
Submitted:
12 June 2025
Posted:
16 June 2025
You are already at the latest version
Abstract
Viral hepatitis continues to pose a significant public health issue in Nigeria, where the various types of viral hepatitis (hepatitis A, B, C, D, and E) are endemic. Even with vaccines and antiviral treatments available, the burden of disease remains due to limited healthcare access, socio-economic inequalities, and insufficient public health infrastruc-ture. The high rates of hepatitis B and C, along with the common occurrence of hepatitis A and E, highlight the urgent need for comprehensive and culturally appropriate in-tervention strategies. Traditional medicine (TM), particularly the utilization of indigenous medicinal plants, plays an essential role in managing hepatitis in marginalized com-munities. Ethnobotanical studies have discovered numerous plant species with potential antiviral properties. However, incorporating these remedies into mainstream healthcare is challenged by concerns regarding safety, standardization, and regulatory control. This review examines the epidemiology of viral hepatitis in Nigeria, the role of TM in its treatment, and the developing regulatory framework overseeing herbal remedies. It stresses the necessity of clinical validation, standardized protocols, and better training for practitioners to ensure the safe and effective incorporation of TM into national hepatitis control efforts.
Keywords:
viral hepatitis
; epidemiology
; endemic diseases
; medicinal plants
; herbal remedies
; regulatory oversight
1. Introduction
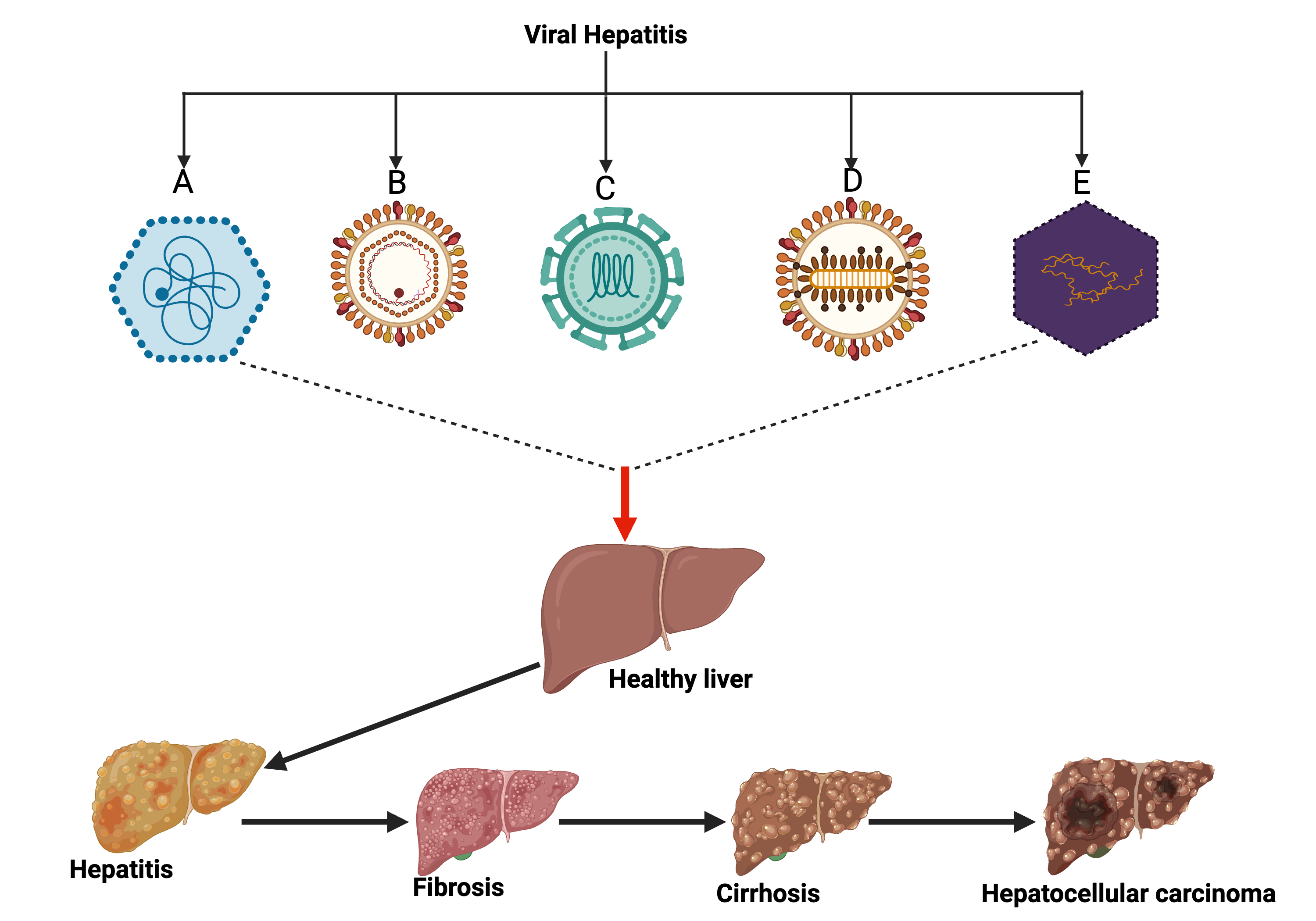
Viral hepatitis (Figure 1) includes a set of infectious diseases caused by five (5) main virus types: hepatitis A virus (HAV), hepatitis B virus (HBV), hepatitis C virus (HCV), hepatitis D virus (HDV), and hepatitis E virus (HEV) [1,2]. These viruses target the liver, resulting in conditions that range from acute self-limiting infections to chronic liver damage, cirrhosis, and hepatocellular carcinoma (HCC) [3,4,5,6]. Viral hepatitis poses a significant global health challenge, resulting in approximately 1.1 million deaths in 2019 and rising to 1.3 million in 2022. Among the five hepatitis types, B and C account for most of the morbidity and mortality due to their chronic nature and the potential for severe complications. Hepatitis B alone was responsible for 83% of these fatalities, while hepatitis C contributed 17%. In the WHO-focused countries, 80% of hepatitis-related deaths occur, with Africa alone bearing 55% of the worldwide viral hepatitis burden [7]. Africa, which hosts a large share of the world's population, bears a disproportionately high burden of viral hepatitis [8]. The continent experiences high rates of hepatitis B and C [9], with transmission influenced by socio-economic factors, cultural customs, and deficiencies in healthcare systems [10,11,12,13]. In areas with poor sanitation, hepatitis A and E, mainly spread through contaminated food and water [14,15,16], remain prevalent, while hepatitis D, linked to hepatitis B as a co-infection or superinfection [17,18], presents another challenge in regions where hepatitis B is often endemic.
Despite the existence of efficacious preventive measures, including vaccines for hepatitis A and B and curative modalities for hepatitis C, the endeavor to control viral hepatitis in Africa is impeded by a multitude of factors. Limited access to healthcare services, inadequate surveillance systems, social stigma, and deficient public health resources [19,20,21] collectively compound the persistent challenges. Additionally, socio-economic inequalities and political instability in certain areas worsen the disease burden, hindering advancement towards global health goals, particularly the WHO’s aims to eliminate viral hepatitis as a public health threat by 2030. Additionally, socio-economic inequalities and political instability in certain areas worsen the disease burden[22,23,24,25], hindering advancement towards global health goals, particularly the WHO’s aim to eliminate viral hepatitis as a public health threat by 2030 [7].
Viral hepatitis presents a major public health challenge in Nigeria. The country is divided into six geopolitical zones: North-Central, North-East, North-West, South-East, South-South, and South-West (Figure 2). Hepatitis A and E are endemic in Nigeria, primarily spread through the fecal-oral route, with hepatitis E specifically endangering pregnant women [26,27]. Hepatitis B is widespread and a primary contributor to liver disease, although vaccination initiatives are currently underway through the national immunization program[28,29]. Nigerians with limited access to direct-acting antivirals are affected by hepatitis C [30]. Hepatitis D, which co-infects individuals with hepatitis B, is less frequently reported but causes more severe liver complications [31,32]. To tackle these infections effectively, enhancements in vaccination, sanitation, surveillance, and accessibility of antiviral treatments are necessary. This review aims to provide a thorough overview of viral hepatitis in Nigeria, highlighting its epidemiology and transmission dynamics. It also explores the role of traditional medicine, particularly indigenous ethnomedicinal practices, in managing hepatitis while assessing the regulatory frameworks and challenges involved in integrating these practices into the national healthcare system.
2. Epidemiology of Viral Hepatitis in Nigeria
Viral hepatitis remains a significant public health issue globally. Its prevalence and incidence vary significantly across regions and populations. Differences in healthcare access, socio-economic status, cultural practices, and public health infrastructure influence these variations [8,12,15,18,22,23]. There are five (5) hepatitis viruses known to healthcare. They include hepatitis HAV, HBV, HCV, HDV, and HEV [33,34]. They tend to have a considerable impact on human health, with the ability to cause acute and chronic infections [1]. HAV and HEV are transmitted by contaminated water and food [35], while HBV and HCV are mainly transmitted through bloodborne [36,37]. Despite them having different routes of transmission, they all share common transmission routes, such as having close contact within a household, transfusion of blood, transplantation of an infected allograft, transmission from a pregnant mother to her child, and unprotected sex with an infected person [1,34,35,36,38].
HAV
HAV is classified within the hepatoviral genus of the Picornaviridae family [39]. HAV (Figure 3) exists in two infectious forms: quasi-enveloped and non-enveloped (naked) virions. The quasi-spheroids, which are surrounded by lipid membranes, primarily reside in the circulatory system and cell culture medium. As they move through the biliary canaliculus, bile acids act as detergents, effectively removing the lipid envelope and producing naked virions, which are then excreted in faeces[40]. HAV has a single-stranded positive-sense RNA genome that is roughly 7.5 kilobases long [41]. Additionally, HAV is notably resistant to extreme physical and environmental conditions, including high temperatures, acidic environments, and freezing, allowing it to survive for hours or even months [42,43]. This increased resistance results from the virus’s structurally strong, folding-dependent, and cohesive capsid [44]. The interaction between its environmental stability and the high viral load found in the faeces of infected individuals highlights the critical link between Hepatitis A Virus (HAV) transmission and poor hygiene or insufficient sanitation systems, especially through wastewater contamination [45].
HAV transmission usually occurs through a faecal-oral route, either directly via person-to-person contact or indirectly through consuming contaminated food or water. In developed countries, most outbreaks stem from direct contact, while sporadic cases tend to be linked to foodborne transmission. Nonetheless, recent outbreaks in industrialized nations have increasingly involved contaminated food items[46]; many have been associated with imported frozen foods, including berries, vegetables, and various ready-to-eat products [47]. Although infrequent, HAV transmission through bloodborne routes is still a possibility due to the temporary viremic phase in infected individuals. Historically, those receiving regular blood transfusions, particularly patients with hemophilia, were considered at greater risk and prioritized for vaccination[48,49].
Worldwide, approximately 100 million HAV infections are reported annually, resulting in nearly 1.5 million symptomatic cases and between 15,000 - 30,000 deaths each year [50]. A recent analysis of the Global Burden of Disease (GBD) 2019 database indicates that hepatitis A exhibits the highest incidence among the four primary types of acute viral hepatitis: A, B, C, and E [51]. Nonetheless, the global age-standardized incidence rate of HAV has remained consistent from 1990 - 2019, while there has been a significant decrease in age-standardized disability-adjusted life years (DALYs) over that time, which suggests improved disease outcomes [52]. The incidence rates of hepatitis A differ significantly across countries and are closely tied to their socio-demographic index (SDI). Low and middle-income nations, especially in Africa and South Asia [53], bear the heaviest burden of HAV infection. The effects of HAV are frequently evaluated through seroprevalence surveys that detect anti-HAV immunoglobulin G (IgG), indicating past exposure to the virus [54].
In Nigeria, extensive research has been conducted on the seroprevalence of HAV across various regions (Figure 4). For instance, Sule et al. . [55] examined HAV prevalence in Osogbo, Osun State, where they found that 98.9% of participants displayed positive results for anti-HAV-IgG antibodies. In another investigation, Afegbua et al. [56] examined the seroprevalence of HAV infections among schoolchildren and adolescents in Kaduna, Nigeria. They noted that seropositivity differed by age, with rates of 4.6% in children aged 11-15 years and 40% in those under five. This variation was linked to poor sewage disposal and parental education levels.
Similarly, Ikobah et al. [26] analysed the seroprevalence and risk factors of HAV infection among children in Cross River State, Nigeria, finding that 224 subjects were positive for total anti-HAV antibodies, leading to a prevalence rate of 55.2%: 101 males (45.1%) and 123 females (54.9%). Additionally, Ogefere and Egbe [57] looked into HAV seroprevalence in Benin City, Nigeria, identifying three samples testing positive for anti-HAV IgM, attributing the high prevalence in Benin City to substandard hygiene practices. Collectively, these studies highlight the prevalence of HAV in Nigeria.
HBV
HBV (Figure 5) continues to pose a major global health threat, especially in developing countries where prevalence rates are considerably higher [58]. Over 2 billion people around the world are estimated to have been infected with HBV at some stage, with 350-400 million living with chronic infections [59]. The risk of developing a chronic HBV infection decreases with the age at which the infection occurs [60]. Neonates infected at birth, particularly those born to HBsAg and HBeAg positive mothers, face a 90% chance of becoming chronic carriers. Chronic HBV infection is responsible for about 80% of global HCC cases, making it a leading cause of liver-related deaths, particularly in Africa and Asia [61].
While 90-95% of adults typically clear acute HBV infections without long-term complications, an estimated 5-10% become chronic carriers. Among chronic carriers, roughly 25% will die from liver-related complications such as cirrhosis, while others may remain long-life carriers or eventually clear the virus [62]. HBV mainly spreads via unprotected sex, contact with infected blood or blood products, and using contaminated medical instruments or personal items. [63]. Importantly, perinatal transmission poses a major risk for severe liver diseases in early adulthood [60].
In Nigeria, the HBV infection rate, illustrated in Figure 6, remains significantly high, positioning the country among areas with considerable endemic transmission[64]. Iloh and Ikwudinma [65] estimate that around eighteen (18) million Nigerians are presently infected with HBV. A meta-analysis by Fakunle et al. [28] covering the years from 2000 to 2013 uncovered pooled prevalence rates of 13.6% in adults and 11.5% in children. Furthermore, other studies have shown particularly elevated prevalence rates in specific subpopulations: blood donors (25.7%)[66], surgeons (23.4%) [29], and infants (16.3%) [29]. Although pregnant women are often perceived as lower risk, a study by Mbaawuaga et al. [67] revealed HBV prevalence rates reaching 11% in this demographic. Various studies conducted across different regions of Nigeria have emphasized the prevalence of HBV infection, particularly among pregnant women. In Southwestern Nigeria, different seroprevalence rates of HBV were identified among pregnant women attending antenatal care in Ekiti State (4.0%) by Lesi et al. [68], Lagos State (6.08%) by Rabiu et al. [69], and Osun State (7.1%) by Opaleye et al., [70]. reported prevalence rates of 4.0%, 6.08% and 7.1%, respectively, among pregnant women attending antenatal care in Ekiti, Lagos, and Osun States. In addition, seroprevalence rates of 7.4% were observed by Shittu et al. [71] in Ondo State, 8.0% by Okonko et al. [72] in Ogun State, and 8.3% Anaedobe et al. [73] in Oyo State. In Southeastern Nigeria, prevalence rates among pregnant women have been reported. Studies by Ikeako et al. [74] reported a seroprevalence rate of 3.4% in Enugu State, Chima et al. [75] and Onwuakor et al. [76] reported similar seroprevalence rates of 7.1%. In South-South Nigeria, a seroprevalence rate of 2% among pregnant women was reported by Awanye et al. [77] in Port Harcourt. Seroprevalence rates of 6.6% and 7.9% were observed by Utoo et al. [78] in Cross River and Bayelsa States, respectively. In comparison, Oazuwa and Erhunwunselmade [79] documented a significantly higher prevalence of 21.1% among blood donors in Delta State. These findings point to an upward trend in HBV prevalence in South-South Nigeria.
In North-Central Nigeria, the prevalence of HBV also varies by state. A seroprevalence of 7.3% was documented by Terwase and Emeka [80] among staff quarter residents in the Federal Capital Territory (Abuja). Pregnant women in Kwara and Niger states had rates of 12.7% and 12.8%, respectively [81]. Higher prevalence rates were found in Kogi State (14.0% among farmers) [82], Plateau State (14.5% among individuals living with HIV) [83], and Nasarawa State (17.1% among female sex workers) [84]. The highest prevalence in the region was reported in Benue State at 20.0% among blood donors [85]. In North-West Nigeria, although HBV prevalence is lower, it is still a concern. Kaduna State had a rate of 3.9% among pregnant women[86], while Kano State reported 6% among HIV-positive individuals [64]. Sokoto State showed a slightly increased prevalence of 6.5% among pregnant women, according to Saidu et al. [87]. In the Northeast, Ndako et al. [88] and Imaranezor et al. [89] reported HBV prevalence rates of 5.3% and 6.0% among students in Gombe and Taraba states, respectively. Aliyu et al. [90] documented an 8.0% prevalence among children in Maiduguri, Borno State, while Okoye and Samba [91] noted a 9.0% rate in Mubi, Adamawa State. Alarmingly, the adjacent states of Bauchi and Yobe recorded seroprevalence rates of 18.0% and 49.0%, respectively, among blood donors and students [92].
HCV
HCV (Figure 7), a single-stranded RNA virus, infects both humans and chimpanzees, inducing comparable hepatic disease in the hosts. The predominant route of HCV transmission is parenteral, although sexual transmission also occurs [93]. HCV is notably more infectious than Human Immunodeficiency Virus (HIV), with estimates suggesting it is up to four times more transmissible and capable of causing infection with a lower inoculum [94]. Globally, HCV is recognized as a major contributor to chronic liver disease, including cirrhosis and HCC [95].
The WHO estimates that around 170 million people globally are chronically infected with HCV, with approximately 3 to 4 million new infections occurring each year [96]. Although comprehensive data on HCV-associated morbidity and mortality in Africa are scarce, existing patterns suggest these metrics may exceed global estimates. The WHO reports approximately 75% of individuals infected with HCV develop chronic liver disease. Among this population, an estimated 1.6% progress to HCC, a malignancy characterized by a dismal prognosis and a mortality rate exceeding 80% [97]. HCV is transmitted through several well-documented routes, including exposure to infected blood, blood products, tissues, and organs; unsafe medical practices; healthcare-related exposures such as needle stick injuries [98]; intravenous drug use [99]; sexual contact [100]; transmission between mother and child during pregnancy [101]; and body piercing procedures [102]. In Africa, blood transfusion remains a significant transmission route, as only about 19% of donated blood is routinely screened for anti-HCV antibodies [103]. The primary barrier to comprehensive screening is the high cost of laboratory diagnostics. Additionally, inconsistent and inadequate screening protocols for blood donors further compound the risk of HCV. The prevalence of HCV has been widely documented in Nigeria (Figure 8). Adedeji et al.[30] investigated the seroprevalence patterns of HCV among internally displaced persons in Borno State, Nigeria. They found a seroprevalence rate of 1.3% for anti-HCV in pregnant and breast-feeding mothers. In Niger Delta, Nigeria, Ejele et al. [104] detected Anti-HCV in 11 subjects. The highest prevalence was found in individuals aged 30 to 39, while the lowest was observed in those aged 40 to 49. Furthermore, it was reported that HCV infection was more common among less educated subjects compared to highly educated participants. These studies confirm a high prevalence of anti-HCV and call for urgent health education and awareness in Nigeria to prevent the further spread of HCV.
HDV
HDV illustrated in Figure 9, is a single-stranded RNA virus featuring a compact genome of approximately 1700 ribonucleotides[105]. This genome is only slightly larger than that of certain plant viroids, placing HDV among the smallest viruses known to infect humans [106]. HDV operates as a defective satellite virus, dependent on HBsAg for its infection and replication. Its envelope is exclusively made up of surface proteins derived from HBV[105]. The HDV genome contains a single open reading frame that transcribes two variants of the hepatitis delta antigen (HDAg): S-HDAg (small HDAg) and L-HDAg (large HDAg). S-HDAg is crucial for both the initiation and continuation of viral replication. In contrast, L-HDAg plays a role in suppressing replication and assisting in HDV enveloping with HBV surface proteins [105]. Moreover, the HDV genome also includes several open reading frames (ORFs) whose functions remain largely unexplored, despite the active transcription of HDAg [107]. The two isoforms of HDAg are: small HDAg (S-HDAg), which consists of 195 amino acids, and large HDAg (L-HDAg), comprising 214 amino acids [107].
The prevalence of HDV in Nigeria shows significant variation across different regions (Figure 10), with rates documented between 4.3% - 31.6% in the Southwest [108,109], 18.9% and 10.8% in Abuja and Sokoto State[110]. In contrast, Benue State exhibits a lower antigen prevalence of 2.7% among HBsAg-positive individuals in the North-Central region, while Kano State reports a rate of 5.43% in the Northwest [111,112]. Such variations may indicate differences in healthcare accessibility, economic status, and cultural practices that affect disease spread. Research carried out in Cross River and Ekiti States found no HDV cases among patients undergoing antiretroviral therapy (ART) and pregnant women, respectively [113,114]. Another study reported regional variation in HBV prevalence across Nigeria, supporting the association between HDV distribution and HBV-endemic regions. Since HDV infection is contingent upon co-infection with HBV, areas with high HBV prevalence are likely to serve as HDV hotspots. This correlation highlights the necessity of region-specific public health interventions for HDV prevention and control. Such targeted strategies are especially critical in high-risk zones like the Northeastern part of the country, where proximity to Cameroon may enhance cross-border viral transmission, potentially contributing to increased HDV incidence in the region [115].
The investigation conducted by Ifeorah et al.[115] found that 64.7% of participants who were positive for HDV RNA were male. This trend aligns with the results of Nwokediuko and Ijeoma[116], who noted that the prevalence of HDV was 13% in males and 10.5% in females. Furthermore, research by Nwika et al. and Okonkwo et al. [117,118] showed that male patients had elevated liver enzyme levels and were at a higher risk for complications linked to HBV/HDV co-infection. Similarly, the findings of Ifeorah et al. and Okpokam et al. confirmed that the rates of HDV co-infection were higher in males than females[27,119]. However, a study from Plateau State, Nigeria, reported a greater HDV prevalence in females (14.8%) compared to males (5.5%), especially among those co-infected with HIV[120]. This discrepancy suggests that gender-related risk behaviors and vulnerabilities may vary between regions and demographics. In Southwest Nigeria, studies indicate that the peak incidence of hepatitis D virus (HDV) infection occurs in younger to middle-aged adults, particularly within the age groups of 21 – 30 and 31 – 40 [108,121]. Ifeorah et al. [27] also identified a significant prevalence among individuals under 20 years of age. Another study by Ifeorah et al. revealed that adults aged 41–50 years, especially those engaging in high-risk sexual behaviors, showed the highest prevalence of HDV [122]. In contrast, Lukman et al.'s research found no notable statistical connection between age and HDV infection[123]. These divergent patterns likely mirror age-related differences in exposure to risk factors, influenced by disparities in healthcare access, vaccination rates, and shifting behaviors over time.
HEV
HEV (Figure 11) is categorized as a single-stranded RNA virus within the Hepevirus genus of the Hepeviridae family. It is a significant agent of acute viral hepatitis globally [124]. Structurally, HEV exists in three forms: naked virion, quasi-enveloped virion and enveloped virus[125,126,127]. Human-infecting HEV strains are classified under the species Orthhepevirus A, which encompasses (HEV-1 to HEV-8) based on whole genome phylogenetic analysis [128]. Notably, genotypes HEV-1 through HEV-4 are established as human pathogens, with emerging evidence suggesting HEV-7 can also infect humans [129]. Genotypes HEV-1 and HEV-2 are exclusively associated with humans and are typically linked to outbreaks in resource-limited settings resulting from water contamination[124]. In contrast, HEV-3 and HEV-4 exhibit zoonotic potential, capable of transmitting to humans from various animals, primarily through the consumption of inadequately cooked animal products or direct contact with infected animals. The prevalence of genotypes 1 and 2 is particularly noted in numerous low-income regions, especially in specific areas of sub-Saharan Africa [130].
HEV has been reported in different areas of Nigeria (Figure 12). In the North-East region, an outbreak led to 1,815 suspected cases and eight reported deaths, underscoring the virus’s significant public health impact [131]. Despite the public health relevance of HEV, data on its seroprevalence, geographic distribution, and risk factors in Nigeria remain limited. Existing studies have reported highly variable anti-HEV seroprevalence rates across different regions of the country, ranging from 7% to as high as 93% [31]. Molecular evidence has also confirmed the circulation of HEV genotypes 1 and 2 in human populations within Nigeria [132]. Socioeconomic inequalities and limited access to vital services—especially clean drinking water and reliable healthcare—between urban and rural regions may play a role in the spread and persistence of HEV infections. In rural areas, these structural deficiencies are usually more significant, heightening the risk of encountering contaminated water sources. For example, Osun state, which encompasses both urban and rural environments, serves as a relevant area to explore these dynamics.
In a study conducted by Osundare et al. [133], the distribution of HEV infection in Osun State, Nigeria, was investigated, revealing a seroprevalence of 15.0% for total anti-HEV antibodies in the sampled communities. This estimate is comparable to the 13.4% seroprevalence found in Ekiti State, Nigeria[134]. The similarity in these findings may be influenced by shared cultural practices, similar socioeconomic conditions, and geographical proximity, as both states are situated in the South-West region of Nigeria. In contrast, higher anti-HEV seroprevalence rates have been reported in other studies across Nigeria. For instance, Ola et al. [31] found a prevalence of 44% among health workers and 93% among non-health workers in Ibadan, Oyo State, also in South-West Nigeria. Furthermore, Junaid et al. [32] reported a seroprevalence of 47.9% among apparently healthy individuals in Plateau State. The elevated rates observed in these studies may be partly due to the smaller sample sizes used, which can affect the variability and generalizability of their results. In the same study, individuals in rural communities exhibited a higher anti-HEV total antibody seroprevalence (20.1%) than those from urban communities (9.2%). Notably, the lowest seroprevalence rates were observed in Ede (8.0%) and Osogbo (11.4%), both urban settlements[133]. This disparity may be attributed to the relatively greater availability of social amenities in urban areas, including access to potable water supply, improved housing, better sanitation, reliable road infrastructure, and enhanced healthcare services, all of which may contribute to reduced HEV transmission.
In comparison, the seroprevalence of total anti-HEV antibodies was significantly high in the communities of Esa-Odo (22.0%), Ore (21.0%), and Oke-Osun (19.4%) [133]. These areas are largely rural and agricultural, indicating that farming practices may play a role in the increased seroprevalence. Contributing factors could include the use of animal dung as fertilizer, inadequate farm hygiene, and the consumption of stream water that may be contaminated with human or animal feces, all of which could enhance HEV transmission risk. The observations made by Osundare et al. support the findings of Junaid et al. [32], who noted a correlation between rural living and elevated anti-HEV seroprevalence. While the overall seroprevalence of antibodies was comparably high across Esa-Ode, Ore, and Oke-Osun, notable differences were observed in the rates of anti-HEV IgM seroprevalence: Esa-Ode and Ore recorded higher rates of 10.0% and 6.8%, respectively[133].
3. Role of Traditional Medicine in Treatment Practices
TM along with its active components are vital in treating hepatitis in Africa, providing distinctive antiviral and liver-protective benefits. They deliver positive therapeutic outcomes through antiviral effects and immunomodulation in patients with chronic hepatitis B. [135,136]. Demie et al. [137] and Aschale et al. [138] opined that medicinal plants gained widespread use in Ethiopian culture to treat certain diseases, including hepatitis, due to a lack of modern medicine. Social acceptability, affordability, accessibility, and effectiveness are other drivers of its use. Traditional treatment practices often emphasize symptom management and elicit elevated interest in natural bioactive compounds [139,140]. Natural products, usually extracted from plants or herbs and their derivatives have demonstrated significant potency against viral agents like viral hepatitis. They are considered to be the most economically beneficial treatment option with minimal side effects [141]. They impact different phases of the viral life cycle, including replication, release, and specific host interactions [142].
Numerous medicinal plants have undergone various in vitro and in vivo tests to investigate their bioactive properties and hepatoprotective mechanisms. Results have identified a diverse range of compounds, including terpenoids, alkaloids, flavonoids, furyl compounds, polyphenols, isoquinolines, lignans, coumarins, proteins, and other substances that inhibit viral DNA or RNA synthesis while promoting DNA repair and enhancing immune function[143,144]. Research indicates that R. nepalensis [145], S. incanum [146], and A. abyssinicus [147] exhibit anti-hepatitis properties. Additionally, combinations of R. nepalensis with S. incanum, as well as with C. macrostachyus and V. apiculata, have been shown to reduce serum HBV-DNA levels in treated patients145. Other herbs that have been studied for their hepatoprotective effects include Silybum marianum (L.) Gaertn., Glycyrrhiza glabra, Phyllanthus amarus Schumach. & Thonn., Schisandra chinensis (Turcz.), Capparis spinosa L., Solanum nigrum L., Ginkgo biloba L., Salvia miltiorrhiza Bunge., Astragalus membranaceus (Fisch.) Bunge, Cichorium intybus (L.), Sapindus mukorossi Gaertn., Woodfordia fruticosa (L.) Kurz, Vitex trifolia (L.), Cuscuta chinensis (Lam.), Lycium barbarum, Angelica sinensis (Oliv.) Diels, and Litsea coreana (H. Lev.), all of which have been explored for their hepatoprotective potentials and underlying mechanisms of action [148].
3.1. Selected Medicinal Plants Effective for Hepatitis Treatment and Their Possible Mechanism of Action
Silybum marianum (L.) Gaertn
Silybum marianum (L.) Gaertn, commonly known as Milk Thistle (Figure 13), is widely recognized as a natural herbal remedy for various chronic inflammatory liver conditions, including hepatitis, cirrhosis, fatty liver disease, and other liver-related injuries [149]. The bioactive compound extracted from S. marianum, silymarin (Figure 13), has been extensively studied in preclinical research and is known for its antioxidant and hepatoprotective properties[150,151,152]. Silymarin is a complex mixture of active compounds primarily consisting of flavonolignans (such as silibinin, isosilibinin, silichristin, and silidianin), flavonoids (like taxifolin and quercetin), and other polyphenolic substances[153]. According to Lu et al. [154], silymarin has shown effectiveness in treating both chronic and acute viral hepatitis, alcoholic liver disease, and liver cirrhosis. It is registered as a treatment for liver ailments in numerous countries across Europe, Asia, America, Africa, and Australia and has received approval for clinical trials targeting Hepatitis C virus infection[155]. Numerous studies have explored silymarin’s mechanisms of liver protection. Tunca et al.[156] concluded that silymarin reduces metabolic pyrimidine activation by lowering the concentration of cytochrome P450 1A1 proteins and modulating the expression of inducible nitric oxide synthase, which together provide a protective effect against pyridine-induced liver damage in Syrian hamsters. Additionally, silymarin helps sustain the liver’s glutathione levels by stabilizing membrane permeability and inhibiting lipid peroxidation [152].
Furthermore, silymarin protects the liver from toxic substances, such as carbon tetrachloride, by suppressing the production of tumor necrosis factor-alpha (TNF-α), interferon-gamma, and interleukin-2 (IL-2) and IL-4 [157,158]. This action effectively inhibits the activation of hepatic nuclear factor kappa B (NF-κB) (Figure 14), a crucial step in mitigating inflammation and safeguarding the liver from viral infections [157,159]. Silymarin achieves this by preventing the translocation of NF-κB to the nucleus, where it binds to various cytokine genes and suppresses their expression[160]. Moreover, silymarin can lower cellular uptake of xenobiotics by blocking organic ion transporters on hepatocyte surfaces[161] and inhibiting TNF-α expression induced by the toxin α-amanitin from poisonous mushrooms[162]. The hepatoprotective effect of silymarin is largely ascribed to its antioxidant activity, which counteracts the free radicals responsible for lipid peroxidation and contributes to cellular enzyme dysfunction, ultimately leading to fibrosis and cirrhosis.
Glycyrrhiza glabra (Licorice)
Glycyrrhizin (Figure 15), a natural compound derived from the roots of liquorice (Glycyrrhiza glabra), is widely recognized in folk medicine for treating various ailments, particularly liver diseases and drug-induced liver injuries[163]. Liquorice possesses anti-inflammatory and antioxidant properties, having been utilized to treat chronic hepatitis with notable improvements in liver histology and reductions in serum aminotransferases compared to placebo treatments [164,165]. It contains numerous phytocompounds, such as coumarins (including glycyrin, heniarin, liqcoumarin, and umbelliferone), flavonoids (flavonols and isoflavones), chalcones, and terpenoids (such as glycyrrhizic or glycyrrhizinic acid), with glycyrrhizic acid identified as the main active biological component [166]. Research by Kimura et al.[167] indicates that intraperitoneal administration of glycyrrhizin and epidermal growth factor (EGF) can significantly promote liver regeneration and restore liver function, likely through the stimulation of EGF receptors. Studies have demonstrated that glycyrrhizin can substantially reduce steatosis and necrosis in liver cells, inhibit interstitial inflammation and liver fibrosis, and support the regeneration of healthy cells[168,169]. Additionally, it acts to inhibit CD4+ T-cells and TNF-mediated cytotoxicity [170]. The extract of liquorice root stabilizes cellular membranes and enhances the endogenous production of interferons [171]. Notably, 18-β glycyrrhetinic acid has exhibited antiviral properties against multiple DNA and RNA viruses, potentially due to the activation of NF-kB and the induction of IL-8 [172]. Research by Ashfaq et al. has shown that liquorice generates a dose-dependent antiviral effect against HCV, comparable to interferon alpha, which may result from its capacity to decrease membrane fluidity and upregulate Cox-2 or related pathways[173].
Phyllanthus amarus Schumach & Thonn
P. amarus (Figure 16) is a small plant that typically grows in tropical areas and has been traditionally employed by practitioners to address various health issues, such as hepatitis B, jaundice, hypotension, inflammation, and oxidative stress [174,175]. Over 500 phytocompounds derived from different Phyllanthus species have been linked to notable bioactivities in cases like jaundice and digestive issues [176]. Phyllanthin (Figure 16), a bioactive compound derived from P. amarus leaves, has traditionally been employed in the treatment of various liver diseases Hanh, et al. [177]. Research by Xin-Hua et al. [178] revealed that the extract did not show a significant difference in the rates of negative conversion for HBeAg and HBV-DNA compared to interferon, indicating its potential therapeutic effect on chronic HBV. Studies suggest that its antioxidant properties may provide hepatoprotective effects against ethanol-induced oxidative damage in primary cultures of rat hepatocytes[179]. In cell culture experiments, P. amarus disrupts HBV enhancer I (EN I), which is essential for viral gene expression, leading to the downregulation of HBV mRNA transcription and replication[180].
Schisandra chinensis (Turcz.)
Schisandra chinensis (Figure 17), commonly referred to as the flavored fruit, is a deciduous woody vine renowned for its various traditional medicinal applications. The fruit is rich in dibenzocyclooctene lignans, primarily including schisandrin, schisandrin A, schisandrin B, and schisandrin C (Figure 16). Notably, research by Wu et al.[181] demonstrated that the combination of Schisandrin C and Luteolin effectively reduces hepatitis B virus (HBV) infection by inhibiting HBV replication and enhancing cGAS-STING pathway activation in macrophages. Furthermore, Zhao et al. [182] found that Schisandrin C triggered the cGAS-STING pathway, resulting in increased production of interferon β (IFN β) and enhanced expression of downstream genes. In their study, they noted that Schisandrin C exhibited anti-HBV effects, significantly decreasing the levels of HBeAg, HBcAg, HBsAg, and HBV DNA in a mouse model of HBV replication induced by hydrodynamic injection, while simultaneously elevating the production of IFN β and the expression of interferon-stimulated genes such as IFIT1, ISG15, and CXCL10. Mechanistically, Schisandrin C facilitated the interaction between TANK-binding kinase 1 (TBK1) and STING, essential for the phosphorylation of IRF3 and subsequent production of IFN β. Various bioactive compounds, such as triterpenoids, phenolic acids, flavonoids, polysaccharides, essential oils, vitamins, and phytosterols, play a significant role in the pharmacological activities and clinical potential of S. chinensis [183]. Research has highlighted the hepatoprotective properties of S. chinensis[184], establishing its fruit and extracts as effective agents in managing both chemical and viral liver injuries [185]. The hepatoprotective effects stem from multiple mechanisms, notably improved liver detoxification and tissue regeneration. A key mechanism includes the modulation of cytochrome P450 enzymes (like CYP3A and CYP2E1), which are essential for the metabolism of xenobiotics, thereby enhancing the hepatic clearance of toxins and drugs[186]. Following treatment with S. chinensis ethanol extract, significant reductions in glutamate oxaloacetate transaminase, glutamate pyruvate transaminase, and alkaline phosphatase levels were observed in rats' livers after acetaminophen-induced injury. Additionally, the extract was found to prevent centrilobular hepatic necrosis and elevate antioxidant levels, including glutathione peroxidase, superoxide dismutase, and catalase [187]. Furthermore, after treatment with S. chinensis, there was an increase in the synthesis and levels of intracellular glutathione (GSH) in hepatocytes, offering protection against oxidative damage[183].
Capparis spinosa L.
C. spinosa L. (commonly known as caper, Figure 18) is a plant native to the arid regions of Western and Central Asia. This plant has been utilized in traditional medicine for centuries to address various ailments, including rheumatism, gout, gastrointestinal issues, diabetes, as well as kidney and liver diseases[188,189,190]. Phytochemical analyses have identified several beneficial compounds within C. spinosa (Figure 18), such as flavonoids (including rutin, quercetin, and catechin), alkaloids (like spermidines and indoles), and glucosinolates (notably glucocapparin) [189,191]. Additionally, it contains minor quantities of other valuable compounds like kaempferol, stigmasterol, campesterol, tocopherols, and carotenoids[192]. At moderate levels, C. spinosa is also rich in vitamin C, carbohydrates, proteins, dietary fiber, and lipids [191]. Biological studies have demonstrated its antimicrobial, anti-inflammatory, immunomodulatory, antioxidant, and antiviral properties [189]. The extract of C. spinosa may positively influence liver health, as it has been linked to reduced gluconeogenesis and decreased fat accumulation in diabetic rats induced by streptozotocin. Furthermore, it is a key ingredient in Liv-52, a herbal remedy extensively used in Indian traditional medicine for treating various liver conditions[193]. A study involving 36 cirrhotic patients indicated that treatment with Liv-52 significantly lowered serum levels of ALT and AST, likely due to the protective effects endowed by its constituent herbs.
Solanum nigrum L.
S. nigrum (Black Nightshade) is a widely recognized herb that flourishes in temperate climate zones[194]. This plant has been utilized in TM as a powerful hepatoprotective agent[195]. The fruit of S. nigrum is thought to possess antitumor properties [196] and is traditionally used as a nerve tonic in Mexican folk medicine[197]. Research indicates that its hepatoprotective effects and other therapeutic benefits may be attributed to enhanced free radical scavenging and the inhibition of lipid peroxidation[198,199]. One study demonstrated that treatment with an aqueous extract of S. nigrum significantly reduced levels of serum alkaline phosphatase (ALP), serum glutamic-pyruvic transaminase (SGPT), serum glutamic oxaloacetic transaminase (SGOT), total bilirubin, and hydroxyl and superoxide radicals induced by CCl₄ in rats [200]. Additionally, research reported that at non-toxic concentrations, the methanolic extract of S. nigrum resulted in a 37% inhibition of HCV RNA expression, while a chloroform extract of S. nigrum seeds led to a more than 50% decrease in viral titer concentration [201].
Ginkgo biloba L.
G. biloba L. is a significant herb in Traditional Chinese Medicine, renowned for its therapeutic benefits against a range of diseases, supported by both human and animal studies. Its potential applications include treatment for Alzheimer’s disease, multi-infarct dementia, coronary heart disease, cerebral insufficiency, and renal ischemia-reperfusion injury [202,203,204]. This herb has demonstrated cardioprotective, anti-asthmatic, anti-diabetic, hepatoprotective, and photoprotective effects, along with mechanisms for DNA repair, as well as antioxidant and anti-inflammatory properties [205]. The therapeutic efficacy of G. biloba can largely be attributed to its diverse active components, which include two terpene lactones, flavonoids, and organic acids [206]. Many studies have linked G. biloba to hepatoprotective effects. Following treatment with G. biloba, levels of cellular antioxidant enzymes like glutathione peroxidase (GPX), glutathione S-transferase (GSTs), glutathione reductase, superoxide dismutase (SOD), catalase (CAT), and non-protein thiols have been shown to increase, further indicating its hepatoprotective characteristics [207].

Table 1.0.
Some medicinal plants, their bioactive agents and hepatoprotective potentials.
| Medicinal Plants | Major Bioactive Agents | Hepatoprotective Effects | References |
|---|---|---|---|
| Picrorhiza kurroa | Picroside I, picroside II, apocyanin, and cucurbitacins | It enhances antioxidant activities and scavenges the superoxide anion (O2•−). | [208,209] |
| Adrographis paniculata | Andrographolide | It inhibits viral replication and reduces liver inflammation and injury. It also modulates the NF-kB pathway, thereby decreasing the production of pro-inflammatory cytokines (IL-6, IL-1β, TNF-α), scavenges free radicals and enhances antioxidant activities. | [210-212] |
| Eclipta alba | Wedelolactone, demethylwedelolactone | It stimulates regeneration of hepatocytes, regulates the levels of hepatic microsomal drug-metabolizing enzymes, and inhibits HCV replication | [213,214] |
| Carica papaya | Papain, phenolic compounds, flavonoids, alkaloids (carpaine), cyanogenic chemicals (benzyl glucosinolates) | It decreases lipid peroxidation, pro-inflammatory cytokines such as tumour NF-α and IL-6, AST and ALT activies, and improves enzymatic antioxidants CAT and SOD. | [215] |
| Phyllanthus niruri L. | Quercetin rhamnoside, quercetin glucoside, gallic acid, geranin | It inhibits cellular DNA polymerase activity during HBV replication, HBV DNA synthesis and secretion of HBsAg and HBcAg | [216-218] |
| Musa sapientum L. | Alkaloids, phenols, terpenoids, flavonoids, phytosterols | It mediates antioxidant activities, improves hepatocyte regeneration, and inhibits the expression of inflammatory cytokines. Promotes the production of anti-inflammatory cytokines | [219] |
| Syzygium aromaticum L. | Eugenol, β-caryophyllene | It inhibits hepatic cell proliferation into fibroblasts, mediates antioxidant and anti-inflammatory activities, and enhances liver defence mechanism | [220,221] |
| Psidium guajava L. | Flavonoids, gallic acids, catechins, epicatechins | It lowers elevated levels of serum AST, ALT, ALP, and bilirubin, and neutralizes free radicals. | [222,223] |
| Ziziphus mauritiana L. | Phenolic compounds, flavonoids, tannins, alkaloids, saponins | It lowers AST, ALT, ALP, total bilirubin and lipid peroxide levels, prevents lipid peroxidation, and increases levels of glutathione and vitamin E | [224,225] |
| Entada africana Guill. & Perr. | Flavonoids, triterpenes, saponins, sugar | It enhances the expression of heme oxygenase-1 and 2’-5’ oligoadenylate synthetase-3, inhibits cytochrome P450 2E1 (CYP2E1), activates Nuclear factor-erythroid 2-related factors-2 (Nrf2) signaling pathway, and Inhibits HCV replication | [226,227] |
| Allium sativum L. | Allicin, alliin, diallyl sulfide, ajoene | Inhibit viral cell cycle. Reduction of cellular oxidative stress. Reduces viral load and improves liver function. Regulates lipid metabolism | [228,229] |
| Morus alba | Alkaloids (1-deoxynojirimycin), flavonoids, polyphenols | It inhibits the maturation of HBV, suppresses the glycosylation of viral envelop glycoproteins, reduces HBsAg, HBeAg, and HBV DNA, and inhibits the activity of HCV NS3 protease | [230,231] |
| Phyllanthus amarus Schum. & Thonn. | Lignans (phyllanthin and hypophyllanthin), flavonoids (quercetin) | It inhibits viral DNA polymerase and replication, mediates antioxidant and immunomodulatory activities, scavenges free radicals, and reduces lipid peroxidation of hepatic and intracellular membranes. | [232,233] |
| Momordica charantia L. | MAP30, α-momorcharin, triterpenes, saponins, flavonoids | It reduces liver inflammation, scavenges free radicals, reduces oxidative stress, inhibits viral DNA replication, HBV proteins (HBsAg and HBeAg) secretion in HepG2 cells, and stimulates hepatocyte regeneration | [234-236] |
| Adansonia digitata L. | Triterpenoids, flavonoids, tannin, carotenoids | It neutralizes free radicals, increases GSH, CAT, and SOD levels, reduces serum levels of AST, ALT, ALP, total bilirubin, and total proteins as well as lowers serum TNF-α level. | [237,238] |
| Schisandra chinensis | Schisandrin, Schisandrin A, Schisandrin B, and Schisandrin C | It enhances the activation of the cGAS-STING pathway. When combined with luteolin, it HBV replication and further stimulating the activation of the cGAS-STING pathway in macrophages. | [181,182] |
4. Safety Concerns and Regulation of Traditional Medicine in Nigeria
TM remains a crucial part of Nigeria's healthcare system, with a considerable portion of the population depending on herbal remedies and traditional practices for their primary healthcare needs. Nonetheless, concerns over these practices' safety, standardization, and regulation have led to efforts to establish more robust regulatory frameworks. The National Agency for Food and Drug Administration and Control (NAFDAC) is Nigeria's primary authority regulating traditional herbal medicines. NAFDAC's mandate encompasses registering, listing, and monitoring herbal products to ensure their safety and efficacy[239]. Herbal products undergo thorough evaluation for quality and safety[240]. Products that assert therapeutic claims supported by clinical trials receive complete registration and are renewable every five years [239]. Conversely, those lacking such evidence are listed with a disclaimer indicating that NAFDAC has not evaluated their claims, and this listing is subject to renewal every two years[239]. NAFDAC emphasizes the necessity of adherence to Good Manufacturing Practices (GMP) to minimize contamination and ensure product consistency [240].
Nevertheless, challenges persist due to insufficient standardization and documentation among practitioners. Despite regulatory efforts, several safety issues associated with TM practices in Nigeria have been identified. Research indicates that numerous herbal products may have dangerous components, including heavy metals like lead and mercury, as well as aflatoxins, which present serious health hazards [241]. Elevated levels of microbial contamination in herbal preparations have been reported, surpassing acceptable limits set by the World Health Organisation (WHO) [240]. A study among residents in Ikorodu, Lagos, revealed that while most believed herbal medicines were safe, a notable percentage experienced adverse effects, underscoring the need for public education on potential risks [242].
Numerous factors impede the effective regulation of TM in Nigeria. The variability in preparation methods and dosages complicates the establishment of consistent safety and efficacy standards [241]. A significant number of traditional practitioners depend on oral transmission of knowledge, resulting in a lack of formal records essential for evaluation and regulation. Furthermore, there exists a dearth of scientific studies validating the safety and efficacy of numerous traditional remedies, which hinders their integration into mainstream healthcare [242]. Practitioners frequently exhibit reluctance to disclose formulations due to concerns regarding exploitation, thereby obstructing collaborative research efforts[239,240]. To enhance the safety and regulation of TM in Nigeria, it is recommended that the government of Nigeria should strengthen the capacity of regulatory bodies, NAFDAC and the Lagos State Traditional Medicine Board (LSTMB), to enforce compliance with safety standards.
Scientific studies on traditional remedies should also be encouraged to establish evidence-based practices and implement training programs for traditional practitioners on Good Manufacturing Practices (GMP). Furthermore, efforts must be made to raise public awareness about herbal medicines' potential risks and benefits. NAFDAC should strive to build trust between traditional practitioners and researchers to facilitate knowledge sharing and integration into the national health system. By addressing these challenges through concerted efforts, Nigeria can effectively harness the benefits of TM while ensuring public safety and aligning with global best practices.
5.0. Future Perspectives
TM continues to be a crucial component of healthcare in Nigeria, particularly in managing chronic conditions like viral hepatitis. As the nation faces the dual challenges of a high prevalence of hepatitis and limited access to conventional treatments, the integration of TM presents both opportunities and obstacles. Recent studies emphasize the widespread use of medicinal plants for managing viral diseases, including hepatitis, in various regions of Nigeria. For example, an ethnobotanical survey conducted in northern Nigeria identified 131 plant species used by traditional healers to treat viral infections, with notable references to Phyllanthus amarus, Senna occidentalis, and Garcinia kola for hepatitis management. These findings highlight the rich biodiversity and traditional knowledge that can be leveraged for therapeutic purposes[243].
Nevertheless, the safety and efficacy of these remedies remain areas of concern. A study comparing the effectiveness of herbal and conventional interventions for Hepatitis B Virus (HBV) management indicated that although 73% of patients adopted herbal remedies, there was a significant variance in health outcomes, underscoring the need for standardized treatment protocols[244]. The lack of regulation surrounding many traditional remedies presents significant health risks. Studies show that patients seeking alternative treatments for hepatitis have encountered dangerous substances because of poorly regulated herbal products. These situations highlight the pressing need for strict regulatory frameworks to protect patient safety. Additionally, the lack of thorough clinical trials and standardized dosing protocols makes it difficult to integrate TM into mainstream healthcare. Although agencies like NAFDAC have started initiatives to register and oversee herbal products, a substantial portion of the informal sector continues to be largely unregulated.
To effectively utilize TM in the management of hepatitis, several strategic actions are essential. First, conducting clinical trials to assess the efficacy and safety of commonly used herbal remedies is crucial, as this process will support evidence-based integration into healthcare systems. Additionally, developing standardized methods for extraction and preparation will ensure consistent dosing and reduce variability in therapeutic outcomes. Training programs focusing on hygiene, accurate diagnosis, and referral systems should be established to bridge the gap between traditional and modern medicine. Educating the public about the benefits and potential risks of TM will empower patients to make informed healthcare choices. Furthermore, enhancing the capacity of regulatory bodies to monitor and evaluate herbal products will help mitigate risks associated with adulteration and contamination. Therefore, the integration of TM in managing viral hepatitis in Nigeria can significantly enhance healthcare delivery, especially in underserved areas. However, this process must be approached cautiously to maintain safety, efficacy, and quality. Through collaborative efforts among traditional practitioners, researchers, and regulatory bodies, Nigeria can establish a holistic and inclusive healthcare system that honors cultural heritage while prioritizing patient safety.
Author Contributions
Conceptualization, U.O.A, E.A.U, P.E.E, and S.O.; Methodology, U.O.A, E.G.U and D.C.E.; Software, U.O.A, D.C.E, C.E.O, C.C.A. and A.A; Validation, U.O.A, E.A.U, P.E.E, and S.O.; Formal analysis, U.O.A, E.G.U, D.C.E, C.E.O; Investigation, U.O.A, E.G.U, D.C.E, C.E.O, C.C.A, F.C.J, A.K.O, I.V.A, C.O.O., C.U.O., C.E.I; Data curation, U.O.A, D.C.E, CEO, CCA; Writing - original draft preparation, U.O.A, E.G.U, D.C.E., C.E.O, C.C.A, F.C.J, I.V.A, and C.O.O; Writing - review and editing, U.O.A, C.U.O., E.A.U, P.E.E, and S.O.; Visualization, U.O.A, E.G.U, C.C.A, V.C.N, and A.A; Project administration, U.O.A, E.A.U, P.E.E, and S.O. All authors have read and agreed to the published version of the manuscript.
Funding
The author(s) received no financial support for this article's research, authorship, and/or publication.
Institutional Review Board Statement
Not applicable to this study.
Informed Consent Statement
Not applicable.
Data Availability Statement
The dataset could be available on request.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviation
| ALP | - Alkaline Phosphatase |
| ALT | - Alanine Aminotransferase |
| ART | - Antiretroviral Therapy |
| AST | - Aspartate Aminotransferase |
| CAT | - Catalase |
| CCl₄ | - Carbon Tetrachloride |
| cGAS-STING | – Cyclic GMP-AMP synthase – Stimulator of interferon genes |
| COX-2 | - Cyclooxygenase 2 |
| DALYs | - Decline in Age-Standardised Disability adjusted life years |
| DNA | - Deoxyribonucleic Acid |
| EGF | - Epidermal growth factor |
| EN I | - Enhancer I |
| GBD | - Global Burden of Disease |
| GBD | - Global Burden of Disease |
| GMP | - Good Manufacturing Practices |
| GPX | - Glutathione peroxidase |
| GSH | - Glutathione |
| GST | - Glutathione S-transferase |
| HAV | - Hepatitis A Virus |
| HBcAg | - Hepatitis B Core Antigen |
| HBeAg | - Hepatitis B e-antigen |
| HBsAG | - Hepatitis B surface antigen |
| HBsAg | - Hepatitis B Surface Antigen |
| HBV | - Hepatitis B Virus |
| HCC | - Hepatocellular carcinoma |
| HCV | - Hepatitis C Virus |
| HDAg | - Hepatitis delta antigen |
| HDV | - Hepatitis D Virus |
| HEV | - Hepatitis E Virus |
| HIV | - Human Immunodeficiency Virus |
| IFIT1 | - Interferon Alpha/Beta Receptor 1 |
| IFN-γ | - Interferon-gamma |
| IgG | - Immunoglobulin G |
| IgM | - Immunoglobulin M |
| IL | -Interleukin |
| ISG15 | - Interferon Stimulated Gene 15 |
| L-HDAg | - Large Hepatitis Delta Antigen |
| LSTMB | - Lagos State Traditional Medicine Board |
| MDA | - Malondialdehyde |
| NAFDAC | - National Agency for Food Drug Administration and Control |
| NF-κb | - Nuclear factor kappa B |
| ORFs | - Open Reading Frame |
| RNA | - Ribonucleic Acid |
| S-HDAg | - Small Hepatitis Delta Antigen |
| SDI | - Social Demographic Index |
| SGOT | - Serum glutamic oxaloacetic transaminase |
| SGPT | - Serum glutamic-pyruvic transaminase (SGPT) |
| SOD | - Superoxide dismutase |
| TBK1 | - TANK-binding kinase 1 |
| TM | - Traditional medicine |
| TNF-α | - Tumour necrosis factor - alpha |
| WHO | - World Health Organization |
References
- Lanini, S.; Ustianowski, A.; Pisapia, R.; Zumla, A.; Ippolito, G. Viral Hepatitis: Etiology, Epidemiology, Transmission, Diagnostics, Treatment, and Prevention. Infect Dis Clin North Am 2019, 33, 1045–1062. [Google Scholar] [CrossRef] [PubMed]
- Jefferies, M.; Rauff, B.; Rashid, H.; Lam, T.; Rafiq, S. Update on global epidemiology of viral hepatitis and preventive strategies. World J Clin Cases 2018, 6, 589–599. [Google Scholar] [CrossRef] [PubMed]
- Owumi, S.E.; Kazeem, A.I.; Wu, B.; Ishokare, L.O.; Arunsi, U.O.; Oyelere, A.K. Apigeninidin-rich Sorghum bicolor (L. Moench) extracts suppress A549 cells proliferation and ameliorate toxicity of aflatoxin B1-mediated liver and kidney derangement in rats. Sci Rep 2022, 12, 7438. [Google Scholar] [CrossRef]
- Ringelhan, M.; McKeating, J.A.; Protzer, U. Viral hepatitis and liver cancer. Philos Trans R Soc Lond B Biol Sci 2017, 372. [Google Scholar] [CrossRef]
- Péneau, C.; Zucman-Rossi, J.; Nault, J.C. Genomics of Viral Hepatitis-Associated Liver Tumors. J Clin Med 2021, 10. [Google Scholar] [CrossRef] [PubMed]
- Devarbhavi, H.; Asrani, S.K.; Arab, J.P.; Nartey, Y.A.; Pose, E.; Kamath, P.S. Global burden of liver disease: 2023 update. J Hepatol 2023, 79, 516–537. [Google Scholar] [CrossRef]
- WHO. Global hepatitis report 2024: action for access in low- and middle-income countries; ISBN 978-92-4-009167-2 World Health Organization, Geneva., 2024. https://www.who.int/publications/i/item/9789240091672.
- Lemoine, M.; Eholié, S.; Lacombe, K. Reducing the neglected burden of viral hepatitis in Africa: strategies for a global approach. J Hepatol 2015, 62, 469–476. [Google Scholar] [CrossRef]
- Ondigui, J.L.N.; Kenmoe, S.; Kengne-Ndé, C.; Ebogo-Belobo, J.T.; Takuissu, G.R.; Kenfack-Momo, R.; Mbaga, D.S.; Tchatchouang, S.; Kenfack-Zanguim, J.; Fogang, R.L.; et al. Epidemiology of occult hepatitis B and C in Africa: A systematic review and meta-analysis. J Infect Public Health 2022, 15, 1436–1445. [Google Scholar] [CrossRef]
- Lekskulchai, V. Prevalence of Hepatitis B and C Virus Infections: Influence of National Health Care Policies and Local Clinical Practices. Med Sci Monit Basic Res 2021, 27, e933692. [Google Scholar] [CrossRef]
- Adane, T.; Getawa, S. The prevalence and associated factors of hepatitis B and C virus in hemodialysis patients in Africa: A systematic review and meta-analysis. PLoS One 2021, 16, e0251570. [Google Scholar] [CrossRef]
- Girmay, G.; Bewket, G.; Amare, A.; Angelo, A.A.; Wondmagegn, Y.M.; Setegn, A.; Wubete, M.; Assefa, M. Seroprevalence of viral hepatitis B and C infections among healthcare workers in Ethiopia: A systematic review and meta-analysis. PLoS One 2024, 19, e0312959. [Google Scholar] [CrossRef]
- Sonderup, M.W.; Afihene, M.; Ally, R.; Apica, B.; Awuku, Y.; Cunha, L.; Dusheiko, G.; Gogela, N.; Lohouès-Kouacou, M.J.; Lam, P.; et al. Hepatitis C in sub-Saharan Africa: the current status and recommendations for achieving elimination by 2030. Lancet Gastroenterol Hepatol 2017, 2, 910–919. [Google Scholar] [CrossRef]
- Odoom, A.; Boamah, I.; Sagoe, K.W.C.; Kotey, F.C.N.; Donkor, E.S. Zoonotic and Food-Related Hazards Due to Hepatitis A and E in Africa: A Systematic Review and Meta-Analysis. Environmental Health Insights 2024, 18, 11786302241299370. [Google Scholar] [CrossRef]
- Bhagwandin, K.; Thaver-Kleitman, J.; Subramoney, K.; Manamela, M.J.; Prabdial-Sing, N. Exploring the Epidemiological Surveillance of Hepatitis A in South Africa: A 2023 Perspective. Viruses 2024, 16. [Google Scholar] [CrossRef] [PubMed]
- Bane, A.; Sultan, A.; Ahmed, R. Increasing Burden of Acute Hepatitis A among Ethiopian Children, Adolescents, and Young adults: A Change in Epidemiological Pattern and Need for Hepatitis A Vaccine. Ethiop J Health Sci 2022, 32, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Stockdale, A.J.; Chaponda, M.; Beloukas, A.; Phillips, R.O.; Matthews, P.C.; Papadimitropoulos, A.; King, S.; Bonnett, L.; Geretti, A.M. Prevalence of hepatitis D virus infection in sub-Saharan Africa: a systematic review and meta-analysis. Lancet Glob Health 2017, 5, e992–e1003. [Google Scholar] [CrossRef] [PubMed]
- Tuaillon, E.; Kania, D.; Gordien, E.; Van de Perre, P.; Dujols, P. Epidemiological data for hepatitis D in Africa. Lancet Glob Health 2018, 6, e33. [Google Scholar] [CrossRef]
- Jaquet, A.; Muula, G.; Ekouevi, D.K.; Wandeler, G. Elimination of Viral Hepatitis in Low and Middle-Income Countries: Epidemiological Research Gaps. Curr Epidemiol Rep 2021, 8, 89–96. [Google Scholar] [CrossRef]
- Sonderup, M.W.; Spearman, C.W. Global Disparities in Hepatitis B Elimination-A Focus on Africa. Viruses 2022, 14. [Google Scholar] [CrossRef]
- Lemoine, M.; Eholié, S.; Lacombe, K. Reducing the neglected burden of viral hepatitis in Africa: Strategies for a global approach. Journal of Hepatology 2015, 62, 469–476. [Google Scholar] [CrossRef]
- Jacobsen, K.; Koopman, J. The effects of socioeconomic development on worldwide hepatitis A virus seroprevalence patterns. International Journal of Epidemiology 2005, 34, 600–609. [Google Scholar] [CrossRef] [PubMed]
- Koroglu, M.; Jacobsen, K.H.; Demiray, T.; Ozbek, A.; Erkorkmaz, U.; Altindis, M. Socioeconomic indicators are strong predictors of hepatitis A seroprevalence rates in the Middle East and North Africa. Journal of Infection and Public Health 2017, 10, 513–517. [Google Scholar] [CrossRef] [PubMed]
- Chattu, V.K.; Knight, W.A.; Adisesh, A.; Yaya, S.; Reddy, K.S.; Di Ruggiero, E.; Aginam, O.; Aslanyan, G.; Clarke, M.; Massoud, M.R.; et al. Politics of disease control in Africa and the critical role of global health diplomacy: A systematic review. Health Promot Perspect 2021, 11, 20–31. [Google Scholar] [CrossRef]
- Cook, C.T.; Kalu, K. The political economy of health policy in Sub-Saharan Africa. Med Law 2008, 27, 29–51. [Google Scholar]
- Ikobah, J.M.; Okpara, H.C.; Ekanem, E.E.; Udo, J.J. Seroprevalence and predictors of hepatitis A infection in Nigerian children. Pan Afr Med J 2015, 20, 120. [Google Scholar] [CrossRef]
- Ifeorah, I.; Bakarey, A.; Adeniji, J.; Onyemelukwe, F. Seroprevalence of hepatitis B and delta viruses among HIV-infected population attending anti-retroviral clinic in selected health facilities in Abuja, Nigeria. Journal of Immunoassay and Immunochemistry 2017, 38, 608–619. [Google Scholar] [CrossRef]
- Fakunle, Y.M.; Abdurrahman, M.B.; Whittle, H.C. Hepatitis-B virus infection in children and adults in Northern Nigeria: a preliminary survey. Trans R Soc Trop Med Hyg 1981, 75, 626–629. [Google Scholar] [CrossRef] [PubMed]
- Belo, A.C. Prevalence of hepatitis B virus markers in surgeons in Lagos, Nigeria. East Afr Med J 2000, 77, 283–285. [Google Scholar] [CrossRef]
- Adedeji, A.; Nnaji, I.; Muhammad, F.; Amaza, R.; Adewusi, A.; Ojo, J.; Ojenya, E.; Mustapha, A.; Gassi, S.; Klink, P.; et al. Seroprevalence patterns of viral hepatitis B, C, and E among internally displaced persons in Borno State, Nigeria. IJID Reg 2024, 13, 100481. [Google Scholar] [CrossRef]
- Ola, S.O.; Odaibo, G.N.; Olaleye, O.D.; Ayoola, E.A. Hepatitis B and E viral infections among Nigerian healthcare workers. Afr J Med Med Sci 2012, 41, 387–391. [Google Scholar]
- Junaid, S.A.; Agina, S.E.; Abubakar, K.A. Epidemiology and Associated Risk Factors of Hepatitis E Virus Infection in Plateau State, Nigeria. Virology 2014, 5, VRT.S15422. [Google Scholar] [CrossRef] [PubMed]
- Melnick, J.L.; Howard, C.R. Classification and Taxonomy of Hepatitis Viruses: Summary of a Workshop. Tokyo, 1994; pp. 47-49.
- Usuda, D.; Kaneoka, Y.; Ono, R.; Kato, M.; Sugawara, Y.; Shimizu, R.; Inami, T.; Nakajima, E.; Tsuge, S.; Sakurai, R.; et al. Current perspectives of viral hepatitis. World J Gastroenterol 2024, 30, 2402–2417. [Google Scholar] [CrossRef]
- Nemes, K.; Persson, S.; Simonsson, M. Hepatitis A Virus and Hepatitis E Virus as Food- and Waterborne Pathogens-Transmission Routes and Methods for Detection in Food. Viruses 2023, 15. [Google Scholar] [CrossRef]
- Pintilie, H.; Brook, G. Commentary: A review of risk of hepatitis B and C transmission through biting or spitting. J Viral Hepat 2018, 25, 1423–1428. [Google Scholar] [CrossRef]
- Gerlich, W.H. [Hepatitis B and C. Risk of transmission from infected health care workers to patients]. Bundesgesundheitsblatt Gesundheitsforschung Gesundheitsschutz 2004, 47, 369–378. [Google Scholar] [CrossRef] [PubMed]
- Lappalainen, M.; Chen, R.W.; Maunula, L.; von Bonsdorff, C.; Plyusnin, A.; Vaheri, A. Molecular epidemiology of viral pathogens and tracing of transmission routes: hepatitis-, calici- and hantaviruses. J Clin Virol 2001, 21, 177–185. [Google Scholar] [CrossRef]
- Wang, X.; Ren, J.; Gao, Q.; Hu, Z.; Sun, Y.; Li, X.; Rowlands, D.J.; Yin, W.; Wang, J.; Stuart, D.I.; et al. Hepatitis A virus and the origins of picornaviruses. Nature 2015, 517, 85–88. [Google Scholar] [CrossRef] [PubMed]
- Hirai-Yuki, A.; Hensley, L.; Whitmire, J.K.; Lemon, S.M. Biliary Secretion of Quasi-Enveloped Human Hepatitis A Virus. mBio 2016, 7. [Google Scholar] [CrossRef]
- Najarian, R.; Caput, D.; Gee, W.; Potter, S.J.; Renard, A.; Merryweather, J.; Van Nest, G.; Dina, D. Primary structure and gene organization of human hepatitis A virus. Proc Natl Acad Sci U S A 1985, 82, 2627–2631. [Google Scholar] [CrossRef]
- Siegl, G.; Weitz, M.; Kronauer, G. Stability of hepatitis A virus. Intervirology 1984, 22, 218–226. [Google Scholar] [CrossRef]
- Ramsay, C.N.; Upton, P.A. HEPATITIS A AND FROZEN RASPBERRIES. The Lancet 1989, 333, 43–44. [Google Scholar] [CrossRef] [PubMed]
- Costafreda, M.I.; Pérez-Rodriguez, F.J.; D'Andrea, L.; Guix, S.; Ribes, E.; Bosch, A.; Pintó, R.M. Hepatitis A virus adaptation to cellular shutoff is driven by dynamic adjustments of codon usage and results in the selection of populations with altered capsids. J Virol 2014, 88, 5029–5041. [Google Scholar] [CrossRef] [PubMed]
- Tjon, G.M.; Coutinho, R.A.; van den Hoek, A.; Esman, S.; Wijkmans, C.J.; Hoebe, C.J.; Wolters, B.; Swaan, C.; Geskus, R.B.; Dukers, N.; et al. High and persistent excretion of hepatitis A virus in immunocompetent patients. J Med Virol 2006, 78, 1398–1405. [Google Scholar] [CrossRef]
- Severi, E.; Verhoef, L.; Thornton, L.; Guzman-Herrador, B.R.; Faber, M.; Sundqvist, L.; Rimhanen-Finne, R.; Roque-Afonso, A.M.; Ngui, S.L.; Allerberger, F.; et al. Large and prolonged food-borne multistate hepatitis A outbreak in Europe associated with consumption of frozen berries, 2013 to 2014. Euro Surveill 2015, 20, 21192. [Google Scholar] [CrossRef]
- Di Cola, G.; Fantilli, A.C.; Pisano, M.B.; Ré, V.E. Foodborne transmission of hepatitis A and hepatitis E viruses: A literature review. Int J Food Microbiol 2021, 338, 108986. [Google Scholar] [CrossRef] [PubMed]
- Migueres, M.; Lhomme, S.; Izopet, J. Hepatitis A: Epidemiology, High-Risk Groups, Prevention and Research on Antiviral Treatment. Viruses 2021, 13. [Google Scholar] [CrossRef]
- da Silva, S.G.; Leon, L.A.; Alves, G.; Brito, S.M.; Sandes Vde, S.; Lima, M.M.; Nogueira, M.C.; Tavares Rde, C.; Dobbin, J.; Apa, A.; et al. A Rare Case of Transfusion Transmission of Hepatitis A Virus to Two Patients with Haematological Disease. Transfus Med Hemother 2016, 43, 137–141. [Google Scholar] [CrossRef]
- World Health, O. WHO immunological basis for immunization series: module 18: hepatitis A; World Health Organization: Geneva, 2019. [Google Scholar]
- Zeng, D.Y.; Li, J.M.; Lin, S.; Dong, X.; You, J.; Xing, Q.Q.; Ren, Y.D.; Chen, W.M.; Cai, Y.Y.; Fang, K.; et al. Global burden of acute viral hepatitis and its association with socioeconomic development status, 1990-2019. J Hepatol 2021, 75, 547–556. [Google Scholar] [CrossRef]
- Liu, Z.; Shi, O.; Zhang, T.; Jin, L.; Chen, X. Disease burden of viral hepatitis A, B, C and E: A systematic analysis. J Viral Hepat 2020, 27, 1284–1296. [Google Scholar] [CrossRef]
- Jacobsen, K.H. Globalization and the Changing Epidemiology of Hepatitis A Virus. Cold Spring Harb Perspect Med 2018, 8. [Google Scholar] [CrossRef]
- Lee, D.Y.; Chae, S.J.; Cho, S.R.; Choi, W.; Kim, C.K.; Han, M.G. Nationwide seroprevalence of hepatitis A in South Korea from 2009 to 2019. PLoS One 2021, 16, e0245162. [Google Scholar] [CrossRef] [PubMed]
- Sule, W.F.; Kajogbola, A.T.; Adewumi, M.O. High prevalence of anti-hepatitis A virus immunoglobulin G antibody among healthcare facility attendees in Osogbo, Nigeria. J Immunoassay Immunochem 2013, 34, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Afegbua, S.L.; Bugaje, M.A.; Ahmad, A.A. Seroprevalence of hepatitis A virus infection among schoolchildren and adolescents in Kaduna, Nigeria. Trans R Soc Trop Med Hyg 2013, 107, 627–630. [Google Scholar] [CrossRef]
- Ogefere, H.O.; Egbe, C.A. Seroprevalence of IgM antibodies to hepatitis A virus in at-risk group in Benin City, Nigeria. Libyan J Med 2016, 11, 31290. [Google Scholar] [CrossRef]
- Ott, J.J.; Stevens, G.A.; Groeger, J.; Wiersma, S.T. Global epidemiology of hepatitis B virus infection: new estimates of age-specific HBsAg seroprevalence and endemicity. Vaccine 2012, 30, 2212–2219. [Google Scholar] [CrossRef]
- Portilho, M.M.; Martins, P.P.; Lampe, E.; Villar, L.M. A comparison of molecular methods for hepatitis B virus (HBV) DNA detection from oral fluid samples. J Med Microbiol 2012, 61, 844–851. [Google Scholar] [CrossRef]
- Zenebe, Y.; Mulu, W.; Yimer, M.; Abera, B. Sero-prevalence and risk factors of hepatitis B virus and human immunodeficiency virus infection among pregnant women in Bahir Dar city, Northwest Ethiopia: a cross sectional study. BMC Infect Dis 2014, 14, 118. [Google Scholar] [CrossRef]
- Zhu, R.X.; Seto, W.K.; Lai, C.L.; Yuen, M.F. Epidemiology of Hepatocellular Carcinoma in the Asia-Pacific Region. Gut Liver 2016, 10, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Sadoh, A.E.; Ofili, A. Hepatitis B infection among Nigerian children admitted to a children's emergency room. Afr Health Sci 2014, 14, 377–383. [Google Scholar] [CrossRef]
- Eke, A.C.; Eke, U.A.; Okafor, C.I.; Ezebialu, I.U.; Ogbuagu, C. Prevalence, correlates and pattern of hepatitis B surface antigen in a low resource setting. Virol J 2011, 8, 12. [Google Scholar] [CrossRef]
- Aba, H.O.; Aminu, M. Seroprevalence of hepatitis B virus serological markers among pregnant Nigerian women. Ann Afr Med 2016, 15, 20–27. [Google Scholar] [CrossRef]
- Iloh, G.U.; Ikwudinma, A.O. Sero-epidemiology of Hepatitis B Surface Antigenaemia among Adult Nigerians with Clinical Features of Liver Diseases Attending a Primary-Care Clinic in a Resource-Constrained Setting of Eastern Nigeria. N Am J Med Sci 2013, 5, 293–300. [Google Scholar] [CrossRef]
- Bada, A.S.; Olatunji, P.O.; Adewuyi, J.O.; Iseniyi, J.O.; Onile, B.A. Hepatitis B surface antigenaemia in Ilorin, Kwara State, Nigeria. Cent Afr J Med 1996, 42, 139–141. [Google Scholar] [PubMed]
- Em, M.; Enenebeaku, M.; Okopi, J.A.; Damen, J. Hepatitis B Virus (HBV) Infection among Pregnant Women in Makurdi, Nigeria. African Journal of Biomedical Research 2010, 11. [Google Scholar] [CrossRef]
- Lesi, O.A.; Kehinde, M.O.; Omilabu, S.A. Prevalence of the Hepatitis B “e” Antigen in Nigerian Patients with Chronic Liver Disease. Nigerian Quarterly Journal of Hospital Medicine 2008. [CrossRef]
- Rabiu, K.A.; Akinola, O.I.; Adewunmi, A.A.; Omololu, O.M.; Ojo, T.O. Risk factors for hepatitis B virus infection among pregnant women in Lagos, Nigeria. Acta Obstet Gynecol Scand 2010, 89, 1024–1028. [Google Scholar] [CrossRef]
- Opaleye, O.; Saheed, S.; Familua, F.; Olowe, A.; Ojurongbe, O.; Bolaji, O.; Odewale, G.; Ojo, J. Seroprevalence of Hepatitis B Surface Antigen and Antibody among Pregnant Women Attending a Tertiary Health Institution in Southwestern Nigeria. IOSR Journal of Dental and Medical Sciences 2014, 13, 67–71. [Google Scholar] [CrossRef]
- Shittu, M.; Ajao, K.; Adeniji, T.; Awe, C. Seroprevalence of Hepatitis B Surface Antigenemia and Hepatitis C Virus among Intending Blood Donors at Mother and Child Hospital, Akure, Nigeria. International Journal of Medicine and Medical Sciences 2014, 47, 2051–5731. [Google Scholar]
- Okonko, I.; Fa, S.; Ta, A.; Augustine, U.; Adeolu, A.; Ojezele, M.; Nwanze, J.; Fadeyi, A. Seroprevalence of HBsAg among patients in Abeokuta, South Western Nigeria. Global Journal of Medical Research 2010, Okonko IO, Soleye FA, Amusan TA, Udeze AO, Alli JA, Ojezele MO, Nwanze JC, Fadeyi A. 2010. Seroprevalence of HBsAg among patients in Abeokuta, South Western Nigeria. Global Journal of Medical Research 10(2): 40-49, 40-49.
- Anaedobe, C.G.; Fowotade, A.; Omoruyi, C.E.; Bakare, R.A. Prevalence, sociodemographic features and risk factors of Hepatitis B virus infection among pregnant women in Southwestern Nigeria. Pan Afr Med J 2015, 20, 406. [Google Scholar] [CrossRef]
- Ikeako, L.; Ezegwui, H.; Ajah, L.; Dim, C.; Okeke, T. Seroprevalence of Human Immunodeficiency Virus, Hepatitis B, Hepatitis C, Syphilis and Co-infections among Antenatal Women in a Tertiary Institution in South-East Nigeria. Ann Med Health Sci Res 2014, 4, S259–263. [Google Scholar] [CrossRef]
- Chima, C.; Opara, D.; Ahiara, J.; Obeagu, C.; Nwosu, D.; Opara, U.; Dike-Ndudim, J.; Ahiara, C.; Obeagu, E. STUDIES ON HEPATITIS B VIRUS INFECTION IN EBONYI STATE NIGERIA USING HBSAG AS MARKERS: RAPID ASSESSMENT SURVEY. 2022, 2, 185-203.
- Onwuakor, C.; V. C, E.; Nwankwo, I.; J.O, I. Sero-prevalence of Hepatitis B Surface Antigen (HBsAg) amongst Pregnant Women Attending Antenatal Clinic at the Federal Medical Centre Umuahia, Abia State, Nigeria. American Journal of Public Health Research 2014, 2, 255–259. [Google Scholar] [CrossRef]
- Awanye, A.M.; Stanley, C.N.; Orji, P.C.; Sasovworho, S.; Okonko, I.O.; Ibezi, C.N.E. Seroprevalence of hepatitis B virus surface antigens and antibodies among healthcare workers in selected hospitals in Rivers State, Nigeria. West African Journal of Pharmacy (2023, 34 132 - 149. [CrossRef]
- Utoo, B.T. Hepatitis B surface antigenemia (HBsAg) among pregnant women in southern Nigeria. Afr Health Sci 2013, 13, 1139–1143. [Google Scholar] [CrossRef] [PubMed]
- Osazuwa, F.; Erhumwunseimade, P. LETTER TO THE EDITOR REMUNERATED OR NON-REMUNERATED BLOOD DONATION: HOW DO WE ENSURE THE SAFETY OF BLOOD IN NIGERIA? 2013, 1-2. [CrossRef]
- Terwase, J.M.; Emeka, C.K. Prevalence of Hepatitis B Surface Antigen among Residents of Julius Berger Staff Quarters, Kubwa, Abuja. 2015.
- Atilola, G.; Tomisin, O.; Randle, M.; Isaac, K.O.; Odutolu, G.; Olomu, J.; Adenuga, L. Epidemiology of HBV in Pregnant Women, South West Nigeria. J Epidemiol Glob Health 2018, 8, 115–123. [Google Scholar] [CrossRef] [PubMed]
- Okonko, I.; Sule, W.; Ebute, A.J.; Donbraye, E.; Fadeyi, A.; Augustine, U.; lli, J.A. Farming and Non-Farming Individuals Attending Grimard Catholic Hospital, Anyigba, Kogi State, Nigeria Were Comparable in Hepatitis B Surface Antigen Seroprevalence. Current Research Journal of Biological Sciences 2010. [Google Scholar]
- Osasona, O.; Ariyo, O.; Ariyo, E.; Oguzie, J.; Olumade, T.; George, U.; Adewale-Fasoro, O.; Oguntoye, O. Comparative serologic profiles of hepatitis B Virus (HBV) between HIV/HBV co-infected and Hbv mono-infected patients in Ile-Ife, Nigeria. Journal of Immunoassay and Immunochemistry 2020, 42. [Google Scholar] [CrossRef]
- Forbi, J.C.; Onyemauwa, N.; Gyar, S.D.; Oyeleye, A.O.; Entonu, P.; Agwale, S.M. High prevalence of hepatitis B virus among female sex workers in Nigeria. Rev Inst Med Trop Sao Paulo 2008, 50, 219–221. [Google Scholar] [CrossRef]
- Olusayo, A.; Okwori, E.E.; Egwu, C.; Audu, F. Seroprevalence of hepatitis B surface antigen among prospective blood donors in an urban area of Benue State. Internet Journal of Hematology 2009, 5. [Google Scholar]
- Aminu, M.; Md, V. HEPATITIS B INFECTION IN NIGERIA: A REVIEW; 2014.
- Saidu, A.; Salihu, Y.; Umar, A.A.; Muhammad, B.; Abdullahi, I.N. Seroprevalence of Hepatitis B Surface Antigen among Pregnant Women Attending Ante-Natal Clinics in Sokoto Metropolis. 2015.
- Ndako, J.; Yahaya, A.; Amira, J.; Olaolu, T.; Adelani-Akande, T. Hepatitis B Virus (HBV) Infection among Alcoholic Consumers at a Local Community, North-East Nigeria. The Journal of Natural Science, Biology and Medicine 2013, 3. [Google Scholar]
- Imarenezor, N.; Brown, S.; Yakubu, O.; Soken, D. Survey of Hepatitis B and C among students of Federal. 2016.
- Aliyu, B.; Alhaji Isa, M.; Gulumbe, B. Prevalence of Hepatitis B virus infection among children attending mohammed shuwa memorial hospital Maiduguri, Borno state, Nigeria. 2020.
- Okoye, I.; Samba, S. Sero-Epidemic Survey Of Hepatitis B In A Population Of Northern Nigeria. Animal Research International 2008, 3. [Google Scholar] [CrossRef]
- El-Ishaq, A.; Mohammed, F. Prevalence of HepaTitis B Surface Antigen Among Blood Donors and Patients Attending General Hospital Potiskum. Ext J App Sci. 2015, 3, 199–203. [Google Scholar]
- Schillie, S.; Wester, C.; Osborne, M.; Wesolowski, L.; Ryerson, A.B. CDC Recommendations for Hepatitis C Screening Among Adults - United States, 2020. MMWR Recomm Rep 2020, 69, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Te, H.S.; Jensen, D.M. Epidemiology of hepatitis B and C viruses: a global overview. Clin Liver Dis 2010, 14, 1–21. [Google Scholar] [CrossRef] [PubMed]
- Sy, T.; Jamal, M.M. Epidemiology of hepatitis C virus (HCV) infection. Int J Med Sci 2006, 3, 41–46. [Google Scholar] [CrossRef] [PubMed]
- Madhava, V.; Burgess, C.; Drucker, E. Epidemiology of chronic hepatitis C virus infection in sub-Saharan Africa. Lancet Infect Dis 2002, 2, 293–302. [Google Scholar] [CrossRef]
- Maheshwari, A.; Thuluvath, P.J. Management of acute hepatitis C. Clin Liver Dis 2010, 14, 169–176. [Google Scholar] [CrossRef]
- Xia, X.; Luo, J.; Bai, J.; Yu, R. Epidemiology of hepatitis C virus infection among injection drug users in China: systematic review and meta-analysis. Public Health 2008, 122, 990–1003. [Google Scholar] [CrossRef]
- Tohme, R.A.; Holmberg, S.D. Is sexual contact a major mode of hepatitis C virus transmission? Hepatology 2010, 52, 1497–1505. [Google Scholar] [CrossRef]
- Jafari, S.; Copes, R.; Baharlou, S.; Etminan, M.; Buxton, J. Tattooing and the risk of transmission of hepatitis C: a systematic review and meta-analysis. Int J Infect Dis 2010, 14, e928–940. [Google Scholar] [CrossRef]
- Owusu-Ofori, S.; Temple, J.; Sarkodie, F.; Anokwa, M.; Candotti, D.; Allain, J.P. Predonation screening of blood donors with rapid tests: implementation and efficacy of a novel approach to blood safety in resource-poor settings. Transfusion 2005, 45, 133–140. [Google Scholar] [CrossRef]
- Lam, N.C.; Gotsch, P.B.; Langan, R.C. Caring for pregnant women and newborns with hepatitis B or C. Am Fam Physician 2010, 82, 1225–1229. [Google Scholar]
- Jeannel, D.; Fretz, C.; Traore, Y.; Kohdjo, N.; Bigot, A.; E, P.G.; Jourdan, G.; Kourouma, K.; Maertens, G.; Fumoux, F.; et al. Evidence for high genetic diversity and long-term endemicity of hepatitis C virus genotypes 1 and 2 in West Africa. J Med Virol 1998, 55, 92–97. [Google Scholar] [CrossRef]
- Ejele, O.A.; Nwauche, C.A.; Erhabor, O. Seroprevalence of hepatitis C virus in the Niger Delta of Nigeria. Niger Postgrad Med J 2006, 13, 103–106. [Google Scholar] [CrossRef] [PubMed]
- Urban, S.; Neumann-Haefelin, C.; Lampertico, P. Hepatitis D virus in 2021: virology, immunology and new treatment approaches for a difficult-to-treat disease. Gut 2021, 70, 1782–1794. [Google Scholar] [CrossRef]
- Flores, R.; Owens, R.A.; Taylor, J. Pathogenesis by subviral agents: viroids and hepatitis delta virus. Current Opinion in Virology 2016, 17, 87–94. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.G.; Lemon, S.M. Hepatitis delta virus antigen forms dimers and multimeric complexes in vivo. J Virol 1993, 67, 446–454. [Google Scholar] [CrossRef]
- Japhet, O.A.A.M.O. Hepatitis Delta Virus in Patients Referred for Malaria Parasite Test in Ile-Ife, Nigeria. Methodology 2017, 36. [Google Scholar]
- Akande, K.O.; Adeola, F.; and Adekanmbi, O. The effect of Hepatitis D co-infection on the immunologic and molecular profile of Hepatitis B in asymptomatic Chronic Hepatitis B patients in southwest Nigeria. Journal of Immunoassay and Immunochemistry 2020, 41, 272–280. [Google Scholar] [CrossRef]
- Abdulkareem, L.O.; Ndububa, D.A.; Uhunmwangho, A.O.; Yunusa, T. Hepatitis D virus antibodies and liver function profile among patients with chronic hepatitis B infection in Abuja, Nigeria. J Infect Dev Ctries 2021, 15, 141–146. [Google Scholar] [CrossRef]
- Mbaawuaga, E.M.; Iroegbu, C.U.; Ike, A.C. Hepatitis B virus (HBV) serological patterns in Benue State, Nigeria. Open Journal of Medical Microbiology 2014, 4, 1–10. [Google Scholar] [CrossRef]
- Waiya, S.; Taura, D.; Shehu, A.; Yahaya, S.; Ali, M.; Garba, M. Prevalence of hepatitis D virus antigens among sero-positive hepatitis B surface antigen (HBsAg) patients attending Aminu Kano teaching hospital (AKTH), Kano. Arch Immunol Allergy 2018, 1, 67–74. [Google Scholar]
- Inyang-Etoh, P.C.; Obi, O.A.; Udonkang, M.I. Prevalence of hepatitis B, C, and D among patients on highly active antiretroviral drug therapy (HAART) in calabar metropolis, Nigeria. Journal of Medical and Allied Science 2018, 8, 17–22. [Google Scholar]
- Egbebi, A.; Okiki, P.; Oyinloye, J.; Daramola, G.; Ogunfolakan, O. Prevalence of Hepatitis B and D Antibodies Among Pregnant Women Attending Antenatal Clinic at Ekiti State University Teaching Hospital, Ado-Ekiti, Ekiti State, Nigeria. J. Adv. Microbiol 2022, 22, 97–103. [Google Scholar] [CrossRef]
- Ifeorah, I.M.; Gerber, A.; Dziri, S.; Bakarey, S.A.; Le Gal, F.; Aglavdawa, G.; Alloui, C.; Kalu, S.O.; Ghapouen, P.-A.B.; Brichler, S. The prevalence and molecular epidemiology of hepatitis delta virus in Nigeria: The results of a nationwide study. Viruses 2024, 16, 1236. [Google Scholar] [CrossRef] [PubMed]
- Nwokediuko, S.; Ijeoma, U. Seroprevalence of antibody to HDV in Nigerians with hepatitis B virus-related liver diseases. Nigerian Journal of Clinical Practice 2009, 12. [Google Scholar]
- Okonkwo, U.C.; Okpara, H.C.; Inaku, K.; Aluka, T.M.; Chukwudike, E.S.; Ogarekpe, Y.; Emin, E.J.; Hodo, O.; Otu, A.A. Prevalence and risk factors of Hepatitis D virus antibody among asymptomatic carriers of Hepatitis B virus: a community survey. African Health Sciences 2022, 22, 504–510. [Google Scholar] [CrossRef]
- Nwika, G.N.; Awortu, J.Z.; Mgbeoma, E.E. Prevalence of hepatitis D virus among hepatitis B positive blood donors in Port Harcourt, Nigeria. Int. Blood Res. Rev 2023, 14, 48–56. [Google Scholar] [CrossRef]
- Okpokam, D.; Kooffreh-Ada, M.; Okhormhe, Z.; Akpabio, E.; Akpotuzor, J.; Nna, V. Hepatitis D virus in chronic liver disease patients with hepatitis B surface antigen in University of Calabar Teaching Hospital, Calabar, Nigeria. 2015.
- Anejo-Okopi, J.; Okpara, J.; Dabol, J.; Adetunji, J.; Adeniyi, D.; Amanyi, D.; Ujah, O.; David, V.; Omaiye, P.; Audu, O. Hepatitis delta virus infection among HIV/HBV and HBV-mono infected patients in Jos, Nigeria. Hosts Viruses 2021, 8, 23–28. [Google Scholar]
- Opaleye, O.O.; Japhet, O.M.; Adewumi, O.M.; Omoruyi, E.C.; Akanbi, O.A.; Oluremi, A.S.; Wang, B.; Tong, H.v.; Velavan, T.P.; Bock, C.-T. Molecular epidemiology of hepatitis D virus circulating in Southwestern Nigeria. Virology Journal 2016, 13, 1–8. [Google Scholar] [CrossRef]
- feorah, I.; Bakarey, A.; Adeniji, J.; Onyemelukwe, F. Hepatitis C and delta viruses among HBV positive cohort in Abuja Nigeria. 2019.
- Abdulkareem, L.O.; Ndububa, D.A.; Uhunmwangho, A.O.; Yunusa, T. Hepatitis D virus antibodies and liver function profile among patients with chronic hepatitis B infection in Abuja, Nigeria. The Journal of Infection in Developing Countries 2021, 15, 141–146. [Google Scholar] [CrossRef]
- Webb, G.W.; Dalton, H.R. Hepatitis E: an underestimated emerging threat. Ther Adv Infect Dis 2019, 6, 2049936119837162. [Google Scholar] [CrossRef]
- Nimgaonkar, I.; Ding, Q.; Schwartz, R.E.; Ploss, A. Hepatitis E virus: advances and challenges. Nat Rev Gastroenterol Hepatol 2018, 15, 96–110. [Google Scholar] [CrossRef] [PubMed]
- Das, A.; Rivera-Serrano, E.E.; Yin, X.; Walker, C.M.; Feng, Z.; Lemon, S.M. Cell entry and release of quasi-enveloped human hepatitis viruses. Nature Reviews Microbiology 2023, 21, 573–589. [Google Scholar] [CrossRef]
- Yin, X.; Feng, G. Hepatitis E Virus Entry. Viruses 2019, 11, 883. [Google Scholar] [CrossRef]
- Purdy, M.A.; Harrison, T.J.; Jameel, S.; Meng, X.-J.; Okamoto, H.; Van der Poel, W.H.M.; Smith, D.B.; Consortium, I.R. ICTV Virus Taxonomy Profile: Hepeviridae. Journal of General Virology 2017, 98, 2645–2646. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.H.; Tan, B.H.; Teo, E.C.; Lim, S.G.; Dan, Y.Y.; Wee, A.; Aw, P.P.; Zhu, Y.; Hibberd, M.L.; Tan, C.K.; et al. Chronic Infection With Camelid Hepatitis E Virus in a Liver Transplant Recipient Who Regularly Consumes Camel Meat and Milk. Gastroenterology 2016, 150, 355–357.e353. [Google Scholar] [CrossRef] [PubMed]
- Nelson, K.E.; Labrique, A.B.; Kmush, B.L. Epidemiology of Genotype 1 and 2 Hepatitis E Virus Infections. Cold Spring Harb Perspect Med 2019, 9. [Google Scholar] [CrossRef]
- Wang, B.; Akanbi, O.A.; Harms, D.; Adesina, O.; Osundare, F.A.; Naidoo, D.; Deveaux, I.; Ogundiran, O.; Ugochukwu, U.; Mba, N.; et al. A new hepatitis E virus genotype 2 strain identified from an outbreak in Nigeria, 2017. Virology Journal 2018, 15, 163. [Google Scholar] [CrossRef]
- Buisson, Y.; Grandadam, M.; Nicand, E.; Cheval, P.; van Cuyck-Gandre, H.; Innis, B.; Rehel, P.; Coursaget, P.; Teyssou, R.; Tsarev, S. Identification of a novel hepatitis E virus in Nigeria. J Gen Virol 2000, 81, 903–909. [Google Scholar] [CrossRef]
- Osundare, F.A.; Klink, P.; Majer, C.; Akanbi, O.A.; Wang, B.; Faber, M.; Harms, D.; Bock, C.-T.; Opaleye, O.O. Hepatitis E Virus Seroprevalence and Associated Risk Factors in Apparently Healthy Individuals from Osun State, Nigeria. Pathogens 2020, 9, 392. [Google Scholar] [CrossRef]
- Adesina, O.; Japhet, M.; Donbraye, E.; Kumapayi, T.; Kudoro, A. Anti hepatitis E virus antibodies in sick and healthy Individuals in Ekiti State, Nigeria. African Journal of Microbiology Research 2009, 3, 533–536. [Google Scholar]
- Tu, A.; Zhu, X.; Dastjerdi, P.Z.; Yin, Y.; Peng, M.; Zheng, D.; Peng, Z.; Wang, E.; Wang, X.; Jing, W. Evaluate the clinical efficacy of traditional Chinese Medicine as the neoadjuvant treatment in reducing the incidence of hepatocellular carcinoma in patients with hepatitis B-related cirrhosis: A systematic review and meta-analysis. Heliyon 2024, 10, e24437. [Google Scholar] [CrossRef]
- Ge, F.; Yang, Y.; Bai, Z.; Si, L.; Wang, X.; Yu, J.; Xiao, X.; Liu, Y.; Ren, Z. The role of Traditional Chinese medicine in anti-HBV: background, progress, and challenges. Chin Med 2023, 18, 159. [Google Scholar] [CrossRef] [PubMed]
- Demie, G.; Negash, M.; Awas, T. Ethnobotanical study of medicinal plants used by indigenous people in and around Dirre Sheikh Hussein heritage site of South-eastern Ethiopia. J Ethnopharmacol 2018, 220, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Aschale, Y.; Wubetu, M.; Abebaw, A.; Yirga, T.; Minwuyelet, A.; Toru, M. A Systematic Review on Traditional Medicinal Plants Used for the Treatment of Viral and Fungal Infections in Ethiopia. J Exp Pharmacol 2021, 13, 807–815. [Google Scholar] [CrossRef] [PubMed]
- Chaudhary, A.N.; Arif, A.M; Shafi B., S; Kushwaha A. S., P; P, S.A. Emerging role of natural bioactive compounds in navigating the future of liver disease. iLIVER 2025, 4. [Google Scholar] [CrossRef]
- Arunsi, U.O.; Chioma, O.E.; Etusim, P.E.; Owumi, S.E. Indigenous Nigeria medicinal herbal remedies: A potential source for therapeutic against rheumatoid arthritis. Experimental Biology and Medicine 2022, 247, 1148–1178. [Google Scholar] [CrossRef]
- Roy, A.; Datta, S. Medicinal Plants against Ischemic Stroke. Curr Pharm Biotechnol 2021, 22, 1302–1314. [Google Scholar] [CrossRef]
- Roy, A.; Roy, M.; Gacem, A.; Datta, S.; Zeyaullah, M.; Muzammil, K.; Farghaly, T.A.; Abdellattif, M.H.; Yadav, K.K.; Simal-Gandara, J. Role of bioactive compounds in the treatment of hepatitis: A review. Front Pharmacol 2022, 13, 1051751. [Google Scholar] [CrossRef]
- Alhazmi, H.A.; Najmi, A.; Javed, S.A.; Sultana, S.; Al Bratty, M.; Makeen, H.A.; Meraya, A.M.; Ahsan, W.; Mohan, S.; Taha, M.M.E.; et al. Medicinal Plants and Isolated Molecules Demonstrating Immunomodulation Activity as Potential Alternative Therapies for Viral Diseases Including COVID-19. Front Immunol 2021, 12, 637553. [Google Scholar] [CrossRef]
- Lagunas-Rangel, F.A.; Bermudez-Cruz, R.M. Natural Compounds That Target DNA Repair Pathways and Their Therapeutic Potential to Counteract Cancer Cells. Front Oncol 2020, 10, 598174. [Google Scholar] [CrossRef]
- Beykaso, G.; Teklehaymanot, T.; Mulu, A.; Berhe, N.; Alemayehu, D.H.; Giday, M. Medicinal Plants in Treating Hepatitis B Among Communities of Central Region of Ethiopia. Hepat Med 2023, 15, 265–277. [Google Scholar] [CrossRef] [PubMed]
- Malik, Z.A.; Bhat, J.A.; Ballabha, R.; Bussmann, R.W.; Bhatt, A.B. Ethnomedicinal plants traditionally used in health care practices by inhabitants of Western Himalaya. J Ethnopharmacol 2015, 172, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Ntemafack, A.; Ayoub, M.; Hassan, Q.p.; Gandhi, S.G. A systematic review of pharmacological potential of phytochemicals from Rumex abyssinicus Jacq. S Afr J Bot 2023, 154, 11–25. [Google Scholar] [CrossRef]
- Ilyas, U.; Katare, D.P.; Aeri, V.; Naseef, P.P. A Review on Hepatoprotective and Immunomodulatory Herbal Plants. Pharmacogn Rev 2016, 10, 66–70. [Google Scholar] [CrossRef]
- Freitag, A.F.; Cardia, G.F.; da Rocha, B.A.; Aguiar, R.P.; Silva-Comar, F.M.; Spironello, R.A.; Grespan, R.; Caparroz-Assef, S.M.; Bersani-Amado, C.A.; Cuman, R.K. Hepatoprotective Effect of Silymarin (Silybum marianum) on Hepatotoxicity Induced by Acetaminophen in Spontaneously Hypertensive Rats. Evid Based Complement Alternat Med 2015, 2015, 538317. [Google Scholar] [CrossRef]
- Valenzuela, A.; Garrido, A. Biochemical bases of the pharmacological action of the flavonoid silymarin and of its structural isomer silibinin. Biol Res 1994, 27, 105–112. [Google Scholar]
- Song, Z.; Deaciuc, I.; Song, M.; Lee, D.Y.; Liu, Y.; Ji, X.; McClain, C. Silymarin protects against acute ethanol-induced hepatotoxicity in mice. Alcohol Clin Exp Res 2006, 30, 407–413. [Google Scholar] [CrossRef]
- Kwon, D.Y.; Jung, Y.S.; Kim, S.J.; Kim, Y.S.; Choi, D.W.; Kim, Y.C. Alterations in sulfur amino acid metabolism in mice treated with silymarin: a novel mechanism of its action involved in enhancement of the antioxidant defense in liver. Planta Med 2013, 79, 997–1002. [Google Scholar] [CrossRef]
- Javed, S.; Kohli, K.; Ali, M. Reassessing bioavailability of silymarin. Altern Med Rev 2011, 16, 239–249. [Google Scholar]
- Lu, C.; Lu, Y.; Chen, J.; Zhang, W.; Wu, W. Synchronized and sustained release of multiple components in silymarin from erodible glyceryl monostearate matrix system. Eur J Pharm Biopharm 2007, 66, 210–219. [Google Scholar] [CrossRef]
- Ferenci, P.; Scherzer, T.M.; Kerschner, H.; Rutter, K.; Beinhardt, S.; Hofer, H.; Schoniger-Hekele, M.; Holzmann, H.; Steindl-Munda, P. Silibinin is a potent antiviral agent in patients with chronic hepatitis C not responding to pegylated interferon/ribavirin therapy. Gastroenterology 2008, 135, 1561–1567. [Google Scholar] [CrossRef] [PubMed]
- Tunca, R.; Sozmen, M.; Citil, M.; Karapehlivan, M.; Erginsoy, S.; Yapar, K. Pyridine induction of cytochrome P450 1A1, iNOS and metallothionein in Syrian hamsters and protective effects of silymarin. Exp Toxicol Pathol 2009, 61, 243–255. [Google Scholar] [CrossRef]
- Li, C.C.; Hsiang, C.Y.; Wu, S.L.; Ho, T.Y. Identification of novel mechanisms of silymarin on the carbon tetrachloride-induced liver fibrosis in mice by nuclear factor-kappaB bioluminescent imaging-guided transcriptomic analysis. Food Chem Toxicol 2012, 50, 1568–1575. [Google Scholar] [CrossRef] [PubMed]
- Gharagozloo, M.; Velardi, E.; Bruscoli, S.; Agostini, M.; Di Sante, M.; Donato, V.; Amirghofran, Z.; Riccardi, C. Silymarin suppress CD4+ T cell activation and proliferation: effects on NF-kappaB activity and IL-2 production. Pharmacol Res 2010, 61, 405–409. [Google Scholar] [CrossRef]
- Trappoliere, M.; Caligiuri, A.; Schmid, M.; Bertolani, C.; Failli, P.; Vizzutti, F.; Novo, E.; di Manzano, C.; Marra, F.; Loguercio, C.; et al. Silybin, a component of sylimarin, exerts anti-inflammatory and anti-fibrogenic effects on human hepatic stellate cells. J Hepatol 2009, 50, 1102–1111. [Google Scholar] [CrossRef]
- Manna, S.K.; Mukhopadhyay, A.; Van, N.T.; Aggarwal, B.B. Silymarin suppresses TNF-induced activation of NF-kappa B, c-Jun N-terminal kinase, and apoptosis. J Immunol 1999, 163, 6800–6809. [Google Scholar] [CrossRef] [PubMed]
- Faulstich, H.; Jahn, W.; Wieland, T. Silybin inhibition of amatoxin uptake in the perfused rat liver. Arzneimittelforschung 1980, 30, 452–454. [Google Scholar]
- El-Bahay, C.; Gerber, E.; Horbach, M.; Tran-Thi, Q.H.; Rohrdanz, E.; Kahl, R. Influence of tumor necrosis factor-alpha and silibin on the cytotoxic action of alpha-amanitin in rat hepatocyte culture. Toxicol Appl Pharmacol 1999, 158, 253–260. [Google Scholar] [CrossRef]
- Li, S.; Odedina, S.; Agwai, I.; Ojengbede, O.; Huo, D.; Olopade, O.I. Traditional medicine usage among adult women in Ibadan, Nigeria: a cross-sectional study. BMC Complement Med Ther 2020, 20, 93. [Google Scholar] [CrossRef]
- Hasan, M.K.; Ara, I.; Mondal, M.S.A.; Kabir, Y. Phytochemistry, pharmacological activity, and potential health benefits of Gly cyrrhiza glabra. Heliyon 2021, 7, e07240. [Google Scholar] [CrossRef]
- van Rossum, T.G.; Vulto, A.G.; de Man, R.A.; Brouwer, J.T.; Schalm, S.W. Review article: glycyrrhizin as a potential treatment for chronic hepatitis C. Aliment Pharmacol Ther 1998, 12, 199–205. [Google Scholar] [CrossRef] [PubMed]
- Asl, M.N.; Hosseinzadeh, H. Review of pharmacological effects of Glycyrrhiza sp. and its bioactive compounds. Phytother Res 2008, 22, 709–724. [Google Scholar] [CrossRef] [PubMed]
- Kimura, M.; Moro, T.; Motegi, H.; Maruyama, H.; Sekine, M.; Okamoto, H.; Inoue, H.; Sato, T.; Ogihara, M. In vivo glycyrrhizin accelerates liver regeneration and rapidly lowers serum transaminase activities in 70% partially hepatectomized rats. Eur J Pharmacol 2008, 579, 357–364. [Google Scholar] [CrossRef] [PubMed]
- Li, J.Y.; Cao, H.Y.; Liu, P.; Cheng, G.H.; Sun, M.Y. Glycyrrhizic acid in the treatment of liver diseases: literature review. Biomed Res Int 2014, 2014, 872139. [Google Scholar] [CrossRef]
- Korenaga, M.; Hidaka, I.; Nishina, S.; Sakai, A.; Shinozaki, A.; Gondo, T.; Furutani, T.; Kawano, H.; Sakaida, I.; Hino, K. A glycyrrhizin-containing preparation reduces hepatic steatosis induced by hepatitis C virus protein and iron in mice. Liver Int 2011, 31, 552–560. [Google Scholar] [CrossRef]
- Shiki, Y.; Shirai, K.; Saito, Y.; Yoshida, S.; Mori, Y.; Wakashin, M. Effect of glycyrrhizin on lysis of hepatocyte membranes induced by anti-liver cell membrane antibody. J Gastroenterol Hepatol 1992, 7, 12–16. [Google Scholar] [CrossRef] [PubMed]
- Abe, Y.; Ueda, T.; Kato, T.; Kohli, Y. [Effectiveness of interferon, glycyrrhizin combination therapy in patients with chronic hepatitis C]. Nihon Rinsho 1994, 52, 1817–1822. [Google Scholar]
- Shaneyfelt, M.E.; Burke, A.D.; Graff, J.W.; Jutila, M.A.; Hardy, M.E. Natural products that reduce rotavirus infectivity identified by a cell-based moderate-throughput screening assay. Virol J 2006, 3, 68. [Google Scholar] [CrossRef]
- Zuo, J.; Meng, T.; Wang, Y.; Tang, W. A Review of the Antiviral Activities of Glycyrrhizic Acid, Glycyrrhetinic Acid and Glycyrrhetinic Acid Monoglucuronide. Pharmaceuticals (Basel) 2023, 16. [Google Scholar] [CrossRef]
- Marhaeny, H.D.; Widyawaruyanti, A.; Widiandani, T.; Fuad Hafid, A.; Wahyuni, T.S. Phyllanthin and hypophyllanthin, the isolated compounds of Phyllanthus niruri inhibit protein receptor of corona virus (COVID-19) through in silico approach. J Basic Clin Physiol Pharmacol 2021, 32, 809–815. [Google Scholar] [CrossRef]
- Kumaran, A. , Karunakaran, R. J. In vitro antioxidant activities of methanol extracts of five Phyllanthus species from India. LWT - Food Science and Technology 2007, 40, 344–352. [Google Scholar] [CrossRef]
- Mao, X.; Wu, L.F.; Guo, H.L.; Chen, W.J.; Cui, Y.P.; Qi, Q.; Li, S.; Liang, W.Y.; Yang, G.H.; Shao, Y.Y.; et al. The Genus Phyllanthus: An Ethnopharmacological, Phytochemical, and Pharmacological Review. Evid Based Complement Alternat Med 2016, 2016, 7584952. [Google Scholar] [CrossRef] [PubMed]
- Hanh, N.D.; Sinchaipanid, N.; Mitrevej, A. Physicochemical characterization of phyllanthin from Phyllanthus amarus Schum. et Thonn. Drug Dev Ind Pharm 2014, 40, 793–802. [Google Scholar] [CrossRef]
- Xin-Hua, W.; Chang-Qing, L.; Xing-Bo, G.; Lin-Chun, F. A comparative study of Phyllanthus amarus compound and interferon in the treatment of chronic viral hepatitis B. Southeast Asian J Trop Med Public Health 2001, 32, 140–142. [Google Scholar] [PubMed]
- Chirdchupunseree, H.; Pramyothin, P. Protective activity of phyllanthin in ethanol-treated primary culture of rat hepatocytes. J Ethnopharmacol 2010, 128, 172–176. [Google Scholar] [CrossRef]
- Ott, M.; Thyagarajan, S.P.; Gupta, S. Phyllanthus amarus suppresses hepatitis B virus by interrupting interactions between HBV enhancer I and cellular transcription factors. Eur J Clin Invest 1997, 27, 908–915. [Google Scholar] [CrossRef]
- Wu, Z.; Zhao, X.; Li, R.; Wen, X.; Xiu, Y.; Long, M.; Li, J.; Huang, X.; Wen, J.; Dong, X.; et al. The combination of Schisandrin C and Luteolin synergistically attenuates hepatitis B virus infection via repressing HBV replication and promoting cGAS-STING pathway activation in macrophages. Chin Med 2024, 19, 48. [Google Scholar] [CrossRef]
- Zhao, J.; Xu, G.; Hou, X.; Mu, W.; Yang, H.; Shi, W.; Wen, J.; Liu, T.; Wu, Z.; Bai, J.; et al. Schisandrin C enhances cGAS-STING pathway activation and inhibits HBV replication. J Ethnopharmacol 2023, 311, 116427. [Google Scholar] [CrossRef]
- Ehambarampillai, D.; Wan, M.L.Y. A comprehensive review of Schisandra chinensis lignans: pharmacokinetics, pharmacological mechanisms, and future prospects in disease prevention and treatment. Chin Med 2025, 20, 47. [Google Scholar] [CrossRef]
- Donnapee, S.; Li, J.; Yang, X.; Ge, A.H.; Donkor, P.O.; Gao, X.M.; Chang, Y.X. Cuscuta chinensis Lam.: A systematic review on ethnopharmacology, phytochemistry and pharmacology of an important traditional herbal medicine. J Ethnopharmacol 2014, 157, 292–308. [Google Scholar] [CrossRef]
- Chan, S.W. Panax ginseng, Rhodiola rosea and Schisandra chinensis. Int J Food Sci Nutr 2012, 63 Suppl 1, 75–81. [Google Scholar] [CrossRef]
- Seo, H.J.; Ji, S.B.; Kim, S.E.; Lee, G.M.; Park, S.Y.; Wu, Z.; Jang, D.S.; Liu, K.H. Inhibitory Effects of Schisandra Lignans on Cytochrome P450s and Uridine 5'-Diphospho-Glucuronosyl Transferases in Human Liver Microsomes. Pharmaceutics 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Yen, F.L.; Wu, T.H.; Lin, L.T.; Lin, C.C. Hepatoprotective and antioxidant effects of Cuscuta chinensis against acetaminophen-induced hepatotoxicity in rats. J Ethnopharmacol 2007, 111, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, B.; Alam, T.; Varshney, M.; Khan, S.A. Hepatoprotective activity of two plants belonging to the Apiaceae and the Euphorbiaceae family. J Ethnopharmacol 2002, 79, 313–316. [Google Scholar] [CrossRef]
- Tlili, N.; Elfalleh, W.; Saadaoui, E.; Khaldi, A.; Triki, S.; Nasri, N. The caper (Capparis L.): ethnopharmacology, phytochemical and pharmacological properties. Fitoterapia 2011, 82, 93–101. [Google Scholar] [CrossRef]
- Mollica Adriano, G.Z. , Marcello Locatelli, Azzurra Stefanu, Andrei Mocan, Giorgia Macedonio, Simone Carradori, Olakunle Onaolapo, Adejoke Onaolapo, Juliet Adegoke, Marufat Olaniyan, Abdurrahman Aktumsek, Ettore Novellino Anti-diabetic and anti-hyperlipidemic properties of Capparis spinosa L.: In vivo and in vitro evaluation of its nutraceutical potential. Journal of Functional Foods 2017, 35, 32–42. [Google Scholar] [CrossRef]
- Zhang, H.; Ma, Z.F. Phytochemical and Pharmacological Properties of Capparis spinosa as a Medicinal Plant. Nutrients 2018, 10. [Google Scholar] [CrossRef]
- Saleem, H.; Khurshid, U.; Sarfraz, M.; Ahmad, I.; Alamri, A.; Anwar, S.; Alamri, A.S.; Locatelli, M.; Tartaglia, A.; Mahomoodally, M.F.; et al. Investigation into the biological properties, secondary metabolites composition, and toxicity of aerial and root parts of Capparis spinosa L.: An important medicinal food plant. Food Chem Toxicol 2021, 155, 112404. [Google Scholar] [CrossRef]
- Huseini, H.F.; Alavian, S.M.; Heshmat, R.; Heydari, M.R.; Abolmaali, K. The efficacy of Liv-52 on liver cirrhotic patients: a randomized, double-blind, placebo-controlled first approach. Phytomedicine 2005, 12, 619–624. [Google Scholar] [CrossRef]
- Li, J.; Li, Q.; Feng, T.; Li, K. Aqueous extract of Solanum nigrum inhibit growth of cervical carcinoma (U14) via modulating immune response of tumor bearing mice and inducing apoptosis of tumor cells. Fitoterapia 2008, 79, 548–556. [Google Scholar] [CrossRef]
- Liu, F.P.; Ma, X.; Li, M.M.; Li, Z.; Han, Q.; Li, R.; Li, C.W.; Chang, Y.C.; Zhao, C.W.; Lin, Y.X. Hepatoprotective effects of Solanum nigrum against ethanol-induced injury in primary hepatocytes and mice with analysis of glutathione S-transferase A1. J Chin Med Assoc 2016, 79, 65–71. [Google Scholar] [CrossRef] [PubMed]
- Son, Y.O.; Kim, J.; Lim, J.C.; Chung, Y.; Chung, G.H.; Lee, J.C. Ripe fruit of Solanum nigrum L. inhibits cell growth and induces apoptosis in MCF-7 cells. Food Chem Toxicol 2003, 41, 1421–1428. [Google Scholar] [CrossRef] [PubMed]
- Verma, S.K. , Rai, M. K., Asthana, P., Jaiswal, V. S., Jaiswal, U. In vitro plantlets from alginate-encapsulated shoot tips of Solanum nigrum L. In vitro plantlets from alginate-encapsulated shoot tips of Solanum nigrum L. 2010, 124, 517–521. [Google Scholar] [CrossRef]
- Prashanth Kumar, V.; Shashidhara, S.; Kumar, M.M.; Sridhara, B.Y. Cytoprotective role of Solanum nigrum against gentamicin-induced kidney cell (Vero cells) damage in vitro. Fitoterapia 2001, 72, 481–486. [Google Scholar] [CrossRef]
- Sultana, S.; Perwaiz, S.; Iqbal, M.; Athar, M. Crude extracts of hepatoprotective plants, Solanum nigrum and Cichorium intybus inhibit free radical-mediated DNA damage. J Ethnopharmacol 1995, 45, 189–192. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.M.; Tseng, H.C.; Wang, C.J.; Lin, J.J.; Lo, C.W.; Chou, F.P. Hepatoprotective effects of Solanum nigrum Linn extract against CCl(4)-induced oxidative damage in rats. Chem Biol Interact 2008, 171, 283–293. [Google Scholar] [CrossRef]
- Javed, T.; Ashfaq, U.A.; Riaz, S.; Rehman, S.; Riazuddin, S. In-vitro antiviral activity of Solanum nigrum against Hepatitis C Virus. Virol J 2011, 8, 26. [Google Scholar] [CrossRef]
- Akdere, H.; Tastekin, E.; Mericliler, M.; Burgazli, K.M. The protective effects of Ginkgo biloba EGb761 extract against renal ischemia-reperfusion injury in rats. Eur Rev Med Pharmacol Sci 2014, 18, 2936–2941. [Google Scholar]
- Kleijnen, J.; Knipschild, P. Ginkgo biloba. Lancet 1992, 340, 1136–1139. [Google Scholar] [CrossRef]
- Singh, S.K.; Srivastav, S.; Castellani, R.J.; Plascencia-Villa, G.; Perry, G. Neuroprotective and Antioxidant Effect of Ginkgo biloba Extract Against AD and Other Neurological Disorders. Neurotherapeutics 2019, 16, 666–674. [Google Scholar] [CrossRef]
- Mohanta, T.K.; Tamboli, Y.; Zubaidha, P.K. Phytochemical and medicinal importance of Ginkgo biloba L. Nat Prod Res 2014, 28, 746-752. Nat Prod Res 2014, 28, 746–752. [Google Scholar] [CrossRef] [PubMed]
- Birks, J.; Grimley Evans, J. Ginkgo biloba for cognitive impairment and dementia. Cochrane Database Syst Rev 2009, CD003120. [Google Scholar] [CrossRef] [PubMed]
- Naik, S.R.; Panda, V.S. Hepatoprotective effect of Ginkgoselect Phytosome in rifampicin induced liver injury in rats: evidence of antioxidant activity. Fitoterapia 2008, 79, 439–445. [Google Scholar] [CrossRef] [PubMed]
- Almeleebia, T.M.; Alsayari, A.; Wahab, S. Pharmacological and Clinical Efficacy of Picrorhiza kurroa and Its Secondary Metabolites: A Comprehensive Review. Molecules 2022, 27. [Google Scholar] [CrossRef]
- Soren, P.; Sharma, R.; Mal, G.; Singh, B.; Kumar, P.; Patil, R.D.; Singh, B. Hepatoprotective activity of Picrorhiza kurroa and Berberis lycium is mediated by inhibition of COX-2 and TGF-β expression in lantadenes-induced sub-chronic toxicity in guinea pigs. Phytomedicine Plus 2022, 2, 100288. [Google Scholar] [CrossRef]
- Qin, X.; Wang, X.; Tian, M.; Dong, Z.; Wang, J.; Wang, C.; Huang, Q. The role of Andrographolide in the prevention and treatment of liver diseases. Phytomedicine 2023, 109, 154537. [Google Scholar] [CrossRef]
- Sareer, O.; Ahmad, S.; Umar, S. Andrographis paniculata: a critical appraisal of extraction, isolation and quantification of andrographolide and other active constituents. Nat Prod Res 2014, 28, 2081–2101. [Google Scholar] [CrossRef]
- Kumar, S.; Ratha, K.K.; Jaiswal, S.; Rao, M.M.; Acharya, R. Exploring the potential of andrographis paniculata and its bioactive compounds in the management of liver diseases: A comprehensive food chemistry perspective. Food Chemistry Advances 2024, 4. [Google Scholar] [CrossRef]
- Manvar, D.; Mishra, M.; Kumar, S.; Pandey, V.N. Identification and evaluation of anti hepatitis C virus phytochemicals from Eclipta alba. J Ethnopharmacol 2012, 144, 545–554. [Google Scholar] [CrossRef]
- Naik, K.S.; Gurushanthaiah, M.; Kavimani, M.; Prabhu, K.; Lokanadham, S. Hepatoprotective Role of Eclipta alba against High Fatty Diet Treated Experimental Models - A Histopathological Study. Maedica (Bucur) 2018, 13, 217–222. [Google Scholar] [CrossRef]
- Deenin, W.; Malakul, W.; Boonsong, T.; Phoungpetchara, I.; Tunsophon, S. Papaya improves non-alcoholic fatty liver disease in obese rats by attenuating oxidative stress, inflammation and lipogenic gene expression. World J Hepatol 2021, 13, 315–327. [Google Scholar] [CrossRef] [PubMed]
- Jung, J.; Kim, N.K.; Park, S.; Shin, H.J.; Hwang, S.G.; Kim, K. Inhibitory effect of Phyllanthus urinaria L. extract on the replication of lamivudine-resistant hepatitis B virus in vitro. BMC Complement Altern Med 2015, 15, 255. [Google Scholar] [CrossRef] [PubMed]
- Slagle, B.L.; Andrisani, O.M.; Bouchard, M.J.; Lee, C.G.; Ou, J.H.; Siddiqui, A. Technical standards for hepatitis B virus X protein (HBx) research. Hepatology 2015, 61, 1416–1424. [Google Scholar] [CrossRef]
- Gupta, A.; Pandey, A.K. Plant Secondary Metabolites With Hepatoprotective Efficacy. Nutraceuticals and Natural Product Pharmaceuticals 2019, 71–104. [Google Scholar] [CrossRef]
- Dikshit, P.; Tyagi, M.K.; Shukla, K.; Sharma, S.; Gambhir, J.K.; Shukla, R. Hepatoprotective effect of stem of Musa sapientum Linn in rats intoxicated with carbon tetrachloride. Ann Hepatol 2011, 10, 333–339. [Google Scholar] [CrossRef]
- Batiha, G.E.; Alkazmi, L.M.; Wasef, L.G.; Beshbishy, A.M.; Nadwa, E.H.; Rashwan, E.K. Syzygium aromaticum L. (Myrtaceae): Traditional Uses, Bioactive Chemical Constituents, Pharmacological and Toxicological Activities. Biomolecules 2020, 10. [Google Scholar] [CrossRef]
- Ali, S.; Prasad, R.; Mahmood, A.; Routray, I.; Shinkafi, T.S.; Sahin, K.; Kucuk, O. Eugenol-rich Fraction of Syzygium aromaticum (Clove) Reverses Biochemical and Histopathological Changes in Liver Cirrhosis and Inhibits Hepatic Cell Proliferation. J Cancer Prev 2014, 19, 288–300. [Google Scholar] [CrossRef]
- Roy, C.K.; Kamath, J.V.; Asad, M. Hepatoprotective activity of Psidium guajava Linn. leaf extract. Indian J Exp Biol 2006, 44, 305–311. [Google Scholar]
- Ugbogu, A.E.; Emmanuel, O.; Uche, M.E.; Dike, D.E.; Okoro, B.C.; Ibe, C.; Ude, V.C.; Ekweogu, C.N.; Ugbogu, O.C. The ethnobotanical, phytochemistry and pharmacological activities of Psidium guajava L. Arabian Journal of Chemistry 2022, 15. Arabian Journal of Chemistry 2022, 15. [Google Scholar] [CrossRef]
- Oyibo, A.; Gbadegesin, M.A.; Odunola, O.A. Ethanol extract of Vitellaria paradoxa (Gaertn, F) leaves protects against sodium arsenite - induced toxicity in male wistar rats. Toxicol Rep 2021, 8, 774–784. [Google Scholar] [CrossRef]
- Dahiru, D.; Obidoa, O. Evaluation of the antioxidant effects of Ziziphus mauritiana Lam. Leaf extracts against chronic ethanol-induced hepatotoxicity in rat liver. Afr J Tradit Complement Altern Med 2007, 5, 39–45. [Google Scholar] [CrossRef] [PubMed]
- Kouam, A.F.; Owona, B.A.; Fifen, R.; Njayou, F.N.; Moundipa, P.F. Inhibition of CYP2E1 and activation of Nrf2 signaling pathways by a fraction from Entada africana alleviate carbon tetrachloride-induced hepatotoxicity. Heliyon 2020, 6, e04602. [Google Scholar] [CrossRef] [PubMed]
- Tietcheu, B.R.G.; Sass, G.; Njayou, N.F.; Mkounga, P.; Tiegs, G.; Moundipa, P.F. Anti-hepatitis C virus activity of crude extract and fractions of Entada africana in genotype 1b replicon systems. Am J Chin Med 2014, 42, 853–868. [Google Scholar] [CrossRef] [PubMed]
- Rouf, R.; Uddin, S.J.; Sarker, D.K.; Islam, M.T.; Ali, E.S.; Shilpi, J.A.; Nahar, L.; Tiralongo, E.; Sarker, S.D. Antiviral potential of garlic (Allium sativum) and its organosulfur compounds: A systematic update of pre-clinical and clinical data. Trends Food Sci Technol 2020, 104, 219–234. [Google Scholar] [CrossRef]
- Shang, A.; Cao, S.Y.; Xu, X.Y.; Gan, R.Y.; Tang, G.Y.; Corke, H.; Mavumengwana, V.; Li, H.B. Bioactive Compounds and Biological Functions of Garlic (Allium sativum L.). Foods 2019, 8. [Google Scholar] [CrossRef]
- Jacob, J.R.; Mansfield, K.; You, J.E.; Tennant, B.C.; Kim, Y.H. Natural iminosugar derivatives of 1-deoxynojirimycin inhibit glycosylation of hepatitis viral envelope proteins. J Microbiol 2007, 45, 431–440. [Google Scholar]
- Geng, C.A.; Ma, Y.B.; Zhang, X.M.; Yao, S.Y.; Xue, D.Q.; Zhang, R.P.; Chen, J.J. Mulberrofuran G and isomulberrofuran G from Morus alba L.: anti-hepatitis B virus activity and mass spectrometric fragmentation. J Agric Food Chem 2012, 60, 8197–8202. [Google Scholar] [CrossRef]
- Ogunmoyole, T.; Awodooju, M.; Idowu, S.; Daramola, O. Phyllanthus amarus extract restored deranged biochemical parameters in rat model of hepatotoxicity and nephrotoxicity. Heliyon 2020, 6, e05670. [Google Scholar] [CrossRef] [PubMed]
- Patel, J.R.; Tripathi, P.; Sharma, V.; Chauhan, N.S.; Dixit, V.K. Phyllanthus amarus: ethnomedicinal uses, phytochemistry and pharmacology: a review. J Ethnopharmacol 2011, 138, 286–313. [Google Scholar] [CrossRef]
- Fan, J.M.; Zhang, Q.; Xu, J.; Zhu, S.; Ke, T.; Gao, D.F.; Xu, Y.B. Inhibition on Hepatitis B virus in vitro of recombinant MAP30 from bitter melon. Mol Biol Rep 2009, 36, 381–388. [Google Scholar] [CrossRef]
- Waiyaput, W.; Payungporn, S.; Issara-Amphorn, J.; Panjaworayan, N.T. Inhibitory effects of crude extracts from some edible Thai plants against replication of hepatitis B virus and human liver cancer cells. BMC Complement Altern Med 2012, 12, 246. [Google Scholar] [CrossRef] [PubMed]
- Yao, X.; Li, J.; Deng, N.; Wang, S.; Meng, Y.; Shen, F. Immunoaffinity purification of alpha-momorcharin from bitter melon seeds (Momordica charantia). J Sep Sci 2011, 34, 3092–3098. [Google Scholar] [CrossRef]
- Hanafy, A.; Aldawsari, H.M.; Badr, J.M.; Ibrahim, A.K.; Abdel-Hady Sel, S. Evaluation of Hepatoprotective Activity of Adansonia digitata Extract on Acetaminophen-Induced Hepatotoxicity in Rats. Evid Based Complement Alternat Med 2016, 2016, 4579149. [Google Scholar] [CrossRef] [PubMed]
- Silva, M.L.; Rita, K.; Bernardo, M.A.; Mesquita, M.F.; Pintao, A.M.; Moncada, M. Adansonia digitata L. (Baobab) Bioactive Compounds, Biological Activities, and the Potential Effect on Glycemia: A Narrative Review. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- NAFDAC. The Role Of NAFDAC In Traditional Herbal Medicine Development And Approval In Nigeria. Control, N. A. f. F. a. D. A. a., Ed.; Abuja: 2019; p. 13. NAFDAC. The Role Of NAFDAC In Traditional Herbal Medicine Development And Approval In Nigeria. Control, N. A. f. F. a. D. A. a. Eds.
- Oguntade, A.E.; Oluwalana, I.B. Structure, control and regulation of the formal market for medicinal plants' products in Nigeria. Afr J Tradit Complement Altern Med 2011, 8, 370–376. [Google Scholar] [CrossRef]
- Modibbo, M.R.; Ibrahim, H.; Sulaiman, M.Y.; Zakir, B. Maganin Gargajiya: Assessing the Benefits, Challenges, and Evidence of Traditional Medicine in Nigeria. Cureus 2024, 16, e71425. [Google Scholar] [CrossRef] [PubMed]
- Awodele, O.; Amagon, K.I.; Usman, S.O.; Obasi, P.C. Safety of herbal medicines use: case study of ikorodu residents in Lagos, Nigeria. Curr Drug Saf 2014, 9, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Abubakar, I.B.; Kankara, S.S.; Malami, I.; Danjuma, J.B.; Muhammad, Y.Z.; Yahaya, H.; Singh, D.; Usman, U.J.; Ukwuani-Kwaja, A.N.; Muhammad, A.; et al. Traditional medicinal plants used for treating emerging and re-emerging viral diseases in northern Nigeria. Eur J Integr Med 2022, 49, 102094. [Google Scholar] [CrossRef]
- John, A.J.; Odula, I.L.; Etinosa, O.B.; Ifeanyi, O.V. Effectiveness of herbal and conventional management interventions of Hepatitis B virus. Afr J Infect Dis 2025, 19, 1–12. [Google Scholar] [CrossRef]
Figure 1.
Classification and disease burden of viral hepatitis.
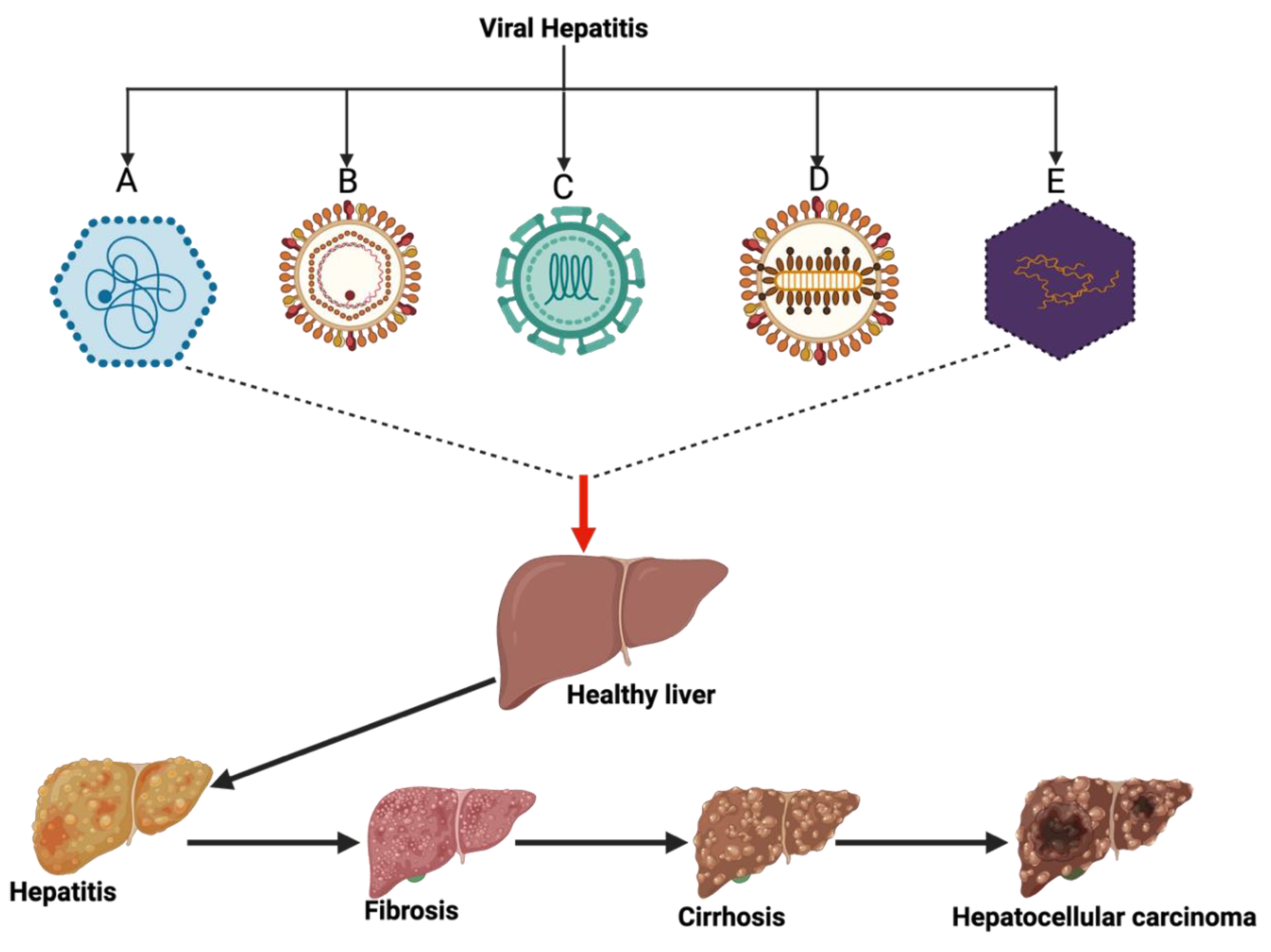
Figure 2.
Map of Nigeria showing the six geopolitical zones.
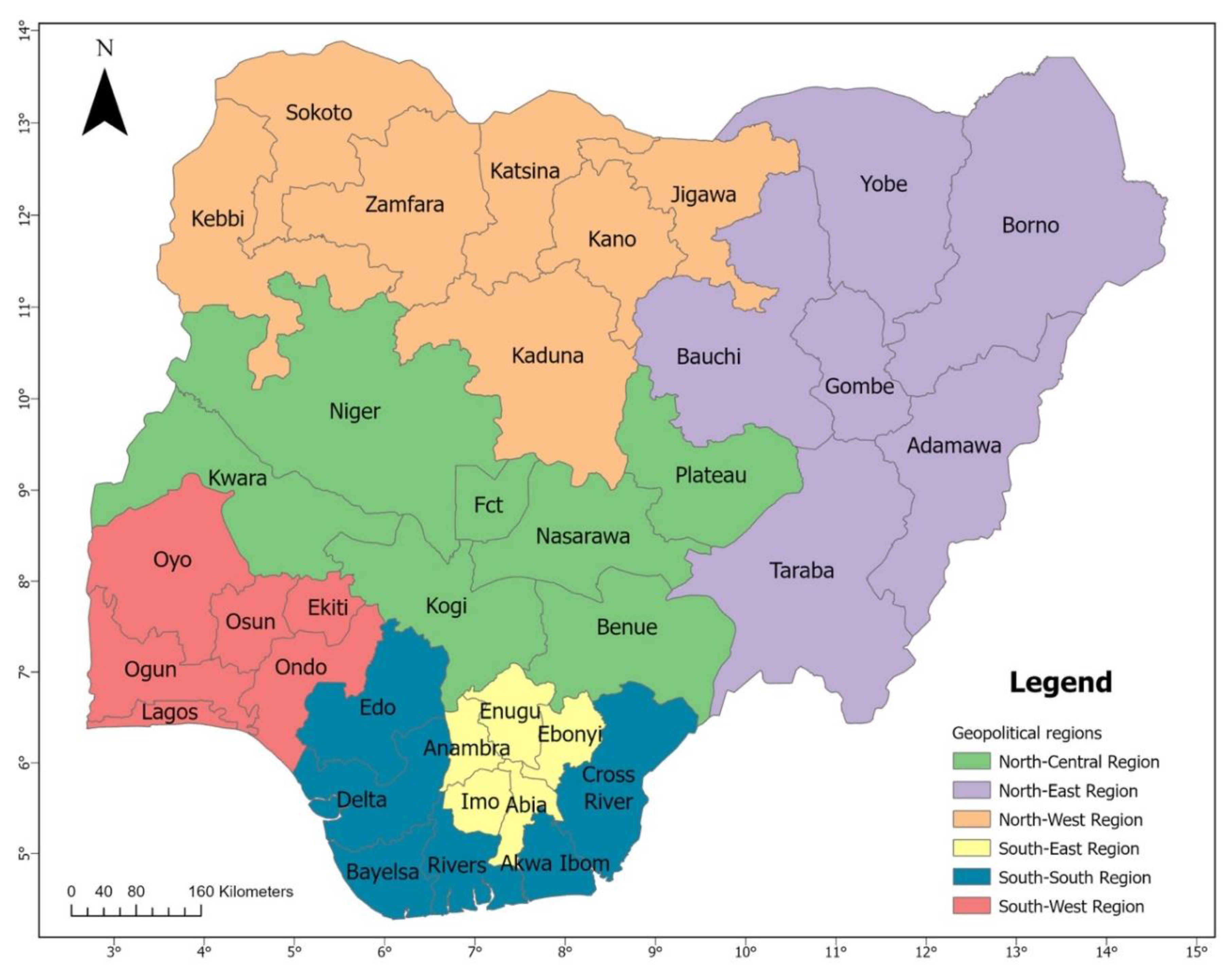
Figure 3.
Structure of HAV. Generated with Biorender.com.
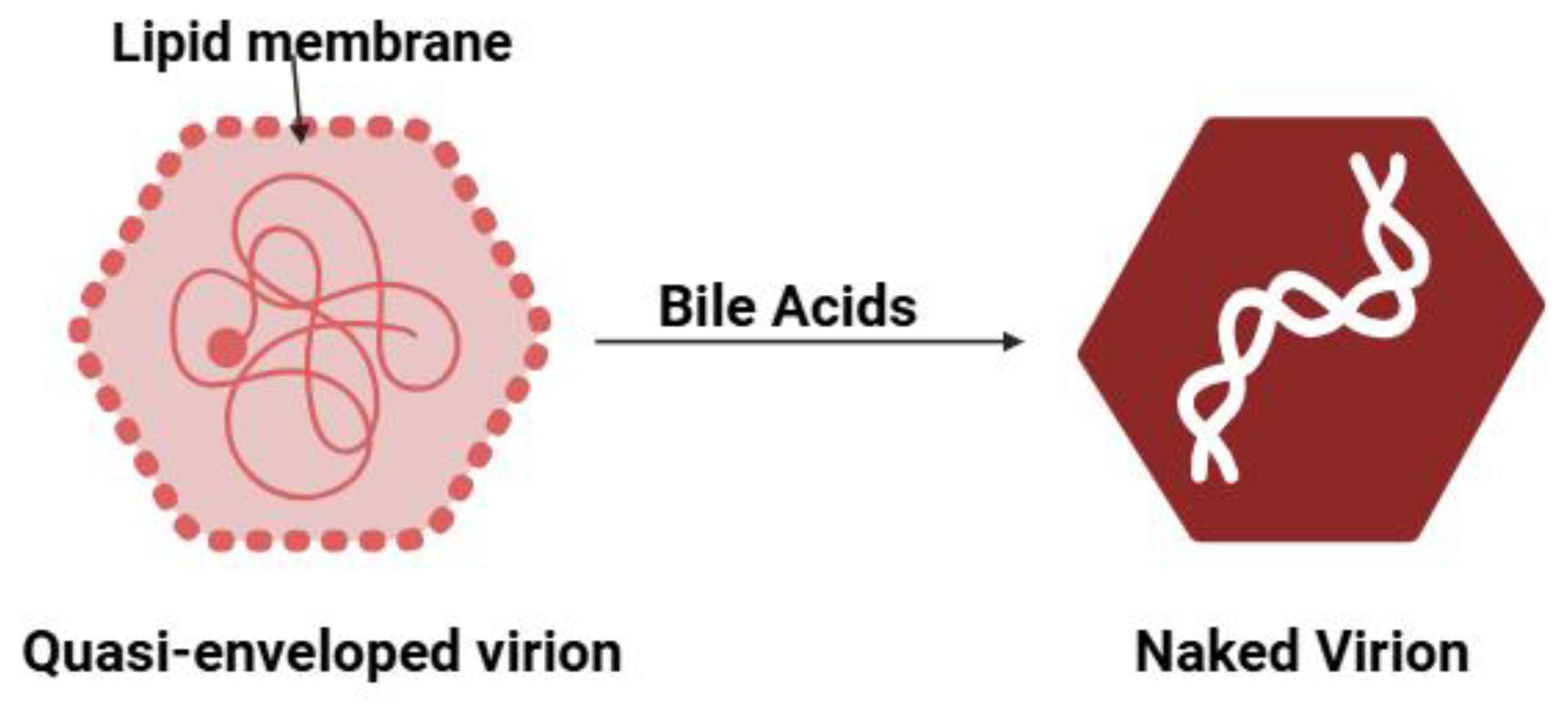
Figure 4.
Map of Nigeria showing the distribution of HAV.
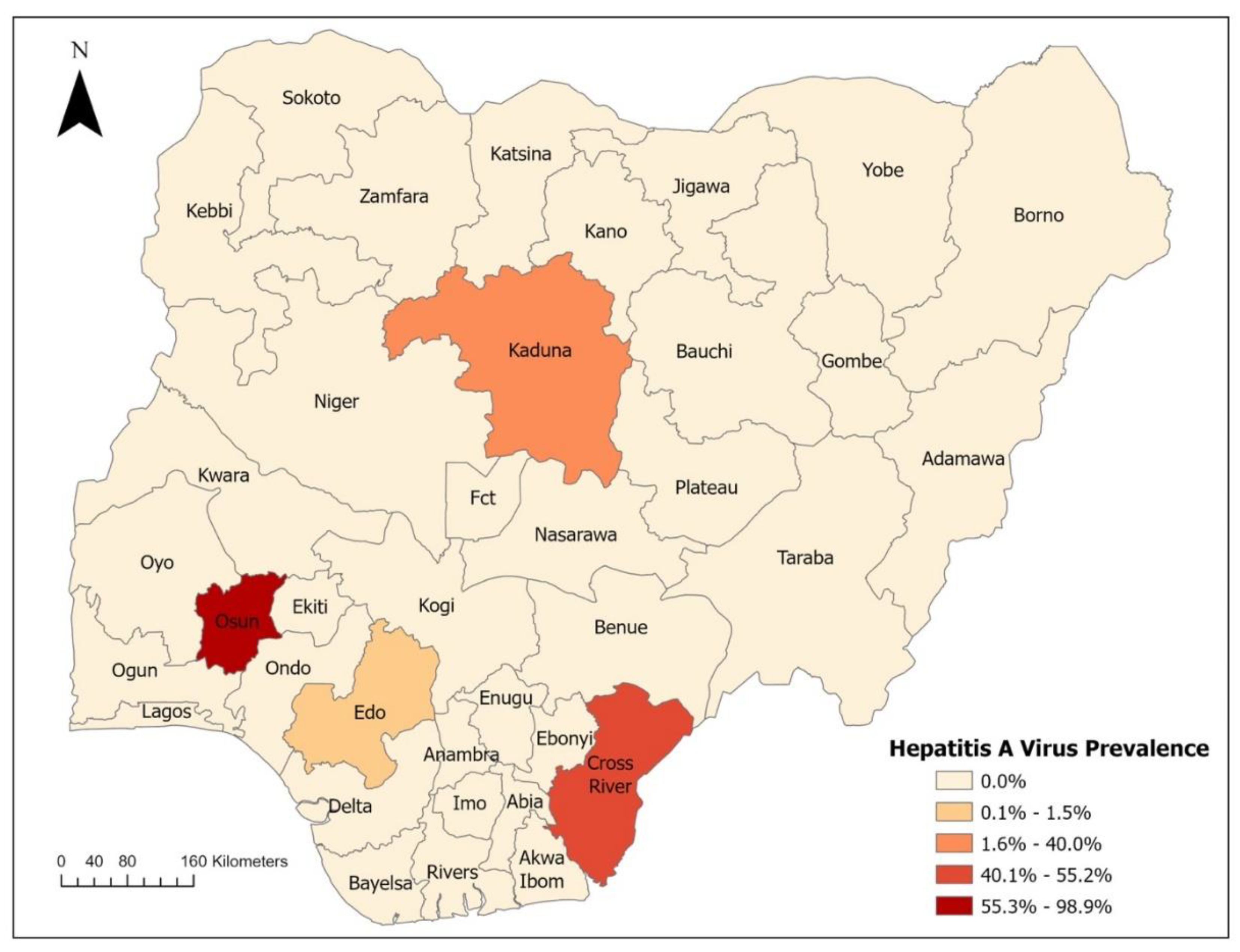
Figure 5.
A Structure of HBV. Generated with Biorender.com.
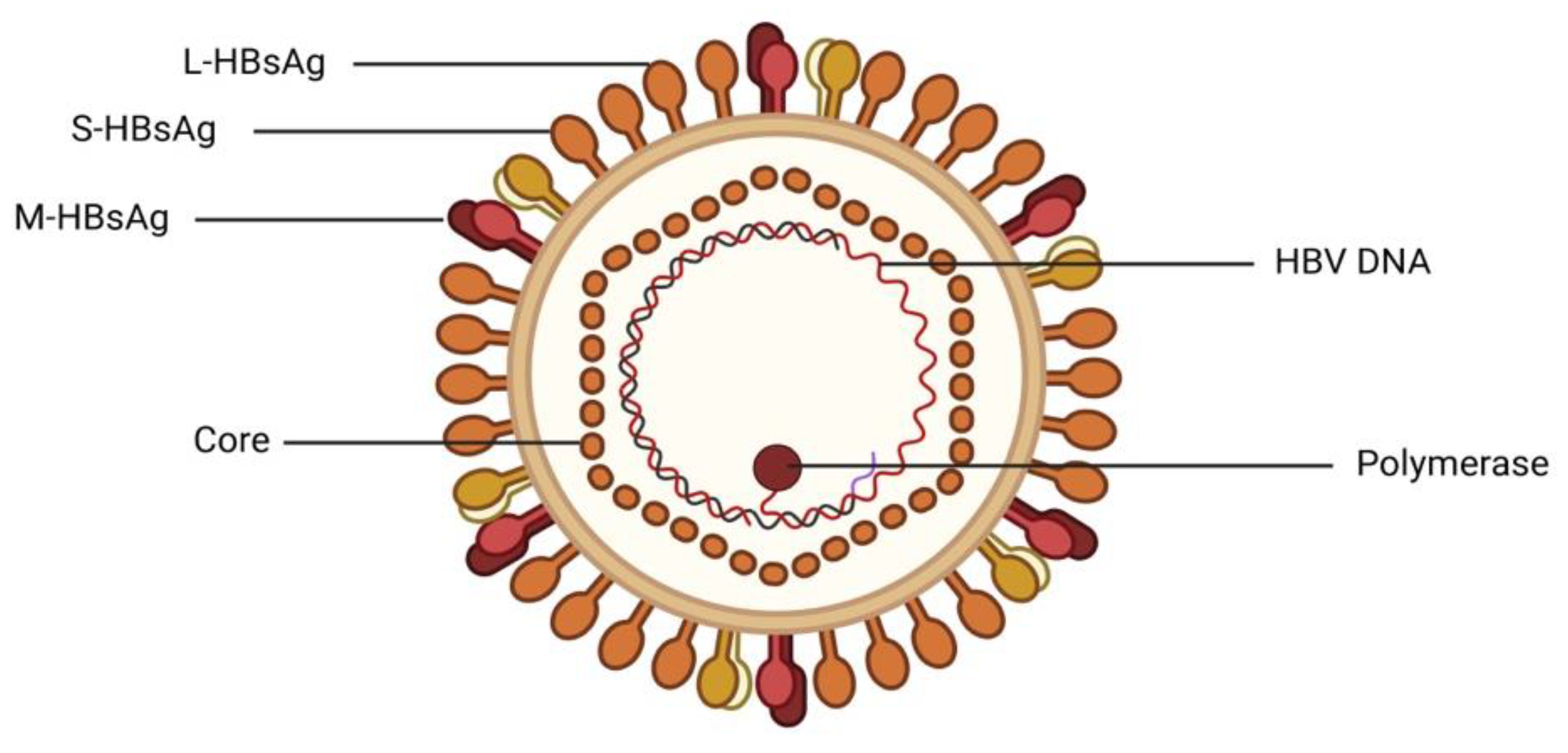
Figure 6.
Map of Nigeria showing the distribution of HBV.
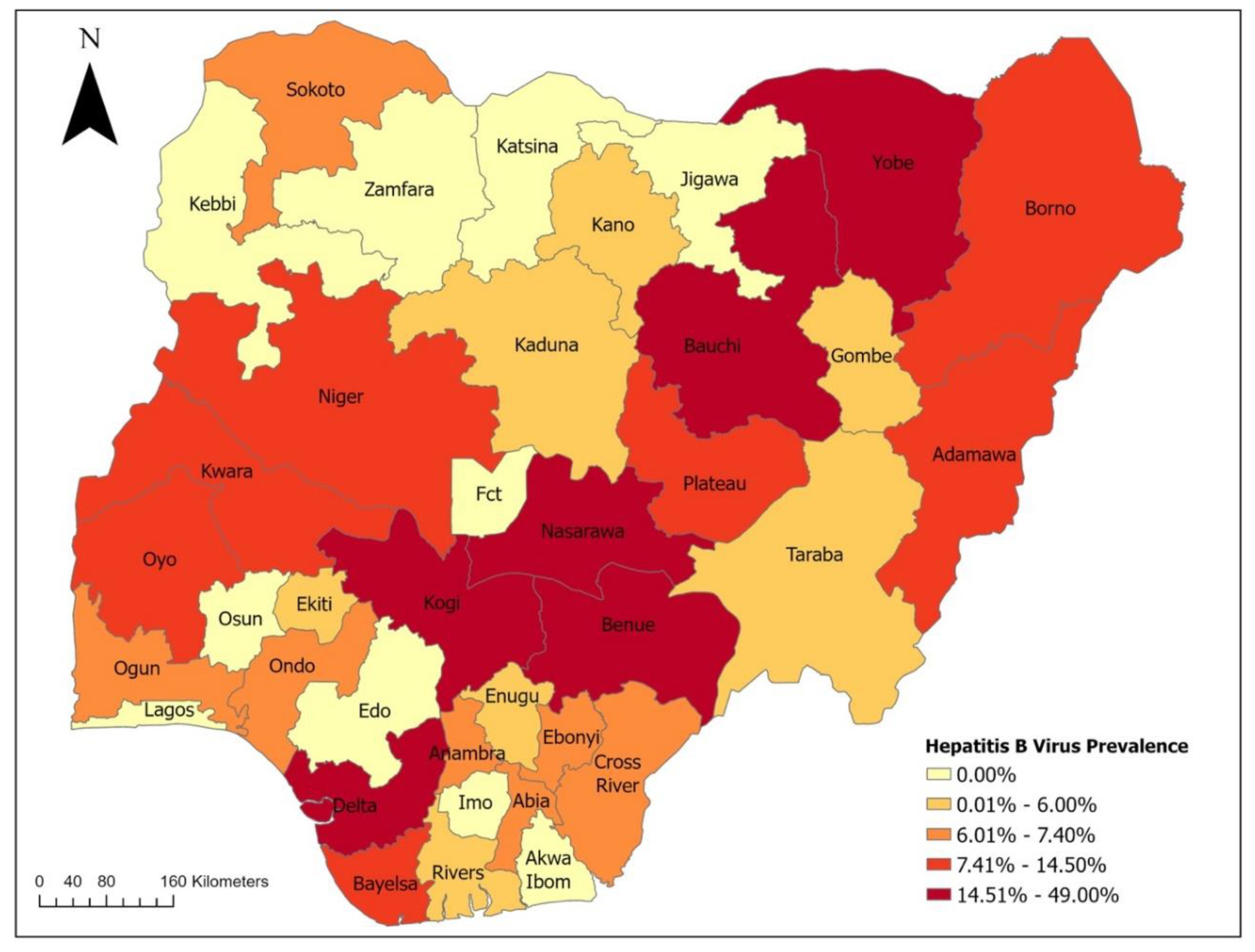
Figure 7.
A Structure of HCV. Generated with Biorender.com.
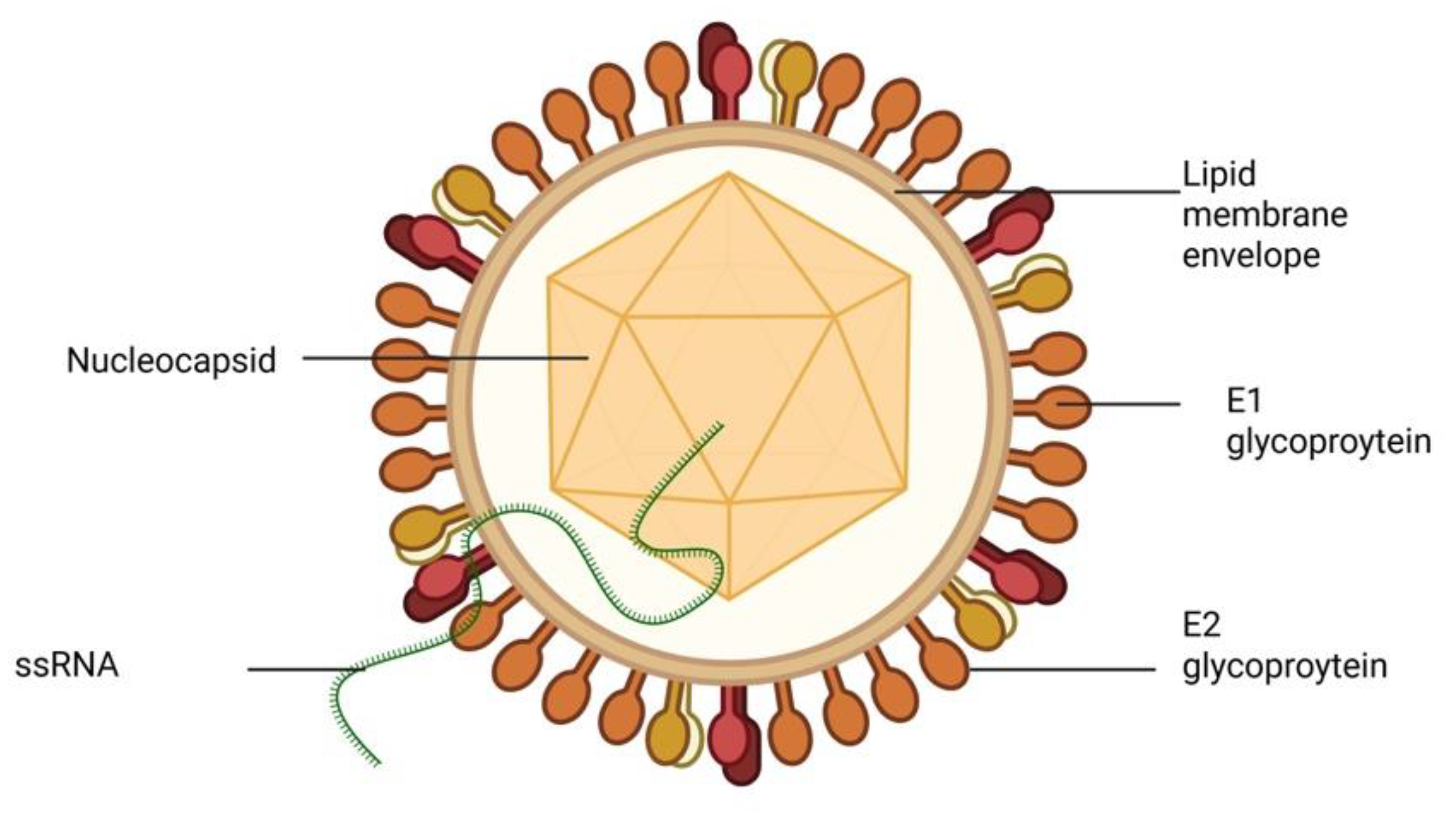
Figure 8.
Map of Nigeria showing the distribution of HCV.
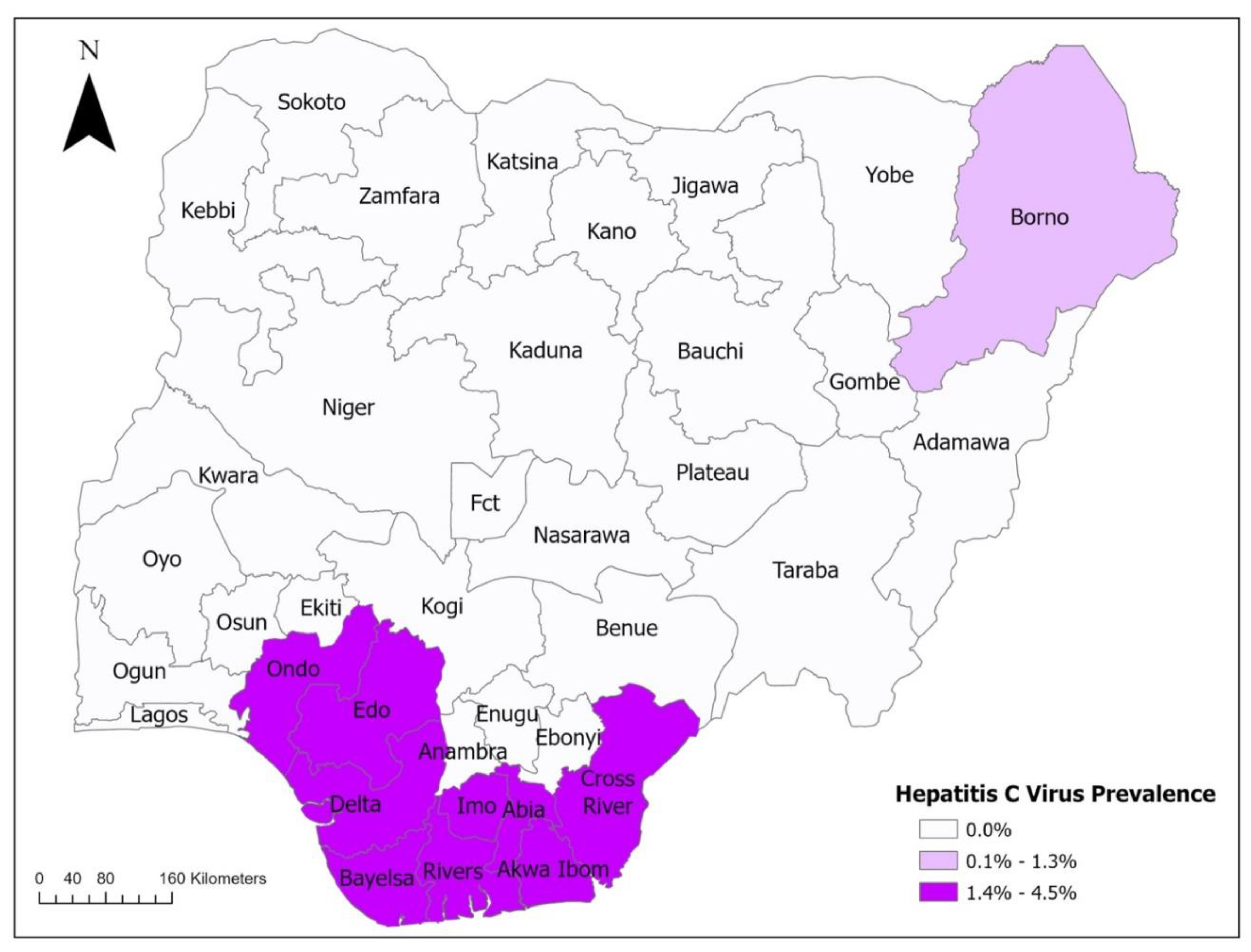
Figure 9.
A Structure of HDV. Generated with Biorender.com.
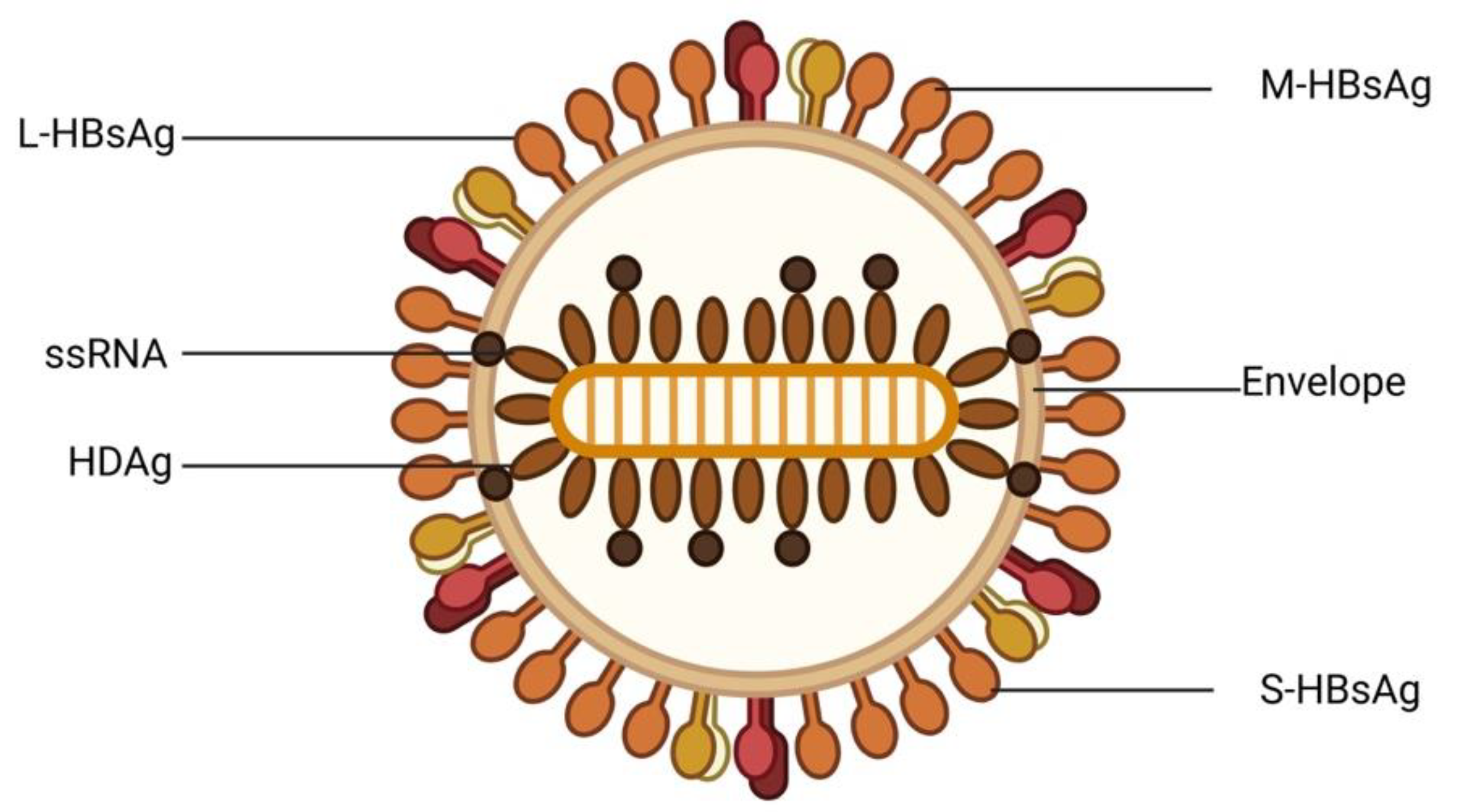
Figure 10.
Map of Nigeria showing the distribution of HDV.
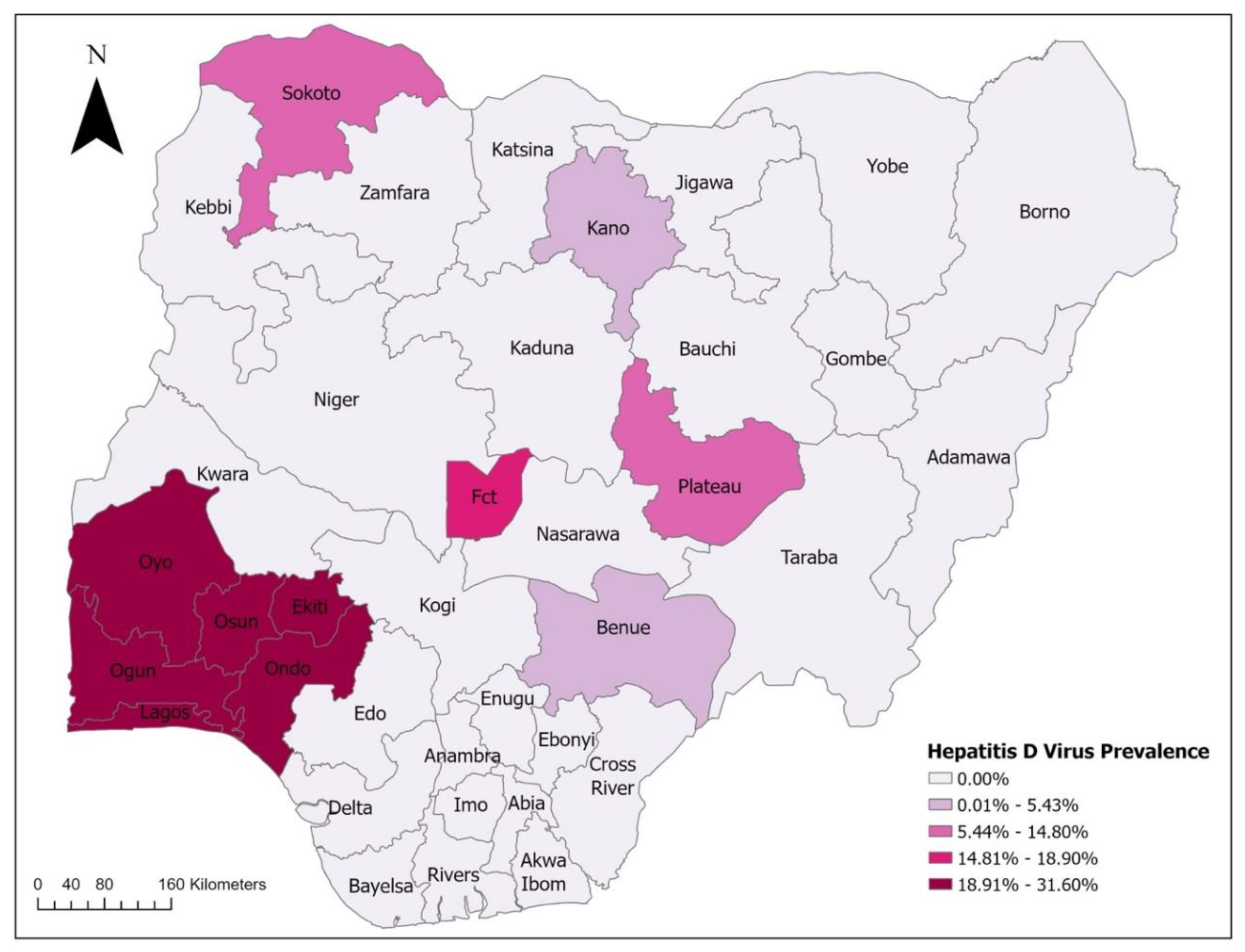
Figure 11.
A Structure of HEV. Generated with Biorender.com.
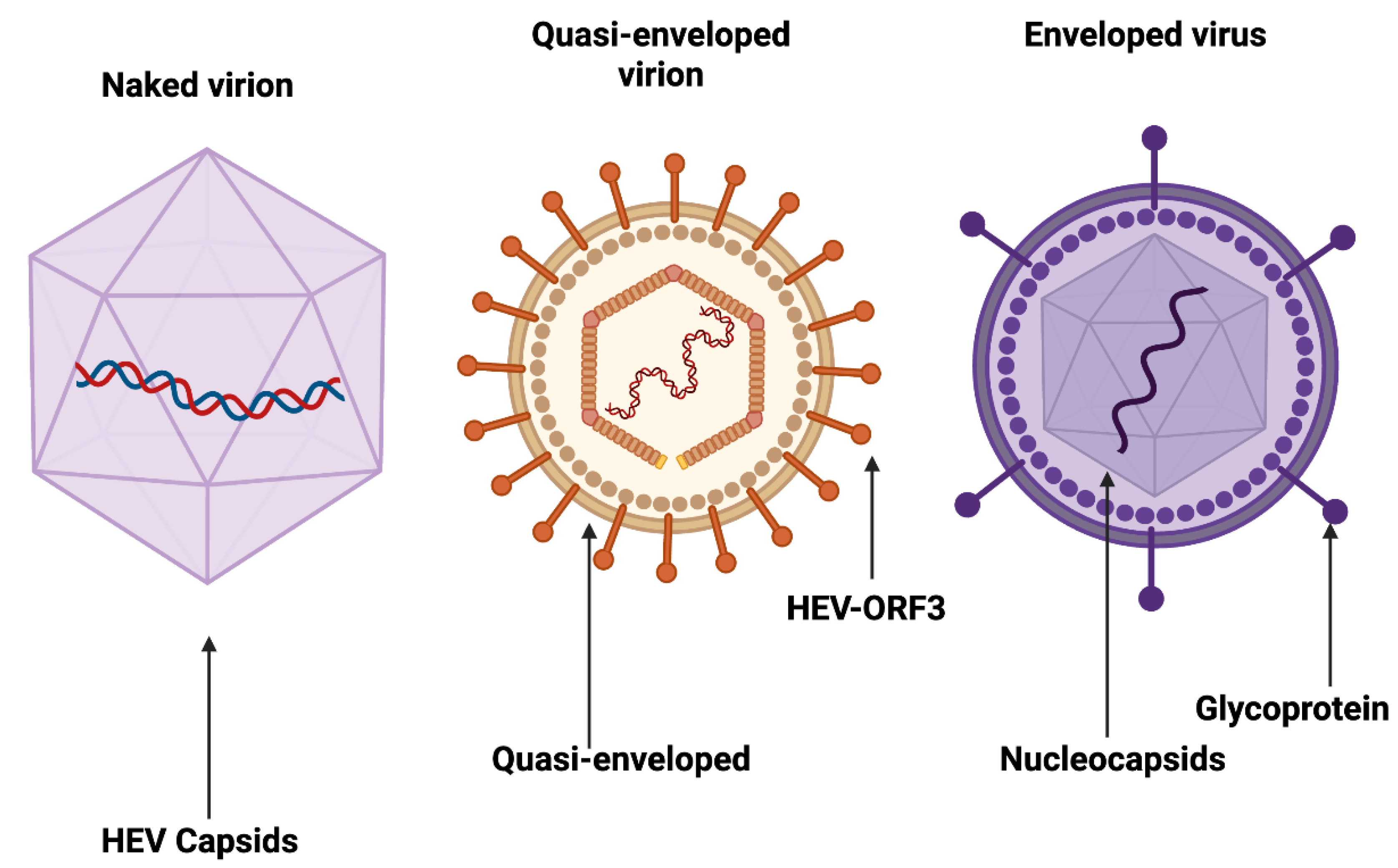
Figure 12.
Map of Nigeria showing the distribution of HEV.
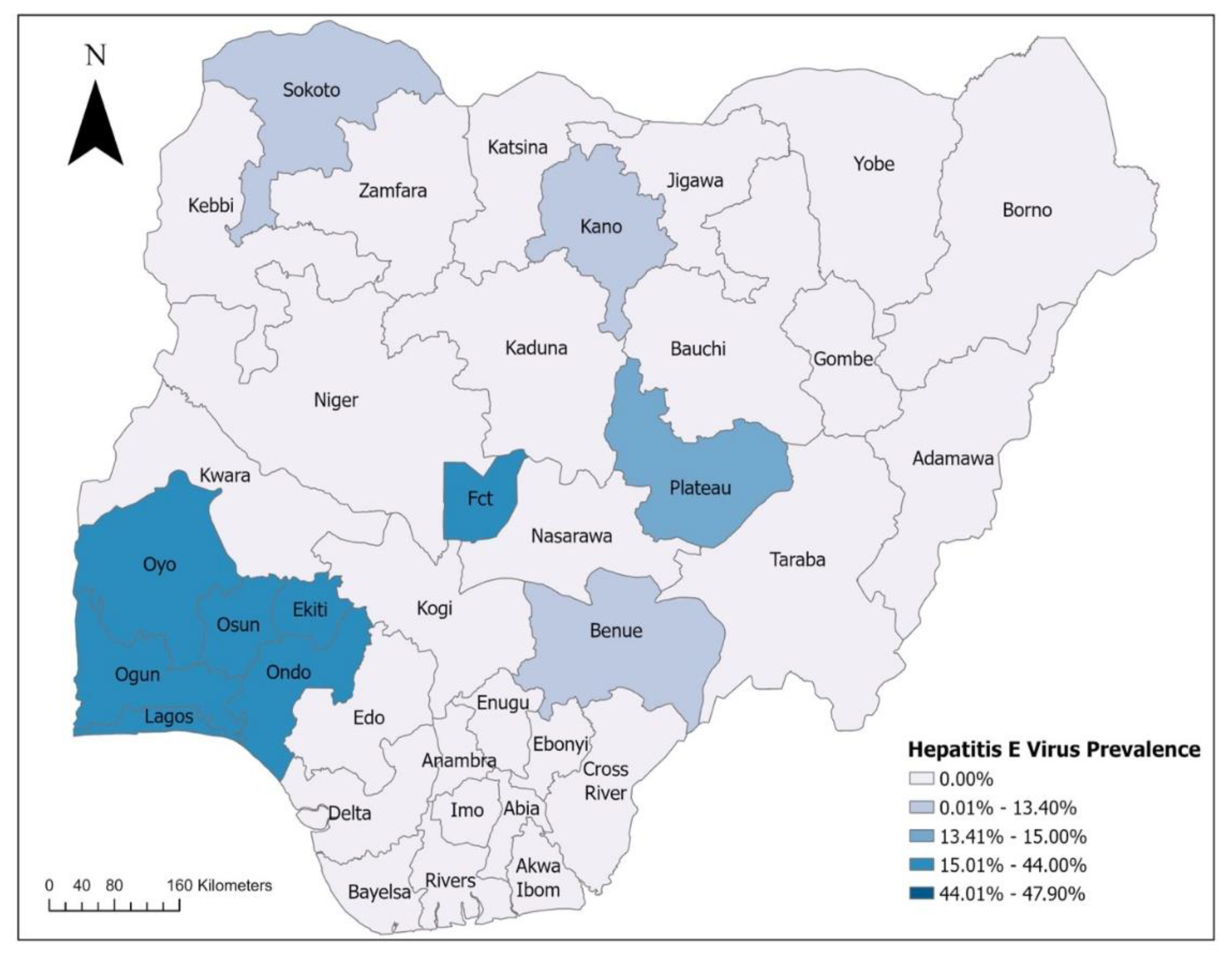
Figure 13.
A Structure of Silybum marianum (L.) Gaertn. Generated with Biorender.com.
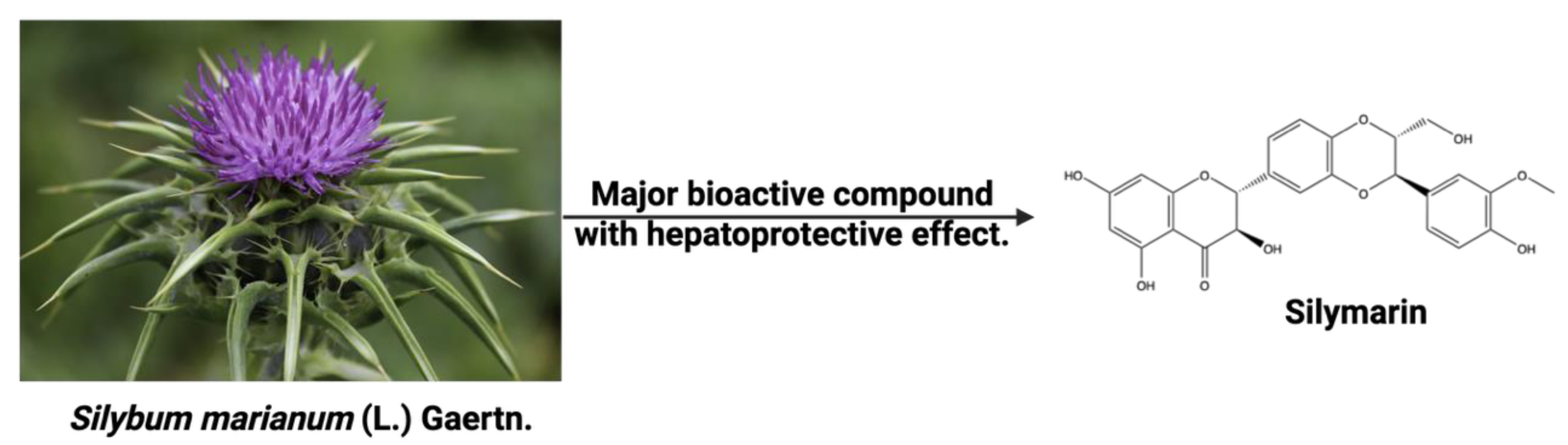
Figure 14.
Pharmacological effect of silymarin on the regulation of NF-κB. Generated with Biorender.com.
Figure 14.
Pharmacological effect of silymarin on the regulation of NF-κB. Generated with Biorender.com.
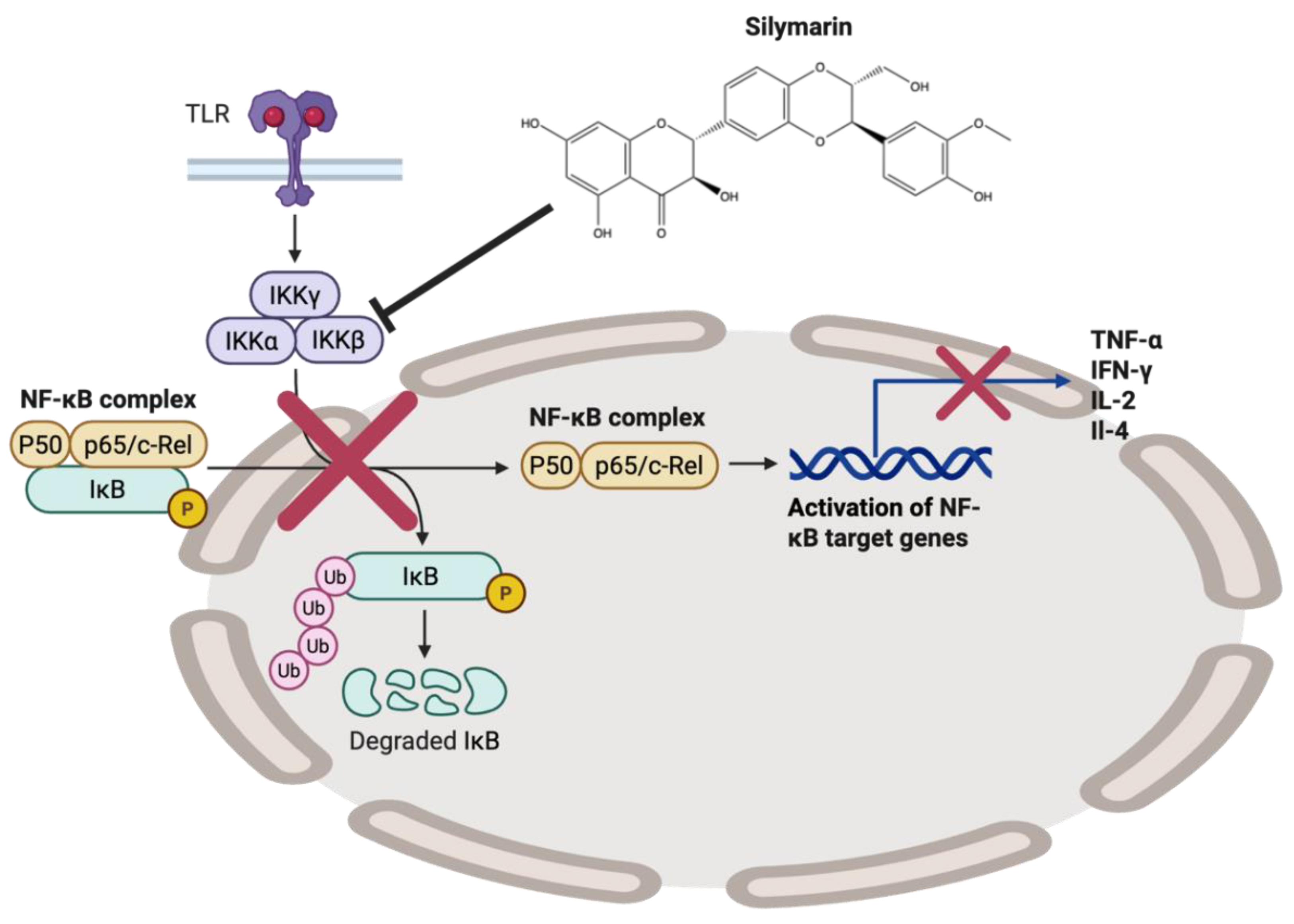
Figure 15.
A Structure of Glycyrrhizin extracted from Glycyrrhiza glabra. Generated with Biorender.com.
Figure 15.
A Structure of Glycyrrhizin extracted from Glycyrrhiza glabra. Generated with Biorender.com.
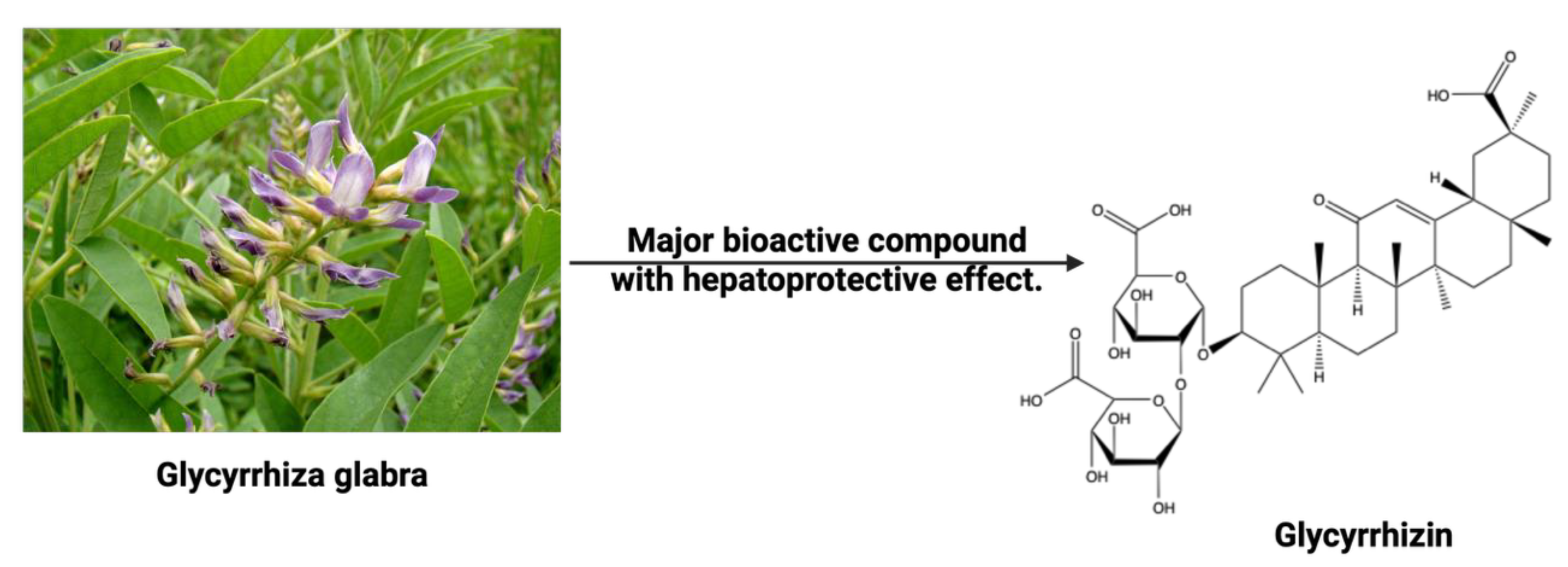
Figure 16.
A Structure of phyllanthin extracted from Phyllanthus amarus.
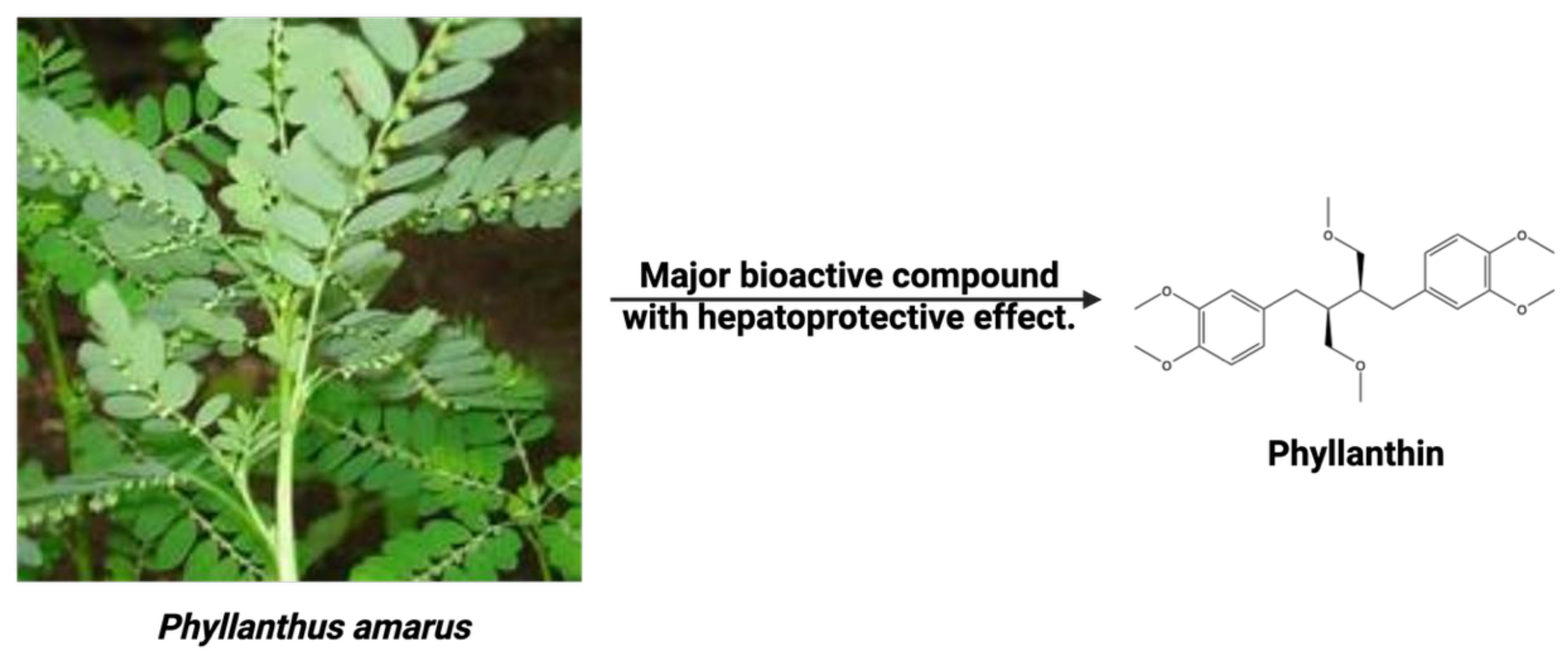
Figure 17.
Structures of the major bioactive compounds in Schisandra chinensis. Generated with Biorender.com.
Figure 17.
Structures of the major bioactive compounds in Schisandra chinensis. Generated with Biorender.com.
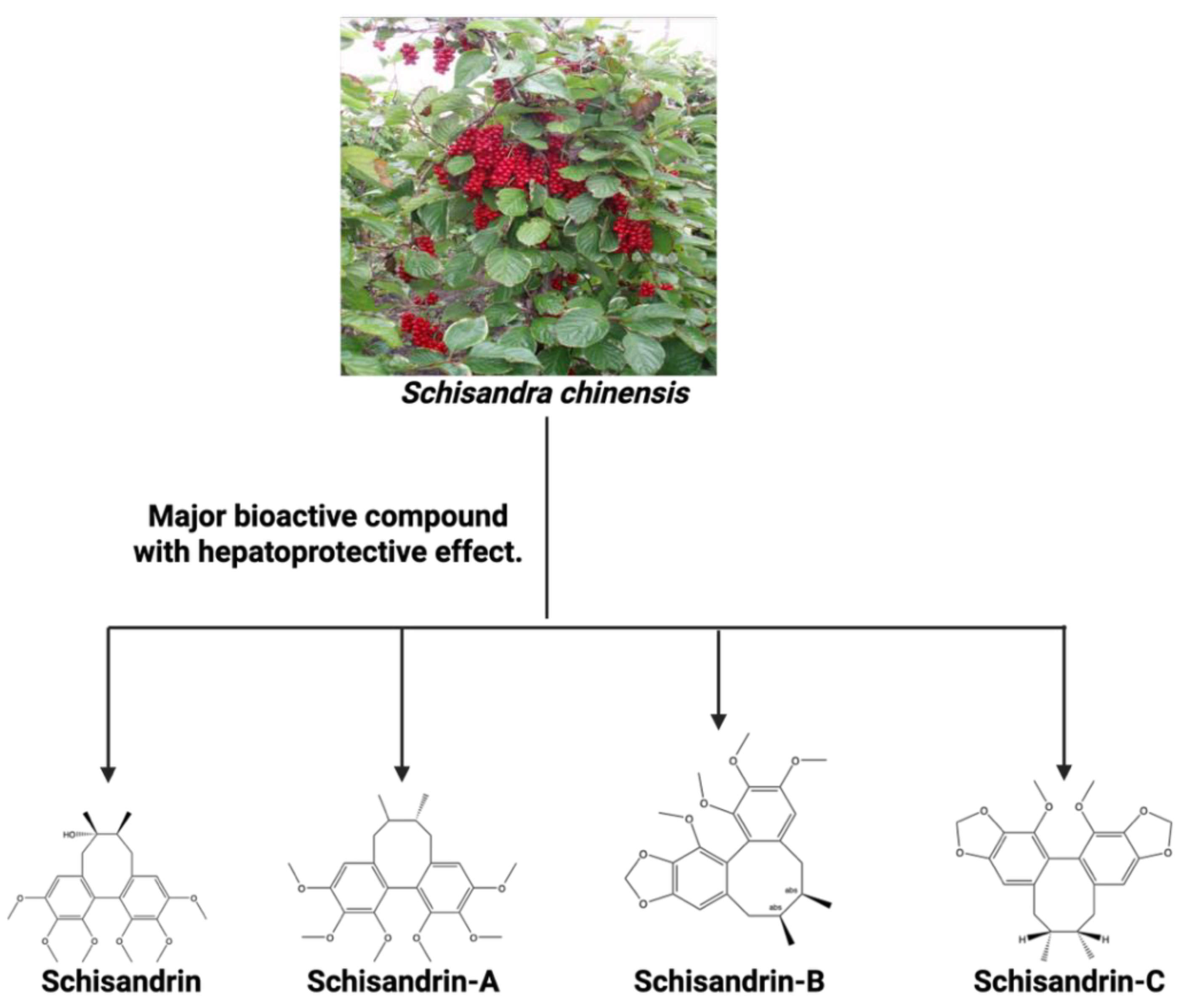
Figure 18.
Structures of the major bioactive compounds in C. spinosa. Generated with Biorender.com.
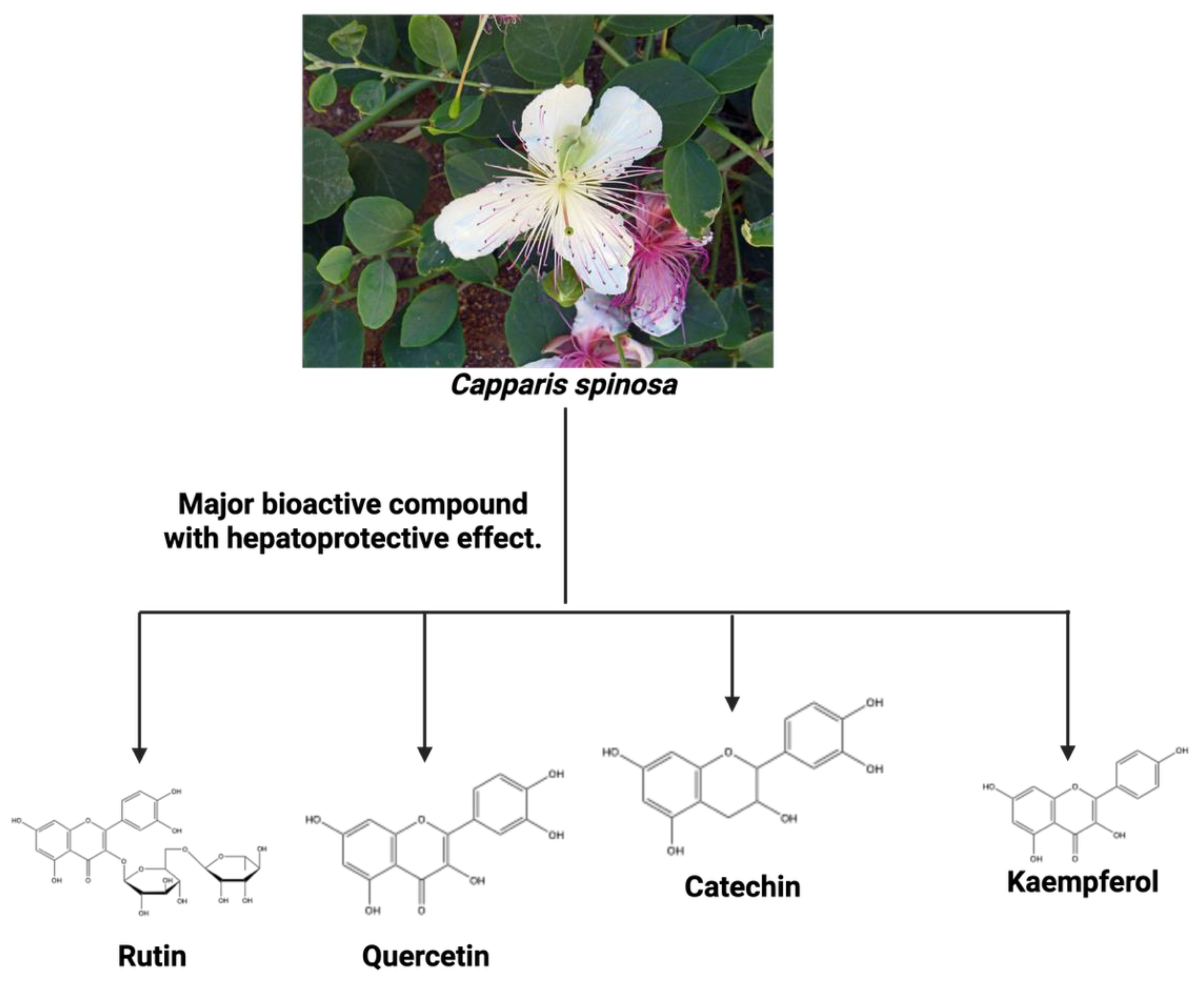
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



