
Submitted:
27 June 2025
Posted:
01 July 2025
You are already at the latest version
Abstract
Background/Objectives: Radical cystectomy via midline laparotomy is associated with significant postoperative pain, often necessitating substantial opioid use, which may impair immune function and delay recovery. The rectus sheath block (RSB) is commonly employed as part of multimodal analgesia to improve postoperative pain control; however, its duration is limited with single-injection techniques. Dexamethasone has increasingly been used as a perineural adjuvant to prolong peripheral nerve block effects and enhance analgesia. This study aimed to evaluate the analgesic efficacy of adding perineural dexamethasone to RSB in patients undergoing radical cystectomy. Methods: In this randomized controlled trial, 52 adult patients scheduled for radical cystectomy were randomly assigned to receive ultrasound-guided bilateral RSB with either 0.25% ropivacaine alone or 0.25% ropivacaine combined with 4 mg of dexamethasone per side following skin closure. Postoperative pain intensity was assessed using a numeric rating scale (NRS) at 3, 6, 12, 18, 24, and 48 hours postoperatively. Cumulative intravenous patient-controlled analgesia (IV-PCA) fentanyl consumption and the incidence of rebound pain—defined as an increase in NRS from ≤ 3 to ≥ 7 within 24 hours after block resolution—were also recorded. Results: The addition of dexamethasone significantly reduced cumulative fentanyl consumption. Pain scores were consistently lower in the dexamethasone group compared to the ropivacaine-only group at all time points, except 3 hours postoperatively. The incidence of rebound pain was also markedly lower in the dexamethasone group. Conclusions: Perineural dexamethasone as an adjuvant to RSB provides effective, prolonged analgesia, reduces opioid requirements, and lowers the incidence of rebound pain in patients undergoing radical cystectomy.
Keywords:
radical cystectomy
; rectus sheath block
; dexamethasone
; postoperative pain
; analgesia
; opioid consumption
; rebound pain
; ultrasound-guided regional anesthesia
1. Introduction
Midline laparotomy, commonly performed in colorectal, gynecological, upper gastrointestinal, and urological procedures, accounts for a significant proportion of surgeries worldwide [1]. This widely utilized surgical approach, involving a vertical midline abdominal incision, is frequently associated with various postoperative complications, including pain, pulmonary issues, delayed gastrointestinal motility, and venous thromboembolism [2,3]. In radical cystectomy, which necessitates a large abdominal incision, intraoperative opioid requirements are typically higher, and patients often experience more severe postoperative pain. It is well established that the intensity of perioperative pain can negatively impact the immune system [4]. In cancer surgery, preserving immune competence during the perioperative period is crucial for reducing the risk of intraoperative tumor dissemination and postoperative cancer recurrence [5]. Moreover, the average age of patients undergoing radical cystectomy is increasing, with many presenting with comorbidities involving vital organs such as the heart and lungs. As a result, the importance of effective and balanced postoperative pain management in this patient population continues to grow [6].
To optimize postoperative analgesia, multimodal analgesic strategies are commonly employed, combining non-opioid medications such as paracetamol and nonsteroidal anti-inflammatory drugs (NSAIDs), regional anesthetic techniques, and opioids [7]. Single-injection peripheral nerve blocks (PNBs) have become an essential component of these protocols, providing effective analgesia in the immediate postoperative period (7). PNBs have been shown to reduce opioid consumption, decrease the incidence of postoperative nausea and vomiting (PONV), and facilitate earlier hospital discharge [8,9]. However, since postoperative pain often persists for 24–72 hours, patients may experience a sudden increase in pain intensity — termed ‘rebound pain’ — as the nerve block effect diminishes [10]. A retrospective cohort study of outpatient surgery patients who received preoperative PNBs reported a 49.6% incidence of rebound pain. Risk factors associated with rebound pain include younger age, female sex, surgeries involving bone, and the absence of perioperative intravenous dexamethasone administration [11].
The use of adjuvant drugs in single-injection PNBs, such as alpha-2 agonists, dexamethasone, midazolam, and NSAIDs, has been shown to prolong the duration of local anesthetic effects and reduce dose-dependent adverse effects of local anesthetics. [12]. Among these agents, dexamethasone, a glucocorticoid commonly used to suppress inflammatory responses, has gained significant attention as an adjuvant in regional anesthesia. It is frequently co-administered with local anesthetics to extend the duration of analgesia provided by single-injection PNBs. [13,14,15,16]. Furthermore, dexamethasone has demonstrated effectiveness in reducing postoperative pain and opioid consumption across various surgical procedures. Its combined anti-inflammatory, immunomodulatory, and analgesia-prolonging properties make it a valuable component of multimodal analgesic strategies [17,18].
Although thoracic epidural analgesia is considered the gold standard for postoperative pain management in abdominal surgery, its application is often restricted by contraindications and potential risks. While severe complications are uncommon, epidural analgesia carries the risk of adverse events such as spinal epidural hematoma, abscess formation, and direct neural injury. Common side effects include hypotension, sedation, and pruritus, and its use is contraindicated in patients requiring anticoagulation therapy — a situation increasingly encountered in clinical practice [19]. Moreover, epidural analgesia can be technically demanding, with reported failure rates ranging from 6% to 37% [20].
As alternatives, fascial plane block techniques targeting the peripheral nerves of the abdominal wall have gained widespread use. A meta-analysis comparing continuous peripheral nerve catheters with epidural analgesia for laparotomy found no significant difference in pain scores within the first 48 hours postoperatively [21]. Furthermore, a systematic review and meta-analysis evaluating non-neuraxial analgesic techniques for midline laparotomy concluded that both single-injection rectus sheath block (RSB) and transversus abdominis plane (TAP) block are effective in reducing pain and PONV within the first 6 hours after surgery [22]. Additionally, continuous RSB and TAP block were identified as the most effective non-neuraxial analgesic techniques for reducing 24-hour and 48-hour morphine consumption, resting pain, and pooled opioid-related adverse effects [22].
The RSB is a regional anesthesia technique particularly suitable for midline abdominal incisions. The abdominal wall is innervated by thoracic spinal nerves (T6–L1), which pass through the transversus abdominis and internal oblique muscles, forming an extensive network within the transversus abdominis plane and near the deep inferior epigastric artery. The RSB targets these nerves as they course from the posterior layer of the rectus sheath into the rectus abdominis muscle [23], providing effective analgesia across the central anterior abdominal wall, from the xiphoid process to the pubic symphysis [24,25].
To date, no studies have investigated postoperative pain outcomes or the incidence of rebound pain following single-injection RSB combined with perineural dexamethasone in patients undergoing radical cystectomy. We hypothesized that the addition of dexamethasone to RSB would reduce opioid consumption, improve postoperative analgesia, and lower the incidence of rebound pain. Therefore, this study aimed to compare postoperative pain outcomes and the incidence of rebound pain between patients receiving RSB with and without dexamethasone.
2. Materials and Methods
This study was conducted in accordance with the Declaration of Helsinki and was approved by the Institutional Review Board of Ewha Womans University Mokdong Hospital (EUMC 2024-09-029-003, November 25, 2024). The study was registered with the Clinical Trial Registry of Korea (KCT0010081, December 26, 2024, cris.nih.go.kr). The first patient was enrolled on January 7, 2025, and written informed consent was obtained from all participants.
2.1. Study Design and Participants
Patients scheduled to undergo radical cystectomy for bladder cancer were eligible for inclusion. Patients aged ≥ 20 years with an American Society of Anesthesiologists physical status of 1–3, who were scheduled for elective radical cystectomy under general anesthesia with a single-injection RSB between January 2025 and May 2025, were enrolled. Exclusion criteria included coagulation disorders, neuropathic conditions, allergy to local anesthetics, severe cardiopulmonary disease, systemic steroid use, uncontrolled diabetes, chronic opioid use, psychiatric disorders, and an inability to comprehend pain scoring or operate the intravenous patient-controlled analgesia (PCA) device.
2.2. Randomization
Patients were randomly assigned to either the ropivacaine-only group or the ropivacaine with dexamethasone group. A researcher not involved in the study generated the random allocation sequence using a computer-generated randomization table. Allocation concealment was ensured using sealed opaque envelopes. The patients, attending anesthesiologists, outcome assessors, and surgeons were all blinded to group assignments.
2.3. Anesthesia
General anesthesia was induced with glycopyrrolate (0.2 mg), propofol (2 mg/kg), fentanyl (1 μg/kg), and rocuronium (0.6 mg/kg), followed by tracheal intubation. Anesthesia was maintained with 50% oxygen in air and sevoflurane, with the bispectral index maintained between 40 and 60. Additional boluses of fentanyl were administered as needed, with a maximum total intraoperative dose of 2 μg/kg. Continuous remifentanil infusion was not used, as it has been associated with postoperative hyperalgesia [26]. All surgeries were performed by a single surgeon. At the end of the procedure, all patients received 200 mg of intravenous sugammadex for neuromuscular blockade reversal and 0.3 mg of ramosetron for PONV prophylaxis. Tracheal extubation was performed in the operating room after confirming complete neuromuscular recovery.
2.4. Rectus Sheath Block Technique
All RSBs were performed by a single anesthesiologist in the operating room immediately after wound closure, under strict aseptic conditions. A linear array ultrasound probe (Sonosite, Bothell, WA, USA) was placed transversely at or just above the umbilicus, with an imaging depth of 4–6 cm. A 22G Tuohy needle was inserted a few millimeters from the probe using an in-plane technique at an approximate 45° angle to the skin. The rectus muscle and two hyperechoic parallel lines representing the posterior rectus sheath and transversalis fascia were identified. Under direct visualization, the needle tip was advanced into the desired plane, where 20 mL of 0.25% ropivacaine, either with 4 mg of dexamethasone (in the ropivacaine with dexamethasone group) or without (in the ropivacaine-only group), was injected to hydrodissect the rectus muscle away from the posterior sheath. The same procedure was repeated on the contralateral side. Block failure was confirmed in the post-anesthesia care unit (PACU) if the patient did not exhibit reduced cold sensation over the abdominal area [27].
2.5. Postoperative Pain Management
Postoperative pain was assessed using a numeric rating scale (NRS) ranging from 0 (no pain) to 10 (worst imaginable pain). An intravenous patient-controlled analgesia (IV-PCA) device (Accumate® 1200; Woo Young Meditech, Seoul, Korea) was initiated upon arrival in the PACU. The device was set to deliver a continuous infusion of 1 mL/hour with a 1 mL bolus (100 mL solution containing 20 µg/kg fentanyl and 0.3 mg ramosetron), with a 15-minute lockout interval. Patients were instructed to press the PCA button whenever they felt their RSB was no longer providing adequate analgesia. PCA usage data were collected using the AccuLinker software (Accumate® 1200 version 1.1; Woo Young Meditech).
2.6. Outcome Assessment
The primary outcome variables were the total fentanyl dose delivered via IV-PCA for postoperative analgesia at 3, 6, 12, 18, 24, and 48 hours postoperatively, as well as the pain scores recorded at these same time points. A resident assessed patients at these predefined intervals to record pain scores and monitor for potential complications. The secondary outcome was the incidence of rebound pain, which was defined as a transition from well-controlled to severe pain, typically occurring within 12–24 hours after the resolution of the nerve block. Specifically, the incidence of rebound pain was determined by identifying patients whose pain increased from mild (NRS pain score ≤ 3) at the time the block was last confirmed to be effective (assessed at 3 hours postoperatively) to severe pain (NRS pain score ≥ 7) within 24 hours following the PNB [11]. Additionally, the incidence of PONV within 24 hours postoperatively and any adverse events related to the RSB were evaluated.
2.7. Statistical Analysis
A priori power analysis was conducted using G*Power software, version 3.1 (Heinrich Heine University, Düsseldorf, Germany). Based on a previous study reporting a pain score of 3.54 ± 0.98 at 6 hours postoperatively in patients receiving single-injection RSB during midline laparotomy [28], it was assumed that adding dexamethasone would reduce pain by 30%. A sample size of 23 patients per group was required to achieve 95% power with a two-tailed α of 0.05. Allowing for a 10% dropout rate, 26 patients per group (total of 52) were included.
Statistical analyses were performed using SPSS version 18.0 (IBM Corp., Chicago, IL, USA). The Shapiro–Wilk test was used to assess the normality of continuous variables. Continuous data are presented as mean ± standard deviation or median with interquartile range (IQR), depending on distribution. Categorical variables are expressed as frequencies and percentages. Between-group comparisons were performed using the Student’s t-test or Mann–Whitney U test for continuous variables and the chi-square test for categorical variables, as appropriate. A p-value of < 0.05 was considered statistically significant.
3. Results
A total of 60 patients scheduled for radical cystectomy were screened for eligibility. Of these, three did not meet the inclusion criteria, and five declined to participate. Consequently, 52 patients were enrolled, with 26 allocated to the ropivacaine-only group and 26 to the ropivacaine with dexamethasone group. There were no dropouts or missing data during the 48-hour follow-up (Figure 1).
Baseline demographic and clinical characteristics were comparable between groups, with no statistically significant differences (Table 1).
3.1. Primary Outcomes
The total fentanyl dose administered via IV-PCA was significantly lower in the ropivacaine with dexamethasone group at all time points except 3 and 6 hours postoperatively. Median pain scores were also consistently lower in the ropivacaine with dexamethasone group except at the 3- and 18-hour assessments (Table 2).
3.2. Secondary Outcomes
Rebound pain occurred in eight patients (30.8%) in the ropivacaine-only group and in one patient (3.8%) in the ropivacaine with dexamethasone group, representing a statistically significant difference.
PONV within 24 hours postoperatively was observed in three patients (11.5%) in the ropivacaine-only group and two (7.7%) in the ropivacaine with dexamethasone group, with no significant between-group differences. No complications related to the nerve block procedure were observed in either group.
4. Discussion
This study demonstrated that the addition of dexamethasone to RSB significantly reduced postoperative fentanyl consumption and lowered pain scores at most measurement time points, except at 3 hours after surgery. Additionally, the incidence of rebound pain was significantly lower in the ropivacaine with dexamethasone group compared to the ropivacaine-only group.
RSB has gained popularity with the increasing use of ultrasound-guided techniques in surgeries involving midline abdominal incisions. It is commonly performed alongside general anesthesia to reduce opioid consumption and improve postoperative pain control [25,29]. Although the effectiveness of RSB in abdominal surgery has shown some variability, several studies have demonstrated its analgesic benefits in laparotomy. For example, in patients undergoing open gastrectomy, RSB reduced intraoperative remifentanil requirements and decreased PCA bolus use within the first 2 hours postoperatively compared to controls [30]. Similarly, in patients undergoing laparotomy for mesenteric vascular occlusion, RSB significantly lowered pain scores at 2, 4, and 6 hours postoperatively and reduced opioid consumption over 24 hours [31]. Bashandy et al. [32] also reported significantly lower PACU pain scores and reduced morphine consumption over the first two postoperative days in the RSB group versus general anesthesia alone for midline incision surgeries. However, most previous studies have shown that the analgesic effect of RSB is most pronounced within the first 6 postoperative hours, with opioid-sparing benefits lasting up to 24 hours. In contrast, our study is the first to investigate the addition of perineural dexamethasone as an adjuvant to RSB, and our results demonstrated not only a reduction in pain scores and opioid consumption for up to 48 hours, but also a significant decrease in the incidence of rebound pain. Unlike RSB, several studies have examined the effects of adding dexamethasone to the TAP block, another widely used fascial plane block. A meta-analysis reported modest reductions in pain scores at 2, 6, and 12 hours postoperatively, as well as decreased 24-hour opioid consumption when perineural dexamethasone was used as an adjuvant [33]. These findings suggest that dexamethasone enhances the analgesic efficacy and prolongs the duration of fascial plane blocks — a result consistent with our study’s outcomes.
In our study, no significant differences in fentanyl consumption or pain scores were observed at 3 hours postoperatively. This likely reflects the immediate analgesic effect of the local anesthetic administered during the RSB in both groups. This observation aligns with a meta-analysis reporting that dexamethasone reduced pain at rest during the intermediate (8–12 h) and late (24 h) postoperative periods and decreased cumulative morphine consumption [34]. In addition, the use of a higher concentration and volume of local anesthetic for single-injection PNBs may result in greater analgesic efficacy during the immediate postoperative period, leading to enhanced opioid-sparing effects in the early postoperative phase [22]. The recommended injection volume for ultrasound-guided RSB is 0.1 to 0.2 mL/kg (typically 15–20 mL per side in adults), with the concentration of the local anesthetic adjusted to avoid exceeding the maximum recommended dose [35]. In our study, a relatively high volume of local anesthetic (20 mL of 0.25% ropivacaine per side) was administered. As a result, RSB with local anesthetic alone provided effective postoperative pain relief during the immediate period following radical cystectomy.
Among patients undergoing laparoscopic surgery, those in the preoperative RSB group tended to experience a longer time to the first analgesic request and a lower risk of requiring analgesic administration within the first 24 hours compared to those in the postoperative RSB group [36]. However, in our study, RSB was performed after skin closure and before extubation. This decision was based on evidence indicating that preemptive analgesia provides limited benefits in postoperative pain control, despite the original rationale of administering analgesics before noxious stimuli to prevent central sensitization. Recent studies increasingly emphasize that the adequacy and continuity of perioperative analgesia are more important determinants of postoperative pain outcomes than the timing of its administration [37,38]. Animal models of incisional pain have consistently demonstrated that a single analgesic intervention—whether peripheral or neuraxial—administered before incision does not reduce postoperative pain behaviors beyond the expected duration of its pharmacologic effect [39]. Clinical trials have reported similar findings, and a systematic review by Møiniche et al. also concluded that preemptive analgesia does not provide significant benefits for postoperative pain control [37]. Once nociceptive afferent blockade resolves, the surgical wound is capable of reinitiating central sensitization [37]. Therefore, it is not the timing alone, but rather the duration and efficacy of perioperative analgesic interventions that are critical for managing postoperative pain and preventing central sensitization. Additionally, given the prolonged duration of radical cystectomy, performing RSB at the beginning of surgery could result in rebound pain coinciding with the immediate postoperative period, potentially compromising effective pain control. For these reasons, performing RSB at the conclusion of surgery was considered a more appropriate and effective strategy within our protocol.
Preventive analgesia aims to block the development of sustained pain and includes any intervention during the perioperative period that reduces pain-induced sensitization [40]. Central neuronal sensitization contributes significantly to postoperative pain and may underlie the development of persistent pain following tissue trauma [41]. Continuous PNBs have been proposed as a strategy to prevent rebound pain by providing prolonged afferent blockade and reducing the risk of central sensitization [27]. However, continuous nerve catheters require more time and expertise to insert, carry the risk of displacement, are more challenging to manage, and may increase healthcare costs [42,43]. In contrast, single-injection PNBs are easier to perform, provide reliable analgesia in the immediate postoperative period, and reduce perioperative opioid requirements, despite their temporary duration [44].
A meta-analysis confirmed that both intravenous and perineural dexamethasone are effective in preventing rebound pain after PNBs, with perineural administration providing superior results [45]. Several meta-analyses comparing perineural and intravenous dexamethasone have demonstrated that perineural administration more effectively prolongs block duration [45,46,47]. Proposed mechanisms for this effect include reduced systemic absorption of local anesthetic via local vasoconstriction [48], inhibition of neuronal potassium channels [49], and suppression of nociceptive C-fiber activity [50]. An animal study using a mouse sciatic nerve block model also reported that perineural dexamethasone reduced bupivacaine-induced rebound hyperalgesia by preserving Schwann cell and myelin integrity and reducing transient neurotoxicity [51].
A meta-analysis demonstrated that the analgesic effect of dexamethasone increases with dose until reaching a plateau, beyond which further increases yield minimal additional benefit. Specifically, adding 4 mg of perineural dexamethasone to a long-acting local anesthetic extended analgesia from 11.1 to 16.5 hours, while increasing the dose to 8 mg provided only an additional 1 hour of analgesia [52]. Based on these findings, we selected a 4 mg dose of dexamethasone in our study.
The estimated incidence of PONV is approximately 30% in the general surgical population and can exceed 80% in high-risk groups [53]. Patient-specific risk factors include female sex, a history of PONV or motion sickness, nonsmoking status, and younger age. Certain surgical procedures, such as laparoscopic, bariatric, gynecological, and cholecystectomy surgeries, are also associated with higher PONV risk [53]. The median incidence of PONV in the PACU has been reported to be lower in RSB recipients compared to general anesthesia alone [32], and a meta-analysis found that perineural dexamethasone reduced the incidence of PONV by 72% [33]. However, in our study, the overall incidence of PONV was low, with no significant difference between the groups. This may be attributed to the nature of the surgical procedure, which is not typically associated with a high incidence of PONV, the predominantly elderly and male patient population, and the routine administration of a 5-HT3 receptor antagonist to all patients at the end of surgery.
This study has several limitations. First, it was conducted at a single center with a relatively small sample size and was not adequately powered to detect differences in all outcomes. Second, postoperative pain assessment using the NRS is inherently subjective and may be influenced by individual variability. Third, the findings of this study are specific to RSB and may not be generalizable to other regional anesthesia techniques or different surgical procedures. Fourth, as no control group without a regional nerve block was included, it remains uncertain whether the occurrence of rebound pain outweighed the early analgesic benefits of RSB. Fifth, intravenous dexamethasone was not evaluated in this study; thus, it is unclear whether this route of administration would have yielded comparable effects on rebound pain. Sixth, the follow-up period was limited to 48 hours postoperatively, and therefore, the potential long-term impact of RSB on chronic postoperative pain or prolonged opioid use could not be assessed. Finally, factors such as intraoperative anesthetic management, surgical technique variability, and patient psychological factors were not controlled or analyzed, all of which may influence postoperative pain perception and analgesic requirements.
5. Conclusions
This study demonstrated that the addition of perineural dexamethasone to RSB significantly reduced postoperative opioid usage and pain scores in patients undergoing radical cystectomy, with analgesic benefits lasting up to 48 hours. Additionally, the incidence of rebound pain was markedly lower in the ropivacaine with dexamethasone group compared to the ropivacaine-only group. These findings suggest that perineural dexamethasone is a safe and effective adjuvant for enhancing the analgesic efficacy of RSB in this surgical population.
Author Contributions
Conceptualization, S.H.Y. and W.-J.K.; methodology, S.H.Y. and W.-J.K.; software, W.-J.K.; validation, W.-J.K.; formal analysis, S.H.Y.; investigation, S.H.Y.; resources, W.-J.K.; data curation, S.H.Y. and M.H.B.; writing—original draft preparation, S.H.Y.; writing—review and editing, W.-J.K.; visualization, W.-J.K.; supervision, W.-J.K.; project administration, W.-J.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Ewha Womans University Mokdong Hospital (EUMC 2024-09-029-003, November 25, 2024).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
Data available on request due to restrictions.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| NSAIDs | nonsteroidal anti-inflammatory drugs |
| PNB | peripheral nerve block |
| PONV | postoperative nausea and vomiting |
| RSB | rectus sheath block |
| TAP | transversus abdominis plane |
| PACU | post-anesthesia care unit |
| NRS | numeric rating scale |
| IV-PCA | intravenous patient-controlled analgesia |
References
- Howle, R.; Ng, S.C.; Wong, H.Y.; Onwochei, D.; Desai, N. Comparison of analgesic modalities for patients undergoing midline laparotomy: a systematic review and network meta-analysis. Can J Anaesth 2022, 69, 140–176. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.R.; Baig, M.A.; Brito, V.; Bader, F.; Bergman, M.I.; Alfonso, A. Postoperative pulmonary complications after laparotomy. Respiration 2010, 80, 269–274. [Google Scholar] [CrossRef]
- Bragg, D.; El-Sharkawy, A.M.; Psaltis, E.; Maxwell-Armstrong, C.A.; Lobo, D.N. Postoperative ileus: Recent developments in pathophysiology and management. Clin Nutr 2015, 34, 367–376. [Google Scholar] [CrossRef]
- Juneja, R. Opioids and cancer recurrence. Curr Opin Support Palliat Care 2014, 8, 91–101. [Google Scholar] [CrossRef]
- Snyder, G.L.; Greenberg, S. Effect of anaesthetic technique and other perioperative factors on cancer recurrence. Br J Anaesth 2010, 105, 106–115. [Google Scholar] [CrossRef] [PubMed]
- Jin, F.; Chung, F. Minimizing perioperative adverse events in the elderly. Br J Anaesth 2001, 87, 608–624. [Google Scholar] [CrossRef]
- Hughes, M.J.; Ventham, N.T.; McNally, S.; Harrison, E.; Wigmore, S. Analgesia after open abdominal surgery in the setting of enhanced recovery surgery: a systematic review and meta-analysis. JAMA Surg 2014, 149, 1224–1230. [Google Scholar] [CrossRef] [PubMed]
- Fredrickson, M.J.; Krishnan, S.; Chen, C.Y. Postoperative analgesia for shoulder surgery: a critical appraisal and review of current techniques. Anaesthesia 2010, 65, 608–624. [Google Scholar] [CrossRef]
- Abdallah, F.W.; Halpern, S.H.; Aoyama, K.; Brull, R. Will the Real Benefits of Single-Shot Interscalene Block Please Stand Up? A Systematic Review and Meta-Analysis. Anesth Analg 2015, 120, 1114–1129. [Google Scholar] [CrossRef]
- Lavand’homme, P. Rebound pain after regional anesthesia in the ambulatory patient. Curr Opin Anaesthesiol 2018, 31, 679–684. [Google Scholar] [CrossRef]
- Barry, G.S.; Bailey, J.G.; Sardinha, J.; Brousseau, P.; Uppal, V. Factors associated with rebound pain after peripheral nerve block for ambulatory surgery. Br J Anaesth 2021, 126, 862–871. [Google Scholar] [CrossRef] [PubMed]
- Swain, A.; Nag, D.S.; Sahu, S.; Samaddar, D.P. Adjuvants to local anesthetics: Current understanding and future trends. World J Clin Cases 2017, 5, 307–323. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Rodseth, R.; McCartney, C.J. Effects of dexamethasone as a local anaesthetic adjuvant for brachial plexus block: a systematic review and meta-analysis of randomized trials. Br J Anaesth 2014, 112, 427–439. [Google Scholar] [CrossRef]
- Huynh, T.M.; Marret, E.; Bonnet, F. Combination of dexamethasone and local anaesthetic solution in peripheral nerve blocks: A meta-analysis of randomised controlled trials. Eur J Anaesthesiol 2015, 32, 751–758. [Google Scholar] [CrossRef]
- Kawanishi, R.; Yamamoto, K.; Tobetto, Y.; Nomura, K.; Kato, M.; Go, R.; Tsutsumi, Y.M.; Tanaka, K.; Takeda, Y. Perineural but not systemic low-dose dexamethasone prolongs the duration of interscalene block with ropivacaine: a prospective randomized trial. Local Reg Anesth 2014, 7, 5–9. [Google Scholar] [CrossRef]
- Sakae, T.M.; Marchioro, P.; Schuelter-Trevisol, F.; Trevisol, D.J. Dexamethasone as a ropivacaine adjuvant for ultrasound-guided interscalene brachial plexus block: A randomized, double-blinded clinical trial. J Clin Anesth 2017, 38, 133–136. [Google Scholar] [CrossRef]
- Liang, S.; Xing, M.; Jiang, S.; Zou, W. Effect of Intravenous Dexamethasone on Postoperative Pain in Patients Undergoing Total Knee Arthroplasty: A Systematic Review and Meta-Analysis. Pain Physician 2022, 25, E169–E183. [Google Scholar]
- Singh, N.P.; Makkar, J.K.; Yadav, N.; Goudra, B.G.; Singh, P.M. The analgesic efficacy of intravenous dexamethasone for post-caesarean pain: A systematic review with meta-analysis and trial sequential analysis. Eur J Anaesthesiol 2022, 39, 498–510. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.; Popping, D.M. Is epidural analgesia still a viable option for enhanced recovery after abdominal surgery. Curr Opin Anaesthesiol 2018, 31, 622–629. [Google Scholar] [CrossRef]
- Popping, D.M.; Elia, N.; Van Aken, H.K.; Marret, E.; Schug, S.A.; Kranke, P.; Wenk, M.; Tramer, M.R. Impact of epidural analgesia on mortality and morbidity after surgery: systematic review and meta-analysis of randomized controlled trials. Ann Surg 2014, 259, 1056–1067. [Google Scholar] [CrossRef]
- Bailey, J.G.; Morgan, C.W.; Christie, R.; Ke, J.X.C.; Kwofie, M.K.; Uppal, V. Continuous peripheral nerve blocks compared to thoracic epidurals or multimodal analgesia for midline laparotomy: a systematic review and meta-analysis. Korean J Anesthesiol 2021, 74, 394–408. [Google Scholar] [CrossRef]
- Barry, G.; Sehmbi, H.; Retter, S.; Bailey, J.G.; Tablante, R.; Uppal, V. Comparative efficacy and safety of non-neuraxial analgesic techniques for midline laparotomy: a systematic review and frequentist network meta-analysis of randomised controlled trials. Br J Anaesth 2023, 131, 1053–1071. [Google Scholar] [CrossRef] [PubMed]
- Rozen, W.M.; Tran, T.M.; Ashton, M.W.; Barrington, M.J.; Ivanusic, J.J.; Taylor, G.I. Refining the course of the thoracolumbar nerves: a new understanding of the innervation of the anterior abdominal wall. Clin Anat 2008, 21, 325–333. [Google Scholar] [CrossRef] [PubMed]
- Sandeman, D.J.; Dilley, A.V. Ultrasound-guided rectus sheath block and catheter placement. ANZ J Surg 2008, 78, 621–623. [Google Scholar] [CrossRef] [PubMed]
- Osaka, Y.; Kashiwagi, M.; Nagatsuka, Y.; Oosaku, M.; Hirose, C. [Ultrasound-guided rectus sheath block for upper abdominal surgery]. Masui 2010, 59, 1039–1041. [Google Scholar]
- Fletcher, D.; Martinez, V. Opioid-induced hyperalgesia in patients after surgery: a systematic review and a meta-analysis. Br J Anaesth 2014, 112, 991–1004. [Google Scholar] [CrossRef]
- Woo, J.H.; Lee, H.J.; Oh, H.W.; Lee, J.W.; Baik, H.J.; Kim, Y.J. Perineural dexamethasone reduces rebound pain after ropivacaine single injection interscalene block for arthroscopic shoulder surgery: a randomized controlled trial. Reg Anesth Pain Med 2021, 46, 965–970. [Google Scholar] [CrossRef]
- Melesse, D.Y.; Chekol, W.B.; Tawuye, H.Y.; Denu, Z.A.; Agegnehu, A.F. Assessment of the analgesic effectiveness of rectus sheath block in patients who had emergency midline laparotomy: Prospective observational cohort study. International Journal of Surgery Open 2020, 24, 27–31. [Google Scholar] [CrossRef]
- Yassin, H.M.; Abd Elmoneim, A.T.; El Moutaz, H. The Analgesic Efficiency of Ultrasound-Guided Rectus Sheath Analgesia Compared with Low Thoracic Epidural Analgesia After Elective Abdominal Surgery with a Midline Incision: A Prospective Randomized Controlled Trial. Anesth Pain Med 2017, 7, e14244. [Google Scholar] [CrossRef]
- Hong, S.; Kim, H.; Park, J. Analgesic effectiveness of rectus sheath block during open gastrectomy: A prospective double-blinded randomized controlled clinical trial. Medicine (Baltimore) 2019, 98, e15159. [Google Scholar] [CrossRef]
- Elbahrawy, K.; El-Deeb, A. Rectus sheath block for postoperative analgesia in patients with mesenteric vascular occlusion undergoing laparotomy: A randomized single-blinded study. Anesth Essays Res 2016, 10, 516–520. [Google Scholar] [CrossRef] [PubMed]
- Bashandy, G.M.; Elkholy, A.H. Reducing postoperative opioid consumption by adding an ultrasound-guided rectus sheath block to multimodal analgesia for abdominal cancer surgery with midline incision. Anesth Pain Med 2014, 4, e18263. [Google Scholar] [CrossRef]
- Chen, Q.; An, R.; Zhou, J.; Yang, B. Clinical analgesic efficacy of dexamethasone as a local anesthetic adjuvant for transversus abdominis plane (TAP) block: A meta-analysis. PLoS One 2018, 13, e0198923. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, E.; Kern, C.; Kirkham, K.R. A systematic review and meta-analysis of perineural dexamethasone for peripheral nerve blocks. Anaesthesia 2015, 70, 71–83. [Google Scholar] [CrossRef] [PubMed]
- Chin, K.J.; McDonnell, J.G.; Carvalho, B.; Sharkey, A.; Pawa, A.; Gadsden, J. Essentials of Our Current Understanding: Abdominal Wall Blocks. Reg Anesth Pain Med 2017, 42, 133–183. [Google Scholar] [CrossRef]
- Nakazawa, M.; Fukushima, T.; Shoji, K.; Momosaki, R.; Mio, Y. Preoperative versus postoperative ultrasound-guided rectus sheath block for acute postoperative pain relief after laparoscopy: A retrospective cohort study. Medicine (Baltimore) 2024, 103, e37597. [Google Scholar] [CrossRef] [PubMed]
- Moiniche, S.; Kehlet, H.; Dahl, J.B. A qualitative and quantitative systematic review of preemptive analgesia for postoperative pain relief: the role of timing of analgesia. Anesthesiology 2002, 96, 725–741. [Google Scholar] [CrossRef]
- Katz, J.; Clarke, H.; Seltzer, Z. Review article: Preventive analgesia: quo vadimus? Anesth Analg 2011, 113, 1242–1253. [Google Scholar] [CrossRef]
- Brennan, T.J.; Taylor, B.K. Analgesic treatment before incision compared with treatment after incision provides no improvement in postoperative pain relief. The Journal of Pain 2000, 1, 96–98. [Google Scholar] [CrossRef]
- Pogatzki-Zahn, E.M.; Zahn, P.K. From preemptive to preventive analgesia. Curr Opin Anaesthesiol 2006, 19, 551–555. [Google Scholar] [CrossRef]
- Brennan, T.J.; Kehlet, H. Preventive analgesia to reduce wound hyperalgesia and persistent postsurgical pain: not an easy path. Anesthesiology 2005, 103, 681–683. [Google Scholar] [CrossRef]
- Adhikary, S.D.; Armstrong, K.; Chin, K.J. Perineural entrapment of an interscalene stimulating catheter. Anaesth Intensive Care 2012, 40, 527–530. [Google Scholar] [CrossRef] [PubMed]
- Bowens, C., Jr.; Briggs, E.R.; Malchow, R.J. Brachial plexus entrapment of interscalene nerve catheter after uncomplicated ultrasound-guided placement. Pain Med 2011, 12, 1117–1120. [Google Scholar] [CrossRef]
- Hughes, M.S.; Matava, M.J.; Wright, R.W.; Brophy, R.H.; Smith, M.V. Interscalene brachial plexus block for arthroscopic shoulder surgery: a systematic review. J Bone Joint Surg Am 2013, 95, 1318–1324. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.S.; Lai, H.C.; Jhou, H.J.; Chan, W.H.; Chen, P.H. Rebound pain prevention after peripheral nerve block: A network meta-analysis comparing intravenous, perineural dexamethasone, and control. J Clin Anesth 2024, 99, 111657. [Google Scholar] [CrossRef] [PubMed]
- Pehora, C.; Pearson, A.M.; Kaushal, A.; Crawford, M.W.; Johnston, B. Dexamethasone as an adjuvant to peripheral nerve block. Cochrane Database Syst Rev 2017, 11, CD011770. [Google Scholar] [CrossRef] [PubMed]
- Albrecht, E.; Renard, Y.; Desai, N. Intravenous versus perineural dexamethasone to prolong analgesia after interscalene brachial plexus block: a systematic review with meta-analysis and trial sequential analysis. Br J Anaesth 2024, 133, 135–145. [Google Scholar] [CrossRef]
- Shishido, H.; Kikuchi, S.; Heckman, H.; Myers, R.R. Dexamethasone decreases blood flow in normal nerves and dorsal root ganglia. Spine (Phila Pa 1976) 2002, 27, 581–586. [Google Scholar] [CrossRef]
- Attardi, B.; Takimoto, K.; Gealy, R.; Severns, C.; Levitan, E.S. Glucocorticoid induced up-regulation of a pituitary K+ channel mRNA in vitro and in vivo. Recept Channels 1993, 1, 287–293. [Google Scholar]
- Johansson, A.; Hao, J.; Sjolund, B. Local corticosteroid application blocks transmission in normal nociceptive C-fibres. Acta Anaesthesiol Scand 1990, 34, 335–338. [Google Scholar] [CrossRef]
- An, K.; Elkassabany, N.M.; Liu, J. Dexamethasone as adjuvant to bupivacaine prolongs the duration of thermal antinociception and prevents bupivacaine-induced rebound hyperalgesia via regional mechanism in a mouse sciatic nerve block model. PLoS One 2015, 10, e0123459. [Google Scholar] [CrossRef] [PubMed]
- Zufferey, P.J.; Chaux, R.; Lachaud, P.A.; Capdevila, X.; Lanoiselee, J.; Ollier, E. Dose-response relationships of intravenous and perineural dexamethasone as adjuvants to peripheral nerve blocks: a systematic review and model-based network meta-analysis. Br J Anaesth 2024, 132, 1122–1132. [Google Scholar] [CrossRef] [PubMed]
- Gan, T.J.; Belani, K.G.; Bergese, S.; Chung, F.; Diemunsch, P.; Habib, A.S.; Jin, Z.; Kovac, A.L.; Meyer, T.A.; Urman, R.D.; et al. Fourth Consensus Guidelines for the Management of Postoperative Nausea and Vomiting. Anesth Analg 2020, 131, 411–448. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
CONSORT flow diagram.
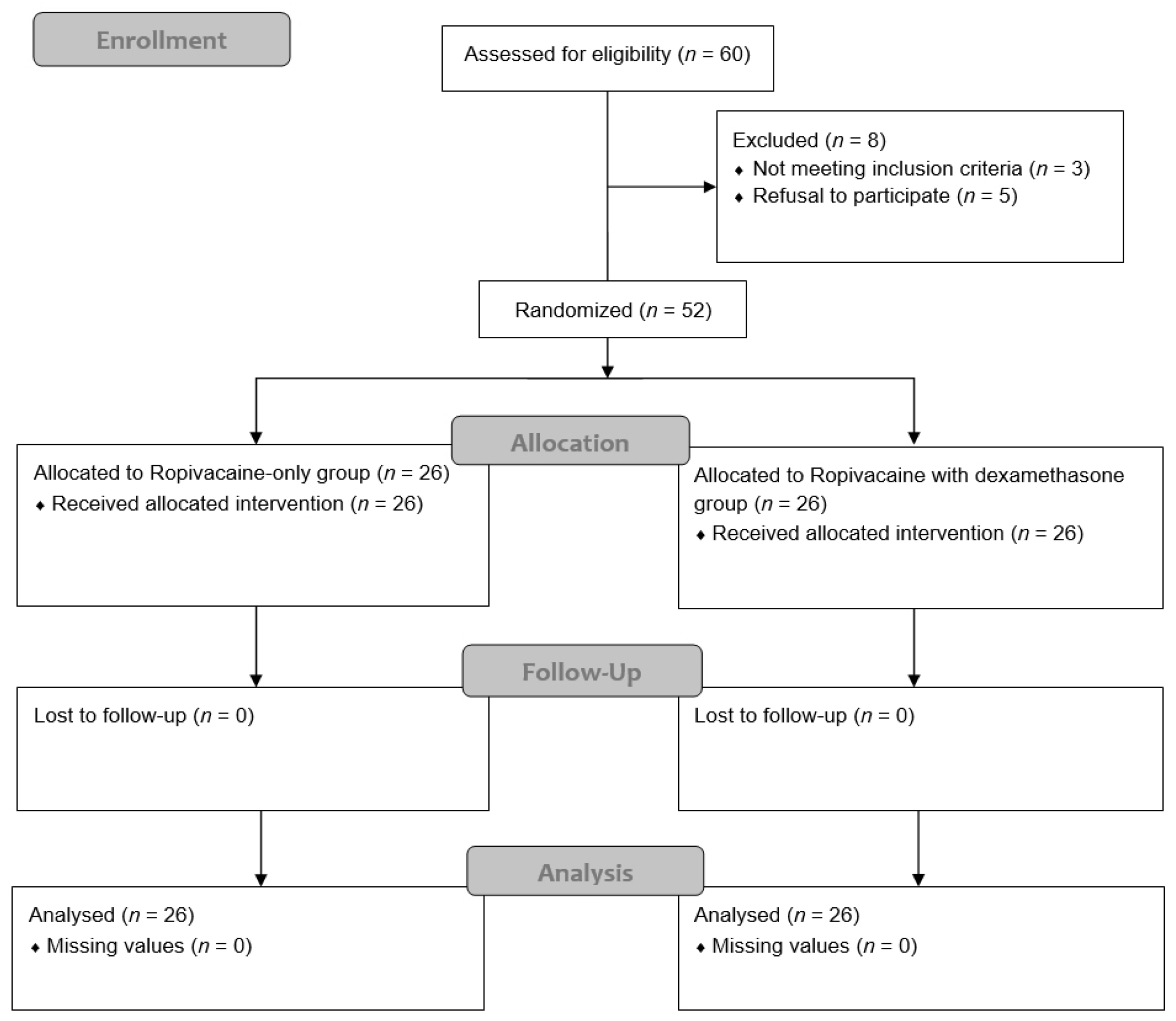

Table 1.
Demographic data.
| Ropivacaine-only group (n = 26) | Ropivacaine with dexamethasone group (n = 26) | p-value | |
|---|---|---|---|
| Age (y) | 68.50 [8.50] | 67.50 [9.25] | 0.275 |
| Height (cm) | 167.00 [9.65] | 167.10 [8.98] | 0.498 |
| Weight (kg) | 66.66 ± 11.86 | 65.66 ± 10.17 | 0.745 |
| Sex (M/F) | 21 (81) / 5 (19) | 21 (81) / 5 (19) | 1.000 |
| Operation time (min) | 252.50 [61.25] | 225.00 [31.25] | 0.184 |
| Anesthesia time (min) | 287.50 [67.50] | 265.00 [33.75] | 0.152 |
| ASA (1/2/3) | 0 (0) / 23 (88) / 3 (12) | 3 (11) /21 (81) / 2 (8) | 0.193 |
| Diabetes mellitus | 7 (27) | 9 (35) | 0.548 |
| Hypertension | 16 (62) | 13 (50) | 0.402 |
| Pulmonary disease | 1 (4) | 3 (12) | 0.298 |
| Intraoperative fentanyl (µg) | 100.00 [50.00] | 100.00 [50.00] | 0.627 |
Data are presented as the mean ± standard deviation, median [interquartile range], or number of patients (%). ASA, American Society of Anesthesiologists.
Table 2.
Postoperative total fentanyl use and pain scores.
| Ropivacaine-only group (n = 26) | Ropivacaine with dexamethasone group (n = 26) | p-value | |
|---|---|---|---|
| Total fentanyl dose (µg) | |||
| Postoperative 3 h | 101.70 [43.05] | 84.44 [33.72] | 0.164 |
| Postoperative 6 h | 179.20 [138.60] | 148.50 [100.03] | 0.059 |
| Postoperative 12 h | 294.95 [173.48] | 247.95 [131.98] | 0.041 |
| Postoperative 18 h | 420.35 [259.30] | 359.80 [140.50] | 0.022 |
| Postoperative 24 h | 521.50 [332.58] | 459.80 [175.42] | 0.032 |
| Postoperative 48 h | 913.70 [246.95] | 806.30 [300.45] | 0.024 |
| Numeric rating scale | |||
| Postoperative 3 h | 2.00 [2.00] | 2.00 [1.00] | 0.113 |
| Postoperative 6 h | 6.00 [2.25] | 4.50 [2.25] | 0.002 |
| Postoperative 12 h | 5.00 [2.00] | 3.00 [2.00] | 0.000 |
| Postoperative 18 h | 4.00 [2.00] | 3.00 [2.00] | 0.057 |
| Postoperative 24 h | 3.00 [1.50] | 2.50 [1.25] | 0.024 |
| Postoperative 48 h | 2.00 [2.25] | 1.00 [1.00] | 0.003 |
Data are presented as the median [interquartile range]. Bold indicates statistical significance.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



