
Submitted:
24 June 2025
Posted:
25 June 2025
You are already at the latest version
Abstract
. Background: Frailty syndrome significantly worsens the prognosis of elderly people. An integral part of aging is sarcopenia and malnutrition. There is a lack of knowledge about the overlap of these states, as well as diagnostic methods and treatment. Methods: 170 patients >65 years were assessed for frailty using the Fried frailty scale. The risk of sarcopenia was measured using the SARC-F scale, and the risk of malnutrition was measured using the Mini Nutritional Assessment (MNA) scale. Serum albumin, protein, and fibrinogen levels were measured. Fat-free body mass and respiratory parameters were measured: peak expiratory flow (PEF) and forced expiratory volume- one second (FEV1). Results: 53 patients were classified as robust (31%), 96 as prefrail (57%), and 21 as frail (12%). Frail patients had significantly reduced serum albumin and increased fibrinogen compared to the pre-frail and robust groups (p<0.05). 38% of frail patients are at risk of sarcopenia, and 52% are at risk of malnutrition. Frail patients have lower PEF and FEV1 values. The decrease in respiratory parameters correlates with fat-free body mass and muscle strength. Conclusions: Patients with frailty are the group at most significant risk of malnutrition and sarcopenia compared to their healthy peers and patients in the prefrail stage. MNA and SARC-F scales combined with routine screening of elderly patients with frailty may allow for effective identification of patients at risk of malnutrition and sarcopenia.
Keywords:
frailty
; malnutrition
; sarcopenia
; elderly
; biomarkers
; Mini Nutritional Assessment
; SARC-F
1. Introduction
Frailty syndrome is defined as a decrease in the body's reserves and a simultaneous increase in susceptibility to endogenous and exogenous stress factors [1]. The importance of frailty is increasing with the global aging of the population. At the same time, risk factors for developing frailty include a wide range of sociodemographic, clinical, lifestyle-related, and biological factors [2]. Moreover, frailty is not simply aging, but a progressive process that worsens quality of life, functionality, and increases overall risk [3]. Patients defined as frail have a significantly increased risk of falls, bone fractures, disability, dementia, hospitalization, and death compared to their healthy peers [4].
An essential aspect of developing knowledge about frailty syndrome is the search for its biomarkers. Many candidates have been described so far, among metabolic, hematological, and immunological molecules [5], including tumor necrosis factor alpha, interleukin 6 [5], C-reactive protein, hemoglobin, free testosterone, and 25-hydroxyvitamin D [6]. Due to the multifaceted nature of frailty, identifying reliable biomarkers poses a significant challenge. However, to better understand the pathophysiology of frailty and find targets for potential treatment, finding biomolecules associated with frailty seems to be one of the most critical goals in modern geriatrics.
The integral elements coexisting with frailty syndrome are sarcopenia and malnutrition [7], which, together with cachexia, are defined as symptoms of tissue loss. It is suggested that up to ⅔ of elderly patients suffer from at least one of these syndromes. [8]. In addition, the overlap of these three catabolic states is frequently observed [9]. Sarcopenia is one of the common elements of aging, but its severity is further exacerbated in frailty. Additionally, it is not routinely diagnosed in everyday practice, although it significantly increases the risk of falls and disability in elderly patients. [10].
Sarcopenia and poor nutritional status complement each other in the frail elderly patient phenotype. Better nutritional status correlates with better performance in elderly patients [11]. Moreover, malnutrition increases the level of multimorbidity [12].
Implementing an interdisciplinary approach and a broad assessment of elderly patients is widely advocated. One of the basic tools in evaluating malnutrition is the Mini Nutritional Assessment (MNA) scale, created in the 1990s. It is based on a questionnaire with a maximum of 30 points. Patients who score less than 24 points are classified as at risk of malnutrition, and those who score less than 17 points are classified as malnourished. A shortened form of the scale, MNA-SF, is also in use. Despite the passage of time, the MNA scale remains a simple and effective screening tool in the elderly patient population [13]. The SARC-F scale is also a quick tool designed to determine the risk of sarcopenia. It is based on five questions about: strength, assistance with walking, rising from a chair, climbing stairs, and falls. The maximum score is 10, and a score above 4 points is considered to be the basis for determining the risk of sarcopenia [14].
In recent years, knowledge and awareness of frailty have improved significantly. Scales for rapid diagnosis of frailty have been enhanced, and risk assessment scales have been created. Moreover, it has been demonstrated that it is possible to prevent frailty and inhibit its development effectively [15]. However, the pathophysiological mechanisms of frailty and its causative factors have not yet been fully elucidated. There is also no consensus on how to manage frail and pre-frail patients. A notable knowledge gap concerns the relationship between frailty, malnutrition, and sarcopenia.
Cardiovascular diseases are the leading cause of mortality worldwide. They mainly affect elderly patients. On the other hand, frailty causes the progression of existing cardiovascular diseases. For this reason, studying frailty in cardiology patient cohorts is crucial [15,16]. A special group of patients is those burdened with coronary artery disease (CAD). Patients with CAD and frailty have a significantly reduced quality of life, and properly implemented treatment improves their functionality. At the same time, patients with CAD are often excluded from studies on new treatment methods [17]; therefore, understanding the overlap between CAD and frailty seems to be a priority.
Considering all these questions, it was decided to examine a cohort of elderly CAD patients for frailty. The MNA and SARC-F questionnaire scales were used to assess the overlap of sarcopenia and malnutrition syndromes and their effectiveness in evaluating elderly patients. The concentration of potential biomarkers was also analyzed: albumin, total protein, and fibrinogen as biomarkers of the body's protein metabolism. To analyze the phenomenon of respiratory sarcopenia, the thickness of the diaphragm and respiratory parameters were measured: peak expiratory flow (PEF) and forced expiratory volume-one second (FEV1).
2. Materials and Methods
The study included 270 patients hospitalized between 2022 and 2024 in the 2nd Clinical Department of Cardiology in Zabrze, Poland. This is an ancillary analysis of the FRAPICA study (ClinicalTrials.org NCT03209414) [18]. The inclusion criteria for the study included age > 65 years, informed consent to participate in the project, and angiographically confirmed coronary artery disease. During hospitalization, the severity of frailty syndrome was assessed using the Linda Fried scale and the Clinical Frailty Scale.
The degree of frailty was diagnosed using the Frailty Phenotype Score [1] using the following criteria:
- Slowness—reduced gait speed at a distance of 5m at usual pace. The patient must repeat 3 times, and the results are averaged. If a patient walks for >6 seconds, the criterion is positive.
- Weakness is assessed with a maximal handgrip strength test. It is carried out in the dominant arm. We use the electronic hand dynamometer EH101 (VETEK AB, Sweden). A patient must repeat the test three times, and the maximal value is recorded. The test is positive for frailty when strength is lower than 20 kg for women and 30 kg for men.
- The Minnesota Leisure Time Activity questionnaire assesses low physical activity. The result is positive when calorie expenditure per week is lower than 270 kcal/week in women and <383 kcal/week in men. We have prepared a Microsoft Excel-based template for rapid questioning and easy calculation of all activities and respective calorie expenditure. We are assessing physical activity over the past 12 months.
- Exhaustion self-reported by a patient. It is evaluated by answering two questions from the Center for Epidemiologic Studies Depression Scale Revised (CESD-R) scale. The patient must answer the following questions: “How often did you feel like everything you did was an effort in the past week? How often did you feel you could not get going in the past week?” The possible answers are often (≥3 days) or not, when the feeling is present in 0 to 2 days. A positive answer is when the patient says “often.”
- Weight loss exceeding 10 pounds (approximately 4.5 kg) unintentionally in the past year.
We recognize frailty if ≥3 out of 5 criteria are met. Patients in whom 1 or 2 criteria are present are assigned as pre-frail. Patients who did not meet any of the criteria are marked as robust.
Each patient had a blood sample taken, and the total protein, albumin, and fibrinogen concentration was determined in the hospital laboratory. Additionally, information on comorbidities, weight, height, and Body Mass Index (BMI) was collected from medical records. Fat-free body mass (FFBM) was assessed using Harpenden’s skinfold caliper and Baty’s body assessment software v. 17 (Baty International Ltd., Burgess Hill, UK). Respiratory parameters: peak expiratory flow (PEF) and forced expiratory volume in one second (FEV1) were measured using an Asmaplan 1 peakflowmeter (Vitalograph, Ireland). Additionally, diaphragm thickness was measured with ultrasound [19]. During hospitalization, each patient was assessed based on the SARC-F questionnaires and the full version of the MNA scale. The following scales were used to determine patients: Instrumental Activities of Daily Living (IADL) and Clinical Frailty Scale (CFS).
Data were analyzed for normality of distribution and equality of variances. Quantitative data were presented as means and standard deviations, and qualitative data were presented as numbers and percentages. Analysis of variance was used to compare groups, and in case of significant differences in subgroups, the Student's t test was used. A p-value below 0.05 was considered statistically significant. The analysis was performed using the Statistica 13.3 program (Tibco, licensed for the Silesian Medical University).
3. Results
3.1. Demographic and Medical Data
The mean age of the recruited patients was 73.8 years. Of the 170 patients recruited to the study, 53 were classified as robust (31%), 96 as prefrail (57%), and 21 as frail (12%). The groups: robust, pre-frail, and frail, were homogeneous regarding gender. The majority of patients recruited to the study were men (66%). No statistically significant differences in the age of patients were observed between the individual groups (p>0.05). For the separate groups (robust, non-frail, and frail), statistically significant differences were observed in height (p<0.05), but not weight, fat-free body mass (FFBM), and body mass index (BMI) (p>0.05). Patients did not differ in terms of diaphragm thickness. The most significant percentage of patients were patients with hypertension (82%) and hypercholesterolemia (74%). Patients with frailty syndrome show significantly lower values of respiratory parameters: PEF and FEV1, than patients in the robust and pre-frail stages. Demographic and medical data of patients are presented in Table 1.
3.2. Potential Biomarkers Concentration
Among the studied groups, a statistically significant difference was observed in albumin concentrations, with the lowest values in patients diagnosed with frailty (p<0.05). Regarding total protein concentrations, the groups did not differ from each other (p>0.05). Statistical significance was also noted for fibrinogen concentrations, with the highest value for frail patients (Table 2 and Figure 1). Multiple comparisons of p-values analysis showed no differences in albumin and fibrinogen values between the robust and pre-frail groups, i.e., similar values of these parameters. Therefore, the group of patients referred to as frail has the most pronounced disturbances in biomarker concentrations. In contrast, albumin and fibrinogen concentrations are not indicators differentiating the states referred to as robust and pre-frail.
3.3. Components of Linda’s Fried Frailty Definition
The analysis of the average results of the individual components of the Linda Fried scale showed powerful correlations between the groups (robust, prefrail, and frail). The strength in the strongest hand expressed in kilograms and the time to cover a distance of 5 meters increases with the increasing severity of the frailty. The average value of muscle strength, 23.2 kg, is below the cut-off point for men, who constituted the majority in the frail group. Similarly, the average value of walking speed, 6.13 s, exceeds the norm for both sexes. Similarly, patients with frailty syndrome are characterized by the lowest level of physical activity in comparison with patients from the non-frail and robust groups. In the studied group, a subjective feeling of exhaustion occurs in 38% of patients. In contrast, none of the patients who qualified for the robust group showed signs of exhaustion; this percentage was significantly higher in the prefrail and frail groups (50% and 81%, respectively). Weight loss was noted less frequently: in 19% of patients in the entire group, 21% in the prefrail group, and 62% in the frail group. Similarly, no patient in the robust group noted weight loss. The analysis of the Fried frailty scale criteria in the study group is presented in Table 3.
3.4. Skale oceny Stanu Odżywienia, Ryzyka Sarkopenii i Stanu Funkcjonalnego Pacjentów
Taking into account all patient assessment scales analyzed in the study (Table 4), a statistically significant correlation was noted between the frailty stage and the obtained results (p<0.001 for each scale). The median value of the SARC-F scale for the general, robust, and frail groups was 0. In contrast, patients with frailty syndrome obtained results with a median of 3, which is evidence of a strong association between frailty and sarcopenia. Similarly, the median scores of the MNA scale in the robust and pre-frail groups were similar (27 and 26 points, respectively). In comparison, the median score of the scale in the frail group significantly differed from the other groups (23.5 points, which is the cut-off value for a condition defined as at risk of malnutrition). Differences in the medians of the CFS and IADL scales showed similar trends. It is worth noting, however, that the median values of the CFS scale in the robust and prefrail groups showed the same values, which questions the validity of using this scale in screening the state defined as prefrail. Multiple comparisons of p-value analysis showed no differences between the prefrail and robust stages in any of the analyzed scales.
3.5. Stratification Analysis According to Frailty Stage, MNA, and SARC-F Score
Analysis of variance allowed for observing differences in the concentration of the studied variables depending on the stage of frailty and the separate groups in the SARC-F and MNA scales, as indicated by the results of the conducted statistical tests (Figure 2). Patients who obtained a score of <3 on the SARC-F scale were classified as not at risk of sarcopenia, and those who received more than 4 points were classified as at risk of sarcopenia. Patients who obtained a score of more than 24 points on the MNA scale were classified as patients not at risk of malnutrition, and those who received a score below 24 points as at risk of malnutrition. Out of 21 patients with frailty syndrome, as many as 8 (38%) obtained a score of more than 4 points on the SARC-F scale (at risk of sarcopenia). Moreover, 11 of them (52%) exhibit features indicative of a risk of malnutrition (MNA > 24).
The stratification results for albumin, total protein, and fibrinogen levels are presented in Table 5. It was demonstrated that the SARC-F scale can effectively identify patients with reduced total protein and albumin levels (p < 0.01). Similarly, belonging to the group at risk of malnutrition, as expressed in the MNA scale, can help predict a decrease in serum albumin (p<0.01). For fibrinogen, significant differences were observed in the classification according to the Fried frailty scale. Increased fibrinogen values characterize patients with developed frailty.
The patients’ affiliation to individual groups in the MNA and SARC-F scales also influenced the functional results. Combining the Fried frailty scale and MNA scales allows for the identification of patients with reduced body mass (p < 0.05). Both the MNA and SARC-F scales indicate that patients have reduced gait speed and hand-grip strength (p < 0.05). The combination of the Fried frailty scale and MNA suggests a group of patients with reduced PEF values, but for FEV1, the only effective predictor is the frailty scale itself. Morphometric and functional assessment of patients stratified by phenotype frailty, SARC-F, and/or MNA classification is presented in Table 6..
Analyzing the entire study group, clear correlations of quantitative values can be observed. Hand grip strength shows strongly positive correlations with respiratory parameters: PEF (R=0.53), FEV1 (R=0.55), and fat-free body mass (R=0.60). Fat-free body mass also correlates with PEF (0.40) and FEV1 (0.40). The constellation of these relationships indicates a possible relationship between the decrease in muscle strength associated with the decline in fat-free body mass, which also affects the strength of respiratory muscles, and thus the functional parameters of the lungs. The remaining correlations are presented in Table 7.
4. Discussion
In summary, a homogeneous cohort of patients aged 65 and older was collected. Of the 170 patients, 53 were classified as robust (31%), 96 as prefrail (57%), and 21 as frail (12%). Patients defined as frail had significantly reduced serum albumin values and increased fibrinogen values compared to the pre-frail and robust groups. Each of the analyzed components of the Fried frailty scale strongly correlates with the severity of frailty. The analysis did not reveal significant differences in the concentration of laboratory parameters and the results of the analyzed scales between the pre-frail and robust stages, indicating a need to develop reliable tools for differentiating these states. Stratification of patients according to the risk of malnutrition and sarcopenia, determined using the MNA and SARC-F scales, may help identify patients at the highest risk. At the same time, our results confirm the multidirectional nature of disorders in frailty: decline in physical functions, morphological disorders, respiratory disorders, multimorbidity, and apparent differences in the clinical condition of patients defined as frail.
We confirm that malnutrition is a significant problem in elderly patients. Albumin levels are strongly correlated with the nutritional status of patients. The study showed a significant decrease in albumin levels in patients with frailty. These results are consistent with previous reports in the literature. Albumin is a potential biomarker of both frailty and sarcopenia. Frail patients have significantly lower albumin levels than their healthy peers, regardless of age [5,6]. In addition, higher albumin levels are correlated with a lower risk of developing frailty [6]. Moreover, the integral reduction in albumin concentration is associated with a decrease in other parameters such as estimated glomerular filtration rate (eGFR) or trace elements [20].
Similarly, patients with higher total protein levels are less likely to develop frailty [6]. Our study found no differences in total protein concentration between the groups. However, belonging to the group at risk of sarcopenia expressed on the SARC-F scale is associated with a statistically significant decrease in total protein concentration, regardless of the severity of frailty. Nevertheless, not total protein, but albumin is the most responsive parameter to functional state (strength, speed of movement) and a potential candidate to complete the frailty phenotype.
Our study also showed a significant difference in fibrinogen concentration between patients with frailty and healthy individuals. Frail patients have increased fibrinogen concentrations, which is confirmed in the literature. In addition, fibrinogen concentration increases with age. The underlying cause of this phenomenon may be the pathophysiology of frailty, in which the coagulation state is an integral component and influences catabolic processes (including sarcopenia and malnutrition) [21]. He et al. also showed higher fibrinogen values in frail patients, but it was not a biomarker of frailty progression [22]. However, research on the role of fibrinogen in the frailty syndrome is scarce and requires further analysis.
An integral element of the study was the analysis of the effectiveness of assessing elderly patients using the MNA and SARC-F scales, which indicated the risk of two main threats to frailty syndrome: sarcopenia and malnutrition. It was shown that patients with frailty syndrome achieve higher values on the SARC-F scale compared to the pre-frail and robust groups. On the other hand, they achieve lower results on the MNA scale compared to their peers. Additionally, these scales effectively identify integral disorders resulting from frailty syndrome, including decreased muscle strength, reduced walking speed, and decreased respiratory function in patients. Stratification of patients according to their affiliation with high-risk groups, as determined by the MNA, SARC-F, and Fried frailty scale, may indicate a group of patients at particularly high risk, which requires intensive preventive and therapeutic measures. These observations have been confirmed in other clinical studies. Patients with reduced walking speed achieve lower values on the MNA scale [23]. In the study by Li et al., the MNA score was shown to correlate with the skeletal muscle index. This study confirms our reports, where frailty and malnutrition are associated with sarcopenia [24]. Additionally, it has been suggested that the MNA malnutrition score is a potential predictor of poor physical fitness in elderly patients [11]. On the other hand, it is believed that not the abbreviated nutritional assessment (MNA) but the complete assessment using the Global Leadership Initiative on Malnutrition (GLIM) effectively identifies patients at 5-year risk of sarcopenia [25].
The demonstrated correlations between lean body mass, muscle strength, and respiratory parameters, PEF, and FEV1 are worth noting. Moreover, patients burdened with frailty syndrome, regardless of sarcopenia and malnutrition, are characterized by reduced baseline values of respiratory parameters. However, no difference in diaphragm thickness was demonstrated depending on the stage of frailty syndrome, despite different results of studies available in the literature [26]. However, in recent years, "respiratory sarcopenia" has been gaining importance, defined as the coexistence of a decrease in respiratory muscle mass and respiratory dysfunction, just as a decrease in skeletal muscle strength correlates with a reduction in muscle strength [27]. Additionally, it has been shown that an increase in PEF is associated with an improvement in cognitive functions in elderly patients [28], and mental disorders are an essential component of frailty. Similarly, increased PEF in elderly people is associated with a lower risk of renal function deterioration [29]. Therefore, we suggest including PEF and FEV1 measurement using a peakflowmeter in the routine evaluation of elderly patients, as a quick, simple, and cheap test.
Our conclusion regarding the necessity of simultaneous assessment of nutritional status, sarcopenia, and frailty is further supported by the findings of the study by Wei et al., where the simultaneous coexistence of frailty and malnutrition is associated with a worse prognosis and mortality. In contrast, poor nutrition alone without physical frailty is not correlated with an increased risk [30]. On the other hand, the meta-analysis and systematic review by Verlaan et al. indicate that ⅔ of malnourished patients were also frail, and of the frail patients, only 10% were malnourished [31]. In our study, more than 50% of patients with frailty syndrome presented features of malnutrition risk. The literature also supports the distribution of patients in the study. In the study by Atay et al., similarly to our report, most patients were in the prefrail stage, which emphasizes the validity of future actions aimed at fully characterizing this group of patients [32].
In general, recent reports indicate that in every field of medicine, nutritional status affects the prognosis and condition of patients. Considering the cohort of the presented study (patients with diagnosed coronary artery disease), the relationship between nutritional status and cardiological comorbidities is significant. It has been shown that nutritional status expressed by the MNA scale is an independent predictor of all-cause death and re-hospitalization in patients with heart failure [33]. On the other hand, malnutrition increases the risk of postoperative delirium in elderly patients [34,35], which may be important in the invasive and surgical treatment of coronary artery disease and other cardiological diseases.
The diagnosis of malnutrition and sarcopenia, therefore, requires intensive efforts. Particular attention is paid to leucine and protein supplementation and resistance training to increase muscle mass and thus improve prognosis [36]. Other analyses indicate the need for vitamin D supplementation in women and testosterone in men [37]. In addition, a personalized diet in malnourished patients improves physical functions and quality of life [38]. Protein intake above the recommended dietary allowance (RDA) is associated with significant improvement in motor function in elderly patients, which is a protective factor against decreased muscle strength, falls, and disability [39]. On the other hand, the meta-analysis by Coelho-Junior et al. showed that protein intake is not correlated with frailty. Nevertheless, frail patients consume significantly less animal-derived protein than robust patients [40]. Without a doubt, future research should focus on developing standardized protocols and guidelines for preventing and treating sarcopenia and malnutrition in elderly patients.
A significant limitation of the presented study was the sample size, which did not allow for drawing more solid conclusions. Additionally, the study was observational, which impedes clear conclusions (underpowered). Nevertheless, the study provides new information on the relationship between frailty and malnutrition, which should be developed in future studies. Additionally, the study only included the classification of frailty syndrome using the Fried frailty scale. The unquestionable advantage of this scale is the simplicity and speed of clinical assessment of the patient. The advantage of the Fried frailty scale is also the specification of the state referred to as pre-frail, which is potentially reversible [41]. However, more than 50 other tools have been described to diagnose frailty. There is a need to standardize frailty assessment protocols in clinical trials to compare results and facilitate everyday clinical practice in diagnosing frailty [42].
5. Conclusions
Our study confirms the distinctiveness of patients defined as frail. Patients affected by frailty exhibit lower muscle strength, slower gait, reduced physical activity levels, and poorer respiratory parameters. Frailty is also associated with decreased serum albumin concentration and increased fibrinogen. MNA and SARC-F scales combined with routine screening of elderly patients with frailty may allow for effective identification of patients at risk of malnutrition and sarcopenia, which additionally worsen the prognosis. In conclusion, we prove that the development of frailty is multifactorial and individual components of frailty overlap. Thus, the management of frail patients should be based on the work of an interdisciplinary team, with a particular emphasis on addressing malnutrition and sarcopenia.
Author Contributions
Conceptualization: J.C., B.P.-C. and A.T.; Methodology: J.C., B.P.-C. and A.T.; Software: J.C. and A.T.; Validation: B.P.-C. and A.T.; Investigation: J.C., M.S., M.K., M.J., I.D., D.S. and J.B.; Writing—original draft preparation: J.C., M.S., M.K., M.J., I.D., D.S., J.B. and A.T.; Writing—review and editing: J.C., M.S., M.K., M.J., I.D., D.S., J.B. and A.T.; Visualization: J.C., B.P.-C. and A.T.; Supervision: B.P.-C. and A.T.; Project administration: J.C. and A.T.; Funding acquisition: A.T. and J.C. All authors have read and agreed to the published version of the manuscript.
Funding
J.C. has received a grant “Studenckie Granty Badawcze Europejskiego Miasta Nauki” no RW/105/2024 from “Konsorcjum Akademickie Europejskie Miasto Nauki”. A.T. has received grants BNW-1-171/K/3/K, and PCN-1-235/K/2/K from the Medical University of Silesia.
Institutional Review Board Statement
This study was conducted following the Declaration of Helsinki and approved by the Ethics Committee of the Medical University of Silesia (3 October 2017 (KNW/0022/KB1/39/I/17)); (8 February 2022 (PCN/CBN/0022/KB1/39/II/17/22)).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The original contributions presented in the study are included in the article; further inquiries can be directed to the corresponding authors.
Acknowledgments
The authors declare no specific acknowledgments.
Abbreviations
The following abbreviations are used in this manuscript:
| MNA | Mini Nutritional Assessment |
| MNA-SF | Mini Nutritional Assessment Short Form |
| FRAPICA | Frailty Syndrome in Daily Practice of Interventional Cardiology Ward |
| BMI | Body Mass Index |
| FFBM | Fat-free body mass |
| PEF | Peak expiratory flow |
| FEV1 | Forced Expiratory volume- one second |
| IADL | Instrumental Activites of Daily Living |
| CFS | Clinical Frailty Scale |
| COPD | Chronic obstructive pulmonary disease |
| MI | Myocardial Infarction |
| PCI | Percutaneous coronary intervention |
| CABG | Coronary artery bypass grafting |
References
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G.; et al. Frailty in Older Adults: Evidence for a Phenotype. J. Gerontol. A. Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef] [PubMed]
- Hoogendijk, E.O.; Afilalo, J.; Ensrud, K.E.; Kowal, P.; Onder, G.; Fried, L.P. Frailty: Implications for Clinical Practice and Public Health. The Lancet 2019, 394, 1365–1375. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Cohen, A.A.; Xue, Q.-L.; Walston, J.; Bandeen-Roche, K.; Varadhan, R. The Physical Frailty Syndrome as a Transition from Homeostatic Symphony to Cacophony. Nat. Aging 2021, 1, 36–46. [Google Scholar] [CrossRef]
- Chu, W.; Chang, S.; Ho, H. Adverse Health Effects of Frailty: Systematic Review and Meta-Analysis of Middle-Aged and Older Adults With Implications for Evidence-Based Practice. Worldviews Evid. Based Nurs. 2021, 18, 282–289. [Google Scholar] [CrossRef]
- Picca, A.; Coelho-Junior, H.J.; Calvani, R.; Marzetti, E.; Vetrano, D.L. Biomarkers Shared by Frailty and Sarcopenia in Older Adults: A Systematic Review and Meta-Analysis. Ageing Res. Rev. 2022, 73, 101530. [Google Scholar] [CrossRef]
- Mailliez, A.; Guilbaud, A.; Puisieux, F.; Dauchet, L.; Boulanger, É. Circulating Biomarkers Characterizing Physical Frailty: CRP, Hemoglobin, Albumin, 25OHD and Free Testosterone as Best Biomarkers. Results of a Meta-Analysis. Exp. Gerontol. 2020, 139, 111014. [Google Scholar] [CrossRef]
- Roberts, S.; Collins, P.; Rattray, M. Identifying and Managing Malnutrition, Frailty and Sarcopenia in the Community: A Narrative Review. Nutrients 2021, 13, 2316. [Google Scholar] [CrossRef] [PubMed]
- Gingrich, A.; Volkert, D.; Kiesswetter, E.; Thomanek, M.; Bach, S.; Sieber, C.C.; Zopf, Y. Prevalence and Overlap of Sarcopenia, Frailty, Cachexia and Malnutrition in Older Medical Inpatients. BMC Geriatr. 2019, 19, 120. [Google Scholar] [CrossRef]
- Faxén-Irving, G.; Luiking, Y.; Grönstedt, H.; Franzén, E.; Seiger, Å.; Vikström, S.; Wimo, A.; Boström, A.-M.; Cederholm, T. Do Malnutrition, Sarcopenia and Frailty Overlap in Nursing-Home Residents? J. Frailty Aging 2021, 10, 17–21. [Google Scholar] [CrossRef]
- Feng, Z.; Xia, J.; Yu, J.; Wang, J.; Yin, S.; Yang, J.; Wu, T.; Zhang, Z.; Yan, W.; Wang, S.; et al. Pathophysiological Mechanisms Underlying Sarcopenia and Sarcopenic Obesity: A Systematic Review and Meta-Analysis of Biomarker Evidence. Int. J. Mol. Sci. 2025, 26, 5113. [Google Scholar] [CrossRef]
- Amasene, M.; Besga, A.; Medrano, M.; Urquiza, M.; Rodriguez-Larrad, A.; Tobalina, I.; Barroso, J.; Irazusta, J.; Labayen, I. Nutritional Status and Physical Performance Using Handgrip and SPPB Tests in Hospitalized Older Adults. Clin. Nutr. 2021, 40, 5547–5555. [Google Scholar] [CrossRef] [PubMed]
- Amasene, M.; Medrano, M.; Echeverria, I.; Urquiza, M.; Rodriguez-Larrad, A.; Diez, A.; Labayen, I.; Ariadna, B.-B. Malnutrition and Poor Physical Function Are Associated With Higher Comorbidity Index in Hospitalized Older Adults. Front. Nutr. 2022, 9, 920485. [Google Scholar] [CrossRef]
- Bauer, J.M.; Kaiser, M.J.; Anthony, P.; Guigoz, Y.; Sieber, C.C. The Mini Nutritional Assessment®—Its History, Today’s Practice, and Future Perspectives. Nutr. Clin. Pract. 2008, 23, 388–396. [Google Scholar] [CrossRef] [PubMed]
- Malmstrom, T.K.; Morley, J.E. SARC-F: A Simple Questionnaire to Rapidly Diagnose Sarcopenia. J. Am. Med. Dir. Assoc. 2013, 14, 531–532. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, M.; Li, J.; Ruan, L.; Wu, X.; Zhang, C.; Chen, L. Physical Frailty, Genetic Predisposition, and Incident Arrhythmias. J. Cachexia Sarcopenia Muscle 2024, 15, 1463–1472. [Google Scholar] [CrossRef]
- Shi, Q.; Huang, J.; Wan, J.; Zhong, Z.; Sun, Y.; Zhou, Y.; Li, J.; Tan, X.; Yu, B.; Lu, Y.; et al. Physical Frailty, Genetic Predisposition, and Incident Heart Failure. JACC Asia 2024, 4, 547–556. [Google Scholar] [CrossRef] [PubMed]
- Qayyum, S.; Rossington, J.A.; Chelliah, R.; John, J.; Davidson, B.J.; Oliver, R.M.; Ngaage, D.; Loubani, M.; Johnson, M.J.; Hoye, A. Prospective Cohort Study of Elderly Patients with Coronary Artery Disease: Impact of Frailty on Quality of Life and Outcome. Open Heart 2020, 7, e001314. [Google Scholar] [CrossRef]
- Wołoszyn-Horák, E.; Salamon, R.; Chojnacka, K.; Brzosko, A.; Bieda, Ł.; Standera, J.; Płoszaj, K.; Stępień, E.; Nowalany-Kozielska, E.; Tomasik, A. Frailty Syndrome in Daily Practice of Interventional Cardiology Ward—Rationale and Design of the FRAPICA Trial: A STROBE-Compliant Prospective Observational Study. Medicine (Baltimore) 2020, 99, e18935. [Google Scholar] [CrossRef]
- Yetkin, N.A.; Akın, S.; Kocaslan, D.; Baran, B.; Rabahoglu, B.; Oymak, F.S.; Tutar, N.; Gulmez, İ. The Role of Diaphragmatic Ultrasound in Identifying Sarcopenia in COPD Patients: A Cross-Sectional Study. Int. J. Chron. Obstruct. Pulmon. Dis. 2025, Volume 20, 1–9. [Google Scholar] [CrossRef]
- Yamamoto, M.; Adachi, H.; Enomoto, M.; Fukami, A.; Nakamura, S.; Nohara, Y.; Sakaue, A.; Morikawa, N.; Hamamura, H.; Toyomasu, K.; et al. Lower Albumin Levels Are Associated with Frailty Measures, Trace Elements, and an Inflammation Marker in a Cross-Sectional Study in Tanushimaru. Environ. Health Prev. Med. 2021, 26, 25. [Google Scholar] [CrossRef]
- Kanapuru, B.; Ershler, W.B. Inflammation, Coagulation, and the Pathway to Frailty. Am. J. Med. 2009, 122, 605–613. [Google Scholar] [CrossRef] [PubMed]
- He, L.; Yang, J.; Fang, Y. Longitudinal Analysis on Inflammatory Markers and Frailty Progression: Based on the English Longitudinal Study of Aging. Eur. Geriatr. Med. 2024, 15, 1323–1330. [Google Scholar] [CrossRef]
- Dilektasli, A.G.; Öztürk, N.A.A.; Kerimoğlu, D.; Odabaş, A.; Yaman, M.T.; Dogan, A.; Demirdogen, E.; Guclu, O.A.; Coşkun, F.; Ursavas, A.; et al. Slow Gait Speed Is Associated with Frailty, Activities of Daily Living and Nutritional Status in in-Patient Pulmonology Patients. Aging Clin. Exp. Res. 2025, 37, 133. [Google Scholar] [CrossRef]
- Li, Q.; Shang, N.; Gao, Q.; Guo, S.; Yang, T. Prevalence of Sarcopenia and Its Association with Frailty and Malnutrition among Older Patients with Sepsis-a Cross-Sectional Study in the Emergency Department. BMC Geriatr. 2025, 25, 377. [Google Scholar] [CrossRef] [PubMed]
- Lengelé, L.; Bruyère, O.; Beaudart, C.; Reginster, J.-Y.; Locquet, M. Malnutrition, Assessed by the Global Leadership Initiative on Malnutrition (GLIM) Criteria but Not by the Mini Nutritional Assessment (MNA), Predicts the Incidence of Sarcopenia over a 5-Year Period in the SarcoPhAge Cohort. Aging Clin. Exp. Res. 2021, 33, 1507–1517. [Google Scholar] [CrossRef]
- Siniscalchi, C.; Nouvenne, A.; Cerundolo, N.; Meschi, T.; Ticinesi, A. ; on behalf of the Parma Post-Graduate Specialization School in Emergency-Urgency Medicine Interest Group on Thoracic Ultrasound Diaphragm Ultrasound in Different Clinical Scenarios: A Review with a Focus on Older Patients. Geriatrics 2024, 9, 70. [Google Scholar] [CrossRef] [PubMed]
- Sato, S.; Miyazaki, S.; Tamaki, A.; Yoshimura, Y.; Arai, H.; Fujiwara, D.; Katsura, H.; Kawagoshi, A.; Kozu, R.; Maeda, K.; et al. Respiratory Sarcopenia: A Position Paper by Four Professional Organizations. Geriatr. Gerontol. Int. 2023, 23, 5–15. [Google Scholar] [CrossRef]
- Wang, Y.; Huang, J.; Tao, Y.; Zhang, Y.; Zhou, X.; Mao, H. The Relationship between Lung Function and Cognitive Impairment among Middle-Aged and Older Adults: The Mediating Role of Depressive Symptoms. J. Psychosom. Res. 2025, 193, 112148. [Google Scholar] [CrossRef]
- Han, S.; Xu, Y.; Wang, Y. Association between Pulmonary Function and Rapid Kidney Function Decline: A Longitudinal Cohort Study from CHARLS. BMJ Open Respir. Res. 2024, 11, e002107. [Google Scholar] [CrossRef]
- Wei, K.; Nyunt, M.-S.-Z.; Gao, Q.; Wee, S.-L.; Yap, K.-B.; Ng, T.-P. Association of Frailty and Malnutrition With Long-Term Functional and Mortality Outcomes Among Community-Dwelling Older Adults: Results From the Singapore Longitudinal Aging Study 1. JAMA Netw. Open 2018, 1, e180650. [Google Scholar] [CrossRef]
- Verlaan, S.; Ligthart-Melis, G.C.; Wijers, S.L.J.; Cederholm, T.; Maier, A.B.; De Van Der Schueren, M.A.E. High Prevalence of Physical Frailty Among Community-Dwelling Malnourished Older Adults–A Systematic Review and Meta-Analysis. J. Am. Med. Dir. Assoc. 2017, 18, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Atay, K.; Aydin, S.; Canbakan, B. Sarcopenia and Frailty in Cirrhotic Patients: Evaluation of Prevalence and Risk Factors in a Single-Centre Cohort Study. Medicina (Mex.) 2025, 61, 821. [Google Scholar] [CrossRef] [PubMed]
- Joaquín, C.; Alonso, N.; Lupón, J.; De Antonio, M.; Domingo, M.; Moliner, P.; Zamora, E.; Codina, P.; Ramos, A.; González, B.; et al. Mini Nutritional Assessment Short Form Is a Morbi-Mortality Predictor in Outpatients with Heart Failure and Mid-Range Left Ventricular Ejection Fraction. Clin. Nutr. 2020, 39, 3395–3401. [Google Scholar] [CrossRef]
- Moellmann, H.L.; Alhammadi, E.; Boulghoudan, S.; Kuhlmann, J.; Mevissen, A.; Olbrich, P.; Rahm, L.; Frohnhofen, H. Risk of Sarcopenia, Frailty and Malnutrition as Predictors of Postoperative Delirium in Surgery. BMC Geriatr. 2024, 24, 971. [Google Scholar] [CrossRef]
- Mazzola, P.; Ward, L.; Zazzetta, S.; Broggini, V.; Anzuini, A.; Valcarcel, B.; Brathwaite, J.S.; Pasinetti, G.M.; Bellelli, G.; Annoni, G. Association Between Preoperative Malnutrition and Postoperative Delirium After Hip Fracture Surgery in Older Adults. J. Am. Geriatr. Soc. 2017, 65, 1222–1228. [Google Scholar] [CrossRef]
- Gielen, E.; Beckwée, D.; Delaere, A.; De Breucker, S.; Vandewoude, M.; Bautmans, I.; the Sarcopenia Guidelines Development Group of the Belgian Society of Gerontology and Geriatrics (BSGG); Bautmans, I.; Beaudart, C.; Beckwée, D.; et al. Nutritional Interventions to Improve Muscle Mass, Muscle Strength, and Physical Performance in Older People: An Umbrella Review of Systematic Reviews and Meta-Analyses. Nutr. Rev. 2021, 79, 121–147. [Google Scholar] [CrossRef] [PubMed]
- the Sarcopenia Guidelines Development group of the Belgian Society of Gerontology and Geriatrics (BSGG); De Spiegeleer, A.; Beckwée, D.; Bautmans, I.; Petrovic, M. Pharmacological Interventions to Improve Muscle Mass, Muscle Strength and Physical Performance in Older People: An Umbrella Review of Systematic Reviews and Meta-Analyses. Drugs Aging 2018, 35, 719–734. [Google Scholar] [CrossRef]
- Arıcı, H.; Tor, Y.B.; Altınkaynak, M.; Erten, N.; Saka, B.; Bayramlar, O.F.; Karakuş, Z.N.; Akpınar, T.S. Personalized Diet With or Without Physical Exercise Improves Nutritional Status, Muscle Strength, Physical Performance, and Quality of Life in Malnourished Older Adults: A Prospective Randomized Controlled Study. Nutrients 2025, 17, 675. [Google Scholar] [CrossRef]
- Coelho-Júnior, H.J.; Calvani, R.; Tosato, M.; Landi, F.; Picca, A.; Marzetti, E. Protein Intake and Physical Function in Older Adults: A Systematic Review and Meta-Analysis. Ageing Res. Rev. 2022, 81, 101731. [Google Scholar] [CrossRef]
- Coelho-Junior, H.J.; Calvani, R.; Picca, A.; Tosato, M.; Landi, F.; Marzetti, E. Protein Intake and Frailty in Older Adults: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2022, 14, 2767. [Google Scholar] [CrossRef]
- Yakabi, A.; Ishizaka, M.; Watanabe, M.; Matsumoto, C.; Ito, A.; Endo, Y.; Hara, T.; Igawa, T.; Kubo, A.; Itokazu, M. A Longitudinal Study of Frailty Reversibility through a Multi-Component Dementia Prevention Program.
- Faller, J.W.; Pereira, D.D.N.; De Souza, S.; Nampo, F.K.; Orlandi, F.D.S.; Matumoto, S. Instruments for the Detection of Frailty Syndrome in Older Adults: A Systematic Review. PLOS ONE 2019, 14, e0216166. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Correlations between the stage of frailty syndrome and the concentration of fibrinogen, albumin, and total protein.
Figure 1.
Correlations between the stage of frailty syndrome and the concentration of fibrinogen, albumin, and total protein.
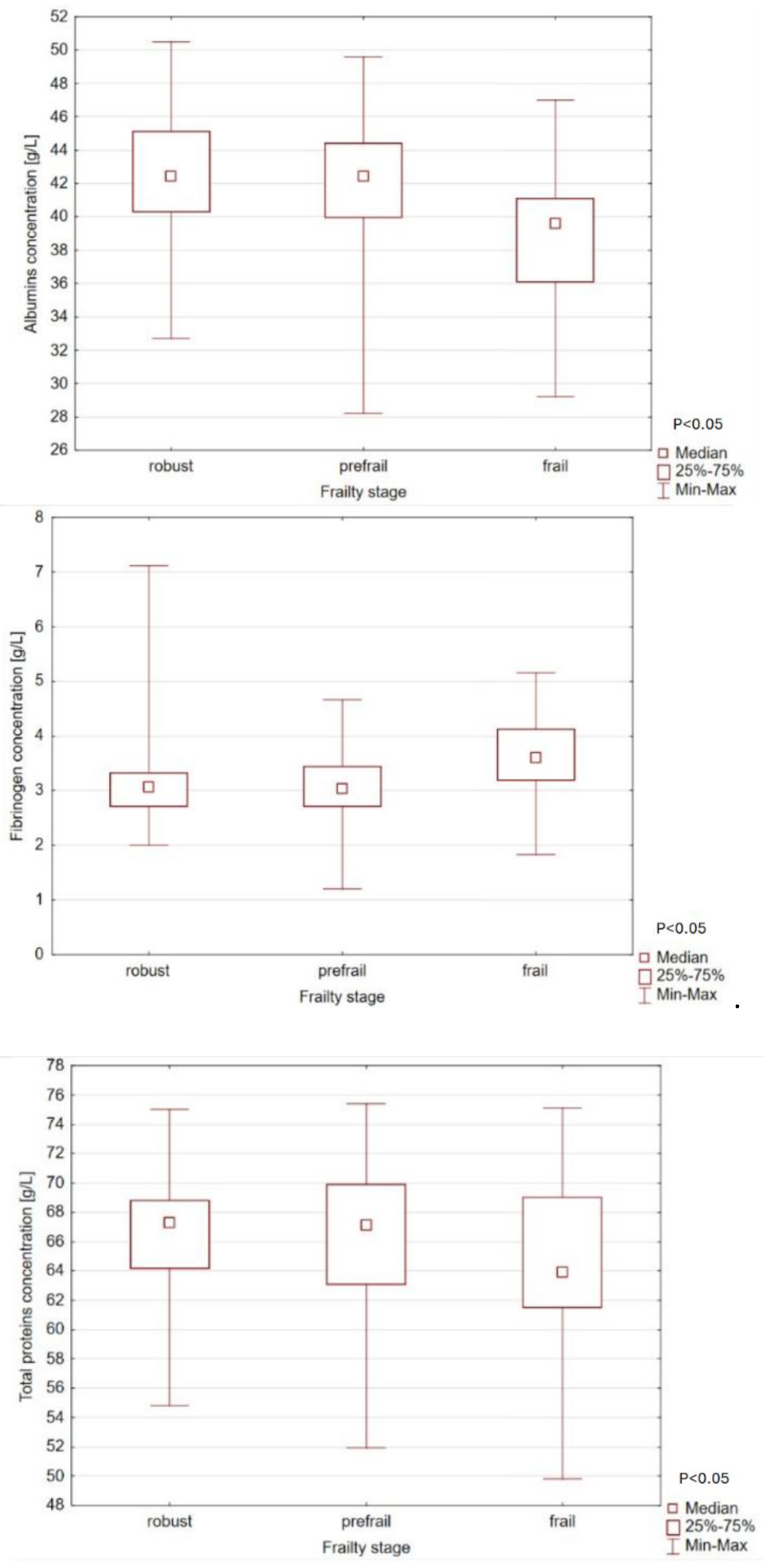
Figure 2.
Method of assigning patients to risk groups for sarcopenia and malnutrition.
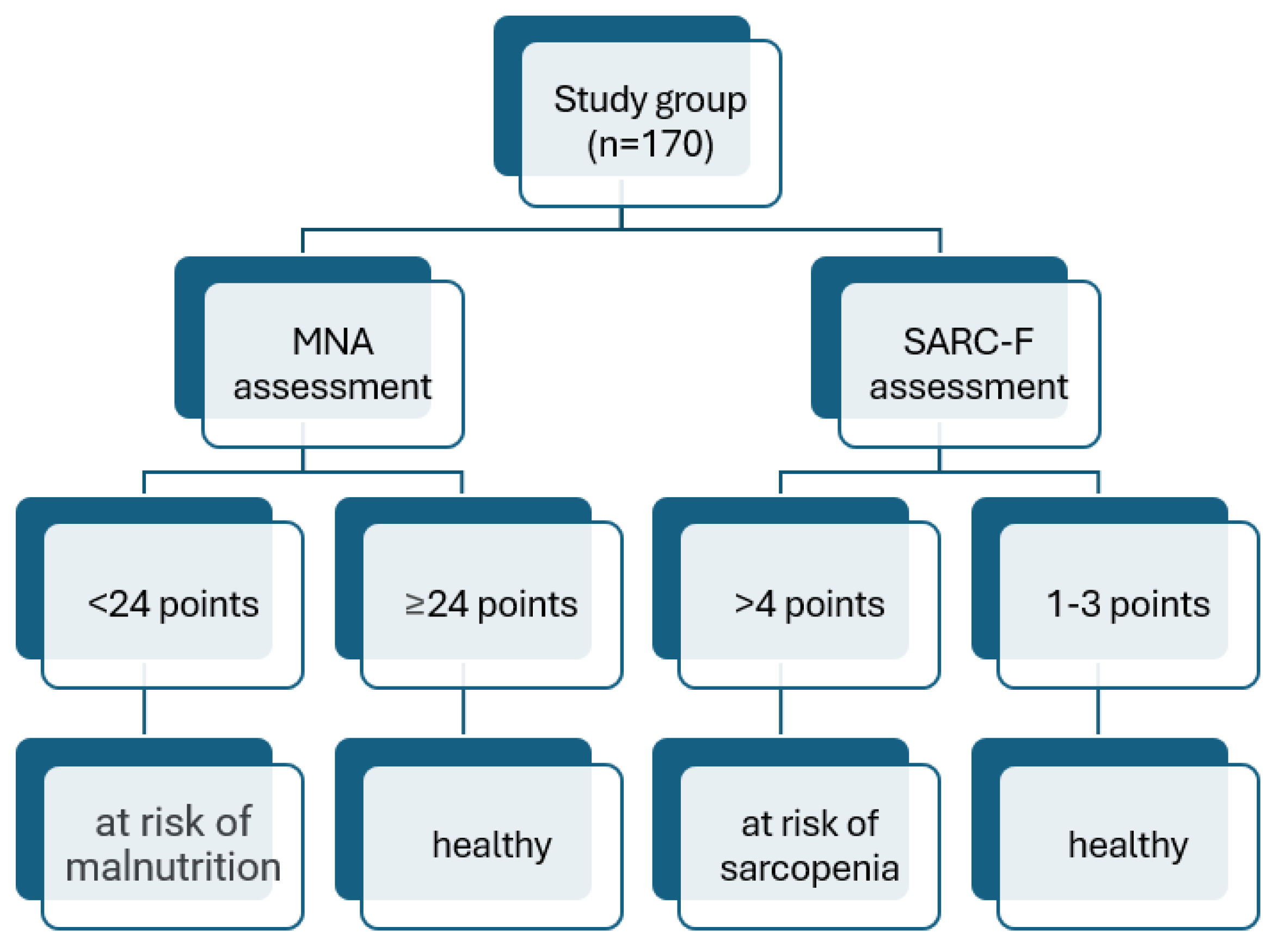

Table 1.
Patients' demographic and medical data. Normally distributed variables are presented as mean ± standard deviation. Non-normally distributed data are presented as median (quartile 1-quartile 3).
Table 1.
Patients' demographic and medical data. Normally distributed variables are presented as mean ± standard deviation. Non-normally distributed data are presented as median (quartile 1-quartile 3).
| General n=170 | Robust n=53 | Prefrail n=96 | Frail n=21 | Significance | |
|---|---|---|---|---|---|
| Age, mean ± SD | 73,8 ± 5,6 | 72,8 ± 5,2 | 73,8 ± 5,5 | 76,3 ± 6,7 | NS |
| Men/women, n/n | 113/57 | 42/11 | 59/37 | 12/9 | NS |
| Weight (kg), mean ± SD | 82,6 ± 13,4 | 82,8 ± 11,0 | 82,7 ± 14,6 | 81,8 ± 13,1 | NS |
| Height (cm), mean ± SD | 168,6 ± 7,9 | 170,6 ± 6,5 | 168,3 ± 8,0 | 165,3 ± 9,2 | <0,05 |
| BMI(kg/cm2), mean ± SD | 29,1 ± 4,7 | 28,5 ± 3,7 | 29,1 ± 4,6 | 30,5 ± 6,7 | NS |
| FFBM (kg), mean ± SD | 56,2 ± 9,2 | 57,3 ± 8,9 | 55,8 ± 9,7 | 55,1 ± 7,2 | NS |
| Diaphragm thickness (cm), mean ± SD | 3,7 ± 0,9 | 3,7 ± 0,8 | 3,7 ± 0,9 | 3,5 ± 0,93 | NS |
| PEF (L/min), mean ± SD |
316,3 ± 130,1 | 345,2 ± 135,7 | 311,9 ± 128,1 | 266,0 ± 117,0 | <0,05 |
| FEV1 (L), mean ± SD |
1,95 ± 0,7 | 2,1 ± 0,7 | 1,9 ± 0,7 | 1,5 ± 0,6 | <0,05 |
| Hypertension, n (%) | 139 (82%) | 46 (87%) | 76 (79%) | 17 (81%) | NS |
| Hipercholesterolemia, n (%) | 126 (74%) | 41 (77%) | 75 (78%) | 10 (48%) | <0,05 |
| Diabetes, n (%) | 74 (44%) | 21 (40%) | 44 (46%) | 9 (43%) | NS |
| Atrial fibrillation, n (%) |
40 (24%) | 8 (15%) | 24 (25%) | 8 (38%) | NS |
| Renal failure, n (%) | 15 (9%) | 4 (8%) | 7 (7%) | 4 (19%) | NS |
| COPD/asthma, n (%) | 25 (15%) | 7 (13%) | 16 (17%) | 2 (1%) | NS |
| Malignancy, n (%) | 19 (11%) | 10 (19%) | 7 (7%) | 2 (10%) | NS |
| History of MI, n (%) | 45 (27%) | 16 (30%) | 24 (25%) | 5 (24%) | NS |
| History of PCI, n (%) | 67 (39%) | 23 (43%) | 38 (40%) | 6 (29%) | NS |
| History of CABG, n (%) |
18 (11%) | 7 (13%) | 9 (9%) | 2 (10%) | NS |
BMI- body mass index, CABG- coronary artery bypass grafting, FFBM- fat-free body mass, MI- myocardial infarction, PCI- percutaneous coronary intervention, PEF- peak expiratory flow, FEV1- forced expiratory volume- one second, NS- non-significant, SD- standard deviation,.
Table 2.
Mean values of total protein, albumin, and fibrinogen concentrations depending on the severity of frailty syndrome expressed as “mean ± SD”.
Table 2.
Mean values of total protein, albumin, and fibrinogen concentrations depending on the severity of frailty syndrome expressed as “mean ± SD”.
| General n=170 | Robust n=53 | Prefrail n=96 | Frail n=21 | Significance | |
|---|---|---|---|---|---|
| Whole protein (g/L) | 66,2 ± 5,0 | 66,4 ± 4,45 | 66,4 ± 5,0 | 64,6 ± 6,4 | NS |
| Albumins (g/L) | 41,8 ± 3,8 | 42,5 ± 3,5 | 42,0 ± 3,7 | 39,3 ± 4,2 | <0,05 |
| Fibrinogen (g/L) | 3,1 ± 0,7 | 3,1 ± 0,8 | 3,1 ± 0,6 | 3,6 ± 0,7 | <0,05 |
Table 3.
Analysis of the results of individual frailty criteria according to Linda Fried, depending on the stage of frailty.
Table 3.
Analysis of the results of individual frailty criteria according to Linda Fried, depending on the stage of frailty.
| General n=170 | Robust n=53 | Prefrail n=96 | Frail n=21 | Significance | |
|---|---|---|---|---|---|
| Hand strength (kg) | 30,4 ± 9,8 | 35,2 ± 8,2 | 29,3 ± 9,9 | 23,2 ± 7,0 | <0,001 |
|
Level of physical activity, (kcal/week) |
1159 (585-2050) | 1453 (830-2738) | 1229 (645-1881) | 464 (242-909) | <0,001 |
|
Slowness, (s/5meters) |
4,14 (3,4-5,27) | 3,66 (2,99- 4,31) | 4,3 (3,73- 5,26) | 6,13 (5,0-8,27) | <0,001 |
|
Exhaustion, n (%) |
65 (38%) | 0 (0%) | 48 (50%) | 17 (81%) | <0,001 |
|
Weight loss, n (%) |
33 (19%) | 0 (0%) | 20 (21%) | 13 (62%) | <0,001 |
Table 4.
Median scores of MNA, CFS, IADL, and SARC-F scales according to the frailty stage.
| General n=170 | Robust n=53 | Prefrail n=96 | Frail n=21 | Significance | |
|---|---|---|---|---|---|
| SARC-F | 0 (0-2) | 0 (0-0) | 0 (0-0) | 3 (2-4) | <0,001 |
| MNA | 26,5 (24,5-27,5) | 27 (26-28) | 26 (24,5- 27,5) | 23,5 (20-27,2) | <0,001 |
| CFS | 3 (2-3) | 3 (2-3) | 3 (2-3) | 4 (3-5) | <0,001 |
| IADL | 24 (24-24) | 24 (24-24) | 24 (24-24) | 23 (21-24) | <0,001 |
MNA- Mini Nutritional Assessment, CFS- Clinical Frailty Scale, IADL- Instrumental Activities of Daily Living.
Table 5.
Blood plasma protein, albumin, and fibrinogen concentrations stratified by phenotype frailty, SARC-F, and/or MNA classification.
Table 5.
Blood plasma protein, albumin, and fibrinogen concentrations stratified by phenotype frailty, SARC-F, and/or MNA classification.
| Robust | Pre-frail | Frail | Significance | ||
|---|---|---|---|---|---|
|
Total protein, g/L (X ± SEM) |
SARC-F 0-3 | 66.7 ± 0.7 (n=49) | 66.7 ± 0.5 (n=86) | 65.9 ± 1.4 (n=13) | P= 0.72 (frailty) P<0.01 (SARC-F) NS (both) |
| SARC-F 4-10 | 64.3 ± 2.2 (n=5) | 62.5 ± 1.6 (n=10) | 62.6 ± 1.7 (n=8) | ||
| MNA >24 | 66.5 ± 0.7 (n=48) | 66.6 ± 0.6 (n-75) | 65.7 ± 1.6 (n=10) | P=0.23 (frailty) P=0.25 (MNA) NS (both) |
|
| MNA<24 | 66.3 ± 2.1 (n=6) | 64.9 ± 1.1 (n=20) | 63.7 ± 1.5 (n=11) | ||
|
Albumin, g/L (X ± SEM) |
SARC-F 0-3 | 42.9 ± 0.5 (n=49) | 42.1 ± 0.4 (n=85) | 40.6 ± 1.0 (n=13) | P= 0.16 (frailty) P<0.01 (SARC-F) NS (both) |
| SARC-F 4-10 | 39.5 ± 1.7 (n=5) | 39.5 ± 1.2 (n=10) | 37.6 ± (n=8) | ||
| MNA >24 | 42.6 ± 0.5 (n=48) | 42.5 ± 0.4 (n=74) | 42.2 ± 1.2 (n=10) | P<0.05 (frailty) P<0.01 (MNA) NS (both) |
|
| MNA<24 | 42.5 ± 1.5 (n=6) | 39.5 ± 0.8 (n=20) | 37.8 ± 1.1 (n=11) | ||
|
Fibrynogen,g/L (X ± SEM) |
SARC-F 0-3 | 3.1 ± 0.1 (n=49) | 3.1 ± 0.1 (n=85) | 3.4 ± 0.2 (n=13) | P<0.05 (frailty) P=0.11 (SARC-F) NS (both) |
| SARC-F 4-10 | 3.3 ± 0.3 (n=5) | 3.1 ± 0.2 (n=10) | 3.8 ± 0.2 (n=8) | ||
| MNA >24 | 3.1 ± 0.1 (n=48) | 3.1 ± 0.1 (n=74) | 3.7 ± 0.2 (n=10) | P<0.05 (frailty) P=0.97 (MNA) NS (both) |
|
| MNA<24 | 3.2 ± 0.3 (n=6) | 3.1 ± 0.2 (n=20) | 3.5 ± 0.2 (n=11) |
Table 6.
Morphometric and functional assessment of patients stratified by phenotype frailty, SARC-F, and/or MNA classification.
Table 6.
Morphometric and functional assessment of patients stratified by phenotype frailty, SARC-F, and/or MNA classification.
| Robust | Pre-frail | Frail | Significance | ||
|---|---|---|---|---|---|
| Body weight, kg (X±SEM) | SARC-F 0-3 | 85.0±2.1 (n=49) | 82.2±0.5 (n=86) | 81.6±4.2 (n=13) | P=0.67 (frailty) P=0.78 (SARC-F) NS (both) |
| SARC-F 4-10 | 77.0±6.7 (n=5) | 86.8±4.7 (n=10) | 82.0±5.3 (n=8) | ||
| MNA ≥24 | 82.7±2.1 (n=48) | 83.4±1.7 (n=75) | 85.8±4.7 (n=10) | P=0.09 (frailty) P=0.80 (MNA) P<0.05 (both) |
|
| MNA <24 | 96.7±6.1 (n=6) | 79.7±3.3 (n=20) | 78.1±4.5 (n=11) | ||
| Fat-free body mass, kg (X±SEM) | SARC 0-3 | 57.9±1.3 (n=49) | 55.3±1.0 (n=85) | 55.1±2.5 (n=13) | P=0.38 (frailty) P=0.71 (SARC-F) NS (both) |
| SARC 4-10 | 50.8±4.1 (n=5) | 60.0±2.9 (n=10) | 55.1±3.2 (n=8) | ||
| MNA ≥24 | 57.4±1.3 (n=48) | 56.1±1.1 (n=75) | 56.9±2.9 (n=10) | P=0.83 (frailty) P=0.29 (MNA) NS (both) |
|
| MNA <24 | 55.9±3.8 (n=6) | 54.6±2.1 (n=20) | 53.5±2.8 (n=11) | ||
| Diaphragm thickness, mm (X±SEM) | SARC 0-3 | 3.7±0.1 (n=49) | 3.8±0.1 (n=85) | 3.6±0.2 (n=13) | P=0.11 (frailty) P=0.24 (SARC-F) P=0.05 (both) |
| SARC 4-10 | 4.1±0.4 (n=5) | 3.0±0.3 (n=10) | 3.2±0.3 (n=8) | ||
| MNA ≥24 | 3.7±0.1 (n=48) | 3.7±0.1 (n=73) | 3.2±0.3 (n=10) | P=0.48 (frailty) P=0.32 (MNA) NS (both) |
|
| MNA <24 | 3.8±0.3 (n=6) | 3.6±0.2 (n=20) | 3.7±0.3 (n=11) | ||
| Gait speed, sec/5 m (X±SEM) | SARC-F 0-3 | 3.7±0.6 (n=49) | 4.4±0.5 (n=49) | 10.9±1.2 (n=49) | P<0.01 (frailty) P=0.78 (SARC-F) P<0.01 (both) |
| SARC-F 4-10 | 5.2±1.9 (n=5) | 7.1±1.4 (n=5) | 7.6±1.5 (n=5) | ||
| MNA ≥24 | 3.8±0.6 (n=48) | 4.3±0.5 (n=75) | 13.1±1.3 (n=10) | P<0.001 (frailty) P=0.09 (MNA) P<0.001 (both) |
|
| MNA <24 | 4.0±1.7 (n=6) | 6.0±0.9 (n=20) | 6.5±1.3 (n=11) | ||
| Hand-grip strength, kg (X±SEM) | SARC-F 0-3 | 36.3±1.3 (n=49) | 29.1±1.0 (n=86) | 23.7±2.5 (n=13) | P<0.05 (frailty) P<0.05 (SARC-F) NS (both) |
| SARC-F 4-10 | 26.2±4.0 (n=5) | 27.2±2.9 (n=10) | 22.3±3.2 (n=8) | ||
| MNA ≥24 | 35.8±1.3 (n=48) | 29.3±1.1 (n=75) | 22.2±2.9 (n=10) | P<0.001 (frailty) P=0.58 (MNA) NS (both) |
|
| MNA <24 | 32.0±3.7 (n=6) | 27.9±2.1 (n=20) | 24.0±2.8 (n=11) | ||
| PEF, L/min (X±SEM) | SARC-F 0-3 | 355.0±18.9 (n=46) | 311.1±14.2 (n=82) | 301.0±35.6 (n=13) | P=0.20 (frailty) P=0.09 (SARC-F) NS (both) |
| SARC-F 4-10 | 261.0±57.4 (n=5) | 331.5±45.4 (n=8) | 209.0±45.4 (n=8) | ||
| MNA ≥24 | 348.6±19.0 (n=45) | 326.3±15.1 (n=71) | 206.6±40.2 (n=10) | P=0.17 (frailty) P=0.70 (MNA) P<0.05 (both) |
|
| MNA <24 | 324.8±52.0 (n=6) | 270.0±30.0 (n=18) | 319.9±38.4 (n=11) | ||
| FEV1, L/sec (X±SEM) | SARC-F 0-3 | 2.1±0.1 (n=46) | 1.9±0.1 (n=82) | 1.7±0.2 (n=13) | P<0.01 (frailty) P=0.62 (SARC-F) NS (both) |
| SARC-F 4-10 | 1.9±0.3 (n=5) | 2.3±0.2 (n=8) | 1.3±0.3 (n=8) | ||
| MNA ≥24 | 2.1±0.1 (n=45) | 2.0±0.1 (n=71) | 1.3±0.2 (n=10) | P<0.05 (frailty) P=0.76 (MNA) P=0.06 (both) |
|
| MNA <24 | 1.6±0.3 (n=6) | 1.9±0.2 (n=18) | 1.8±0.2 (n=11) |
Table 7.
Correlation matrix of morphometric, laboratory, and functional parameters for the entire study population.
Table 7.
Correlation matrix of morphometric, laboratory, and functional parameters for the entire study population.
| Weight (kg) | Total protein (g/L) | Albumine (g/L) |
Fibrinogen (g/L) |
Fat-free body mass (kg) | Gait speed (s/5m) |
Hand-grip strength (kg) |
PEF (L/min) | FEV1 (L) | |
|---|---|---|---|---|---|---|---|---|---|
| Weight (kg) | 1,000000 | ||||||||
| Total protein (g/L) | 0,191716 | 1,000000 | |||||||
|
Albumine (g/L) |
0,246710 | 0,660288 | 1,000000 | ||||||
| Fibrinogen (g/L) | -0,023185 | -0,059822 | -0,189781 | 1,000000 | |||||
| Fat-free body mass (kg) | 0,664106 | 0,117959 | 0,092637 | -0,077040 | 1,000000 | ||||
| Gait speed (s/5m) | 0,048854 | 0,070348 | 0,012195 | 0,181632 | 0,013272 | 1,000000 | |||
| Hand-grip strength (kg) | 0,269100 | 0,167254 | 0,190060 | -0,146748 | 0,604307 | -0,134229 | 1,000000 | ||
| PEF (L/min) | 0,213588 | 0,070256 | 0,050982 | -0,184499 | 0,401548 | -0,127684 | 0,527768 | 1,000000 | |
| FEV1 (L) | 0,148817 | 0,064965 | 0,106164 | -0,228724 | 0,404278 | -0,110982 | 0,549269 | 0,748768 | 1,000000 |
| Diaphragm thickness (mm) | 0,115202 | 0,236871 | 0,207127 | -0,074889 | 0,049726 | -0,128065 | 0,152133 | 0,157801 | 0,132104 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



