Submitted:
16 June 2025
Posted:
17 June 2025
You are already at the latest version
Abstract
Background: Non-alcoholic fatty liver disease (NAFLD) is a global public health issue. Although liver biopsy remains the gold standard for diagnosing hepatosteatosis, its invasiveness, high cost, and associated risks limit its widespread use. Therefore, there is a need for reliable, non-invasive, and cost-effective biomarkers to aid in the early detection of NAFLD. Our objective was to determine the utility of the triglyceride (TG) to high-density lipoprotein (HDL) ratio in predicting non-alcoholic fatty liver disease. Methods: This retrospective cross-sectional study included 2588 patients who met the inclusion criteria. Demographic data and laboratory results were collected from electronic health records and recorded. Experienced radiologists performed abdominal ultrasonography to assess fatty liver in line with EASL 2021 criteria. The TG/HDL ratio and other non-invasive scores (APRI, FIB-4, ALT/AST, TG/Glucose) were calculated. Results: TG/HDL ratio was significantly higher in NAFLD patients (AUROC: 0.682), outperforming other non-invasive indices. At the optimal cut-off value of 1.86, sensitivity was 80.7% and specificity 45.5%. The TG/HDL ratio correlated positively with markers of glycemic control, inflammation, and liver enzymes. Conclusions: The TG/HDL ratio is an accessible and valuable parameter in predicting non-alcoholic fatty liver disease. It offers a non-invasive alternative to liver biopsy and potentially prevents complications from non-alcoholic fatty liver disease or diagnostic approaches.
Keywords:
dyslipidemia
; HDL cholesterol
; non-alcoholic fatty liver disease
; triglyceride
; triglyceride/HDL ratio
1. Introduction
Non-alcoholic fatty liver disease (NAFLD) is becoming increasingly prevalent globally [1,2]. This is due to the rising prevalence of metabolic syndrome and obesity, as well as changes in dietary habits. The true prevalence of NAFLD patients is unknown, as it is the most common (approximately 90%) cause of asymptomatic aspartate aminotransferase (AST) and alanine aminotransferase (ALT) elevation in patients presenting to clinics, and the majority of cases are asymptomatic [1]. In some screening-based studies conducted in the adult population, the prevalence of NAFLD was found to be 17-33% (75% in obese patients), and the prevalence of non-alcoholic steatohepatitis (NASH) was approximately 3% [3]. NAFLD is not only confined to the liver but is increasingly recognized as a hepatic manifestation of systemic metabolic dysfunction and is closely associated with a significantly increased risk of type 2 diabetes mellitus, insulin resistance, obesity and cardiovascular diseases [4]. NAFLD is characterized by fat accumulation in the liver and is the most common cause of chronic liver disease. Sedentary life, some drugs (such as steroid hormones, tamoxifen, and cisplatin), environmental and genetic factors may also play a role in the development of NAFLD [5].
For the diagnosis of NAFLD, steatosis should be demonstrated on radiological imaging or tissue histology, causes that may lead to hepatic steatosis should be excluded, and excessive alcohol consumption and other causes of chronic liver disease should be ruled out [6]. The gold standard in the diagnosis of hepatosteatosis is liver biopsy. However, it is mostly not preferred in the diagnosis of hepatosteatosis because it is an invasive procedure, is not cost-effective, and has complications such as bleeding or liver injury. Therefore, non-invasive or less invasive techniques are used to diagnose hepatosteatosis whenever possible [7]. Imaging modalities used in the diagnosis of NAFLD include abdominal ultrasound (US) imaging, computed tomography (CT), and magnetic resonance imaging (MRI). US is often the first preferred imaging method because it is easily accessible and does not contain ionizing radiation [8].
Fibrosis may develop on the background of NASH in the later stages of the disease, and the risk of liver cirrhosis and hepatocellular carcinoma may increase in advanced cases. Therefore, detecting fibrosis in NAFLD patients in the early stages and determining appropriate treatment strategies is essential. In addition to invasive methods such as liver biopsy, non-invasive scores such as AST to platelet ratio index (APRI), Fibrosis-4 (FIB-4) score, and ALT to AST ratio are also used to evaluate fibrosis in NAFLD. These scores are simple, non-invasive tests widely used in routine clinical practice and aid clinical decision-making to assess liver fibrosis in the foreground. Studies show that these scores can predict hepatic fibrosis and NAFLD [9,10].
Hypertriglyceridemia and low high-density lipoprotein (HDL) cholesterol levels play an essential role in the pathophysiology of NAFLD and are components of metabolic syndrome. Intense triglyceride (TG) accumulation is observed in hepatocytes, especially in patients with NAFLD. Our study aimed to determine whether the TG to HDL ratio is superior to other scoring systems in predicting NAFLD and whether this ratio can be used rapidly and reliably in diagnosing and following hepatosteatosis.
2. Patients and Methods
2.1. Study Participants
This study has a retrospective cross-sectional study design. The University of Health Sciences, Haseki Training and Research Hospital Institutional Ethics Committee reviewed and approved the study protocol (reference number: 02-2023, date of approval: 11.01.2023). Also, the ethics committee anonymized and approved the database information with no need for consent. Data from electronic health records and laboratory databases of 5962 patients admitted to Haseki Training and Research Hospital Internal Medicine outpatient clinic between March 2022 and March 2023 and underwent abdominal ultrasonography were analyzed retrospectively. Exclusion criteria included significant alcohol intake (≥140 grams/week ethanol consumption for women, ≥210 grams/week ethanol consumption for men), being under 18 years of age, hepatotoxic drug or anti-hyperlipidemic agent usage, acute hepatitis, pregnancy, and having a disease affecting the liver. Inclusion criteria were being over 18 years of age, availability of fasting triglyceride and HDL measurements, and ultrasonographic evidence of being with or without hepatic steatosis. A total of 2588 patients who fulfilled the necessary criteria were included in the study, as seen in flow diagram of the study (Figure 1).
2.2. Laboratory and Radiological Analysis
Demographic data (such as age and gender) and clinical characteristics (comorbidities and medications used) were recorded. The tests (AST, ALT, TG, HDL cholesterol, total cholesterol, complete blood count, HbA1c, albumin, glucose, creatinine, uric acid, and hemogram) obtained after fasting for at least eight hours were recorded. Non-invasive scoring (APRI, FIB-4, ALT/AST ratio, TG/Glucose ratio) and TG/HDL ratio were calculated using these data. The indices were calculated using established formulae from prior studies. ROC analysis was used to identify the diagnostic performance of each index. The optimal cut-off value was determined using the Youden Index. Hepatic steatosis was evaluated semiquantitatively by abdominal ultrasonography performed by experienced radiologists blinded to clinical and laboratory data. NAFLD diagnosis was based on the presence of hepatic steatosis according to the European Association for the Study of the Liver (EASL) 2021 criteria, after exclusion of secondary causes and significant alcohol intake.
2.3. Statistical Analysis:
Statistical analysis was performed using SPSS 26.0 for Windows (Armonk, NY: IBM Corp.). Numeric values were expressed as the mean ± standard deviation. Descriptive statistics AND Kolmogorov-Smirnov tests were performed, and skewness/kurtosis values were evaluated to assess whether the data had been normally distributed. Normally-distributed variables were assessed using a t-test, and irregular variables were evaluated using the Mann-Whitney U test. Comparisons of numerical variables in more than two groups were made using the One Way ANOVA test if there was a normal distribution or the Kruskal Wallis test if there was no normal distribution. Subgroup analyses were interpreted according to Bonferroni correction. Categorical variables were evaluated with the chi-square test. Sensitivity and specificity values of non-invasive scoring and triglyceride/HDL ratio for predicting hepatosteatosis were calculated. Receiver operating characteristic (ROC) analyses were performed to determine the diagnostic accuracy of the related laboratory results and ratios. The Pearson correlation coefficient was used to assess the linear relationship between variables, while the Spearman correlation was used to evaluate the monotonic relationship. Descriptive statistics were presented as mean ± standard deviation and p-values ≤0.05 were considered significant
3. Results
Of the patients included in the study, 1631 were female, and 957 were male. 811 female and 459 male patients did not have NAFLD, while 820 female and 498 male patients had NAFLD. There was no statistically significant difference in the incidence of NAFLD between genders (p:0.249). The mean age of the patients was 45.31±12.50 years, 49.07±10.34 years in the group with NAFLD, and 41.42±13.33 years in the group without hepatosteatosis. When the grades of hepatosteatosis were evaluated, it was seen that 878 patients had grade 1 hepatosteatosis, 411 patients had grade 2 hepatosteatosis, and 29 patients had grade 3 hepatosteatosis out of 1318 patients with NAFLD.
Among the laboratory parameters, white blood cell (WBC), neutrophil count, glucose, HbA1c, AST, ALT, alkaline phosphatase (ALP), lactate dehydrogenase (LDH), albumin, total cholesterol, TG, c-reactive protein (CRP) values were statistically significantly higher in patients with NAFLD and HDL values were significantly higher in patients without hepatosteatosis (Table 1 and Table 2). There was no statistically significant correlation between platelet (PLT) count and the presence or absence of hepatosteatosis.
When the patients were analyzed according to non-invasive disease assessment methods, triglyceride/HDL ratio, APRI score, FIB-4 score, ALT/AST ratio, and TG/Glucose ratio were statistically significantly higher in patients with NAFLD (all p-values: <0.001), (Table 3). In subgroup analysis according to gender, the TG/HDL ratio was 2.48±2.32 (median: 1.84) in patients without NAFLD and 3.64±2.75 (median: 2.94) in patients with NAFLD. In men, this ratio was 3.31±3.49 (median:2.39) in those without NAFLD and 4.81±3.96 (median:3.72) in those with NAFLD (Figure 2). All of these differences were statistically significant (p<0.001).
When ROC analysis was performed to evaluate the predictive value of TG/HDL ratio and other non-invasive parameters for NAFLD, the AUROC for TG/HDL ratio was 0.682 (95% CI: 0.662–0.703), outperforming APRI (0.565), FIB-4 (0.591) and ALT/AST ratio (0.668), (Figure 3, Table 4). The optimal cut-off value for the TG/HDL ratio was identified as 1.86, yielding a sensitivity of 80.7% and specificity of 45.5% for NAFLD detection (Table 5).
As shown in Table 6, when the correlation of the TG/HDL ratio with other biochemical findings and parameters was analyzed, it was observed that it was positively correlated with the parameters except for FIB-4, LDH, and PLT count.
4. Discussion
The findings of this study demonstrate the clinical relevance of the TG/HDL ratio as a practical tool in the early identification of NAFLD. The observed AUROC of 0.682, with high sensitivity at a low cut-off value, supports its utility particularly in identifying early-stage disease, such as grade 1 steatosis, which comprised the majority of our NAFLD cohort.
Non-alcoholic fatty liver disease (NAFLD) is an increasingly common health problem not only in Turkey but also worldwide due to the increasing prevalence of metabolic syndrome, obesity, and changes in dietary habits. Current studies suggest that the global prevalence of NAFLD is approximately 25% [11]. Imaging methods are most commonly used to diagnose NAFLD. However, routine imaging may delay diagnosis and contribute to unnecessary healthcare costs, and patients are exposed to unnecessary radiation in methods such as computed tomography. In patients with suspected NAFLD, it is essential that a simple value such as TG/HDL ratio, which readily derived from routine laboratory tests, helps us to make a diagnosis. In this way, both time and labor loss can be prevented.
The review by Younossi ZM and the study by Tabacu L et al. reported that the incidence of NAFLD increased with age [12,13]. Similarly, our study found that the mean age of patients with hepatosteatosis was higher than those without hepatosteatosis.
In a study conducted by Summart et al. in Thailand, it was observed that the prevalence of NAFLD was higher in women (especially in the postmenopausal period) than in men [14]. In a study conducted by Eguchi et al. in Japan and published in 2012, it was observed that the incidence of NAFLD in men was approximately three times higher than in women [15]. In our study, although the prevalence was higher in men, no statistically significant difference was observed in the prevalence of NAFLD between genders. This lack of statistical difference may reflect to differences in the lifestyle and dietary habits of the opposite sexes in different societies.
Increased hepatic insulin resistance plays a vital role in the pathophysiology of NAFLD. It has been demonstrated in many studies and review articles that metabolic syndrome and diabetes mellitus are more common pathologies in patients with NAFLD compared to the average population [12,16]. In a meta-analysis by Ballestri et al. in which the data of 117020 patients in 20 different studies were evaluated, it was concluded that the incidence of Type 2 DM was approximately doubled in patients with NAFLD [17]. Similarly, our study found that glucose and HbA1c values were statistically significantly higher in patients with hepatosteatosis and were positively correlated with TG/HDL ratio.
It has been reported that serum aminotransferase (AST and ALT) levels may slightly increase in patients with hepatosteatosis secondary to hepatocyte inflammation [18,19]. The presence of these values in the normal range does not exclude the disease. In our evaluation, AST and ALT were statistically significantly increased in patients with hepatosteatosis. In addition, studies are showing that the ALT/AST ratio is a parameter that can be used to support the diagnosis of NAFLD [9,20,21]. Some studies have shown that aminotransferase levels, primarily ALT, increase as fibrosis increases in NAFLD patients [22]. Because of this increase in ALT, which increases more precisely and more markedly than AST in hepatocyte damage, the ALT/AST ratio has been higher in patients with hepatosteatosis than those without hepatosteatosis. Our analysis found that the ALT/AST ratio was higher in patients with NAFLD in a manner that supported the literature data. Similarly, inflammation indicators WBC and CRP were higher in NAFLD patients due to inflammation in hepatocytes and were positively correlated with TG/HDL ratio. These findings also supported previous studies [23].
Dyslipidemia, one of the components of metabolic syndrome, frequently accompanies NAFLD. Studies have shown that significantly elevated triglycerides and low HDL levels are observed more frequently in patients with hepatosteatosis [24,25]. Increased triglyceride accumulation in hepatocytes is considered one of the main pathophysiologic mechanisms in NAFLD [26]. In support of these findings, Li et al. found that triglyceride levels were higher and HDL cholesterol levels were lower in patients with hepatosteatosis than those without NAFLD [27]. In addition, some studies show that the triglyceride/HDL ratio is higher in patients with hepatosteatosis than in the average population [28,29,30]. A study by Wu et al. showed that an increase in the Triglyceride/HDL ratio was associated with an increase in the stage of hepatosteatosis, especially with advanced hepatosteatosis [28]. Similar results are available between total cholesterol levels and NAFLD. In two different studies conducted with patients with chronic hepatitis B and type 2 diabetes mellitus, total cholesterol levels and total cholesterol/HDL cholesterol ratios were found to be higher in patients with hepatosteatosis, similar to our study [31,32].
The search for parameters that can rapidly and accurately detect NAFLD, a global health problem, continues. Although histological confirmation remains the diagnostic gold standard for NAFLD, its invasive nature, associated risks, and ethical considerations limit its use in large-scale or retrospective studies. In contrast, abdominal ultrasonography offers a practical and non-invasive alternative. A comprehensive meta-analysis by Hernaez et al., which included 49 studies, demonstrated that ultrasonography has a pooled sensitivity of 84.8% and specificity of 93.6% for detecting moderate to severe hepatic steatosis when compared with histology [8]. These findings support its reliability in epidemiological and clinical research settings. Accordingly, our study utilized ultrasonographic diagnosis in alignment with European Association for the Study of the Liver (EASL) 2021 guidelines, and evaluations were performed by experienced radiologists blinded to clinical and laboratory data to reduce observer bias. Therefore, studies have been conducted to evaluate whether non-invasive parameters such as APRI, FIB-4, and ALT/AST ratio, which are mainly developed to predict fibrosis in the liver in daily practice, are also predictive for NAFLD, and many different results have been found. In the study conducted by Sayar et al. in patients with chronic hepatitis B infection, it was observed that a high APRI score was not associated with the presence of NAFLD [33]. In our study, TG/HDL ratio was significantly higher in patients with NAFLD. A study conducted by Yin et al. evaluating high-risk metabolic dysfunction-related steatohepatitis patients showed that APRI had a sensitivity of 24.7% and FIB-4 had a sensitivity of 26.9% for steatohepatitis [34]. Another study conducted in Portugal observed that APRI had a sensitivity of 65.4% and FIB-4 had a sensitivity of 61.5% at different cut-off values [35]. While TG/HDL exhibited the highest AUROC among evaluated markers, its moderate predictive power underscores the need for composite indices or integration into multifactorial models.
Similarly, the ALT/AST ratio was thought to be used to predict NAFLD like other non-invasive parameters. However, it was observed that the sensitivity remained as low as 55% at the determined cut-off value [36]. In our study, when the TG/HDL ratio was evaluated according to the cut-off value, it was found that the TG/HDL ratio's sensitivity for NAFLD was higher compared to other studies' findings. Considering that the majority of the patient group in our study had grade 1 hepatosteatosis, the TG/HDL ratio seems to be an accessible and helpful parameter in predicting NAFLD, especially in the initial stage.
Our findings demonstrate that the TG/HDL ratio is a valuable predictor of NAFLD. This non-invasive parameter offers a practical alternative to liver biopsy, reducing the risks and costs associated with invasive procedures. The TG/HDL ratio can be easily calculated from routine laboratory tests, making it an accessible tool for early diagnosis and management of NAFLD. From a public health perspective, the TG/HDL ratio could be integrated into primary care screening algorithms, particularly for high-risk populations such as individuals with obesity, diabetes, or metabolic syndrome. Its simplicity may allow earlier identification of hepatic steatosis, enabling preventive lifestyle interventions and targeted follow-up. While promising, the current findings require validation in prospective cohorts and in populations with histologic confirmation of NAFLD. Further research may also clarify sex-specific thresholds or utility in pediatric and geriatric groups.
The large sample size and use of multiple validated indices strengthen the reliability of our findings. Also, several limitations should be acknowledged. The reliance on ultrasonographic findings without histological confirmation may have introduced variability in the diagnosis of NAFLD. Due to the retrospective nature of the study, data regarding patients' dietary habits, physical activity levels, and specific medication use (e.g., statins, antidiabetics) were not consistently available in the medical records and thus could not be included in the analysis. These factors are indeed relevant to both lipid metabolism and NAFLD progression and should be considered in future prospective studies. In addition, as a retrospective cross-sectional study, our findings are limited to associations rather than causation. However, the large sample size and use of multiple non-invasive indices provide a valuable snapshot of TG/HDL’s diagnostic potential in routine practice.
5. Conclusions
Our study confirms the utility of the TG/HDL ratio as a non-invasive biomarker for hepatic steatosis. Given its simplicity and strong association with NAFLD in our cohort, the TG/HDL ratio holds promise as an accessible adjunctive tool in primary screening protocols, particularly when imaging or biopsy are not feasible. Although more studies are needed on this subject, its widespread use could enhance early diagnosis and management, potentially reducing NAFLD-related complications, especially in patients at risk for hepatosteatosis. Future studies incorporating histologic endpoints and longitudinal outcomes will be critical to establishing the prognostic value of this biomarker.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: title; Table S1: title; Video S1: title.
Author Contributions
Conceptualization, E.H. and H.E.A.; methodology, H.E.A. and S.A.; software, E.H. and B.C.; validation, E.H., N.K., and İ.E.; formal analysis, S.İ.Ş, E.Ç.Ö. and H.E.A.; investigation, E.H.; resources, E.H. and N.K.; data curation, E.H., A.Ö.U. and İ.E. ; writing—original draft preparation, E.H. and S.A.; writing—review and editing, E.H., S.İ.Ş., E.Ç.Ö. and H.E.A.; visualization, E.H. and İ.E.; supervision, E.H. and H.E.A.; project administration, E.H. and S.A.; funding acquisition, N.K. and İ.E. All authors have read and agreed to the published version of the manuscript..
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Haseki Training and Research Hospital (protocol code: 02-2023 and date of approval: 11 January 2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| NAFLD | Non-alcoholic fatty liver disease |
| TG | Triglyceride |
| HDL | High-density lipoprotein |
| AST | Aspartate aminotransferase |
| ALT | Alanine aminotransferase |
| NASH | Non-alcoholic steatohepatitis |
| US | Ultrasound |
| CT | Computed tomography |
| MRI | Magnetic resonance imaging |
| APRI | AST to platelet ratio index |
| FIB-4 | Fibrosis-4 |
| EASL | European Association for the Study of the Liver |
| ROC | Receiver operating characteristic |
| WBC | White blood cell |
| ALP | Alkaline phosphatase |
| LDH | Lactate dehydrogenase |
| CRP | C-reactive protein |
| PLT | Platelet |
References
- Pouwels S, Sakran N, Graham Y, et al. Non-alcoholic fatty liver disease (NAFLD): a review of pathophysiology, clinical management and effects of weight loss. BMC Endocr Disord. 2022 Mar 14;22(1):63. [CrossRef] [PubMed] [PubMed Central]
- Zhang F, Han Y, Zheng L, et al. Association between chitinase-3-like protein 1 and metabolic-associated fatty liver disease in patients with type 2 diabetes mellitus. Ir J Med Sci. 2024 Aug;193(4):1843-1853. [CrossRef] [PubMed]
- McCullough, AJ. The clinical features, diagnosis and natural history of nonalcoholic fatty liver disease. Clin Liver Dis. 2004 Aug; 8(3): 521-33, viii. [CrossRef] [PubMed]
- Reccia I, Kumar J, Akladios C, et al. Non-alcoholic fatty liver disease: A sign of systemic disease. Metabolism. 2017 Jul;72:94-108. [CrossRef]
- Lombardi R, Iuculano F, Pallini G, et al. Nutrients, Genetic Factors, and Their Interaction in Non-Alcoholic Fatty Liver Disease and Cardiovascular Disease. Int J Mol Sci. 2020 Nov 19;21(22):8761. [CrossRef] [PubMed] [PubMed Central]
- Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of non-alcoholic fatty liver disease: practice Guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Hepatology. 2012;55(6):2005-23. [CrossRef] [PubMed]
- Schwenzer NF, Springer F, Schraml C, et al. Non-invasive assessment and quantification of liver steatosis by ultrasound, computed tomography and magnetic resonance. J Hepatol. 2009;51(3):433-45. Epub 20090611. [CrossRef] [PubMed]
- Hernaez R, Lazo M, Bonekamp S, et al. Diagnostic accuracy and reliability of ultrasonography for the detection of fatty liver: a meta-analysis. Hepatology. 2011 Sep 2;54(3):1082-1090. [CrossRef] [PubMed]
- Zou Y, Zhong L, Hu C, et al. Association between the alanine aminotransferase/aspartate aminotransferase ratio and new-onset non-alcoholic fatty liver disease in a nonobese Chinese population: a population-based longitudinal study. Lipids Health Dis. 2020 Nov 25;19(1):245. [CrossRef]
- Rigamonti AE, Bondesan A, Rondinelli E, et al. The Role of Aspartate Transaminase to Platelet Ratio Index (APRI) for the Prediction of Non-Alcoholic Fatty Liver Disease (NAFLD) in Severely Obese Children and Adolescents. Metabolites. 2022 Feb 8;12(2):155. [CrossRef] [PubMed]
- Powell EE, Wong VW, Rinella M. Non-alcoholic fatty liver disease. Lancet. 2021 Jun 5;397(10290):2212-2224. [CrossRef]
- Younossi, ZM. Non-alcoholic fatty liver disease–a global public health perspective. Journal of hepatology. 2019;70(3):531-44.
- Tabacu L, Swami S, Ledbetter M, et al. Socioeconomic status and health disparities drive differences in accelerometer-derived physical activity in fatty liver disease and significant fibrosis. PLoS One. 2024 ;19(5):e0301774. 9 May. [CrossRef]
- Summart U, Thinkhamrop B, Chamadol N, et al. Gender differences in the prevalence of nonalcoholic fatty liver disease in the Northeast of Thailand: A population-based cross-sectional study. F1000Res. 2017;6:1630. Epub 20170904. [CrossRef]
- Eguchi Y, Hyogo H, Ono M, et al. Prevalence and associated metabolic factors of nonalcoholic fatty liver disease in the general population from 2009 to 2010 in Japan: a multicenter large retrospective study. J Gastroenterol. 2012;47(5):586-95. Epub 20120211. [CrossRef]
- Kim KS, Hong S, Han K, et al. Association of non-alcoholic fatty liver disease with cardiovascular disease and all cause death in patients with type 2 diabetes mellitus: nationwide population based study. BMJ. 2024 Feb 13;384:e076388. [CrossRef]
- Ballestri S, Zona S, Targher G, et al. Nonalcoholic fatty liver disease is associated with an almost twofold increased risk of incident type 2 diabetes and metabolic syndrome. Evidence from a systematic review and meta-analysis. J Gastroenterol Hepatol. 2016;31(5):936-44. [CrossRef]
- Amernia B, Moosavy SH, Banookh F, et al. FIB-4, APRI, and AST/ALT ratio compared to FibroScan for the assessment of hepatic fibrosis in patients with non-alcoholic fatty liver disease in Bandar Abbas, Iran. BMC Gastroenterol. 2021;21(1):453. [CrossRef]
- Leoni S, Tovoli F, Napoli L, et al. Current guidelines for the management of non-alcoholic fatty liver disease: A systematic review with comparative analysis. World J Gastroenterol. 2018;24(30):3361-73. [CrossRef]
- Long MT, Pedley A, Colantonio LD, et al. Development and Validation of the Framingham Steatosis Index to Identify Persons With Hepatic Steatosis. Clin Gastroenterol Hepatol. 2016 Aug;14(8):1172-1180.e2. [CrossRef]
- Lin MS, Lin HS, Chang ML, et al. Alanine aminotransferase to aspartate aminotransferase ratio and hepatitis B virus on metabolic syndrome: a community-based study. Front Endocrinol (Lausanne). 2022 Jul 29;13:922312. [CrossRef]
- Thong VD, Quynh BTH. Correlation of Serum Transaminase Levels with Liver Fibrosis Assessed by Transient Elastography in Vietnamese Patients with Nonalcoholic Fatty Liver Disease. Int J Gen Med. 2021;14:1349-55. [CrossRef]
- Jamialahmadi T, Bo S, Abbasifard M, et al. Association of C-reactive protein with histological, elastographic, and sonographic indices of non-alcoholic fatty liver disease in individuals with severe obesity. J Health Popul Nutr. 2023 Apr 7;42(1):30. [CrossRef]
- Hoekstra M, Van Eck M. High-density lipoproteins and non-alcoholic fatty liver disease. Atheroscler Plus. 2023 Aug 19;53:33-41. [CrossRef]
- Tomizawa M, Kawanabe Y, Shinozaki F, et al. Triglyceride is strongly associated with nonalcoholic fatty liver disease among markers of hyperlipidemia and diabetes. Biomed Rep. 2014 Sep;2(5):633-636. [CrossRef]
- Kawano Y, Cohen DE. Mechanisms of hepatic triglyceride accumulation in non-alcoholic fatty liver disease. J Gastroenterol. 2013;48(4):434-41. Epub 20130209. [CrossRef]
- Li X, Zhan F, Peng T, et al. Association between the Triglyceride-Glucose Index and Non-Alcoholic Fatty Liver Disease in patients with Atrial Fibrillation. Eur J Med Res. 2023 Sep 19;28(1):355. [CrossRef]
- Wu KT, Kuo PL, Su SB, et al. Nonalcoholic fatty liver disease severity is associated with the ratios of total cholesterol and triglycerides to high-density lipoprotein cholesterol. J Clin Lipidol. 2016;10(2):420-5.e1. [CrossRef]
- Fukuda Y, Hashimoto Y, Hamaguchi M, et al. Triglycerides to high-density lipoprotein cholesterol ratio is an independent predictor of incident fatty liver; a population-based cohort study. Liver Int. 2016;36(5):713-20. Epub 20151105. [CrossRef]
- Chen Z, Qin H, Qiu S, et al. Correlation of triglyceride to high-density lipoprotein cholesterol ratio with nonalcoholic fatty liver disease among the non-obese Chinese population with normal blood lipid levels: a retrospective cohort research. Lipids Health Dis. 2019;18(1):162. [CrossRef]
- Zhou YG, Tian N, Xie WN. Total cholesterol to high-density lipoprotein ratio and nonalcoholic fatty liver disease in a population with chronic hepatitis B. World J Hepatol. 2022 Apr 27;14(4):791-801. [CrossRef]
- Ozkan, S. Incidence of nonalcoholic fatty liver disease in type 2 diabetic patients. Yeditepe Medical Journal 2016;12(37-38): 960-967. [CrossRef]
- Sefa Sayar M, Bulut D, Acar A. Evaluation of hepatosteatosis in patients with chronic hepatitis B virus infection. Arab J Gastroenterol. 2023 Feb;24(1):11-15. [CrossRef]
- Yin JY, Yang TY, Yang BQ, et al. FibroScan-aspartate transaminase: A superior non-invasive model for diagnosing high-risk metabolic dysfunction-associated steatohepatitis. World J Gastroenterol. 2024 ;30(18):2440-2453. 14 May. [CrossRef]
- Rigor J, Diegues A, Presa J, et al. Noninvasive fibrosis tools in NAFLD: validation of APRI, BARD, FIB-4, NAFLD fibrosis score, and Hepamet fibrosis score in a Portuguese population. Postgrad Med. 2022 May;134(4):435-440. [CrossRef]
- Nanji AA, French SW, Freeman JB. Serum alanine aminotransferase to aspartate aminotransferase ratio and degree of fatty liver in morbidly obese patients. Enzyme. 1986;36(4):266-9. [CrossRef]
Figure 1.
Flow diagram of participants.
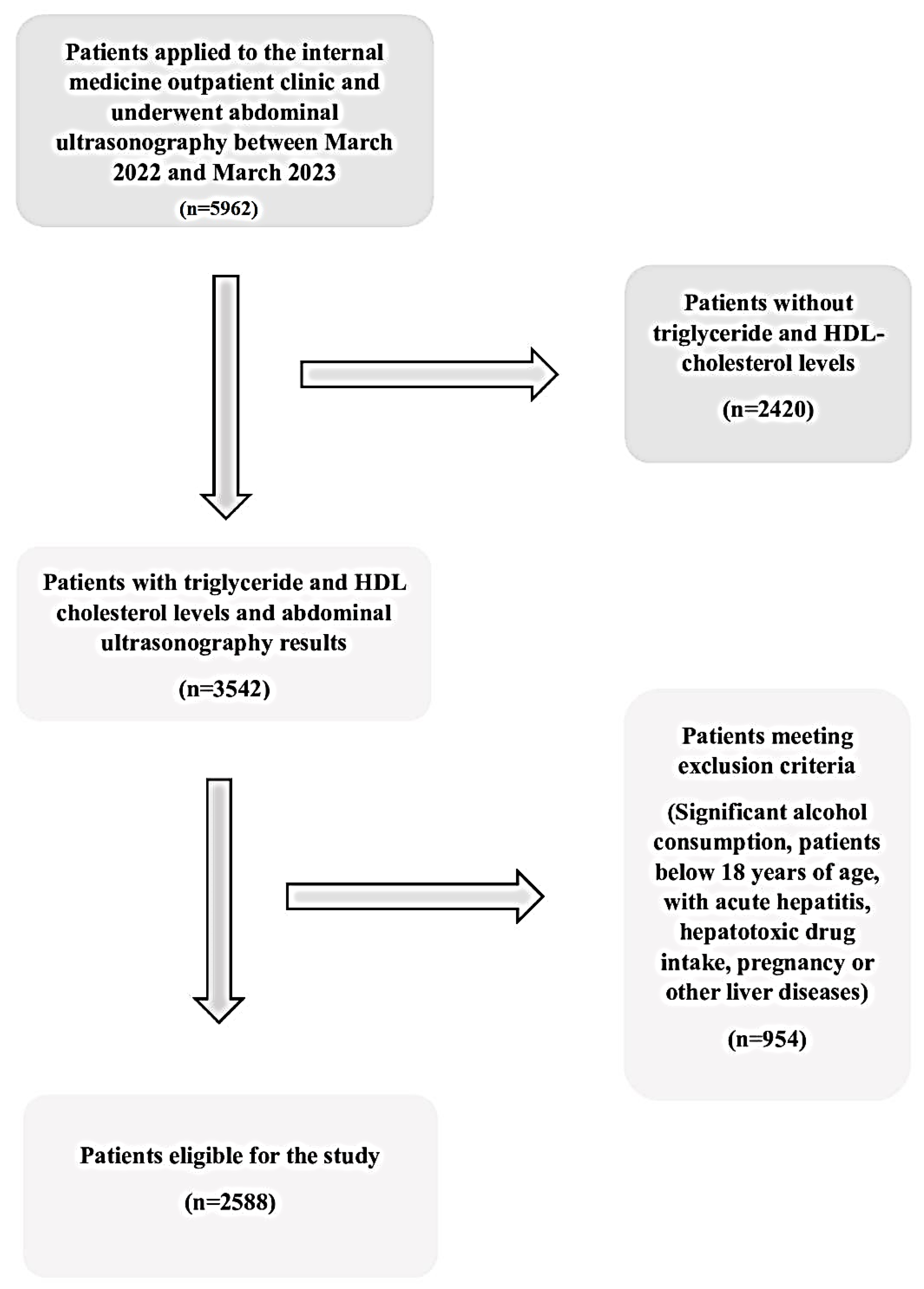
Figure 2.
Boxplot graphic of TG/HDL ratio according to NAFLD presence and gender.
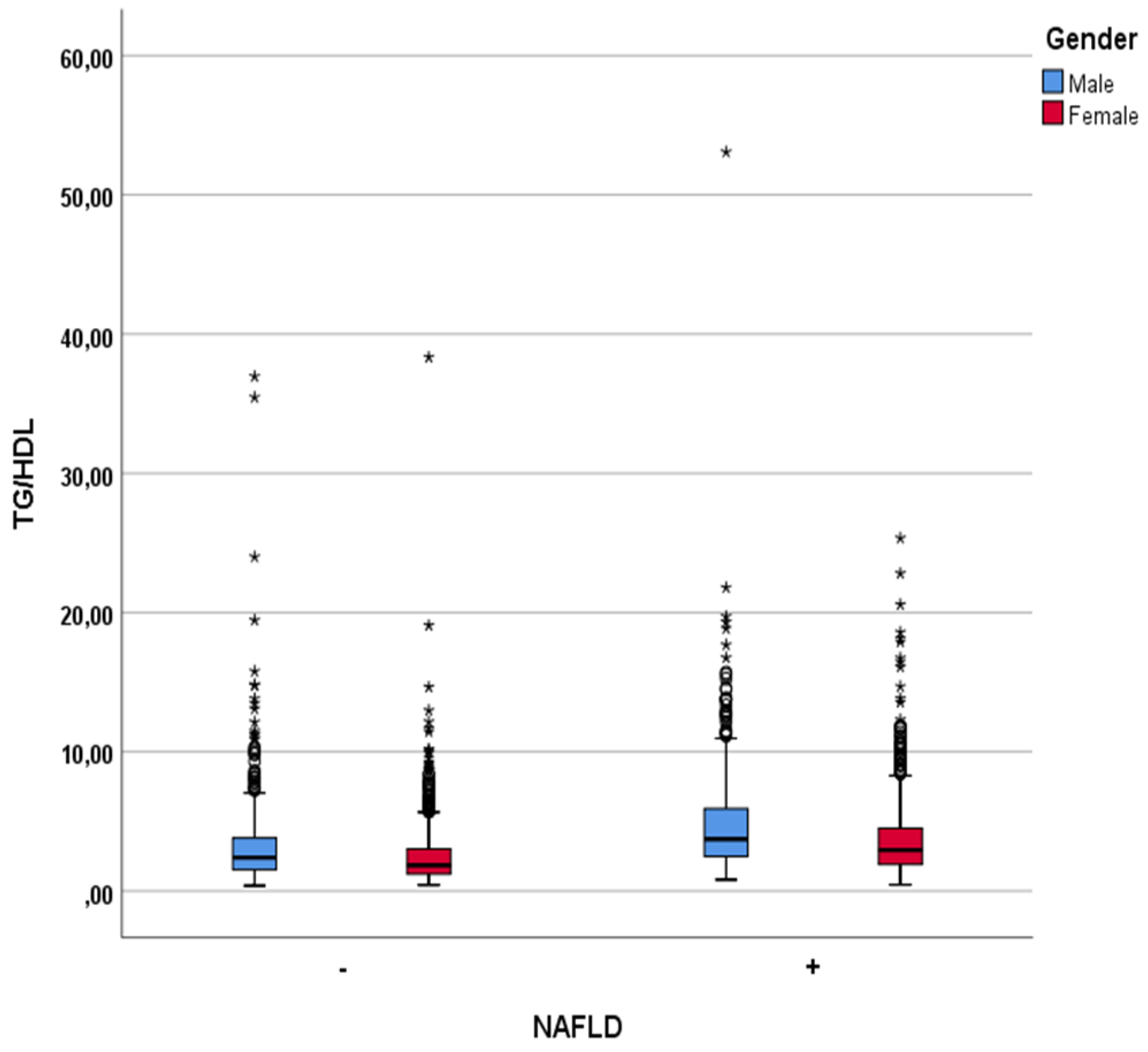
Figure 3.
ROC curve analysis of non-invasive parameters for predicting NAFLD.
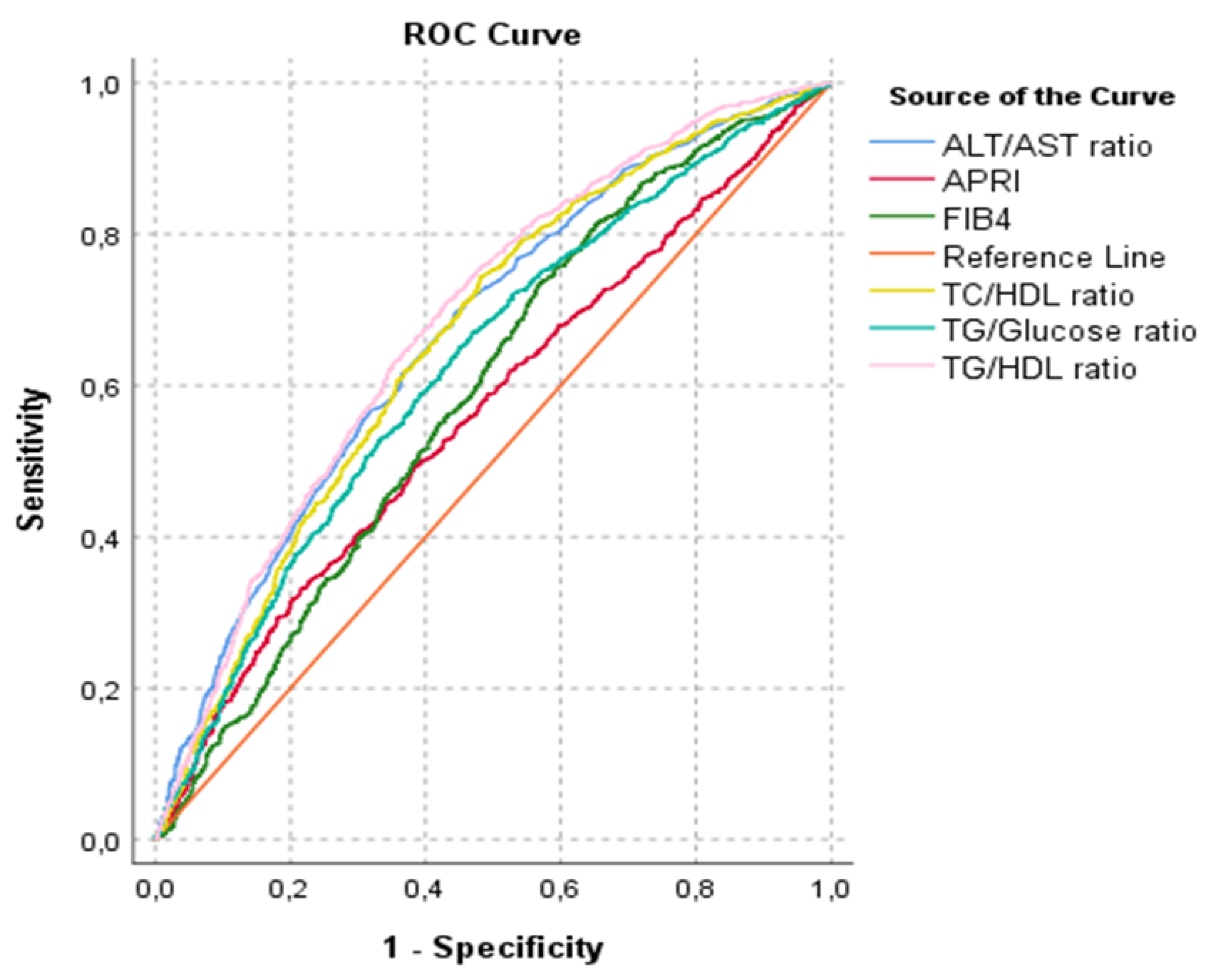

Table 1.
Descriptive characteristics and laboratory findings of entire patient group.
| Characteristics and Findings |
Entire patients (n:2588) |
|---|---|
| Gender (F/M) | 1631/957 |
| Age (years) | 45.31±12.50 |
| WBC (109/L) | 7.35±1.93 |
| Neutrophil (109/L) | 4.32±1.50 |
| Hemoglobin (g/L) | 13.58±1.78 |
| Platelets (109/L) | 258.81±70.92 |
| Glucose (>mg/dl) | 109.34±41.40 |
| HbA1c (%) | 6.25±1.48 |
| AST (U/L) | 24.80±38.88 |
| ALT (U/L) | 29.91±49.99 |
| ALP (IU/L) | 84.37±36.09 |
| LDH (U/L) | 182.75±47.96 |
| Creatinine (>mg/dl) | 0.75±0.16 |
| Triglyceride (>mg/dl) | 147.42±93.89 |
| HDL cholesterol (>mg/dl) | 49.28±12.82 |
| Total cholesterol (>mg/dl) | 189.23±41.0 |
| Uric acid (>mg/dl) | 4.70±1.31 |
| Albumin (g/l) | 45.63±3.0 |
| CRP (mg/l) | 4.91±9.32 |
n: number of patients, F: female, M: male, WBC: white blood cell, HbA1c: hemoglobin A1c, AST: aspartate aminotransferase, ALT: alanine aminotransferase, ALP: alkaline phosphatase, LDH: lactate dehidrogenase, HDL: high-density lipoprotein, CRP: c-reactive protein.
Table 2.
Characteristics and laboratory findings of NAFLD and non-NAFLD groups.
| Characteristics and Findings |
Patients without NAFLD (n:1270) |
Patients with NAFLD (n:1318) |
p-Value |
|---|---|---|---|
| Age (years) | 41.42±13.33 | 49.07±10.34 | <0.001 |
| Gender (F/M) | 811/459 | 820/498 | 0,249 |
| WBC (109/L) | 7.11±1,91 | 7,58±1.92 | <0.001 |
| Neutrophil (109/L) | 4.23±1.56 | 4.40±1.45 | 0.005 |
| Hemoglobin (g/L) | 13,4±1,85 | 13,76±1,70 | <0.001 |
| Platelets (109/L) | 257.26±76.02 | 260.31±65.62 | 0.275 |
| Glucose (>mg/dl) | 100.63±31.48 | 117.73±47.61 | <0.001 |
| HbA1c (%) | 5.88±1.30 | 6.52±1.54 | <0.001 |
| AST (U/L) | 22.67±30.62 | 26.84±45.33 | <0.001 |
| ALT (U/L) | 24.02±36.87 | 35.60±59.45 | <0.001 |
| ALP (IU/L) | 82.38±42.0 | 86.45±28.49 | 0.013 |
| LDH (U/L) | 178.05±46.45 | 187.77±49.06 | <0.001 |
| Creatinine (>mg/dl) | 0.74±0.15 | 0.76±0.16 | <0.001 |
| Triglyceride (>mg/dl) | 122.67±80.57 | 171.27±99.50 | <0.001 |
| HDL cholesterol (>mg/dl) | 51.26±13.54 | 47.37±11.78 | <0.001 |
| Total cholesterol (>mg/dl) | 181.16±40.62 | 197.02±39.88 | <0.001 |
| Uric acid (>mg/dl) | 4.34±1.22 | 5.06±1,30 | <0.001 |
| Albumin (g/l) | 45.41±3.28 | 45.83±2.70 | 0.002 |
| CRP (mg/l) | 4.31±9.85 | 5,49±8.75 | 0.007 |
1 n: number of patients, NAFLD: non-alcoholic fatty liver disease, F: female, M: male, WBC: white blood cell, HbA1c: hemoglobin A1c, AST: aspartate aminotransferase, ALT: alanine aminotransferase, ALP: alkaline phosphatase, LDH: lactate dehidrogenase, HDL:high-density lipoprotein, CRP:c-reactive protein. 2 p<0.05: statistically significance, significant values are shown in bold.
Table 3.
Association of non-invasive parameters with NAFLD.
| Patients without NAFLD (n:1270) |
Patients with NAFLD (n:1318) |
p-Value | |
|---|---|---|---|
| TG/HDL ratio | 2.79±2.83 | 4.08±3.30 | <0.001 |
| TC/HDL ratio | 3.75±1.39 | 4.36±1.24 | <0.001 |
| ALT/AST ratio | 0.99±0.39 | 1.23±0.49 | <0.001 |
| APRI | 0.32±0.64 | 0.35±0.62 | <0.001 |
| FIB-4 score | 0.85±0.80 | 0.93±0.50 | <0.001 |
| TG/Glucose ratio | 1.24±0.74 | 1.54±0.88 | <0.001 |
1 n: number of patients, TG: triglyceride, HDL: high-density lipoprotein, TC: total cholesterol, ALT: alanine aminotransferase, APRI: AST to platelet ratio index, FIB-4: fibrosis 4) 2 p<0.05: statistically significance, significant values are shown in bold.
Table 4.
AUROC and %95 CI of non-invasive parameters for predicting NAFLD.
| AUROC for NAFLD (%95 CI) | p-Value | |
|---|---|---|
| Tg/HDL ratio | 0.682 (0.662-0.703) | <0.001 |
| TC/HDL ratio | 0.661 (0.640-0.682) | <0.001 |
| ALT/AST ratio | 0.668 (0.647-0.689) | <0.001 |
| APRI | 0.565 (0.543-0.587) | <0.001 |
| FIB-4 | 0.591 (0.569-0.613) | <0.001 |
| Tg/Glucose ratio | 0.626 (0.604-0.647) | <0.001 |
1 n: number of patients, TG: triglyceride, HDL: high-density lipoprotein, TC: total cholesterol, ALT: alanine aminotransferase, APRI: AST to platelet ratio index, FIB-4: fibrosis 4). 2 p<0.05: statistically significance, significant values are shown in bold.
Table 5.
Distribution of patients according to the determined cut-off value of the TG/HDL ratio.
| TG/HDL Ratio | N of Patients Without NAFLD | N of Patients with NAFLD |
Total | p-Value |
|---|---|---|---|---|
| <1.86 | 578 | 254 | 832 |
<0.001 |
| ≥1.86 | 692 | 1064 | 1756 | |
| Total | 1270 | 1318 | 2588 |
1 (n: number of patients, TG: triglyceride, HDL: high-density lipoprotein, NAFLD: non-alcoholic fatty liver disease) 2 p<0.05: statistically significance, significant value is shown in bold.
Table 6.
Correlations of TG/HDL ratio with demographic and clinical parameters.
| Parameter | r (95% CI) | p |
|---|---|---|
| Age | 0.139 (0.066-0.210) | <0.001 |
| WBC | 0.183 (0.114-0.246) | <0.001 |
| Hgb | 0.213 (0.140-0.287) | <0.001 |
| PLT | -0.008 (-0.083-0.062) | 0.818 |
| Creatinine | 0.174 (0.102-0.237) | <0.001 |
| AST | 0.146 (0.077-0.212) | <0.001 |
| ALT | 0.229 (0.158-0.296) | <0.001 |
| Uric acid | 0.272 (0.208-0.337) | <0.001 |
| Glucose | 0.244 (0.179-0.309) | <0.001 |
| HbA1c | 0.242 (0.168-0.311) | <0.001 |
| LDH | 0.021 (-0.044-0.090) | 0.554 |
| APRI | 0.109 (0.038-0.178) | 0.002 |
| FIB-4 | 0.061 (-0.010-0.134) | 0.084 |
| ALT/AST ratio | 0.249 (0.183-0.315) | <0.001 |
| TG/Glucose ratio | 0.795 (0.763-0.825) | <0.001 |
1 WBC: white blood cell, Hgb: hemoglobin, PLT: platelets, AST: aspartate aminotransferase, ALT: alanine aminotransferase, LDH: lactate dehidrogenase, APRI: AST to platelet ratio index, FIB-4: fibrosis 4 score, TG: triglyceride 2 p<0.05: statistically significance, significant values are shown in bold.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



