
Submitted:
26 June 2025
Posted:
30 June 2025
You are already at the latest version
Abstract
Internalisation of sociocultural ideals and beliefs about weight and shape has long been recognised as an important predictor of disordered eating. However, thin-ideal internalisation and weight bias internalisation (WBI) are generally examined separately in the literature and within sociocultural models of eating disorders. Additionally, self-compassion has been identified as a protective factor against disordered eating, but its role in mitigating the impact of internalisation of these sociocultural ideals and beliefs has not been investigated. The current study aimed to investigate (1) the unique contribution of thin-ideal internalisation and WBI in predicting eating disorder behaviours and cognitions and (2) the role of self-compassion in moderating the relationship between thin-ideal/WBI and eating pathology. Four hundred and seventy-five (475) cisgender women completed an anonymous online survey. Results indicated that both thin-ideal internalisation and WBI uniquely contributed to the prediction of eating pathology after controlling for body mass index. Self-compassion buffered the effect of thin-ideal internalisation on restraint, and the effect of WBI on eating concern. Results support consideration of both thin-ideal internalisation and WBI in sociocultural models of eating disorders and as targets for eating disorder interventions, particularly those based on self-compassion therapy.
Keywords:
disordered eating
; thin-ideal internalisation
; weight bias internalisation
; self-compassion
1. Introduction
The global prevalence of eating disorders has continued to rise in recent decades, more than doubling from 3.5% in 2000 to 7.8% in 2018 [1]. In addition to those who meet diagnostic criteria for eating disorders, it is likely that an even larger proportion of individuals experience sub-threshold eating pathology [2]. Thus, developing a further understanding of the aetiology of disordered eating and effective treatment approaches remains a key focus for research.
A significant body of research on the factors that contribute to the development and maintenance of disordered eating, particularly among women, has highlighted the influential role of sociocultural ideals and beliefs about body weight and shape [3,4,5]. Western societies have long promoted the ‘thin ideal’, equating a slim physique with feminine beauty and virtue. This ideal is reinforced through sociocultural influences such as the media (e.g., advertising, magazines, television), peers, and family members [6]. Corresponding to the thin ideal is the stigmatisation of overweight and obesity, through the negative stereotyping of individuals with larger bodies as ‘lazy’ and ‘undisciplined’ with the implication that they are personally responsible for their weight [6,7,8]. Research indicates that these stigmatising beliefs manifest in the community, with heavier individuals being teased, treated unfairly or discriminated against based on their weight [9]. Individuals may experience weight stigma from a range of sources including classmates, colleagues, doctors, family members, and friends, with individuals of higher body mass index (BMI) reporting more frequent weight stigmatising experiences [9,10].
Research has demonstrated that internalisation of the thin ideal and weight bias contributes to the development and maintenance of disordered eating [3,4,5]. Thin-ideal internalisation can be defined as the “extent to which an individual cognitively ‘buys into’ socially defined ideals of attractiveness [associated with thinness] and engages in behaviours designed to produce an approximate of these ideals” [5] (p. 181). Weight bias internalisation (WBI) is defined as the awareness, agreement, and application of negative weight stereotypes to the self, resulting in devaluation of oneself based on body weight [11]. Research has found that WBI is positively correlated with BMI, such that individuals with higher BMIs experience greater levels of WBI [4].
Sociocultural models of eating disorders predominantly focus on the role of thin-ideal internalisation in eating disorder development and maintenance [6,12]. A leading sociocultural model of eating disorders, the tripartite influence model of body image and eating disturbance [6], suggests that individuals experience sociocultural pressure to be thin which is reinforced by sources including the media, family and peers. Pressure to be thin leads to thin-ideal internalisation and appearance comparisons to others, which in turn leads to body dissatisfaction and disordered eating. The dual pathway model of bulimia nervosa [12] proposes a similar model, suggesting that pressure to be thin leads to thin-ideal internalisation and, in turn, body dissatisfaction. This then leads to dietary restraint and negative affect, ultimately resulting in bulimic pathology.
These models have garnered significant support within the literature. Research has demonstrated that exposure to the thin ideal in the media is positively associated with thin-ideal internalisation and the frequency of cognitions and behaviours related to anorexia and bulimia [13]. Findings have also highlighted negative outcomes associated with thin-ideal internalisation including increased body dissatisfaction, negative affect, dieting and bulimic symptoms [5,14]. Additionally, longitudinal research has shown that thin-ideal internalisation is predictive of future onset of both sub-threshold and threshold bulimia [15].
Based on evidence for sociocultural models of disordered eating, interventions have been developed that aim to reduce disordered eating and prevent eating disorder onset by targeting thin-ideal internalisation. One such program with an extensive evidence-base is the cognitive dissonance-based intervention, the Body Project [16,17]. This intervention involves participants generating critiques of the thin ideal through verbal, written and behavioural tasks; for example, identifying costs of pursuing the thin ideal and engaging in role-plays that involve convincing others not to pursue the ideal [17]. Findings reveal that the Body Project leads to significant reductions in thin-ideal internalisation, body dissatisfaction, negative affect, dieting and eating disorder symptoms [16]. Additionally, these effects are greater than those produced by alternative interventions such as educational videos or the Healthy Weight program [16,18]. Although this intervention was initially designed for use with women, further research has demonstrated that it can be modified to target eating disorder risk factors among other population groups, including men, male athletes and homosexual men. These modified versions of the Body Project have led to reductions in body dissatisfaction, including dissatisfaction with muscularity, muscle dysmorphia, drive for muscularity and dissatisfaction with body fat [19].
While most research into WBI focusses on individuals with overweight or obesity, findings suggest that WBI is positively associated with binge eating and purging behaviours among individuals of varying BMIs [3,4]. Individuals with higher WBI experience greater levels of disordered eating as well as greater levels of depression and anxiety, poorer self-esteem and body image, and lower motivation/self-efficacy to participate in health promoting behaviour e.g., physical exercise [11]. A study by Romano et al. [3] suggested that the mechanisms behind the association of WBI and disordered eating may be like those proposed by the tripartite influence model. Findings provided support for a model wherein weight stigmatising experiences predict WBI, which in turn predicts body dissatisfaction, leading to disordered eating. Therefore, both models suggest that both pressures to be thin (i.e., to meet body ideals) or pressure not to be fat (i.e., to avoid weight stigma) from sociocultural influences lead to internalisation of societal ideals/beliefs around body weight and shape, which then lead to body dissatisfaction and subsequently, eating pathology [3,6].
To date, thin-ideal internalisation and WBI have largely been examined separately within the literature, with a paucity of research examining the unique and combined effects of these two factors in disordered eating. While both constructs relate to internalisation of societal ideals or beliefs around body weight and shape, they are theoretically distinct [20]. Supporting this notion are research findings demonstrating that thin-ideal internalisation and WBI differ in their relationships to related constructs. For example, WBI is positively correlated with BMI and is predominantly associated with binge eating, whereas thin-ideal internalisation does not appear to be correlated with BMI and is predominantly associated with dieting and bulimic pathology, including purging behaviours [4,15,20,21]. A recent study by Nutter et al. [22] suggested that the relationship between thin-ideal internationalisation and anti-fat attitudes, a form of weight stigma, is mediated by appearance comparisons. However, the relationship between thin-ideal internalisation and WBI was not examined.
A recent study by Harris [20] examined the moderating effect of BMI in the relationship between thin-ideal internalisation, WBI and body dissatisfaction in a sample of college-aged individuals. Results indicated that both thin-ideal internalisation and WBI were independently related to body dissatisfaction. Additionally, thin-ideal internalisation and WBI were strongly correlated with one another across all levels of BMI. These findings highlight the need to consider the role of both aspects of internalisation in the aetiology of eating disorders. Further research is required to better understand the unique contribution of each construct in the prediction of eating disorder cognitions and behaviours and how targeting both forms of internalisation may enhance the effectiveness of intervention strategies [20]. As noted by Morton et al. [23], given that internalisation of weight-related sociocultural ideals/beliefs is considered extremely common within the population, it is beneficial to understand protective factors which may prevent individuals who have internalised these views from developing disordered eating.
In addition to vulnerability factors related to disordered eating, researchers have identified protective factors which may ameliorate the risk of developing eating pathology. One such protective factor is self-compassion [24,25,26], which refers to an individual’s ability to direct compassion inwardly and treat themselves with kindness (versus self-judgement), mindfulness (versus over identification) and common humanity (versus isolation) [27,28]. Research suggests that individuals who exhibit greater self-compassion experience higher levels of overall psychological wellbeing, including lower psychopathology such as depression, anxiety and stress [29] and higher psychological strengths including happiness and optimism [30].
Within the eating disorder literature, self-compassion has been negatively associated with body dissatisfaction and disordered eating patterns [24,25,26,31,32]. Self-compassion has also been negatively associated with shape and weight concern and body preoccupation [26]. A systematic review of 28 studies showed that self-compassion was consistently linked with better body image and lower eating pathology through simple mediation and serial mediation pathways involving maladaptive body image and eating disorder risk factors, and with some evidence of buffering effects [24]. A comparative study of university students and patients with diagnosed eating disorders reported significantly lower levels of self-compassion and greater fear of self-compassion in the patient group [25]. Longitudinal research suggests that low self-compassion may be predictive of eating disorder risk, with results of a study by Linardon [31] indicating that higher levels of self-compassion at baseline predicted a lower likelihood of experiencing the onset of eating disorder symptoms at an eight-month follow-up.
When considered within sociocultural models of eating disorders, research suggests that self-compassion may function as a protective factor against societal pressures related to disordered eating [33,34,35]. Findings from a study by Tylka et al. [35] indicated that individuals with higher levels of self-compassion perceived less sociocultural pressure to be thin. Self-compassion also acted as a buffer in the relationship between pressure to be thin (media) and thin-ideal internalisation and disordered eating, such that when self-compassion was low, pressure to be thin was more strongly related to both thin ideal-internalisation and disordered eating [35].
Based on relationships between self-compassion and numerous factors related to disordered eating, researchers have begun investigating the efficacy of self-compassion interventions for reducing disordered eating and associated risk factors. A meta-analysis by Turk and Waller [36] revealed that self-compassion-focussed interventions were effective in reducing body image concerns and disordered eating. Self-compassion interventions may also be effective in reducing risk factors for eating disorder development such as internalisation of sociocultural ideals [34,37]. Gobin et al. [34] demonstrated that implementation of a brief self-compassion intervention prior to exposure to thin ideal images on social media prevented subsequent increases in weight and appearance dissatisfaction that were experienced by individuals who did not receive the intervention. Self-compassion interventions have also demonstrated effectiveness in reducing WBI, with a recent study by Hopkins [37] finding that a brief digital, mindful self-compassion intervention delivered over 28 days led to significant reductions in WBI when compared to a waitlist control. While research has demonstrated that self-compassion may serve as a protective factor against the internalisation of sociocultural ideals and beliefs relating to weight and shape, there is a need to investigate whether self-compassion moderates the relationship between thin-ideal internalisation/WBI and disordered eating.
The aims of the present study are twofold. Firstly, the current study aims to extend the literature regarding sociocultural factors associated with disordered eating by investigating the unique contributions of thin-ideal internalisation and WBI in predicting eating disorder cognitions and behaviours. Secondly, the study aims to investigate the potential protective role of self-compassion in moderating the relationship between (a) thin-ideal internalisation and (b) WBI and disordered eating. Based on previous findings by Harris [20], it is hypothesised that thin-ideal internalisation and WBI will independently predict eating pathology. Due to the current lack of research related to the moderating role of self-compassion in these relationships, the moderated effects analysis was considered exploratory and no a priori hypotheses were generated.
2. Materials and Methods
Participants were recruited via a student research experience program at an Australian university and the researchers’ social media networks as part of a larger study that aimed to investigate the mediating effect of self-compassion in the relationship between body positive media and body image mental health literacy, thin-ideal internalisation, self-esteem and weight bias internalisation in cisgender women. An additional eligibility criterion for the larger study was that participants had not previously viewed the body positivity documentary film, Embrace (see Embrace: The Documentary (2016) - IMDb).
Four hundred and eighty (480) women participated in the first survey. Two univariate outliers for BMI were deleted and three multivariate outliers were deleted, reducing the final sample to 475. Age ranged from 18 to 67 years (M = 31.48, SD = 10.62). Most participants identified as Australian/Caucasian (67%), and remaining participants identified as European (7%), South Asian (7%), Asian (6%), African (3%), Middle Eastern (3%) Pacific Islander (1%), or multi-ethnicity (4%). Body Mass Index (BMI) ranged from 14.54 to 66.6 (SD = 7.14), with 46% of participants falling within the healthy weight range, 4% within the underweight range and 50% falling within pre-obesity to obesity range [38]. The average Eating Disorder Examination-Questionnaire global score for the sample was above the clinical cut-off of greater than or equal to 2.5 [39], at 3.06 (SD = 1.23).
Survey measures are described below.
The Modified Weight Bias Internalisation Scale (WBIS-M) [41] is an 11-item scale that measures the extent to which individuals evaluate themselves based on negative, weight-based stereotypes. Derived from the Weight Bias Internalisation Scale [42], the WBIS-M is suitable for individuals from a range of BMI categories. Responses are based on a 7-point Likert scale from 1 (strongly disagree) to 7 (strongly agree) with higher overall scores (averaged) indicating greater WBI.
The Internalisation Scale of the Sociocultural Attitudes toward Appearance Questionnaire 4 – Revised (SATAQ-4R) [40] contains five questions that measure internalisation of the thin ideal using a five-point Likert scale from 1 (definitely disagree) to 5 (definitely agree), with higher scores (averaged) indicating greater levels of internalisation.
The State Self-Compassion Scale – Long Form (SSCS-L) [43] is an 18-item scale that assesses self-kindness, self-judgment, common humanity, isolation, mindfulness, and over-identification in the moment on a Likert scale from 1 (not at all true for me) to 5 (very true for me). Higher overall scores (averaged) indicate greater levels of state self-compassion.
The Eating Disorder Examination – Questionnaire (EDE-Q) [44] is a 28-item measure of eating disorder cognitions and behaviours in the preceding 28 days. The measure consists of four subscales: Eating Concern, Restraint, Shape Concern and Weight Concern respectively. A global score is obtained by averaging the respondents’ subscale scores. Higher scores indicate greater levels of eating pathology, with a global score of 2.5 or greater indicating eating pathology [39].
The Shape Concern (concern about the body’s appearance) and Weight Concern (concern about the body’s measured weight) subscales are often utilised to assess body dissatisfaction. Concern has been raised regarding conceptual overlap between EDE-Q items that measure Weight Concern and WBIS items [45,46] (e.g., EDE-Q items: ‘Have you had a strong desire to lose weight?’, ‘Has your weight influenced how you think about (judge) yourself as a person?’, ‘How dissatisfied have you been with your weight?’ and WBIS items: ‘I wish I could drastically change my weight’, ‘My weight is a major way that I judge my value as a person’, ‘I am ok being the weight that I am’). As such, Weight Concern was not investigated as an outcome variable in the current study.
Participants were asked to provide their age, sex and ethnicity, and current weight (kilograms [kg]) and height (metres [m]) for calculation of BMI (weight [kg] / (height [m]2).
The study was advertised online via Sona Systems (used to host the student research experience program [REP]) and social media. Prospective participants received a link to the online survey which they could volunteer to complete via Qualtrics at their convenience. After reading the consent information statement, participants completed screening questions for the eligibility criteria, with those who did not meet criteria were directed out of the survey immediately. The remaining participants completed the measures, as ordered above, and one additional questionnaire for the larger study. Consent was implied by submission of a completed survey. As part of the larger study, eligible participants were required to complete a second survey three days later. Following completion of both surveys, REP participants were awarded course credit in exchange for their participation. There were no other incentives.
3. Results
3.1. Data Screening
All analyses were conducted using IBM SPSS Statistics. First, the data were examined for missing values. One case was missing a single value on the self-compassion measure, which was replaced using mean imputation. There were no other missing data. BMI and Eating Concern were positively skewed. No transformation was applied to BMI to preserve the original metric of the variable; however, square root transformation was effectively applied to Eating Concern. All other variables were normally distributed. Table 1 presents the raw means, standard deviations, bivariate correlations, and Cronbach’s alpha (see diagonal where applicable) for key study variables and potential covariates i.e., age and BMI. All scales displayed good internal consistency. Variables that failed to correlate significantly with the eating pathology outcomes at the bivariate level were excluded from subsequent multiple regression models.
3.2. Self-Compassion as a Moderator of the Relationship Between Thin-Ideal Internalisation and WBI and Eating Pathology
Moderated regression analysis was used to examine (1) the unique contribution of Thin-ideal Internalisation and WBI in the prediction of eating pathology, (2) the interaction of Thin-ideal internalisation and Self-compassion in the prediction of eating pathology, and (3) the interaction of WBI and Self-compassion in the prediction of eating pathology. Total scores for Thin-ideal Internalisation, WBI and Self-compassion were mean centred prior to analysis. Interaction terms were computed based on these mean-centred variables to prevent multicollinearity between the main effects and interaction effects [47]. Separate moderated regression analyses were conducted with Restraint, Eating Concern, and Shape Concern as outcomes. The general structure of the regression equation was the same for all models; however, where applicable, Age and BMI were controlled and entered at the first step, prior to entry of other predictors. The direction of significant interaction effects was examined using simple slope analysis.
3.2.1. Restraint
The regression model exploring predictors of Restraint included BMI at step one, Thin-ideal Internalisation, WBI, and Self-compassion at step two, and the two interaction terms (Thin-ideal Internalisation x Self-compassion, WBI x Self-compassion) at step three (see Table 2). R was significantly different from zero at the end of each step. After step three, with all predictors included in the regression model, R = .50, F (6, 468) = 26.27, p < .001. Thin-ideal Internalisation and WBI were significant, positive predictors of Restraint and the interaction between Thin-ideal Internalisation and Self-compassion was significant. The final model accounted for 24% of the variance in Restraint. Thin-ideal Internalisation was the strongest predictor of Restraint.
A plot of the interaction between Thin-ideal Internalisation and Self-compassion in the prediction of Restraint (Figure 1) showed that at low values of Thin-ideal Internalisation, there is little difference in the effect of low versus high values of Self-compassion on Restraint. However, at high values of Thin-ideal Internalisation, low values of Self-compassion exacerbate its effect on Restraint. Restraint is highest when Thin-ideal Internalisation is high and Self-compassion is low. Simple slope analysis revealed that the slope of the regression line for low Self-compassion was significantly different from zero, t (195) = 3.44, p = .001.
3.2.2. Eating Concern
The regression model exploring predictors of Eating Concern included Age and BMI at step one, Thin-ideal Internalisation, WBI and Self-compassion at step two, and the two interaction terms at step three (see Table 3). R was significantly different from zero at the end of each step. The addition of the interaction terms at Step 3 produced a significant change in R2 (p = .005). After step three, with all predictors included R = .72, F (7, 467) = 73.62, p < .001. Both Thin-ideal Internalisation and WBI contributed uniquely to prediction and were significant, positive predictors of Eating Concern. In addition, Self-compassion was a significant, negative predictor of Eating Concern and the interaction between WBI and Self-compassion was significant. Overall, the final model explained 52% of the variance in Eating Concern. WBI was the strongest predictor of Eating Concern.
A plot of the interaction between WBI and Self-compassion in the prediction of Eating Concern (Figure 2) indicated that at low values of WBI, there is little difference in the effect of low versus high values of Self-compassion on Eating Concern. However, at high values of WBI, low values of Self-compassion exacerbate its effect on Eating Concern. Thus, Eating Concern is highest when WBI is high and Self-compassion is low. Simple slope analysis revealed that the slope of the regression line for low Self-compassion was significantly different from zero, t (195) = 3.44, p = .001.
3.2.3. Shape Concern
The regression model for Shape Concern included Age and BMI at step one, thin-ideal internalisation, WBI and self-compassion at step two, and the two interaction terms at step three (see Table 4). R was significantly different from zero at the end of each step. After step three, with all predictors included R = .83, F (7, 467) = 147.41, p < .001. The addition of the interaction terms at step three did not produce a significant change in R2 and neither interaction term reached significance at the p<.05 level, indicating that there was no interaction between Thin-ideal Internalisation and Self-compassion or WBI and Self-compassion in the prediction of Shape Concern. In the final model, Age, WBI, and Thin-ideal Internalisation were significant, positive predictors of Shape Concern, each contributing uniquely to prediction. In addition, Self-compassion was a significant, negative predictor of Shape Concern. WBI was the strongest predictor of Shape Concern. Overall, the final model accounted for 69% of the variance in Shape Concern.
4. Discussion
It has long been posited that thin-ideal internalisation and WBI are important contributing factors to the development and maintenance of disordered eating [3,4,5], however these constructs have generally been examined separately within the literature. The current study sought to examine the unique contribution of both constructs in predicting restraint, eating concern, and shape concern to build a more comprehensive understanding of how the internalisation of different sociocultural ideals and beliefs about weight and shapes affects eating pathology. The study also aimed to explore the potential role of self-compassion in moderating the relationship between both forms of internalisation and eating disorder cognitions and behaviours. Findings from the current study suggest that inclusion of both thin-ideal internalisation and WBI in sociocultural models of eating pathology may lead to the development of more effective intervention strategies for reducing disordered eating. Additionally, findings support previous research [24,25,31] by revealing that lower self-compassion may exacerbate the effect of eating disorder risk factors on some outcomes. These findings lend further support to the utility of self-compassion therapy-based interventions for the reduction of disordered eating [36].
In line with previous studies [see e.g., 20, 22] the findings support consideration of thin-ideal internalisation and WBI as distinct but related theoretical constructs. Thin-ideal internalisation and WBI were moderately correlated and differed in their associations with BMI and restraint, eating concern and shape concern. Consistent with previous studies [see e.g., 20], BMI and thin-ideal internalisation were not correlated, while BMI and WBI were positively correlated. This is likely due to the demonstrated link between BMI and weight stigmatising experiences; individuals with higher BMI report more weight stigmatising experiences which in turn lead to higher internalisation of anti-fat attitudes and beliefs [3,48].
The current findings extend upon recent research on thin-ideal internalisation and WBI in the prediction of body dissatisfaction [20] by demonstrating their unique contribution to the prediction of a broader range of eating disorder cognitions and behaviours. Results indicated that, after controlling for BMI, both variables independently contributed to predicting restraint, eating concern and shape concern. While thin-ideal internalisation was the strongest predictor of restraint, WBI was the strongest predictor of both eating concern and shape concern. These findings suggest that inclusion of both thin-ideal internalisation and WBI in sociocultural models of body image and eating disturbance in future research is likely to improve conceptual understanding of eating disorder cognitions and behaviours and inform the development of more effective prevention and intervention programs.
The tripartite influence model [6] posits that sociocultural pressure to be thin results in thin-ideal internalisation, leading to body dissatisfaction and disordered eating. Expansion of this model to incorporate WBI includes consideration of sociocultural factors related to the development of WBI including anti-fat attitudes, negative obesity stereotypes, and weight-related discrimination, which may come from a range of sources [3,48]. Therefore, the model could be extended to include both sociocultural pressures to be thin and sociocultural stigmatisation of overweight/obesity as antecedents of thin-ideal internalisation and/or WBI, which then contribute to body dissatisfaction [see 20] and disordered eating. Further research is needed to examine whether pressure to be thin is positively related to WBI and whether weight stigmatising experiences are positively related to thin-ideal internalisation so that sociocultural models of eating disorders can be expanded and integrated to include pathways between constructs from both the thin-ideal internalisation and weight stigma literature.
As expected, based on past research [33,35], self-compassion was negatively correlated with both thin-ideal internalisation and WBI, such that individuals with higher self-compassion reported lower thin-ideal and weight bias internalisation. Congruent with previous findings [24,25,31], self-compassion was also a negative predictor of eating disorder cognitions. However, self-compassion did not predict restraint after accounting for thin-ideal internalisation and WBI. It may be that fear of self-compassion (e.g., weakness, loss of control) rather than self-compassion per se is a stronger predictor of restrained eating [see e.g., 49]
In terms of the moderating role of self-compassion in the relationship between the internalisation constructs and restraint, eating concern and shape concern, the results differed across outcome variables. Self-compassion moderated the effect of thin-ideal internalisation, but not WBI, on restraint. In contrast, self-compassion moderated the effect of WBI but not thin-ideal internalisation on eating concern. Notably, thin-ideal internalisation and WBI were the strongest predictors of restraint and eating concern respectively. These stronger predictors may be more sensitive to variability in vulnerability/resistance factors. For individuals with lower levels of self-compassion (i.e., critical, judgemental and emotionally unforgiving), there was a stronger association between thin-ideal internalisation and restraint, and weight bias and eating concern. In contrast, those with higher levels of self-compassion appeared to be protected from the effects of these sociocultural influences. This is consistent with previous research citing the protective role of self-compassion in eating pathology [24,25,31] and reinforces the utility of strengthening self-compassion within eating disorder interventions [36].
Finally, self-compassion did not moderate the relationship between thin-ideal internalisation or WBI and shape concern, however the main effects explained a higher proportion of the total variance for this outcome. While previous research has demonstrated that self-compassion is negatively correlated with thin-ideal internalisation and WBI [33,35], the current results suggest that when individuals have already internalised these body ideals/beliefs, self-compassion does not buffer their effects on shape concern even if it buffers their effects on related eating pathology. Notably, of the three EDE-Q subscales examined, shape concern showed the highest average score suggesting that is was more of a concern than restraint or eating concern in this (non-clinical) sample.
Results of the current study should be interpreted in the context of study limitations. Firstly, participants were predominantly female university students identifying as Australian/Caucasian and with little variability in age. Due to the lack of representation of various gender, socioeconomic and ethnic groups within this study, the generalisability of the findings may be limited and examination of expanded sociocultural models of disordered eating in more diverse populations is warranted in future research. Also, among the sample utilised for the current study, there were generally low rates of eating pathology reported, with low mean scores for some EDE-Q subscales, particularly restraint. It would be beneficial to replicate this study with populations displaying greater levels of eating pathology (e.g., clinical populations) to understand whether the current findings are generalisable to these groups. A further limitation of this study was the cross-sectional design, resulting in an inability to draw causal conclusions regarding the relationships among variables. Future longitudinal research could examine the causal pathways between thin-ideal internalisation, WBI, self-compassion and eating disorder cognitions and behaviours to more effectively inform prevention and intervention programs. Future research may also consider mediated pathways from the sociocultural influences to disordered eating via self-compassion. For example, it is possible that WBI decreases self-compassion which in turn increases eating disorder cognitions and behaviours. The belief that one is less attractive or less deserving due to their weight [41] is inconsistent with the self-compassionate stance of kindness and nonjudgement [27].
The results of the current study have implications for future research and practice related to the prevention and treatment of disordered eating. As discussed, the results support the inclusion of WBI alongside thin-ideal internalisation in current sociocultural models of disordered eating, providing evidence for the unique contribution of each construct to eating pathology. Further research is required to determine intersecting pathways between other constructs in thin ideal and weight stigma models (e.g., weight stigmatising experiences to thin-ideal internalisation, and sociocultural pressures to be thin to WBI) and the generalisability of extended models to more diverse and clinical samples.
Expansion of sociocultural models of eating disorders, in turn, suggests an extension of current intervention strategies aimed at targeting the sociocultural factors associated with disordered eating. For example, interventions such as the Body Project, which utilise dissonance-based strategies to reduce thin-ideal internalisation may be adapted to include additional components targeting the reduction of WBI. Previous research has demonstrated the effective adaptation of dissonance-based strategies utilised in the Body Project in targeting drive for muscularity in men [19], suggesting that these strategies can be adapted to address various forms of body image internalisation. It is likely that adapting this intervention to target both thin-ideal internalisation and WBI will increase the efficacy of the intervention in reducing disordered eating. It is expected that the adaptation of interventions to address both thin-ideal internalisation and WBI may be particularly effective in increasing the efficacy of interventions for individuals with higher BMI, given the significant correlation between BMI and WBI [20,22] which was also observed in the current study. Further research may also investigate the impact of interventions that address both forms of internalisation across BMI categories
5. Conclusions
In conclusion, the current study highlights the complementary nature of the thin-ideal internalisation and weight bias internalisation by demonstrating that including both sociocultural constructs in predictive models provides a more comprehensive understanding of eating disorder cognitions and behaviours. In addition, the findings suggest that self-compassion may buffer the effects of thin-ideal internalisation on restraint and weight bias internalisation on eating concern. Future research should expand sociocultural models of body image and eating disturbance to include both forms of internalisation to improve theoretical understanding and predictive accuracy and inform future interventions.
Author Contributions
Conceptualization – Developing research ideas and goals: Sharon Grant (S.G), Gillian Montague (G.M); Methodology – Designing research methods and models: S.G, G.M; Software – Writing and implementing code: N/A; Validation – Ensuring reproducibility and accuracy: G.M; Formal analysis – Applying statistical or computational techniques: G.M; Investigation – Conducting experiments or data collection: G.M, Tabi Eidipour (T.E); Resources – Providing materials, tools, or funding: N/A; Data curation – Managing and maintaining research data: G.M, T.E, S.G; Writing – Original Draft – Creating the initial manuscript: G.M; Writing – Review & Editing – Revising and refining the manuscript: S.G; Visualization – Creating figures, tables, or data presentations: G.M; Supervision – Overseeing research activities and mentoring: S.G; Project administration – Managing research projects: G.M, T.E; Funding acquisition – Securing financial support: N/A. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (Human Research Ethics Committee) of Swinburne University of Technology (protocol code 20247230-18174 and date of approval 26/03/2024).”
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author due to conditions of ethical approval.
Acknowledgments
Thank you to Lachlan Poznanski for repeating the analyses with the larger (full) data set reported herein.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BMI WBI |
Body mass index Weight bias internalisation |
References
- Galmiche, M.; Déchelotte, P.; Lambert, G.; Tavolacci, M. P. Prevalence of eating disorders over the 2000–2018 period: a systematic literature review. American Journal of Clinical Nutrition 2019, 109((5)), 1402–1413. [Google Scholar] [CrossRef]
- Access Economics, Deloitte. Paying the price, second edition: The economic and social impact of eating disorders in Australia; 2024; Available online: https://butterfly.org.au/wp-content/uploads/2024/02/Paying-the-Price_Second-Edition_2024_FINAL.pdf.
- Romano, K. A.; Heron, K. E.; Henson, J. M. Examining associations among weight stigma, weight bias I ternalization, body dissatisfaction, and eating disorder symptoms: Does weight status matter? Body Image 2021, 37, 38–49. [Google Scholar] [CrossRef]
- Schvey, N. A.; White, M. A. The internalization of weight bias is associated with severe eating pathology among lean individuals. Eating Behaviors 2015, 17, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Thompson, J. K.; Stice, E. Thin-ideal internalization: Mounting evidence for a new risk factor for body-image disturbance and eating pathology. Current Directions in Psychological Science 2001, 10((5)), 181–183. [Google Scholar] [CrossRef]
- Thompson, J. K.; Heinberg, L. J.; Altabe, M.; Tantleff-Dunn, F. Exacting beauty: theory, assessment, and treatment of body image disturbance, 1st ed.; American Psychological Association, 1999. [Google Scholar]
- Crandall, C. S. Prejudice against fat people: Ideology and self-interest. Journal of Personality and Social Psychology 1994, 66((5)), 882–894. [Google Scholar] [CrossRef] [PubMed]
- Puhl, R. M.; Heuer, C. A. The stigma of obesity: A review and update. Obesity 2009, 17((5)), 941–964. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, B.; de la Piedad Garcia, X.; Kite, J.; Hill, B.; Cooper, K.; Flint, S. Weight stigma in Australia: a public health call to action. Public Health Research & Practice 32(3) 2022. [Google Scholar] [CrossRef]
- Puhl, R. M.; Lessard, L. M.; Pearl, R. L.; Himmelstein, M. S.; Foster, G. D. International comparisons of weight stigma: Addressing a void in the field. International Journal of Obesity 2021, 45((9)), 1976–1985. [Google Scholar] [CrossRef]
- Pearl, R. L.; Puhl, R. M. Weight bias internalization and health: a systematic review. Obesity Reviews 2018, 19((8)), 1141–1163. [Google Scholar] [CrossRef]
- Stice, E. Review of the evidence for a sociocultural model of bulimia nervosa and an exploration of the mechanisms of action. Clinical Psychology Review 1994, 14((7)), 633–661. [Google Scholar] [CrossRef]
- Grabe, S.; Ward, L. M.; Hyde, J. S. The role of the media in body image concerns among women: A meta-analysis of experimental and correlational studies. Psychological Bulletin 2008, 134((3)), 460–476. [Google Scholar] [CrossRef]
- Culbert, K. M.; Racine, S. E.; Klump, K. L. Research review: What we have learned about the causes of eating disorders-a synthesis of sociocultural, psychological, and biological research. Journal of Child Psychology and Psychiatry 2015, 56((11)), 1141–1164. [Google Scholar] [CrossRef]
- Stice, E. Interactive and mediational etiologic models of eating disorder onset: Evidence from prospective studies. Annual Review of Clinical Psychology 2016, 12((1)), 359–381. [Google Scholar] [CrossRef]
- Stice, E.; Marti, C. N.; Shaw, H.; Rohde, P. Meta-analytic review of dissonance-based eating disorder prevention programs: Intervention, participant, and facilitator features that predict larger effects. Clinical Psychology Review 2019, 70, 91–107. [Google Scholar] [CrossRef] [PubMed]
- Stice, E.; Mazotti, L.; Weibel, D.; Agras, W. S. Dissonance prevention program decreases thin-ideal internalization, body dissatisfaction, dieting, negative affect, and bulimic symptoms: A preliminary experiment. International Journal of Eating Disorders 2000, 27((2)), 206–217. [Google Scholar] [CrossRef]
- Stice, E.; Shaw, H.; Burton, E.; Wade, E. Dissonance and healthy weight eating disorder prevention programs: A randomized efficacy trial. Journal of Consulting and Clinical Psychology 2006, 74((2)), 263–275. [Google Scholar] [CrossRef] [PubMed]
- Hendricks, E.; Jenkinson, E.; Falconer, L.; Griffiths, C. How effective are psychosocial interventions at improving body image and reducing disordered eating in adult men? A systematic review. Body Image 2023, 47, 101612–101612. [Google Scholar] [CrossRef]
- Harris, E. R. Understanding the relative contributions of internalised weight stigma and thin ideal internalisation on body dissatisfaction across body mass index. Master's thesis, Ohio University, 2023. OhioLINK. chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/https://etd.ohiolink.edu/acprod/odb_etd/ws/send_file/send?accession=ohiou168259303369045&disposition=inline. [Google Scholar]
- Levinson, J. A.; Kinkel-Ram, S.; Myers, B.; Hunger, J. M. A systematic review of weight stigma and disordered eating cognitions and behaviors. Body Image 2024, 48, 101678–101678. [Google Scholar] [CrossRef]
- Nutter, S.; Russell-Mayhew, S.; Saunders, J. F. Towards a sociocultural model of weight stigma. Eating and Weight Disorders 2021, 26((3)), 999–1005. [Google Scholar] [CrossRef]
- Morton, C.; Mooney, T. A.; Lozano, L. L.; Adams, E. A.; Makriyianis, H. M.; Liss, M. Psychological inflexibility moderates the relationship between thin-ideal internalization and disordered eating. Eating Behaviors 2020, 36, 101345–101345. [Google Scholar] [CrossRef]
- Braun, T. D.; Park, C. L.; Gorin, A. Self-compassion, body image, and disordered eating: A review of the literature. Body Image 2016, 17, 117–131. [Google Scholar] [CrossRef] [PubMed]
- Kelly, A. C.; Vimalakanthan, K.; Carter, J. C. Understanding the roles of self-esteem, self-compassion, and fear of self-compassion in eating disorder pathology: An examination of female students and eating disorder patients. Eating Behaviors 2014, 15((3)), 388–391. [Google Scholar] [CrossRef] [PubMed]
- Wasylkiw, L.; MacKinnon, A. L.; MacLellan, A. M. Exploring the link between self-compassion and body image in university women. Body Image 2012, 9((2)), 236–245. [Google Scholar] [CrossRef]
- Neff, K. Self-Compassion: An alternative conceptualization of a healthy attitude toward oneself. Self and Identity 2003, 2((2)), 85–101. [Google Scholar] [CrossRef]
- Neff, K. D. Self-Compassion: Theory, method, research, and intervention. Annual Review of Psychology 2023, 74((1)), 193–218. [Google Scholar] [CrossRef]
- MacBeth, A.; Gumley, A. Exploring compassion: A meta-analysis of the association between self-compassion and psychopathology. Clinical Psychology Review 2012, 32((6)), 545–552. [Google Scholar] [CrossRef] [PubMed]
- Neff, K. D.; Rude, S. S.; Kirkpatrick, K. L. An examination of self-compassion in relation to positive psychological functioning and personality traits. Journal of Research in Personality 2007, 41((4)), 908–916. [Google Scholar] [CrossRef]
- Linardon, J. Positive body image, intuitive eating, and self-compassion protect against the onset of the core symptoms of eating disorders: A prospective study. International Journal of Eating Disorders 2021, 54((11)), 1967–1977. [Google Scholar] [CrossRef] [PubMed]
- Webb, J. B.; Forman, M. J. Evaluating the indirect effect of self-compassion on binge eating severity through cognitive–affective self-regulatory pathways. Eating Behaviors 2013, 14((2)), 224–228. [Google Scholar] [CrossRef]
- Fekete, E. M.; Herndier, R. E.; Sander, A. C. Self-compassion, internalized weight stigma, psychological well-being, and eating behaviors in women. Mindfulness 2021, 12((5)), 1262–1271. [Google Scholar] [CrossRef]
- Gobin, K. C.; McComb, S. E.; Mills, J. S. Testing a self-compassion micro-intervention before appearance-based social media use: Implications for body image. Body Image 2022, 40, 200–206. [Google Scholar] [CrossRef]
- Tylka, T. L.; Russell, H. L.; Neal, A. A. Self-compassion as a moderator of thinness-related pressures' associations with thin-ideal internalization and disordered eating. Eating Behaviors 2015, 17, 23–26. [Google Scholar] [CrossRef] [PubMed]
- Turk, F.; Waller, G. Is self-compassion relevant to the pathology and treatment of eating and body image concerns? A systematic review and meta-analysis. Clinical Psychology Review 2020, 79, 101856–101856. [Google Scholar] [CrossRef]
- Hopkins, C. M. Reduction of internalized weight bias via mindful self-compassion: Theoretical framework and results from a randomized controlled trial. Doctoral thesis, Duke University, 2022. ProQuest Dissertations Publishing. [Google Scholar]
- World Health Organisation. A healthy lifestyle-WHO recommendations. WHO. 6 May 2010. Available online: https://www.who.int/europe/news-room/fact-sheets/item/a-healthy-lifestyle---who-recommendations.
- Rø; Reas, D. L.; Stedal, K. Eating disorder examination questionnaire (EDE-Q) in Norwegian adults: Discrimination between female controls and eating disorder patients. European Eating Disorders Review 2015, 23((5)), 408–412. [Google Scholar] [CrossRef] [PubMed]
- Schaefer, L. M.; Harriger, J. A.; Heinberg, L. J.; Soderberg, T.; Kevin Thompson, J. Development and validation of the sociocultural attitudes towards appearance questionnaire-4-revised (SATAQ-4R). International Journal of Eating Disorders 2017, 50((2)), 104–117. [Google Scholar] [CrossRef]
- Pearl, R. L.; Puhl, R. M. Measuring internalized weight attitudes across body weight categories: Validation of the modified weight bias internalization scale. Body Image 2014, 11((1)), 89–92. [Google Scholar] [CrossRef] [PubMed]
- Durso, L. E.; Latner, J. D. Understanding self-directed stigma: Development of the weight bias internalization scale. Obesity 2008, 16((S2)), S80–S86. [Google Scholar] [CrossRef]
- Neff, K. D.; Tóth-Király, I.; Knox, M. C.; Kuchar, A.; Davidson, O. The development and validation of the state self-compassion scale (long-and short form). Mindfulness 2021, 12((1)), 121–140. [Google Scholar] [CrossRef]
- Fairburn, C. G.; Belgin, S. Eating disorder examination questionnaire (EDE-Q 6.0). In Cognitive behavior therapy and eating disorders; Guilford Press, 2008; pp. 303–313. [Google Scholar]
- Romano, K. A.; Heron, K. E.; Sandoval, C. M.; Howard, L. M.; MacIntyre, R. I.; Mason, T. B. A meta-analysis of associations between weight bias internalization and conceptually-related correlates: A step towards improving construct validity. Clinical Psychology Review 2022, 92, 102127–102127. [Google Scholar] [CrossRef]
- Saunders, J. F.; Nutter, S.; Russell-Mayhew, S. Examining the conceptual and measurement overlap of body dissatisfaction and internalized weight stigma in predominantly female samples: A meta-analysis and measurement refinement study. Frontiers in Global Women's Health 2022, 3, 877554–877554. [Google Scholar] [CrossRef]
- Cohen, J. Applied multiple regression/correlation analysis for the behavioral sciences, 3rd edition ed.; L. Erlbaum Associates, 2003. [Google Scholar]
- O'Brien, K. S.; Latner, J. D.; Puhl, R. M.; Vartanian, L. R.; Giles, C.; Griva, K.; Carter, A. The relationship between weight stigma and eating behavior is explained by weight bias internalization and psychological distress. Appetite 2016, 102, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Geller, J.; Samson, L.; Maiolino, N.; et al. Self-compassion and its barriers: predicting outcomes from inpatient and residential eating disorders treatment. Journal of Eating Disorders 2022, 10, 114. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Two-way interaction between thin-ideal internalisation and self-compassion in the prediction of restraint.
Figure 1.
Two-way interaction between thin-ideal internalisation and self-compassion in the prediction of restraint.
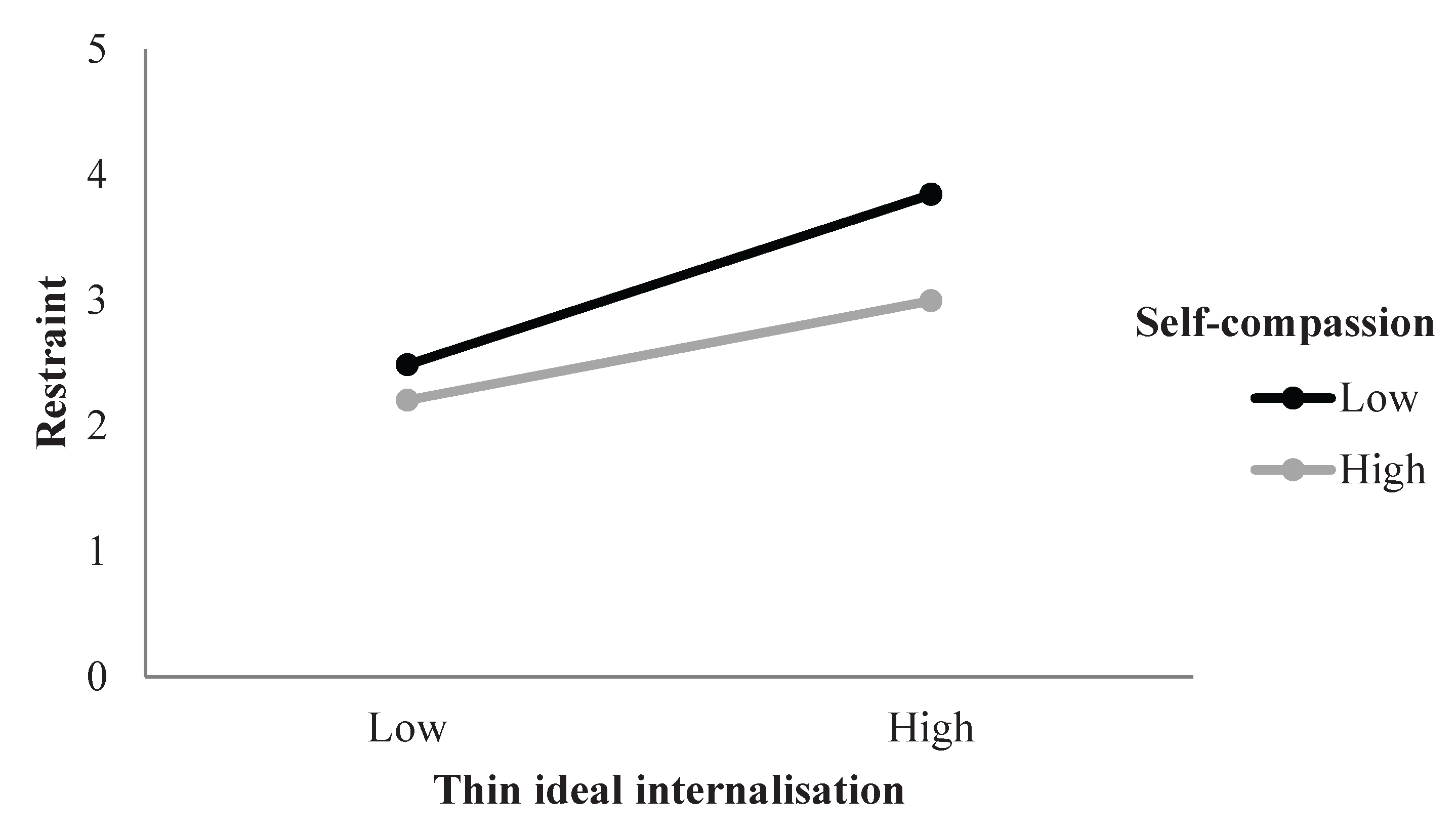
Figure 2.
Two-way interaction between WBI and self-compassion in the prediction of eating concern.
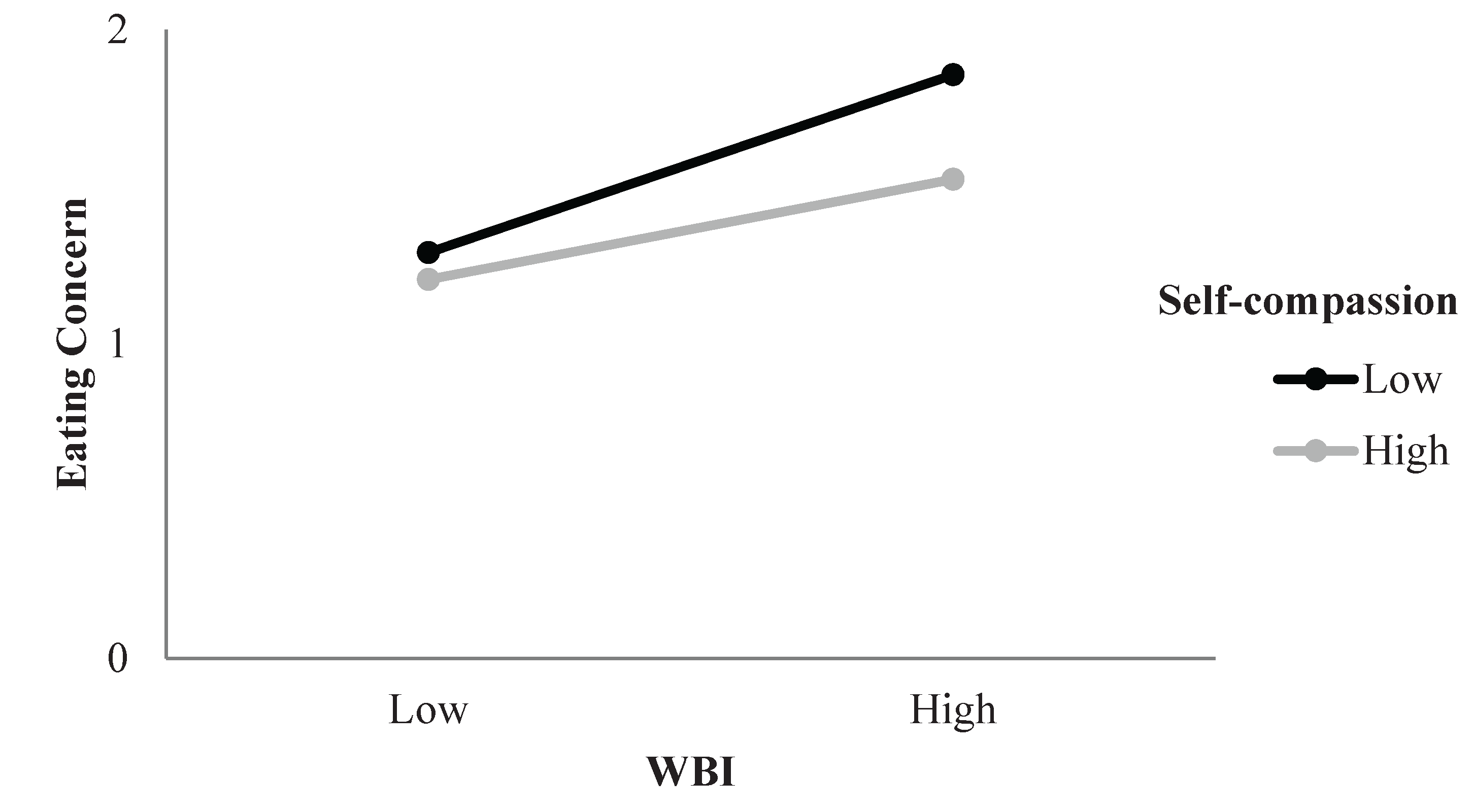

Table 1.
Descriptive statistics and correlations.
| Mean | SD | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Age | 31.48 | 10.62 | - | |||||||
| 2 | BMI | 26.66 | 7.14 | .24 | - | ||||||
| 3 | Self-compassion | 3.11 | 0.71 | .21 | -.09 | 0.92 | |||||
| 4 | WBIS | 3.95 | 1.51 | -.13 | .41 | -.54 | 0.94 | ||||
| 5 | Thin-ideal Internalisation | 3.22 | 0.92 | -.28 | -.05 | -.35 | .54 | 0.82 | |||
| 6 | Restraint | 2.92 | 1.67 | 0.01 | .09 | -.28 | .43 | .43 | 0.84 | ||
| 7 | Eating Concern | 1.50 | 0.44 | -.21 | .13 | -.50 | .67 | .53 | .60 | 0.83 | |
| 8 | Shape Concern | 4.04 | 1.71 | -.10* | .30 | -.52 | .81 | .57 | .59 | .78 | 0.91 |
Notes. N = 475; Cronbach’s alpha coefficients are presented on the diagonal. Significant correlations are shown in bold |r| = .09 are significant at p < .05; |r| = .13 are significant at p < .01; |r| = .24 are significant at p < .001.
Table 2.
Hierarchical regression of thin-ideal internalisation, WBIS, self-compassion, ‘thin-ideal internalisation x self-compassion’ and ‘WBIS x self-compassion’ on restraint.
Table 2.
Hierarchical regression of thin-ideal internalisation, WBIS, self-compassion, ‘thin-ideal internalisation x self-compassion’ and ‘WBIS x self-compassion’ on restraint.
| Step | Variable | R2 | Adjusted R2 | R2 Change | B | β | sr2 |
|---|---|---|---|---|---|---|---|
| 1 | BMI | 0.01 | 0.01 | 0.01 | 0.02 | 0.09 | 0.01 |
| 2 | BMI | 0.24 | 0.24 | 0.24 | 0.000 | -0.00 | 0.00 |
| Self-compassion | -0.12 | -0.05 | 0.00 | ||||
| Thin-ideal Internalisation | 0.50*** | 0.28*** | 0.05*** | ||||
| WBI | 0.28*** | 0.25*** | 0.03*** | ||||
| 3 | BMI | 0.25 | 0.24 | 0.01 | 0.00 | 0.01 | 0.00 |
| Self-compassion | -0.14 | -0.06 | 0.00 | ||||
| Thin-ideal internalization | 0.50*** | 0.28*** | 0.05*** | ||||
| WBI | 0.27*** | 0.24*** | 0.02*** | ||||
| Thin-ideal internalisation x Self-compassion | -0.27* | -0.11* | 0.01* | ||||
| WBI x Self-compassion | 0.040 | 0.028 | 0.001 |
*p<.05, ***p<.001.
Table 3.
Hierarchical regression of thin-ideal internalisation, WBI, self-compassion, ‘thin-ideal internalisation x self-compassion’ and ‘WBIS x self-compassion’ on eating concern.
Table 3.
Hierarchical regression of thin-ideal internalisation, WBI, self-compassion, ‘thin-ideal internalisation x self-compassion’ and ‘WBIS x self-compassion’ on eating concern.
| Step | Variables | R2 | Adjusted R2 | R2 Change | B | β | sr2 |
|---|---|---|---|---|---|---|---|
| 1 | BMI | 0.08 | 0.07 | 0.08 | 0.01*** | 0.19*** | 0.03*** |
| Age | -0.01*** | -0.25*** | 0.06*** | ||||
| 2 | BMI | 0.51 | 0.51 | 0.44 | -0.005 | -0.08 | 0.00 |
| Age | -0.00 | -0.04 | 0.00 | ||||
| Self-compassion | -0.10*** | -0.16*** | 0.02*** | ||||
| Thin-ideal internalisation | 0.09*** | 0.19*** | 0.02*** | ||||
| WBI | 0.15*** | 0.51*** | 0.11*** | ||||
| 3 | BMI | 0.53 | 0.52 | 0.01 | -0.01 | -0.08 | 0.00 |
| Age | -0.00 | -0.03 | 0.00 | ||||
| Self-compassion | -0.11*** | -0.18*** | 0.02*** | ||||
| Thin-ideal internalisation | 0.09*** | 0.18*** | 0.02*** | ||||
| WBI | 0.15*** | 0.50*** | 0.10*** | ||||
| Thin-ideal internalisation x Self-compassion | 0.00 | 0.00 | 0.00 | ||||
| WBI x Self-compassion | -0.04** | -0.11** | 0.01** |
**p<.01, ***p<.001.
Table 4.
Hierarchical regression of WBIS, thin-ideal internalisation, self-compassion, ‘WBIS x self-compassion’ and ‘thin-ideal internalisation x self-compassion’ on shape concern.
Table 4.
Hierarchical regression of WBIS, thin-ideal internalisation, self-compassion, ‘WBIS x self-compassion’ and ‘thin-ideal internalisation x self-compassion’ on shape concern.
| Step | Variables | R2 | Adjusted R2 | R2 Change | B | Β | sr2 |
|---|---|---|---|---|---|---|---|
| 1 | BMI | 0.12 | 0.12 | 0.12 | 0.08*** | 0.34*** | 0.11*** |
| Age | -0.03*** | -0.18*** | 0.03*** | ||||
| 2 | BMI | 0.69 | 0.69 | 0.57 | 0.01 | 0.03 | 0.00 |
| Age | 0.01* | 0.06* | 0.00* | ||||
| Self-compassion | -0.27*** | -0.11*** | 0.01*** | ||||
| Thin-ideal internalisation | 0.41*** | 0.22*** | 0.03*** | ||||
| WBI | 0.70*** | 0.62*** | 0.16*** | ||||
| 3 | BMI | 0.69 | 0.68 | 0.00 | 0.01 | 0.03 | 0.00 |
| Age | 0.01* | 0.06* | 0.00* | ||||
| Self-compassion | -0.27*** | -0.11*** | 0.01*** | ||||
| Thin-ideal internalisation | 0.41*** | 0.22*** | 0.03*** | ||||
| WBI | 0.70*** | 0.62*** | 0.16*** | ||||
| Thin-ideal internalisation x Self-compassion | 0.05 | 0.02 | 0.00 | ||||
| WBI x Self-compassion | -0.02 | -0.02 | 0.00 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



