Submitted:
10 June 2025
Posted:
12 June 2025
Read the latest preprint version here
Preprints on COVID-19 and SARS-CoV-2
Abstract
Colonization of Legionella spp. in engineered water systems constitutes a major public health threat. In this study, a six-year environmental surveillance (2020–2025) of Legionella colonization in five different types of facilities in Crete, Greece, is presented, including hotels, cruise ships, and healthcare facilities with primary healthcare facilities, public hospitals, and private clinics. A total of 1,081 water samples were collected and analyzed, with the overall positivity calculated using culture-based methods. Only 16.46% of the samples exceeded the regulatory limit (>10³ CFU/L) in the total sample, with the overall Legionella positivity being 44.59%. Colonization by facility category showed higher rates in primary healthcare facilities with 85.96%, followed by public hospitals with 46.36%, passenger ships with 36.93%, and hotels with 38.08%, and finally private clinics. The association of environmental risk factors with Legionella positivity revealed a strong effect at hot water temperatures < 50°C (RR = 2.05) and free chlorine residuals < 0.2 mg/L (RR = 2.22) (p < 0.0001). Serotyping analysis revealed primarily an overall dominance of serogroups 2-15 of L. pneumophila; nevertheless, serogroup 1 was particularly prevalent in hospitals, ships, and hotels. Based on these findings, the requirement for continuous environmental monitoring, as well as risk management plans tailored to each facility with preventive thermochemical controls, is highlighted. Finally, operational disruptions such as those experienced during the COVID-19 pandemic, especially in primary care facilities and marine systems, require special attention.
Keywords:
Legionella spp.
; Environmental surveillance
; Water safety plans
; Healthcare facilities
; Passenger ships
; Hotels
; Thermochemical disinfection
; COVID-19 pandemic
; Risk assessment
1. Introduction
Water distribution systems are important parts of public infrastructure because they provide clean drinking water and help stop the spread of waterborne diseases [1,2,3]. Nonetheless, under certain physicochemical and operational conditions, these engineered systems can unintentionally become breeding grounds for opportunistic pathogens like Legionella spp. (especially L. pneumophila), which are gram-negative bacteria that cause Legionnaires' disease, a severe form of atypical pneumonia that is very serious and causes a lot of illness and death, especially in older people and people with weakened immune systems [4,5,6,7,8,9]. According to the ECDC Legionnaires' Disease Annual Epidemiological Report for 2021, 29 countries reported 10,723 cases, of which 10,004 (93%) were confirmed [10]. The rate of notifications per 100,000 people went up to 2.4, which is higher than any other year that was looked at. Italy, France, Spain, and Germany together made up 75% of recorded cases, even though their populations only made up about 50% of the EU/EEA population. 704 of the 8,054 cases with a known outcome ended in death (9%) [11].
Legionella loves warm water and is quite good at living in constructed systems with stagnant water, not enough treatment, and the right temperature ranges [12]. Biofilms and host protozoa let it live longer and spread faster. Outbreaks often happen in places with high risk, such hospitals, hotels, and ships, since their plumbing is complicated, they don't use water all the time, and they have different ways of keeping things clean [13,14,15,16,17,18].
Studies have shown that water systems in buildings like hotels, hospitals, and ships are quite likely to be colonized by Legionella, making them high-risk potent places for Legionella colonization [19,20,21,22,23,24,25,26,27]. For instance, Alexandropoulou et al. found that L. pneumophila was quite common in Greek healthcare facilities, and that temperature and system design affected its spread [20]. Naher also found that hotel hot water systems are high-risk places, and he pointed to bad temperature management and the lack of water safety plans (WSPs) as two of the main reasons why [21]. In our previous work, Papadakis et al. examined hotel water systems across the island of Crete. Between 2000 and 2019, it was observed that about 63% of the hotels inspected, after a case notification of Legionnaires' disease, were found to be colonized with Legionella spp [22]. The study also highlighted the important things that need to manage water distribution systems in order to remain clean and disinfected. One of these was the successful implementation of WSPs to improve hotel water supply and sanitation systems.
Long-term building closures and less water use during the COVID-19 epidemic made it easy for Legionella to grow [23,24,28,29]. Rhoads and Hammes pointed out that microbial growth increased during the lockdown-related standstill, which shows how important flushing measures can be [30]. During the pandemic, Kunz et al. saw that U.S. hotels and motels were less likely to follow Legionella control strategies, which made the risk of outbreaks even higher [31].
Public health authorities are increasingly calling for integrated control measures, like WSPs that use Hazard Analysis and Critical Control Points (HACCP) principles, to help reduce the risk of legionellosis in complex healthcare and hospitality systems [32,33] and have demonstrated effectiveness in reducing Legionella risk in complex healthcare and hospitality systems [34,35]. Disinfection strategies involving the application of agents such as monochloramine, chlorine dioxide, and hydrogen peroxide have demonstrated efficacy in reducing Legionella colonization, particularly when embedded within comprehensive monitoring and maintenance frameworks [36,37]. Nevertheless, the dynamics of Legionella colonization remain highly context-dependent, necessitating localized risk assessments that consider building design, usage patterns, and endemic microbiological profiles.
To our knowledge, this is the first longitudinal environmental surveillance study in Greece to systematically assess Legionella colonization trends across multiple high-risk facility types—including hospitals, outpatient clinics, hotels, and passenger ships—during and after the COVID-19 pandemic.
The present study aims to evaluate and compare Legionella spp. colonization levels across these diverse facilities on the island of Crete from 2020 to 2025. The goal is to identify facility-specific risk factors and assess the impact of pandemic-related disruptions on water system hygiene, thereby informing future prevention strategies and water safety policy implementation in complex aquatic environments.
2. Materials and Methods
2.1. Study design and sample collection
From 2020 to 2025, this multiparametric environmental monitoring study was conducted covering the entire territory of the Region of Crete, Greece. The study was conducted by the Public Health Authority of the Region of Crete in collaboration with the Regional Public Health Laboratory and the Department of Clinical Microbiology and Microbial Pathogenesis. The aim of the study was to assess the prevalence of Legionella spp. colonization and risk factors in water distribution systems in complex infrastructures used by the public.
Sampling included five categories of facilities: (1) hotels - accommodation facilities, (2) passenger ships and three different health care facilities, including (3) primary care units, (4) public hospitals and (5) private clinics (Table 1). In total, samples employed by 41 different facilities were studied to ensure a wide spatial and typological distribution. Each location was inspected and sampled after reports or randomly sampled by public and environmental health officials, following standardized procedures. Specifically for hotels, a total of 13 hotels associated with travel-associated Legionnaires' disease (TALD) were inspected, following their reporting to the European Legionnaires' Disease Surveillance Network (ELDSNet) for the period 2020 to 2025.
Systematic sample collection included 1,081 water samples from multiple points in the water distribution network for each facility. The sampling points are listed in Table 2 comprising: municipal pipe inlets, water storage tanks and hot water boilers and heaters, terminal outlets (showers, faucets and taps in patient or visitor rooms), swimming pools and hot tubs, where applicable, and outlets proximal or peripheral to the facility’s primary water source. The strategy followed intentionally targeted high-risk nodes within the facility’s plumbing systems, with an emphasis on aerosol-generating outlets as well as known outlets based on temperature profiles or user reports associated with colonization. Their grouping based on sampling characteristics was direct vs. indirect flow paths; cold vs. hot water; proximal (close) vs. distal (far) outlet locations.
The samples were taken following international and European standards, namely ISO 5667-1:2020 and ISO 5667-1:2023 as well as the European Technical Guidelines for the Prevention, Control and Investigation of Infections Caused by Legionella spp. (ECDC) [38,39,40].
Briefly, the sample collection procedure followed is as follows: a sterile 1 liter container containing 20 mg of sodium thiosulfate was used to neutralize the presence of disinfectant residues. The samples were stored at a temperature of 5 ± 3 °C, in shaded conditions and their transport to the regional microbiology laboratory for analysis was carried out within 24 hours under controlled conditions. The measurements of the physicochemical parameters were made directly on site using calibrated portable devices. Measurements included: Free residual chlorine concentration (mg/L), Water temperature (°C) after 2 minutes of rinsing, pH levels, Turbidity where applied, Sampling point type (direct vs. indirect; hot vs. cold; near vs. far), Facility metadata (disinfection method, capacity, water source, and presence or absence of a documented Water Safety Plan (WSP)).
2.2. Microbiological Analysis
Microbiological testing for the detection and quantification of Legionella spp. from water samples was performed by culture according to the International Standard method ISO 11731:2017 [41].
Briefly, water samples were concentrated by filtration and were re-suspended in Distilled Deionized water. A volume of the suspension (200 μL) was spread on (BCYE), Buffered Charcoal Yeast extract without l-cysteine (BCY), and Glycine Vancomycin Polymyxin Cycloheximide (GVPC) agar (Biomérieux, France). For the Petri dishes (Culture plates): (a) directly after filtration; (b) after incubation at 50 °C for 30 min and (c) after the addition of an acid buffer (0.2 mol/L solution of HCL, pH 2.2). The detection limit of the procedure was 50 CFU/L. The inoculated plates were incubated for up to 10 days at 36 ± 1 °C a 2.5% CO₂ atmosphere with increased humidity. Suspected colonies were randomly chosen for subculture on BCY, BCYE and GVPC agar.
A matrix-assisted laser desorption ionization time-of-flight mass spectrometry (MALDI-TOF MS, Bruker Microflex LT) equipped with a micro-SCOUT ion source was used for the identification of individual Legionella colonies against its microbial database (v 3.1.2.0). Spectra were recorded using the flex Control software with the default parameters for optimization set by the manufacturer (Bruker Daltonics, Leipzig, Germany). For each spectrum, 240 laser shots were collected and analyzed (6 × 40 laser shots from 120 different positions of the target spot). All identifications were evaluated according to the manufacturer scoring scheme.
Acid and heat pretreatment steps were employed to reduce background flora and enhance Legionella recovery. The detection limit of the method was 50 CFU/L, allowing for reliable quantification within the regulatory action range. Confirmed colonies were further serotyped to distinguish L. pneumophila serogroups (especially SG1 vs. SG2–15) and identify non-pneumophila species, providing key epidemiological insights into pathogen virulence and potential disease risk.
2.3. Risk Assessment and Statistical Analysis
To better calculate the risk, we used two different approaches. The first one was in accordance with the recommendations of the European Legionnaires’ disease Surveil-lance Network (ELDSNet), at which the microbiological results of the water samples were analytically and statistically analyzed according to the number of Legionella bacteria in the water sample, which could represent a particular risk to human health. An insignificant risk was noted at ≤103 CFU/L, medium risk at >103 CFU/L but <104 CFU/L, and high risk at ≥104 CFU/L.
All statistical analyses were conducted using the IBM SPSS Statistics Version 30 statistical package, the Epi Info 2000 version 7.2.0.1 (Centers for Disease Control and Pre-vention, Atlanta, GA, USA) and the MedCalc relative risk calculator statistical software free online version [42,43,44]; Descriptive statistics included frequencies, proportions, and Wilson 95% confidence intervals. Relative Risks (RR) with 95% confidence intervals were calculated for key non-compliant conditions, and logistic regression was applied to identify independent predictors of positivity. The analyses were calculated to assess categorical risk variables from water distribution systems and faculty characteristics, associated with Legionellae-positive test results. Linear regression was used to explore trends and quantify associations between Legionella concentrations and physicochemical parameters. The results were considered statistically significant when the p value was <0.05 and highly significant when the p value was p <0.0001.
3. Results
3.1. Sampling Scope and Facility Comparison
Between 2020 and 2025, a total of 1081 water samples were collected at 5 high-risk facilities on Crete, namely public hospitals, private clinics, primary healthcare units, hotels and passenger ships (Table 1). Most samples were performed in public hospitals (40.70%, 440 samples), which comprise complex and significant infrastructures, with elevated risks for Legionella colonization and possibly outbreak sites, according to the literature[45,46]. On the contrary, the other two healthcare facilities – primary healthcare units (114 samples) and private clinics (112 samples) – contribute around 12 % each. Finally, the sampling of hotels and passenger ships comprised 22 %, 239 samples, and 17%, 176 of the datasets, respectively. All facility types were sufficiently covered with water samples that ensured a profound comparative analysis.
The 95% Wilson confidence intervals of the sampling for public hospitals (n=440) were limited between 37.81%–43.66%, which enhanced consistency. Nevertheless, the relative interval values of the private clinics and primary healthcare units were wider, with 8.68% to 12.32% and 8.85% to 12.52% respectively, indicating higher statistical uncertainty. On the other hand, intermediate confidence interval values are shown for the passenger ships and hotels, with 14.20%–18.60% and 19.74%–24.68%, respectively. The sampling strategy allowed for statistically valid comparisons between the facilities with the provision of equal representation across the different facility types. This approach resolves a well-known issue with environmental monitoring studies conducted in several places, where proportional representation needs to be handled while taking logistical and practical limitations into consideration [47].
Sampling strategy included 1,081 samples from several places of the internal water systems of each facility type, including municipal inlets, storage tanks, hot water heaters and boilers, taps that were close to and far away from the water source, and, if there were any, showers and recreational water systems like pools, saunas or jacuzzi (Table 2). Specifically, 600 (57.92%) samples came from direct outlets, and 436 (42.08%) came from indirect or distal plumbing locations. The Wilson 95% confidence intervals for these two groups were 54.88%–60.89% and 39.11%–45.12%, respectively. In terms of temperature division, 600 samples (55.50%) were from cold water systems and 481 samples (44.50%) were from hot water systems. This enabled a comprehension of the effect of temperature on Legionella colonization. In this area, the confidence interval values were lower (cold: 52.53%–58.44%; hot: 41.56%–47.47%). Also, spatial stratification was used based on how far the water had to travel from the point of entry. 66 samples (40.74%) were obtained from proximal (close) points and 96 samples (59.26%) from distal (far) points, which provided insights into the consequences of standstill and the potential for biofilm development. The wider confidence intervals seen in this group (proximal: 33.10%–48.73%; distal: 51.27%–66.90%) are due to the smaller sample sizes and the variability inherent in spatial sampling.
3.2. Legionella Positivity and Temporal Trends
Out of 1,081 samples from all five types of facilities, 482 (44.59%) tested positive for Legionella spp with concentration levels varying from 50 to more than 10,000 CFU/L. The positive results are listed in Table 3, divided into three groups according to: low concentration levels (<10³ CFU/L), medium (≥10³ to <10⁴ CFU/L), and high (≥10⁴ CFU/L). An enhanced positivity rate of samples was found for the primary healthcare units, with 85.96% testing positive and a large 20.17% placed into the high-risk category (≥10⁴ CFU/L). In contrast, public hospitals showed a lower overall positivity rate of 46.36%, with only 1.81% of samples exceeding the higher threshold. Private clinics had the lowest overall positivity rate at 21.42%. No samples had more than 10⁴ CFU/L, and only 6.25% of them were in the medium-risk group level. From these results, we can conclude that the smaller outpatient facilities have a lot of colonization issues, probably because their infrastructure is getting old, or they don't clean regularly, or/and they don't have formal water safety plans. The wider but less intense colonization pattern in public hospitals suggests a probable contribution of the centralized monitoring and institutional water management protocols. Whereas, in private clinics the results indicate a better water management, possibly due to newer infrastructure and plumbing systems that are easier to use and have fewer distal points. Next, samples from passenger ships showed a positivity rate of 36.93%, with 6.25% of them exceeding the 10⁴ CFU/L threshold. The large storage tanks, long periods of time when the water doesn't move (like during the off-season or when a ship is docked), and not enough space for thermal and residual disinfection control seems to influence and challenge the maritime water systems. Finally, hotels had a moderate positivity rate of 38.08%, and most of the positive samples were below the 10³ CFU/L threshold. Still, 10.04% were in the medium-risk range and 4.60% were over 10⁴ CFU/L. This shows that more regular preventive maintenance is needed, especially in seasonal businesses where water stagnation is a common problem. According to the European Drinking Water Directive (EU) 2020/2184, Legionella spp. concentrations equal to or surpassing 10³ CFU/L require immediate remedial actions [48]. Based on this standard, 178 samples (16.46%) from all types of facilities went over this legal limit. This shows how important it is to keep an eye on the environment and take pointed measures in places that are at high risk.
Figure 1 shows the positivity rate on the legal limit threshold of ≥10³ CFU/L as a function of the different facility types. The primary healthcare units showed an enhanced level of contamination with 36.83% of total samples above the threshold, while a very moderate positivity rate is showed for public hospitals, at 17.94%, and hotels, at 14.64%. Passenger ships and private clinics showed a much lower level of contamination at 8.52%, and a minimal positivity rate, at 6.25%. From these results, it becomes apparent that the primary healthcare facilities face a major difficulty controlling the growth of Legionella. This can be attributed to lack of WSP’s or regulations and limited chemical and physical (thermal) control over their water systems. On the other hand, settings provided with the implementation of frequent inspections and centralized management appear to regulate Legionella contamination.
In order to elucidate further the positivity rate for the surveillance of Legionella spp for a six-year period between 2020 and 2025 was studied. The temporal analysis shown in Figure 2 shows a profound variation in the positivity rates of Legionella over the predetermined period. The positivity rate in 2020 was found to be 14.75%, referring to a period prior to the onset of C0VID-19 pandemic. An abrupt increase was observed in 2021, with 58.82% positivity, followed by a sharp reduction in 2022 at 14.71%. These results indicate disorders with the operation of the facilities, such as extended periods of closures, limited water use, at the beginning of the pandemic (2021), which facilitated the proliferation of several microorganisms in stationary systems. This seemingly followed by an improvement in the reopening of the facilities with restrictions and interferences taking place on operating procedures. In the following years 2023 and 2024 the positivity rates decreased gradually to 11.76% and 15.15%, respectively, with the standardization of the operating regulations. Nevertheless, in 2025 an almost 4-fold increase in positivity rate at 57.53%, is observed which is comparable to the post-lockdown period. This temporal pattern underscores the vulnerability of engineered water systems to prolonged inactivity and highlights the critical importance of proactive monitoring and maintenance during periods of partial or full occupancy interruption.
Next, analysis of the sample types revealed a higher presence of Legionella species, in hot water systems rather than cold water systems. Table 4 summarizes the Legionella-positive samples by sample type and collection point. Overall, 252 samples tested positive out of 481 hot water samples in total, which is ascribed to 52.28%, whereas 230 samples tested positive in Legionella, at 47.42% among 600 cold water samples in total. For hot water samples, positivity rates found negligible difference between direct outlets and indirect outlets, 50.71% and 50%, respectively. Nevertheless, distal sampling points demonstrated lower positivity rate at 48% than the proximal sampling points at 34.37%, potentially reflecting thermal decay and sediment buildup at terminal points. For cold water samples, again a negligible difference between direct outlets and indirect outlets, while far away points showed a slight lower positivity rate of 23.80% than the close points at 28%.
3.3. Serogroup Distribution and Facility Colonization Risks
In order to determine the distribution of Legionella species and serogroups for all facilities, a total of 482 Legionella-positive samples were serotyped. As shown in Figure 3 and listed in Table 5, the majority of the isolates (65.35%) were serogroups 2–15 of L. pneumophila. Serogroup 1 of L. pneumophila, often associated with clinical diseases, accounted for 36.09% of the positive samples. Only 2.70% were associated with species other than pneumophila. Serogroup 3 (11.38%) was the dominant serogroup among the serogroups 2–15 of L. pneumophila. Next, serogroup 8 accounted for 7.49%, serogroup 6 covered 5.00%, serogroup 2 represented 1.57%, serogroup 7 represented 0.65%, serogroup 9 accounted for 0.37%, and serogroup 4 formed 0.19%. Public hospitals recorded the highest number of positive samples (204·42.32%), with the distribution of serogroups favoring sg2–15 (54.41%) over sg1 (46.56%). Out of 98 samples from primary care units (20.33%), sg2–15 was the predominant type, constituting 81.63%. This suggests that the strains are spreading in the environment and may exhibit reduced pathogenicity. Next, passenger ships (13.49%) and hotels (18.88%) exhibited similar serogroup patterns, mainly consisting of sg2–15. In contrast, private clinics represented only 4.98% of all positive samples, with 70.83% of these classified as sg2–15. Non-pneumophila species were not detected. L. pneumophila serogroup 1 was mainly found in public hospitals (95 isolates; 46.56% of positives in hospitals), followed by passenger ships (36.92%) and hotels (38.59%). This indicates the clinical significance of colonization in these areas.
3.4. Temporal evolution, Positivity Trends and Post-COVID Risk Profile
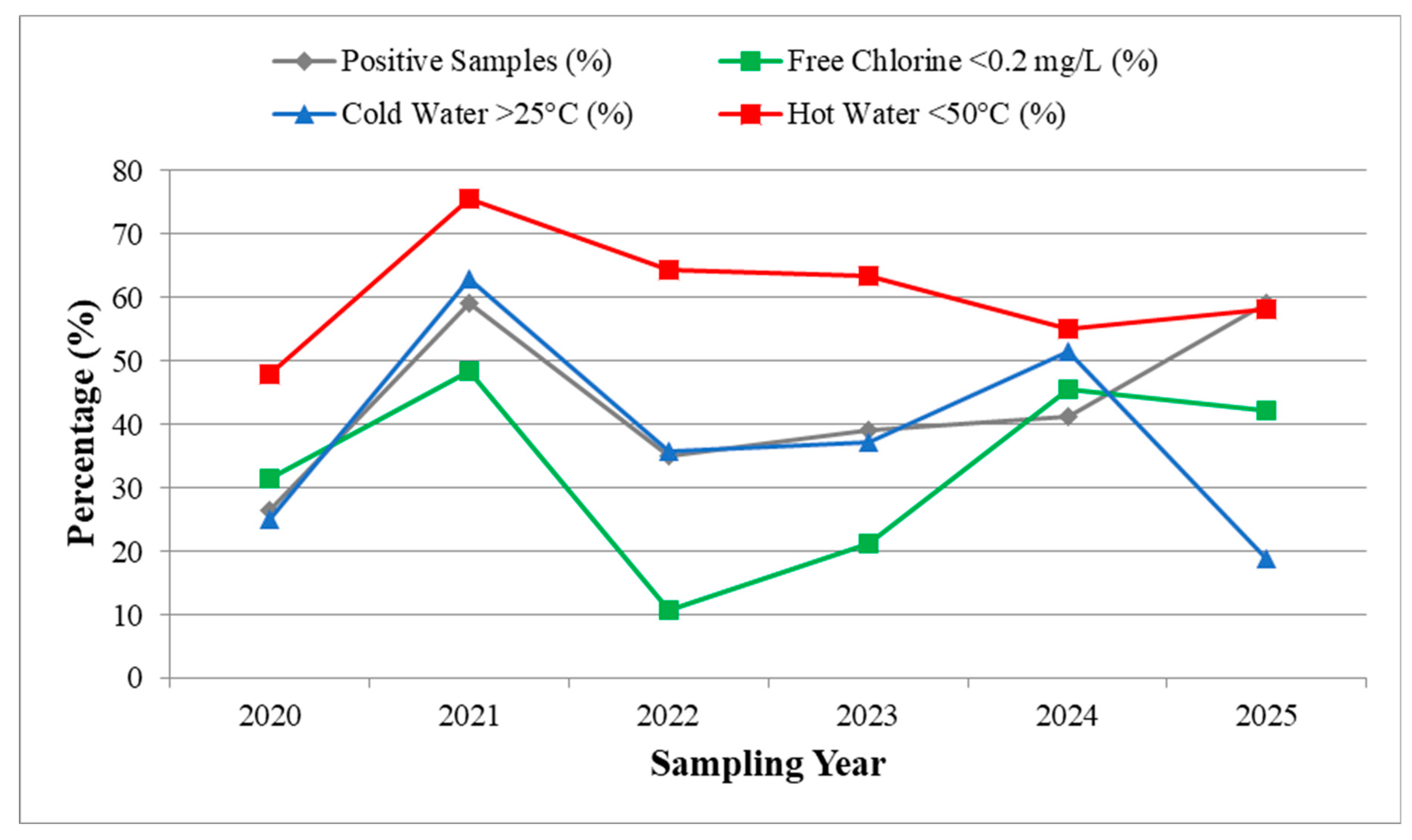
The temporal trend among Legionella positivity and the environmental non-compliances was determined from 2020 to 2025. The hot water non-compliance (<50 °C), low free chlorine levels (<0.2 mg/L), and cold water >25 °C, shown in Figure 3, peaks with highly increased positivity rates and especially in 2021 and 2025. In 2025, the decrease in thermal non-compliance along with the steady increase in positivity and chemical deviation, suggests that there are possible malfunctions in operating systems or maintenance processes. This supports the idea that the contamination risks stem from the combination of thermal and chemical instabilities, not just by one parameter.
Figure 3 shows declinations in the water quality and Legionella proliferation between 2020 and 2025. It is noted that 2020 is the initial pandemic year. A relatively low positivity rate, 26.42%, was observed in 2020. Nonetheless, the chlorine levels (<0.2 mg/L) was 31.58% of samples and extensive hot water temperatures below the 50 °C safety standard. These parameters indicate signs of inadequate compliance with standards, likely resulting from prolonged water stagnation, reduced facility operation during lockdowns, and omissions in maintenance and disinfection. In 2021, there is an extensive increase in Legionella positivity with its value rising to 59.17%. This rise coincides with a significant increase in water quality violations since chlorination and temperature parameters showed chlorine insufficiency (<0.2 mg/L) and temperature noncompliance in hot 75.53% and cold 63.04% samples respectively. For this reason, extensive bacterial amplification was presented.
On the other hand, in 2022 and 2023 positivity rates exhibited a modest level compared to the 2021 year, with values dropped to 34.97% and 39.22%, respectively. The samples obtained in these years showed better chlorine levels compliance, mainly due to strict regulations during COVID-19. Nevertheless, in 2024, non-compliances and violations re-emerged, with 45.56% of samples not meeting the chlorine criteria and 51.48% of cold-water samples exceeding 25°C. In 2025, there was a significant improvement with only 18.75% of samples above the limit, however the remaining parameters remained suboptimal, with the overall positivity increasing again to 59.23%. It is evident that the irregular and incomplete recovery of water systems in the post-pandemic era, where persistent challenges in maintaining thermal and chemical balance continue to compromise microbial safety.
Figure 4.
Temporal comparison of Legionella positivity and physicochemical non-compliance (2020–2025). Yearly percentages of positive samples (grey), free chlorine levels <0.2 mg/L (green), cold water >25 °C (blue), and hot water <50 °C (red) across all facilities.
Figure 4.
Temporal comparison of Legionella positivity and physicochemical non-compliance (2020–2025). Yearly percentages of positive samples (grey), free chlorine levels <0.2 mg/L (green), cold water >25 °C (blue), and hot water <50 °C (red) across all facilities.
3.4.1. Hotels: Post-COVID Risk Profile
A focused analysis of hotel establishments (n = 9) from 2020 to 2025 and their comparison with the pre-pandemic era demonstrates the impact of the pandemic on water system hygiene. Table S1 lists the rates of Legionella positivity in hotels for the period 2020-2025. In 2020, Legionella positivity in hotels was at a level of 26.42%, slightly lower than the national average of positivity in hotels for the period 2000-2019 of 38.08% reported in our previous study [22]. However, a rapid increase in positivity was observed during and after the COVID-19 pandemic, reaching 59.17% in 2021 and again 59.23% in 2025, values that far exceed both the 2020 baseline and the national average of positivity in hotels for the period 2000-2019. It is noted that the 2021 peak coincided with the widespread reopening of facilities after a prolonged period of inactivity. Partial improvement was noted in 2022 and 2023 with positivity falling to 34.97% and 39.22% respectively, but levels increased again in 2024 with values of 41.19% reaching a second peak in 2025.
Table S2 lists the environmental risk factors monitored alongside positivity. In 2021, 48.45% of hotel samples with Legionella detections had free chlorine levels below 0.2mg/L. 75.53% of hot water samples were below 50°C. and 63.04% of cold water samples exceeded 25°C. These non-compliances align with periods of higher colonization and correspond to a more than two-fold increased risk for positivity (Table 6, Figure 5). Thermal and chemical instability remained problematic throughout 2025, while there were compliances for cold water (18.75% >25°C).
A comparative analysis of concentration zones (Table S1) also showed a shift from high risk (>10⁴ CFU/L) to more persistent low and medium risk colonization in the post-COVID years, likely reflecting partial mitigation through disinfection. However, this pattern suggests that hotel systems continue to harbor viable Legionella reservoirs despite improved operational surveillance, especially in accommodations associated with TALD and reinforce the importance of robust, proactive maintenance strategies before and after closure periods [49].
3.5. Environmental Risk Factors and Relative Risk Analysis
Environmental and operational risk factors are then presented in Figure 5 and detailed in Table 6. Hot water temperature below 50°C emerged as the most critical with a relative risk (RR) of 2.05 and odds ratio (OR) of 6.54 for Legionella positivity (p < 0.0001). Also striking was the effect of hot water below 35°C, which showed a RR of 3.58 and an OR of 4.74, reflecting a significantly increased colonization potential in hypothermophilic conditions. Free residual chlorine concentrations below 0.2 mg/L were also significantly associated with colonization (RR = 2.22, p < 0.0001), demonstrating the importance of continuous chemical disinfection (Table 6).
A weak but statistically significant association (RR = 2.53, p = 0.04) was found with increased turbidity levels, which is likely due to the support provided by sediment and biofilm for microbial growth (Table 6, Figure 5). As expected, no significant association was found between Legionella positivity and cold water temperatures above 25 °C (RR = 1.12, p = 0.1), sampling locations in remote areas (RR = 1.11, p = 0.22) or direct water outlets (RR = 0.96, p = 0.29). These findings reinforce the principle that thermal and chemical parameters have the main role in the risk of colonization compared to spatial factors.
Statistical analysis can highlight which parameter plays critical in Legionella proliferation. Figure 5 then shows the relative risk (RR) of Legionella positivity in relation to three important physicochemical factors of non-compliance: cold water temperature >25°C, free residual chlorine <0.2mg/L and hot water temperature <50°C. An RR greater than 1 means that the specified condition makes contamination more likely. The strongest association is seen with non-compliance with the hot water rules (RR > 2), which is due to low chlorine levels. Weak - non-significant association is shown for high values of non-compliance for cold water temperatures
Linear regression supported these results showing a strong association between non-compliance with hot water regulations and Legionella detection (β = 3578.0, p < 0.0001), with a moderate explanatory power (r² = 0.07). There was a weak association between lack of free chlorine (β = 366.5, p = 0.0897) and cold water temperature that had no statistically significant predictive value (β = 245.4, p = 0.2056). Spearman's rank correlation supported these patterns by showing a strong unidirectional association between Legionella detection and non-compliance with hot water regulations (ρ = 0.42, p < 0.0001).
Systemic vulnerabilities can be identified by the correlation of physicochemical parameters with non-compliances by facility type (Table S3). 61.06% of all samples was found to be non-compliant for hot water temperatures (<50 °C). Passenger ships and private clincs showed the highest rate with 92.31% and 65.78%, respectively. In advance, passenger ships found to present low residual chlorine (<0.2 mg/L) with 63.33% and primary healthcare units 42.19%. 36.34% of all samples displayed low residual chlorine (<0.2 mg/L), while non-conformities on cold water temperature violations (>25 °C) were found in 44.14% of cases, mostly 59.55% of cases attributed to hotel samples. Finally, pH values were observed with no deviations, implying that chemical buffering systems remained within acceptable ranges across all facilities.
Table S2 presents the temporal trends in the prevalence of risk factors among Legionella-positive samples. In 2021 and 2025, years characterized by increased positivity, there were simultaneous peaks of non-compliance with thermal and chlorinated requirements. Linear regression confirmed the predictive power of suboptimal hot water temperatures for colonization (β = 3578.0, p < 0.0001; r² = 0.07), while chlorine deficiency showed a weaker association (β = 366.5, p = 0.0897). Cold water temperature did not show significant predictive value (p = 0.2056).
Finally, the risk assessment of positive samples based on CFU/L specifications (Figure 6) showed that high-risk samples (≥10⁴ CFU/L) made up a larger percentage of samples in primary care units (20.17%) and on passenger ships (6.25%). Private clinics didn't have any high-concentration samples, whereas public hospitals and hotels had a lot less (1.81% and 0.57%, respectively). This distribution shows both variances in how things work and possible holes in the preventative maintenance measures.
4. Discussion
This study is a 6-year large-scale study analyzing the presence of Legionella spp. colonies in water distribution systems from 5 different high-risk facilities in Crete, Greece. This longitudinal study covers the period before, during and after the COVID-19 pandemic, analyzing its footprint in water distribution systems. The five types of facilities studied concern triage points from public hospitals, private clinics, primary healthcare units, hotels and passenger ships. Analysis of the data revealed differences in the extent and burden of Legionella, their serogroup, as well as in environmental risk factors. These results clarify the need to implement strategies for the safety of human water consumption per facility as well as a method of targeted environmental surveillance [50].
In this study, an overall positivity rate of 44.59% for all Legionella species colonizing the water supply systems of the facilities is revealed. This is in agreement with corresponding surveillance studies across Europe. However, our analysis shows that there is a different risk profile per facility. The highest positivity rate of 85.96% is presented in primary healthcare units with a parallel presence of a high percentage of samples ≥10⁴ CFU/L at 20.17%. One would expect that hospitals, due to their complexity, would present higher levels of Legionella colonization, compared to small primary healthcare units. This fact can be attributed to insufficient resources of these small units for maintenance or the failure to implement automated disinfection systems or water safety plans. In similar findings, Whiley et al. previously showed that decentralized healthcare settings are more prawned in Legionella contamination [51].
Interestingly, public hospitals showed a positivity rate at lower levels of 46.36%, although significant. In these facilities, the positive fact is that only 1.81% of the samples exceeded 10⁴ CFU/L. However, the presence of widespread levels of serogroup 1 of L. pneumophila with 46.56% of the positive samples rings alarm bells, as serogroup 1 has been recognized for its virulence and its involvement in epidemics of hospital infections. These results are consistent with the study by Buse et al., which examined large water tanks in large plumbing systems where persistent Legionella colonization occurred in healthcare settings [48]. Based on these, it is critical that public health professionals focus on developing new applications/technologies with the goal of monitoring Legionella colonization and providing early warning of elevated levels of contamination, as well as monitoring and evaluating control and maintenance strategies. By using systems that do not compromise water quality, informed regulatory frameworks can be derived and intervention in hospital and non-hospital settings can be guided. Public health authorities should promote the adoption of such innovations—with the aim of saving energy, maintaining water infrastructure, and ensuring the hygiene and integrity of the water supply [52,53,54].
A different risk situation emerged for passenger ships, likely attributable to complex hydraulic systems, the existence of water storage tanks for long periods of inactivity, when ships are berthed in the off-season, or travel restrictions related to the pandemic. On passenger ships, their overall positivity was 36.93% but showed a high concentration of samples ≥10⁴ CFU/L at 6.25% and the highest frequency of non-compliance with hot water temperature at 92.31%. Previous studies by Leoni et al., highlighted the high risk of Legionella colonization on ships due to the lack of ample space for some redesign of systems and the difficulty in maintaining a continuous water flow [55] . This poses a unique challenge for microbial control on passenger ships, therefore coordination between central and local authorities is essential to ensure preparedness and develop targeted risk assessments and contingency plans and to inform national strategies for water safety in maritime infrastructure [56].
Comparable to passenger ships, the positivity in hotels did not exceed the moderate rate of 38.08%. A notable difference was in the non-compliance with the high cold water temperature which was found at 59.55%. A significant percentage of samples at 13.29% presented a medium load rate (within 10³–10⁴ CFU/L) with a small presence above 10⁴ CFU/L, which predisposes to low-level colonization.
The positivity rates from hotels, where visitors were reported as a TALD case in ELDSNet, (n=13) and the visitor’s room was known (n=6), was found to be 55% over total 40 samples [57]. Specifically, these samples were serotyped and found: 90.90% attributed to L. pneumophila serogroup 2–15 (L. pneumophila serogroup 2 at 22.73%, L. pneumophila serogroup 3 at 13.63%, L. pneumophila serogroup 6 at 22.73% and L. pneumophila serogroup 8 at 4.55%), while 9.09% was found for L. pneumophila serogroup 1. The high contamination rate demonstrates the need for the implementation of strict restrictive measures as a prevention in the tourism and hospitality sectors. Legionella is known to thrive and persist in accommodation facilities such as guest rooms, bungalows, hotel units or campsites and is often associated with outbreaks of TALD. The risk in these areas is attributed to complex plumbing infrastructure, intermittent water use and features such as saunas and hot tubs [58].
Further analysis in hotel units revealed fluctuations in Legionella infection risk over time between 2020 and 2025 (Figure 3, Supplementary Table S2). Positivity rates experienced two peaks, one in 2021 at 59.17% and the second in 2025 at 59.23%, with exceedances well above the baseline level in hotel facilities, before the pandemic [22]. These peaks are related to microbial amplification, during the stagnation on periods of inactivity and reopening of these buildings. Moreover, through the analysis of risk factors, the presence of non-compliances in key physicochemical factors was confirmed, since in 2021 it was shown that over 75% of hot water samples did not comply with the requirements (<50°C) with 48.45% of the samples also failing in chlorine requirements (<0.2mg/L). The comparative distribution of positive samples by CFU/L category (Supplementary Table S1) showed that over time in the post-pandemic era until 2025, the samples tend to show medium and low-level Legionella colonization. However, this persistence even at low levels requires attention and the need for regular monitoring and prevention applications in hotel facilities.
In contrast to the phenomena of increased positivity rate and non-compliance observed in the remaining health and non-health facilities that we mentioned, private clinics presented the lowest rates in all parameters. It is noted that for the entire reporting period, the analysis included zero high-load samples. The image reflected for private clinics is that they have an advantage due to newer infrastructure and plumbing networks, but they also operate under strict accreditation standards with high compliance with cleaning and disinfection protocols. Nevertheless, there is a possibility of colonization even in low-risk environments, as shown by the presence of serogroups 2-15 of L. pneumophila in a percentage of 70.83% of positive samples.
Seroepidemiology in all facilities revealed the predominant presence of serogroups 2-15 of L. pneumophila with 63.83% of the positive samples. This is fully in line with the rules of environmental surveillance, where it is common to find the presence of serogroups 2-15 in environmental isolates, compared to sg1 which appears less frequently and mainly in clinical cases. However, in the present study a high prevalence of sg1 was observed in public hospitals, hotels and passenger ships, which reinforces the requirement for the use of seroepidemiological study and the necessity of regular serogroup typing during environmental surveillance. Our findings are in line with those of Vincenti et al., who reported similar serogroup distributions in southern Italy. In their study, the role of sg2-15 in colonization and the clinical significance of sg1 were emphasized [19].
The study of physicochemical parameters identified suboptimal hot water temperature (<50°C) and low free residual chlorine (<0.2mg/L) as statistically significant risk factors. The relative risk of colonization was more than doubled (RR = 2.05) in association with hot water systems maintained below 50°C, while even higher values (RR = 3.58) were observed when temperatures fell below 35°C. According to the WHO and the CDC, thermal control is a cornerstone of Legionella prevention and is confirmed by the findings of this study [59,60]. Subsequently, the risk of positivity was shown to be twice as high with RR values = 2.22 in association with chlorine levels below 0.2mg/L, which is indicative of inadequate chlorination and demonstrates the importance of maintaining continuous biocide residues in complex water supply systems [61,62].
In contrast, the analysis of physicochemical parameters, in all samples, shows that cold water temperatures >25°C, remote sampling locations and direct versus indirect exits were not statistically significant factors for the prediction of colonization. In conclusion, thermal and chemical control remain the most reliable risk predictors of the types of facilities studied with the remaining factors perhaps playing a critical role under certain system configurations, as reported in other studies [63].
During the COVID-19 pandemic, hotels have been experiencing the effects of prolonged closures, which may be associated with an increased risk of Legionella infections. In particular, prolonged closures result in stagnant water and disrupted maintenance routines, providing a breeding ground for pathogens such as Legionella, among others. However, to our knowledge, there are few representative field studies comparing pre-pandemic colonization levels in buildings with those observed under lockdown conditions [49]. This lack of baseline data complicates retrospective assessments but highlights the importance of continuous surveillance during system inactivity[50].
Temporal trend studies provided interesting information on the impact of operational disruptions on water safety. In 2021, which is the year after the first lockdown related to the COVID-19 pandemic, the highest positivity rate was recorded. According to international studies, water stagnation, maintenance suspension and generally reduced use of facilities in the reference facilities contributed to a trend of proliferation of all microbes including those of Legionella spp. [64,65]. A secondary peak in 2025 suggests that temporary improvements implemented during the pandemic may have waned over time, underscoring the need for institutionalized, not reactive, water safety protocols.
By comparing multiple parameters (Figure 3), which monitor the occurrence of Legionella positivity with key indicators of environmental non-compliance during the period 2020-2025, the coincidence of the highest positivity rates in 2021 and 2025 is highlighted, with peaks at hot water temperatures <50°C, free chlorine residuals <0.2mg/L and cold water >25°C. It is worth noting that the sharp decrease in thermal non-compliance in 2025 - despite the increased positivity - suggests a synergistic role of thermal and chemical instability in increasing the risk of colonization.
Regression analyses confirmed that the strongest independent predictor of colonization, with a statistically significant correlation with values of β = 3578.0, p < 0.0001, was non-compliance with hot water temperature. In contrast, the weak correlation of chlorine residuals highlights the limitations of chemical disinfection alone when not combined with strict temperature control.
In summary, this study highlights the need to develop and implement risk management strategies, differentiated and adapted to each facility. There is a requirement for targeted surveillance in both public hospitals and primary care settings, taking into account vulnerable patient populations. Seasonal risk assessments and planning of a water safety plan on board are a priority for passenger ships. Hotel operators should emphasize thermal controls even during off-season periods with low occupancy and ensure continuity in water use. Finally, in private clinics, the appearance of low risk may be a positive sign, but should not be overlooked as minimal colonization can present serious risks for immunocompromised patients and vulnerable groups.
This study was conducted in an analysis based on a large sample size, a longitudinal design and a typological diversity. The geographical restriction to a single island region as well as the plate counting method for Legionella detection constitute limitations of the study. Future studies should incorporate molecular diagnostics, such as qPCR and sequence-based typing (SBT), to enhance detection sensitivity and monitor strain evolution.
5. Conclusions
The present study constitutes a six-year environmental monitoring of Legionella species for five types of high-risk facilities in the region of Crete, namely public hospitals, private clinics, primary care units, hotels and passenger ships. The results show that infection rates, bacterial loads and environmental risk factors vary significantly, per facility. This highlights the complexity of water system design, operational practices, and public health outcomes.
The data studied highlighted primary health care units as the most vulnerable facilities, showing Legionella positivity rates above 85% with extensive high load samples ≥10⁴ CFU/L. These findings indicate systemic deficiencies in water safety monitoring, thermal regulation and disinfection practices, particularly in smaller outpatient clinics. Extensive colonization was also observed in samples obtained from public hospitals, with high rates of L. pneumophila serogroup 1, a strain known to be associated with frequent clinical illnesses. A comparable colonization risk was found on passenger ships, especially on ships that have been inactivated for prolonged time. This comprise an important finding as passenger ships have traditionally not been included in water safety frameworks, which highlights the need for implementation of maritime-specific protocols.
Moderate positivity rates were observed in the hotels studied, however, moderate contamination was maintained in the cold water systems, possibly due to seasonal occupancy and inconsistent flushing. Notably, persistence of colonization was observed in hotels associated with TALD, and surveillance showed that post-pandemic positivity is comparable to pre-pandemic TALD findings. It is noteworthy that severe colonization events can extend to non-healthcare facilities.
Private clinics were the least affected, with no samples exceeding the regulatory threshold of 10⁴ CFU/L. However, the detection of L. pneumophila serogroups 2–15 in these settings suggests that colonization remains possible even in well-maintained infrastructure.
Study on environmental parameters revealed that the strongest independent risk factor for Legionella proliferation is hot water temperatures below 50°C, which is in line with all guidelines of the European Study Group for Legionella Infections (ESGLI) and is consistent with a threefold increase in risk under hypothermophilic conditions. A significant correlation was observed at free chlorine levels below 0.2mg/L, confirming the role of prolonged disinfection in microbial control. Temporal analysis revealed that peaks in positivity were closely associated with pandemic-related building closures and maintenance outages [66].
Legionella colonization in hotel water systems has been shown to increase during the COVID-19 pandemic and has remained elevated post-COVID. These findings reinforce low residual chlorine concentrations and suboptimal water temperatures as identified environmental risk factors contributing to the proliferation of pathogens. Given the recurrent detection of Legionella in hotel facilities, regular environmental monitoring should be considered as a preventive measure. Especially in cases related to TALD, the guest room, the microbiological quality of the water in it, and the surrounding areas such as garden irrigation systems, showers, fountains, etc. should be thoroughly searched and checked.
The water distribution systems of all facilities studied belong - according to the European legislation, Directive (EU) 2020/2184 of the European Parliament and of the Council of 16 December 2020 on the quality of water intended for human consumption (recast) - to the category of priority premises [67]. To conclude, facilities should apply individualized risk assessment approaches and one such is the implementation of integrated WSPs. WSPs should emphasize regular monitoring, automated thermal control and remedial disinfection protocols.
Moving forward, national and regional public health agencies should integrate Legionella risk management into broader water safety and civil protection policies. Investments in infrastructure modernization—particularly in primary healthcare and maritime transport—alongside regulatory enforcement and workforce training, will be essential to reducing colonization risk and preventing outbreaks.
Future research should incorporate molecular diagnostics, strain typing, and digital monitoring tools to improve detection sensitivity and enable early warning systems. Enhancing the resilience of engineered water systems against Legionella and other microbial threats will depend on the integration of microbiological surveillance, engineering design, and adaptive governance.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Comparative Distribution of Legionella-Positive Samples by CFU/L Concentration Band.; Table S2: Year-by-Year Legionella Positivity and Water Quality Indicators in Hotel Water Systems (2020–2025) and Table S3: Frequency and percentage of non-compliance with physicochemical parameters by facility type and year of monitoring (2020–2025).
Author Contributions
For conceptualization, methodology, and validation A.P. (Antonios Papadakis), E.K., D.C. and P. A. (Psaroulaki Anna) are responsible; formal analysis, investigation, and data curation, was conducted by A.P., E.K., E.A.C., D.C. and P.A.; writing—original draft preparation, A.P. and E.K..; writing—review and editing, A.P. and P. A.; supervision, and project administration A..P, D.C. and P. A.. All authors have read and agreed to the published version of the manuscript.Funding: This research received no external funding.
Data Availability Statement
Not applicable.
Acknowledgments
We would like to thank all the environmental health inspectors of the Local Public Health Authorities of Crete Island who collected the environmental samples during all these years.
Conflicts of Interest
The authors have declared no conflict of interest.
References
- Renwick, D.V.; Heinrich, A.; Weisman, R.; Arvanaghi, H.; Rotert, K. Potential Public Health Impacts of Deteriorating Distribution System Infrastructure. J Am Water Works Assoc 2019, 111, 42–53. [Google Scholar] [CrossRef] [PubMed]
- Public Water Supply Distribution Systems Assessing and Reducing Risks | National Academies Available online:. Available online: https://www.nationalacademies.org/our-work/public-water-supply-distribution-systems-assessing-and-reducing-risks (accessed on 6 June 2025).
- Public Water Supply Distribution Systems: Assessing and Reducing Risks -- First Report; National Academies Press: Washington, D.C., 2005. ISBN 978-0-309-09628-7.
- LeChevallier, M.W.; Prosser, T.; Stevens, M. Opportunistic Pathogens in Drinking Water Distribution Systems—A Review. Microorganisms 2024, 12, 916. [Google Scholar] [CrossRef] [PubMed]
- Brady, M.F.; Awosika, A.O.; Nguyen, A.D.; Sundareshan, V. Legionnaires Disease. In StatPearls; StatPearls Publishing: Treasure Island (FL), 2025. [Google Scholar]
- Rello, J.; Allam, C.; Ruiz-Spinelli, A.; Jarraud, S. Severe Legionnaires’ Disease. Annals of Intensive Care 2024, 14, 51. [Google Scholar] [CrossRef]
- Papageorgiou, K.; Chronis, E.; Tzouanopoulos, A.; Steris, V.; Koutsopoulos, D.; Tzavaras, I.; Paraskevopoulos, K.; Karolidis, S. Prevalence of Legionella Spp. in the Water Distribution Systems of Northern Greece. EUR J ENV PUBLIC HLT 2023, 7, em0147. [Google Scholar] [CrossRef]
- Papadakis, A.; Chochlakis, D.; Sandalakis, V.; Keramarou, M.; Tselentis, Y.; Psaroulaki, A. Legionella Spp. Risk Assessment in Recreational and Garden Areas of Hotels. International Journal of Environmental Research and Public Health 2018, 15, 598. [Google Scholar] [CrossRef]
- Mnisi, Z.F.; Delair, Z.; Singh, A. Legionella in Urban and Rural Water, a Tale of Two Environments. Water 2025, 17, 1491. [Google Scholar] [CrossRef]
- Legionnaires’ Disease - Annual Epidemiological Report for 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/legionnaires-disease-annual-epidemiological-report-2021 (accessed on 5 June 2025).
- Legionnaires’ Disease - Annual Epidemiological Report for 2021. Available online: https://www.ecdc.europa.eu/en/publications-data/legionnaires-disease-annual-epidemiological-report-2021 (accessed on 3 June 2025).
- Hoge, C.W.; Breiman, R.F. Advances in the Epidemiology and Control of Legionella Infections. Epidemiologic Reviews 1991, 13, 329–340. [Google Scholar] [CrossRef]
- van Hoof, J.; Hornstra, L.M.; van der Blom, E.; Nuijten, O.W.; van der Wielen, P.W. The Presence and Growth of Legionella Species in Thermostatic Shower Mixer Taps: An Exploratory Field Study. Building Services Engineering Research & Technology 2014, 35, 600–612. [Google Scholar] [CrossRef]
- Laganà, P.; Gioffrè, M.E.; Delia, S.A.; Facciolà, A. Legionella Spp. in Thermal Facilities: A Public Health Issue in the One Health Vision. Water 2023, 15, 689. [Google Scholar] [CrossRef]
- Kyritsi, M.A.; Mouchtouri, V.A.; Katsioulis, A.; Kostara, E.; Nakoulas, V.; Hatzinikou, M.; Hadjichristodoulou, C. Legionella Colonization of Hotel Water Systems in Touristic Places of Greece: Association with System Characteristics and Physicochemical Parameters. International Journal of Environmental Research and Public Health 2018, 15, 2707. [Google Scholar] [CrossRef]
- Taylor, M.; Ross, K.; Bentham, R. Legionella, Protozoa, and Biofilms: Interactions within Complex Microbial Systems. Microb Ecol 2009, 58, 538–547. [Google Scholar] [CrossRef] [PubMed]
- Lau, H. y.; Ashbolt, N. j. The Role of Biofilms and Protozoa in Legionella Pathogenesis: Implications for Drinking Water. Journal of Applied Microbiology 2009, 107, 368–378. [Google Scholar] [CrossRef] [PubMed]
- Valster, R.M.; Wullings, B.A.; van der Kooij, D. Detection of Protozoan Hosts for Legionella Pneumophila in Engineered Water Systems by Using a Biofilm Batch Test. Appl Environ Microbiol 2010, 76, 7144–7153. [Google Scholar] [CrossRef]
- Vincenti, S.; Nurchis, M.C.; Boninti, F.; Sapienza, M.; Raponi, M.; Pattavina, F.; Pesaro, C.; D’Alonzo, C.; Damiani, G.; Laurenti, P. An Innovative Device for the Hot Water Circuit in Hospitals to Save Energy Without Compromising the Safety and Quality of Water: Preliminary Results. Water 2025, 17, 692. [Google Scholar] [CrossRef]
- Alexandropoulou, I.G.; Ntougias, S.; Konstantinidis, T.G.; Parasidis, T.A.; Panopoulou, M.; Constantinidis, T.C. Environmental Surveillance and Molecular Epidemiology of Waterborne Pathogen Legionella Pneumophila in Health-Care Facilities of Northeastern Greece: A 4-Year Survey. Environ Sci Pollut Res 2015, 22, 7628–7640. [Google Scholar] [CrossRef]
- Naher, N.; Bari, M.L.; Ahmed, S. Risk Assessment and Detection of Legionella Species in the Water System of A Luxury Hotel in Dhaka City, Bangladesh. Bangladesh Journal of Microbiology 2023, 40, 33–39. [Google Scholar] [CrossRef]
- Papadakis, A.; Keramarou, M.; Chochlakis, D.; Sandalakis, V.; Mouchtouri, V.A.; Psaroulaki, A. Legionella Spp. Colonization in Water Systems of Hotels Linked with Travel-Associated Legionnaires’ Disease. Water 2021, 13, 2243. [Google Scholar] [CrossRef]
- Mellou, K.; Mplougoura, A.; Mandilara, G.; Papadakis, A.; Chochlakis, D.; Psaroulaki, A.; Mavridou, A. Swimming Pool Regulations in the COVID-19 Era: Assessing Acceptability and Compliance in Greek Hotels in Two Consecutive Summer Touristic Periods. Water 2022, 14, 796. [Google Scholar] [CrossRef]
- Papadakis, A.A.; Tsirigotakis, I.; Katranitsa, S.; Donousis, C.; Papalexis, P.; Keramydas, D.; Chaidoutis, E.; Georgakopoulou, V.E.; Spandidos, D.A.; Constantinidis, T.C. Assessing the Impact of the COVID-19 Pandemic Health Protocols on the Hygiene Status of Swimming Pools of Hotel Units. Medicine International 2023, 3, 1–10. [Google Scholar] [CrossRef]
- Arrigo, I.; Galia, E.; Fasciana, T.; Diquattro, O.; Tricoli, M.R.; Serra, N.; Palermo, M.; Giammanco, A. Four-Year Environmental Surveillance Program of Legionella Spp. in One of Palermo’s Largest Hospitals. Microorganisms 2022, 10. [Google Scholar] [CrossRef]
- Goutziana, G.; Mouchtouri, V.A.; Karanika, M.; Kavagias, A.; Stathakis, N.E.; Gourgoulianis, K.; Kremastinou, J.; Hadjichristodoulou, C. Legionella Species Colonization of Water Distribution Systems, Pools and Air Conditioning Systems in Cruise Ships and Ferries. BMC Public Health 2008, 8, 390. [Google Scholar] [CrossRef] [PubMed]
- Kourentis, L.; Anagnostopoulos, L.; Tsinaris, Z.; Galanopoulos, A.P.; Van Reusel, D.; Van den Bogaert, R.; Helewaut, B.; Steenhout, I.; Helewaut, H.; Damman, D.; et al. Legionella Spp. Colonization on Non-Passenger Ships Calling at Belgian Ports. Medical Sciences Forum 2022, 13, 15. [Google Scholar] [CrossRef]
- Proctor, C.R.; Rhoads, W.J.; Keane, T.; Salehi, M.; Hamilton, K.; Pieper, K.J.; Cwiertny, D.M.; Prévost, M.; Whelton, A.J. Considerations for Large Building Water Quality after Extended Stagnation. AWWA Water Sci 2020, 2, e1186. [Google Scholar] [CrossRef] [PubMed]
- Papadakis, A.; Chochlakis, D.; Koufakis, E.; Carayanni, V.; Psaroulaki, A. Recreational Water Safety in Hotels: Lessons from the COVID-19 Pandemic and the Way Forward for a Safe Aquatic Environment. Tourism and Hospitality 2024, 5, 1167–1181. [Google Scholar] [CrossRef]
- Rhoads, W.J.; Hammes, F. Growth of Legionella during COVID-19 Lockdown Stagnation. Environ. Sci.: Water Res. Technol. 2021, 7, 10–15. [Google Scholar] [CrossRef]
- Kunz, J.M.; Hannapel, E.; Vander Kelen, P.; Hils, J.; Hoover, E.R.; Edens, C. Effects of the COVID-19 Pandemic on Legionella Water Management Program Performance across a United States Lodging Organization. International Journal of Environmental Research and Public Health 2023, 20, 6885. [Google Scholar] [CrossRef]
- Water Safety Plan Manual: Step-by-Step Risk Management for Drinking-Water Suppliers, Second Edition. Available online: https://www.who.int/publications/i/item/9789240067691 (accessed on 6 June 2025).
- Water Safety Planning: A Roadmap to Supporting Resources. Available online: https://www.who.int/publications/m/item/water-safety-planning-a-roadmap-to-supporting-resources (accessed on 6 June 2025).
- Borella, P.; Bargellini, A.; Marchegiano, P.; Vecchi, E.; Marchesi, I. Hospital-Acquired Legionella Infections: An Update on the Procedures for Controlling Environmental Contamination. Ann Ig 2016, 28, 98–108. [Google Scholar] [CrossRef]
- Mentula, S.; Kääriäinen, S.; Jaakola, S.; Niittynen, M.; Airaksinen, P.; Koivula, I.; Lehtola, M.; Mauranen, E.; Mononen, I.; Savolainen, R.; et al. Tap Water as the Source of a Legionnaires’ Disease Outbreak Spread to Several Residential Buildings and One Hospital, Finland, 2020 to 2021. Euro Surveill 2023, 28, 2200673. [Google Scholar] [CrossRef] [PubMed]
- Donohue, M.J.; O’Connell, K.; Vesper, S.J.; Mistry, J.H.; King, D.; Kostich, M.; Pfaller, S. Widespread Molecular Detection of Legionella Pneumophila Serogroup 1 in Cold Water Taps across the United States. Environ. Sci. Technol. 2014, 48, 3145–3152. [Google Scholar] [CrossRef]
- Marchesi, I.; Ferranti, G.; Mansi, A.; Marcelloni, A.M.; Proietto, A.R.; Saini, N.; Borella, P.; Bargellini, A. Control of Legionella Contamination and Risk of Corrosion in Hospital Water Networks Following Various Disinfection Procedures. Appl Environ Microbiol 2016, 82, 2959–2965. [Google Scholar] [CrossRef]
- European Technical Guidelines for the Prevention, Control and Investigation of Infections Caused by Legionella Species. Available online: https://www.ecdc.europa.eu/en/publications-data/european-technical-guidelines-prevention-control-and-investigation-infections (accessed on 6 June 2025).
- ISO 5667-1:2020. Available online: https://www.iso.org/standard/72369.html (accessed on 6 June 2025).
- ISO 5667-1:2023. Available online: https://www.iso.org/standard/84099.html (accessed on 6 June 2025).
- ISO 11731:2017. Available online: https://www.iso.org/standard/61782.html (accessed on 6 June 2025).
- Schoonjans, F. MedCalc’s Relative Risk Calculator. Available online: https://www.medcalc.org/calc/relative_risk.php (accessed on 9 June 2025).
- IBM SPSS Statistics. Available online: https://www.ibm.com/products/spss-statistics?lot=5&mhsrc=ibmsearch_a&mhq=spss (accessed on 9 June 2025).
- Epi InfoTM | CDC. Available online: https://www.cdc.gov/epiinfo/index.html (accessed on 9 June 2025).
- Buse, H.Y.; Schoen, M.E.; Ashbolt, N.J. Legionellae in Engineered Systems and Use of Quantitative Microbial Risk Assessment to Predict Exposure. Water Res 2012, 46, 921–933. [Google Scholar] [CrossRef] [PubMed]
- Legionella Diversity and Spatiotemporal Variation in the Occurrence of Opportunistic Pathogens within a Large Building Water System. Available online: https://www.mdpi.com/2076-0817/9/7/567 (accessed on 5 June 2025).
- Hamilton, K.A.; Hamilton, M.T.; Johnson, W.; Jjemba, P.; Bukhari, Z.; LeChevallier, M.; Haas, C.N. Health Risks from Exposure to Legionella in Reclaimed Water Aerosols: Toilet Flushing, Spray Irrigation, and Cooling Towers. Water Research 2018, 134, 261–279. [Google Scholar] [CrossRef] [PubMed]
- Directive - 2020/2184 - EN - EUR-Lex. Available online: https://eur-lex.europa.eu/eli/dir/2020/2184/oj/eng (accessed on 5 June 2025).
- Molina, J.J.; Bennassar, M.; Palacio, E.; Crespi, S. Impact of Prolonged Hotel Closures during the COVID-19 Pandemic on Legionella Infection Risks. Front Microbiol 2023, 14, 1136668. [Google Scholar] [CrossRef] [PubMed]
- Buchholz, U.; Brodhun, B.; Lehfeld, A.-S. Incidence of Legionnaires’ Disease among Travelers Visiting Hotels in Germany, 2015–2019. Emerging Infectious Diseases 2024, 30, 13. [Google Scholar] [CrossRef]
- Hayes-Phillips, D.; Bentham, R.; Ross, K.; Whiley, H. Factors Influencing Legionella Contamination of Domestic Household Showers. Pathogens 2019, 8, 27. [Google Scholar] [CrossRef]
- Buse, H.Y.; Morris, B.J.; Gomez-Alvarez, V.; Szabo, J.G.; Hall, J.S. Legionella Diversity and Spatiotemporal Variation in the Occurrence of Opportunistic Pathogens within a Large Building Water System. Pathogens 2020, 9, 567. [Google Scholar] [CrossRef]
- Vincenti, S.; Nurchis, M.C.; Boninti, F.; Sapienza, M.; Raponi, M.; Pattavina, F.; Pesaro, C.; D’Alonzo, C.; Damiani, G.; Laurenti, P. An Innovative Device for the Hot Water Circuit in Hospitals to Save Energy Without Compromising the Safety and Quality of Water: Preliminary Results. Water 2025, 17, 692. [Google Scholar] [CrossRef]
- Romano Spica, V.; Borella, P.; Bruno, A.; Carboni, C.; Exner, M.; Hartemann, P.; Gianfranceschi, G.; Laganà, P.; Mansi, A.; Montagna, M.T.; et al. Legionnaires’ Disease Surveillance and Public Health Policies in Italy: A Mathematical Model for Assessing Prevention Strategies. Water 2024, 16, 2167. [Google Scholar] [CrossRef]
- Leoni, E.; Catalani, F.; Marini, S.; Dallolio, L. Legionellosis Associated with Recreational Waters: A Systematic Review of Cases and Outbreaks in Swimming Pools, Spa Pools, and Similar Environments. Int J Environ Res Public Health 2018, 15, 1612. [Google Scholar] [CrossRef]
- Anagnostopoulos, L.; Kourentis, L.; Papadakis, A.; Mouchtouri, V.A. Re-Starting the Cruise Sector during the COVID-19 Pandemic in Greece: Assessing Effectiveness of Port Contingency Planning. International Journal of Environmental Research and Public Health 2022, 19, 13262. [Google Scholar] [CrossRef]
- European Legionnaires’ Disease Surveillance Network (ELDSNet) - Operating Procedures. Available online: https://www.ecdc.europa.eu/en/publications-data/european-legionnaires-disease-surveillance-network-eldsnet-operating-procedures (accessed on 10 June 2025).
- Yao, X.H.; Shen, F.; Hao, J.; Huang, L.; Keng, B. A Review of Legionella Transmission Risk in Built Environments: Sources, Regulations, Sampling, and Detection. Front. Public Health 2024, 12. [Google Scholar] [CrossRef] [PubMed]
- CDC Legionella (Legionnaires’ Disease and Pontiac Fever). Available online: https://www.cdc.gov/Legionella/index.html (accessed on 9 June 2025).
- Legionellosis (Legionnaires’ Disease). Available online: https://www.who.int/news-room/questions-and-answers/item/legionellosis-legionnaires-disease (accessed on 9 June 2025).
- Legionellosis. Available online: https://www.who.int/news-room/fact-sheets/detail/legionellosis (accessed on 6 June 2025).
- Legionnaires’ Disease. Available online: https://www.ecdc.europa.eu/en/legionnaires-disease (accessed on 6 June 2025).
- Vatansever, C.; Turetgen, I. Investigation of the Effects of Various Stress Factors on Biofilms and Planktonic Bacteria in Cooling Tower Model System. Arch Microbiol 2021, 203, 1411–1425. [Google Scholar] [CrossRef] [PubMed]
- Rhoads, W.J.; Hammes, F. Growth of Legionella during COVID-19 Lockdown Stagnation. Environ. Sci.: Water Res. Technol. 2021, 7, 10–15. [Google Scholar] [CrossRef]
- Martin, R.L.; Harrison, K.; Proctor, C.R.; Martin, A.; Williams, K.; Pruden, A.; Edwards, M.A. Chlorine Disinfection of Legionella Spp., L. pneumophila, and Acanthamoeba under Warm Water Premise Plumbing Conditions. Microorganisms 2020, 8, 1452. [Google Scholar] [CrossRef]
- Leaflet for Managers of Tourist Accommodation on How to Reduce the Risk of Legionnaires’ Disease. Available online: https://www.ecdc.europa.eu/en/publications-data/leaflet-managers-tourist-accommodation-how-reduce-risk-legionnaires-disease (accessed on 10 June 2025).
- Directive - 2020/2184 - EN - EUR-Lex. Available online: https://eur-lex.europa.eu/eli/dir/2020/2184/oj/eng (accessed on 10 June 2025).
Figure 1.
Legionella Positivity by Facility Type.
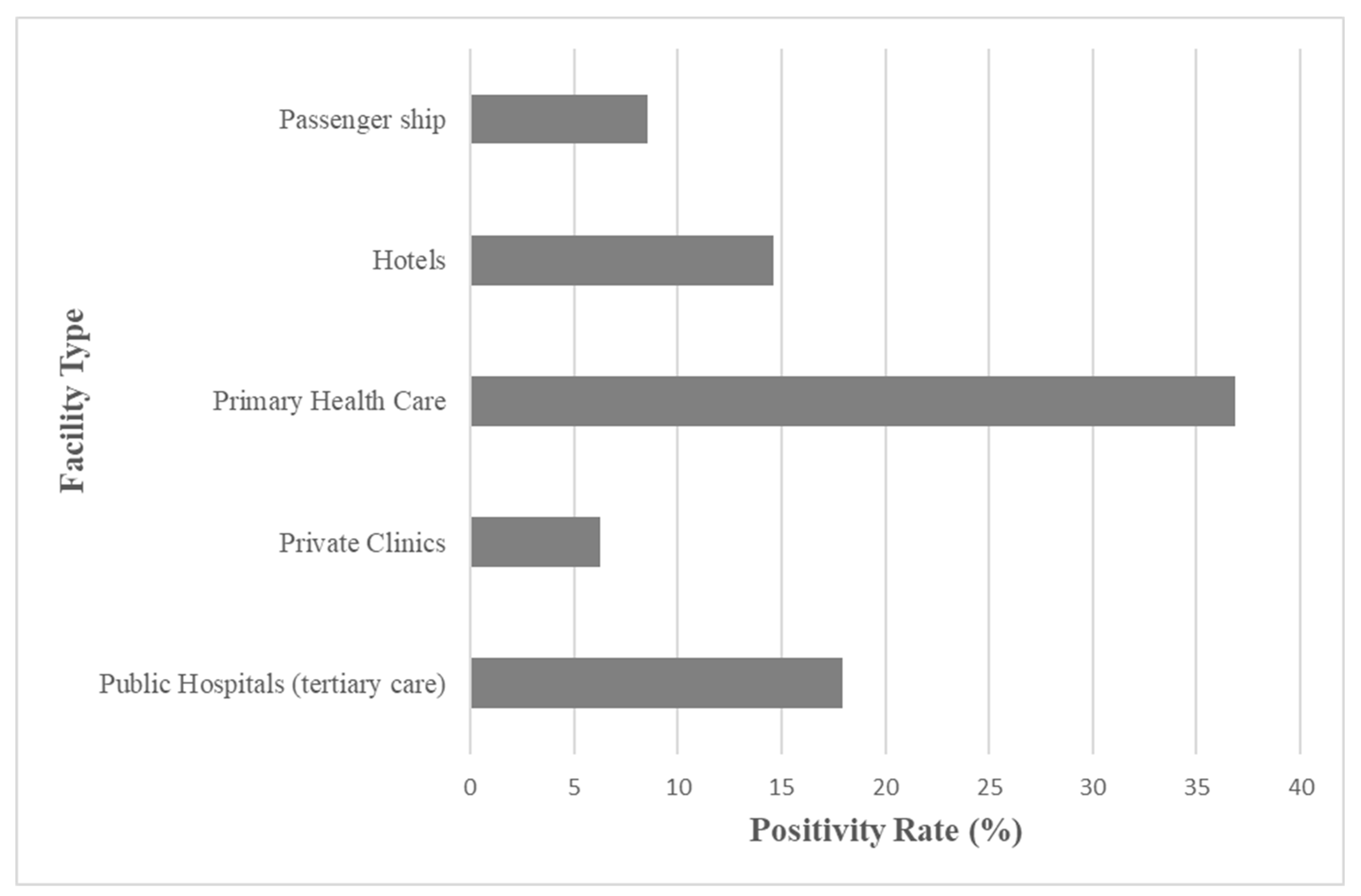
Figure 2.
Legionella Temporal Trends (2020-2025).
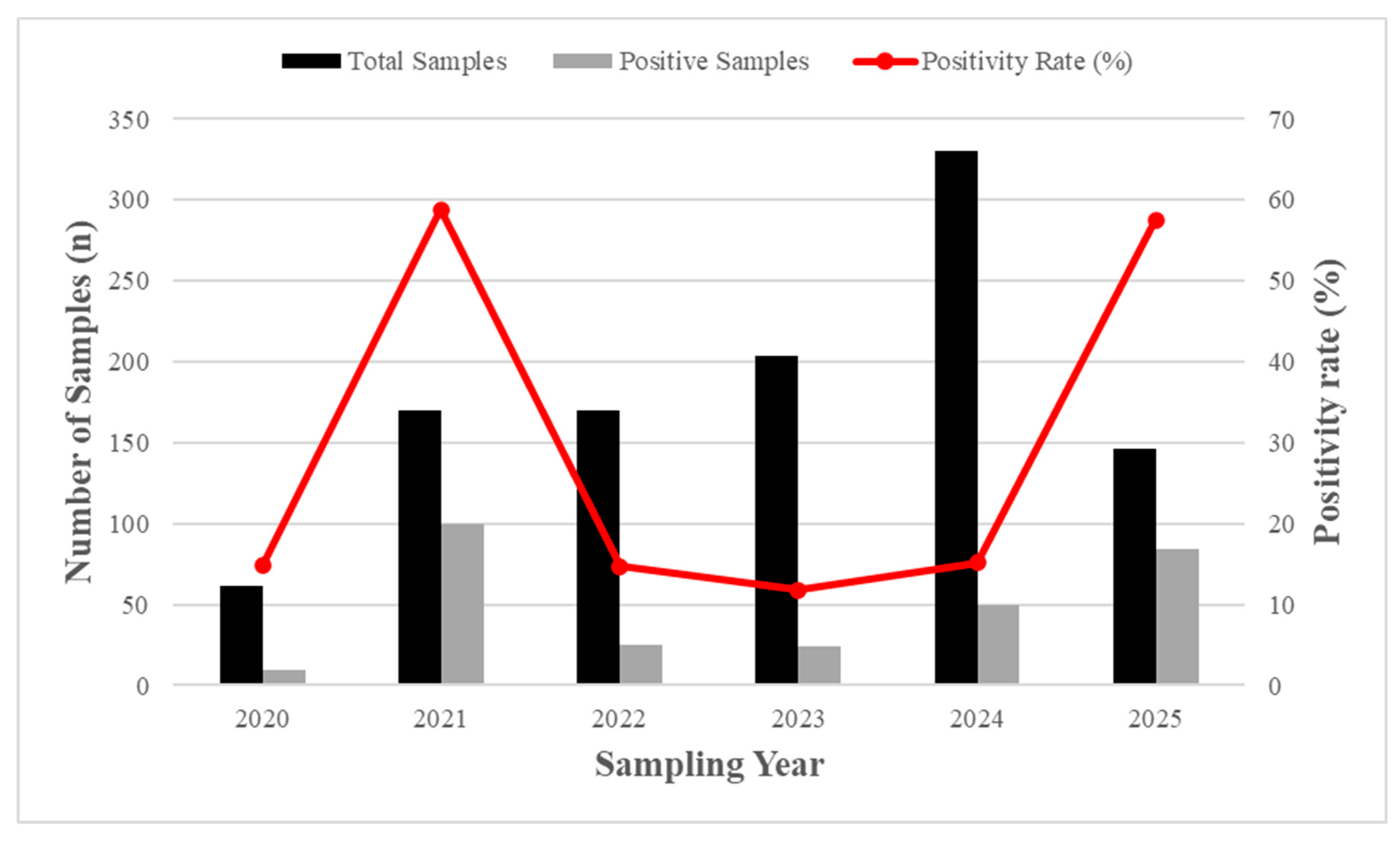
Figure 3.
Distribution of Legionella Serogroups in Positive Samples (n = 482).
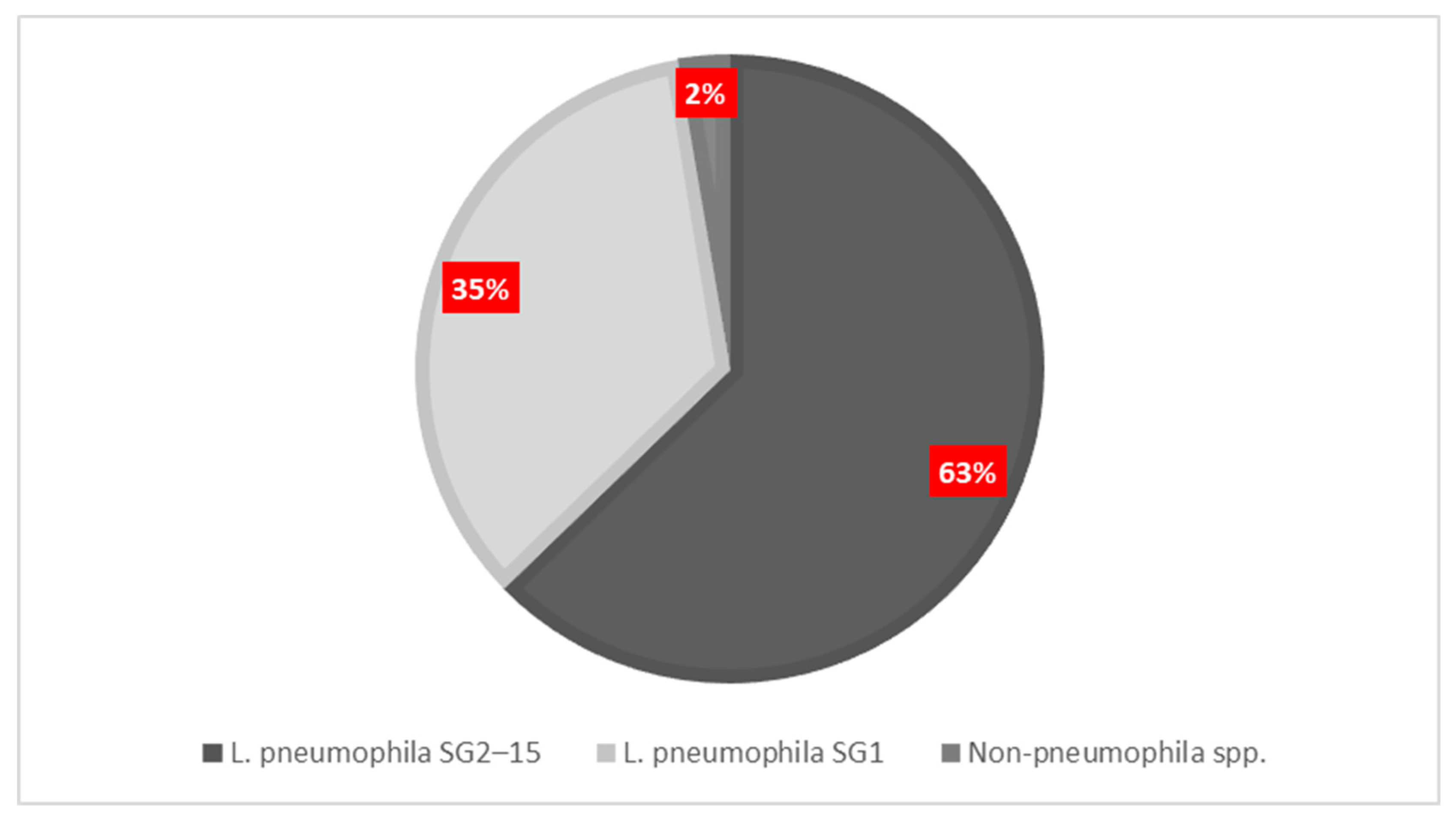
Figure 5.
Relative risk (p < 0.0001) of Legionella detection under physicochemical non-compliance conditions (2020–2025).
Figure 5.
Relative risk (p < 0.0001) of Legionella detection under physicochemical non-compliance conditions (2020–2025).
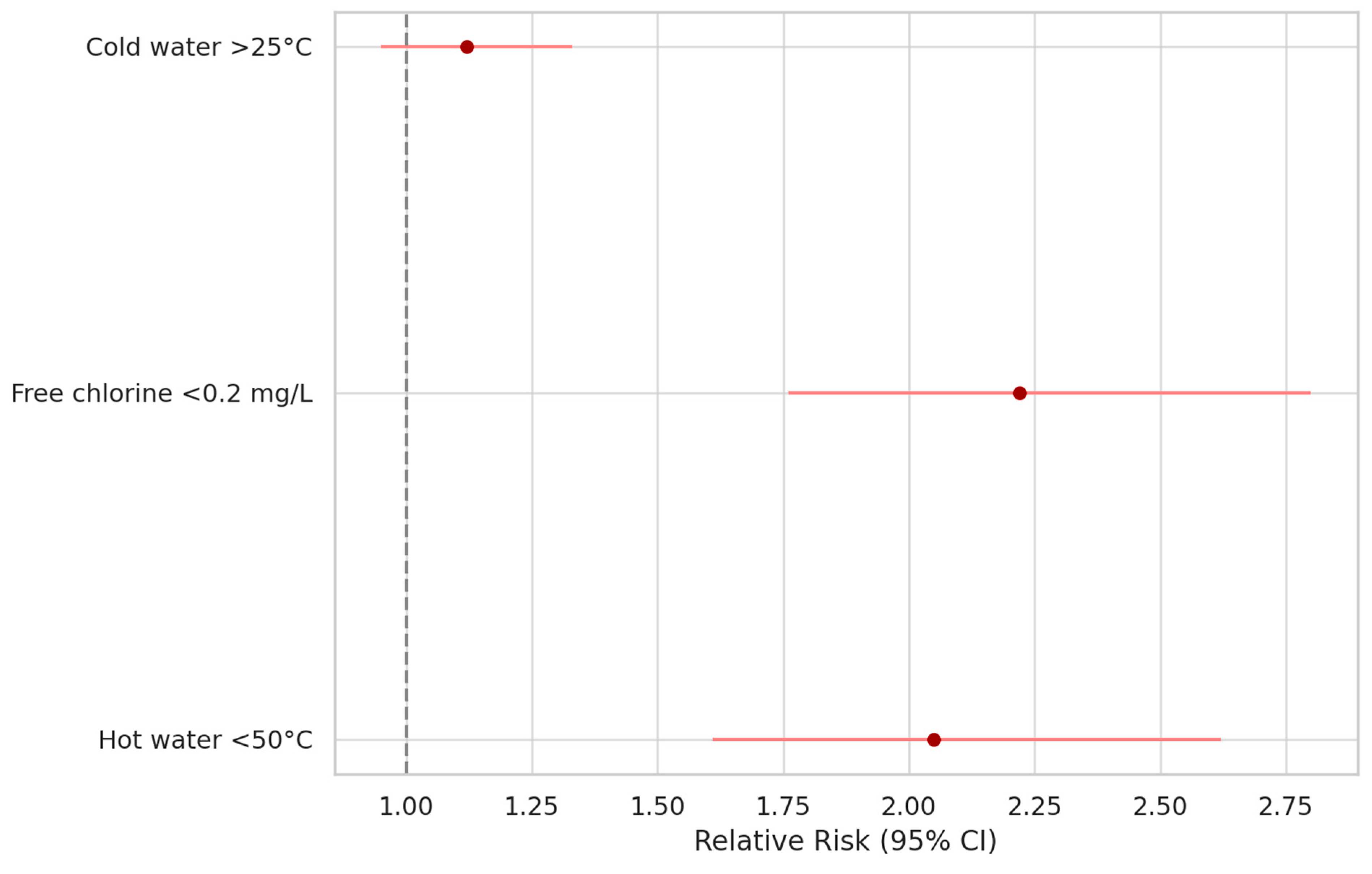
Figure 6.
Risk classification of Legionella spp. positive samples by facility type, based on CFU/L thresholds: low (<10³), medium (10³–<10⁴), and high (≥10⁴). Primary health care units exhibit the highest proportion of high-risk samples (20.17%), followed by passenger ships (6.25%) and hotels (4.60%).
Figure 6.
Risk classification of Legionella spp. positive samples by facility type, based on CFU/L thresholds: low (<10³), medium (10³–<10⁴), and high (≥10⁴). Primary health care units exhibit the highest proportion of high-risk samples (20.17%), followed by passenger ships (6.25%) and hotels (4.60%).
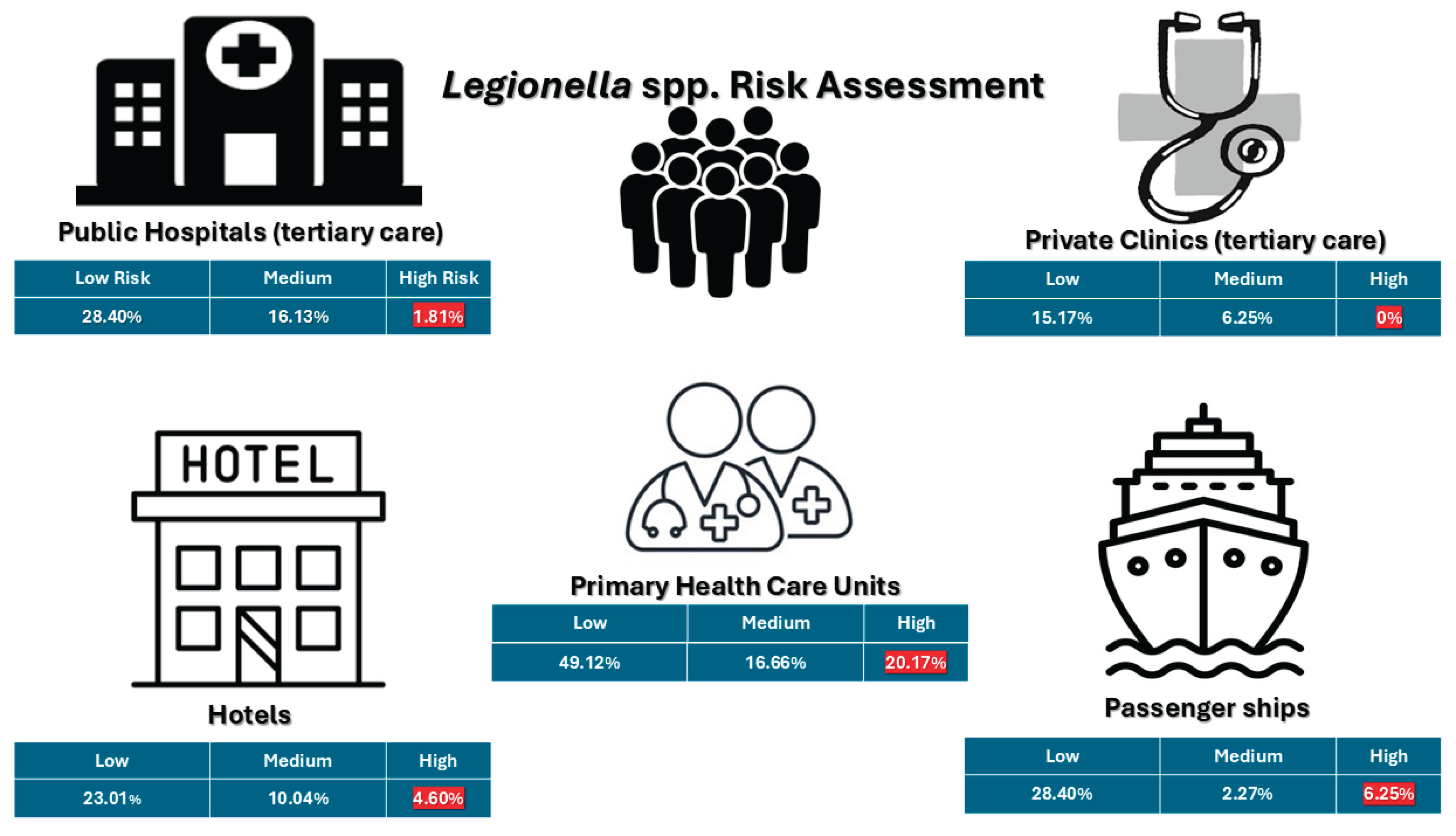

Table 1.
Distribution of water samples by facility type.
| Facilities | Frequency | Percent | Cum. Percent | Wilson 95% LCL | Wilson 95% UCL |
|---|---|---|---|---|---|
| Public Hospitals | 440 | 40.70% | 100.00% | 37.81% | 43.66% |
| Hotels | 239 | 22.11% | 22.11% | 19.74% | 24.68% |
| Passenger ships | 176 | 16.28% | 38.39% | 14.20% | 18.60% |
| Primary Health care units | 114 | 10.55% | 48.94% | 8.85% | 12.52% |
| Private Clinics | 112 | 10.36% | 59.30% | 8.68% | 12.32% |
| Total | 1081 | 100.00% | 100.00% |
Table 2.
Number of samples collected from different sampling points.
| Sampling description | Frequency | Percent | Cum. Percent | Wilson 95% LCL | Wilson 95% UCL |
|---|---|---|---|---|---|
| Close point | 66 | 40.74% | 40.74% | 33.10% | 48.73% |
| Far point | 96 | 59.26% | 100.00% | 51.27% | 66.90% |
| Direct | 600 | 57.92% | 57.92% | 54.88% | 60.89% |
| Indirect | 436 | 42.08% | 100.00% | 39.11% | 45.12% |
| Cold water | 600 | 55.50% | 55.50% | 52.53% | 58.44% |
| Hot water | 481 | 44,50% | 100,00% | 41,56% | 47,47% |
Table 3.
Number of positive samples on Legionella concentration collected from different facilities.
Table 3.
Number of positive samples on Legionella concentration collected from different facilities.
| Facility | Number of samples | <103 cfu/L | >=103 and <104 cfu/L | >=104 cfu/L | Total positive samples (>50 cfu/L) |
|---|---|---|---|---|---|
| Public Hospitals (tertiary-level care) | 440 | 125 (28.40%) | 71 (16.13%) | 8 (1.81%) | 204 (46.36%) |
| Private Clinics | 112 | 17 (15.17%) | 7 (6.25%) | 0 | 24 (21.42%) |
| Primary Health Care | 114 | 56 (49.12%) | 19 (16.66%) | 23 (20.17%) | 98 (85.96%) |
| Hotels | 239 | 55 (23.01%) | 24 (10.04%) | 11 (4.60%) | 91 (38.08%) |
| Passenger ship | 176 | 50 (28.40%) | 4 (2.27%) | 11 (6.25%) | 65 (36.93%) |
| Total | 1081 | 303 (28.03%) | 125 (11.56%) | 53 (4.90%) | 482 (44.59%) |
Table 4.
Legionella-positive samples by sample type and collection point.
| Sample Type | Number of Samples (n) | Positive Samples (n, percentage) |
|---|---|---|
| Hot water (total) | 481 | 252 (52.28%) |
| └─ Direct outlet | 258 | 131 (50.71%) |
| └─ Indirect outlet | 206 | 103 (50%) |
| └─ Far away point | 50 | 24 (48%) |
| └─ Close point | 32 | 11 (34.37%) |
| Cold water (total) | 600 | 230 (47.72%) |
| └─ Direct outlet | 342 | 134 (39.18%) |
| └─ Indirect outlet | 230 | 83 (36.08%) |
| └─ Far away point | 46 | 12 (23.80%) |
| └─ Close point | 34 | 11 (28%) |
Table 5.
Distribution of Legionella serogroups detected across different facility types.
| Facility | Total Positive Samples (n, %) | L. pneumophila SG1 (n, %) | L. pneumophila SG2–15 (n, %) | Other Legionella spp. (n, %) |
|---|---|---|---|---|
| Hotels | 91 (18.88%) | 27 (5.60%) | 66 (13.69%) | 6 (1.24%) |
| Passenger ships | 65 (13.49%) | 24 (4.5%) | 41 (8.50%) | 0 (0.00%) |
| Primary Health Care | 98 (20.33%) | 21 (12.07%) | 80 (16.60%) | 0 (0.00%) |
| Private Clinics | 24 (4.98%) | 7 (1.45%) | 17 (3.53%) | 0 (0.00%) |
| Public Hospitals | 204 (42.32%) | 95 (19.70%) | 111 (23.03%) | 7 (1.45%) |
| Total | 482 (44.59%) | 174 (36.09%) | 315 (65.35%) | 13 (2.70%) |
Table 6.
Risk factors for Legionella colonization per physicochemical parameters and water sampling sites.
Table 6.
Risk factors for Legionella colonization per physicochemical parameters and water sampling sites.
| Risk Factor | Odds Ratio (Cross Product) | Odds Ratio (MLE) | Risk Ratio (RR) | Risk Difference (RD%) | p-V |
|---|---|---|---|---|---|
| Free residual chlorine < 0.2 mg/L | 2.2213 | 2.2175 | 2.2175 | 18.6545 | <0.0001 |
| Cold water temperature > 25 °C | 1.2380 | 1.2375 | 1.1252 | 5.2736 | 0.1 |
| Hot water temperature < 50 °C | 6.5394 | 6.5073 | 2.054 | 41.5504 | <0.0001 |
| Hot water temperature < 35 °C | 4.7365 | 4.7202 | 3.5792 | 22.3196 | <0.0001 |
| Turbidity (non-compliant) | 2.5662 | 2.5639 | 2.5313 | 1.3503 | 0.04 |
| Direct water sample (vs. outlet) | 0.9341 | 0.9342 | 0.9610 | -1.6562 | 0.29 |
| Sampling at distal (far) outlet point | 1.3534 | 1.3504 | 1.1124 | 6.8915 | 0.22 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



