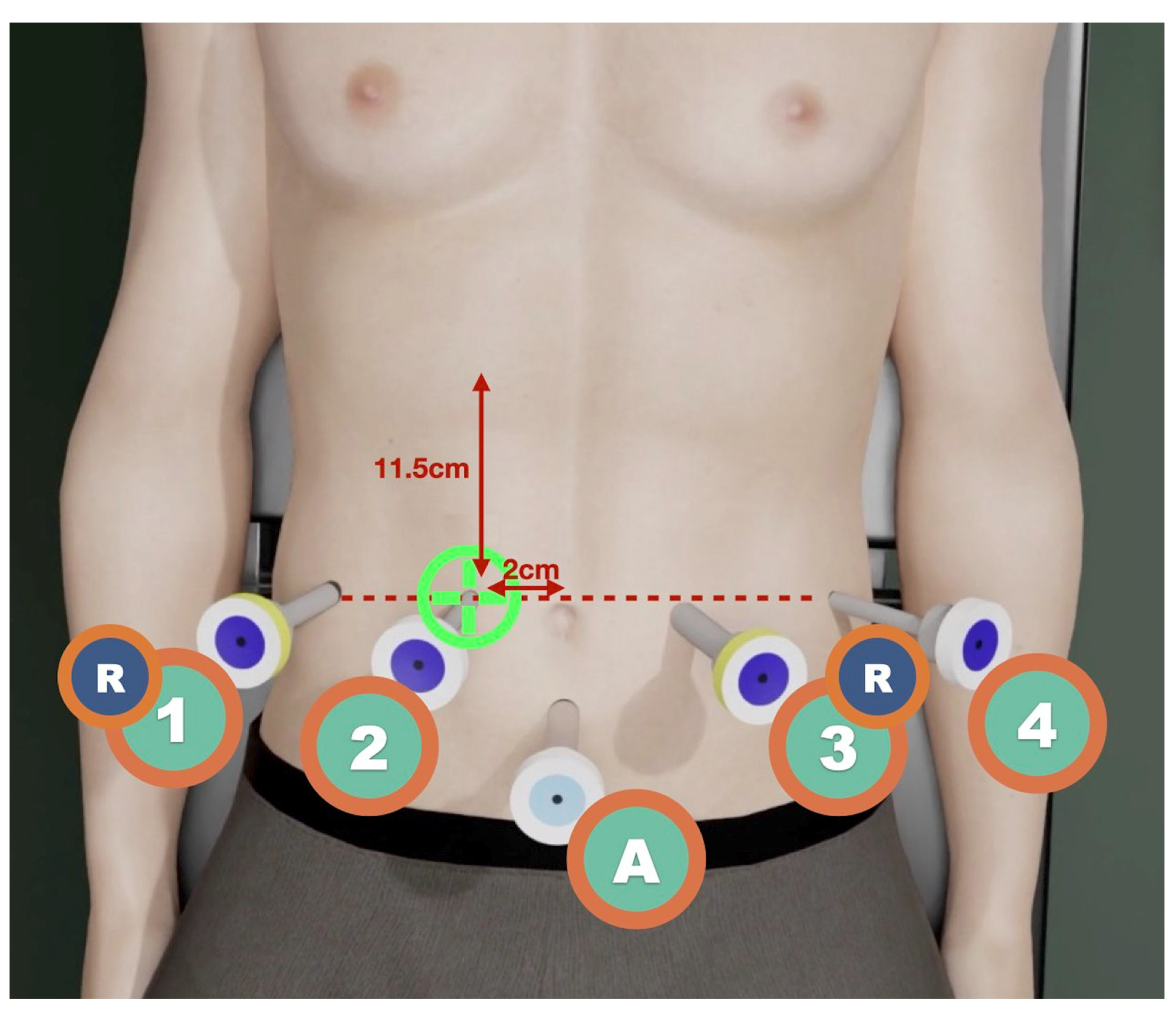
Figure 2.
Intraoperative view during uncinate process resection. The trunk of Henle(HT) is isolated using a vessel loop for vascular control and divided using a Hem-o-lok clip.
Figure 2.
Intraoperative view during uncinate process resection. The trunk of Henle(HT) is isolated using a vessel loop for vascular control and divided using a Hem-o-lok clip.
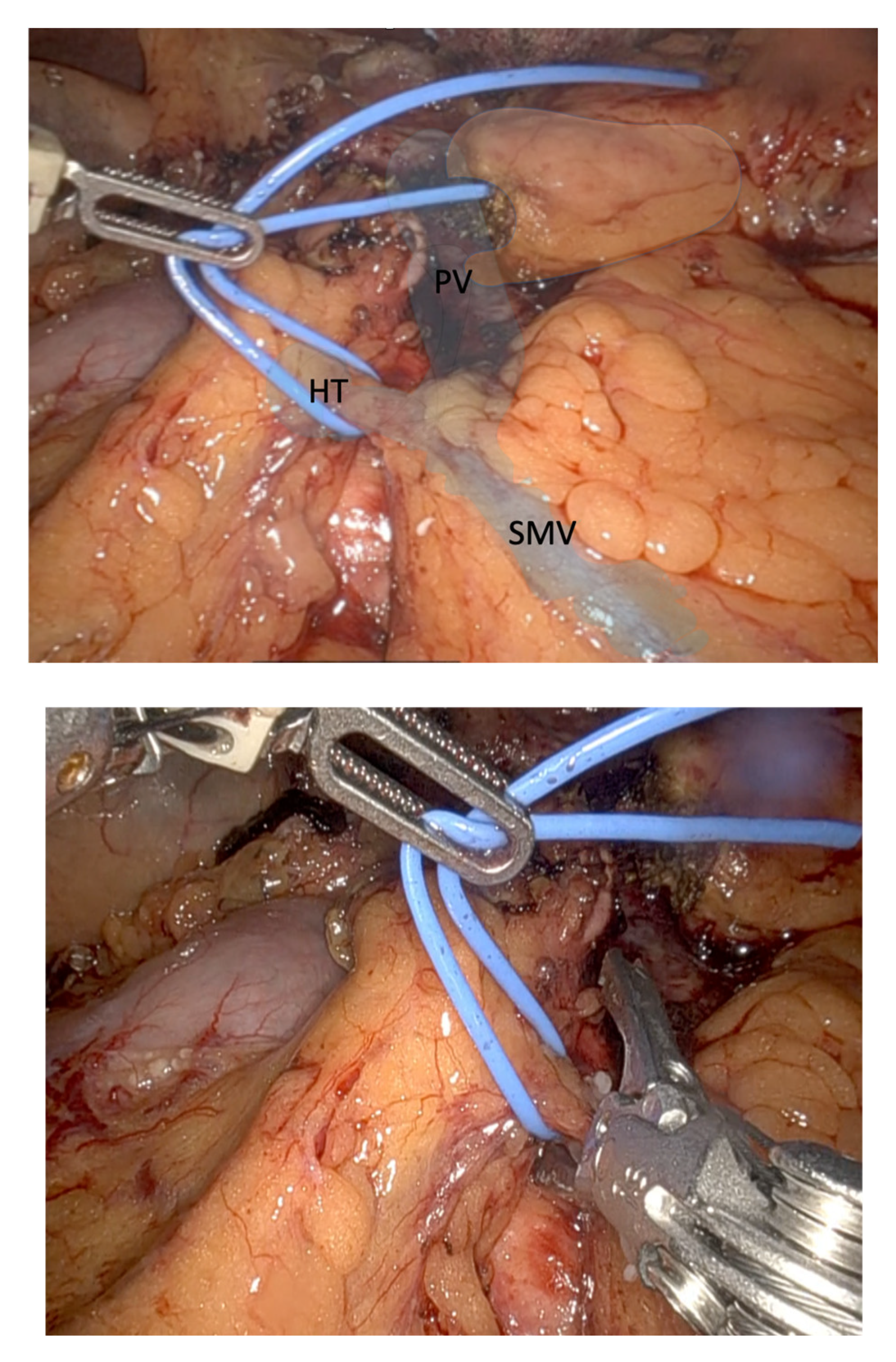
Figure 3.
The posterosuperior pancreaticoduodenal vein, also referred to as Belcher’s vein, is isolated using a vessel loop. A Hem-o-lok clip is applied to achieve vascular control. The portal vein (PV), superior mesenteric vein (SMV) and Belcher’s vein (BV) were identified.
Figure 3.
The posterosuperior pancreaticoduodenal vein, also referred to as Belcher’s vein, is isolated using a vessel loop. A Hem-o-lok clip is applied to achieve vascular control. The portal vein (PV), superior mesenteric vein (SMV) and Belcher’s vein (BV) were identified.
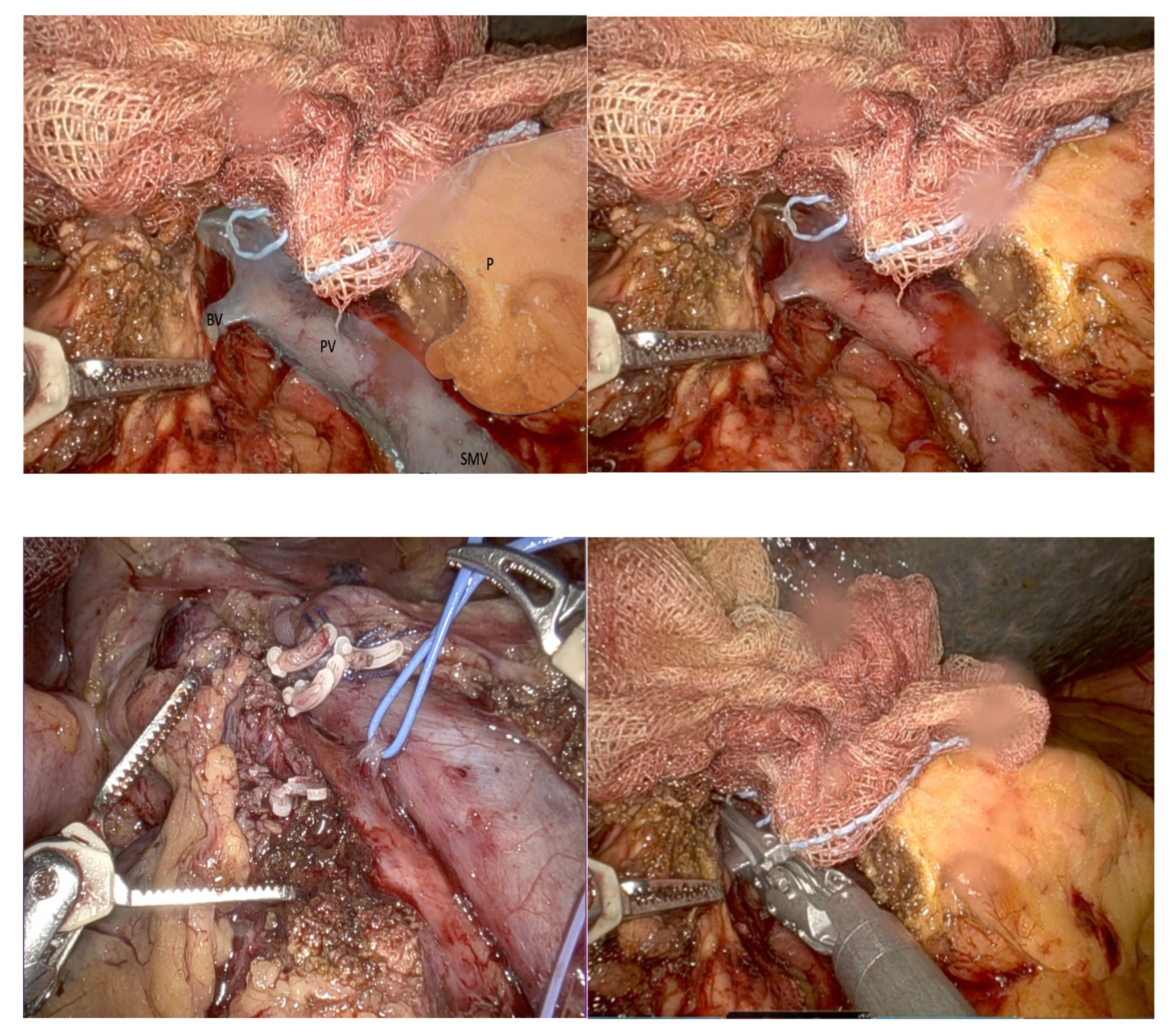
Figure 4.
Key tributaries of portal vein, Belcher’s vein and superior mesenteric vein taken from Desai et al. [15].
Figure 4.
Key tributaries of portal vein, Belcher’s vein and superior mesenteric vein taken from Desai et al. [15].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



