
Submitted:
01 July 2025
Posted:
02 July 2025
You are already at the latest version
Abstract
Congenital portosystemic shunts (CPSS) are often associated with life-threatening systemic complications, which may be detected by identifying hypergalactosemia in newborn screening (NBS). However, diagnosing CPSS at an early stage is not easy. The purpose of this study was to predict CPSS early using screening values and general blood tests. The medical records of 153 patients with hypergalactosemia who underwent NBS in Saitama Prefecture between December 1, 1997 and October 31, 2023 were retrospectively analyzed. We provided the final diagnosis of analyzed patients. Of the 153 patients, 44 (29%) were in the CPSS group and 83 (54%) were in the transient galactosemia group. Using the initial screening items and the six blood test items, we attempted to extract a CPSS group from the transient galactosemia group. Finally, a model for CPSS prediction was established. From multiple logistic regression analysis, filtered blood galactose-1 phosphate/galactose, serum total bile acid, and ammonia were adopted as explanatory variables for the prediction model. If the cut-off value for predicted disease probability value (P) was > 0.378, CPSS was identified with 88.6% sensitivity (95%CI 75.4–96.2%) and 78.3% specificity (95%CI 67.9–86.6%). This predictive model might allow prediction of CPSS and early intervention.
Keywords:
congenital portosystemic shunt
; hypergalactosemia
; newborn screening
; galactose-1 phosphate/galactose
; total bile acid
; ammonia
1. Introduction
Galactosemia is an inborn error of galactose metabolism. This pathology has been included in various neonatal screening programs since 1977 in Japan. The enzyme deficiency can be detected by hypergalactosemia. However, causes of hypergalactosemia also include congenital portosystemic shunt (CPSS), citrin deficiency and transient galactosemia [1].
CPSS is a rare congenital malformation, occurring in 1 in 30,000 newborns [2]. Several reports from Japan have described CPSS as a frequent cause of hypergalactosemia identified from newborn screening [3].
CPSS can lead to various complications such as hyperammonemia, neurological complications, hepatic encephalopathy, liver tumors, and hepatopulmonary syndrome. Shunts can be categorized into two kinds: intrahepatic, which largely resolve spontaneously; and extrahepatic, which usually require surgical correction or, in some cases, liver transplantation [4]. Therefore, depending on the shunt type and size, intervention before symptoms appear may be desirable [5].
The diagnosis of CPSS requires imaging. Ultrasonography (US) is the modality of choice for every patient based on its ease of use, utility, non-invasiveness, and the ability to avoid radiation exposure. However, CPSS may be missed on US due to limited imaging features and interference from gastrointestinal gas [6,7,8]. To compensate for this insufficient ability of US, a study in Japan reported that using filtered blood galactose (Gal), galactose-1 phosphate (Gal-1-P), serum total bile acid (TBA) and blood ammonia (NH3) enabled detection of CPSS [8], although the number of cases under investigation was small and no similar studies have been reported.
The purpose of this study was to determine the utility of differentiating CPSS using screening values and general blood tests.
2. Materials and Methods
2.1. Newborn Screening
This retrospective study was conducted in the Division of Mass Screening at Saitama Prefectural Children’s Medical Center, from December 1, 1997 to October 31, 2023.
Dried blood spots (DBS) were collected approximately 1–2 hours after feeding between 4 and 6 days after birth. Screening parameters included Gal, total Gal (TGal), Gal-1-P, UDP-galactose-4-epimerase (GALE) activity, and galactose-1-phosphate uridylyltransferase (GALT) activity. Gal and Gal-1-P were measured using a microplate enzyme assay method [9]. Values before the addition of alkaline phosphatase (ALP) were taken as Gal, while values after the addition of ALP were taken as TGal. Gal-1-P was calculated as [TGal - Gal] × 1.44. The activities of GALT and GALE were measured using spot test and fluorescence detection methods [10,11]. GALE activity measurements began from 2013.
2.2. Cut-Off Values
The cut-off values for immediate confirmatory testing were set at Gal ≥ 10 mg/dL or TGal ≥ 20 mg/dL from 1997 to the end of 2012, and Gal ≥ 10 mg/dL or Gal-1-P ≥ 20 mg/dL from the start of 2013. The Gal-1-P cut-off was raised to ≥ 25 mg/dL in August 2018 to improve screening specificity. Newborns with Gal ≥ 3 mg/dL or TGal ≥ 7 mg/dL in 1997–2003, with Gal ≥ 3 mg/dL or TGal ≥ 8 mg/dL in 2004–2012, or with Gal ≥ 3 mg/dL or Gal-1-P ≥ 15 mg/dL after 2013 underwent retesting. In this study, to standardize the timing of testing for all cases, values from the initial newborn screening were used.
2.3. Confirmatory Testing
Confirmatory blood testing included alanine aminotransferase (ALT), albumin, blood ammonia (NH3), direct bilirubin, prothrombin time (PT%), TBA, and plasma amino acid analysis. These values were collected approximately 1–2 hours after feeding. Abdominal ultrasonography was performed as an imaging examination, and contrast-enhanced computerized tomography (CT) was performed for consenting patients.
2.4. Handling for Hypergalactosemia
When blood galactose level was ≥10 mg/dL, we basically used lactose-free formula. Genetic testing was considered when each of GALT deficiency, systemic GALE deficiency, or citrin deficiency was suspected [12]. If the cause of galactosemia could not be identified, we performed a galactose loading test (normal formula load test) at 2–3 months after birth [13]. If Gal level increased after loading, genetic testing for galactose mutarotase (GALM) deficiency was considered after its discovery in 2018 [13]. All other cases were carefully followed-up as transient galactosemia.
2.5. Definitions of CPSS and Transient Galactosemia
Cases of CPSS were defined as those cases showing vascular malformation on imaging. Cases of transient galactosemia were defined as those cases for which causes of galactosemia were unclear. This group might have included cases with delayed closure of the ductus venosus or heterozygous enzyme deficiency.
2.6. Types of CPSS
Various shunt classifications have been reported [14,15,16]. In this study, malformation of an intrahepatic portal vein or of a portal vein that does not flow into the liver were categorized as extrahepatic shunt. Cases with a shunt vessel between the intrahepatic portal vein branch, the hepatic vein or inferior vena cava, or patent ductus venous (PDV) were defined as intrahepatic shunt.
2.7. Statistical Analysis
To predict CPSS, we statistically compared screening items and confirmatory blood testing for the two groups of CPSS and transient galactosemia.
The unpaired t-test, Mann–Whitney U test and Fisher’s exact test were employed to compare 12 variables between patients in the CPSS and transient groups. Values of p < 0.05 were considered statistically significant. Receiver operating characteristic (ROC) analyses were performed to evaluate the ability to predict CPSS. Using these ROC analyses, we determined the cut-off values that yielded the highest Youden index [17]. To correlate Gal-1-P/Gal, TBA, and NH3 with significant CPSS, we applied multiple logistic regression analyses with variable selection by backward elimination. All analyses were performed using SAS JMP version 16.2.0 (SAS Institute Inc., NC, USA), EZR version 1.64 [18] and Medcalc version 22.030 (MedCalc Software, Mariakerke, Belgium). In this paper, “P” and “p-value” denote the predicted disease probability estimated with our clinical prediction model and the statistical probability value obtained with statistical tests, respectively. Internal validation of models was carried out by correcting measures of predictive performance for “optimism” or overfit using bootstrap methods in the rms packages (version 6.7-1) in R using 1,000 resamplings [19,20].
3. Results
In total, 1,412,327 blood samples from newborns were tested, while 173 cases (0.012%) of hypergalactosemia came to two hospitals (Saitama Medical University Hospital or Saitama Prefectural Children’s Medical Center) for confirmatory testing. After excluding patients with missing values, a final total of 153 cases screened after 2002 were analyzed (Figure 1).
From December 1st, 1977, to October 31st, 2023, we identified 173 cases (0.012%) from 1,412,327 screened newborns. These 173 cases underwent confirmatory tests due to the above the cut-off value. Twenty individuals were excluded due to missing data, resulting in a final total of 153 newborns analyzed.
For cases with a final diagnosis of hypergalactosemia, 18 cases (12%) showed enzyme deficiency including heterozygotes, 44 cases (29%) were CPSS, 7 cases (5%) were citrin deficiency, 83 cases (54%) were transient cases and 1 case (1%) involved biliary atresia. In the cases of enzyme deficiency, GALE deficiency (peripheral type) accounted for the largest number of cases (11 cases). All cases of GALT deficiency were heterozygous. GALM deficiency was discovered in 2018, with cases before that time potentially being classified to the transient group. Cases of CPSS comprised 32 cases (73%) of intrahepatic shunt and 12 cases (27%) of extrahepatic shunt, with intrahepatic shunts significantly more common (Table 1).
Most cases of CPSS closed spontaneously during the first 2 years of life. Surgical intervention was required in 13 of 44 CPSS patients (30%; Table 2). Of these 13 cases, 10 were extrahepatic and 3 intrahepatic, with extrahepatic shunts more common (p-value < 0.001). For extrahepatic CPSS, pre-emptive closure is the consensus even for asymptomatic patients, as spontaneous closure is considered unlikely and this type is associated with more severe complications [4]. For this reason, surgical interventions were performed for 10 of the 12 extrahepatic shunts. Except in one case for which the details were unknown, surgical intervention was performed for 4 symptomatic and 8 asymptomatic cases. Even in asymptomatic cases, procedures for closing shunts were applied if closure was not confirmed by about 2 years old (Table 2).
Comparing CPSS and transient cases using screening items and confirmatory blood tests, significant differences were identified in Gal, TGal, Gal-1-P, Gal-1-P/Gal, albumin, NH3, and TBA (p-value < 0.05 each) (Table 3). To avoid multicollinearity, Gal-1-P/Gal was selected from the ROC results out of Gal, TGal, Gal-1-P, and Gal-1-P/Gal. Repeated multiple logistic regression analysis was performed using Gal-1-P/Gal and other variables, selecting explanatory variables for the predictive model by backward elimination (Table 4). Finally, Gal-1-P/Gal, TBA, and NH3 were selected as explanatory variables that were statistically significant and used in the predictive model equation [20]:
The ROC of the prediction equation (Figure 2) showed that the highest value of the Youden index (area under the curve [AUC]=0.837) was seen at P=0.378. Using P > 0.378 as the cut-off, sensitivity was 88.6% (95% confidence interval [CI] 75.4–96.2%) and specificity was 78.3% (95%CI 67.9–86.6%). Values of P could be changed considering sensitivity and specificity (Table S1). Figure 3 presents the results of applying P > 0.378 for the CPSS and transient groups. Most cases of CPSS could be suspected using P > 0.378. Five cases of CPSS showed false-negative results. Four of these cases involved delayed closure of the PDV, with all having high initial Gal-1-P levels (Figure 3). Validation of the prediction model was carried out using the bootstrap method. The AUC for the ROC was 0.827 (bootstrap optimism-corrected c = 0.655), and the optimism-corrected calibration slope was 0.9. Mean absolute error was 0.043, showing good fitness of the model.
ROC of the prediction equation calculated using filtered blood galactose-1 phosphate, blood total bile acid and ammonia as statistically significant explanatory variables for predicting CPSS.
Most cases of CPSS could be suspected using P > 0.378. Five cases of CPSS (orange filled circles) showed false-negative results. If P > 0.378 was used as the cut-off value for predicted disease probability, CPSS was identified with 88.6% sensitivity (95%CI 75.4–96.2%) and 78.3% specificity (95%CI 67.9–86.6%).
We showed two representative cases. Case 12 in Table 2 is an example of us being able to close the shunt during the asymptomatic period with the help of our prediction model. She was born to non-consanguineous parents at 40 weeks, 6 days of gestation. Her birth weight was 2170 g (0.1%ile) and height was 45.5 cm (0.7%ile). Phototherapy was performed at seven days due to neonatal jaundice. The initial newborn screening results were: Gal 7.2 mg/dL, TGal 15.7, and Gal-1-P 12.2 mg/dL. As Gal was ≥ 3 mg/dL, patient underwent retesting. The results were: Gal 4.2 mg/dL, TGal 8.9, and Gal-1-P 6.8 mg/dL, so confirmatory testing was carried out. Gal-1-P/Gal, TBA, and NH3 levels were 1.69, 150.6 μmol/L, and 102 μg/dL, respectively. Prediction probability (P) was 0.91. No shunt vessel was detected on abdominal ultrasound, whereas intrahepatic shunt of the portal vein to left hepatic vein was identified on contrast-enhanced CT She underwent endovascular closure with coils at 1 year and 8 months old because, although she was asymptomatic, the shunt was considered unlikely to close.
The second case required surgical treatment despite a low P value of 0.25 (Case 6 in Table 2). Case 6 was the second child born to non-consanguineous parents, delivered at 39 weeks and 1 day of gestation. His birth weight was 3300 g and height was 50.5 cm; Apgar scores were 2 and 4 at 1 and 5 min, respectively, and the patient was admitted to the neonatal intensive care due to neonatal asphyxia. The initial newborn screening results showed: Gal 3.4 mg/dL, TGal 12.8, and Gal-1-P 13.5 mg/dL. As Gal was ≥ 3 mg/dL, the patient underwent retesting. The results were: Gal 5.1 mg/dL, TGal 8.1, and Gal-1-P 4.2 mg/dL, so confirmatory testing was carried out. Gal-1-P/Gal, TBA, and NH3 were 3.97, 28.3 μmol/L, and 40 μg/dL respectively. P was 0.25, revealing a false-negative result. Abdominal ultrasound showed an extrahepatic shunt of the splenic vein to the left renal vein. The patient underwent vascular ligation at the age of 3 years 8 months old because, although he was asymptomatic, the shunt remained open.
4. Discussion
Galactosemia type 1 was first described in 1908 [21]. After that, with the intention of preventing disease by restricting galactose intake from the onset of symptoms, the NBS began to measure galactose from DBS [22,23]. However, congenital enzyme deficiency has become recognized as uncommon in hypergalactosemia [1]. In this study, enzyme deficiency accounted for only 12% of cases. CPSS was the most common, accounting for 29% of cases, excluding transient cases (Table 1).
The overall incidence of CPSS is estimated to be 1:30,000~40,000 births, and 1:50,000 for those that persist beyond early life [2]. In this study, the prevalence of CPSS was 1 in 32,098, similar to previous reports [2]. Reports from Japan have examined the frequency of CPSS in hypergalactosemia, varying from 7% to 43% depending on the cut-off value, screening items, and number of cases [3,24]. Taken all together, cases of CPSS in Japan appear to have been mostly detected during NBS.
CPSS patients may present with hypoglycemia, hyperammonemia, and jaundice in the neonatal period, and are at risk of pulmonary hypertension, hepatic encephalopathy, and liver tumors later in life [4]. Uchida et al. reported that the main complications related to CPSS were hyperammonemia (85.2%), liver masses (25.4%), hepatopulmonary shunts (13.9%), and pulmonary hypertension (11.5%). Shunt closure improved most symptoms, except liver masses and pulmonary hypertension. Further, more than half of CPSS patients were detected by NBS [25]. Similar reports have described CPSS detection by the NBS [3,24,25,26,27]. Based on the above results, suspecting CPSS at the time of NBS is important.
CPSS is diagnosed by imaging tests. Non-invasive abdominal ultrasound is the initial imaging modality for diagnosing CPSS, but may not accurately demonstrate the associated intra- or extrahepatic shunts due to factors such as limited imaging features and gastrointestinal gas interference [6]. In such cases, contrast-enhanced CT or MRI with radiation exposure need to be considered. In this study, several cases of CPSS were missed on US, but detected on contrast-enhanced CT. CPSS is thus not easily diagnosed and may be missed [6,7,8].
Regarding CPSS treatment, intrahepatic CPSS diagnosed at birth or in utero is generally recommended to be monitored for spontaneous closure during the first 2 years of life, provided no significant clinical complications arise. If the shunt does not close spontaneously and remains patent in the second year of life, or if the patient experiences systemic complications of portosystemic shunting regardless of age, the consensus is thus shunt closure is important. For extrahepatic CPSS, pre-emptive closure even in asymptomatic patients is the consensus, as spontaneous closure is unlikely, extrahepatic shunts are associated with more severe complications, and the severest cases require liver transplantation [5,28,29,30]. In this study, eight of the 13 cases that underwent surgical treatment were asymptomatic (Table 2). Early detection is clearly a key factor in the ability to provide strict follow-up and accurate treatment. That is, if a high probability of CPSS can be accurately recognized at NBS, the prognosis will be improved.
One report from Japan used screening items and confirmatory blood tests to detect CPSS, as in this study [8]. The small number of cases in that study made generalization of the results difficult. In this study, we were able to set the sensitivity and specificity to construct a prediction model by increasing the number of cases analyzed and extending the observation period. However, these data were only from Saitama Prefecture and represents approximately one-sixteenth of the Japanese population. Gal-1-P/Gal was collected on days 4 to 6 after birth, while TBA and NH3 were collected from day 14 to two months after birth. In other words, this study combined values from two different periods. This difference in the timing of blood collection may have led to some cases of physiological PDV being classified as transient. Murayama et al. [31] reported that functional closure of the ductus venosus occurs at 10.2 days old in babies with 29–32 weeks of gestation, 7.1 days old in babies with 33–36 weeks of gestation, and 4.6 days old in babies with 37–41 weeks of gestation. Considering that most of our cases were full-term, although about half of the cases showed a patent ductus venosus at the time of DBS collection, we believe that functional closure had been achieved by the time of the confirmation test. In the future, the effects of physiological PDV could be resolved by performing DBS collection and confirmatory testing at the same time.
By combining the three items (Gal-1-P/Gal, TBA, and NH3), we were able to establish a cut-off value that can be used to predict CPSS from an early stage. Further, the ROC was ≥0.8 (Figure 2), which can be considered to reflect excellent discrimination performance [32]. CPSS is reportedly generally suspected if TBA and NH3 levels are elevated [33,34,35]. In this study, we were able to create a useful model for predicting CPSS through combining these factors. In fact, Case 12 (Table 2) was considered for shunt closure while asymptomatic based on our prediction model (Figure 2 and Figure 3). Sensitivity and specificity could be easily adjusted to desired values that would increase the positive predictive value (Table S1).
Despite setting the cut-off value to give the best sensitivity and specificity, five CPSS cases showed false-negative results (Figure 3). Four of those five cases had PDV and high initial Gal-1-P levels. In three of the four PDV cases, the ductus venosus closed within five months. The last false-negative case (Case 6 in Table 2) had an extrahepatic shunt and required surgical treatment. We consider that Case 6 (Table 2) was due to high Gal-1-P and low TBA levels, but the reason for this remains a cause for concern.
Unfortunately, no significant differences in P were identified between the surgical and spontaneous closure cases (p-value = 0.35). That means more reliable results from a large-scale study are needed.
This study only included data from two facilities in Saitama Prefecture. In the future, we hope that a large-scale prospective cohort study will be conducted that also includes the timing of sample collection, leading to the construction of a more reliable predictive model. The present study has shown that this goal is feasible.
5. Conclusions
When the cut-off for the predicted probability of disease was P > 0.378 using Gal-1-P/Gal, TBA, and NH3, CPSS was able to be identified with 88.6% sensitivity (95%CI 75.4–96.2%) and 78.3% specificity (95%CI 67.9–86.6%). Using this predictive model, we might be able to detect CPSS early, leading to early intervention.
Supplementary Materials
The following are available online at website of this paper posted on Preprints.org, Table S1: Sensitivity and specificity of predicted disease probability (p).
Author Contributions
Conceptualization, S.S.-A. and A.O.; Methodology, S.S.-A., A.O. and R.A.; Formal analysis, S.S.-A. and R.A.; Investigation, S.A., I.M., M.A., M.M., S.F., R.I., T.K., A.T. and H.M.; Data curation, A.I.-O. and R.A.; Writing – original draft preparation, S.S.-A.; Writing – review & editing, S.S.-A.; Visualization, S.S.-A.; Supervision, A.O. and C.N. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was approved by the Saitama Medical School Hospital Institutional Review Board (IRB log no. 20113.01, approved on 5 October 2020).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Nishimura, Y.; Tajima, G.; Bahagia, A.D.; Sakamoto, A.; Ono, H.; Sakura, N.; Naito, K.; Hamakawa, M.; Yoshii, C.; Kubota, M.; et al. Differential Diagnosis of Neonatal Mild Hypergalactosaemia Detected by Mass Screening: Clinical Significance of Portal Vein Imaging. J. Inherit. Metab. Dis. 2004, 27, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Papamichail, M.; Pizanias, M.; Heaton, N. Congenital Portosystemic Venous Shunt. Eur. J. Pediatr. 2018, 177, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Nishigaki, S.; Etani, Y.; Shoji, Y.; Yamada, H.; Matayoshi, K.; Ioi, A.; Inaoka, K.; Takeshima, K.; Ida, S. Clinical Feature of Galactosaemia Identified by Neonatal Mass Screening. J. Mass Screen. 2014, 24, 61–67. [Google Scholar]
- Laverdure, N.; Lallier, M.; Dubois, J.; Paganelli, M. Congenital Absence of the Portal Vein: Define the Portosystemic Shunt, Avoid Liver Transplantation. Can. Liver J. 2021, 4, 322–327. [Google Scholar] [CrossRef]
- McLin, V.A.; Franchi-Abella, S.; Brütsch, T.; Bahadori, A.; Casotti, V.; De Ville De Goyet, J.; Dumery, G.; Gonzales, E.; Guérin, F.; Hascoet, S.; et al. Expert Management of Congenital Portosystemic Shunts and Their Complications. JHEP Rep. 2024, 6, 100933. [Google Scholar] [CrossRef]
- Xu, S.; Zhang, P.; Hu, L.; Zhou, W.; Cheng, G. Case Report: Clinical Features of Congenital Portosystemic Shunts in the Neonatal Period. Front. Pediatr. 2021, 9, 778791. [Google Scholar] [CrossRef]
- Konstas, A.A.; Digumarthy, S.R.; Avery, L.L.; Wallace, K.L.; Lisovsky, M.; Misdraji, J.; Hahn, P.F. Congenital Portosystemic Shunts: Imaging Findings and Clinical Presentations in 11 Patients. Eur. J. Radiol. 2011, 80, 175–181. [Google Scholar] [CrossRef]
- Matsuoka, R.; Mochizuki, H.; Kubota, M. Value of the Gal-1-P/Gal Ratio and the Serum Total Bile Acid at the Differential Diagnosis of Hypergalactosemia Detected by Newborn Screening. J. Mass Screen. 2015, 25, 39–45. [Google Scholar]
- Fujimura, Y.; Kawamura, M.; Naruse, H. Simultaneous Quantitative Estimation of Galactose-1-Phosphate and Galactose in Blood for the Diagnosis of Galactosemia. Tohoku J. Exp. Med. 1982, 137, 289–295. [Google Scholar] [CrossRef]
- Beutler, E.; Baluda, M.C. Improved Method for Measuring Galactose-1-Phosphate Uridyl Transferase Activity of Erythrocytes. Clin. Chim. Acta 1966, 13, 369–379. [Google Scholar] [CrossRef]
- Fujimura, Y. A New Mass Screening Method of Detecting UDP-Galactose-4-Epimerase Deficiency.
- Kikuchi, A.; Arai-Ichinoi, N.; Sakamoto, O.; Matsubara, Y.; Saheki, T.; Kobayashi, K.; Ohura, T.; Kure, S. Simple and Rapid Genetic Testing for Citrin Deficiency by Screening 11 Prevalent Mutations in SLC25A13. Mol. Genet. Metab. 2012, 105, 553–558. [Google Scholar] [CrossRef] [PubMed]
- Wada, Y.; Kikuchi, A.; Arai-Ichinoi, N.; Sakamoto, O.; Takezawa, Y.; Iwasawa, S.; Niihori, T.; Nyuzuki, H.; Nakajima, Y.; Ogawa, E.; et al. Biallelic GALM Pathogenic Variants Cause a Novel Type of Galactosemia. Genet. Med. 2019, 21, 1286–1294. [Google Scholar] [CrossRef] [PubMed]
- Morgan, G.; Superina, R. Congenital Absence of the Portal Vein: Two Cases and a Proposed Classification System for Portasystemic Vascular Anomalies. J. Pediatr. Surg. 1994, 29, 1239–1241. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, N.; Niwa, T.; Kirikoshi, H.; Fujita, K.; Yoneda, M.; Saito, S.; Nakajima, A. Clinical Classification of Congenital Extrahepatic Portosystemic Shunts. Hepatol. Res. 2010, 40, 585–593. [Google Scholar] [CrossRef]
- Park, J.H.; Cha, S.H.; Han, J.K.; Han, M.C. Intrahepatic Portosystemic Venous Shunt. Am. J. Roentgenol. 1990, 155, 527–528. [Google Scholar] [CrossRef]
- Youden, W.J. Index for Rating Diagnostic Tests. Cancer 1950, 3, 32–35. [Google Scholar] [CrossRef]
- Kanda, Y. Investigation of the Freely Available Easy-to-Use Software ‘EZR’ for Medical Statistics. Bone Marrow Transplant. 2013, 48, 452–458. [Google Scholar] [CrossRef]
- Jr, F.E.H. Regression Modeling Strategies: With Applications to Linear Models, Logistic and Ordinal Regression, and Survival Analysis; Springer: Cham, 2015; ISBN 978-3-319-19424-0. [Google Scholar]
- Steyerberg, E.W. Clinical Prediction Models: A Practical Approach to Development, Validation, and Updating; Statistics for Biology and Health; Springer International Publishing: Cham, 2019; ISBN 978-3-030-16398-3. [Google Scholar]
- Badiu Tișa, I.; Achim, A.C.; Cozma-Petruț, A. The Importance of Neonatal Screening for Galactosemia. Nutrients 2022, 15, 10. [Google Scholar] [CrossRef]
- Gatti, R.A.; Manfield, P.; Yi-Yung Hsia, D. Screening Newborn Infantsfor Galactosemia. J. Pediatr. 1966, 69, 1126–1129. [Google Scholar] [CrossRef]
- Aufrance, O.E.; Jones, W.N.; Harris, W.H. Screening for Galactosemia and Phenylketonuria. JAMA 1964, 190, 1126. [Google Scholar] [CrossRef]
- Nishimura, Y.; Tajima, G.; Ono, H.; Naito, K.; Sakura, N.; Yoshii, C.; Hamakawa, M. Overview of 60 Cases of Hypergalactosemia Caused by Portosystemic Shunt Detected by Neonatal Mass Screening Test in Hiroshima Prefecture. Jpn. J. Mass Screen. 18, 29–34.
- Uchida, H.; Shinkai, M.; Okuyama, H.; Ueno, T.; Inoue, M.; Yasui, T.; Hiyama, E.; Kurihara, S.; Sakuma, Y.; Sanada, Y.; et al. Impact of Portal Flow on the Prognosis of Children With Congenital Portosystemic Shunt: A Multicentric Observation Study in Japan. J. Pediatr. Surg. 2024, 59, 1791–1797. [Google Scholar] [CrossRef] [PubMed]
- Nagasaka, H.; Miida, T.; Yorifuji, T.; Hirano, K.; Inui, A.; Fujisawa, T.; Tsukahara, H.; Hayashi, H.; Inomata, Y. Metabolic Improvements in Intrahepatic Porto-Systemic Venous Shunt Presenting Various Metabolic Abnormalities by 4-Phenylacetate. Clin. Chim. Acta 2013, 419, 52–56. [Google Scholar] [CrossRef]
- Kim, M.J.; Ko, J.S.; Seo, J.K.; Yang, H.R.; Chang, J.Y.; Kim, G.B.; Cheon, J.-E.; Kim, W.S. Clinical Features of Congenital Portosystemic Shunt in Children. Eur. J. Pediatr. 2012, 171, 395–400. [Google Scholar] [CrossRef]
- Sokollik, C.; Bandsma, R.H.J.; Gana, J.C.; Van Den Heuvel, M.; Ling, S.C. Congenital Portosystemic Shunt: Characterization of a Multisystem Disease. J. Pediatr. Gastroenterol. Nutr. 2013, 56, 675–681. [Google Scholar] [CrossRef]
- Nii, A.; Takehara, H.; Kuyama, H.; Shimada, M. Successful Preemptive Surgical Division of Type 2-Congenital Extrahepatic Portosystemic Shunt in Children. J. Med. Invest. 2009, 56, 49–54. [Google Scholar] [CrossRef]
- Robinson, E.B.; Jordan, G.; Katz, D.; Sundaram, S.S.; Boster, J.; Brigham, D.; Ladd, P.; Chan, C.M.; Shay, R.L.; Ochmanek, E.; et al. Congenital Portosystemic Shunts: Variable Clinical Presentations Requiring a Tailored Endovascular or Surgical Approach. JPGN Rep. 2023, 4, e279. [Google Scholar] [CrossRef]
- Murayama, K. Significant Correlations between the Flow Volume of Patent Ductus Venosus and Early Neonatal Liver Function: Possible Involvement of Patent Ductus Venosus in Postnatal Liver Function. Arch. Dis. Child. - Fetal Neonatal Ed. 2005, 91, F175–F179. [Google Scholar] [CrossRef]
- Hosmer, D.W.; Lemeshow, S.; Sturdivant, R.X. Applied Logistic Regression; Wiley Series in Probability and Statistics; 3. Aufl. Wiley: Hoboken, N.J, 2013; ISBN 978-0-470-58247-3. [Google Scholar]
- Ifuku, T.; Suzuki, S.; Nagatomo, Y.; Yokoyama, R.; Yamamura, Y.; Nakatani, K. Congenital Portosystemic Venous Shunt Associated with 22q11.2 Deletion Syndrome: A Case Report. BMC Pediatr. 2022, 22, 379. [Google Scholar] [CrossRef]
- Takama, Y.; Nakamura, T.; Santo, K.; Yoneda, A. Liver Resection for a Congenital Intrahepatic Portosystemic Shunt in a Child with Hyperammonemia and Hypermanganesemia: A Case Report. Surg. Case Rep. 2020, 6, 73. [Google Scholar] [CrossRef]
- Cho, Y.; Tokuhara, D.; Shimono, T.; Yamamoto, A.; Higashiyama, S.; Kotani, K.; Kawabe, J.; Okano, Y.; Shiomi, S.; Shintaku, H. Role of Per-Rectal Portal Scintigraphy in Long-Term Follow-up of Congenital Portosystemic Shunt. Pediatr. Res. 2014, 75, 658–662. [Google Scholar] [CrossRef]
Figure 1.
Flow diagram of patients analyzed in this study.
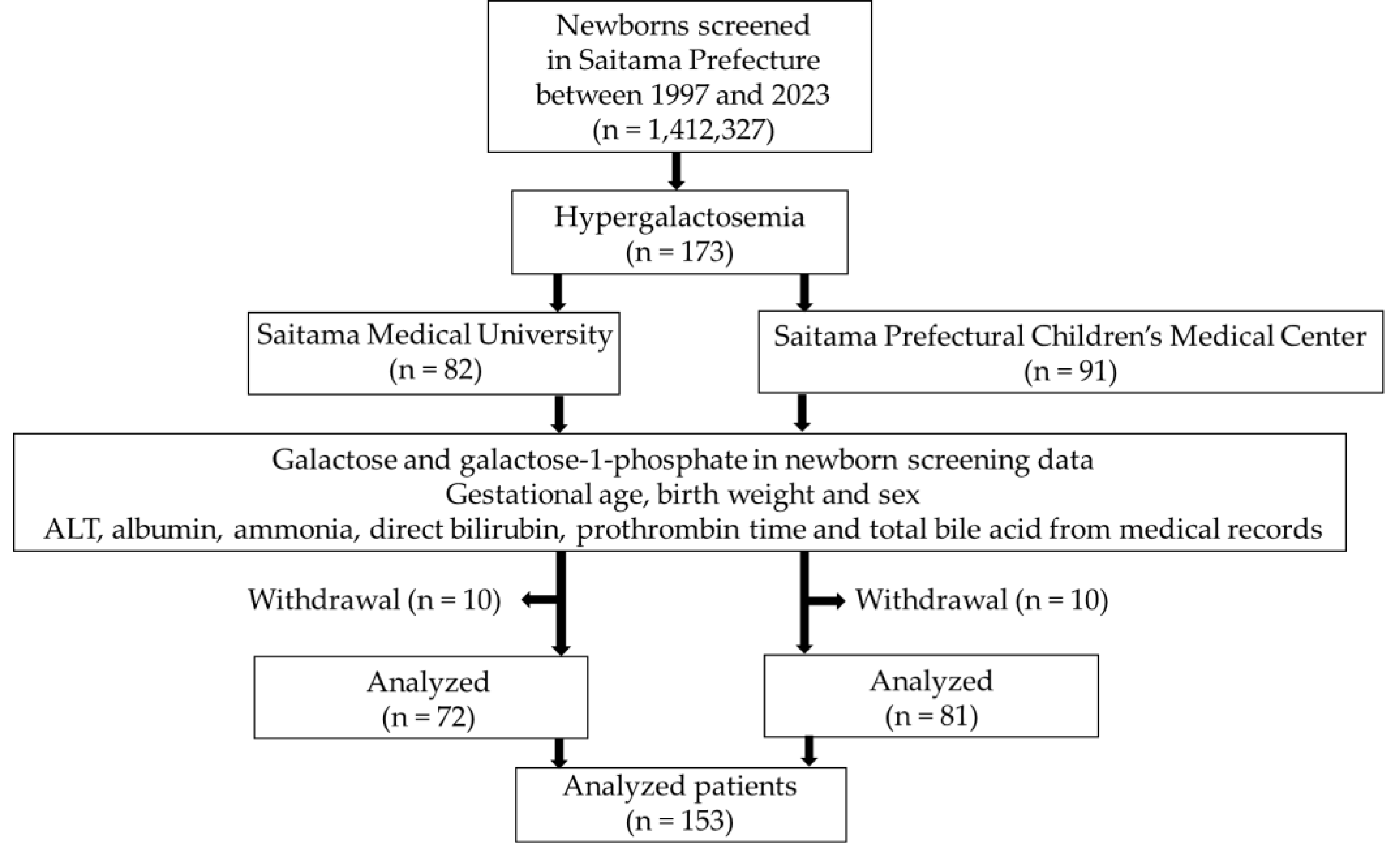
Figure 2.
Receiver operating curve (ROC) for predicted probability of congenital portosystemic shunt (CPSS).
Figure 2.
Receiver operating curve (ROC) for predicted probability of congenital portosystemic shunt (CPSS).
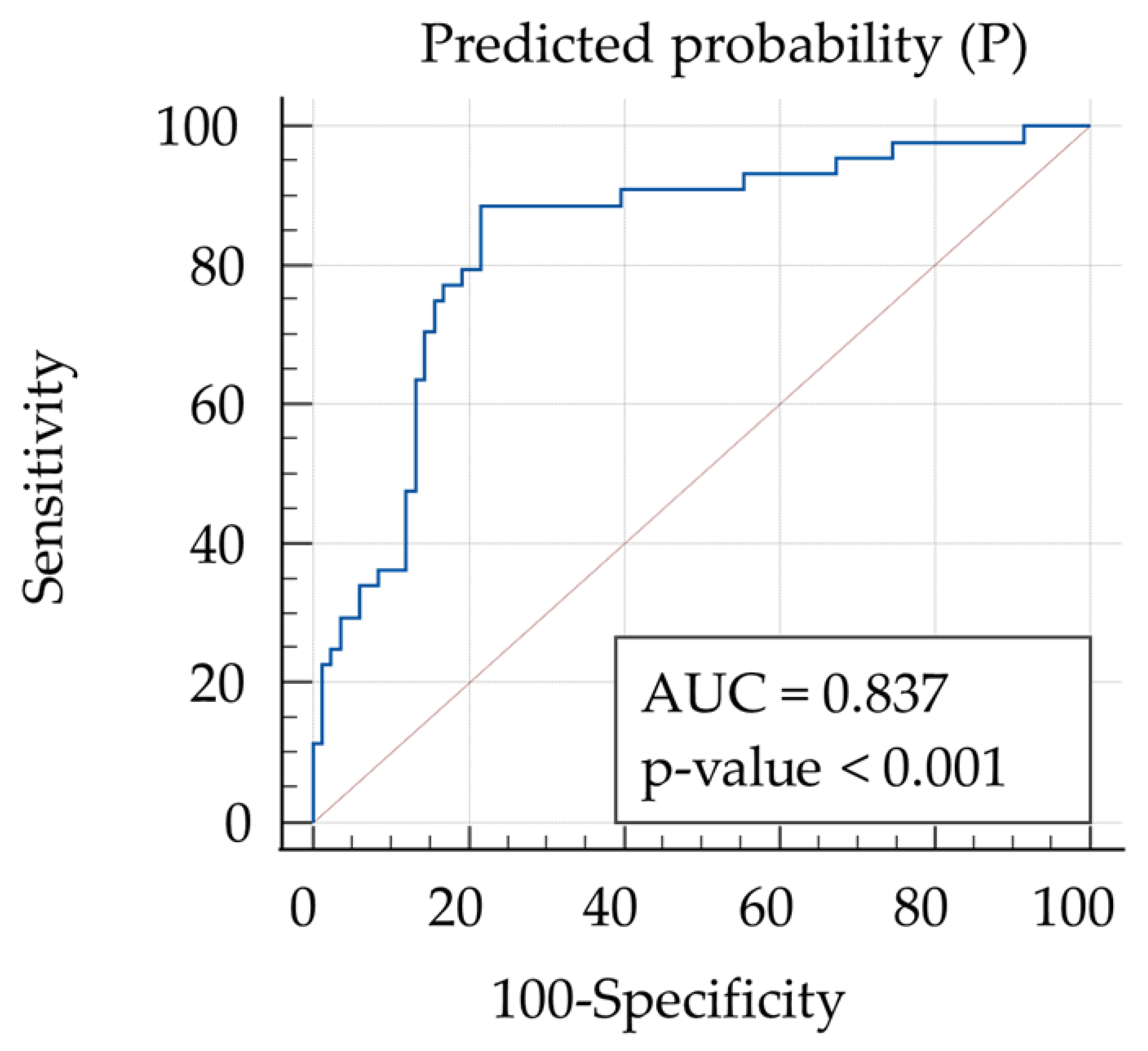
Figure 3.
Results of using P > 0.378 for the CPSS group and Transient group.
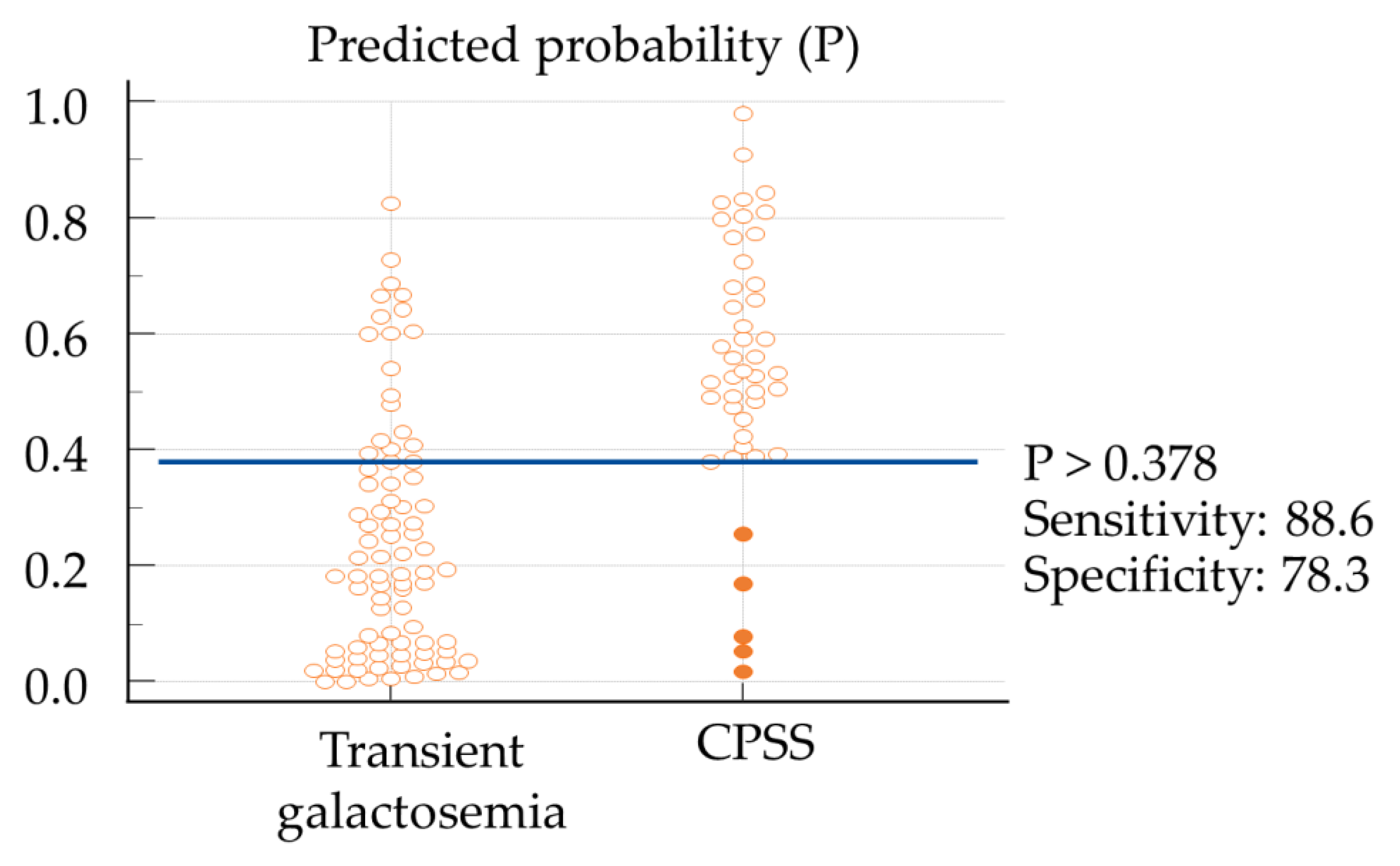

Table 1.
Final diagnosis of analyzed patients.
| Analyzed patients (n = 153) | |
| Final diagnosis | n (%) |
| Enzyme deficiency | 18* (12%) |
| Portosystemic shunt | 44 (29%) |
| Intrahepatic | 32 |
| Extrahepatic | 12 |
| Citrin deficiency | 7 (5%) |
| Transient galactosemia | 83 (54%) |
| Other | 1 (0%) |
*GALT heterozygous, 2 cases; GALK, 2 cases; GALE, 11 cases; GALM, 3 cases.
Table 2.
Characteristics of patients with surgical interventions.
| Case | Type of shunt | Anatomy | Clinical features |
Treatment | Gal-1-P /Gal |
TBA (μmol/L) |
NH3 (μg/dL) |
P |
|---|---|---|---|---|---|---|---|---|
| 1 | extrahepatic | IMV-LFV | no symptom | endovascular | 2.73 | 56.7 | 90 | 0.65 |
| 2 | extrahepatic | PV-LRV | no symptom | endovascular | 1.25 | 47.2 | 132 | 0.83 |
| 3 | extrahepatic | absence of PV | no symptom | LT | 0.62 | 20.0 | 53 | 0.38 |
| 4 | extrahepatic | hypoplastic PV, SMV-LHV | MR | endovascular | 1.69 | 26.6 | 56 | 0.39 |
| 5 | extrahepatic | absence of PV, SMV-azygos vein | unclear | unclear | 0.80 | 80.0 | 68 | 0.66 |
| 6 | extrahepatic | SV-LRV | no symptom | endovascular | 3.97 | 28.3 | 40 | 0.25 |
| 7 | extrahepatic | SV-LRV | MR | endovascular | 1.98 | 72.6 | 45 | 0.47 |
| 8 | extrahepatic | hypoplastic PV, SV-LRV | Hypermanganesemia, hepatic atrophy |
surgical | 0.70 | 77.4 | 109 | 0.83 |
| 9 | extrahepatic | PV-RA | no symptom | surgical | 2.88 | 114.8 | 81 | 0.77 |
| 10 | extrahepatic | SV-LRV | no symptom | surgical | 1.67 | 68.0 | 54 | 0.52 |
| 11 | intrahepatic | PDV | heart failure with COA |
operation for COA | 0.80 | 137.2 | 68 | 0.81 |
| 12 | intrahepatic | PV-LHV | no symptom | endovascular | 1.69 | 150.6 | 102 | 0.91 |
| 13 | intrahepatic | PDV | no symptom | endovascular | 0.69 | 12.6 | 84 | 0.52 |
Gal-1-P, galactose-1 phosphate; Gal, galactose; TBA, blood total bile acid; NH3, ammonia; IMV, inferior mesenteric vein; FV, femoral vein; PV, portal vein; RV, renal vein; SMV, superior mesenteric vein; RA, right atrium; PDV, patent ductus venosus; SV, splenic vein; HV, hepatic vein; COA, coarctation of the aorta; MR, mental retardation; LT, liver transplantation.
Table 3.
Clinical characteristics of patients with portosystemic shunt and temporary galactosemia.
| CPSS (n = 44) |
Transient galactosemia (n = 83) |
p-value | |
|---|---|---|---|
| Birth weight, g, mean (SD) | 2887.4 (422.0) | 2988.7 (409.1) | 0.19 |
| Sex ratio, male:female | 24:20 | 52:31 | 0.45 |
| Galactose, mg/dL, median (IQR) | 5.65 (4.00-9.58) | 2.80 (1.20-4.60) | <0.001 |
| Total galactose, mg/dL, mean (SD) | 12.95 (5.48) | 17.70 (6.75) | <0.001 |
| Gal-1-P, mg/dL, median (IQR) | 7.20 (3.67-11.40) | 21.30 (8.64-27.80) | <0.001 |
| Gal-1-P/Gal, median (IQR) | 1.05 (0.61-1.95) | 7.69 (1.34-20.90) | <0.001 |
| ALT, U/L, median (IQR) | 18.00 (14.00-26.75) | 18.00 (14.00-22.00) | 0.37 |
| Albumin, g/dL, mean (SD) | 3.63 (0.35) | 3.80 (0.34) | 0.009 |
| Ammonia, μg/dL, median (IQR) | 63 (53-82) | 54 (42-64) | 0.002 |
| Prothrombin time, % median (IQR) | 86.00 (73.55-94.90) | 89.00 (83.00-96.30) | 0.07 |
| Total bile acid, μmol/L, median (IQR) | 53.50 (28.75-79.90) | 17.90 (11.00-41.20) | <0.001 |
| Direct bilirubin, mg/dL, median (IQR) | 0.45 (0.20-0.80) | 0.40 (0.20-0.60) | 0.46 |
Table 4.
Crude and adjusted odds ratios according to logistic regression analysis.
| Crude OR | 95%CI | Adjusted OR | 95%CI | Adjusted OR | 95%CI | p-value | |
|---|---|---|---|---|---|---|---|
| (enter) | (selected variables) | ||||||
| Birth weight, g | 1.00 | 0.99-1.00 | 1.00 | 0.99-1.01 | |||
| Sex, male | 0.72 | 0.34-1.51 | 0.54 | 0.18-1.53 | |||
| Gal-1-P/Gal | 0.87 | 0.80-0.94 | 0.89 | 0.81-0.96 | 0.89 | 0.82-0.96 | <.001 |
| ALT, IU/L | 1.03 | 0.99-1.07 | 1.03 | 0.97-1.10 | |||
| Albumin, g/dL | 0.23 | 0.07-0.71 | 0.27 | 0.05-1.30 | |||
| Ammonia, μg/dL | 1.03 | 1.01-1.05 | 1.03 | 1.00-1.06 | 1.02 | 1.00-1.05 | 0.03 |
| Prothrombin time, % | 0.98 | 0.95-1.01 | 0.97 | 0.93-1.00 | |||
| Total bile acid, mg/dL | 1.02 | 1.01-1.04 | 1.02 | 1.00-1.03 | 1.01 | 1.00-1.03 | 0.02 |
| Direct bilirubin, mg/dL | 1.84 | 0.73-4.62 | 0.37 | 0.10-1.30 | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



