
Submitted:
30 June 2025
Posted:
30 June 2025
You are already at the latest version
Abstract
Background/Objectives: Sarcopenia is characterized by the gradual and generalized loss of muscle mass, strength, and/or physical performance with advancing age. Ra-diofrequency ablation (RFA) of the medial branch nerves is a well-established and ef-fective intervention for treating lumbar facetogenic pain. Although sarcopenia is asso-ciated with poor outcomes following epidural steroid injections and lumbar spine sur-geries, its effect on clinical outcomes in patients undergoing RFA for facetogenic pain remains unexplored. Therefore, this study aims to evaluate the influence of sarcopenia on treatment outcomes in this patient population. Methods: Patients were classified into sarcopenia and non-sarcopenia groups based on predefined psoas muscle index (PMI) thresholds. The primary outcomes included changes in back pain intensity and the proportion of responders at 1, 3, and 6 months following RFA. The secondary out-come was the identification of demographic, clinical, and sarcopenia-related factors that predicted treatment response at each follow-up interval. Results: Both groups demonstrated statistically significant improvements in pain scores compared to base-line at all follow-up points. However, the median pain scores remained significantly higher in the sarcopenia group at 3 months post-RFA. Despite this, the proportion of responders did not significantly differ between the two groups at any time point. At 3 months post-RFA, the absence of prior spinal surgery was identified as a significant predictor of treatment response. Six months post-RFA, favorable outcomes were sig-nificantly associated with the absence of diabetes, no history of spinal surgery, and a higher PMI. Conclusions: Sarcopenia may affect the degree of pain improvement fol-lowing medial branch nerve RFA. Additionally, patient-specific factors such as diabe-tes, prior spinal surgery, and PMI should be incorporated in predicting treatment outcomes.
Keywords:
Radiofrequency Ablation
; Osteoarthritis
; Spine
; Sarcopenia
; Zygapophyseal Joint
1. Introduction
Chronic low back pain is a significant healthcare concern that reduces the quality of life, impairs functionality, and increases disability. Among the various causes of chronic low back pain, facetogenic pain accounts for approximately 34.1% of all cases [1], with its prevalence increasing with age [2]. Diagnosing lumbar facetogenic pain remains challenging due to its heterogeneous etiology, variable clinical presentation, inconclusive physical examination findings, inconsistent radiologic evidence, and the requirement for confirmation through diagnostic medial branch blocks (MBBs) [3,4]. Neither Magnetic Resonance Imaging (MRI) nor Computed Tomography (CT) provides definitive findings that can reliably diagnose lumbar facet-mediated pathology as the exclusive source of pain [5].
Currently, the standard for diagnosing lumbar facetogenic pain involves diagnostic facet blocks, including both intra-articular facet joint injections and MBBs [6]. MBBs are considered more predictive of successful outcomes following lumbar radiofrequency ablation (RFA) than intra-articular facet injections; however, both approaches have demonstrated greater predictive value compared to sham procedures [7]. Each facet joint receives innervation from two medial branches arising from the posterior primary rami — one from the corresponding spinal level and another from the level above. For example, the inferior portion of the L4-L5 facet joint is innervated by the L4 medial branch, while the superior portion receives input from the L3 medial branch. These branches are typically targeted at the transverse processes of L5 and L4 for diagnostic blocks or denervation procedures. In this context, two target points are typically addressed: one for the medial branch and another for the facet joint branch itself [8]. RFA of the medial branch nerves that innervate the facet joints is a well-established treatment modality with high success rates for managing lumbar facetogenic pain [9]. A systematic review concluded that there is strong evidence supporting short-term, and moderate evidence for long-term, pain relief in managing lumbar facet joint pain using radiofrequency thermoneurolysis [10].
According to the European Working Group on Sarcopenia in Older People (EWGSOP), sarcopenia is characterized by the gradual and generalized loss of muscle mass, strength, and/or physical performance with advancing age [11]. Its development and progression involve the interplay of multiple complex biological mechanisms. Firstly, aging results in a reduction in both the number and cross-sectional area (CSA) of muscle fibers, leading to overall muscle atrophy. Secondly, imbalances in protein metabolism — specifically, between muscle protein synthesis and degradation — contribute to the progressive decline in muscle mass. Additionally, age-related hormonal alterations, including decreased levels of anabolic hormones such as growth hormone and testosterone, along with elevated concentrations of catabolic agents like cortisol and pro-inflammatory cytokines, further exacerbate muscle deterioration. Finally, changes in gene expression and disruptions in cellular processes such as apoptosis can adversely affect muscle tissue health and play a pivotal role in the pathogenesis of sarcopenia [12].
Various tools and methodologies are available for assessing appendicular skeletal muscle mass (ASM) [13]. Common techniques include dual-energy X-ray absorptiometry and bioelectrical impedance analysis. Beyond these, several radiological indices have been introduced to estimate muscle quantity. Parameters such as the psoas muscle index (PMI), psoas-lumbar vertebral index (PLVI), and paraspinal muscle index (PSMI) are frequently employed to assess overall skeletal muscle mass and central sarcopenia [14,15,16]. Among them, PMI has demonstrated a strong correlation with conventional sarcopenia assessment tools and is considered a reliable method for evaluating muscle health [17]. Notably, PMI is extensively used in research, particularly in Asian countries such as Japan and South Korea [18,19,20]. Similarly, PLVI has been identified as a simple and valid radiological marker for central sarcopenia and has shown clinical utility as a surrogate indicator of frailty, especially in patients undergoing spinal surgery [15,21,22]. PSMI has likewise been proposed as an objective metric reflecting paraspinal muscle quality and sarcopenia severity [16].
The use of these imaging parameters offers several practical advantages for sarcopenia assessment. First, they provide objective, quantifiable data that are relatively easy to obtain compared to conventional screening tools. Second, they eliminate the need for physical performance assessments. Third, because cross-sectional imaging studies are often already conducted during diagnostic evaluations, additional testing is usually unnecessary. Lastly, these measurements can be performed without requiring patient cooperation or detailed medical history, which is especially advantageous in elderly individuals with cognitive impairments or communication difficulties.
Recent studies have identified sarcopenia as a significant factor associated with adverse postoperative outcomes, increased morbidity, and elevated mortality rates across a range of medical conditions [12]. While sarcopenia has been linked to unfavorable prognoses following epidural procedures [23,24,25] and lumbar spine surgeries [26], to date, no study has specifically examined its impact on clinical outcomes in patients with facetogenic pain undergoing RFA of the medial branch nerves. Accordingly, the purpose of this study is to investigate the effect of sarcopenia on treatment outcomes within this particular patient group.
2. Materials and Methods
This study was approved by the Institutional Review Board (IRB) of Ewha Womans University Mokdong Hospital (EUMC 2024-10-001-001), which waived the requirement for informed consent. Electronic medical records of patients who underwent RFA of the lumbar medial branch nerves between September 2019 and November 2023 were retrospectively reviewed for inclusion. All patients underwent two diagnostic MBBs with 0.5 mL of 2% lidocaine at each target level following negative aspiration for blood [27]. An MBB was considered successful if it produced a > 50% reduction in pain intensity. Patients who met this criterion were subsequently evaluated for RFA when clinically appropriate.
The inclusion criteria were (1) age > 60 years, (2) predominantly axial low back pain lasting at least 3 months, and (3) inadequate response to conservative treatments, including physical therapy, integrative therapies, or pharmacological management.
The exclusion criteria were (1) any epidural injection or other spinal interventions within 1 month before RFA, (2) incomplete medical records, (3) absence of lumbar computed tomography (CT) imaging, and (4) follow-up duration of < 6 months.
Radiofrequency Ablation Procedure
Patients were placed in a prone position on a standard fluoroscopy table. The lumbar spine was prepared using a sterile technique, and a C-arm fluoroscope was positioned ipsilaterally with oblique and caudad-cephalad direction to optimize the alignment of the cannula parallel to the target nerve trajectory. A 22-gauge curved RF cannula with a 10-mm active tip was advanced under a coaxial view until it contacted the bone between the superomedial border of the transverse process and the inferolateral neck of the superior articular process at levels > L5. For L5 dorsal ramus ablation, the cannula was positioned in the groove between the S1 articular process and the sacral ala.
At each level, sensory stimulation at 50 Hz and motor stimulation at 2 Hz were performed to confirm accurate electrode placement by eliciting contraction of the multifidus muscle. Once proper positioning was confirmed, 0.5 mL of 2% lidocaine mixed with 10 mg of triamcinolone was injected through each cannula to minimize procedural discomfort, enhance lesion size, and reduce post-procedural neuritis [28]. Thermal lesions were then created using an RF generator at 80°C for 90 s, repeated three times.
Clinical Data Collection
Demographic and clinical data included age, sex, height, body mass index (BMI), diabetes mellitus status, spinal surgery history at the RFA-treated site, presence of compression fractures or spondylolisthesis at the RFA-treated site, pain duration before RFA, baseline and post-procedural pain scores using the 11-point Numeric Rating Scale (NRS) at 1, 3, and 6 months, number of responders at each time point, treated levels, and RFA laterality. A responder was defined as a patient who experienced a ≥ 30% reduction in pain score at follow-up without an increase in analgesic use compared to that at baseline [29]. Sarcopenia-related parameters included the PMI, PLVI, and PSMI. The PMI was calculated by manually outlining the bilateral psoas muscles at the L3 vertebral level. Their total CSA was measured before normalizing it to the height squared (mm²/m²) of the patient [14,30,31]. The PLVI was determined by dividing the mean CSA of the bilateral psoas muscles by the CSA of the L4 vertebral body at the inferior endplate level. This was calculated using the following formula: (left psoas CSA + right psoas CSA) / 2 / L4 vertebral body CSA [21,22]. The PSMI was calculated by measuring the CSA of the multifidus and erector spinae muscles at the L3–L4 disc level, then normalizing their sum to the height squared (mm²/m²) of the patient [25].
All imaging measurements were manually performed using picture archiving and communication system (PACS) software, independently reviewed by two pain physicians blinded to the clinical data of the patient.
Outcome Measures
Patients were categorized into sarcopenia and non-sarcopenia groups using PMI thresholds at the L3 level: < 564.2 mm²/m² for men and < 414.5 mm²/m² for women [14,30]. The primary outcomes were changes in back pain intensity, assessed via the NRS, and the proportion of responders at 1, 3, and 6 months post-RFA. The secondary outcome was to identify demographic, clinical, and sarcopenia-related predictors of treatment response at these time points.
Statistical Analysis
Statistical analyses were conducted using SPSS version 18.0 (IBM Corp., Chicago, IL, USA). The Shapiro–Wilk test was used to assess the normality of continuous variables. Continuous variables are presented as mean ± standard deviation (SD) or median with interquartile range (IQR), depending on data distribution. Categorical variables are expressed as frequencies and percentages.
Between-group comparisons were performed using the student’s t-test or Mann–Whitney U test for continuous variables and the chi-square test for categorical variables, as appropriate. Intra-group comparisons were assessed using Wilcoxon signed-rank tests. A P-value of < 0.05 was considered statistically significant.
To identify predictors of RFA response, logistic regression analyses were performed. Variables with P-values < 0.10 in univariate analyses were included in the multivariate logistic regression model. A P-value of < 0.05 was considered significant in the multivariate analysis.
3. Results
During the study period, 116 patients who underwent RFA were assessed for eligibility. Of these, 14 patients were excluded based on the study criteria: five patients were < 60 years of age, and nine had incomplete clinical data. Ultimately, 102 patients were included in the final analysis and categorized into two groups: non-sarcopenia (67 patients) and sarcopenia (35 patients) (Figure 1).
Table 1 summarizes the baseline demographic and sarcopenia-related characteristics of the study population. The sarcopenia group had significantly lower BMI, lower rates of prior spinal surgery, and a lower prevalence of spondylolisthesis, along with significantly reduced PLVI and PSMI values compared to the non-sarcopenia group.
Both groups demonstrated statistically significant improvements in pain scores compared to baseline at all follow-up points. However, the median pain scores remained significantly higher in the sarcopenia group at 3 months post-RFA (Figure 2A). Nevertheless, the proportion of responders did not significantly differ between both groups at any time point (Figure 2B).
Univariate logistic regression analysis revealed that factors such as age, sex, height, BMI, compression fractures, spondylolisthesis, PLVI, and PSMI were not significantly associated with treatment response (P > 0.10). Table 2 shows the results of the multivariate logistic regression analysis. At 3 months post-RFA, the absence of prior spinal surgery significantly predicted treatment response. At 6 months post-RFA, a favorable treatment response correlated with the absence of diabetes, no history of spinal surgery, and a higher PMI.
No serious adverse events or complications related to the RFA procedures were documented in the medical records of the patients.
4. Discussion
In this study, we evaluated the effect of sarcopenia on clinical outcomes following RFA for chronic lumbar facetogenic pain. Although patients with sarcopenia and those without sarcopenia experienced significant pain reduction, the sarcopenia group demonstrated higher median pain scores at 3 months post-procedure. Multivariate analysis identified the absence of prior spinal surgery as a significant predictor of treatment response at 3 months. At 6 months, the absence of diabetes, no history of spinal surgery, and a higher PMI were significant predictors of a favorable outcome.
Several previous studies have investigated the relationship between sarcopenia and outcomes of non-surgical spinal interventions in patients with lumbar spinal disease. For example, in a study examining the effects of percutaneous epidural balloon neuroplasty—using the same PMI threshold as our study—no significant differences in median NRS scores for back and leg pain were found between patients with and without sarcopenia throughout the study period. Both groups, however, showed significant improvement at 1, 3, and 6 months compared to baseline [30]. This finding contrasts with our results, which demonstrated a diminished analgesic effect of RFA in the sarcopenia group, particularly in those with low PMI at 3 months post-procedure.
Additionally, two studies have assessed the analgesic efficacy of epidural steroid injections in elderly patients with symptomatic degenerative lumbar spinal disease by categorizing patients into good and poor analgesia groups. One study aimed to determine whether pre-procedural handgrip strength or PMI could predict analgesic outcomes, and found that handgrip strength was significantly higher in the good analgesia group than in the poor analgesia group, whereas PMI did not differ between the two groups [24]. Another study investigated the impact of paraspinal muscle degeneration, including assessments of muscle size and fat infiltration, reporting that the grade of fat infiltration in the paraspinal muscles was significantly higher in the poor analgesia group, while the CSA of the paraspinal muscles did not differ between groups [25]. Similarly, a study evaluating the relationship between paraspinal muscle degeneration and pain relief after percutaneous epidural adhesiolysis in patients with degenerative lumbar spinal disease identified higher fatty infiltration of the paraspinal muscles as an independent factor associated with poorer analgesic outcomes in patients aged 65 years or older. In contrast, no significant association was found between the CSA of the paraspinal muscles and pain relief following the procedure [32]. These results are partly consistent with and partly contradictory to our findings, as PMI was a significant predictor of treatment response to RFA in our study, whereas PSMI was not.
In previous studies, fat infiltration of the paraspinal muscles appeared to be associated with poor analgesic outcomes. However, in our study, we did not include fat infiltration as a parameter for evaluating sarcopenia for several reasons. First, many studies have failed to demonstrate a clear association between pain and the presence or severity of facet arthropathy on CT or MRI [33]. Nonetheless, CT or MRI was routinely performed prior to RFA to exclude other potential etiologies, such as discogenic back pain. Although imaging alone is insufficient for diagnosing facetogenic pain, MRI is generally more expensive than CT in Korea. Furthermore, Berg et al. [34] recommended that researchers consider incorporating CT rather than relying solely on MRI in studies of facet arthropathy, as CT provides superior reliability in assessing the overall grade of facet arthropathy, including osteophyte formation and hypertrophy. Consequently, in clinical practice, MRI evaluations have often not been performed prior to RFA.
As discussed, existing studies on non-surgical spinal interventions have produced mixed results. One plausible explanation is that previous research has largely focused on epidural procedures, with no studies specifically targeting patients with facet-mediated pain. This distinction is clinically significant, as the pain-generating mechanisms and therapeutic responses in lumbar spinal disorders are highly heterogeneous. These findings highlight the inadequacy of a one-size-fits-all approach and support a growing emphasis on mechanism-based, individualized therapeutic strategies in spinal care. Future prospective studies are needed to develop comprehensive, personalized predictive models integrating these variables to improve clinical decision-making and patient outcomes.
The psoas muscles play an important role in spinal biomechanics and maintain lumbar stability during upright posture [35]. Our findings indicate that the RFA of the medial branch nerve is less effective in patients with a reduced PMI and that PMI predicts treatment success at 6 months post-procedure. Although PMI has not been previously studied as a prognostic factor in facetogenic pain, studies report its value in predicting postoperative outcomes following spinal surgery. In a study conducted on the Asian population, patients with sarcopenia and low PMI experienced longer hospital stays than those without sarcopenia despite similar rates of postoperative complications [36]. In another study of patients > 65 years of age, those with low PMI require more blood transfusions and experience longer intensive care unit stays after elective thoracolumbar spine surgery, indicating that PMI is a valuable predictor of postoperative recovery in this population [37]. Bourassa-Moreau et al. [38] report that decreased psoas CSA is associated with postoperative adverse events and increased 3-month mortality following surgery for metastatic spine disease. Similarly, Gakhar et al. [39] report that a reduced psoas area is a predictor of 1-year mortality in patients undergoing surgical decompression for spinal metastases.
Our findings indicate no association between PLVI and overall treatment success. Although PLVI is employed to predict prognosis in patients undergoing spinal surgery and interventional procedures study findings remain inconsistent. For example, elderly patients with low PLVI undergoing single-segment lumbar fusion report significantly higher back pain and disability scores and quality-of-life scores [40]. Similarly, patients with osteoporotic vertebral compression fractures and low PLVI experience poorer outcomes in terms of postoperative pain, functional recovery, and higher refracture rates [41]. In contrast, patients with low PLVI scores did not experience higher rates of postoperative surgical site infections [42], and low PLVI was not identified as an independent risk factor for infection or proximal junctional disease in patients undergoing lumbar arthrodesis for degenerative disc disease [43].
Sarcopenia significantly lowers the multifidus and erector spinae muscle index [44], and degeneration of the paraspinal muscles strongly correlates with facet joint osteoarthritis [45]. Consistent with these findings, our findings also showed that patients with sarcopenia exhibited lower PSMI. However, PSMI did not correlate with treatment response in our study. Similar studies suggest that PMI serves as a more reliable predictor of surgical outcomes than other methods, such as the CSA of the paraspinal muscles, which lacks association with outcomes following lumbar fusion [46,47]. Furthermore, sarcopenia defined by paraspinal muscle CSA has not been found to influence the clinical success of lumbar fusion in patients with degenerative spondylolisthesis [47]. This may be attributed to the fact that, with aging and degenerative changes, muscle tissue is frequently replaced by fat, while the overall CSA can remain relatively preserved, thereby diminishing its prognostic value [48].
In addition to sarcopenia-related variables, our findings indicate a strong trend linking the absence of diabetes and no prior spinal surgery to better treatment response. In a study examining the effects of RFA on the medial branch nerves in elderly patients [8], the presence of failed back surgery syndrome was identified as an independent factor negatively affecting rates of excellent and good outcomes. Spinal fusion sometimes serves as a treatment option for facetogenic pain, with many surgeons intentionally or inadvertently performing medial branch rhizotomies during pedicle screw placement [49]. Although limited, studies investigating the association between diabetes and epidural steroid injections report that patients with diabetes and poor glycemic control tend to experience reduced pain relief, based on a retrospective cohort study [50]. Furthermore, our multivariate logistic regression analysis revealed that pain duration did not significantly predict responder status. This finding aligns with previous studies showing that pain duration did not significantly influence treatment success [51].
The two groups differ significantly in demographic characteristics, BMI, history of prior spinal surgery, and the presence of spondylolisthesis. Although the underlying causes remain unclear, several explanations may be considered. While sarcopenic individuals may exhibit increased fat mass in sarcopenic obesity, the progressive decline in muscle mass is typically associated with lower BMI [52]. Moreover, a systematic review and meta-analysis report that sarcopenia is associated with poorer postoperative quality of life in elderly patients with lumbar degenerative disease [53], prompting surgeons to favor conservative management in this population. Additionally, as degenerative spondylolisthesis often results from chronic mechanical stress and increased axial loading on the lumbar spine, reduced physical activity commonly observed in patients with sarcopenia may lower their risk of developing this condition [54].
This study has some limitations. First, physical functions measured through objective assessments, such as gait speed and muscle strength, were not included in the evaluation of sarcopenia. Second, this is a single-center study involving a relatively small patient cohort, predominantly of South Korean ethnicity. Third, patients were divided into two groups based on their PMI values, assuming those with lower values have sarcopenia. However, no consensus currently exists regarding the optimal cutoff value. Fourth, treatment response was defined solely by changes in NRS scores, without considering changes in other important outcomes such as physical functional status or patient satisfaction.
5. Conclusions
Sarcopenia may influence the degree of pain relief achieved following RFA of the medial branch nerves. Additionally, patient-specific factors such as diabetes, history of spinal surgery, and PMI should be taken into account when predicting treatment outcomes. These considerations can contribute to more effective, personalized, patient-centered management of lumbar facet arthropathy.
Author Contributions
Conceptualization, K.W.-J.; methodology, K.W.-J.; software, K.W.-J.; validation, K.W.-J.; formal analysis K.W.-J.; investigation, Y.S.H.; resources, Y.S.H.; data curation, Y.S.H.; writing—original draft preparation, Y.S.H.; writing—review and editing, K.W.-J.; visualization, K.W.-J.; supervision, K.W.-J.; project administration, K.W.-J. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of Ewha Womans University Mokdong Hospital (EUMC 2024-10-001-001), approval date is October 17, 2024.
Informed Consent Statement
Patient consent was waived due to a Retrospective Analysis.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
We thank Lee HA for performing the statistical consultation.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| MBB | medial branch block |
| RFA | Radiofrequency ablation |
| PMI | psoas muscle index |
| PLVI | psoas-lumbar vertebral index |
| PSMI | paraspinal muscle index |
| CT | computed tomography |
| MRI | Magnetic Resonance Imaging |
| BMI | body mass index |
| NRS | Numeric Rating Scale |
| CSA | cross-sectional area |
References
- Manchikanti, L.; Kosanovic, R.; Pampati, V.; Cash, K.A.; Soin, A.; Kaye, A.D.; Hirsch, J.A. Low Back Pain and Diagnostic Lumbar Facet Joint Nerve Blocks: Assessment of Prevalence, False-Positive Rates, and a Philosophical Paradigm Shift from an Acute to a Chronic Pain Model. Pain Physician 2020, 23, 519–530. [Google Scholar] [CrossRef] [PubMed]
- Laplante, B.L.; Ketchum, J.M.; Saullo, T.R.; DePalma, M.J. Multivariable analysis of the relationship between pain referral patterns and the source of chronic low back pain. Pain Physician 2012, 15, 171–178. [Google Scholar]
- Manchikanti, L.; Pampati, V.; Soin, A.; Vanaparthy, R.; Sanapati, M.R.; Kaye, A.D.; Hirsch, J.A. Trends of Expenditures and Utilization of Facet Joint Interventions in Fee-For-Service (FFS) Medicare Population from 2009-2018. Pain Physician 2020, 23, S129–S147. [Google Scholar] [CrossRef] [PubMed]
- Hao, D.; Yong, R.J.; Cohen, S.P.; Stojanovic, M.P. Medial Branch Blocks and Radiofrequency Ablation for Low Back Pain from Facet Joints. N Engl J Med 2023, 389, e53. [Google Scholar] [CrossRef] [PubMed]
- Cohen, S.P.; Doshi, T.L.; Kurihara, C.; Dolomisiewicz, E.; Liu, R.C.; Dawson, T.C.; Hager, N.; Durbhakula, S.; Verdun, A.V.; Hodgson, J.A.; et al. Waddell (Nonorganic) Signs and Their Association With Interventional Treatment Outcomes for Low Back Pain. Anesth Analg 2021, 132, 639–651. [Google Scholar] [CrossRef]
- Cohen, S.P.; Hurley, R.W.; Christo, P.J.; Winkley, J.; Mohiuddin, M.M.; Stojanovic, M.P. Clinical predictors of success and failure for lumbar facet radiofrequency denervation. Clin J Pain 2007, 23, 45–52. [Google Scholar] [CrossRef]
- Lee, D.W.; Pritzlaff, S.; Jung, M.J.; Ghosh, P.; Hagedorn, J.M.; Tate, J.; Scarfo, K.; Strand, N.; Chakravarthy, K.; Sayed, D.; et al. Latest Evidence-Based Application for Radiofrequency Neurotomy (LEARN): Best Practice Guidelines from the American Society of Pain and Neuroscience (ASPN). J Pain Res 2021, 14, 2807–2831. [Google Scholar] [CrossRef]
- Chen, Y.S.; Liu, B.; Gu, F.; Sima, L. Radiofrequency Denervation on Lumbar Facet Joint Pain in the Elderly: A Randomized Controlled Prospective Trial. Pain Physician 2022, 25, 569–576. [Google Scholar]
- Falco, F.J.; Manchikanti, L.; Datta, S.; Sehgal, N.; Geffert, S.; Onyewu, O.; Zhu, J.; Coubarous, S.; Hameed, M.; Ward, S.P.; et al. An update of the effectiveness of therapeutic lumbar facet joint interventions. Pain Physician 2012, 15, E909–953. [Google Scholar] [CrossRef]
- Boswell, M.V.; Colson, J.D.; Sehgal, N.; Dunbar, E.E.; Epter, R. A systematic review of therapeutic facet joint interventions in chronic spinal pain. Pain Physician 2007, 10, 229–253. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyere, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef] [PubMed]
- Bentov, I.; Kaplan, S.J.; Pham, T.N.; Reed, M.J. Frailty assessment: from clinical to radiological tools. Br J Anaesth 2019, 123, 37–50. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef]
- Amini, N.; Spolverato, G.; Gupta, R.; Margonis, G.A.; Kim, Y.; Wagner, D.; Rezaee, N.; Weiss, M.J.; Wolfgang, C.L.; Makary, M.M.; et al. Impact Total Psoas Volume on Short- and Long-Term Outcomes in Patients Undergoing Curative Resection for Pancreatic Adenocarcinoma: a New Tool to Assess Sarcopenia. J Gastrointest Surg 2015, 19, 1593–1602. [Google Scholar] [CrossRef] [PubMed]
- Ebbeling, L.; Grabo, D.J.; Shashaty, M.; Dua, R.; Sonnad, S.S.; Sims, C.A.; Pascual, J.L.; Schwab, C.W.; Holena, D.N. Psoas:lumbar vertebra index: central sarcopenia independently predicts morbidity in elderly trauma patients. Eur J Trauma Emerg Surg 2014, 40, 57–65. [Google Scholar] [CrossRef]
- Pinter, Z.W.; Salmons, H.I.t.; Townsley, S.; Omar, A.; Freedman, B.A.; Currier, B.L.; Elder, B.D.; Nassr, A.N.; Bydon, M.; Wagner, S.C.; et al. Multifidus Sarcopenia Is Associated With Worse Patient-reported Outcomes Following Posterior Cervical Decompression and Fusion. Spine (Phila Pa 1976) 2022, 47, 1426–1434. [Google Scholar] [CrossRef] [PubMed]
- Rodge, G.A.; Goenka, U.; Jajodia, S.; Agarwal, R.; Afzalpurkar, S.; Roy, A.; Goenka, M.K. Psoas Muscle Index: A Simple and Reliable Method of Sarcopenia Assessment on Computed Tomography Scan in Chronic Liver Disease and its Impact on Mortality. J Clin Exp Hepatol 2023, 13, 196–202. [Google Scholar] [CrossRef]
- Shimizu, T.; Miyake, M.; Hori, S.; Ichikawa, K.; Omori, C.; Iemura, Y.; Owari, T.; Itami, Y.; Nakai, Y.; Anai, S.; et al. Clinical Impact of Sarcopenia and Inflammatory/Nutritional Markers in Patients with Unresectable Metastatic Urothelial Carcinoma Treated with Pembrolizumab. Diagnostics (Basel) 2020, 10. [Google Scholar] [CrossRef]
- Tsukagoshi, M.; Yokobori, T.; Yajima, T.; Maeno, T.; Shimizu, K.; Mogi, A.; Araki, K.; Harimoto, N.; Shirabe, K.; Kaira, K. Skeletal muscle mass predicts the outcome of nivolumab treatment for non-small cell lung cancer. Medicine (Baltimore) 2020, 99, e19059. [Google Scholar] [CrossRef]
- Kim, J.S.; Kim, W.Y.; Park, H.K.; Kim, M.C.; Jung, W.; Ko, B.S. Simple Age Specific Cutoff Value for Sarcopenia Evaluated by Computed Tomography. Ann Nutr Metab 2017, 71, 157–163. [Google Scholar] [CrossRef]
- Sim, J.H.; Lee, S.H.; Kim, J.W.; Koh, W.U.; Kim, H.T.; Ro, Y.J.; Kim, H.J. Low Psoas Lumbar Vertebral Index Is Associated with Mortality after Hip Fracture Surgery in Elderly Patients: A Retrospective Analysis. J Pers Med 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- An, S.M.; Chae, J.S.; Lee, H.J.; Cho, S.; Im, J. Association of Psoas: Lumbar Vertebral Index (PLVI) with Postherpetic Neuralgia in Patients Aged 60 and Older with Herpes Zoster. J Clin Med 2024, 13. [Google Scholar] [CrossRef]
- Kwon, H.J.; Kim, C.S.; Kim, S.; Yoon, S.H.; Koh, J.; Kim, Y.K.; Choi, S.S.; Shin, J.W.; Kim, D.H. Association between fatty infiltration in the cervical multifidus and treatment response following cervical interlaminar epidural steroid injection. Korean J Pain 2023, 36, 358–368. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Park, S.J.; Yoon, K.B.; Jun, E.K.; Cho, J.; Kim, H.J. Influence of Handgrip Strength and Psoas Muscle Index on Analgesic Efficacy of Epidural Steroid Injection in Patients With Degenerative Lumbar Spinal Disease. Pain Physician 2022, 25, E1105–E1113. [Google Scholar]
- Kim, H.J.; Rho, M.; Yoon, K.B.; Jo, M.; Lee, D.W.; Kim, S.H. Influence of cross-sectional area and fat infiltration of paraspinal muscles on analgesic efficacy of epidural steroid injection in elderly patients. Pain Pract 2022, 22, 621–630. [Google Scholar] [CrossRef] [PubMed]
- Inose, H.; Yamada, T.; Hirai, T.; Yoshii, T.; Abe, Y.; Okawa, A. The impact of sarcopenia on the results of lumbar spinal surgery. Osteoporos Sarcopenia 2018, 4, 33–36. [Google Scholar] [CrossRef]
- Van Zundert, J.; Mekhail, N.; Vanelderen, P.; van Kleef, M. Diagnostic medial branch blocks before lumbar radiofrequency zygapophysial (facet) joint denervation: benefit or burden? Anesthesiology 2010, 113, 276–278. [Google Scholar] [CrossRef]
- Dobrogowski, J.; Wrzosek, A.; Wordliczek, J. Radiofrequency denervation with or without addition of pentoxifylline or methylprednisolone for chronic lumbar zygapophysial joint pain. Pharmacol Rep 2005, 57, 475–480. [Google Scholar]
- Dworkin, R.H.; Turk, D.C.; Wyrwich, K.W.; Beaton, D.; Cleeland, C.S.; Farrar, J.T.; Haythornthwaite, J.A.; Jensen, M.P.; Kerns, R.D.; Ader, D.N.; et al. Interpreting the clinical importance of treatment outcomes in chronic pain clinical trials: IMMPACT recommendations. J Pain 2008, 9, 105–121. [Google Scholar] [CrossRef]
- Han, Y.A.; Kwon, H.J.; Lee, K.; Son, M.G.; Kim, H.; Choi, S.S.; Shin, J.W.; Kim, D.H. Impact of Sarcopenia on Percutaneous Epidural Balloon Neuroplasty in Patients with Lumbar Spinal Stenosis: A Retrospective Analysis. Medicina (Kaunas) 2023, 59. [Google Scholar] [CrossRef]
- Zager, Y.; Khalilieh, S.; Ganaiem, O.; Gorgov, E.; Horesh, N.; Anteby, R.; Kopylov, U.; Jacoby, H.; Dreznik, Y.; Dori, A.; et al. Low psoas muscle area is associated with postoperative complications in Crohn's disease. Int J Colorectal Dis 2021, 36, 543–550. [Google Scholar] [CrossRef]
- Kang, M.; Kim, S.H.; Jo, M.; Jung, H.E.; Bae, J.; Kim, H.J. Evaluation of Paraspinal Muscle Degeneration on Pain Relief after Percutaneous Epidural Adhesiolysis in Patients with Degenerative Lumbar Spinal Disease. Medicina (Kaunas) 2023, 59. [Google Scholar] [CrossRef] [PubMed]
- Gellhorn, A.C.; Katz, J.N.; Suri, P. Osteoarthritis of the spine: the facet joints. Nat Rev Rheumatol 2013, 9, 216–224. [Google Scholar] [CrossRef]
- Berg, L.; Thoresen, H.; Neckelmann, G.; Furunes, H.; Hellum, C.; Espeland, A. Facet arthropathy evaluation: CT or MRI? Eur Radiol 2019, 29, 4990–4998. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.B.; Park, S.W.; Lee, Y.S.; Nam, T.K.; Park, Y.S.; Kim, Y.B. The Effects of Spinopelvic Parameters and Paraspinal Muscle Degeneration on S1 Screw Loosening. J Korean Neurosurg Soc 2015, 58, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.A.; Wong, W.S.; Zheng, Y.; Leow, B.H.W.; Low, Y.L.; Tan, L.F.; Teo, K.; Nga, V.D.W.; Yeo, T.T.; Lim, M.J.R. Effect of psoas muscle index on early postoperative outcomes in surgically treated spinal tumours in an Asian population. J Clin Neurosci 2024, 126, 214–220. [Google Scholar] [CrossRef]
- Pernik, M.N.; Hicks, W.H.; Akbik, O.S.; Nguyen, M.L.; Luu, I.; Traylor, J.I.; Deme, P.R.; Dosselman, L.J.; Hall, K.; Wingfield, S.A.; et al. Psoas Muscle Index as a Predictor of Perioperative Outcomes in Geriatric Patients Undergoing Spine Surgery. Global Spine J 2023, 13, 2016–2024. [Google Scholar] [CrossRef]
- Bourassa-Moreau, E.; Versteeg, A.; Moskven, E.; Charest-Morin, R.; Flexman, A.; Ailon, T.; Dalkilic, T.; Fisher, C.; Dea, N.; Boyd, M.; et al. Sarcopenia, but not frailty, predicts early mortality and adverse events after emergent surgery for metastatic disease of the spine. Spine J 2020, 20, 22–31. [Google Scholar] [CrossRef]
- Gakhar, H.; Dhillon, A.; Blackwell, J.; Hussain, K.; Bommireddy, R.; Klezl, Z.; Williams, J. Study investigating the role of skeletal muscle mass estimation in metastatic spinal cord compression. Eur Spine J 2015, 24, 2150–2155. [Google Scholar] [CrossRef]
- Sun, K.; Zhu, H.; Huang, B.; Li, J.; Liu, G.; Jiao, G.; Chen, G. MRI-based central sarcopenia negatively impacts the therapeutic effectiveness of single-segment lumbar fusion surgery in the elderly. Sci Rep 2024, 14, 5043. [Google Scholar] [CrossRef]
- Sun, K.; Liu, J.; Zhu, H.; Wang, J.; Wan, H.; Huang, B.; Zhang, Q.; Chen, G. Lower psoas mass indicates worse prognosis in percutaneous vertebroplasty-treated osteoporotic vertebral compression fracture. Sci Rep 2024, 14, 13880. [Google Scholar] [CrossRef] [PubMed]
- Ruffilli, A.; Manzetti, M.; Cerasoli, T.; Barile, F.; Viroli, G.; Traversari, M.; Salamanna, F.; Fini, M.; Faldini, C. Osteopenia and Sarcopenia as Potential Risk Factors for Surgical Site Infection after Posterior Lumbar Fusion: A Retrospective Study. Microorganisms 2022, 10. [Google Scholar] [CrossRef]
- Ruffilli, A.; Manzetti, M.; Barile, F.; Ialuna, M.; Cerasoli, T.; Viroli, G.; Salamanna, F.; Contartese, D.; Giavaresi, G.; Faldini, C. Complications after Posterior Lumbar Fusion for Degenerative Disc Disease: Sarcopenia and Osteopenia as Independent Risk Factors for Infection and Proximal Junctional Disease. J Clin Med 2023, 12. [Google Scholar] [CrossRef]
- Fang, T.; Xue, Z.; Zhou, Q.; Gao, J.; Mi, J.; Yang, H.; Zhou, F.; Liu, H.; Zhang, J. Impact of Paraspinal Sarcopenia on Clinical Outcomes in Intervertebral Disc Degeneration Patients Following Percutaneous Transforaminal Endoscopic Lumbar Discectomy. Orthop Surg 2025, 17, 1332–1339. [Google Scholar] [CrossRef]
- Yu, B.; Jiang, K.; Li, X.; Zhang, J.; Liu, Z. Correlation of the Features of the Lumbar Multifidus Muscle With Facet Joint Osteoarthritis. Orthopedics 2017, 40, e793–e800. [Google Scholar] [CrossRef] [PubMed]
- Akbik, O.S.; Al-Adli, N.; Pernik, M.N.; Hicks, W.H.; Hall, K.; Aoun, S.G.; Bagley, C.A. A Comparative Analysis of Frailty, Disability, and Sarcopenia With Patient Characteristics and Outcomes in Adult Spinal Deformity Surgery. Global Spine J 2023, 13, 2345–2356. [Google Scholar] [CrossRef]
- McKenzie, J.C.; Wagner, S.C.; Sebastian, A.; Casper, D.S.; Mangan, J.; Stull, J.; Hilibrand, A.S.; Vaccaro, A.R.; Kepler, C. Sarcopenia does not affect clinical outcomes following lumbar fusion. J Clin Neurosci 2019, 64, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Teichtahl, A.J.; Urquhart, D.M.; Wang, Y.; Wluka, A.E.; Wijethilake, P.; O'Sullivan, R.; Cicuttini, F.M. Fat infiltration of paraspinal muscles is associated with low back pain, disability, and structural abnormalities in community-based adults. Spine J 2015, 15, 1593–1601. [Google Scholar] [CrossRef]
- Markwalder, T.M.; Merat, M. The lumbar and lumbosacral facet-syndrome. Diagnostic measures, surgical treatment and results in 119 patients. Acta Neurochir (Wien) 1994, 128, 40–46. [Google Scholar] [CrossRef]
- Wong, F.; Namdari, B.; Dupler, S.; Kovac, M.F.; Makarova, N.; Dalton, J.E.; Turan, A. No difference in pain reduction after epidural steroid injections in diabetic versus nondiabetic patients: A retrospective cohort study. J Anaesthesiol Clin Pharmacol 2016, 32, 84–88. [Google Scholar] [CrossRef]
- Streitberger, K.; Muller, T.; Eichenberger, U.; Trelle, S.; Curatolo, M. Factors determining the success of radiofrequency denervation in lumbar facet joint pain: a prospective study. Eur Spine J 2011, 20, 2160–2165. [Google Scholar] [CrossRef] [PubMed]
- Romero-Corral, A.; Montori, V.M.; Somers, V.K.; Korinek, J.; Thomas, R.J.; Allison, T.G.; Mookadam, F.; Lopez-Jimenez, F. Association of bodyweight with total mortality and with cardiovascular events in coronary artery disease: a systematic review of cohort studies. Lancet 2006, 368, 666–678. [Google Scholar] [CrossRef] [PubMed]
- Wu, W.T.; Lee, T.M.; Han, D.S.; Chang, K.V. The Prevalence of Sarcopenia and Its Impact on Clinical Outcomes in Lumbar Degenerative Spine Disease-A Systematic Review and Meta-Analysis. J Clin Med 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, L.; Hunter, D.J. Diagnosis and conservative management of degenerative lumbar spondylolisthesis. Eur Spine J 2008, 17, 327–335. [Google Scholar] [CrossRef]
Figure 1.
CONSORT flow diagram.
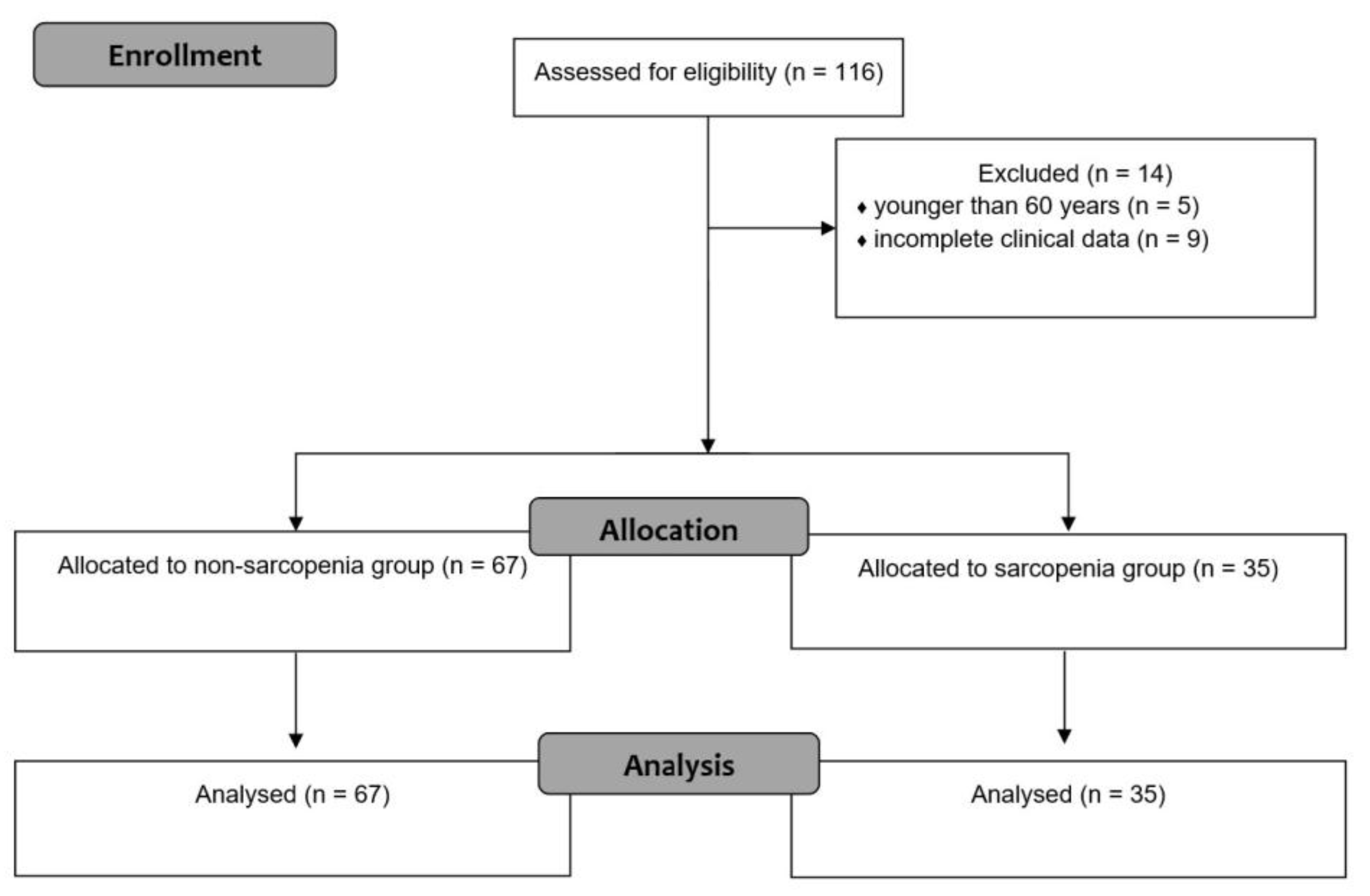
Figure 2.
Pain scores and proportion of responders. (A) Numeric Rating Scale scores for back pain. (B) Proportion of responders. *P < 0.05, baseline vs. post-RFAs; Wilcoxon signed-rank test. †P < 0.05, non-sarcopenia vs. sarcopenia; Mann–Whitney U test.
Figure 2.
Pain scores and proportion of responders. (A) Numeric Rating Scale scores for back pain. (B) Proportion of responders. *P < 0.05, baseline vs. post-RFAs; Wilcoxon signed-rank test. †P < 0.05, non-sarcopenia vs. sarcopenia; Mann–Whitney U test.
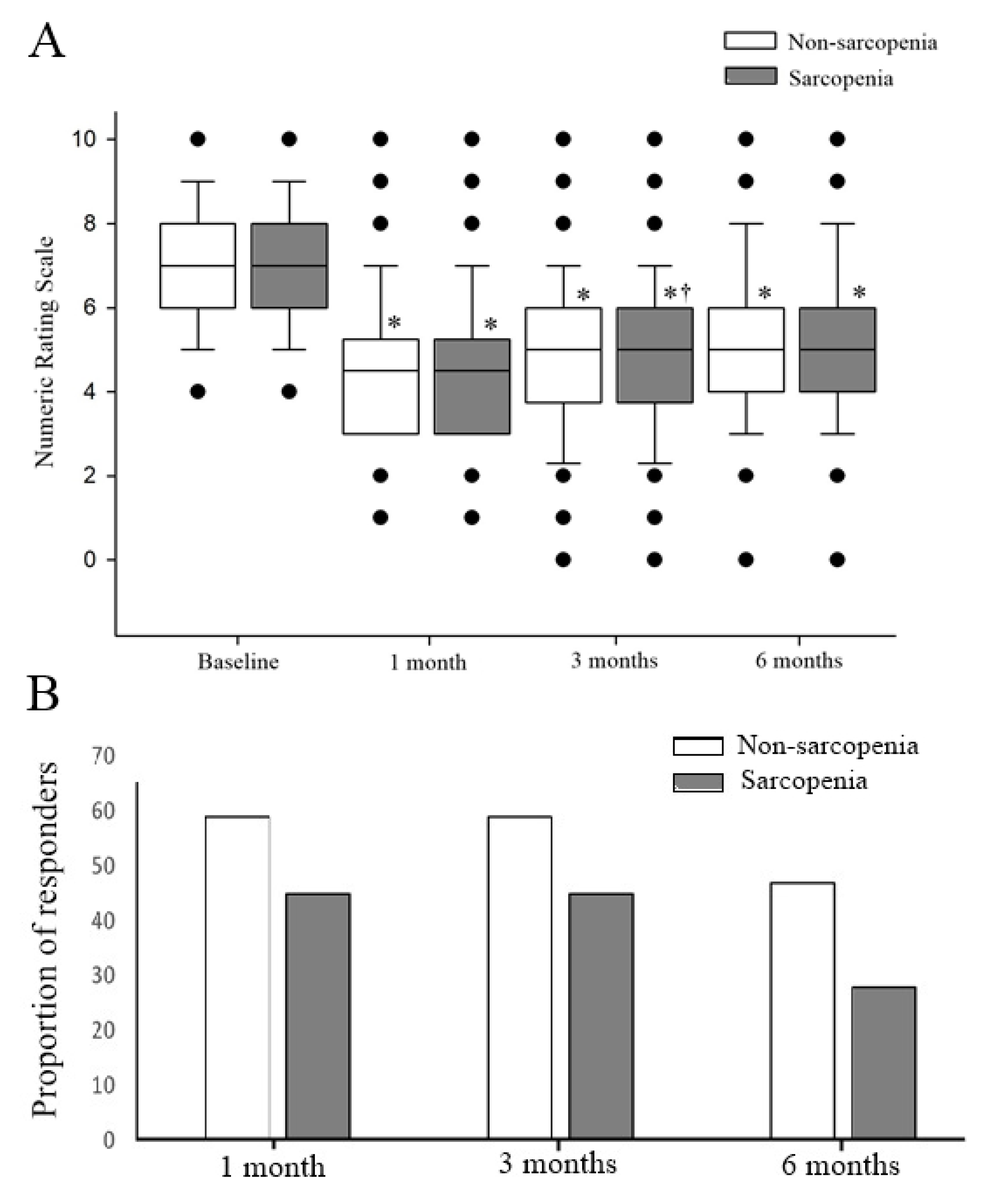

Table 1.
Demographic characteristics.
| Non-sarcopenia (N = 67) | Sarcopenia (N = 35) | P-value | |
|---|---|---|---|
| Age (years) | 77.00 [11.00] | 73.00 [10.00] | 0.086 |
| Sex (M/F) | 19 (28.4) / 48 (71.6) | 7 (20.0) / 28 (80.0) | 0.358 |
| Height (cm) | 155.00 [11.00] | 155.00 [8.00] | 0.748 |
| BMI (kg/m2) | 25.00 [4.00] | 22.00 [4.00] | 0.000 |
| Diabetes mellitus | 17 (25.4) | 4 (11.4) | 0.098 |
| Surgery history | 15 (22.4) | 2 (5.7) | 0.032 |
| Compression fracture | 11 (16.4) | 6 (17.1) | 0.926 |
| Spondylolisthesis | 32 (47.8) | 9 (25.7) | 0.031 |
| Duration (months) | 8.00 [19.00] | 14.00 [30.00] | 0.152 |
| Number of levels treated (2 / 3 / 4) | 28 (42) / 36 (54) / 3 (4) | 15 (43) / 18 (51) / 2 (6) | 0.951 |
| Laterality (Left / Right) | 39 (58.2) / 28 (41.8) | 17 (48.6) / 18 (54.4) | 0.353 |
| PLVI | 0.597 ± 0.179 | 0.470 ± 0.154 | 0.001 |
| PSMI (mm²/m²) | |||
| Ipsilateral | 2780.02 [1014.80] | 2388.90 [727.40] | 0.000 |
| Contralateral | 2878.90 [823.10] | 2461.08 [580.41] | 0.000 |
Data are presented as the mean ± standard deviation, median [interquartile range], or number of patients (%). Bold indicates statistical significance. BMI, Body mass index; PLVI, psoas-lumbar vertebral index; PSMI, Paraspinal muscles index.
Table 2.
Factors associated with treatment response based on multivariate logistic regression analysis.
Table 2.
Factors associated with treatment response based on multivariate logistic regression analysis.
| Variable | Reference group | OR | 95% CI | P-value |
|---|---|---|---|---|
| 3 months after RFA | ||||
| Duration | - | 0.982 | 0.961–1.004 | 0.110 |
| Surgery history | No surgery history | 0.246 | 0.065–0933 | 0.039 |
| 6 months after RFA | ||||
| Diabetes mellitus | No diabetes mellitus | 0.298 | 0.104–0.853 | 0.024 |
| Surgery history | No surgery history | 0.165 | 0.046–0.589 | 0.006 |
| PMI | - | 1.003 | 1.000–1.006 | 0.042 |
Bold indicates statistical significance. CI, confidence interval; OR, odds ratio; PMI, psoas muscle index; RFA, Radiofrequency ablation.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



