Submitted:
19 June 2025
Posted:
23 June 2025
You are already at the latest version
Abstract
Objective: This randomized controlled trial evaluated the efficacy of lavender-neroli oil aromatherapy in managing dental anxiety and pain in children undergoing inferior alveolar nerve block (IANB) anesthesia. Methods: Fifty-four children aged 6–11 years were randomly assigned to either a control group or an aromatherapy group. Children in the intervention group inhaled lavender-neroli oil via a nitrous oxide nasal mask for 5 minutes before and during IANB administration. Anxiety and pain levels were assessed pre- and post-treatment using the Facial Image Scale (FIS), Face-Legs-Activity-Cry-Consolability (FLACC) scale, and vital signs (heart rate, blood pressure, oxygen saturation). Results: Results demonstrated significantly lower anxiety, heart rate, blood pressure, and pain scores in the aromatherapy group compared to the control group (p < 0.05), with no significant change in oxygen saturation. Conclusions: Lavender-neroli aromatherapy is a safe, low-cost, and effective adjunct to reduce anxiety and discomfort during pediatric dental anesthesia.
Keywords:
pediatric dentistry
; aromatherapy
; lavender-neroli oil
; dental anxiety
1. Introduction
Dental anxiety is a prevalent and persistent issue among children, often hindering their ability to receive appropriate dental care. With reported prevalence ranging from 13% to 23.9% [1,2], anxiety significantly impacts children’s willingness to undergo dental procedures [3]. Triggers include the visual and tactile presence of needles, high-pitched sounds of dental handpieces, and distinctive odors associated with dental materials [4,5].
The dental environment contains many anxious sensory stimuli, such as the sight and sensation of the needle, the sight and sounds of handpieces, and the smell of dental materials (eugenol, the smell associated with drilling) [4,5].
Children with elevated dental fear are more likely to present with untreated caries and compromised oral health due to avoidance behaviors. This emphasizes the necessity of managing pediatric dental anxiety to ensure successful treatment outcomes [6].
Many pharmacological and non-pharmacological methods have been used to elevate dental anxiety. Some parents reject pharmacological techniques, including nitrous oxide and general anesthesia, due to the risks associated with them in comparison to the importance of primary teeth maintenance and the need for specialized equipment [7]. Moreover, with pharmacological methods, even with the presence of specialists, life-threatening risks can occur, such as loss of protective airway reflex, cardiovascular instability, and respiratory depression [8].
Recently, the effectiveness of aromatherapy as one of the complementary alternative medicines has been suggested for reducing anxiety and pain during medical procedures [9,10,11].
Aromatherapy seeks to achieve therapeutic benefits such as increased calmness, improved physical well-being, and reduction in anxiety and pain. It relies on essential oils extracted from raw plant materials, which are defined as the cultivated plant parts that naturally produce essential oils. These parts may include flowers, leaves, peels, fruits, bark, or seeds [11,12]. Furthermore, aromatherapy has garnered attention for its potential to reduce anxiety, attributed to its perceived safety profile with minimal side effects, ease of application, and affordability compared to synthetic drugs [13].
Essential oils are a mixture of different compounds that enter the body by inhalation, skin massages, baths, and orally to obtain analgesic, anxiolytic, sedative, and inflammation effects [14]. Inhalation is the most common way associated with aromatherapy and affects the smell sense [15], as the odor from essential oils can affect the limbic system, where emotions develop in the brain, including the amygdala and hippocampus, and produce anxiolytic effects [16].
Lavender oil extract from Lavandula angustifolia flowers is one of the most important essential oils used in aromatherapy, gaining popularity due to its anxiolytic, analgesic, and sedative properties [17]. It belongs to the Lamiaceae family with sedative activity due to its constituents of linalool and linalyl acetate [18]. Neroli is an essential oil extracted by hydrodistillation from citrus aurantium or bitter orange flowers, which belong to the Rutaceae family [19]. It's widely used in aromatherapy due to its effect on the central nervous system, including sedative, analgesic, and anti-inflammation properties [20].
Recently, several studies have shown the effectiveness of contemporary alternative approaches, such as aromatherapy with multiple essential oils, in reducing anxiety and pain during needle insertion in healthy volunteers, hemodialyzed patients, and children [9,11]. Moreover, the effect of aromatherapy in reducing dental anxiety has been studied in waiting rooms [21,22]. As for the pediatric patient, it has been studied during prophylaxis and invasive dental treatment [23,24,25,26,27], where these studies mostly used lavender or sweet orange oils only. However, no study has focused on the effectiveness of an essential oils mixture on children’s anxiety during anesthesia injection. In a previous study, lavender with neroli oil was used as a blend in combination with music therapy during IANB injection in children [28]. This study aimed to investigate the efficacy of a lavender-neroli oil mixture alone, without other factors, in reducing dental anxiety, vital signs, and pain during inferior alveolar nerve block (IANB) anesthesia injections in children.
2. Materials and Methods
2.1. Study Design, Settings, and Ethical Approval
This single-blinded, randomized clinical trial employed a two-arm, parallel superiority design with a 1:1 allocation ratio, conducted from October 2021 to January 2023 at the Department of Pediatric Dentistry. This study adhered to the ethical guidelines of the Declaration of Helsinki and its later amendments and received ethical approval from the Local Research Ethics Committee of the Faculty of Dentistry (Approval No. UDDS-502-220420121/SRC-3183). The project was registered at the clinical trials government with an identifier (NCT05759286) on 08/03/2023.
2.2. Sample Size Calculation
The sample size was estimated using G* Power 3.1.9.4 (Heinrich-Heine-Universität, Düsseldorf, Germany) based on the changes in pulse rate values. A minimum total sample size of 54 patients (27 in each group) was found to be sufficient for a level of significance of 0.05, a power of 85%, and an effect size estimated from previous research [29].
2.3. Recruitment and Eligibility Criteria
Two hundred and fifteen children aged between 6 and 11 years were referred to the Department of Pediatric Dentistry during the study period for a dental procedure in the mandibular jaw. The children were investigated by the principal investigator (R.Ab.), who searched for healthy children who have sufficient cognitive skills to complete the self-report scale, who need dental treatment recommended anesthesia with alveolar nerve block injection, and who recorded grade 2 on the Frankel behavior scale (positive). One-hundred and fifty children met these inclusion criteria. Children were excluded if parents refused to participate in this study, if children had asthma, cold, or any respiratory hypersensitive, if children took analgesics or NSAIDs in the last 8 hours if children had a mental or physical disability, and those who had allergic to the used oils in this study. Finally, fifty-four children were included in the current study. All included children whose parents agreed to participate in the study signed an informed consent sheet after hearing all of the details about the trial and its therapeutic nature.
Collecting patients was done over 6 months between June and November 2022. However, the long period for this research was due to registering the research and obtaining ethical approval from the Damascus University committee, preparing research material and choosing the appropriate blends and methods, collecting information and references, and writing the paper.
2.4. Randomization
Children were assigned to the control group, or the aromatherapy group, using the simple randomization method at an allocation ratio of 1:1, and a random sequence was created by (Y.A.T) using the website www.random.org, which was accessed on 10 October 2021.
Thus, children were assigned to two groups: Group 1, the control group (n=27), and Group 2, the aromatherapy group (n=27).
2.5. Blinding
As the current study was an interventional study, the treating clinician was aware of whether the child had undergone aromatherapy or not due to the aromatic spread of the essential oils in the treatment room. Moreover, the children involved in this study were not blinded. Although children in both groups wear an aromatherapy mask, they will be aware if they smell essential oils or not. The assessment of the treatment outcomes was completed by two trained Ph.D. student researchers who were calibrated to the evaluation criteria and blinded to the type of therapy that is used, where children of both groups wear a modified nitrous mask. The assessment was done by viewing a video recorded from a camera mounted over the patient's head showing the vital signs meter and the patient's body for objective pain assessment, where the assessors had previously good experience in using the FLACC scale. The inter-rater reliability for assessors was tested using the Kappa statics, which revealed high compatibility for both assessors 0.932 and 0.879 [30].
2.6. Intervention Procedures
After taking demographic information and being informed by parents, the children were randomly divided into two groups.
Control group: The child was asked to put the nasal nitrous oxide mask with the box on it, which was empty and didn’t include any aroma as a placebo effect.
Aromatherapy group: First, a mixture of lavender-neroli oils was prepared by a specialist in the Faculty of Pharmacology Department of Pharmacognosy (R.Al.). Essential oils were obtained from (Biocham Natural Extract.co, Damascus, Syria). (100% lavender oil (L. Angustifolia), and 100% neroli oil (citrus arauntium)).
The main components of essential oils were determined by Gas Chromatography (GC) and found to be 37% linalool, 11.6% camphor, 9.9% 1.8 cineole, 5.5% linalyl acetate in lavender oil, and 23.4% linalool, 15.5% linalyl acetate,12.3% trans-Nerolidol, 11.9% limonene, 7.7% β pinene in neroli oils, this data was provided by the delivering company. The main components of lavender oil, including linalool and linalyl acetate, were confirmed using Gas Chromatography (GC), consistent with prior literature [Wang & Heinbockel, 2018].
2.3 mL of lavender oil was mixed with 0.9 mL of neroli oil, and the total mixture was diluted to 20 mL using grapeseed oil.
In the dental treatment, the child was asked to inhale the aroma of the oil mixture through a modified nasal nitrous oxide mask (Accturon, Hu-Friedy Mfg. Co., LLC). A 3D printed box, which was perforated from the top and bottom to allow passing the air, was applied on the circle hole of the mask; three drops of the oil mixture were poured by a disposable pipette with a 3 mm tip diameter (Sunnypack, Dallas, Australia) on three cotton balls which were put in the box cavity (Figure 1; A, B, and C).
Children in this group inhaled the aromatic oils for 5 minutes before and during anesthesia using special masks that differed from the masks in the control group. They were treated in a different room from the children of the control group for the children of the control group not to be affected by the trace of essential oils remaining in the masks or the room of the aromatherapy group (Figure 1 D). The 5-minute inhalation period was selected based on prior research suggesting that short-term exposure (3–5 minutes) to essential oil vapors is sufficient to elicit a measurable psychophysiological calming effect in children [Wajda et al., 2017]. Additionally, pilot observations during protocol development indicated that children responded positively within this timeframe.
Children in both groups received IANB injections by the same research using lidocaine 2% with 1:80000 epinephrine (Huons Lidocaine HCL, Seoul, Korea) and a 27-gauge needle (Kohope, Shanghai, China), which was used at a depth of 15 ml where 1ml of the anesthetic’s solution was injected [31].
2.7. Outcomes and Measurements
Dental anxiety and pain scores were defined as primary outcome measures, whereas vital signs, blood pressure, heart rate, and oxygen saturation were considered secondary outcome measures.
A dental anxiety assessment was conducted using the Facial Image Scale (FIS). It consists of a row of 5 faces ranging from very happy to very sad, and the child points to the face that reflects his feelings. The scale scored 1 to the most positive face and 5 to the most negative face [32,33].
The Arabic version of the Face-Legs-Arms-Cry-Consolability (FLACC) scale was used to measure pain during anesthesia injection, as it is a reliable tool to assess pain in children aged between 6 and 14 years in dental treatment [34]. Five pain behaviors are included in FLACC; each category of behavior is measured on a 0-2 scale, so the hole scale scores ranged between 0-10 [2].
For vital signs, heart rate and oxygen saturation were recorded using pulse oximeters (Meditech Equipment, Shandong, China), whereas an electronic blood pressure monitor took diastolic and systolic blood pressure with a cuff on the elbow (O2 medical systems, Hyderabad, India).
Vital signs were recorded before and after 1 minute of anesthesia.
2.8. Statical Analysis
The data of the present study were analyzed using the statistical package for social sciences software (Version 20, IBM SPSS Inc., Chicago, IL, USA). Sample Descriptive statistics were used by number and percentage for gender and the mean and standard division for age.
The normality of the data distribution was determined using the Kolmogorov-Smirnov test, where data of all outcomes showed normal distribution. The confidence was determined at 95% with a level of significant 0.05.
The differences in FIS variables between groups were analyzed using the Mann-Whitney U test, and intra-group comparisons before and after anesthesia were done using the Wilcoxon signed-rank test.
Paired t-test was used to analyze heart rate, diastolic and systolic blood pressure, and oxygen saturation differences at different time interventions within the group.
Differences in the group in heart rate, diastolic and systolic blood pressure, oxygen saturation, and FLACC were analyzed using an independent t-test.
3. Results
The flow chart of this study is described in Figure 2.
Fifty-four children, with a mean age of 8.2 ± 1.3 years (15 boys and 12 girls) for the control group and 8.1 ± 1.5 years (12 boys and 15 girls) for the aromatherapy group, participated in the study.
There were no significant differences in dental anxiety according to FIS (P=0.916) and vital signs, including heart rate (0.825), diastolic and systolic blood pressure (P=0.182 and P=1.00, respectively), and O2 saturation (P=0.563) between the control group and the aromatherapy group before anesthesia injection (Table 1).
After anesthesia, there was a significant statically reduction in FIS score in the aromatherapy group compared to the control group (P=0.001). (Table1)
For vital signs, heart rate, diastolic and systolic blood pressure were significantly reduced in the aromatherapy group compared to the control(P=0.000) (P=0.013) (P=0.038), and no significant differences were shown in O2 saturation between the two groups(P=0.744) (Table 1).
FLACC in the aromatherapy group showed significantly lower pain perception compared to the control after anesthesia injection (P=0.042) (Table 1).
Within-group comparison, there are no significant differences in FIS between before and after anesthesia in the aromatherapy group (p=0.600), whereas a significant increase was shown after anesthesia injection in the control group compared to the baseline (p=0.000). (Table 2)
4. Discussion
Anesthesia injections, especially INAB injections, are considered the most invasive procedures that provoke anxiety and pain during dental treatment in children [35].
The findings of this study revealed the effectiveness of inhalation of an aromatic oils blend containing lavender-neroli oils in reducing dental anxiety and pain during IANB injection in children.
The choice of this oil mixture depended on a previous study [36], which suggested the effectiveness of aromatherapy in reducing stress and enhancing sleep in children with skin burns.
Anxiety is a subjective feeling which differs from one person to another [33]. In this study, the FIS, a self-report anxiety scale, was used to determine the effect of aromatherapy on anxiety for ease of conduct in children [32,33].
Anxiety scores were statistically lower in the aromatherapy group compared to control.
Aromatic oils have a physiological effect on the nervous system and a psychological effect on the sense of smell, which contributes to their calming effect. Moreover, it is widely believed that fragrances have the power to alter the emotional state of humans [21]. It is worth noting that the odor from oil molecules stimulates the limbic system, which controls memories and feelings and, in turn, releases neurotransmitters that promote relaxation and happiness, such as morphine, serotonin, and epinephrine [11,16].
Furthermore, the components in essential oils play an important role in their anxiolytic effects. Gas chromatography showed that the main component of lavender oil was linalool and linalyl acetate, whereas neroli consists mainly of linalool, linalyl acetate, and limonene. Linalool has sedative and anxiolytic effects by acting like benzodiazepine receptors and binding with α-amino butyric acid receptors (GABA) [37]. Additionally, Linalyl acetate has a necrotic effect on the patient’s behavior and acts as a sedative [12,13].
Moreover, neroli oil has calming effects by suppressing the inflammatory mechanism of anxiety [10]. Limonene decreased neuroinflammation factors such as Nitric oxide (NO), Cyclooxygenase -2(CoX-2)-interleukin 6(IL-6), interleukin-1β(IL-1β), and tumor necrosis factor α (TNF-α) [38].
There is an interchangeable relation between pain and anxiety; fearful children can increase the sense of pain and cause hyperalgesia [13]. In this study, FLACC scores in the aromatherapy group showed a significant decrease in pain perception during IANB injection in children compared to the control group. This result could be due to the anesthetic properties of linalool, which are found in neroli and lavender oils. Linalool affects the somatic sensory system by selectively inhibiting the Na+ ion channel, producing analgesic properties [14].
Pain and anxiety trigger the Sympathetic tone of the autonomic nervous system, which increases physiological markers such as heart rate, blood pressure, and change in respiratory rate [39].
In this study, there was a decrease in heart rate and diastolic blood pressure with no change in systolic blood pressure in the aromatherapy group after anesthesia, whereas all vital signs, including heart rate, systolic and diastolic blood pressure, were increased in the control group after anesthesia injection.
Lavender oil increases Parasympathetic activity, which contrasts with the work of the Sympathetic nervous system and reduces the physiological parameters that induce more relaxation and calm [40].
Compared to the control group, all vital signs were decreased in the aromatherapy group except O2 levels, which had no significant change in the aromatherapy and control group. This could be because the children in both groups inhale through a nasal mask, which affects saturation levels. Wearing a mask increases the difficulty of breathing due to moisture and CO2 levels in the dead space of the mask [41].
The results of this study follow the previous studies [13,23,24,27], which found the effectiveness of aromatherapy in reducing anxiety and pain during invasive dental procedures, including anesthesia injection.
In a previous study [28], music was used in combination with the Lavender-Neroli oil blend aromatherapy during IANB injection, as music can reduce anxiety by releasing dopamine and opioids from the nucleus accumbens and other parts of the limbic system, thereby stimulating the reward mechanism in the brain [42]. The results of this study revealed the effectiveness of aromatherapy with music in managing dental anxiety, but in contrast with this study music combination with aromatherapy was not effective in reducing pain during anesthesia. Although citrus aroma has relaxation properties, it also can play a stimulation role [43]. Music can also alter the brainstem reflex and increase attention [44], which could increase the child’s sensory pain during injection.
Arslan et al. [23] revealed that lavender aroma does not prevent pain during anesthesia injection, which could be because, in this study, inhalation was done through a med patch before treatment, reducing the effectiveness of aromatherapy during treatment. In the current study, the child was asked to inhale the aromatic oils through a nasal mask during treatment, which increased the effectiveness of aromatherapy and helped distract the child from their pain during anesthesia.
In contrast to this study, Toet and colleagues showed that neither apple nor orange aroma was effective in reducing anxiety in the waiting room of a large dental clinic [43]. The results were affected by the noise from patients entering and exiting, as well as the effect of other smells from dental materials. In another study [26], it was indicated that the use of sweet orange oil does not significantly reduce dental anxiety and circulation activity during class I GIC restoration, a non-invasive dental procedure. This is considered because it does not provoke pain and fear. Moreover, the study of Nord and colleagues revealed no significant results on the effect of lavender and ginger aromas in providing comfort to children during peri-anesthesia procedures [45]. The FLACC scale in this study was administered by children's parents, which affected the results and made them less reliable due to the lack of training. Another reason is that the sample did not specify whether it included children with or without disabilities.
In the current study, no adverse effects were recorded, so aromatherapy can be considered a safe method to reduce dental anxiety and pain in children during invasive dental procedures. No adverse effects related to aromatherapy were observed in either group. Essential oils were diluted in grapeseed oil to minimize irritation and applied via indirect inhalation using cotton balls in a ventilated 3D-printed chamber. Children with a history of asthma or allergies were excluded to enhance safety. Both groups were closely monitored, and no respiratory distress, allergic reactions, or other adverse effects were observed.
Although the natural origin of aromatherapy, it still has some side effects, such as skin irritation and allergies after topical application due to the ingredients of essential oils [15]. Essential oils should be diluted in vegetable oils to avoid irritation for topical use [11]. Some side effects can occur when inhalation of essential oils, and this is related to the allergic odor and asthma more than essential oils themself [12]. In the current study, essential oils were diluted in grape seed oil, which is considered one of the carrier oils with no odor, used to dilute essential oils for added safety and to prevent them from reaching sensitive areas. Furthermore, the mixture odor was inhaled through the 3D-printed box, which is applied to the nitrous oxide nasal mask, allowing it to be easily removed and providing oxygen to the patient in emergencies if respiratory sensitivity occurs.
The use of non-pharmacological methods, such as music, distraction techniques, and natural products like lavender, shows promising potential for improving child behavior and satisfaction during dental treatment in pediatric dentistry. Combining pharmacological approaches with non-pharmacological methods—for example, electronic dental anesthesia/transcutaneous electrical nerve stimulation with music, nitrous oxide with lavender and music, or nitrous oxide with lavender and distraction—may represent the future of pediatric dental care [46,47,48,49]. These integrative strategies warrant further exploration and research.
The strength of this study was that anxiety and pain, along with physiological markers, were recorded; another strength is that aromatherapy was inhaled directly by the patient rather than diffusing it into the air. However, this study had some limitations; no control aroma was used for comparison with the mixture of aromatic oils. Hence, the aroma of the essential oils masks the clinic smell and distracts the patient. Additionally, the study wasn’t conducted using a split-mouth design, which could have affected the results, as the child in the experimental group wasn't matched with a child in the control group.
5. Conclusions
The results of this study revealed the effectiveness of aromatherapy with lavender-neroli oils as a safe, low-cost, and simple non-pharmacological method for reducing dental anxiety and pain in children during dental anesthesia injection. Further studies should be conducted with multiple essential oils and in different dental procedures to confirm its efficacy in various dental procedures.
Author Contributions
R.A. conceptualized the idea, provided the treatment, and contributed to the writing and documentation. C.K. and R.A.L. conceptualized the idea and supervised the MSc thesis for R.A. Y.A.T. contributed to writing and documentation, data interpretation, and the revision, formatting, and re-editing of the manuscript. Z.D.B. contributed to the interpretation of data and the revision, formatting, and re-editing of the manuscript. All authors read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Local Research Ethics Committee of the Faculty of Dentistry, Damascus University (UDDS-502-220420121/SRC-3183).
Informed Consent Statement
Informed consent was obtained from all subjects/caregivers involved in the study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgments
The presented research is part of the MSc study of Rama Abdalhai, approved by the Local Research Ethics Committee of the Faculty of Dentistry (UDDS-502-220420121/SRC-3183).
Conflicts of Interest
The authors declare no conflict of interest.
References
- Grisolia BM, Dos Santos APP, Dhyppolito IM, Buchanan H, Hill K, Oliveira BH. Prevalence of dental anxiety in children and adolescents globally: A systematic review with meta-analyses. Int J Paediatr Dent. 2021 Mar;31(2):168-183. [CrossRef] [PubMed]
- Crellin DJ, Harrison D, Santamaria N, Huque H, Babl FE. The Psychometric Properties of the FLACC Scale Used to Assess Procedural Pain. J Pain. 2018 Aug;19(8):862-872. [CrossRef] [PubMed]
- Shukla H, Kulkarni S, Wasnik MB, Rojekar N, Bhattad D, Kolekar P. Acceptance of Parents for Behavior Management Technique with Reference to Previous Dental Expertise and Dental Anxiety. Int J Clin Pediatr Dent. 2021;14(Suppl 2):S193-S198. [CrossRef] [PubMed] [PubMed Central]
- Shindova MP, Belcheva AB. Dental fear and anxiety in children: a review of the environmental factors. Folia Med (Plovdiv). 2021 Apr 30;63(2):177-182. [CrossRef] [PubMed]
- Appukuttan, DP. Strategies to manage patients with dental anxiety and dental phobia: literature review. Clin Cosmet Investig Dent. 2016 Mar 10;8:35-50. [CrossRef] [PubMed] [PubMed Central]
- Zinke A, Hannig C, Berth H. Comparing oral health in patients with different levels of dental anxiety. Head Face Med. 2018 Nov 20;14(1):25. [CrossRef] [PubMed] [PubMed Central]
- Seangpadsa K, Smutkeeree A, Leelataweewud P. Parental acceptance of behavior management techniques for preschool children in dental practice: Revisited. J Indian Soc Pedod Prev Dent. 2020 Jul-Sep;38(3):274-279. [CrossRef] [PubMed]
- Coté CJ, Wilson S. Guidelines for Monitoring and Management of Pediatric Patients Before, During, and After Sedation for Diagnostic and Therapeutic Procedures. Pediatr Dent. 2019 Jul 15;41(4):259-260. [PubMed]
- Bikmoradi A, Khaleghverdi M, Seddighi I, Moradkhani S, Soltanian A, Cheraghi F. Effect of inhalation aromatherapy with lavender essence on pain associated with intravenous catheter insertion in preschool children: A quasi-experimental study. Complement Ther Clin Pract. 2017 Aug;28:85-91. [CrossRef] [PubMed]
- Moslemi F, Alijaniha F, Naseri M, Kazemnejad A, Charkhkar M, Heidari MR. Citrus aurantium Aroma for Anxiety in Patients with Acute Coronary Syndrome: A Double-Blind Placebo-Controlled Trial. J Altern Complement Med. 2019 Aug;25(8):833-839. [CrossRef] [PubMed]
- Reyes MCGM, Reyes MCGM, Ribay KGL, Paragas ED Jr. Effects of sweet orange aromatherapy on pain and anxiety during needle insertion among patients undergoing hemodialysis: A quasi-experimental study. Nurs Forum. 2020 Jul;55(3):425-432. [CrossRef] [PubMed]
- Babar Ali, Naser Ali Al-Wabel, Saiba Shams, Aftab Ahamad, Shah Alam Khan, Firoz Anwar, Essential oils used in aromatherapy: A systemic review, Asian Pacific Journal of Tropical Biomedicine. 2015 Aug; 5(8): 601-611. ISSN 2221-1691. [CrossRef]
- Alkanan SAM, Alhaweri HS, Khalifa GA, Ata SMS. Dental pain perception and emotional changes: on the relationship between dental anxiety and olfaction. BMC Oral Health. 2023 Mar 26;23(1):175. [CrossRef] [PubMed] [PubMed Central]
- Wang ZJ, Heinbockel T. Essential Oils and Their Constituents Targeting the GABAergic System and Sodium Channels as Treatment of Neurological Diseases. Molecules. 2018 May 2;23(5):1061. [CrossRef] [PubMed] [PubMed Central]
- MICHALAK, Monika. Aromatherapy and methods of applying essential oils. Archives of Physiotherapy and Global Researches, 2018, 22.2: 25-31.
- Lv XN, Liu ZJ, Zhang HJ, Tzeng CM. Aromatherapy and the central nerve system (CNS): therapeutic mechanism and its associated genes. Curr Drug Targets. 2013 Jul;14(8):872-9. [CrossRef] [PubMed]
- Wajda M, Gover A, Franco L, blanck T. 2017. “Review of Lavender Aromatherapy: Past, Present, and Future.” Austin Therapeutics 4(1). www.austinpublishinggroup.com.
- Donelli D, Antonelli M, Bellinazzi C, Gensini GF, Firenzuoli F. Effects of lavender on anxiety: A systematic review and meta-analysis. Phytomedicine. 2019 Dec;65:153099. [CrossRef] [PubMed]
- Scandurra C, Mezzalira S, Cutillo S, Zapparella R, Statti G, Maldonato NM, Locci M, Bochicchio V. The Effectiveness of Neroli Essential Oil in Relieving Anxiety and Perceived Pain in Women during Labor: A Randomized Controlled Trial. Healthcare (Basel). 2022 Feb 14;10(2):366. [CrossRef] [PubMed] [PubMed Central]
- Mannucci, C., Calapai, F., Cardia, L., Inferrera, G., D'Arena, G., Di Pietro, M.,... & Calapai, G. (2018). Clinical Pharmacology of Citrus aurantium and Citrus sinensis for the Treatment of Anxiety. Evidence-based complementary and alternative medicine: eCAM, 2018.
- Venkataramana, M., Pratap, K. V. N. R., Padma, M., Kalyan, S., Reddy, A. A., & Sandhya, P. (2016). Effect of aromatherapy on dental patient anxiety: A randomized controlled trial. Journal of Indian Association of Public Health Dentistry, 14(2), 131-134.
- Zabirunnisa M, Gadagi JS, Gadde P, Myla N, Koneru J, Thatimatla C. Dental patient anxiety: Possible deal with Lavender fragrance. J Res Pharm Pract. 2014 Jul;3(3):100-3. [CrossRef] [PubMed] [PubMed Central]
- Arslan I, Aydinoglu S, Karan NB. Can lavender oil inhalation help to overcome dental anxiety and pain in children? A randomized clinical trial. Eur J Pediatr. 2020 Jun;179(6):985-992. [CrossRef] [PubMed]
- Nirmala K, Kamatham R. Effect of Aromatherapy on Dental Anxiety and Pain in Children Undergoing Local Anesthetic Administrations: A Randomized Clinical Trial. J Caring Sci. 2021 Aug 23;10(3):111-120. [CrossRef] [PubMed] [PubMed Central]
- Jafarzadeh M, Arman S, Pour FF. Effect of aromatherapy with orange essential oil on salivary cortisol and pulse rate in children during dental treatment: A randomized controlled clinical trial. Adv Biomed Res. 2013 Mar 6;2:10. [CrossRef] [PubMed] [PubMed Central]
- SONI, Sheena; BHATIA, Rupinder; OBEROI, Jyoti. Evaluation of the efficacy of aromatherapy on anxiety level among pediatric patients in a dental setting: a randomized control trial. International Journal of Oral Care and Research, 2018, 6.2: 44-9.
- Ghaderi, Faezeh, and Neda Solhjou. 2020. “The Effects of Lavender Aromatherapy on Stress and Pain Perception in Children during Dental Treatment: A Randomized Clinical Trial.” Complementary Therapies in Clinical Practice 40.
- Abdalhai, R., Kouchaji, C., & Alkhatib, R. (2024). The effect of aromatherapy with Lavender-Neroli oil and music in management of pediatric dental anxiety: a randomized control trial. BDJ open, 10(1), 5.
- PRADOPO, Seno; SINAREDI, Betadion Rizki; JANUARISCA, Bernadeth Vindi. Pandan Leaves (Pandanus Amaryllifolius) aromatherapy and relaxation music to reduce dental anxiety of pediatric patients. Journal of International Dental and Medical Research, 2017, 10.3: 933-937.
- McHugh, ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb). 2012;22(3):276-82. [PubMed] [PubMed Central]
- Dean, Jeffrey A. 2021. Mcdonald and Avery’s Dentistry for the Child and Adolescent. 11 Edition. ed. Jeffrey A. Dean. Elsevier Health Science pp 327-330.
- Tiwari S, Kulkarni P, Agrawal N, Mali S, Kale S, Jaiswal N. Dental Anxiety Scales Used in Pediatric Dentistry: A Systematic Review and Meta-analysis. J Contemp Dent Pract. 2021 Nov 1;22(11):1338-1345. [PubMed]
- FATHIMA, Faazila; JEEVANANDAN, Ganesh. Validation of a facial image scale to assess child dental anxiety. Drug Invent Today, 2018, 10: 2825-8.
- Dak Albab, Rahaf, and Hisham Shakhashero. 2016. “The Validity and Reliability of the Arabic Version of FLACC Scale: A Clinical Trial.” Journal of Anesthesia & Clinical Research 7(8).
- Aditya PVA, Prasad MG, Nagaradhakrishna A, Raju NS, Babu DN. Comparison of effectiveness of three distraction techniques to allay dental anxiety during inferior alveolar nerve block in children: A randomized controlled clinical trial. Heliyon. 2021 Sep 29;7(9):e08092. [CrossRef] [PubMed] [PubMed Central]
- O'Flaherty LA, van Dijk M, Albertyn R, Millar A, Rode H. Aromatherapy massage seems to enhance relaxation in children with burns: an observational pilot study. Burns. 2012 Sep;38(6):840-5. [CrossRef] [PubMed]
- Harada H, Kashiwadani H, Kanmura Y, Kuwaki T. Linalool Odor-Induced Anxiolytic Effects in Mice. Front Behav Neurosci. 2018 Oct 23;12:241. [CrossRef] [PubMed] [PubMed Central]
- Eddin LB, Jha NK, Meeran MFN, Kesari KK, Beiram R, Ojha S. Neuroprotective Potential of Limonene and Limonene Containing Natural Products. Molecules. 2021 Jul 27;26(15):4535. [CrossRef] [PubMed] [PubMed Central]
- Hyde J, Ryan KM, Waters AM. Psychophysiological Markers of Fear and Anxiety. Curr Psychiatry Rep. 2019 Jun 4;21(7):56. [CrossRef]
- Malcolm BJ, Tallian K. Essential oil of lavender in anxiety disorders: Ready for prime time? Ment Health Clin. 2018 Mar 26;7(4):147-155. [CrossRef] [PubMed] [PubMed Central]
- Nwosu ADG, Ossai EN, Onwuasoigwe O, Ahaotu F. Oxygen saturation and perceived discomfort with face mask types, in the era of COVID-19: a hospital-based cross-sectional study. Pan Afr Med J. 2021 Jul 16;39:203. [CrossRef] [PubMed] [PubMed Central]
- Raglio, A. (2023). A noval music-based theraeutic approach: the therapeutic music listening. Front in Human Nerouscience, 17:1204593-1204593. [CrossRef]
- Toet A, Smeets MA, van Dijk E, Dijkstra D, van den Reijen L. Effects of Pleasant Ambient Fragrances on Dental Fear: Comparing Apples and Oranges. Chemosens Percept. 2010 Dec;3(3-4):182-189. [CrossRef] [PubMed] [PubMed Central]
- van der Weijden, F. N., etal. (2022). The effect of playing background music during dental treatment on dental anxiety and physiological parameters: A systematic review and meta-analysis. Psychology of Music, 50(2):365–388. [CrossRef]
- Nord D, Belew J. Effectiveness of the essential oils lavender and ginger in promoting children's comfort in a perianesthesia setting. J Perianesth Nurs. 2009 Oct;24(5):307-12. [CrossRef] [PubMed]
- Attar RH, Baghdadi ZD. Comparative efficacy of active and passive distraction during restorative treatment in children using an iPad versus audiovisual eyeglasses: a randomised controlled trial. Eur Arch Paediatr Dent. 2015 Feb;16(1):1-8. [CrossRef] [PubMed]
- Baghdadi, ZD. Evaluation of audio analgesia for restorative care in children treated using electronic dental anesthesia. J Clin Pediatr Dent. 2000 Fall;25(1):9-12. [PubMed]
- Baghdadi, ZD. Evaluation of electronic dental anesthesia in children. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1999 Oct;88(4):418-23. [CrossRef] [PubMed]
- Haralambidis C, Nicozisis J. High-frequency neuromodulation with the dental pain eraser for nonpharmacologic pain relief in orthodontic practice. J Clin Orthod. 2024 Septemeber;58(9):567-572. [PubMed]
Figure 1.
Modified nasal nitrous oxide mask; A: 3D printed box, B: Top and Bottom cover of the box, and C: Final shape of the box and the nasal mask.
Figure 1.
Modified nasal nitrous oxide mask; A: 3D printed box, B: Top and Bottom cover of the box, and C: Final shape of the box and the nasal mask.

Figure 2.
The flow chart of this study.
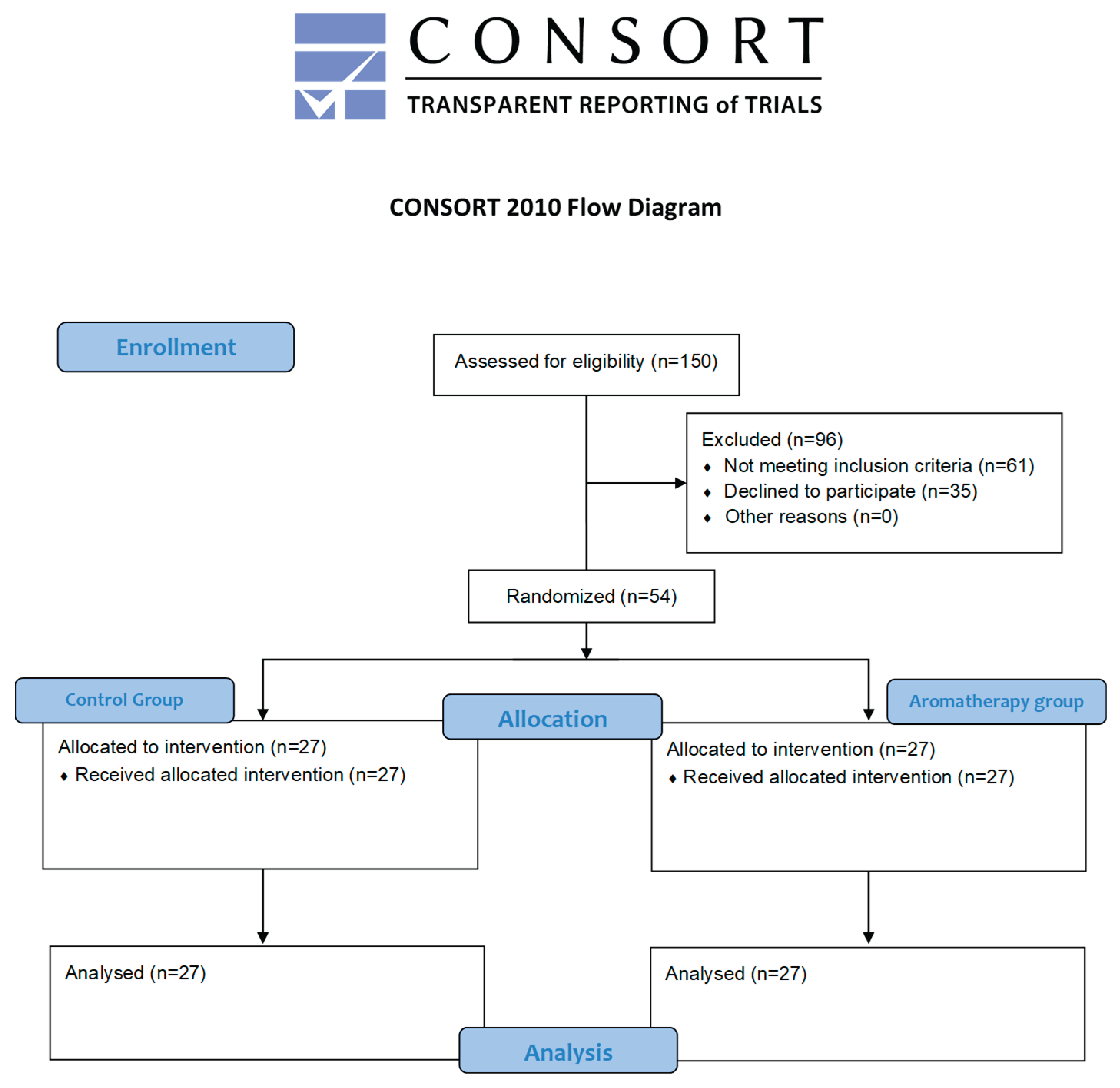
Figure 3.
Change in vital signs in the control group.
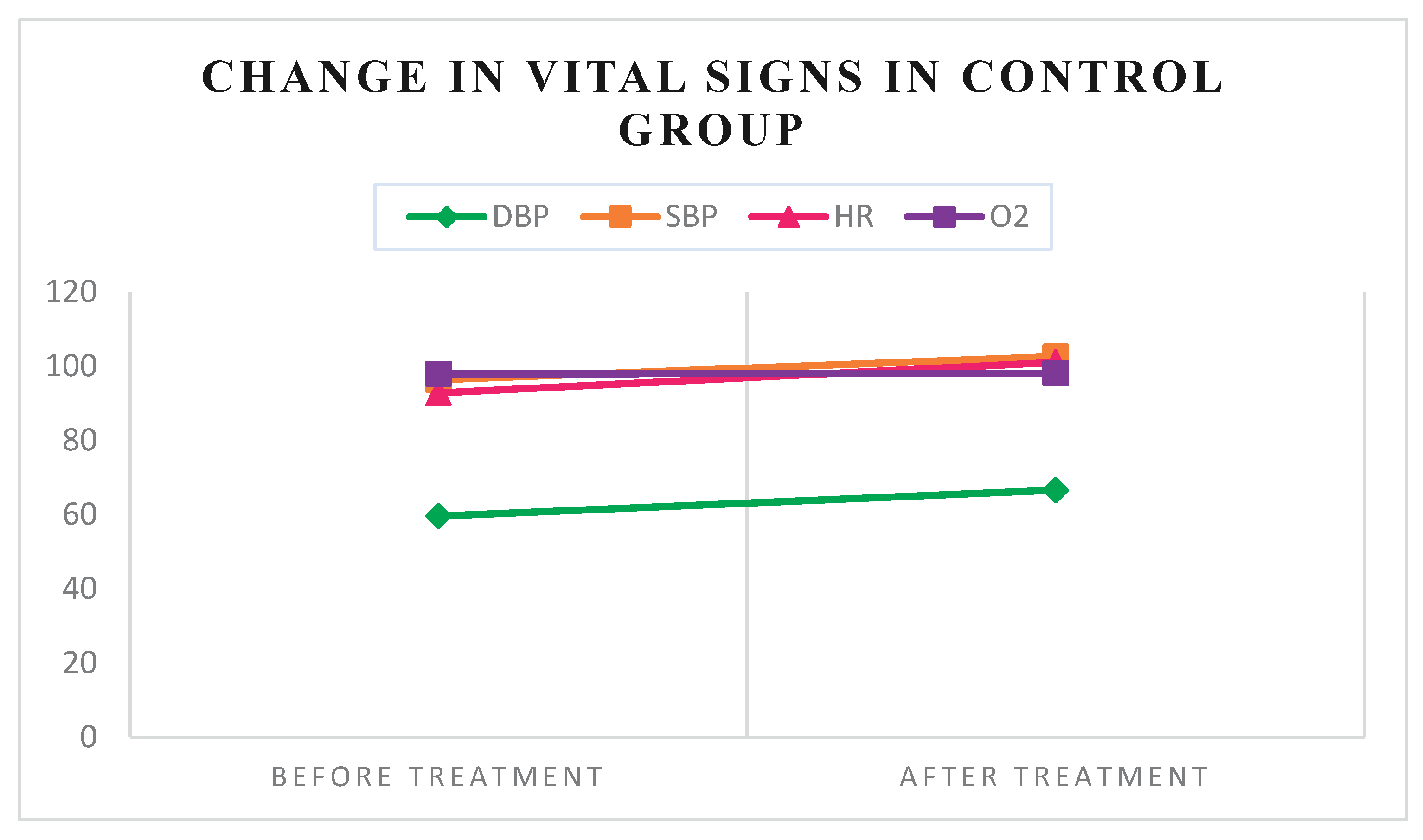
Figure 4.
Change in vital signs in the aromatherapy group.
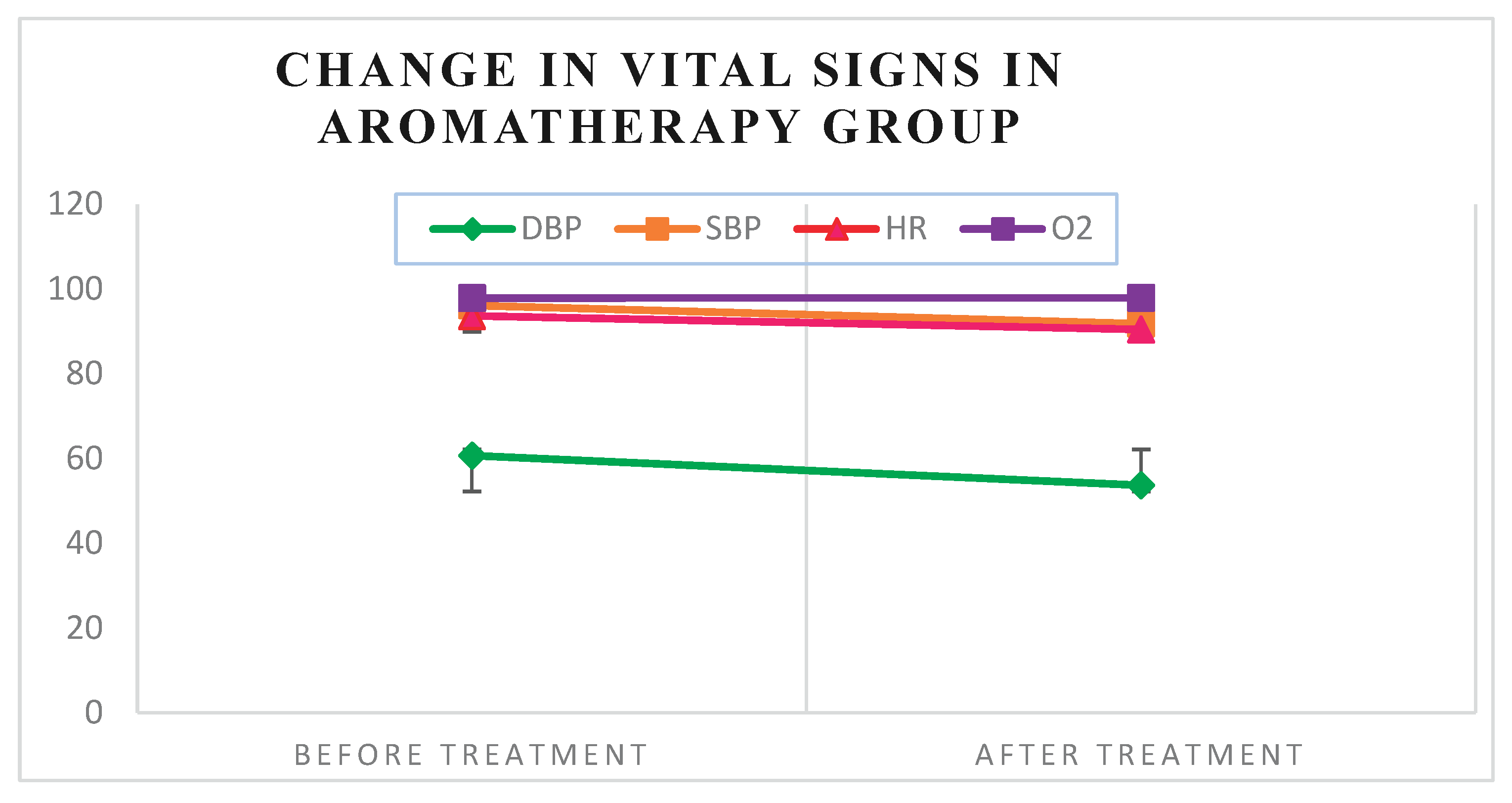

Table 1.
Inter groups comparison.
| Before anesthesia | After anesthesia | |||||
|---|---|---|---|---|---|---|
| Variables | Control group | Aromatherapy group | P-Value | Control Group | Aromatherapy group | p-Value |
| FIS* | 58.34 | 55.11 | 0.916 | 79.88 | 51.7 | 0.001S |
| DBP$ | 59.57 ±11.59 | 60.7 ±12.07 | 0.182 | 66.61 ±16.31 | 53.67 ±10.34 | 0.013S |
| SBP$ | 96.36 ±9.97 | 96.11 ±13.46 | 1.00 | 102.61 ±11.33 | 91.81 ±12.57 | 0.038S |
| HR$ | 92.79 ±15.76 | 93.63 ±16.83 | 0.825 | 101.04 ±19.43 | 90.48 ±17.11 | 0.000S |
| SPO2$ | 98.07 ±1.24 | 97.85 ±1.61 | 0.563 | 98.11±1.13 | 97.93 ±1.33 | 0.744 |
| FLACC$ | ----- | ----- | ----- | 3.11 ±2.42 | 1.51 ±1.87 | 0.042S |
| FIS: Facial Image Scale, DBP: Diastolic blood pressure, SBP: Systolic blood pressure, HR: Heart rate, SPO2: O2 Oxygen saturation, FLACC: Face-Legs-Activity-Cry-Consolability.Mean ranks were used for the FIS scale, whereas means ±Standard Deviation (SD) was used for vital signs and the FLACC scale. *: Differences in mean ranks of FIS between groups were analyzed using the Mann-Whitney U test. $: Differences in means of vital signs and FLACC scale between groups were analyzed using an independent T-test. S: Significant differences between groups. | ||||||
Table 2.
Within group comparison.
| Variables | Before treatment | After treatment | After-beforeMean differences ±SD | p-value | |
|---|---|---|---|---|---|
| Control group | FIS* | 58.34 | 79.88 | 0.000S | |
| DBP$ | 59.57 ±11.59 | 66.61 ±16.31 | 7.04 ±15.57 | 0.024S | |
| SBP$ | 96.36 ±9.97 | 102.61 ±11.33 | 6.25 ±10.46 | 0.004S | |
| HR$ | 92.79 ±15.76 | 101.04 ±19.43 | 8.25 ±10.17 | 0.000S | |
| SPO2$ | 97.93 ±1.09 | 98.11 ±1.13 | 0.18 ±1.33 | 0.485 | |
| Aromatherapy group | FIS* | 55.11 | 51.7 | 0.6 | |
| DBP$ | 60.7 ±12.07 | 53.67 ±10.34 | -7.04 ±13.32 | 0.011S | |
| SBP$ | 96.11 ±13.46 | 91.81 ±12.57 | -4.30 ±13.47 | 0.109 | |
| HR$ | 93.63 ±16.83 | 90.48 ±17.11 | -3.15 ±7.69 | 0.043S | |
| O2$ | 97.85 ±1.61 | 97.93 ±1.33 | 0.07 ±1.44 | 0.791 | |
|
*: FIS Means rank Differences in value before and after treatment were analyzed using the Wilcoxon signed-rank test. $: Means differences in value before and after treatment were analyzed using paired t-test. S: Significant differences were found within the group | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



