
Submitted:
01 July 2025
Posted:
02 July 2025
You are already at the latest version
Abstract
Background: Subacromial impingement or pain syndrome (SAPS) is the most common cause of chronic shoulder pain. Current surgeries do not reduce long-term pain, suggesting they miss the root etiology. Previously, we described the Human Disharmony Loop (HDL), where the unique lower trunk innervation to the pectoralis minor (PM) tips the scapula into dyskinesis and deforms its connections, including tugging the acromion down and impinging the subacromial structures. We hypothesize that SAPS patients who meet HDL criteria would benefit significantly from PM tenotomy.
Methods: Patients with SAPS who met HDL diagnostic criteria were treated with PM tenotomy and brachial plexus neurolysis, with additional secondary distal neurolysis if needed. Outcomes included pain and shoulder ROM in the abduction plane. 6-month follow-up minimum was required.
Results: N = 140 patients were included. Median age was 49. Prior surgeries included 27% subacromial decompression/acromioplasty, 21% rotator cuff repair, 16% biceps tenodesis, 4% SLAP repair, 2% labral repair, 7% distal clavicle resection, 10% re-verse total shoulder arthroplasty (rTSA), 1% rib resection with scalenectomy, 16% cervical spine fusion, 28% distal neurolysis. Median pain decreased from 8 to 2 and median shoulder ROM increased from 90 to 180 degrees. Positive impingement signs on exam decreased from 100% to 11%. (p< 0.01)
Conclusions: In a large series of SAPS patients, evaluation and treatment for the HDL significantly reduced pain and restored motion. These findings strongly suggest that SAPS itself is a subset of the HDL: the ventral PM disturbing the scapula constitutes the anatomic basis and optimal surgical target behind SAPS.
Keywords:
subacromial impingement
; shoulder pain
; scapula
; dyskinesia
; pectoralis minor
; weakness
1. Introduction
The most common reason patients present to a shoulder surgeon is chronic pain.[1,2] Worldwide, large proportions of the population suffer from shoulder pain on a daily to yearly basis.[3] One-third of the population endorses shoulder pain at any given point in time.[4] Shoulder pain is the third most common cause of disability.[5,6] Elite athletes are no exception.[7]
The most common diagnosis given for shoulder pain is subacromial pain syndrome (SAPS) [8,9], previously described as impingement syndrome[10], accounting for up to 65% of visits to shoulder specialists.[8] Patients with SAPS present with anterior shoulder pain, radiating pain to the mid-arm, and pain/weakness with overhead reach chiefly during the 60-120 degree mid-arc of abduction.[11] Clinically, SAPS presents as subacromial bursitis, tendinopathy or tears of the rotator cuff, and tendonitis of the bicipital tendon – the three anatomical structures within the subacromial space bounded by the overlying lateral acromion and underlying humeral head.[1] SAPS occurs along a spectrum from bursitis alone to degenerative tendinopathy to frank cuff tears.[12] Surgery is generally advised after failure to prove despite 3-6 months of maximum conservative management.[4]
The most common surgical treatments for SAPS include subacromial decompression or acromioplasty, bursectomy, CA ligament release, coplaning, and rotator cuff repair.[4] Acromioplasty in particular has increased in popularity recently.[13] However, high quality evidence-based reviews repeatedly demonstrate these procedures do not reduce the chief complaint of shoulder pain or improve function.[11,14-18] The highest quality research concludes subacromial decompression provides no benefit over sham arthroscopy[19] or conservative management alone.[9,15] Acromioplasty adds no benefit to rotator cuff repair.[20,21] Even for symptomatic rotator cuff tears, whether surgical repair provides any long-term clinical benefit is uncertain.[22] Hence, some have contended SAPS is a “medical myth” and that “surgical treatment should have no role in the treatment of these patients”[11], while others propose to discard the term “impingement” altogether.[18,23,24]
Thus, the contemporary state of the field can be summarized as follows: the most common surgical treatments performed by shoulder surgeons, for the most common diagnosis of SAPS, for the most common presenting complaint of shoulder pain, simply do not demonstrate efficacy.
Nonetheless, these patients are clearly suffering with a specific and reproducible set of shoulder symptoms[11], and demonstrate a predictable proximal etiology of inflammation and degeneration of anatomic structures in the subacromial space.[9] The ultimate etiology, however, remains unknown. Contentious debate continues between two predominant schools of thought.[12] The extrinsic hypothesis argues that the overlying anterior acromion, coracoacromial (CA) ligament, and acromioclavicular (AC) joint impinge and degrade the subacromial bursa, rotator cuff, and bicipital tendon.[25] The intrinsic hypothesis counters that inherent degradation of these structures due to diminished vascular supply, tensile forces, and/or aging first generates the inflammation.[2] Given the inefficacy for interventions that target the extrinsic sources, recent tides have turned in favor of the intrinsic proponents, but neither provides satisfactory causative explanations.[2] Yet many still favor the extrinsic hypothesis as “the surgical findings observed in the subacromial space during shoulder arthroscopy are hard to be explained if not for a contact between the rotator cuff and the acromion.”[9] We conclude the true anatomic cause of SAPS has yet to be described, i.e., the circle has yet to be squared.
Previously, we described the Human Disharmony Loop (HDL), a clinical model of upper limb and shoulder pain.[26] (Figure 1) The scapula, which coordinates motion and stability between the body (thorax) and arm (humerus), is balanced by the ventral pectoralis minor (PM) versus dorsal peri-scapular muscles. The PM uniquely carries lower trunk innervation. This asymmetry generates an unstable equilibrium that predisposes the scapula to dyskinesia (protraction).[26] One pathoanatomic sequelae includes lowering the acromion, narrowing the subacromial space, and impinging the bursa, cuff, and bicipital tendon. Three terminal symptoms include anterior shoulder pain, weakness with overhead reach, and radiating pain.[26] The HDL is diagnosed by strict anatomic and symptomatic criteria purely from history and physical exam.[26] (Figure 2) In our first two reports, we noted in subgroup analysis that SAPS patients improved dramatically with near-complete elimination of pain and restoration of shoulder motion following HDL treatment. Hence, we hypothesize that the PM pulling down on the coracoid and disturbing scapula mechanics may constitute the true hidden anatomic cause behind SAPS. Importantly, this would ‘square the circle’ by explaining both the repeated intra-operative findings and the inefficacy of current surgeries. In this paper, we test this hypothesis and report the outcomes of HDL treatment to treat pain and weakness in SAPS patients.
2. Materials and Methods
This is a prospective case series of patients treated at two sites by a uniform treatment protocol. All were evaluated by a fellowship-trained board-certified hand, sports, or shoulder surgeon. Inclusion criteria included: age > 18 years, a diagnosis of SAPS, and meeting HDL diagnostic criteria. (Figure 2) Exclusion criteria included: follow-up < 6 months. Patients were diagnosed with SAPS based on the presence of painful arc test and at least one positive Neer’s or Hawkin’s test. All patients trialed at least 3 months of therapy before being offered surgery. Patients were evaluated pre-operatively and at 2, 6, 12, and 24 weeks post-operatively. At each visit, patients completed a self-reported pain questionnaire. Shoulder abduction range of motion (ROM) values were measured. Scapula dyskinesia was classified into four stages: none (no protraction), dynamic (protraction with overhead reach only), static reversible (protraction at rest but manually reversible via the examiner), static irreversible (protraction at rest not manually reversible via the examiner). Each patient underwent open PM tenotomy with brachial plexus neurolysis using standardized technique, followed by dedicated PT emphasizing scapula retraction training and upper trapezius and rhomboid strengthening.[26] Patients were surveilled for residual neuropathy and offered secondary neurolysis at 3 months for lingering neuropathic lesions causing persistent pain and/or weakness. Outcomes included pain and shoulder ROM in the abduction plane. Institutional Review Board (IRB) approval was obtained, and need for consent was waived as the data was anonymous and posed minimal risk to patients. Statistical analysis was performed using Student’s t-test and chi-squared analysis to compare continuous and categorical variables of interest, respectively, using STATA v19.0.
3. Results
N = 140 patients were included. Median age was 49. Sex was 41% male and 59% female. Prior surgical treatments included 27% subacromial decompression or acromioplasty, 21% rotator cuff repair, 16% biceps tenodesis, 4% SLAP repair, 2% labral repair, 7% distal clavicle resection, 10% reverse total shoulder arthroplasty (rTSA), 1% rib resection with scalenectomy, 16% cervical spine fusion, 28% distal neurolysis. Of the 52 patients with pre-operative MRIs, findings included 80% supraspinatus pathology, 4% subscapularis pathology, 17% bicipital tendonitis, 15% SLAP tear, 12% labral tear. 88% of patients endorsed symptom relief with a medial retrocoracoid injection. (Table 1)
Median preoperative pain was 8/10. Median shoulder abduction ROM was 90 degrees. Baseline scapular dyskinesia was 3% dynamic, 49% static reversible, 49% static irreversible. Six months postoperatively, median pain decreased to 2/10. Median shoulder ROM increased to 180 degrees, and presence of positive impingement signs on exam went from 100% to 11%. Post-operative scapular dyskinesia redistributed to 94% none, 6% dynamic, 0% static reversible, 0% static irreversible. All differences were statistically significant (p<0.01). 19% of patients required secondary neurolysis for the axillary (6%), radial (9%), ulnar (10%), and median (6%) nerves. (Table 2)
4. Discussion
In this study, PM tenotomy with infraclavicular brachial plexus neurolysis dramatically reduced pain and restored shoulder abduction in SAPS patients who met HDL criteria. Our findings lend strong credence that the clandestine anatomic cause producing SAPS is the deforming pull of the PM on the coracoid from below, which tilts the acromion inferior and medial, narrows the subacromial space, and secondarily impinges the subacromial bursa, rotator cuff, and bicipital tendon. We assert based on these findings that SAPS is a subset of the Human Disharmony Loop. (Figure 3)
The HDL is a unifying chronic pain and dysfunction syndrome which articulates clear anatomic pathways producing a variety of overlapping clinical shoulder pain diagnoses. The peri-scapular chain coordinates scapulothoracic motion: the dorsal stabilizers innervated by the C5-6 upper trunk versus the sole anterior PM which uniquely carries C8-T1 lower trunk innervation. Due to this asymmetry, the PM can overpower the dorsal chain and tip the scapula into protraction. Previous anatomic explanations of SAPS have focused on rotator cuff dysfunction, which exerts a direct effect on the proximal humerus, and therefore can only displace the scapula indirectly through glenohumeral articular linkage. In contrast, only the PM pulls the scapula in the direction of protraction, which is the combination of lateral translation, internal rotation, and anterior tilt. This dyskinesia deforms the numerous connections of the scapula and pathologizes the full kinetic chain of the upper limb girdle. One effect is to inferiorly displace and internally rotate the acromion, and consequently the AC joint and CA ligament, all of which impinge the subacromial space.
Anatomically, this explains the intra-operative observations seen repeatedly: subacromial bursitis, rotator cuff tendinopathy to eventual tears, bicipital tendonitis, and CA ligament deep surface fraying. But it also answers why current surgical interventions that target these supposed offending overlying structures via subacromial decompression/acromioplasty, CA ligament debridement, and distal clavicle excision doesn’t ameliorate pain or improve function – because they are also victims and not culprits. The root source is the deforming tug from below of the PM onto the coracoid. (Figure 4) Contemporary debate has raged between the many alleged extrinsic (acromion morphology, glenohumeral instability, AC joint degeneration, CA ligament degeneration, coracoid impingement) versus intrinsic (muscle weakness, shoulder overuse, degenerative tendinopathy) causes of SAPS. However, both suffer from incomplete mechanistic explanations[2] and invoke a myriad of proximate causes which are themselves left unexplained. In contrast, the HDL provides a linear anatomic pathway: the unique neural asymmetric innervation of the PM tips the scapula into protraction, pulls the acromion down, impinges the subacromial structures, inflames and degrades the bursa, cuff, and bicipital tendon, and produces the chief complaints of pain and overhead reach weakness. (Figure 5) MRIs show the pathological sequelae within the subacromial space which then become surgical targets, but not the pathological cause.
Previously, scapular dyskinesis, shoulder impingement, and PM tightness have been well-known to occur simultaneously, but which was causative versus contributory remained unknown.[27] PM tightness is traditionally described as occurring concomitantly with impingement and cuff pathology[28] and associated with but secondary to abnormal scapulothoracic motion.[29,30] Thus, while PM release has certainly been shown to improve scapular mechanics, widen the subacromial space, and decrease pain[31-33], it has been noted in this literature that “the cause of PM tightness is not fully understood”.[32] Indeed, the causative relationships between the entities of PM tightness, scapular dyskinesis, and shoulder impingement has remained clouded in uncertainty and baffled surgeons. In contrast, the HDL uniquely identifies the asymmetric lower trunk innervation to the PM as the root anatomic source predisposing the human scapula to dyskinesis[26], then clarifies a specific anatomic pathway illustrating how PM tightness causes scapular dyskinesis which causes subacromial impingement. (Table 3) (Figure 6) As such, the HDL can accurately identify both which patients will benefit from PM tenotomy, and which terminal symptoms will improve.
Thus, the HDL demystifies the century-long uncertainty: true cause of subacromial impingement is neither extrinsic nor intrinsic but scapular. The results of our study – significant reductions in pain with near-full restoration of shoulder abduction – followed normalization of scapular kinesis, supporting this conclusion. (Figure 7) The prior surgical history and MRI findings of patients in the study further challenge existing models of SAPS. Many patients had prior subacromial decompressions, cuff repair, biceps tenodesis, and distal clavicle excision, but with enduring pain and weakness. Furthermore, those with preoperative MRIs displayed anatomic findings predicted by the HDL pathway: supraspinatus tendinopathy or tears, bicipital tendonitis, and SLAP tears. (Figure 4 and Figure 5)
The HDL also elucidates the otherwise-unexplained radiating pain frequently seen in SAPS, as radiating neuropathy is a separate terminal symptom.[26] Furthermore, it answers a broad set of known yet unexplained observations. Scapula protraction is observed in SAPS patients.[11,34] Patients who demonstrate impingement on exam also exhibit both a protracted scapula and dorsal peri-scapular muscle weakness[35,36], both of which are key HDL elements. Exercises that strength the dorsal peri-scapular stabilizers and reverse protraction of the scapula also reduce the need for surgery.[37] Overhead sports athletes with shoulder pain demonstrate a shorter and tighter PM on exam.[38-40] SAPS patients exhibit a significantly more active PM than asymptomatic patients when performing overhead shoulder elevation, while the other peri-scapular muscles remain similar.[41] Stabilization of the scapula reduces pain and disability in SAPS patients.[42] Scapular dyskinesis produces shoulder pain in athletes through secondary pathologic effects on the biceps-labrum complex.[43] Prior investigations have missed the underlying etiology, including: acromion morphology[44] does not correlate with chronic impingement[45], subacromial steroid injection is equally effective as acupuncture in pain reduction[46], neither presence of a rotator cuff tear nor acromiohumeral distance correlates with pain[11,47], physical examination tests for impingement suffer from poor diagnostic accuracy.[48]
This study suffers from several limitations. As a non-randomized case series limited to two sites, our results must be replicated before establishing generalizability and causality. SAPS was diagnosed based on a combination of two clinical criteria, although no gold standard exists.[9] Furthermore, the lack of bursoscopic evaluation at the time of PM tenotomy did not verify the pathoanatomic changes associated with clinical exam and MRI findings. Our results only apply to SAPS patients who meet HDL criteria, and future studies need to investigate the relationship between the HDL and internal or subcoracoid impingement. Importantly, the need for secondary distal neurolysis in 19% of patients suggests that SAPS occurs concomitantly with distal neuropathy consistent with the well-known “double crush” phenomenon. Notably, 11% of patients did exhibit continued impingement after treatment, showing that isolated impingement can persist, albeit uncommonly. We advocate ‘breaking the loop’ first, surveying for residual neuropathy or impingement, and addressing lingering pain generators later, only if they remain bothersome to the patient. Future studies should utilize a consensus diagnostic standard and randomize PM tenotomy versus standard of care in large multi-institutional trials to demonstrate causality and generalizability of our study findings.
Nonetheless, in a large series of SAPS patients, PM tenotomy with brachial plexus neurolysis (and secondary distal neurolysis if necessary) predictably and dramatically reduced pain and restored motion. We propose that SAPS itself is a subset of the HDL: the ventral PM disturbing the scapula constitutes the anatomic basis and optimal surgical target behind SAPS.
Author Contributions
Dr. Ketan Sharma, Dr. Jaicharan Iyengar, and Dr. James Friedman contributed equally to the conceptualization, methodology, validation, analysis, investigation, data curation, writing of this project. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of St. Luke’s Clinic (protocol 2024-0107 on 10/14/24) and St. Joseph’s Medical Center (7/11/24).
Informed Consent Statement
Patient consent was waived by the ethics committee as all data was anonymous, the study was observational only and involved standard of care treatments, and the study posed minimal risk to the included patients.
Data Availability Statement
The original contributions presented in this study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author(s).
Acknowledgments
In this section, you can acknowledge any support given which is not covered by the author contribution or funding sections. This may include administrative and technical support, or donations in kind (e.g., materials used for experiments).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PM | Pectoralis minor |
| SAPS | Subacromial pain syndrome |
| HDL | Human disharmony loop |
| MRI | Magnetic Resonance Imaging |
| ROM | Range of motion |
| CA | Coraco-acromial |
| AC | Acromio-clavicular |
| IRB | Institutional Review Board |
| TSA | Total shoulder arthroplasty |
| SLAP | Superior Labrum Anterior Posterior |
References
- Greenberg, D.L. Evaluation and treatment of shoulder pain. Med Clin North Am 2014, 98, 487–504. [Google Scholar] [CrossRef]
- Horowitz, E.H.; Aibinder, W.R. Shoulder Impingement Syndrome. Phys Med Rehabil Clin N Am 2023, 34, 311–334. [Google Scholar] [CrossRef] [PubMed]
- Lucas, J.; van Doorn, P.; Hegedus, E.; Lewis, J.; van der Windt, D. A systematic review of the global prevalence and incidence of shoulder pain. BMC Musculoskelet Disord 2022, 23, 1073. [Google Scholar] [CrossRef] [PubMed]
- Garving, C.; Jakob, S.; Bauer, I.; Nadjar, R.; Brunner, U.H. Impingement Syndrome of the Shoulder. Dtsch Arztebl Int 2017, 114, 765–776. [Google Scholar] [CrossRef]
- Brattberg, G.; Parker, M.G.; Thorslund, M. The prevalence of pain among the oldest old in Sweden. Pain 1996, 67, 29–34. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Ditsios, K.; Middleton, W.D.; Hildebolt, C.F.; Galatz, L.M.; Teefey, S.A. The demographic and morphological features of rotator cuff disease. A comparison of asymptomatic and symptomatic shoulders. J Bone Joint Surg Am 2006, 88, 1699–1704. [Google Scholar] [CrossRef] [PubMed]
- Myklebust, G.; Hasslan, L.; Bahr, R.; Steffen, K. High prevalence of shoulder pain among elite Norwegian female handball players. Scand J Med Sci Sports 2013, 23, 288–294. [Google Scholar] [CrossRef]
- Umer, M.; Qadir, I.; Azam, M. Subacromial impingement syndrome. Orthop Rev (Pavia) 2012, 4, e18. [Google Scholar] [CrossRef]
- Consigliere, P.; Haddo, O.; Levy, O.; Sforza, G. Subacromial impingement syndrome: management challenges. Orthop Res Rev 2018, 10, 83–91. [Google Scholar] [CrossRef]
- Neer, C.S. , 2nd. Anterior acromioplasty for the chronic impingement syndrome in the shoulder: a preliminary report. J Bone Joint Surg Am 1972, 54, 41–50. [Google Scholar] [CrossRef]
- Dhillon, K.S. Subacromial Impingement Syndrome of the Shoulder: A Musculoskeletal Disorder or a Medical Myth? Malays Orthop J 2019, 13, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.K.; Flatow, E.L. Subacromial impingement syndrome. J Am Acad Orthop Surg 2011, 19, 701–708. [Google Scholar] [CrossRef]
- Vitale, M.A.; Arons, R.R.; Hurwitz, S.; Ahmad, C.S.; Levine, W.N. The rising incidence of acromioplasty. J Bone Joint Surg Am 2010, 92, 1842–1850. [Google Scholar] [CrossRef]
- Dorrestijn, O.; Stevens, M.; Winters, J.C.; van der Meer, K.; Diercks, R.L. Conservative or surgical treatment for subacromial impingement syndrome? A systematic review. J Shoulder Elbow Surg 2009, 18, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Gebremariam, L.; Hay, E.M.; Koes, B.W.; Huisstede, B.M. Effectiveness of surgical and postsurgical interventions for the subacromial impingement syndrome: a systematic review. Arch Phys Med Rehabil 2011, 92, 1900–1913. [Google Scholar] [CrossRef] [PubMed]
- Karjalainen, T.V.; Jain, N.B.; Page, C.M.; Lahdeoja, T.A.; Johnston, R.V.; Salamh, P.; Kavaja, L.; Ardern, C.L.; Agarwal, A.; Vandvik, P.O.; et al. Subacromial decompression surgery for rotator cuff disease. Cochrane Database Syst Rev 2019, 1, CD005619. [Google Scholar] [CrossRef]
- Lahdeoja, T.; Karjalainen, T.; Jokihaara, J.; Salamh, P.; Kavaja, L.; Agarwal, A.; Winters, M.; Buchbinder, R.; Guyatt, G.; Vandvik, P.O.; et al. Subacromial decompression surgery for adults with shoulder pain: a systematic review with meta-analysis. Br J Sports Med 2020, 54, 665–673. [Google Scholar] [CrossRef]
- Diercks, R.; Bron, C.; Dorrestijn, O.; Meskers, C.; Naber, R.; de Ruiter, T.; Willems, J.; Winters, J.; van der Woude, H.J.; Dutch Orthopaedic, A. Guideline for diagnosis and treatment of subacromial pain syndrome: a multidisciplinary review by the Dutch Orthopaedic Association. Acta Orthop 2014, 85, 314–322. [Google Scholar] [CrossRef]
- Beard, D.J.; Rees, J.L.; Cook, J.A.; Rombach, I.; Cooper, C.; Merritt, N.; Shirkey, B.A.; Donovan, J.L.; Gwilym, S.; Savulescu, J.; et al. Arthroscopic subacromial decompression for subacromial shoulder pain (CSAW): a multicentre, pragmatic, parallel group, placebo-controlled, three-group, randomised surgical trial. Lancet 2018, 391, 329–338. [Google Scholar] [CrossRef]
- Chahal, J.; Mall, N.; MacDonald, P.B.; Van Thiel, G.; Cole, B.J.; Romeo, A.A.; Verma, N.N. The role of subacromial decompression in patients undergoing arthroscopic repair of full-thickness tears of the rotator cuff: a systematic review and meta-analysis. Arthroscopy 2012, 28, 720–727. [Google Scholar] [CrossRef]
- Song, L.; Miao, L.; Zhang, P.; Wang, W.L. Does concomitant acromioplasty facilitate arthroscopic repair of full-thickness rotator cuff tears? A meta-analysis with trial sequential analysis of randomized controlled trials. Springerplus 2016, 5, 685. [Google Scholar] [CrossRef] [PubMed]
- Karjalainen, T.V.; Jain, N.B.; Heikkinen, J.; Johnston, R.V.; Page, C.M.; Buchbinder, R. Surgery for rotator cuff tears. Cochrane Database Syst Rev 2019, 12, CD013502. [Google Scholar] [CrossRef] [PubMed]
- Cools, A.M.; Michener, L.A. Shoulder pain: can one label satisfy everyone and everything? Br J Sports Med 2017, 51, 416–417. [Google Scholar] [CrossRef]
- Lewis, J. The End of an Era? J Orthop Sports Phys Ther 2018, 48, 127–129. [Google Scholar] [CrossRef]
- Bigliani, L.U.; Levine, W.N. Subacromial impingement syndrome. J Bone Joint Surg Am 1997, 79, 1854–1868. [Google Scholar] [CrossRef]
- Sharma, K.; Friedman, J.M. The Human Disharmony Loop: A Case Series Proposing the Unique Role of the Pectoralis Minor in a Unifying Syndrome of Chronic Pain, Neuropathy, and Weakness. J Clin Med 2025, 14. [Google Scholar] [CrossRef]
- Castelein, B.; Cagnie, B.; Cools, A. Scapular muscle dysfunction associated with subacromial pain syndrome. J Hand Ther 2017, 30, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Kibler, W.B.; McMullen, J. Scapular dyskinesis and its relation to shoulder pain. J Am Acad Orthop Surg 2003, 11, 142–151. [Google Scholar] [CrossRef]
- Min, K.S.; Pham, B.; Scala, V. Arthroscopic pectoralis minor release in the beach chair position. JSES Rev Rep Tech 2022, 2, 174–177. [Google Scholar] [CrossRef]
- Richards, J.A.; Munshi, M.-A.H.; Woodard, D.R.; DeFroda, S.F.; Nuelle, C.W.; Richard Ma, S.-Y. Arthroscopic Pectoralis Minor Release. Arthroscopy Techniques 2025, 14. [Google Scholar] [CrossRef]
- Hendrix, S.T.; Hoyle, M.; Tokish, J.M. Arthroscopic Pectoralis Minor Release. Arthrosc Tech 2018, 7, e589–e594. [Google Scholar] [CrossRef]
- Provencher, M.T.; Kirby, H.; McDonald, L.S.; Golijanin, P.; Gross, D.; Campbell, K.J.; LeClere, L.; Sanchez, G.; Anthony, S.; Romeo, A.A. Surgical Release of the Pectoralis Minor Tendon for Scapular Dyskinesia and Shoulder Pain. Am J Sports Med 2017, 45, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Servasier, L.; Jeudy, J.; Raimbeau, G.; Bigorre, N. Arthroscopic release of the pectoralis minor tendon as an adjunct to acromioplasty in the treatment of subacromial syndrome associated with scapular dyskinesia. Orthop Traumatol Surg Res 2022, 108, 103211. [Google Scholar] [CrossRef]
- Struyf, F.; Nijs, J.; Baeyens, J.P.; Mottram, S.; Meeusen, R. Scapular positioning and movement in unimpaired shoulders, shoulder impingement syndrome, and glenohumeral instability. Scand J Med Sci Sports 2011, 21, 352–358. [Google Scholar] [CrossRef] [PubMed]
- Lewis, J.S.; Wright, C.; Green, A. Subacromial impingement syndrome: the effect of changing posture on shoulder range of movement. J Orthop Sports Phys Ther 2005, 35, 72–87. [Google Scholar] [CrossRef] [PubMed]
- Ludewig, P.M.; Braman, J.P. Shoulder impingement: biomechanical considerations in rehabilitation. Man Ther 2011, 16, 33–39. [Google Scholar] [CrossRef]
- Holmgren, T.; Hallgren, H.B.; Oberg, B.; Adolfsson, L.; Johansson, K. Effect of specific exercise strategy on need for surgery in patients with subacromial impingement syndrome: randomised controlled study. Br J Sports Med 2014, 48, 1456–1457. [Google Scholar] [CrossRef]
- Harrington, S.; Meisel, C.; Tate, A. A cross-sectional study examining shoulder pain and disability in Division I female swimmers. J Sport Rehabil 2014, 23, 65–75. [Google Scholar] [CrossRef]
- Reeser, J.C.; Joy, E.A.; Porucznik, C.A.; Berg, R.L.; Colliver, E.B.; Willick, S.E. Risk factors for volleyball-related shoulder pain and dysfunction. PM R 2010, 2, 27–36. [Google Scholar] [CrossRef]
- Tate, A.; Turner, G.N.; Knab, S.E.; Jorgensen, C.; Strittmatter, A.; Michener, L.A. Risk factors associated with shoulder pain and disability across the lifespan of competitive swimmers. J Athl Train 2012, 47, 149–158. [Google Scholar] [CrossRef]
- Castelein, B.; Cagnie, B.; Parlevliet, T.; Cools, A. Scapulothoracic muscle activity during elevation exercises measured with surface and fine wire EMG: A comparative study between patients with subacromial impingement syndrome and healthy controls. Man Ther 2016, 23, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Ravichandran, H.; Janakiraman, B.; Gelaw, A.Y.; Fisseha, B.; Sundaram, S.; Sharma, H.R. Effect of scapular stabilization exercise program in patients with subacromial impingement syndrome: a systematic review. J Exerc Rehabil 2020, 16, 216–226. [Google Scholar] [CrossRef] [PubMed]
- Clarsen, B.; Bahr, R.; Andersson, S.H.; Munk, R.; Myklebust, G. Reduced glenohumeral rotation, external rotation weakness and scapular dyskinesis are risk factors for shoulder injuries among elite male handball players: a prospective cohort study. Br J Sports Med 2014, 48, 1327–1333. [Google Scholar] [CrossRef]
- Nicholson, G.P.; Goodman, D.A.; Flatow, E.L.; Bigliani, L.U. The acromion: morphologic condition and age-related changes. A study of 420 scapulas. J Shoulder Elbow Surg 1996, 5, 1–11. [Google Scholar] [CrossRef]
- Aydin, A.; Yildiz, V.; Kalali, F.; Yildirim, O.S.; Topal, M.; Dostbil, A. The role of acromion morphology in chronic subacromial impingement syndrome. Acta Orthop Belg 2011, 77, 733–736. [Google Scholar]
- Johansson, K.; Bergstrom, A.; Schroder, K.; Foldevi, M. Subacromial corticosteroid injection or acupuncture with home exercises when treating patients with subacromial impingement in primary care--a randomized clinical trial. Fam Pract 2011, 28, 355–365. [Google Scholar] [CrossRef] [PubMed]
- Park, S.W.; Chen, Y.T.; Thompson, L.; Kjoenoe, A.; Juul-Kristensen, B.; Cavalheri, V.; McKenna, L. No relationship between the acromiohumeral distance and pain in adults with subacromial pain syndrome: a systematic review and meta-analysis. Sci Rep 2020, 10, 20611. [Google Scholar] [CrossRef]
- Hegedus, E.J.; Goode, A.P.; Cook, C.E.; Michener, L.; Myer, C.A.; Myer, D.M.; Wright, A.A. Which physical examination tests provide clinicians with the most value when examining the shoulder? Update of a systematic review with meta-analysis of individual tests. Br J Sports Med 2012, 46, 964–978. [Google Scholar] [CrossRef]
Figure 1.
The Human Disharmony Loop. The HDL is a clinical model of human upper limb pain centered on an unstable equilibrium around the scapula due to the unique lower trunk innervation to the pectoralis minor. The central loop has three elements, each causing anatomic sequelae. Diverse groups of patients can enter via each element, seen in green. The anatomic sequelae then produce coracoid tenderness and four distinct groups of clinical symptoms (bottom row).
Figure 1.
The Human Disharmony Loop. The HDL is a clinical model of human upper limb pain centered on an unstable equilibrium around the scapula due to the unique lower trunk innervation to the pectoralis minor. The central loop has three elements, each causing anatomic sequelae. Diverse groups of patients can enter via each element, seen in green. The anatomic sequelae then produce coracoid tenderness and four distinct groups of clinical symptoms (bottom row).
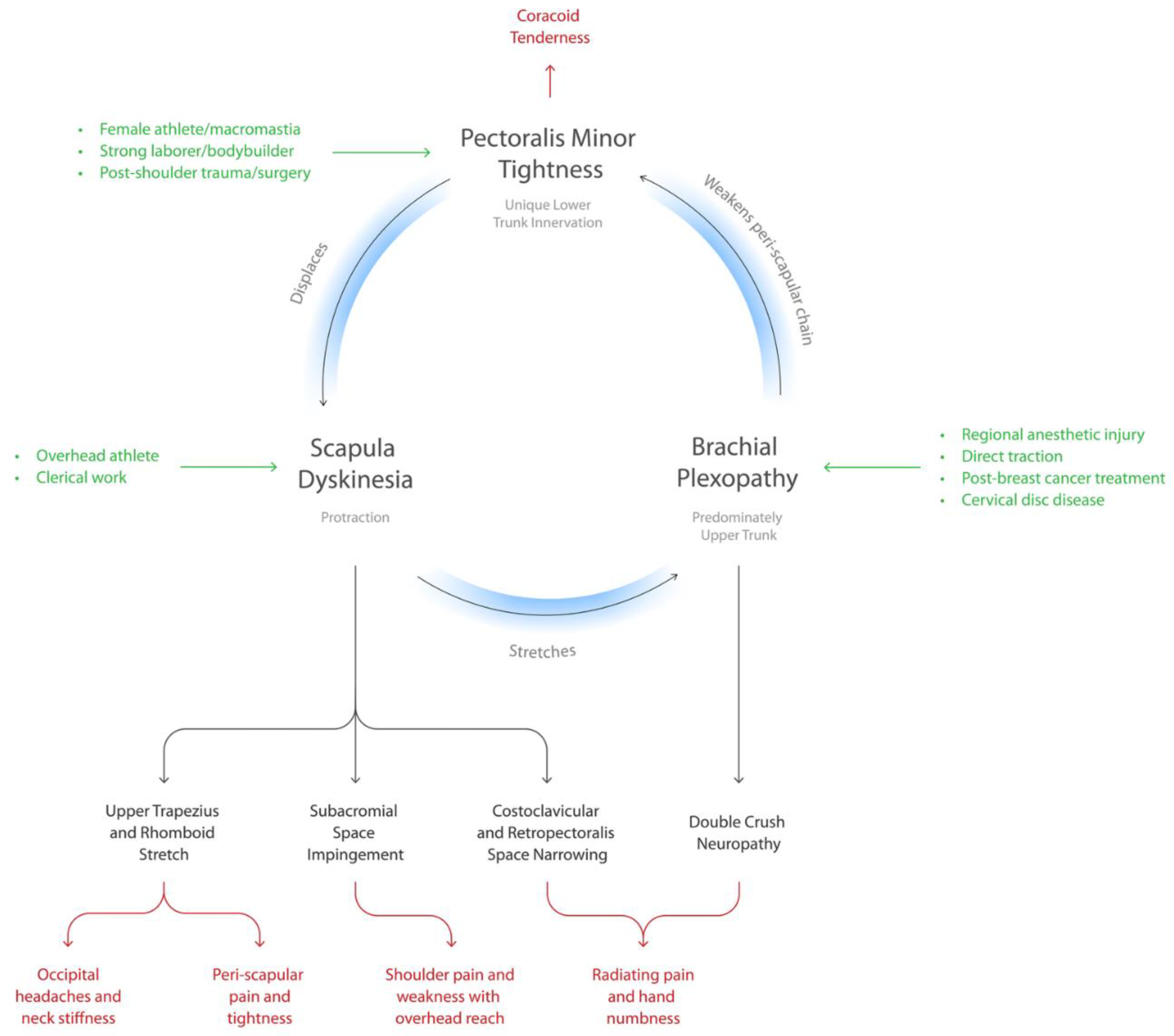
Figure 2.
HDL Diagnosis. Diagnosis of HDL is based on two anatomic and one symptomatic criterion and is derived purely from history and physical exam.
Figure 2.
HDL Diagnosis. Diagnosis of HDL is based on two anatomic and one symptomatic criterion and is derived purely from history and physical exam.
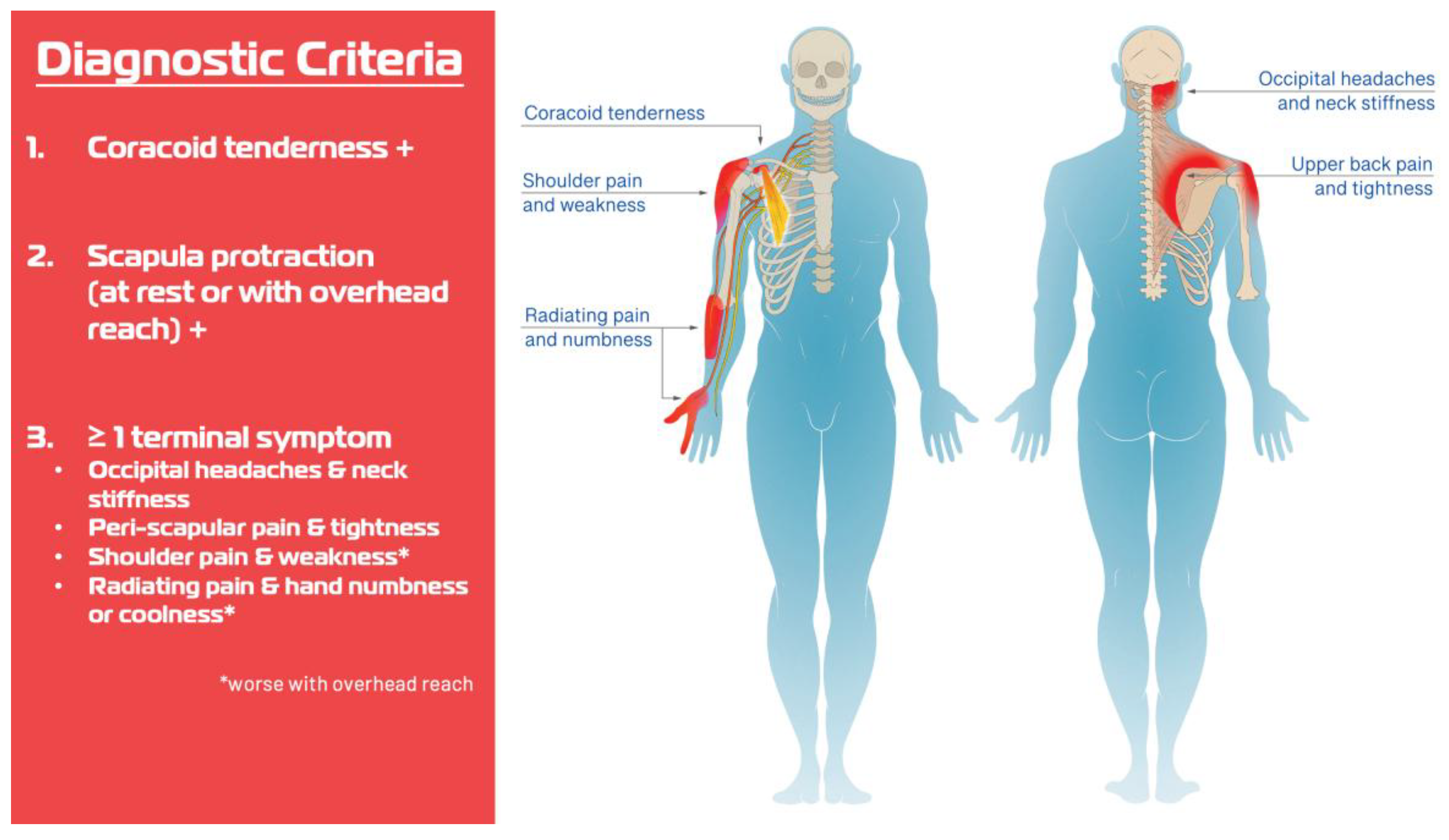
Figure 3.
Subacromial Pain Syndrome (SAPS) as a Subset of the Human Disharmony Loop (HDL) SAPS is the subset of the HDL where the scapular protraction pulls the acromion down, thereby impinging the subacromial structures, producing cuff tendinopathy, subacromial bursitis, bicipital tendonitis, and causing shoulder pain and weakness with overhead reach. Current treatments target a pathological effect and miss the true anatomic cause, explaining their inefficacy.
Figure 3.
Subacromial Pain Syndrome (SAPS) as a Subset of the Human Disharmony Loop (HDL) SAPS is the subset of the HDL where the scapular protraction pulls the acromion down, thereby impinging the subacromial structures, producing cuff tendinopathy, subacromial bursitis, bicipital tendonitis, and causing shoulder pain and weakness with overhead reach. Current treatments target a pathological effect and miss the true anatomic cause, explaining their inefficacy.
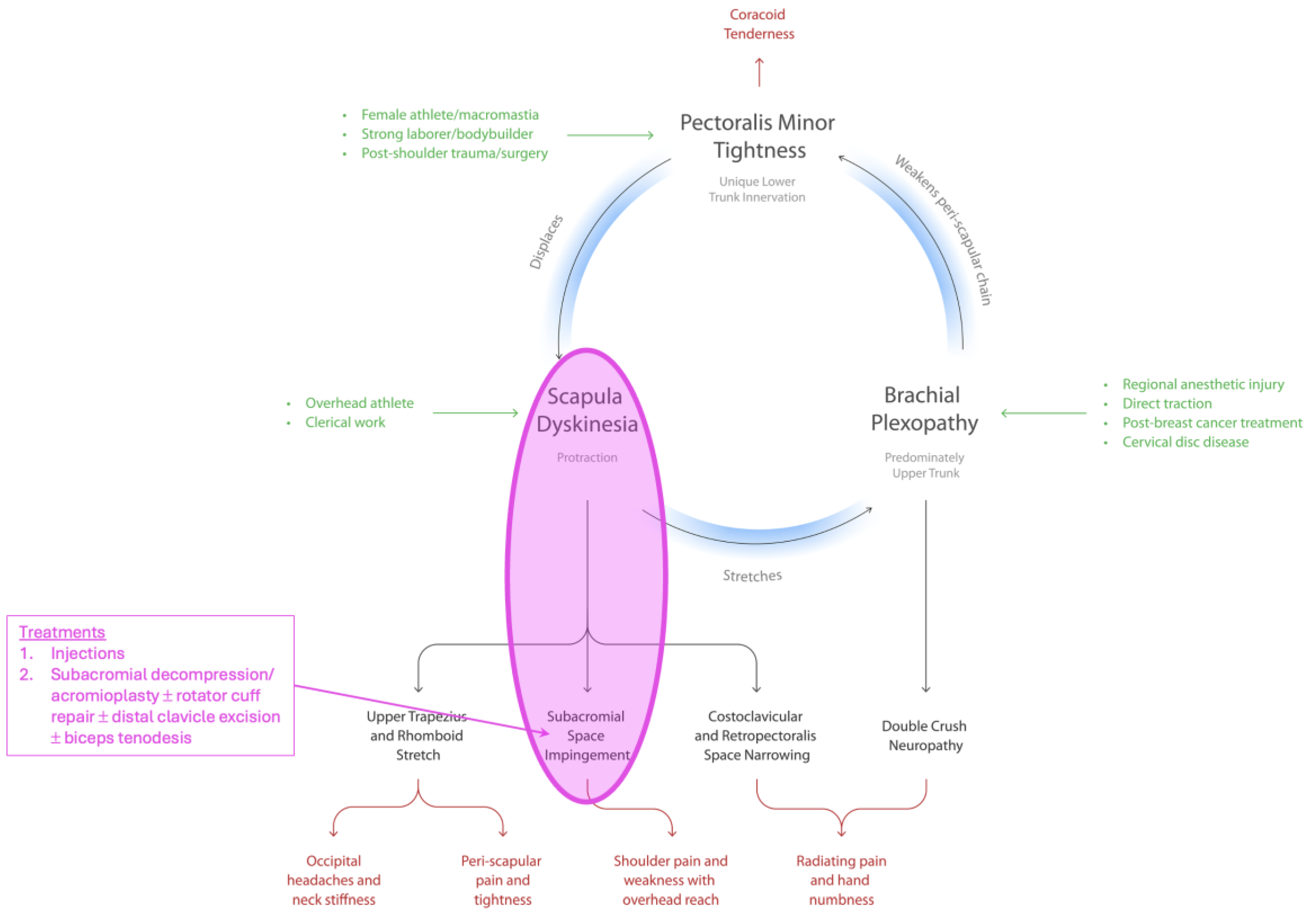
Figure 4.
Subacromial Pain Syndrome Pathoanatomy: Frontal. On frontal view, the root pathological source is the deforming force from below of the PM tugging down onto the coracoid (blue arrow, right), which lowers the acromion and its associated structures, thereby impinging the subacromial space and producing subacromial bursitis, cuff tendinopathy to eventual tears, and bicipital tendonitis.
Figure 4.
Subacromial Pain Syndrome Pathoanatomy: Frontal. On frontal view, the root pathological source is the deforming force from below of the PM tugging down onto the coracoid (blue arrow, right), which lowers the acromion and its associated structures, thereby impinging the subacromial space and producing subacromial bursitis, cuff tendinopathy to eventual tears, and bicipital tendonitis.
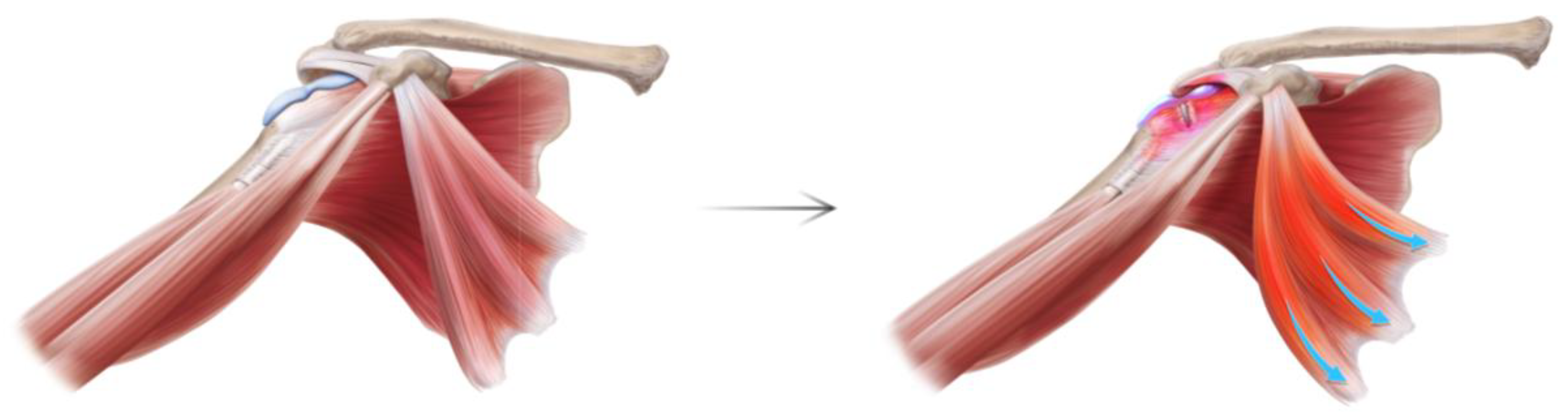
Figure 5.
Subacromial Pain Syndrome Pathoanatomy: Sagittal. On sagittal view, the root pathological source is the deforming force from ventral of the PM tugging down onto the coracoid (blue arrow, right), which lowers the acromion and its associated structures, thereby impinging the subacromial space and producing subacromial bursitis, cuff tendinopathy to eventual tears, and bicipital tendonitis.
Figure 5.
Subacromial Pain Syndrome Pathoanatomy: Sagittal. On sagittal view, the root pathological source is the deforming force from ventral of the PM tugging down onto the coracoid (blue arrow, right), which lowers the acromion and its associated structures, thereby impinging the subacromial space and producing subacromial bursitis, cuff tendinopathy to eventual tears, and bicipital tendonitis.
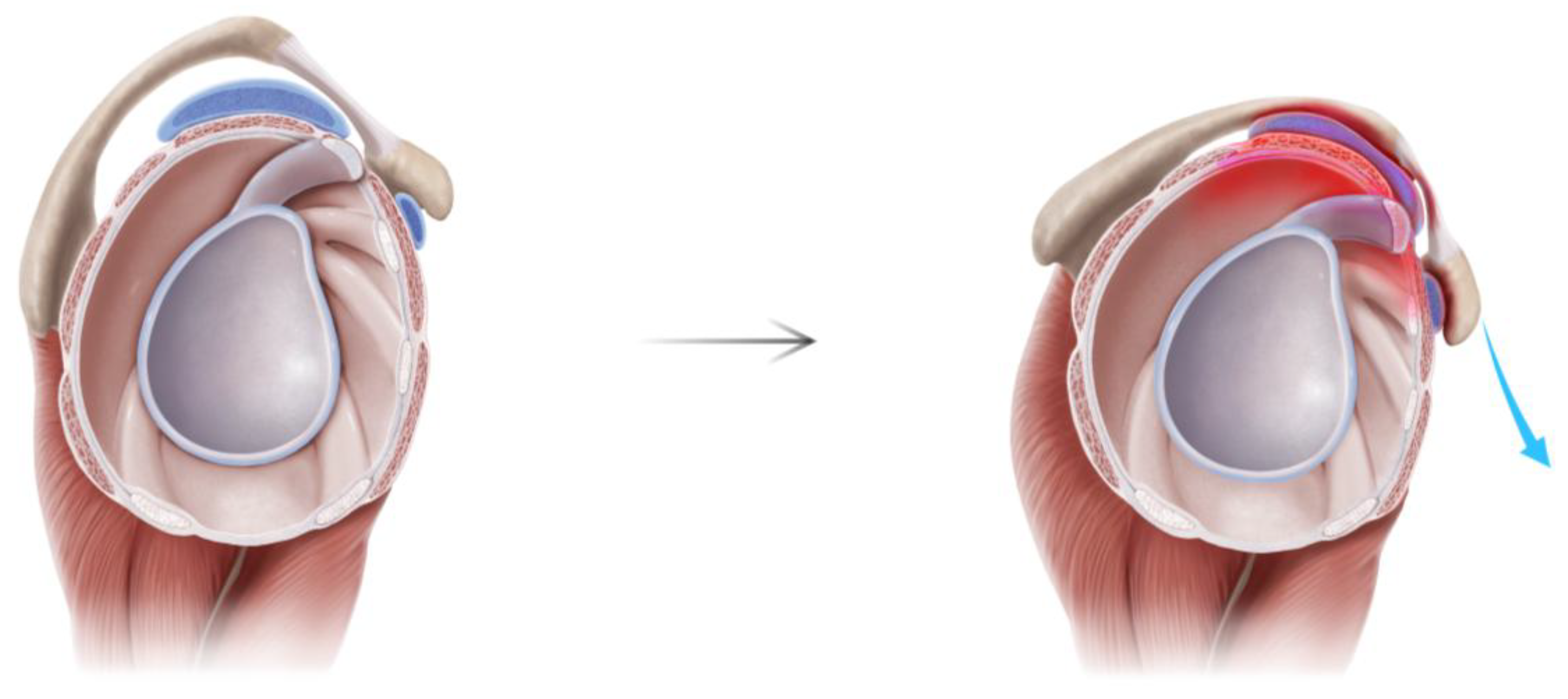
Figure 6.
Illustrative Differences between Pectoralis Minor Syndrome versus Human Disharmony Loop. PMS only accounts for distal neuropathic symptoms, cannot explain the etiology of PM tightness, and the relationship between PM tightness to scapular dyskinesis and subacromial impingement remains shrouded in mystery. In contrast, the HDL answers the etiology behind PM tightness, can account for all symptoms including neuropathy, shoulder weakness, upper back pain, and articulates clear cause and effect regarding these other syndromes.
Figure 6.
Illustrative Differences between Pectoralis Minor Syndrome versus Human Disharmony Loop. PMS only accounts for distal neuropathic symptoms, cannot explain the etiology of PM tightness, and the relationship between PM tightness to scapular dyskinesis and subacromial impingement remains shrouded in mystery. In contrast, the HDL answers the etiology behind PM tightness, can account for all symptoms including neuropathy, shoulder weakness, upper back pain, and articulates clear cause and effect regarding these other syndromes.
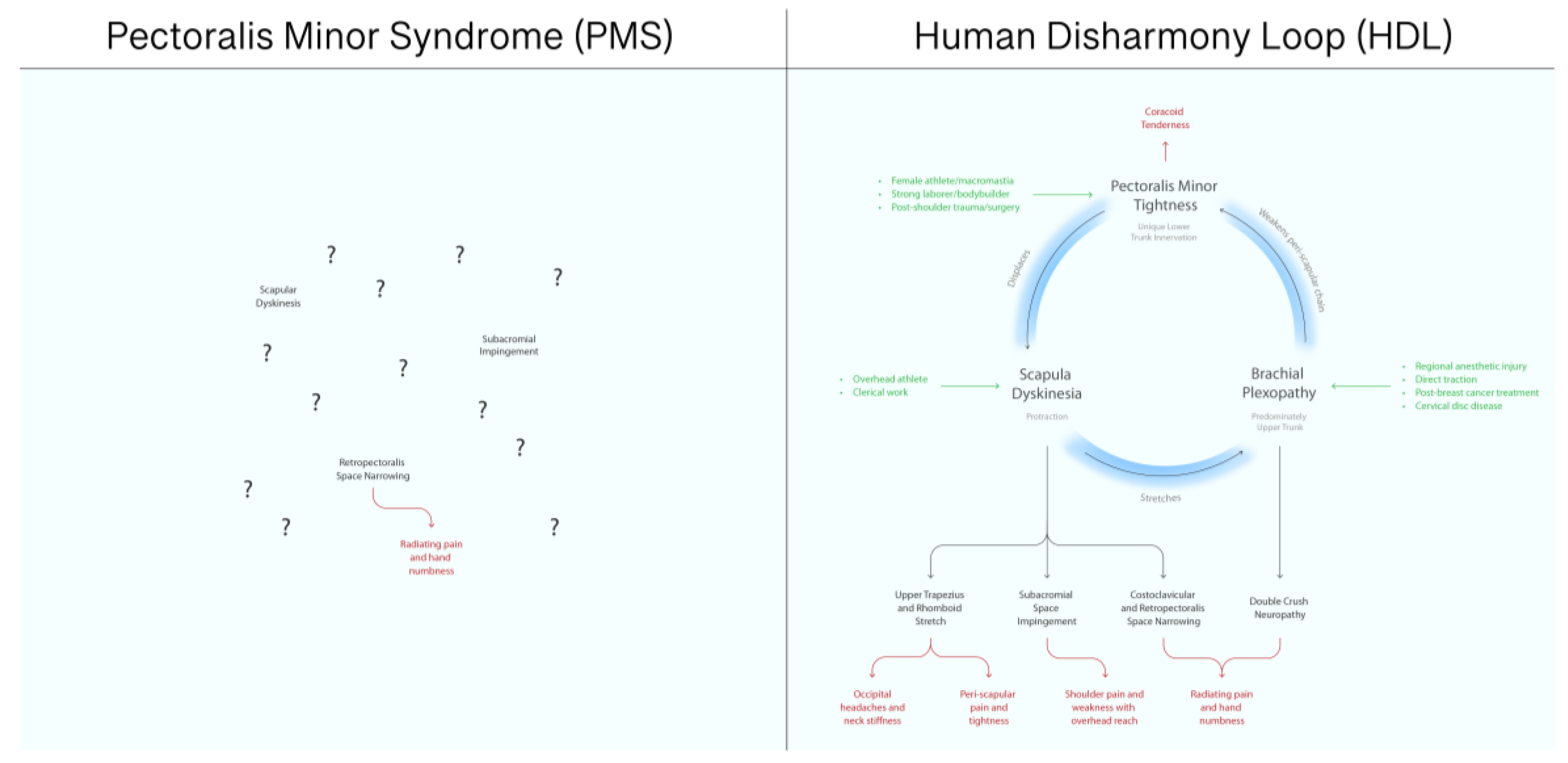
Figure 7.
Normalization of Scapular Dyskinesia Produces Improvements in Range of Motion and Pain. Normalization of scapular dyskinesia following PM tenotomy produced full restoration of ROM and significant reduction in pain, demonstrating that the root cause underlying subacromial impingement and pain is neither extrinsic nor intrinsic but scapular. .
Figure 7.
Normalization of Scapular Dyskinesia Produces Improvements in Range of Motion and Pain. Normalization of scapular dyskinesia following PM tenotomy produced full restoration of ROM and significant reduction in pain, demonstrating that the root cause underlying subacromial impingement and pain is neither extrinsic nor intrinsic but scapular. .
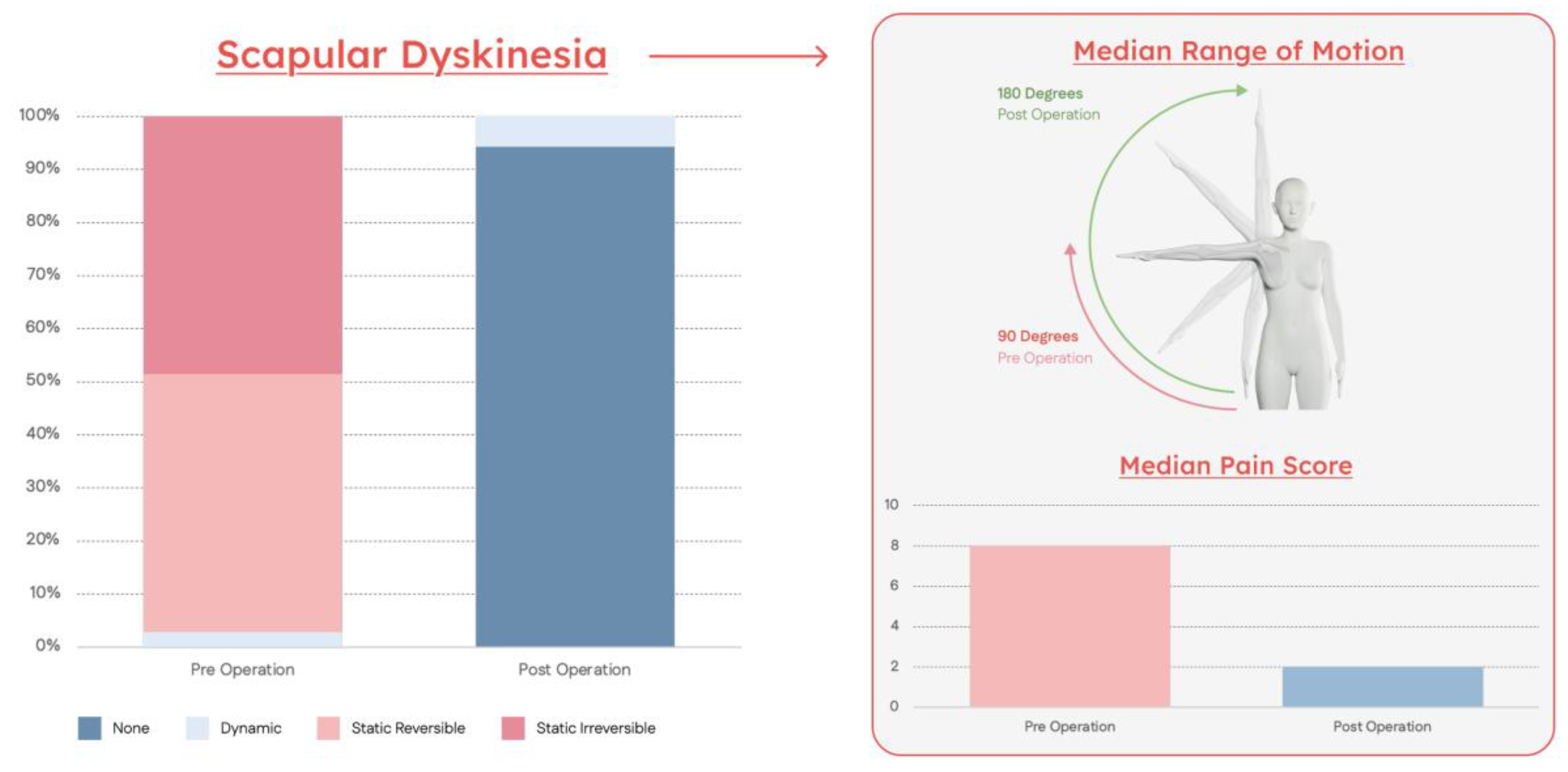

Table 1.
Patient Characteristics.
| Variable | N = 140 |
|---|---|
| Age | 49 [37–60] |
| Sex | Male 58 (41%) Female 82 (59%) |
| BMI | 29 [25–33] |
| Workers Compensation | 35 (25%) |
| Surgical History | |
| Subacromial decompression | 38 (27%) |
| Rotator cuff repair | 29 (21%) |
| Biceps tenodesis | 23 (16%) |
| SLAP repair Labral repair Bankart repair |
5 (4%) 3 (2%) 2 (2%) |
| Distal clavicle resection | 10 (7%) |
| Clavicle ORIF | 1 (1%) |
| Reverse total shoulder arthroplasty | 14 (10%) |
| 1st rib resection + scalenectomy | 2 (1%) |
| Cervical spine fusion | 22 (16%) |
| Distal neurolysis (carpal, cubital) | 39 (28%) |
| MRI Findings Supraspinatus tendinopathy or tear Subscapularis tendinopathy or tear Bicipital tendonitis SLAP tear Labral tear |
(n = 52) 42 (81%) 2 (4%) 9 (17%) 8 (15%) 6 (12%) |
| Laterality | Right 80 (57%) Left 60 (43%) |
| Hand Dominance | Right 114 (81%) Left 26 (19%) |
| Medial Coracoid Injection | Provided Relief 99 (88%) |
1. Median with [inter-quartile range].
Table 2.
Clinical Outcomes.
| Symptom | Preoperative | Postoperative | P-Value |
|---|---|---|---|
| Pain | 8 [6–9] | 2 [0–3] | <0.01 |
| Scapular Dyskinesia Stage | |||
| Stage I | 0 (0%) | 132 (94%) | |
| Stage II | 4 (3%) | 8 (6%) | <0.01 |
| Stage III | 68 (49%) | 0 (0%) | |
| Stage IV | 68 (49%) | 0 (0%) | |
| Shoulder Abduction ROM | 90 [90–100] | 180 [180] | <0.01 |
| Positive Impingement Signs | 140 (100%) | 15 (11%) | <0.01 |
| Neuropathic Lesions1 | |||
| Scalene muscles | 86 (61%) | 3 (2%) | |
| Suprascapular notch | 88 (63%) | 0 (0%) | |
| Quadrilateral space | 127 (91%) | 17 (12%) | <0.01 |
| Radial tunnel | 96 (69%) | 28 (20%) | |
| Cubital tunnel | 37 (26%) | 31 (22%) | |
| Carpal tunnel | 72 (51%) | 33 (24=%) | |
| Secondary Neurolysis2 | 27 (19%) | ||
| Suprascapular | 0 (0%) | ||
| Quadrilateral space | N/A | 9 (6%) | N/A |
| Radial | 13 (9%) | ||
| Cubital | 14 (10%) | ||
| Carpal | 9 (6%) |
1 Neuropathic lesions were considered positive with a positive scratch-collapse test at each anatomic location 2 Patients were surveilled for residual neuropathy and offered secondary neurolysis at 3 months for persistent symptoms.
Table 3.
Key Differences between Pectoralis Minor Syndrome (PMS) versus Human Disharmony Loop (HDL).
Table 3.
Key Differences between Pectoralis Minor Syndrome (PMS) versus Human Disharmony Loop (HDL).
| PMS | HDL | |
|---|---|---|
| Etiology | Unknown | Unique asymmetric lower trunk innervation |
| Mechanism | Compressive neuropathy | Deformation of scapula |
| Symptoms | Distal neuropathy only | All: headaches, neck pain, shoulder impingement, myofascial trigger points, and distal and proximal neuropathy |
| Anatomic Relationships to Other Chronic Pain Entities | Completely unknown | Clearly specifies cause and effect |
| Prognostic Value | Minimal | Strong |
| Epidemiology | Very rare | Ubiquitous |
| Relative Importance in Upper Limb Chronic Pain | After-thought | Central |
PMS and the HDL are extremely distinct clinical syndromes whose critical differences are highlighted here. In summary, unlike PMS, the HDL can (1) explain the etiology of PM tightness, (2) account for all symptoms seen and not just distal neuropathy, and (3) specify clear casual pathways with subacromial pain syndrome and scapular dyskinesis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



