
Submitted:
26 June 2024
Posted:
27 June 2024
You are already at the latest version
Abstract
Aim: To evaluate the clinical findings of glucose 6 phosphate dehydrogenase(G6PD) and pyruvate kinase(PK) deficiency in prolonged jaundice. To determine whether systemic-immune-inflammation index(SII), neutrophil-to-lymphocyte ratio(NLR) and platelet-to-lymphocyte ratio (PLR) can be used in the diagnosis of neonatal prolonged jaundice. Methods: In full term neonates with hyperbilirubinemia who were admitted to Medicine Hospital between January 2019 and January 2024 with the complaint of jaundice, 167 infants with a serum bilirubin level above 10 mg/dL, whose jaundice persisted after the 10th day, were included in the study. Results: G6PD was negatively correlated with NLR, SII, age, and Hct. There was a negatively poor correlation between G6PD and NLR and a negatively moderate correlation between G6PD and SII when adjusted for age and Hct. PK showed no significant correlation with G6PD, NLR, PLR, SII, age, and Hct. A linear relationship was observed between G6PD and SII and NLR. Conclusions: NLR and SII can be easily calculated in the evaluation of prolonged jaundice in G6PD deficiency has a considerable advantage. NLR and SII levels may contribute by preventing further tests for prolonged jaundice and regulating its treatment. It may be useful to form an opinion in emergencies and in the early period.
Keywords:
Prolonged jaundice
; breast milk
; glucose 6 phosphate dehydrogenase
; pyruvate kinase
; systemic-immune-inflammation index
; neutrophil-to-lymphocyte ratio
Introduction
At least two-thirds of newborns become clinically jaundiced in the first week of life [1].
Prolonged jaundice is defined as bilirubin level above 10 mg/dL on the 14th day after birth in a term baby and on the 21st day in a premature baby [2,3]. The most common cause of prolonged jaundice is breast milk jaundice, but it is important because it can also be a symptom of a serious underlying disease [4]. The most important step in the follow-up of these babies is to determine the etiology.
In babies with prolonged jaundice, a detailed history should be taken and a detailed physical examination should be performed. Then, as initial tests, direct-indirect bilirubin levels, mother-baby blood groups, direct Coombs test, complete blood count, peripheral smear, glucose 6 phosphate dehydrogenase (G6PD) enzyme level, thyroid function tests [thyroid stimulating hormone (TSH), thyroxine). (free T4)], urinalysis, urine culture and reducing substance in urine should be investigated [2].
Erythrocyte enzyme defects involved in the etiology of neonatal jaundice are G6PD, pyruvate kinase (PK), 5′ nucleotidase, glucose phosphate isomerase, glutathione synthetase and fructokinase. G6PD deficiency is the most common enzyme deficiency and shows X-dependent transition. G6PD deficiency is more common in male babies. Clinical findings vary. It presents with jaundice as a result of hemolysis that develops in babies who are under oxidant stress, have acidosis, hypoglycemia or infection during the neonatal period. Jaundice usually develops between 24 and 72 hours [5,6,7,8]. Another important enzyme deficiency is PK deficiency, which is an autosomal recessive inheritance and causes hemolytic jaundice in the neonatal period. Diagnosis can be made by enzyme determination in patients with hemolytic hyperbilirubinemia [8].
The role of inflammation in the etiology of prolonged neonatal jaundice is not fully known. Levels of blood-based systemic inflammation markers (complete blood count (CBC), hemoglobin, neutrophil-to-lymphocyte ratio (NLR), erythrocyte distribution width, etc.), which are considered prognostic indicators for many diseases, have been investigated [6,9].
New generation inflammation markers have been studied in limited numbers in neonatal prolonged jaundice. The aim of the study was to determine the clinical findings of G6PD and PK deficiency in neonatal prolonged jaundice, to prevent further examinations for prolonged jaundice, and to contribute by regulating its treatment. At the same time, it is to determine whether systemic-immune-inflammation index (SII), NLR and platelet-to-lymphocyte ratio (PLR) can be used in addition to conventional CBC parameters in the diagnosis of neonatal prolonged jaundice.
Materials and Methods
Study Design and Participants
Ethical approval of this study was obtained by the Non-Interventional Ethics Committee of the Medical Faculty of Istanbul Atlas University (26.10.2022; No: E-22686390-050.99-21197). The study was performed in accordance with the Helsinki Declaration, and informed consent was obtained from the families of all patients prior to their inclusion in the study.
In full term neonates with hyperbilirubinemia who were admitted to Medicine Hospital between January 2019 and January 2024 with the complaint of jaundice, 167 infants with a serum bilirubin level above 10 mg/dL, whose jaundice persisted after the 10th day, were included in the study. A flow chart of the selection of cases is shown in Figure 1. Detailed history was taken from the families of infants with prolonged jaundice. The age of the cases was calculated in days, and the day of birth was accepted as day zero. The day of onset of jaundice was determined as the day the family first noticed jaundice. Newborns with jaundice above physiologic values and prolonged jaundice with no other cause to explain jaundice were included in the study. In the postnatal period, the day of onset of jaundice, first feeding, time of first urination, first fecal output and complaints were questioned. Newborns diagnosed with prolonged jaundice with a total bilirubin level above 10 mg/dL were followed in the clinic. Clinically, pathologic findings on physical examination were evaluated. Other systemic examinations were performed in terms of activity, skin color, neonatal reflexes and focus of infection.
In our clinic, phototherapy and exchange transfusion decisions were made according to the bilirubin threshold values recommended by the American Academy of Pediatrics (AAP) [10]. The decision to discharge the patients was made by the research doctor according to Nelson Texts icteric neonatal discharge protocol [1].
Breast milk jaundice was diagnosed by exclusion, in infants who were exclusively breastfed and older than 14 days, with no other identifiable pathogenic factors for jaundice.
Inclusion criteria
i) Patients with prolonged jaundice exceeding 15 days and total bilirubin values exceeding 10 mg/dL; ii) Patients who appear icteric on physical examination during routine controls; iii) Patients with hemolytic anemia and negative direct coombs; iv) Patients who attended regularly for up to 3 months, as patients were invited for the first 6 monthly check-ups; v) Prolonged jaundice was differentiated by looking at direct and indirect bilirubin and those who were negative by measuring direct coombs were included.
Exclusion Criteria
Premature infants, infants undergoing phototherapy and blood exchange, congenital malformations, congenital infections, bacterial infection, hypoxic ischemic encephalopathy, respiratory distress, neonatal hemolytic disease, sepsis, transfusion exchange were excluded from the study. The mother had hypertensive, renal, hepatic, or hematologic diseases, was taking any medication, or was a tobacco user. Patients with thyroid stimulating hormone (TSH) levels higher than 20 mU/L were considered congenital hypothyroidism and excluded from the study. Those with TSH levels within normal limits were included.
Direct Coombs test positivity was accepted as one of the diagnostic criteria in Rh incompatibility, whereas direct Coombs test positivity was not required in ABO incompatibility.
Laboratory Assessments
Venous blood samples were taken from all patients at the time of admission. For CBC, 0.5-2 ml blood was drawn into purple capped ethylenediaminetetraacetic acid (EDTA) tubes and measured in an automatic blood count device (Sysmex XN 1000, Roche Diagnostics GmbH, Mannheim, Germany) within 1 hour at the latest. The NLR and PLR were calculated as [platelet count x neutrophil count]/lymphocyte count. The SII was calculated as platelet count × neutrophil count/lymphocyte count [11]. Reticulocytes were done manually by Brilliant Cresyl blue with correction formula, Routine biochemical parameters were measured in an autoanalyzer (ARCHITECT c8000 Abbott, USA).
Measurement of Glucose 6 Phosphate Dehydrogenase (G6PD)
The G6PD activity in whole blood was measured by G6PD kits (Ben Srl Biochemical Enterprise, Milan, Italy) that used a spectrophotometric assay on Roche Cobas c 501, following the manufacturer’s instructions.
Measurement of Pyruvate Kinase (PK)
The PK activity in whole blood was measured by pyruvate kinase kits (Ben Srl Biochemical Enterprise, Milan, Italy) that used spectrophotometric assay on Roche Cobas Mira, following the manufacturer’s instructions.
Statistical Analysis
Statistical Package for the Social Sciences version 29.0 software package for Windows (IBM Corp., Armonk, NY, USA) was used for data evaluation and analysis. Jamovi 2.3.18 was used to create figures. Categorical variables are presented as frequencies (n) and percentages (%), and numerical variables are presented as mean ± standard deviation and median (25. Percentile- 75th percentile). The Kolmogorov‒Smirnov test was applied for normality analysis. The Mann-Whitney U test was used to compare continuous variables between two independent groups. The Spearman correlation and linear regression analysis were used to determine the association between two continuous variables. Also, a partial correlation was used to show relationship between two continuous variables whilst controlling for the effect of other continuous variables. A value of p < 0.05 was accepted as statistically significant.
Results
The mean age was 31±6 days and 63.5% of the patients were male. All patients had negative direct Coombs test, negative urine culture and normal abdominal USG. All patients were breastfed, and 12 patients (7.2%) were also receiving formula. ABO incompatibility was present in 6% (n:10), Rh incompatibility in 9% (n:15), and reductant substance in 16.25% (n:27) of the patients. Seven patients (4.2%) were hospitalized, and the median hospitalization median was 1(1-1) day. The median day of jaundice onset was 2(1-2) days. The median time to fall below TB=8 was 80 (80-80) days. The mean gestational week of the patients was 37±1 weeks (Table 1).
Table 2 shows the laboratory results of the patients. The WBC median was 9110 (7910-11100), Hct median 37.1 (32.5-41.4), PLT median 328 (277-400), NLR median 0.3 (0.21-0.37), PLR median 55.38 (43.05-70.76) and SII median 95.73 (64.61-125.96) (Table 2).
There was no statistically significant difference in NLR, PLR, SII, G6PD, PK values according to gender, hospitalization status, formula use, ABO incompatibility, Rh incompatibility and reductant substance (Table 3).
G6PD was negatively perfectly correlated with NLR (r: -1; p<0.001; Figure 2), negatively strongly correlated with SII (r: -0.837; p<0.001, Figure 3), poor correlated with age (r:0.296; p<0.001), and poor correlated with Hct (r: -0.285; p<0.001). There was no significant correlation between G6PD and PK (r:0.00; p:0.960). There was no significant correlation between PK and NLR, PLR, SII, age, Hct (Table 4). Furthermore, when adjusted for age and Hct, there was a negatively poor correlation between G6PD and NLR (r: -0.212; p:0.006) and a negatively moderate correlation between G6PD and SII (r: -0.470; p<0.001) (Table 5).
According to the results of linear regression analysis, 1-unit increase in NLR decreased G6PD by 1.407 units when adjusted for age and Hct (Unstandardized (B): -1.407 (-2.411/-0.402); p:0.006). When adjusted for age and Hct, 100-unit increase in SII decreased G6PD by 2.581 units (Unstandardized (B): -2.581 (-3.331/-1.831); p<0.001). The R square of model 1 with NLR, age and Hct was 0.198, while the R square of model 2 with SII, age and Hct was 0.346 (Table 6).
Discussion
Prolonged jaundice is clinically detected jaundice that exceeds the physiologic jaundice period. Among the enzymopathies, G6PD and PK deficiencies are the most common defects in diverse ethnic groups [5,7]. The majority of prolonged jaundice in term newborns is caused by indirect hyperbilirubinemia, and a significant part of this is breast milk jaundice. Prolonged jaundice in newborns can sometimes be associated with underlying inflammation or infection. [12,13]. The most important finding of the study, G6PD was negatively perfectly correlated with NLR, negatively strongly correlated with SII, poor correlated with age, and poor correlated with Hct. Furthermore, when adjusted for age and Hct, there was a negatively poor correlation between G6PD and NLR and a negatively moderate correlation between G6PD and SII. Neonates did not have obvious signs of hemolysis such as anemia and reticulocytosis. A 1 unit (about 1 standard deviation) increase of NLR reduces G6PD by 1,407. A 100 unit (almost 1 standard deviation) increase of SII reduces G6PD by 2,581. The explanatory power of the models is also very different. The model with NLR is 0.198; the model with SII is 0.346. Therefore, SII can be used as a better measure than NLR. The association between G6PD deficiency and markers of inflammation such as NLR and SII may suggest a potential link between inflammation and the pathophysiology of prolonged jaundice in term newborns with G6PD deficiency.
Most newborn babies are clinically jaundiced. Jaundice is frequently mild, self-limiting and generally accepted as physiologic However, some jaundices do not regress as expected and prolonged jaundice may occur [14,15]. There are various factors in the etiology of prolonged jaundice and determination of the cause is important since the treatment, follow-up and prognosis of each of them differ [16,17]. In current study, all patients were breastfed, and 12 patients (7.2%) were also receiving formula. When the cases were evaluated etiologically, all of the newborns consisted of prolonged jaundice due to breast milk. There were no cases of prolonged jaundice due to urinary tract infection and sepsis, prolonged jaundice due to hemolytic diseases and prolonged jaundice due to congenital hypothyroidism. The cases admitted to the study with prolonged jaundice included those in whom no underlying cause could be identified and who were considered to have prolonged neonatal jaundice due to breast milk. It has been reported that approximately one third of breastfed babies are clinically jaundiced in the third week of life and two thirds of these babies have high indirect hyperbilirubinemia [18]. Although it was first suggested that pregnanediol, which is found in breast milk and is an inhibitor of hepatic glucuronyl transferase enzyme, may cause jaundice, it is currently accepted that it is not the primary factor but has a contribution in the event [18,19]. The mechanism that attracts the most attention and is currently discussed is that an undefined factor presents in breast milk increases intestinal absorption of bilirubin. In addition, it has also been suggested that increased bilirubin absorption rather than high bilirubin production increases breast milk jaundice [18,20]. Although breast milk-induced jaundice may last up to the 16th week, it returns to normal in all babies during this period [18,21]. Although breast milk jaundice is a prolongation of normal physiologic jaundice, pathologic causes of jaundice should be ruled out in extremely high values [18]. In our study, the diagnosis of breast milk jaundice was made after excluding other pathologic causes of jaundice. In our study, the diagnosis of breast milk jaundice was made after excluding other pathologic causes of jaundice. In previous studies, it was reported that serum bilirubin levels were 10-17 mg/dL in the majority of breastfed infants [21,22] and the findings in our study are compatible with these studies. Therefore, other etiologies should be considered especially in infants with elevated bilirubin levels above 17 mg/dL. In addition, hemogram, total, direct and indirect bilirubin levels and thyroid function tests should be evaluated to determine the etiology in bilirubin levels below 17 mg/dL. In breast milk jaundice, treatment is not applied up to bilirubin levels of 20 mg/dL, phototherapy may be applied at bilirubin levels above 25 mg/dL [18]. Therefore, phototherapy was not applied to the cases in our study. Since we did not consider Gilbert syndrome clinically according to the present values, we did not perform UGT1A1 gene sequence analysis.
G6PD enzyme deficiency is the most common X-linked erythrocyte enzyme defect. In the context of prolonged jaundice, G6PD deficiency is relevant because it can predispose individuals to hemolysis (destruction of red blood cells), leading to an increase in bilirubin levels and exacerbating jaundice. The National Institute for Health and Clinical Excellence (NICE) recommends the analysis of direct bilirubin, urine culture, G6PD, CBC, and blood group in the evaluation of prolonged jaundice [14]. In current study, it was determined that G6PD deficiency in the infant led to the development of jaundice. There was no statistically significant difference in G6PD values according to gender, hospitalization status, formula use, ABO incompatibility, Rh incompatibility and reductant substance. These findings suggest that G6PD values were not significantly influenced by gender, hospitalization status, formula use, ABO incompatibility, Rh incompatibility, or the presence of specific reductant substances in the study population. It’s essential to consider these results in the context of the specific study population and methodology used to ensure the reliability and generalizability of the findings.
PK deficiency is an autosomal recessive enzyme deficiency that can be encountered in all populations and is less common compared to G6PD deficiency. In contrast to G6PD deficiency, reticulocytosis, jaundice and anemia are present from the beginning. Jaundice can occur at levels high enough to require exchange transfusion. The enzyme deficiency is not only qualitative, but also due to a structural defect or lack of stabilization. PK deficiency should also be considered in a baby with prolonged jaundice and hemolytic anemia if spherocytosis is absent and the coombs test is negative [23]. In current study, there was no statistically significant difference in PK values according to gender, hospitalization status, formula use, ABO incompatibility, Rh incompatibility and reductant substance. Overall, these findings suggest that PK values were not significantly influenced by gender, hospitalization status, formula use, ABO incompatibility, Rh incompatibility, or the presence of specific reductant substances in the study population. There was no significant correlation between G6PD and PK activities. Despite these findings, it’s important to consider these results within the context of the specific study population and methodology used to ensure the reliability and generalizability of the findings. PK deficiency should be considered in infants with negative Coombs test and hemolytic anemia, in case of prolonged jaundice without erythrocyte membrane defect [24,25,26].
In recent years, inflammatory parameters such as NLR, PLR, and SII have been used as an indicator in various diseases [27,28,29,30,31,32,33,34]. Karabulut et al. [28] suggested that NLR and mean platelet volume (MPV) may be used in addition to conventional parameters such as CRP in the diagnosis and subsequent management of early-onset neonatal sepsis. Kurt et al. [27] reported that the decrease in NLR and lymphocyte/monocyte ratio (LMR) after phototherapy could potentially be used in the evaluation of phototherapy’s effect on peripheral blood cells. Li et al. [29] demonstrated that there existed a relationship between NLR and the presence of neonatal sepsis. Cakır et al. [30] suggested that systemic inflammation response index (SIRI) may be a useful biomarker for predicting moderate to severe bronchopulmonary dysplasia (BPD) and a marker of clinical importance in the follow-up of infants with BPD. In current study, although CRP levels are within normal limits, G6PD was negatively strongly correlated with NLR and SII. This implies that lower G6PD levels are associated with higher systemic inflammation, as reflected by an elevated SII. These correlations suggest that in individuals with jaundice, lower G6PD levels (indicating G6PD deficiency) are associated with higher levels of systemic inflammation, as measured by NLR and SII. This association may have clinical implications for managing jaundice, particularly in individuals with G6PD deficiency, as inflammation can exacerbate symptoms and complications associated with jaundice. Furthermore, when adjusted for age and Hct, there was a negatively correlation between G6PD and NLR and SII. Adjusting for age and hematocrit helps to control for potential confounding factors and allows for a more precise assessment of the relationship between G6PD levels and markers of systemic inflammation (NLR and SII) in the context of jaundice. These findings suggest that G6PD deficiency may contribute to increased systemic inflammation in individuals with jaundice, independent of age and Htc levels. However, it’s essential to interpret these results cautiously and consider other potential confounders or factors that may influence the relationship between G6PD levels and markers of inflammation. Further research is needed to validate these findings and understand the underlying mechanisms linking G6PD deficiency and inflammation in individuals with jaundice. Although the findings in our study need to be supported by prospective randomized studies, we think that the use of NLR and SII as an easily calculable method in clinical practice may be useful in predicting prolonged jaundice.
The mechanism of prolonged jaundice in otherwise healthy breastfeeding newborns is still unclear. Since prolonged jaundice may be the first sign of G6PD deficiency, the enzyme level should be checked in newborns diagnosed with prolonged jaundice and G6PD should be preferred over PK in prolonged neonatal jaundice due to breast milk jaundice. In communities where G6PD deficiency is prevalent, hyperbilirubinemia can be detected early in cord blood and neurotoxicity can be prevented. The explanatory power of the models is also very different. The model with NLR is 0.198; the model with SII is 0.346. Therefore, SII can be used as a better measure than NLR. The fact that these values are included in a routine test such as a CBC provides convenience in terms of use. Cases with elevated NLR and SII after birth should be followed up more closely and it should be kept in mind that prolonged jaundice may develop.
Funding
The author declared that this study has received no financial support.
Institutional Review Board Statement
This prospective study was approved by the Istanbul Atlas University ethics committee, Istanbul (26.10.2022; No: E-22686390-050.99-21197) and was conducted in accordance with the Declaration of Helsinki. Informed consent was obtained from the legal guardian(s) of subjects.
Informed Consent Statement
Not applicable.
Data Availability Statement
Participant-level data are available from the corresponding author.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Behrman RE, Kliegman RM, Jenson HB. Jaundice and hyperbilirubinemia in the newborn. In: Nelson Textbook of Pediatrics. 16th ed. Saunders; 2021, part 11, chap 102:753-766.
- Giannattasio A, Ranucci G, Raimondi F. Prolonged neonatal jaundice. Ital J Pediatr. 2015;41(Suppl 2):A36. [CrossRef]
- Kaplan M, Merlop P, Regev R. Israel guidelines for the mamagement of neonatal hyperbilirubinemia and prevention of kernicterus. J Perinatol 2008;28:389-97. [CrossRef]
- Weng YH, Cheng SW, Yang CY, Chiu YW. Risk assessment of prolonged jaundice in infants at one month of age: A prospective cohort study. Sci Rep. 2018;8(1):14824. [CrossRef]
- Kassahun W, Tunta A, Abera A, Shiferaw M. Glucose-6-phosphate dehydrogenase deficiency among neonates with jaundice in Africa; systematic review and meta-analysis. Heliyon. 2023;9(7):e18437. [CrossRef]
- Zakerihamidi M, Moradi A, Boskabadi H. Comparison of severity and prognosis of jaundice due to Rh incompatibility and G6PD deficiency. Transfus Apher Sci. 2023;62(4):103714. [CrossRef]
- Abdel Fattah M, Abdel Ghany E, Adel A, Mosallam D, Kamal S. Glucose-6-phosphate dehydrogenase and red cell pyruvate kinase deficiency in neonatal jaundice cases in egypt. Pediatr Hematol Oncol. 2010;27(4):262-271. [CrossRef]
- Grace RF, Barcellini W. Management of pyruvate kinase deficiency in children and adults. Blood. 2020;136(11):1241-1249. [CrossRef]
- Cunningham AD, Hwang S, Mochly-Rosen D. Glucose-6- Phosphate dehydrogenase deficiency and the need for a novel treatment to prevent kernicterus. Clin Perinatol 2016;43:341-54. [CrossRef]
- Kemper AR, Newman TB, Slaughter JL, et al. Clinical Practice Guideline Revision: Management of Hyperbilirubinemia in the Newborn Infant 35 or More Weeks of Gestation. Pediatrics. 2022;150(3): e2022058859. [CrossRef]
- Okuyan O, Elgormus Y, Sayili U, Dumur S, Isık OE, Uzun H. The Effect of Virus-Specific Vaccination on Laboratory Infection Markers of Children with Acute Rotavirus-Associated Acute Gastroenteritis. Vaccines (Basel). 2023;11(3):580. [CrossRef]
- Ullah S, Rahman K, Hedayati M. Hyperbilirubinemia in Neonates: Types, Causes, Clinical Examinations, Preventive Measures and Treatments: A Narrative Review Article. Iran J Public Health 2016.45(5): 558- 568.
- Hall V, Avulakunta ID. Hemolytic diseases of the newborn. In: StatPearls [Internet]. Treasure Island, FL: StatPearls Publishing; 2023. Updated November 22, 2022. Accessed August 20, 2023.
- Rodie MD, Barclay A, Harry C, et al. NICE recommendations for the formal assessment of babies with prolonged jaundice: too much for well infants? Arch Dis Child. 2011;96(1):112-3. [CrossRef]
- Bhutani VK, Maisels MJ, Stark AR, Buonocore G: Expert Committee for Severe Neonatal Hyperbilirubinemia, Eurepean Society for Pediatric Research and American Academy of Pediatrics. Management of Jaundice and Prevention of Severe Hyperbilirubinemia in Infants ≥35 Weeks Gestation. Neonatology 2008; 94: 63-7. [CrossRef]
- Satrom KM, Farouk ZL, Slusher TM. Management challenges in the treatment of severe hyperbilirubinemia in low- and middle-income countries: Encouraging advancements, remaining gaps, and future opportunities [published correction appears in Front Pediatr. 2023 May 02;11:1181023]. Front Pediatr. 2023;11:1001141. [CrossRef]
- Gao C, Guo Y, Huang M, He J, Qiu X. Breast Milk Constituents and the Development of Breast Milk Jaundice in Neonates: A Systematic Review. Nutrients. 2023;15(10):2261. [CrossRef]
- Gartner LM. Breastfeeding and jaundice. J Perinatol 2001; 21: 25-9. [CrossRef]
- Arias IM, Gartner LM, Seifter S, Furman M. Prolonged neonatal unconjugated hyperbilirubinemia associated with breast feeding and a steroid, pregnane-3 (alpha), 20 (beta)-diol in maternal milk that inhibits glucuronide formation in vitro. J Clin Invest 1964;43: 2037-47. [CrossRef]
- Buiter HD, Dijkstra SS, Oude Elferink RF, Bijster P, Woltil HA, Verkade HJ. Neonatal jaundice and stool production in breast-or formula-fed term infants. Eur J Pediatr 2008; 167: 501-7. [CrossRef]
- Eghbalian F, Raeisi R, Faradmal J, Asgharzadeh A. The Effect of Clofibrate and Phototherapy on Prolonged Jaundice due to Breast Milk in Full-Term Neonates. Clin Med Insights Pediatr. 2023; 17:11795565231177987. [CrossRef]
- Ozdemir A, Kurtoglu S, Halis H, Bastug O. An evaluation of ursodeoxycholic acid treatment in prolonged unconjugated hyperbilirubinemia due to breast milk. Niger J Clin Pract. 2023;26(9):1226-1233. [CrossRef]
- Christensen RD, Eggert LD, Baer VL, et al. Pyruvate kinase deficiency as a cause of extreme hyperbilirubinemia in neonates from a polygamist community. J Perinatol 2010;30:233-6. [CrossRef]
- Aygün E, Yilmaz Semerci S. Prolonged Jaundice in Newborn [Internet]. Topics on Critical Issues in Neonatal Care. IntechOpen; 2022.
- McMahon JR, Stevenson DK, Oski FA. Physiologic Jaundice. In: Taeusch HW,Ballard RA, eds. Avery’s Disease of the Newborn 7th ed. Philadelphia, WBSaunders, 1998, pp 1003-1007.
- Yang YK, Lin CF, Lin F, et al. Etiology analysis and G6PD deficiency for term infants with jaundice in Yangjiang of western Guangdong. Front Pediatr. 2023; 11:1201940. [CrossRef]
- Kurt A, Tosun MS, Altuntaş N, Erol S. Effect of Phototherapy on Peripheral Blood Cells in Hyperbilirubinemic Newborns. J Coll Physicians Surg Pak. 2020;30(5):547-549. [CrossRef]
- Karabulut B, Alatas SO. Diagnostic Value of Neutrophil to Lymphocyte Ratio and Mean Platelet Volume on Early Onset Neonatal Sepsis on Term Neonate. J Pediatr Intensive Care. 2021;10(2):143-147. [CrossRef]
- Li T, Dong G, Zhang M, et al. Association of Neutrophil-Lymphocyte Ratio and the Presence of Neonatal Sepsis. J Immunol Res. 2020; 2020:7650713. [CrossRef]
- Cakir U, Tayman C, Tugcu AU, Yildiz D. Role of Systemic Inflammatory Indices in the Prediction of Moderate to Severe Bronchopulmonary Dysplasia in Preterm Infants. Arch Bronconeumol. 2023;59(4):216-222. [CrossRef]
- Zhang S, Luan X, Zhang W, Jin Z. Platelet-to-Lymphocyte and Neutrophil-to-Lymphocyte Ratio as Predictive Biomarkers for Early-onset Neonatal Sepsis. J Coll Physicians Surg Pak. 2021;31(7):821-824. [CrossRef]
- Pan R, Ren Y, Li Q, et al. Neutrophil-lymphocyte ratios in blood to distinguish children with asthma exacerbation from healthy subjects. Int J Immunopathol Pharmacol. 2023; 37:3946320221149849. [CrossRef]
- Chang LS, Lin YJ, Yan JH, Guo MM, Lo MH, Kuo HC. Neutrophil-to-lymphocyte ratio and scoring system for predicting coronary artery lesions of Kawasaki disease. BMC Pediatr. 2020;20(1):398. [CrossRef]
- Cine HS, Uysal E, Gurbuz MS. Is neutrophil-to-lymphocyte ratio a prognostic marker for traumatic brain injury in the pediatric population? Eur Rev Med Pharmacol Sci. 2023;27(20):9729-9737. [CrossRef]
Figure 1.
A flow chart of the selection of cases.
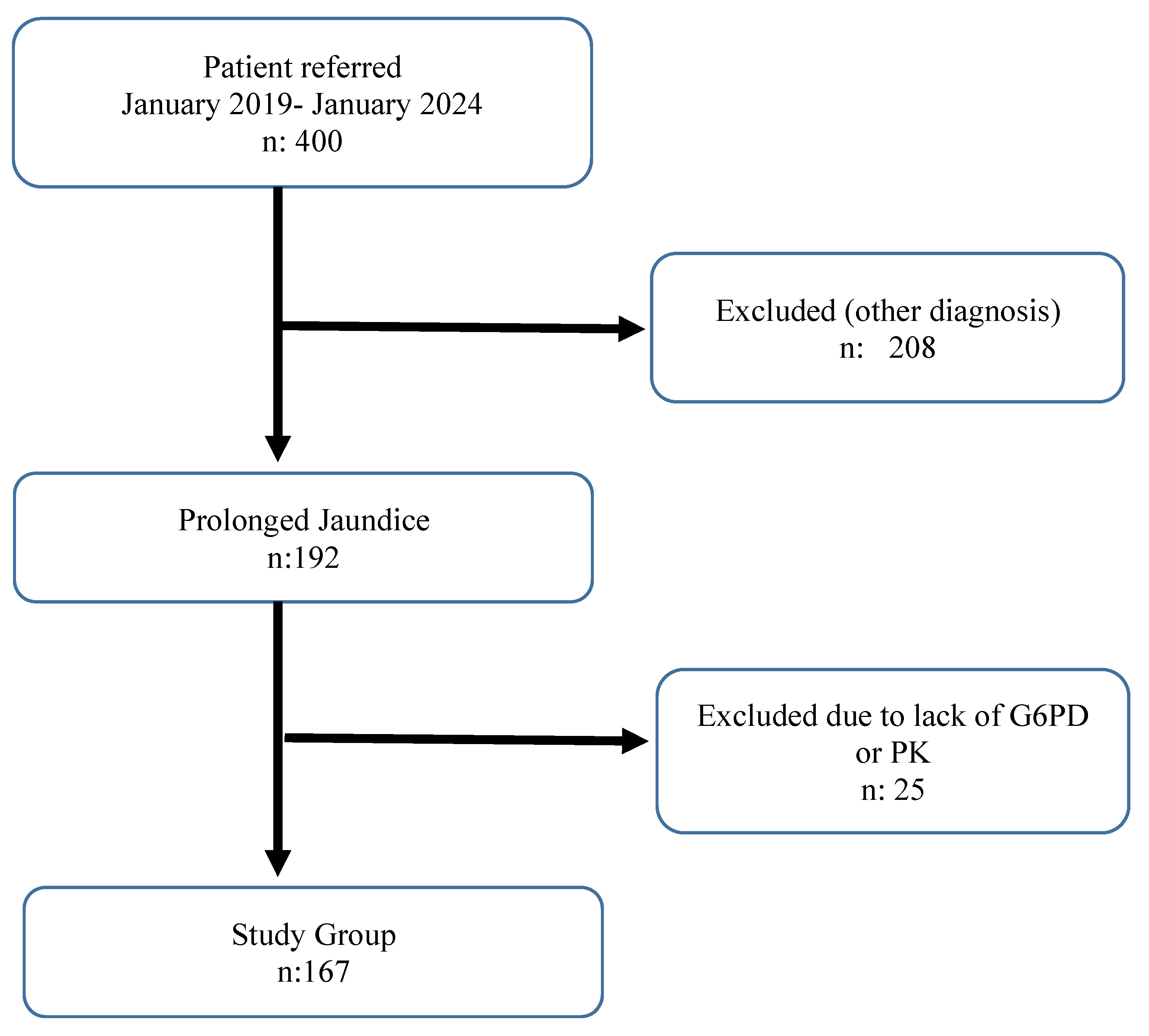
Figure 2.
The correlation between G6PD and NLR.
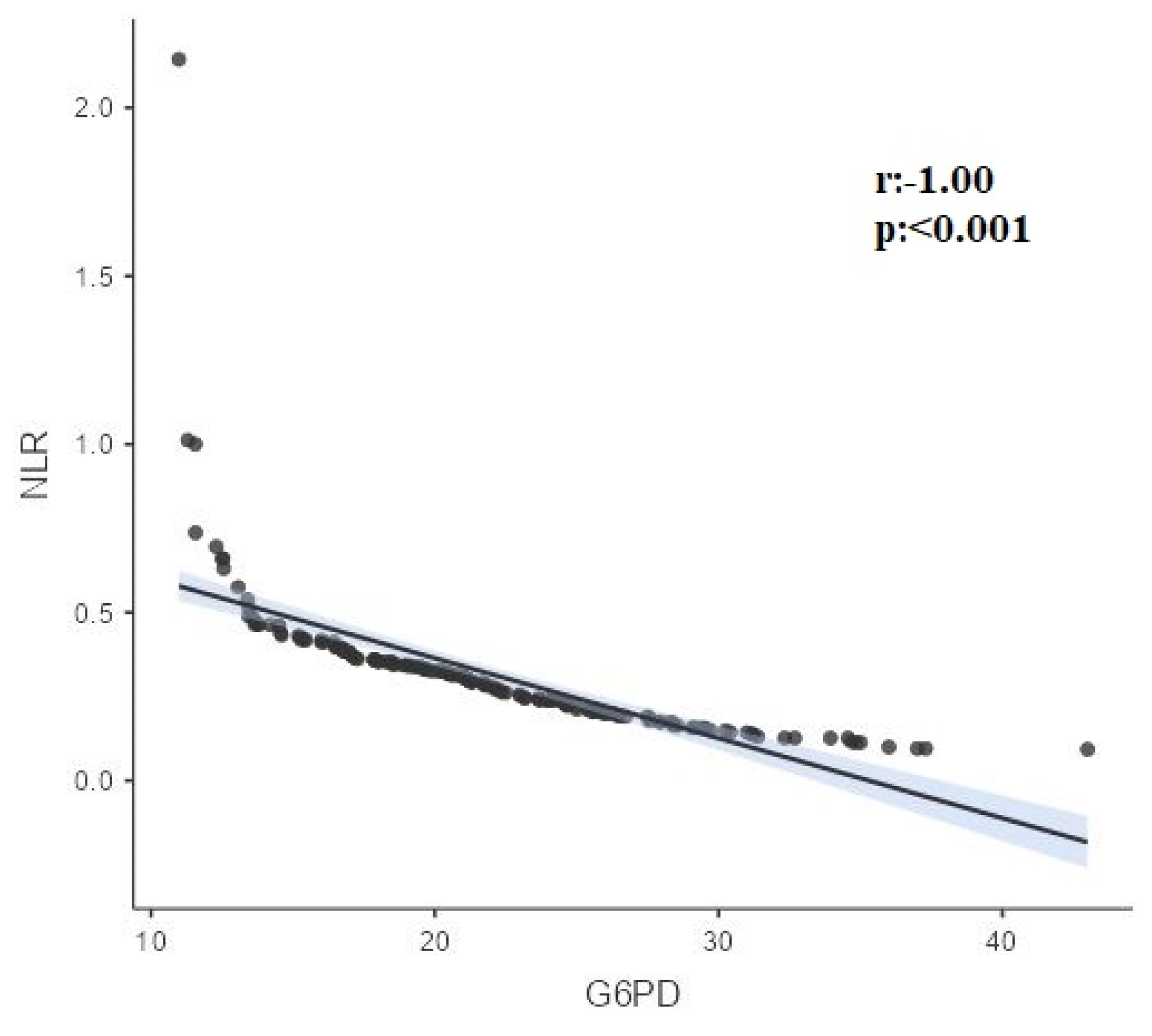
Figure 3.
The correlation between G6PD and SII.
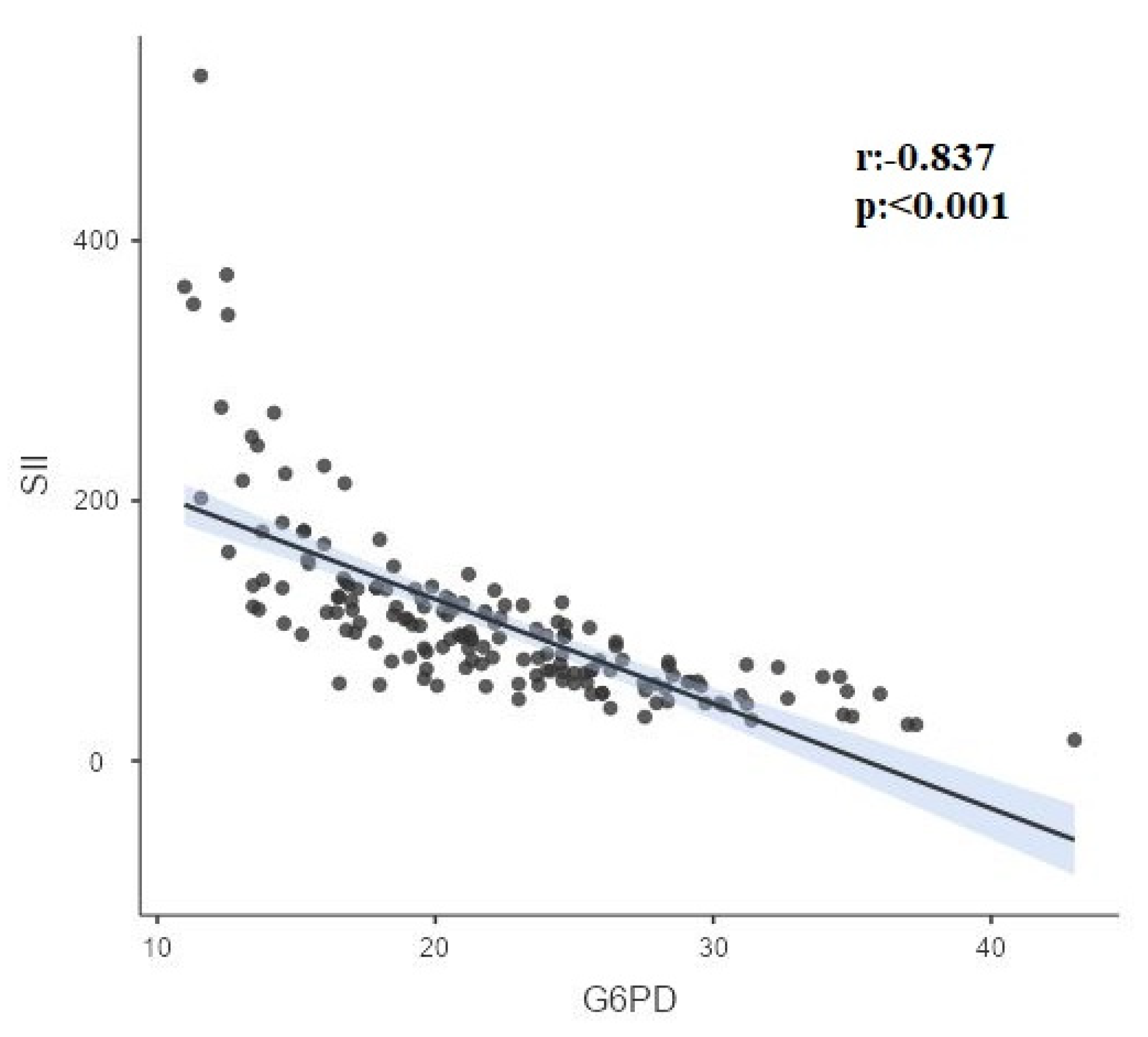

Table 1.
Demographic and clinical characteristics of the patients.
| n mean±std |
% Median(Q1-Q3) |
|
|---|---|---|
| Gender | ||
| Male | 106 | 63.5% |
| Female | 61 | 36.5% |
| Age (days) | 31±6 | 30(28-33) |
| Direct Cooms test | ||
| Negative | 167 | 100.0% |
| Urine Culture | ||
| No reproduction | 167 | 100.0% |
| Abdominal USG | ||
| Normal | 167 | 100.0% |
| Breast feeding | ||
| Yes | 167 | 100.0% |
| Formula | ||
| No | 155 | 92.8% |
| Yes | 12 | 7.2% |
| ABO incompatibility | ||
| No | 157 | 94.0% |
| Yes | 10 | 6.0% |
| Rh incompatibility | ||
| No | 152 | 91.0% |
| Yes | 15 | 9.0% |
| Reductant substance | ||
| No | 140 | 83.8% |
| Yes | 27 | 16.2% |
| Hospitalization | ||
| No | 160 | 95.8% |
| Yes | 7 | 4.2% |
| Length of stay | 2±2 | 1(1-1) |
| Day of onset of jaundice | 2±0 | 2(1-2) |
| Time to fall below TB=8 (days) | 78±6 | 80 (80-80) |
| Gestational week | 37±1 | 37(36-38) |
Table 2.
Laboratory and clinical characteristics of patients.
| Mean±std | Median (Q1-Q3) | Reference values | |
|---|---|---|---|
| WBC (103cells/µL) | 9687±2580 | 9110 (7910-11100) | 9.4-38 |
| Hemoglobin (g/dL) | 13.22±2.27 | 13.1(11.6-14.8) | 13.4-19.8 |
| Hct (%) | 37.49±6.7 | 37.1(32.5-41.4) | 41-65 |
| Reticulocyte (%) | 2.10 ± 0.80 | 1.93(0.50-2.12) | 0.5%–2.5% |
| PLT (103/uL) | 344±95 | 328(277-400) | 150-400 |
| LYMPH (103cells/µL) | 6.14±1.57 | 5.98(5.01-6.84) | 2.8-9.1 |
| NEU (103cells/µL) | 2.04±2.45 | 1.69(1.2-2.22) | 1.8-5.4 |
| NLR | 0.38±0.91 | 0.3(0.21-0.37) | |
| PLR | 59.28±22.28 | 55.38(43.05-70.76) | |
| SII | 114.88±112.5 | 95.73(64.61-125.96) | |
| MONO (103cells/µL) | 1.31±4.39 | 0.94(0.7-1.27) | 0-1.7 |
| C-reactive protein (mg/L) | 2.28±1.42 | 2.3(1.1-3.5) | >5 |
| Sodium (mmol/L) | 139.26±2.99 | 139(137-141) | 136-145 |
| Potassium (mmol/L) | 4.53±0.58 | 4.6(4-5) | 3.5-5.1 |
| Urea (mg/dL) | 8.3±5.14 | 6.8(4.6-12) | 5-20 |
| Creatinine (mg/dL) | 0.45±0.34 | 0.42(0.35-0.51) | Male: 0.74-1.35 Female: 0.59-1.04 |
| Total biluribin (mg/ dL) | 12.54±2.67 | 12.26(10.86-14.21) | 0.2-16.6 |
| Direct biluribin (mg/ dL) | 0.60±0.45 | 0.54 (0.48-0.62) | 0.3-0.7 |
| G6PD (U/g Hb) | 21.95±6.19 | 21.3(17.11-25.63) | 7.00-16.50 |
| Pyruvate kinase (mU/109 RBC/mL) | 284.07±91.56 | 278(198-356) | 111-406 |
| fT4 (ng/dL) | 1.13±0.29 | 1.09(1.01-1.19) | 1.05-3.21 |
| TSH (mU/ L) | 3.37±1.88 | 3.14(2.2-4.25) | 0.73-4.77 |
| AST (U/L) | 39.11±12.19 | 38(31-47) | 25-75 |
| ALT (U/L) | 23.80±8.93 | 24(17-36) | 7-56 |
| GGT (U/L) | 110.50±31.04 | 125(88-136) | 12-147 |
| ALP (U/L) | 250.67±40.34 | 287 (248-315) | Male: 75-316 Female: 48-406 |
| Protein (g/ dL) | 5.53±0.59 | 5.6(5.2-5.89) | 6.0-8.3 |
| Albumin (g/ dL) | 3.63±0.56 | 3.6(3.24-4.1) | 1.90 to 4.90 |
WBC, white blood cell; Hb, hemoglobin; Hct, hematocrit; PLT, platelet; LYM, lymphcite; NEU, neutrophil; NLR, neutrophil-to-lymphocyte ratio; PLR, platelet-to-lymphocyte ratio; SII, systemic-immune-inflammation index; MONO, monocyte¸ G6PD, glucose 6 phosphate dehydrogenase; fT4, free thyroxine; TSH, thyroid stimulating hormone; GGT, gamma-glutamil transferaz; ALP, alkaline phosphatase.
Table 3.
The comparison of inflammatory markers (NLR, PLR, SII) and G6PD, PK according to some characteristics of patients.
Table 3.
The comparison of inflammatory markers (NLR, PLR, SII) and G6PD, PK according to some characteristics of patients.
| NLR | p | PLR | p | SII | p | G6PD | p | PK | p | |
|---|---|---|---|---|---|---|---|---|---|---|
| Gender | ||||||||||
| Male | 0.3(0.21-0.38) | 0.286 | 56.61(43.05-73.12) | 0.854 | 97.7(63.14-132.09) | 0.379 | 21.22(16.78-25) | 0.288 | 265(188-354) | 0.071 |
| Female | 0.28(0.18-0.35) | 53.58(44.15-70.24) | 90.92(65.69-114.08) | 21.82(18.23-27.56) | 302(231-358) | |||||
| Hospitalization | ||||||||||
| No | 0.3(0.21-0.37) | 0.701 | 56.61(43.33-70.69) | 0.539 | 95.81(65.67-123.94) | 0.917 | 21.27(17.16-25.58) | 0.701 | 279.5(196.5-356) | 0.358 |
| Yes | 0.21(0.17-0.74) | 50.11(40.65-78.44) | 76.17(45.68-201.94) | 25.45(11.57-28.39) | 245(212-345) | |||||
| Formula | ||||||||||
| No | 0.3(0.2-0.38) | 0.862 | 55.35(43.05-70.63) | 0.406 | 94.69(64.61-125.96) | 0.488 | 21.23(17.02-25.63) | 0.865 | 280(204-356) | 0.095 |
| Yes | 0.26(0.24-0.33) | 61.7(51.71-73.23) | 108.31(86.5-121.12) | 22.68(19.44-24.49) | 243(188-280.5) | |||||
| ABO incompatibility | ||||||||||
| No | 0.3(0.21-0.37) | 0.254 | 56.7(43.81-70.76) | 0.287 | 95.88(67.35-125.96) | 0.082 | 21.2(17.11-25.55) | 0.257 | 278(195-356) | 0.744 |
| Yes | 0.25(0.15-0.32) | 48.02(40.03-62.84) | 67.65(47.27-111.85) | 23.33(20.44-29.72) | 278(235-354) | |||||
| Rh incompatibility | ||||||||||
| No | 0.3(0.21-0.37) | 0.991 | 55.37(43.05-70.58) | 0.455 | 95.34(65.13-125.96) | 0.878 | 21.25(17.16-25.63) | 0.989 | 274(201-354) | 0.437 |
| Yes | 0.28(0.21-0.44) | 58.74(44.53-99.4) | 99.17(64.61-106.78) | 21.82(14.56-25.55) | 312(189-400) | |||||
| Reductant substance | ||||||||||
| No | 0.3(0.21-0.36) | 0.931 | 55.37(42.88-70.69) | 0.788 | 94.82(63.87-124.67) | 0.512 | 21.22(17.24-25.63) | 0.934 | 272(189-355) | 0.328 |
| Yes | 0.29(0.23-0.39) | 56.7(44.56-75.42) | 95.88(71.54-131.06) | 21.78(16.74-24.65) | 303(228-356) | |||||
Table 4.
Correlation of G6PD and PK with NLR, PLR, SII, Age and HCT.
| Variables | r-p | PK | NLR | PLR | SII | Age | Hct |
|---|---|---|---|---|---|---|---|
| G6-PD | r | 0.00 | -1.000 | -0.12 | -0.837 | 0.296 | -0.285 |
| p | 0.960 | <0.001 | 0.132 | <0.001 | <0.001 | <0.001 | |
| PK | r | 0.00 | 0.05 | 0.05 | -0.04 | -0.04 | |
| p | 0.968 | 0.501 | 0.510 | 0.617 | 0.613 | ||
| NLR | r | 0.12 | 0.837 | -0.295 | 0.285 | ||
| p | 0.132 | <0.001 | <0.001 | <0.001 | |||
| PLR | r | 0.472 | 0.07 | -0.290 | |||
| p | <0.001 | 0.340 | <0.001 | ||||
| SII | r | -0.227 | 0.191 | ||||
| p | 0.003 | 0.014 | |||||
| Age | r | -0.286 | |||||
| p | <0.001 |
Table 5.
Results of partial correlation analysis of G6PD with NLR and SII adjusted for age and Hct.
| NLR | SII | ||
|---|---|---|---|
| G6PD | Correlation coefficient (r) | -0.212 | -0.470 |
| p value | 0.006 | <0.001 |
Table 6.
Linear regression analysis results for G6PD.
| Model | Unstandardized Coefficients (B) | 95,0% Confidence Interval for B | P value | R Square |
|---|---|---|---|---|
| Model 1 | 0.198 | |||
| (Constant) | 23.786 | 16.210/31.363 | <0.001 | |
| Age (days) | 0.199 | 0.061/0.338 | 0.005 | |
| HCT | -0.199 | -0.340/-0.059 | 0.006 | |
| NLR | -1.407 | -2.411/-0.402 | 0.006 | |
| Model 2 | 0.346 | |||
| (Constant) | 24.339 | 17.565/31.113 | <0.001 | |
| Age (days) | 0.152 | 0.026/0.278 | 0.018 | |
| HCT | -0.110 | -0.238/0.018 | 0.091 | |
| SII(100 unit) | -2.581 | -3.331/-1.831 | <0.001 |
Dependent variable: G6-PD; All models included age (days) and HCT. Model 1 include the NLR, Model 2 include SII.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



