
Submitted:
22 June 2025
Posted:
24 June 2025
You are already at the latest version
Abstract
Lipedema is a chronic, estrogen-sensitive adipose tissue disorder characterized by disproportionate subcutaneous fat accumulation, fibrosis, inflammation, and resistance to fat mobilization. Despite its high prevalence, lipedema remains poorly understood and frequently misdiagnosed. This narrative review proposes a novel pathophysiological model in which menopause acts as a critical turning point in the progression of lipedema, driven by estrogen receptor imbalance (ERβ predominance over ERα), intracrine estrogen excess, and adipose tissue dysfunction. We demonstrate how menopause-induced estrogen deficiency amplifies adipose tissue dysfunction by suppressing ERα signaling, enhancing ERβ activity, and disrupting mitochondrial function, insulin sensitivity, and lipid oxidation. Concurrently, the upregulation of aromatase and 17β-HSD1, combined with the suppression of 17β-HSD2, sustains localized estradiol excess, perpetuating inflammation, fibrosis, and immune dysregulation. The molecular signature observed in lipedema closely mirrors that of other estrogen-driven gynecological disorders, such as endometriosis, adenomyosis, and uterine fibroids. Understanding these molecular mechanisms highlights the pivotal role of menopause as a catalyst for disease progression and provides a rationale for targeted therapeutic strategies, including hormonal modulation and metabolic interventions. This review reframes lipedema as an estrogen receptor–driven gynecological disorder, offering a new perspective to improve clinical recognition, diagnosis, and management of this neglected condition.
Keywords:
lipedema
; menopause
; estrogen receptors
; ERα and Erβ
; intracrine estrogen
; adipose tissue dysfunction
; aromatase
; 17β-hydroxysteroid dehydrogenase
1. Introduction
Lipedema is an inflammatory disease of the subcutaneous adipose tissue, characterized by a disproportionate, symmetrical, and painful accumulation of fat that is resistant to caloric deficit [1]. It has a strong hormonal component, with evidence suggesting an imbalance in the distribution of estrogen receptors within the adipose tissue, leading to adipocyte hypertrophy, inflammation, and fibrosis [2]. The condition tends to emerge or worsen during periods of significant hormonal fluctuation in a woman’s life, such as menarche, pregnancy, and menopause [3,4].
Menopause represents a critical window for the onset or exacerbation of cardiometabolic alterations, including increased insulin resistance, dyslipidemia, and low-grade systemic inflammation. These changes are accompanied by a progressive redistribution of body fat, with an increase in visceral adipose tissue, even in the absence of significant weight gain [5].
Consequently, the prevalence of metabolic syndrome rises substantially during the perimenopausal period, which may synergistically interact with the inflammatory microenvironment of adipose tissue affected by lipedema. This interaction further promotes endothelial dysfunction, greater fluid retention, and exacerbation of pain and resistance to fat mobilization [6].
Additionally, greater fluctuations in systemic estradiol levels during the menopausal transition profoundly affect adipose tissue metabolism by altering the expression of estrogen receptors. This shift favors a predominance of estrogen receptor beta (ERβ) over alpha (ERα), thereby amplifying local inflammation and aggravating lipedema [2,6].
Longitudinal studies indicate that the menopausal transition is associated with both structural and functional vascular changes, such as increased carotid intima-media thickness, arterial stiffness, and endothelial dysfunction [7]. Combined with the loss of estradiol’s vasodilatory and anti- inflammatory effects, these changes may further impair the already compromised microvascular and lymphatic systems in patients with lipedema, worsening venous congestion, edema, and perpetuation of chronic pain.
In this context, the present narrative review aims to critically integrate current knowledge on the hormonal influence in the pathophysiology of lipedema, with a particular focus on menopause as a clinical and molecular catalyst for disease progression. This paper will address the mechanisms of estrogen dysregulation, intracrine estrogen production, progesterone resistance, the metabolic impact of hormonal deficiency, and the therapeutic implications for managing lipedema in climacteric women.
2. Methodology
This work is a narrative review aimed at developing an integrated pathophysiological model that explains how menopause acts as a critical turning point in the clinical progression of lipedema, with a focus on estrogen receptor imbalance, intracrine estrogen production, and adipose tissue dysfunction.
The selection of literature was based on a comprehensive search of the PubMed, Scopus, and Web of Science databases up to May 2025. Keywords used included combinations of: “lipedema”, “estrogen receptors”, “ERα”, “ERβ”, “intracrine estrogen”, “adipose tissue dysfunction”, “menopause”, “aromatase”, “17β-HSD”, “progesterone resistance”, “fibrosis”, and “inflammation”. No language or date restrictions were applied to maximize the retrieval of relevant studies.
The literature included original research articles, molecular studies, clinical studies, and previous reviews that specifically addressed the molecular biology of estrogen signaling, adipose tissue endocrinology, and gynecological hormone-sensitive disorders (e.g., endometriosis, adenomyosis, and uterine fibroids) in relation to lipedema.
Articles were selected based on their relevance to the following domains:
- (1)
- estrogen receptor signaling (ERα, ERβ) in adipose tissue;
- (2)
- intracrine estrogen metabolism via aromatase, 17β-HSD1, and 17β-HSD2 enzymes;
- (3)
- the role of menopause-induced estrogen deficiency in adipose tissue dysfunction;
- (4)
- the immunometabolic consequences of receptor imbalance, including inflammation and fibrosis;
- (5)
- parallels between lipedema and other estrogen-driven gynecological disorders.
This methodology does not follow the structure of a systematic review but rather integrates mechanistic evidence from molecular endocrinology, adipose biology, and gynecology to propose a novel conceptual framework. The purpose is to advance the scientific understanding of lipedema as a hormone-driven disorder, particularly in the context of menopause.
3. Discussion
3.1. The Role of Estradiol and Its Receptors
The effect of estradiol on tissues is not absolute but depends on the functional balance between its two main nuclear receptors, ERα and ERβ, which often exert opposing and complementary actions.
ERα presents a predominantly anabolic, proliferative, and homeostatic profile, favoring the healthy expansion of subcutaneous adipose tissue, insulin sensitivity, extracellular matrix balance, and cardiovascular protection. On the other hand, ERβ acts as a negative modulator, with antiproliferative and antiadipogenic effects, functioning as a physiological brake on the effects of ERα. However, when there is pathological overexpression of ERβ—as occurs in lipedema—this balance is disrupted, leading to the loss of ERα’s beneficial effects on tissue homeostasis. This contributes to adipocyte dysfunction, chronic inflammation, fibrosis, and resistance to lipid mobilization, characterizing the pathological environment of lipedema [6,8].
The interdependence of these receptors is evidenced by the fact that both compete for the same estrogen response elements (EREs) in the DNA and for the same estradiol molecule, dynamically modulating the biological effects of the hormone. In menopause and in conditions such as lipedema, there is a reduction in ERα expression and a relative increase in ERβ expression, resulting in adipocyte dysfunction, inflammation, fibrosis, and insulin resistance [9]. This mechanism explains why estrogen deficiency leads not only to the loss of cardiovascular protection but also to metabolic deterioration and increased central adiposity.
Another relevant aspect is the capacity of subcutaneous adipose tissue to synthesize estrogens locally through steroidogenic enzymes such as aromatase (CYP19A1) and 17β-HSD, favoring a sustained autocrine/paracrine cycle of estrogenic activation. This local production could intensify signaling via ERβ, with reduced action on ERα, and consequently promote the progressive growth of the affected adipose depots. The combination of a local environment with an imbalance in estrogen receptors, increased intratissue estrogen production, and alterations in the expression of nuclear coregulators may, therefore, constitute a central axis in the pathophysiology of lipedema [3].
Under physiological conditions, there is a functional balance between ERα and ERβ receptors. However, in women with lipedema, this balance is lost. Histological studies demonstrate that in the affected areas, there is a reduction in ERα expression and a relative increase in ERβ, which leads to an alteration in local sensitivity to estrogenic action, favoring a phenotype resistant to fat mobilization [2,10,11].
Estrogen signaling in adipose tissue critically regulates the distribution of female body fat, with ERα promoting lipogenesis and triglyceride storage in the gluteofemoral regions. This regulation occurs both through increased free fatty acid uptake via activation of lipoprotein lipase (LPL) and through the suppression of lipolysis via upregulation of α2A adrenergic receptors, along with greater stimulation of angiogenesis via VEGF. This, associated with ERβ dominance—which is common in lipedema—inhibits mitochondrial biogenesis, reducing the oxidative capacity of the tissue [2].
3.2. Intracrine Production of Estradiol in Adipose Tissue
Adipose tissue acts not only as a hormonal target but as an active center of estrogen synthesis. Local estrogen production and intracrine signaling via ERα and ERβ directly influence lipogenesis, lipolysis, and tissue health in pre- and postmenopausal women, supporting the idea of an autonomous and functional hormonal microenvironment [13]. In lipedema, there is enzymatic dysregulation in the affected adipose tissue: the expression of 17β-hydroxysteroid dehydrogenase type 1 and 7—an enzyme that converts estrone into active estradiol—increases 2-fold in lipedema adipocytes [10,14], along with greater CYP19A1 (aromatase) activity. This asymmetry creates an autonomous hyperestrogenic microenvironment in lipedematous tissue, sustaining a cycle of pathological adipogenesis even in the presence of low systemic estradiol levels [2,10,11].
In menopause, there is an android redistribution of fat caused by the reduction in estradiol levels. At the same time, lipedematous tissue maintains local hyperestrogenism via overexpression of aromatase/17β-HSD1, preferentially activating ERβ, causing dysregulated adipogenesis and fibrosis [2].
3.3. Progesterone Resistance
Progesterone plays a fundamental protective role in adipose tissue homeostasis, acting on adipocyte differentiation, modulation of inflammation, and inhibition of steroidogenic enzymes [12]. However, in lipedema, there is consistent evidence of tissue resistance to progesterone, especially in the affected regions.
This resistance is manifested by the reduction in the expression and activity of 17β-HSD2, which converts active estradiol into inactive estrone. The deficiency of this enzyme keeps estradiol biologically active for a longer time, favoring continuous estrogenic signaling via ERβ and aggravating adipogenesis and chronic inflammation.
Lipedema shares pathophysiological mechanisms with several estrogen-dependent gynecological diseases, such as endometriosis, adenomyosis, and uterine fibroids [14]. These mechanisms involve increased activity of 17β-HSD1 and aromatase, which convert estrone (E₁) into estradiol (E₂), associated with the reduction of 17β-HSD caused by resistance to progesterone action, responsible for inactivating E₂ into E₁, resulting in local accumulation of estradiol in adipose tissue. This trapping of estradiol intensifies signaling via the ERβ receptor, favoring inflammation, fibrosis, and pathological expansion of adipose tissue—central characteristics of lipedema [15,16].
This mechanism creates a self-sustaining cycle of lipedema worsening. Progesterone ceases to fulfill its stabilizing function, and intracrine estradiol keeps the adipose tissue in an activated inflammatory state and resistant to regression—a scenario characteristic of lipedema, especially after menopause. More active estradiol in adipose tissue poorly responsive to progesterone perpetuates a state favorable to the progression of the disease [2,14].
3.4. How Menopause Affects Lipedema
The menopausal transition is marked by a progressive decline in estradiol levels and an alteration in the balance of estrogen receptors, with reduced ERα activity and a relative increase in ERβ.
This imbalance disrupts the homeostasis of female adipose tissue and triggers metabolic, inflammatory, and structural changes that impact both subcutaneous and visceral fat depots.(Figure 1).
Metabolically, estrogen deficiency promotes a redistribution of body fat from a gynoid to an android pattern, with visceral fat accumulation—even in the absence of weight gain. This phenomenon is associated with increased lipoprotein lipase (LPL) activity in visceral tissue, tissue hypoxia (↑HIF-1α), inflammation (↑IL-6, IL-18), and reduced lipogenesis [6,17].
In addition, a state of low-grade chronic inflammation is established, characterized by the activation of inflammatory pathways NF-κB and JNK, increased infiltration of pro-inflammatory macrophages (M1), and elevated cytokines TNF-α, IL-6, and IL-1β. At the same time, mitochondrial dysfunction reduces the basal metabolic rate, promoting sarcopenia, fat accumulation, and insulin resistance [18,19].
In the context of lipedema, this new hormonal and metabolic configuration acts as a catalyst for the disease. The imbalance between ERα (↓) and ERβ (↑)—described both in menopause and in lipedema—amplifies the anti-lipolytic, pro-inflammatory, and pro-fibrotic effects in subcutaneous adipose tissue [20,21,22]. This scenario promotes PPARγ activation, increased glucose uptake (via GLUT4) and free fatty acid uptake (via LPL), associated with suppression of lipolysis (↑αAR/↓βAR) and mitochondrial dysfunction.
Another key mechanism is the intensification of intracrine estradiol production in the affected adipose tissue, mediated by the overexpression of the enzymes aromatase and 17β-HSD1. In the absence of the systemic hormonal control typical of the reproductive years, this local pathway perpetuates adipogenesis, inflammation, and fibrosis. The coexisting progesterone resistance further worsens this scenario by reducing the activity of the enzyme 17β-HSD2, responsible for converting active estradiol into inactive estrone, thereby amplifying local estrogenic signaling [2,10,14].
From an immunological perspective, there is a shift from an anti-inflammatory phenotype— characterized by the predominance of M2 (CD163+) macrophages—to a pro-inflammatory profile, with an increase in M1 macrophages and greater expression of inflammatory cytokines such as IL-6, TNF-α, and IL-1β [14,21], which accelerates the development of fibrosis and lymphatic dysfunction.
Clinically, both the worsening of pre-existing conditions and the onset of late-onset lipedema after menopause are observed, often presenting with more severe forms that are resistant to conventional treatment [23]. This pattern is directly related to the new hormonal environment of the climacteric, characterized by systemic estradiol deficiency, ERβ dominance, progesterone resistance, and low-grade chronic inflammation. Recognizing this pattern is essential for diagnostic and early intervention strategies, especially in women in perimenopause or early menopause.
Even in the absence of weight gain, menopause promotes a preferential redistribution of fat to the visceral compartment, with a relative reduction in fat in the lower limbs. In lipedema, where subcutaneous tissue already presents inflammation, resistance to lipid mobilization, and metabolic dysfunction, the loss of estrogenic regulation worsens this condition, intensifying fat accumulation in already compromised areas [9,24].
Therefore, in the context of lipedema, menopause not only exacerbates pre-existing mechanisms—such as inflammation, fibrosis, lymphatic dysfunction, and resistance to lipid mobilization—but also acts as a trigger for the emergence of more severe and refractory forms of the disease.
3.5. Therapeutic Implications
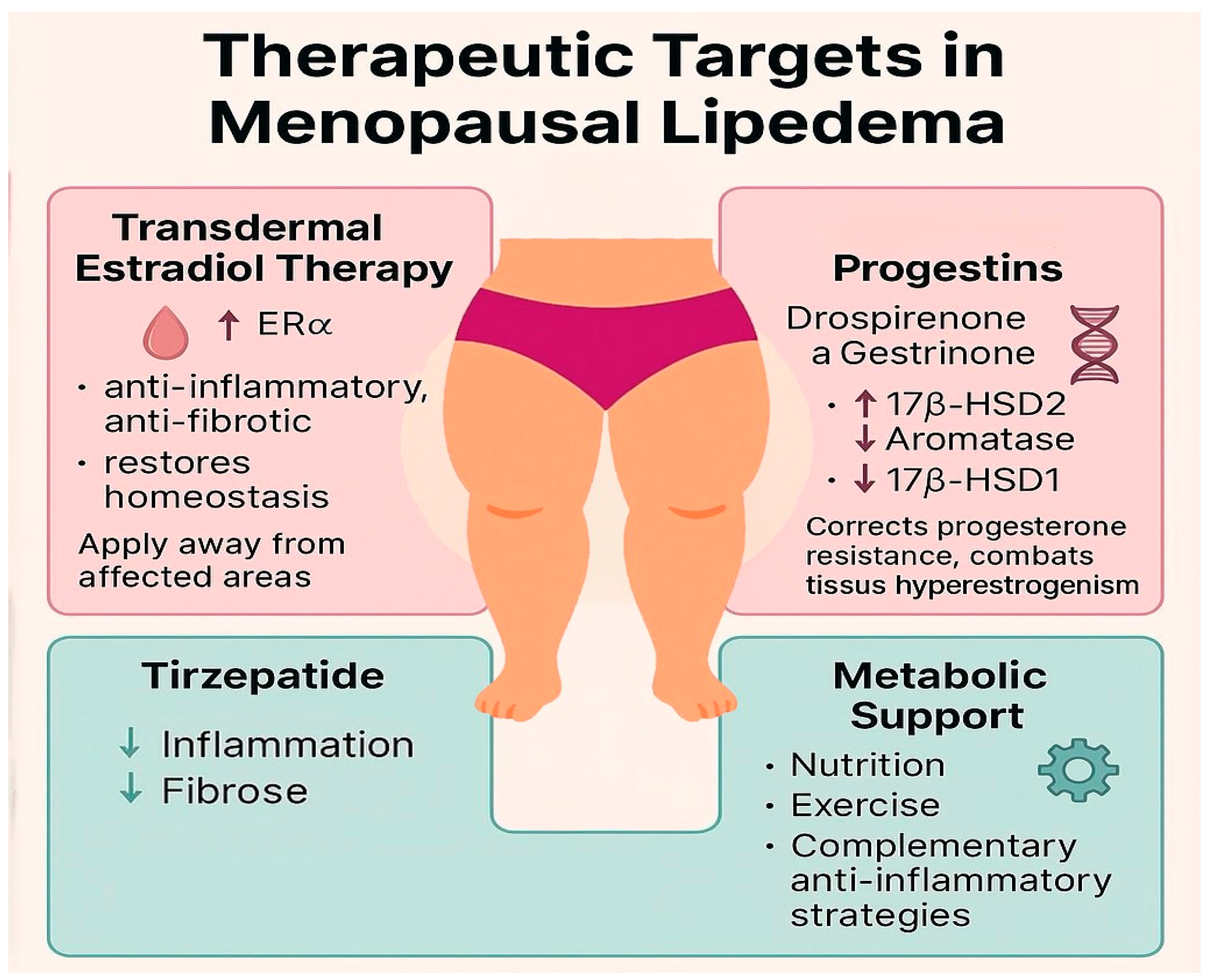
The understanding of menopause as a catalyst for the progression of lipedema profoundly redefines the therapeutic approach to this condition. The identification of specific hormonal and metabolic targets, especially in the context of estrogen deficiency during the climacteric, allows for more personalized, preventive, and potentially more effective strategies (Figure 2).
Hormone replacement therapy, especially with transdermal bioidentical estradiol, constitutes a fundamental intervention in protecting adipose tissue against the deleterious changes induced by menopause. Robust evidence indicates that estradiol, via predominant activation of the ERα receptor, plays a central role in preserving metabolic homeostasis, modulating inflammation, and preventing tissue fibrosis [6,25].
The timing of HRT initiation is a critical factor for its benefits. Starting estrogen replacement early, during the menopausal transition or in the first years after menopause, is essential to avoid dysregulation of the balance between estrogen receptors—characterized by the reduction of ERα and the relative increase of ERβ. This imbalance is central in the pathogenesis of inflammation, fibrosis, and lymphatic dysfunction observed in lipedema [7,24]. This concept, aligned with the HRT timing hypothesis, already consolidated in cardiovascular and neurocognitive health, should also be equally applied to the pathophysiology of adipose tissue.
In addition to the therapeutic window, the route of administration and the site of estradiol application are relevant clinical considerations in the context of lipedema. Given the hyperactivity of intracrine estradiol production in the affected adipose tissue—sustained by increased expression of aromatase and 17β-HSD1, along with reduced action of 17β-HSD2—the best recommendation is the use of transdermal formulations (patches or gel) applied away from regions affected by lipedema, such as the back, scapula, and inner part of the arms (if there is no disease). This approach minimizes local stimuli to dysregulated steroidogenesis, contributing to better control of inflammation and fibrosis.
The choice between progestins or progesterone depends mainly on the stage of the climacteric and the presence of associated gynecological diseases. It is known that during the menopausal transition (STRAW -2 and -1), the choice of progestins combined with estradiol use can be a good option due to the fluctuations of estradiol in this phase. Progestins would have a central effect in reducing the amplitude of pulsatile LH and FSH secretion, minimizing the risk of bleeding associated with HRT, and they also have greater efficacy in the HRT of women with gynecological diseases such as adenomyosis, endometriosis, and uterine fibroids. Among the progestins that may be effective in lipedema, there are two: Drospirenone and Gestrinone [17,26].
Drospirenone is a fourth-generation progestin derived from spironolactone, which combines antiandrogenic and antimineralocorticoid properties, as well as modulatory effects on inflammation and adipose tissue metabolism. Its main benefit in lipedema lies in its ability to act on progesterone resistance, which is one of the physiopathological pillars of the disease, in addition to offering direct anti-inflammatory effects via activation of progesterone receptors, especially PRβ. This activation leads to the reduction of pro-inflammatory cytokines such as TNF- α and IL-1β and to the increase of anti-inflammatory cytokines such as IL-10 [14,27].
In addition, drospirenone exerts a significant anti-adipogenic effect, inhibiting the differentiation of preadipocytes and the accumulation of triglycerides, an effect that occurs mainly through the antagonism of mineralocorticoid receptors [32]. This directly impacts the tissue environment of lipedema, helping to reduce fluid retention, chronic inflammation, and fibrosis, especially in the more advanced stages of the disease. Data in postmenopausal women suggest that the association of drospirenone with estradiol improves fat distribution, reduces central fat mass, and improves the adipokine profile—effects that can be highly relevant in the metabolic and tissue management of lipedema [14,30].
Gestrinone is a synthetic progestogen with a potent modulatory action on intracrine steroidogenesis, having been used for decades in the treatment of estrogen-dependent gynecological conditions such as endometriosis, adenomyosis, and uterine fibroids. Its action in lipedema occurs precisely because it shares pathophysiological mechanisms with these diseases, especially in the context of progesterone resistance, aromatase overexpression, and the imbalance of the enzymes 17β-HSD1 (increased) and 17β-HSD2 (reduced). Gestrinone exerts a direct effect by inhibiting aromatase and 17β-HSD1, while simultaneously increasing the expression of 17β-HSD2, favoring the conversion of estradiol (E2) into estrone (E1), which has much lower estrogenic potency. This effect reduces the hyperstimulation of estradiol receptors, particularly ERβ in adipose tissue, which is one of the drivers of inflammation, fibrosis, and lipedema expansion [14].
In addition to its effects on estradiol metabolism, gestrinone acts on overcoming progesterone resistance by stimulating the expression of PRβ receptors, which helps restore local hormonal balance. Consequently, there is a reduction in chronic inflammation, fibrosis, and the uncontrolled expansion of the affected adipose tissue. Contrary to common assumptions, its benefits in lipedema are not related to the androgenic or anabolic effects of the molecule but rather to its ability to reorganize pathological intracrine hormonal signaling, bringing control over disease progression, especially in women with associated gynecological comorbidities [14,26].
In women with established menopause, the use of micronized progesterone (P4) is possible and viable. It plays an essential role in endometrial protection and neuroendocrine modulation, but its effects on adipose tissue affected by lipedema are considered metabolically neutral, with no direct impact on the pathophysiological mechanisms of the disease. Unlike synthetic progestins such as drospirenone and gestrinone, which act directly on intracrine modulation, P4 does not present relevant action on these enzymes, nor antiadipogenic, antifibrotic, or robust anti- inflammatory effects in adipose tissue [15,16,31]. Studies show that despite the presence of progesterone receptors in subcutaneous adipose tissue [15], the activation of these receptors by natural progesterone is not sufficient to reverse the pattern of progesterone resistance observed in lipedema, nor to modulate the local expression of aromatase and 17β-HSD enzymes, which are critical in perpetuating tissue hyperestrogenism. P4 has a safe and well-established role in endometrial protection within hormone replacement therapy, as well as in the modulation of sleep, anxiety, and neuroprotection, but it does not exert a therapeutic impact on inflammation, fibrosis, or adipocyte expansion characteristic of lipedema, unlike progestins such as drospirenone and gestrinone, which have proven additional mechanisms on these metabolic pathways [28,32].
Metabolic treatment is also a fundamental pillar in the management of lipedema, especially during the climacteric. Tirzepatide represents an emerging therapeutic strategy with high potential in the management of lipedema [33], particularly when associated with the metabolic and hormonal changes of the climacteric. Both conditions share central pathophysiological mechanisms such as low-grade chronic inflammation, tissue fibrosis, mitochondrial dysfunction, insulin resistance, and pathological remodeling of subcutaneous adipose tissue, which are amplified by the menopausal transition.
The menopausal transition, in turn, worsens these mechanisms through the reduction of systemic estradiol levels, intensification of insulin resistance, mitochondrial dysfunction, and increased central adiposity, creating an unfavorable metabolic environment that acts as a catalyst for the progression of lipedema [34].
In this context, tirzepatide, a dual agonist of GLP-1 and GIP receptors, offers an action profile that simultaneously addresses the metabolic and inflammatory dysfunctions common to lipedema and the climacteric. Its anti-inflammatory effects are mediated by modulating macrophage polarization, with a reduction of the pro-inflammatory M1 phenotype and an increase of the anti- inflammatory M2 phenotype, in addition to inhibiting crucial inflammatory pathways such as ERK and NF-κB, and reducing the expression of pro-inflammatory cytokines including TNF-α, IL-6, and MCP-1 [35,36].
At the same time, tirzepatide exerts antifibrotic effects and highly relevant metabolic reprogramming in the pathophysiology of lipedema and metabolic syndrome of the climacteric. Experimental data demonstrate its ability to stimulate thermogenesis through the induction of the mitochondrial uncoupling protein UCP1 in brown adipose tissue, favoring increased energy expenditure and the conversion of white adipocytes into beige adipocytes [38]. Moreover, GIP receptor activation promotes the mobilization of resistant subcutaneous fat, characteristic of lipedema, with improvement in mitochondrial function, increased lipid oxidation, and regulation of genes involved in energy homeostasis and extracellular matrix remodeling [37,38].
These effects transcend simple weight control. By acting on metabolic, inflammatory, and fibrotic pathways, tirzepatide offers unique benefits in the context of lipedema associated with the climacteric—a condition in which fat accumulation is not merely the result of a positive energy balance but rather of a complex hormonal, inflammatory, and bioenergetic dysfunction sustained by intracrine estrogen production, estrogen receptor imbalance, and progesterone resistance.
Results already consolidated in models of other fibrotic and metabolic diseases—such as metabolic-associated steatohepatitis (MASH) and heart failure with preserved ejection fraction (HFpEF)—corroborate the potential of tirzepatide in reducing not only adipose tissue volume but also in attenuating processes of chronic inflammation, fibrosis, and mitochondrial dysfunction, which are directly implicated in the progression of lipedema during the climacteric [39].
Therefore, by integrating metabolic, anti-inflammatory, antifibrotic, and tissue reprogramming effects, tirzepatide stands out as a therapeutic intervention with unique potential to address the clinical challenges imposed by the intersection of lipedema with the metabolic and hormonal changes of menopause, offering a physiopathologically grounded and metabolically restorative approach.
4. Conclusions
This narrative review, despite its limitations—especially for being a narrative review based on pathophysiological models and observational data still lacking robust validation in clinical trials specific to lipedema—offers an expanded and coherent understanding of the mechanisms that make menopause a critical point in the progression of the disease.
The systemic decline of estradiol, combined with the exacerbated intracrine production of estradiol in the affected adipose tissue—sustained by the overexpression of aromatase and 17β- HSD1 and the deficiency of 17β-HSD2—associated with the imbalance of estrogen receptors (ERβ > ERα), creates a hormonal and inflammatory microenvironment that accelerates processes of adipocyte hypertrophy, inflammation, fibrosis, and resistance to lipid mobilization.
In addition to hormonal mechanisms, menopause induces profound metabolic changes, with increased insulin resistance, low-grade chronic inflammation, mitochondrial dysfunction, and redistribution of fat to the visceral compartment—phenomena that synergistically add to the pathophysiology of lipedema, making this phase of life particularly critical for disease progression.
In this scenario, it becomes evident the need for strategic therapeutic changes during the climacteric. Transdermal hormone therapy with estradiol, as long as it is applied away from the affected areas (such as the back and the inner part of the arms), emerges as a central intervention in modulating the imbalance between ERα and ERβ, in protecting against inflammation, and in preventing fibrosis.
Equally important, the use of progestins with metabolic and anti-inflammatory action, such as drospirenone and gestrinone, goes beyond endometrial protection. These molecules act directly on the modulation of progesterone resistance, the reduction of aromatase and 17β-HSD1, and the partial restoration of intracrine balance, combating the mechanisms that sustain the progression of lipedema.
Complementing this therapeutic axis, tirzepatide emerges as an innovative metabolic strategy with unique benefits in the context of climacteric lipedema. By acting on the GLP-1 and GIP pathways, tirzepatide offers multiple effects aligned with the main metabolic dysfunctions of menopause and lipedema, including: reduction of insulin resistance; improvement of mitochondrial function; activation of thermogenesis and increased energy expenditure; reduction of chronic inflammation and tissue fibrosis; and a direct action in adipose tissue remodeling, breaking the cycle of inflammation-fibrosis-hypertrophy.
Unlike isolated GLP-1 analogs, the dual action of tirzepatide allows not only fat loss but also the partial reversal of the tissue dysfunction characteristic of lipedema, especially when this dysfunction is amplified by the hormonal and metabolic changes of the climacteric.
Therefore, recognizing menopause as a decisive pathophysiological milestone in lipedema not only strengthens the understanding of the mechanisms of disease worsening but also redefines the therapeutic approach. The integration of personalized hormonal modulation (transdermal estradiol and specific progestins) with advanced metabolic interventions, such as tirzepatide, constitutes a concrete opportunity to transform the care of these women into a scientific, individualized, and more effective strategy.
5. Limitation
This review is based on an integrative pathophysiological model derived from observational data, molecular biology, and extrapolations from related estrogen-dependent disorders. Despite the biological plausibility and strong mechanistic rationale, the lack of specific randomized clinical trials in lipedema populations represents a limitation. Future studies should aim to validate these mechanisms and the proposed therapeutic interventions.
References
- Wold LE, Hines EA Jr, Allen EV. Lipedema of the legs; a syndrome characterized by fat legs and edema. Ann Intern Med. 1951 May;34(5):1243-50. [CrossRef] [PubMed]
- Katzer K, Hill JL, McIver KB, Foster MT. Lipedema and the Potential Role of Estrogen in Excessive Adipose Tissue Accumulation. Int J Mol Sci. 2021 Oct 29;22(21):11720. [CrossRef] [PubMed] [PubMed Central]
- Forner-Cordero I, Szolnoky G, Forner-Cordero A, Kemény L. Lipedema: an overview of its clinical manifestations, diagnosis and treatment of the disproportional fatty deposition syndrome - systematic review. Clin Obes. 2012 Jun;2(3-4):86-95. Epub 2012 Aug 3. [CrossRef] [PubMed]
- Torre YS, Wadeea R, Rosas V, Herbst KL. Lipedema: friend and foe. Horm Mol Biol Clin Investig. 2018 Mar 9;33(1):/j/hmbci.2018.33.issue-1/hmbci-2017-0076/hmbci-2017-0076.xml. [CrossRef] [PubMed] [PubMed Central]
- Santoro N, Sutton-Tyrrell K. The SWAN song: Study of Women's Health Across the Nation's recurring themes. Obstet Gynecol Clin North Am. 2011 Sep;38(3):417-23. [CrossRef] [PubMed] [PubMed Central]
- Simpson ER, Merrill JC, Hollub AJ, Graham-Lorence S, Mendelson CR. Regulation of estrogen biosynthesis by human adipose cells. Endocr Rev. 1989 May;10(2):136-48. [CrossRef] [PubMed]
- El Khoudary SR, Aggarwal B, Beckie TM, Hodis HN, Johnson AE, Langer RD, Limacher MC, Manson JE, Stefanick ML, Allison MA; American Heart Association Prevention Science Committee of the Council on Epidemiology and Prevention; and Council on Cardiovascular and Stroke Nursing. Menopause Transition and Cardiovascular Disease Risk: Implications for Timing of Early Prevention: A Scientific Statement From the American Heart Association. Circulation. 2020 Dec 22;142(25):e506-e532. Epub 2020 Nov 30. [CrossRef] [PubMed]
- Ahmed F, Kamble PG, Hetty S, Fanni G, Vranic M, Sarsenbayeva A, Kristófi R, Almby K, Svensson MK, Pereira MJ, Eriksson JW. Role of Estrogen and Its Receptors in Adipose Tissue Glucose Metabolism in Pre- and Postmenopausal Women. J Clin Endocrinol Metab. 2022 Apr 19;107(5):e1879-e1889. [CrossRef] [PubMed] [PubMed Central]
- Foryst-Ludwig A, Kintscher U. Metabolic impact of estrogen signalling through ERalpha and ERbeta. J Steroid Biochem Mol Biol. 2010 Oct;122(1-3):74-81. Epub 2010 Jul 3. [CrossRef] [PubMed]
- Szél E, Kemény L, Groma G, Szolnoky G. Pathophysiological dilemmas of lipedema. Med Hypotheses. 2014 Nov;83(5):599-606. Epub 2014 Aug 23. [CrossRef] [PubMed]
- Poojari, A.; Dev, K.; Rabiee, A. Lipedema: Insights into Morphology, Pathophysiology, and Challenges. Biomedicines 2022, 10, 3081. [CrossRef] [PubMed]
- O'Brien SN, Welter BH, Mantzke KA, Price TM. Identification of progesterone receptor in human subcutaneous adipose tissue. J Clin Endocrinol Metab. 1998 Feb;83(2):509-13. [CrossRef] [PubMed]
- DiSilvestro D, Petrosino J, Aldoori A, Melgar-Bermudez E, Wells A, Ziouzenkova O. Enzymatic intracrine regulation of white adipose tissue. Horm Mol Biol Clin Investig. 2014 Jul;19(1):39-55. [CrossRef] [PubMed] [PubMed Central]
- Viana DPC, Câmara LC. Hormonal links between lipedema and gynecological disorders: therapeutic roles of gestrinone and drospirenone. J Adv Med Med Res. 2025;37(24):1–9. [CrossRef]
- Zeitoun K, Takayama K, Sasano H, Suzuki T, Moghrabi N, Andersson S, Johns A, Meng L, Putman M, Carr B, Bulun SE. Deficient 17beta-hydroxysteroid dehydrogenase type 2 expression in endometriosis: failure to metabolize 17beta-estradiol. J Clin Endocrinol Metab. 1998 Dec;83(12):4474-80. [CrossRef] [PubMed]
- Cooke PS, Nanjappa MK, Ko C, Prins GS, Hess RA. Estrogens in male physiology. J Clin Endocrinol Metab. 1997;82(2):379–84. [CrossRef]
- Kuryłowicz A. Estrogens in Adipose Tissue Physiology and Obesity-Related Dysfunction. Biomedicines. 2023 Feb 24;11(3):690. [CrossRef] [PubMed] [PubMed Central]
- Renke G, Kemen E, Scalabrin P, Braz C, Baesso T, Pereira MB. Cardio-Metabolic Health and HRT in Menopause: Novel Insights in Mitochondrial Biogenesis and RAAS. Curr Cardiol Rev. 2023;19(4):e060223213459. [CrossRef] [PubMed] [PubMed Central]
- Geraci A, Calvani R, Ferri E, Marzetti E, Arosio B, Cesari M. Sarcopenia and Menopause: The Role of Estradiol. Front Endocrinol (Lausanne). 2021 May 19;12:682012. [CrossRef] [PubMed] [PubMed Central]
- Yang W, Jiang W, Liao W, Yan H, Ai W, Pan Q, Brashear WA, Xu Y, He L, Guo S. An estrogen receptor α-derived peptide improves glucose homeostasis during obesity. Nat Commun. 2024 Apr 22;15(1):3410. [CrossRef] [PubMed] [PubMed Central]
- Lizcano F, Guzmán G. Estrogen Deficiency and the Origin of Obesity during Menopause. Biomed Res Int. 2014;2014:757461. Epub 2014 Mar 6. [CrossRef] [PubMed] [PubMed Central]
- Clegg DJ, Brown LM, Woods SC, Benoit SC. Gonadal hormones determine sensitivity to central leptin and insulin. Diabetes. 2006;55(4):978–87. [CrossRef]
- Tomada I. Lipedema: From Women’s Hormonal Changes to Nutritional Intervention. Endocrines. 2025;6(2):24. [CrossRef]
- Pernoud LE, Gardiner PA, Fraser SD, Dillon-Rossiter K, Dean MM, Schaumberg MA. A systematic review and meta-analysis investigating differences in chronic inflammation and adiposity before and after menopause. Maturitas. 2024 Dec;190:108119. Epub 2024 Sep 26. [CrossRef] [PubMed]
- Kim JH, Cho HT, Kim YJ. The role of estrogen in adipose tissue metabolism: insights into glucose homeostasis regulation. Endocr J. 2014;61(11):1055-67. [CrossRef] [PubMed]
- Renke G, Antunes M, Sakata R, Tostes F. Effects, Doses, and Applicability of Gestrinone in Estrogen-Dependent Conditions and Post-Menopausal Women. Pharmaceuticals (Basel). 2024 Sep 22;17(9):1248. [CrossRef] [PubMed] [PubMed Central]
- Makabe T, Koga K, Miyashita M, Takeuchi A, Sue F, Taguchi A, Urata Y, Izumi G, Takamura M, Harada M, Hirata T, Hirota Y, Wada-Hiraike O, Fujii T, Osuga Y. Drospirenone reduces inflammatory cytokines, vascular endothelial growth factor (VEGF) and nerve growth factor (NGF) expression in human endometriotic stromal cells. J Reprod Immunol. 2017 Feb;119:44-48. Epub 2016 Dec 29. [CrossRef] [PubMed]
- Caprio M, Antelmi A, Chetrite G, Muscat A, Mammi C, Marzolla V, Fabbri A, Zennaro MC, Fève B. Antiadipogenic effects of the mineralocorticoid receptor antagonist drospirenone: potential implications for the treatment of metabolic syndrome. Endocrinology. 2011 Jan;152(1):113-25. Epub 2010 Nov 17. [CrossRef] [PubMed]
- Tankó LB, Christiansen C. Effects of 17beta-oestradiol plus different doses of drospirenone on adipose tissue, adiponectin and atherogenic metabolites in postmenopausal women. J Intern Med. 2005 Dec;258(6):544-53. [CrossRef] [PubMed]
- Karakus, S., et al. (2012). Effects of drospirenone plus estradiol on body fat distribution in postmenopausal women. Climacteric, 15(1), 42–48. [CrossRef]
- Stuenkel CA. Menopausal Hormone Therapy and the Role of Estrogen. Clin Obstet Gynecol. 2021 Dec 1;64(4):757-771. [CrossRef] [PubMed]
- Stuenkel, C. A., et al. (2015). Treatment of symptoms of the menopause: An Endocrine Society Clinical Practice Guideline. Journal of Clinical Endocrinology & Metabolism, 100(11), 3975–4011. [CrossRef]
- Viana, D. P. C., & Câmara, L. C. (2025, February 28). Metabolic therapy for lipedema: Can tirzepatide overcome the treatment gap? Journal of Pharmaceutical Research International, 37(3), 21–28.
- Jeong, H. G., & Park, H. (2022, October 8). Metabolic disorders in menopause. Metabolites, 12(10), 954. [CrossRef]
- Xia Y, Jin J, Sun Y, Kong X, Shen Z, Yan R, Huang R, Liu X, Xia W, Ma J, Zhu X, Li Q, Ma J. Tirzepatide's role in targeting adipose tissue macrophages to reduce obesity- related inflammation and improve insulin resistance. Int Immunopharmacol. 2024 Dec 25;143(Pt 2):113499. Epub 2024 Oct 29. [CrossRef] [PubMed]
- Wynn TA, Vannella KM. Macrophages in Tissue Repair, Regeneration, and Fibrosis. Immunity. 2016 Mar 15;44(3):450-462. [CrossRef] [PubMed] [PubMed Central]
- Samms RJ, Zhang G, He W, Ilkayeva O, Droz BA, Bauer SM, Stutsman C, Pirro V, Collins KA, Furber EC, Coskun T, Sloop KW, Brozinick JT, Newgard CB. Tirzepatide induces a thermogenic-like amino acid signature in brown adipose tissue. Mol Metab. 2022 Oct;64:101550. Epub 2022 Jul 31. [CrossRef] [PubMed] [PubMed Central]
- Regmi, A., Aihara, E., Christe, M. E., Varga, G., Beyer, T. P., Ruan, X., Beebe, E., O’Farrell, L. S., Bellinger, M. A., Austin, A. K., Lin, Y., Hu, H., Konkol, D. L., Wojnicki, S., Holland, A. K., Friedrich, J. L., Brown, R. A., Estelle, A. S., Badger, H. S., Gaidosh, G. S., Kooijman, S., Rensen, P. C. N., Coskun, T., Thomas, M. K., & Roell, W. (2024). Tirzepatide modulates the regulation of adipocyte nutrient metabolism through long-acting activation of the GIP receptor. Cell Metabolism, 36(7), 1534–1549.e7.
- Cifarelli V. Lipedema: Progress, Challenges, and the Road Ahead. Obes Rev. 2025 May 27:e13953. Epub ahead of print. [CrossRef] [PubMed]
Figure 1.
Menopause as a driver of lipedema progression. Hormonal imbalance (↓ERα / ↑ERβ), insulin resistance, mitochondrial dysfunction, and immune dysregulation (M1 macrophage predominance) converge to exacerbate adipocyte dysfunction, inflammation, fibrosis, edema, and pain in lipedema.
Figure 1.
Menopause as a driver of lipedema progression. Hormonal imbalance (↓ERα / ↑ERβ), insulin resistance, mitochondrial dysfunction, and immune dysregulation (M1 macrophage predominance) converge to exacerbate adipocyte dysfunction, inflammation, fibrosis, edema, and pain in lipedema.
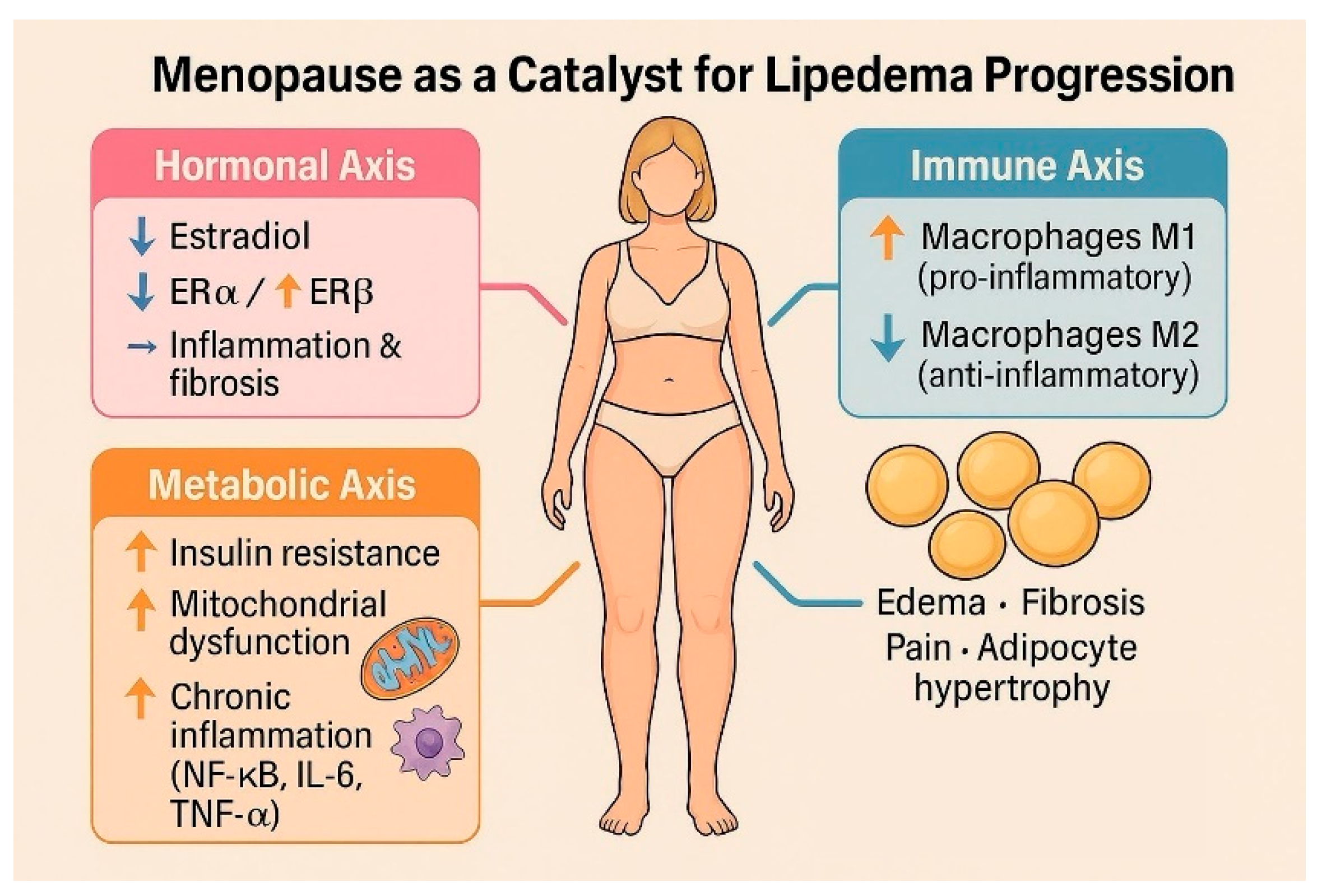
Figure 2.
Therapeutic strategies for menopausal lipedema. An integrated approach combining transdermal estradiol therapy (to restore ERα signaling), targeted progestins (drospirenone or gestrinone) to modulate intracrine estrogen production and progesterone resistance, tirzepatide for metabolic and antifibrotic effects, and lifestyle-based metabolic support.
Figure 2.
Therapeutic strategies for menopausal lipedema. An integrated approach combining transdermal estradiol therapy (to restore ERα signaling), targeted progestins (drospirenone or gestrinone) to modulate intracrine estrogen production and progesterone resistance, tirzepatide for metabolic and antifibrotic effects, and lifestyle-based metabolic support.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



