
Submitted:
05 June 2025
Posted:
11 June 2025
You are already at the latest version
Abstract
Background: Falls in older adults are a leading cause of morbidity, particularly when compounded by polypharmacy. There is mixed evidence of efficacy of medicine reviews, but there is little work exploring this in the ambulance setting. A new referral pathway enabling ambulance staff to connect patients to primary care pharmacists aimed to address this. This study explored staff and patient experiences with the pathway and its potential to improve medicine safety after the fall.
Methods: A mixed-method service evaluation was conducted to assess the implementation and impact of this pathway. Routine data from an ambulance trust and pharmacist proformas were used to address objectives relating to referral rates, clinical appropriateness, and fall recurrence. Patient and staff stakeholder perspectives were gathered through two cross-sectional surveys designed to explore emotional, behavioral, and practical responses to the intervention. Quantitative data were analyzed descriptively and using ordinal logistic regression where appropriate. Free-text responses were analyzed thematically.
Results: Between May 2019 and March 2020, referrals were initiated for 775 older adults after ambulance attendance for a fall, with pharmacists completing medicine reviews on 340 patients. Survey data revealed improvements in patients’ emotional responses to their medicines. Ambulance clinicians identified patient disclosure, stockpiling, and the presence of expired medicines as key indicators of poor medicines management and valued the ability to refer patients.
Conclusion: Overall, referral to the pathway demonstrates a marginal improvement in recontact rates in the short-term but does not necessarily represent an improvement in overall patient safety. The cost of such an intervention and patient expectations needs further exploration to prove efficacy and patient satisfaction.
Keywords:
emergency medical services
; accidental falls
; pharmacists
; referral and consultation
; medicine review
; medicines
1. Introduction
Falls among older adults (≥ 65 years) are a major health concern, with 7.6% of falls resulting in moderate or severe injuries [1]. Even without injury, falls often lead to a fear of falling, negatively impacting quality of life [2,3]. Those most at risk - older, frailer individuals, especially those with dementia or a history of falls – represent some of the most vulnerable in society [4]. Reducing falls and their consequences is therefore a national health priority [5].
In England, 42.5% of ambulance-attendances for falls result in patients being discharged at the scene [6]. Guidelines recommend these patients should be referred for further assessment of frailty, social care needs, and fall risk factors [7]. Polypharmacy (≥ 4 medicines) is a well-established fall risk [8], highlighted in recommendations in the World Guidelines for Falls Prevention and Management for Older Adults [9] and National Institute for Health and Care Excellence guidance [10]. Despite this, no specific guidance exists for managing polypharmacy in the ambulance setting.
Pharmacist-led medicine review is perceived as an important part of managing falls risk, especially in older adults [11]. Existing literature indicates medicine reviews are effective in reducing the number of medicines prescribed and therefore drug costs [12,13,14,15]. However, there is conflicting evidence around the impact of medicine review on falls risk, with some authors reporting clear efficacy [16,17,18], and some reporting little to no benefit [19,20,21,22,23,24]. While studies have explored the impact of medicine review in inpatient and community populations, limited evidence exists of how medicine reviews may fit within the ambulance service setting [25,26,27].
In response, a local quality improvement initiative connected ambulance-attendances for falls with primary care pharmacists. This study evaluated whether the initiative improved patient safety by reducing recurrent falls. Objectives were to:
- Determine the rate and suitability of referrals and subsequent clinical impact.
- Quantify medicine optimization for patients who underwent medicine review.
- Explore patient experiences and feelings around referrals and their medicines.
- Explore ambulance healthcare professionals’ perceptions of the value of referral.
2. Materials and Methods
A multi-methods approach was used, combining service evaluation and stakeholder surveys. Reporting followed SQUIRE [28] and CROSS [29] guidelines (Tables S1 & S2).
2.1. Context
This initiative took place in a single, well-resourced, ethnically and socially diverse urban district in northern England (population ~800,000), featuring a teaching hospital trust, intermediate care trust and a regional ambulance service with five local stations. The local primary care confederation included 87 GP practices and a coordinated pharmacy team.
2.2. Improvement Initiative
Eligible patients (see Table 1) seen face-to-face by ambulance clinicians after a fall and discharged at home were referred through a non-urgent pathway (Figure S1).
In the improvement group, referrals were also sent to the primary care pharmacy team. Pharmacists conducted medicine reviews (face-to-face, telephone, or records-based), with changes made at pharmacists’ discretion. Outcomes were shared with the patient’s GP and ambulance trust via proforma.

Table 1.
Screening criteria.
| Inclusion | Exclusion |
| Aged ≥ 65 | Aged < 65 |
| Face-to-face assessment by an ambulance clinician | No face-to-face contact |
| Primary reason for ambulance attendance was fall | Patient conveyed to hospital |
| Taking ≥ 1 medicine (prescribed or otherwise) | Not taking medicines |
| Fall in a residential address | Fall in public or patient is a care/nursing home resident |
| Registered with a local confederation GP | Registered with a GP outside the confederation |
| Non-urgent referral made | No referral made |
2.3. Service Evaluation
The first two objectives were addressed using routine data from the ambulance trust and pharmacist proformas (see Table 2). Data were collected from 13th May 2019 to 22nd March 2020 (paused due to COVID-19). Fall recurrence was tracked via 30-day follow-up using NHS numbers. Comparisons were made between referred and non-referred patients in the same area.
2.4. Stakeholder Surveys
To explore the experiences and perceptions of those involved, two cross-sectional surveys were conducted: one for patients referred for medicine review and one for ambulance staff (see Table 2).
2.4.1. Patient Survey
A postal survey was sent to all patients who were referred through the medicine review pathway. Each survey pack contained a covering letter, a participant information sheet, consent form, a 12-question booklet (Figure S2), and a pre-paid return envelope. Completion of the consent form or return of the survey was accepted as consent to participate.
The survey included four sections: demographics, emotional perspectives about medicines and review, and impact of review activities on emotional outcomes.
Patients selected emotional descriptors (e.g. “safe”, “frustrated”) before and after review to indicate how they felt about their medicines. A change in emotional direction (e.g. from negative to neutral) was used to assess impact with statistical significance determined using McNemar’s test.
To assess the influence of review features (e.g. setting, communication style, shared decisions) on emotional outcomes, ordinal logistical regression (R) using a proportional odds model was used [31] and assumptions determined by Harrell’s [32] method, adjusting for age, gender, ethnicity, review format, and key review activities.
A free-text field allowed participants to identify what they intended to change post-review. Responses were thematically analyzed.
Data were anonymized and entered into a digital format for analysis, including incomplete questionnaires. A sample size of 132 was targeted based on detecting a 20% increase in positive emotion with 90% power and 5% significance [33].
2.4.2. Ambulance Clinician Survey
Patient-facing ambulance staff of all grades were invited to complete an online survey promoted through staff bulletins and in-person events. The online survey (Figure S3) consisted of twelve questions covering: demographic profile (e.g. role, working hours), perceived frequency of patients with medicine-related difficulties, indicators used to identify such patients, and perceived value of primary care pharmacy referral option.
Participants ranked ten predefined indicators of medicine-related difficulties (e.g. confusion, medicine errors). Weighted averages were calculated from rankings to prioritize key factors.
Perceptions of referral value were rated using a five-point Likert scale. Correlation between value perception and demographics (e.g. role, working hours) were explored using ordinal logistic regression (R) and reported as an odds ratio with 95% confidence intervals.
A free-text field followed a case study, which was designed to identify a person who was struggling to manage their medicines. Participants were asked to share how they would manage the person’s case. Additionally, participants were asked to express what they felt would alert them to someone who was struggling with managing their medicines. Responses were anonymized and then independently coded into themes by two ambulance service researchers (FB [non-clinical], EM [clinical]).
A target sample of 330 responses was set based on a conservative 10% response rate from 3,294 eligible staff members.
2.5. Ethical Considerations
Health Research Authority approval was gained for the stakeholder surveys (IRAS 263976). Approval from the Research Ethics Committee and Confidentiality Advisory Group was obtained for the patient survey (19/YH/0211). All data were handled in accordance with the Data Protection Act 2018 and United Kingdom General Data Protection Regulations. Returned booklets without signed consent were included if the survey was completed, with participation indicating assent.
3. Results
Between 13th May 2019 and 22nd March 2020, the ambulance trust received 11,831 fall-related 999 calls, of which 2,610 calls were in the study area. For 820 patients, non-urgent falls referrals were made by ambulance crews to the ambulance trust’s clinical support line. 775 of these were also referred to the primary care confederation, with 340 (43.9%) undergoing a medicine review (Table 3).
Among referred cases, 73.9% had experienced a fall in the previous year, and 77.0% met the definition of polypharmacy (≥4 medicines). Demographics were similar across groups, although ambulance crews more frequently flagged medicine concerns in patients who did not receive a review (25.1% vs. 18.8%). The median time from referral to review decision was significantly shorter for those who were reviewed (9 days) compared to those who were not (28 days).
Among non-reviewed cases, 92 had documented reasons, including referral process errors (n=32), inability to contact patients (n=12), recent hospitalization (n=12), review deemed unnecessary (n=12), care home residency (n=6), recent review elsewhere (n=5), and other reasons (n=13). For most others, no reason was recorded but was likely due to capacity constraints. Additionally, 32 referrals from May to July 2019 were lost due to human error and excluded from analysis.
3.1. Referral Rate, Suitability, and Clinical Impact
Among reviewed patients (see Table 4), most medicine reviews were conducted remotely—36.8% via notes and 22.6% by telephone—while only 2.1% were face-to-face. However, review method was not recorded in 38.5% of cases, limiting interpretation.
Frailty data showed a bimodal distribution, with most patients categorized as either not frail or moderate/severely frail. Only 1.8% were identified as mildly frail – potentially due to limitations in frailty assessment tools or reporting practices.
Of the patients who received a medicine review, 77.4% were considered appropriate. As this was only recorded for reviewed cases, comparisons with non-reviewed patients – who made up 56.1% of referrals – are limited.
Recontact rates (Table S4) were assessed by comparing the 127 patients who received a review with 2,483 local over-65s who had called the ambulance service for falls. No referred participants recontacted the ambulance trust within a week of discharge, compared to 2.1% of the reference group. The difference at 30 days was not statistically significant (98.0% vs. 94.0%, p = 0.11).
3.2. Medicine Optimisation
Polypharmacy was prevalent, with 91% (n = 308) of reviewed patients prescribed ≥4 medicines (Table 3). The median number of medicines (Table 5) remained unchanged before and after review (9; IQR 6-12). However, 272 patients had adjustments to their prescriptions, including 122 with medicines deprescribed and 11 prescribed new ones. Pharmacists recommended 149 additional changes (43.8%), such as dose/timing adjustments, medicine switches, or referrals for further review.
Pharmacists identified medicines as a likely contributor to falls in 22.2% of cases (Table 5), with 12.6% considered high risk. However, this was not recorded in 62.6% of reviews, limiting broader analysis. Pharmacists changed medicines related to falls risks for 46 patients, of which 28 were high-risk medicines.
3.3. Patient Experiences and Feelings
Of 265 patients referred for a medicine review between 7th August 2019 and 23rd March 2020, 218 were sent a postal survey; 48 responded (22%), representing a third (36.4%) of the target sample size. Table 6 provides a breakdown of the demography of respondents.
Respondents were predominantly older adults (mean age 83.59) with a slight female bias (54.2%). Most identified as White British (95.9%). Given the lack of ethnic diversity, ethnicity was excluded from the statistical model.
Most respondents (91.7%) took medicines (n = 44), with 62.5% taking five or more. Respondents reported that their reviews were undertaken face-to-face (31.2%), via telephone (27.1%) or could not recall the method (29.2%), which was inconsistent with Table 4, where most reviews appeared to be notes-based. This discrepancy may stem from patients being unaware that a review occurred if it was a notes review with no observable changes – indeed, four participants were unaware that they’d had a medicine review at all.
Figure 1.
Breakdown of medicine review activity by method of review.
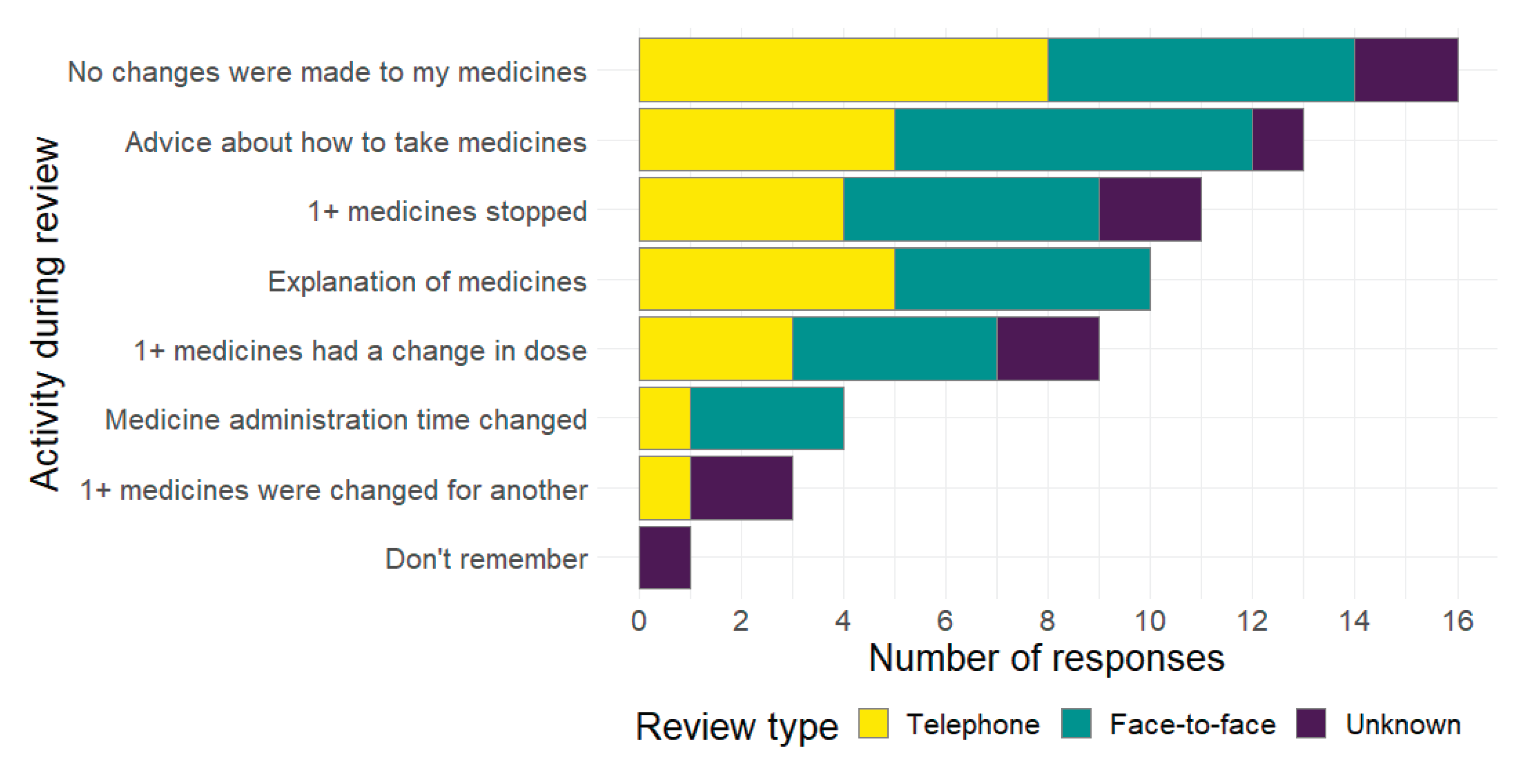
A third of respondents (n=16) reported no medicine change, many described adjustments, including stopping or switching medicines, or changes in dose/timing. Additionally, 23 received advice or information. Outcomes were broadly similar across review types.
Free-text responses (n=30) indicated that nearly half reported no change in behavior post-review. Others mentioned using aids (e.g. alarms, dosette boxes), falls prevention strategies (e.g. mobility aids, reducing hazards, increasing light levels) or awaiting specialist input (e.g. hospice, pain clinic, ear-nose-throat).
Thirty-eight participants reported emotions before and after review. Emotional change was reported in 8 participants (16.7%), with 7 reporting a positive change (p = 0.07). Most (n=23) reported neutrality before and after review (Table 7).
Proportional odds modelling revealed wide confidence intervals for all factors except age (1.00, 0.91–1.11) (Table S5).
3.4. Ambulance Healthcare Professional Perceptions
A total of 146 responses (44% of the target sample) were received between May 2019 and May 2020. Table 8 indicates a summary of respondent profile. Only 12.3% (n=18) had made a referral to the non-urgent falls pathway for a medicine review. Most respondents were full-time (76.7%), non-specialist paramedics (44.5%), and frequently attended fall-related calls. Despite limited direct experience with the referral process, 85.6% (n=125) perceived referral for medicine review as “important” or “very important”. No significant differences in perceptions were found between those who had made referrals and those who had not.
Self-reported data on clinical practice (Table S6) revealed that, on average, 45.0% of fallen patients were not conveyed to hospital. Of these, 80.0% were referred to a falls pathway, 30.0% primary care, and 40.0% were thought to have difficulty managing their medicine.
The most important indicators that patients were having difficulty managing their medicines were: patients stating that they were not taking their medicines as prescribed and the presence of unused and expired medicines around the home. Less influential factors were difficulty in taking or timing medicines, or disorganized storage (e.g. keeping medicines in multiple or hard-to-reach locations) (Table S7).
Ordinal regression modeling of staff demographics revealed no apparent correlation with the value placed on referral (Table S8).
Free-text responses supported this: the most common method of identifying difficulties was direct observation of a person’s living situation (n=121), followed by disclosure from the patient or their carer (n=72), the patient’s clinical presentation (n=44) and observation of the patient (n=7).
Managing difficulty with medicines, or care planning, overwhelmingly involved referral to another service (n=110, e.g. primary care, intermediate care, or falls response services). Other strategies included discussing and confirming medicine regimens with patients or carers (n=32), safety netting advice (n=27) and immediate mitigations (n=19), such as disposing of out-of-date medicines, liaising with care services, and clearly identifying to patients which medicines they should be taking, and when.
4. Discussion
Falls in older adults can have significant health impacts, both physical and psychological. Polypharmacy is a key risk factor in this population, with 77% of referred patients taking four or more medicines. This study set out to explore, using a multi-methods approach, whether there were patient safety benefits to pharmacist-led medicine review following an ambulance at-scene discharge for falls.
The results demonstrated that almost all patients referred to the non-urgent pathway were also referred for a medicine review. More than three in every four cases reviewed (77.4%) were considered appropriate referrals by pharmacists, suggesting that ambulance clinicians demonstrated sound clinical judgement in identifying suitable patients. Although this demonstrates the feasibility of the pathway and that there is a role for medicine reviews in this space, the majority of patients referred for review (56.1%) did not receive one. Reasons for this were poorly reported - 78.9% (n=343) of these cases did not provide an explanation - with referral process errors and inability to contact patients being the leading reasons for non-review. A similar initiative by Nymoen et al. [34] reported a similar non-review rate (56.3%) in a Norwegian ED, as did Mikolaizak et al [35] (54%) in an Australian post-ambulance-discharge assessment study. Organizational capacity and funding were cited by authors and were likely shared contributory factor with this study, especially given that the decision to review study participants took longer in those who were not reviewed (28 vs. 9 days). A recent scoping review of organizational implementation frameworks for polypharmacy management [36] identified resource limitations and poor information transfer as major barriers - factors echoed in this evaluation. The same review identified facilitators such as public funding, safety-orientated regulatory environments, and generation of local evidence, which may be relevant for future implementation efforts. Limited pharmacist capacity may indicate a need to more exclusively screen patients for referral.
While polypharmacy is a well-recognised risk factor in falls [11,37], it may be too broad and non-specific an indicator to reliably identify patients at the highest risk of fall. PrescQIPP [30], STOPPFall [38] and the National Falls Prevention Coordination Group [39] provide lists of medicines known to increase risk of fall, many of which are psychotropics. Given that deprescribing of psychotropic drugs has demonstrated potential to reduce falls risk [21,40], referring only patients who take psychotropics, and other falls risk increasing drugs may result in a more effective resource use and greater impact on recurrent fall rates.
Adherence to follow-up has been suggested to be related to patient perceptions of the pharmacist role [34,35], which may indicate that pharmacists’ clinical skills beyond medicines supply need to be recognized and embraced by patients [41]. However, since data were collected for this study, NHS healthcare strategy has triggered an increase in the number of pharmacists working in a primary care capacity [42], with a focus on prioritizing medicine reviews for those who have fallen or are severely frail [43]. This may mean that the public is more aware of the role of pharmacists in this space.
The financial impact of the intervention, including both the implementation costs and any resulting medicine changes, were not explored by this study. This represents a critical gap, as cost-effectiveness is key to the long-term viability of resource-intensive health interventions. Notably, there was no change to the median number of medicines prescribed pre- and post-review (n = 9 [6,7,8,9,10,11,12]), and only a small proportion (13.5%) of reviews involved any changes to medicines contributing to falls risk. Among all 775 referrals, only 28 high-risk medicines were changed.
Previous studies offer mixed findings on the impact of similar interventions. Bonner et al [44] completed a systematic review of four studies exploring the effectiveness of non-urgent fall referral, and discovered a consistently non-significant improvement in recontact rates. Shaya et al. [45], in a small study of pharmacist-led medicine reviews of younger diabetics post-acute care in the United States, reported a non-significant reduction in medicine and service costs at 180 days (cost ratio 0.65, p = 0.13). In contrast, Siddle et al. [46], demonstrated a significant reduction in inpatient admissions following paramedic-led health visits in the United States (140 to 26, p = 0.00), but reported a non-significant increase in urgent and emergency care service usage. In the present study, a modest (though statistically non-significant) improvement in non-recontact rates was observed (98% vs 94%, p = 0.11). The Norwegian Nymoen et al [34] study reported similarly non-significant improvements in recontact rates (51.0% vs 53.2%; p = 0.546), in line with similar ED-based studies reporting no statistically significant impact on reattendance, readmission, or other health service utilization [47,48,49]. Nymoen [34] did however describe four ward-based medicine review studies which did significantly reduce ED revisit [50,51,52,53], hospital readmission [51,52,53], and healthcare costs [51]; this, along with findings in this study, raises the question as to whether the urgent and emergency care sector is the most effective environment to review medicines.
However, the utility of recontact as a primary outcome is questionable. As others have argued [45,46], reductions in short-term re-contacts may reflect system-level incentives rather than meaningful improvements in patient outcomes. Recontact in this study did not mean ambulance attendance, given a significant number of calls are referred to urgent care services or are managed by reactive specialist responders (similar to those described by Siddle [46]). More meaningful outcomes – such as admission to hospital, injury and fall rates, fear of falling, reattendance outcomes and costs associated with these events – were not assessed and may offer better insight into the intervention’s true value. The wider impact from a patient’s perspective was measured by Mikolaizak et al [35] in an Australian study of multifactorial review following ambulance discharge but no significant improvement in quality of life was identified.
Patients surveyed in this study indicated apparent apathy in their feelings towards their medicines, both before and after review. This limited the utility of regression analysis in identifying components of the medicine review linked to emotional change. Patient expectation of medicine review may be the underlying cause for this finding. Qualitative interviews with patients experiencing polypharmacy [54] revealed that patients expect a medicine review to be focused on their lived experience of taking their prescribed medicines - including side effects, concerns, and treatment efficacy. Instead, many participants in such studies [54] reported uncertainty in the role and expertise of the reviewing pharmacist and felt the whole process was simply to check a box. A scoping review by Peters et al. [55] reported that few patients were able to recall being given medicine advice sheets by paramedics, which correlates with 29.2% of this study’s participants reporting they did not realize they had a medicine review. Peters et al [55] describe that many patients did not engage in follow-up. Considering this and our finding of apathy, there may be a significant missed opportunity to better understand patient ideas, concerns, and expectations, and therefore deliver more tailored patient-centered care. Locally, further improvement initiatives were started to address the need to engage service users in the medicine review process, including producing multi-language printable resources [56] and videos [57] for patients and healthcare professionals.
Ambulance staff in this study expressed strong support for pharmacist-led medicine review after falls, but the specific rationale for this was not explored. Ambulance staff reported unique insights from in-home assessments, such as witnessing stockpiling or expired medicine. This contrasts with work by Nymoen et al [34] in hospital, where issues around medicine adherence accounted for only 9.4% of problems identified. Previous reports, including those by Crockett et al. [26], have described positive experiences of paramedic-led multidisciplinary community teams targeting the management of patients with serial admission for heart failure. Similarly, Hertig et al. [58]reported the use of final year student pharmacists as part of a paramedic-led home visit team, reporting that most visits resulted in identifying medicine-related problems and providing patient education. Current ambulance service guidelines for falls in older adults [59] acknowledge the risk of certain drug classes (e.g. psychotropics, diuretics), but lack reference to broader prescribing safety resources such as the PrescQIPP guidance [30]. Incorporating pharmacists into multidisciplinary falls pathways may improve identification and management of medicine-related risks. However, questions remain about the cost-effectiveness and sustainable funding of such models.
Despite the majority of surveyed paramedics reporting frequent falls-related attendances and high rates of non-conveyance, only 12% indicated that they had used the medicine review referral pathway over a 10-month period. Based on the estimated number of eligible patients per clinician during this time (approximately 70), the disparity between reported attitudes and actual behaviour warrants further research. This discrepancy may reflect a well-documented overestimation bias commonly associated with self-reported adherence to best practices. Eccles et al. [60] found that while there is a generally predictable relationship between intention and behaviour among health professionals, actual behaviour is more likely to align with intention when measurement relies on self-report, potentially inflating estimates of compliance. Furthermore, Hrisos et al. [61] highlighted the limited validity of clinician self-report as a proxy for actual clinical behaviour, noting inconsistencies and a lack of reliable correlation when compared with direct observational methods. Thus, while paramedics expressed support for the concept of pharmacist-led medicine review, operational constraints, competing clinical priorities, and uncertainty around pathway eligibility may have contributed to low uptake. It is also possible that clinicians’ decision not to refer – whether due to time pressure, lack of pathway visibility, or low perceived value of the non-medicine aspects of the referral – represent an additional gap between potential and actual usage. This raises a further challenge in estimating the true proportion of falls cases that should be referred but are not, underscoring the complexity of translating guideline-aligned intentions into practice. These findings reinforce the need for caution when interpreting self-reported data in implementation research and underscore the value of objective system-level metrics or audit data in accurately assessing intervention fidelity.
4.1. Limitations
All elements of this project were suspended in March 2020 due to the COVID-19 pandemic response in the United Kingdom. Redeployment of clinical staff to frontline roles and national reprioritization of research capacity delayed analysis of results significantly. Given the delay between data acquisition and analysis presented in this article, authors invite readers to share the careful consideration applied during interpretation and evaluation of results.
Key statistical analyses, including regression models and McNemar’s test, did not produce statistically significant results – possibly due to small sample sizes and low event rates. Many proformas were returned with incomplete data, with 62.6% of reviews not having the risk level of medicines recorded. Studies reviewed by Peters [55] faced similar issues of incomplete data capture and subsequent low sample. Future research should explore the use of electronic technologies and stricter methods to capture this data. Medicine reviews now benefit from a dedicated code on NHS primary care systems, which may help future researchers better identify participants and review activities.
Surveys asked patients how many medicines they were taking before the review, but this was not categorized based on the study definition of polypharmacy (0, 1-4, 5+ vs. ≥4), meaning the rate of polypharmacy between those referred and those responding could not be compared.
Recontact rates, while a pragmatic measure, likely underestimated broader clinical impact. The control group may have included patients requiring hospital conveyance, unlike the more selectively referred group. Additionally, referral decisions may reflect selection bias, with patients perceived to be at higher risk of serial falls by the ambulance clinician more likely to be referred than those viewed to have isolated falls.
The study’s urban setting within a public health system limits generalizability to low-resource settings, rural and coastal environments, or private sector care systems. Rural regions often suffer from a city-centric approach to service prioritization and require bespoke approaches to managing cases in these communities [55].
4.2. Future research
While the causative nature of falls is unlikely to have changed significantly since this data was collected, it should be considered that there are emergent stakeholders in the management of adults who fall. Virtual wards and frailty services, non-medical prescribers (including specialist paramedics), and non-clinical falls services all have a key role to play in managing these patients. Exploration of patients managed by these stakeholders may yield further information about effectiveness and potential opportunities to intervene with these skillsets, especially considering there may be an existing reluctance to adhere to recommendations by subject matter experts (pharmacists).
The economic impact of such an intervention should be further explored to understand the cost of achieving specific measures, which should also be more carefully selected. Specific changes to medicines (e.g. changes to dosage, changes to timing) should be mapped against meaningful patient outcomes (e.g. serial fall, fracture within months, fear of falling) to more clearly understand whether medicine review has an impact on patients’ lives, which may be achievable through the use of new medicine review coding practices.
Further research should explore how those taking medicines feel about their medicines, especially in the context of fall risk, to help better understand patient expectations and needs. Additionally, given that medicine review as an isolated intervention may not prove effective, further research should consider the exploration of longitudinal and holistic approaches to sharing management of medicines between the patient and the healthcare professional.
Finally, research in a more diverse range of settings may reveal demographic patterns, especially in marginal rural and coastal communities. Investigation of participant feelings should focus on a more ethnically diverse range of perspectives.
5. Conclusions
Referral to a pharmacist-led medicine review pathway following ambulance attendance for a fall demonstrated a marginal improvement in recontact rates in the short-term, with limited evidence of improved patient safety. While reviews were often clinically appropriate, their impact was constrained by low completion rates, unclear communication with patients, and minimal emotional engagement. Despite strong paramedic support for the referral pathway, actual referral rates were lower than expected, suggesting a disconnect between reported and actual practice. To realise the pathway’s potential, future work should address efficacy, implementation barriers, costs, and alignment with patient expectations.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Figure S1: Non-urgent falls pathway; Figure S2: Patient survey booklet; Figure S3: Staff survey; Table S1: SQUIRE checklist; Table S2: CROSS checklist; Table S3: PrescQIPP medicine list; Table S4: Recontact rates; Table S5: Proportional odds model (patients); Table S6: Self-reported practices by ambulance healthcare professionals when managing falls; Table S7: Perceived risk factors for patients having difficulty managing their medicine ordered by weight mean; Table S8: Ordinal regression for staff characteristics.
Author Contributions
Conceptualization, Heather Smith, Emily Turner, Heather Edmonds, Peter Webster, Graham Prestwich, Fiona Bell and Rebecca McLaren; Data curation, Richard Pilbery; Formal analysis, William Mulrooney, Caitlin Wilson and Richard Pilbery; Funding acquisition, Fiona Bell and Rebecca McLaren; Methodology, William Mulrooney, Caitlin Wilson, Richard Pilbery and Fiona Bell; Project administration, Richard Pilbery, Ruth Fisher and Fiona Bell; Validation, Richard Pilbery, Ruth Fisher and Sarah Whiterod; Writing – original draft, William Mulrooney, Caitlin Wilson and Richard Pilbery; Writing – review & editing, William Mulrooney, Caitlin Wilson, Richard Pilbery, Ruth Fisher, Sarah Whiterod, Heather Smith, Heather Edmonds, Peter Webster, Graham Prestwich and Fiona Bell. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Institute for Health Research Yorkshire and Humber Patient Safety Translational Research Centre, grant Safety Innovational Challenge Fund, number SICF19/03/3a.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The surveys completed were approved by the Health Research Authority (IRAS 263976, 19/07/2019) and the National Health Service Research Ethics Committee (19/YH/0211, 19/07/2019). The service evaluation aspect was registered with the Yorkshire Ambulance Service NHS Trust.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets generated and analysed during the current study are not publicly available as sharing the raw data would violate the agreement to which participants consented; however, the datasets are available from the corresponding author on reasonable request.
Acknowledgments
We would like to thank the patients, pharmacists, and ambulance staff for participating in this study. We would also like to extend thanks to Elisha Miller, who supported the study through data coding and processing, and Professor Dawn Teare, who advised on statistical analysis.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| SQUIRE | Standards for Quality Improvement Reporting Excellence (2.0) |
| CROSS | Checklist for Reporting of Survey Studies |
| CI | Confidence Interval |
| OR | Odds Ratio |
| IQR | Interquartile Range |
References
- Stevens, J., J. Mahoney, and H. Ehrenreich. "Circumstances and Outcomes of Falls among High Risk Community-Dwelling Older Adults." Injury Epidemiology 1 (2014). [CrossRef]
- Jørstad, E., K. Hauer, C. Becker, and S. Lamb. "Measuring the Psychological Outcomes of Falling: A Systematic Review." Journal of the American Geriatrics Society 53, no. 3 (2005): 501-10. [CrossRef]
- Schoene, D., C. Heller, Y. Aung, C. Sieber, W. Kemmler, and E. Freiberger. "A Systematic Review on the Influence of Fear of Falling on Quality of Life in Older People: Is There a Role for Falls?" Clinical Interventions in Aging 14 (2019): 701-19. [CrossRef]
- Hollinghurst, R., N. Williams, R. Pedrick-Case, L. North, S. Long, R. Fry, and J. Hollinghurst. "Annual Risk of Falls Resulting in Emergency Department and Hospital Attendances for Older People: An Observational Study of 781,081 Individuals Living in Wales (United Kingdom) Including Deprivation, Frailty and Dementia Diagnoses between 2010 and 2020." Age and Ageing 51, no. 8 (2022). [CrossRef]
- Public Health England. "Falls and Fracture Consensus Statement: Supporting Commissioning for Prevention." London, 2017.
- O'Cathain, A., E. Knowles, L. Bishop-Edwards, J. Coster, A. Crum, R. Jacques, C. James, R. Lawson, M. Marsh, R. O'Hara, A. Siriwardena, T. Stone, J. Turner, and J. Williams. "Understanding Variation in Ambulance Service Non-Conveyance Rates: A Mixed Methods Study." Health Services and Delivery Research 6, no. 19 (2018): 45. [CrossRef]
- Joint Royal Colleges Ambulance Liaison Committee (JRCALC), and Association of Ambulance Chief Executives (AACE). "Falls in Older Adults." In Jrcalc Clinical Guidelines. Bridgwater: Class Publishing Ltd, 2022.
- Dhalwani, N., R. Fahami, H. Sathanapally, S. Seidu, M. Davie, and K. Khunti. "Association between Polypharmacy and Falls in Older Adults: A Longitudinal Study from England." BMJ Open 16, no. 7 (2017). [CrossRef]
- Montero-Odasso, M., N. van der Velde, F. Martin, M. Petrovic, M. Tan, J. Ryg, S. Aguilar-Navarro, N. Alexander, C. Becker, H. Blain, R. Bourke, I. Cameron, R. Camicioli, L. Clemson, J. Close, K. Delbaere, L. Duan, G. Duque, S. Dyer, E. Freiberger, D. Ganz, F. Gómez, J. Hausdorff, D. Hogan, S. Hunter, J. Jauregui, N. Kamkar, R. Kenny, S. Lamb, N. Latham, L. Lipsitz, T. Liu-Ambrose, P. Logan, S. Lord, L. Mallet, D. Marsh, K. Milisen, R. Moctezuma-Gallegos, M. Morris, A. Nieuwboer, M. Perracini, F. Pieruccini-Faria, A. Pighills, C. Said, E. Sejdic, C. Sherrington, D. Skelton, S. Dsouza, M. Speechley, S. Stark, C. Todd, B. Troen, T. van der Cammen, J. Verghese, E. Vlaeyen, J. Watt, T. Masud, and the Task Force on Global Guidelines for Falls in Older Adults. "World Guidelines for Falls Prevention and Management for Older Adults: A Global Initiative." Age and Ageing 51, no. 9 (2022). [CrossRef]
- National Institute of Health and Care Excellence. "Falls: Assessment and Prevention in Older People and in People 50 and over at Higher Risk [Ng249]." 2025.
- Smith, H. "Role of Medicines Management in Preventing Falls in Older People." Nursing Older People (2022). [CrossRef]
- Crawford, P., R. Plumb, P. Burns, S. Flanagan, and C. Parsons. "A Quantitative Study on the Impact of a Community Falls Pharmacist Role, on Medicines Optimisation in Older People at Risk of Falls." BMC Geriatrics 24 (2024). [CrossRef]
- Curtin, D., E. Jennings, R. Daunt, S. Curtin, M. Randles, P. Gallagher, and D. O'Mahony. "Deprescribing in Older People Approaching End of Life: A Randomized Controlled Trial Using Stoppfrail Criteria." Journal of the American Geriatrics Society 68, no. 4 (2019): 762-69. [CrossRef]
- Marvin, V., E. Ward, A. Poots, K. Heard, A. Rajagopalan, and B. Jubraj. "Deprescribing Medicines in the Acute Setting to Reduce the Risk of Falls." European Journal of Hospital Pharmacy 24, no. 1 (2017): 10-15. [CrossRef]
- Wright, D., R. Holland, D. Alldred, C. Bond, C. Hughes, G. Barton, F. Poland, L. Shepstone, A. Arthur, L. Birt, J. Blacklock, A. Blyth, S. Cheilari, A. Daffu-O'Reilly, L. Dalgarno, D. Desborough, J. Ford, K. Grant, J. Gray, C. Handford, B. Harry, H. Hill, J. Inch, P. Myint, N. Norris, M. Spargo, V. Maskrey, D. Turner, L. Watts, and A. Zermansky. The Care Home Independent Pharmacist Prescriber Study (Chipps): Development and Implementation of an Rct to Estimate Safety, Effectiveness and Cost-Effectiveness, Programme Grants for Applied Research. Southampton: National Institute for Health and Care Research, 2023.
- Ming, Y., A. Zecevic, S. Hunter, W. Miao, and R. Tirona. "Medication Review in Preventing Older Adults’ Fall-Related Injury: A Systematic Review & Meta-Analysis." Canadian Geriatrics Journal 24, no. 3 (2021). [CrossRef]
- Zermansky, A., D. Alldred, D. Petty, D. Raynor, N. Freemantle, J. Eastaugh, and P. Bowie. "Clinical Medication Review by a Pharmacist of Elderly People Living in Care Homes—Randomised Controlled Trial." Age and Ageing 35, no. 6 (2006): 586-91. [CrossRef]
- Pit, S., J. Byles, D. Henry, L. Holt, V. Hansen, and D. Bowman. "A Quality Use of Medicines Program for General Practitioners and Older People: A Cluster Randomised Controlled Trial." Medical Journal of Australia 187, no. 1 (2007): 23-30. [CrossRef]
- Phelan, E., B. Williamson, B. Balderson, A. Cook, A. Piccorelli, M. Fujii, K. Nakata, V. Graham, M. Theis, J. Turner, C. Tannenbaum, and S. Gray. "Reducing Central Nervous System–Active Medications to Prevent Falls and Injuries among Older Adults: A Cluster Randomized Clinical Trial." JAMA Network Open 7, no. 7 (2024). [CrossRef]
- Seppala, L., N. Kamkar, E. van Poelgeest, K. Thomsen, J. Daams, J. Ryg, T. Masud, M. Montero-Odasso, S. Hartikainen, M. Petrovic, and N. van der Velde. "Medication Reviews and Deprescribing as a Single Intervention in Falls Prevention: A Systematic Review and Meta-Analysis." Age and Ageing 51, no. 9 (2022): afac191. [CrossRef]
- Gillespie, L., M. Robertson, W. Gillespie, C. Sherrington, S. Gates, L. Clemson, and S. Lamb. "Interventions for Preventing Falls in Older People Living in the Community." Cochrane Database of Systematic Reviews, no. 9 (2012). [CrossRef]
- Cameron, I., S. Dyer, C. Panagoda, G. Murray, K. Hill, R. Cumming, and N. Kerse. "Interventions for Preventing Falls in Older People in Care Facilities and Hospitals." Cochrane Database of Systematic Reviews, no. 9 (2018). [CrossRef]
- Almutairi, H., A. Stafford, C. Etherton-Beer, and L. Flicker. "Optimisation of Medications Used in Residential Aged Care Facilities: A Systematic Review and Meta-Analysis of Randomised Controlled Trials." BMC Geriatrics 20, no. 236 (2020). [CrossRef]
- Lee, J., A. Negm, R. Peters, E. Wong, and A. Holrbook. "Deprescribing Fall-Risk Increasing Drugs (Frids) for the Prevention of Falls and Fall-Related Complications: A Systematic Review and Meta-Analysis." BMJ Open 11, no. 2 (2021). [CrossRef]
- Acquisto, N., J. Cushman, A. Rice, and C. Edwards. "Collaboration by Emergency Medicine Pharmacists and Prehospital Services Providers." American Journal of Health-System Pharmacy 77, no. 12 (2020): 918-21. [CrossRef]
- Crockett, B., K. Jasiak, T. Walroth, K. Degenkolb, A. Stevens, and C. Jung. "Pharmacist Involvement in a Community Paramedicine Team." Journal of Pharmacy Science 30, no. 2 (2016): 223-28. [CrossRef]
- Hayball, P., R. Elliot, and S. Morris. "Ambulance Pharmacist – Why Haven't We Thought of This Role Earlier?" Pharmacy Practice and Research 45, no. 3 (2015): 318-21. [CrossRef]
- Ogrinc, G., L. Davies, D. Goodman, P. Batalden, F. Davidoff, and D. Stevens. "Squire 2.0 (Standards for Quality Improvement Reporting Excellence): Revised Publication Guidelines from a Detailed Consensus Process " BMJ Quality & Safety 25, no. 12 (2016): 986-92. [CrossRef]
- Sharma, A., N. T. Tran Minh Duc, T. Luu Lam Thang, N. Hai Nam, S. J. Ng, K. Said Abbas, N. Tien Huy, A. Marušić, C. L. Paul, J. Kwok, J. Karbwang, C. de Waure, F. J. Drummond, Y. Kizawa, E. Taal, J. Vermeulen, G. H. M. Lee, A. Gyedu, K. Gia To, M. L. Verra, É. M. Jacqz-Aigrain, W. K. G. Leclercq, S. T. Salminen, C. D. Sherbourne, B. Mintzes, S. Lozano, U. S. Tran, M. Matsui, and M. Karamouzian. "A Consensus-Based Checklist for Reporting of Survey Studies (Cross)." Journal of General Internal Medicine 36, no. 10 (2021): 3179-87. [CrossRef]
- PrescQIPP. "Care Homes - Medication and Falls." 4-8, 2014.
- Agresti, A. Analysis of Ordinal Categorical Data. 2nd ed, Wiley Series in Probability and Statistics. Hoboken: Wiley, 2010.
- Harrell, F. Regression Modeling Strategies: With Application to Linear Models Logistic Regression, and Survival Analysis, Springer Series in Statistics. New York: Springer-Verlag, 2001.
- Julious, S., M. Campbell, and D. Altman. "Estimating Sample Sizes for Continuous, Binary, and Ordinal Outcomes in Paired Comparisons: Practical Hints." Journal of Biopharmaceutical Statistics 9, no. 2 (1999): 241-51. [CrossRef]
- Nymoen, L., T. Flatebø, T. Moger, E. Øie, E. Molden, and K. Viktil. "Impact of Systematic Medication Review in Emergency Department on Patients' Post-Discharge Outcomes - a Randomised Controlled Clinical Trial." PLoS ONE 17, no. 9 (2022). [CrossRef]
- Mikolaizak, A., S. Lord, A. Tiedeman, P. Simpson, G. Caplan, J. Bendall, K. Howard, L. Webster, N. Payne, S. Hamilton, J. Lo, E. Ramsay, S. O'Rourke, L. Roylance, and J. Close. "A Multidisciplinary Intervention to Prevent Subsequent Falls and Halth Service Use Following Fall-Related Paramedic Care: A Randomised Controlled Trial." Age and Ageing 46 (2017): 200-08. [CrossRef]
- Al Bulushi, S., T. McIntosh, A. Grant, D. Stewart, and S. Cunningham. "Implementation Frameworks for Polypharmacy Management within Healthcare Organisations: A Scoping Review." International Journal of Clinical Pharmacy 45 (2023): 343-54. [CrossRef]
- Seppala, L., E. van de Glind, J. Daams, K. Ploegmakers, M. de Vries, A. Wermelink, and N. van der Velde. "Fall-Risk-Increasing Drugs: A Systematic Review and Meta-Analysis: Iii. Others." Journal of the American Medical Directors Association 19, no. 4 (2018): 372e.1-72.e8. [CrossRef]
- Seppala, L., M. Petrovic, J. Ryg, G. Bahat, E. Topinkova, K. Szczerbińska, T. van der Cammen, S. Hartikainen, B. Ilhan, F. Landi, Y. Morrissey, A. Mair, M. Gutiérrez-Valencia, M. Emmelot-Vonk, M. Mora, M. Denkinger, P. Crome, S. Jackson, A. Correa-Pérez, W. Knol, G. Soulis, A. Gudmundsson, G. Ziere, M. Wehling, D. O'Mahony, A. Cherubini, and N. van der Velde. "Stoppfall (Screening Tool of Older Persons Prescriptions in Older Adults with High Fall Risk): A Delphi Study by the Eugms Task and Finish Group on Fall-Risk-Increasing Drugs." Age and Ageing 50, no. 4 (2021): 1189-99. [CrossRef]
- Alićehajić-Bečić, Ð., and H. Smith. "Medicines and Falls." National Falls Prevention Coordination Group, 2023.
- Campbell, A., M. Robertson, M. Gardner, R. Norton, and D. Buchner. "Psychotropic Medication Withdrawal and a Home-Based Exercise Program to Prevent Falls: A Randomized, Controlled Trial." Journal of the American Geriatrics Society 47, no. 7 (2015): 850-53.
- Hindi, A., E. Schafheutle, and S. Jacobs. "Patient and Public Perspectives of Community Pharmacies in the United Kingdom: A Systematic Review." Health Expectations 21, no. 2 (2017): 409-28. [CrossRef]
- Chopra, E., T. Choudhary, A. Hazen, S. Shrestha, I. Dehele, and V. Paudyal. "Clinical Pharmacists in Primary Care General Practices: Evaluation of Current Workforce and Their Distribution." Journal of Pharmaceutical Policy and Practice 15, no. 101 (2022). [CrossRef]
- NHS England. "Structured Medication Reviews and Medicines Optimisation: Guidance." In Network Contract Directed Enhanced Service, 2021.
- Bonner, M., M. Capsey, and J. Batey. "A Paramedic's Role in Reducing Number of Falls and Fall-Related Emergency Service Use by over 65s: A Systematic Review." British Paramedic Journal 6, no. 1 (2021): 46-52. [CrossRef]
- Shaya, F., V. Chirikov, C. Rochester, R. Zaghab, and K. Kucharski. "Impact of a Comprehensive Pharmacist Medication-Therapy Management Service." Journal of Medical Economics 18, no. 10 (2015): 828-37. [CrossRef]
- Siddle, J., P. Pang, C. Weaver, E. Weinstein, D. O'Donnell, T. Arkins, and C. Miramonti. "Mobile Integrated Health to Reduce Post-Discharge Acute Care Visits: A Pilot Study." The American Journal of Emergency Medicine 36, no. 5 (2018): 843-45. [CrossRef]
- Graabæk, T., U. Hedegaard, M. Christensen, M. Clemmensen, T. Knudsen, and L. Aagaard. "Effect of a Medicines Management Model on Medication-Related Readmissions in Older Patients Admitted to a Medical Acute Admission Unit—a Randomized Controlled Trial." 25 (2019): 88-96. [CrossRef]
- Kitchen, S., K. McGrail, M. Wickham, M. Law, and C. Hohl. "Emergency Department-Based Medication Review on Outpatient Health Services Utilization: Interrupted Time Series." BMC Health Services Research 20 (2020): 254. [CrossRef]
- Santolaya-Perrín, R., B. Calderón-Hernanz, G. Jiménez-Díaz, N. Galán-Ramos, M. Moreno-Carvajal, J. Rodríguez-Camacho, P. Serra-Simó, J. García-Ortiz, J. Tarradas-Torras, A. Ginés-Palomares, and I. Sánchez-Navarro. "The Efficacy of a Medication Review Programme Conducted in an Emergency Department." International Journal of Clinical Pharmacy 41 (2019): 757-66. [CrossRef]
- De Oliveira, G., L. Castro-Alves, M. Kendall, and R. McCarthy. "Effectiveness of Pharmacist Intervention to Reduce Medication Errors and Health-Care Resources Utilization after Transitions of Care: A Meta-Analysis of Randomized Controlled Trials." Journal of Patient Safety 17, no. 5 (2021): 375-80. [CrossRef]
- Gillespie, U., A. Alassaad, D. Henrohn, H. Garmo, M. Hammarlund-Udenaes, H. Toss, Å. Kettis-Lindblad, H. Melhus, and C. Mörlin. "A Comprehensive Pharmacist Intervention to Reduce Morbidity in Patients 80 Years or Older - a Randomized Controlled Trial." JAMA Internal Medicine 169, no. 9 (2009): 894-900. [CrossRef]
- Hawes, E., W. Maxwell, S. White, J. Mangun, and F. Lin. "Impact of an Outpatient Pharmacist Intervention on Medication Discrepancies and Health Care Resource Utilization in Posthospitalization Care Transitions." Journal of Primary Care & Community Health 5, no. 1 (2013): 14-18. [CrossRef]
- Phatak, A., R. Prusi, B. Ward, L. Hansen, M. Williams, E. Vetter, N. Chapman, and M. Postelnick. "Impact of Pharmacist Involvement in the Transitional Care of High-Risk Patients through Medication Reconciliation, Medication Education, and Postdischarge Call-Backs (Ipitch Study)." Journal of Hospital Medicine 11 (2015): 39-44.
- McCahon, D., P. Duncan, R. Payne, and J. Horwood. "Patient Perceptions and Experiences of Medication Review: Qualitative Study in General Practice." BMC Primary Care 23 (2022). [CrossRef]
- Peters, A., D. Lim, and N. Naidoo. "Down with Falls! Paramedicine Scope Regarding Falls Amongst Older Adults in Rural and Remote Communiies: A Scoping Review." Austrailian Journal of Rural Health 31 (2023): 605-16. [CrossRef]
- Health Innovation Network. "Resources to Support Patients Having a Structured Medication Review." https://thehealthinnovationnetwork.co.uk/programmes/medicines/polypharmacy/patient-information/ (.
- Health Innovation Yorkshire & Humber. "Resources to Tackle Polypharmacy." Available online: https://www.healthinnovationyh.org.uk/resources-to-tackle-polypharmacy/ (accessed on 3rd June 2025).
- Hertig, R., R. Ackerman, B. Zagar, and S. Tart. "Pharmacy Student Involvement in a Transition of Care Program." Currents in Pharmacy Teaching and Learning 9, no. 5 (2017): 841-47. [CrossRef]
- Association of Ambulance Chief Executives (AACE), and Joint Royal Colleges Ambulance Liaison Committee (JRCALC). Jrcalc Clinical Guidelines. Bridgwater: Class Professional Publishing, 2022.
- Eccles, M., S. Hrisos, J. Francis, E. Kaner, H. Dickinson, F. Beyer, and M. Johnston. "Do Self- Reported Intentions Predict Clinicians' Behaviour: A Systematic Review." Implementation Science 1 (2006): 28. [CrossRef]
- Hrisos, S., M. Eccles, J. Francis, H. Dickinson, E. Kaner, F. Beyer, and M. Johnston. "Are There Valid Proxy Measures of Clinical Behaviour? A Systematic Review." Implementation Science 4 (2009): 37. [CrossRef]
Table 2.
Objectives and measures.
| Objective | Measure | |
| Referral Rate, Suitability, and Clinical Impact | 1 | Referral rates |
| 2 | Referral appropriateness | |
| 3 | Fall and/or ambulance recurrence | |
|
Medicine Optimisation |
4 | Polypharmacy reduction. |
| 5 | Deprescribing of fall-risk medicines as per PrescQIPP [30] (Table S3) | |
| Patient Experiences | 6 | Change in emotions about their medicines post-review |
| 7 | Impact of specific review activities on emotions | |
|
Ambulance Staff Perceptions |
8 | Key indicators of medicine management difficulty |
| 9 | Perceived frequency of such cases | |
| 10 | Perceived value of pharmacist referral | |
| 11 | Influence of clinician demographics on referral value perception | |
Table 3.
Summary of cases referred to the medicine review pathway.
| Case Demographic |
All referred n = 775 |
Received medicine review n = 340 (43.9%) |
Did not receive medicine review n = 435 (56.1%) |
| Age median (interquartile range) | 84 (77–89) | 84 (77–89) | 84 (77–90) |
| Patient fallen in last 12 months | |||
| Yes | 573 (73.9%) | 243 (71.5%) | 330 (75.9%) |
| No | 159 (20.5%) | 79 (23.2%) | 80 (18.4%) |
| Not recorded | 43 (5.6%) | 18 (5.3%) | 25 (5.7%) |
| Patient prescribed ≥4 medicines | 597 (77.0%) | 264 (77.6%) | 333 (76.6%) |
| Ambulance crew concerned about medicines | 173 (22.3%) | 64 (18.8%) | 109 (25.1%) |
| Time from referral to initial review decision median days (interquartile range) | 10 (4–27) | 9 (3–21) | 28 (10–109) |
Table 4.
Demographics of reviewed patients.
| Case Demographic | Value |
| Frailty n (%) | |
| Severe | 86 (25.3%) |
| Moderate | 106 (31.2%) |
| Mild | 6 (1.8%) |
| Not frail | 128 (37.6%) |
| Not recorded | 14 (4.1%) |
| Pharmacist review type n (%) | |
| Face-to-face | 7 (2.1%) |
| Telephone | 77 (22.6%) |
| Notes based | 125 (36.8%) |
| Not recorded | 131 (38.5%) |
| Referral considered appropriate n (%) | |
| Yes | 263 (77.4%) |
| No | 67 (19.7%) |
| Not recorded | 10 (2.9%) |
Table 5.
Summary of changes to medicine during review.
| Proforma Field | Value |
| Number of medicines median (interquartile range) | |
| Prior to review | 9 (6–12) |
| After review | 9 (6–12) |
| Stopped by pharmacist | 0 (0–0) |
| Changes recommended by pharmacists n (%) | 149 (43.8%) |
| Pharmacist categorisation of medicine fall risk as per PrescQIPP n (%) | |
| Yes | 76 (22.2%) |
| High risk | 43 (12.6%) |
| Medium risk | 11 (3.2%) |
| Possible risk | 13 (3.8%) |
| Risk present but level not recorded | 9 (2.6%) |
| No | 51 (15.0%) |
| Not recorded | 213 (62.6%) |
Table 6.
Demographic summary of patient experience survey.
| Survey Question | Result |
| Age mean (standard deviation) | 83.59 (9.99) |
| Gender n (%) | |
| Male | 26 (54.2%) |
| Female | 21 (43.8%) |
| N/A | 1 (2.1%) |
| Ethnic group n (%) | |
| Asian/Asian British Indian | 1 (2.1%) |
| White British | 44 (91.7%) |
| White Irish | 2 (4.2%) |
| N/A | 1 (2.1%) |
| How many medicines were you taking? n (%) | |
| 0 | 1 (2.1%) |
| 1 to 4 | 14 (29.2%) |
| 5 or more | 30 (62.5%) |
| Don’t know | 1 (2.1%) |
| N/A | 2 (4.2%) |
| How was your medicines review undertaken? n (%) | |
| Face-to-face | 15 (31.2%) |
| Telephone | 13 (27.1%) |
| Don’t know | 14 (29.2%) |
| N/A | 6 (12.5%) |
Table 7.
Reported patient emotions before and after review.
| Reported emotion before review (n) | Reported emotion after review (n) | ||
| Negative | Neutral | Positive | |
| Negative | 2 | 3 | 4 |
| Neutral | 0 | 23 | 0 |
| Positive | 0 | 1 | 5 |
Table 8.
Ambulance healthcare professional survey results summary.
| Question |
Overall n (%) |
Referred n (%) |
Not referred n (%) |
| Total responses | 146 (100%) | 18 (12.3%) | 128 (87.7%) |
| Respondent role | |||
| Advanced Paramedic | 7 (4.8%) | 0 (0%) | 7 (5.5%) |
| Emergency Care Assistant | 21 (14.4%) | 1 (5.6%) | 20 (15.6%) |
| Emergency Medical Technician | 9 (6.2%) | 3 (16.7%) | 6 (4.7%) |
| Manager | 13 (8.9%) | 1 (5.6%) | 12 (9.4%) |
| Newly Qualified Paramedic | 21 (14.4%) | 1 (5.6%) | 20 (15.6%) |
| Paramedic | 65 (44.5%) | 11 (61.1%) | 54 (42.2%) |
| Specialist Paramedic | 6 (4.1%) | 1 (5.6%) | 5 (3.9%) |
| Student Paramedic | 4 (2.7%) | 0 (0%) | 4 (3.1%) |
| Working arrangement | |||
| Full-time (37.5 hours a week) | 112 (76.7%) | 16 (88.9%) | 96 (75.0%) |
| Part-time (including bank) | 34 (23.3%) | 2 (11.1%) | 32 (25.0%) |
| How frequently do you attend an incident involving a patient over the age 65 years who has fallen, on average? | |||
| More than once a shift | 55 (37.7%) | 8 (44.4%) | 47 (36.7%) |
| Once a shift | 63 (43.2%) | 8 (44.4%) | 55 (43.0%) |
| Once a week | 12 (8.2%) | 1 (5.6%) | 11 (8.6%) |
| Once a month | 16 (11.0%) | 1 (5.6%) | 15 (11.7%) |
| Have you or your crewmate referred a patient to a pharmacist for a community medicine review? | |||
| Yes | 18 (12.3%) | 18 (100%) | 0 (0%) |
| No, and work in the study area | 22 (15.1%) | 0 (0%) | 22 (17.2%) |
| No, but do not work in the study area | 102 (69.9%) | 0 (0%) | 102 (79.7%) |
| Unsure | 4 (2.7%) | 0 (0%) | 4 (3.1%) |
| How important do you feel it is to have the option to refer patients who have fallen and who are taking multiple medicines, to a community pharmacist for review? | |||
| Very important | 79 (54.1%) | 12 (66.7%) | 67 (52.3%) |
| Important | 46 (31.5%) | 4 (22.2%) | 42 (32.8%) |
| Neutral | 16 (11.0%) | 1 (5.6%) | 15 (11.7%) |
| Unimportant | 2 (1.4%) | 0 (0%) | 2 (1.6%) |
| Very unimportant | 1 (0.7%) | 0 (0%) | 1 (0.8%) |
| N/A | 2 (1.4%) | 1 (5.6%) | 1 (0.8%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



